

Abstract
According to Traditional Chinese Medicine “acupuncture is believed to restore the balance between Yin and Yang” and this can be understood in the Western medicine terminology as a “modulation of the equilibrium between parasympathetic and sympathetic activity”. The vast majority of studies concerning the mechanisms of action of acupuncture have been conducted on its influence on pain, and it has been proposed that acupuncture may indirectly relieve chronic pain by its effects on autonomic nervous system function. Several studies have shown that acupuncture recruits brain networks involved in the integration of multiple other brain functions: for example, the limbic-paralimbic-neocortical network, which plays a major role in modulating the affective dimensions of pain processing and the integration of emotional, sensorimotor, autonomic and immunological functions. It has been recently proposed that mechanical signaling through the connective tissue, along with transmission of the matrix deformation through the fascial system network, can explain the therapeutic effect of acupuncture. This model of acupunture, which involves the transduction of mechanical signals through the connective planes and produces a secondary involvement of neurophysiological mechanism, appears to fit very closely to the ancient model. It is also compatible with the proposed neurophysiological explanation. Furthermore, it appears to be fruitful also in manual therapy approaches. Drawing on the basis of the “Fascial network hypothesis of meridians”, in which there is an overlap between the channels network described by Traditional Chinese Medicine and the newly-defined fascial system, I propose an intervention through a combination of acupoints that have been selected due to their relationship between “extraordinary acupuncture channels”, the myofascial sequences described by Stecco, and the emotional and adaptive function as contemplated by a psychosomatic model used in posturology. This intervention is aimed at treating both stress and postural imbalance.
Key Words: acupuncture, neuromodulation, posturology, fascial system, osteopathy
Ethical Publication Statement
The author confirms that he read the Journal’s position on issues involved in ethical publication and affirms that this report is consistent with those guidelines.
In the contest of Traditional Chinese Medicine (TCM), acupuncture has been practiced for over 3000 years demonstrating clinical effects on a wide range of disorders. "Acupuncture is believed to restore the balance between Yin and Yang” which, translated into the western medicine terminology, can also been understood as the “modulation of the imbalance between parasympathetic and sympathetic activity”.1
Acupuncture and neuroscience: from reflexology to limbic neuromodulation
For this reason, acupuncture has been proposed to treat stress-related diseases through modulating the imbalance between the sympathetic and parasympathetic activities.²
In fact, it has been shown that changes in parasympathetic nervous activity, as measured by heart rate variability (HRV), correlate with the amount of “de-qi sensation” (tingling, numbness, heaviness or other feelings that occur during acupuncture session) upon mechanical manipulation of the needle.3,4 Several studies have shown that somatic afferents from the skin and muscle, induced by sensory mechanical stimulation trough the needle insertion, are involved in the control of various autonomic function trough the somato-autonomic reflex mediated by the nucleus tractus solitarius (NTS), primary brainstem relay for visceral information, by their projections to the dorsal motor nucleus of vagal (DMV) and to the rostral ventrolateral medulla (RVLM), whose neurons provide drive to the sympathetic preganglionic neurons located in the intermediolateral nucleus of the spinal cord.1,5-7 Indeed, acupuncture has been proposed as a useful therapy to activate the vagal anti-inflammatory pathway in the brainstem⁸, confirmed by neuroimaging studies in the so-called “acupoint-brain-organ theory“.