

ABSTRACT
Kidney disease affects almost 15% of the US population, and prevalence is anticipated to grow as the population ages and the obesity epidemic continues due to Western dietary practices. The densely caloric Western diet, characterized by high animal protein and low fruit and vegetable content, has fueled the growth of chronic diseases, including chronic kidney disease. The glomerulus or filtering unit of the kidney is very susceptible to barotrauma, and diets high in animal protein impede the glomerulus’ ability to protect itself from hemodynamic injury. High animal protein intake combined with low intake of fruits and vegetables also leads to a high net endogenous acid production requiring augmentation of ammonium excretion in order to prevent acidosis. This higher workload of the kidney to maintain a normal serum bicarbonate level may further exacerbate kidney disease progression. This article reviews the potential mechanisms whereby several key characteristics of the typical Western diet may impact kidney disease incidence and progression. Reducing animal protein intake and egg yolk and increasing intake of fruits and vegetables and fiber may prevent or delay end-stage renal disease, but few clinical trials have examined vegetarian diets for management of chronic kidney disease. More research is needed to determine optimal dietary patterns for the prevention of kidney disease and its progression.
Keywords: chronic kidney disease, plant protein, animal protein, acidosis, kidney, protein, nutrition, obesity, Western diet
Introduction
Chronic kidney disease (CKD) affects almost 15% of the US population or 30 million US adults (1). Of these, approximately 661,000 individuals have suffered kidney failure requiring dialysis or transplantation. Many people afflicted with CKD may be most concerned about their kidneys failing and fear dialysis, but due to the heightened cardiovascular disease risk that accompanies CKD, the overwhelming majority will not live long enough for their kidneys to fail (2). Among adults older than age 65 y, the presence of CKD is associated with a 2-fold higher prevalence of cardiovascular disease (2). In addition, the presence of CKD reduces overall survival after a heart attack or stroke (3). Thus, the excess cardiovascular disease risk that accompanies CKD is really the main driver of morbidity and mortality in this population. Although genetic factors definitely play a role in disease incidence and progression, especially for cases in which kidney failure occurs before age 50 y, the majority of cases are rooted in nutritional factors and largely preventable. Currently, it is estimated that >24% of CKD cases in industrialized countries can be attributed to nutritional factors (4). In the United States, diabetes and hypertension account for at least 70% of all cases of kidney failure (5). During the next several decades, CKD incidence will increase as the US population ages within a setting of unabated obesity (6).
Health systems should place strong emphasis on CKD prevention because of the substantial economic impact this disease has on both the patient and the payer. Even during earlier CKD stages when renal replacement therapy is not needed, the total health expenditures for CKD are often higher than costs associated with heart failure or stroke. Out-of-pocket costs incurred by patients are also higher for CKD than for heart failure or stroke (7). Most end-stage renal disease (ESRD) costs are paid by Medicare, and these costs now exceed $33 billion annually but are projected to expand as the total number of individuals with ESRD continues to grow (8). Total Medicare spending for all CKD stages exceeded $98 billion in 2015, and spending will continue to increase over time without substantial prevention efforts (8).
Impact of Dietary Factors on Kidney Disease Progression
Strong adherence to Western dietary patterns is associated with increased risk of CKD as defined by the presence of moderate to severely increased levels of urine albumin excretion and/or a rapid decline in glomerular filtration rate (GFR; ≥3 mL · min−1 · 1.73 m−2) (9, 10). However, associations between diet and incident CKD may be largely mediated by insulin resistance and development of the metabolic syndrome, diabetes, and hypertension (11). In fact, it has been estimated that >90% of cases of type 2 diabetes and 65% of hypertension cases, the two major causes of kidney disease, could be prevented if all US adults adhered to a healthy lifestyle and diet (12, 13).
Dietary practices alone are likely not sufficient to induce kidney damage in most individuals because mammals have a redundant set of nephrons, the working unit of the kidney. A nephron contains a tuft of capillaries surrounded by a capsule that captures the fluid filtered through the glomerular capillary wall and surrounding podocytes (Figure 1), called a glomerulus, and tubules that originate from the glomerulus and carry the glomerular filtrate through the kidney to the renal pelvis. These tubules reabsorb fluid, electrolytes, and bicarbonate from the filtrate and also secrete electrolytes and other substances such as antimicrobial peptides. The function of kidneys is reflected by the GFR, which is defined as the amount of blood filtered of some substance per unit time and reported in mL · min−1 · 1.73 m−2 body surface area. The total GFR is the total sum of each nephron GFR. Most individuals have ∼900,000 nephrons per kidney; thus, with two kidneys, the average total nephron number is 1.8 million. When the nephron number is high, each individual nephron does not need to work at maximum capacity. Thus, normal kidney function can be sustained even after substantial nephron loss. This is why healthy individuals can donate a kidney, losing 50% of their total nephrons, and still maintain a normal GFR. However, not all persons are born with a redundant set of nephrons (14, 15), and these individuals may have the highest risk of developing kidney disease during their lifetime. As a person ages, nephron senescence occurs, and this nephron dropout may be accelerated by long-term exposure to chronic diseases such as diabetes and hypertension. With nephron loss, the remaining nephrons must work at a higher capacity to maintain a normal total GFR. Similarly, single nephron GFR must increase with substantial weight gain (e.g., morbid obesity) because the metabolic demands of the body have substantially increased. To increase single nephron GFR, the glomerulus increases in size to increase the capillary surface area for filtration. If the increase in glomerular capillary surface area is not adequate to sufficiently increase single nephron GFR, then GFR may increase further via preferential vasodilation of the afferent arteriole, leading to increased hydrostatic pressure inside the glomerular capillary.
FIGURE 1.
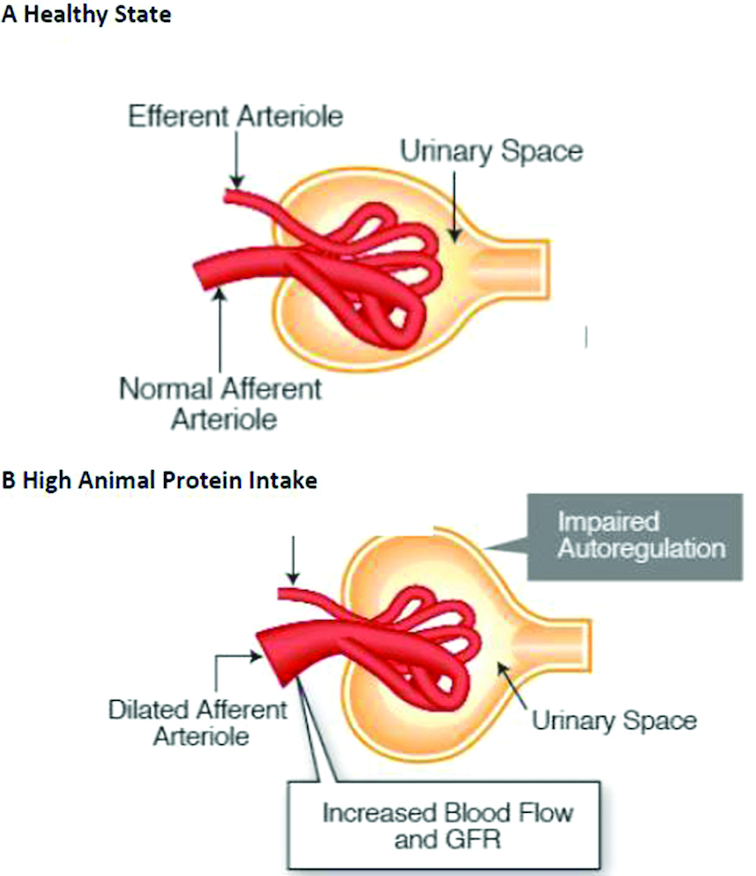
Glomerulus in the healthy state (A) and a glomerulus in the setting of high animal protein intake (B). Note that the afferent arteriole is dilated in the setting of high animal protein intake, which impairs autoregulation. GFR, glomerular filtration rate.
The requirement to work at a higher capacity leaves the nephron vulnerable to the potential deleterious effects of Western dietary patterns characterized by high intake of red meat and animal fat and highly processed foods preserved with phosphate and sodium and low intake of fresh fruits and vegetables (10). For a person with non-dialysis-dependent CKD, dietary changes remain a low-cost but effective intervention for prevention of CKD progression. Attention to diet should be emphasized when CKD is first diagnosed, a time period when interventions are most likely to be effective. Although multiple factors of the Western diet may influence kidney disease progression, this article focuses on three key dietary factors—animal protein, salt, and fruit and vegetable intake—and discusses areas of research need.
Protein
The typical US diet contains approximately twice the protein intake recommended by US dietary guidelines (16). Among persons with reduced nephron number, a high amount of animal protein intake may lead to further nephron loss via hemodynamic glomerular capillary injury. High animal protein intake interferes with the kidney's ability to autoregulate glomerular capillary blood flow by triggering humoral and local mediators that vasodilate the afferent arteriole (Figure 1) (17–20). After a meat meal, both renal blood flow and GFR increase. In fact, when persons with normal kidney function transition from low to high animal protein intake, both renal blood flow and GFR may increase up to 30% (21, 22). This augmentation of renal blood flow is limited to animal protein intake, and persons following a vegetarian diet typically have lower GFR compared with persons consuming animal protein (17). This afferent arteriolar dilatation occurs due to amino acids triggering multiple humoral and local mediators that vasodilate the afferent arteriole (17–20). A single mediator of this vasodilation has never been completely substantiated, and it is likely that multiple factors operate collectively. Potential mediators of this vasodilatation include l-3,4-dihydroxyphenylalanine, prostaglandins, NO, and N-methyl-d-aspartate (23).
To understand why high intake of animal protein accelerates loss of kidney function, it is important to examine how the kidney protects itself from hemodynamic injury. Each nephron is really an arteriole suspended in urine without support of bone, muscle, fat, or connective tissue. One can think of the nephron as a water balloon: If the pressure inside that balloon becomes too high, it will burst due to increased wall tension. Any elevation in glomerular intracapillary pressure will increase capillary wall tension according to the law of LaPlace, shown in Equation (1) (24).
 |
(1) |
The nephron protects itself from this hemodynamic injury by vasoconstricting the afferent arteriole (input of blood flow into the nephron) and/or vasodilating the efferent arteriole (output of blood flow from nephron) in order to maintain a constant amount of glomerular intracapillary pressure (Figure 1). The effects of high protein intake may be most operative in the setting of reduced working nephron number because each individual nephron is working at a higher capacity via augmentation of glomerular capillary surface area and potentially preferential vasodilation of the afferent arteriole. Elevated systemic pressures will be transmitted to the delicate glomerular capillary and may result in elevated capillary wall tension, scarring, and nephron loss (24–27). Thus, reduced nephron number where single nephron GFR must increase combined with high intake of animal protein may counteract the autoregulatory vasoconstriction needed to protect the glomerular capillary against elevated systemic pressures.
