

Abstract
Purpose:
Based on promising predinical data, we conducted a single-arm phase II trial to assess the clinical benefit rate (CBR) of neratinib, defined as complete/partial response (CR/PR) or stable disease (SD) ≥24 weeks, in HER2mut nonamplified metastatic breast cancer (MBC). Secondary endpoints included progression-free survival (PFS), toxicity, and circulating tumor DNA (ctDNA) HER2mut detection.
Experimental Design:
Tumor tissue positive for HER2mut was required for eligibility. Neratinib was administered 240 mg daily with prophylactic loperamide. ctDNA sequencing was performed retrospectively for 54 patients (14 positive and 40 negative for tumor HER2mut).
Results:
Nine of 381 tumors (2.4%) sequenced centrally harbored HER2mut (lobular 7.8% vs. ductal 1.6%; P = 0.026). Thirteen additional HER2mut cases were identified locally. Twenty-one of these 22 HER2mut cases were estrogen receptor positive. Sixteen patients [median age 58 (31–74) years and three (2–10) prior metastatic regimens] received neratinib. The CBR was 31% [90% confidence interval (CI),13%–55%], including one CR, one PR, and three SD ≥24 weeks. Median PFS was 16 (90% CI, 8–31) weeks. Diarrhea (grade 2, 44%; grade 3, 25%) was the most common adverse event. Baseline ctDNA sequencing identified the same HER2mut in 11 of 14 tumor-positive cases (sensitivity, 79%; 90% CI, 53%–94%) and correctly assigned 32 of 32 informative negative cases (specificity, 100%; 90% CI, 91%–100%). In addition, ctDNA HER2mut variant allele frequency decreased in nine of 11 paired samples at week 4, followed by an increase upon progression.
Conclusions:
Neratinib is active in HER2mut, nonamplified MBC. ctDNA sequencing offers a noninvasive strategy to identify patients with HER2mut cancers for clinical trial participation.
Introduction
HER2 (ERBB2) is a well-established therapeutic target in breast cancer (1–13), and HER2-negative (nonamplified) breast cancers overall do not benefit from HER2-directed drugs (14). However, the recent identification of recurrent HER2 mutations (HER2mut) in a subset of HER2 gene nonamplified breast cancer suggested an additional HER2 targeting opportunity (3, 15–25). HER2 mutations cluster in the tyrosine kinase and extracellular dimerization domains of HER2, leading to enhanced kinase activity and tumorigenesis in preclinical models (16, 26, 27). Importantly HER2mut render tumor cells sensitive to HER2-targeted agents, especially neratinib (16, 26, 27), a potent irreversible pan-HER inhibitor (28–34). We therefore conducted a phase II trial of neratinib in patients with HER2mut, nonamplified metastatic breast cancer (MBC; Mutant HER2 trial: MutHER). The primary endpoint was clinical benefit rate (CBR). Secondary endpoints included progression-free survival (PFS), toxicity profile, HER2mut frequency in MBC, and analysis of ctDNA for HER2mut detection and response monitoring. The Clinical-trials.gov# is NCT01670877.
Materials and Methods
Patients
Patients with HER2-negative (0 or 1+ by immunohistochemistry or nonamplified by FISH) MBC, at least 18 years old, Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) ≤2, measurable or evaluable disease by RECIST 1.1, and adequate organ function were preregistered for HER2mut screening by DNA sequencing of archival primary or metastatic tumor performed centrally at the Clinical Laboratory Improvement Amendment (CLIA)-certified Washington University Genomic and Pathology Service (GPS). Patients were eligible for screening while receiving other treatment. The initial requirement of at least one prior systemic therapy was subsequently removed to improve accrual. Local HER2 mutation testing in a local CLIA laboratory was also allowed.
Eligibility criteria for registration included tumor positive for somatic HER2mut identified by CLIA-certified laboratories, recent disease progression, adequate organ function, QTc interval ≤450 msec (men) or ≤470 msec (women), and left ventricular ejection fraction ≥ institutional lower limit of normal, ≥1 week wash-out from radiotherapy or systemic therapy. Patients receiving other cancer therapy, strong CYP3A4 inducers or inhibitors, uncontrolled concurrent illness, ≥grade 2 diarrhea, being pregnant, or breastfeeding were not eligible. Treated brain metastases stable for ≥3 months without steroids were allowed. This study was conducted in accordance with the Declaration of Helsinki and the principles of Good Clinical Practice, and was approved by each center’s Regulatory and Ethics Committees. All participants provided written informed consent.
Study design and treatment
The primary objective was rate of CB defined as complete/partial response (CR/PR) or stable disease (SD) ≥24 weeks. Secondary objectives included HER2mut frequency and clinic-pathologic characteristics of these patients, PFS on neratinib, toxicity profile, and analysis of ctDNA for HER2mut detection and response monitoring.
Sample size was calculated based on Simon’s Optimal two-stage design to enroll 10 patients in the first stage and 19 patients in the second stage to allow 80% power and a one-sided 0.05 significance level to detect an anticipated 20% CBR against the null hypothesis of 5%. At least one CB was required to proceed to the second stage. The primary endpoint is met if at least four of 29 achieved CB. After observing that almost all HER2mut tumors were ER+, the protocol was amended to add fulvestrant to the regimen (if ER+). This pragmatic decision led to an early stop of enrollment to neratinib monotherapy. Here, we report the results from the 16 patients who received neratinib monotherapy prior to the activation of this amendment.
Patients were started with neratinib orally at 240 mg daily in a 28-day cycle. Diarrhea prophylaxis with loperamide was mandatory during the first cycle of therapy. Loperamide was administered at an initial dose of 4 mg with the first dose of neratinib on cycle 1 day 1, followed by 2 mg every 4 hours for 3 days, then 2 mg every 6 to 8 hours during the first cycle of therapy, and as needed. Subjects were allowed to escalate neratinib dose to 320 mg daily if no intolerable grade 2 or higher treatment-related adverse events (AE) were experienced during a complete cycle of treatment. A maximum of three dose reductions in 40-mg decrements were permitted for toxicities. AEs were accessed by NCI CTCAE 4.0 weekly during the first cycle and day 1 of subsequent cycles. Patients underwent tumor evaluation by RECIST 1.1 every two cycles and echocardiograms every four cycles.
