

Abstract
Background
Onychomycosis refers to fungal infections of the nail apparatus that may cause pain, discomfort, and disfigurement. This is an update of a Cochrane Review published in 2007; a substantial amount of new research warrants a review exclusively on toenails.
Objectives
To assess the clinical and mycological effects of topical drugs and device‐based therapies for toenail onychomycosis.
Search methods
We searched the following databases up to May 2019: the Cochrane Skin Group Specialised Register, CENTRAL, MEDLINE, Embase and LILACS. We also searched five trials registers, and checked the reference lists of included and excluded studies for further references to relevant randomised controlled trials.
Selection criteria
Randomised controlled trials of topical and device‐based therapies for onychomycosis in participants with toenail onychomycosis, confirmed by positive cultures, direct microscopy, or histological nail examination. Eligible comparators were placebo, vehicle, no treatment, or an active topical or device‐based treatment.
Data collection and analysis
We used standard methodological procedures expected by Cochrane. Primary outcomes were complete cure rate (normal‐looking nail plus fungus elimination, determined with laboratory methods) and number of participants reporting treatment‐related adverse events.
Main results
We included 56 studies (12,501 participants, average age: 27 to 68 years), with mainly mild‐to‐moderate onychomycosis without matrix involvement (where reported). Participants had more than one toenail affected. Most studies lasted 48 to 52 weeks; 23% reported disease duration (variable). Thirty‐five studies specifically examined dermatophyte‐caused onychomycosis. Forty‐three studies were carried out in outpatient settings. Most studies assessed topical treatments, 9% devices, and 11% both.
We rated three studies at low risk of bias across all domains. The most common high‐risk domain was performance bias. We present results for key comparisons, where treatment duration was 36 or 48 weeks, and clinical outcomes were measured at 40 to 52 weeks.
Based on two studies (460 participants), compared with vehicle, ciclopirox 8% lacquer may be more effective in achieving complete cure (risk ratio (RR) 9.29, 95% confidence interval (CI) 1.72 to 50.14; low‐quality evidence) and is probably more effective in achieving mycological cure (RR 3.15, 95% CI 1.93 to 5.12; moderate‐quality evidence). Ciclopirox lacquer may lead to increased adverse events, commonly application reactions, rashes, and nail alteration (e.g. colour, shape). However, the 95% CI indicates that ciclopirox lacquer may actually make little or no difference (RR 1.61, 95% CI 0.89 to 2.92; low‐quality evidence).
Efinaconazole 10% solution is more effective than vehicle in achieving complete cure (RR 3.54, 95% CI 2.24 to 5.60; 3 studies, 1716 participants) and clinical cure (RR 3.07, 95% CI 2.08 to 4.53; 2 studies, 1655 participants) (both high‐quality evidence) and is probably more effective in achieving mycological cure (RR 2.31, 95% CI 1.08 to 4.94; 3 studies, 1716 participants; moderate‐quality evidence). Risk of adverse events (such as dermatitis and vesicles) was slightly higher with efinaconazole (RR 1.10, 95% CI 1.01 to 1.20; 3 studies, 1701 participants; high‐quality evidence). No other key comparison measured clinical cure.
Based on two studies, compared with vehicle, tavaborole 5% solution is probably more effective in achieving complete cure (RR 7.40, 95% CI 2.71 to 20.24; 1198 participants), but probably has a higher risk of adverse events (application site reactions were most commonly reported) (RR 3.82, 95% CI 1.65 to 8.85; 1186 participants (both moderate‐quality evidence)). Tavaborole improves mycological cure (RR 3.40, 95% CI 2.34 to 4.93; 1198 participants; high‐quality evidence).
Moderate‐quality evidence from two studies (490 participants) indicates that P‐3051 (ciclopirox 8% hydrolacquer) is probably more effective than the comparators ciclopirox 8% lacquer or amorolfine 5% in achieving complete cure (RR 2.43, 95% CI 1.32 to 4.48), but there is probably little or no difference between the treatments in achieving mycological cure (RR 1.08, 95% CI 0.85 to 1.37). We found no difference in the risk of adverse events (RR 0.60, 95% CI 0.19 to 1.92; 2 studies, 487 participants; low‐quality evidence). The most common events were erythema, rash, and burning.
Three studies (112 participants) compared 1064‐nm Nd:YAG laser to no treatment or sham treatment. We are uncertain if there is a difference in adverse events (very low‐quality evidence) (two studies; 85 participants). There may be little or no difference in mycological cure at 52 weeks (RR 1.04, 95% CI 0.59 to 1.85; 2 studies, 85 participants; low‐quality evidence). Complete cure was not measured.
One study (293 participants) compared luliconazole 5% solution to vehicle. We are uncertain whether luliconazole leads to higher rates of complete cure (very low‐quality evidence). Low‐quality evidence indicates there may be little or no difference in adverse events (RR 1.02, 95% CI 0.90 to 1.16) and there may be increased mycological cure with luliconazole; however, the 95% CI indicates that luliconazole may make little or no difference to mycological cure (RR 1.39, 95% CI 0.98 to 1.97). Commonly‐reported adverse events were dry skin, paronychia, eczema, and hyperkeratosis, which improved or resolved post‐treatment.
Authors' conclusions
Assessing complete cure, high‐quality evidence supports the effectiveness of efinaconazole, moderate‐quality evidence supports P‐3051 (ciclopirox 8% hydrolacquer) and tavaborole, and low‐quality evidence supports ciclopirox 8% lacquer. We are uncertain whether luliconazole 5% solution leads to complete cure (very low‐quality evidence); this outcome was not measured by the 1064‐nm Nd:YAG laser comparison. Although evidence supports topical treatments, complete cure rates with topical treatments are relatively low.
We are uncertain if 1064‐nm Nd:YAG laser increases adverse events compared with no treatment or sham treatment (very low‐quality evidence). Low‐quality evidence indicates that there is no difference in adverse events between P‐3051 (ciclopirox hydrolacquer), luliconazole 5% solution, and their comparators. Ciclopirox 8% lacquer may increase adverse events (low‐quality evidence). High‐ to moderate‐quality evidence suggests increased adverse events with efinaconazole 10% solution or tavaborole 5% solution.
We downgraded evidence for heterogeneity, lack of blinding, and small sample sizes. There is uncertainty about the effectiveness of device‐based treatments, which were under‐represented; 80% of studies assessed topical treatments, but we were unable to evaluate all of the currently relevant topical treatments.
Future studies of topical and device‐based therapies should be blinded, with patient‐centred outcomes and an adequate sample size. They should specify the causative organism and directly compare treatments.
Plain language summary
Are topical and device‐based treatments effective in people with fungal infections of the toenails?
Review question
We reviewed evidence about the effect of topical and device‐based treatments for fungal infections of the toenails (toenail onychomycosis) when compared against each other, placebo (an identical but inactive treatment), vehicle (inactive ingredients that help deliver an active treatment), or no treatment. We assessed adults, whose infection was diagnosed based on studying nail samples.
Background
Toenail onychomycosis causes pain, discomfort, and disfigurement. Topical and device‐based treatments can have less likelihood of drug interactions or side effects than oral drugs. Antifungal medications are either fungistatic (inhibiting fungal growth) or fungicidal (killing fungal pathogens). The shared goal of devices (e.g. laser, photodynamic therapy) is fungus destruction.
Study characteristics
In searches up to May 2019, we found 56 studies including 12,501 men or women (average age: 27 to 68 years) who had mainly mild‐to‐moderate toenail onychomycosis. Onychomycosis duration was under‐reported, but varied from months to years. Approximately 63% of the studies assessed onychomycosis caused by dermatophytes (fungi). Most studies lasted 48 to 52 weeks and were conducted in an outpatient setting. The studies used either device‐based or topical treatments, including lacquers and creams, alone or in combination, compared to each other, to no treatment, to vehicle, or to placebo.
Key results
For the following key results, treatment lasted 36 or 48 weeks, and outcomes were measured at 40 to 52 weeks (side effects were measured throughout the study).
Compared to vehicle (no treatment), efinaconazole 10% topical solution is better at achieving complete cure (i.e. normal‐looking nail coupled with fungus elimination determined using laboratory methods) (high‐quality evidence). Tavaborole 5% solution (when compared to vehicle) and P‐3051 (ciclopirox 8% hydrolacquer) (when compared to two other treatments: ciclopirox 8% lacquer or amorolfine 5%) are probably better at achieving this outcome (both moderate‐quality evidence). Ciclopirox 8% lacquer may lead to higher complete cure rates than vehicle, but rates are low (not all patients can be expected to achieve complete cure) (low‐quality evidence).
Ciclopirox 8% lacquer and efinaconazole 10% are probably more effective at eliminating the fungus (mycological cure) than vehicle, but for P‐3051 (ciclopirox 8% hydrolacquer) there is probably little or no difference compared to the two comparator treatments (all moderate‐quality evidence). Tavaborole 5% improves mycological cure compared to vehicle (high‐quality evidence).
We found no evidence of a difference in side effects, including redness, rash, and burning, between P‐3051 (ciclopirox 8% hydrolacquer) and the two other treatments (low‐quality evidence), and ciclopirox 8% lacquer may increase side effects, including application‐site reactions, rashes, and changes in the nail compared with vehicle, although treatment effects vary, so it is possible that it may actually make little or no difference (low‐quality evidence). Compared to vehicle, participants were slightly more likely to experience side effects (commonly dermatitis and fluid‐filled sacs) with efinaconazole 10% (high‐quality evidence) and probably more likely to experience side effects with tavaborole 5% (commonly, application‐site reactions, such as dermatitis, redness, and pain) (moderate‐quality evidence).
We are uncertain of the effect of luliconazole 5% on complete cure when compared to vehicle (very low‐quality evidence); there may be little or no difference between these groups in side effects (dry skin, eczema, and thickening of the skin were commonly reported, but improved after stopping treatment), and luliconazole 5% solution might increase mycological cure; however, the effects of this treatment vary, so it is possible that it may actually make little or no difference to mycological cure (both low‐quality evidence).
Three studies compared laser to no treatment or sham treatment, and there may be little or no difference in mycological cure (low‐quality evidence). Complete cure was not measured, and we are uncertain if there is a difference in side effects between groups (very low‐quality evidence).
Efinaconazole 10% solution is more effective in achieving clinical cure than vehicle (high‐quality evidence); none of the other key comparisons measured this outcome.
Quality of the evidence
We base our conclusions on varied evidence quality. For complete cure, mycological cure, and side effects, quality ranged from low to high, with very low‐quality evidence found for three key results.
Many studies were small, had design issues, and did not directly compare therapies. No studies reported quality of life.
Summary of findings
Background
Please see Table 7 for a glossary of unfamiliar terms.
1. Glossary of terms.
| Term | Definition |
| Allylamine | Class of antifungal molecules used to treat skin and nails. Examples include butenafine and terbinafine |
| Azole | Class of antifungal compounds used to treat skin and nails, characterised by a 5‐membered nitrogen heterocyclic ring. Examples include ketoconazole and fluconazole |
| Benzoxaborole | Class of small molecules characterised by a boron atom. The antifungal tavaborole is a member of this class |
| Cross‐contamination | Unintentional transfer of a micro‐organism from 1 object or person to another |
| Dermatophytes | Infectious fungi that feed on the keratin present in the skin, hair, and nails, which usually cause an inflammatory response at the site of infection |
| Distal | Away from the cuticle, toward the end of the nail |
| Dystrophic | Progressive damage or deformity characterised by the wasting away of tissue or both |
| Fungicidal | To kill fungal cells |
| Fungistatic | To impede the growth and reproduction of fungal cells |
| Hydroxypyridone | Class of compounds with antifungal properties used to treat skin and nails. Example: ciclopirox |
| Hyponychium | The skin beneath the distal free edge of the nail |
| Iontophoresis | A method whereby ionic medicinal compounds are introduced into the body by applying an electrical current to the skin |
| Keratin | A key protein in the structure of skin, hair, and nails |
| Lateral | To the sides (of the nail) |
| PCR | Polymerase chain reaction, a molecular biology technique that uses DNA amplification to identify organisms, such as fungi |
| Proximal | Close to (the cuticle) |
| Metalloproteases | Enzymes in the body that break down proteins and contain a metal ion to aid in this process |
| Morpholine derivative | An antifungal based on the organic compound morpholine. Example: amorolfine |
| Mycological | Concerning fungi |
| Nail apparatus | Refers to the nail and associated underlying structures (Figure 1) |
| Onycholysis | Detachment of the nail from the nail bed |
| Subungual | Underneath the nail |
| Synthetase | A biological enzyme that acts in the body to combine molecules or compounds together |
| Tinea pedis | Also known as 'athlete's foot', an infection of skin of the feet typically caused by dermatophytes |
Description of the condition
Onychomycosis is a fungal infection of the nail apparatus (Zaias 1972). It is primarily caused by dermatophytes, which are infectious fungi that feed on the keratin present in the skin, hair, and nails, that usually cause an inflammatory response at the site of infection (Welsh 2010). Yeasts and non‐dermatophyte moulds can also cause onychomycosis, either alone or in combination with dermatophytes (Gupta 2012; Welsh 2010). Fungi are ubiquitous in the environment and are found in greater abundance in warm or damp areas that foster growth (e.g. public change rooms and showers of athletic facilities, sweaty shoes) (Lipner 2018). For fungal infection to occur, a portal of entry to the nail unit has to exist; this usually occurs when there is trauma (i.e. injury) to the seal or space between the nail bed and nail plate (Figure 1) (Lipner 2018). Trauma (i.e. nail deformity) can also occur from long‐term wear of ill‐fitting or tight shoes (Lipner 2018). Many people seek treatment for cosmetic purposes, but onychomycosis is an infectious condition, so it is critical that it is treated to prevent cross‐contamination to family members, and secondary complications such as tinea pedis (Szepietowski 2006). Patients with onychomycosis report decreased quality of life and may restrict their activities because of embarrassment about the aesthetic appearance of their nails (Reich 2011).
1.
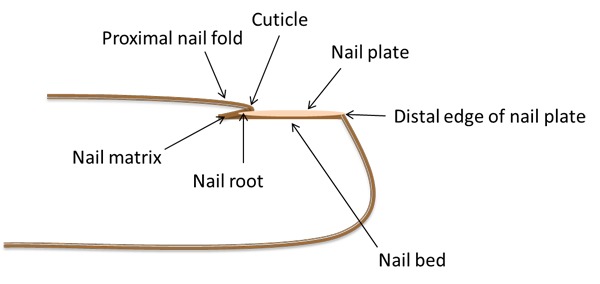
Anatomy of the nail
Clinical presentation
Onychomycosis has several clinical presentations, including distal and lateral subungual (under the nail) onychomycosis (DLSO), proximal subungual onychomycosis, superficial white onychomycosis, and total dystrophic onychomycosis (Hay 2011). DLSO is the most common form of onychomycosis and often presents as a result of tinea pedis (Hay 2011). DLSO affects the nail plate, nail bed, and hyponychium, which is the skin beneath the distal free edge of the nail, and may present with streaks of pigmentation in the nail and uneven borders, which distinguishes it from simple onycholysis, where the nail detaches from the nail bed (Hay 2011). Proximal subungual onychomycosis is initiated at the proximal nail fold and is usually whitish in colour, while superficial white onychomycosis is localised to the centre of the nail plate with a white, chalky appearance (Hay 2011). Total dystrophic onychomycosis is the most severe form of onychomycosis; it affects the entire nail plate and results in nail thickening along with complete loss of normal nail architecture (Hay 2011). The severity of onychomycosis can be described as mild, moderate, or severe. Published studies will assign a label of mild‐moderate disease if less than approximately 60% of the nail is showing symptoms (i.e. discolouration). This upper limit is variable: studies will use values between 50% and 75% and use the term mild‐moderate disease (Elewski 2013c; Elewski 2015a; Gupta 2000a; Iorizzo 2016). It is often at the clinician's discretion to determine what is mild‐moderate and severe disease.
Figure 1 presents the anatomy of the nail, including the distal, lateral, and proximal areas of the nail.
Epidemiology
Onychomycosis accounts for approximately 50% of reported nail disorders (Faergemann 2003). A systematic review (Sigurgeirsson 2014) reported the population‐based prevalence of onychomycosis as 4.3% in Europe and North America and found it was more prevalent in men in North America and Europe and in women in South America. The review reported that onychomycosis was more common in toenails than in fingernails, with clinic‐based studies indicating toenail infections to be 10 times more common than fingernail infections. Infection was most commonly caused by the dermatophyte fungal organism Trichophyton rubrum (44.9%), followed by yeasts (21.2%), other dermatophytes (20.1%), and moulds (13.3%; Sigurgeirsson 2014).
Risk factors and comorbidities
Onychomycosis is associated with a number of medical conditions and with age (Baran 2011). Patient characteristics such as advancing age, family members with tinea pedis or onychomycosis, genetics, and obesity may increase the risk of onychomycosis (Baran 2011; Rosen 2015). Some medical conditions occur concurrently with onychomycosis, such as diabetes, immunosuppression, peripheral vascular disease, and psoriasis, and can also increase risk for onychomycosis (Baran 2011; Döner 2011; Rosen 2015). There is an increased prevalence of onychomycosis in individuals with psoriasis, diabetes, immunosuppression, peripheral vascular disease, and obesity (Baran 2011; Döner 2011; Gupta 1997; Gupta 2000; Ozkan 2013). It is critical to treat and to monitor onychomycosis in individuals with these conditions, as secondary complications are a concern. Poor circulation, compromised immune systems, and inability to adequately care for the feet may exacerbate a fungal infection and provide opportunity for systemic fungal or bacterial infections to develop, with potential for cellulitis and septicaemia (Döner 2011; Fukunaga 2013; Gupta 2000; Ozkan 2013). Symptoms of psoriasis may worsen and treatment become complicated by the presence of fungus (Crowley 2015; Rigopoulos 2017; Ventura 2017). It is well documented in diabetes that complications with inadequate foot and nail care include foot ulcers and cellulitis, with progression to amputation and sometimes even death (Akkus 2017; Papini 2013; Rossaneis 2013). These patients may also have contraindications for the oral antifungals terbinafine and itraconazole due to drug‐drug interactions or a higher risk of adverse events (Baran 2008; Barber 2006).
Description of the intervention
Topical drugs for onychomycosis generally come in the form of lacquers or solutions directly applied to the surface of the nail (Gupta 2013). Device‐based therapies may include, but are not limited to, laser systems, iontophoresis, photodynamic therapy, and ultrasound (Gupta 2013). Topical drugs or devices are used in cases of mild‐to‐moderate onychomycosis and where oral antifungal drugs are contraindicated due to comorbidities or concerns with adverse events (Gupta 2014b). Oral treatments for fungal infections of the toenails are also commonly used (Gupta 2015a), but they are outside the scope of this review.
How the intervention might work
Topical drugs
Antifungal drugs can either be fungistatic, preventing further growth of fungal cells, or fungicidal, killing fungal cells entirely. Most antifungal drugs inhibit cell membrane synthesis, but others target protein translation and fungal proteases (Gupta 2013). Topical drugs are usually applied daily for 12 months in order to allow the normal nail to grow and replace the regions damaged by infection, although a few studies have used between six and 12 months (Gupta 2014b). Drugs formulated for topical application in onychomycosis include those from the allylamine (e.g. butenafine, terbinafine), azole (e.g. clotrimazole, efinaconazole, miconazole), hydroxypyridone (e.g. ciclopirox), morpholine‐derivative (e.g. amorolfine, Kunzea oil), and benzoxaborole (e.g. tavaborole) classes (Gupta 2013; Gupta 2014a). The azoles, allylamines, and morpholine‐derivative drugs inhibit ergosterol biosynthesis, an essential component of the cell wall (Gupta 1994). The hydroxypyridone‐class drug ciclopirox inhibits metalloproteases by binding metal ions (metalloproteases are enzymes that help with fungal cell survival) (Valeant 2004). The benzoxaborole‐class drugs inhibit protein translation by inhibiting the fungal leucine transfer ribonucleic acid (tRNA) synthetase (Rock 2007).
Application of topical treatments is usually daily for 12 months (Elewski 2013c; Elewski 2015a; Gupta 2000a), with amorolfine applied once or twice weekly for 12 months (Galderma 2011; Iorizzo 2016). Topical treatments come in cream, lacquer, and solutions of varying concentrations (e.g. 5% to 10%) and are applied to the nail plate and skin surrounding the nail. In the case of lacquers, alcohol solution is used to remove buildup of lacquer on the nails; daily removal with amorolfine and weekly removal with ciclopirox is recommended (Dermik 2003; Galderma 2011). Debridement, i.e. removal of infected nail by trimming or filing, or both, by patients as required or monthly by healthcare professionals may be advised, particularly in the case of lacquers (Dermik 2003; Galderma 2011). For ciclopirox, a hydrolacquer solution (P‐3051), based on a film‐forming, water‐soluble vehicle, has been formulated which eliminates the need for nail filing or alcohol removal (Baran 2009). Chemical removal or softening of the nails can be achieved using urea paste or creams with the aim of increasing the effectiveness of topical treatments that are used in combination or to allow easier removal of infected nail (Gupta 2014b; Lahfa 2013). Topical treatments do not generally have drug interactions, which is useful where patients are already taking multiple oral medications (Lipner 2019). Adverse events are usually related to skin reactions around the nail, such as rash, itching, or burning (Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b). The standard topical treatment will depend on geographical location; where there is more than one option, clinicians will use their expertise to determine treatment.
Devices
Devices have diverse mechanisms of action. Laser device systems are thought to act through selective photothermolysis, which is the conversion of light energy into heat energy that is confined to a specific target (Anderson 1983). The specific target in this case is fungi, which selectively absorb heat that leads to cell death (Gupta 2016b). Iontophoresis devices use an electrical current to increase the penetration of a topically‐applied drug into the nail plate (Amichai 2010). Photodynamic therapy uses a narrow‐spectrum light source to activate topically‐applied photosensitisers (Piraccini 2008). The activation of the photosensitiser creates cellular damage that kills fungal cells (Piraccini 2008). Treatment with devices occurs in a clinical setting and may require weekly or monthly visits. As with topicals, devices do not interact with other medications, and if adverse events occur they are generally associated with transient pain or discomfort with laser treatment (Hollmig 2014; Karsai 2017; Lipner 2019). Devices are considered alternatives to antifungal treatments and in the USA are approved to improve visual appearance, not to cure the infection (Lipner 2019). This Cochrane Review did not identify any new devices with novel mechanisms of action.
Why it is important to do this review
A Cochrane Review on dermatophyte infections of the feet and nails was published in 2007 (Crawford 2007). Since then, a substantial amount of research on topical drugs and device‐based therapies for the treatment of onychomycosis has emerged in the scientific literature, warranting a review exclusively on toenails. Topical drugs and devices are important therapeutic options for mild‐to‐moderate onychomycosis. The advantage of effective topical therapies for onychomycosis is that they are not distributed throughout the body systemically, which may mean there is less likelihood of drug interactions or adverse events.
As these categories of therapies increase, it is important that healthcare professionals have accurate information about the optimal dosage and treatment regimens, so they can effectively treat patients with new drugs and devices.
The plans for this review were published as a protocol (Gupta 2016a).
Objectives
To assess the clinical and mycological effects of topical drugs and device‐based therapies for onychomycosis.
Methods
Criteria for considering studies for this review
Types of studies
We include randomised controlled trials (RCTs) of topical and device‐based therapies for onychomycosis. We exclude cross‐over trials. This is because cross‐over trials are only appropriate when the intervention does not produce a permanent change in patient status. The endpoint with onychomycosis treatment is cure, and a cross‐over following cure would not be appropriate.
Types of participants
We include men and women over 18 years of age who have onychomycosis of the toenails. Infection was diagnosed based on studying nail samples using direct microscopic examination (potassium hydroxide), culture, periodic acid‐Schiff stain (PAS), or molecular biology (e.g. polymerase chain reaction (PCR)). Some studies may have reported results of fingernails and toenails combined; in these cases, we tried to obtain results for toenails alone and when this was not possible, we excluded the study.
Types of interventions
We include RCTs that compared a topical or device‐based therapy with placebo, vehicle, no treatment, or an active comparator that was topical or device‐based.
Types of outcome measures
We assessed outcomes based on the following time points: less than 12 weeks, between 12 and 36 weeks, between 36 and 52 weeks, and more than 52 weeks. We excluded studies lasting less than 12 weeks. Our primary outcomes are presented in a 'Summary of findings' table.
Primary outcomes
Complete cure rate: the proportion of participants with 0% nail plate involvement and mycological cure at follow‐up.
Adverse events: the proportion of participants who reported at least one event, whether or not related to the intervention. In addition and where possible, we reported adverse events based on the likelihood of their being related to the interventions, as judged by the study investigator(s).
Secondary outcomes
Mycological cure rate: the proportion of participants who achieved negative mycological testing as defined by the study at follow‐up.
Clinical cure rate: the proportion of participants who achieved 0% nail plate involvement at follow‐up.
Compliance: the proportion of participants who completed the study protocol without deviations, as defined by study investigators.
Time to recurrence.
Quality of life: this was described based on measures included by study investigators.
Pharmaco‐economics: the cost of the treatment was described.
Search methods for identification of studies
We aimed to identify all relevant RCTs, regardless of language or publication status (published, unpublished, in press, or in progress).
Electronic searches
The Cochrane Skin Information Specialist searched the following databases up to 7 May 2019:
the Cochrane Skin Group Specialised Register, using the search strategy in Appendix 1;
the Cochrane Central Register of Controlled Trials (CENTRAL) 2019, Issue 5, in the Cochrane Library, using the strategy in Appendix 2;
MEDLINE via Ovid (from 1946), using the strategy in Appendix 3;
Embase via Ovid (from 1974), using the strategy in Appendix 4; and
Latin American and Caribbean Health Science Information database (LILACS), from 1982, using the strategy in Appendix 5.
Trial registries
We (KF, RM) searched the following trials registers up to 13 May 2019 using the following terms: onychomycosis or tinea unguium.
the ISRCTN registry (www.controlled‐trials.com);
ClinicalTrials.gov (www.clinicaltrials.gov);
the Australian New Zealand Clinical Trials Registry (www.anzctr.org.au);
the World Health Organization International Clinical Trials Registry platform (ICTRP) (apps.who.int/trialsearch); and
the EU Clinical Trials Register (www.clinicaltrialsregister.eu).
Searching other resources
References from published papers
We checked the bibliographies of included and excluded studies for additional references to relevant RCTs.
We handsearched the Mycoses journal from 1957 to 1990 for additional studies. Later editions of the journal are indexed in MEDLINE and Embase, so it was not necessary to handsearch them.
Unpublished literature
We conducted online searches of pharmaceutical company websites and the US Food and Drug Administration (FDA) website.
We contacted experts in the field of dermatology seeking information about unpublished trials, including those listed in trial registries and conference abstracts.
Conference proceedings
We handsearched the following conference proceedings for relevant trials for years that the Cochrane Skin Group had not already handsearched:
British Association of Dermatologists (1982 to 2013);
Annual Meetings of the American Academy of Dermatology (1990 to 2013);
European Academy of Dermatology and Venereology (1996 to 2013);
European Society for Dermatological Research (1970 to 2012); and
Australasian College of Dermatologists (1996 to 2013).
Adverse effects
We did not perform a separate search for adverse effects of the target intervention. However, we examined data on adverse effects from the included studies that we identified.
Data collection and analysis
Selection of studies
We managed studies using Microsoft Excel 2010 software. Two review authors, KF and SV, screened the references and each performed independent study selection. We piloted the study selection criteria on a subsample of the articles (approximately 10) in order to validate the criteria and ensure that they were consistently interpreted for all studies. We examined all articles and documents retrieved to determine if they complied with the inclusion and exclusion criteria. We discussed disagreements in order to reach a consensus. If we could not reach consensus, we consulted a third review author (RM).
Data extraction and management
Two review authors (from KF, RM, or SV) independently extracted the data for each included study using a standard form, including the study design, number of participants randomised into each treatment group, baseline characteristics, health intervention, treatment regimen and duration, treatment success and failure, safety, tolerability, the number of participants lost to follow‐up, the duration of follow‐up, and pharmaco‐economic data. We piloted the forms on a small group of studies to ensure completeness. We discussed disagreements in order to reach a consensus. If we could not reach consensus, a third review author performed additional data extraction. The first review author (KF) entered the data into Review Manager 5 (Review Manager 2014), and the second review author (RM or SV) verified the data. We were not blinded to authors, institutions, or journals during data extraction.
Assessment of risk of bias in included studies
Two authors, KF and RM, independently evaluated risks of bias in individual studies using Cochrane's 'Risk of bias' tool (Higgins 2017), resolving disagreements by discussion. The 'Risk of bias' ('RoB') table includes the following domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, within‐study selective outcome reporting, and other potential sources of bias (e.g. reporting outcomes for subgroups rather than all participants; reporting data for each group to which participants were randomised in a multiple‐arm intervention study, rather than combining multiple arms).
Measures of treatment effect
We analysed dichotomous outcomes using a risk ratio (RR) with a 95% confidence interval (CI).
We quantified significantly different outcomes as the number needed to treat for an additional beneficial/harmful outcome(NNTB/H), based on the following formula: NT = 1/ARC * (1‐RR) (Centre for Evidence‐Based Medicine). We used the RRs from the meta‐analysis and the moderate assumed control risk (ARC) calculated in GRADEpro GDT (Guideline Development Tool) (GRADEPro).
Unit of analysis issues
The participant was the unit of analysis, with clinical trials designating one target toenail per participant as the unit of analysis. We did not consider nail data in clinical studies that used individual nails as the unit of analysis, including multiple toenails per participant in their data set. The exception to this was in the case of studies where multiple toenails per participant were included if outcomes were reported per participant. We did not consider participant‐controlled data. We excluded within‐participant designs because onychomycosis is contagious and can spread to other nails in the same foot of a single patient or between feet in a single patient. Furthermore, the effect of the intervention may also carry. Between‐participant designs control this by treating all nails with the same intervention. We excluded cross‐over trials with the aim of any treatment for onychomycosis as cure, which is a permanent change in patient status. Where studies had multiple intervention arms, all arms are mentioned in the Characteristics of included studies table.
Dealing with missing data
If data were missing or in a format that precluded extraction, we contacted the study authors to request that information. We prioritised intention‐to‐treat (ITT) data and converted per‐protocol data into ITT data wherever possible (e.g. when attrition data were available). We considered participants who discontinued a study to be treatment failures. If we were unable to acquire all missing data, we performed analyses with the available data.
Assessment of heterogeneity
We assessed the heterogeneity of the included studies for clinical and statistical factors. Clinical factors may include population age, comorbidities, and disease severity. We quantified statistical heterogeneity using the I2 statistic (Higgins 2019). The Handbook provides a range of values for moderate (30% to 60%), substantial (50% to 90%), and considerable (75% to 100%) heterogeneity.
Assessment of reporting biases
We planned to investigate selective reporting of outcomes in analyses with 10 studies or more (Dwan 2008), generating funnel plots of the data to determine if reporting asymmetry was present. We did not do this, as none of our analyses had 10 studies or more.
Data synthesis
We performed data synthesis using Review Manager 5 (Review Manager 2014). We calculated risk ratios (dichotomous data) using the Mantel‐Haenszel model. Where meta‐analysis was possible (e.g. at least two trials), we conducted the analyses using a random‐effects model. For studies with multiple intervention arms, we selected the relevant interventions. Where possible, we combined intervention arms so that we could include a single comparison in the meta‐analysis. When this was not possible, we used the relevant intervention arms in the analysis and identified them in the footnotes of the forest plot. Where we estimated results for individual studies with low numbers of events (fewer than 10 in total) or where the total sample size was fewer than 30 participants and we used a risk ratio, we reported the proportion of events in each group together with a P value from a Fisher's Exact test.
If meta‐analysis was not possible due to the number of trials (fewer than two), we assessed the studies for the data collected qualitatively.
Subgroup analysis and investigation of heterogeneity
When we found moderate statistical heterogeneity (I2 statistic greater than 50%), we conducted subgroup analysis. We analysed any clinical sources of heterogeneity, such as participant age and onychomycosis severity, if we had sufficient studies (at least two studies with a combined sample size of 30 or more for each group being compared (Dijkman 2009)).
Sensitivity analysis
In analyses with considerable heterogeneity (I2 statistic greater than 75%), we conducted a sensitivity analysis to determine if removing studies with identified risks of bias contributed to the overall heterogeneity.
'Summary of findings' tables
We present the data for the primary outcomes (complete cure and adverse events) and for two of our secondary outcomes (mycological cure and clinical cure) in six 'Summary of findings' tables. We assessed the quality of the evidence across the outcome measures that were reported in the 'Summary of findings' tables using the GRADE assessment and GRADEpro GDT software (GRADEPro; Ryan 2016a; Ryan 2016b). The comparisons for which we created tables were: ciclopirox 8% lacquer versus vehicle; P‐3051 (ciclopirox 8% hydrolacquer) versus comparators; efinaconazole 10% solution versus vehicle; tavaborole 5% solution versus vehicle; luliconazole 5% solution versus vehicle; 1064‐nm Nd:YAG laser versus control.
