

Abstract
Background/Aim:
To provide the most recent estimate of childhood obesity and determine the trend in childhood obesity in Riyadh city over the past two decades, by comparing our results with previous studies that published data comparable to our study in terms of geography, sample age (6–16 years), and use of World Health Organization (WHO) cut-offs to define obesity.
Patients and Methods:
A cross-sectional study was conducted in 2015 among school children in Riyadh city. A sample of 7930 children (67% girls) aged 6–16 years were randomly selected. Body mass index for age and gender above +1 and below +2 standard deviation scores (SDS) defined overweight (SDS, z-scores) and >+2 SD scores defined obesity.
Results:
The overall prevalence of overweight and obesity was 13.4% (14.2% for girls and 12% for boys; P= 0.02) and 18.2% (18% for girls and 18.4% for boys; P = 0.73), respectively. When compared with the WHO-based national prevalence rate of obesity reported in 2004 (≈9.3%), the obesity rate has doubled over a 10-year period. There was a significantly higher prevalence of obesity in adolescents (>11 years) than in children (20.2% vs 15.7%; P < 0.01). Overweight and obesity increased significantly with higher levels of socioeconomic status. Obese children were at 1.5 and 2 times risk of developing gas bloating and vomiting than non-obese children.
Conclusion:
The prevalence of overweight and obesity has risen alarmingly among Saudi children and adolescents over the past decade and should make a strong case to initiate and monitor effective implementation of obesity prevention measures.
Keywords: Adolescents, children, obesity, overweight, Saudi Arabia
INTRODUCTION
Overweight and obesity correlate significantly with increased risk of comorbidities such as metabolic syndrome, type 2 diabetes, cardiovascular diseases, fatty liver diseases, psychological disturbance, and premature death.[1,2,3,4] This has prompted the World Health Organization (WHO) to consider obesity as one of the most important public-health threats for children.[5] In 2015, a total of 107.7 million children and 603.7 million adults were obese indicating that the prevalence of obesity has doubled since 1980.[6]
Obesity and socioeconomic status (SES) have been consistently related worldwide.[7] Over the past 30 years, Saudi Arabia has witnessed significant economic prosperity and lifestyle changes including sedentary life style and dietary habits that have led to increase in obesity prevalence among children and adults. Several studies reported on the prevalence of pediatric obesity in Saudi Arabia; however, the majority are old and very few studies reported on the trends in the prevalence of obesity among children and adolescents. Also, the variability in the type of cut-offs used to define obesity in these studies (WHO vs International Obesity Task Force vs Center for Disease Control) limits the comparison between these studies. The release of the WHO child growth references for ages 5–19 years in 2007, based on selected multinational samples of children, provided a better standard for comparison between and within countries.[8]
Because of their public health importance, up-to-date information on prevalence and monitoring of trends in childhood obesity is crucial for developing and evaluating success of interventions for prevention of obesity in any country. The purpose of this study was to provide the most recent estimate of childhood obesity and determine the trend in childhood obesity in Riyadh city over the past two decades by comparing our results with previous studies that published data comparable to our study in terms of geography, sample age (6–16 years), and use of WHO cut-offs to define obesity. Furthermore, we investigated the effect of parental SES on obesity rate and whether obesity is associated with gastrointestinal (GI) symptoms.
PATIENTS AND METHODS
Study design and setting
The study was a cross-sectional population-based study to measure the weight, height, and body mass index (BMI) of healthy asymptomatic school-aged Saudi children (age 6–16 years) of both sexes, attending primary and intermediate schools in Riyadh, in 2015.
Study population
The details of the methodology of the celiac mass screening study, from which the study population for this study was recruited, is described elsewhere.[9] In brief, a total of 104 schools (61 primary schools and 43 intermediate schools; 53 male schools and 51 female schools) were randomly selected from the five “administrative” geographic regions of Riyadh city (North, South, East, West, and Center) using probability proportionate sampling procedure. Parents of 10,046 students have signed the informed consents and accepted to participate in the study; however, 7931 students (mean age 11.22 ± 2.62 years) provided complete data for the analysis.
Study procedures
-
Anthropometric measurements
The weight and height of the participants were measured in the school by a trained team of doctors and nurses. Weight was measured with the students wearing light clothing and no shoes, using an electronic scale to the nearest 100 g. Height was measured using a wall-mounted stadiometer, with the children not wearing shoes. The measurements were recorded to the nearest 0.1 cm. BMI was calculated as the ratio of weight (kg) to the square of height (m).