⁹ The vast majority of studies about the mechanism of action of acupuncture has been conducted on its action on pain, but it has been proposed that acupuncture may relieve chronic pain basically trough its indirect effect on the autonomic nervous system.10 The quantitative relationship between number of manipulation inducing de-qi sensation, increased parasympathetic activity measured by heart rate variability (HRV) and the positive correlation with alpha, gamma and delta power at EEG measurement, suggest that autonomic changes induced by manipulation of the needle are mediated trough higher central nervous system, especially trough the forebrain, and are beneficial to relieve chronic pain by inhibiting sympathetic nervous activity, through descending pathways on autonomic nervous system.10 A great number of human neuroimaging studies, dramatically increased since 2000, have reported cerebral hemodynamic responses in the somatosensory and motor areas, basal ganglia, cerebellum and limbic system during acupuncture stimulation at acupoints, compared to stimulation at nonacupoints,11 with a strong relationship between decrease of the hemodynamic responses in the medial pre-frontal cortex (mPFC), anterior and posterior cingulate cortex, amygdala, hippocampus and parahippocampus, hypothalamus, parasympathetic activity measured by heart rate variability (HRV) and the de-qi sensation, while it has been shown an increase activity in the insular cortex.12,13 Comparing with the “acupoint-brain-organ theory“ these studies have confirmed that acupuncture recruits brain networks involved in the integration of multiple brain functions: the limbic-paralimbic-neocortical network, which plays a major role in modulating the affective dimensions of pain processing and the integration of emotion, sensorimotor, autonomic and immunological functions:14 the autonomic nervous system activity changes are induced, trough de-qi sensation, by the deactivation of several emotional areas in the higher brain, instead of a somato-autonomic reflex involving the brainstem. Indeed, acupuncture may mediate its effects on pain, anxiety and stress-related diseases via deactivation of the limbic-paralimbic-neocortical circuits, brain areas that are overlapping with the “default mode network” (DMN), which is also recruit by acupuncture stimuli.15,16 As seen, in the western medical research concerning the mechanism able to explain the therapeutical effect of acupuncture, the majority of models are based on the systemic mechanism involving the nervous system, but there isn’t a global overlap between the anatomy of the peripheral nervous system and the distribution of the “channels” described in the TCM. In addition, two experimental studies have shown different functional magnetic resonance imaging (fMRI) activation pattern in the brain induced by stimulation of different acupoints in the same spinal segment, while acupoints on the same “channel” had shown similar activation/deactivation patterns, although non belonging to the same spinal segment.17,18 On this basis it seems that the neurophysiological model is only a partial explanation to address the whole mechanism of action of acupuncture: in the next paragraph I propose a review of the literature regarding the “fascial network hypothesis of meridian” as a more integrated model useful for this purpose.
From fascial network hypothesis of meridians to fascial neuromodulation
According to the recent “task force” Fascia Nomenclature Committee (FNC) of the Fascia Research Society (FRS)19, in the fascial system definition they’re flowing morphological and functional properties of the connective tissue, related to a “network interacting, interrelated, interdependent tissue forming a complex whole, all collaborating to perform movement”.20 The definition ultimately proposed is: “three-dimensional continuum of soft, collagen-containing, loose and dense fibrous connective tissue that permeate the body…such us adipose tissue, adventitiae and neurovascular sheaths, aponeuroses, deep and superficial fascia, epinerium, joint capsules, ligaments, membranes, meninges, myofascial expansions, periostea, retinacula, septa, tendons, visceral fasciae, and all the intramuscular and intermuscular including endo-/peri-/epimysium. The fascial system interpenetrate and surrounds all organs, muscles, bones and nerve fibers, endowing the body with a functional structure, and providing an environment that enables all body systems to operate in an integrated manner”.21 According toTCM, acupuncture points are linked together in a network of “channels” through with flows “meridian qi”22 and, despite the definition of this “channels” remains elusive (NHI Consensus Statement 1997), there are several studies supporting the anatomical and functional correspondence between the meridians network and the fascial system network.23-27 In one of these papers23 the Authors proposed a model of anatomical and physiological equivalents between TCM and the so called “Fasciology”, related to yin-yang doctrine28, suggesting relationship between: meridians and connective tissue plan, acupuncture points and convergence of connective tissue plan, qi and energetic phenomena, (including movement, metabolism, signaling and information exchange), meridian qi and biochemical/bioelectrical signaling trough the connective tissue. Ancient acupuncture texts describes 12 principal meridians running longitudinally along the surface of the body, as well as deep internal branch of each