Results
Description of studies
Results of the search
Searches of electronic databases, clinical trial registries, and conference proceedings yielded 1745 records. We found an additional 23 records from checking the reference lists of included and excluded studies. After removing duplicates, we had 1402 unique records for screening. We excluded 1259 records based on title/abstract review. We assessed the full text of 143 records for eligibility. We excluded 51 records (Characteristics of excluded studies). We identified 13 ongoing studies (see Characteristics of ongoing studies) and 22 studies awaiting classification (see Characteristics of studies awaiting classification).
We included 56 studies reported in 57 references (see Characteristics of included studies). We included 12 of these studies in the meta‐analysis, and described the results of the remaining 44. Of these 44 studies, seven were published recently (2014 to 2019) and are depicted individually using forest plots. For a further description of our screening process, see the study flow diagram (Figure 2). We contacted authors for 48 of the 56 included studies and received a response, positive or negative, for 29 of the 48 studies (Table 8).
2.
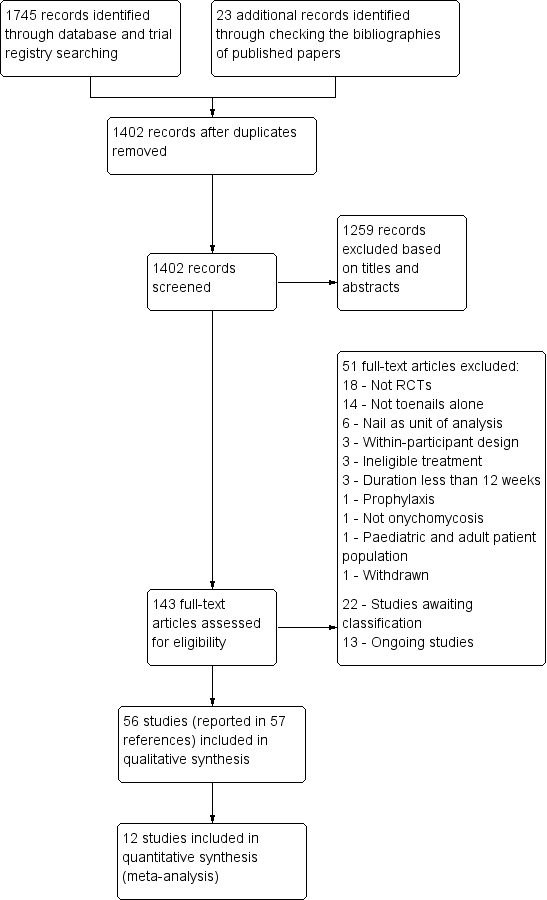
Study flow diagram.
2. Correspondence with study authors.
| Study | Contact & Date | Information Requested | Response |
| Included studies | |||
| ACTRN12614000946617 | Dr. J. Thomas Email correspondence July 2017 |
Update on study | Email response received July 2017. Manuscript is currently under review. |
| ACTRN12614001238662 | Dr. T. Altaei Email correspondence July 2017 June 2019 |
Update on study | Email response received July 2017. No further response. Manuscript is currently in preparation for publication. |
| Alberdi 2019 | Dr. C. Gomez Email correspondence June 2019 |
Allocation concealment and blinding procedures; was the study registered? | Email response received June 2019. Responses recorded in Characteristics of included studies table. |
| Amichai 2010 | Dr. B. Amichai Email correspondence May 2017 |
Randomisation and blinding procedures; treatment received by protocol violations and those experiencing AEs |
No response |
| Baran 2009 | Dr. R. Baran Email correspondence August 2017 |
Blinding procedures; reasons for attrition | No response |
| Bonhert 2019 | Dr. N. Sadick Email correspondence June 2019 |
Randomisation, allocation concealment, blinding procedures; any information on adverse events for efinaconazole; was the trial registered? | No response |
| Buck 1994 | Dr. D. Buck Research Gate August 2017 |
Treatment allocation of drop‐outs | No response |
| Eertmans 2018 | Dr. F. Eertmans Email correspondence June 2019 |
Allocation concealment, outcome assessor blinding | Email response received June 2019. Responses recorded in Characteristics of included studies table |
| Elewski 2013c; Elewski 2013d | Mr. B. Bulley Email correspondence August 2017 |
What do the percentages of AEs not related to study drug in the article refer to? | Email response received August 2017: total number of AEs reported, not number of patients. For study 1, 1047 and 352 (efinaconazole and vehicle) and study 2, 908 and 278 (efinaconazole and vehicle) |
| Elewski 2015a; Elewski 2015b | Dr. N. Lowe, Sandoz Email correspondence May 2017 |
Randomisation and blinding procedures | Email response received May 2017. Responses recorded in Characteristics of included studies table |
| EUCTR2005‐005905‐51 | Ms. M.A. Rhyne, GSK Email correspondence September 2018 |
Randomisation and blinding procedures; are results available?; reasons for attrition | Email response received Sept 2018. Inquiry being directed to appropriate person |
| EUCTR2006‐000974‐54 | Ms. F. Sidou, Galderma Email correspondence August 2017 |
Randomisation and blinding procedures; are results available?; possible conflicts of interest for study investigators | Email response received August 2017: Unable to assist. If find any information on person who conducted the study, will inform ‐ No further correspondence |
| EUCTR2006‐005895‐42 | Dr. J.‐P. Meyer, Evolva Holdings SA Research Gate September 2018 |
Randomisation and blinding procedures; are results available?; reasons for attrition | No response |
| EUCTR2008‐003215‐13 | Bayer website contact form August 2017 Consumer relations Email correspondence September 2017 |
Randomisation and blinding procedures; are results available? reasons for attrition; possible conflicts of interest for study investigators | No response |
| EUCTR2016‐001242‐25 | Dr. J. Dobmeyer, Blueberry Therapeutics Email correspondence June 2019 |
Randomisation, allocation concealment, blinding procedures; any update on study results? | Email response received July 2019. Responses recorded in Characteristics of included studies table |
| Gupta 2000a; Gupta 2000b | Dr. A.K. Gupta | Randomisation and blinding procedures | No further information available |
| Gupta 2006 | Dr. A.K. Gupta | Randomisation and blinding procedures; attrition data | No further information available |
| Hartmane 2013 | Dr. M. Caserini, Polichem Email correspondence August 2017 |
Randomisation and blinding procedures; availability of results, poster or published; reasons for attrition | Email response received Aug. 2017 Study was presented as an abstract and is not published yet. |
| Hollmig 2014 | Dr. J.Y. Tang Email correspondence September 2018 |
Allocation concealment procedure | Email response received Sept. 2018 Responses recorded in Characteristics of included studies table. |
| Ijzerman 2010 | Dr. M. Ijzerman, Millendo Ms. L. Scallion, NanoBio Email correspondence May 2017 |
Is there more information about this study? Has it been published or are there e‐posters? | Email response received May 2017 No longer at company. Provided L. Scallion’s contact information. ‐ No further response |
| Iorizzo 2016 | Dr. M. Iorizzo Email correspondence September 2017 |
Randomisation procedures; any attrition data | Email response received Sept. 2017 Responses recorded in Characteristics of included studies table |
| Koren 2018 | Dr. A. Koren Email correspondence June 2019 |
Randomisation, allocation concealment, blinding procedures; was the study registered? | Email response received June 2019 Responses recorded in Characteristics of included studies table |
| Kumar 2001 | Dr. K. Kulkarni Email correspondence September 2017 |
Randomisation and blinding procedures; trial registration | No response |
| Lahfa 2013 | Dr. M. Lahfa Email correspondence August 2017 |
Reasons for participant withdrawal | No response |
| Lu 2005 | Dr. Lu Email correspondence May 2017 Apricus Biosciences Web contact form September 2018 |
Randomisation and blinding procedures; are results available? | Automatic email response: no longer with company ‐ No further response from web form |
| Montana 1994 | Dr. R.K. Scher Email correspondence August 2017 Columbia Dermatology Email correspondence September 2018 |
Randomisation and blinding procedures; attrition data | Email response received August 2017 Unable to provide information. Referred to Columbia Dermatology. ‐ No further correspondence |
| NCT01080079 | NitrcBio Therapeutics Email Correspondence September 2017 |
Are results available for the trial? | No response |
| NCT01145807 | Dr. E. Tschen Email Correspondence September 2017 |
Are results available for the trial? | No response |
| NCT01246518 | Dr. K. Rensfeldt, Moberg Pharma Email Correspondence September 2018 |
Randomisation and allocation concealment procedures; are results available or published? | Email response received Oct 2018. Data is not available. Trial procedures documented in Characteristics of included studies table. |
| NCT01400594 | Hisamitsu Pharmaceutical Web contact form September 2018 |
Randomisation, allocation concealment, blinding procedures; attrition data; are results available or published? | No response |
| NCT02022215 | Meiji Seika Pharma Email Correspondence September 2017 |
Are results available for the trial? | No response |
| NCT02343627 | Taro Pharmaceuticals USA Email Correspondence September 2017 |
Are results available for the trial? | No response, results posted on clinicaltrials.gov 22 August 2018 |
| NCT03141840 | Dr. I. Mouratidou‐Kontorinis Email Correspondence June 2019 |
Randomisation, allocation concealment, blinding procedures; attrition data; are results available or published? | Email response received June 2019. Data is not yet available. Trial procedures documented in Characteristics of included studies table |
| Parekh 2017 | Leodevico L. Ilag Email correspondence April 2019 |
Were fingernails and toenails treated? | Email response received April 2019. Confirmed that toenails were included in study and that fingernails were not |
| Paul 2013 | Dr. C. Paul Email correspondence August 2017 |
Randomisation procedures | Email forwarded to Pierre Fabre. Response received September 2017. Responses recorded in Characteristics of included studies table |
| Romero‐Cerecero 2008 | Dr. O. Romero‐Cerecero Email correspondence August 2017 |
Randomisation and blinding procedures; trial registration | No response |
| Romero‐Cerecero 2009 | Dr. O. Romero‐Cerecero Dr. J. Tortoriello Email correspondence August 2017 |
Randomisation and blinding procedures; trial registration; treatment regimen | No response |
| Schalka 2012 | Dr. S. Schalka Email correspondence August 2017 |
Randomisation and blinding procedures; trial registration | No response |
| Stein 2014 | Dr. L. Stein Gold Email correspondence May 2017 |
Are results available or published? | Email response received May 2017. No additional information available |
| Syed 1998; Syed 1999 | Dr. T.A. Syed Research Gate August 2017 |
Randomisation procedures | No response |
| Toledo‐Bahena 2014 | Dr. N. Lowe, Sandoz Email correspondence May 2017 |
Randomisation and blinding procedures | Email response received May 2017. Responses recorded in Characteristics of included studies table. |
| Tschen 2013 | Mr. B. Bulley Email correspondence May 2017 |
Blinding procedures; mycological cure rate for control group | Email response received May 2017. Responses recorded in Characteristics of included studies table. |
| Waibel 2013 | Dr. J. Waibel Email correspondence August 2017 |
Randomisation and blinding procedures | No response |
| Watanabe 2017 | Dr. S. Watanabe Email correspondence August 2017 |
Blinding procedures | No response |
| Excluded studies | |||
| Bassiri‐Jahromi 2012 | Dr. S. Bassiri‐Jahromi Email correspondence September 2017 |
Attrition data and outcome data | No response |
| El‐Tatawy 2015 | Dr. R. El‐Tatawy Email correspondence September 2017 |
Is data available for toenails alone? | No response |
| Emtestam 2012 | Dr. A. Toft, Moberg Pharma Email correspondence September 2017 |
Are results/attrition data available for toenails alone? | Email response received September 2017 Unable to find requested information |
| Gilaberte 2017 | Dr. Y. Gilaberte Email correspondence September 2017 |
Is data available for toenails alone? | Email response received October 2017 A separate analysis was not performed |
| Halmy 2005 | Dr. K. Halmy Email correspondence August 2017 |
Are data available? Has the study been published? | No response |
| Kim 2016b | Dr. S.J. Lee Email correspondence September 2017 |
Is data available for toenails alone? | No response |
| Lauharanta 1992 | Dr. J. Lauharanta Research Gate September 2017 |
Definitions of efficacy outcomes, data available for toenails alone? | No response |
| Li 2014 | Dr. Y. Li Email correspondence September 2017 |
Is data available for toenails alone? | No response |
| Menéndez 2011 | Dr. S. Menendez Email correspondence May 2017 |
Did this study include both fingernails and toenails? If yes, are data available for toenails alone? | Email response received May 2017 Yes, the study included both fingernails and toenails. Original data not accessible |
| Tietz 2013 | Dr. H. Merk Email correspondence September 2017 |
Is data available for toenails alone? | No response |
| Zhang 2012a | Dr. Zhang Email correspondence September 2017 |
Is data available for toenails alone? | No response |
| Zhou 2016 | Dr. B.R. Zhou Email correspondence September 2017 |
Is data available for toenails alone? | No response |
| Ongoing studies | |||
| DRKS00007709 | Dr. Raulin Email correspondence September 2018 |
Update on study | No response |
| EUCTR2016‐001204‐39 | Dr. C. Strid, Moberg Pharma Email correspondence September 2018 |
Update on study | Email response received September 2018 The study has not been completed yet |
| NCT02961634 | Dr. A.C. Prazias Massei Email correspondence MIP Brasil Farma Online Contact Form September 2018 |
Update on study | Email undeliverable No response |
| NCT03814343 | Dr. C. Leeyaphan Email correspondence May 2019 |
Is the study performed on toenail, fingernails, or both? | Email response received May 2019 Study is performed with toenails only |
| Studies awaiting classification | |||
| Anonymous 2002 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Barquero 2007 | Dr. N. Barquero Research Gate November 2017 |
What are the ages of the patients? Was this study randomised? | No response |
| Butareva 1986 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Emokpare 1977 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| EUCTR2008‐002427‐90 | Substipharm Email correspondence September 2018 |
Update on study data, how was onychomycosis diagnosed? | No response |
| George 1991 | Email correspondence May 2017 Email with CSG November 2017 |
Full‐text article | No response CSG: article not available in register |
| Grant 1974 | Email correspondence May 2017 Email with CSG November 2017 |
Full‐text article | No response CSG: article not available in register |
| JPRN‐JapicCTI‐101143 | Hisamitsu Pharmaceutical Web contact form September 2018 |
Were fingernails and/or toenails evaluated? Are results available or published? | No response |
| Klima 1976 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | article not available in register |
| Kull 1972 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Mathur 1973 | Online journal contact form May 2017 Email with CSG November 2017 |
Full‐text article | No response CSG: article not available in register |
| NCT00253305 | Mr. J. Piper, MediQuest Therapeutics Email correspondence September 2018 |
Update on study, are results available? How long did participants receive treatment for? | No response |
| Park 2017 | Beom Joon Kim Email correspondence April 2019 |
Were fingernails and toenails treated? | No response |
| Ramm 1994 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Rüping 1993a | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Rüping 1993b | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Schubert 1973 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Weuta 1972 | Cochrane Skin Group (CSG) Email correspondence November 2017 |
Full‐text article | Article not available in register |
| Yao 2016 | Dr. X.H. Wang Email correspondence May 2017 |
Were fingernails and toenails treated? How were patients mycologically diagnosed? | No response |
Included studies
Trial settings
All 56 studies were RCTs, with a total of 12,501 participants. Twenty‐four studies were described as multicentre. Twenty‐two studies were published in 2010 or earlier. Forty‐three studies were conducted in outpatient dermatology settings; 23 studies had at least one trial site in the USA and 18 studies had a European trial site.
Trial design
Thirty‐nine studies were two‐arm studies (ACTRN12614000946617; ACTRN12614001238662; Alberdi 2019; Amichai 2010; Bonhert 2019; Buck 1994; Eertmans 2018; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2006‐005895‐42; EUCTR2008‐003215‐13; Gupta 2000a; Gupta 2000b; Hollmig 2014; Iorizzo 2016; Karsai 2017; Koren 2018; Kumar 2001; Lahfa 2013; Montana 1994; NCT01080079; NCT01246518; NCT01400594; NCT02343627; NCT03141840; NCT03289871; Nijenhuis‐Rosien 2019; Parekh 2017; Paul 2013; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Schalka 2012; Sigurgeirsson 2016; Syed 1998; Syed 1999; Watanabe 2017).
The remaining 17 studies had three arms or more (Auvinen 2015; Baran 2009; Elewski 2013a; EUCTR2005‐005905‐51; EUCTR2006‐000974‐54; EUCTR2016‐001242‐25; Gupta 2006; Hartmane 2013; Ijzerman 2010; Lu 2005; NCT01145807; NCT02022215; NCT02933879; Stein 2014; Toledo‐Bahena 2014; Tschen 2013; Waibel 2013). All interventions are described in the Characteristics of included studies tables. For studies with multiple intervention arms that were included in meta‐analyses, the relevant interventions were identified and used in the analysis. For example, Tschen 2013 includes three efinaconazole arms; in our meta‐analysis, we used the efinaconazole arm that was consistent with that assessed in the Phase 3, two‐arm studies (Elewski 2013c; Elewski 2013d) and thus the approved treatment for patient use. Treatments used in meta‐analyses are identified in the footnotes of forest plots. For single studies, we list all interventions and available results in Table 9. All topical treatment studies used one target toenail per person, usually the big toenail, to evaluate treatment. Device trials evaluated multiple nails per person; however, we were able to include the studies because treatment outcomes were reported per person, so all affected nails had to be cured for a person to be considered cured (Hollmig 2014; Karsai 2017; Waibel 2013).
3. Summary of single studies.
| Treatments (n) | Treatment duration | Complete cure | Adverse events | Mycological cure | Clinical cure | |
| Topical treatment versus vehicle/placebo | ||||||
| Baran 2009a | P‐3051 (ciclopirox 8% hydrolacquer), n = 182 | Once daily for 48 weeks | 10/182 RR 10.90, 95% CI 0.65 to 184.03 |
14/180 RR 0.63, 95% CI 0.30 to 1.31 |
156/182 RR 1.28, 95% CI 1.10 to1.49 |
‐ |
| Placebo, n = 97 | 0/97 | 12/97 | 65/97 | ‐ | ||
| Post hoc analysis: < 50% nail involvement at baseline measured at 60 weeks | ‐ | ‐ | ‐ | ‐ | ‐ | |
| P‐3051 (ciclopirox 8% hydrolacquer), n = 119 | Once daily for 48 weeks | 18/119 RR 9.53, 95% CI 1.30 to 69.74 |
‐ | 98/119 RR 1.08, 95% CI 0.92 to 1.27 |
‐ | |
| Placebo, n = 63 | 1/63 | ‐ | 48/63 | ‐ | ||
| Elewski 2013ab | Terbinafine nail solution (TNS), n = 259 |
Once daily for 24 weeks | 3/259 RR 1.49, 95% CI 0.25 to 8.87 |
306/526 RR 0.96, 95% CI 0.87 to 1.06 |
33/259 RR 2.05, 95% CI 1.16 to 3.64 |
6/259 RR 1.00, 95% CI 0.33 to 3.05 |
| Vehicle, n = 258 | 2/258 | 308/507 | 16/258 | 6/258 | ||
| TNS, n = 271 | Once daily for 48 weeks | 6/271 RR 12.28, 95% CI 0.70 to 216.94 |
176/269 RR 0.91, 95% CI 0.81 to 1.02 |
51/271 RR 3.44, 95% CI 1.95 to 6.06 |
10/271 RR 1.05, 95% CI 0.43 to 2.54 |
|
| Vehicle, n=256 | 0/256 | 183/254 | 14/256 | 9/256 | ||
| EUCTR2006‐000974‐54 | Amorolfine 10% lacquer, n = 31 | Daily for 2 weeks, then weekly until 6 months | ‐ | 7/31 | ‐ | ‐ |
| Amorolfine 4% lacquer, n = 30 | ‐ | 11/30 | ‐ | ‐ | ||
| Vehicle lacquer, n = 34 | ‐ | 7/34 | ‐ | ‐ | ||
| Amorolfine 5% lacquer, n = 32 | ‐ | 12/32 | ‐ | ‐ | ||
| EUCTR2008‐003215‐13b | Bifonazole 1% cream and urea 40% paste, n = 347 | 14 ‐ 28 days urea followed by cream for 28 days | ‐ | 12/328 RR 0.67, 95% CI 0.33 to 1.37 |
156/347 RR 1.09, 95% CI 0.92 to 1.30 |
‐ |
| Placebo cream and urea 40% paste, n = 345 | ‐ | 18/330 | 142/345 | ‐ | ||
| Gupta 2006b | 1% terbinafine nail lacquer (TNL), n = 12 |
Daily for 6 weeks | ‐ | 0/12 | 4/12 | ‐ |
| 5% TNL, n = 12 | ‐ | 1/12 | 5/12 | ‐ | ||
| 10% TNL, n = 12 | ‐ | 2/12 | 6/12 | ‐ | ||
| 1% TNL, n = 20 | Daily for 12 weeks | ‐ | 1/20 | 6/20 | ‐ | |
| 5% TNL, n = 20 | ‐ | 1/20 | 8/20 | ‐ | ||
| 10% TNL, n = 20 | ‐ | 0/20 | 11/20 | ‐ | ||
| Ciclopirox 8% lacquer, n = 12 | ‐ | 0/12 | 5/12 | ‐ | ||
| Placebo lacquer, n = 12 | ‐ | 0/12 | 4/12 | ‐ | ||
| Kumar 2001b | Herbal capsule and cream, n = 21 |
Twice daily for 12 weeks | ‐ | ‐ | 17/21 RR 5.94, 95% CI 2.03 to 17.34 |
‐ |
| Placebo capsule and cream, n = 22 |
‐ | ‐ | 3/22 | ‐ | ||
| Lahfa 2013b | 40% urea with plastic dressing + bifonazole, n = 53 | Urea combination daily for 3 weeks, then bifonazole cream for 8 weeks | 13/53 RR 1.28, 95% CI 0.61 to 2.65 |
4/53 RR 0.56, 95% CI 0.17, to .80 |
20/53 RR 0.70, 95% CI 0.46 to 1.07 |
19/53 RR 1.33, 95% CI 0.75 to 2.37 |
| 40% urea with 1% bifonazole + bifonazole, n =52 | 10/52 | 7/52 | 28/52 | 14/52 | ||
| Montana 1994 | Fungoid tincture, n = 10 | Twice daily for 12 months | ‐ | 9/20 | Culture: 5/10 KOH: 5/10 RR 5.00, 95% CI 0.70 to 35.50 |
‐ |
| Vehicle, n = 10 | ‐ | Culture: 1/10 KOH: 1/10 |
‐ | |||
| NCT02343627a | NVXT solution, n = 35 | Once daily for 60 days | ‐ | 7/35 RR 0.75, 95% CI 0.16 to 3.52 |
14/35 RR 3.33, 95% CI 0.63 to 17.57 |
‐ |
| Vehicle, n = 12 | ‐ | 3/12 | 2/12 | ‐ | ||
| NCT02933879a | NVXT topical solution, n = 64 | Once daily for 8 weeks | 1/64 | 19/64 | 7/64 | 1/64 |
| NVXT topical solution, n = 61 | Once daily for 2 x 8‐week periods, separated by 32 weeks | 0/61 RR 0.31, 95% CI 0.0 to 7.50 vs placebo |
14/62 RR 1.01, 95% CI 0.52 to 1.96 vs placebo |
13/61 RR 1.01, 95% CI 0.50 to 2.03 vs placebo |
1/61 RR 0.93, 95% CI 0.06 to 14.59 vs placebo |
|
| Placebo, n = 57 | 1/57 | 13/58 | 12/57 | 1/57 | ||
| Syed 1998a | Butenafine HCl 2% and 20% urea, n = 50 |
Twice daily for 7 days | 44/50 RR 19.20, 95% CI 1.28 to 288.53 |
5/50 RR 2.37, 95% CI 0.14 to 39.84 |
‐ | ‐ |
| Placebo, n = 10 | 0/10 | 0/10 | ‐ | ‐ | ||
| Syed 1999a | Butenafine HCl 2% and 5% Melaleuca alternifolia oil, n = 40 |
3 times/day, max. 8 weeks with occlusive dressing | 32/40 RR 33.29, 95% CI 2.14 to 517.19 |
4/40 RR 4.61, 95% CI 0.26 to 81.63 |
‐ | ‐ |
| Placebo (Melaleuca alternifolia oil), n = 20 |
0/20 | 0/20 | ‐ | ‐ | ||
| Toledo‐Bahena 2014a | 2.5% tavaborole solution, n = 33 | Once daily for 3 months, then 3 times/week for 3 months | ‐ | 14/33 | 32/33 | ‐ |
| 5% tavaborole solution, n = 31 | ‐ | 13/31 RR 0.94, 95% CI 0.57 to 1.55 vs vehicle |
29/31 RR 1.11, 95% CI 0.97 to 1.28 vs vehicle |
‐ | ||
| 7.5% tavaborole solution, n = 60 | ‐ | 30/60 | 57/60 | ‐ | ||
| Vehicle, n = 63 | ‐ | 28/63 | 53/63 | ‐ | ||
| Topical treatment versus topical treatment | ||||||
| Buck 1994a | 100% Melaleuca alternifolia (Tea tree oil), n = 64 | Twice daily for 6 months | ‐ | 5/64 RR 1.38, 95% CI 0.35 to 5.51 |
7/64 RR 1.45, 95% CI 0.45 to 4.68 |
‐ |
| 1% clotrimazole solution, n = 53 | ‐ | 3/53 | 4/53 | ‐ | ||
| Elewski 2013bb | TNS, n = 507 | Once daily for 48 weeks | 6/507 RR 1.24, 95% CI 0.38 to 4.02 |
285/493 RR 1.02, 95% CI 0.91 to 1.13 |
82/507 RR 1.03, 95% CI 0.78 to 1.36 |
8/507 RR 0.82, 95% CI 0.33 to 2.07 |
| Amorolfine 5% nail lacquer, n = 522 | Twice weekly with nail filing for 48 weeks | 5/522 | 291/512 | 82/522 | 10/522 | |
| Hartmane 2013 | P‐3058 5%, n = 18 | Daily for 24 weeks | ‐ | ‐ | Culture: 18/18 KOH: 14/18 |
‐ |
| P‐3058 10%, n = 19 | ‐ | ‐ | Culture: 16/19 KOH: 13/19 |
‐ | ||
| P‐3058 10%, n = 20 | Weekly for 24 weeks | ‐ | ‐ | Culture: 18/20 KOH: 15/20 |
‐ | |
| Paul 2013b | Chemical nail avulsion (RV4104A ointment) + ciclopirox cream + ciclopirox lacquer, n = 71 | Avulsion ointment for 3 weeks, then cream for 8 weeks, then lacquer for 25 weeks | ‐ | 13/72 RR 0.37, 95% CI 0.21 to 0.64 |
35/71 RR 1.46, 95% CI 0.98 to 2.18 |
‐ |
| Amorolfine nail lacquer, n = 71 | Twice weekly for 36 weeks | ‐ | 34/70 | 24/71 | ‐ | |
| Romero‐Cerecero 2008c | A. pichinchensis extract 10%, n = 55 | 3 times/week for 1st month; 2 times/week for 2nd month; weekly for 4 months | 27/55 RR 0.90, 95% CI 0.63 to 1.29 |
0/55 RR 0.14, 95% CI 0.01 to 2.70 |
29/55 RR 0.97, 95% CI 0.68 to 1.37 |
35/55 RR 0.92, 95% CI 0.71 to 1.20 |
| Ciclopirox 8%, n = 55 | 30/55 | 3/55 | 30/55 | 38/55 | ||
| Romero‐Cerecero 2009 | A. pichinchensis extract 12.6%, n = 62 | 6 months | 37/62 RR 0.94, 95% CI 0.71 to 1.25 |
0/62 | ‐ | 37/62 RR 0.94, 95% CI 0.71 to 1.25 |
| A. pichinchensis extract 16.8%, n = 60 | 38/60 | 0/60 | ‐ | 38/60 | ||
| Schalka 2012a | Ciclopirox nail lacquer, n = 20 | Daily for 6 months | ‐ | 0/20 | 14/20 RR 0.98, 95% CI 0.66,1.45 |
‐ |
| Ciclopirox nail lacquer, n = 21 | 3 times/week for 1st month; 2 times/week for 2nd month; weekly for 4 months | ‐ | 0/21 | 15/21 | ‐ | |
| Tschen 2013b | Efinaconazole 10% solution without semi‐occlusion, n = 39 | Daily for 36 weeks | 10/39 | 30/39 | 34/39 | ‐ |
| Efinaconazole 10% solution with semi‐occlusion, n = 36 | 8/36 | 25/36 | 30/36 | ‐ | ||
| Efinaconazole 5% solution without semi‐occlusion, n = 38 | 6/38 | 25/38 | 33/38 | ‐ | ||
| Vehicle, n = 22 | 2/22 | 14/22 | 16/22 | ‐ | ||
| Devices | ||||||
| Amichai 2010c | 1% terbinafine HCl with iontophoretic patch, n = 20 | Overnight 5 days/week, 4 weeks | ‐ | 2/38 | 16/20 RR 1.80, 95% CI 1.03 to 3.15 |
‐ |
| 1% terbinafine HCl patch without iontophoresis, n = 18 | ‐ | 8/18 | ‐ | |||
| Waibel 2013a | 1064 nm laser, n = 7 | Weekly for 4 weeks | ‐ | 0/7 | 7/7 | ‐ |
| 1319 nm laser, n = 7 | ‐ | 0/7 | 6/7 | ‐ | ||
| BroadBand light, n = 7 | ‐ | 0/7 | 7/7 | ‐ | ||
Definitions of mycological cure: anegative culture alone; bnegative KOH microscopy and negative culture; cnegative KOH microscopy alone
Participants
Sample sizes varied from 10 to 1044 participants (median: 119). The age of the participants across studies ranged from 27 to 68 years of age. As per eligibility criteria, all participants were aged 18 and over. All studies, with the exception of Gupta 2006 and Lu 2005, specified the inclusion of both genders. With the exception of one study, in which a specific patient group was used (Chinese participants with onychomycosis) (Gupta 2006), all studies were open to general dermatology patients diagnosed with onychomycosis. Approximately 63% (35 studies) specifically examined onychomycosis caused by dermatophytes alone, requiring confirmation of dermatophyte infection prior to study entry (Amichai 2010; Auvinen 2015; Baran 2009; Buck 1994; Elewski 2013a; Elewski 2013b; Elewski 2015a; Elewski 2015b; EUCTR2005‐005905‐51; EUCTR2006‐000974‐54; EUCTR2006‐005895‐42; Gupta 2000a; Gupta 2000b; Gupta 2006; Hartmane 2013; Ijzerman 2010; Karsai 2017; Koren 2018; Kumar 2001; Lahfa 2013; Lu 2005; NCT01080079; NCT01246518; NCT01400594; NCT02022215; NCT02343627; NCT02933879; NCT03141840; Parekh 2017; Paul 2013; Romero‐Cerecero 2008; Syed 1998; Syed 1999; Toledo‐Bahena 2014; Watanabe 2017). Nine studies included infections caused by yeasts, either alone or in combination with dermatophytes (Alberdi 2019; Bonhert 2019; Eertmans 2018; Elewski 2013c; Elewski 2013d; Iorizzo 2016; Schalka 2012; Sigurgeirsson 2016; Tschen 2013), and three studies included non‐dermatophyte moulds in combination with dermatophytes (Hollmig 2014; NCT01145807; Schalka 2012), two studies included non‐dermatophyte infections alone (Alberdi 2019; Iorizzo 2016), and 11 studies did not clearly specify (ACTRN12614000946617; ACTRN12614001238662; Eertmans 2018EUCTR2008‐003215‐13; EUCTR2016‐001242‐25; Montana 1994; NCT03289871; Nijenhuis‐Rosien 2019; Romero‐Cerecero 2009; Stein 2014; Waibel 2013). Where reported, most participants had more than one toenail affected by onychomycosis, with nine studies reporting an average number of toenails affected of four or more (Baran 2009; Elewski 2013a; Elewski 2013b; EUCTR2006‐000974‐54; Iorizzo 2016; Nijenhuis‐Rosien 2019; Romero‐Cerecero 2009; Sigurgeirsson 2016; Tschen 2013) and four studies reporting an average number of toenails affected of fewer than four (Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b). Two studies used the number of toenails affected as an exclusion criterion: for EUCTR2008‐003215‐13 no more than three affected toenails per person were allowed, and for Lahfa 2013 no more than two toenails were allowed.