Central tumor DNA sequencing for HER2 mutation
Central tumor DNA sequencing for HER2 mutation was performed at the GPS laboratory. Sanger technology was initially used to sequence exons 8 and 18 to 24 of HER2, which applied to approximately 20% of samples by October 2014. Subsequently, a PCR based next-generation sequencing (NGS) assay was used to sequence all HER2 coding exons. PCR was performed using the 48.48 high-throughput access array system (Fluidigm Corp.). Cluster generation and sequencing were performed using Illumina’s HiSeq2500 Reagent Kit (200 cycles), and 2 × 101 paired-end sequence reads were generated. Each patient’s DNA was processed in three independent technical replicates to generate and sequence three independent amplicon libraries. Variant call was performed on all BAM files together by a combination of commercially available and custom-developed scripts to generate a multi-sample variant call file. Variants were called if at least three of the four BAM files had evidence for the variant, and the average variant frequency was ≥10%.
Cell-free tumor DNA sequencing
Digital sequencing of cell-free DNA was performed by Guardant Health, Inc. (Guardant360, www.guardanthealth. com/guardant360/), a CLIA-certified and College of American Pathologists (CAP)-accredited clinical laboratory. Note that 5 to 30 ng of ctDNA was isolated from plasma (two 10-mL Streck tubes drawn for each patient), and sequencing libraries were prepared with custom in-line barcode molecular tagging and complete sequencing at 15,000 × read depth. The panel utilizes hybrid capture followed by NGS of all exons in 30 genes, including HER2, and critical exons (those reported as having a somatic mutation in COSMIC) of 40 additional genes to detect and report single-nucleotide variants and small indels in 70 genes, copy-number amplifications in 18 genes, and select fusions (Supplementary Fig. S1). Postsequencing bioinformatics matches the complementary strands of each barcoded DNA fragment to remove false-positive results (35). The variant allele fraction (VAF) was computed as the number of mutated DNA molecules divided by the total number (mutated plus wild type) of DNA fragments at that allele; VAF was reported as a percentage.
Statistical analysis
The CBR was calculated as the proportion of CR, PR, or SD≥24 weeks with 90% exact binomial confidence intervals (CIs) by RECIST 1.1. Response duration was defined as the duration between the first scan demonstrating disease response and that at progression. PFS was defined as weeks from treatment initiation to progression or death. The associations of HER2 mutations with histology subtype (lobular vs. ductal), hormone receptor status (ER+/PR+ vs. ER−/PR−), and the source of sample (primary vs. metastatic) were assessed using Fisher exact tests. The diagnostic ability of ctDNA sequencing for HER2 mutations was summarized by sensitivity and specificity, with corresponding 90% CI. The association between ctDNA-mutant VAF and clinical outcomes (PFS and tumor size change) was also assessed using Spearman correlation coefficients. The data were analyzed using the standard package of SAS (Version 9.3, SAS Institute).
Results
Screening for HER2 mutation
Between December 1, 2013, and August 15, 2015, 636 women with HER2 nonamplified MBC, median age 56 (range, 23–87) years, were consented for central HER2 sequencing at Washington University CLIA-certified GPS laboratory (Supplementary Fig. S2). Among the 579 patients eligible for preregistration, 517 had tissue available for testing (Table 1). Adequate quantity and quality of tumor DNA were extracted and successfully sequenced for 381 of 517 (74%) samples (primary n = 256, metastasis n = 125) with nine of 381 (2.4%) samples positive for at least one HER2 mutation. Notably, all nine cases with HER2 mutations were also positive for ER and/or PR. The incidence of HER2 mutation was nine of 277 (3.2%) in hormone receptor-positive cases in contrast with the 0 of 82 (0%) in triple-negative breast cancers. However, the difference in HER2 mutation incidence by hormone receptor status did not reach statistical significance (P = 0.219), likely because of the small sample size. Lobular cancers had a significantly higher incidence of HER2 mutations, 7.8% (4/51), compared with ductal histology, 1.6% (5/309), (P = 0.026; Table 1). There was no difference in the detection rate of HER2 mutations in tumors from primary (2.3%) or metastatic sites (2.4%).
Table 1.
Incidence of HER2-activating mutations by histology, hormone receptor status, and tumor tissue source for patients whose tumor samples successfully sequenced at GPS laboratory
| Positive for HER2 mutation, N (%) |
P | |
|---|---|---|
| Histology | ||
| Invasive ductal carcinoma (n = 309) | 5 (1.6%) | 0.026a |
| Invasive lobular carcinoma (n = 51) | 4 (7.8%) | |
| Invasive ductal/lobular carcinoma (n = 12) | 0 (0%) | |
| Otherb (n = 9) | 0 (0%) | |
| Hormone receptor status | ||
| ER+ and/or PR+ (n = 277) | 9 (3.2%) | 0.219 |
| ER− PR− HER2− (n = 82) | 0 (0%) | |
| Unknown (n = 17) | 0 (0%) | |
| Samples tested | ||
| Primary breast cancer (n = 256) | 6 (2.3%) | >0.99 |
| Metastatic site (n = 125) | 3 (2.4%) | |
| Total (n = 381) | 9 | |
Comparison between ductal carcinoma (n = 309) vs. lobular carcinoma (n = 51).
Others include metaplastic (n = 2); mucinous (n = 3); and unknown (n = 4).
An additional 13 patients with HER2mut were identified by an outside CLIA-lab (Supplementary Fig. S2). Figure 1 shows the distribution of the HER2 mutations identified in all 22 cases. L755S was the most common mutation (n = 7,32%). The median patient age was 58 (range, 31–72) years, 15 of22 (68%) were ductal, seven of 22 (32%) were lobular cancers, and 21 of 22 (95%) were ER+. Retrospectively, 21 of 22 patients presented initially with early-stage disease. The median recurrence-free survival from surgery to recurrence was 35.9 (90% CI, 15.4–93.8) months.
