

Abstract
Introduction
China’s one-child policy was replaced by a new universal two-child policy in 2015; however, few studies have addressed the intent to have a second child and resulting related issues.
Methods
We performed a cross-sectional study on 11 991 Chinese women, 18–49 years of age, from 11 provinces in 2016–2017, in order to assess the intent for a second child among Chinese women of childbearing age and other related factors after the introduction of China’s new universal two-child policy.
Results
We found that the overall prevalence of the intent to have a second child was 39.4% and that economic, childrearing, and health barriers affected fertility intent. Multivariate logistic regression models showed that the age range of 25–39 years (aOR 1.28–1.30), living in Eastern (aOR 1.28, 95% CI 1.10 to 1.50) or Central China (aOR 1.52, 95% CI 1.27 to 1.78), living in a rural area (aOR 1.62, 95% CI 1.47 to 1.78), being a farmer (aOR 1.43, 95% CI 1.09 to 1.88), having a higher household income (aOR 1.13, 95% CI 1.00 to 1.28), having a history of abortion (aOR 1.18, 95% CI 1.05 to 1.31), and already having one child (aOR 3.65 for girls, aOR 2.70 for boys) were associated with a greater intent to have a second child (all p<0.05). Conversely, economic, health, childrearing, and educational barriers were associated with a lower intent to have a second child (aOR 0.65–0.75).
Conclusion
Four in ten women of childbearing age demonstrated an intent for a second child. We maintain that fertility-related factors be given full consideration when promoting the two-child policy.
Keywords: fertility, two-child policy, China
Key messages.
Four in ten women of childbearing age planned to have a second child during the first 2 years of China’s universal two-child policy.
Economic, childrearing, and health barriers affected fertility intent.
The age range of 25-39 years, living in rural areas, being a farmer, possessing a higher household income, having a history of abortion, and already having one child were associated with intent for a second child.
Introduction
The total fertility rate in China declined from an estimated 2.9 births per woman in 1979 to between 1.5 and 1.7 births per woman currently.1 The government of China announced the one-child policy in 1979, considering population containment as essential to elevating China out of the severe poverty caused by decades of economic mismanagement.2 Each couple in China was thereby allowed to give birth to one child. After three decades of the one-child policy, China had to face the new challenges of accelerated population ageing, a skewed sex ratio, and the decline in the working-age population.1 2 In order to optimise population structure and cope with accelerated population ageing, the Chinese government changed its policy in 2013, allowing couples (in which at least one of the marital partners was an only child) to have two children.1 In October 2015, the Chinese government announced that all couples would be allowed to have two children, which marked the official end of the one-child policy and the beginning of the new, universal two-child policy.1
This political change was presumably designed to stimulate flagging birth rates in China, which threaten to undermine the economic growth tthat the country has enjoyed in recent decades.3 However, only 1.45 million (13.2%) of the 11 million eligible couples applied for permission to have a second child by May 2015.1 4 Fertility intent is regarded as a predictor of fertility behaviour;5 and in addition to policy, intent to procreate is also influenced by individual, social, economic and cultural factors.4 6 Several investigators have reported on the intent to have a second child in China (which varies from 13.2% to 69.3%) and its associated factors, including age, occupation, educational level, and gender of the first child.4–8 However, these studies were principally conducted in particular populations or settings, such as a rural population, women attending outpatient gynaecology clinics, or women from one specific province. Studies that focus on fertility intent among Chinese women in the general population at the national level are still limited. Thus, we conducted a cross-sectional study to assess the intention to have a second child among Chinese women of childbearing age after the enactment of China’s new universal two-child policy, so as to determine the short-term effects of this policy on fertility plans and to provide suggestions on policymaking.
