

Abstract
We previously hypothesized that the ubiquitous, but patterned correlations among all dimensions of psychopathology reflect a hierarchy of progressively more nonspecific causal influences, with a general factor of psychopathology—also dubbed the p factor—reflecting the most transdiagnostic causal influences. We further hypothesized that the general factor is a manifestation of individual differences in one or more trait-like dispositions, particularly negative emotionality, that are nonspecifically associated with risk for essentially every dimension of psychopathology. We tested the hypothesis that this and other dispositions measured in childhood/adolescence significantly predict general and specific second-order dimensions of psychopathology in early adulthood. The latent general factor of psychopathology itself was correlated over time from 10–17 to 23–31 years of age even though it was defined by different informants and different dimensions of symptoms. Using a measure of dispositions that minimizes item contamination with psychopathology symptoms, parent-rated negative emotionality in childhood and adolescence predicted the general factor of psychopathology based on self-reported symptoms in early adulthood, whereas parent-rated daring predicted the specific adult externalizing psychopathology factor after correction for multiple tests. In addition, youth-rated negative emotionality and daring predicted specific adult externalizing psychopathology. These results over a span of 12 years suggests that the general factor is relatively stable over time and that associations of dispositional traits with second-order dimensions of psychopathology are enduring, sometimes across informants.
Keywords: negative emotionality, daring, prosociality, general factor, p factor, psychopathology
General Scientific Summary:
Over a span of 12 years, parent-rated negative emotionality during childhood and adolescence predicted the general factor of psychopathology and specific externalizing psychopathology during adulthood. The psychobiological processes associated with parent-rated negative emotionality may constitute one of the mechanisms underlying the general factor of psychopathology.
We hypothesized that a general factor of psychopathology, defined by the correlations among every form of psychopathology, arises from broadly shared causes and mechanisms (Lahey et al., 2012; Lahey, Krueger, Rathouz, Waldman, & Zald, 2017; Lahey, Van Hulle, Singh, Waldman, & Rathouz, 2011). If supported, this hypothesis will require a reconceptualization of the causal structure of psychopathology, as it implies that there are important nonspecific causes that increase the risk for any form of psychopathology in addition to factors that increase risk for specific forms of psychopathology.
Bifactor models including a general factor, also called the p factor (Caspi et al., 2014), often fit better than correlated-factors models that estimate only second-order factors such as internalizing and externalizing psychopathology (reviewed by Lahey et al., 2017). Nonetheless, because fit statistics do not reliably distinguish substantively different models with similar fits to the data, it is necessary to choose among alternative models on the basis of their scientific utility and criterion validity—associations with independently measured external variables not used to define the general factor (Bonifay, Lane, & Reise, 2017).
There is growing evidence of the criterion validity of the general factor across the life span. In a longitudinal study of a large sample of Swedish twins, the general factor estimated in childhood predicted independently measured adverse clinical and social outcomes during adolescence over and above the specific internalizing and externalizing factors (Pettersson, Lahey, Lundström, Larsson, & Lichtenstein, 2018). In cross-sectional studies, scores on independent tests of intelligence and executive functions are inversely associated with the general factor (Caspi et al., 2014; Castellanos-Ryan et al., 2016; Huang-Pollock, Shapiro, Galloway-Long, & Weigard, 2017; Lahey et al., 2015; Martel et al., 2017). Additionally, the general factor of psychopathology is correlated with independently measured single nucleotide polymorphisms (SNPs) (Jones et al., 2018; Neumann et al., 2016). Moreover, patterns of SNP-based genetic correlations across disorders support the hypothesis of broadly pleiotropic genetic influences shared through the general factor (Docherty et al., 2017; Smoller et al., 2018). There also is evidence that the general psychopathology factor may be associated with variations in brain structure and function (Kaczkurkin et al., 2017; Ricardo Sato et al., 2016; Romer et al., 2018; Snyder, Hankin, Sandman, Head, & Davis, 2017).
Given this evidence of criterion validity, a next task is to discover the psychological and biological nature of the general factor. Here we elucidate the nature of the general factor by examining prospective associations between negative emotionality and the general factor of psychopathology. Cross-sectional studies have found that negative emotionality/neuroticism is correlated with almost every form of psychopathology (Krueger & Tackett, 2003; Lahey, 2009; Widiger & Oltmanns, 2017), broadly shares genetic influences with multiple forms of psychopathology (Khan, Jacobson, Gardner, Prescott, & Kendler, 2005), and is robustly associated with the general psychopathology factor in childhood and adolescence at phenotypic (Caspi et al., 2014) and genetic levels (Tackett et al., 2013). Thus, it is likely that the general factor partly reflects variations in negative emotionality.
No studies have yet examined prospective associations between child/adolescent dispositions and the general factor in adulthood. Indeed, it is not yet clear that the general factor of psychopathology is the same construct when defined at different periods of development (Lahey et al., 2017). Therefore, findings that the general factor defined in childhood and in adulthood is stable over time and associated with the same dispositions would provide important evidence on the possible continuity of the general factor across development.
Importantly, several theorists have hypothesized that variation in child temperament influences the likelihood of developing future psychopathology (Caspi, Henry, McGee, Moffitt, & Silva, 1995; Thomas & Chess, 1957). Support for this hypothesis comes from longitudinal studies that demonstrate significant predictive correlations between measures of infant and child temperament and later psychopathology. One possible explanation of such predictive correlations is that individual differences in child temperament transact with their environments to both (1) influence the likelihood of adaptive and maladaptive experiences, (2) and moderate the child’s responses to such experiences (Bell, 1977; Belsky & Pluess, 2009; Sameroff, 2009). This hypothesis has received support from studies that have, for example, found interactions between child temperament and parenting styles (Overbeek, 2017; Slagt, Dubas, Dekovic, & van Aken, 2016), stress (Schermerhorn et al., 2013), and family transitions (Ruschena, Prior, Sanson, & Smart, 2005) in predicting future psychopathology.
Nonetheless, three issues limit the value of findings from previous prospective studies of dispositions and later psychopathology:
The intervals of time covered have been relatively short and have not extended from childhood into adulthood.
Psychopathology outcomes measured in previous prospective studies have been limited to a narrow range of problems.
Previous studies of the association between measures of dispositions and psychopathology were confounded in two important ways. First, many previous studies used parent ratings of both dispositions and outcomes, raising the possibility that correlations reflect only common method variance. Exceptions involve the use of observational measures of dispositions and independent measures of later psychopathology (Biederman et al., 2001), but this has not been common. Second, many items in the measures of dispositional traits used in these studies are synonyms or antonyms of symptoms of psychopathology, raising concerns that any predictive correlations are artifacts of item contamination (Lahey, 2004). One solution to the latter problem has been to delete overlapping items from existing scales (Lemery, Essex, & Smider, 2002; Lengua, West, & Sandler, 1998). This changes the disposition scales, however, and it is not clear if previous psychometric properties the scales apply or, indeed, what the reduced scales measure.
In the present study, we use a dispositional scale developed from the outset without items that overlap with symptoms of psychopathology (Lahey, Applegate, et al., 2008; Lahey, Rathouz, Applegate, Tackett, & Waldman, 2010). Thus, unlike general-purpose measures of temperament and personality (Rothbart, Ahadi, Hershey, & Fisher, 2001; Shiner & Caspi, 2003; Simonds, Kieras, Rueda, & Rothbart, 2007), the Child and Adolescent Dispositions Scale (CADS) does not measure dispositions that are also considered dimensions of psychopathology when extreme. For example, the CADS does not assess effortful control (Simonds et al., 2007) because the defining items are mostly antonyms of the symptoms of attention-deficit/hyperactivity disorder. Similarly, positive emotionality is not measured because most defining items are antonyms of dysphoria and anhedonia.