Figure 1.
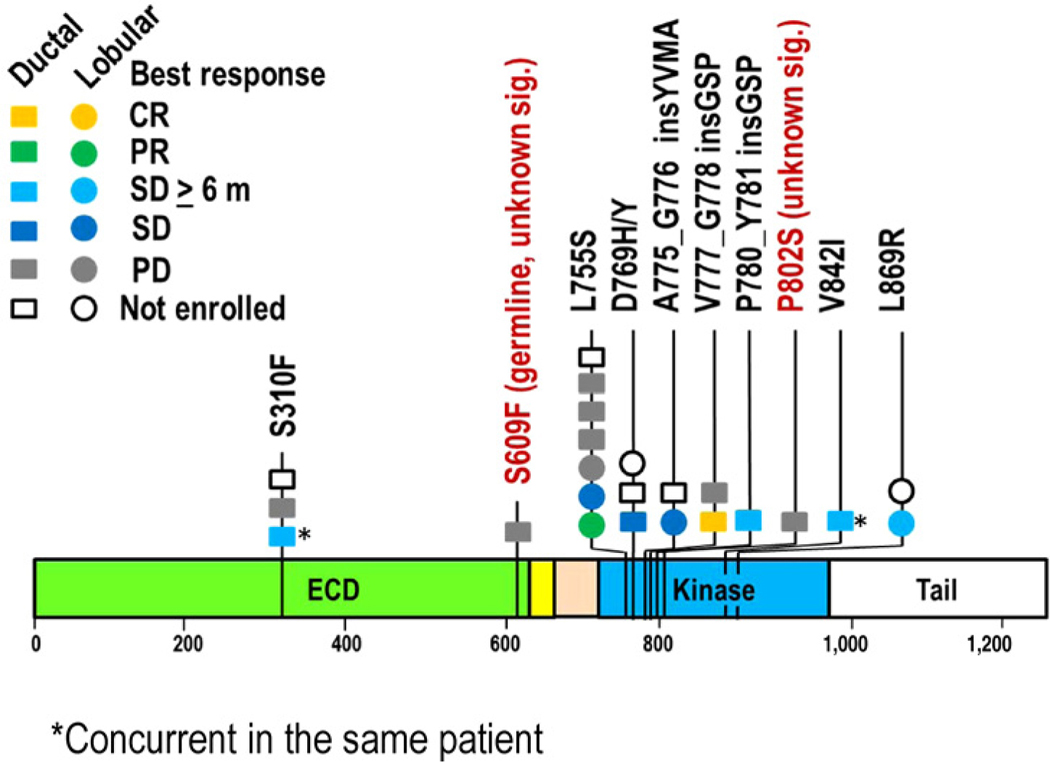
HER2 mutations identified by tumor DNA sequencing at Central and other laboratories. Each circle (lobular) or square (ductal) represents a single patient except in a case of concurrent S310F and V842I mutations (indicated by *).
Clinical characteristics for patients receiving neratinib
Sixteen patients received neratinib monotherapy, including 14 with known-activating mutations and two of unknown significance (no preclinical data; Fig. 1; Supplementary Fig. S2). Table 2 details the patient characteristics. As of data cutoff, all patients had stopped study therapy due to progression (n = 15, 94%) or AE (n = 1, 6%).
Table 2.
Characteristics of the 16 patients who received neratinib (N, %)a
| Age, years | |
| Median (range) | 58 (31–74) |
| Race | |
| White/African American/Asian | 13 (81%)/1 (6%)/2 (13%) |
| ECOG PS | |
| 0/1/2 | 9 (56%)/7 (44%)/0 (0%) |
| Menopausal status | |
| Pre-/postmenopausal | 2 (12%)/14(88%) |
| Histology | |
| Ductal/lobular | 11 (67%)/5 (31.3%) |
| Hormone receptor status | |
| ER+PR+/ER+PR−/ER−PR−HER2− | 7 (44%)/8 (50%)/1 (6%) |
| HER2 status | |
| Nonamplified/amplified | 16 (100%)/0 (0%) |
| Evaluable disease by RECIST | |
| Measurable/nonmeasurable | 13 (81%)/3 (19%) |
| Disease magnitude | |
| Visceral/nonvisceral | 11 (69%)/5 (31%) |
| Prior number of metastatic regimens | |
| Any/endocrine/chemo (median, range) | 3 (2–10)/2 (0–3)/2 (0–6) |
| Reason off study | |
| Adverse event/progressive disease | 1 (6%)/15 (94%) |
Unless otherwise specified.
Adverse events
All 16 patients were evaluable for AE (Table 3). Treatment was well tolerated, and most AEs were grades 1 and 2, with one patient who discontinued therapy due to AE (grade 3 fatigue and dehydration). The most common grade 2 and above AEs included diarrhea (69%), anorexia (44%), and fatigue (31%), and there were no grade 4 AEs. Diarrhea (n = 4, 25%) was the only treatment-related grade 3 AE that occurred in more than one patient, but the duration was short, lasting a median of 1.5 days (range, 1–3 days). Neratinib was reduced to 200 mg daily in four (25%) patients due to grade 3 diarrhea (n = 2), grade 2 nausea/anorexia (n = 1), and grade 3 fatigue/dehydration leading to neratinib discontinuation (n = 1). Neratinib was escalated to 320 mg daily in five patients (three PD, two SD ≥24 weeks) in cycles two (n = 4) and four (n = 1) and continued until disease progression, except in one patient who subsequently reduced to 240 mg 10 days after due to grade 2 nausea/anorexia and diarrhea.
Table 3.