meridian, reaching internal organs, and many other systems of meridians, connecting the whole body as an integrated sum of physiological, physical and emotional functions.22 It has been proposed that mechanical signaling through the connective tissue, and the transmission of the matrix deformation along the fascial system network, can explain the therapeutic effect of acupuncture.29 There is a relationship between the “needle grasp” phenomena, which follow the contraction of fibroblast surrounding the needle after manipulation, and the “de-qi” sensation with it’s propagation along the channel, which is consistent with the stimulation of the sensory mechanoreceptors and with the wave of stimulation along the planes of connective tissue filaments.23 The downstream effect induced by this matrix deformation, including activation of signalling-transduction pathways, cellular polymerization and changes in gene expression, with effects on blood flow and cytokines synthesis, may result in a long-term modulation of the activity of sensory afferents inside the connective tissue (whose sensitization is involved in many chronic diseases, such us neurogenic inflammation and chronic pain) and/or changes in central synapses, indeed in a neuromodulation cascade that follows the processing of the mechanical sensory stimuli.23 A model that involves signal transduction through connective planes, with secondary involvement of neurophysiological mechanism explaining the effect of acupuncture, is very similar to the ancient TCM model, and it is also compatible the proposed neurophysiological model. The TCM model’s description of the so-called “Biao-Li connection” between the skin and deeper structure of the whole body, operated by the 15 “Luo channels”, that run in the “space between skin and muscles”22 is consistent with some recent suggestion concerning the neuroanatomical organization of the free endings fibers, located in the membranous layer of the superficial fascia, and connected with deeper physiological substrates that regulate the homeostatic emotions and the sympathovagal balance.30 These interoceptive unmyelinated afferents, with a very low mechanical threshold, represent about the 80% of the afferent nerves.31,32 The fMRI studies revealed that stimulation of these fibers results in activation of the insular cortex instead of the primary somatosensory cortex, after taking synapses in the lamina I, strongly connected with the sympathetic cell columns, and in the parabrachial nucleus of the brainstem, strongly associated with the activity of amygdala and hypothalamus.33-38 The anterior limbic insular cortex is linked in an emotional network with the cingulate cortex, for the motor and behavioral expression of emotions, and for self-recognition.39 These studies strongly confirm the neuromodulation property of the mechanical stimulation of the fascial tissue, not only induced by acupuncture, but also trough manual therapy, (such as in shiatsu, tuina massage, fascial manipulation and osteopathy), because of the fascial receptivity to pressure31,32 and the role of the touch into the interoceptive and limbic pathways, including the default mode network. 40-43
Table 1.
Extraordinary vessels and master points.
| CV - | LU7 | YinHV - | KI6 |
| TV - | SP4 | YinLV - | PC6 |
| GV + | SI3 | YangHV + | BL62 |
| BV + | GB41 | YangLV + | TE5 |
Clinical application for stress and posture: a proposal for a postural neuromodulation protocol
The term “posture” indicates the position of the body in space and has the purpose of maintaining the body in balance, during the dynamic movements and stasis. Several factors contribute to the posture, including neurophysiological, biomechanical and psychoemotive factors, linked to the evolution of the species.44,45 Posturology is the way to study the posture fromdifferent points including: a neurophysiological model, based on the study of postural tone and balance functions; a biomechanical model, that analyzes the relationship between body attitudes and gravity and that studies the organization of the myofascial chains in relation to complex mechanisms antigravity; a psychosomatic model,36 that analyzes the relationship between the defense and adaptive function of myofascial chains to environmental stress during childhood.46,47 I believe that neurophysiological and biomechanical aspects of the posture are not distinguishable from the emotional development of the character,48 because of the role that the stress system plays in regulating body physiology in a survival function and its capability to induce brain plasticity.49-52 I believe that the global phenomen of “posture” represent the sum of the emotional, physiological and muscular adaptation to the external (gravity) and internal load during the early stages of life.
