

Abstract
Suicide represents a major challenge to public mental health. In order to provide empirical evidence for prevention strategies, we hypothesized current levels of low socioeconomic status (SES) and high social isolation (SI) to be linked to increased suicide rates in N = 390 administrative districts since SES and SI are associated with mental illness. Effects of SES on suicide rates were further expected to be especially pronounced in districts with individuals showing high SI levels as SI reduces the reception of social support and moderates the impact of low SES on poor mental health. We linked German Microcensus data to register data on all 149,033 German suicides between 1997 and 2010 and estimated Prentice and Sheppard’s model for aggregate data to test the hypotheses, accounting for spatial effect correlations. The findings reveal increases in district suicide rates by 1.20% (p < 0.035) for 1% increases of district unemployment, suicide rate decreases of −0.39% (p < 0.028) for 1% increases in incomes, increases of 1.65% (p < 0.033) in suicides for 1% increases in one-person-households and increases in suicide rates of 0.54% (p < 0.036) for 1% decreases in single persons’ incomes as well as suicide rate increases of 3.52% (p < 0.000) for 1% increases in CASMIN scores of individuals who moved throughout the year preceding suicide. The results represent appropriate starting points for the development of suicide prevention strategies. For the definition of more precise measures, future work should focus on the causal mechanisms resulting in suicidality incorporating individual level data.
Keywords: suicide, public mental health, social determinants, prevention, socioeconomic status, social isolation
Introduction
Suicide constitutes a substantial public health problem: In Europe, the local age-adjusted numbers amounted to 12.84 deaths per 100,000 individuals in 2016, according to WHO data (1). This constitutes the second highest suicide rate across all WHO global regions. In order to improve the situation, suicide prevention has been given highest priority on the agenda of the European Comission (2). In addition to this, the reduction of suicide mortality has been defined as one of the target 3.4 indicators of the United Nations’ sustainable development goals for 2030 (3).
With regard to prevention, it is of particular significance that sociodemographic characteristics mediate suicide risks: A systematic review of population level studies revealed associations of poverty and suicide rates (4). According to recent studies (5, 6) increases in suicide rates are linked to rising unemployment rates. Moreover, there exists evidence for an inverse relationship between social cohesion and suicide (7–9). Adding to these findings, the aim of this study is to provide empirical evidence on potential associations of individual level indicators of socioeconomic status (SES) and social isolation (SI) with district suicide rates. While suicide itself is a complex phenomenon determined by genetic, cultural and behavioral factors (10, 11), such associations help to identify populations at risk.
Concerning suicide risks linked to SES, a meta-analysis by Li et al. (12) found the highest relative and population attributable risks of committing suicide for males in low ranked occupational classes and for persons with low educational achievement. Among women, relative risk ratios and population attributable risks were highest for unemployed individuals and individuals with low education. Regarding relations of education and suicide, suicides were also 2.12 times more often observed in the lowest educational group as compared to individuals with the highest educational levels across 35 countries in a study combining census and mortality register data (13). Unemployment turned out to be associated with suicide in a more recent meta-analysis (14). Relative risks of these associations were reduced after controlling for prior mental health. Financial strain, as captured by a family income to poverty threshold ratio has been found to be positively related to suicide attempts and ideations in a household survey among U.S. adults (15). As further crucial measures of SES, income-based indicators of individual level inequalities were positively related to suicide risks among both genders in a longitudinal study incorporating official Swedish mortality data (16).
In contrast to these results, several studies yielded less conclusive findings. While the most recent meta-analysis revealed positive associations of suicide with low education and unemployment, the authors regard these as not clinically significant due to small effect sizes (17). Overall, the study concluded that the results warrant further research on the effects of demographics on suicidal behavior. Among Malaysian in-patients, low social class predicted transitions from suicide ideations to attempt whereas unemployment and low educational levels did not confer any significant increases in suicide attempts (18). In addition, contradictory results were reported by Lukaschek et al. (19) who failed to find a significant effect of unemployment on suicides among in-patients in six German psychiatric hospitals. Regarding in-patient samples, it is important to note that these are not necessarily representative of all individuals that die by suicide. The findings by Chan et al. (18) and Lukaschek et al. (19) might possibly not apply to suicide in general.
Low SES does not increase suicide risks per se. On the one hand, there exist links of SES and psychopathology (20–23). On the other, quantitative meta-studies reveal associations of mental disorders and suicide (24, 25), avoiding the methodological problems of psychological autopsy (26). These findings suggest mental-ill health as a possible mechanism that links low SES levels to increases in suicide risks, allowing for causality in two directions. While poor mental health may be triggered by low SES, low SES may also represent the consequence of psychopathology. Several longitudinal studies investigating both explanatory approaches suggest an interaction of mental health and SES over the life course of individuals (27, 28).
Exploring potential mechanisms that explain SES effects on suicide does not lie within the scope of this study. In order to inform public health policies, we tested the hypothesis that lower levels of contemporary SES are correlated with higher suicide rates (Hypothesis I).
Our second hypothesis relates suicides to social isolation (SI). We define SI as a lack of social network quality. In this context, social network quality itself is understood as the extent to which existing ties provide the resources an organism can draw on in order to achieve its life goals (29). SI possibly acts as a root cause for feelings of thwarted belongingness. In combination with perceived burdensomeness, thwarted belongingness is seen as critical to the development of suicide ideation in Joiner’s (30) psychological model of suicide. This, in turn, leads to increased suicide risks in individuals. In accordance with the theory, the empirical evidence on links of SI with increased suicide risks is well established. Proxying for SI in a study incorporating 21,169 suicides, a Danish study revealed associations of single marital status and suicide (31). These results have been confirmed in Sweden (32), the U.S. (33), Great Britain (34), Finland (35), Austria, Belgium, Denmark, Norway and Switzerland (36) and Canada (37). Likewise, Agerbo et al. (38) found a relation between increased risks of suicide and living alone as well as being divorced. Utilizing relocations as SI proxies, several studies found these to be associated with completed and attempted suicides in adolescents (39, 40) and elderly people (41, 42).
There exists a solid body of evidence on associations between SI and mental health outcomes (43–45). Again, this suggests psychopathology as a potential pathway through which SI affects suicidality. It is important to note, however, that individuals suffering from mental illness exhibit impairments in social functioning, which leads to a disruption of personal networks (46). For this reason, not only does SI possibly affect mental health but mental health also impacts on SI levels. As is the case with SES and mental health, associations between SI and mental health outcomes do not determine the direction of causality. While this needs to be addressed with additional studies allowing for causal conclusions, we tested the second hypothesis that higher levels of SI are associated with higher suicide rates (Hypothesis II).