Grade 2 and above AEs at least possibly related to neratinib (N = 16)
| AE | Grade 2, N (%) | Grade 3, N (%) | Total, N (%) |
|---|---|---|---|
| Diarrhea | 7 (44%) | 4 (25%)* | 11 (69%) |
| Anorexia | 7 (44%) | 0 | 7 (44%) |
| Fatigue | 4 (25%) | 1 (6%) | 5 (31%) |
| Anemia | 3 (19%) | 0 | 3 (19%) |
| Nausea | 3 (19%) | 0 | 3 (19%) |
| Dehydration | 1 (6%) | 1 (6%) | 2 (13%) |
| Dyspepsia | 2 (13%) | 0 | 2 (13%) |
| Hypophosphatemia | 2 (13%) | 0 | 2 (13%) |
| Vomiting | 2 (13%) | 0 | 2 (13%) |
| Syncope | 0 | 1 (6%) | 1 (6%) |
NOTE: AEs that are grade 2 or above experienced by more than one patient or any occurrence of grade 3 AEs are included.
Antitumor activity
One of the 10 patients enrolled in the first stage achieved CB; therefore, the study continued to the second stage until the activation of the protocol amendment for subsequent patients to receive the combination of fulvestrant and neratinib if ER+. In total, 16 patients received neratinib monotherapy. The median number of metastatic regimens received prior to study entry was three (range, 2–10). Five patients experienced CB including one CR (6%), one PR (6%), and three SD ≥24 weeks (19%). The CBR was 31% (90% CI, 13%–55%), which met the primary endpoint. The median response duration in patients who achieved CB was 24 (range, 24–66) weeks. PFS and changes in tumor size were shown in Figure 2A and B, respectively. An example of response is illustrated in Figure 2C. Among the 15 patients with ER+ breast cancer, only one (pt 16) received a CDK4/6 inhibitor (ribociclib) for metastatic disease prior to study enrollment. This patient experienced prolonged disease stabilization on neratinib (PFS 37 weeks). Treatment benefit was observed across different HER2 mutations including L755S, V777_G778 insGSP, P780_Y781 insGSP, V842I, S310F, and L869R. Multi-gene panel next-generation tumor sequencing results were available for 13 patients: common co-occurring mutations included CDH1 (5/13), PIK3CA (4/13), and TP53 (6/13).
Figure 2.
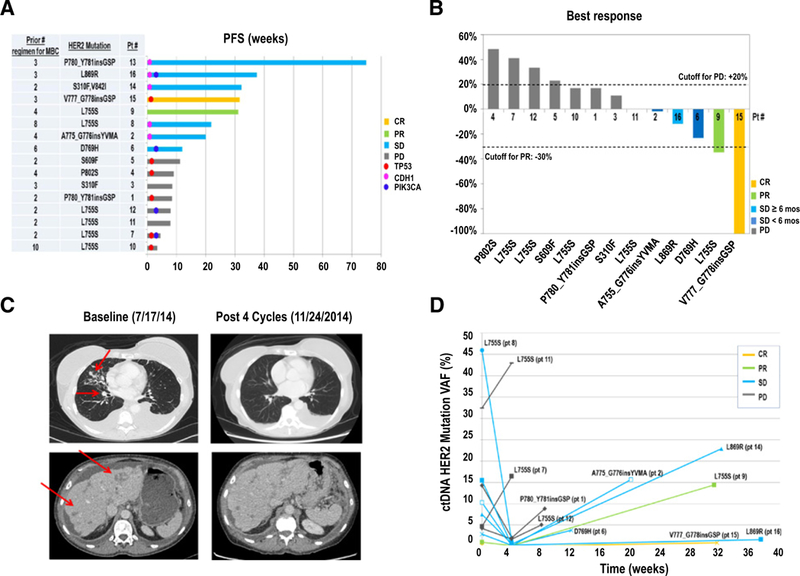
Antitumor activity of neratinib. A, Swimmer Plot of time to progression (TTP) for patients with HER2-activating mutations. Co-occurring mutations in TP53, CDH1, and PIK3CA by tumor DNA sequencing are indicated. B, Percentage change in target lesion at best response compared with baseline. Patients with measurable diseases are included. C, Representative CT images of a patient on study. Sixty-four-year old woman (Pt 9) with ER+/HER2− metastatic breast cancer, HER2 L755S, prior disease progression on fulvestrant, and exemestane plus everolimus in the metastatic setting, achieved a partial response on neratinib. D, ctDNA HER2 mutation variant allele frequency in response to neratinib. HER2 mutation VAFs at baseline, 4 weeks, and progression are plotted for individual patients (n = 11).
Plasma cell-free tumor DNA sequencing
ctDNA sequencing for HER2mut detection and response monitoring was performed using a 70-gene digital sequencing assay (Guardant Health; Supplementary Fig. S1). Plasma collected from patients with HER2-activating mutations was analyzed at baseline as positive controls (n = 14) and additionally tested following 4 weeks on neratinib (n = 13) and upon progression (n = 9). Because a sample size of at least 30 negative controls was required to ensure 90% confidence of >90% testing specificity, plasma collected at preregistration for 40 patients negative for HER2mut by tumor sequencing at GPS was analyzed.
Among the 14 positive control cases, two were negative for any HER2mut by ctDNA sequencing despite the detection of other genetic alterations in the same sample, and 11 were positive for the same HER2mut as by tumor testing (sensitivity: 11/14; 79%, 90% CI, 53%–94%; Supplementary Table S1). One other patient (Pt 14), SD ≥ 24 weeks on neratinib, had discrepant HER2mut alleles by tumor and ctDNA sequencing. ctDNA sequencing identified HER2 L869R and D769Y at baseline, in contrast to the S310F and V842I detected in the breast cancer specimen collected from several years prior to trial enrollment. Interestingly, the ctDNA VAFs for both HER2 L869R and D769Y were reduced at week 4, and increased at progression, accompanied by the emergence of several other HER2 mutations, including the T798I mutation in the kinase domain of HER2 analogous to the EGFR T790M “gate-keeper” drug resistance mutation (Fig. 3A refs. 36–38).
Figure 3.