-
Data collection
A health advocator in each school distributed envelopes to all students. Each envelop contained the following: (1) an informed consent form and (2) a survey to collect data on demographics and SES. All students whose parents signed the informed consent underwent measurement of growth parameters. The parental SES was measured by collecting data on four main indicators: parents' educational level, family income, habitation, and parents' jobs. We have used a point scale of 1–20 as follows: educational level, 6 points; family income monthly, 6 points; type of residence, 4 points; type of work, 4 points. In the Saudi community, we believe that the middle SES is more wider than the lower or high SES; therefore, we subcategorized the middle class into low middle and high middle class. An overall score of ≤5 from a maximum of 20 defined the low SES, 6–10 as low middle SES, 11–15 as high middle SES, and >15 as high SES. Participants were categorized into six educational levels: postgraduate degree (6 points), university graduate (5 points), high school graduate (4 points), intermediate school graduate (3 points), primary school graduate (2 points), and illiterate (1 point). Monthly family income was graded as following: >8000 US $ (6 points), 5000–8000 US $ (5 points), 2500–5000 US $ (4 points), 1500–2500 US $ (3 points), <1500 US $ (2 points), and no income (1 point). The habitation was categorized into four types: palace (4 points), villa (3 points), apartment (2 points), and small traditional house (1 point). Occupation of parents was classified as follows: trader/business man/professional (4 points), office clerk (3 points), worker (2 points), and unemployed (1 point). The term “professional” referred to a job that required a high educational degree (like bachelor's/master's degree, or PhD). “Worker” referred to a working-class person who performs service-oriented work or manual labor while office clerk referred to an administrative desk job. We have considered the higher income occupation to refer to the occupation of parents regardless of whether it is for the father or mother.
Definitions
Obesity and overweight were defined using the WHO 2007 growth standards.[8] BMI for age and gender above +1 and below +2 SDS defined overweight (standard deviation scores [SDS], z-scores) and >+2 SDS defined obesity. z-Scores of weight, height, and BMI for students aged 5–18 years were determined using the WHO AnthroPlus software.[10]
Ethical considerations
This study was approved by the institutional review board (no. 11-066) and the Ministry of Education in Saudi Arabia. All study participants, or their legal guardians, provided informed written consent prior to study enrollment.
Statistical analysis
Categorical variables such as gender, age groups, region, and SES are presented in frequencies and percentages, whereas continuous variables such as age and socioeconomic score are expressed as mean ± SD. Independent sample t-test was used to determine the mean significant differences between categorical variables and other continuous variables. Chi-square/Fisher's exact test was applied based on whether the cell expected frequency is smaller than 5, and it was applied to determine the significant association between categorical variables. Binary logistic regression was applied to find out significant predictor/risk factor among categorical variables and study variables. P value <0.05 two-tailed was considered as statistically significant. Multivariate analysis using binary logistic regression was conducted to determine factors associated with overweight and obesity. All data were entered and analyzed through statistical package SPSS version 25 (SPSS Inc., Chicago, IL, USA).
RESULTS
Participants' characteristics
Table 1 shows the general characteristics of the 7931 participants (67% girls). A majority of the participants belong to families in the middle socioeconomic class (87%) and only a minority belong to low (4.1%) and high socioeconomic class (8.9%).
Table 1.