According to the postural myofascial sequences acting on sagittal, frontal and transverse planes described from Stecco,27 I like to distinguish three different typology based on the three-dimensional synchronic adaptation of the myofascial chains, trough chronic tone increase, to a specific childhood distress: 1. an asymmetrical hypertone of deep chains consequent to a deficiency of skin-to-skin contact and breast feeding during the first year of life, in the so-called “schizo-oral character”. 2. an hypertonic anteropulsion, mediopulsion and intrarotation sequences like a consequence of a continuous punitive distress, in the so-called “masochist character”; and 3. an hypertone in retropulsion, lateropulsion and extrarotation sequences in the case of a continuous boost to the competition, in the so-called “narcissist character”. Some studies have reported balance and postural changes after acupoints stimulation53-56and authors have compared myofascial chains with TCM’s “ordinary meridians”.24,27,57 On the basis of the posture definition suggested above, in this proposal I would like to suggest that myofascial postural sequences described from Stecco27 are better represented by TCM “extraordinary vessels” instead of the “ordinary meridians”. According to TCM, “extraordinary vessels” represent a complex network regulating and integrating the “ordinary channels”, having functions of “balance left and right, up and down, front and back, inside and outside of the whole body”.58 “Extraordinary vessels” are frequently used to the treat at the same time neurological, psycho-emotional and muscular diseases, and the constitutional issue of the patient, because they represent the deep expression of the emotional history and of the character style, with his self-defense mechanism, that follows all the childhood experiences shaping the personal way of adapting to the evolutionary stress: it has been proposed that treatment based on “extraordinary vessels” can increase self-recognition.59 According to TCM theory, “if the ordinary channels are like rivers running through the body, the extraordinary channels represent the tiny currents of water that run between the grains of the soil and between the roots of plants”.60 Indeed, like the postural myo-fascial sequences (Stecco’s definition) influence the single myo-fascial units (Stecco’s definition), “extraordinary channels” are a separate system that influences the ordinary channels, even in terms of fetal neuroembryologic development: they are the original vessels during gestation, existing from the moment the first cell divides60, being proven to exist by 8 week post conception61, and ending their development at 7 years old, when ordinary channels start to been structured.62 The ontogenetic development of the “extraordinary meridians” appears strongly closed with the development of proprioceptive sensibility and with the training stages of character described above. Others links between “extraordinary vessels theory” and the psychosomatic interpretation of the posture like described above are represented by their role on controlling muscular chains on the respect of their emotional and adaptive functions. For example the channel called “thoroughfare vessel chong mai TV” is linked with ancestral muscles, such us the rectal abdomen, the iliopsoas and the spinal muscles, but has a branch reaching the eyes and a descending branch reaching the feet, that are both crucially addressed in posturology.45,48 Also the so-called “belt vessel dai mai BV” channel has an action on ancestral muscles, but it’s used to relieve tensions on the lateral muscles of the legs, like the “yin heel vessel yinqiao mai YinHV” and “yang heel vessel yangqiao mai YangHV” vessels, that control the tone of the intrarotation and extrarotation muscles of the legs, respectively.58 In my proposal there it’s an overlap between postural sequences describes by Stecco27 and the “extraordinary vessels”: anteropulsion relates to the “conception vessel ren mai CV”, retropulsion with “governor vessel du mai GV”, mediopulsion with “yin link vessel yinwei mai YinLV”, lateropulsion with “yang link vessel yangwei mai YangLV”, intrarotation with “yin heel vessel yinqiao mai YinHV” and extrarotation with “yang heel vessel yanqiao mai YangHV”; while “thoroughfare vessel chong mai TV” and “belt vessel dai mai BV” both have an action on the ancestral muscles linked at the vertebral column. How to use “extraordinary vessels”? According to TCM, there are 8 “extraordinary vessels”, 4 characterized by a negative polarity “yin” (-) and 4 by a positive polarity “yang” (+) and there are 8 “master point”, one for each channel, that “opens the whole channel”.58 These channels are never used alone but always coupling 2 “master point” opening channels because of an overlap of areas influenced by 2 channels; the coupling can been chose between channels with the same polarity or with opposite polarity, like in Table 1. Figures 1 and 2 (reproduced with permission from Marcelli S. Daily qi-flow circuit)63 show the course of the eight extraordinary channels, the acupoints from which they are composed, their master points and the associated points with same polarity. How can we choose coupling combination to respect an action on the three-dimensionality of the standing posture and together in relationship with the emotional representation of the posture? It has been proposed that the couple “CV and YinHV” is related with the psychological tendency to “carry a weight” and with an exaggerated sense of responsibility, such us in “masochist character”, while the couple “GV and YangHV” is related with an explosive self-affirmation, like in the “narcissist character”.62 Indeed, the classification proposed above in 3 different typologies can be helpful for this understanding. In the so-called “masochist character”, basing on the relationship with muscular sequences seen above, we can pair all the “yin channels” together as follows: KI6 Zhaohai and LU7 Lieque bilateral, SP4 Gongsun and PC6 Neiguan bilateral, working, at the same time, on the anteropulsion, mediopulsion and intrarotation sequences. In the “narcissist character” we can couple all the “yang channels” as follows: BL62 Shenmai with SI3 Houxi bilateral, and GB41 Linqi Piede with TE5Waiguan bilateral. In the so-called “schizo-oral character” we can combined couple presenting same polarity together with couple characterized by opposite polarity, choosing the “master points” based on the asymmetrical hypertone of the sequences on the three space plans, but coupling the feet points with the arm point presenting same polarity in the contralateral arm, useful to have an action on the torsional chains.