Methods
Study design and study population
We conducted a cross-sectional study among Chinese women of childbearing age between 2016 and 2017. Participants were selected using a two-stage, stratified sampling method. First, according to the population proportions of the Eastern, Central and Western regions (approximately 5:4:2) in China, we randomly selected provinces in each region (five in the Eastern, 4 in the Central and two in the Western regions). Eleven out of 31 provinces were selected, including five provinces/cities (Beijing, Shanghai, Zhejiang, Fujian and Guangdong) in the Eastern region, four provinces (Henan, Hfourbei, Jiangxi and Hunan) in the Central region and two provinces (Sichuan and Shaanxi) in the Western region. We then selected 1200 participants randomly from each province via an online survey platform (Wen Juan Xing) that was based on their registered information by province. The online survey platform (Wen Juan Xing) was established in 2005 and has 20.29 million Chinese internet users. The inclusion criteria were women 18–49 years of age from 11 provinces in China between 2016 and 2017. The exclusion criteria were women who declined to participate in the survey. A total of 13 200 women aged 18–49 years were selected via the online survey platform and invited to participate in this survey by web, email or text message. Web-based questionnaires were then sent to the selected individuals who agreed to participate in the survey, and participants completed the questionnaires online by mobile phone or computer. Finally, 11 991 of 13 200 women from 11 provinces responded and completed the questionnaires, a response rate of 90.8%. This study was approved by the Institutional Review Board of the Chinese Association of Maternal and Child Health Studies.
Data collection
We used a self-designed questionnaire to collect information from the participants, covering sociodemographic information (age, ethnicity, educational level, occupation, marriage, residence, and annual household income) and reproductive status (current number of children, gender of children, and history of abortion). Fertility intent was investigated with the questions “Do you want to have more children in the future?" (answer Yes or No) and “If you want to have more children, how many more children do you want to have?”. We also investigated gender preferences and barriers to having more children, including economic, childrearing, health, educational, and other barriers. Economic barriers referred to the cost of raising more children. Childrearing barriers referred to the shortage of time or labour in raising more children. Health barriers referred to reasons related to personal health status. Educational barriers referred to the stress of fulfilling the educational needs of children. In the present study, our primary outcome was the prevalence of the intent to have a second child, which was defined as the proportion of women who had the intent to have two or more children among all the women surveyed.
Patient and public involvement
Patients and members of the public were not involved in the development of the study.
Statistical analysis
Categorical variables are shown as proportions. We calculated the prevalence of intent to have a second child and its 95% CI and used the χ² test to compare the rates of second-child intent in different characteristic groups. Univariate and multivariate logistic regression models were used to examine the relative factors associated with intent to have a second child. All factors (independent variables) in the univariate analysis were added to the multivariate model; these were age group, year, ethnicity, region, area of residence, educational level, marital status, occupation, annual household income, history of abortion, having a first child, and barriers. The dependent variable was the intent to have a second child or not. Adjusted odds ratios (aORs) and their 95% CIs were calculated by a backward stepwise method. We performed sensitivity analyses that adjusted for a continuous age variable instead of a five-level age-group variable. We analysed subgroups that were stratified by parity. Two-sided p values <0.05 were considered statistically significant. All analyses were performed with SPSS version 18.0.
Results
Characteristics and fertility intent of the study population
Of the 11 991 women included in the study, 50.8% were 30 years of age or older, 16.0% had a history of abortion, 43.9% had no children, and 43.7% had one child. Approximately 1/3 (1459, 32.9%) of the unmarried women and 2855 (37.8%) of the married women intended to conceive again in the future (online supplementary table 1). Fertility intent was higher in 2017 than in 2016 among unmarried women, married women without any children, and married women with two or more children (all p<0.05).
bmjsrh-2018-200197supp001.pdf (36.5KB, pdf)
Intent to have a second child and related barriers
Of the 11 991 women, the overall rate of second-child intent was 39.4% (95% CI 38.5% to 40.3%; table 1). Among women with one child, the second-child intent rate was 39.5% (95% CI 38.1% to 40.8%). Among women without second-child intent, economic barriers constituted the largest factor (47.7%) affecting fertility intent, followed by childrearing barriers (17.1%) and health barriers (15.6%). The proportion of health barriers increased from 14.5% in 2016 to 16.1% in 2017 (table 2), and women over 35 years of age noted greater health barriers than did women under 35 years, but fewer economic barriers than women aged <35 years (all p<0.001).
Table 1.