Negative emotionality is operationalized in the CADS by items tapping frequent and intense responses to frustrations, losses, and threats with any kind of negative emotions. It is conceptually similar to the constructs of negative affectivity (Rothbart et al., 2001) and neuroticism, which is known to be correlated with essentially every form of psychopathology (Lahey, 2009; Widiger & Oltmanns, 2017). Although CADS negative emotionality is defined without items that resemble symptoms of psychopathology, youth-rated CADS and neuroticism measured by the NEO-FFI (Costa & McCrae, 1992) correlate moderately (r = .48, p < .0001) at age 12 years (Lahey et al., 2010). The prosociality scale quantifies caring about others, attempting to please them, and guilt over misbehaviors. Prosociality is a widely studied construct (Knafo-Noam, Uzefovsky, Israel, Davidov, & Zahn-Waxler, 2015) that is similar to dispositional sympathy (Murphy, Shepard, Eisenberg, Fabes, & Guthrie, 1999) and can be viewed as the inverse of callousnesss (Frick, Ray, Thornton, & Kahn, 2014; Lahey, 2014; Waldman et al., 2011). Children rated high on the CADS daring scale find intense and risky situations to be attractive and rewarding. Daring is related to the constructs of sensation-seeking (Russo et al., 1993; Zuckerman & Aluja, 2015) and low harm avoidance (Luby, Svrakic, McCallum, Przybeck, & Cloninger, 1999).
The present prospective study examines the extent to which CADS dispositions measured in childhood/adolescence predict general and specific higher-order dimensions of psychopathology 12 years later in adulthood. These tests control for demographic factors to minimize the possibility that dispositions and psychopathology are correlated solely because both are related to sociodemographic disadvantage (Lahey, 2015). If future research determines that some dispositional traits are causally related to the origins of psychopathology, prevention and intervention efforts targeting dispositional factors in youth may reduce rates of later psychopathology (Barlow, Sauer-Zavala, Carl, Bullis, & Ellard, 2014).
METHOD
Participants and Procedures
Participants were selected from the Wave 1 of the Tennessee Twin Study (TTS) (Lahey, Rathouz, et al., 2008) for the Wave 2 evaluation 10–15 years (median = 12 years) later. All participants provided consent/assent.
Wave 1 Sample
The Wave 1 sample is representative of 6–17 year-old twins in Tennessee’s five metropolitan statistical areas (MSAs) in 2000–2001. The Tennessee Department of Health identified all twin pairs born in Tennessee in the eligible age range; 2431 twin pairs were eliminated because they lived outside an MSA. A random sample was selected from the remaining families, stratified by age and geographic subareas, proportional to the number of families. Of 4012 selected households, 3592 (89.5%) were located and screened, with 2646 of screened families being eligible (co-residence with the caretaker at least half time during the past 6 months and twins and caretakers spoke English). Interviews were completed with 2,063 adult caretakers (90.8% biological mothers), with a 70% response rate. When caretakers were interviewed, 98% of both twins were interviewed. After excluding pairs in which either twin had been given a diagnosis of autism, psychosis, or seizure disorder, the sample consisted of 3,990 twins in 1,995 complete pairs. Caretakers classified 71% of the twins as non-Hispanic white, 24% African American, 2% as Hispanic, and 3% as other groups.
Wave 1 Measures
The CADS is a reliable and well-validated measure of three dispositions (Lahey, Applegate, et al., 2008; Lahey et al., 2010) (Lahey et al., 2004). Items are rated on a 1 (not at all) to 4 (very much) response scale in interviews, separately by parents and youth (Piacentini, Cohen, & Cohen, 1992). The CADS was originally developed to study antisocial behavior (Lahey & Waldman, 2003), with antisocial behavior predicted to be associated positively with negative emotionality and daring and inversely with prosociality. These CADS dimensions correlate with conduct disorder cross-sectionally (Lahey, Applegate, et al., 2008; Lahey et al., 2010; Taylor, Allan, Mikolajewski, & Hart, 2013) and prospectively predict adolescent antisocial and risky behavior (Shaw, Hyde, & Brennan, 2012; Sitnick, Brennan, Forbes, & Shaw, 2014; Trentacosta, Hyde, Shaw, & Cheong, 2009), and adult antisocial personality disorder (Lahey, Class, et al., 2018).
Cross-sectional analyses also found that CADS negative emotionality was associated with symptoms of both depression and anxiety disorders within and across informants (Lahey, Applegate, et al., 2008). Additionally, CADS negative emotionality shares phenotypic and genetic variance with both internalizing and externalizing psychopathology defined in a correlated-factors model (Mikolajewski, Allan, Hart, Lonigan, & Taylor, 2013). Furthermore, CADS daring is inversely associated with anxiety within and across informants (Lahey, Applegate, et al., 2008).
Wave 2 Sample
Twin pairs for Wave 2 assessments were recruited in four replicates in reverse order of their age in Wave 1 (16–17, 14–15, 12–13, and 10–11 years) to minimize the age distribution in Wave 2. Twin pairs were eligible if the last known address of both twins was within 300 miles of Vanderbilt University (95.2% of twins). Wave 2 replicates were selected by oversampling on Wave 1 psychopathology scores based on the greater rating of each symptom from the parent or youth. High-risk pairs were selected with certainty if either twin had symptom ratings on the total number of internalizing, attention-deficit/hyperactivity disorder, or the combination of ODD and CD symptoms in the top 10% of that age range. In addition, 19–23% of the remainder of each replicate was randomly selected with two constraints: (1) monozygotic pairs were oversampled by randomly excluding 40% of the randomly selected dizygotic pairs, and (2) the number selected from the remainder of the sample varied slightly to equate replicate sizes (100–105 pairs).
Three pairs of twins could not be located and 37 pairs refused screening. Eighteen selected pairs of twins across replicates were declared out of scope due to previous participation in a pilot study, mental or physical incapacity, residence outside the U.S., imprisonment, or death. A total of 114 screened individual twins were ineligible for neuroimaging for feasibility (e.g., body weight) and safety reasons, but were eligible for assessment of psychopathology. Interviews regarding psychopathology were completed for 72% of the screened sample during 2013–2016, including 248 complete twin pairs (49.6% monozygotic; 66.9% high risk) and 3 individuals without their twin. The 499 interviewed participants were 23–31 years of age (median 26 years); 52.1% female; and self-identified as 71.5% Non-Hispanic white, 25.2% African American, and 3.2% other racial-ethnic groups.
Wave 2 Measures
Assessments were conducted at Vanderbilt University before neuroimaging or by telephone for scan-ineligible participants. Diagnostic and Statistical Manual, Fifth Edition (DSM5) symptoms were assessed using the young adult version of the Diagnostic Interview for Children (YA-DISC) (Abram et al., 2015; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000; Witkiewitz et al., 2013). The modules used in these analyses queried diagnostic criteria for adult attention-deficit/hyperactive disorder (ADHD), major depressive disorder (MDD), generalized anxiety disorder (GAD), post-traumatic stress disorder (PTSD), agoraphobia, panic attacks, social phobia, specific phobia, manic episodes, obsessive-compulsive disorder (OCD), antisocial personality disorder (APD), and nicotine, alcohol, and marijuana misuse during the last 12 months. Because few skip patterns are in the YA-DISC, the instrument yields measures of the number of symptoms of each dimension of psychopathology even if a participant does not meet full criteria for a DSM5 diagnosis. Nonetheless, questions about abuse and dependence were only administered to those reporting use of the substance. Similarly, questions regarding symptoms of PTSD in the past year were only administered to participants who reported a traumatic event that they thought about during the last year. All GAD symptoms were queried only if the participant reported the cardinal symptom of frequent worry for at least 6 months in a row during the last year and were asked in the context of “when you were worried.” Therefore, not all possible PTSD, GAD, and substance use symptoms could contribute to symptom counts. Although participants were asked about all symptoms of depression, contingent questions used to set a threshold for the presence of each symptom based on frequency and duration were asked only for persons reporting dysphoria and anhedonia, which may have resulted in higher prevalence of endorsed depression symptoms.