Fig 1.
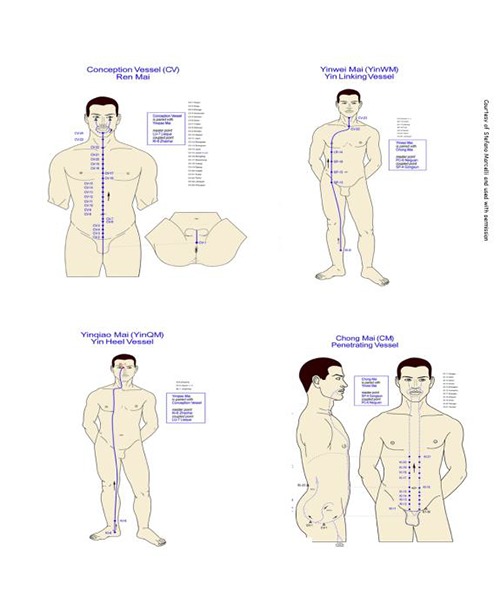
Course of the eight extraordinary channels, the acupoints from which they are composed, their master points and the associated points with same polarity. Reproduced with permission from Marcelli S. Daily qi-flow circuit. Copyright © 2016 www.geneticacupuncture.com
Fig 2.
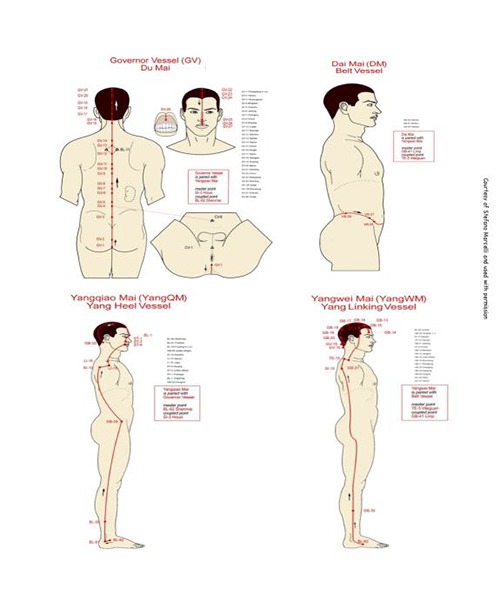
Course of the eight extraordinary channels, the acupoints from which they are composed, their master points and the associated points with same polarity. Reproduced with permission from Marcelli S. Daily qi-flow circuit. Copyright © 2016 www.geneticacupuncture.com
Acknowledgments
The author thanks Fabio Scoppa and Riccardo Cassiani Ingoni for critical discussions of the typescript.
List of acronyms
- DMN
default mode network
- DMV
dorsal motor nucleus of vagal
- EEG
electroencephalographic
- fMRI
functional magnetic resonance imaging
- FNC
Fascia Nomenclature Committee
- FRS
Fascia Research Society
- HRV
heart rate variability
- mPFC
pre-frontal cortex
- Names of meridians and points
according to 1993 World Health Organization Standard Nomenclature
- NHI
National Health Institute
- NTS
nucleus tractus solitarius
- RVLM
rostral ventrolateral medulla
- TCM
Traditional Chinese Medicine
Funding Statement
Funding: No funding was obtained for this research project.