Most studies did not report the disease duration of the participants enrolled (ACTRN12614000946617; ACTRN12614001238662; Amichai 2010; Baran 2009; Bonhert 2019; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; EUCTR2008‐003215‐13; EUCTR2016‐001242‐25; Gupta 2006; Hartmane 2013; Hollmig 2014; Ijzerman 2010; Iorizzo 2016; Karsai 2017; Kumar 2001; Lu 2005; Montana 1994; NCT01080079; NCT01145807; NCT01246518; NCT01400594; NCT02022215; NCT02343627; NCT02933879; NCT03141840; NCT03289871; Nijenhuis‐Rosien 2019; Parekh 2017; Paul 2013; Romero‐Cerecero 2009; Stein 2014; Toledo‐Bahena 2014; Tschen 2013; Waibel 2013; Watanabe 2017). In fact, only 13 of 56 studies reported disease duration in some way (Alberdi 2019; Auvinen 2015; Buck 1994; EUCTR2006‐000974‐54; Gupta 2000a; Gupta 2000b; Koren 2018; Lahfa 2013; Romero‐Cerecero 2008; Schalka 2012; Sigurgeirsson 2016; Syed 1998; Syed 1999). Many participants had a disease duration of five years or longer in Auvinen 2015 (75%), EUCTR2006‐000974‐54 (mean seven years), Gupta 2000a and Gupta 2000b (group means ranging from 10.8 to 11.8 years), Koren 2018 (mean 11.7 years), Romero‐Cerecero 2008 (29%), and Sigurgeirsson 2016 (62%), while shorter disease durations of a few months to three years were reported in Buck 1994; Schalka 2012; Syed 1998; and Syed 1999; lastly, Lahfa 2013 reported mean disease durations of 4.1 and 6.3 years, whlie Alberdi 2019 reported a disease duration of three to five years.
Matrix/lunula involvement was specified as excluded in 23 studies (ACTRN12614001238662; Amichai 2010; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; EUCTR2006‐000974‐54; Hartmane 2013; Ijzerman 2010; Iorizzo 2016; NCT01080079; NCT01145807; NCT02343627; NCT02933879; NCT03141840; NCT03289871; Paul 2013; Romero‐Cerecero 2008; Schalka 2012; Sigurgeirsson 2016; Tschen 2013; Watanabe 2017), while 33 studies did not specify whether matrix involvement was included or excluded (ACTRN12614000946617; Alberdi 2019; Auvinen 2015; Baran 2009; Bonhert 2019; Buck 1994; Elewski 2015a; Elewski 2015b; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; EUCTR2008‐003215‐13; EUCTR2016‐001242‐25; Gupta 2000a; Gupta 2000b; Gupta 2006; Hollmig 2014; Karsai 2017; Koren 2018; Kumar 2001; Lahfa 2013; Lu 2005; Montana 1994; NCT01246518; NCT01400594; NCT02022215; Nijenhuis‐Rosien 2019; Parekh 2017; Romero‐Cerecero 2009; Stein 2014; Syed 1998; Syed 1999; Toledo‐Bahena 2014; Waibel 2013).
Forty studies enrolled participants with mild to moderate onychomycosis (ACTRN12614000946617; ACTRN12614001238662; Amichai 2010; Baran 2009; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; EUCTR2008‐003215‐13; EUCTR2016‐001242‐25; Gupta 2000a; Gupta 2000b; Gupta 2006; Hartmane 2013; Ijzerman 2010; Iorizzo 2016; Lahfa 2013; Montana 1994; NCT01080079; NCT01145807; NCT01246518; NCT02022215; NCT02343627; NCT02933879; NCT03141840; NCT03289871; Paul 2013; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Schalka 2012; Sigurgeirsson 2016; Stein 2014; Toledo‐Bahena 2014; Tschen 2013; Watanabe 2017), while 12 studies did not specify severity (Auvinen 2015; Bonhert 2019; Buck 1994; EUCTR2006‐000974‐54; Karsai 2017; Koren 2018; Lu 2005; NCT01400594; Nijenhuis‐Rosien 2019; Syed 1998; Syed 1999; Waibel 2013), one study enrolled severe onychomycosis (Parekh 2017), and three studies did not exclude participants based on disease severity (Alberdi 2019; Hollmig 2014; Kumar 2001).
Interventions
Trials evaluated several topical antifungal treatments including, but not limited to, topical solutions (efinaconazole, luliconazole, tavaborole and terbinafine HCl), lacquers (ciclopirox, amorolfine, ciclopirox 8% hydrolacquer, terbinafine), creams (butenafine hydrochloride, bifonazole), devices (1064‐nm neodymium‐garnet lasers (1064‐nm Nd:YAG)), and a combination thereof.
Classes of drugs
Classes of drugs were included as follows:
13 studies included allylamines (Amichai 2010; Elewski 2013a; Elewski 2013b; EUCTR2016‐001242‐25; Gupta 2006; Hartmane 2013; Lu 2005; NCT01080079; NCT01145807; NCT01246518; NCT01400594; Syed 1998; Syed 1999);
9 studies included azoles (Bonhert 2019; Buck 1994; Elewski 2013c; Elewski 2013d; EUCTR2008‐003215‐13; Lahfa 2013; Stein 2014; Tschen 2013; Watanabe 2017);
3 studies included benzoxaboroles (Elewski 2015a; Elewski 2015b; Toledo‐Bahena 2014);
11 studies included hydroxypyridones (Baran 2009; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; Gupta 2000a; Gupta 2000b; Gupta 2006; Iorizzo 2016; Lu 2005; Paul 2013; Romero‐Cerecero 2008; Schalka 2012); and
8 included morpholine‐derivatives (ACTRN12614000946617; Auvinen 2015; Eertmans 2018; Elewski 2013b; EUCTR2006‐000974‐54; Koren 2018; NCT03289871; Sigurgeirsson 2016).
Comparator arm
11 studies had a placebo arm (ACTRN12614001238662; Kumar 2001; NCT01080079; NCT01400594; NCT02343627; NCT02933879; NCT03141840; Nijenhuis‐Rosien 2019; Parekh 2017; Syed 1998; Syed 1999);
11 studies had a vehicle arm (Elewski 2013a; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2016‐001242‐25; Gupta 2000a; Gupta 2000b; Montana 1994; Stein 2014; Watanabe 2017);
2 studies used no treatment as a control (Hollmig 2014; Karsai 2017); and
22 studies used an active comparator (ACTRN12614000946617; ACTRN12614001238662; Alberdi 2019; Amichai 2010; Auvinen 2015; Bonhert 2019; Buck 1994; Eertmans 2018; Elewski 2013b; EUCTR2008‐003215‐13; EUCTR2016‐001242‐25; Iorizzo 2016; Koren 2018; Lahfa 2013; NCT01246518; NCT03289871; Paul 2013; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Schalka 2012; Sigurgeirsson 2016; Waibel 2013).
Thirteen studies had multiple comparison groups; 11 of these studies had a vehicle/placebo arm and active comparator(s) (Baran 2009; EUCTR2005‐005905‐51; EUCTR2006‐000974‐54; EUCTR2016‐001242‐25; Gupta 2006; Ijzerman 2010; Lu 2005; NCT01145807; NCT02022215; Toledo‐Bahena 2014; Tschen 2013) and the remaining two studies only had active comparators (Hartmane 2013; Waibel 2013).
Intervention arm
3 studies compared efinaconazole 10% solution to vehicle (Elewski 2013c; Elewski 2013d; Tschen 2013);
3 studies compared tavaborole 5% solution to vehicle (Elewski 2015a; Elewski 2015b; Toledo‐Bahena 2014);
2 studies compared ciclopirox 8% hydrolacquer to comparator lacquers such as ciclopirox 8% and amorolfine 5% (Baran 2009; Iorizzo 2016);
2 studies compared ciclopirox 8% lacquer to vehicle (Gupta 2000a; Gupta 2000b);
1 study each evaluated different ciclopirox 8% lacquer regimens (Schalka 2012) and ciclopirox 8% hydrolacquer concentrations (Hartmane 2013); and
2 studies compared luliconazole solution with vehicle (Stein 2014; Watanabe 2017).
Amorolfine lacquer was often used as a comparator, to other topical lacquers such as Abicin 30% nail lacquer (Auvinen 2015), to topical solutions such as terbinafine HCl (Elewski 2013b) and Kunzea oil (ACTRN12614000946617), to photodynamic therapy (PDT) (Koren 2018), and to sequential therapy of urea ointment and ciclopirox (Paul 2013). Other treatments such as mastic paint (ACTRN12614001238662), NVXT solution (NCT02933879), and ABL01 (NCT03141840) were compared to placebo.
Device‐based therapies included three studies comparing 1064‐nm Nd:YAG laser monotherapy to an untreated group (Hollmig 2014; Karsai 2017) or sham control group (Nijenhuis‐Rosien 2019), one study comparing different laser treatments (Waibel 2013), one study drilling holes into nails to facilitate drug delivery (EUCTR2006‐005895‐42), two studies using photodynamic therapy (PDT) (Alberdi 2019; Koren 2018), two studies using iontophoresis (Amichai 2010; NCT01080079), and one study using intense pulsed light (IPL) therapy (Alberdi 2019).
One study investigated amorolfine lacquer while using nail varnish (Sigurgeirsson 2016).
Study duration ranged from 12 weeks to 52 weeks, with most studies 48 to 52 weeks in length.
Frequency
The frequency with which topical treatments were applied varied, with the most common regimen being once daily for 36 to 48 weeks (22 studies: Auvinen 2015; Baran 2009; Bonhert 2019; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2006‐005895‐42; Gupta 2000a; Gupta 2000b; Ijzerman 2010; Iorizzo 2016; Montana 1994; NCT01246518; NCT01400594; NCT02022215; Paul 2013; Stein 2014; Tschen 2013; Watanabe 2017; two additional studies twice daily ACTRN12614000946617; NCT01145807). One study specified application for 48 weeks without frequency (EUCTR2016‐001242‐25). Daily application was common among other treatment durations as 10 studies adopted it (Amichai 2010; EUCTR2008‐003215‐13; NCT02343627; Syed 1999 (three times daily) for four to eight weeks; EUCTR2005‐005905‐51; Gupta 2006; Lahfa 2013; Lu 2005 for three months; Eertmans 2018; Hartmane 2013 for six months). Twice‐daily application for other durations was used in three studies: Buck 1994 for six months; Kumar 2001 for three months; Syed 1998 for seven days. Alternate frequencies of topical application were: four times daily for one month (ACTRN12614001238662), twice daily for three months, then daily for three months (Parekh 2017), weekly for three months (Sigurgeirsson 2016) or six to 12 months (NCT03141840), daily for two weeks, then weekly to six months (EUCTR2006‐000974‐54), daily for three months, then three times a week for three months (Toledo‐Bahena 2014), daily for two eight‐week periods separated by 32 weeks (NCT02933879), and a six‐month application with a first month of three times a week, a second month of twice a week, and the last four months of weekly application (Romero‐Cerecero 2008; Schalka 2012).
Device‐based treatments occurred weekly (Waibel 2013) or every other week (Hollmig 2014; Nijenhuis‐Rosien 2019 (with an additional treatment at week 12)) for three to four weeks, every other week for 16 weeks (Alberdi 2019), weekly every four to six weeks (Karsai 2017), six treatments with one every three weeks (Koren 2018), or twice daily (NCT03289871) for six months, while NCT01080079 and Romero‐Cerecero 2009 did not specify frequency of application.
Co‐interventions
Co‐interventions were infrequent, with six studies using debriding/filing with topical treatments; Baran 2009, Gupta 2000a and Gupta 2000b used filing with ciclopirox 8% lacquer treatment, Elewski 2013a and Elewski 2013b used filing with amorolfine 5% lacquer treatment, and Buck 1994 used debridement with tea tree oil and clotrimazole treatment.
Outcome measures
All studies, with the exception of ACTRN12614000946617, Kumar 2001 and NCT01080079, addressed one or both primary objectives, reporting complete cure rates or adverse events, or both. Eight studies did not address mycological cure rate (EUCTR2005‐005905‐51; EUCTR2006‐000974‐54; NCT01080079; NCT01400594; NCT02022215; Romero‐Cerecero 2009; Stein 2014; Syed 1998). We accepted mycological cure as reported by study investigators.
Twenty‐eight studies defined mycological cure as negative KOH microscopy or PAS and negative culture (ACTRN12614001238662; Alberdi 2019; Auvinen 2015; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2008‐003215‐13; Gupta 2000a; Gupta 2000b; Gupta 2006; Ijzerman 2010; Iorizzo 2016; Karsai 2017; Kumar 2001; Lahfa 2013; Lu 2005; NCT01246518; NCT02343627; NCT02933879; Nijenhuis‐Rosien 2019; Parekh 2017; Paul 2013; Syed 1999; Tschen 2013).
Studies also used less rigorous criteria, with three studies defining mycological cure as negative KOH microscopy alone (Amichai 2010; Romero‐Cerecero 2008; Watanabe 2017), 10 studies as negative culture alone (ACTRN12614000946617; Baran 2009; Buck 1994; Hollmig 2014; Koren 2018; NCT03289871; Schalka 2012; Sigurgeirsson 2016; Toledo‐Bahena 2014; Waibel 2013), three studies reported both microscopy and culture but separately (Bonhert 2019; Hartmane 2013; Montana 1994), two studies used molecular biology techniques (EUCTR2016‐001242‐25; NCT03141840), and two studies left cure undefined (EUCTR2006‐005895‐42; NCT01145807). Seven studies evaluated recurrence (Gupta 2000a; Gupta 2000b; Gupta 2006; Nijenhuis‐Rosien 2019; Syed 1998; Syed 1999; Watanabe 2017), three studies provided pharmaco‐economic information (Auvinen 2015; Buck 1994; Paul 2013), and two studies reported compliance with treatment (Auvinen 2015; Romero‐Cerecero 2008).
No studies reported the impact of treatment on quality of life, but three studies stated that they would measure patient‐reported outcomes; one (Nijenhuis‐Rosien 2019) did not include the outcome in the publication and two have yet to post results (EUCTR2016‐001242‐25; NCT03141840).
The most common assessment time point was 36 to 52 weeks from baseline, which was either immediately after treatment completion or within four‐week follow‐up after treatment completion. For some single studies 12 weeks and six months were also used as time point assessments from baseline, coinciding with treatment completion.
Excluded studies
We excluded 51 records from the review (see Characteristics of excluded studies). Of these, the most common reasons for exclusion were as follows:
non‐randomised studies (18 records: Anonymous 2000; Anonymous 2015; Bergstrom 2009; Botter 1971; Canavan 2018; Dina 2017; Fredriksson 1974; Furtado 2005; Hay 1988; Krasaeath 2016; Meyerson 1992; Morgado 2017; Rand 1996; Shemer 2016; Sotiriou 2010; Souza 2014; Tardivo 2015; Zaug 1995);
combining the results of onychomycosis for toenails and fingernails, which prevented toenail data from being extracted (14 records: Bassiri‐Jahromi 2012; El‐Tatawy 2015; Emtestam 2012; Gilaberte 2017; Halmy 2005; Kim 2016b; Lauharanta 1992; Li 2014; Mahgoub 1975; Many 1964; Menéndez 2011; Tietz 2013; Zhang 2012a; Zhou 2016);
using nails as the unit of analysis rather than participants (six records: Kim 2016a; Landsman 2010; Landsman 2012; Lu 2016; Malay 2009; Reinel 1992);
using a within‐participant design as a control group (three records: Harris 2010; Ortiz 2014; Schaller 2017);
less than 12 weeks in duration (three records: Chan 2005; Jimenez‐Faraj 2018; Mensing 1992);
using an ineligible treatment (three records: Schlockermann 1957 used a combination of surgery and antifungal medication; Gupta 2005 studied a combination of ciclopirox lacquer and oral terbinafine; Oberste‐Lehn 1974 studied oral clotrimazole);
Sigurgeirsson 2010 was an extension trial investigating amorolfine as prophylaxis in patients who achieved cure with oral treatment;
Kamalam 1980 did not study onychomycosis, but rather fungal infections of the skin;
NCT03094468 is a registered trial that has since been withdrawn due to project development priorities changing, and was excluded; and
Abd El‐Aal 2019 included both paediatric and adult participants.
Studies awaiting classification
Twenty‐two records are classified as awaiting classification and are detailed in 'Characteristics of studies awaiting classification' (Anonymous 2002; Bagatell 1977; Barquero 2007; Butareva 1986; Emokpare 1977; EUCTR2008‐002427‐90; George 1991; Grant 1974; JPRN‐JapicCTI‐101143; Klima 1976; Kull 1972; Mathur 1973; NCT00253305; NCT02549001; Park 2017; Ramm 1994; Rüping 1993a; Rüping 1993b; Schubert 1973; Weuta 1972; Xu 2017; Yao 2016). We did not have enough information to assess these studies for inclusion, but they may be added to the review as information becomes available.
Ongoing studies
Thirteen records are ongoing studies from clinical trial registries and are detailed in 'Characteristics of ongoing studies' (ACTRN12618000131257; ChiCTR‐INR‐17013504; DRKS00007709; EUCTR2016‐001204‐39; EUCTR2016‐003784‐19; JapicCTI‐183840; NCT02644551; NCT02812043; NCT02859519; NCT02866032; NCT02961634; NCT03098342; NCT03814343). Any of these records may be added to the review as information becomes available.
Topical investigational products are being compared to vehicle or placebo, including HXP124 (ACTRN12618000131257), RJ‐0265 (ciclopirox formulation) (EUCTR2016‐003784‐19), ME‐1111 (JapicCTI‐183840), CELEXT07 (NCT02644551), terbinafine HCl 10% (NCT02859519), and amphotericin B (NCT03814343). Topical agents are also being compared to comparators: RJ‐0265 versus ciclopirox 8% (EUCTR2016‐003784‐19), ME‐1111 versus efinaconazole (JapicCTI‐183840), terbinafine HCl 10% solution versus ciclopirox 8% (EUCTR2016‐001204‐39; NCT02866032), CELEXT07 versus ciclopirox 8% (NCT02644551), and a combination of Nailner and ciclopirox 8% versus ciclopirox 8% (NCT02961634).
Photodynamic therapy is compared to amorolfine (NCT03098342). Three studies are investigating laser therapy: 1064‐nm Nd:YAG laser (DRKS00007709) and 2940‐nm Er:YAG (ChiCTR‐INR‐17013504), each in combination with amorolfine, versus amorolfine alone, and 1064‐nm laser versus amorolfine versus combination laser plus amorolfine (NCT02812043).
Risk of bias in included studies
Two review authors (KF and RM) independently assessed the included studies for risks of bias using the Cochrane 'Risk of bias' assessment tool as outlined in the Methods. We report assessments in the Characteristics of included studies, and summarise them in Figure 3 and Figure 4. We judged three of the 56 studies to be at low risk across the seven domains (Elewski 2015a; Elewski 2015b; Nijenhuis‐Rosien 2019). We rated seven studies at high risk in one domain but low risk for the other domains (Auvinen 2015; Eertmans 2018; Elewski 2013c; Elewski 2013d; Parekh 2017; Toledo‐Bahena 2014; Tschen 2013), while 11 studies were at low risk on all but two domains (ACTRN12614000946617; Alberdi 2019; Buck 1994; EUCTR2016‐001242‐25; Hollmig 2014; Iorizzo 2016; Karsai 2017; Koren 2018; NCT02933879; NCT03141840; Sigurgeirsson 2016). Selective reporting (reporting bias) was the domain with the largest number of studies judged to be high risk.
3.
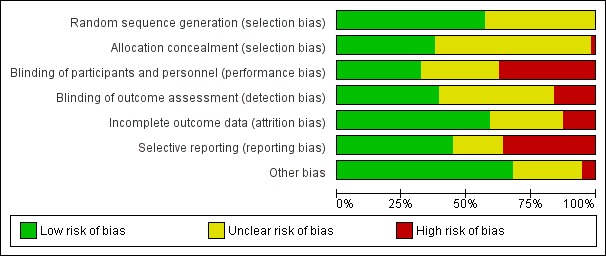
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
4.

Risk of bias summary: review authors' judgements about each 'Risk of bias' item for each included study.
Allocation
Sequence generation
We judged 32 studies to be at low risk of bias for random sequence generation, as the sequence generation method was clearly stated in all of them (ACTRN12614000946617; ACTRN12614001238662; Alberdi 2019; Auvinen 2015; Baran 2009; Buck 1994; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2016‐001242‐25; Hollmig 2014; Iorizzo 2016; Karsai 2017; Koren 2018; Kumar 2001; Lahfa 2013; NCT01246518; NCT02933879; NCT03141840; Nijenhuis‐Rosien 2019; Parekh 2017; Paul 2013; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Sigurgeirsson 2016; Toledo‐Bahena 2014; Tschen 2013; Watanabe 2017). We rated the remaining 24 studies at unclear risk of bias for sequence generation, as there was no information provided.
Allocation concealment
We judged 21 studies to be at low risk for selection bias due to clearly‐stated allocation concealment procedures (ACTRN12614000946617; Alberdi 2019; Auvinen 2015; Buck 1994; Eertmans 2018; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2016‐001242‐25; Hollmig 2014; Iorizzo 2016; Karsai 2017; NCT01246518; NCT02933879; NCT03141840; Nijenhuis‐Rosien 2019; Parekh 2017; Paul 2013; Toledo‐Bahena 2014; Tschen 2013). We rated the remaining 35 studies as unclear due to a lack of information, except for Koren 2018, which we judged as high risk for selection bias, due to investigators being aware of randomisation procedures.
Blinding
Performance bias
We judged 18 studies to be at low risk for performance bias (ACTRN12614000946617; Buck 1994; Elewski 2013a; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; Kumar 2001; NCT02933879; NCT03141840; Nijenhuis‐Rosien 2019; Parekh 2017; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Syed 1998; Syed 1999; Toledo‐Bahena 2014; Tschen 2013). These studies described procedures for ensuring that participants and study personnel were blinded. We rated 21 studies at high risk for performance bias, as these were unblinded or single‐blinded studies (Alberdi 2019; Amichai 2010; Auvinen 2015; Baran 2009; Bonhert 2019; Eertmans 2018; Elewski 2013b; EUCTR2006‐005895‐42; EUCTR2016‐001242‐25; Hartmane 2013; Hollmig 2014; Iorizzo 2016; Karsai 2017; Koren 2018; Lahfa 2013; NCT01246518; NCT03289871; Paul 2013; Schalka 2012; Sigurgeirsson 2016; Waibel 2013). The remaining 17 studies were at unclear risk, due to lack of information.
Detection bias
We judged 22 studies as being at low risk for detection bias, as it was clear in these studies that the individuals evaluating clinical outcomes were blinded to the treatment of participants (ACTRN12614000946617; Auvinen 2015; Baran 2009; Bonhert 2019; Eertmans 2018; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2016‐001242‐25; Hartmane 2013; Iorizzo 2016; Karsai 2017; Koren 2018; Lahfa 2013; NCT02933879; NCT03141840; Nijenhuis‐Rosien 2019; Parekh 2017; Sigurgeirsson 2016; Toledo‐Bahena 2014; Tschen 2013). We assessed nine studies as being at high risk as outcome assessment was not blinded (Alberdi 2019; Amichai 2010; Elewski 2013b; EUCTR2006‐005895‐42; Hollmig 2014; NCT01246518; NCT03289871; Paul 2013; Waibel 2013), with the remaining 25 studies judged as unclear due to a lack of information.
Incomplete outcome data
We judged 33 studies to be at low risk for attrition bias. These studies accounted for all participants and, where there were study withdrawals, reported study discontinuations and reasons for withdrawals for all study arms (Alberdi 2019; Auvinen 2015; Bonhert 2019; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2013c; Elewski 2013d; Elewski 2015a; Elewski 2015b; EUCTR2006‐000974‐54; EUCTR2016‐001242‐25; Gupta 2000a; Gupta 2000b; Hartmane 2013; Hollmig 2014; Iorizzo 2016; Karsai 2017; Koren 2018; Kumar 2001; Nijenhuis‐Rosien 2019; Parekh 2017; Paul 2013; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Schalka 2012; Sigurgeirsson 2016; Syed 1998; Syed 1999; Toledo‐Bahena 2014; Tschen 2013; Waibel 2013; Watanabe 2017). We rated 16 studies at unclear risk as information was unavailable and not stated in the record (ACTRN12614000946617; ACTRN12614001238662; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; Gupta 2006; Ijzerman 2010; NCT01080079; NCT01145807; NCT01246518; NCT01400594; NCT02022215; NCT02343627; NCT02933879; NCT03141840; NCT03289871; Stein 2014). We judged the remaining seven studies to be at high risk due to not stating reasons for participants discontinuing the study (Baran 2009; EUCTR2008‐003215‐13; Lahfa 2013; Lu 2005) or not specifying the treatment group to which participants who were lost to follow‐up belonged (Amichai 2010; Buck 1994; Montana 1994).
Selective reporting
We judged 25 studies to be at low risk of reporting bias (ACTRN12614000946617; Alberdi 2019; Auvinen 2015; Buck 1994; Eertmans 2018; Elewski 2013a; Elewski 2013b; Elewski 2015a; Elewski 2015b; EUCTR2005‐005905‐51; EUCTR2008‐003215‐13; EUCTR2016‐001242‐25; Hollmig 2014; Ijzerman 2010; Koren 2018; Lahfa 2013; NCT02022215; NCT02343627; NCT02933879; NCT03141840; NCT03289871; Nijenhuis‐Rosien 2019; Sigurgeirsson 2016; Stein 2014; Syed 1998). The outcomes reported in these studies were similar to those listed in the studies' respective trial protocols, or where the trial protocol is the included record, clearly defined outcomes were stated, or, where a study pre‐dates clinical trial registries, clearly defined outcomes were stated in the Methods section and reported in the Results. We rated 20 studies at high risk of bias where the outcomes were not clearly defined, or where there were discrepancies between outcomes stated in the trial registries and outcomes reported in publications (ACTRN12614001238662; Bonhert 2019; Elewski 2013c; Elewski 2013d; EUCTR2006‐000974‐54; EUCTR2006‐005895‐42; Hartmane 2013; Iorizzo 2016; Karsai 2017; Montana 1994; NCT01080079; NCT01145807; NCT01246518; NCT01400594; Parekh 2017; Paul 2013; Syed 1999; Toledo‐Bahena 2014; Tschen 2013; Watanabe 2017). We judged the remaining 11 studies to be at unclear risk of bias, as we were unable to locate clinical trial registries to assess risks of bias (Amichai 2010; Baran 2009; Gupta 2000a; Gupta 2000b; Gupta 2006; Kumar 2001; Lu 2005; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Schalka 2012; Waibel 2013).
Other potential sources of bias
We judged 38 studies to be at low risk of other potential sources of bias. We determined this domain to be at high risk in three studies: Elewski 2013a pooled safety data for treatment groups, while Hartmane 2013 and NCT02933879 pooled clinical outcome data across treatment groups. Data per group were therefore not presented. We classified 15 studies as being at unclear risk of bias; these studies did not have results available to be able to assess other sources of bias (ACTRN12614000946617; ACTRN12614001238662; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; EUCTR2016‐001242‐25; Ijzerman 2010; NCT01080079; NCT01145807; NCT01246518; NCT01400594; NCT02022215; NCT02343627; NCT03141840; NCT03289871; Stein 2014).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6
Summary of findings for the main comparison. Ciclopirox 8% lacquer compared to vehicle for fungal infections of the toenails.
| Ciclopirox 8% lacquer compared to Vehicle for fungal infections of the toenails | ||||||
| Patient or population: people with fungal infections of the toenails Setting: outpatient clinics Intervention: ciclopirox 8% lacquer Comparison: vehicle | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with Vehicle | Risk with Ciclopirox 8% lacquer | |||||
| Complete cure: 48 weeks | Study population | RR 9.29 (1.72 to 50.14) | 460 (2 RCTs) | ⊕⊕⊝⊝ Lowa | NNTB = 3 | |
| 4 per 1000 | 41 per 1000 (8 to 219) | |||||
| Adverse events (directly related to treatment, collected over the course of the studies; they are not measured/reported for specific time points) | Study population | RR 1.61 (0.89 to 2.92) | 460 (2 RCTs) | ⊕⊕⊕⊝ Lowb | The most commonly reported adverse events were application site reactions (transient tingling, burning, or pain with treatment use), rashes (mild erythema in the skin surrounding the nail), and alterations in nail colour or shape. These adverse reactions did not require additional treatment. | |
| 70 per 1000 | 112 per 1000 (62 to 204) | |||||
| Mycological cure: 48 weeks | Study population | RR 3.15 (1.93 to 5.12) | 460 (2 RCTs) | ⊕⊕⊕⊝ Moderateb | NNTB = 2 | |
| 96 per 1000 | 303 per 1000 (185 to 492) | |||||
| Clinical cure ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; NNTB: Number needed to treat for an additional beneficial outcome | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by two levels to low‐quality evidence: one level due to imprecision as there are very large and variable confidence intervals across both studies, with low event rates (fewer than 100). Also downgraded by one level due to risk of bias, as most information is from studies at unclear risk of bias. bDowngraded by two levels to low‐quality evidence: one level due to imprecision since the 95% CI includes both a meaningful increase in risk, and no increase in risk, and one level due to risk of bias, as most information is from studies at unclear risk of bias.
Summary of findings 2. Efinaconazole 10% solution compared to vehicle for fungal infections of the toenails.
| Efinaconazole 10% solution compared to vehicle for fungal infections of the toenails | ||||||
| Patient or population: People with fungal infections of the toenails Setting: outpatient clinics Intervention: Efinaconazole 10% solution Comparison: Vehicle | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with Vehicle | Risk with Efinaconazole 10% solution | |||||
| Complete cure: 40 to 52 weeks | Study population | RR 3.54 (2.24 to 5.60) | 1716 (3 RCTs) | ⊕⊕⊕⊕ High | NNTB = 2 | |
| 46 per 1000 | 162 per 1000 (102 to 256) | |||||
| Adverse events (collected over the course of the studies; they are not measured/reported for specific time points) | Study population | RR 1.10 (1.01 to 1.20) | 1701 (3 RCTs) | ⊕⊕⊕⊕ High | ‐ | |
| 600 per 1000 | 660 per 1000 (606 to 720) | |||||
| Mycological cure: 40 to 52 weeks | Study population | RR 2.31 (1.08 to 4.94) | 1716 (3 RCTs) | ⊕⊕⊕⊝ Moderatea | NNTB = 2 We performed a sensitivity analysis omitting Tschen 2013 from the analysis, with this providing high‐quality evidence for mycological cure with efinaconazole treatment |
|
| 196 per 1000 | 454 per 1000 (212 to 970) | |||||
| Clinical cure: 40 to 52 weeks | Study population | RR 3.07 (2.08 to 4.53) | 1655 (2 RCTs) | ⊕⊕⊕⊕ High | ‐ | |
| 63 per 1000 | 192 per 1000 (130 to 283) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; NNTB: Number needed to treat for an additional beneficial outcome | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by one level to moderate‐quality evidence due to inconsistency. Heterogeneity is present, as suggested by a high I2 statistic (95%) and a low P value in the Chi2 test. There is no overlap in the confidence intervals between the Phase 2 study (Tschen 2013) and the Phase 3 studies (Elewski 2013a).
Summary of findings 3. Tavaborole 5% solution compared to vehicle for fungal infections of the toenails.
| Tavaborole 5% solution compared to vehicle for fungal infections of the toenails | ||||||
| Patient or population: People with fungal infections of the toenails Setting: outpatient clinics Intervention: Tavaborole 5% solution Comparison: Vehicle | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) |
Relative effect (95% CI) |
№ of participants (studies) |
Quality of the evidence (GRADE) |
Comments | |
| Risk with vehicle | Risk with tavaborole 5% solution | |||||
| Complete cure: 52 weeks | Study population | RR 7.40 (2.71 to 20.24) | 1198 (2 RCTs) | ⊕⊕⊕⊝ Moderatea | NNTB = 2 | |
| 10 per 1000 | 74 per 1000 (27 to 203) | |||||
| Adverse events (directly related to treatment, collected over the course of the studies; they are not measured/reported for specific time points) |
Study population | RR 3.82 (1.65 to 8.85) | 1186 (2 RCTs) | ⊕⊕⊕⊝ Moderatea | Application‐site reactions were the majority of reported adverse events related to treatment and included exfoliation, dermatitis, erythema, and pain | |
| 15 per 1000 | 58 per 1000 (25 to 134) | |||||
| Mycological cure: 52 weeks | Study population | RR 3.40 (2.34 to 4.93) | 1198 (2 RCTs) | ⊕⊕⊕⊕ High | NNTB = 1 | |
| 98 per 1000 | 332 per 1000 (229 to 482) | |||||
| Clinical Cure ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; NNTB: Number needed to treat for an additional beneficial outcome | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by one level to moderate‐quality evidence due to imprecision. Very large and variable confidence intervals across both studies, with low event rates (fewer than 100).