General characteristics of the 7931 students
| Age (years) | Median 11 (range, 5-18) | Mean 11.22±2.62 |
|---|---|---|
| Gender | Male | 2943 (37%) |
| Female | 4988 (63%) | |
| Father’s education no data=130 (1.6%) | Illiterate | 582 (7.3%) |
| Primary | 1157 (14.6%) | |
| Intermediate | 1241 (15.6%) | |
| High school | 2326 (29.3%) | |
| Bachelors | 1992 (25.1%) | |
| Master’s/doctorate | 502 (6.3%) | |
| Mother’s education no data=135 (1.7%) | Illiterate | 1003 (12.6%) |
| Primary | 1361 (17.2%) | |
| Intermediate | 1308 (16.5%) | |
| High school | 1963 (24.8%) | |
| Bachelors | 2060 (26.0%) | |
| Master’s/doctorate | 1003 (12.6%) | |
| Family income no data=374 (4.7%) | No income | 407 (5.1%) |
| <1500 US $ | 1549 (19.5%) | |
| 1500–2500 US $ | 2277 (28.7%) | |
| 2500–5000 US $ | 2218 (28.0%) | |
| 5000–8000 US $ | 719 (9.1%) | |
| >8000 US $ | 386 (4.9%) | |
| Occupation | Unemployed | 2117 (26.7%) |
| Worker | 4567 (57.6%) | |
| Office clerk | 693 (8.7%) | |
| Trader/professional | 553 (7.0%) | |
| Residence No data=126 (1.6%) | Traditional house | 1067 (13.5%) |
| Apartment | 2592 (32.7%) | |
| Villa | 4107 (51.8%) | |
| Palace | 38 (0.5%) | |
| Socioeconomic status | Low socioeconomic | 328 (4.1%) |
| Lower middle socioeconomic | 2581 (32.5%) | |
| Higher middle socioeconomic | 4317 (54.4%) | |
| High socioeconomic | 705 (8.9%) |
Anthropometric measurements
The overall prevalence of overweight and obesity was 13.4% (14.2% for girls and 12% for boys; P = 0.02) and 18.2% (18% for girls and 18.4% for boys; P = 0.73), respectively. The prevalence rates of overweight and obesity based on age [pediatric group (6–11 years) vs adolescent group (>11 years)] are shown in Figure 1. There was a significantly higher prevalence of obesity in adolescents than in children (20.2% vs 15.7%; P < 0.01). In addition, there was a significantly higher prevalence of overweight (14.6% vs 12%; P < 0.03) in adolescents than in children. Females appeared to be more overweight than males (14.2% vs 12%; P < 0.02) [Table 2]. Overall, there was no sex difference between obese males and females (18.4% vs 18%; P = 0.74) [Table 3]; however, on subgroup analysis, adolescent boys were more obese than adolescent girls (55.9% vs 50.1%; P = 0.031) [Table 4].
Figure 1.
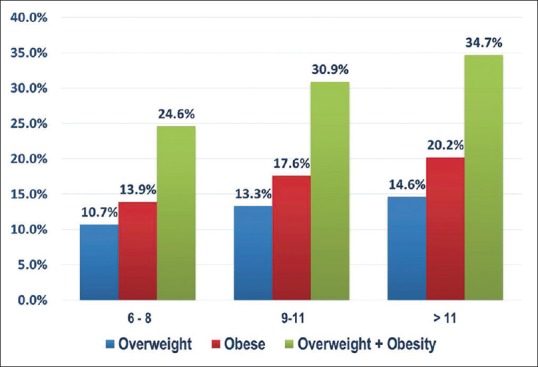
Prevalence of overweight and obesity based on age group
Table 2.
Comparison of overweight group versus normal body mass index group
| Total sample size 7931 | Overweight group 1065 (13.4%) | Normal BMI group=5153 (65%) | OR (95% CI) | P | |
|---|---|---|---|---|---|
| Age (years) | Age (mean±SD) | 11.48±2.48 | 11.11±2.64 | 0.929 (0.908-0.951) | <0.001* |
| Gender | Male (2943) (12%) | 355 (33.3%) | 1909 (37.0%) | 0.85 (0.739-0.977) | 0.022* |
| Female (4987) (14.2%) | 710 (66.7%) | 3244 (63.0%) | |||
| Father’s education | Illiterate | 69 (6.5%) | 395 (7.7%) | 0.83 (0.64-1.087) | 0.180 |