Statistical Analyses
Analyses performed using Mplus 8.1 (Muthén & Muthén, 2018) accounted for stratification and clustering with twin pairs and used weights to account both for the inverse of the probability of participation in Wave 2 based on selection and for nonresponse. These weights corrected any biases due to nonresponse relative to demographic characteristics and Wave 1 measures of psychopathology, dispositions, and working memory. These weights allow valid parameter estimates when weighted back to the full Wave 1 TTS sample (Korn & Graubard, 1999). Similar weights were used in analyses for a previously published paper on the measurement of the general factor of psychopathology (Lahey, Zald, et al., 2018); here the weights were updated by including maternal education and replacing two measures of working memory with a composite measure of working memory. Correlations among these weights and among the resulting standardized factor loadings in the psychopathology measurement models were r = >0.99.
Primary Analyses
Correlated-factors measurement model.
The CADS dispositions were first regressed on latent factors of internalizing and externalizing psychopathology defined in a correlated-factors measurement model (not including a general factor). The specific internalizing factor was defined by agoraphobia, GAD, PTSD, specific phobia, social phobia, OCD, depression, and mania. The specific externalizing factor was defined by alcohol, marijuana, nicotine, APD, inattentive, hyperactive/impulsive, and mania symptom counts. This measurement model used fixed nonstandardized loadings from a separate CFA based on Lahey, Zald, et al., (2018).
Bifactor measurement model.
The bifactor measurement model was based on the best-fitting model presented previously (Lahey, Zald, et al., 2018). In new CFAs using updated weights, all 14 psychopathology dimensions were allowed to load freely on the general factor. The specific internalizing and externalizing factors were defined as in the correlated-factors model except that mania loaded only on the general factor. Correlations among the general factor and specific internalizing and externalizing factors were set to zero (Brown, 2006). Thus, the general factor was defined by the common variance across all symptom dimensions, whereas the specific internalizing and externalizing factors reflected residual covariance among the internalizing and externalizing dimensions when the general factor was modelled.
SEMs.
To use the same correlated-factors or bifactor measurement models in each regression analysis, nonstandardized factor loadings were fixed in the psychopathology measurement models of all structural equation models (SEMs) based on the CFA measurement models. In separate SEMs for each CADS informant for each measurement model, the psychopathology factors were simultaneously regressed on the three manifest CADS measures of negative emotionality, daring, and prosociality, along with the demographic covariates (sex, age in Wave 1, age in Wave 2, maternal education, log of total family income, and race-ethnicity). Maximum likelihood estimation with robust standard errors (MLR) was used to account for non-normality in the distributions of the first-order symptom dimensions and adjust standard errors. Although the predicted prospective associations between child and adolescent CADS dispositions and latent psychopathology factors in adulthood were based on cross-sectional associations findings for same variables using Wave 1 TTS data (Tackett et al., 2013), we conservatively corrected for multiple testing using a 5% false discovery rate (FDR) applied to two-tailed tests.
Exploratory, Supplemental, and Sensitivity Analyses
We conducted exploratory analyses testing interactions between dispositions and demographic factors. Analyses of the stability of the general factor of psychopathology across childhood/adolescence and early adulthood are described in the text preceding Supplemental Tables S3 and S4. We also conducted sensitivity analyses to examine the extent to which modeling decisions influenced findings. Specifically, we examined our decisions to fix unstandardized loadings in the bifactor psychopathology measurement model in the SEMs (Table S5), to treat counts of psychopathology symptoms as continuous under MLR (Table S6 and S7), and to analyze parent and youth ratings of CADS dispositions separately (Table S8). Analyses were performed by the last author in collaboration with other authors.
RESULTS
Demographic characteristics of participants are presented in Table 1. To describe levels of psychopathology in Wave 2, Table 1 presents the prevalence of 18 DSM-IV categorical mental disorders according to YA-DISC algorithms (Shaffer, Fisher, Piacentini, & Lucas, 2008) by sex. Consistent with oversampling participants based on Wave 1 psychopathology, 50.3% met criteria for at least one Wave 2 mental disorder (46.2% of females; 54.8% of males) in the past year and 26.8% met criteria for ≥ 2 diagnoses. Table S1 also shows that the CADS dispositions were modestly correlated across raters. Frequencies of the numbers of symptoms of each first-order dimension of psychopathology are presented in Table S2.
Table 1.
Demographic characteristics and the prevalence of DSM-IV mental disorders in the sample.
| Characteristic |
|||
| Sex (% female) | 52.1 | ||
| Race-ethnic group (%) | |||
| Non-Hispanic white | 71.5 | ||
| African American | 25.2 | ||
| Other groups | 3.2 | ||
| Monozygotic twin (%) | 49.5 | ||
| Years of education completed (mean, SD) | 14.3 (2.3) | ||
| Still in school (%) | 26.0 | ||
| Age in years (mean, SD) | |||
| Wave 1 | 13.6 (2.5) | ||
| Wave 2 | 26.0 (1.8) | ||
| Diagnoses | Females | Males | Full Sample |
| N = 260 | N = 239 | N = 499 | |
| N (%) | N (%) | N (%) | |
| Specific phobia | 31 (11.9) | 17 (7.1) | 48 (9.6) |
| Agoraphobia | 21 (8.1) | 11 (4.6) | 32 (6.4) |
| Panic disorder | 11 (4.2) | 11 (4.6) | 22 (4.4) |
| Post-traumatic stress disorder | 10 (3.8) | 4 (1.7) | 14 (2.8) |
| Social anxiety disorder | 23 (8.8) | 6 (6.7) | 39 (7.8) |
| Obsessive-compulsive disorder | 15 (5.8) | 15 (6.3) | 30 (6.0) |
| Generalized anxiety disorder | 13 (5.0) | 7 (2.9) | 20 (4.0) |
| Major depression | 22 (8.5) | 17 (7.1) | 39 (7.8) |
| Dysthymia | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Attention-deficit/hyperactivity disorder | 7 (2.7) | 11 (4.6) | 18 (3.6) |
| Alcohol abuse | 25 (9.6) | 48 (20.2) | 73 (14.7) |
| Alcohol dependence | 8 (3.1) | 20 (8.4) | 28 (5.6) |
| Cannabis abuse | 13 (5.0) | 27 (11.3) | 40 (8.0) |
| Cannabis dependence | 5 (1.9) | 12 (5.0) | 17 (3.4) |
| Nicotine dependence | 20 (8.1) | 27 (12.3) | 47 (10.1) |
| Antisocial personality disorder | 15 (5.8) | 48 (20.1) | 63 (12.6) |
| Hypomania | 5 (1.9) | 6 (2.5) | 11 (2.2) |
| Mania | 1 (0.4) | 1 (0.4) | 2 (0.4) |
Results Based on the Correlated-Factors Model of Psychopathology
Parent-rated CADS negative emotionality significantly predicted both the internalizing and externalizing factors defined in the correlated-factors model after FDR correction (Figures S1 and S2 and Table 2). Youth-rated CADS negative emotionality significantly predicted internalizing psychopathology and youth-rated prosociality significantly predicted externalizing psychopathology after FDR correction.
Table 2.