Factors associated with the intent to have a second child among 11 991 women of childbearing age
| Factor | n (%) | Intent | Univariate model | Multivariate model | ||
| To have a second child (n (%)) | cORs (95% CI) | P value | aORs (95% CI) | P value | ||
| Total | 11 991 | 4725 (39.4) | ||||
| Year | ||||||
| 2016 | 3647 (30.4) | 1316 (36.1) | 1 | 1 | ||
| 2017 | 8344 (69.6) | 3409 (40.9) | 1.22 (1.13 to 1.33) | <0.001 | 1.31 (1.17 to 1.48) | <0.001 |
| Age (years) | ||||||
| <25 | 2748 (22.9) | 556 (20.2) | 1 | 1 | ||
| 25–29 | 3151 (26.3) | 1308 (41.5) | 2.80 (2.49 to 3.15) | <0.001 | 1.28 (1.10 to 1.50) | 0.002 |
| 30–34 | 2588 (21.6) | 1390 (53.7) | 4.57 (4.05 to 5.16) | <0.001 | 1.30 (1.09 to 1.55) | 0.004 |
| 35–39 | 1812 (15.1) | 900 (49.7) | 3.89 (3.41 to 4.43) | <0.001 | 1.29 (1.15 to 1.44) | 0.016 |
| ≥40 | 1692 (14.1) | 571 (33.7) | 2.01 (1.75 to 2.30) | <0.001 | 0.99 (0.82 to 1.19) | 0.902 |
| Region | ||||||
| Eastern | 8422 (70.2) | 3275 (38.9) | 1.23 (1.07 to 1.41) | 0.004 | 1.28 (1.10 to 1.49) | 0.001 |
| Central | 2582 (21.5) | 1113 (43.1) | 1.46 (1.25 to 1.70) | <0.001 | 1.50 (1.27 to 1.78) | <0.001 |
| Western | 987 (8.2) | 337 (34.1) | 1 | 1 | ||
| Ethnicity | ||||||
| Han | 11 651 (97.2) | 4595 (39.4) | 1 | |||
| Other | 340 (2.8) | 130 (38.2) | 0.95 (0.76 to 1.19) | 0.654 | ||
| Residence | ||||||
| Rural | 4595 (38.3) | 1974 (43.0) | 1.27 (1.18 to 1.37) | <0.001 | 1.62 (1.47 to 1.78) | <0.001 |
| Urban | 7396 (61.7) | 2751 (37.2) | 1 | 1 | ||
| Educational level | ||||||
| Primary school or below | 109 (0.9) | 36 (33.0) | 1 | |||
| Junior high school | 1632 (13.6) | 746 (45.7) | 1.71 (1.13 to 2.57) | 0.011 | ||
| Senior high school | 1088 (9.1) | 493 (45.3) | 1.68 (1.11 to 2.55) | 0.015 | ||
| College or higher | 9162 (76.4) | 3450 (37.7) | 1.22 (0.82 to 1.83) | 0.322 | ||
| Marriage | ||||||
| Single | 4441 (37.0) | 941 (21.2) | 1 | 1 | ||
| Married | 7550 (63.0) | 3784 (50.1) | 3.74 (3.43 to 4.07) | <0.001 | 1.74 (1.50 to 2.02) | <0.001 |
| Occupation | ||||||
| Factory worker | 1614 (13.5) | 710 (44.0) | 1 | 1 | ||
| Farmer | 300 (2.5) | 176 (58.7) | 1.81 (1.41 to 2.32) | <0.001 | 1.43 (1.09 to 1.88) | 0.010 |
| Manager | 3323 (27.7) | 1432 (43.1) | 0.96 (0.86 to 1.09) | 0.551 | 1.07 (0.94 to 1.22) | 0.323 |
| Rural migrant worker | 1392 (11.6) | 681 (48.9) | 1.22 (1.06 to 1.41) | 0.007 | 1.11 (0.95 to 1.30) | 0.200 |
| Clerk | 1714 (14.3) | 594 (34.7) | 0.68 (0.59 to 0.78) | <0.001 | 0.86 (0.71 to 1.03) | 0.103 |
| Student | 1592 (13.3) | 240 (15.1) | 0.23 (0.19 to 0.27) | <0.001 | 0.63 (0.51 to 0.79) | <0.001 |
| Other | 2056 (17.1) | 892 (43.4) | 0.98 (0.86 to 1.11) | 0.714 | 1.02 (0.88 to 1.18) | 0.806 |
| Annual household income (RMB) | ||||||