| Primary | 132 (12.4%) | 784 (15.2%) | 0.79 (0.647-0.961) | 0.018* | |
| Intermediate | 162 (15.2%) | 826 (16.0%) | 0.94 (0.783-1.129) | 0.506 | |
| High school | 312 (29.3%) | 1483 (28.8%) | 1.03 (0.887-1.185) | 0.735 | |
| Bachelors | 292 (27.4%) | 1263 (24.5%) | 1.16 (1.003-1.35) | 0.046* | |
| Master’s/doctorate | 82 (7.7%) | 317 (6.2%) | 1.27 (0.989-1.638) | 0.061 | |
| Mother’s education | Illiterate | 117 (11.0%) | 711 (13.8%) | 0.77 (0.626-0.949) | 0.014* |
| Primary | 158 (14.8%) | 919 (17.8%) | 0.8 (0.668-0.964) | 0.019* | |
| Intermediate | 185 (17.4%) | 855 (16.6%) | 1.06 (0.887-1.259) | 0.535 | |
| High school | 273 (25.6%) | 1214 (23.6%) | 1.12 (0.961-1.302) | 0.148 | |
| Bachelors | 296 (27.8%) | 1307 (25.4%) | 1.13 (0.977-1.313) | 0.099 | |
| Master’s/doctorate | 15 (1.4%) | 62 (1.2%) | 1.17 (0.665-2.07) | 0.581 | |
| Family income | No income | 50 (4.7%) | 253 (4.9%) | 0.95 (0.699-1.302) | 0.767 |
| <1500 US $ | 187 (17.6%) | 1062 (20.6%) | 0.82 (0.691-0.974) | 0.024* | |
| 1500–2500 US $ | 303 (28.5%) | 1516 (29.4%) | 0.95 (0.824-1.104) | 0.527 | |
| 2500–5000 US $ | 330 (31.0%) | 1387 (26.9%) | 1.22 (1.056-1.408) | 0.007* | |
| 5000–8000 US $ | 85 (8.0%) | 452 (8.8%) | 0.9 (0.708-1.149) | 0.403 | |
| >8000 US $ | 64 (6.0%) | 229 (4.4%) | 1.37 (1.033-1.829) | 0.028* | |
| Occupation | Unemployed | 270 (25.4%) | 1414 (27.4%) | 0.9 (0.772-1.044) | 0.163 |
| Worker | 615 (57.7%) | 2973 (57.7%) | 1 (0.877-1.145) | 0.975 | |
| Office clerk | 93 (8.7%) | 436 (8.5%) | 1.04 (0.819-1.308) | 0.773 | |
| Trader/professional | 87 (8.2%) | 329 (6.4%) | 1.3 (1.02-1.668) | 0.034 | |
| Residence | Traditional house | 129 (12.1%) | 721 (14.0%) | 0.85 (0.693-1.035) | 0.104 |
| Apartment | 322 (30.2%) | 1772 (34.4%) | 0.83 (0.717-0.954) | 0.009* | |
| Villa | 587 (55.1%) | 2559 (49.7%) | 1.24 (1.09-1.421) | 0.001* | |
| Palace | 7 (0.7%) | 21 (0.4%) | 1.62 (0.686-3.813) | 0.268 | |
| SES | Low SES | 37 (3.5%) | 211 (4.1%) | 0.84 (0.591-1.203) | 0.364 |
| Lower middle SES | 311 (29.2%) | 1774 (34.4%) | 0.79 (0.68-0.907) | 0.001* | |
| Higher middle SES | 615 (57.7%) | 2737 (53.1%) | 1.21 (1.056-1.378) | 0.006* | |
| High SES | 102 (9.6%) | 430 (8.3%) | 1.16 (0.927-1.459) | 0.190 | |
| Socioeconomic score | 11.70±3.22 | 11.29±3.26 | 0.948 (0.931-0.965) | <0.001* | |
| Abdominal distension | 85 (8.0%) | 330 (6.4%) | 1.267 (0.989-1.624) | 0.060 | |
| Diarrhea | 59 (5.5%) | 307 (6.0%) | 0.925 (0.695-1.233) | 0.598 | |
| Constipation | 91 (8.5%) | 525 (10.2%) | 0.823 (0.652-1.039) | 0.102 | |
| Abdominal pain | 265 (24.9%) | 1346 (26.1%) | 0.936 (0.804-1.090) | 0.401 | |
| Vomiting | 49 (4.6%) | 241 (4.7%) | 0.983 (0.717-1.346) | 0.915 | |
*Statistically significant result. BMI: Body mass index, OR: Odds ratio, CI: Confidence interval, SD: Standard deviation, SES: Socioeconomic status
Table 3.