References
- 1.Takahashi T. Mechanism of acupuncture on neuromodulation in the gut - a review. Neuromodulation 2011;14:8-12. doi:10.1111/j.1525-1403.2010.00295.x [DOI] [PubMed] [Google Scholar]
- 2.Li QQ, Shi GX, Xu Q, et al. Acupuncture effect and central autonomic regulation. Evid Based Complement Alternat Med 2013:267959. doi:10.1155/2013/267959 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hui KK, Nixon EE, Vangel MG, et al. Characterization of the "deqi" response in acupuncture. BMC Complement Altern Med 2007. 31;7:33. doi:10.1186/1472-6882-7-33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hori E, Takamoto K, Urakawa S, et al. Effects of acupuncture on the brain hemodynamics. Auton Neu-rosci 2010. 28;157(1-2):74-80. doi:10.1016/j.autneu.2010.06.007 [DOI] [PubMed] [Google Scholar]
- 5.Nishijo K, Mori H, Yosikawa K, Yazawa K. Decreased heart rate by acupuncture stimulation in humans via facilita-tion of cardiac vagal activity and suppression of cardiac sympathetic nerve. Neurosci Lett 1997. 23;227:165-8. [DOI] [PubMed] [Google Scholar]
- 6.Wang JD, Kuo TB, Yang CC. An alternative method to enhance vagal activities and suppress sympathetic activities in humans. Auton Neurosci 2002. 30;100:90-5. [DOI] [PubMed] [Google Scholar]
- 7.Haker E, Egekvist H, Bjerring P. Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. J Auton Nerv Syst 2000. 14;79:52-9. [DOI] [PubMed] [Google Scholar]
- 8.Tracey KJ. The inflammatory reflex. Nature 2002;420(6917):853-9. Doi:10.1038/nature01321. [DOI] [PubMed] [Google Scholar]
- 9.Cho ZH, Hwang SC, Wong EK, et al. Neural substrates, experimental evidences and functional hypothesis of acupuncture mechanisms. Acta Neurol Scand 2006;113:370-7. Review. doi:10.1111/j.1600-0404.2006.00600.x [DOI] [PubMed] [Google Scholar]
- 10.Sakai S, Hori E, Umeno K, Kitabayashi N, et al. Specific acupuncture sensation correlates with EEGs and autonom-ic changes in human subjects. Auton Neurosci 2007;133:158-69. doi:10.1016/j.autneu.2007.01.001 [DOI] [PubMed] [Google Scholar]
- 11.Huang W, Pach D, Napadow V, et al. Characterizing acupuncture stimuli using brain imaging with FMRI - a systematic review and meta-analysis of the literature. PLoS One 2012;7. doi:10.1371/journal.pone.0032960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Takamoto K, Urakawa S, Sakai K, et al. Effects of acupuncture needling with specific sensation on cerebral hemo-dynamics and autonomic nervous activity in humans. Int Rev Neurobiol 2013;111:25-48. Doi:10.1016/B978-0-12-411545-3.00002-X. [DOI] [PubMed] [Google Scholar]
- 13.Sun J, Zhu Y, Yang Y, et al. What Is the de-qi-Related Pattern of BOLD Responses? A Review of Acupuncture Studies in fMRI. Evid Based Complement Alternat Med 2013;2013:297839. doi:10.1155/2013/297839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fang J, Jin Z, Wang Y, et al. The salient characteristics of the central effects of acupuncture needling: limbic-paralimbic-neocortical network modulation. Hum Brain Mapp 2009;30:1196-206. doi:10.1002/hbm.20583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Liang P, Wang Z, Qian T, Li K. Acupuncture stimulation of Taichong (Liv3) and Hegu (LI4) modulates the default mode network activity in Alzheimer's disease. Am J Alzheimers Dis Other Demen 2014;29:739-48. doi:10.1177/1533317514 536600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Long X, Huang W, Napadow V, et al. Sustained Effects of Acupuncture Stimulation Investigated with Centrality Mapping Analysis. Front Hum Neurosci 2016;10:510. doi.org/10.3389/fnhum.2016.00510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhang WT, Jin Z, Luo F, et al. Evidence from brain imaging with fMRI supporting functional specificity of acu-points in humans. Neurosci Lett 2004;354:50-3. [DOI] [PubMed] [Google Scholar]
- 18.Li L, Liu H, Li YZ, et al. The human brain response to acupuncture on same-meridian acupoints: evidence from an fMRI study. J Altern Complement Med 2008;14:673-8. doi:10.1089/acm.2008.0036. [DOI] [PubMed] [Google Scholar]