Summary of findings 4. P‐3051 (ciclopirox 8% hydrolacquer) compared to comparators for fungal infections of the toenails.
| P‐3051 (ciclopirox 8% hydrolacquer) compared to comparatorsa for fungal infections of the toenails | ||||||
| Patient or population: People with fungal infections of the toenails Setting: outpatient clinics Intervention: P‐3051 (ciclopirox 8% hydrolacquer) Comparison: Comparatorsa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with Comparatorsa | Risk with P‐3051 (ciclopirox 8% hydrolacquer) | |||||
| Complete cure: 48 to 52 weeks | Study population | RR 2.43 (1.32 to 4.48) | 490 (2 RCTs) | ⊕⊕⊕⊝ Moderateb | NNTB = 6 | |
| 52 per 1000 | 127 per 1000 (69 to 235) | |||||
| Adverse events (collected over the course of the studies; they are not measured/reported for specific time points) |
Study population | RR 0.60 (0.19 to 1.92) | 487 (2 RCTs) | ⊕⊕⊝⊝ Lowc | The most commonly reported adverse events reported by Baran 2009 included erythema, redness, and burning, while the one participant reporting an adverse reaction in Iorizzo 2016 was unrelated to treatment (foot trauma) | |
| 121 per 1000 | 73 per 1000 (23 to 233) | |||||
| Mycological cure: 48 to 52 weeks | Study population | RR 1.08 (0.85 to 1.37) | 490 (2 RCTs) | ⊕⊕⊕⊝ Moderated | NNTB = 13 | |
| 875 per 1000 | 945 per 1000 (744 to 1000) | |||||
| Clinical cure ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; NNTB: Number needed to treat for an additional beneficial outcome | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aComparators were ciclopirox 8% lacquer (Baran 2009) and amorolfine 5% (Iorizzo 2016). bDowngraded by one level to moderate‐quality evidence due to imprecision, as very low event rates (fewer than 100). cDowngraded by two levels to low‐quality evidence: one level due to inconsistency as there is wide variation in the effect estimates of the two studies. Also downgraded by one level due to imprecision as the confidence interval is large with the upper and lower limits indicating a different effect of the intervention, and event rates are low. dDowngraded by one level to moderate‐quality evidence due to inconsistency, as there is no overlap in confidence intervals and the I2 and Chi2 statistics suggest evidence of high heterogeneity.
Summary of findings 5. 1064‐nm Nd:YAG laser compared to no treatment or sham treatment for fungal infections of the toenails.
| 1064‐nm Nd:YAG laser compared to control for fungal infections of the toenails | ||||||
| Patient or population: People with fungal infections of the toenails Setting: outpatient clinics Intervention: 1064‐nm Nd:YAG laser Comparison: no treatment or sham treatment | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with no treatment | Risk with 1064‐nm Nd:YAG laser | |||||
| Complete cure ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Adverse events (collected over the course of the studies; they are not measured/reported for specific time points) | See comment | See comment | RR 4.85 (0.24 to 97.11) | 85 (2 RCTs) | ⊕⊝⊝⊝ Very lowa | No adverse effects were reported with the intervention in the study, rated at high risk of bias. |
| Mycological cure: 52 weeks | Study population | RR 1.04 (0.59 to 1.85) | 85 (2 RCTs) | ⊕⊕⊝⊝ Lowc | No participants in one of the studies achieved mycological cure. | |
| 302 per 1000 | 314 per 1000 (178 to 559) | |||||
| Clinical cure ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by three levels to very low‐quality evidence: one level due to risk of bias, as one of two studies that reported the outcome did not blind study personnel or participants and was rated at high risk of bias. Downgraded by one level due to inconsistency, as the effect estimate has wide variation with effects in both direction. Finally, downgraded by two levels due to imprecision, as the confidence interval is large, with the upper and lower limits indicating a different effect of the intervention, and contains both the null effect and appreciable harm. The sample size and event rates are low (fewer than 100). bDowngraded by three levels to very low‐quality evidence: one level due to risk of bias, as the one study available for this comparison was not a blinded study and thus had high risk of bias for blinding of participants, personnel, and outcome assessors. Downgraded by one level due to inconsistency, as the effect estimate has wide variation with effects in both directions. Finally, downgraded by two levels due to imprecision as there is only one study available for this comparison, the confidence interval is large with the upper and lower limits indicating a different effect of the intervention, and contains both the null effect and appreciable benefit. The sample size and event rates are low. cDowngraded by two levels to low‐quality evidence: one level due to risk of bias as one of the two studies that reported the outcome did not blind study personnel or participants and was rated at high risk of bias. Also downgraded by one level due to imprecision, as there is a low number of events (fewer than 100) and a very low sample size.
Summary of findings 6. Luliconazole 5% solution compared to vehicle for fungal infections of the toenails.
| Luliconazole 5% solution compared to vehicle for fungal infections of the toenails | ||||||
| Patient or population: People with fungal infections of the toenails Setting: outpatient clinics Intervention: Luliconazole 5% solution Comparison: Vehicle | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with Vehicle | Risk with Luliconazole 5% solution | |||||
| Complete cure: 48 weeks | Study population | RR 2.96 (1.18 to 7.41) | 293 (1 RCT) | ⊕⊝⊝⊝ Very lowa | NNTB = 3 | |
| 51 per 1000 | 149 per 1000 (60 to 374) | |||||
| Adverse events (collected over the course of the studies; they are not measured/reported for specific time points) | Study population | RR 1.02 (0.90 to 1.16) | 293 (1 RCT) | ⊕⊕⊝⊝ Lowb | Commonly‐reported adverse events included dry skin, contact dermatitis, paronychia, eczema, and hyperkeratosis | |
| 768 per 1000 | 783 per 1000 (691 to 891) | |||||
| Mycological cure: 48 weeks | Study population | RR 1.39 (0.98 to 1.97) | 293 (1 RCT) | ⊕⊕⊝⊝ Lowb | NNTB = 6 | |
| 293 per 1000 | 407 per 1000 (287 to 577) | |||||
| Clinical Cure ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; NNTB: Number needed to treat for an additional beneficial outcome | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by three levels to very low‐quality evidence. Downgraded by one level due to risk of bias as blinding of participants, personnel, and outcome assessors is unclear and there is high risk of reporting bias in the one study that is available for this comparison. Also downgraded by a further two levels due to imprecision, as there is only one study available for this comparison, the confidence interval is large, and sample size and event rates are low. bDowngraded by two levels to low‐quality evidence. Downgraded by one level due to risk of bias, as blinding of participants, personnel, and outcome assessors is unclear and there is high risk of reporting bias in the one study that is available for this comparison. Also downgraded by one level due to imprecision, as there is only one study available for this comparison, and sample size and event rates are low.
1. Topical treatment versus vehicle/placebo
Ciclopirox 8% lacquer versus vehicle
Two identical clinical trials (Gupta 2000a; Gupta 2000b) compared ciclopirox 8% lacquer with vehicle lacquer in a total of 460 participants (Table 1). Treatment duration was daily application for 48 weeks, with clinical outcomes also assessed at 48 weeks. There were no discernible differences in the trial populations. Population demographics of the two identical trials were similar, with predominantly male participants (study 1: 78.5%, study 2: 77.2%) and T. rubrum as the most common organism causing infection (study 1: 96.9%, study 2: 95.4%) (Gupta 2000a; Gupta 2000b).
Primary outcomes
Complete cure
See Analysis 1.1
1.1. Analysis.
Comparison 1 Ciclopirox 8% lacquer vs vehicle, Outcome 1 Complete cure: 36 ‐ 52 weeks.
Pooling these two clinical trials yielded 16 participants (16/231 = 6.9%) achieving complete cure with ciclopirox 8% lacquer versus one participant (1/229 = 0.4%) receiving vehicle lacquer (risk ratio (RR) 9.29, 95% confidence interval (CI) 1.72 to 50.14; I2 = 0%; NNTB = 3; low quality of evidence). Ciclopirox 8% lacquer may lead to complete cure for participants compared to those receiving vehicle lacquer.
Adverse events
See Analysis 1.2
1.2. Analysis.
Comparison 1 Ciclopirox 8% lacquer vs vehicle, Outcome 2 Adverse events (directly related to treatment).
There may be an increased risk of participants reporting adverse events deemed by investigators to be due to treatment with ciclopirox 8% lacquer (26/231 = 11.3%) compared with vehicle lacquers (16/229 = 7%) (RR 1.61, 95% CI 0.89 to 2.92; I2 = 0%; low quality of evidence); however, the 95% indicates that ciclopirox lacquer may actually make little or no difference. The most commonly reported adverse events were application site reactions (transient tingling, burning, or pain with treatment use), rashes (mild erythema in the skin surrounding the nail), and alterations in nail colour or shape. These adverse reactions did not require additional treatment.
Secondary outcomes
Mycological cure
See Analysis 1.3
1.3. Analysis.
Comparison 1 Ciclopirox 8% lacquer vs vehicle, Outcome 3 Mycological cure: 36 ‐ 52 weeks.
Thirty‐one per cent of participants (71/231) achieved mycological cure, defined as negative KOH and negative culture, after treatment with ciclopirox 8% lacquer, while 9.6% of participants achieved mycological cure after treatment with vehicle lacquer (22/229). Mycological cure probably increases with ciclopirox 8% lacquer (RR 3.15, 95% CI 1.93 to 5.12; I2 = 16%, NNTB = 2; moderate quality of evidence).
Clinical cure
Clinical cure rate was not a clinical outcome in these studies.
Compliance
These studies did not report compliance.
Time to recurrence
In these two trials (Gupta 2000a; Gupta 2000b), participants who achieved complete cure at 48 weeks with ciclopirox 8% lacquer or vehicle were followed for an additional 12 weeks. Of the 17 participants who were eligible, 10 were treatment failures. We were unable to perform analysis on these data as the treatment assignment of the participants followed was not available.
Quality of life
These studies did not include quality‐of‐life measures.
Pharmaco‐economics
These studies did not include pharmaco‐economic data.
Efinaconazole 10% solution versus vehicle
Two identical Phase 3 clinical trials (Elewski 2013c; Elewski 2013d) and a Phase 2 trial (Tschen 2013), compared efinaconazole 10% solution with vehicle in a total of 1716 participants (Table 2). Treatment duration was daily application for 36 (Tschen 2013) or 48 weeks (Elewski 2013c; Elewski 2013d), with clinical outcomes assessed four weeks after the end of treatment. Tschen 2013 had multiple arms of efinaconazole and we selected for analysis the efinaconazole treatment arm consistent with Phase 3 trials and regulatory approval (10% solution without semi‐occlusion). All arms of the Tschen 2013 trial are presented in Table 9.
Primary outcomes
Complete cure
See Analysis 2.1
2.1. Analysis.
Comparison 2 Efinaconazole 10% solution vs vehicle, Outcome 1 Complete cure: 40 ‐ 52 weeks.
Pooling these studies resulted in 215 participants (215/1278 = 16.8%) receiving efinaconazole 10% solution achieving complete cure and 20 participants (20/438 = 4.6%) receiving vehicle achieving complete cure (RR 3.54, 95% CI 2.24 to 5.60; I2 = 3%; NNTB = 2; high quality of evidence). Efinaconazole 10% solution leads to complete cure when compared to vehicle.
Adverse events
See Analysis 2.2
2.2. Analysis.
Comparison 2 Efinaconazole 10% solution vs vehicle, Outcome 2 Adverse events.
Participants were more likely to experience adverse events with efinaconazole 10% solution compared to vehicle (RR 1.10, 95% CI 1.01 to 1.20; I2 = 0%, NNTH = 15; high quality of evidence). Sixty‐six per cent of participants experienced an adverse event with efinaconazole 10% solution (831/1266 = 65.6%) and 60% of participants experienced an adverse event with vehicle (261/435 = 60%). The most common adverse events reported in the Phase 3 trials (Elewski 2013c; Elewski 2013d) that were likely to be related to treatment were dermatitis (efinaconazole: 23/653 versus vehicle: 0/213, Elewski 2013c) and vesicles (efinaconazole: 21/1227 versus vehicle 0/413, Elewski 2013c; Elewski 2013d) at the application site; most adverse events were probably not related to treatment application and included the common cold or nasopharyngitis (efinaconazole: 141/1227 versus vehicle 40/413), sinusitis (efinaconazole: 47/1227 versus vehicle: 9/413), and upper respiratory tract infection (efinaconazole: 73/1227 versus vehicle: 24/413, Elewski 2013c; Elewski 2013d for all). Four adverse events related to efinaconazole were reported in the Phase 2 trial: one instance of ingrowing toenail in the efinaconazole 10% without semi‐occlusion group (included in analysis) and one instance each of blister, contact dermatitis, and erythema in the efinaconazole 5% solution group (Tschen 2013).
Secondary outcomes
Mycological cure
See Analysis 2.3
2.3. Analysis.
Comparison 2 Efinaconazole 10% solution vs vehicle, Outcome 3 Mycological cure: 40 ‐ 52 weeks.
Fifty‐five per cent of participants (706/1278 = 55.2%) achieved mycological cure, defined as negative KOH and negative culture, after treatment with efinaconazole 10% solution, while 19.6% of participants (86/438) achieved mycological cure after treatment with vehicle. Mycological cure probably increases with efinaconazole 10% solution (RR 2.31, 95% CI 1.08 to 4.94; I2 = 95%; NNTB = 2; moderate quality of evidence). The large heterogeneity in the analysis could be due to the small sample size of Tschen 2013, or to the differences in treatment length and outcome assessment times between the Phase 2 (Tschen 2013) and Phase 3 (Elewski 2013c; Elewski 2013d) studies. In a sensitivity analysis removing Tschen 2013, results indicate that mycological cure increases with efinaconazole 10% solution (RR 3.22, 95% CI 2.59 to 4.01; I2 = 0%, NNTB = 1; high quality of evidence).
Clinical cure
See Analysis 2.4
2.4. Analysis.
Comparison 2 Efinaconazole 10% solution vs vehicle, Outcome 4 Clinical cure: 40 ‐ 52 weeks.
Clinical cure was reported in Elewski 2013c and Elewski 2013d. Clinical cure increases with efinaconazole 10% solution (242/1239 = 19.5%) compared to vehicle (26/416 = 6.3%); RR 3.07, 95% CI 2.08 to 4.53; I2 = 0%, NNTB = 3; high quality of evidence.
Compliance
These studies did not report compliance.
Time to recurrence
These studies did not assess time to recurrence.
Quality of life
These studies did not include quality‐of‐life measures.
Pharmaco‐economics
These studies did not include pharmaco‐economic data.
Tavaborole 5% solution versus vehicle
Two identical Phase 3 trials (Elewski 2015a; Elewski 2015b) compared tavaborole 5% solution versus vehicle in a total of 1198 participants (Table 3). Treatment duration was daily application for 48 weeks, with clinical outcomes assessed at 52 weeks.
Primary outcomes
Complete cure
See Analysis 3.1
3.1. Analysis.
Comparison 3 Tavaborole 5% solution vs vehicle, Outcome 1 Complete cure: 36 ‐ 52 weeks.
Combining these two clinical trials yielded 62 participants (62/799 = 7.8%) achieving complete cure with tavaborole 5% solution versus four participants (4/399 = 1.0%) receiving vehicle (RR 7.40, 95% CI 2.71 to 20.24; I2 = 0%, NNTB = 2; moderate quality of evidence). Treatment with tavaborole 5% solution probably increases complete cure rates compared to vehicle.
Adverse events
See Analysis 3.2; Analysis 3.3
3.2. Analysis.
Comparison 3 Tavaborole 5% solution vs vehicle, Outcome 2 Adverse events.
3.3. Analysis.
Comparison 3 Tavaborole 5% solution vs vehicle, Outcome 3 Adverse events (directly related to treatment).
There was little or no difference between tavaborole 5% solution (482/791 = 60.9%) and vehicle (244/395 = 61.8%) in the number of participants reporting adverse events (RR 0.98, 95% CI 0.85 to 1.13; I2 = 56%; high quality of evidence). The moderate heterogeneity in the analysis may be due to a difference in the number of participants with adverse events in the vehicle groups across the two studies. Any adverse event, whether or not related to treatment, is included in this analysis. More specifically, Elewski 2015a and Elewski 2015b identified adverse events related to treatment and analysis showed that tavaborole 5% solution is probably more likely to lead to participants experiencing treatment‐related adverse events (48/791 = 6.1%) compared to participants receiving vehicle (6/395 = 1.5%; RR 3.82, 95% CI 1.65 to 8.85; I2 = 0%; NNTB = 6; moderate quality of evidence). Most reported adverse events related to treatment were application site reactions, and included exfoliation, dermatitis, erythema, and pain.
Secondary outcomes
Mycological cure
See Analysis 3.4
3.4. Analysis.
Comparison 3 Tavaborole 5% solution vs vehicle, Outcome 4 Mycological cure: 36 ‐ 52 weeks.
One‐third of participants (266/799 = 33.3%) achieved mycological cure, defined as negative KOH and negative culture, after treatment with tavaborole 5% solution, while 9.8% of participants (39/399) achieved mycological cure after treatment with vehicle. Mycological cure increases with tavaborole 5% solution (RR 3.40, 95% CI 2.34 to 4.93; I2 = 26%; NNTB = 1; high quality of evidence).
Clinical cure
Clinical cure rate was not a clinical outcome in these studies.
Compliance
These studies did not report compliance.
Time to recurrence
These studies did not assess time to recurrence.
Quality of life
These studies did not include quality‐of‐life measures.
Pharmaco‐economics
These studies did not include pharmaco‐economic data.
2. Topical treatment versus topical treatment
P‐3051 (ciclopirox 8% hydrolacquer) versus comparators
Two studies (Baran 2009; Iorizzo 2016) reported clinical trials comparing P‐3051 (ciclopirox 8% hydrolacquer) with other treatments in a total of 490 participants (Table 4). Baran 2009 compared P‐3051 to ciclopirox 8% lacquer, with both treatments applied daily for 48 weeks and clinical outcomes assessed at 52 and 60 weeks; this study also compared P‐3051 to placebo but placebo data were not included in the analysis (see Table 9). Iorizzo 2016 compared P‐3051 to amorolfine 5%, applied daily or twice‐weekly for 48 weeks, respectively, with clinical outcomes also assessed at 48 weeks.
Primary outcomes
Complete cure
See Analysis 4.1
4.1. Analysis.
Comparison 4 P‐3051 (ciclopirox 8% hydrolacquer) vs comparators, Outcome 1 Complete cure: 48 ‐ 52 weeks.
Thirty‐one participants (31/242 = 12.8%) achieved complete cure with daily use of P‐3051 (ciclopirox 8% hydrolacquer), while 13 participants (13/248 = 5.2%) achieved complete cure with comparator treatments. P‐3051 (ciclopirox 8% hydrolacquer) will probably lead to complete cure compared to comparator treatments (RR 2.43, 95% CI 1.32 to 4.48; I2 = 0%; NNTB = 6; moderate quality of evidence). A post hoc analysis of Baran 2009 analysed participants with less than 50% nail involvement, whereas the clinical trial enrolled participants with up to 60% nail involvement. At 60 weeks, 18 participants (18/119 = 15.1%) achieved complete cure with P‐3051, while seven participants (7/129 = 5.8%) achieved complete cure with the comparator ciclopirox 8% lacquer (RR 2.79, 95% CI 1.21 to 6.44).
Adverse events
See Analysis 4.2
4.2. Analysis.
Comparison 4 P‐3051 (ciclopirox 8% hydrolacquer) vs comparators, Outcome 2 Adverse events.
The risk of experiencing adverse events was similar for participants who received treatment with P‐3051 (ciclopirox 8% hydrolacquer, 15/240 = 6.3%) or one of the comparators (30/247 = 12.1%; RR 0.60, 95% CI 0.19 to 1.92; I2 = 18%; low quality of evidence). There were no adverse events related directly to P‐3051 (Baran 2009; Iorizzo 2016) or to amorolfine 5% (Iorizzo 2016), but two participants reported adverse events directly related to ciclopirox 8% lacquer (Baran 2009). The most commonly‐reported adverse events reported by Baran 2009 included erythema, redness, and burning, while the one participant reporting an adverse reaction in Iorizzo 2016 was unrelated to treatment (foot trauma). There may be little or no difference in adverse events experienced with ciclopirox 8% hydrolacquer and comparators (amorolfine 5% and ciclopirox 8% lacquer).
Secondary outcomes
Mycological cure
See Analysis 4.3; Analysis 4.4
4.3. Analysis.
Comparison 4 P‐3051 (ciclopirox 8% hydrolacquer) vs comparators, Outcome 3 Mycological cure: 48 ‐ 52 weeks.
4.4. Analysis.
Comparison 4 P‐3051 (ciclopirox 8% hydrolacquer) vs comparators, Outcome 4 Mycological cure (participants with dermatophyte infections): 48 ‐ 52 weeks.
The difference in mycological cure rates between P‐3051 (ciclopirox 8% hydrolacquer) and comparator treatments indicates that there is probably little or no difference between the treatments (RR 1.08, 95% CI 0.85 to 1.37; I2 = 91%; NNTB = 13; moderate quality of evidence). Eighty‐nine per cent of participants who received P‐3051 experienced mycological cure (216/242 = 89.3%), while 87.5% (217/248) of participants who received comparator treatments experienced mycological cure. We did not perform sensitivity analysis on this outcome, as there were only two studies in the analysis. We conducted a sensitivity analysis to investigate the measure of effect in the population of participants who only had dermatophyte infections, as Iorizzo 2016 included participants with dermatophyte, non‐dermatophyte mould, or yeast infections, and Baran 2009 included participants with only dermatophyte infections. As in the full analysis, there is probably little or no difference between the treatments (RR 1.07, 95% CI 0.85 to 1.33; I2 = 88%; moderate quality of evidence). An alternative explanation for the high heterogeneity may be differences in outcome definition. Baran 2009 defined mycological cure as negative culture, while Iorizzo 2016 defined mycological cure as negative KOH and negative culture. As with complete cure, a post hoc analysis of Baran 2009 limited participants to less than 50% nail involvement. At 60 weeks, 98 participants (98/119 = 82.4%) achieved negative culture, while 97 participants (97/129 = 75%) achieved negative culture with the comparator ciclopirox 8% lacquer (RR 1.10, 95% CI 0.96 to 1.25).
Clinical cure
Clinical cure rate was not a clinical outcome in these studies.
Compliance
These studies did not report compliance.
Time to recurrence
These studies did not assess time to recurrence.
Quality of life
These studies did not include quality‐of‐life measures.
Pharmaco‐economics
These studies did not include pharmaco‐economic data.
3. Device versus control
1064‐nm Nd:YAG laser versus no treatment/sham device
Three studies (Hollmig 2014; Karsai 2017; Nijenhuis‐Rosien 2019) reported clinical trials comparing 1064‐nm Nd:YAG laser with no treatment or sham treatment in a total of 112 participants (Table 5). Two sessions (Hollmig 2014) or four sessions (Karsai 2017; Nijenhuis‐Rosien 2019) of treatment with 1064‐nm Nd:YAG were compared to no treatment or sham treatment, with clinical outcomes assessed at 12 (Hollmig 2014) and 52 weeks (Hollmig 2014; Karsai 2017; Nijenhuis‐Rosien 2019).
Primary outcomes
Complete cure
Complete cure rate was not a clinical outcome in these studies.
Adverse events
See Analysis 5.1
5.1. Analysis.
Comparison 5 1064‐nm Nd:YAG laser vs no treatment/sham, Outcome 1 Adverse events.
There was no difference in adverse events (RR 4.85, 95% CI 0.24 to 97.11; Fishers exact test P = 0.24; very low quality of evidence) between laser and sham treatment (Nijenhuis‐Rosien 2019), with Karsai 2017 reporting no adverse events. Due to the very low quality of the evidence, we are uncertain about the adverse events that laser treatment may or may not deliver. During treatment, participants rating pain on a seven‐point visual analogue scale (minimum 1, maximum 7) reported a median score of 5 with treatment (Karsai 2017).
Secondary outcomes
Mycological cure
See Analysis 5.2; Analysis 5.3
5.2. Analysis.
Comparison 5 1064‐nm Nd:YAG laser vs no treatment/sham, Outcome 2 Mycological cure: 12 weeks.
5.3. Analysis.
Comparison 5 1064‐nm Nd:YAG laser vs no treatment/sham, Outcome 3 Mycological cure: 36 ‐ 52 weeks.
Due to the very low quality of the evidence, we are uncertain about the effects laser treatment may or may not have at 12 weeks. There was no difference in mycological cure, defined as negative culture (RR 1.18, 95% CI 0.26 to 5.31; NNTB = 24; Fishers exact test P = 1.0; very low quality of evidence), between laser treatment and no treatment (Hollmig 2014). Twelve months after the end of treatment, there may be little to no difference in mycological cure (RR 1.04, 95% CI 0.59 to 1.85; NNTB = 80; low quality of evidence) between laser treatment and controls (Karsai 2017; Nijenhuis‐Rosien 2019).
Clinical cure
Clinical cure rate was not a clinical outcome in these studies.
Compliance
These studies did not report compliance.
Time to recurrence
These studies did not assess time to recurrence. Nijenhuis‐Rosien 2019 defined recurrence as the same‐species infection occurring at baseline and week 52, with negative biological results at week 30. Three participants in the sham treatment group and six participants in the laser group experienced recurrent infection.
Quality of life
These studies did not include quality‐of‐life measures.
Pharmaco‐economics
These studies did not include pharmaco‐economic data.
Description of studies not included in meta‐analyses
A number of studies met the inclusion criteria for this review, but these were single studies of interventions that we were unable to use in our meta‐analyses. Whenever possible, we have included forest plots of studies published in the last four years (2014 to present) to illustrate the results of studies that may be considered emerging treatments, and to summarise the interventions and outcomes of the remaining studies. 'Summary of findings' tables are provided for interventions that may currently be clinically relevant.
1. Topical treatment versus vehicle
Luliconazole 5% solution versus vehicle
See Analysis 6.1; Analysis 6.2; Analysis 6.3; Table 6
6.1. Analysis.
Comparison 6 Luliconazole 5% solution vs vehicle, Outcome 1 Complete cure: 48 weeks.
6.2. Analysis.
Comparison 6 Luliconazole 5% solution vs vehicle, Outcome 2 Adverse events.
6.3. Analysis.
Comparison 6 Luliconazole 5% solution vs vehicle, Outcome 3 Mycological cure: 48 weeks.
Watanabe 2017 conducted a study comparing luliconazole 5% solution with vehicle solution after 48 weeks of daily application. We are uncertain whether treatment with luliconazole 5% solution leads to complete cure, because we consider the evidence to be of very low quality (RR 2.96, 95% CI 1.18 to 7.41; 293 participants; NNTB = 3). There may be little or no difference in the occurrence of adverse events (RR 1.02, 95% CI 0.90 to 1.16; 293 participants; low quality of evidence) and mycological cure rate (negative KOH microscopy) (RR 1.39, 95% CI 0.98 to 1.97; 293 participants; NNTB = 6; low quality of evidence) between luliconazole 5% solution and vehicle. Commonly‐reported adverse events were dry skin, contact dermatitis, paronychia, eczema, and hyperkeratosis; these improved or resolved immediately after stopping treatment. Participants who achieved complete cure with luliconazole 5% solution (n = 29) or vehicle (n = 5) were followed for an additional four weeks, with no participants experiencing recurrence during this time.
Spirulina bioactive extract versus placebo
See Analysis 7.1
7.1. Analysis.
Comparison 7 Spirulina extract vs placebo, Outcome 1 Mycological cure: 12 ‐ 36 weeks.
A bioactive extract, derived from Arthospira maxima (spirulina) which is a cyanobacterium used as food and marketed as AMYCOT, was compared to placebo (Parekh 2017). Each treatment was applied for a total of 24 weeks; for the first 12 weeks, lotion was applied twice daily and for the last 12 weeks once daily. Mycological cure (negative KOH microscopy and culture) did not differ between the two groups at six months (RR 2.20, 95% CI 0.83 to 5.84; Fishers exact test P = 0.17; 10 participants). No participants reported adverse events in the bioactive extract arm. One participant in the placebo arm reported mild pain in both legs which was unrelated to treatment; as this study also included participants with skin infections, it was not clear if this participant had onychomycosis.
2. Topical treatment versus topical treatment
Spruce resin lacquer versus amorolfine 5% lacquer
See Analysis 8.1; Analysis 8.2; Analysis 8.3
8.1. Analysis.
Comparison 8 Resin lacquer 30% vs amorolfine 5% lacquer, Outcome 1 Mycological cure: 12 ‐ 36 weeks.
8.2. Analysis.
Comparison 8 Resin lacquer 30% vs amorolfine 5% lacquer, Outcome 2 Mycological cure: 36 ‐ 52 weeks.
8.3. Analysis.
Comparison 8 Resin lacquer 30% vs amorolfine 5% lacquer, Outcome 3 Compliance (self‐report).
A resin lacquer, 30% from the purified resin of the Norway spruce tree (Picea abies), was compared to amorolfine 5% lacquer (Auvinen 2015). Each treatment was applied for nine months; resin lacquer 30% was applied once daily and amorolfine 5% lacquer was applied once weekly. Mycological cure (negative KOH microscopy and culture) was not different between the two groups at five months (RR 0.62, 95% CI 0.21 to 1.85; 48 participants) or at 10 months (RR 1.63, 95% CI 0.30 to 8.90; Fishers exact test P = 0.66; 48 participants). No participants in either group achieved clinical cure at 12 to 36 or 36 to 52 weeks. No adverse events were reported for either treatment. There was no difference between treatment groups for self‐reporting compliance, as compliance was close to 100% in both groups (RR 1.04, 95% CI 0.93 to 1.16; 48 participants). The cost of treatment per participant for nine months was reported to be EUR 41.60 for resin lacquer and EUR 56.30 for amorolfine.
Amorolfine 5% lacquer with nail varnish versus amorolfine 5% lacquer with no nail varnish
See Analysis 9.1; Analysis 9.2
9.1. Analysis.
Comparison 9 Amorolfine 5% nail lacquer: nail varnish vs no nail varnish, Outcome 1 Adverse events.
9.2. Analysis.
Comparison 9 Amorolfine 5% nail lacquer: nail varnish vs no nail varnish, Outcome 2 Mycological cure: 12 weeks.
Sigurgeirsson 2016 compared treatment with amorolfine 5% nail lacquer once weekly in the presence of nail varnish (applied 24 hours after treatment) versus no nail varnish once weekly for 12 weeks. After 12 weeks, there was no difference between groups in mycological cure, defined as negative culture (RR 1.00, 95% CI 0.90 to 1.12; 50 participants), and no clear difference in adverse events (RR 2.78, 95% CI 0.12 to 65.08; Fishers exact test P = 1.0; 50 participants).
Acetic acid‐based peelable nail polish versus amorolfine 5% lacquer
See Analysis 10.1
10.1. Analysis.
Comparison 10 Acetic acid‐based peelable nail polish vs amorolfine 5% lacquer, Outcome 1 Mycological cure: 12 ‐ 36 weeks.
An aqueous, acetic acid‐based, peelable nail polish applied once daily for 180 days was compared to amorolfine 5% lacquer applied weekly for 180 days (Eertmans 2018). After 180 days, there was no difference between groups in mycological cure, defined as negative KOH (RR 1.11, 95% CI 0.70 to 1.75; 102 participants). Scores on the nail quality‐of‐life scale decreased by 27.9 units for the peelable nail polish and by 26.7 units for amorolfine 5% lacquer compared to baseline, and did not differ from each other.
3. Device versus device
Photodynamic therapy (PDT) versus Intense pulsed light (IPL)
See Analysis 11.1; Analysis 11.2
11.1. Analysis.
Comparison 11 Photodynamic therapy vs intense pulsed light therapy, Outcome 1 Complete cure: 12 ‐ 36 weeks.
11.2. Analysis.
Comparison 11 Photodynamic therapy vs intense pulsed light therapy, Outcome 2 Mycological cure: 12 ‐ 36 weeks.
Alberdi 2019 compared photodynamic therapy (PDT) mediated by methylene blue (MB) with intense pulsed light (IPL) treatment. All participants were pre‐treated with 40% urea to soften nails followed by up to eight sessions of PDT or IPL spaced every one to two weeks. At week 28, there was no difference between groups in complete cure (RR 0.88, 95% CI 0.57 to 1.34; 46 participants) or mycological cure, defined as negative PAS and negative culture (RR 0.88, 95% CI 0.57 to 1.34; 46 participants).
4. Combination therapy versus combination therapy
Fractional ablative CO2 laser (FACL) + photodynamic therapy (PDT) versus FACL + amorolfine 5% lacquer
See Analysis 12.1; Analysis 12.2
12.1. Analysis.
Comparison 12 Fractional laser and photodynamic therapy vs fractional laser and amorolfine 5% lacquer, Outcome 1 Mycological cure: 12 weeks.