The mechanical distension of glomerular capillaries and heightened capillary wall shear stress also lead to stretching of mesangial cells, which are smooth muscle-like cells lying adjacent to and in between the glomerular capillaries. Physical stretching of mesangial cells stimulates their production of collagen and extracellular matrix, which leads to nephron scarring (28–30). Activated mesangial cells also stimulate the production of TGF-β1 by endothelial cells lining the inner glomerular capillary. TGF-β1 then further stimulates mesangial cells to produce extracellular matrix, exacerbating glomerular scarring (31).
High-protein diets are also associated with increased urine albumin excretion in adults with multiple kidney disease risk factors (32, 33), and low-protein diets may reduce urinary albumin excretion. In a healthy state, urine albumin excretion is very low due to structural barriers in the glomerular capillary wall that prevent proteins such as albumin from entering the urinary space. High protein intake may accelerate apoptosis of podocytes, cells that surround the external layer of the glomerular capillary and act mainly as a barrier to prevent proteins from escaping the blood into the urinary space during glomerular filtration (Figure 2). Diets high in protein sources such as meat cooked at high heat contain high amounts of advanced glycation end products (AGEs) (34, 35), which are highly reactive aldehydes that can bind to receptors or link with cell wall proteins and alter cell structure and function, leading to cell death. AGEs may be formed via nonenzymatic Maillard reactions or other pathways that lead to glycation and oxidation of reducing sugars with free amino groups, and they can occur with cooking of proteins or endogenously (36). Receptors for AGEs are found on podocytes, and expression of these receptors increases in diabetes (35). In the setting of high circulating AGE levels, these glycoxidation products can lead to podocyte apoptosis via activation of a forkhead transcription factor that turns on genes involved in cell cycle arrest and apoptosis (37). Podocyte susceptibility to injury from AGEs will be heightened in the setting of glomerular hypertrophy and capillary dilatation because a single podocyte must cover a larger surface area (Figure 2). This stretching of podocytes can lead to partial detachment from the glomerular capillary and heighten their susceptibility to injury. Podocytes may provide structural support for glomerular capillaries, and reductions in podocyte density may also heighten nephron susceptibility to hemodynamic injury (38, 39).
FIGURE 2.
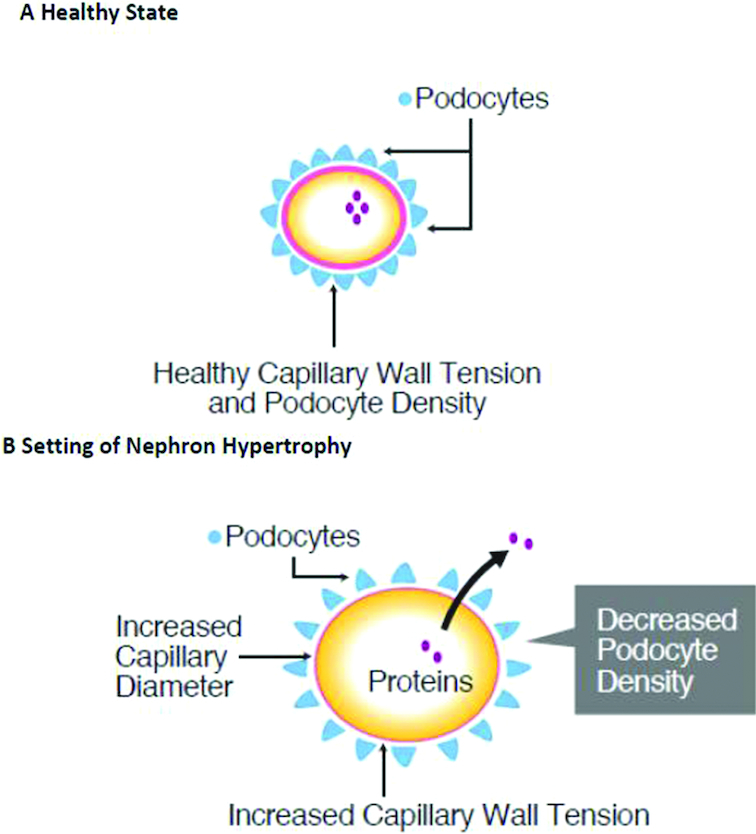
Distribution of podocytes around a glomerular capillary wall in a glomerulus in a healthy state (A) and in the setting of glomerular hypertrophy (B). Note that in the setting of glomerular hypertrophy, the density of podocyte distribution is decreased while the capillary diameter is increased, which leads to heightened capillary wall tension.
Receptors for AGEs are also found on mesangial cells, and when activated, they stimulate production of collagen and matrix, which accelerates glomerular sclerosis (40, 41). Diets high in protein may also suppress mitochondrial autophagy via activation of the mammalian target of a rapamycin complex 1 pathway (42, 43). Autophagy suppression results in reduced mitochondrial quality, and these damaged mitochondria accumulate in tubular cells of the kidney, which then incites inflammation and oxidative stress (43).
Kidney disease progression may also occur via nonhemodynamic mechanisms as a result of gut-derived uremic toxins such as trimethylamine N-oxide (TMAO) and p-cresyl sulfate, along with others in the setting of high protein and egg yolk intake. Although research is emerging regarding other gut-derived uremic toxins, existing evidence suggests that elevated TMAO levels accelerate CKD progression (44, 45) by enhancing phosphorylation of Smad3, a regulator of fibrosis via transduction of TGF-β and acceleration of glomerular scarring (44, 46). In the gastrointestinal tract, bacteria from the phyla Firmicutes and Proteobacteria metabolize phosphatidylcholine, choline, and l-carnitine into TMAO, which is then filtered and excreted by the kidney (Figure 3). TMAO levels are inversely associated with GFR and are generally increased in persons with CKD, depending on diet (47). Although diets high in red meat and egg yolks can lead to higher levels of TMAO (44), there appear to be substantial inter-individual differences in TMAO levels in response to dietary intake of TMAO precursors such as egg yolks and red meat (48, 49). After challenged with a TMAO precursor such as carnitine, individuals who are long-term meat eaters tend to have higher concentrations of TMAO compared with those who follow a vegetarian diet (50). Such differences in response to TMAO precursors may be a function of the uniqueness of the gastrointestinal microbiome shaped by long-term dietary habits. Endosymbiotic bacteria such as Bifidobacterium inhibit gram-negative pathogen growth and thus reduce the production of gut-derived uremic toxins (51–54). Unfortunately, existing trials of probiotics and oral adsorbents to reduce gut-derived uremic toxins have shown no impact on kidney disease progression (54, 55).
FIGURE 3.

Dietary sources of choline, phosphatidylcholine, and l-carnitine include red meat, cheese, and egg yolk. Choline, phosphatidylcholine, and l-carnitine are metabolized in the gut, leading to production of trimethylamine N-oxide and p-cresyl sulfate. These uremic toxins are excreted by the kidney, and in the setting of reduced kidney function, circulating levels may increase and contribute to atherosclerosis. CKD, chronic kidney disease.
Clinical Trials of Protein Restriction for CKD
One of the largest clinical trials to examine the association between protein intake and kidney disease progression was the Modification of Diet in Renal Disease (MDRD) study (56). The MDRD study randomized 585 adults with established CKD (predominantly nondiabetic) and GFR of 25 to 55 mL · min−1 · 1.73 m−2 to either a usual-protein diet (1.3 g·kg−1·d−1) or a low-protein diet (0.58 g·kg−1·d−1) and followed them over time for loss of GFR. Although the decline in GFR was slower with the low-protein diet, differences in GFR decline did not meet statistical significance and the overall findings were null. Multiple clinical trials of protein restriction have been summarized in meta-analyses, and findings show a moderate effect of protein restriction on GFR decline (57–59); however, results are mixed. Among adults with established CKD, moderate protein restriction (∼0.7 g·kg−1·d−1) compared with a standard protein intake (∼1.0 g·kg−1·d−1) is associated with a 0.95 mL · min−1 · 1.73 m−2 (95% CI: 0.11, 1.79) slower kidney function decline. However, effects differ by diabetes status, with markedly weaker effects noted in patients with type 2 diabetes (57). Among a total of 10 trials, very-low-protein diets reduced risk of progression to ESRD by 35% (95% CI: 0.49, 0.85) among adults with advanced kidney disease (59). Very-low-protein diets require supplementation with essential amino acids and close monitoring to ensure adequate caloric and macronutrient intake (56). A recent meta-analysis found no significant mortality risk with very-low-protein diets compared with low- or normal-protein diets in adults with CKD (59); however, the risks of this intervention should not be discounted. Long-term follow-up of the MDRD study found that individuals with a baseline GFR of 13–24 mL · min−1 · 1.73 m−2 assigned to a very-low-protein diet (0.28 g·kg−1·d−1) supplemented with a mixture of essential keto acids and amino acids showed an almost 2-fold increased risk of death (95% CI: 1.15, 3.20) but no significant difference in kidney failure risk (HR: 0.83; 95% CI: 0.62, 1.12) compared with participants allocated to a protein intake of 0.58 g·kg−1·d−1 (60). Low-protein diets also increase the risk of protein-energy wasting, sarcopenia, and frailty, which can negatively impact quality of life (42). Such risks must be considered because low-protein diets may not be appropriate for some patients with CKD, especially those who are older and at risk for malnutrition.
An important limitation of previous controlled trials of protein restriction is that dietary trials have largely focused on restricting total protein rather than on the type of protein intake (animal compared with vegetable). Protein type may be more important for kidney disease progression than the total amount of protein intake. One cohort study that examined kidney disease outcomes during a 15-y period among 63,257 Chinese adults with a mean BMI (kg/m2) of 23 found no dose-dependent association between quartiles of total protein intake and ESRD risk (61). However, higher red meat intake was associated with increased risk of ESRD, whereas non-red meat sources of protein were not associated with ESRD (61).