Social support represents a substantial social network resource for individuals in order to cope with stressful life events (47, 48) and has been shown to moderate the impact of environmental conditions on symptoms of poor mental health (49–52). Effects of low SES should thus be aggravated in socially isolated individuals. Hence, we also evaluated if interactions between lower levels of SES and higher levels of SI are linked with higher suicide rates (Hypothesis III).
Data and Methods
Data
For the observation period 1997 to 2010, data on suicides were obtained from the German death record edited by the federal statistical office (DESTATIS). The dataset lists all yearly German deaths by cause as coded by the ICD system (53, 54). With regard to these data, it is relevant that German data protection regulations do not permit individual level analyses. Hence, suicide deaths were examined as aggregated rates at the level of administrative districts. It needs to be considered in this respect that, after German reunification, extensive administrative reforms including new territorial definitions of district populations were implemented in Eastern Germany. Reformed areas were therefore grouped to greater regions such that they resembled the territorial status of the observation period’s last year, yielding a total of N = 390 districts. Non-reform-associated differences in district specific suicide rates are hereby properly identified.
In order to gain information on the socioeconomic conditions of district populations, the numerical identifiers of districts included in the record data were utilized to merge this dataset with the data provided by the German Microcensus. Based on a random household sample, the Microcensus is the official survey on living conditions in Germany. Selected respondents are legally bound to answer items on education, labor force participation, income, family and housing situation. As it can be inferred from Table 1, the survey’s population sample size is large enough to permit district level analyses: In all observation years but 2005, it corresponds to at least 0.74% of the population sizes in 95% of the districts. A drawback of the Microcensus is, however, that one quarter of the observation units is replaced every year. Periods longer than four years are thus not covered by panel data. In order to examine suicide deaths over a longer time frame, the employed dataset was constructed from annually repeated cross sections over the course of T = 14 years, i.e. N × T = 5,460 district observations.
Table 1.
Summary of microcensus sample sizes per district by year.
| Year | Mean | Min. | Max. | 5th Perc. of % Dis. Pop. |
|---|---|---|---|---|
| 1997 | 4,694 | 305 | 31,233 | 0.78 |
| 1998 | 4,640 | 315 | 30,381 | 0.77 |
| 1999 | 4,568 | 325 | 29,720 | 0.76 |
| 2000 | 4,480 | 322 | 29,034 | 0.74 |
| 2001 | 4,473 | 343 | 28,732 | 0.74 |
| 2002 | 4,420 | 347 | 28,604 | 0.75 |
| 2003 | 4,429 | 328 | 28,580 | 0.75 |
| 2004 | 4,403 | 321 | 28,491 | 0.74 |
| 2005 | 4,295 | 292 | 27,795 | 0.59 |
| 2006 | 4,337 | 332 | 28,130 | 0.74 |
| 2007 | 4,207 | 318 | 27,034 | 0.74 |
| 2008 | 4,243 | 323 | 27,298 | 0.75 |
| 2009 | 4,285 | 320 | 27,675 | 0.77 |
| 2010 | 4,256 | 297 | 27,369 | 0.76 |
Min., Minimum; Max., Maximum; 5th Perc. of % Dis. Pop.: 5th Percentile of Percentage of District Population.
Source: German Microcensus & Area Population Numbers of Germany, 1997 to 2010 - ed.by the German Federal Statistical Office (DESTATIS), own calculations were performed with STATA 15.0.
Measures and Descriptive Statistics
We define suicide as coded by the ICD 9 categories E950–E959 for 1997 and as the lethal consequence of intentional self-harm corresponding to the ICD 10 codes X60–X84 for the years from 1998 onwards, respectively (53, 54). All 149,033 cases of suicide death according to this definition were extracted from the death record to calculate district specific suicide rates. The different coding categories introduced with the 10th ICD revision in 1998 may be associated with structural breaks in reported suicide numbers and hence lead to biased estimates of suicide rates. To detect any of these breaks, yearly changes in suicide numbers per district were regressed on a dummy variable indicating the year of the ICD change controlling for district specific time trends and time fixed effects. As no significant results were found ICD 9 and ICD 10 codings of suicide are regarded as equivalent measures.
Because population structures vary over time and region, suicide rates were age- and gender-adjusted based on the 2013 European standard population to ensure the comparability across all districts. The gender specific distribution of district suicide rates over time can be inferred from Table 2. An illustration of the spatial distribution of the observation period means of the adjusted district suicide rates is provided by Figure 1.
Table 2.
Summary of age and gender standardized district suicide rates by year and gender.
| Year | Females | Males | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | S.D. | Min. | Max. | Mean | S.D. | Min. | Max. | |
| 1997 | 4.04 | 1.90 | 0.44 | 12.19 | 12.95 | 4.97 | 2.88 | 31.07 |
| 1998 | 3.65 | 1.75 | 0.54 | 11.95 | 12.49 | 4.42 | 3.07 | 31.52 |
| 1999 | 3.69 | 1.97 | 0.54 | 21.46 | 11.72 | 4.35 | 1.66 | 32.18 |
| 2000 | 3.61 | 1.80 | 0.29 | 11.63 | 11.69 | 4.20 | 2.50 | 28.06 |
| 2001 | 3.49 | 1.75 | 0.55 | 11.53 | 11.73 | 4.42 | 3.06 | 26.04 |
| 2002 | 3.47 | 1.70 | 0.56 | 10.87 | 11.50 | 4.48 | 2.87 | 37.37 |
| 2003 | 3.41 | 1.66 | 0.29 | 13.07 | 11.50 | 4.21 | 1.82 | 30.71 |
| 2004 | 3.25 | 1.91 | 0.00 | 17.61 | 10.71 | 3.77 | 0.00 | 28.58 |
| 2005 | 3.25 | 1.79 | 0.00 | 11.71 | 10.36 | 4.22 | 0.00 | 28.59 |
| 2006 | 2.99 | 1.71 | 0.30 | 11.25 | 10.04 | 3.83 | 2.44 | 33.44 |
| 2007 | 2.74 | 1.41 | 0.35 | 8.92 | 9.46 | 3.71 | 2.35 | 25.13 |
| 2008 | 2.97 | 1.70 | 0.36 | 11.96 | 9.54 | 3.93 | 1.43 | 34.26 |
| 2009 | 2.81 | 1.67 | 0.35 | 14.07 | 9.67 | 3.60 | 1.31 | 27.48 |
| 2010 | 3.00 | 1.70 | 0.42 | 13.13 | 9.95 | 3.56 | 2.74 | 29.47 |
Min., Minimum; Max., Maximum; S.D., Standard Deviation.