12.2. Analysis.
Comparison 12 Fractional laser and photodynamic therapy vs fractional laser and amorolfine 5% lacquer, Outcome 2 Mycological cure: 36 ‐ 52 weeks.
Fractional ablative CO2 laser (FACL) was applied to toenails prior to treatment with photodynamic therapy (PDT) mediated by 20%‐ALA or amorolfine 5% lacquer (Koren 2018). At 12 and 36 weeks, there was no difference between groups in mycological cure, defined as negative culture (12 weeks: RR 1.31, 95% CI 0.78 to 2.19; 60 participants; 36 weeks: RR 2.00, 95% CI 0.67 to 5.94; 60 participants).
Other single studies
There are 21 studies with reported data to describe (Table 9). Eight studies reported the primary outcome of complete cure (Elewski 2013a; Elewski 2013b; Lahfa 2013; NCT02933879; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Syed 1998; Syed 1999) and 19 studies reported the primary outcome of adverse events (Amichai 2010; Buck 1994; Elewski 2013a; Elewski 2013b; EUCTR2006‐000974‐54; EUCTR2008‐003215‐13; Gupta 2006; Lahfa 2013; Montana 1994; NCT02343627; NCT02933879; Paul 2013; Romero‐Cerecero 2008; Romero‐Cerecero 2009; Schalka 2012; Syed 1998; Syed 1999; Toledo‐Bahena 2014; Waibel 2013). Six studies reported the secondary outcome of clinical cure (Elewski 2013a; Elewski 2013b; Lahfa 2013; NCT02933879; Romero‐Cerecero 2008; Romero‐Cerecero 2009) while 17 studies reported mycological cure (Amichai 2010; Buck 1994; Elewski 2013a; Elewski 2013b; EUCTR2008‐003215‐13; Gupta 2006; Hartmane 2013; Kumar 2001; Lahfa 2013; Montana 1994; NCT02343627; NCT02933879; Paul 2013; Romero‐Cerecero 2008; Schalka 2012; Toledo‐Bahena 2014; Waibel 2013).
The outcomes reported most frequently were adverse events and mycological cure. Adverse events reported were mild to moderate, and resolved with cessation of treatment. Studies most commonly reported application‐site reactions with treatment application, including local irritation/discomfort, erythema (redness), oedema or mild inflammation (swelling), pain or warmth, contact dermatitis, and tinea pedis (Amichai 2010; Buck 1994; Elewski 2013a; Elewski 2013b; EUCTR2006‐000974‐54; EUCTR2008‐003215‐13; Gupta 2006; Lahfa 2013; Montana 1994; NCT02343627; NCT02933879; Paul 2013; Romero‐Cerecero 2008; Syed 1998; Syed 1999; Toledo‐Bahena 2014). There were no adverse events reported with treatment of A.pichinchensis extract (Romero‐Cerecero 2008; Romero‐Cerecero 2009) or ciclopirox 8% lacquer (Schalka 2012), although other studies using ciclopirox 8% lacquer did report application‐site reactions (Gupta 2000a; Gupta 2000b; Romero‐Cerecero 2008). Acute pain was associated with laser use in Waibel 2013, which subsided once treatment was complete.
For mycological cure, studies reported statistical differences between treatment and vehicle or comparator for terbinafine nail solution (Elewski 2013a), and terbinafine 1% patch with iontophoresis (Amichai 2010).
Mycological cure did not differ between active treatment and comparator for:
1064‐nm laser (Waibel 2013);
A. pichinchensis extract versus ciclopirox (Romero‐Cerecero 2008);
ciclopirox 8% lacquer regimens (Schalka 2012);
tea tree oil versus clotrimazole (Buck 1994);
tavaborole 2.5%, 5%, or 7.5% versus vehicle (Toledo‐Bahena 2014);
terbinafine nail solution versus amorolfine 5% (Elewski 2013b);
bifonazole versus placebo (both following urea 40% paste; EUCTR2008‐003215‐13);
40% urea ointment with plastic dressing versus bifonazole‐urea combination (Lahfa 2013); and
sequential treatment (40% urea ointment with plastic dressing, ciclopiroxolamine cream, ciclopirox film‐forming solution) versus amorolfine 5% (Paul 2013).
No statistical analysis of mycological cure rates was provided in Gupta 2006, Hartmane 2013, Kumar 2001, Montana 1994, NCT02343627, or NCT02933879. Of the studies reporting mycological cure, Elewski 2013a, Elewski 2013b, Lahfa 2013, NCT02933879 and Romero‐Cerecero 2008 reported our primary outcome of complete cure. There were no statistical differences between treatments in complete cure rates in any of these studies.
Lastly, there were 16 studies that met our inclusion criteria that did not have published results or did not have extractable data. Four of these studies were published conference abstracts or published studies, investigating a novel compound, NB‐002 (Ijzerman 2010), varying concentrations of terbinafine HCl lacquer (Lu 2005), luliconazole 10% solution (Stein 2014), and efinaconazole 10% solution in combination with 1064‐nm Nd:YAG laser (Bonhert 2019). There was not enough information to extract outcomes from these studies.
The remaining 12 studies are clinical trial registry entries (ACTRN12614000946617; ACTRN12614001238662; EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; EUCTR2016‐001242‐25; NCT01080079; NCT01145807; NCT01246518; NCT01400594; NCT02022215; NCT03141840; NCT03289871) that have been completed; however, results are not posted or published. Four of these clinical trial registry entries are for trials registered in the year 2010 or earlier, with no updates past the year 2012 (EUCTR2005‐005905‐51; EUCTR2006‐005895‐42; NCT01080079; NCT01145807). It is possible that the results of these trials, as well as the conference abstracts which are also old, are negative and will not be published. The remaining eight trial registry entries were recently completed and data may be available at a later date (ACTRN12614000946617; ACTRN12614001238662; EUCTR2016‐001242‐25; NCT01246518; NCT01400594; NCT02022215; NCT03141840; NCT03289871).
Discussion
Summary of main results
We included 56 studies (12,501 participants) in this review, with some publications reporting more than one study (e.g. Elewski 2013a; Elewski 2013b). We included 12 studies published in the year 2000 or later in our meta‐analyses. The remaining 44 studies were single studies investigating various topical and device‐based interventions that prevented further quantitative analysis, or they were clinical trial entries where the studies have been completed but results have not yet been posted. Eighty per cent of the studies assessed topical treatments alone, 9% device treatments, and 11% of the studies investigated both topical and device treatments, but there was a lack of included studies investigating amorolfine lacquer as an intervention of interest and urea creams/paste alone and not in combination treatments. The most common device included was the 1064‐nm Nd:YAG laser. We were unable to include many device‐based studies and even in the case of the 1064‐nm Nd:YAG laser, there were only three included studies of laser monotherapy. Uncertainty in these areas therefore remains, as we cannot comment on the effectiveness of these interventions.
Clinical cure was measured for only one of our key comparisons and quality of life was not reported by any included study.
Ciclopirox 8% lacquer versus vehicle
Two studies in 460 participants (analysed for each of the following outcomes) provided low‐quality evidence indicating that when compared to vehicle, ciclopirox 8% lacquer may be better at producing complete cure and is probably more effective in producing mycological cure. Ciclopirox 8% lacquer may lead to an increase in the number of participants reporting adverse events related to treatment; however, the 95% confidence interval indicates that ciclopirox 8% lacquer may actually make little or no difference (low‐quality evidence). Common adverse events included reactions to treatment application such as tingling or burning, and mild rash. Clinical cure was not measured in these studies. Outcomes were measured after 48 weeks of treatment.
Efinaconazole 10% solution versus vehicle
Two phase 3 studies and one phase 2 study, with a total of 1716 participants, provided high‐quality evidence that efinaconazole 10% solution is more effective in achieving complete cure (1716 participants, 3 studies) and clinical cure (1655 participants, 2 studies) compared to vehicle. Efinaconazole 10% solution also leads to slightly more adverse events directly related to treatment than vehicle (high‐quality evidence) (1701 participants, 3 studies), with application site reactions the most commonly reported events (e.g. dermatitis and vesicles). Mycological cure probably increases with efinaconazole 10% solution (moderate‐quality evidence) (1716 participants, 3 studies). Treatment duration lasted either 36 weeks (one study) or 48 weeks (two studies), with clinical outcomes assessed four weeks after the end of treatment.
Tavaborole 5% solution versus vehicle
Two studies of 1198 participants (analysed for each of the following outcomes) provided high‐quality evidence that when compared with vehicle, tavaborole 5% solution improves mycological cure, and moderate‐quality evidence that it probably increases complete cure. However, it probably leads to more adverse events directly related to treatment than vehicle, with the most common adverse events reported being application‐site reactions such as dermatitis, erythema, exfoliation, and pain (1186 participants, moderate‐quality evidence). Clinical cure was not measured in these studies. Treatment duration was 48 weeks, with clinical outcomes assessed at 52 weeks.
P‐3051 (ciclopirox 8% hydrolacquer) versus comparators
P‐3051 (ciclopirox 8% hydrolacquer) was compared to either ciclopirox 8% lacquer or amorolfine 5% lacquer in two studies evaluating a total of 490 participants. Moderate‐quality evidence suggests that P‐3051 probably increases complete cure compared to comparators, and there is probably little or no difference between the treatments in producing mycological cure.
We found no evidence of a difference in the number of adverse events reported with P‐3051 versus comparators (low‐quality evidence) (487 participants). The most common adverse events reported included erythema, burning, and redness. Clinical cure was not measured in these studies. Treatment duration was 48 weeks, with clinical outcomes assessed at 48 to 52 weeks.
1064‐nm Nd:YAG laser versus no treatment or sham treatment
Three studies compared 1064‐nm Nd:YAG laser to no treatment or sham treatment. Very low‐quality evidence means we are uncertain if there is a difference between groups in the number of participants experiencing adverse events (85 participants). There may be little or no difference in the laser's effect on mycological cure (measured at 52 weeks; 85 participants, low‐quality evidence). Complete cure and clinical cure were not measured in these trials.
Luliconazole 5% solution versus vehicle
Luliconazole 5% solution was investigated in a single study of 293 participants analysed for each of the following outcomes. Because of very low‐quality evidence, we are uncertain of the comparative effect luliconazole 5% solution has on complete cure. There may be little or no difference in adverse events between luliconazole 5% solution and vehicle (low‐quality evidence). There may be increased mycological cure with luliconazole 5% solution, but the 95% confidence interval indicates that luliconazole 5% solution may make little or no difference (low‐quality evidence). Commonly‐reported adverse events were dry skin, contact dermatitis, paronychia, eczema, and hyperkeratosis; these improved or resolved immediately after stopping treatment. This study did not measure clinical cure. Treatment was applied for 48 weeks, with outcomes assessed at the end of treatment.
Overall completeness and applicability of evidence
Major topical interventions for toenail onychomycosis were evaluated with meta‐analyses: ciclopirox 8% lacquer, P‐3051 (ciclopirox 8% hydrolacquer), efinaconazole 10% solution, and tavaborole 5% solution. Included studies for each of these interventions reported our primary outcomes of complete cure and adverse events, as well as the secondary outcome of mycological cure. The most common device therapy, 1064‐nm Nd:YAG laser, was evaluated with meta‐analysis for adverse events and mycological cure. Mycological cure, defined as negative KOH microscopy and negative culture by regulatory authorities, is an informative outcome, indicating that the fungus causing the infection has been eradicated. However, only 28 studies used this definition. We accepted mycological cure as reported by study investigators. Large clinical studies will use this definition of mycological cure; smaller clinical studies will use one technique (e.g. microscopy alone) rather than a combination. An improvement in clinical appearance of the nail without eradication of the fungus may contribute to infection recurrence.
Complete cure is a suitable primary outcome, defined as mycological cure in addition to clearance of all clinical symptoms. Onychomycosis is difficult to treat and it is worth noting that complete cure rates are still low. Not all patients can expect to achieve complete cure with these treatments. We are confident that the results of this review are applicable to the general population afflicted with mild‐to‐moderate toenail onychomycosis caused by dermatophytes. Only one study enrolled severe onychomycosis. Every study in the analyses enrolled some participants with dermatophyte onychomycosis. Applicability of the results to infections caused by non‐dermatophyte moulds or yeasts is uncertain, as only one RCT in our meta‐analyses identified non‐dermatophyte or yeast infections alone (Iorizzo 2016). Of all the included studies, there were nine that included yeasts and five that included non‐dermatophyte moulds, either alone or in combination with dermatophytes. We were unable to evaluate the remaining secondary outcomes of clinical cure, with the exception of the comparison of efinaconazole versus vehicle (studies often use varying definitions, making comparisons difficult); compliance; time to recurrence; quality of life; and pharmaco‐economics. Few studies reported any of these outcomes, and no studies reported quality of life.
The review has externality validity, as it was able to evaluate the primary outcomes for most of the commonly‐used topical and device‐based treatments; however, we were unable to evaluate all of the currently relevant topical and device‐based treatments for toenail onychomycosis. For example, we could not evaluate the evidence for use of urea‐based treatment alone and amorolfine lacquer. These are older treatments where RCTs were, to our knowledge, either not conducted or published. Amorolfine is used as a comparator in our included trials (ACTRN12614000946617; Auvinen 2015; Elewski 2013b; Iorizzo 2016; Koren 2018) but was not evaluated as the drug of interest, whereas urea is used in combination with topical treatments (EUCTR2008‐003215‐13; Lahfa 2013; Paul 2013; Syed 1998). In the case of laser therapy, there are many published studies for onychomycosis; however, only four of these (Hollmig 2014; Karsai 2017; Nijenhuis‐Rosien 2019; Waibel 2013) met the inclusion criteria for this review, and only two could be included in a meta‐analysis due to widely varying methods and outcome measures. Furthermore, we included only two studies of photodynamic therapy (PDT) and no meta‐analysis was possible. There is therefore uncertainty about the effectiveness of device‐based treatments that we could not resolve. Clinicians, researchers and patients are interested in the potential of device‐based therapies, but many questions remain about the effectiveness of lasers and other devices. Other topical treatments that we did not meta‐analyse are not commonly used and require further evidence. These include region‐specific treatments such as spruce resin lacquer, and A. pichinchensis that may be viable alternatives to common treatments (e.g. amorolfine, ciclopirox) in the future. Our results therefore do not sufficiently address the objective of the review: to assess the clinical and mycological effects of topical and device‐based therapies for onychomycosis.
Two limitations that prevented studies of both topical and device‐based treatments from being included in this review deserve mention: we did not include RCTs that evaluated interventions in both toenails and fingernails and that did not present data in a way that allowed extraction of data for toenails alone.
Unit of analysis is also an issue, particularly with device‐based studies. We set out to include studies in the current review that designated one toenail as the nail that was evaluated and usually this was the great (big) toenail; this was the case for studies of topical treatments. We found three laser studies where the number of people achieving cure could be evaluated, although these studies used many toenails per person (if a person was cured, all nails were cured). This allowed for inclusion of laser devices in this review, but we should emphasise that analysing data in this way is not in line with how drug trials are performed, and that this impedes our ability to evaluate devices in the same way as drugs and our ability to compare modalities. Most studies that include many toenails per person in the analysis will report the number of nails achieving cure, rather than the number of people achieving cure. A per‐nail analysis may result in cure rates higher or lower than a per‐person analysis, as people differ in responsiveness to treatment.
It is worth noting that there were 16 studies that met the inclusion criteria for this review but did not have results available. These studies were conference abstracts or clinical trial entries where the studies have been completed. Eight of these studies were last updated within three years; it is possible that data are forthcoming and may be included in a future review. The others have not been updated for some time, and highlight the difficulty in assessing investigative treatments.
Quality of the evidence
The five major comparisons for which meta‐analyses were performed are summarised in 'Summary of findings' tables (Table 1; Table 2; Table 3; Table 4; Table 5). We also include a 'Summary of findings' table for one additional comparison in which there were single studies available and hence no meta‐analyses performed (Table 6). We did this to highlight potential clinically relevant therapies for onychomycosis published in recent years.
Limitations in study design or execution
Most studies included in our meta‐analyses did not raise concerns about methodology, and questions that arose were often addressed through author correspondence. The exceptions were ciclopirox 8% lacquer and 1064‐nm Nd:YAG laser; additional information was not available and we downgraded the evidence by one level due to missing information (unclear risk of bias) and lack of blinding, respectively. We also downgraded the evidence by one level for the single study of luliconazole 5% solution, due to missing information.
Inconsistency of results
For most of the outcomes analysed, results across studies were consistent and did not cause concern. We downgraded evidence for mycological cure with P‐3051 (ciclopirox 8% hydrolacquer) and efinaconazole 10% solution by one level due to inconsistency. In both cases, there was evidence of heterogeneity among studies. Adverse events of P‐3051 and 1064‐nm Nd:YAG laser were also downgraded by one level due to wide variation in the effects observed across studies. Wide variation in the effect observed for mycological cure at 12 weeks in a single study of laser therapy resulted in downgrading evidence by one level.
Indirectness of results
We did not downgrade any studies due to indirectness. Participants in studies were representative of the general patient population. Interventions assessed were similar to what would be observed in clinical practice and were applied by the participants. All studies reported outcomes at appropriate time points.
Imprecision of results
There were few studies in our analyses. Imprecision was due mostly to small sample sizes which lead to a small number of detected events and large confidence intervals. We downgraded evidence by one level for complete cure in the ciclopirox 8% lacquer and tavaborole 5% solution analyses, for adverse events in the P‐3051 and tavaborole 5% solution analyses, for mycological cure in the P‐3051 and 1064‐nm Nd:YAG laser analysis, and by two levels for adverse events in the laser analysis. We also downgraded the single study of luliconazole by one level for adverse events and mycological cure, and by two levels for complete cure.
Publication bias
We did not downgrade evidence for publication bias. The comprehensive literature search is very likely to have limited bias for our comparisons. However, it is possible that older clinical trial registries and conference abstracts produced negative results and were not published. Even if results do not warrant publication in a peer‐reviewed journal, it would be informative if negative results were posted to clinical trial registries.
Potential biases in the review process
An obvious potential source of bias is that the lead author of this review is also the lead author of one included study comparing ciclopirox 8% lacquer to vehicle (Gupta 2000a; Gupta 2000b; Table 1) and an author on additional studies on terbinafine nail lacquer (Elewski 2013a; Elewski 2013b; Gupta 2006) and tavaborole (Elewski 2015a; Elewski 2015b). To prevent this from affecting the review process, other review authors (KF, SV, RM) who have academic research backgrounds and are not clinicians performed the screening and selection of sources to be included in the review, as well as the evaluation of risks of bias and judging evidence quality with GRADE. The lead author (AKG) accepted the judgements of the academic team and participated in all other facets of the review, including clinical and research implications.
We made every attempt to be objective and avoid bias in evaluating the evidence. We conducted an extensive search for eligible studies, and contacted study authors for additional data and methodological details. However, the fact that 22 studies awaiting classification have not yet been incorporated may be a potential source of bias. Additionally, incomplete correspondence with study investigators and sponsors limited our ability to assess risks of bias, particularly of randomisation and allocation concealment. We were unable to obtain results or updates on results for many of the clinical trial registry entries.
Toenails and fingernails have different rates of growth, with fingernails growing faster than toenails. This means that fingernails may respond more favourably to interventions. As fingernail onychomycosis is not as common as toenail onychomycosis, including a few fingernails in a clinical study could inflate the cure rates and misrepresent the efficacy of the intervention. We excluded studies where data were reported for fingernails and toenails combined, and we might therefore have excluded some potentially useful data on toenails. Lastly, after seeing the data, we decided to include forest plots of single studies of treatments published since 2014. We considered that these may be emerging treatments that stakeholders should know about.
At least two authors independently screened and selected studies, extracted data, assessed risks of bias, and graded the quality of the evidence.
Agreements and disagreements with other studies or reviews
When the last Cochrane Review on topical treatments for fungal infections of the toenail was published (Crawford 2007), there was very limited information available and the review also included topical treatments for fungal infection of the skin of the foot. Most of the studies included in the present review were published since 2007, justifying the need for a comprehensive review of toenails alone. Consequently, the information in the present review does not agree or disagree with the previous review, and offers new information to the evidence base. The one exception to this is the use of ciclopirox 8% lacquer for fungal infections of the toenails. Crawford 2007 concluded that ciclopirox 8% lacquer was a poor choice for nail infections as cure rates were low. This is similar to the conclusion of our review, where we have found low‐quality evidence to suggest that ciclopirox 8% lacquer may lead to complete cure compared with vehicle.
In a network meta‐analysis using RCTs of oral and topical onychomycosis treatments, the odds ratios of achieving mycological cure for efinaconazole 10% solution, tavaborole 5% solution, and ciclopirox 8% lacquer were each found to be significantly superior to vehicle (Gupta 2015b). This is consistent with the current review's results as moderate‐quality (ciclopirox 8% lacquer, efinaconazole 10% solution) or high‐quality evidence (tavaborole 5% solution) supports these topical treatments producing mycological cure.
Odds ratios for terbinafine nail solution and amorolfine 5% lacquer were also found to be significantly superior to vehicle (Gupta 2015b). Gupta 2015b included trials with a minimum 48 weeks duration and did not include Paul 2013; since this analysis was published, additional studies using amorolfine have been published (e.g. Auvinen 2015; Koren 2018; Sigurgeirsson 2016). Our review was unable to perform a meta‐analysis for terbinafine nail solution and amorolfine, as studies with overlapping comparisons were lacking (ACTRN12614000946617; Auvinen 2015; Eertmans 2018; EUCTR2006‐000974‐54; Iorizzo 2016; Koren 2018; NCT03289871; Paul 2013; Sigurgeirsson 2016). This highlights the advantages of the network meta‐analysis technique; although the evidence network may be thin, one can be created using a limited number of studies for a comparison. Repeating the analysis of Gupta 2015b while including all treatments would allow the amorolfine studies our review identified to be analysed in a similar network. To our knowledge, there has not been a network meta‐analysis evaluating complete or clinical cure.
Based on low‐quality evidence and very few studies, the results of our review suggest that there is uncertainty about the effectiveness of laser treatment for onychomycosis. A systematic review published in 2014 concluded that the evidence for laser treatment was limited and identified methodological concerns (Bristow 2014), which included small sample sizes, lack of control groups, and variable follow‐up periods. Gupta 2017 reports weighted pooled rates for mycological cure, but the lack of control data and consistently‐defined clinical outcomes precluded further quantitative analysis. We have included only four studies of laser therapy in our review, and the reasons for excluding other laser studies reflected the concerns of the aforementioned reviews, namely, many laser studies are not randomised, do not employ control groups, and/or report data by nail rather than by participant.
Currently, device‐based treatments are not approved for treatment of onychomycosis in the USA (e.g. are not approved to produce complete or mycological cure) but rather, are approved to temporarily increase the amount of clear nail (Lipner 2019; U.S. FDA 2015).
In patients that achieve complete cure, recurrence is a possibility. Although we were unable to report time to recurrence in this review, recurrence is common in toenail onychomycosis. Rates of recurrence following oral antifungal treatment in the published literature range from 10% to 53% (Piraccini 2010; Sigurgeirsson 2002; Tosti 1998), with recurrence more likely to occur within the first two years following cure (Sigurgeirsson 2002). Recurrence following topical or device‐based treatments should be considered a possibility.
Authors' conclusions
Implications for practice.
Some topical treatments for toenail onychomycosis are a viable alternative to traditional oral therapies in mild‐to‐moderate severity of onychomycosis, although it should be noted that we did not compare topical therapies to oral therapies in this review.
In comparison with vehicle, there is high‐quality evidence that efinaconazole 10% solution is more effective in achieving complete cure, low‐quality evidence that ciclopirox 8% lacquer may better lead to complete cure, and moderate‐quality evidence in support of tavaborole 5% solution and P‐3051 (ciclopirox 8% hydrolacquer) probably being more likely to achieve complete cure, although for P‐3051 the comparators are ciclopirox 8% lacquer or amorolfine 5%, rather than vehicle. However, not all patients can be expected to achieve complete cure, since reported cure rates in clinical studies, while better than vehicle, are still low.
Treatment‐related adverse events with efinaconazole (slightly increases adverse events compared with vehicle; high‐quality evidence) and tavaborole (probably increases adverse events compared with vehicle; moderate‐quality evidence) were limited to application‐site reactions, with erythema, rash, and burning reported for P‐3051 and its comparators ciclopirox 8% lacquer or amorolfine 5%, although for this comparison adverse events may not have been directly related to treatment, and we found no evidence of a difference in the risk of adverse events between the groups (low‐quality evidence). For ciclopirox 8% lacquer, application site reactions, rashes, and alterations in nail colour or shape were the most common events, and this intervention may lead to an increase in the number of participants reporting adverse events related to treatment compared with vehicle; however, the 95% confidence interval indicates that ciclopirox 8% lacquer may actually make little or no difference (low‐quality evidence).
In terms of mycological cure, when compared with vehicle, tavaborole 5% solution increases this outcome, and ciclopirox 8% lacquer and efinaconazole 10% probably increase the outcome. For mycological cure, there is probably little or no difference between P‐3051 (ciclopirox 8% hydrolacquer) and its comparators (ciclopirox 8% lacquer or amorolfine 5%).
Studies evaluating ciclopirox 8%, P‐3051, efinaconazole, or tavaborole topical treatments included infections caused by dermatophytes. Infections caused by non‐dermatophyte moulds, yeast, or mixed infections (a combination of dermatophytes and nondermatophyte moulds or yeast) may also benefit from these treatments and their use in everyday practice will be dictated by regulatory restrictions, clinicians' experience, and patient preferences. The study populations were representative of the general population afflicted with mild‐to‐moderate toenail onychomycosis caused by dermatophytes.
There is currently not enough evidence to recommend or discourage the use of luliconazole 5% solution, 1064‐nm Nd:YAG laser, or photodynamic therapy. We included a small number of device‐based studies and could not meet our objective in drawing conclusions on the clinical and mycological effectiveness of device‐based interventions. There were a number of topical interventions about which we could not draw conclusions (Table 9). These include combinations of creams with urea, and treatments specific to geographic areas such as Finland (spruce resin lacquer) and Mexico (A. pichinchensis). We could not evaluate treatments that no published RCTs have assessed, such as amorolfine or urea‐based treatment alone.
Only one of our key comparisons measured clinical cure: efinaconazole 10% is more effective in achieving this outcome when compared with vehicle; high‐quality evidence. Most of the included trials did not measure the secondary outcomes of compliance, time to recurrence, or pharmaco‐economics, with no studies reporting quality of life.
The 22 studies in Studies awaiting classification may alter the conclusions of the review once assessed.
Implications for research.
More randomised controlled studies of device‐based therapies (e.g. 1064‐nm Nd:YAG, photodynamic therapy, iontophoresis) are needed. Unlike drug treatments, there are no generally accepted outcomes that device‐based studies adopt. The US Food and Drug Administration (FDA) has published non‐binding guidance suggesting objective clinical measures that could be used for onychomycosis treatment, including mycological cure, defined as negative microscopy and negative culture (U.S. FDA 2015). Additional clinical outcomes that have been suggested for devices differ from those used for drug treatments; rather than focusing on complete cure, the non‐binding guidance suggests 0% nail involvement (clinical cure) if less than 12 mm of nail is infected prior to treatment (U.S. FDA 2015).
Patient‐centred outcomes are lacking in clinical studies. Further research could be conducted into patient satisfaction with treatment results, improvements in quality of life (e.g. social interactions, confidence), and compliance (e.g. ease and convenience of the intervention). Informal discussion has taken place as to what realistic and useful clinical outcomes may be for onychomycosis studies (Elewski 2016). Complete cure rates for topical treatments, while better than vehicle, are low, and there are no other consistently‐reported clinical outcomes. It may be worth considering attempts in line with Cochrane Skin Core Outcomes Set Initiative to guide studies worldwide (CS‐COUSIN). For both drug‐ and device‐based studies, clinical outcomes should be reported at a patient level, i.e. one target nail for analysis, usually the great (big) toenail.
Research to characterise therapy efficacy in patients with severe onychomycosis is warranted, as well as those with mild‐to‐moderate onychomycosis. Data are absent on the recurrence of onychomycosis following topical and device‐based treatment, and given documented recurrence with oral antifungal therapy, the same should be investigated with topical and device‐based interventions.
Of concern to both patients and physicians is the cost of treatments for onychomycosis. Clinical studies very rarely undertake cost‐effectiveness analysis.
There is also a paucity of studies that perform head‐to‐head comparisons of topical treatments. For example, there are no direct comparisons of amorolfine and ciclopirox with efinaconazole, luliconazole, or tavaborole. Device‐based treatments have not been compared to topical treatments in randomised controlled trials. Direct comparisons of treatments in clinical studies with the inclusion of cost‐effectiveness data will provide valuable information that can aid clinicians and patients in making treatment decisions. Network meta‐analysis may be considered in the future to overcome the lack of direct comparisons in clinical studies. Further research into, for example, region‐specific treatments, such as spruce resin lacquer or A. pichinchensis, or urea‐based treatments, would provide evidence for further onychomycosis treatment options.
Future investigations of topical and device‐based interventions would benefit from characterising outcomes of success according to causative organism. Current studies focus on dermatophyte infections and evidence for treatment success in nondermatophyte and mixed infections would be informative. All future studies, both topical and device‐based, should strive to maintain blinding of at least participants and outcome assessors. Adequate sample size will limit imprecision associated with small numbers of detected events. Heterogeneity among studies may be limited by characterising outcomes according to causative organism and, in the case of mycological cure, adopting the definition of negative KOH microscopy and negative culture.
Regardless of the modality, topical or device, future randomised controlled trials should adhere, and continue to adhere, to the reporting standards laid out in the Consolidated Standards of Reporting Trials (CONSORT) statement (Schulz 2010), to allow a fair and accurate assessment of the evidence for these interventions.
Acknowledgements
The authors wish to acknowledge Dr Jessie L Carviel for creation of Figure 1 and Melissa A MacLeod, MSc, for guidance about referees' comments. Thank you to Professor Erika Ota and Dr Christian Surber for help translating articles. Additionally, thank you to the many individuals who took the time to respond to our inquiries about their studies.
The Cochrane Skin Group editorial base wishes to thank Sue Jessop who was the Cochrane Dermatology Editor; Jeremy Hugh who was the External Content Expert; Laurence Le Cleach who was the Methods Editor for this review; Matthew Grainge who was the Statistical Editor; and the consumer referee, Muhammad Imran Omar. We would also like to thank Kate Cahill for copy‐editing the review.
Appendices
Appendix 1. Cochrane Skin Specialised Register (CRSW) search strategy
onychomycos* or tinea unguium or ((fungal or fungus) near (toenail* or toe* or nail*)) or (ringworm near (toenail* or toe* or nail*))
Appendix 2. CENTRAL (Cochrane Library) search strategy
#1 MeSH descriptor: [Onychomycosis] explode all trees #2 ((fungal or fungus) near (toenail* or toe* or nail*)):ti,ab,kw #3 (ringworm near (toenail* or toe* or nail*)):ti,ab,kw #4 onychomycos*:ti,ab,kw #5 tinea unguium:ti,ab,kw #6 {or #1‐#5}
Appendix 3. MEDLINE (Ovid) search strategy
1. exp Onychomycosis/ 2. ((fungal or fungus) adj4 (toenail$ or toe$ or nail$)).mp. 3. (ringworm adj4 (toenail$ or toe$ or nail$)).mp. 4. Onychomycos$.mp. 5. tinea unguium.mp. 6. or/1‐5 7. randomised controlled trial.pt. 8. controlled clinical trial.pt. 9. randomized.ab. 10. placebo.ab. 11. clinical trials as topic.sh. 12. randomly.ab. 13. trial.ti. 14. 7 or 8 or 9 or 10 or 11 or 12 or 13 15. exp animals/ not humans.sh. 16. 14 not 15 17. 6 and 16
[Lines 7‐16: Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximizing version (2008 revision)]
Appendix 4. Embase (Ovid) search strategy
1. exp onychomycosis/ or exp toenail onychomycosis/ 2. ((fungal or fungus) adj4 (toenail$ or toe$ or nail$)).mp. 3. (ringworm adj4 (toenail$ or toe$ or nail$)).mp. 4. onychomycos$.mp. 5. tinea unguium.mp. 6. or/1‐5 7. crossover procedure.sh. 8. double‐blind procedure.sh. 9. single‐blind procedure.sh. 10. (crossover$ or cross over$).tw. 11. placebo$.tw. 12. (doubl$ adj blind$).tw. 13. allocat$.tw. 14. trial.ti. 15. randomised controlled trial.sh. 16. random$.tw. 17. or/7‐16 18. exp animal/ or exp invertebrate/ or animal experiment/ or animal model/ or animal tissue/ or animal cell/ or nonhuman/ 19. human/ or normal human/ 20. 18 and 19 21. 18 not 20 22. 17 not 21 23. 6 and 22
Appendix 5. LILACS search strategy
onychomycos$ or onicomicosis
We searched using these terms and the Controlled clinical trials topic‐specific query filter.