Comparison of obese group versus normal BMI group
| Variables | Obese group=1439 (18%) | Normal BMI group=5153 (65%) | OR (95% CI) | P | |
|---|---|---|---|---|---|
| Age | Age (mean±SD) | 11.52±2.529 | 11.1±2.64 | 0.927 (0.906-0.949) | <0.001* |
| Gender | Male (2943) (18.4%) | 540 (37.5%) | 1909 (37.0%) | 1.02 (0.905-1.152) | 0.739 |
| Female (4987) (18%) | 899 (62.5%) | 3244 (63.0%) | |||
| Father’s education | Illiterate | 90 (6.3%) | 395 (7.7%) | 0.8 (0.634-1.018) | 0.070 |
| Primary | 201 (14.0%) | 784 (15.2%) | 0.9 (0.765-1.07) | 0.241 | |
| Intermediate | 213 (14.8%) | 826 (16.0%) | 0.91 (0.773-1.072) | 0.259 | |
| High school | 439 (30.5%) | 1483 (28.8%) | 1.09 (0.956-1.234) | 0.202 | |
| Bachelors | 379 (26.3%) | 1263 (24.5%) | 1.1 (0.964-1.258) | 0.156 | |
| Master’s/doctorate | 91 (6.3%) | 317 (6.2%) | 1.03 (0.809-1.31) | 0.811 | |
| Mother’s education | Illiterate | 137 (9.5%) | 711 (13.8%) | 0.66 (0.542-0.797) | <0.001 |
| Primary | 228 (15.8%) | 919 (17.8%) | 0.87 (0.74-1.016) | 0.078 | |
| Intermediate | 226 (15.7%) | 855 (16.6%) | 0.94 (0.798-1.099) | 0.422 | |
| High school | 405 (28.1%) | 1214 (23.6%) | 1.27 (1.114-1.45) | <0.001 | |
| Bachelors | 393 (27.3%) | 1307 (25.4%) | 1.11 (0.969-1.261) | 0.136 | |
| Master’s/doctorate | 21 (1.5%) | 62 (1.2%) | 1.22 (0.739-2.002) | 0.441 | |
| Family income | No income | 84 (5.8%) | a253 (4.9%) | 1.2 (0.931-1.548) | 0.158 |
| <1500 US $ | 247 (17.2%) | 1062 (20.6%) | 0.8 (0.685-0.93) | 0.004* | |
| 1500–2500 US $ | 368 (25.6%) | 1516 (29.4%) | 0.82 (0.722-0.941) | 0.004* | |
| 2500–5000 US $ | 432 (30.0%) | 1387 (26.9%) | 1.16 (1.024-1.324) | 0.020* | |
| 5000–8000 US $ | 164 (11.4%) | 452 (8.8%) | 1.34 (1.107-1.616) | 0.002* | |
| >8000 US $ | 80 (5.6%) | 229 (4.4%) | 1.27 (0.974-1.644) | 0.077 | |
| Occupation | Unemployed | 360 (25.0%) | 1414 (27.4%) | 0.88 (0.772-1.009) | 0.067 |
| Worker | 811 (56.4%) | 2973 (57.7%) | 0.95 (0.842-1.065) | 0.365 | |
| Office clerk | 139 (9.7%) | 436 (8.5%) | 1.16 (0.947-1.414) | 0.154 | |
| Trader/professional | 129 (9.0%) | 329 (6.4%) | 1.44 (1.167-1.786) | 0.001* | |
| Residence | Traditional house | 180 (12.5%) | 721 (14.0%) | 0.88 (0.738-1.047) | 0.148 |
| Apartment | 392 (27.2%) | 1772 (34.4%) | 0.71 (0.628-0.813) | <0.001* | |
| Villa | 832 (57.8%) | 2559 (49.7%) | 1.39 (1.235-1.563) | <0.001* | |
| Palace | 10 (0.7%) | 21 (0.4%) | 1.71 (0.804-3.64) | 0.159 | |
| SES | Low SES | 71 (4.9%) | 211 (4.1%) | 1.22 (0.923-1.601) | 0.164 |
| Lower middle SES | 392 (27.2%) | 1774 (34.4%) | 0.71 (0.627-0.812) | 0.001* | |
| Higher middle SES | 820 (57.0%) | 2737 (53.1%) | 1.17 (1.039-1.316) | 0.009* | |
| High SES | 156 (10.8%) | 430 (8.3%) | 1.34 (1.101-1.62) | 0.003* | |
| Socioeconomic score | 11.76±3.388 | 11.29±3.25 | 0.957 (0.940-0.974) | <0.001* | |
| Consanguinity | 493 (34.3%) | 1987 (38.6%) | 0.83 (0.735-0.939) | 0.003* | |
| Abdominal distension | 172 (12.0%) | 330 (6.4%) | 1.981 (1.633-2.409) | <0.001* | |
| Diarrhea | 91 (6.3%) | 307 (6.0%) | 1.065 (0.836-1.356) | 0.606 | |
| Constipation | 121 (8.4%) | 525 (10.2%) | 0.809 (0.658-0.995) | 0.045* | |
| Abdominal pain | 351 (24.4%) | 1346 (26.1%) | 0.912 (0.769-1.044) | 0.112 | |
| Vomiting | 103 (7.2%) | 241 (4.7%) | 1.571 (1.237-1.994) | <0.001 | |
*Statistically significant result. BMI: Body mass index, OR: Odds ratio, CI: Confidence interval, SD: Standard deviation, SES: Socioeconomic status
Table 4.