Standardized regression coefficients when internalizing and externalizing dimensions of psychopathology measured at 23–31 years of age were defined in a separate correlated-factors model and simultaneously regressed on CADS dimensions of daring, negative emotionality, and prosociality measured at 10–17 years of age and demographic covariates.a Separate models were fitted for CADS ratings by parent and youth informants (N = 499).
| Parent-rated CADS dispositions | ||||
| Estimate | Standard Error | 95% Confidence Interval | p < | |
| Response variable: Internalizing factor of psychopathology | ||||
| Daring | −0.088 | 0.055 | −0.196 – 0.020 | 0.108 |
| Negative emotionality | 0.163 | 0.057 | 0.051 – 0.275 | 0.004 |
| Prosociality | −0.037 | 0.065 | −0.164 – 0.090 | 0.568 |
| Response variable: Externalizing factor of psychopathology | ||||
| Daring | 0.022 | 0.064 | −0.103 – 0.147 | 0.724 |
| Negative emotionality | 0.228 | 0.062 | 0.106 – 0.350 | 0.000 |
| Prosociality | −0.118 | 0.057 | −0.230 - -0.006 | 0.040 |
| Youth self-rated CADS dispositions | ||||
| Estimate | Standard Error | 95% Confidence Interval | P < | |
| Response variable: Internalizing factor of psychopathology | ||||
| Daring | −0.049 | 0.096 | −0.237 – 0.139 | 0.613 |
| Negative emotionality | 0.127 | 0.048 | 0.033 – 0.221 | 0.008 |
| Prosociality | −0.139 | 0.074 | −0.284 – 0.006 | 0.060 |
| Response variable: Externalizing factor of psychopathology | ||||
| Daring | 0.105 | 0.061 | −0.015 – 0.225 | 0.084 |
| Negative emotionality | 0.136 | 0.070 | −0.001 – 0.273 | 0.051 |
| Prosociality | −0.212 | 0.050 | −0.310 - −0.114 | 0.000 |
Covariates = sex, age in Wave 1, age in Wave 2, maternal education, log of total family income, and race-ethnicity. Note: CADS = Child and Adolescent Dispositions Scale. Bold indicates statistically significant after adjustment for 18 tests at a 5% false discovery rate.
Results Based on the Bifactor Model of Psychopathology
Results of the regressions of each latent psychopathology factor on parent-rated CADS dispositions are shown in Figure 1 and Table 3 (top rows). After FDR correction, parent-rated negative emotionality in Wave 1 significantly predicted the general factor of adult psychopathology. In addition, parent-reported daring significantly predicted the specific externalizing factor in adulthood; no parent-rated disposition predicted specific internalizing psychopathology in adulthood.
Figure 1.
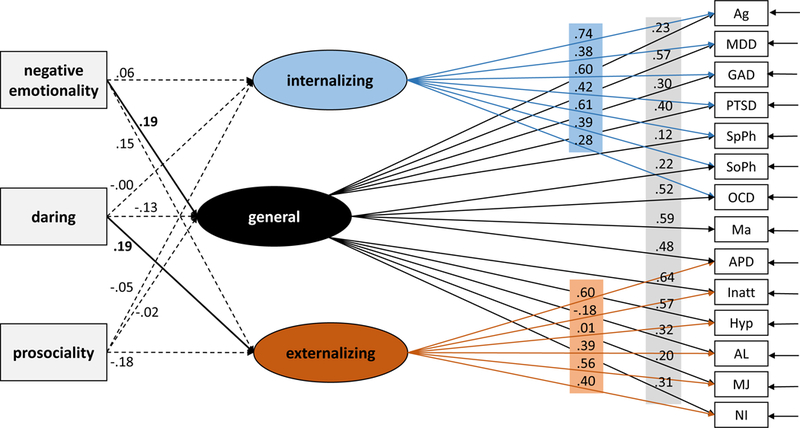
Standardized regression coefficients and factor loadings for the bifactor model of parent-reported dispositions at youth aged 10 to 17 years old predicting latent psychopathology factor scores. Note: Bold and solid arrows indicate statistically significant regression coefficient after false discovery rate adjustment.
Table 3.
Standardized regression coefficients when latent general, specific internalizing, and specific externalizing dimensions of psychopathology measured at 23–31 years of age were in defined in a separate bifactor model and simultaneously regressed on CADS dimensions of daring, negative emotionality, and prosociality measured at 10–17 years of age and demographic covariates.a Separate models were fitted for CADS ratings by parent and youth informants (N = 499).
| Parent-rated CADS dispositions | ||||
| Estimate | Standard Error | 95% Confidence Interval | p < | |
| Response variable: Internalizing factor of psychopathology | ||||
| Daring | −0.134 | 0.087 | −0.305 – 0.037 | 0.124 |
| Negative emotionality | 0.191 | 0.063 | 0.068 – 0.314 | 0.002 |
| Prosociality | −0.019 | 0.063 | −0.142 – 0.104 | 0.759 |
| Response variable: Specific internalizing factor of psychopathology | ||||
| Daring | −0.003 | 0.080 | −0.160 – 0.154 | 0.975 |
| Negative emotionality | 0.061 | 0.058 | −0.053 – 0.175 | 0.292 |
| Prosociality | −0.051 | 0.067 | −0.182 – 0.080 | 0.453 |
| Response variable: Specific externalizing factor of psychopathology | ||||
| Daring | 0.187 | 0.066 | 0.058 – 0.316 | 0.005 |
| Negative emotionality | 0.152 | 0.067 | 0.201 – 0.283 | 0.023 |
| Prosociality | −0.175 | 0.071 | −0.31 - -0.035 | 0.014 |
| Youth self-rated CADS dispositions | ||||
| Estimate | Standard Error | 95% Confidence Interval | P < | |
| Response variable: General factor of psychopathology | ||||
| Daring | −0.021 | 0.088 | −0.193 – 0.151 | 0.810 |
| Negative emotionality | 0.039 | 0.073 | −0.104 – 0.182 | 0.591 |
| Prosociality | −0.166 | 0.078 | −0.319 - -0.013 | 0.034 |
| Response variable: Specific internalizing factor of psychopathology | ||||
| Daring | −0.026 | 0.139 | −0.298 – 0.246 | 0.853 |
| Negative emotionality | 0.129 | 0.065 | 0.002 – 0.256 | 0.048 |
| Prosociality | −0.060 | 0.079 | −0.215 – 0.095 | 0.450 |
| Response variable: Specific externalizing factor of psychopathology | ||||
| Daring | 0.192 | 0.074 | 0.047 – 0.337 | 0.010 |
| Negative emotionality | 0.197 | 0.060 | 0.079 – 0.315 | 0.001 |
| Prosociality | −0.140 | 0.082 | −0.301 – 0.021 | 0.085 |
Covariates = sex, age in Wave 1, age in Wave 2, maternal education, log of total family income, and race-ethnicity; CADS = Child and Adolescent Dispositions Scale. Bold indicates statistically significant after adjustment for 18 tests at a 5% false discovery rate.
Results for youth-reported CADS dimensions are shown in Figure 2 and the bottom of Table 3. After FDR correction, youth-rated dispositions did not significantly predict the general factor in adulthood. Youth-reported negative emotionality and daring at 10–17 years significantly predicted the specific externalizing factor in adulthood, but no youth-rated disposition predicted the specific internalizing factor.
Figure 2.
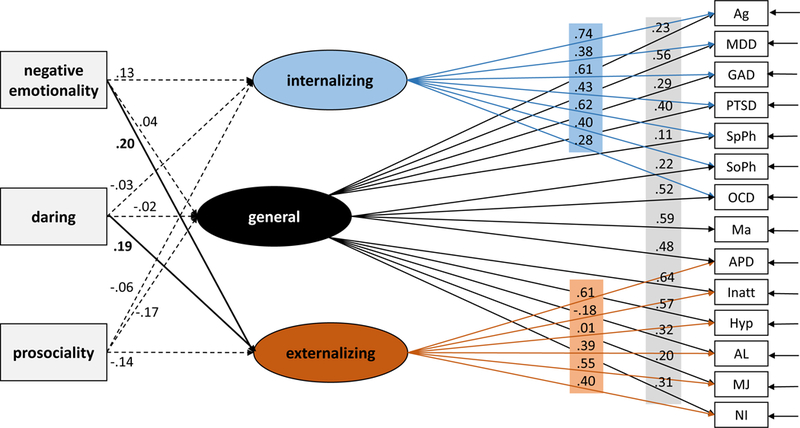
Standardized regression coefficients and factor loadings for the bifactor model of youth-reported dispositions at age 10–17 years old predicting latent psychopathology factor scores. Note: Bold and solid arrows indicate statistically significant regression coefficient after false discovery rate adjustment.