Data and analyses
Comparison 1. Ciclopirox 8% lacquer vs vehicle.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete cure: 36 ‐ 52 weeks | 2 | 460 | Risk Ratio (M‐H, Random, 95% CI) | 9.29 [1.72, 50.14] |
| 2 Adverse events (directly related to treatment) | 2 | 460 | Risk Ratio (M‐H, Random, 95% CI) | 1.61 [0.89, 2.92] |
| 3 Mycological cure: 36 ‐ 52 weeks | 2 | 460 | Risk Ratio (M‐H, Random, 95% CI) | 3.15 [1.93, 5.12] |
Comparison 2. Efinaconazole 10% solution vs vehicle.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete cure: 40 ‐ 52 weeks | 3 | 1716 | Risk Ratio (M‐H, Random, 95% CI) | 3.54 [2.24, 5.60] |
| 2 Adverse events | 3 | 1701 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [1.01, 1.20] |
| 3 Mycological cure: 40 ‐ 52 weeks | 3 | 1716 | Risk Ratio (M‐H, Random, 95% CI) | 2.31 [1.08, 4.94] |
| 4 Clinical cure: 40 ‐ 52 weeks | 2 | 1655 | Risk Ratio (M‐H, Random, 95% CI) | 3.07 [2.08, 4.53] |
Comparison 3. Tavaborole 5% solution vs vehicle.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete cure: 36 ‐ 52 weeks | 2 | 1198 | Risk Ratio (M‐H, Random, 95% CI) | 7.40 [2.71, 20.24] |
| 2 Adverse events | 2 | 1186 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.85, 1.13] |
| 3 Adverse events (directly related to treatment) | 2 | 1186 | Risk Ratio (M‐H, Random, 95% CI) | 3.82 [1.65, 8.85] |
| 4 Mycological cure: 36 ‐ 52 weeks | 2 | 1198 | Risk Ratio (M‐H, Random, 95% CI) | 3.40 [2.34, 4.93] |
Comparison 4. P‐3051 (ciclopirox 8% hydrolacquer) vs comparators.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete cure: 48 ‐ 52 weeks | 2 | 490 | Risk Ratio (M‐H, Random, 95% CI) | 2.43 [1.32, 4.48] |
| 2 Adverse events | 2 | 487 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.19, 1.92] |
| 3 Mycological cure: 48 ‐ 52 weeks | 2 | 490 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.85, 1.37] |
| 4 Mycological cure (participants with dermatophyte infections): 48 ‐ 52 weeks | 2 | 460 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.85, 1.33] |
Comparison 5. 1064‐nm Nd:YAG laser vs no treatment/sham.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Adverse events | 2 | 85 | Risk Ratio (M‐H, Random, 95% CI) | 4.85 [0.24, 97.11] |
| 2 Mycological cure: 12 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Mycological cure: 36 ‐ 52 weeks | 2 | 85 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.59, 1.85] |
Comparison 6. Luliconazole 5% solution vs vehicle.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete cure: 48 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Mycological cure: 48 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 7. Spirulina extract vs placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mycological cure: 12 ‐ 36 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 8. Resin lacquer 30% vs amorolfine 5% lacquer.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mycological cure: 12 ‐ 36 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Mycological cure: 36 ‐ 52 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Compliance (self‐report) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 9. Amorolfine 5% nail lacquer: nail varnish vs no nail varnish.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Mycological cure: 12 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 10. Acetic acid‐based peelable nail polish vs amorolfine 5% lacquer.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mycological cure: 12 ‐ 36 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 11. Photodynamic therapy vs intense pulsed light therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete cure: 12 ‐ 36 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Mycological cure: 12 ‐ 36 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 12. Fractional laser and photodynamic therapy vs fractional laser and amorolfine 5% lacquer.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mycological cure: 12 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Mycological cure: 36 ‐ 52 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
ACTRN12614000946617.
| Methods | RCT (parallel) Study design: Single blind Sample size calculation: No Diagnosis mycology: Mycological culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: Weeks 40 ± 2 Time points of measurements: Weeks 40 ± 2 Location: Royal Hobart Hospital, Tasmania, Australia |
|
| Participants | Total n: 93 Age: ≥ 18 years old Sex: Men and women (ratio unknown) Inclusion criteria: Entry criteria required a clinical diagnosis of onychomycosis (based on clinical manifestations and positive mycology (mycological culture) involving ≤ 20% of the area of one of the great toenails and a minimum age of 18 Exclusion criteria: The main exclusion criteria were other nail conditions (psoriasis, bacterial infections, contact dermatitis, nail bed tumours, yellow nail syndrome, traumatic onychodystrophies, lichen planus, pachonychia congenita and idiopathic onycholysis) confounding onychomycosis assessment, pregnancy, breast‐feeding, and a known history of allergy to essential oils. All participants had a 6‐week washout period for systemic antifungal therapy and 4 weeks for topical antifungal treatment prior to receiving the study design Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown Participant enrolment: August 2007 to January 2009 |
|
| Interventions | Treatment duration: Kunzea oil twice daily (morning and evening) or nail lacquer once a week for 40 ± 2 weeks Drug in study arm 1: Neat Kunzea oil (100% steam distilled, produced from the Kunzea ambigua plant), n = unknown Drug in study arm 2: Loceryl nail lacquer (containing 5% amorolfine), n = unknown |
|
| Outcomes | Mycological cure (negative culture) at weeks 40 ± 2 Clinical severity score graded on a visual analogue scale at weeks 40 ± 2 Change in amount of clear nail (digital photographs) and diseases nail (tracings) at weeks 40 ± 2 Adverse events: not reported |
|
| Notes | The study was government‐funded and affiliated with a university. Trial completed, no results posted. Email response: Manuscript is currently under review |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "participants were randomly allocated into one of two groups (test or control) using a computer‐generated randomisation schedule" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "randomisation was provided by the study sponsor, using an independent statistician" "code was kept secure by a staff member (University of Tasmania) who was not part of the research team." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Test formulations were prepared in the compounding pharmaceutical laboratory...University of Tasmania, under the supervision of a registered pharmacist...study medications were packed in identical containers...university staff to send the medications (via express registered post) directly to the patients...enabled the clinical investigator (performing assessments) and other study personnel to be blinded." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "university staff to send the medications (via express registered post) directly to the patients...enabled the clinical investigator (performing assessments) and other study personnel to be blinded." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register are defined |
| Other bias | Unclear risk | Comment: Multiple treatment arm study; however, there are no results to assess |
ACTRN12614001238662.
| Methods | RCT (parallel) Study design: Unknown Sample size calculation: Unknown Diagnosis mycology: Unknown Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: At 4 months Time points of measurement: Months 1 and 4 Location: College of Dentistry/Hawler Medical University, Erbil, Kurdistann, Iraq |
|
| Participants | Total n: 75 Age: 18 ‐ 75 years old Sex: Men and women (ratio unknown) Inclusion criteria: 18 to 75 years of age inclusive, diagnosed with onycholysis, onychomycosis or onychorrhexis of the nail, at least one target which has: 25% ‐ 75% involvement of the area of the nail unit (including destroying or missing parts of the nail plate), at least 2 mm of uninvolved nail growth as measured from the proximal nail fold to the most proximal point to the disease process and with no lunular involvement, nail unit hyperkeratosis at the most distal edge which measures no greater than 3 mm Exclusion criteria: Any significant disease of the hepatic, renal, endocrine (including diabetes mellitus), immune systems, or other health conditions which could interfere with or confound the results of study assessments, pre‐existing chronic foot pain, neurologic deficit or skin disease / injury in treated foot. In the case of female subjects, are pregnant, nursing or planning to become pregnant within the study period. History of clinically significant abnormal laboratory values, including liver function test results equal to or greater than twice the upper limit of normal. Disease‐like psoriatic toenails, significant toenail abnormalities/dystrophies, toenail injuries or any other condition in the toenail, which could interfere with study evaluations Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown Participant enrolment: April 2014 ‐ July 2014 |
|
| Interventions | Treatment duration: Applied 4 times daily for 1 month Drug in study arm 1: Mastic paint (0.1 ml/site), n = unknown Drug in study arm 2: Topically‐applied glycerin (0.1 ml/site), n = unknown |
|
| Outcomes | Mycological cure (KOH and culture) at months 1 and 4 Clinical cure at months 1 and 4 Complete cure at months 1 and 4 Adverse events: not reported |
|
| Notes | The study is not funded by industry or affiliated with a university Email response: Manuscript is currently in preparation for publication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "table created by computer" Comment: Method of randomisation likely appropriate |
| Allocation concealment (selection bias) | Unclear risk | Quote: "by numbered containers" Comment: Not enough information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Selective reporting (reporting bias) | High risk | Comment: Clinical outcomes are not defined. Mycological cure is defined |
| Other bias | Unclear risk | Comment: Multiple treatment arm study; however, there are no results to assess |
Alberdi 2019.
| Methods | RCT (parallel) Study design: Open Sample size calculation: No Diagnosis mycology: PAS and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: 12 weeks Time points of measurements: Weeks 16 and 28 Location: Hospital Clinico San Carlos, Madrid, Spain |
|
| Participants | Total n: 46 Age: Mean ± SD: Photodynamic therapy (PDT) 64.4 ± 17.3; Intense pulsed light (IPL) 64.1 ± 11.4 Sex: PDT: 4 men and 16 women, 3 not stated, lost to follow‐up; IPL: 9 men and 11 women, 3 not stated, lost to follow‐up Inclusion criteria: People with any severity of onychomycosis in the first toe, with mycological diagnosis of positive PAS and positive culture. Patients with prior treatment with oral or topical antifungal agents that was unsuccessful, and/or presence of comorbidity and/or poly‐medication that could generate risk when combined with systemic antifungal agents, negative to undergo antifungal treatment were enrolled Exclusion criteria: Under 18 years of age, contraindications for the use of methylene blue, any diseases causing nail abnormalities and would interfere with evaluation, pregnancy, lactation, use of systemic antifungals within 4 ‐ 24 weeks prior to enrolment Disease duration: 3 ‐ 5 years Comparable at baseline: Unknown Causative species: Dermatophytes, non‐dermatophyte moulds, and yeast: Trichophyton species n = 15, T. rubrum n = 13, T. mentagrophytes n = 6, Candida species n = 2, Candida parapsilosis n = 2, Candida famata n = 1, Aspergillus fumigatus n = 2, Rhodotula n = 1, Microsporum n = 2, Fusarium n = 1, Microsporum + Epidermophyton n = 1 Number of people lost to follow‐up: PDT n = 3; IPL n = 3; all 6 participants decided the study was too time‐consuming Trial duration: unknown |
|
| Interventions | Treatment duration: once every 1 ‐ 2 weeks for 8 treatments, approximately 16 weeks; pre‐treatment with 40% urea for 1 ‐ 7 days Intervention in study arm 1: Methylene blue mediated photodynamic therapy, n = 23 Intervention in study arm 2: Intense pulsed light laser therapy, n = 23 |
|
| Outcomes | Clinical improvement measured with Onychomycosis Severity Index (OSI) at weeks 16 and 28 Mycological response (negative PAS and negative culture) at weeks 16 and 28 Complete cure (negative PAS and culture, and 100% growth of healthy nail) at weeks 16 and 28 Adverse events: reported |
|
| Notes | This study was funded by government grants The authors have no conflicting affiliations or financial conflicts to declare |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomly allocated into two different treatment groups by means of a computer‐generated random list" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: "Patients were randomly allocated by a software program that generates a random list. This software was used by a nurse of the private clinic. Operator and investigator did not intervene in this process." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Email response: "Participants and operator were not blinded." Comment: The treatments (photodynamic therapy and intense pulse light) are very different and it is very likely that participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Email response: "the nail treated by methylene blue remained blue during the experiment." Comment: It was likely that outcome assessors were aware of treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Email response: Study was not registered in a clinical trial register Comment: Although not registered, the outcomes specified in Method are reported in Results |
| Other bias | Low risk | Comment: Not a multiple intervention trial, outcomes reported for interventions |
Amichai 2010.
| Methods | RCT (parallel) Study design: Not blinded Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 8 and 12 weeks Time points of measurements: Weeks 2, 4, 8 and 12 Location: Israel (city/institution not stated) |
|
| Participants | Total n = 38 Age: (range): At least 18 (20 ‐ 60) years Sex: men 22/38 (58%), women 16/38 (42%) Inclusion criteria: Otherwise healthy people, aged at least 18 years, with distal and lateral subungual onychomycosis that involved 25% – 75% of the big toenail, caused by dermatophyte Exclusion criteria: People with matrix involvement, dermatophytoma or yellow streaks were excluded Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow‐up: Protocol violations n = 2; follow‐up n = 1; treatment groups unknown Trial duration: unknown |
|
| Interventions | Treatment duration: Treatment period was overnight wear (6 ‐ 8 hours), every day, 5 days a week, for 4 weeks Drug in study arm 1: 1% terbinafine HCl and an iontophoretic patch (current density of 100 uA /cm2), n = 20 Drug in study arm 2: 1% terbinafine HCl patch without iontophoresis, n = 18 |
|
| Outcomes | Clinical improvement of the target nail (outgrowth of at least 1.5 mm of new clinically‐unaffected nail plate) at weeks 2, 4, 8, 12 Mycological cure (negative direct microscopy) at weeks 2, 4, 8, 12 Mycological improvement (reduced number of fungal elements in nail specimen and decreased rate of fungal culture growth during and after treatment) of the target nail at weeks 2, 4, 8, 12 Adverse events: reported |
|
| Notes | One of 4 authors is an employee of industry, while author is affiliated with industry (relationship not specified) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients enrolled in the study were divided randomly into two groups" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: No information was available. Study appears to be an open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: No information was available. Study appears to be an open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "Two patients did not finish the study due to protocol violations." Comment: No information on treatment group of protocol violations. Data indicate that 1 additional participant was lost to follow‐up; treatment unknown |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Auvinen 2015.
| Methods | RCT (parallel) Study design: Single blind (investigator blind) Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: No (however, results indicate the big toenail was evaluated) Statistical comparison for outcomes: Yes Duration of follow‐up: At 4 and 10 months Time points of measurements: Weeks 20 and 42 (in‐person), participants contacted by phone during weeks 6, 13 and 29 Location: Helsinki University Hospital, Helsinki, Finland |
|
| Participants | Total n: 73 Age: Mean ± SD (range): resin lacquer: 64 ± 10 (41 ‐ 87), amorolfine: 63 ± 11 (43 ‐ 87), terbinafine: 64 ± 9 (38 ‐ 77) Sex: Resin lacquer: men 21/23 (91%), women 2/23 (9%), amorolfine: men 20/25 (80%), women 5/25 (20%), terbinafine: men 17/25 (68%), women 8/25 (32%) Inclusion criteria: Positive dermatophyte culture and a positive KOH stain Exclusion criteria: Negative dermatophyte culture or KOH stain; onychomycosis caused by yeasts or nondermatophyte moulds; liver failure, determined by plasma c‐glutamyl transferase levels > 120 U L 1 (2 9 upper limit of normal range); kidney failure, determined by plasma creatinine levels > 100 lmol L 1 (upper limit of normal range); a known hypersensitivity to resin, amorolfine or terbinafine; potential adverse cross‐reactions between resin, amorolfine or terbinafine and any concurrently‐taken medication; and any prior topical or oral antifungal treatment administered, for any reason, in the year before the beginning of the study Disease duration: Resin lacquer: 1 ‐ 3 years, 3 participants; 3 ‐ 5 years, 1 participant; 5 ‐ 10 years, 6 participants; 10 years, 13 participants Amorolfine: 1 ‐ 3 years, 4 participants; 3 ‐ 5 years, 3 participants; 5 ‐ 10 years, 3 participants; 10 years, 15 participants Terbinafine: 1 ‐ 3 years, 4 participants; 3 ‐ 5 years, 3 participants; 5 ‐ 10 years, 5 participants; 10 years, 13 participants Comparable at baseline: Yes Causative species: Resin lacquer: T. rubrum n = 20 (87%), T. mentagrophytes n = 3 (13%). Amorolfine: T. rubrum n = 24 (96%), T. mentagrophytes n = 1 (4%). Terbinafine: T. rubrum n = 21 (84%), T. mentagrophytes n = 4 (16%) Number of people lost to follow‐up: Terbinafine: adverse events n = 2, participant‐based refusal n = 1. Amorolfine: subjectively assessed lack of efficacy n = 1 Participant enrolment: Began October 2013, end date not stated, treatment started January 2014 |
|
| Interventions | Drug in study arm 1: topical resin lacquer (Abicin 30% nail lacquer), once daily for 9 months, n = 23 Drug in study arm 2: 5% amorolfine hydrochloride, once weekly for 9 months, n = 25 Drug in study arm 3: oral terbinafine (250 mg), daily for 3 months, n = 25 |
|
| Outcomes | Mycological cure (negative KOH staining and negative culture) at 4 and 10 months Clinical cure (normal appearance of the nail) at 4 and 10 months Participant compliance (self‐reporting throughout study) Cost effectiveness (average treatment cost per participant based on retail price) Adverse events: reported |
|
| Notes | 2 authors of 6 are shareholders in the company developing the investigational product. This company also provided funding for the study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was in permuted blocks of six with an allocation ratio of 1:1:1" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "Treatment was concealed from the investigators; therefore, a research coordinator allocated patients to the three arms according to the randomisation list, and delivered the treatments to the patients." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: Participants were not blinded, potentially influencing results |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "This was an investigator‐blinded study...The final analysis and assessment of the treatment outcome was carried out in a blinded manner, without the investigators knowing to which treatment arm the patient belonged at any given time." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes specified in Methods were reported. Outcomes specified in trial protocol were all reported. NCT0185150 |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Baran 2009.
| Methods | RCT (parallel) Study design: 2 arms (P‐3051 and placebo) were double‐blinded, while the third arm (market reference: ciclopirox) was open label Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 12 weeks Time points of measurements: Weeks 48, 52, and 60 Location: Italy (sites, n = 6), Germany (n = 2), France (n = 2), Poland (n = 4), Latvia (n = 1), Czech Republic (n = 8) |
|
| Participants | Total n: 467 randomised participants, 466 participants with associated data (1 participant in the P‐3051 group does not have associated data, explanation not stated) Age: Mean ± SD: placebo 49.5 ± 12.43, P‐3051 49.47 ± 12.44, reference 50.38 ± 11.09, all participants 49.84 ± 11.89 Sex: Placebo: men 26/97 (26.8%), women 71/97 (73.2%); P‐3051: men 75/181 (41.4%), women 106/181 (58.6%); reference: men 70/188 (37.2%), women 118/188 (62.8%). All participants: men 36.7%, women 63.3%. Inclusion criteria: Patients with distal subungual, mild‐to‐moderate onychomycosis of at least 1 big toenail (target nail) entered the trial. The target nail for efficacy analysis was chosen between the 2 big toenails, as the most affected within the eligibility criteria. According to the protocol, participants had an infected area ≥ 25% and ≤ 60% of target nail. Only people with dermatophyte infection, confirmed by both KOH microscopy and culture, were randomised to treatment. Exclusion criteria: People with nail psoriasis, who were positive for yeasts or non‐dermatophyte moulds on the nail specimen, and/or who were immunosuppressed were excluded. Local treatment of mycotic infections, with localisation other than in the nails, was allowed Disease duration: Unknown Comparable at baseline: The 3 groups were similar with respect to sex, age, weight, number of affected toenails, and in causative pathogen Causative species: Any dermatophyte: n = 466 (100%). T. mentagrophytes: placebo n = 97 (39.2%), P‐3051 n = 181 (36.8%), ciclopirox n = 188 (37.8%), all participants n = 466 (37.7%). T. rubrum: placebo n = 97 (52.6%), P‐3051 n = 181 (54.4%), ciclopirox n = 188 (50.5%), all participants (n = 466) (52.5%). T. spp: placebo n = 97 (5.1%), P‐3051 n = 181 (5.5%), ciclopirox n = 188 (6.9%), all participants n = 466 (6.0%). E floccosum: placebo n = 97 (1.0%), P‐3051 n = 181 (1.6%), ciclopirox n = 188 (2.7%), all participants n = 466 (2.1%). Other dermatophytes: placebo n = 97 (2.1%), P‐3051 n = 181 (1.7%), ciclopirox n = 188 (2.1%), all participants n = 466 (1.9%) Number of people lost to follow‐up: P‐3051 n = 25; reference n = 32; placebo n = 22 Trial duration: unknown |
|
| Interventions | Treatment duration: daily for 48 weeks Drug in study arm 1: P‐3051 (ciclopirox 80 mg/g, water, ethanol, hydroxypropyl chitosan, cetyl stearyl alcohol, ethyl acetate), n = 182 Drug in study arm 2: Ciclopirox 80 mg/g (ethyl acetate, isopropyl alcohol, butyl monoester of poly[methyl vinyl ether/maleic acid] in isopropyl alcohol) (Market reference), n = 188 Drug in study arm 3: Placebo (matching vehicle of P‐3051, water, ethanol, hydroxypropyl chitosan, cetyl stearyl alcohol, ethyl acetate), n = 97 |
|
| Outcomes | Mycological cure (negative culture) at weeks 48 and 60 Complete cure (negative KOH and culture, and 100% growth of healthy nail) at weeks 48 and 60 Responder (negative KOH and culture, and decrease of diseased nail area to ≤ 10% (including zero) of total) Growth rate of healthy nail every 12 weeks Adverse events: reported |
|
| Notes | Quote: "The clinical study was 100% supported by [industry]" and the sponsor "is the holder of all rights related to the study." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "uneven random allocation of treatments by blocks of 5 (2:2:1) was performed" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Placebo was the matching vehicle of P‐3051; thus, the treatment was double‐blind between the two arms P‐3051 and placebo; the third arm (market reference) was open label, both because the appearance of the reference product and the treatment procedure were different [from the other 2 groups]". Comment: Adequate participant blinding for 2 of 3 treatment groups. Knowledge of the open arm introduces bias |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The final evaluation of the primary and secondary clinical endpoints was centrally made in blind by the International Study Coordinator, who acted as blinded evaluator." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: Based on reported cure rates, participants discontinued the study. Reasons for discontinuation are not reported |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Bonhert 2019.
| Methods | RCT (parallel) Study design: Open (evaluating investigator blinded) Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 4 weeks Time points of measurements: Weeks 48, 52 Location: United States of America (city/institution not stated) |
|
| Participants | Total n: 30 Age: Mean 51 (range 29 ‐ 69) Sex: unknown (authors state men = 18, women = 13) Inclusion criteria: Patients 18 ‐ 70 years of age with a clinical diagnosis of DLSO affecting at least 1 great toenail. Toenail had to be uninfected length of 3 mm or more from the proximal nail fold and 3 mm or less in thickness. Diagnosis confirmed with positive KOH microscopy and positive culture of dermatophytes or mixed dermatophyte/Candida ≤ 42 days before baseline. Contraception and negative pregnancy test for women required Exclusion criteria: Use of laser/light‐based fungal therapy within 3 months, or topical antifungal therapy applied to the foot or nails within 1 month of study entry. HIV‐positive, infection, tinea pedis, immunosuppression and liver toxicity, non‐dermatophyte infection, and intolerance to efinaconazole were also excluded Disease duration: Unknown Comparable at baseline: Clinical index of onychomycosis was similar between the 2 groups Causative species: Dermatophytes or mixed dermatophyte/Candida Number of people lost to follow‐up: None Trial duration: unknown |
|
| Interventions | Treatment duration: daily for 48 weeks, laser treatment every 4 weeks for 6 treatments at the beginning of the study in conjunction with daily topical use Drug in study arm 1: Efinaconazole 10% solution, n = 15 Intervention in study arm 2: Efinaconazole 10% solution and 1064 nm Nd:YAG laser, n = 15 |
|
| Outcomes | Complete cure (negative KOH and culture, and 0% nail involvement with no onycholysis and subungual hyperkeratosis) at week 52 Effective treatment (negative KOH and culture, and ≤ 10% nail involvement) at week 52 KOH and fungal cultures at weeks 48 and 52 Adverse events: reported Participant satisfaction |
|
| Notes | The study was funded by industry. There is no conflict of interest statement for authors. Author affiliations are academic in nature | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: The differences in treatment application (topical vs laser + topical) indicates that participants and personnel were probably not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "evaluating investigator blinded"; "efficacy assessments will be performed on the target nail for each subject by the same blinded evaluating investigator" Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All 30 patients enrolled completed the study and adhered to the protocol." Comment: All participants were accounted for. |
| Selective reporting (reporting bias) | High risk | Comment: Outcomes stated in Methods are not reported in the Results (complete cure, adverse events) |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but outcomes are reported for all interventions |
Buck 1994.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Yes Diagnosis mycology: Culture Big toenail specified: No Statistical comparisons for outcomes: Yes Duration of follow‐up: At 3 months Time points of measurements: Months 1, 3 (with phone calls), 6 Location: United States of America (city/institution not stated) |
|
| Participants | Total n: 117 Age: Average: clotrimazole 59 years, tea tree oil 61 years. Sex: Clotrimazole: men 15/53 (28%), women 38/53 (72%). Tea tree oil: men 15/64 (23%), women 49/64 (77%) Inclusion criteria: All patients presenting to 1 of 3 sites between June 1991 and December 1991 with distal subungual toe onychomycosis proven by culture were enrolled Exclusion criteria: Use of immune‐suppressant therapy within the previous 6 months, had used a topical agent on the toenails in the previous 2 weeks, had a history of psoriasis, or had known HIV infection Disease duration: Nail disease for more than 1 year: clotrimazole 49/53 (92%), tea tree oil 59/64 (92%) Comparable at baseline: Yes. Causative species: Clotrimazole: T. rubrum n = 41 (77%), T. mentagrophytes n = 10 (19%). Tea Tree Oil: T. rubrum n = 53 (83%), T. mentagrophytes n = 8 (13%). Number of people lost to follow‐up: Moved or their telephone had been disconnected: clotrimazole n = 4; tea tree oil n = 1; 4 additional participants discontinued due to adverse events, treatment allocation unknown Participant enrolment: June 1991 ‐ December 1991 |
|
| Interventions | Treatment duration: Twice daily for 6 months Drug in study arm 1: 100% Melaleuca alternifolia (Tea Tree) Oil, n = 64 Drug in study arm 2: 1% clotrimazole solution, n = 53 |
|
| Outcomes | Mycological cure (culture) at 6 months Clinical assessment (recorded as full, partial, or no resolution of nail appearance) at 1, 3, and 6 months Participant assessment by phone call at 3‐month follow‐up ("Were symptoms and nail appearance resolved, improved, stayed the same, or worsened?") Adverse events: reported |
|
| Notes | Industry provided technical and financial support | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The treatment groups were randomised by the pharmacy by means of a computerized random‐number generator." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Comment: Randomisation was performed by the pharmacy, who then prepared and distributed identical treatments to investigators |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "...pharmacy filled 60‐cc standardized bottles with solutions...that appeared identical...the type of medication was blinded to both patient and provider" Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method. Unclear if provider and investigator are the same individuals |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: Participants lost to follow‐up identified by treatment; but participants lost due to adverse events not specified by treatment |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes specified in Methods reported in Results. Study pre‐dates trial registry in the USA |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Eertmans 2018.
| Methods | RCT (parallel) Study design: Open (evaluator‐blinded) Sample size calculation: Yes Diagnosis mycology: KOH Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: None Time points of measurements: Days 0, 30, 60, 120, 180 Location: Military Hospital of Tunis, Université Tunis El Manar, Tunis, Tunisia |
|
| Participants | Total n: 102 Age: 18+ years of age Sex: men 25/50 (50%) test product, 25/49 (51%) reference; women 25/50 (50%) test product, 24/49 (49%) reference. 2 and 1 participants were lost to follow up in the test product and reference groups, respectively. Inclusion criteria: Ability to operate medical device, 18 years of age and older with superficial onychomycosis on at least 1 great toenail or light to moderate disto‐lateral onychomycosis without matrix involvement, confirmed with KOH staining, no systemic antifungal within 6 months of study and no topical antifungal within 3 months of study, use of contraception since at least 12 weeks before study until 1 month after the study. Exclusion criteria: Enrolment in another clinical trial, pregnant, nursing, or women planning to become pregnant, allergy to product constituents, serious or progressive disease such as diabetes, peripheral circulatory disease, HIV, psoriasis, lichen planus, immunosuppression, other cutaneous disease on the nails Disease duration: Unknown Comparable at baseline: Yes Causative species: Dermatophytes, non‐dermatophyte moulds, and yeast; test product: 34/50 positive culture, 94.3% dermatophytes; reference product: 25/49 positive culture, 88.6% dermatophytes Number of people lost to follow‐up: test product n = 2, reference product n = 1 Trial duration: October 26, 2016 (first patient, first visit) ‐ August 26, 2017 (last patient, last visit) |
|
| Interventions | Drug in study arm 1: Test product, an aqueous, acetic acid‐based, peelable nail polish, once a day for 180 days, n = 52 Drug in study arm 2: Reference product, amorolfine 5% nail lacquer, once a week for 180 days, n = 50 |
|
| Outcomes | Percentage of healthy nail as assessed using digital photography versus baseline at days 30, 60, 120, 180 Clinical efficacy assessed on a 5‐point scale for onycholysis, nail dystrophy, nail discolouration, nail thickening at days 30, 60, 120, 180 Negative KOH at day 0, 180 Evaluation of product tolerance at days 30, 60, 120, 180 Quality of life using NailQoL questionnaire at days 60, 180 Subjective evaluation with participant questionnaire at days 30, 60, 120, 180 Adverse events: tolerance to product and quality of life assessed |
|
| Notes | Industry‐funded. 2 of 4 authors are employees of the industry who funded the study. 1 author is the clinical investigator of the study and 1 author has no conflicts to declare | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Prior to the study, a randomisation list was calculated by an external statistician using SAS software (version 9.4). For this purpose, block randomisation with a block size of two was used." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: "The [randomisation list] was generated by the CRO who performed the clinical trial." Comment: Allocation concealment appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Discernible differences in the product properties (e.g. different bottle, odour) and in the administration process allowed patients to recognize both trial products." Email response: Unblinded clinical staff member who was not involved in diagnosis or follow‐up provided product to participants Comment: Participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "For each photograph, a blinded dermatologist traced the healthy surface. Next, a second evaluator, also blinded, determined the percentage of healthy surface" Email response: Assessors of mycology were blinded. Clinical evaluators were not involved with providing product to participants Comment: A blinded evaluator was used for efficacy outcomes but safety was recorded by unblinded investigators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in trial protocol are explicit. The same outcomes are specified and reported in the publication. NCT03382717 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Elewski 2013a.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 4 and 28 weeks Time points of measurements: Week 52 Location: unknown |
|
| Participants | Total n: 1044 Age: Mean ± SD 24‐week treatment: terbinafine nail solution (TNS) 53.7 ± 12.86 years; Vehicle 52.7 ± 12.51 years; 48‐week treatment: terbinafine nail solution (TNS) 54.0 ± 11.78 years; Vehicle 53.9 ± 12.09 years Sex: 24‐week treatment: TNS: male 200/259 (77.2%), female 59/259 (22.8%). Vehicle: male 190/258 (73.6%), female 68/258 (26.4%); 48‐week treatment: TNS: male 204/271 (75.3%), female 67/271 (24.7%). Vehicle: male 194/256 (75.8%), female 62/256 (24.2%) Inclusion criteria: aged 12 – 75 years with mild‐to‐moderate toe onychomycosis of the great toenail due to dermatophytes. Mild‐to‐moderate toe onychomycosis was defined as a toenail involvement of ≥ 25% to ≤ 75% without spikes and without matrix (lunula) involvement, and nail infection was confirmed by positive KOH microscopy and culture of a dermatophyte Exclusion criteria: nail abnormalities, obscuring appearance of infection‐free normal nail (including traumatic or onychogryphotic nail) or in whom the target toenail had < 2 mm unaffected nail plate length beyond the proximal fold, severe plantar tinea pedis requiring systemic therapy, mixed infections (dermatophyte and non‐dermatophyte), dermatophytoma (thick masses of fungal hyphae between the nail plate and nail bed), systemic or topical anti‐fungal therapy within 6 months or 3 months, respectively, and those who used any commercial topical nail medication within 1 month. People with severe diabetic foot neuropathy, malignancy, and sensitivity to the study medication Disease duration: Unknown Comparable at baseline: Unknown Causative species: 24‐week treatment: TNS: T. rubrum n = 252 (97.3%), T. mentagrophytes n = 5 (1.9%), Other n = 1 (0.4%); Vehicle: n = 237 (91.9%), T. mentagrophytes n = 18 (7.0%), Other n = 2 (0.8%). 48‐week treatment: TNS: T. rubrum n = 255 (94.1%), T. mentagrophytes n = 14 (5.2%); Vehicle: T. rubrum n = 240 (93.8%), T. mentagrophytes n = 14 (5.5%), Other 1/256 (0.4%) Number of people lost to follow‐up: 24‐week treatment, TNS (45 discontinued): adverse events (n = 1), unsatisfactory therapeutic effect (n = 5), protocol deviation (n = 3), consent withdrawn (n = 17), loss to follow‐up (n = 19). Vehicle (45 discontinued): adverse events (n = 1), serious adverse events (n = 1), unsatisfactory therapeutic effect (n = 5), protocol deviation (n = 2), consent withdrawn (n = 17), loss to follow‐up (n=18), death (n = 1). 48‐week treatment, TNS (48 discontinued): adverse events (n = 1), serious adverse events (n = 1), unsatisfactory therapeutic effect (n = 4), protocol deviation (n = 3), consent withdrawal (n = 18), loss to follow‐up (n = 20), death (n = 1). Vehicle (35 discontinued): adverse events (n = 1), unsatisfactory therapeutic effect (n = 2), protocol deviation (n = 1), consent withdrawn (n = 15), loss to follow up (n = 15), other (n = 1) Trial duration: unknown |
|
| Interventions | Drug in study arm 1: Topical terbinafine HCl Nail Solution (TNS) once daily for 24 weeks, n = 259 Drug in study arm 2: Vehicle once daily for 24 weeks, n = 258 Drug in study arm 3: Topical terbinafine HCl Nail Solution (TNS) once daily for 48 weeks, n = 271 Drug in study arm 4: Vehicle once daily for 48 weeks, n = 256 |
|
| Outcomes | Complete cure (no residual clinical involvement and negative KOH and culture) at week 52 Mycologoical cure (negative KOH microscopy and culture) at week 52 Clinical effectiveness (≤ 10% residual involvement of the nail, negative KOH and culture) at week 52 Clinical cure (no residual clinical involvement) at week 52 Adverse events: reported |
|
| Notes | 7 of 16 authors are employees of industry, 5 additional authors have ties to industry (e.g., consultant, investigator) and 4 authors have no conflicts of interest. The study was financially supported by an unrestricted grant from industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Subjects were randomised using a validated automated system in equal ratios." Comment: Specific randomisation method that is suitable was specified. |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Terbinafine nail solution or vehicle were supplied in identical packaging." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in trial protocol are explicit. The same outcomes are specified and reported verbatim in the publication. Clinical cure was added to the publication as an outcome. NCT00443820 and NCT00443898 |
| Other bias | High risk | Quote: "The 24 week and 48 week treatment groups were pooled for data collected up to week 28." Comment: Safety outcomes for individual treatment groups not reported separately |
Elewski 2013b.