Subgroup analysis of obesity based on gender
| Age group | Total (n=7931) | Obese |
P | ||
|---|---|---|---|---|---|
| Total (n=1439) | Males (n=540) | Females (n=899) | |||
| ≤6-8 | 1442 (17.9%) | 198 (13.7%) | 65 (12%) | 133 (14.8%) | 0.142 |
| 9-11 | 2778 (35%) | 489 (17.6%) | 173 (32%) | 316 (35.2%) | 0.227 |
| >11 | 3701 (46.7%) | 752 (20.3%) | 302 (55.9%) | 450 (50.1%) | |
Effect of SES
-
Overweight
High middle SES was significantly associated with overweight when compared with lower SES [Table 2]. On univariate logistic regression, the proxies of higher SES, such as high educational level of father, high family income, living in villa, and parents' professional job, showed higher risk of overweight [Table 2]. On the other hand, the proxies of lower SES, such as parents' lower educational level, family income <1500 US $, and living in apartment, showed significantly less risk of overweight [Table 2]. A multivariate logistic model showed that family income >8000 US $ [odds ratio (OR) 1.554; confidence interval (CI) = 1.079–2.238)] was significantly associated with overweight status.
-
Obesity
Similar to overweight, obesity increases with increased levels of SES. On univariate logistic regression, the proxies of higher SES, such as high family income (>2500 US $), living in villa, and parents' professional job, showed higher risk of obesity [Table 3]. On the other hand, the proxies of lower SES, such as family income <1500 US $ and living in apartment, showed significantly less risk of overweight [Table 3]. Parents' education did not increase the risk of obesity. The multivariate regression of obesity as an outcome showed that obesity was affected by upper middle SES (OR 1.447; CI = 1.139–1.839).
Obesity and GI symptoms
Using univariate and multivariate regression analyses, obese children were at 1.5 and 2 times risk to develop abdominal distension and vomiting than non-obese children [Table 3], while the GI symptoms in the overweight group did not differ from non-overweight group [Table 2].
DISCUSSION
In this large sample representative of Saudi children and adolescents aged 6–16 years, we showed that the WHO-based prevalence rate of obesity in Riyadh city increased from 12.7% in 2006[11] to 18.2% in 2015, a rate that is similar to the obesity rate in pediatric population in the United States. Also, when compared with the WHO-based national prevalence rate of obesity reported in 2004 (≈9.3%),[12] the obesity rate has doubled over a 10-year period.
Although the rise in the prevalence of obesity is global,[13,14,15] data from some Western countries have shown a decline or stabilization of obesity levels, especially in children.[16] For example, in the United States, the overall prevalence of pediatric obesity was 16.9% in 2011–2012 and remained unchanged compared with that in 2003–2004.[17] In Germany, a study of children aged 4–16 years found a significant decline in overweight or obesity between 2004 and 2008 among children aged 4–7 years and a stabilization in other ages.[18] Our data make it clear that childhood obesity is a rising problem in Saudi Arabia and show that the risk of becoming overweight and obese among children is linked with higher levels of SES. Saudi Arabia has witnessed significant economic prosperity over the past 30 years; according to our study, two-thirds of the Saudi families (≈64%) belong to high middle or high SES. The high socioeconomic standards, especially family income, are associated with lifestyle changes including sedentary life and dietary habits that predispose to obesity. Factors associated with the occurrence of obesity in the Saudi community have been well investigated in several previous studies,[7,19,20,21,22,23] and researchers often conclude with recommendations to conduct educational campaigns and proposing interventions. However, no childhood obesity prevention or management interventions have been published yet in the local literature. Intervention programs implemented in some Western countries have helped in slowing and reducing obesity rates.[16,17,18] These intervention measures included behavioral modification, ban on fast-food advertising and delivery to houses, offering healthy foods in schools, creation of play/sports grounds in schools and within districts, and availability of indoor and outdoor facilities to enable public to engage in physical activities and sports during different climatic conditions.[16,17,18] Hence, it is now imperative to design multifaceted, national, obesity prevention programs with special focus on children.