Source: German Death Record, 1997 to 2010 - ed. by the German Federal Statistical Office (DESTATIS), own calculations were performed with STATA 15.0.
Figure 1.
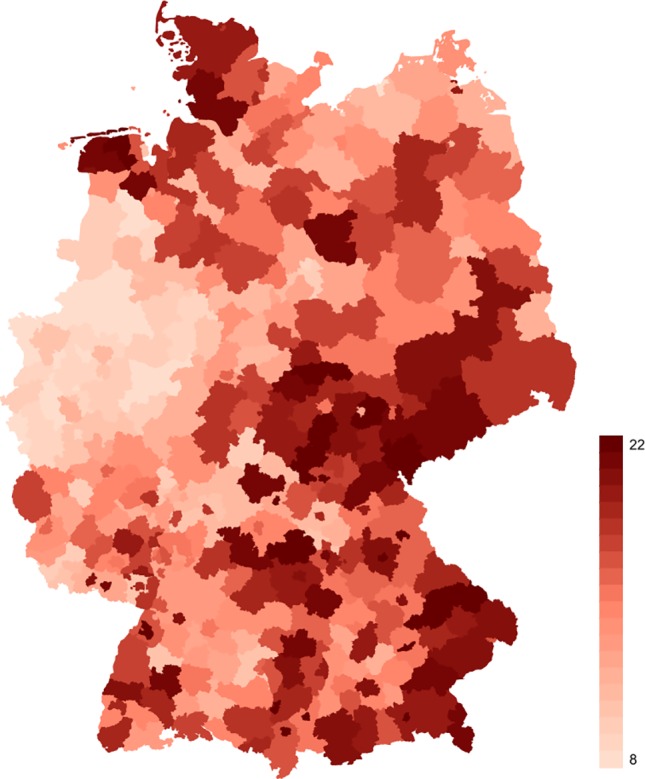
Observation period means of age- and gender-adjusted district suicide rates in Germany. The legend on the right hand side provides color codes for suicide rate values ranging from 8 (minimum) to 22 (maximum) per 100,000 inhabitants. Source: German Death Record, Area Population Numbers of Germany, 1997 to 2010, and 2013 European Standard Population - ed. by the German Federal Statistical Office (DESTATIS). Stata 15.0 was used to perform own calculations and create this figure.
Furthermore, as can be seen from Figure 2, the yearly means of the adjusted district suicide rates in Germany declined between the years from 1997 to 2010. Potential reasons for this consist in better help seeking behaviors and treatments of patients suffering from mental illness, better training of physicians to recognize suicidal behavior and the set up of intervention programs at community levels (55). In order to permit the identification of changes in suicide rates associated with SES and SI, this general linear downward trend in the data was accounted for by including a variable indicating the observation year in the models.
Figure 2.

Yearly means of age- and gender-adjusted district suicide rates in Germany. Suicides per 100,000 inhabitants shown on the y-axis, observation years shown on the x-axis. Source: German Death Record, 1997 to 2010 - ed. by the German Federal Statistical Office (DESTATIS), STATA 15.0 was used to create this figure.
SES was operationalized employing measures for educational achievements, occupational status and log income. Educational achievements were quantified according to the scheme provided by the “Comparative Analyses of Social Mobility in Industrial Nations (CASMIN)” (56). The CASMIN scheme constitutes an internationally comparable measure that distinguishes hierarchical educational classes constructed from combinations of school and vocational degrees. The classes reach from 1a (inadequately completed general education) to 3b (higher tertiary education) and represent the boundaries of the respective country’s educational system on the one hand and differentiate between required educational levels for certain labor market positions on the other (57).
The “International Socio-Economic-Index of Occupational Status (ISEI)” (58) was applied for the measurement of occupational status. This index relies on a continuous scoring system with values ranging from 16 (low Status) to 85 (high status). For unemployed individuals, scores of the last occupation were utilized. Beyond that, unemployment and, as it is not included in the ISEI scheme, minor employment were recorded in own variables and included in the analysis.
As another significant component of SES, we calculated the log of the equivalent household income from the income variables provided by the Microcensus. The highest psychosocial distress should result from the lowest SES conditions. In order to proxy especially for these situations, two variables indicating the receipt of social benefits due to unemployment (“ALG I/II” in Germany) and the number of received public transfers were added to the models, too.
Similar to previous studies, SI was proxied with two variables on single marital status and living in a one-person-household and a dummy variable recording a possible relocation throughout the year before the survey was conducted (“Moved last Year”). Being divorced or widowed was considered as having a single status in this context.
Age categories as provided with the European standard population were employed for the standardization of suicide rates. In order to control for exponentially increasing suicide risks with age in Germany (59) and continuous age effects, we therefore added continuous measures of age and age squared from the register dataset as controls. Table 3 summarizes all independent variables over time.
Table 3.
Independent variables.
| Variable | Mean | S.D. | N |
|---|---|---|---|
| ISEI | 42.60 | 15.73 | 4,598,937 |
| CASMIN | 3.40 | 2.16 | 7,873,911 |
| No. Public Transfers | 0.24 | 0.51 | 9,923,291 |
| Age | 53.93 | 4.07 | 7,324,663 |
| Median | I.Q.R. | N | |
| Income (household equiv.) | 1230.77 | 1043.71 | 9,239,242 |
| % | S.D. (in %) | N | |
| Minor employment | 4.00 | 19.50 | 7,646,280 |
| Unemployment | 4.96 | 21.71 | 9,941,490 |
| ALG I/II | 4.64 | 21.03 | 9,941,494 |
| Moved last year | 6.92 | 25.39 | 6,438,498 |
| Single | 51.88 | 49.96 | 9,941,494 |
| One-person-household | 17.54 | 38.03 | 9,836,123 |
| Gender (male) | 73.44 | 8.78 | 7,324,663 |
S.D., Standard Deviation; I.Q.R., Interquartile Range
Source: German Microcensus & Death Record, 12997 to 2010 – ed. by the German Federal Statistical Office (DESTATIS), own calculations were performed with STATA 15.0.