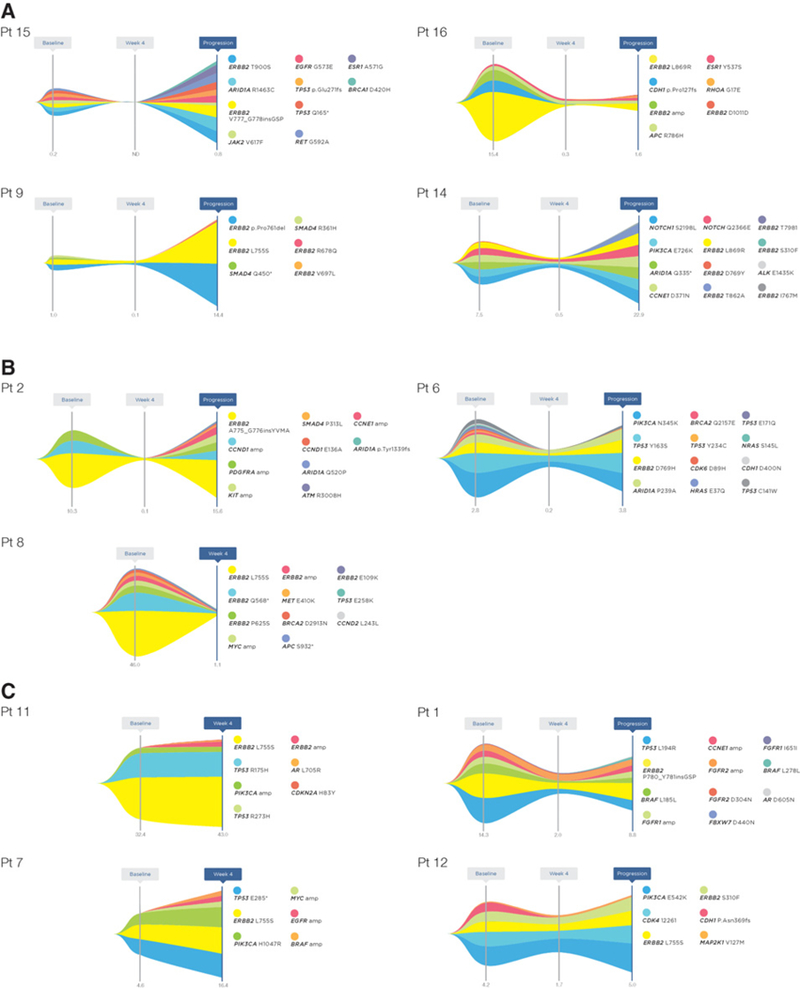
Variant allele frequency maps of ctDNA-detected mutations in individual patients in response to neratinib treatment. Variant allele frequencies (VAFs) of ctDNA-detected mutations over time are shown for the 11 patients with detectable HER2 mutation at baseline and with available blood samples at subsequent time points (n = 11 at 4 weeks, and n = 8 at progression). A includes four patients who achieved clinical benefit (CR in Pt 15, PR in Pt 9, SD ≥24 weeks in Pts 16 and 14). B, three patients who had best response of SD but lasted less than 24 weeks (Pt 2, Pt 6, and Pt 8). C, four patients who had PD as the best response (Pt 11, Pt 7, Pt 1, and Pt 12). Numbers at the bottom of each graph represent the VAFs of the HER2 mutation colored in yellow, which were also used to plot Fig. 2D. All ctDNA alterations are shown except for patients 14 and 6 due to space limits in the figure. The complete list of mutations and their VAFs is detailed in Supplementary Table S3.
Among the 40 negative control cases, 32 were informative for ctDNA sequencing interpretation (eight had no detectable ctDNA mutations), and all 32 were negative for HER2mut despite the detection of other somatic mutations in each case. Therefore, the specificity of ctDNA for HER2mut detection was 32 of 32 (100%; 90% CI, 91%–100%; Supplementary Table S1). The overall concordance rate between plasma and tumor HER2 sequencing results was 43 of46 (93.5%; 90% CI, 87%–100%; Supplementary Tables S1 and S2).
We further queried the ctDNA sequencing data from 1,834 advanced breast cancer patients clinically tested at Guardant Health between October 2015 and August 2016 using the same assay. HER2-activating mutations in the absence of HER2 amplification were identified in 48 of 1,584 (3.0%) evaluable patients. The incidence and distribution (Supplementary Fig. S3) were similar to prior tumor-based analyses (16).
Among the 11 patients (four PD and seven non-PD as best response by RECIST) with baseline HER2 mutation detected by ctDNA who also had subsequent blood collections, HER2mut VAF decreased at week 4 in nine patients, including all seven patients with non-PD as their best response. The HER2mut VAF at week 4 was reduced to nondetectable in the patient with CR (Pt 15). Although two patients with PD as the best response (Pts 1 and 12) demonstrated a decrease in HER2mut VAFs at week 4, their HER2mut VAFs subsequently increased at week 8, when progression was radiographically detected. In contrast, the other two of four patients with PD as the best response (Pts 7 and 11) had a rise in HER2mutVAFs at week 4, consistent with early progression (Fig. 2D and 3; Supplementary Table S2). The absolute levels of HER2mut VAFs at week 4 were significantly associated with PFS (Spearman correlation coefficient rho = 20.69, P = 0.017, n = 11) and tumor size change (rho = 0.67, P = 0.05, n = 9). All patients had a rise in HER2mut VAFs upon disease progression.
A number of genetic alterations were also identified in ctDNA sequencing, which co-occur with HER2 mutations (Supplementary Table S3), with the VAFs of HER2 mutations among the highest in each case. The VAFs of these co-occurring genetic alterations trended similarly to that of HER2 mutations (Fig. 3). These data further support HER2 mutations being a driver event in HER2mut breast cancers which can be treated with neratinib.
Discussion
HER2-targeted agents have markedly improved outcomes for patients with HER2-positive breast cancer (2, 5–9). In this phase II study, single-agent neratinib, an irreversible pan-HER inhibitor, demonstrated a CBR of 31% (90% CI, 13%–55%), in a heavily pretreated patient population with HER2-mutated nonamplified MBC. Neratinib was well tolerated with limited duration of grade 3 diarrhea (median = 1.5 days) and only one patient discontinuing therapy due to AE. The incidence of HER2-activating mutations in primary breast cancer approximates 2% to 3% overall, with an approximately threefold higher incidence in lobular cancers (3, 15–17). Therefore, approximately 5,000 to 7,500 (2%–3% of 250,000; ref. 39) new breast cancers each year in the United States likely have a HER2 mutation at diagnosis. The overall prevalence of HER2 mutation in MBC can only be estimated, but in the United States, at least 200,000 patients are likely to be living with advanced disease today based on a relapse risk of 30% and median survival of 3 years (40). Based on the incidence of 2% to 3%, 4,000 to 6,000 patients have a HER2-mutant metastatic tumor. This prevalence is sufficient to conduct randomized trials to establish a standard of care if HER2 mutation screening were widely available.