| <30 000 | 3650 (30.4) | 1151 (31.5) | 1 | 1 | ||
| 30 000–80 000 | 4406 (36.7) | 1847 (41.9) | 1.57 (1.43 to 1.72) | <0.001 | 0.99 (0.88 to 1.10) | 0.798 |
| >80 000 | 3935 (32.8) | 1727 (43.9) | 1.70 (1.55 to 1.87) | <0.001 | 1.13 (1.00 to 1.28) | 0.047 |
| History of abortion | ||||||
| No | 10 073 (84.0) | 3758 (37.3) | 1 | 1 | ||
| Yes | 1918 (16.0) | 967 (50.4) | 1.71 (1.55 to 1.88) | <0.001 | 1.18 (1.05 to 1.31) | 0.004 |
| First child | ||||||
| Boy | 3639 (30.3) | 1811 (49.8) | 3.47 (3.16 to 3.80) | <0.001 | 2.70 (2.33 to 3.13) | <0.001 |
| Girl | 3091 (25.8) | 1745 (56.5) | 4.54 (4.12 to 5.00) | <0.001 | 3.65 (3.14 to 4.24) | <0.001 |
| None | 5261 (43.9) | 1169 (22.2) | 1 | 1 | ||
| Barriers to having more children | ||||||
| Economic barrier | 5576 (46.5) | 2110 (37.8) | 0.65 (0.56 to 0.76) | <0.001 | 0.37 (0.31 to 0.43) | <0.001 |
| Health barrier | 1862 (15.5) | 731 (39.3) | 0.69 (0.59 to 0.82) | <0.001 | 0.39 (0.32 to 0.47) | <0.001 |
| Childrearing barrier | 2040 (17.0) | 794 (38.9) | 0.68 (0.58 to 0.81) | <0.001 | 0.32 (0.27 to 0.39) | <0.001 |
| Educational barrier | 1752 (14.6) | 723 (41.3) | 0.75 (0.64 to 0.90) | <0.001 | 0.38 (0.32 to 0.46) | <0.001 |
| Other | 761 (6.3) | 367 (48.2) | 1 | 1 | ||
aOR, adjusted odds ratio; cOR, crude odds ratio;RMB, renminbi.
Table 2.
Barriers to the intent to have a second child among women without an intent for a second child
| Factor* | Total | 2016 | 2017 | |||
| n | % | n | % | n | % | |
| Economic barrier | 3466 | 47.7 | 1138 | 48.8 | 2328 | 47.2 |
| Childrearing barrier | 1246 | 17.1 | 436 | 18.7 | 810 | 16.4 |
| Health barrier | 1131 | 15.6 | 337 | 14.5 | 794 | 16.1 |
| Educational barrier | 1029 | 14.2 | 326 | 14.0 | 703 | 14.2 |
| Other | 394 | 5.4 | 94 | 4.0 | 300 | 6.1 |
*χ² test, p<0.001.
Factors related to fertility intent for a second child
The intent for a second child in 2017 (40.9%) was higher than in 2016 (36.1%, p<0.001), and its prevalence varied from a nadir of 20.2% in women aged <25 years to a peak (53.7%) in women aged 30–34 years and then declined (table 1). The trends were similar between 2016 and 2017 (figure 1). Intent for a second child was higher in Central China (43.1%) relative to Eastern (38.9%) and Western China (34.1%, p<0.001), higher in rural areas (43.0%) compared with urban areas (37.2%, p<0.001), and higher in women with a history of abortion (50.4%) relative to women without such a history (37.3%, p<0.001). The rate increased commensurately with increasing annual household income (χtrend 2=118.82, p<0.001). Women whose first child was a girl also displayed a greater intent to have a second child (56.5%) compared with women whose first child was a boy (49.8%, p<0.001).
Figure 1.