To place rater differences in context, we tested the statistical significance of differences between parent and youth raters by iteratively (a) repeating SEMs for parent ratings, substituting youth ratings for one psychopathology factor regressed on one disposition at a time, (b) using the unstandardized coefficient for that youth-rated disposition in a second SEM for parent ratings in which the coefficient for the same parent rating was equated to the coefficient for the youth rating, and (c) testing the Satorra-Bentler difference X2. No informant differences were significant at p < .05.
Stability of the General Factor
As presented in Supplemental Tables S3 and S4, each 1 SD unit greater Wave 1 general factor score during childhood and adolescence predicted an average 0.32 SD (95% CI 0.12 −0.52) unit greater Wave 2 factor score during adulthood controlling for demographic factors, p < .002 (significant after FDR correction). The Wave 1 specific internalizing factor did not significantly predict the Wave 2 specific internalizing factor and the specific externalizing factor was only correlated over time at a nominally significant level (β = 0.23, p < .04).
Results of Exploratory of Tests of Interactions
The 54 tests of interactions between CADS dispositions and sex, age in Wave 2, and maternal education in predicting general, specific internalizing, and specific externalizing factors based on the bifactor model yielded two significant interactions after FDR correction. For youth CADS ratings, the sex-by-negative emotionality interaction was significant for externalizing psychopathology, β = −0.87, p < .0001, indicating that youth-rated negative emotionality predicted specific externalizing psychopathology among males, β = 0.38, p < .001, but not among females, β = 0.02, p < .819. We also found a significant interaction, β = 1.49, p < .0001, where youth-rated prosociality inversely predicted general psychopathology among males, β = - .32, p < 0.002, but not among females, β = 0.02, p < 0.729.
DISCUSSION
Dispositions and Later Psychopathology
These findings suggest that individual differences in some child and adolescent dispositions predict second-order factors of psychopathology 10–12 years later in a transdiagnostic manner, although the associations that were significant differed according to the measurement model of psychopathology and the disposition’s rater. Findings based on the correlated-factors model (Table 2) revealed transdiagnostic associations of parent-rated negative emotionality with psychopathology. Each 1 SD unit difference in higher parent-rated negative emotionality was associated on average with both 0.16 SD (95% CI.05 - .28) higher externalizing scores and 0.23 SD (95% CI.11 - .35) higher internalizing scores in adulthood. For youth ratings of CADS dimensions, negative emotionality predicted internalizing but not externalizing psychopathology, whereas low youth-rated prosociality predicted externalizing psychopathology in adulthood after FDR correction.
Comparisons of the results based on correlated-factors (Table 2) and bifactor models (Table 3) provide the most complete picture of the transdiagnostic relations of dispositions with psychopathology:
1. Daring.
In correlated factors models, neither parent- nor youth-rated daring significantly predicted either externalizing or internalizing adult psychopathology. In the bifactor model, however, both parent- and youth-rated CADS daring scores significantly predicted the specific externalizing factor after FDR correction. Importantly, this suggests that high levels of daring in childhood and adolescence only predict the residual variance that defines specific externalizing psychopathology in early adulthood when the general factor also is modeled.
2. Negative emotionality.
Table 3 shows that youth whose parents rated them 1 SD unit higher than average on negative emotionality were expected to have a general psychopathology score .19 SD (95% CI .07 - .31) higher than average. In contrast to the significant associations with both internalizing and externalizing psychopathology in the correlated-factors model, however, parent-rated negative emotionality was significantly related to neither specific internalizing nor specific externalizing psychopathology in the bifactor model after FDR correction. Thus, the transdiagnostic associations of parent-rated negative emotionality with both internalizing and externalizing psychopathology in correlated-factors models (Table 2) at least partly reflect an association of parent-rated negative emotionality with the common variance shared by internalizing and externalizing factors that is captured by the general factor (Table 3).
The corresponding comparisons of results for youth-rated negative emotionality have potentially different implications. Youth-rated negative emotionality was associated with internalizing psychopathology in the correlated-factors model, but not with the specific internalizing factor in adulthood in the bifactor model. Instead, each 1 SD unit difference in higher youth-rated negative emotionality was associated with a .20 SD (95% CI 0.08 – 0.32) higher score on specific externalizing psychopathology in adulthood in bifactor models. Because youth-rated negative emotionality did not predict the general factor, it may only predict specific aspects of externalizing psychopathology.
3. Prosociality.
In correlated-factors models, parent-rated prosociality was not significantly associated with internalizing or externalizing psychopathology, but an inverse association of youth-rated prosociality with externalizing psychopathology was significant after FDR correction in correlated-factors models (Table 2). In the bifactor model, youth-rated prosociality only showed only a nominal association with the general factor, which may suggest the predictive variance was not specific to externalizing psychopathology as indicated by the correlated-factors model.
Comparison of Results of Cross-sectional and Prospective Tests of Associations
It is important to compare the present findings of prospective associations between dispositions rated in Wave 1 and psychopathology assessed in Wave 2 of the TTS with the results of our previous cross-sectional test of associations between the CADS dispositions and second-order factors of psychopathology during childhood and adolescence in Wave 1 of the TTS (Tackett et al., 2013). Notably, parent-rated negative emotionality was significantly associated with the general factor of psychopathology in both cross-sectional and prospective analyses after FDR correction, suggesting that this association is robust across the important differences between the cross-sectional and prospective analyses. The cross-sectional and prospective tests were conducted at meaningfully different ages using different diagnostic interviews and informants. In Wave 1, a combination of parent and youth ratings were used to define symptoms, whereas symptoms in Wave 2 were reported only by the young adults. Furthermore, the symptom dimensions assessed in the two waves only partially overlapped, with separation anxiety disorder, ODD, and CD assessed in only Wave 1, and APD, alcohol use disorder, cannabis use disorder, nicotine dependence, and mania assessed in only Wave 2. Nonetheless, as reported in Supplemental Table S4, the Wave 1 general factor score significantly predicted the Wave 2 general factor score, indicating a degree of homotypic continuity of the general factor over 12 years in spite of marked differences in operationalization. The continuity was less than perfect, however, leaving room for meaningful differences between the general factors of psychopathology defined at different ages. Therefore, the finding that parent-rated negative emotionality was significantly associated with the general factor in both childhood/adolescence and early adulthood strengthens the inference of a theoretically important and enduring association between the constructs of parent-rated negative emotionality and the general factor of psychopathology.
Differences in other findings between the cross-sectional and prospective analyses may be attributable to differences in Wave 1 sample sizes (N = 3,138 in cross-sectional versus 499 in prospective tests). Parent-rated negative emotionality and parent-rated prosociality were both associated with specific externalizing in cross-sectional analyses, but the same associations were only nominally significant in prospective analyses. In cross-sectional analyses, parent-rated daring was positively associated with specific externalizing and inversely associated with specific internalizing psychopathology, but daring was only significantly associated with specific externalizing psychopathology in prospective analyses. Fewer associations were found between youth-rated dispositions and psychopathology in both sets of analyses. Nonetheless, youth-rated daring was modestly associated with specific externalizing psychopathology in both crosssectional and prospective analyses. Youth-rated negative emotionality was modestly associated with the general factor in the Wave 1 cross-sectional analyses, but not in prospective analyses. Youth-rated prosociality was modestly related to specific externalizing psychopathology in only cross-sectional analyses.