| Methods | RCT (parallel) Study design: Open‐label, active‐controlled Sample size calculation: Yes Diagnosis mycology: KOH microscopy and culture of a dermatophyte Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: 4 weeks Time points of measurements: Week 52 Location: unknown |
|
| Participants | Total n: 1029 Age: Mean ± SD: terbinafine nail solution (TNS) 52.8 ± 12.15 years; amorolfine 52.6 ± 12.97 years Sex: TNS: men 349/507 (68.8%), women 158/507 (31.2%). Amorolfine: male 372/522 (71.3%), women 150/522 (28.7%) Inclusion criteria: aged 12 – 75 years with mild‐to‐moderate toe onychomycosis of the great toenail due to dermatophytes. Mild‐to‐moderate toe onychomycosis was defined as a toenail involvement of ≥ 25% to ≤ 75% without spikes and without matrix (lunula) involvement, and nail infection was confirmed by positive KOH microscopy and culture of a dermatophyte Exclusion criteria: nail abnormalities, obscuring appearance of infection‐free normal nail (including traumatic or onychogryphotic nail) or in whom the target toenail had < 2 mm unaffected nail plate length beyond the proximal fold, severe plantar tinea pedis requiring systemic therapy, mixed infections (dermatophyte and non‐dermatophyte), dermatophytoma (thick masses of fungal hyphae between the nail plate and nail bed), systemic or topical anti‐fungal therapy within 6 months or 3 months, respectively, and those who used any commercial topical nail medication within 1 month. People with severe diabetic foot neuropathy, malignancy, and sensitivity to the study medication Disease duration: Unknown Comparable at baseline: Unknown Causative species: TNS: T. rubrum 484/507 (95.5%), T. mentagrophytes 17/507 (3.4%), Other 6/507 (1.2%). Amorolfine: T. rubrum 488/522 (93.5%), T. mentagrophytes 25/522 (4.8%), Other 9/522 (1.7%) Number of people lost to follow‐up: TNS (66 discontinued): adverse events (n = 1), unsatisfactory therapeutic effect (n = 10), protocol deviation (n = 4), consent withdrawal (n = 20), loss to follow‐up (n = 27), others (n = 3), missing (n = 1). Vehicle (76 discontinued): adverse events (n = 6), unsatisfactory therapeutic effect (n = 11), protocol deviation (n = 3), consent withdrawal (n = 26), loss to follow‐up (n = 30) Trial duration: unknown |
|
| Interventions | Drug in study arm 1: Topical terbinafine HCl Nail Solution (TNS) once daily for 48 weeks, n = 507 Drug in study arm 2: amorolfine 5% nail lacquer, twice weekly with nail filing per package insert for 48 weeks, n = 522 |
|
| Outcomes | Complete cure (no residual clinical involvement and negative KOH and culture) at week 52 Mycologoical cure (negative KOH microscopy and culture) at week 52 Clinical effectiveness (≤ 10% residual involvement of the nail, negative KOH and culture) at week 52 Clinical cure (no residual clinical involvement) at week 52 Adverse events: reported |
|
| Notes | 7 of 16 authors are employees of industry, 5 additional authors have ties to industry (e.g. consultant, investigator) and 4 authors have no conflicts of interest. The study was financially supported by an unrestricted grant from industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Subjects were randomised using a validated automated system in equal ratios." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: Participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: Participants and personnel were not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in trial protocol are explicit. The same outcomes are specified and reported verbatim in the publication. Clinical cure was added to the publication as an outcome. NCT00459537 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Elewski 2013c.
| Methods |
Study 1 RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparison for outcomes: Yes Duration of follow‐up: At 4 weeks Time points of measurements: Weeks 12, 24, 36, 48, 52 Locations: United States (sites, n = 34), Canada (n = 7), Japan (n = 33) (cities/institutions not stated) |
|
| Participants | Total n: 870 Age: Mean (range): efinaconazole 52.4 years (20.0 ‐ 71.0), vehicle 51.9 years (18.0 ‐ 70.0) Sex: Efinaconazole: men 489/656 (74.5%), women 167/656 (25.5%). Vehicle: men 158/214 (73.8%), women 56/214 (26.2%). Total: men 647/870 (74.4%), women 223/870 (25.6%) Inclusion criteria: 18 to 70 years of age, clinical diagnosis of DLSO affecting at least 1 great toenail, target toenail uninfected length 3 mm or more (from the proximal nailfold), thickness 3 mm or less, evidence of toenail growth, positive KOH microscopy result, and culture of dermatophyte or mixed dermatophyte/Candida ≤ 42 days before baseline. Women of childbearing age were required to use birth control Exclusion criteria: History of immunosuppression and/or clinical signs indicative of possible immunosuppression, known HIV infection, uncontrolled diabetes mellitus, presence of toenail infection other than dermatophytes, severe moccasin tinea pedis at screening/baseline, any disease/condition that might have caused toenail abnormalities or interfered with the evaluation, and previous target toenail surgery. Patients were not excluded for concomitant drugs that inhibit cytochrome P450 3A4 Disease duration: Unknown Comparable at baseline: Yes Causative species: Dermatophtyes or mixed dermatophyte/Candida Number of people lost to follow‐up: Efinaconazole: adverse events (n = 21), participant request (n = 31), lost to follow‐up (n = 20), other (n = 9) Vehicle: adverse events (n = 1), participants request (n = 12), protocol violation (n = 1), lost to follow‐up (n = 11), other (n = 2) Trial duration: unknown |
|
| Interventions | Treatment duration: Self‐applied once daily for 48 weeks Drug in study arm 1: Efinaconazole 10% solution, n = 656 Drug in study arm 2: Vehicle, n = 214 |
|
| Outcomes | Complete cure (0% clinical involvement of target toenail and mycologic cure (negative KOH and negative culture)) at week 52 Mycological cure (negative KOH and negative culture) at week 52 Treatment success (< 10% clinical involvement of target toenail) at week 52 Complete or almost complete cure (≤ 5% clinical involvement and mycologic cure) Unaffected toenail growth (from baseline) at week 52 Change in number of affected non‐target toenails assessed throughout study Change in quality of life assessed throughout study Adverse events: reported |
|
| Notes | 6 of 11 authors are employees of industry, while the remaining 5 have ties to industry (e.g. advisor, consultant, investigator) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomisation number determined by a computer‐generated randomisation schedule" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "Study drugs were provided in a kit containing identical masked bottles with a randomisation number...Access to the randomisation schedule was permitted after both the database was locked and the study unblinded." Comment: Allocation concealment appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Investigators, sponsor, investigational centre staff, clinical monitors, patients, and all other study personnel were unaware of study drug assignments to individual patients...If the treatment code was broken, the patient was discontinued." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Investigators... were unaware of study drug assignments to individual patients...If the treatment code was broken, the patient was discontinued...A study investigator assessed the outcomes at each visit." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Primary outcomes different between trial protocol (clinical cure) and publication (complete cure); outcomes that do appear in trial protocol are reported in publication. Secondary outcome not defined and vague in trial protocol (clinical efficacy). Multiple outcomes added to publication that are not found in trial protocol. NCT01007708 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Elewski 2013d.
| Methods |
Study 2 RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparison for outcomes: Yes Duration of follow‐up: At 4 weeks Time points of measurements: Weeks 12, 24, 36, 48, 52 Locations: United States (sites, n = 36), Canada (n = 8) (cities/institutions not stated) |
|
| Participants | Total n: 785 Age; 18 to 70 years of age. Mean (range): Efinaconazole 50.6 years (18.0 ‐ 71.0) , Vehicle 50.7 years (18.0 ‐ 70.0) Sex: Efinaconazole: men 464 (80.0%), women 116 (20.0%). Vehicle: male 164 (81.6%), women 37 (18.4%). Total: male 628 (80.4%), women 153 (19.6%) Inclusion criteria: 18 to 70 years of age, clinical diagnosis of DLSO affecting at least 1 great toenail, target toenail uninfected length 3 mm or more (from the proximal nailfold), thickness 3 mm or less, evidence of toenail growth, positive KOH microscopy result, and culture of dermatophyte or mixed dermatophyte/Candida ≤ 42 days before baseline. Women of childbearing age were required to use birth control Exclusion criteria: History of immunosuppression and/or clinical signs indicative of possible immunosuppression, known HIV infection, uncontrolled diabetes mellitus, presence of toenail infection other than dermatophytes, severe moccasin tinea pedis at screening/baseline, any disease/condition that might have caused toenail abnormalities or interfered with the evaluation, and previous target toenail surgery. Patients were not excluded for concomitant drugs that inhibit cytochrome P450 3A4 Disease duration: Unknown Comparable at baseline: Yes Causative species: Dermatophtyes or mixed dermatophyte/Candida Number of people lost to follow‐up: Efinaconazole: adverse events (n = 11), participant request (n = 36), protocol violation (n = 3), lost to follow‐up (n = 29), worsening condition (n = 1), other (n = 5). Vehicle: participant request (n = 19), protocol violation (n = 3), lost to follow‐up (n = 18), pregnancy (n = 1), other (n = 1) Trial duration: unknown |
|
| Interventions | Treatment duration: Self‐applied once daily for 48 weeks Drug in study arm 1: Efinaconazole 10% solution, n = 583 Drug in study arm 2: Vehicle, n = 202 |
|
| Outcomes | Complete cure (0% clinical involvement of target toenail and mycologic cure (negative KOH and negative culture)) at week 52 Mycological cure (negative KOH and negative culture) at week 52 Treatment success (< 10% clinical involvement of target toenail) at week 52 Complete or almost complete cure (≤ 5% clinical involvement and mycologic cure) Unaffected toenail growth (from baseline) at week 52 Change in number of affected non‐target toenails assessed throughout study Change in quality of life assessed throughout study Adverse events: reported |
|
| Notes | 6 of 11 authors are employees of industry, while the remaining 5 have ties to industry (e.g. advisor, consultant, investigator) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomisation number determined by a computer‐generated randomisation schedule" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "Study drugs were provided in a kit containing identical masked bottles with a randomisation number...Access to the randomisation schedule was permitted after both the database was locked and the study unblinded." Comment: Allocation concealment appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Investigators, sponsor, investigational centre staff, clinical monitors, patients, and all other study personnel were unaware of study drug assignments to individual patients...If the treatment code was broken, the patient was discontinued." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Investigators...were unaware of study drug assignments to individual patients...If the treatment code was broken, the patient was discontinued...A study investigator assessed the outcomes at each visit." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Primary outcomes different between trial protocol (clinical cure) and publication (complete cure); outcomes that do appear in trial protocol are reported in publication. Secondary outcome not defined and vague in trial protocol (clinical efficacy). Multiple outcomes added to publication that are not found in trial protocol. NCT01008033 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Elewski 2015a.
| Methods |
Study 1 RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 4 weeks and 12 weeks Time points of measurements: Weeks 2, 6, and every 6 weeks thereafter; at week 48, participants who achieved complete cure or treatment success were followed until week 60 (post‐study follow‐up (PSFU)) Location: United States and Mexico, 27 individual sites (cities/institutions not stated) |
|
| Participants | Total n: 594 Age: Mean ± SD: tavaborole 53.6 ± 12.5, vehicle 53.4 ± 12.3 Sex: Tavaborole: men 324/399 (81.2%); women 75/399 (18.8%); Vehicle: men 158/194 (81.4%); women 36/194 (18.6%) Inclusion criteria: People 18 years of age or older with distal subungual toenail onychomycosis involving 20% to 60% of at least 1 TGT were eligible if they had a positive potassium hydroxide (KOH) wet mount and positive culture for dermatophytes, greater than or equal to 3‐mm clear nail measured from the proximal nail fold to the most proximal visible mycotic border, and distal TGT thickness 3 mm or less Exclusion criteria: Patients with proximal subungual or superficial white onychomycosis, severe disease, dermatophytoma, exclusively lateral disease, yellow/brown spikes, co‐infection with nondermatophyte fungi, anatomic abnormalities of the toes or toenails, active tinea pedis (involving the sides or back of the foot, interdigital, or plantar) requiring treatment, history of chronic moccasin‐type tinea pedis (involving the sides or back of the foot), history of other significant chronic fungal disease, psoriasis, lichen planus, known immunodeficiency, significant peripheral vascular disease, known structural heart disease, or uncontrolled diabetes (haemoglobin A1C 8%). Patients who used topical antifungals on the toenails within 4 weeks or systemic antifungals within 24 weeks were also excluded. Recent use of other topical agents on the toe or toenails, systemic corticosteroids, or immunomodulatory agents was not permitted Disease duration: Unknown Comparable at baseline: Yes Causative species: Dermatophytes Number of people lost to follow‐up: Tavaborole: participant request n = 24, lost to follow‐up n = 18, noncompliance n = 2, adverse events n = 1, other n = 7. Vehicle: participant request n = 11, lost to follow‐up n = 5, noncompliance n = 2, adverse events n = 2, other n = 3 Trial duration: December 2010 ‐ November 2012 |
|
| Interventions | Treatment duration: Once daily for 48 weeks Drug in study arm 1: Tavaborole topical solution 5%, n = 400; PSFU n = 18 Drug in study arm 2: Vehicle, n = 194; PSFU n = 2 |
|
| Outcomes | Mycological cure (KOH and culture) at week 52 Complete cure (no clinical evidence of onychomycosis and mycological cure) at week 52 and 60 Complete or almost complete clear nail (≤ 10% nail affected) at week 52 Complete or almost complete clear nail (≤ 10% nail affected) plus mycological cure at week 52 and 60 (treatment success) Adverse events: reported |
|
| Notes | 2 of 9 authors are employees of industry, while the remaining 7 have ties to industry (e.g. advisor, consultant, investigator). Funded by industry. Disclosures accompanied by a quote: "The authors were fully responsible for the content, editorial decisions, and opinions expressed in the current article. No author received an honorarium related to the development of this manuscript." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "The randomisation (blocks of 6) was stratified by investigational site in a 2:1 ratio to the following treatment groups: tavaborole or vehicle" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: "Treatment assignment was accomplished by a computer generated random sequence implemented through the interactive web randomisation system (IWRS)." Comment: Allocation concealment appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Email response: "Tavaborole or matching vehicle was supplied in amber glass bottles containing 10 mL of investigational product...neither the Investigator nor the subject knew the subject's treatment assignment." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Email response: "...neither the Investigator nor the subject knew the subject's treatment assignment. The Sponsor’s staff involved in clinical management, data management, and statistical evaluation was to remain blinded until a database lock memo was issued and identification of the analysis populations was agreed upon and documented." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in trial protocol are explicit. The same outcomes are specified and reported verbatim in the publication. One variation of the secondary outcome was added to the publication that is not stated in the trial protocol. NCT01302119 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Elewski 2015b.
| Methods |
Study 2 RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 4 weeks Time points of measurements: Weeks 2, 6, and every 6 weeks thereafter; at week 48, patients who achieved complete cure or treatment success were followed until week 60 (post‐study follow‐up (PSFU)) Location: United States and Canada, 32 individual sites (cities/institutions not stated) |
|
| Participants | Total n: 604 randomised Age: Mean ± SD: tavaborole 55.5 ± 11.5, vehicle 55.4 ± 11.0 Sex: Tavaborole: men 323/396 (81.6%), women 73/396 (18.4%), 3 participants were excluded because study treatment was not dispensed. Vehicle: men 174/205 (84.9%), women 31/205 (15.1%) Inclusion criteria: People 18 years of age or older with distal subungual toenail onychomycosis involving 20% to 60% of at least 1 TGT were eligible if they had a positive KOH wet mount and positive culture for dermatophytes, ≥ 3 mm clear nail measured from the proximal nail fold to the most proximal visible mycotic border, and distal TGT thickness 3 mm or less Exclusion criteria: People with proximal subungual or superficial white onychomycosis, severe disease, dermatophytoma, exclusively lateral disease, yellow/brown spikes, co‐infection with nondermatophyte fungi, anatomic abnormalities of the toes or toenails, active tinea pedis (involving the sides or back of the foot, interdigital, or plantar) requiring treatment, history of chronic moccasin‐type tinea pedis (involving the sides or back of the foot), history of other significant chronic fungal disease, psoriasis, lichen planus, known immunodeficiency, significant peripheral vascular disease, known structural heart disease, or uncontrolled diabetes (haemoglobin A1C 8%). Patients who used topical antifungals on the toenails within 4 weeks or systemic antifungals within 24 weeks were also excluded. Recent use of other topical agents on the toe or toenails, systemic corticosteroids, or immunomodulatory agents was not permitted Disease duration: Unknown Comparable at baseline: Yes Causative species: Dermatophtyes Number of participants lost to follow‐up: tavaborole: participant request n = 30, lost to follow‐up n = 10, noncompliance n = 4, adverse events n = 2, other n = 4. Vehicle: participant request n = 20, lost to follow‐up n = 4, noncompliance n = 2, adverse events n = 1, other n = 1 Trial duration: February 2011 ‐ January 2013 |
|
| Interventions | Treatment duration: Once daily for 48 weeks Drug in study arm 1: Tavaborole topical solution 5%, n = 399; PSFU n = 31 Drug in study arm 2: Vehicle, n = 205; PSFU n = 11 |
|
| Outcomes | Mycological cure (KOH and culture) at week 52 Complete cure (no clinical evidence of onychomycosis and mycological cure) at weeks 52 and 60 Complete or almost complete clear nail (≤ 10% nail affected) at week 52 Complete or almost complete clear nail (≤ 10% nail affected) plus mycological cure at week 52 and 60 (treatment success) Adverse events: reported |
|
| Notes | 2 of 9 authors are employees of industry, while the remaining 7 have ties to industry (e.g. advisor, consultant, investigator). Funded by industry. Disclosures accompanied by a quote: "The authors were fully responsible for the content, editorial decisions, and opinions expressed in the current article. No author received an honorarium related to the development of this manuscript." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "The randomisation (blocks of 6) was stratified by investigational site in a 2:1 ratio to the following treatment groups: tavaborole or vehicle." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: "Treatment assignment was accomplished by a computer generated random sequence implemented through the interactive web randomisation system (IWRS)." Comment: Allocation concealment appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Email response: "Tavaborole or matching vehicle was supplied in amber glass bottles containing 10 mL of investigational product...neither the Investigator nor the subject knew the subject's treatment assignment." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Email response: "...neither the Investigator nor the subject knew the subject's treatment assignment. The Sponsor’s staff involved in clinical management, data management, and statistical evaluation was to remain blinded until a database lock memo was issued and identification of the analysis populations was agreed upon and documented." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in trial protocol are explicit. The same outcomes are specified and reported verbatim in the publication. One variation of the secondary outcome was added to the publication that is not stated in the trial protocol. NCT 01270971 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
EUCTR2005‐005905‐51.
| Methods | RCT (parallel) Study design: Double blind for 2 treatments, Single blind for third treatment Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: Unknown Time points of measurements: Week 12 Location: Iceland (city/institution not stated) |
|
| Participants | Total n: 50 Age: 18 ‐ 70 years Sex: Men and women (ratio unknown) Inclusion criteria: Men and women, 18 ‐ 70 years of age inclusive, diagnosed with mild‐to‐moderate distal subungual onychomycosis due to dermatophytes (KOH and culture), involving at least 1 great toenail with < 74% nail involvement Exclusion criteria: Unacceptable contraception, pregnancy or breastfeeding, white superficial or proximal subungual onychomycosis involving the nail matrix, systemic or topical antifungal use within 6 months, history of immunosuppression, peripheral vascular disease, peripheral neuropathy, history of skin disease or allergy/hypersensitivity likely to interfere with study, trial participation for onychomycosis within 6 months or use of investigational drug within 30 days of recruitment, abnormal laboratory results at the discretion of the investigator Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown Trial duration: unknown |
|
| Interventions | Treatment duration: once daily for 12 weeks Drug in study arm 1: Ciclopirox 7.5% solution, n = unknown Drug in study arm 2: Mycoster 8% film‐forming solution, n = unknown Drug in study arm 3: Vehicle lacquer to ciclopirox solution, n = unknown |
|
| Outcomes | Tolerability as measured by the investigator tolerance assessments (inflammation and scaling) and as assessed by participants (burning and pruritus) Adverse events: not reported Percentage of target nail affected compared to baseline |
|
| Notes | Commercial sponsor. Industry funding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information provided in protocol |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register are defined |
| Other bias | Unclear risk | Comment: Multiple treatment arm study, but there are no results to assess |
EUCTR2006‐000974‐54.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: Unknown Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 9 months Time points of measurements: Days 1, 7, 14, 45, 90, 135, 180, 210 and 270 Location: 13 centres in Bulgaria, Czech Republic, Germany, and Iceland (cities/institutions not stated) |
|
| Participants | Total n: 127 Age: 21 ‐ 65 years. Sex: Amorolfine‐NF 10%: women 13/31 (41.9%), men 18/31 (58.1%). Amorolfine‐NF 4%: women 17/30 (56.7%), men 13/30 (43.3%). Loceryl 5%: women 19/34 (55.9%), men 15/34 (44.1%). Vehicle: women 19/32 (59.4%), men 13/32 (40.6%). Total: women 68/127 (53.5%), men 59/127 (46.5%). Inclusion criteria: Distal and lateral subungual onychomycosis due to dermatophytes, involving at least 1 great toenail with at least 25% of the nail surface area affected Exclusion criteria: Involvement of the proximal third of the nail Disease duration (years): Amorolfine ‐ NF 10% mean ± SD: 7.71 ± 6.3, median 5.00 (min, max) (0.4, 20.0). Amorofline‐NF 4% mean ± SD: 7.03 ± 6.7 median 5.00 (Min, Max) (0.3, 30.0). Loceryl 5% Nail Lacquer mean 7.88 ± 7.7 median 5.00 (Min, Max) (1.0, 34.0). Vehicle mean ± SD 6.33 ± 6.2 median 4.50 (Min, Max) (0.3, 25.0). Total 7.24 ± 6.7 median 5.00 (Min, Max) (0.3, 34.0) Comparable at baseline: Yes Causative species: Dermatophyte Number of people lost to follow‐up: Discontinuation ‐ Lack of efficacy: amorolfine‐NF 10% n = 1, Loceryl 5% nail lacquer n = 1, total n = 2. Lost to follow‐up: amorolfine‐NF 10% n = 1, amorolfine NF n = 2, Loceryl 5% nail lacquer n = 1. Vehicle n = 1, total n = 5. Other amorolfine NF 10% n = 1, vehicle n = 2, total n = 3. Participant's request: amorolfine NF 10% n = 4, amorolfine NF 4% n = 1, Loceryl 5% nail lacquer n = 2, vehicle n = 1, total n = 8 Trial duration: September 26, 2006 ‐ May 15, 2008 |
|
| Interventions | Drug in study arm 1: Amorolfine 10% lacquer daily for 2 weeks then weekly until 6 months, n = 31 Drug in study arm 2: Amorolfine 4% lacquer daily for 2 weeks then weekly until 6 months, n = 30 Drug in study arm 3: Vehicle nail lacquer daily for 2 weeks then weekly until 6 months, n = 34 Drug in study arm 4: Loceryl (amorolfine 5% nail lacquer) daily for 2 weeks then weekly until 6 months, n = 32 |
|
| Outcomes | Clinical cure (completely cleared target great toenail) at days 1, 7, 14, 45, 90, 135, 180, 210 and 270 Mycological cure (negative culture) at days 1, 7, 14, 45, 90, 135, 180, 210 and 270 Adverse events: reported |
|
| Notes | Commercial sponsor. Industry funding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information provided in protocol |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for discontinuation were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Results submitted to trial registry limited, with data for analysis not extractable apart from safety outcomes. Planned statistical comparisons and reporting of clinical outcomes do not include all treatment groups. No publication or further data available for cross‐reference |
| Other bias | Low risk | Comment: Multiple intervention trial, but safety reported for all interventions and treatment outcomes analysed without pooling of interventions |
EUCTR2006‐005895‐42.
| Methods | RCT (parallel) Study design: Open Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 12 weeks Time points of measurements: Week 48 and 60 Location: Switzerland (city/institution unknown) |
|
| Participants | Total n: 235 Age: 18 ‐ 75 years Sex: Men and women (ratio unknown) Inclusion criteria: Men and women, 18 ‐ 75 years of age, diagnosed with distal/lateral subungual onychomycosis due to dermatophytes (KOH and culture), involving at least 1 great toenail with 15% to 75% nail involvement Exclusion criteria: Non‐dermatophyte infections, pregnant or lactating women, hypersensitivity to terbinafine or ciclopirox, structural deformities of the toenails, oral antifungals to treat onychomycosis within 6 months, topical antifungals to treat onychomycosis within 3 months, dermatophytoma Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown Trial duration: unknown |
|
| Interventions | Treatment duration: once daily for 48 weeks Drug in study arm 1: Laser method to create perforated holes (once) followed by 10% terbinafine ethanolic solution and 8% terbinafine lacquer, n = unknown Drug in study arm 2: ciclopirox 8% lacquer, n = unknown |
|
| Outcomes | Complete cure (100% clear nail and negative KOH and culture) at week 48 Mycological cure Time to complete cure Effectively treated/almost clear Relapse (in those achieving complete cure) at week 60 Adverse events: not reported |
|
| Notes | Commercial sponsor. Industry funding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information provided in protocol |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: The study was not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: The study was not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Selective reporting (reporting bias) | High risk | Comment: Primary outcome defined clearly. Secondary outcomes provided in clinical trial register not defined |
| Other bias | Unclear risk | Comment: There are no results to assess |
EUCTR2008‐003215‐13.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Yes Diagnosis mycology: microscopy and culture Big toenail specified: No Statistical comparisons for outcomes: Yes Duration of follow‐up: At 6 months Time points of measurements: Day 14, months 3 and 6 Location: Germany (sites, n = 35), Poland (n = 6), Czech Republic (n = 10) |
|
| Participants | Total n: 692 Age: At least 18 years Sex: Men 384/692 (55.5%), women 308/692 (44.5%) Inclusion criteria: Aged at least 18 years with positive clinical and mycological findings of onychomycosis (positive microscopy and positive culture with identification of pathogen). People with psoriasis at head/neck and torso, fontaine stage I (no symptoms), no signs of venous disease or presenting with only ecstatic or reticular veins or with varicose veins (Widmer stage I ‐ II), known rheumatic disease not requiring any treatment, known history of Hepatitis C in the past not requiring any treatment and basalioma or actinic keratodermia could be included in the study Exclusion criteria: Nail mycosis in > 3 nails (each nail not more than 50% infected area, in the target nail between 20% and 50%) Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: n = 692 participants were randomised, n = 653 completed both treatment phases of the study, 325/347 participants (93.7%) in the bifonazole group and 328/345 participants (95.1%) in the placebo group. A total of 629 participants completed the whole study period, i.e. until last V5, 311/347 participants (89.6%) in the bifonazole group and 318/345 participants (92.2%) in the placebo group Trial duration: October 23, 2008 ‐ January 21, 2010 |
|
| Interventions | Treatment duration: the overall treatment duration per participant was 42 days up to 56 days: 1st treatment phase (nail ablation) ‐ 14 days (up to 28 days); 2nd treatment phase (antifungal treatment) 28 days Drug in study arm 1: bifonazole 1% cream and urea 40% paste. Urea: topical application once daily on infected nail areas (14 days up to 28 days). Bifonazole: topical application once daily on infected nail areas (28 days), n = 347 Drug in study arm 2: urea 40% paste and placebo. Urea: topical application once daily on infected nail areas (14 days up to 28 days); Placebo cream: topical application once daily on infected nail areas (28 days), n = 345 |
|
| Outcomes | Complete cure (mycological and clinical cure) at day 14, months 3 and 6 Mycological cure rate (microscopy and culture) at day 14, months 3 and 6 Adverse events: reported |
|
| Notes | Commercial sponsor. Industry funding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information provided in protocol |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: Number of participants discontinuing study provided for each treatment group, but reasons for discontinuation were not provided |
| Selective reporting (reporting bias) | Low risk | Comment: Results to trial registry limited, with data not extractable apart from mycological cure and safety, but results were reported for all stated outcomes |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
EUCTR2016‐001242‐25.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: PCR positive Big toenail specified: No Statistical comparisons for outcome: Unknown Duration of follow‐up: 4 weeks Time points of measurement: At days 28, 46 and weeks 0, 4, 8, 12, 16, 20, 24, 36, 48 and 52 Location: Germany (city/institution unknown) |
|
| Participants | Total n: 46 Age: 18 ‐ 64 years old n = 35; > 65 years old n = 10 Sex: Men and women (ratio unknown) Inclusion criteria: Men and women 18 years old or older, clinical diagnosis of onychomycosis in at least 1 toenail with Onychomycosis Severity Index (OSI) 1 ‐ 15 at screening and baseline (pre‐dose D1) and PCR positive at screening, clinical diagnosis of TP with lesions localised to the interdigital spaces or predominantly interdigital, but may extend to other areas of the foot (the non‐interdigital lesions should not be hyperkeratotic i.e. should not have the characteristics of tinea pedis moccasin), and confirmed by a positive KOH wet mount preparation screening and baseline (pre‐dose D1), sum of the clinical signs and symptom scores of the target TP lesion is at least 2, including a minimum score of at least 1 for erythema AND a minimum score of 1 for either scaling or pruritus (on a scale of 0 ‐ 3, where 1 indicated mild severity), non‐menopausal or non‐surgically sterilised childbearing potential women must have a negative urine HCG at the time of entry into the study with no intentions of becoming pregnant during the study, non‐menopausal or non‐surgically sterilised childbearing potential women must use a medically acceptable form of birth control. Participants must have the mental, literate, and legal ability to give written informed consent, which must comply with the International Council for Harmonisation (ICH) guidelines and local requirements. Reliable contraception is defined as a method which results in a low failure rate, i.e. < 1% per year when used consistently and correctly, such as implants, injectables, some intrauterine contraceptive devices (IUDs), complete sexual abstinence, or a vasectomised partner. Oral contraceptive medications are allowed in this study. Women who are surgically sterile (bilateral tubal ligation, bilateral oophorectomy or hysterectomy) or postmenopausal (defined as no menstrual period within 1 year of screening) are also allowed to participate. Exclusion criteria: PCR negative OM, OSI ≥ 16, KOH negative tinea pedis, known history of hypersensitivity or allergy to or known contraindication to the use of Lamisil®, terbinafine, BB2603 or any of its components/excipients, pregnancy or planning to become pregnant during the study period, breast feeding, severe renal or hepatic impairment with parameters of grade 3 or higher on the corresponding CTCAE scale, presence of other known clinically significant medical and/or psychological illnesses precluding participation, any dermatological condition that could mimic the signs and symptoms of TP or OM, progression of OM by > 50% nail manifestation during the last 2 months before enrolment, use of any systemic (oral) or topical anti‐fungal treatment for onychomycosis in the previous 3 months, use of systemic (oral) antipruritics, including antihistamines, within 72 hours prior to first dosing in the study (Day 1), use of systemic (oral or injectable) corticosteroid or antibiotic therapy within 1 month prior to first dosing in the study (Day 1), use of oral terbinafine or itraconazole (or other oral anti‐fungal) within 3 months prior to first dosing in the study, use of topical corticosteroid, antibiotics or antifungal therapy for tinea pedis within 2 weeks prior to first dosing in the study, use of immunosuppressive medication or radiation therapy within 2 months prior to study entry, use of laser therapy, photodynamic therapy, chemical, surgical, relevant mechanical removal for onychomycosis within the last 3 months, confluent, diffuse moccasin‐type tinea pedis associated with the entire plantar surface, presence of any other infection of the foot or other disease process that might confound the treatment evaluation, history of dermatophyte infections unresponsive to systemic or topical antifungal drugs (other than onychomycosis), use of any investigational agent within 30 days or 5 half‐lives prior to randomisation, whichever is longer, screening blood parameters > 2 times upper limit of normal, unable or unwilling to complete the follow‐up evaluations required for the study, any other condition that, in the opinion of the Investigator, would prevent the person from effectively participating in the study, place the person at risk or affect the assessment of efficacy and safety of the study medication, vulnerable people (such as those kept in detention), individuals involved in the planning and/or conduct of the study (i.e. sponsor or employees of sponsor, CRO employees and relatives thereof), any other condition that, in the opinion of the Investigator, would prevent the person from effectively participating in the study, place the person at risk or affect the assessment of efficacy and safety of the study medication, terbinafine resistance should be noted. Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: 1 participant had toe trauma and lost the target toenail Trial duration: March 28, 2017 ‐ August 13, 2018 |
|
| Interventions | Treatment duration: 48 weeks Drug in study arm 1: BB2603 (terbinafine hydrochloride 0.01%), n = unknown Drug in study arm 2: Lamisil spray 1% (terbinafine hydrochloride), n = unknown Drug in study arm 3: Vehicle spray to BB2603, n = unknown |
|
| Outcomes | Complete cure (negative culture and no clinical signs or symptoms, OSI = 0) at weeks 0, 4, 8, 12, 16, 20, 24, 36, 48 and 52 Mycological cure (PCR) at week 52 Partial cure (negative culture and ≤ 10% nail involvement) at weeks 0, 4, 8, 12, 16, 20, 24, 36, 48 and 52 Clinical improvement (negative culture and reduction in OSI of at least 40% from baseline) at weeks 0, 4, 8, 12, 16, 20, 24, 36, 48 and 52 Adverse events: not reported Participant‐reported outcomes (OnyCOE‐t and lifestyle questionnaire) Pharmacokinetics |
|
| Notes | Sponsored by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "A pre‐specified randomisation system was used to control allocation of individual eligible subjects...randomisation code was provided by CRO prior to the study." Comment: Randomisation method likely appropriate |
| Allocation concealment (selection bias) | Low risk | Email response: "The randomisation scheme and process were developed and managed by the independent CRO pharmacy responsible for study conduct. Sealed envelopes containing the randomisation schedule of the study were opened by the pharmacy for labelling, packaging and randomisation procedures" Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Email response: "[BB2603 and vehicle] were presented as hand‐pump sprays in indistinguishable PVC bottles. Lamisil spray was open label with the marketed packaging." Comment: Adequate participant blinding for 2 of 3 treatment groups. Knowledge of the open arm introduces bias |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Email response: "Investigators [who assessed clinical outcomes] were blinded to treatment allocation." Comment: No information provided in protocol |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Email response: "A total of 46 subjects were randomised...15 patients met pre‐defined stopping criteria and one patient had toe trauma and lost the target toenail." Comment: Participants are accounted for and ITT population is identified. Reasons for discontinuation are provided |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register are clearly defined |
| Other bias | Unclear risk | Comment: Multiple treatment arm study; but there are no results to assess |
Gupta 2000a.