This study demonstrates the feasibility of targeting a rare breast cancer patient population with a multi-institutional, collaborative effort. The logistics of large-scale screening efforts were the major challenge, hampered by insufficient tumor tissue in approximately one-third of patients. ctDNA-based HER2 sequencing provides a noninvasive, highly specific and sufficiently sensitive alternative to invasive approaches to be recommended in a clinical trial setting to assist in patient identification.
This study was proof of concept and had a small sample size. However, the investigation met the predefined primary endpoint and provided strong evidence that HER2 mutation is a valid therapeutic target. Although there have been several single case reports of patients with HER2 mutated, nonamplified MBC responding to HER2-targeted agents, this is the first report of a formal study addressing this question (22, 25). Although the CBR of 31% (90% CI, 13%–55%) is modest, it is significant in a heavily pretreated patient population that received a median of 3 (range, 2–10) prior treatment regimens in the metastatic setting. As an example, single-agent palbociclib showed a CBR of 19% overall, and 29% in the HR+ HER2− subset, in patients with Rb+ advanced breast cancer who had progressed through at least two prior lines of hormonal therapy (41).
In summary, our data indicate efficacy of neratinib for HER2-mutated nonamplified breast cancer and provide a rationale for a large-scale ctDNA-based screening program to identify a sufficient number of patients with HER2-mutant breast cancer to establish a new standard of care. The universal, and in many cases, quite rapid development of acquired resistance despite a clear initial molecular response by HER2 mutation VAF in ctDNA indicates that rational combination therapy is the next step. The strong association between ER positivity and HER2-activating mutations demands dual targeting of ER and HER2 pathways based on the success of combining ER and HER2-targeted agents in HER2-amplified disease (42–44). This phase II trial has therefore been amended to investigate the combination of fulvestrant and neratinib in subsequent patients with ER-positive HER2-mutated nonamplified breast cancer and to allow ctDNA determination of HER2 mutation status as an eligibility criterion (NCT01670877). Other ongoing studies that target HER2-mutated advanced solid tumors include the SUMMIT neratinib basket study (NCT01953926), the NCI-MATCH trial with afatinib (NCT02465060), and My Pathway trial with trastuzumab plus pertuzumab (NCT02091141).
Supplementary Material
Translational Relevance.
Prospective trials in genomically defined populations are needed for next-generation sequencing to guide individualized cancer care. We report a phase II trial of the pan-HER inhibitor neratinib for patients with HER2-mutated (HER2mut), nonamplified metastatic breast cancer (MBC). The study demonstrated a clinical benefit rate of 31% (90% confidence interval, 13%–55%) with manageable toxicities. The screening process was challenged by the low frequency of HER2mut (2.4%) and a high rate of sequencing failure (26%) using archival tumor material. Retrospective plasma ctDNA sequencing showed high specificity and good sensitivity in detecting HER2mut, supporting its use as a screening tool to identify future trial patients. The on-target effect of neratinib was supported by early decreases of ctDNA HER2mut variant allele frequency, which then increased upon clinical progression. The predominance of estrogen receptor positivity of HER2mut MBC provided the rationale for testing fulvestrant plus neratinib in in the next phase of this trial.
Acknowledgments
We thank patients and their families for participation in this study. We thank physicians, nurses, research, and regulatory coordinators for their work, PUMA Biotechnology for trial support, and Army of Women for patient referral. We acknowledge Stephanie Myles for assisting protocol development and Zach Skidmore for graphing Supplementary Fig. S3.
Grant Support
This work is funded in part by Siteman Cancer Center, The Foundation for Barnes-Jewish Hospital Cancer Frontier Team Science Award (C.X. Ma, R. Bose, M.J.C. Ellis, and J. Pfeifer), NCI Cancer Clinical Investigator Team Leadership Award (C.X. Ma), and Puma Biotechnology Inc. M.J.C. Ellis is a McNair Medical Foundation Scholar and a Cancer Prevention Institute of Texas established investigator.
Footnotes
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Disclosure of Potential Conflicts of Interest
C.X. Ma reports receiving commercial research grants from and is a consultant/advisory board member for Novartis, Pfizer, and Puma Biotechnology. R. Bose is a consultant/advisory board member for Genetech. G. Kimmick reports receiving commercial research grants from BioNovo, Bristol-Myers Squibb, GlaxoSmithKlein, Novartis, and Puma Biotechnology. E. Winer is a consultant/advisory board member for Genetech, LEAP, and Tesaro. M. Naughton reports receiving speakers bureau honoraria from Genetech and Novartis. D. Tripathy is a consultant/advisory board member for Puma Biotechnology. M. Cobleigh is a consultant/advisory board member for Puma Biotechnology. C. Anders is a consultant/advisory board member for Angiochem, Eli Lilly, Genentech, Geron, Kadmon, Merrimack, Nektar, Novartis, Sanofi, and to BBB. K.C. Banks holds ownership interest (including patents) in Guardant Health. R.B. Lanman holds ownership interest (including patents) in Guardant Health. R. Bryce and A. Lalani are employees of PUMA Biotechnology. D.F. Hayes reports receiving commercial research grants from Puma Biotechnology, reports receiving other commercial research support from AstraZeneca, Janssen, and Pfizer, and holds ownership interest (including patents) in OncImmune. K. Blackwell is a consultant/advisory board member for Puma Biotechnology. M.J.C. Ellis is an employee of and holds ownership interest (including patents) in Bio-classifier LLC, and is a consultant/advisory board member of AstraZeneca, Novartis, Pfizer, and Puma Technology. No potential conflicts of interest were disclosed by the other authors.
Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/).
Prior presentation: Presented in part at the 2017 American Association for Cancer Research Annual Meeting, the 2016 Annual meeting for the American Society of Clinical Oncology, and the 2014 San Antonio Breast Cancer Symposium.
References
- 1.Slamon DJ, Godolphin W, Jones LA, Holt JA, Wong SG, Keith DE, et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science 1989;244:707–12. [DOI] [PubMed] [Google Scholar]
- 2.Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001;344:783–92. [DOI] [PubMed] [Google Scholar]
- 3.Desmedt C, Zoppoli G, Gundem G, Pruneri G, Larsimont D, Fornili M, et al. Genomic characterization of primary invasive lobularbreast cancer. J Clin Oncol 2016;34:1872–81. [DOI] [PubMed] [Google Scholar]
- 4.Burstein HJ. The distinctive nature of HER2-positive breast cancers. N Engl J Med 2005;353:1652–4. [DOI] [PubMed] [Google Scholar]
- 5.Abramson V, Arteaga CL. New strategies in HER2-overexpressing breast cancer: many combinations of targeted drugs available. Clin Cancer Res 2011;17:952–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Perez EA, Romond EH, Suman VJ, Jeong JH, Davidson NE, Geyer CE Jr., et al. Four-year follow-up of trastuzumab plus adjuvant chemotherapy for operable human epidermal growth factor receptor 2-positive breast cancer: joint analysis of data from NCCTG N9831 and NSABP B-31. J Clin Oncol 2011;29:3366–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Romond EH, Perez EA, Bryant J, Suman VJ, Geyer CE Jr., Davidson NE, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005;353:1673–84. [DOI] [PubMed] [Google Scholar]
- 8.Smith I, Procter M, Gelber RD, Guillaume Sb, Feyereislova A, Dowsett M, et al. 2-year follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer: a randomised controlled trial. Lancet 2007; 369:29–36. [DOI] [PubMed] [Google Scholar]
- 9.Robert N, Leyland-Jones B, Asmar L, Belt R, Ilegbodu D, Loesch D, et al. Randomized phase III study of trastuzumab, paclitaxel, and carboplatin compared with trastuzumab and paclitaxel in women with HER-2A-over-expressing metastatic breast cancer. J Clin Oncol 2006;24:2786–92. [DOI] [PubMed] [Google Scholar]
- 10.Wolff AC, Hammond MEH, Hicks DG, Dowsett M, McShane LM, Allison KH, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J Clin Oncol 2013;31:3997–4013. [DOI] [PubMed] [Google Scholar]
- 11.Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987;235:177–82. [DOI] [PubMed] [Google Scholar]
- 12.Andrulis IL, Bull SB, Blackstein ME, Sutherland D, Mak C, Sidlofsky S, et al. neu/erbB-2 amplification identifies a poor-prognosis group of women with node-negative breast cancer. Toronto Breast Cancer Study Group. J Clin Oncol 1998;16:1340–9. [DOI] [PubMed] [Google Scholar]
- 13.Sjogren S, Inganas M, Lindgren A, Holmberg L, Bergh J. Prognostic and predictive value of c-erbB-2 overexpression in primary breast cancer, alone and in combination with other prognostic markers. J Clin Oncol 1998;16:462–9. [DOI] [PubMed] [Google Scholar]
- 14.Vogel CL, Cobleigh MA, Tripathy D, Gutheil JC, Harris LN, Fehrenbacher L, et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol 2002;20:719–26. [DOI] [PubMed] [Google Scholar]
- 15.Network TCGA.Comprehensive molecular portraits of human breast tumours. Nature 2012;490:61–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bose R, Kavuri SM, Searleman AC, Shen W, Shen D, Koboldt DC, et al. Activating HER2 mutations in HER2 gene amplification negative breast cancer. Cancer Discov 2013;3:224–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ross JS, Wang K, Sheehan CE, Boguniewicz AB, Otto G, Downing SR, et al. Relapsed classic E-cadherin (CDH1)-mutated invasive lobular breast cancer shows a high frequency of HER2 (ERBB2) gene mutations. Clin Cancer Res 2013;19:2668–76. [DOI] [PubMed] [Google Scholar]
- 18.Grellety T, Soubeyran I, Robert J, Bonnefoi H, Italiano A. A clinical case of invasive lobular breast carcinoma with ERBB2 and CDH1 mutations presenting a dramatic response to anti-HER2-directed therapy. Ann Oncol 2016;27:199–200. [DOI] [PubMed] [Google Scholar]
- 19.Ross JS, Ali SM, Wang K, Khaira D, Palma NA, Chmielecki J, et al. Comprehensive genomic profiling of inflammatory breast cancer cases reveals a high frequency of clinically relevant genomic alterations. Breast Cancer Res Treat 2015;154:155–62. [DOI] [PubMed] [Google Scholar]
- 20.Ross JS, Gay LM, Nozad S, Wang K, Ali SM, Boguniewicz A, et al. Clinically advanced and metastatic pure mucinous carcinoma of the breast: a comprehensive genomic profiling study. Breast Cancer Res Treat 2016;155: 405–13. [DOI] [PubMed] [Google Scholar]
- 21.Wen W, Chen WS, Xiao N, Bender R, Ghazalpour A, Tan Z, et al. Mutations in the kinase domain of the HER2/ERBB2 gene identified in a wide variety of human cancers. J Mol Diagn 2015;17:487–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ben-Baruch NE, Bose R, Kavuri SM, Ma CX, Ellis MJ. HER2-mutated breast cancer responds to treatment with single-agent neratinib, a second-generation HER2/EGFR tyrosine kinase inhibitor. J Natl Compr Canc Netw 2015;13:1061–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Boulbes DR, Arold ST, Chauhan GB, Blachno KV, Deng N, Chang WC, et al. HER family kinase domain mutations promote tumor progression and can predict response to treatment in human breast cancer. Mol Oncol 2015; 9:586–600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chumsri S, Weidler J, Ali S, Balasubramanian S, Wallweber G, DeFazio-Eli L, et al. Prolonged response to trastuzumab in a patient with HER2-nonamplified breast cancer with elevated HER2 dimerization harboring an ERBB2 S310F mutation. J Natl Compr Canc Netw 2015;13:1066–70. [DOI] [PubMed] [Google Scholar]