Our study is characterized by several epidemiological features. First, our data indicate that prevalence of overweight and obesity in children increases significantly with age, a finding consistent with some studies in Saudi Arabia.[11,12,20] We postulate that this observation is possibly attributable to a combination of factors including persistence of pediatric obesity during adolescence, new children getting overweight and obese, and progression of overweight children to obesity. Regardless of the cause, this finding is very alarming and indicates absence of effective prevention programs to combat progression of obesity during childhood. Another epidemiological feature is predominance of overweight girls over boys during childhood and similar frequency of obesity between the two genders during adolescence. We postulate that adolescent girls at this age are more concerned with body image and tend to reduce their weight. Another important observation in our study is the significant association of obesity with bloating and vomiting which supports the previously reported data that relate obesity to dyspepsia and gastroesophageal reflux disease.[24,25,26]
Our study has several notable strengths. The main strength is the large randomly selected sample, serving effectively as a representative sample of all school-aged children and adolescents in Riyadh city. We used detailed socioeconomic measures and, for the first time in Saudi Arabia, we investigated the association of obesity with GI symptoms. On the other hand, there are a number of limitations mostly inherent to the cross-sectional study design that does not help infer causal association. A longitudinal study would be best to assess causal relationships and investigate the causes of increase of obesity with advancing age. Also, the study is limited to Riyadh city and its urban population and cannot be generalized to the whole Saudi population. In addition, our study was not designed to assess several important obesogenic life style factors and dietary habits of the participants.
In conclusion, this study indicates that the prevalence of overweight and obesity is rising alarmingly among Saudi children and adolescents over the past decade and should make a strong case to initiate and monitor effective implementation of obesity prevention/intervention programs. Up-to-date information on prevalence and monitoring of trends in childhood obesity in Saudi Arabia is crucial for evaluating success of interventions for prevention of obesity, provided similar cut-off values and references are used consistently.
Financial support and sponsorship
The authors extend their appreciations to King Abdulaziz City for Science and Technology for funding this work through research grant Number: A-T-32-48.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ornelas E, Francica J, Wichi R, Maifrino L. Childhood obesity and its cardiovascular implications: A current view. J Morpholo Sci. 2014;31:1–5. [Google Scholar]
- 2.Kelsey MM, Zaepfel A, Bjornstad P, Nadeau KJ. Age-related consequences of childhood obesity. Gerontology. 2014;60:222–8. doi: 10.1159/000356023. [DOI] [PubMed] [Google Scholar]
- 3.Must A, Anderson SE. Effects of obesity on morbidity in children and adolescents. Nutr Clin Care. 2003;6:4–12. [PubMed] [Google Scholar]
- 4.Alswat K, Aljumah AA, Sanai FM, Abaalkhail F, Alghamdi M, Al Hamoudi WK, et al. Nonalcoholic fatty liver disease burden - Saudi Arabia and United Arab Emirates, 2017-2030. Saudi J Gastroenterol. 2018;24:211–9. doi: 10.4103/sjg.SJG_122_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization. Global strategy on diet, physical activity and health. Geneva: World Health Organization; 2004. pp. 38–55. (WHA57.17) [Google Scholar]
- 6.Bovet P, Chiolero A, Gedeon J. Health effects of overweight and obesity in 195 countries. N Engl J Med. 2017;377:1495–6. doi: 10.1056/NEJMc1710026. [DOI] [PubMed] [Google Scholar]
- 7.Wang Y. Cross-national comparison of childhood obesity: The epidemic and the relationship between obesity and socioeconomic status. Int J Epidemiol. 2001;30:1129–36. doi: 10.1093/ije/30.5.1129. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization Multicentre Growth Reference Study Group. WHO child growth standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76–85. [Google Scholar]