An analysis of the Atherosclerosis Risk in Communities (ARIC) study, a US cohort of 14,882 adults with baseline estimated GFR (eGFR) ≥60 mL · min−1 · 1.73 m−2, also showed significantly higher risk of CKD (eGFR <60 mL · min−1 · 1.73 m−2 combined with a ≥25% eGFR decline at any follow-up study visit relative to baseline eGFR) with increasing intake of red and processed meat. The highest quartile of red and processed meat intake was associated with a 22% higher risk of CKD (95% CI: 1.07, 1.40) compared with the lowest quartile (P-trend = 0.02). In contrast, strong adherence to the Dietary Approaches to Stop Hypertension (DASH) diet—a diet characterized by low intake of red and processed meat and high intake of fruits, vegetables, and low-fat dairy products—was associated with a 14% lower risk of CKD compared with those with the lowest adherence to a DASH-type diet over a median follow-up period of 23 y. The only other individual DASH diet component that was significantly associated with CKD risk was low-fat dairy products. Even after adjustment for demographics, overweight and obesity, diabetes, and hypertension status along with systolic blood pressure levels, a significant trend in CKD risk (P < 0.001) was noted across quintiles of low-fat dairy intake, with the highest quintile associated with a 16% lower risk for CKD (95% CI: 5%, 25%) compared with the lowest quintile.
Clinical trial data remain limited regarding the impact of a vegetarian diet on CKD outcomes. Garneata et al. (62) examined whether a low-protein diet with vegetable sources of protein (0.3 g·kg−1·d−1) supplemented with ketoanalogs slows CKD progression relative to a low-protein diet (0.6 g·kg−1·d−1) with mixed protein sources. A total of 208 adults with eGFR <30 mL · min−1 · 1.73 m−2 and no diabetes were followed for 1.5 y. The rate of renal replacement therapy initiation was significantly lower among participants assigned to the vegetarian protein diet supplemented with ketoanalogs compared with the mixed protein intake (11% compared with 30%; P < 0.001). In addition, a 50% decline in GFR and/or initiation of renal replacement therapy occurred in 13% of the vegetarian protein diet group and 42% of the mixed low-protein intake group (P < 0.001). Note that only 14% of screened individuals were randomized into the trial, so the intervention may not be acceptable to some patients. In addition, the total protein intake may not have differed substantially between the two groups due to use of ketoanalogs.
The most recent nutrition guidelines published in 2010 by the Academy of Nutrition and Dietetics recommend that dietary protein intake be maintained at 0.6–0.8 g· kg−1· d−1 when eGFR is <50 mL · min−1 · 1.73 m−2. When eGFR is <20 mL · min−1 · 1.73 m−2, then a very-low-protein diet (0.3–0.5 g·kg−1·d−1) can be considered as long as keto acid analogs are available in order to meet protein requirements (63). A higher amount of protein intake (0.8 or 0.9 g·kg−1·d−1) is recommended for persons with diabetic nephropathy because meta-analyses have not consistently demonstrated significant lowering of kidney disease progression with protein restriction in this population (57). The type of protein intake is not specified in the recommendations by the Academy, but the guidelines do mention that consumption of red meat increases urine albumin excretion in patients with CKD (63).
Phosphate
Protein sources contain phosphate, with phosphate content in plant protein mainly in the form of phytic acid (64). Absorption of phosphate from phytic acid requires the enzyme phytase, which shows low activity in humans (64). Thus, net gastrointestinal phosphate absorption from plant protein sources is substantially lower than phosphate obtained from animal protein or from foods preserved with inorganic phosphate (65). In animal models, high phosphate intake leads to necrosis of the kidney tubules, interstitial scarring, and nephrocalcinosis, and effects are magnified in the setting of reduced nephron number with partial nephrectomy (66, 67). Restriction of phosphate intake can also ameliorate tubular injury and scarring, and it can ameliorate kidney disease progression in partially nephrectomized animals (68–71) or in experimental animal models of immunologic kidney disease (72). Although habitual phosphate intake in humans does not mirror intake in these animal studies of phosphate injury, use of sodium phosphate enemas for bowel preparation can add >10 g of elemental phosphate and incite phosphate nephropathy and kidney failure (73–76).
To date, high dietary phosphate intake has not been established as a substantial risk factor for kidney disease or its progression, but data are emerging (77). One nonrandomized study of a dietary intervention with 0.3 g·kg−1·d−1 of protein supplemented with ketoanalogs among adults with established proteinuric kidney disease found that participants with lower phosphate intake showed greater reductions in urine protein excretion (78). A post hoc analysis of the PREMIER trial (79) found that reduced urinary phosphate excretion with a dietary intervention was predictive of subsequent decreases in urine albumin excretion among participants with normal kidney function (77). Other studies have shown no substantial difference in kidney disease outcomes with measures of dietary phosphate intake (80, 81), but null findings may be due to the inherent difficulties in assessing dietary phosphate intake (77). Potential mechanisms whereby high dietary phosphate intake may harm the kidney include abrogation of endothelial function (82, 83) and facilitation of calcium deposition in the kidney and vessels (77).
Dietary Fat
Although mortality risk appears heightened among adults with CKD consuming a diet rich in fried foods and animal fat (84), the role of dietary fat in CKD incidence and progression remains poorly studied. Dietary fat does appear to influence glomerular hyperfiltration as defined by a GFR >2 SD above normal (85). However, studies have not consistently demonstrated an association between saturated fat intake and kidney function decline or ESRD (9, 86–88). In contrast, cross-sectional studies have consistently demonstrated an association between higher saturated fat intake and the presence of increased urine albumin excretion (9, 86, 88), but this association may be confounded by the effects of dietary saturated fat on blood pressure (89, 90).
Dietary n–3 PUFAs may be beneficial for slowing kidney disease progression. Supplementation of n–3 PUFAs decreases mesangial cell proliferation and matrix production, enhances endothelial function, and lowers blood pressure (91, 92). A few studies have reported that higher plasma levels of n–3 PUFAs correlate with slower decline in GFR over time in older adults or in adults with established CKD, but findings have not been consistent (93). Randomized controlled trials of n–3 PUFAs on kidney disease progression in adults with established CKD have largely shown no benefit for slowing GFR decline but have demonstrated small reductions in urine protein excretion (91, 93). Existing trials are small with short duration, heterogeneous, and encompass a wide variety of kidney disease etiologies; thus, more studies are needed (91).
Salt
For this discussion, salt refers to sodium chloride. Decades of research has confirmed the deleterious effects of high sodium chloride intake on blood pressure, cardiovascular disease, kidney function, and CKD progression (94). Although sodium is a cation that can bind with multiple anions, research has not demonstrated that intake of sodium bicarbonate, sodium phosphate, or sodium citrate incites injury similar to sodium chloride. Reducing salt intake remains an important intervention for reducing blood pressure in hypertensive individuals (94–96), and reductions in salt intake result in lower blood pressure and also lower urine albumin excretion (97–99). In the Ramipril Efficacy in Nephropathy trial, a randomized trial of ramipril compared with placebo in patients with nondiabetic kidney disease with high urine protein excretion, high salt intake was associated with a blunted response to 5 mg of ramipril daily (100). A meta-analysis of 11 different randomized clinical trials of salt reduction with or without blockade of the renin–angiotensin–aldosterone system (RAAS) supported the benefits of reducing salt intake for treatment of CKD (101). The weighted difference between high and low salt intake was 5.4 g based on 24-h urine collections. The lower salt intake was associated with a 32% (95% CI: 18.8%, 44.3%) lower urine albumin excretion compared with the high salt intake (101). When analyses were limited to participants receiving RAAS inhibitors, lower salt intake was associated with a 41% (95% CI: 27.4%, 56.4%) lower urine albumin excretion compared with high salt intake. The benefits of low salt intake were more pronounced with older age, advanced CKD, and obesity. Unfortunately, most clinical trials examining salt intake are short in duration and do not examine hard endpoints such as cardiovascular outcomes or need for renal replacement therapy.
The results from the previously mentioned meta-analysis (101) along with those of other previous studies (97, 98) suggest that many patients will benefit from salt reduction, especially older individuals and those with obesity and/or low GFR. Kidney disease is characterized by salt sensitivity (102), and high salt intake will increase blood pressure and lead to volume expansion, making blood pressure management more difficult in patients with kidney disease.
A high salt intake may accelerate kidney disease progression independent of blood pressure by impairing renal autoregulatory responses (103–105), but this hypothesis remains controversial (106, 107). In contrast, multiple studies have also demonstrated that high salt intake magnifies oxidative stress in the kidney by stimulating nicotinamide adenine dinucleotide and nicotinamide adenine dinucleotide phosphate superoxide anion generation (108, 109). Scarring after nephron loss can also be amplified with a high salt intake due to upregulation of TGF-β (110, 111).
The average sodium intake among US adults, as estimated by nutrition surveys and timed urine collections, is approximately 4 g/d among men and 3 g/d among women (112–114). Existing nutrition guidelines for CKD recommend sodium intake <2.4 g/d, but ideal intake may vary by age and comorbidities (62). The high salt content of the Western diet will elevate systemic blood pressure, expand extracellular volume, and increase oxidative stress in persons with CKD (108, 109). Patients with CKD should be encouraged to prepare their own meals without added salt and avoid processed foods.
Fruits and Vegetables
The kidneys regulate acid–base balance and must replace bicarbonate that is consumed with buffering of dietary acids. Generation of new bicarbonate (HCO3−) requires tubular excretion of nonvolatile acids and ammonium. Just like total GFR is the sum of single nephron GFR, total excretion of nonvolatile acids and ammonium is the sum of excretion from each individual nephron. With nephron loss, the remaining nephrons must increase their generation of new bicarbonate to prevent metabolic acidosis (115). Nonvolatile acids in the kidney are mainly produced when organic sulfur from methionine and cysteine is oxidized to inorganic sulfates.. These acids are then balanced by alkali obtained from the metabolizing of organic anions such as citrate and malate found in fruits and vegetables. The net endogenous acid production is equivalent to the total amount of endogenous acids minus the alkali from foods absorbed in the intestine (116). When acid load is increased (e.g., after a large meat meal), the kidneys will increase bicarbonate generation above its normal baseline by augmenting the excretion of ammonium (NH4+). Unlike the excretion of nonvolatile acids, the excretion of NH4+ can be increased several fold to maintain acid–base balance (115).
With reduced nephron number and high net endogenous acid load, the tubular ammonium concentration increases and can lead to tubular toxicity and damage. Augmentation of ammonium excretion due to high dietary acid load leads to heightened activity of the renin–angiotensin system within the tubules and increased production of endothelin-1, a potent vasoconstrictor that promotes tissue injury and scarring (117). High dietary acid load also activates the alternate complement cascade in the renal tubules and can lead to kidney injury (118–124). Diets high in fruits and vegetables and low in animal protein are associated with lower endogenous acid load and thus lower workload for each individual nephron.