Finally, values of the ISEI, CASMIN and log income variables were inverted and mean-centered for the calculation of the proposed SES × SI interactions.
Methods
Combining individual and district level data for the estimation of SES and SI effects on suicide rates represents a source of ecological bias. The problem arises in aggregate data analysis if summary measures are employed to calculate effects on marginal outcomes. Distributions of summaries do not determine individual distributions. Because joint individual distributions have to be specified in order to identify effect parameters, however, estimates depending solely on aggregate data are potentially biased. A first related statistical problem is that, without further assumptions, applying summary measures does not identify the functional form of effects on the individual level. To see this, let:
| (1) |
where f (·) denotes a link function. yidt is a binary indicator variable, with yidt = 1 if individual i = 1,2,…,ndt commits suicide in district d = 1,2,…,N at year t = 1,2,…,T and yidt = 0 otherwise. Xidt is a row vector including the controls, the variables on SES and SI and, in order to test Hypothesis III, SES x SI interaction terms. β is a column vector with the respective parameters of interest. Further, πd represents the district baseline probability of suicides, for Xidt = 0. Given that data on suicides is only available as district specific rates, , effects of SES and SI can be estimated by the ecological model
| (2) |
with . As it can be seen from equations (1) and (2) the functional form of individual level effects is only correctly specified if f (·) is assumed to be linear and completely additive in all of its arguments. It follows in any other case that . With regard to this, we therefore apply the aggregate data method firstly introduced by Prentice and Sheppard (60). Accordingly, the following equation is being estimated, normalizing the district specific standardized suicide rate rdt by taking its log:
| (3) |
with an identity link f (·) and a variance fraction ρ. The spatial contiguity matrix W accounts for a spatial correlation of error components τdt among neighboring districts due to omitted district level variables. Spatial correlation effects may result in biased estimates of suicide rates, e.g. if individuals commute between districts that differ in one or more of such unobserved traits. Further, , denotes an idiosyncratic error that is strictly exogenous. As long as this assumption holds, it is also assumed that εdt has a constant variance across time, i.e. no heteroskedasticity, and that the errors are not serially correlated, , for all t≠t-s. A last assumption that is being made is that there is no multicollinearity in the data.
The model specification as defined in (3) also considers two further potential estimation biases: First, another difficulty in assessing suicide rates with combined aggregate and individual data is that marginal distributions may designate district properties only. In this case, observed effects do not reflect any individual characteristics but rather shifts in suicide rates that depend solely on district assignment. This possibility is avoided though if we assume the district specific suicide rates to be independent of each other because this rules out any unobserved time-constant district heterogeneity. Hence, the baseline probability πd is defined as a district fixed effect in (3). A second problem has its roots in the time dimension of the data. Suicide rates may change because of events that commonly affect all individuals across all districts at a certain time t. These events, i.e. exogenous shocks, represent a source of unobserved district-constant heterogeneity, which causes an additional estimation bias. This bias is accounted for by including a time fixed effect νt in (3). This prevents any event at t distorting the estimates of suicide risks in the same period.
Generally, the linear specification of f (·) greatly simplifies the procedure and allows us to employ the quasi-maximum-likelihood fixed effects estimator for longitudinal spatial error models (SEM) developed by Lee and Yu (61) in order to fit (3).
The models’ residuals were tested for autocorrelation and no autocorrelation was detected by Wooldridge’s autocorrelation test (62), F(1,389) = 1.923 (p > F = 0.166). Moreover, Wald tests were conducted for stepwise model selection based on a basic fixed effect (FE) estimation of (3).
Rather than defining fixed effects, an alternate specification rests on the assumption of πd as a random effect with E(πd ǀ Xidt,vt) = 0. Consequently, a random effects estimator (RE) is then applied to (3). In order to compare both estimation strategies a Hausman test (63) was conducted. The results indicate that the fixed effects model is to be preferred over the random effects model, χ2 = 365.28 (p > χ2 = 0.000). For a further specification test, it was also taken into account that current suicide rates may be influenced by accumulated effects of past levels of SES and SI. We estimated a corrected least squares dummy variable model (LSDVC) (64, 65) including Koyck lags (66) of all independent variables in order to assess long run SES and SI effects on suicide rates. The model yields a mean time of only 1.2 months after which suicide rates are affected by changes in SES and SI levels. Given this high adjustment rate of the model, past SES and SI levels barely contribute to current suicide rates. See the Supplementary Material for the results of the additional analyses.
Limitations
The specification of our model takes account of the functional form of SES and SI effects on the individual level and rules out the estimation of any effects that depend entirely on district assignment. It does not address a further problem associated with ecological data analysis, however. Because of the information on joint distributions lost due to the aggregation of suicides in district rates, effects of district SES and SI compositions cannot be differentiated from individual level SES and SI effects. The estimated coefficients rather represent a blend of individual level and district composition effects (67). Thus, individual level effects are only identified under the untestable assumption that there exist no compositional effects. This assumption is not being made in this study. Since they potentially include individual level effects, significant results are rather regarded as indications for further research. As an additional problem, this also implies that the equations do not identify true treatment effects. Hence, our FE specifications do not reveal causal effects even though they rule out unobserved heterogeneity.
Furthermore, SI should be measured by indicators of social network quality. Such indicators are not available in the data. One-person-households and single marital status were therefore used as proxies for SI based on the assumption that both variables are associated with a comparatively lower social integration. It should be acknowledged, however, that one-person-households and single status are related to each other and, for this reason, might be correlated as well.
Results
Table 4 shows the results from the SEM estimation. As can be seen, district suicide rates decrease by −0.39% (p < 0.028) with every percentage point increase in incomes, assuming mean sizes of district proportions of singles, individuals living in one-person-households and persons who moved during the year before suicide. Further, an increase in district unemployment proportions by 1% leads to an 1.20% increase (p < 0.035) in district suicide rates. Contradicting these results however, it is observed that, given mean district shares of singles, relocated persons and one-person-households again, a 1% increase in CASMIN scores results in an increase of suicide rates by 0.98% (p < 0.021).
Table 4.