Rater Differences in Significant Associations of Dispositions
For parent ratings of negative emotionality only, the prospective findings presented in Tables 2 and 3 are consistent with, and extend cross-sectional findings that negative emotionality/neuroticism is correlated with essentially every form of psychopathology (Lahey, 2009; Widiger & Oltmanns, 2017), and hence, with the general factor of psychopathology (Caspi et al., 2014; Tackett et al., 2013). In previous cross-sectional analyses of the Wave 1 TTS sample of 4,000 twins during childhood and adolescence, negative emotionality also was phenotypically and genetically correlated with the general factor, but the magnitude of the association was greater for parent- than youth-rated negative emotionality (Tackett et al., 2013).
Differences in the significant correlates of parent- and youth-rated dispositions are not surprising because they are only modestly correlated. These modest correlations between parent and youth CADS ratings may reflect differences between the raters in maturity, experiences, the situations in which they observe the child, the covertness of some important experiences, and response style differences between the informants. Importantly, there were no significant differences in the magnitudes of associations of parent and youth ratings with psychopathology, but the differences in significant findings for parent and youth ratings are consistent with previous studies reporting low to moderate agreement between informant ratings of temperament and personality traits (Boson, Brandstrom, & Sigvardsson, 2018; Capaldi & Rothbart, 1992; Quilty, Cosentino, & Bagby, 2018; Tackett, 2011).
New research is needed to understand potential informant differences, but because no resolution has been reached at present on a valid method of combining discrepant ratings from parents and youth on dispositional traits (Tackett, 2011), we analyzed the data separately for parent and youth CADS ratings. Sensitivity analyses (Table S8) in which the common variance in parent and youth ratings on the CADS dimensions were similar, though weaker, to those based on parent ratings, suggest the need to treat parent and youth ratings separately until more is known about combining dispositions ratings from multiple informants.
Exploratory Tests of Interactions with Demographic Factors
The exploratory tests of interactions between demographic factors and CADS dispositions revealed little evidence of demographic moderation of predictive associations between dispositions and later psychopathology. The two exceptions were that youth-rated negative emotionality may predict specific externalizing and that youth-rated prosociality may inversely predict the general factor more strongly for males than females in bifactor models. It is important to note, however, that these exploratory tests of interactions were not based on previous findings of interactions and were conducted in a sample not well powered for testing interactions. Thus, the absence of statistically significant interactions with other demographic variables cannot be interpreted as evidence for the absence of other interactions.
Limitations and Conclusions
The present findings are consistent with the hypothesis that the psychobiological processes associated with parent-rated negative emotionality constitute one of the mechanisms that underlie the general factor of psychopathology by increasing risk for all forms of psychopathology (Lahey, 2009; Lahey et al., 2017). Importantly, these prospective findings further suggest that the relation between individual differences in negative emotionality as perceived by parents and the general factor of psychopathology extends from childhood/adolescence into adulthood. Notably, one aspect of the present findings further supports the criterion validity of the general factor. Because the predictive relation between negative emotionality and the general factor of psychopathology was found across informants (i.e., parent-rated negative emotionality predicted the general factor based on self-reported symptoms), it cannot be an artifact of correlated measurement error.
Several limitations of the current study should be considered. First, a larger sample may have identified additional predictive associations between dispositions and later psychopathology. A number of potentially important associations were nominally significant but not significant after FDR correction. Second, we are unable to conclude that the relations between dispositions and psychopathology identified in this cohort study are causal. Third, we cannot distinguish between alternative pathways from socioemotional dispositions to psychopathology. It may be that a spectrum model (Clark, 2005), which suggests that psychopathology may be expressions of early onset, chronic, or pervasive individual differences in functioning (Nigg, 2006; Tackett, 2006), best explains the longitudinal pathway from dispositions to psychopathology. Alternatively, the pathoplasty model suggests that dispositional factors can impact the course and severity of psychopathology, but do not play a causal role on the onset of the pathology (Widiger, 2011). Fourth, the domains of psychopathology covered are incomplete and do not include psychosis or personality disorders. Future longitudinal studies addressing these issues should prove informative.
Supplementary Material
Acknowledgments
Supported by grants MH098098 from the National Institute of Mental Health and CTSA grants UL1-TR000445 and UL1-TR000430.
Contributor Information
Quetzal A. Class, University of Illinois at Chicago
Carol A. Van Hulle, University of Wisconsin-Madison
Paul J. Rathouz, University of Texas, Austin
Brooks Applegate, Western Michigan University.
David H. Zald, Vanderbilt University
Benjamin B. Lahey, University of Chicago
References
- Abram KM, Zwecker NA, Welty LJ, Hershfield JA, Dulcan MK, & Teplin LA (2015). Comorbidity and continuity of psychiatric disorders in youth after detention: A prospective longitudinal study. Jama Psychiatry, 72, 84–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barlow DH, Sauer-Zavala S, Carl JR, Bullis JR, & Ellard KK (2014). The nature, diagnosis, and treatment, of neuroticism: back to the future. Clinical Psychological Science, 2, 344–365. [Google Scholar]
- Bell RQ (1977). Socialization findings re-examined In Bell RQ & Harper RV (Eds.), Child effects on adults (pp. 53–84). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Belsky J, & Pluess M (2009). Beyond diathesis stress: Differential susceptibility to environmental influences. Psychological Bulletin, 135(6), 885–908. doi: 10.1037/a0017376 [DOI] [PubMed] [Google Scholar]
- Biederman J, Hirshfeld-Becker DR, Rosenbaum JF, Herot C, Friedman D, Snidman N, … Faraone SV (2001). Further evidence of association between behavioral inhibition and social anxiety in children. American Journal of Psychiatry, 155(10), 1673–1679. doi: 10.1176/appi.ajp.158.10.1673 [DOI] [PubMed] [Google Scholar]
- Bonifay W, Lane SP, & Reise SP (2017). Three concerns with applying a bifactor model as a structure of psychopathology. Clinical Psychological Science, 5, 184–186. [Google Scholar]
- Boson K, Brandstrom S, & Sigvardsson S (2018). The Junior Temperament and Character Inventory (JTCI): Psychometric properties of multi-informant ratings. Psychological Assessment, 30(4), 550–555. doi: 10.1037/pas0000513 [DOI] [PubMed] [Google Scholar]
- Brown TA (2006). Confirmatory factor analysis for applied research. New York: Guilford. [Google Scholar]
- Capaldi DM, & Rothbart MK (1992). Development and validation of an early adolescent temperament measure. The Journal of Early Adolescence, 12(2), 153–173. doi: 10.1177/0272431692012002002 [DOI] [Google Scholar]
- Caspi A, Henry B, McGee RO, Moffitt TE, & Silva PA (1995). Temperamental origins of child and adolescent behavior problems: From age 3 to age 15. Child Development, 66(1), 55–68. doi: 10.1111/j.1467-8624.1995.tb00855.x [DOI] [PubMed] [Google Scholar]