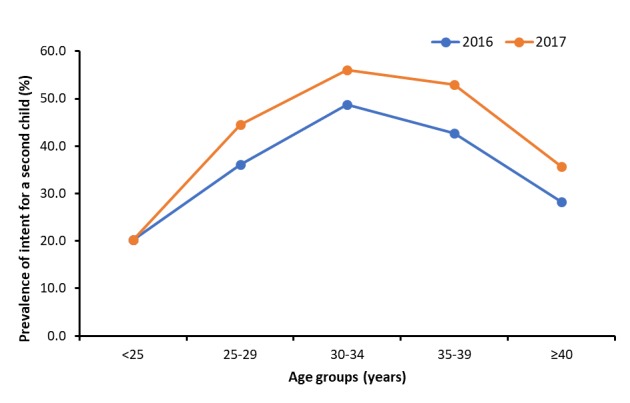
Age-specified prevalence of the intent for a second child among Chinese women in 2016 and 2017.
Multivariate models showed that the age range of 25–39 years (aOR 1.28–1.30), living in Eastern (aOR 1.28, 95% CI 1.10 to 1.50) or Central China (aOR 1.52, 95% CI 1.27 to 1.78), living in a rural area (aOR 1.62; 95% CI 1.47 to 1.78), being a farmer (aOR 1.43, 95% CI 1.09 to 1.88), having a higher household income (aOR 1.13, 95% CI 1.00 to 1.28), having a history of abortion (aOR 1.18, 95% CI 1.05 to 1.31), and already having one child (aOR 3.65 for girls, aOR 2.70 for boys) were associated with a higher intent to have a second child (all p<0.05; table 1). In contrast, economic, health, childrearing, and educational barriers were associated with a reduced intent to have a second child (aOR 0.65–0.75). In the sensitivity analyses, the associations between factors and the intent to have a second child did not change appreciably after adjusting for the continuous variable of age instead of a five-level age group variable. In the subgroup analyses, factors associated with the intent to have a second child were stable (table 3).
Table 3.
Factors associated with the intent to have a second child in the multivariate models stratified by parity
| Characteristics | Multivariate models | |||
| Parity=0 | Parity≥1 | |||
| aOR (95% CI) | P value | aOR (95% CI) | P value | |
| Year | ||||
| 2016 | 1 | 1 | ||
| 2017 | 1.26 (1.03 to 1.54) | 0.023 | 1.36 (1.18 to 1.57) | <0.001 |
| Age (years) | ||||
| <25 | 1 | 1 | ||
| 25–29 | 1.26 (1.06 to 1.50) | 0.008 | 0.74 (0.48 to 1.13) | 0.163 |
| 30–34 | 1.16 (0.90 to 1.49) | 0.263 | 2.22 (1.41 to 3.45) | 0.001 |
| 35–39 | 0.70 (0.47 to 1.04) | 0.075 | 1.96 (1.25 to 3.13) | 0.003 |
| ≥40 | 0.50 (0.30 to 0.84) | 0.009 | 1.33 (1.00 to 1.79) | 0.050 |
| Region | ||||
| Eastern | 1.22 (1.06 to 1.42) | 0.007 | 1.31 (1.16 to 1.49) | <0.001 |
| Central | 1.28 (0.98 to 1.67) | 0.070 | 1.29 (1.07 to 1.55) | 0.008 |
| Western | ||||
| Ethnicity | ||||
| Han | 1 | 1 | ||
| Other | 0.94 (0.67 to 1.34) | 0.743 | 0.73 (0.51 to 1.04) | 0.080 |
| Residence | ||||
| Rural | 1.22 (1.06 to 1.41) | 0.007 | 1.99 (2.27 to 1.74) | <0.001 |
| Urban | 1 | 1 | ||
| Educational level | ||||
| Primary school or below | 1 | 1 | ||
| Junior high school | 1.20 (0.78 to 1.85) | 0.397 | 1.20 (0.78 to 1.84) | 0.415 |
| Senior high school | 1.30 (0.84 to 2.01) | 0.246 | 1.29 (0.83 to 2.00) | 0.252 |
| College or higher | 0.93 (0.61 to 1.41) | 0.723 | 0.91 (0.60 to 1.39) | 0.674 |
| Marriage | ||||
| Single | 1 | 1 | ||
| Married | 1.43 (1.20 to 1.71) | <0.001 | 1.56 (1.17 to 2.08) | 0.002 |
| Occupation | ||||
| Factory worker | 1 | 1 | ||
| Farmer | 1.10 (0.60 to 2.01) | 0.762 | 1.36 (0.98 to 1.89) | 0.068 |
| Manager | 1.31 (1.01 to 1.70) | 0.039 | 1.03 (0.88 to 1.21) | 0.734 |
| Rural migrant worker | 1.04 (0.77 to 1.40) | 0.803 | 1.07 (0.88 to 1.30) | 0.487 |
| Clerk | 0.95 (0.68 to 1.34) | 0.783 | 0.85 (0.68 to 1.07) | 0.165 |
| Student | 0.75 (0.56 to 1.00) | 0.050 | 0.21 (0.04 to 1.18) | 0.076 |
| Other | 1.22 (0.94 to 1.58) | 0.134 | 1.02 (0.86 to 1.22) | 0.809 |