SEM longitudinal regressions of district suicide rates on SES and SI.
| Spatial Error Model ln District Suicide Rate |
||
|---|---|---|
| %−Change (95% − CI) | p - value | |
| SES | ||
| ISEI | 0.1 (−0.93, 1.14) | (1.000) |
| CASMIN | 0.98 (0.09, 1.88) | (0.021) |
| Income | −0.39 (−0.76, −0.03) | (0.028) |
| Minor employment | −0.46 (−1.45, 0.54) | (1.000) |
| Unemployed | 1.20 (0.04, 2.38) | (0.035) |
| No. Public Transfers | 11.98 (−19.66, 56.09) | (1.000) |
| ALG I/II | 0.06 (−0.80, 0.92) | (1.000) |
| SI | ||
| Moved last Year | −2.13 (−3.52, −0.72) | (0.000) |
| Single | 0.46 (−0.42, 1.35) | (0.639) |
| One-Person-Household | 1.65 (0.09, 3.23) | (0.033) |
| SES × SI Interactions | ||
| ISEI (inv.) × Single | 0.27 (−0.73, 1.28) | (1.000) |
| CASMIN (inv.) × Single | −0.96 (−2.16, 0.26) | (0.297) |
| Income (inv.) × Single | 0.54 (0.01, 1.07) | (0.036) |
| ISEI (inv.) × One-Person-Household | −1.15(2.34, −0.05) | (0.072) |
| CASMIN (inv.) × One-Person-Household | −0.72 (−2.43, 1.03) | (1.000) |
| Income (inv.) × One-Person-Household | −0.98 (−1.79, −0.17) | (0.009) |
| ISEI (inv.) × Moved last Year | −0.29 (−2.37, 1.84) | (1.000) |
| CASMIN (inv.) × Moved last Year | 3.52 (1.20, 5.91) | (0.000) |
| Income (inv.) × Moved last Year | 0.15 (−0.63, 0.93) | (1.000) |
| Observations | 5070 | |
The table reports percentage changes of rdt with Bonferroni corrected 95% confidence intervals in square brackets and Bonferroni corrected p-values in parentheses. Control variables are not shown. Results significant at α = 0.05 are printed in bold. “inv.” is abbreviated from inverted.
Source: German Microcensus & Death Record, 1997 to 2010, & 2013 European Standard Population - ed. by the German Federal Statistical Office (DESTATIS), own calculations were performed with STATA 15.0.
Mean values of ISEI, CASMIN and income presumed, a percentage point increase in district population shares of people living in a one-person-household is shown to be associated with an increase in district suicide rates by 1.65% (p < 0.033). An increase in persons moving throughout the last year by 1% is found to decrease suicide rates by −2.13% (p < 0.000), though.
Regarding interactions of SES and SI, a 1% decrease in the incomes of the respective district’s single persons increases district suicide rates by 0.54% (p < 0.036). In addition to this, a decrease in CASMIN scores among individuals with a recent relocation of 1% is associated with an increase in suicide rates by 3.52% (p < 0.000). By contrast, a 1% decrease in the incomes of district individuals living in one-person-households results in a −0.98% decrease in suicide rates (p < 0.009).
Discussion
In light of these results, an inverse relation between SES and suicide rates as claimed by Hypothesis I is partly confirmed by the observed unemployment and income effects. This finding is contradicted by the observation that suicide rates increase with increases in CASMIN scores, however. Due to the employed aggregate data, a reasonable explanation for this finding may exist in district compositions: Average CASMIN levels have been steadily increasing over the entire observation period in Germany (68). Given that the specification of our model does not allow to differentiate between effects of individual characteristics and district composition, it can not be excluded by the observed positive effect that the corresponding individuals boast disproportionally low suicide risks. The same reasoning applies to the results in line with Hypothesis I: Given the data, our model specification does not rule out disproportionally low suicide numbers among unemployed individuals and persons with lower household incomes as compared to employees and individuals with higher incomes.
With regard to SI effects on suicide, the coefficient estimates of the district proportion of persons living in one-person-households partly validate an inverse relation between SI and suicide rates as stated by Hypothesis II. This result also confirms Agerbo et al.’s (38) findings. As these observations represent compound individual and district composition effects, it needs to be noted that our results do not eliminate the possibility that the concerning individuals show lower suicide risks if compared to persons who live in more-than-one-person-households. Vice versa, this is also valid for the negative effects on suicides found for district share increases of individuals moving throughout the year preceding suicide, contradicting Hypothesis II: At the district level, high resident turnover rates prevailing in areas with relatively low suicide rates, e.g. rural regions (69, 70), provide a potential explanation for this observation. This does not preclude higher suicide risks among moving as opposed to non-moving individuals, though.
Moreover, the positive effects of income decreases in population shares of single persons on district suicide rates corroborate the SES × SI interactions proposed by Hypothesis III. Another confirmation is suggested by the estimate that shows an increase in suicide rates to be associated with CASMIN score decreases in persons who moved during the past year. On the contrary, the observed negative effects on suicides of decreases in household incomes of the districts’ persons living in one-person-households clearly contradict the claimed interactions. Once more compositional effects may be a possible reason for the inconsistent observations. Thus, it cannot be ruled out that individuals living in one-person-households who committed suicide show comparatively low income levels. This may hold even true if the means of the respective marginal distributions increase with ascending suicide rates across N × T = 5,460 district observations. The same argument applies to the findings confirming Hypothesis III: Incomes in single persons and CASMIN scores in relocated individuals might increase in districts with ascending suicide rates considering the aggregate data employed in this study.
In view of the inconsistent results regarding Hypotheses I to III, it is generally recommended that future studies should incorporate individual level data in order to separate individual level from district composition effects and further investigate the robustness of our observations. Nonetheless, the results demonstrating positive SES and SI effects on suicide rates serve as appropriate starting points for the development of suicide prevention strategies: First, our findings suggest interventions to especially target the unemployed, individuals living in one-person-households, persons with low incomes and relocated individuals with lower educational levels. In a second step, specific strategies should be designed in order to cover the needs of the individuals under concern. In order to do so, future work should focus on the causal mechanisms resulting in suicidality. This is best accomplished by applying longitudinal data and modeling life course interactions of adversities and mental health. Depending on the results, respective programs may then include alliances between psychiatric centers and welfare offices lowering the threshold for unemployed and poorly earning individuals to seek counseling and treatment. For socially isolated individuals, effective interventions may encompass approaches aiming at the conditions that favor social isolation within local communities. Respective strategies could also involve the strengthening of communal support systems as well as the improvement of transport services and communication technologies. In addition to this, direct interventions may be established that help individuals in maintaining or developing interpersonal connections (71).