The DASH diet is high in fruits and vegetables and low-fat dairy products and low in animal protein. Consumption of a DASH diet is associated with 50% lower net endogenous acid production compared with the typical Western diet (116). Simply increasing alkali intake with fruits and vegetables or with sodium bicarbonate tablets may lower net endogenous acid excretion by more than one-third (125), which may minimize individual nephron workload and slow loss of kidney function (126–128).
Dietary Fiber
The Western diet is associated with low fiber intake, which is often accompanied by elevated levels of inflammatory biomarkers such as serum C-reactive protein, IL-6, and TNF-α receptor 2 (129–132). Elevated inflammatory marker levels indicate increased cardiovascular and mortality risk regardless of CKD status (133–138) and also a heightened risk for both CKD incidence and progression (86, 139–141). Diets high in fiber can reduce cardiovascular disease risk (142–145) and are associated with reduced mortality rates in adults with CKD (146). The American Dietetic Association recommends that adults consume 28 g/d of dietary fiber based on a 2000 kcal/d diet (147) to lower cardiovascular risk. Currently, there are no specific recommendations for levels of dietary fiber intake for adults with CKD, but recommendations for the general population are likely safe and probably beneficial as long as serum potassium and phosphate levels are monitored (146).
Fiber intake may be especially important for individuals with advanced CKD or kidney failure when urea excretion is severely impaired due to low GFR. Urea directly disrupts the gut barrier function by reducing the presence of occludin and zonula occludens proteins in the tight junctions of the gastrointestinal gut barrier, increasing intestinal permeability and translocation of gut bacteria to the systemic circulation, and heightening inflammation. High-fiber diets may be protective in CKD by promoting the growth of commensal bacteria such as Bifidobacterium, an endosymbiotic colonizer of the gut that strengthens the gastrointestinal permeability barrier (53, 148–150). In addition, a high-fiber diet facilitates stool excretion and helps promote urea and potassium excretion (151).
Nutritional Guidelines for Non-Dialysis-Dependent CKD
The National Kidney Foundation–Kidney Disease Outcomes Quality Initiative Guidelines on Hypertension and Antihypertensive Agents in CKD recommended a modified version of the DASH diet for persons with CKD stages 3 and 4 (eGFR between 15 and 59 mL · min−1 · 1.73 m−2) (152). The DASH diet includes higher protein intake than the recommended daily allowance, but the majority of this protein is from dairy products, vegetable sources, and non-red meat. For persons with CKD, the DASH diet may be modified to achieve a protein intake of 0.6–0.8 g·kg−1·d−1 as well as a lower phosphorus (0.8–1.0 g/d) and potassium (2–4 g/d) intake. These recommendations are similar to the American Diabetes Association nutrition guidelines for persons with diabetes and CKD, which state that dietary protein intake should be consistent with the recommended daily allowance of 0.8 g·(kg·ideal body weight)−¹ ·d−1 for people with diabetes and CKD (153). Protein intake may be restricted to 0.6 g·(kg·ideal body weight)−¹ ·d−¹ when GFR decreases to <60 mL · min−1 · 1.73 m−2. High-protein diets should be avoided in persons with established CKD who are not receiving dialysis (154). Dietary fiber intake is encouraged for persons with CKD, but no specific levels of intake are suggested for this population (154). Information on the safety and benefits of vegetarian diets in CKD remains very limited, and this is an area of research need (155). With the introduction of new agents for management of elevated serum potassium levels that are well tolerated, diets can now be liberalized to include more potassium-rich fruits and vegetables.
Medical Nutrition Therapy
Because dietary practices strongly influence CKD incidence and progression, medical nutrition therapy (MNT) is recommended for all patients with CKD (63, 156). Although primary care providers and nephrologists often counsel patients on optimal dietary practices, MNT services provided by a registered dietitian nutritionist provide individualized dietary evaluation and counseling and have been shown to be cost-effective (157–162), improve control of diabetes and hypertension, and even slow CKD progression and delay need for dialysis (56, 58, 163–167). MNT services are not meant to be a single time-point intervention but should instead include periodic monitoring and reassessment of dietary interventions tailored to slow disease progression. Medicare provides 3 h of MNT counseling during the first year for patients with eGFR <50 mL · min−1 · 1.73 m−2 who are not receiving dialysis. During subsequent years, patients may receive 2 h of MNT services per year (168). Additional hours of MNT services can be utilized if the physician determines that a change in diagnosis is necessary or that a medical condition requires dietary changes. Most private insurance companies also cover MNT services similar to Medicare. Unfortunately, less than 10% of adults with CKD receive any dietary care prior to initiation of dialysis (5).
Research Needs
Given the low intake of fruits and vegetables and high intake of animal meat, fat, and processed foods in the majority of the US population, it is imperative that research determine optimal methods for improving the diets of adults, including those with kidney disease. Such research could examine use of telehealth services combined with mobile device applications or policy initiatives to incentivize utilization of medical nutrition therapies. More research is also needed to examine the impact of specific dietary patterns, such as the Mediterranean diet or vegan diets, on kidney disease outcomes. Fruits and vegetables are often avoided by patients with advanced kidney disease due to risk of hyperkalemia. New and safe medications that prevent elevated serum potassium levels (169) can now be incorporated into dietary trials for patients with advanced CKD. Trials of very-low-protein diets have mainly required patients follow the dietary intervention daily. Future trials could examine whether intermittent protein restriction retards kidney disease progression.
In summary, dietary factors are important for determining the workload of each individual nephron. In the setting of CKD and reduced working nephron number, each individual nephron is already at risk for hemodynamic injury. High intake of animal protein and egg yolks combined with low intake of fruits and vegetables is extremely conducive for nephron injury, and mechanisms of injury are not duplicative. Although a modified DASH diet is encouraged for patients with CKD, more studies are needed to determine the benefits and risks of vegetarian diets in this population. Clinicians should consider the dietary patterns, traditions, and culture of their patients when providing dietary advice and utilize medical nutrition therapy services to guide their patients to a healthier diet.
Acknowledgments
The author thanks Tom Mattix for creating the figures. The sole author had responsibility for all parts of the manuscript.
Notes
Published in a supplement to Advances in Nutrition. This supplement was sponsored by the Harding-Buller Foundation of Ohio. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the sponsors. Publication costs for this supplement were defrayed in part by the payment of page charges. The opinions expressed in this publication are those of the authors and are not attributable to the sponsors or the publisher, Editor, or Editorial Board of Advances in Nutrition.
The author reported no funding received for this study.
Author disclosures: The author report no conflicts of interest.
Supplementary data are available at https://academic.oup.com/advances/.
Abbreviations used: AGE, advanced glycation end products; CKD, chronic kidney disease; DASH, Dietary Approaches to Stop Hypertension; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; GFR, glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; MNT, medical nutrition therapy; TMAO, trimethylamine N-oxide.
References
- 1. Centers for Disease Control and Prevention. National Chronic Kidney Disease Fact Sheet, 2017[Internet]. Atlanta (GA): US Department of Health and Human Services, Centers for Disease Control and Prevention; 2017. Available from: https://www.cdc.gov/kidneydisease/pdf/kidney_factsheet.pdf. [Google Scholar]
- 2. United States Renal Data System. 2018 USRDS Annual Data Report: cardiovascular disease in patients with CKD [Internet] National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Disease. Bethesda (MD). 2018. Available from: https://www.usrds.org. [Google Scholar]
- 3. United States Renal Data System. 2015 USRDS Annual Data Report: cardiovascular disease in patients with ESRD [Internet] National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Disease. Bethesda (MD).2018[cited 20 Oct, 2018]. Available from: https://www.usrds.org. [Google Scholar]
- 4. Wang Y, Chen X, Song Y, Caballero B, Cheskin LJ. Association between obesity and kidney disease: a systematic review and meta-analysis. Kidney Int. 2008;73(1):19–33. [DOI] [PubMed] [Google Scholar]
- 5. United States Renal Data System. 2017 USRDS Annual Data Report: end-stage renal disease (ESRD) in the United States. Chapter 1: incidence and prevalence, patient characteristics, and treatment modalities [Internet] National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Disease; Bethesda (MD) 2017[cited 1 May, 2018]. Available from: https://www.usrds.org. [Google Scholar]