- 9.Al-Hussaini A, Troncone R, Khormi M, AlTuraiki M, Alkhamis W, Alrajhi M, et al. Mass screening for celiac disease among school-aged children: Toward exploring celiac iceberg in Saudi Arabia. J Pediatr Gastroenterol Nutr. 2017;65:646–51. doi: 10.1097/MPG.0000000000001681. [DOI] [PubMed] [Google Scholar]
- 10.WHO AnthroPlus version. [Last accessed on 2015 Jan 15]. Available from: http://www.who.int/growthref/tools/en/
- 11.Al Alwan I, Al Fattani A, Longford N. The effect of parental socioeconomic class on children's body mass indices. J Clin Res Pediatr Endocrinol. 2013;5:110–115. doi: 10.4274/Jcrpe.898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.El Mouzan MI, Al Herbish AS, Al Salloum AA, Al Omar AA, Qurachi MM. Regional variation in prevalence of overweight and obesity in Saudi children and adolescents. Saud J Gastroenterol. 2012;18:129–32. doi: 10.4103/1319-3767.93818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Farrag NS, Cheskin LJ, Farag MK. A systematic review of childhood obesity in the Middle East and North Africa (MENA) region: Prevalence and risk factors meta-analysis? Adv Pediatr Res. 2017;4 doi: 10.12715/apr.2017.4.8. doi: 10.12715/apr. 2017.4.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.World Health Assembly. Update on the Commission on Ending Childhood Obesity: Report by the Director-General. Geneva: 2015. A68/10. [Google Scholar]
- 15.Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, andnational prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81. doi: 10.1016/S0140-6736(14)60460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Olds T, Maher C, Zumin S, Péneau S, Lioret S, Castetbon K, et al. Evidence that the prevalence of childhood overweight is plateauing: Data from nine countries. Int J Pediatr Obes. 2011;6:342–60. doi: 10.3109/17477166.2011.605895. [DOI] [PubMed] [Google Scholar]
- 17.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311:806–14. doi: 10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Blüher S, Meigen C, Gausche R, Keller E, Pfäffle R, Sabin M, et al. Age-specific stabilization in obesity prevalence in German children: A cross-sectional study from 1999 to 2008. Int J Pediatr Obes. 2011;6:e199–206. doi: 10.3109/17477166.2010.526305. [DOI] [PubMed] [Google Scholar]
- 19.Shaikh MA, Al Sharaf F, Shehzad K, Shoukat F, Naeem Z, Al Harbi A, et al. Prevalence and trends of overweight and obesity amongst Saudi school children, a study done by using three noninvasive methods. Int J Health Sci. 2016;10:381–7. [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Muhaimeed AA, Dandash K, Ismail MS, Saquib N. Prevalence and correlates of overweight status among Saudi school children. Ann Saudi Med. 2015;35:275–81. doi: 10.5144/0256-4947.2015.275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Lifestyle factors associated with overweight andobesity among Saudi adolescents. BMC Public Health. 2012;12:354. doi: 10.1186/1471-2458-12-354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Al-Nakeeb Y, Lyons M, Collins P, Al-Nuaim A, Al-Hazzaa H, Duncan MJ, et al. Obesity, physical activity and sedentary behavior amongst British and Saudi youth: A cross-cultural study. Int J Environ Res Public Health. 2012;9:1490–506. doi: 10.3390/ijerph9041490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Collison KS, Zaidi MZ, Subhani SN, Al-Rubeaan K, Shoukri M, Al-Mohanna FA. Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health. 2010;10:234. doi: 10.1186/1471-2458-10-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Le Pluart D, Sabate J-M, Bouchoucha M, Hercberg S, Benamouzig R, Julia C. Functional gastrointestinal disorders in 35 447 adults and theirassociation with body mass index. Aliment Pharmacol Ther. 2015;41:758–67. doi: 10.1111/apt.13143. [DOI] [PubMed] [Google Scholar]
- 25.Phatak UP, Pashankar DS. Prevalence of functional gastrointestinal disorders in obese and overweight children. Int J Obes. 2014;38:1324–7. doi: 10.1038/ijo.2014.67. [DOI] [PubMed] [Google Scholar]
- 26.Teitelbaum JE, Sinha P, Micale M, Yeung S, Jaeger J. Obesity is related to multiple functional abdominal diseases. J Pediatr. 2009;154:444–6. doi: 10.1016/j.jpeds.2008.09.053. [DOI] [PubMed] [Google Scholar]