Author Contributions
A-FN conceptualized the study. A-FN, CR-K, and UH designed the study. A-FN undertook the statistical analyses. A-FN, CR-K, and UH interpreted the data. A-FN drafted the manuscript. CR-K and UH critically revised the draft for important intellectual content. All the authors approved the final version of the manuscript.
Funding
The authors acknowledge support from the German Research Foundation (DFG) and Leipzig University within the program of Open Access Publishing. Funding for the provision of the Data by the German Federal Statistical Office (DESTATIS) was provided by UH.
Conflict of Interest
PD Dr. CR-K reports personal fees from Servier, outside the submitted work. Professor Dr. UH reports personal fees from Lundbeck, personal fees from Servier, personal fees from Bayer Pharma, grants from Medice Arzneimittel, and personal fees from Roche, outside the submitted work.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank Professor Dr. Georg Schomerus, University of Leipzig, Germany, Professor Dr. Bernhard Boockmann, IAW Tübingen, Germany, and Dr. Stephan Poppe, University of Leipzig, Germany, as well as the staff from the German Federal Statistical Agency (DESTATIS) for their outstanding support.
Abbreviations
CASMIN, Comparative Analyzes of Social Mobility in Industrial Nations; FE, Fixed Effects (Model); ICD, International Classification of Diseases; ISEI, International Socio-Economic-Index of Occupational Status; LSDVC, Corrected Least Squares Dummy Variable (Model); RE, Random Effects (Model); SEM, Spatial Error Model; SES, Socioeconomic Status; SI, Social Isolation; WHO, World Health Organization.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00898/full#supplementary-material
References
- 1. WHO Global Health Observatory data repository. (2018). Suicide rate estimates, age-standardized Estimates by WHO region.
- 2. EU EU-Compass for Action on Mental Health and Wellbeing. Annual Report 2017. Summary and Analysis of Key Developments in Members States and Stakeholders. European Commision: Brussels: (2017). [Google Scholar]
- 3. UN SDG Indicators Metadata repository. (2018).
- 4. Rehkopf D, Buka S. The association between suicide and the socio-economic characteristics of geographical areas: a systematic review. Psychol Med (2006) 36:145–7. 10.1017/s003329170500588x [DOI] [PubMed] [Google Scholar]
- 5. Stuckler D, Basu S, Suhrcke M, Coutts A, McKee M. The public health effect of economic crises and alternative policy responses in Europe: an empirical analysis. Lancet (2009) 374:315–3. 10.1016/s0140-6736(09)61124-7 [DOI] [PubMed] [Google Scholar]
- 6. Milner A, McClure R, De Leo D. Socio-economic determinants of suicide: an ecological analysis of 35 countries. Social Psychiatry Psychiatric Epidemiol (2012) 47:19–7. 10.1007/s00127-010-0316-x [DOI] [PubMed] [Google Scholar]
- 7. Baller RD, Richardson KK. Social integration, imitation, and the geographic patterning of suicide. Am Sociological Rev (2002) 67(6):873–8. 10.2307/3088974 [DOI] [Google Scholar]
- 8. Barkan SE, Rocque M, Houle J. State and regional suicide rates: a new look at an old puzzle. Sociological Perspect (2013) 56:287–7. 10.1525/sop.2013.56.2.287 [DOI] [Google Scholar]
- 9. Smith NDL, Kawachi I. State-level social capital and suicide mortality in the 50 US states. Social Sci Med (2014) 120:269–7. 10.1016/j.socscimed.2014.09.007 [DOI] [PubMed] [Google Scholar]
- 10. Turecki G, Ernst C, Jollant F, Labonté B, Mechawar N. The neurodevelopmental origins of suicidal behavior. Trends Neurosci (2012) 35:14–3. 10.1016/j.tins.2011.11.008 [DOI] [PubMed] [Google Scholar]
- 11. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet (2016) 387:1227–9. 10.1016/s0140-6736(15)00234-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Li Z, Page A, Martin G, Taylor R. Attributable risk of psychiatric and socio-economic factors for suicide from individual-level, population-based studies: a systematic review. Social Sci Med (2011) 72:608–6. 10.1016/j.socscimed.2010.11.008 [DOI] [PubMed] [Google Scholar]
- 13. Lorant V, de Gelder R, Kapadia D, Borrell C, Kalediene R, Kovács K, et al. Socioeconomic inequalities in suicide in Europe: the widening gap. British J Psychiatry (2018) 212(6):356–61. 10.1192/bjp.2017.32 [DOI] [PubMed] [Google Scholar]
- 14. Milner A, Page A, Lamontagne AD. Cause and effect in studies on unemployment, mental health and suicide: a meta-analytic and conceptual review. Psychol Med (2014) 44:909–7. 10.1017/s0033291713001621 [DOI] [PubMed] [Google Scholar]
- 15. Pan YJ, Stewart R, Chang CK. Socioeconomic disadvantage, mental disorders and risk of 12-month suicide ideation and attempt in the national comorbidity survey replication (NCS-R) in US. Social Psychiatry Psychiatric Epidemiol (2013) 48:71–9. 10.1007/s00127-012-0591-9 [DOI] [PubMed] [Google Scholar]
- 16. Hiyoshi A, Kondo N, Rostila M. Increasing income-based inequality in suicide mortality among working-age women and men, Sweden, 1990–2007: is there a point of trend change? J Epidemiol Community Health (2018) 72:1009–5. 10.1136/jech-2018-210696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Huang X, Ribeiro JD, Musacchio KM, Franklin JC. Demographics as predictors of suicidal thoughts and behaviors: a meta-analysis. PloS ONE (2017) 12:e0180793. 10.1371/journal.pone.0180793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Chan LF, Shamsul AS, Maniam T. Are predictors of future suicide attempts and the transition from suicidal ideation to suicide attempts shared or distinct: a 12-month prospective study among patients with depressive disorders. Psychiatry Res (2014) 220:867–3. 10.1016/j.psychres.2014.08.055 [DOI] [PubMed] [Google Scholar]
- 19. Lukaschek K, Baumert J, Krawitz M, Erazo N, Förstl H, Ladwig KH. Determinants of completed railway suicides by psychiatric in-patients: case–control study. British J Psychiatry (2014) 205:398–6. 10.1192/bjp.bp.113.139352 [DOI] [PubMed] [Google Scholar]