| Annual household income (RMB) | ||||
| <30 000 | 1 | 1 | ||
| 30 000–80 000 | 1.01 (0.85 to 1.21) | 0.888 | 0.95 (0.82 to 1.10) | 0.485 |
| >80 000 | 1.17 (0.95 to 1.44) | 0.140 | 1.12 (0.95 to 1.31) | 0.171 |
| History of abortion | ||||
| No | 1 | 1 | ||
| Yes | 1.81 (1.33 to 2.45) | <0.001 | 1.11 (0.99 to 1.25) | 0.076 |
| Barriers to having more children | ||||
| Economic barrier | 0.68 (0.50 to 0.93) | 0.016 | 0.69 (0.58 to 0.82) | <0.001 |
| Health barrier | 0.96 (0.78 to 1.19) | 0.714 | 0.83 (0.72 to 0.95) | 0.007 |
| Childrearing barrier | 0.83 (0.68 to 0.99) | 0.049 | 0.97 (0.84 to 1.14) | 0.727 |
| Education barrier | 0.92 (0.75 to 1.13) | 0.431 | 0.68 (0.50 to 0.93) | 0.016 |
| Other | 1 | 1 | ||
aOR, adjusted odds ratio; RMB, renminbi.
Discussion
In this cross-sectional study we found that the rate of intent for a second child was 39.4% of 11 991 Chinese women of childbearing age. This was much lower than the rate (61.25%) recorded under the one-child policy6 and was similar to rates reported by others during the two-child policy.9 10 According to the report by the China Women’s Federation in 2017, only 20.5% of parents wanted to have a second child.9 However, Zhao and colleagues,10 in a hospital-based cross-sectional study of 814 nulliparous pregnant women in 2017, reported that 51.2% of women intended to have a second child. The discrepancy between these studies might be related to the different characteristics of the study population, as we found that economic, childrearing, and health factors were the major barriers to fertility intent. Liu and colleagues11 also reported that couples avoided a second conception because of the cost of childrearing and educational and occupational pressures. Most parents regarded a family’s socioeconomic status as a key factor in raising a second child.9 We found that young women considered childraising barriers to be the second most important factor, while women of advanced age considered health to be the second most important factor. It is worth noting that the proportion of health barriers increased from 2016 to 2017, which indicated that parents worried more about maternal and perinatal safety. The quality of women’s eggs declines dramatically with increasing age, leading to an increased risk of pregnancy-related complications for women of advanced age.12 Thus, women of advanced age might give more consideration to health barriers than do younger women.
We found that fertility intent was associated with socioeconomic status, similar to results from previous studies.6 13 14 In our study, the prevalence of intent to have a second child peaked in the 30–34 years age group and gradually declined with increasing age. This trend was consistent with data from North American and European countries13 and might relate to the awareness of women of advanced maternal age (over 35 years) of the higher risks for adverse pregnancy outcomes. Previous studies have shown that women of advanced age exhibited a significantly increased risk of adverse maternal and infant outcomes.15–18 Considerable attention will therefore need to be provided by obstetricians to these older pregnant women.