- 25.Ali SM, Alpaugh RK, Downing SR, Stephens PJ, Yu JQ, Wu H, et al. Response of an ERBB2-mutated inflammatorybreast carcinoma to human epidermal growth factor receptor 2-targeted therapy. J Clin Oncol 2014;32:e88–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Greulich H, Kaplan B, Mertins P, Chen TH, Tanaka KE, Yun CH, et al. Functional analysis of receptor tyrosine kinase mutations in lung cancer identifies oncogenic extracellular domain mutations of ERBB2. Proc Natl Acad Sci U S A 2012;109:14476–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang SE, Narasanna A, Perez-Torres M, Xiang B, Wu FY, Yang S, et al. HER2 kinase domain mutation results in constitutive phosphorylation and activation of HER2 and EGFR and resistance to EGFR tyrosine kinase inhibitors. Cancer Cell 2006;10:25–38. [DOI] [PubMed] [Google Scholar]
- 28.Rabindran SK, Discafani CM, Rosfjord EC, Baxter M, Floyd MB, Golas J, et al. Antitumor activity of HKI-272, an orally active, irreversible inhibitor of the HER-2 tyrosine kinase. Cancer Res 2004;64:3958–65. [DOI] [PubMed] [Google Scholar]
- 29.Tsou H-R, Overbeek-Klumpers EG, Hallett WA, Reich MF, Floyd MB, Johnson BD, et al. Optimization of6,7-disubstituted-4-(arylamino)quinoline-3-carbonitriles as orally active, irreversible inhibitors of human epidermal growth factor receptor-2 kinase activity. J Med Chem 2005;48: 1107–31. [DOI] [PubMed] [Google Scholar]
- 30.Wong KK, Fracasso PM, Bukowski RM, Lynch TJ, Munster PN, Shapiro GI, et al. A phase I study with neratinib (HKI-272), an irreversible pan ErbB receptor tyrosine kinase inhibitor, in patients with solid tumors. Clin Cancer Res 2009;15:2552–8. [DOI] [PubMed] [Google Scholar]
- 31.Burstein HJ, Sun Y, Dirix LY, Jiang Z, Paridaens R, Tan AR, et al. Neratinib, an irreversible ErbB receptor tyrosine kinase inhibitor, in patients with advanced ErbB2-positive breast cancer. J Clin Oncol 2010;28:1301–7. [DOI] [PubMed] [Google Scholar]
- 32.Martin M, Bonneterre J, Geyer CE Jr., Ito Y, Ro J, Lang I, et al. A phase two randomised trial of neratinib monotherapy versus lapatinib plus capecitabine combination therapy in patients with HER2+ advanced breast cancer. Eur J Cancer 2013;49:3763–72. [DOI] [PubMed] [Google Scholar]
- 33.Chan A, Delaloge S, Holmes FA, Moy B, Iwata H, Harvey VJ, et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2016;17:367–77. [DOI] [PubMed] [Google Scholar]
- 34.Feldinger K, Kong A. Profile of neratinib and its potential in the treatment of breast cancer. Breast Cancer: Targets and Therapy 2015;7:147–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lanman RB, Mortimer SA, Zill OA, Sebisanovic D, Lopez R, Blau S, et al. Analytical and clinical validation of a digital sequencing panel for quantitative, highly accurate evaluation of cell-free circulating tumor DNA. PloS one 2015;10:e0140712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kancha RK, von Bubnoff N, Bartosch N, Peschel C, Engh RA, Duyster J. Differential sensitivity of ERBB2 kinase domain mutations towards lapa-tinib. PloS one 2011;6:e26760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rexer BN, Ghosh R, Narasanna A, Estrada MV, Chakrabarty A, Song Y, et al. Human breast cancer cells harboring a gatekeeper T798M mutation in HER2 overexpress EGFR ligands and are sensitive to dual inhibition of EGFR and HER2. Clin Cancer Res 2013;19:5390–401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hanker AB, Red Brewer M, Sheehan JH, Koch JP, Sliwoski GR, Nagy R, et al. An Acquired HER2 T798I gatekeeper mutation induces resistance to neratinib in a patient with HER2 mutant-driven breast cancer. Cancer Discov 2017;7:575–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA: A Cancer J Clin 2016;66:7–30. [DOI] [PubMed] [Google Scholar]
- 40.O’Shaughnessy J Extending survival with chemotherapy in metastatic breast cancer. Oncologist 2005;10:20–9. [DOI] [PubMed] [Google Scholar]
- 41.DeMichele A, Clark AS, Tan KS, Heitjan DF, Gramlich K, Gallagher M, et al. CDK 4/6 inhibitor palbociclib (PD0332991) in Rb+ advanced breast cancer: phase II activity, safety, and predictive biomarker assessment. Clin Cancer Res 2015;21:995–1001. [DOI] [PubMed] [Google Scholar]
- 42.Schwartzberg LS, Franco SX, Florance A, O’Rourke L, Maltzman J, Johnston S. Lapatinib plus letrozole as first-line therapy for HER-2+ hormone receptor-positive metastatic breast cancer. Oncologist 2010;15:122–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Marcom PK, Isaacs C, Harris L, Wong ZW, Kommarreddy A, Novielli N, et al. The combination ofletrozole and trastuzumab as first or second-line biological therapy produces durable responses in a subset of HER2 positive and ER positive advanced breast cancers. Breast Cancer Res Treat 2007; 102:43–9. [DOI] [PubMed] [Google Scholar]
- 44.Kaufman B, Mackey JR, Clemens MR, Bapsy PP, Vaid A, Wardley A, et al. Trastuzumab plus anastrozole versus anastrozole alone forthe treatment of postmenopausal women with human epidermal growth factor receptor 2-positive, hormone receptor-positive metastatic breast cancer: results from the randomized phase III TAnDEM study. J Clin Oncol 2009;27:5529–37. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.