- 20. Fryers T, Melzer D, Jenkins R. Social inequalities and the common mental disorders. Social Psychiatry Psychiatric Epidemiol (2003) 38:229–7. 10.1007/s00127-003-0627-2 [DOI] [PubMed] [Google Scholar]
- 21. Jenkins R, Bhugra D, Bebbington P, Brugha T, Farrell M, Coid J, et al. Debt, income and mental disorder in the general population. Psychol Med (2008) 38:1485–3. 10.1017/s0033291707002516 [DOI] [PubMed] [Google Scholar]
- 22. Bjelland I, Krokstad S, Mykletun A, Dahl AA, Tell GS, Tambs K. Does a higher educational level protect against anxiety and depression? The HUNT study. Social Sci Med (2008) 66:1334–5. 10.1016/j.socscimed.2007.12.019 [DOI] [PubMed] [Google Scholar]
- 23. Lund C, Breen A, Flisher AJ, Kakuma R, Corrigall J, Joska JA, et al. Poverty and common mental disorders in low and middle income countries: a systematic review. Social Sci Med (2010) 71:517–8. 10.1016/j.socscimed.2010.04.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry (2014) 13:153–0. 10.1002/wps.20128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Ferrari AJ, Norman RE, Freedman G, Baxter AJ, Pirkis JE, Harris MG, et al. The burden attributable to mental and substance use disorders as risk factors for suicide: findings from the global burden of disease study 2010. PloS One (2014) 9:e91936. 10.1371/journal.pone.0091936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hjelmeland H, Dieserud G, Dyregrov K, Knizek BL, Leenaars AA. Psychological autopsy studies as diagnostic tools: are they methodologically flawed? Death Studies (2012) 36:605–6. 10.1080/07481187.2011.584015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Kristensen P, Gravseth HM, Bjerkedal T. Influence of early life factors on social inequalities in psychiatric outcomes among young adult Norwegian men. Eur J Public Health (2010) 20:517–3. 10.1093/eurpub/ckq083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Quesnel-Vallée A, Taylor M. Socioeconomic pathways to depressive symptoms in adulthood: evidence from the National Longitudinal Survey of Youth 1979. Social Sci Med (2012) 74:734–3. 10.1016/j.socscimed.2011.10.038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Lin N. Social Capital: A Theory of Social Structure and Action. Cambridge University Press: New York: (2001). 10.1017/cbo9780511815447 [DOI] [Google Scholar]
- 30. Joiner TE. Why people die by suicide. Harvard University Press: Cambridge, MA, US: (2005). [Google Scholar]
- 31. Qin P, Agerbo E, Mortensen P. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a national register–based study of all suicides in Denmark, 1981–1997. Am J Psychiatry (2003) 160:765–2. 10.1176/appi.ajp.160.4.765 [DOI] [PubMed] [Google Scholar]
- 32. Johansson LM, Sundquist J, Johansson SE, Qvist J, Bergman B. The influence of ethnicity and social and demographic factors on Swedish suicide rates. Social Psychiatry Psychiatric Epidemiol (1997) 32:165–0. 10.1007/BF00794616 [DOI] [PubMed] [Google Scholar]
- 33. Kposowa AJ. Marital status and suicide in the National Longitudinal Mortality Study. J Epidemiol Community Health (2000) 54:254–1. 10.1136/jech.54.4.254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Yip PS, Thorburn J. Marital status and the risk of suicide: experience from England and Wales 1982–1996. Psychol Rep (2004) 94:401–7. 10.2466/pr0.94.2.401-407 [DOI] [PubMed] [Google Scholar]
- 35. Martikainen P, Mäki N, Blomgren J. The effects of area and individual social characteristics on suicide risk: a multilevel study of relative contribution and effect modification. Eur J Popul (2004) 20:323–0. 10.1007/s10680-004-3807-1 [DOI] [Google Scholar]
- 36. Lorant V, Kunst AE, Huisman M, Bopp M, Mackenbach J. A European comparative study of marital status and socio-economic inequalities in suicide. Social Sci Med (2005) 60:2431–1. 10.1016/j.socscimed.2004.11.033 [DOI] [PubMed] [Google Scholar]
- 37. Burrows S, Auger N, Gamache P, St-Laurent D, Hamel D. Influence of social and material individual and area deprivation on suicide mortality among 2.7 million Canadians: a prospective study. BMC Public Health (2011) 11:1–11. 10.1186/1471-2458-11-577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Agerbo E, Sterne J, Gunell D. Combining individual and ecological data to determine compositional and contextual socioeconomic risk factors for suicide. Social Sci Med (2007) 64:451–1. 10.1016/j.socscimed.2006.08.043 [DOI] [PubMed] [Google Scholar]
- 39. Qin P, Mortensen PB, Pedersen CB. Frequent change of residence and risk of attempted and completed suicide among children and adolescents. Archives Gen Psychiatry (2009) 66:628–2. 10.1001/archgenpsychiatry.2009.20 [DOI] [PubMed] [Google Scholar]
- 40. Bramson LM, Rickert ME, Class QA, Sariaslan A, Almqvist C, Larsson H, et al. The association between childhood relocations and subsequent risk of suicide attempt, psychiatric problems, and low academic achievement. Psychol Med (2016) 46:969–9. 10.1017/s0033291715002469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Alexopoulos GS. Depression in the elderly. Lancet (2005) 365:1961–0. 10.1016/s0140-6736(05)66665-2 [DOI] [PubMed] [Google Scholar]
- 42. Conwell Y, Duberstein PR, Hirsch JK, Conner KR, Eberly S, Caine ED. Health status and suicide in the second half of life. Int J Geriatric Psychiatry: A J Psychiatry late life allied Sci (2010) 25:371–9. 10.1002/gps.2348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Barnett PA, Gotlib IH. Psychosocial functioning and depression: distinguishing among antecedents, concomitants, and consequences. Psychol Bulletin (1988) 104:97. 10.1037/0033-2909.104.1.97 [DOI] [PubMed] [Google Scholar]