Our results showed that farmers manifested a greater intent to have a second child relative to workers, which were in accordance with results reported by Zheng and colleagues.6 The intent by farmers to have more children might be related to their need for more labourers within the family, especially in rural areas. We also found household income to be significantly positively associated with fertility intent after adjustment for potential confounders, which was consistent with previous studies.19 20 This might be due to the fact that more affluent people might possess greater means to raise and educate more children. However, some studies showed economic level to be negatively associated with fertility intent.13 14 For example, Kim and colleagues14 found that fertility intent was lower in the group with higher monthly household income. The discrepancy might be related to disparities in economic pressures in different geographical areas. Besides socioeconomic factors, we found that a history of abortion was also associated with higher fertility intent; that is, women with a history of abortion were at higher risk for adverse pregnancy outcomes,21 22 which might prompt the wish for a healthier baby. We also found that women with one child had a higher fertility intent compared with women with no children, and the OR was even higher in women whose first child was a girl compared with women whose first child was a boy. This could be partially explained by the traditional preference for boys.1 7
The main strength of our study is that it is the first to estimate the intent to have a second child and to evaluate related factors in the general population during the new two-child policy in China; this could provide useful information for policymakers in providing better family planning services in the future. Our study also has several limitations. First, we collected the data via the web, so that women who were not internet users were not included in the study. Nevertheless, in China there were as many as 751 million internet users in 2017, accounting for one in five of the world's internet users; and 96.3% of them surf the internet by mobile phone.23 Additionally, internet use was more prevalent in women of childbearing age than in other age groups. Second, women from this study were selected via people listed on Wen Juan Xing, and thus selection biases might limit the generalisability of the results. We compared the distribution of age groups in each region in our survey to that in the statistical yearbook and found that the proportion of women under 25 years of age was higher in the Western region, which might lead to the underestimation of fertility intent. Moreover, using the backward stepwise method for model selection might lead to parameter estimates far from zero.24 Third, other risk factors such as fertility-related knowledge and attitude, and the intention of family members, were not investigated in the present study.
In conclusion, four out of 10 women of childbearing age planned to have a second child during China’s universal two-child policy, with economic, childrearing, and health barriers affecting fertility intent. The age range of 25–39 years, living in Eastern or Central China or in rural areas, being a farmer, possessing a higher household income, having a history of abortion, and already having one child were associated with a more pronounced intent to have a second child. We therefore assert that fertility-related factors be given full consideration when promoting the implementation of the new two-child policy.
Footnotes
Contributors: JL searched the literature, analysed the data, interpreted the results, and drafted the manuscript. QM collected the data. SZ and QW revised the manuscript. ML conceived the study, designed the study, supervised the study, interpreted the results, and revised the manuscript.
Funding: This study was funded by the National Natural Science Foundation of China (Grant No. 81703240) and the Chinese Association of Maternal and Child Health Studies (Grant No. AMCHS-2016-1).
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request.
References
- 1. Zeng Y, Hesketh T. The effects of China's universal two-child policy. Lancet 2016;388:1930–8. 10.1016/S0140-6736(16)31405-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Hesketh T, Lu L, Xing ZW. The effect of China's one-child family policy after 25 years. N Engl J Med 2005;353:1171–6. 10.1056/NEJMhpr051833 [DOI] [PubMed] [Google Scholar]
- 3. Sun W, Gordon J, Pacey A. From one to two: the effect of women and the economy on China’s One Child Policy. Hum Fertil 2016;19:1–2. 10.3109/14647273.2016.1168980 [DOI] [PubMed] [Google Scholar]
- 4. National Health and Family Planning Commission Press conference of National Health and Family Planning Commission on July 10th, 2015. Available: http://www.nhc.gov.cn/xcs/s3574/201507/43685ecd0edb4b71b260306af9b7e924.shtml [Accessed 31 Oct 2019].