- Caspi A, Houts RM, Belsky DW, Goldman-Mellor SJ, Harrington H, Israel S, … Moffitt TE (2014). The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2, 119–137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Briere FN, O’Leary-Barrett M, Banaschewski T, Bokde A, Bromberg U, … Consortium I (2016). The structure of psychopathology in adolescence and its common personality and cognitive correlates. Journal of Abnormal Psychology, 125(8), 1039–1052. doi: 10.1037/abn0000193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark LA (2005). Temperament as a unifying basis for personality and psychopathology. Journal of Abnormal Psychology, 114(4), 505–521. doi: 10.1037/0021-843X.114.4.505 [DOI] [PubMed] [Google Scholar]
- Costa PT, & McCrae RR (1992). NEO five-factor inventory. Lutz, FL: Psychological Assessment Resources. [Google Scholar]
- Docherty AR, Moscati A, Dick D, Savage JE, Salvatore JE, Cooke M, … S., K. K. (2017) . Polygenic prediction of the phenome, across ancestry, in emerging adulthood. Psychological Medicine, [Epub ahead of print]. doi: 10.1017/S0033291717003312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frick PJ, Ray JV, Thornton LC, & Kahn RE (2014). Can callous-unemotional traits enhance the understanding, diagnosis, and treatment of serious conduct problems in children and adolescents? A comprehensive review. Psychological Bulletin, 140, 1–57. [DOI] [PubMed] [Google Scholar]
- Huang-Pollock C, Shapiro Z, Galloway-Long H, & Weigard A (2017). Is poor working memory a transdiagnostic risk factor for psychopathology? Journal of Abnormal Child Psychology, 45(8), 1477–1490. doi: 10.1007/s10802-016-0219-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones H, Heron J, Hammerton G, Stochl J, Jones PB, Cannon M, … Team a. M. R. (2018). Investigating the genetic architecture of general and specific psychopathology in adolescence Translational Psychiatry, 8, 145. doi:DOI 10.1038/s41398-018-0204-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaczkurkin AN, Moore TM, Calkins ME, Ciric R, Detre JA, Elliott MA, … Satterthwaite TD (2017). Common and dissociable regional cerebral blood flow differences associate with dimensions of psychopathology across categorical diagnoses. Molecular Psychiatry. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan AA, Jacobson KC, Gardner CO, Prescott CA, & Kendler KS (2005). Personality and comorbidity of common psychiatric disorders. British Journal of Psychiatry, 186, 190–196. [DOI] [PubMed] [Google Scholar]
- Knafo-Noam A, Uzefovsky F, Israel S, Davidov M, & Zahn-Waxler C (2015). The prosocial personality and its facets: genetic and environmental architecture of mother-reported behavior of 7-year-old twins. Frontiers in Psychology, 6. doi: 10.3389/fpsyg.2015.00112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korn EL, & Graubard BI (1999). Analysis of health surveys. New York: Wiley. [Google Scholar]
- Krueger RF, & Tackett JL (2003). Personality and psychopathology: Working toward the bigger picture. Journal of Personality Disorders, 17, 109–128. [DOI] [PubMed] [Google Scholar]
- Lahey BB (2004). Commentary: Role of temperament in developmental models of psychopathology. Journal of Clinical Child and Adolescent Psychology, 33, 88–93. [DOI] [PubMed] [Google Scholar]
- Lahey BB (2009). Public health significance of neuroticism. American Psychologist, 64, 241–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB (2014). What we need to know about callous-unemotional traits: Comment on Frick, Ray, Thornton, and Kahn (2014). Psychological Bulletin, 140, 58–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB (2015). Why Are Children Who Exhibit Psychopathology at High Risk for Psychopathology and Dysfunction in Adulthood? Jama Psychiatry, 72(9), 865–866. doi : 10.1001/jamapsychiatry.2015.0798 [DOI] [PubMed] [Google Scholar]
- Lahey BB, Applegate B, Chronis AM, Jones HA, Williams SH, Loney J, & Waldman ID (2008). Psychometric characteristics of a measure of emotional dispositions developed to test a developmental propensity model of conduct disorder. Journal of Clinical Child and Adolescent Psychology, 37, 794–807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Applegate B, Hakes JK, Zald DH, Hariri AR, & Rathouz PJ (2012). Is there a general factor of prevalent psychopathology during adulthood? Journal of Abnormal Psychology, 121(4), 971–977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Applegate B, Waldman ID, Loft JD, Hankin BL, & Rick J (2004). The structure of child and adolescent psychopathology: Generating new hypotheses. Journal of Abnormal Psychology, 113, 358–385. [DOI] [PubMed] [Google Scholar]
- Lahey BB, Class QA, Zald DH, Rathouz PJ, Applegate B, & Waldman ID (2018). Prospective test of the developmental propensity model of antisocial behavior: from childhood and adolescence into early adulthood. Journal of Child Psychology and Psychiatry, 59, 676–683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Krueger RF, Rathouz PJ, Waldman ID, & Zald DH (2017). A hierarchical causal taxonomy of psychopathology across the life span. Psychological Bulletin, 143, 142–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Rathouz PJ, Applegate B, Tackett JL, & Waldman ID (2010). Psychometrics of a self-report version of the child and adolescent dispositions scale. Journal of Clinical Child and Adolescent Psychology, 39, 351–361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Rathouz PJ, Applegate B, Van Hulle C, Garriock HA, Urbano RC, … Waldman ID (2008). Testing structural models of DSM-IV symptoms of common forms of child and adolescent psychopathology. Journal of Abnormal Child Psychology, 36, 187–206. [DOI] [PubMed] [Google Scholar]
- Lahey BB, Rathouz PJ, Keenan K, Stepp SD, Loeber R, & Hipwell AE (2015). Criterion validity of the general factor of psychopathology in a prospective study of girls. Journal of Child Psychology and Psychiatry, 4, 415–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Van Hulle CA, Singh AL, Waldman ID, & Rathouz PJ (2011). Higherorder genetic and environmental structure of prevalent forms of child and adolescent psychopathology. Archives of General Psychiatry, 68, 181–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, & Waldman ID (2003). A developmental propensity model of the origins of conduct problems during childhood and adolescence In Lahey BB, Moffitt TE, & Caspi A (Eds.), Causes of Conduct Disorder and Juvenile Delinquency (pp. 76–117). New York, NY: Guilford Press Guilford Press. [Google Scholar]
- Lahey BB, Zald DH, Perkins SF, Villalta-Gil V, Werts KB, Van Hulle CA, … Waldman ID (2018). Measuring the hierarchical general factor model of psychopathology in young adults. International Journal of Methods in Psychiatric Research, 27, e1593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lemery KS, Essex MJ, & Smider NA (2002). Revealing the relation between temperament and behavior problem symptoms by eliminating measurement confounding: Expert ratings and factor analyses. Child Development, 73, 867–882. [DOI] [PubMed] [Google Scholar]
- Lengua LJ, West SG, & Sandler IN (1998). Temperament as a predictor of symptomatology in children: Addressing contamination of measures. Child Development, 69(1), 164–181. doi: 10.1111/j.1467-8624.1998.tb06141.x [DOI] [PubMed] [Google Scholar]
- Luby JL, Svrakic DM, McCallum K, Przybeck TR, & Cloninger CR (1999). The Junior Temperament and Character Inventory: Preliminary validation of a child self-report measure. Psychological Reports, S4(3_suppl), 1127–1138. doi: 10.2466/pr0.1999.84.3c.1127 [DOI] [PubMed] [Google Scholar]
- Martel MM, Pan PM, Hoffmann MS, Gadelha A, do Rosario MC, Mari JJ, … Salum GA (2017). A general psychopathology factor (p factor) in children: Structural model analysis and external validation through familial risk and child global executive function. Journal of Abnormal Psychology, 126, 137–148. [DOI] [PubMed] [Google Scholar]
- Mikolajewski AJ, Allan NP, Hart SA, Lonigan CJ, & Taylor J (2013). Negative affect shares genetic and environmental influences with symptoms of childhood internalizing and externalizing disorders. Journal of Abnormal Child Psychology, 41(3), 411–423. doi: 10.1007/s10802-012-9681-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy BC, Shepard SA, Eisenberg N, Fabes RA, & Guthrie IK (1999). Contemporaneous and longitudinal relations of dispositional sympathy to emotionality, regulation, and social functioning. The Journal of Early Adolescence, 19(1), 66–97. doi : 10.1177/0272431699019001004 [DOI] [Google Scholar]