- 6. Hoerger TJ, Simpson SA, Yarnoff BO, Pavkov ME, Rios Burrows N, Saydah SH, Williams DE, Zhuo X. The future burden of CKD in the United States: a simulation model for the CDC CKD Initiative. Am J Kidney Dis. 2015;65(3):403–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Small C, Kramer HJ, Griffin KA, Vellanki K, Leehey DJ, Bansal VK, Markossian TW. Non-dialysis dependent chronic kidney disease is associated with high total and out-of-pocket healthcare expenditures. BMC Nephrol. 2017;18(1):3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. United States Renal Data System. United States Renal Data System Annual Data Report 2013. ESRD Chapter 11: costs of ESRD [Internet] National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Disease. Bethesda (MD). 2016[cited 6 May, 2018]. Available from: https://www.usrds.org. [Google Scholar]
- 9. Lin J, Fung TT, Hu FB, Curhan GC. Association of dietary patterns with albuminuria and kidney function decline in older white women: a subgroup analysis from the Nurses' Health Study. Am J Kidney Dis. 2011;57(2):245–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kramer H. Kidney disease and the Westernization and industrialization of food. Am J Kidney Dis. 2017; 70(1):111–21. [DOI] [PubMed] [Google Scholar]
- 11. Thomas G, Sehgal AR, Kashyap SR, Srinivas TR, Kirwan JP, Navaneethan SD. Metabolic syndrome and kidney disease: a systematic review and meta-analysis. Clin J Am Soc Nephrol. 2011;6(10):2364–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Garrison RJ, Kannel WB, Stokes J 3rd, Castelli WP. Incidence and precursors of hypertension in young adults: the Framingham Offspring Study. Prev Med. 1987;16(2):235–51. [DOI] [PubMed] [Google Scholar]
- 13. Hu FB, Manson JE, Stampfer MJ, Colditz G, Liu S, Solomon CG, Willett WC. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N Engl J Med. 2001;345(11):790–7. [DOI] [PubMed] [Google Scholar]
- 14. Hoy WE, Douglas-Denton RN, Hughson MD, Cass A, Johnson K, Bertram JF. A stereological study of glomerular number and volume: preliminary findings in a multiracial study of kidneys at autopsy. Kidney Int Suppl. 2003;(83):S31–7. [DOI] [PubMed] [Google Scholar]
- 15. Bertram JF, Douglas-Denton RN, Diouf B, Hughson MD, Hoy WE. Human nephron number: implications for health and disease. Pediatr Nephrol. 2011;26(9):1529–33. [DOI] [PubMed] [Google Scholar]
- 16. Moshfegh A, Goldman J, Cleveland L.. What we eat in America, NHANES 2001–2002: usual nutrient intake from foods as compared to Dietary Reference Intakes[Internet]. Washington (DC): US Department of Agriculture, Agricultural Research Service; 2005. Available from: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/0102/usualintaketables2001-02.pdf. [Google Scholar]
- 17. Landau D, Rabkin R. Effect of nutritional status and changes in protein intake on renal function. In: Kopple JD, Massry SG, Kalantar-Zadeh K, editors. Nutritional management of renal disease. 3rd ed Amsterdam: Elsevier; 2012. pp. 197–207. [Google Scholar]
- 18. Don BR, Blake S, Hutchison FN, Kaysen GA, Schambelan M. Dietary protein intake modulates glomerular eicosanoid production in the rat. Am J Physiol. 1989;256(4 Pt 2):F711–8. [DOI] [PubMed] [Google Scholar]
- 19. King AJ, Troy JL, Anderson S, Neuringer JR, Gunning M, Brenner BM. Nitric oxide: a potential mediator of amino acid-induced renal hyperemia and hyperfiltration. J Am Soc Nephrol. 1991;1(12):1271–7. [DOI] [PubMed] [Google Scholar]
- 20. Murakami M, Suzuki H, Ichihara A, Naitoh M, Nakamoto H, Saruta T. Effects of l-arginine on systemic and renal haemodynamics in conscious dogs. Clin Sci. 1991;81(6):727–32. [DOI] [PubMed] [Google Scholar]
- 21. Sabatino A, Regolisti G, Brusasco I, Cabassi A, Morabito S, Fiaccadori E. Alterations of intestinal barrier and microbiota in chronic kidney disease. Nephrol Dial Transplant. 2014;30(6):924–33. [DOI] [PubMed] [Google Scholar]
- 22. Ando A, Kawata T, Hara Y, Yaegashi M, Arai J, Sugino N. Effects of dietary protein intake on renal function in humans. Kidney Int Suppl. 1989;27:S64–7. [PubMed] [Google Scholar]
- 23. Aluko EO, Nna VU, Adekunbi DA. The possible mechanisms through which dietary protein increases renal blood flow and glomerular filtration rate. Br J Med Medical Res. 2015;7(6):458–69. [Google Scholar]
- 24. Griffin KA, Kramer H, Bidani AK. Adverse renal consequences of obesity. Am J Physiol Renal Physiol. 2008;294(4):F685–96. [DOI] [PubMed] [Google Scholar]
- 25. Loutzenhiser R, Griffin K, Williamson G, Bidani A. Renal autoregulation: new perspectives regarding the protective and regulatory roles of the underlying mechanisms. Am J Physiol Regul Integr Comp Physiol. 2006;290(5):R1153–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Bidani AK, Griffin KA. Long-term renal consequences of hypertension for normal and diseased kidneys. Curr Opin Nephrol Hypertens. 2002;11(1):73–80. [DOI] [PubMed] [Google Scholar]
- 27. Brenner BM, Lawler EV, Mackenzie HS. The hyperfiltration theory: a paradigm shift in nephrology. Kidney Int. 1996;49(6):1774–7. [DOI] [PubMed] [Google Scholar]
- 28. Cortes P, Riser B, Narins RG. Glomerular hypertension and progressive renal disease: the interplay of mesangial cell stretch, cytokine formation and extracellular matrix synthesis. Contrib Nephrol. 1996;118:229–33. [DOI] [PubMed] [Google Scholar]
- 29. Cortes P, Zhao X, Riser BL, Narins RG. Role of glomerular mechanical strain in the pathogenesis of diabetic nephropathy. Kidney Int. 1997;51(1):57–68. [DOI] [PubMed] [Google Scholar]
- 30. Riser BL, Cortes P, Zhao X, Bernstein J, Dumler F, Narins RG. Intraglomerular pressure and mesangial stretching stimulate extracellular matrix formation in the rat. J Clin Invest. 1992;90(5):1932–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Lee LK, Meyer TW, Pollock AS, Lovett DH. Endothelial cell injury initiates glomerular sclerosis in the rat remnant kidney. J Clin Invest. 1995;96(2):953–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Wrone EM, Carnethon MR, Palaniappan L, Fortmann SP, Third National Health and Nutrition Examination Survey . Association of dietary protein intake and microalbuminuria in healthy adults: Third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003;41(3):580–7. [DOI] [PubMed] [Google Scholar]
- 33. Hoogeveen EK, Kostense PJ, Jager A, Heine RJ, Jakobs C, Bouter LM, Donker AJ, Stehouwer CD. Serum homocysteine level and protein intake are related to risk of microalbuminuria: the Hoorn study. Kidney Int. 1998;54(1):203–9. [DOI] [PubMed] [Google Scholar]
- 34. Goldberg T, Cai W, Peppa M, Dardaine V, Baliga BS, Uribarri J, Vlassara H. Advanced glycoxidation end products in commonly consumed foods. J Am Diet Assoc. 2004;104(8):1287–91. [DOI] [PubMed] [Google Scholar]
- 35. Meek RL, LeBoeuf RC, Saha SA, Alpers CE, Hudkins KL, Cooney SK, Anderberg RJ, Tuttle KR. Glomerular cell death and inflammation with high-protein diet and diabetes. Nephrol Dial Transplant. 2013;28(7):1711–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Uribarri J, Tuttle KR. Advanced glycation end products and nephrotoxicity of high-protein diets. Clin J Am Soc Nephrol. 2006;1(6):1293–9. [DOI] [PubMed] [Google Scholar]
- 37. Chuang PY, Yu Q, Fang W, Uribarri J, He JC. Advanced glycation endproducts induce podocyte apoptosis by activation of the FOXO4 transcription factor. Kidney Int. 2007;72(8):965–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Wiggins JE, Goyal M, Sanden SK, Wharram BL, Shedden KA, Misek DE, Kuick RD, Wiggins RC. Podocyte hypertrophy, “adaptation,” and “decompensation” associated with glomerular enlargement and glomerulosclerosis in the aging rat: prevention by calorie restriction. J Am Soc Nephrol. 2005;16(10):2953–66. [DOI] [PubMed] [Google Scholar]
- 39. Rennke HG, Klein PS. Pathogenesis and significance of nonprimary focal and segmental glomerulosclerosis. Am J Kidney Dis. 1989;13(6):443–56. [DOI] [PubMed] [Google Scholar]
- 40. Vlassara H, Striker LJ, Teichberg S, Fuh H, Li YM, Steffes M. Advanced glycation end products induce glomerular sclerosis and albuminuria in normal rats. Proc Natl Acad Sci USA. 1994;91(24):11704–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Horie K, Miyata T, Maeda K, Miyata S, Sugiyama S, Sakai H, van Ypersole de Strihou C, Monnier VM, Witztum JL, Kurokawa K. Immunohistochemical colocalization of glycoxidation products and lipid peroxidation products in diabetic renal glomerular lesions: implication for glycoxidative stress in the pathogenesis of diabetic nephropathy. J Clin Invest. 1997;100(12):2995–3004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Kitada M, Ogura Y, Monno I, Koya D. A low-protein diet for diabetic kidney disease: its effect and molecular mechanism, an approach from animal studies. Nutrients. 2018;10(5):10.3390/nu10050544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Kitada M, Takeda A, Nagai T, Ito H, Kanasaki K, Koya D. Dietary restriction ameliorates diabetic nephropathy through anti-inflammatory effects and regulation of the autophagy via restoration of Sirt1 in diabetic Wistar fatty (fa/fa) rats: a model of type 2 diabetes. Exp Diabetes Res. 2011;2011:908185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Tang WH, Wang Z, Kennedy DJ, Wu Y, Buffa JA, Agatisa-Boyle B, Li XS, Levison BS, Hazen SL Gut microbiota-dependent trimethylamine N-oxide (TMAO) pathway contributes to both development of renal insufficiency and mortality risk in chronic kidney disease. Circ Res. 2015;116(3):448–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Rhee EP, Clish CB, Ghorbani A, Larson MG, Elmariah S, McCabe E, Yang Q, Cheng S, Pierce K, Deik A et al.. A combined epidemiologic and metabolomic approach improves CKD prediction. J Am Soc Nephrol. 2013;24(8):1330–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Qu X, Li X, Zheng Y, Ren Y, Puelles VG, Caruana G, Nikolic-Paterson DJ, Li J. Regulation of renal fibrosis by Smad3 Thr388 phosphorylation. Am J Pathol. 2014;184(4):944–52. [DOI] [PubMed] [Google Scholar]
- 47. Pignanelli M, Bogiatzi C, Gloor G, Allen-Vercoe E, Reid G, Urquhart BL, Ruetz KN, Velenosi TJ, Spence JD. Moderate renal impairment and toxic metabolites produced by the intestinal microbiome: dietary implications. J Ren Nutr. 2018;29(1):55–64. [DOI] [PubMed] [Google Scholar]