- 19.Langevin H. Langevin's response to Stecco's fascial nomenclature editorial. J Bodyw Mov Ther 2014;18:444. Doi:10.1016/j.jbmt.2014.04.016. [DOI] [PubMed] [Google Scholar]
- 20.Stecco C, Schleip R. A fascia and the fascial system. J Bodyw Mov Ther 2016;20(1):139-140. doi:10.1016/j.jbmt.2015.11.012. [DOI] [PubMed] [Google Scholar]
- 21.Adstrum S, Hedley G, Schleip R, et al. Defining the fascial system. J Bodyw Mov Ther 2017;21:173-7. doi:10.1016/j.jbmt.2016.11.003. [DOI] [PubMed] [Google Scholar]
- 22.Kaptchuk TJ: Medicina Cinese. Fondamenti e metodo. 1983 Red ed. ristampa 2014. [Google Scholar]
- 23.Langevin HM, Yandow JA. Relationship of acupuncture points and meridians to connective tissue planes. Anat Rec 2002;269:257-65. doi:10.1002/ar.10185. [DOI] [PubMed] [Google Scholar]
- 24.Dorsher PT. Myofascial Meridians as Anatomical Evidence of Acupuncture Channels. Medical Acupuncture 2009;21:2. [Google Scholar]
- 25.Bai Y, Wang J, Wu JP, et al. Review of evidence suggesting that the fascia network could be the anatomical basis for acupoints and meridians in the human body. Evid Based Complement Alternat Med 2011:260510. doi:10.1155/2011/260510 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Maurer N, Nissel H, Egerbacher M, et al. Anatomical Evidence of Acupuncture Meridians in the Human Extracellu-lar Matrix: Results from a Macroscopic and Microscopic Interdisciplinary Multicentre Study on Human Corpses. Evid Based Complement Alternat Med;2019:6976892. doi:10.1155/2019/6976892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stecco L. Fascial manipulation for musculoskeletal pain. Piccin, Padova, Italy: 2004. [Google Scholar]
- 28.Tao H, Yu MC, Yang HY, et al. Correlations between fasciology and yin yang doctrine. J Acupunct Meridian Stud 2011;4:141-6. doi:10.1016/S2005-2901(11)60021-6. [DOI] [PubMed] [Google Scholar]
- 29.Langevin HM, Churchill DL, Cipolla MJ. Mechanical signaling through connective tissue: a mechanism for the therapeutic effect of acupuncture. FASEB J 2001;15:2275-82. doi:10.1096/fj.01-0015hyp. [DOI] [PubMed] [Google Scholar]
- 30.Strigo IA, Craig AD. Interoception, homeostatic emotions and sympathovagal balance. Philos Trans R Soc Lond B Biol Sci 2016;371(1708). doi:10.1098/rstb.2016.0010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Schleip R. Fascial plasticity – a new neurobiological explanation: part 1. Journal of Bodywork and Movement Therapies 2003;7: 11-19. [Google Scholar]
- 32.Schleip R. Fascial plasticity–a new neurobiological explanation: part 2. Journal of Bodywork and Movement Therapies 2003:7:104-16. [Google Scholar]
- 33.Craig AD. How do you feel now? The anterior insula and human awareness. Nat Rev Neurosci 2009;10:59-70. doi:10.1038/nrn2555. [DOI] [PubMed] [Google Scholar]
- 34.Craig AD. Interoception: the sense of the physiological condition of the body. Curr Opin Neurobiol 2003;13:500-5. Review. [DOI] [PubMed] [Google Scholar]
- 35.Davidovic M, Starck G, Olausson H. Processing of affective and emotionally neutral tactile stimuli in the insular cortex. Dev Cogn Neurosci 2019;35:94-103. doi:10.1016/j.dcn.2017.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Liljencrantz J, Olausson H. Tactile C fibers and their contributions to pleasant sensations and to tactile allodynia. Front Behav Neurosci 2014;8:37. doi:10.3389/fnbeh.2014.00037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Björnsdotter M, Morrison I, Olausson H. Feeling good: on the role of C fiber mediated touch in interoception. Exp Brain Res 2010;207:149-55. [DOI] [PubMed] [Google Scholar]
- 38.Olausson HW, Cole J, Vallbo A, et al. Unmyelinated tactile afferents have opposite effects on insular and soma-tosensory cortical processing. Neurosci Lett 2008;436:128-32. doi:10.1007/s00221-010-2408-y. [DOI] [PubMed] [Google Scholar]
- 39.Devue C, Collette F, Balteau E, et al. Here I am: the cortical correlates of visual self-recognition. Brain Res 2007;1143:169-82. doi:10.1016/j.brainres.2007.01.055. [DOI] [PubMed] [Google Scholar]