- 5. Lau BH-P, Huo R, Wang K, et al. Intention of having a second child among infertile and fertile women attending outpatient gynecology clinics in three major cities in China: a cross-sectional study. Hum Reprod Open 2018;2018 10.1093/hropen/hoy014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zheng Y, Yuan J, Xu T, et al. Socioeconomic status and fertility intentions among Chinese women with one child. Hum Fertil 2016;19:43–7. 10.3109/14647273.2016.1154988 [DOI] [PubMed] [Google Scholar]
- 7. Jiang Q, Li Y, Sanchez-Barricarte JJ, et al. Fertility intention, son preference, and second childbirth: survey findings from Shaanxi Province of China. Soc Indic Res 2016;125:935–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wei J, Xue J, Wang D. Socioeconomic determinants of rural women's desired fertility: a survey in rural Shaanxi, China. PLoS One 2018;13:e0202968 10.1371/journal.pone.0202968 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. China Women's Federation Two-child policy's impact on family education, 2017. Available: http://www.womenofchina.cn/womenofchina/html1/data_speaks/1701/579-1.htm [Accessed 13 Nov 2017].
- 10. Zhao J, Shan N, Yang X, et al. Effect of second child intent on delivery mode after Chinese two child policy implementation: a cross sectional and prospective observational study of nulliparous women in Chongqing. BMJ Open 2017;7:e018823 10.1136/bmjopen-2017-018823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Liu F, Bao J, Boutain D, et al. Online responses to the ending of the one-child policy in China: implications for preconception care. Ups J Med Sci 2016:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Li Q, Deng D. New medical risks affecting obstetrics after implementation of the two-child policy in China. Front Med 2017;11:570–5. 10.1007/s11684-017-0552-5 [DOI] [PubMed] [Google Scholar]
- 13. Dribe M, Hacker JD, Scalone F. The impact of socio-economic status on net fertility during the historical fertility decline: a comparative analysis of Canada, Iceland, Sweden, Norway, and the USA. Popul Stud 2014;68:135–49. 10.1080/00324728.2014.889741 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kim J, Sung J. Socioeconomic status and number of children among Korean women: the healthy twin study. J Prev Med Public Health 2013;46:50–60. 10.3961/jpmph.2013.46.1.50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Cheng PJ, Duan T. China's new two-child policy: maternity care in the new multiparous era. BJOG 2016;123 Suppl 3:7–9. 10.1111/1471-0528.14290 [DOI] [PubMed] [Google Scholar]
- 16. Blomberg M, Birch Tyrberg R, Kjølhede P. Impact of maternal age on obstetric and neonatal outcome with emphasis on primiparous adolescents and older women: a Swedish medical birth register study. BMJ Open 2014;4:e005840 10.1136/bmjopen-2014-005840 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Laopaiboon M, Lumbiganon P, Intarut N, et al. Advanced maternal age and pregnancy outcomes: a multicountry assessment. BJOG 2014;121 Suppl 1:49–56. 10.1111/1471-0528.12659 [DOI] [PubMed] [Google Scholar]
- 18. Lean SC, Derricott H, Jones RL, et al. Advanced maternal age and adverse pregnancy outcomes: a systematic review and meta-analysis. PLoS One 2017;12:e0186287 10.1371/journal.pone.0186287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. McQuillan J, Greil AL, Shreffler KM. Pregnancy intentions among women who do not try: focusing on women who are okay either way. Matern Child Health J 2011;15:178–87. 10.1007/s10995-010-0604-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. LC L, Liu YQ;, Yang XQ;, et al. Second child intention and its risk factors among married couples in Shanghai, China. Reprod Contracept 2014;34:914–7. [Google Scholar]
- 21. Oliver-Williams C, Fleming M, Wood AM, et al. Previous miscarriage and the subsequent risk of preterm birth in Scotland, 1980-2008: a historical cohort study. BJOG 2015;122:1525–34. 10.1111/1471-0528.13276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Makhlouf MA, Clifton RG, Roberts JM, et al. Adverse pregnancy outcomes among women with prior spontaneous or induced abortions. Am J Perinatol 2014;31:765–72. 10.1055/s-0033-1358771 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. China Internet Network Information Center The 40th China statistical report on Internet development, 2017. Available: http://cnnic.cn/hlwfzyj/hlwxzbg/hlwtjbg/201708/P020170807351923262153.pdf [Accessed 13 Nov 2017].
- 24. Harrell F. Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. New York: Springer-Verlag, 2001: 67–8. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjsrh-2018-200197supp001.pdf (36.5KB, pdf)