- 48. Cho CE, Caudill MA. Trimethylamine-N-oxide: friend, foe, or simply caught in the cross-fire?. Trends Endocrinol Metab. 2017;28(2):121–30. [DOI] [PubMed] [Google Scholar]
- 49. Tang WH, Wang Z, Levison BS, Koeth RA, Britt EB, Fu X, Wu Y, Hazen SL. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013;368(17):1575–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, Britt EB, Fu X, Wu Y, Li L. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19(5):576–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Kuo SM. The interplay between fiber and the intestinal microbiome in the inflammatory response. Advances in Nutrition. 2013;4(1):16–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Lievin V, Peiffer I, Hudault S, Rochat F, Brassart D, Neeser JR, Servin AL. Bifidobacterium strains from resident infant human gastrointestinal microflora exert antimicrobial activity. Gut. 2000;47(5):646–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Langlands SJ, Hopkins MJ, Coleman N, Cummings JH. Prebiotic carbohydrates modify the mucosa associated microflora of the human large bowel. Gut. 2004;53(11):1610–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Rossi M, Johnson DW, Morrison M, Pascoe EM, Coombes JS, Forbes JM, Szeto CC, McWhinney BC, Ungerer JP, Campbell KL. Synbiotics Easing Renal Failure by Improving Gut Microbiology (SYNERGY): a randomized trial. Clin J Am Soc Nephrol. 2016;11(2):223–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Cha RH, Kang SW, Park CW, Cha DR, Na KY, Kim SG, Yoon SA, Han SY, Chang JH, Park SK et al.. A randomized, controlled trial of oral intestinal sorbent AST-120 on renal function deterioration in patients with advanced renal dysfunction. Clin J Am Soc Nephrol. 2016;11(4):559–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, Striker G. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease: Modification of Diet in Renal Disease Study Group. N Engl J Med. 1994;330(13):877–84. [DOI] [PubMed] [Google Scholar]
- 57. Rughooputh MS, Zeng R, Yao Y. Protein diet restriction slows chronic kidney disease progression in non-diabetic and in type 1 diabetic patients, but not in type 2 diabetic patients: a meta-analysis of randomized controlled trials using glomerular filtration rate as a surrogate. PLoS One. 2015;10(12):e0145505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Kasiske BL, Lakatua JD, Ma JZ, Louis TA. A meta-analysis of the effects of dietary protein restriction on the rate of decline in renal function. Am J Kidney Dis. 1998;31(6):954–61. [DOI] [PubMed] [Google Scholar]
- 59. Hahn D, Hodson EM, Fouque D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst Rev. 2018;10:CD001892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Menon V, Kopple JD, Wang X, Beck GJ, Collins AJ, Kusek JW, Greene T, Levey AS, Sarnak MJ. Effect of a very low-protein diet on outcomes: long-term follow-up of the Modification of Diet in Renal Disease (MDRD) study. Am J Kidney Dis. 2009;53(2):208–17. [DOI] [PubMed] [Google Scholar]
- 61. Lew QJ, Jafar TH, Koh HW, Jin A, Chow KY, Yuan JM, Koh WP. Red meat intake and risk of ESRD. J Am Soc Nephrol. 2016;28(1):304–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Garneata L, Stancu A, Dragomir D, Stefan G, Mircescu G. Ketoanalogue-supplemented vegetarian very low-protein diet and CKD progression. J Am Soc Nephrol. 2016;27(7):2164–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Academy of Nutrition and Dietetics. Chronic Kidney Disease (CKD) Evidence-Based Nutrition Practice Guideline [Internet] 2010. Chicago (IL) [cited 1 Dec, 2018]. Available from: http://www.andeal.org/vault/pq119.pdf. [Google Scholar]
- 64. Iqbal TH, Lewis KO, Cooper BT. Phytase activity in the human and rat small intestine. Gut. 1994;35(9):1233–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Kalantar-Zadeh K, Gutekunst L, Mehrotra R, Kovesdy CP, Bross R, Shinaberger CS, Noori N, Hirschberg R, Benner D, Nissenson AR et al.. Understanding sources of dietary phosphorus in the treatment of patients with chronic kidney disease. Clin J Am Soc Nephrol. 2010;5(3):519–30. [DOI] [PubMed] [Google Scholar]
- 66. Mackay EM, Oliver J. Renal damage following the ingestion of a diet containing an excess of inorganic phosphate. J Exp Med. 1935;61(3):319–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Haut LL, Alfrey AC, Guggenheim S, Buddington B, Schrier N. Renal toxicity of phosphate in rats. Kidney Int. 1980;17(6):722–31. [DOI] [PubMed] [Google Scholar]
- 68. Ross LA, Finco DR, Crowell WA. Effect of dietary phosphorus restriction on the kidneys of cats with reduced renal mass. Am J Vet Res. 1982;43(6):1023–6. [PubMed] [Google Scholar]
- 69. Lumlertgul D, Burke TJ, Gillum DM, Alfrey AC, Harris DC, Hammond WS, Schrier RW. Phosphate depletion arrests progression of chronic renal failure independent of protein intake. Kidney Int. 1986;29(3):658–66. [DOI] [PubMed] [Google Scholar]
- 70. Ibels LS, Alfrey AC, Haut L, Huffer WE. Preservation of function in experimental renal disease by dietary restriction of phosphate. N Engl J Med. 1978;298(3):122–6. [DOI] [PubMed] [Google Scholar]
- 71. Brown SA, Crowell WA, Barsanti JA, White JV, Finco DR. Beneficial effects of dietary mineral restriction in dogs with marked reduction of functional renal mass. J Am Soc Nephrol. 1991;1(10):1169–79. [DOI] [PubMed] [Google Scholar]
- 72. Karlinsky ML, Haut L, Buddington B, Schrier NA, Alfrey AC. Preservation of renal function in experimental glomerulonephritis. Kidney Int. 1980;17(3):293–302. [DOI] [PubMed] [Google Scholar]
- 73. Eckstein J, Savic S, Eugster T, Pargger H, Gurke L, Pechula M, Steiger J, Mayr M. Extensive calcifications induced by hyperphosphataemia caused by phosphate-based enema in a patient after kidney transplantation. Nephrol Dial Transplant. 2006;21(7):2013–6. [DOI] [PubMed] [Google Scholar]
- 74. Connor A, Sykes L, Roberts IS, Weston CE. Acute phosphate nephropathy after sodium phosphate preparations. BMJ. 2008;337:a182. [DOI] [PubMed] [Google Scholar]
- 75. Arikan H, Guler D, Birdal G, Nalcaci S, Aykut E, Ozcan C, Irmak R, Banzragch M, Arzu V. Massive hyperphosphatemia in a patient with neuronal intestinal dysplasia after bowel preparation with oral sodium phosphate. Ren Fail. 2013;35(6):875–8. [DOI] [PubMed] [Google Scholar]
- 76. Schaefer M, Littrell E, Khan A, Patterson ME. Estimated GFR decline following sodium phosphate enemas versus polyethylene glycol for screening colonoscopy: a retrospective cohort study. Am J Kidney Dis. 2016;67(4):609–16. [DOI] [PubMed] [Google Scholar]
- 77. Chang AR, Anderson C. Dietary phosphorus intake and the kidney. Annu Rev Nutr. 2017;37:321–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Di Iorio BR, Bellizzi V, Bellasi A, Torraca S, D'Arrigo G, Tripepi G, Zoccali C. Phosphate attenuates the anti-proteinuric effect of very low-protein diet in CKD patients. Nephrol Dial Transplant. 2013;28(3):632–40. [DOI] [PubMed] [Google Scholar]
- 79. Appel LJ, Champagne CM, Harsha DW, Cooper LS, Obarzanek E, Elmer PJ, Stevens VJ, Vollmer WM, Lin PH, Svetkey LP et al.. Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA. 2003;289(16):2083–93. [DOI] [PubMed] [Google Scholar]
- 80. Selamet U, Tighiouart H, Sarnak MJ, Beck G, Levey AS, Block G, Ix JH. Relationship of dietary phosphate intake with risk of end-stage renal disease and mortality in chronic kidney disease stages 3–5: the Modification of Diet in Renal Disease Study. Kidney Int. 2016;89(1):176–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Chang AR, Miller ER 3rd, Anderson CA, Juraschek SP, Moser M, White K, Henry B, Krekel C, Oh S, Charleston J et al.. Phosphorus additives and albuminuria in early stages of CKD: a randomized controlled trial. Am J Kidney Dis. 2017;69(2):200–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Shuto E, Taketani Y, Tanaka R, Harada N, Isshiki M, Sato M, Nashiki K, Amo K, Yamamoto H, Higashi Y et al.. Dietary phosphorus acutely impairs endothelial function. J Am Soc Nephrol. 2009;20(7):1504–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Nishi T, Shuto E, Ogawa M, Ohya M, Nakanishi M, Masuda M, Katsumoto M, Yamanaka-Okumura H, Sakai T, Takeda E et al.. Excessive dietary phosphorus intake impairs endothelial function in young healthy men: a time- and dose-dependent study. J Med Invest. 2015;62(3–4):167–72. [DOI] [PubMed] [Google Scholar]
- 84. Gutierrez OM, Muntner P, Rizk DV, McClellan WM, Warnock DG, Newby PK, Judd SE. Dietary patterns and risk of death and progression to ESRD in individuals with CKD: a cohort study. Am J Kidney Dis. 2014;64(2):204–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Bouhanick B, Suraniti S, Berrut G, Bled F, Simard G, Lejeune JJ, Fressinaud P, Marre M. Relationship between fat intake and glomerular filtration rate in normotensive insulin-dependent diabetic patients. Diabete Metab. 1995;21(3):168–72. [PubMed] [Google Scholar]
- 86. Lin J, Judd S, Le A, Ard J, Newsome BB, Howard G, Warnock DG, McClellan W. Associations of dietary fat with albuminuria and kidney dysfunction. Am J Clin Nutr. 2010;92(4):897–904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Lin J, Hu FB, Curhan GC. Associations of diet with albuminuria and kidney function decline. Clin J Am Soc Nephrol. 2010;5(5):836–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Nettleton JA, Steffen LM, Palmas W, Burke GL, Jacobs DR Jr. Associations between microalbuminuria and animal foods, plant foods, and dietary patterns in the Multiethnic Study of Atherosclerosis. Am J Clin Nutr. 2008;87(6):1825–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Wang L, Manson JE, Forman JP, Gaziano JM, Buring JE, Sesso HD. Dietary fatty acids and the risk of hypertension in middle-aged and older women. Hypertension. 2010;56(4):598–604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Mente A, Dehghan M, Rangarajan S, McQueen M, Dagenais G, Wielgosz A, Lear S, Li W, Chen H, Yi S et al.. Association of dietary nutrients with blood lipids and blood pressure in 18 countries: a cross-sectional analysis from the PURE study. Lancet Diabetes Endocrinol. 2017;5(10):774–87. [DOI] [PubMed] [Google Scholar]