- 44. Kawachi I, Berkman LF. Social ties and mental health. J Urban Health (2001) 78:458–7. 10.1093/jurban/78.3.458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Santini ZI, Koyanagi A, Tyrovolas S, Haro JM. The association of relationship quality and social networks with depression, anxiety, and suicidal ideation among older married adults: findings from a cross-sectional analysis of the Irish Longitudinal Study on Ageing (TILDA). J Affective Disorders (2015) 179:134–1. 10.1016/j.jad.2015.03.015 [DOI] [PubMed] [Google Scholar]
- 46. Hirschfeld R, Montgomery SA, Keller MB, Kasper S, Schatzberg AF, Möller HJ, et al. Social functioning in depression: a review. J Clin Psychiatry (2000) 61:268–5. 10.4088/jcp.v61n0405 [DOI] [PubMed] [Google Scholar]
- 47. Taylor SE, Stanton AL. Coping resources, coping processes, and mental health. Ann Rev Clin Psychol (2007) 3:377–1. 10.1146/annurev.clinpsy.3.022806.091520 [DOI] [PubMed] [Google Scholar]
- 48. Thoits PA. Stress and health major findings and policy implications. J Health Social Behav (2010) 51:S41–3. 10.1177/0022146510383499 [DOI] [PubMed] [Google Scholar]
- 49. Holahan C, Moos R, Holahan C, Brennan P. Social context, coping strategies, and depressive symptoms: an expanded model with cardiac patients. J Personality Social Psychol (1997) 72:918–8. 10.1037/0022-3514.72.4.918 [DOI] [PubMed] [Google Scholar]
- 50. Schroevers MJ, Ranchor AV, Sanderman R. The role of social support and self-esteem in the presence and course of depressive symptoms: a comparison of cancer patients and individuals from the general population. Social Sci Med (2003) 57:375–5. 10.1016/s0277-9536(02)00366-0 [DOI] [PubMed] [Google Scholar]
- 51. Khatib Y, Bhui K, Stansfeld SA. Does social support protect against depression & psychological distress? Findings from the RELACHS study of East London adolescents. J Adolesc (2013) 36:393–2. 10.1016/j.adolescence.2013.01.001 [DOI] [PubMed] [Google Scholar]
- 52. Suvak M, Taft C, Goodman L, Dutton M. Dimensions of functional social support and depressive symptoms: a longitudinal investigation of women seeking help for intimate partner violence. J Consulting Clin Psychol (2013) 81:455–6. 10.1037/a0031787 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. WHO (1976). The ninth revision of the International Classification of Diseases (ICD-9) (Geneva: World Health Organization; ). [Google Scholar]
- 54. WHO The tenth revision of the International Classification of Diseases (ICD-10) (Geneva: World Health Organization; ) (1992). [Google Scholar]
- 55. Hegerl U, Mergl R, Doganay G, Reschke K, Rummel-Kluge C. Why has the continuous decline in German suicide rates stopped in 2007? PLoS ONE (2013) 8:1–9. 10.1371/journal.pone.0071589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. König W, Lüttinger P, Müller W. A comparative analysis of the development and structure of educational systems. Methodological foundations and the construction of a comparative educational scale. In: University of Mannheim: CASMIN-Project. Working Paper No. 12 (1988).
- 57. Brauns H, Steinmann S. Educational reform in France, West-Germany and the United Kingdom: updating the CASMIN educational classification. ZUMA Nachrichten (1999) 23:7–44. [Google Scholar]
- 58. Ganzeboom HB, Treiman DJ. Internationally comparable measures of occupational status for the 1988 International Standard Classification of Occupations. Social Sci Res (1996) 25:201–9. 10.1006/ssre.1996.0010 [DOI] [Google Scholar]
- 59. Schmidtke A, Sell R, Löhr C. Epidemiologie von Suizidalität im Alter. Zeitschrift für Gerontologie und Geriatrie (2008) 41:3–13. 10.1007/s00391-008-0517-z [DOI] [PubMed] [Google Scholar]
- 60. Prentice R, Sheppard L. Aggregate data studies of disease risk factors. Biometrika (1995) 82:113–5. 10.1093/biomet/82.1.113 [DOI] [Google Scholar]
- 61. Lee LF, Yu J. Estimation of spatial autoregressive panel data models with fixed effects. J Econometrics (2010) 154:165–5. 10.1016/j.jeconom.2009.08.001 [DOI] [Google Scholar]
- 62. Wooldridge JM. Econometric analysis of cross section and panel data. The MIT Press: Cambridge, Massachusetts: (2010). [Google Scholar]
- 63. Nakamura A, Nakamura M. On the relationships among several specification error tests presented by Durbin, Wu, and Hausman. . J Econometric Soc (1981), 49:1583–8. 10.2307/1911420 [DOI] [Google Scholar]
- 64. Kiviet JF. On bias, inconsistency, and efficiency of various estimators in dynamic panel data models. J Econometrics (1995) 68:53–8. 10.1016/0304-4076(94)01643-e [DOI] [Google Scholar]
- 65. Bun MJ, Kiviet JF. On the diminishing returns of higher-order terms in asymptotic expansions of bias. Econ Letters (2003) 79:145–2. 10.1016/s0165-1765(02)00299-9 [DOI] [Google Scholar]
- 66. Koyck LM. Distributed lags and investment analysis. North-Holland Publishing Company: Amsterdam: (1954). [Google Scholar]
- 67. Greenland S. A review of multilevel theory for ecologic analysis. Stat Med (2002) 21:389–5. 10.1002/sim.1024 [DOI] [PubMed] [Google Scholar]
- 68. Moor I, Günther S, Knöchelmann A, Hoebel J, Pförtner TK, Lampert T, et al. Educational inequalities in subjective health in Germany from 1994 to 2014: a trend analysis using the German Socio-Economic Panel study (GSOEP). BMJ Open (2018) 8:e019755. 10.1136/bmjopen-2017-019755 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Hempstead K. The geography of self-injury: Spatial patterns in attempted and completed suicide. Social Sci Med (2006) 62:3186–6. [DOI] [PubMed] [Google Scholar]
- 70. Santana P, Costa C, Cardoso G, Loureiro A, Ferrão J. Suicide in Portugal: Spatial determinants in a context of economic crisis. Health Place (2015) 35:85–4. 10.1016/j.healthplace.2015.07.001 [DOI] [PubMed] [Google Scholar]
- 71. Jopling K, Vasileiou K. (2015). Promising approaches to reducing loneliness and isolation in later life (Age UK - Campaign to end loneliness) (Age UK - Campaign to end loneliness).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.