- 40.Craig AD. Why a soft touch can hurt. J Physiol 2010;588(Pt 1):13. doi:10.1113/jphysiol.2009.185116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Davidovic M, Starck G, Olausson H. Processing of affective and emotionally neutral tactile stimuli in the insular cortex. Dev Cogn Neurosci 2019;35:94-103. doi:10.1016/j.dcn.2017.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Chae Y, Olausson H. The role of touch in acupuncture treatment. Acupunct Med 2017;35: 148-152. doi:10.1136/acupmed-2016011178. [DOI] [PubMed] [Google Scholar]
- 43.Strauss T, Kämpe R, Hamilton JP, et al. Deactivation of default mode network during touch. Sci Rep 2019;9(1):1293. doi:10.1038/s41598-018-37597-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Scoppa F. Posturology: from nonlinear dynamics to transdisciplinarity. Otoneurologia 2000;15:28–48. [Google Scholar]
- 45.Carini F, Mazzola M, Fici C, et al. Posture and posturology, anatomical and physiological profiles: overview and current state of art. Acta Biomed 2017;88:11-16. doi:10.23750/abm.v88i1.5309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Scoppa F. Posturology: the neurophysiological model, the biomechanical model, the psychosomatic model. Otoneurologia 2002;9:3–13. [Google Scholar]
- 47.Traetta T. Caratterologia. Armando Editore, Italy: 2009. [Google Scholar]
- 48.Lowen A: Bioenergetica. Feltrinelli Edizioni, Italy: 2004. [Google Scholar]
- 49.Selye H. Stress and the general adaptation syndrome. Br Med J 1950;1(4667):1383-92. doi:10.1136/bmj.1.4667.1383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Chrousos GP. The hypothalamic-pituitary-adrenal axis and immune-mediated inflammation. N Engl J Med 1995;332:1351-62. Review. doi:10.1056/NEJM199505183322008. [DOI] [PubMed] [Google Scholar]
- 51.McEwen BS. Protective and damaging effects of stress mediators. N Engl J Med 1998;338(3):171-9. Review. doi:10.1056/NEJM199801153380307 [DOI] [PubMed] [Google Scholar]
- 52.McEwen BS. The Brain on Stress: Toward an Integrative Approach to Brain, Body, and Behavior. Perspect Psychol Sci 2013;8:673-5. doi:10.1177/1745691613506907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Huang SW, Wang WT, Yang TH, et al. The balance effect of acupuncture therapy among stroke patients. J Altern Complement Med 2014;20:618-22. doi:10.1089/acm.2014.0003. [DOI] [PubMed] [Google Scholar]
- 54.Gallamini M. Treating balance disorders by ultra-low-level laser stimulation of acupoints. J Acupunct Meridian Stud 2013;6:119-23. doi:10.1016/j. jams.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 55.Scoppa F, Gallamini M, Belloni G. Treating Balance Disorders with Ulllt Acupuncture Stimulation: A Further Pilot Study on Normal Subjects Confirms Clinical Applicability of Treatment. J Nov Physioter. 2016,6:285. [Google Scholar]
- 56.Scoppa F, Bergamaschi M, Ferrari G, Gallamini M, Laser Acupuncture and Auriculotherapy in Postural Instability – A Preliminary Report. J Acupunct Meridian Stud 2011;4:69-74. [DOI] [PubMed] [Google Scholar]
- 57.Stecco L. Agopuntura Medicina Occidentale Manipolazione Fasciale. Piccin Nuova Libraria, Padova, Italy: 2019. [Google Scholar]
- 58.Maciocia G. The Channels of Acupuncture. Churchill Livingstone, 2006. [Google Scholar]
- 59.Farrel YR. Psyco-emotional pain and the eight extraordinary vessels. Singing Dragon, 2016. [Google Scholar]
- 60.Keown D. The spark in the machine. Singing Dragon, 2014. [Google Scholar]
- 61.Dorsher PT, Chiang P. Neuroembryology of the Acupuncture Principal Meridians: Part 3. The Head and Neck. Med Acupunct 2018;30:80-8. doi:10.1089/acu.2018.1271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Bottalo F. Manuale di Xi Shu. Xenia Edizioni, 2017. [Google Scholar]
- 63.Marcelli S. Daily qi-flow circuit. App for smartphone. https://www.geneticacupuncture.com/allacupoints/all-the-names-of-the-acupuncture-points-LINKED.htm [Google Scholar]