- 91. Miller ER 3rd, Juraschek SP, Appel LJ, Madala M, Anderson CA, Bleys J, Guallar E. The effect of n–3 long-chain polyunsaturated fatty acid supplementation on urine protein excretion and kidney function: meta-analysis of clinical trials. Am J Clin Nutr. 2009;89(6):1937–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Grande JP, Walker HJ, Holub BJ, Warner GM, Keller DM, Haugen JD, Donadio JV Jr, Dousa TP. Suppressive effects of fish oil on mesangial cell proliferation in vitro and in vivo. Kidney Int. 2000;57(3):1027–40. [DOI] [PubMed] [Google Scholar]
- 93. Huang X, Lindholm B, Stenvinkel P, Carrero JJ. Dietary fat modification in patients with chronic kidney disease: n–3 fatty acids and beyond. J Nephrol. 2013;26(6):960–74. [DOI] [PubMed] [Google Scholar]
- 94. Wong MM, Arcand J, Leung AA, Thout SR, Campbell NR, Webster J. The science of salt: a regularly updated systematic review of salt and health outcomes (December 2015–March 2016). J Clin Hypertens (Greenwich). 2017;19(3):322–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MM et al.. A clinical trial of the effects of dietary patterns on blood pressure: DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117–24. [DOI] [PubMed] [Google Scholar]
- 96. Dyer AR, Elliott P, Shipley M. Urinary electrolyte excretion in 24 hours and blood pressure in the INTERSALT Study: II. Estimates of electrolyte–blood pressure associations corrected for regression dilution bias: the INTERSALT Cooperative Research Group. Am J Epidemiol. 1994;139(9):940–51. [DOI] [PubMed] [Google Scholar]
- 97. McMahon EJ, Bauer JD, Hawley CM, Isbel NM, Stowasser M, Johnson DW, Campbell KL. A randomized trial of dietary sodium restriction in CKD. J Am Soc Nephrol. 2013;24(12):2096–103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Campbell KL, Johnson DW, Bauer JD, Hawley CM, Isbel NM, Stowasser M, Whitehead JP, Dimeski G, McMahon E. A randomized trial of sodium-restriction on kidney function, fluid volume and adipokines in CKD patients. BMC Nephrol. 2014;15:57,2369-15-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Hwang JH, Chin HJ, Kim S, Kim DK, Kim S, Park JH, Shin SJ, Lee SH, Choi BS, Lim CS. Effects of intensive low-salt diet education on albuminuria among nondiabetic patients with hypertension treated with olmesartan: a single-blinded randomized, controlled trial. Clin J Am Soc Nephrol. 2014;9(12):2059–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Vegter S, Perna A, Postma MJ, Navis G, Remuzzi G, Ruggenenti P. Sodium intake, ACE inhibition, and progression to ESRD. J Am Soc Nephrol. 2012;23(1):165–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. D'Elia L, Rossi G, Schiano di Cola M, Savino I, Galletti F, Strazzullo P. Meta-analysis of the effect of dietary sodium restriction with or without concomitant renin–angiotensin–aldosterone system-inhibiting treatment on albuminuria. Clin J Am Soc Nephrol. 2015;10(9):1542–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Hall JE. Kidney dysfunction mediates salt-induced increases in blood pressure. Circulation. 2016;133(9):894–906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Saeed A, Dibona GF, Marcussen N, Guron G. High-NaCl intake impairs dynamic autoregulation of renal blood flow in ANG II-infused rats. Am J Physiol Regul Integr Comp Physiol. 2010;299(5):R1142–9. [DOI] [PubMed] [Google Scholar]
- 104. Saeed A, DiBona GF, Grimberg E, Nguy L, Mikkelsen ML, Marcussen N, Guron G. High-NaCl diet impairs dynamic renal blood flow autoregulation in rats with adenine-induced chronic renal failure. Am J Physiol Regul Integr Comp Physiol. 2014;306(6):R411–9. [DOI] [PubMed] [Google Scholar]
- 105. Fellner RC, Cook AK, O'Connor PM, Zhang S, Pollock DM, Inscho EW. High-salt diet blunts renal autoregulation by a reactive oxygen species-dependent mechanism. Am J Physiol Renal Physiol. 2014;307(1):F33–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Abu-Amarah I, Bidani AK, Hacioglu R, Williamson GA, Griffin KA. Differential effects of salt on renal hemodynamics and potential pressure transmission in stroke-prone and stroke-resistant spontaneously hypertensive rats. Am J Physiol Renal Physiol. 2005;289(2):F305–13. [DOI] [PubMed] [Google Scholar]
- 107. Aviv A, Hollenberg NK, Weder AB. Sodium glomerulopathy: tubuloglomerular feedback and renal injury in African Americans. Kidney Int. 2004;65(2):361–8. [DOI] [PubMed] [Google Scholar]
- 108. Kitiyakara C, Chabrashvili T, Chen Y, Blau J, Karber A, Aslam S, Welch WJ, Wilcox CS. Salt intake, oxidative stress, and renal expression of NADPH oxidase and superoxide dismutase. J Am Soc Nephrol. 2003;14(11):2775–82. [DOI] [PubMed] [Google Scholar]
- 109. Weir MR, Fink JC. Salt intake and progression of chronic kidney disease: an overlooked modifiable exposure? A commentary. Am J Kidney Dis. 2005;45(1):176–88. [DOI] [PubMed] [Google Scholar]
- 110. Ying WZ, Sanders PW. Dietary salt modulates renal production of transforming growth factor-beta in rats. Am J Physiol. 1998;274(4 Pt 2):F635–41. [DOI] [PubMed] [Google Scholar]
- 111. Ying WZ, Sanders PW. Dietary salt increases endothelial nitric oxide synthase and TGF-β1 in rat aortic endothelium. Am J Physiol. 1999;277(4 Pt 2):H1293–8. [DOI] [PubMed] [Google Scholar]
- 112. Tayo BO, Luke A, McKenzie CA, Kramer H, Cao G, Durazo-Arvizu R, Forrester T, Adeyemo AA, Cooper RS. Patterns of sodium and potassium excretion and blood pressure in the African diaspora. J Hum Hypertens. 2012;26(5):315–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Eckberg K, Kramer H, Wolf M, Durazo-Arvizu R, Tayo B, Luke A, Cooper RS. Impact of Westernization on fibroblast growth factor 23 levels among individuals of African ancestry. Nephrol Dial Transplant. 2015;30(4):630–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Jackson SL, King SM, Zhao L, Cogswell ME. Prevalence of excess sodium intake in the United States—NHANES, 2009–2012. MMWR Morb Mortal Wkly Rep. 2016;64(52):1393–7. [DOI] [PubMed] [Google Scholar]
- 115. Hamm LL, Nakhoul N, Hering-Smith KS. Acid–base homeostasis. Clin J Am Soc Nephrol. 2015;10(12):2232–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Scialla JJ, Anderson CA. Dietary acid load: a novel nutritional target in chronic kidney disease?. Adv Chronic Kidney Dis. 2013;20(2):141–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. Kohan DE, Barton M. Endothelin and endothelin antagonists in chronic kidney disease. Kidney Int. 2014;86(5):896–904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Wesson DE, Jo CH, Simoni J. Angiotensin II receptors mediate increased distal nephron acidification caused by acid retention. Kidney Int. 2012;82(11):1184–94. [DOI] [PubMed] [Google Scholar]
- 119. Wesson DE, Simoni J, Broglio K, Sheather S. Acid retention accompanies reduced GFR in humans and increases plasma levels of endothelin and aldosterone. Am J Physiol Renal Physiol. 2011;300(4):F830–7. [DOI] [PubMed] [Google Scholar]
- 120. Wesson DE, Simoni J. Acid retention during kidney failure induces endothelin and aldosterone production which lead to progressive GFR decline, a situation ameliorated by alkali diet. Kidney Int. 2010;78(11):1128–35. [DOI] [PubMed] [Google Scholar]
- 121. Wesson DE, Simoni J, Prabhakar S. Endothelin-induced increased nitric oxide mediates augmented distal nephron acidification as a result of dietary protein. J Am Soc Nephrol. 2006;17(2):406–13. [DOI] [PubMed] [Google Scholar]
- 122. Khanna A, Simoni J, Wesson DE. Endothelin-induced increased aldosterone activity mediates augmented distal nephron acidification as a result of dietary protein. J Am Soc Nephrol. 2005;16(7):1929–35. [DOI] [PubMed] [Google Scholar]
- 123. Khanna A, Simoni J, Hacker C, Duran MJ, Wesson DE. Increased endothelin activity mediates augmented distal nephron acidification induced by dietary protein. J Am Soc Nephrol. 2004;15(9):2266–75. [DOI] [PubMed] [Google Scholar]
- 124. Nath KA, Hostetter MK, Hostetter TH. Pathophysiology of chronic tubulo-interstitial disease in rats: interactions of dietary acid load, ammonia, and complement component C3. J Clin Invest. 1985;76(2):667–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Goraya N, Simoni J, Jo CH, Wesson DE. A comparison of treating metabolic acidosis in CKD stage 4 hypertensive kidney disease with fruits and vegetables or sodium bicarbonate. Clin J Am Soc Nephrol. 2013;8(3):371–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Goraya N, Simoni J, Jo C, Wesson DE. Dietary acid reduction with fruits and vegetables or bicarbonate attenuates kidney injury in patients with a moderately reduced glomerular filtration rate due to hypertensive nephropathy. Kidney Int. 2012;81(1):86–93. [DOI] [PubMed] [Google Scholar]
- 127. Mahajan A, Simoni J, Sheather SJ, Broglio KR, Rajab MH, Wesson DE. Daily oral sodium bicarbonate preserves glomerular filtration rate by slowing its decline in early hypertensive nephropathy. Kidney Int. 2010;78(3):303–9. [DOI] [PubMed] [Google Scholar]
- 128. Phisitkul S, Hacker C, Simoni J, Tran RM, Wesson DE. Dietary protein causes a decline in the glomerular filtration rate of the remnant kidney mediated by metabolic acidosis and endothelin receptors. Kidney Int. 2008;73(2):192–9. [DOI] [PubMed] [Google Scholar]
- 129. Ajani UA, Ford ES, Mokdad AH. Dietary fiber and C-reactive protein: findings from national health and nutrition examination survey data. J Nutr. 2004;134(5):1181–5. [DOI] [PubMed] [Google Scholar]
- 130. Johansson-Persson A, Ulmius M, Cloetens L, Karhu T, Herzig KH, Onning G. A high intake of dietary fiber influences C-reactive protein and fibrinogen, but not glucose and lipid metabolism, in mildly hypercholesterolemic subjects. Eur J Nutr. 2014;53(1):39–48. [DOI] [PubMed] [Google Scholar]