- Muthén B, & Muthén L (2018). Mplus 8.1. Los Angeles: Muthén & Muthén. [Google Scholar]
- Neumann A, Pappa I, Lahey BB, Verhulst FC, Medina-Gomez C, Jaddoe VW, … Tiemeier H (2016). SNP heritability of a general psychopathology factor in children. Journal of the American Academy of Child and Adolescent Psychiatry, 55, 1038–1045. [DOI] [PubMed] [Google Scholar]
- Nigg JT (2006). Temperament and developmental psychopathology. Journal of Child Psychology and Psychiatry, 47, 395–422. [DOI] [PubMed] [Google Scholar]
- Overbeek G (2017). Parenting intervention effects on children’s externalizing behavior: the moderating role of genotype and temperament. Current Opinion in Psychology, 15, 143–148. doi: 10.1016/j.copsyc.2017.02.025 [DOI] [PubMed] [Google Scholar]
- Pettersson E, Lahey BB, Lundstrom S, Larsson H, & Lichtenstein P (2018). Criterion validity and utility of the general factor of psychopathology in childhood: Predictive associations with independently measured severe adverse mental health outcomes in adolescence. Journal of the American Academy of Child and Adolescent Psychiatry, 57, 372–383. [DOI] [PubMed] [Google Scholar]
- Piacentini JC, Cohen P, & Cohen J (1992). Combining discrepant diagnostic information from multiple sources: Are complex algorithms better than simple ones? Journal of Abnormal Child Psychology, 20, 51–62. [DOI] [PubMed] [Google Scholar]
- Quilty LC, Cosentino N, & Bagby RM (2018). Response bias and the Personality Inventory for DSM-5: Contrasting self- and informant-report. Personality Disorders: Theory Research and Treatment, 9(4), 346–353. doi: 10.1037/per0000246 [DOI] [PubMed] [Google Scholar]
- Ricardo Sato J, Salum GA, Gadelha A, Crossley N, Vieira G, Manfro GG, … Bressan RA (2016). Default mode network maturation and psychopathology in children and adolescents. Journal of Child Psychology and Psychiatry, 57(1), 55–64. doi: 10.1111/jcpp.12444 [DOI] [PubMed] [Google Scholar]
- Romer AL, Knodt AR, Houts R, Brigidi BD, Moffitt TE, Caspi A, & Hariri AR (2018). Structural alterations within cerebellar circuitry are associated with general liability for common mental disorders. Molecular Psychiatry, 23(4), 1084–1090. doi: 10.1038/mp.2017.57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothbart MK, Ahadi SA, Hershey KL, & Fisher P (2001). Investigations of temperament at three to seven years: The children’s behavior questionnaire. Child Development, 72(5), 1394–1408. doi: 10.1111/1467-8624.00355 [DOI] [PubMed] [Google Scholar]
- Ruschena E, Prior M, Sanson A, & Smart D (2005). A longitudinal study of adolescent adjustment following family transitions. Journal of Child Psychology and Psychiatry, 46(4), 353–363. doi: 10.1111/j.1469-9610.2004.00369 [DOI] [PubMed] [Google Scholar]
- Russo MF, Stokes GS, Lahey BB, Christ MAG, McBurnett K, Loeber R, … Green SM (1993). A sensation seeking scale for children: Further refinement and psychometric development Journal of Psychopathology and Behavioral Assessment, 15(2), 69–86. doi: 10.1007/bf00960609 [DOI] [Google Scholar]
- Sameroff AJE (Ed.) (2009). The transactional model of development: How children and contexts shape each other. Washington, DC: American Psychological Association. [Google Scholar]
- Schermerhorn AC, Bates JE, Goodnight JA, Lansford JE, Dodge KA, & Pettit GS (2013). Temperament moderates associations between exposure to stress and children’s externalizing problems. Child Development, 84(5), 1579–1593. doi: 10.1111/cdev.12076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaffer D, Fisher P, Lucas CP, Dulcan MK, & Schwab-Stone ME (2000). NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): Description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 28–38. [DOI] [PubMed] [Google Scholar]
- Shaffer D, Fisher P, Piacentini JC, & Lucas C (2008). Young Adult Diagnostic Interview Schedule for Children. New York: Columbia University. [Google Scholar]
- Shaw DS, Hyde LW, & Brennan LM (2012). Early predictors of boys’ antisocial trajectories. Development and Psychopathology, 24(3), 871–888. doi: 10.1017/s0954579412000429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiner R, & Caspi A (2003). Personality differences in childhood and adolescence: measurement development, and consequences. Journal of Child Psychology and Psychiatry and Allied Disciplines, 44(1), 2–32. doi: 10.1111/1469-7610.00101 [DOI] [PubMed] [Google Scholar]
- Simonds J, Kieras JE, Rueda MR, & Rothbart MK (2007). Effortful control, executive attention, and emotional regulation in 7–10-year-old children. Cognitive Development, 22, 474–488. [Google Scholar]
- Sitnick SL, Brennan LM, Forbes E, & Shaw DS (2014). Developmental pathways to sexual risk behavior in high-risk adolescent boys. Pediatrics, 133(6), 1038–1045. doi: 10.1542/peds.2013-3976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slagt M, Dubas JS, Dekovic M, & van Aken MAG (2016). Differences in Sensitivity to Parenting Depending on Child Temperament: A Meta-Analysis. Psychological Bulletin, 142(10), 1068–1110. doi: 10.1037/bul0000061 [DOI] [PubMed] [Google Scholar]
- Smoller JW, Andreassen OA, Edenberg HJ, Faraone SV, Glatt SJ, & Kendler KS (2018). Psychiatric genetics and the structure of psychopathology. Molecular Psychiatry, 10.1038/s41380-017-0010-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder HR, Hankin BL, Sandman CA, Head K, & Davis EP (2017). Distinct Patterns of Reduced Prefrontal and Limbic Gray Matter Volume in Childhood General and Internalizing Psychopathology. Clinical Psychological Science, 5(6), 1001–1013. doi: 10.1177/2167702617714563 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tackett JL (2006). Evaluating models of the personality-psychopathology relationship in children and adolescents. Clinical Psychology Review, 26(5), 584–599. doi: 10.1016/j.cpr.2006.04.003 [DOI] [PubMed] [Google Scholar]
- Tackett JL (2011). Parent Informants for Child Personality: Agreement, Discrepancies, and Clinical Utility. Journal of Personality Assessment, 93(6), 539–544. doi: 10.1080/00223891.2011.608763 [DOI] [PubMed] [Google Scholar]
- Tackett JL, Lahey BB, Van Hulle CA, Waldman ID, Krueger RF, & Rathouz PJ (2013). Common genetic influences on negative emotionality and a general psychopathology factor in childhood and adolescence. Journal of Abnormal Psychology, 122, 1142–1153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor J, Allan N, Mikolajewski AJ, & Hart SA (2013). Common genetic and nonshared environmental factors contribute to the association between socioemotional dispositions and the externalizing factor in children. Journal of Child Psychology and Psychiatry, 54, 67–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas A, & Chess S (1957). An approach to the study of sources of individual differences in child behavior. Journal of clinical and experimental psychopathology, 18, 347–357. [PubMed] [Google Scholar]
- Trentacosta CJ, Hyde LW, Shaw DS, & Cheong JW (2009). Adolescent dispositions for antisocial behavior in context: The roles of neighborhood dangerousness and parental knowledge. Journal of Abnormal Psychology, 118, 564–575. doi: 10.1037/a0016394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waldman ID, Tackett JL, Van Hulle CA, Applegate B, Pardini D, Frick PJ, & Lahey BB (2011). Child and adolescent conduct disorder substantially shares genetic influences with three socioemotional dispositions. Journal of Abnormal Psychology, 120, 57–70. doi: 10.1037/a0021351 [DOI] [PubMed] [Google Scholar]
- Widiger TA (2011). Personality and psychopathology. World Psychiatry, 10(2), 103–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widiger TA, & Oltmanns JR (2017). Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry, 16(2), 144–145. doi: 10.1002/wps.20411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witkiewitz K, King K, McMahon RJ, Wu J, Luk J, Bierman KL, … CPPRG. (2013). Evidence for a multi-dimensional latent structural model of externalizing disorders. Journal of Abnormal Child Psychology, 41, 223–237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zuckerman M, & Aluja A (2015). Measures of Sensation Seeking In Boyle GJ, Saklofske DH, & Matthews G (Eds.), Measures of Personality and Social Psychological Constructs (pp. 352–380). Amsterdam: Elsevier. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.