- 131. Ma Y, Griffith JA, Chasan-Taber L, Olendzki BC, Jackson E, Stanek EJ 3rd, Li W, Pagoto SL, Hafner AR, Ockene IS. Association between dietary fiber and serum C-reactive protein. Am J Clin Nutr. 2006;83(4):760–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Ma Y, Hebert JR, Li W, Bertone-Johnson ER, Olendzki B, Pagoto SL, Tinker L, Rosal MC, Ockene IS, Ockene JK et al.. Association between dietary fiber and markers of systemic inflammation in the Women's Health Initiative Observational Study. Nutrition. 2008;24(10):941–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Ahmadi-Abhari S, Luben RN, Wareham NJ, Khaw KT. Seventeen year risk of all-cause and cause-specific mortality associated with C-reactive protein, fibrinogen and leukocyte count in men and women: the EPIC-Norfolk study. Eur J Epidemiol. 2013;28(7):541–50. [DOI] [PubMed] [Google Scholar]
- 134. Oluleye OW, Folsom AR, Nambi V, Lutsey PL, Ballantyne CM; ARIC Study I . Troponin T, B-type natriuretic peptide, C-reactive protein, and cause-specific mortality. Ann Epidemiol. 2013;23(2):66–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. de Boer IH, Katz R, Chonchol MB, Fried LF, Ix JH, Kestenbaum B, Mukamal KJ, Peralta CA, Siscovick DS. Insulin resistance, cystatin C, and mortality among older adults. Diabetes Care. 2012;35(6):1355–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136. Ning H, Van Horn L, Shay CM, Lloyd-Jones DM. Associations of dietary fiber intake with long-term predicted cardiovascular disease risk and C-reactive protein levels (from the National Health and Nutrition Examination Survey Data [2005–2010]). Am J Cardiol. 2014;113(2):287–91. [DOI] [PubMed] [Google Scholar]
- 137. Hamer M, Stamatakis E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J Clin Endocrinol Metab. 2012;97(7):2482–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138. Shlipak MG, Fried LF, Cushman M, Manolio TA, Peterson D, Stehman-Breen C, Bleyer A, Newman A, Siscovick D, Psaty B. Cardiovascular mortality risk in chronic kidney disease: comparison of traditional and novel risk factors. JAMA. 2005;293(14):1737–45. [DOI] [PubMed] [Google Scholar]
- 139. Bash LD, Erlinger TP, Coresh J, Marsh-Manzi J, Folsom AR, Astor BC. Inflammation, hemostasis, and the risk of kidney function decline in the Atherosclerosis Risk in Communities (ARIC) study. Am J Kidney Dis. 2009;53(4):596–605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140. Shankar A, Sun L, Klein BE, Lee KE, Muntner P, Nieto FJ, Tsai MY, Cruickshanks KJ, Schubert CR, Brazy PC et al.. Markers of inflammation predict the long-term risk of developing chronic kidney disease: a population-based cohort study. Kidney Int. 2011;80(11):1231–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Hiramoto JS, Katz R, Peralta CA, Ix JH, Fried L, Cushman M, Sicovick D, Palmas W, Sarnak M, Shlipak MG. Inflammation and coagulation markers and kidney function decline: the Multi-Ethnic Study of Atherosclerosis (MESA). Am J Kidney Dis. 2012;60(2):225–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142. Streppel MT, Ocke MC, Boshuizen HC, Kok FJ, Kromhout D. Dietary fiber intake in relation to coronary heart disease and all-cause mortality over 40 y: the Zutphen Study. Am J Clin Nutr. 2008;88(4):1119–25. [DOI] [PubMed] [Google Scholar]
- 143. Eshak ES, Iso H, Date C, Kikuchi S, Watanabe Y, Wada Y, Wakai K, Tamakoshi A; JACC Study Group . Dietary fiber intake is associated with reduced risk of mortality from cardiovascular disease among Japanese men and women. J Nutr. 2010;140(8):1445–53. [DOI] [PubMed] [Google Scholar]
- 144. Park Y, Subar AF, Hollenbeck A, Schatzkin A. Dietary fiber intake and mortality in the NIH–AARP diet and health study. Arch Intern Med. 2011;171(12):1061–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Li S, Flint A, Pai JK, Forman JP, Hu FB, Willett WC, Rexrode KM, Mukamal KJ, Rimm EB. Dietary fiber intake and mortality among survivors of myocardial infarction: prospective cohort study. BMJ. 2014;348:g2659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146. Krishnamurthy VM, Wei G, Baird BC, Murtaugh M, Chonchol MB, Raphael KL, Greene T, Beddhu S. High dietary fiber intake is associated with decreased inflammation and all-cause mortality in patients with chronic kidney disease. Kidney Int. 2012;81(3):300–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. Slavin JL. Position of the American Dietetic Association: health implications of dietary fiber. J Am Diet Assoc. 2008;108(10):1716–31. [DOI] [PubMed] [Google Scholar]
- 148. Costabile A, Kolida S, Klinder A, Gietl E, Bauerlein M, Frohberg C, Landschütze V, Gibson GR. A double-blind, placebo-controlled, cross-over study to establish the bifidogenic effect of a very-long-chain inulin extracted from globe artichoke (Cynara scolymus) in healthy human subjects. Br J Nutr. 2010;104(7):1007–17. [DOI] [PubMed] [Google Scholar]
- 149. Koleva PT, Valcheva RS, Sun X, Ganzle MG, Dieleman LA. Inulin and fructo-oligosaccharides have divergent effects on colitis and commensal microbiota in HLA-B27 transgenic rats. Br J Nutr. 2012;108(9):1633–43. [DOI] [PubMed] [Google Scholar]
- 150. Davis LM, Martinez I, Walter J, Goin C, Hutkins RW. Barcoded pyrosequencing reveals that consumption of galactooligosaccharides results in a highly specific bifidogenic response in humans. PLoS One. 2011;6(9):e25200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Kalantar-Zadeh K, Fouque D. Nutritional management of chronic kidney disease. N Engl J Med. 2018;378(6):584–5. [DOI] [PubMed] [Google Scholar]
- 152. Kidney Disease Outcomes Quality Initiative (K/DOQI). K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis. 2004;43(5 Suppl 1):S1–290. [PubMed] [Google Scholar]
- 153. Bantle JP, Wylie-Rosett J, Albright AL, Apovian CM, Clark NG, Franz MJ, Hoogwerf BJ, Lichtenstein AH, Mayer-Davis EAmerican Diabetes Association; et al.; American Diabetes Association . Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31(Suppl 1):S61–78. [DOI] [PubMed] [Google Scholar]
- 154. Kidney Disease Outcomes Quality Initiative (K/DOQI). KDOQI clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. Am J Kidney Dis. 2007;49(2 Suppl 2):S12–154. [DOI] [PubMed] [Google Scholar]
- 155. Moorthi RN, Vorland CJ, Hill Gallant KM. Diet and diabetic kidney disease: plant versus animal protein. Curr Diab Rep. 2017;17(3):15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156. Tuttle KR, Bakris GL, Bilous RW, Chiang JL, de Boer IH, Goldstein-Fuchs J, Hirsch IB, Kalantar-Zadeh K, Narva AS, Navaneethan SD et al.. Diabetic kidney disease: a report from an ADA consensus conference. Am J Kidney Dis. 2014;64(4):510–33. [DOI] [PubMed] [Google Scholar]
- 157. Sheils JF, Rubin R, Stapleton DC. The estimated costs and savings of medical nutrition therapy: the Medicare population. J Am Diet Assoc. 1999;99(4):428–35. [DOI] [PubMed] [Google Scholar]
- 158. Pastors JG, Warshaw H, Daly A, Franz M, Kulkarni K. The evidence for the effectiveness of medical nutrition therapy in diabetes management. Diabetes Care. 2002;25(3):608–13. [DOI] [PubMed] [Google Scholar]
- 159. Franz MJ, Powers MA, Leontos C, Holzmeister LA, Kulkarni K, Monk A, Wedel N, Gradwell E. The evidence for medical nutrition therapy for type 1 and type 2 diabetes in adults. J Am Diet Assoc. 2010;110(12):1852–89. [DOI] [PubMed] [Google Scholar]
- 160. Franz MJ, Splett PL, Monk A, Barry B, McClain K, Weaver T, Upham P, Bergenstal R, Mazze RS. Cost-effectiveness of medical nutrition therapy provided by dietitians for persons with non-insulin-dependent diabetes mellitus. J Am Diet Assoc. 1995;95(9):1018–24. [DOI] [PubMed] [Google Scholar]
- 161. Anderson JM. Achievable cost saving and cost-effective thresholds for diabetes prevention lifestyle interventions in people aged 65 years and older: a single-payer perspective. J Acad Nutr Diet. 2012;112(11):1747–54. [DOI] [PubMed] [Google Scholar]
- 162. Riegel GR, Ribeiro PAB, Rodrigues MP, Zuchinali P, Moreira LB. Efficacy of nutritional recommendations given by registered dietitians compared to other healthcare providers in reducing arterial blood pressure: systematic review and meta-analysis. Clin Nutr. 2018;37(2):522–31. [DOI] [PubMed] [Google Scholar]
- 163. National Kidney Foundation. KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850–86. [DOI] [PubMed] [Google Scholar]
- 164. Levey AS, Greene T, Beck GJ, Caggiula AW, Kusek JW, Hunsicker LG, Klahr S. Dietary protein restriction and the progression of chronic renal disease: what have all of the results of the MDRD study shown? Modification of Diet in Renal Disease Study group. J Am Soc Nephrol. 1999;10(11):2426–39. [DOI] [PubMed] [Google Scholar]
- 165. Palmer SC, Maggo JK, Campbell KL, Craig JC, Johnson DW, Sutanto B, Ruospo M, Tong A, Strippoli GF. Dietary interventions for adults with chronic kidney disease. Cochrane Database Syst Rev. 2017;4:CD011998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166. Rhee CM, Ahmadi SF, Kovesdy CP, Kalantar-Zadeh K. Low-protein diet for conservative management of chronic kidney disease: a systematic review and meta-analysis of controlled trials. J Cachexia Sarcopenia Muscle. 2018;9(2):235–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167. de Waal D, Heaslip E, Callas P. Medical nutrition therapy for chronic kidney disease improves biomarkers and slows time to dialysis. J Ren Nutr. 2016;26(1):1–9. [DOI] [PubMed] [Google Scholar]
- 168. US Department of Health and Human Services. Telehealth Services [Internet]. Report No. ICN 901705.2018; [cited 14 Jan, 2018]. Available from https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/TelehealthSrvcsfctsht.pdf. [Google Scholar]
- 169. Beccari MV, Meaney CJ. Clinical utility of patiromer, sodium zirconium cyclosilicate, and sodium polystyrene sulfonate for the treatment of hyperkalemia: an evidence-based review. Core Evid. 2017;12:11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]