| Methods |
Study 1 RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: 12 to 24 weeks Time points of measurements: every 4 weeks of treatment for global evaluations, every 12 weeks for mycology and photography planimetry Location: United States (city/institution not stated) |
|
| Participants | Total n: 223 Age: Mean ± SD (range): ciclopirox 50.4 ± 12.3 (20 ‐ 70); vehicle 48.6 ± 13.2 (18 ‐ 70) Sex: Ciclopirox: men 85/112 (76%), women 27/112 (24%). Vehicle: men 90/111 (81%), women 21/111 (19%) Inclusion criteria: Individuals age 18 to 70 years with distal subungual tinea unguium of at least 1 great toenail (target nail). Before randomisation, participants were to have clinical evidence of onychomycosis with positive KOH preparation and positive dermatophyte culture. Participants had between 20% and 65% area of target nail involved (confirmed by computerised planimetry of standardised photographs) Exclusion criteria: Either white superficial or proximal subungual onychomycosis present. People with abnormalities of the target nail that could have prevented obtaining a normal‐appearing nail if complete cure of the tinea unguium was achieved. Similarly, individuals with a structural deformity of the target nail or foot that could interfere with photography or planimetric analysis were excluded. An individual with a “spike” of onychomycosis extending to the cuticle of the target nail could not enter the study. A person with a history of immunosuppression or clinical signs indicative of possible immunosuppression was not allowed to enrol in the study Disease duration: Mean (range) Ciclopirox 11.8 (0.6 ‐ 44) years. Vehicle 11.1 (0.3 ‐ 50) years Comparable at baseline: Population characteristics were homogeneous between the 2 treatment groups (P > 0.05) Causative species: Ciclopirox T rubrum 108/112 (96%), T. mentagrophytes 4/112 (4%), E. Floccosum 0/112 (0%), other 0/112 (0%). Vehicle T rubrum 108/111 (97%), T. mentagrophytes 3/111 (3%), E. Floccosum 0/111 (0%), other 0/111 (0%) Number of people lost to follow‐up: Withdrawn (withdrawal of consent, unreliability, violation of protocol criteria, lost to follow‐up, and lack of efficacy): treatment n = 23, vehicle n = 27 Trial duration: unknown |
|
| Interventions | Treatment duration: daily for 48 weeks Drug in study arm 1: Ciclopirox nail lacquer 8%, n = 112 Drug in study arm 2: Vehicle, n = 111 |
|
| Outcomes | Treatment success (KOH and culture and < 10% area involvement of the target nail plate as determined by planimetry) at week 48 Mycological cure (negative KOH and culture) at week 48 Treatment cure (KOH and culture and 100% clear nail) at week 48 Adverse events: reported |
|
| Notes | 3 of 3 authors have ties to industry (e.g. consultant) Quote: "This article is part of a supplement sponsored by [industry]". |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly assigned" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information was available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Incomplete information. Only planimetry is stated as being blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial; all outcomes reported for interventions |
Gupta 2000b.
| Methods |
Study 2 RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: 12 to 24 weeks Time points of measurements: every 4 weeks of treatment for global evaluations, every 12 weeks for mycology and photography planimetry Location: United States (city/institution unknown) |
|
| Participants | Total n: 237 Age: Mean ± SD (range): ciclopirox 49.6 ± 11.9 (19 ‐ 70), vehicle 50.1 ± 12.2 (23 ‐ 70) Sex: Ciclopirox: men 94/119 (79%), women 25/119 (21%). Vehicle: men 89/118 (75%), women 29/118 (25%) Inclusion criteria: Individuals age 18 to 70 years with distal subungual tinea unguium of at least 1 great toenail (target nail). Before randomisation, patients were to have clinical evidence of onychomycosis with positive KOH preparation and positive dermatophyte culture. Participants had between 20% to 65% area of target nail involved (confirmed by computerised planimetry of standardised photographs) Exclusion criteria: If either white superficial or proximal subungual onychomycosis was present. Also excluded were people with abnormalities of the target nail that could have prevented obtaining a normal‐appearing nail if complete cure of the tinea unguium was achieved. Similarly, individuals with a structural deformity of the target nail or foot that could interfere with photography or planimetric analysis were excluded. An individual with a “spike” of onychomycosis extending to the cuticle of the target nail could not enter the study. A person with a history of immunosuppression or clinical signs indicative of possible immunosuppression was not allowed to enrol in the study Disease duration: Mean (range) ciclopirox 10.8 (0.5 ‐ 51) years, vehicle 11.6 (0.5 ‐ 50) years Comparable at baseline: Population characteristics were homogeneous between the 2 treatment groups (P > .05) Causative species: Ciclopirox T rubrum 114/119 (96%), T. mentagrophytes 5/119 (4%), E. fluccosum 0/119 (0%), other 0/119 (0%). Vehicle T rubrum 112/118 (95%), T. mentagrophytes 5/118 (5%), 1/118 (0.9%), Other 0/118 (0%) Number of people lost to follow‐up: Withdrawn (withdrawal of consent, unreliability, violation of protocol criteria, lost to follow‐up, and lack of efficacy): treatment n = 23, vehicle n = 24 Trial duration: unknown |
|
| Interventions | Treatment duration: daily for 48 weeks Drug in study arm 1: Ciclopirox nail lacquer 8%, n = 119 Drug in study arm 2: Vehicle, n = 118 |
|
| Outcomes | Treatment success (KOH and culture and < 10% area involvement of the target nail plate as determined by planimetry) at week 48 Mycological cure (negative KOH and culture) at week 48 Treatment cure (KOH and culture and 100% clear nail) at week 48 Adverse events: reported |
|
| Notes | 3 of 3 authors have ties to industry (e.g. consultant) Quote: "This article is part of a supplement sponsored by [industry]" |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly assigned" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information was available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Incomplete information. Only planimetry is stated as being blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Gupta 2006.
| Methods | RCT (parallel) Study design: Not blinded Sample size calculation: No Diagnosis mycology: Not specified Big toenail specified: Yes Statistical comparison for outcomes: No Duration of follow‐up: At 24 weeks Time points of measurements: Weeks 12 and 24 Location: unknown |
|
| Participants | Total n: 120 Age: unknown Sex: unknown Inclusion criteria: Chinese adults with dermatophyte onychomycosis of at least 1 great toenail Exclusion criteria: Unknown Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow‐up: 0 Trial duration: unknown |
|
| Interventions | Treatment duration: daily for 6 or 12 weeks Placebo lacquer‐12 wks, n = 12 1% terbinafine nail lacquer (TNL)‐6 wks, n = 12 1% TNL‐ 12 weeks, n = 20 5% TNL‐6 weeks, n = 12 5% TNL‐12 weeks, n = 20 10% TNL‐6 weeks, n = 12 10% TNL‐12 weeks, n = 20 Ciclopirox 8% nail lacquer (CNL)‐12 weeks, n = 12 |
|
| Outcomes | Treatment success (KOH and culture with a new unaffected length ≥ 3 mm at week 12) at weeks 12 and 24 Mycological success (KOH and culture) at weeks 12 and 24 Adverse events: reported |
|
| Notes | Conference abstract. Author has ties to industry (e.g. investigator, past honoraria and grants). Study partly funded by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information was available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information was available |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information was available |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Multiple intervention study, but outcomes for all interventions reported separately |
Hartmane 2013.
| Methods | RCT (parallel) Study design: Not blinded Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparison for outcomes: Yes Duration of follow up: 24 weeks Time points of measurements: Weeks 12, 24 and 48 Location: unknown |
|
| Participants | Total n: 60 Age: Unknown Sex: Unknown Inclusion criteria: Men and women aged 12 ‐ 80 years of age with mild‐to‐moderate distal subungual onychomycosis due to dermatophytes (confirmed by KOH and culture), having 25% to 60% diseased big toenail area Exclusion criteria: People with history of cardiovascular, renal, neurologic, liver, immunologic or endocrine dysfunction if they are clinically significant. People with a recent history (< 1 year) of myocardial infarction and/or (< 3 years) of heart failure or those with any cardiac arrhythmia requiring drug therapy. People with liver function impairment AST, ALT more than twice above the upper limit of reference range. People with kidney function impairment serum creatinine more than twice above the upper limit of reference range. History of cancer within the past 5 years, excluding treated basal cell carcinoma. Chemotherapy, immunosuppressive therapy in the 12 weeks prior to screening visit. Systemic glucocorticosteroids, antimetabolites and immunostimulants therapy in the 4 weeks prior to screening visit, alcohol or substance abuse, HIV infection or any other immunodeficiency, history of allergic reactions to terbinafine or its excipients, use of an investigational drug or participation in an investigational study within 30 days prior to administration of study medication. Patients using nail polish or other nail cosmetic product on the concerned nails, target nail hyperkeratosis exceeding 4 mm in thickness, proximal subungual involvement, mucocutaneous candidiasis, white superficial onychomycosis, onychomycosis caused by yeasts or non‐dermatophytes mould, "Yellow spikes" on the target nail, lunula involvement, severe plantar or moccasin tinea pedis, nail abnormalities due to conditions like psoriasis or lichen planus, uncontrolled diabetes, recurrent erysipelas at screening visit. Use of systemic antifungal drugs in the 6 months prior to screening visit, use of topical products containing terbinafine in the 3 months prior to screening visit, use of topical antifungal drugs (other than terbinafine) in the 4 weeks prior to screening visit, breast‐feeding women, positive urine pregnancy test at screening (performed on all women of child‐bearing potential or being in non‐surgical post‐menopause for less than 1 year), women of child‐bearing potential or in menopause for less than 1 year not using a reliable method of contraception Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: 3 participants did not complete the study; 2 in 5% group and 1 in the 10% group Trial duration: unknown |
|
| Interventions | Drug in study arm 1: P‐3058 5% daily for 24 weeks, n = 20 (2 did not complete the study, final n = 18) Drug in study arm 2: P‐3058 10% daily for 24 weeks, n = 20 (1 did not complete the study, final n = 19) Drug in study arm 3: P‐3058 10% weekly for 24 weeks, n = 20 |
|
| Outcomes | Cure (culture and KOH) at weeks 12, 24, 48 Adverse events: reported |
|
| Notes | Conference abstract. 3 of six authors are employees of industry. The study was 100% sponsored by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly allocated" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "open label" Comment: Participants and personnel were not blinded=. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "central, blinded assessor" (EUCTR 2008‐002707‐10) Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Attrition rates provided, but reasons for dropout not provided. The ITT was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Primary endpoint identified in protocol not reported in the article. EUCTR 2008‐002707‐10 |
| Other bias | High risk | Comment: Multiple intervention study with clinical outcome data pooled across treatment groups |
Hollmig 2014.
| Methods | RCT (parallel) Study design: Not blinded Sample size calculation: Yes Diagnosis mycology: PAS stain and culture Big toenail specified: No Statistical comparisons for outcomes: Yes Duration of follow‐up: At 3 and 12 months Time points of measurements: Months 3 and 12 Location: Stanford University, Stanford, California, United States |
|
| Participants | Total n: 27 Age: Mean (range): treatment 53 years, control 65 years, (18 ‐ 75) Sex: Treatment: men 10/12 (83%), women 2/12 (16.7%). Control: men 8/10 (80%), women 2/10 (20%) Inclusion criteria: Diagnosis of onychomycosis by clinical toenail morphology confirmed by positive culture. People whose cultures revealed nondermatophyte molds were included if periodic acid Schiff staining‐assisted microscopic evaluation was positive (4 in laser group; 3 in control group). All participants met diagnostic criteria for onychomycosis as defined by prior studies. Participants were not excluded based on the severity of disease or prior treatment regimen Exclusion criteria: Unknown Disease duration: Unknown Comparable at baseline: Participants in the laser and control groups differed in age (64.9 vs 53.4 years, P = 0.03) but not in gender, interval days for follow‐up, extent of clinical nail involvement, or per cent with dermatophyte species at baseline culture Causative species: dermatophyte and non‐dermatophyte moulds Number of people lost to follow‐up: 5 in laser group lost at 3‐month follow‐up, did not return for re‐evaluation after treatment Patient enrolment: July 2011 ‐ December 2011 |
|
| Interventions | Treatment duration: Participants in the laser group underwent 2 treatments separated by 2 weeks Treatment in study arm 1: 1064 nm laser, n = 17 Treatment in study arm 2: control (not treated), n = 10 |
|
| Outcomes | Mycological cure (culture) at months 3 and 12 Proximal nail plate clearance in mm at months 3 and 12 Adverse events: reported |
|
| Notes | All 6 authors have no conflicts of interest to declare. The laser handpiece was loaned to the University department by industry for the study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomised following simple randomisation procedures (computerized random number generator) in a 2:1 ratio into laser or control groups." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: Randomisation was performed by research staff, not study investigators. Comment: Allocation concealment was likely appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: The study was not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: The study was not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in the publication are the same as those in protocol. NCT01666002 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Ijzerman 2010.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: 4 and 8 weeks following treatment Time points of measurements: Weeks 6, 12, 24, 32, 46, 50 Location: United States (city/institution unknown) |
|
| Participants | Total n = 443 (safety population), intent‐to‐treat (ITT) or per‐protocol (PP) populations unknown Age: 18 ‐ 75 years of age, mean 52 years Sex: men n = 372; women n = 71 Inclusion criteria: Men and women between the ages of 18 and 75 with KOH‐ and culture‐confirmed distal subungual onychomycosis of at least 1 great toe, involving 25% to 67% of the great toenail, without lunular or proximal involvement. Culture‐confirmed for a dermatophyte. Must refrain from using any lotions, creams, liquids, or polish on treated toenails or on the skin immediately adjacent to the toenails during the treatment period unless directed to do so by the investigator. Willing to refrain from using topical steroids or topical antifungals on toenails or the skin immediately adjacent to the toenails; or systemic antifungals for the duration of the study Exclusion criteria: Women who are pregnant, plan to become pregnant during the study, or are nursing a child; are hypersensitive to topical creams, ointments, medications, or surfactants; have received systemic antifungal therapy for any reason within 3 months, or topical antifungal therapy on the toenails or skin immediately adjacent to the toenails within 3 weeks prior to the start of the study; or have taken any investigational drug within 4 weeks prior to the start of the study Disease duration: Unknown Comparable at baseline: Uknown Causative species: Unknown Number of people lost to follow‐up: Unknown Trial duration: unknown |
|
| Interventions | Duration: 42 weeks Drug in study arm 1: NB‐002 oil in water emulsion, 0.25% twice daily Drug in study arm 2: NB‐002 oil in water emulsion, 0.5% once daily Drug in study arm 3: NB‐002 oil in water emulsion, 0.5% twice daily Drug in study arm 4: Vehicle once or twice daily |
|
| Outcomes | Complete cure at week 50 Therapeutic success at week 50 Mycologic cure at week 50 Adverse events: reported |
|
| Notes | Conference abstract. Industry provided support | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information was available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information was available |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information was available |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in conference abstract are included in protocol. NCT00453271 |
| Other bias | Unclear risk | Comment: Multiple intervention trial. Unclear from conference abstract if outcomes were reported for each arm separately |
Iorizzo 2016.
| Methods | RCT (parallel) Study design: Open (blinded evaluator) Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: Unknown Time points of measurements: Weeks 4, 8, 12, 24, and 48 Location: Russian Federation and Latvia (cities/institutions not stated) |
|
| Participants | Total n: 120 Age: Mean ± SD: P‐3051 51.45 ± 11.75, amorolfine 53.85 ± 12.21 (18 ‐ 75) years. Sex: P‐3051: men 6/60 (10.0%), women 54/60 (90%). Amororlfine: men 10/60 (16.7%), women 50/60 (83.3%) Inclusion criteria: Patients with mild‐to‐moderate toenail distal lateral subungual onychomycosis, caused by dermatophytes, yeasts and moulds, of at least 1 big toenail (target nail), without the presence of yellow spikes, dermatophytoma or lunula involvement. According to the protocol, participants, 18 – 75 years old, had to sign an informed consent form before enrolment. Those participants with an infected target nail area ≥ 25 and ≤ 75%, and with both positive KOH and culture for fungal nail pathogens at screening, were enrolled in the trial Exclusion criteria: Concomitant severe plantar tinea pedis, other nail abnormalities (such as psoriasis or lichen planus) and the use of any systemic or topical treatment Disease duration: Unknown Comparable at baseline: Both groups were homogeneous with respect to sex, age and weight, as well as to the number of affected toenails, causative pathogens and the percentage of the infected target nail area Causative species: P‐3051: Dermatophytes 43/60 (71.7%), yeast 12/60 (20.0%), nondermatophyte moulds 5/60 (8.3%). Amorolfine: dermatophytes 47/60 (78.3%), yeast 11/60 (18.3%), nondermatophyte moulds 2/60 (3.4%) Number of people lost to follow‐up: Unknown Participant enrolment: Feb 21, 2012 ‐ May 27, 2014 |
|
| Interventions | Drug in study arm 1: P‐3051 (ciclopirox 8%) daily for 48 weeks, n = 60 Drug in study arm 2: Amorolfine 5% twice weekly for 48 weeks, n = 60 |
|
| Outcomes | Mycological cure (culture and KOH) Complete cure (negative KOH microscopy and negative culture with no residual clinical involvement of the target toenail) at weeks 4, 8, 12, 24, and 48 Treatment success (negative KOH microscopy and negative culture as well as nor residual involvement of the target toenail) at weeks 4, 8, 12, 24, and 48 Adverse events: reported |
|
| Notes | All 4 authors have no conflicts of interest. The study was funded by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "Eligible patients have been randomised to one of the two treatment groups according to a permutated blocks random codes generated by the study statistician through a computer program allocating the patient in a progressive temporal sequence to the treatment random number assigned by the system." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "The investigator allocated the treatments...to each patient according to a randomisation list." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: Participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: A blinded evaluator was used for efficacy outcomes; but safety was recorded by unblinded investigators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Email response: "All patients completed the study, none were lost to follow up." Comment: The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Outcomes reported in the publication are different from those in protocol. EUCTR2011‐003087‐70 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, but all outcomes reported for interventions |
Karsai 2017.
| Methods | RCT (parallel) Study design: Single blind (investigator blind) Sample size calculation: No Diagnosis mycology: PAS stain and culture Big toenail specified: No Statistical comparisons for outcomes: Yes Duration of follow‐up: At 12 months Time points of measurements: Month 12 Location: Medizinisches Versorgungszentrum Dres. Raulin and Kollegen, Karlsruhe, Germany |
|
| Participants | Total n: 22 Age: Mean ± SD (range): treatment 69.4 ± 12, control 65.9 ± 17 years, (18 <) Sex: Treatment: men 7/10 (70%), women 3/10 930%). Control: male 9/10 (90%), female 1/10 (10%) Inclusion criteria: Pople over the age of 18 with a clinical diagnosis of distolateral subungual onychomycosis were enrolled consecutively; the diagnosis was confirmed by means of positive dermatophyte culture on a selective agar plate after incubation at 30 °C for 4 weeks. If the fungal culture was negative, a histopathological examination was conducted at an external laboratory using PAS stain on representative nail clippings Exclusion criteria: Nails with a negative PAS stain were not included. Other exclusion criteria were as follows: other diseases of the nails (e.g. nail psoriasis); a history of previous trauma to the target nail; discolouration of the nail (other than ‘yellow streaks’); a history of peripheral arterial disease or diabetes mellitus; peripheral neuropathy of any kind; allergy to amorolfine or any other ingredient in Loceryl cream; application of topical antimycotics (within the 3 months prior to study enrolment); systemic use of antimycotics (within the 12 months prior to study enrolment); pregnancy or lactation Disease duration: Unknown Comparable at baseline: A comparison of both groups’ OSI scores showed no significant differences at baseline (P = 0.9873) Causative species: In both groups, toenails had solely a Trichophyton rubrum infection Number of participants lost to follow‐up: Laser: withdrew by follow‐up (12 months) or stopped treatment n = 0. Control: withdrew by follow‐up (12 months) n = 2; did not return and/or not reachable Trial duration: February 2013 ‐ February 2015 |
|
| Interventions | Treatment duration: 4 treatments at intervals of 4 ‐ 6 weeks with amorolfine prophylaxis for skin of feet and toes Treatment in study arm 1: Short‐pulsed 1064 Nd:YAG laser (PinPointe Footlaser), n = 10 Treatment in study arm 2: Control (not treated), n = 12 |
|
| Outcomes | Mycological cure (culture and PAS) at month 12 Clinical appearance using Onychomycosis severity index (OSI) at month 12 Adverse events: reported |
|
| Notes | Quote: "There is no conflict of interest. None of the authors of the study has financial interests of any kind or is in any way affiliated with manufacturers, wholesalers or retailers of the device under investigation. Funding sources: None" | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "An independent medical assistant randomised the patients to the treatment group or the control group. The randomisation list was generated using a web based program, and the randomised allocation took place by assigning even numbers to the treatment group and odd numbers to the control group" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "An independent medical assistant randomised the patients to the treatment group or the control group." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: Participants and personnel were not blinded to treatment |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The assessment was performed by two independent blinded investigators who were not otherwise involved in the study" Comment: Blinding was appropriate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Outcomes reported in the publication are different from those in protocol. DRKS00007709 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Koren 2018.
| Methods | RCT (parallel) Study design: Open Sample size calculation: No Diagnosis mycology: Culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 3 and 9 months Time points of measurements: Months 3 and 9 Location: Tel Aviv Medical Center, Tel Aviv, Israel |
|
| Participants | Total n: 60 Age: Mean 49 (Range 26 ‐ 66) Sex: Men and women (ratio unknown) Inclusion criteria: People 18 ‐ 60 years of age with a clinical diagnosis of bilateral toenail onychomycosis and positive mycological culture Exclusion criteria: Systemic antifungal treatment during the past 12 months, concomitant nail disease, vascular or microcirculatory disorders, metabolic diseases, immunodeficiency, paresis and paralysis from CNS or PNS injury, pregnancy, and porphyria, photosensitive dermatoses, and allergy to photosensitisers Disease duration: Mean 11.7 years Comparable at baseline: Unknown Causative species: 94% T. rubrum Number of people lost to follow‐up: Amorolfine group n = 4 due to lack of compliance Trial duration: unknown |
|
| Interventions | Treatment duration: 6 treatment sessions at 3‐week intervals with amorolfine applied once weekly for 9 months Intervention in study arm 1: Fractional ablative CO2 laser followed by 20% ALA‐photodynamic therapy, n = 30 Intervention in study arm 2: Fractional ablative CO2 laser followed by amorolfine 5% lacquer, n = 30 |
|
| Outcomes | Clinical improvement at months 3 and 9, measured on a 0 ‐ 5 scale with 0 = no response to treatment and 5 = fully normal‐appearing nail Mycological culture at months 3 and 9 Patient satisfaction Adverse events: reported |
|
| Notes | Quote: "The authors have no conflicts of interest to declare." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "randomly assigned to 2 study groups. An excel table was prepared in advance and patients were added according to the order of referral/admission to the study. The randomisation occurred before the first study visit in which clinical and demographic data were obtained." Comment: Method of randomisation likely appropriate |
| Allocation concealment (selection bias) | High risk | Email response: "The investigators who provided the treatment were aware of the randomisation for the two study groups." Comment: Allocation concealment was not appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "open‐label" Comment: There was no blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "photographs were compared by 2 dermatologists...the dermatologists were blinded to the study groups" Email response: "The clinical picture evaluators and the laboratory mycological evaluators were blinded to the study groups." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Email response: "The trial was not registered." Comment: Outcomes specified in method reported in results |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Kumar 2001.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparisons for outcomes: No Duration of follow‐up: At 2 weeks Time points of measurements: Weeks 2, 4, 6, 8, 10 and 12 Location: Bangalore (city/institution unknown) |
|
| Participants | Total n: 43 Age: Mean (range): 49 years (21 ‐ 70) Sex: Men 64%, women 36% Inclusion criteria: Clinical diagnosis of distal subungual or proximal onychomycosis or the presence of dermatophytes in mycological culture. All participants withdraw their systemic antifungal treatment and topical treatment 1 month prior to taking samples for baseline mycological culture. Participants were screened before starting the trial treatment and those with clinically suspected toenail infection were included. To exclude any possibility of previous treatment with antimycotic agents, it was mandatory that dermatophytes be present and proliferating in the screening culture before a participant could be included in the study, especially for those who were on antifungal therapies Exclusion criteria: Pregnant or lactating women; those with pre‐existing renal, hepatic or gastrointestinal disease, bacterial or yeast infections of the nails or the periungual area, psoriasis and psoriatic changes of the toenail were excluded from the study Disease duration: Unknown Comparable at baseline: The distribution of age, sex, height and weight were identical in both treatment groups Causative species: Nailcare: T. rubrum 13/46 (28.26%), T. mentagrophytes 8/46 (17.39%). Placebo: T. rubrum 15/46 (32.60%), T. mentagrophytes 7/46 (15.21%) Number of people lost to follow‐up: Nailcare n = 5, placebo n = 5; all due to non‐compliance (not attending appointments) Trial duration: unknown |
|
| Interventions | Treatment duration; 2 capsules and cream twice daily for 12 weeks Drug in study arm 1: NailCare (capsule and cream, multiple herbs in medication including Commiphora mukul, Ocimum basilicum and Vetiveria zizanoides), n = 21 Drug in study arm 2: Placebo (capsule and cream), n = 22 |
|
| Outcomes | Mycological cure (KOH and culture) at weeks 2, 4, 6, 8, 10 and 12 Adverse events: not reported |
|
| Notes | No explicit statements of conflicts of interest. Affiliation of 1 of 2 authors is industry. Data extracted were a subset of the participants randomised; we used data from participants that were positive for mycology at baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomly assigned to treatment...according to a computer generated randomisation schedule" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "identical placebo capsule and cream" Comment: Blinding was appropriate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information was available |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Lahfa 2013.
| Methods | RCT (parallel) Study design: Open label (evaluator blind) Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcome: Yes Duration of follow‐up: At 4 weeks Time points of measurements: Days 0, 21, 77 and 105 Location: France (9 sites), Belgium (4 sites), Italy (3 sites), and Poland (10 sites) (cities/institutions not stated) |
|
| Participants | Total n: 105 Age: Mean ± SD (range): 40% urea ointment 54.3 ± 14.9 years, bifonazole‐urea 52.4 ± 14.8 years, (18 <) Sex: Urea ointment: men 33/53 (62.3%), women 20/53 (37.7%). Bifonazole‐Urea: men 33/52 (63.5%), women 19/52 (36.5%) Inclusion criteria: The study included hospital and private outpatients aged 18 years or older with a diagnosis of onychomycosis of the great toenail. Clinical diagnosis of distal‐lateral or lateral subungual onychomycosis of 1 great toenail (the target nail) was required. The target nail plate had to show ≥ 12.5% of the clinically‐infected area and have at least 2 mm of the proximal target nail free of infection. The target nail infection was exclusively from a dermatophyte, as demonstrated both by positive direct microscopy and by positive fungal culture as reported by the central mycological laboratory Exclusion criteria: People with more than 2 infected toenails, people with moccasin‐type tinea pedis, and those suffering from psoriasis, lichen planus, or other abnormalities that could result in clinically abnormal toenail(s). Peopls who had received systemic antifungal therapy or topical antifungal nail lacquer within 3 months or any other topical antifungal therapy applied to the feet or toenails within 2 months prior to the screening visit were excluded. Systemic corticosteroids, systemic antifungal treatment, and any topical treatment applied directly to the feet or the treated nail other than the investigational products provided were prohibited throughout the study Disease duration: Mean ± SD: urea ointment with plastic dressing 4.1 ± 4.3 years. Bifonazole urea 6.3 ± 7.4 years Comparable at baseline: There were no relevant differences between treatment groups in baseline characteristics Causative species: dermatophyte Number of people lost to follow‐up: n = 5 in treatment, n = 4 in bifonazole urea Trial duration: unknown |
|
| Interventions | Treatment duration: daily for 3 weeks, followed by 8 weeks of bifonazole cream (both arms) Drug in study arm 1: 40% Urea ointment with plastic dressing, n = 53 Drug in study arm 2: 40% urea and 1% bifonazole, n = 52 |
|
| Outcomes | Mycological cure (KOH and culture) at days 0, 21, 77 and 105 Complete cure (mycological cure and clinical cure) at days 0, 21, 77 and 105 Clinical cure (no residual clinical signs of onychomycosis) at days 0, 21, 77 and 105 Adverse events: reported |
|
| Notes | 3 of 12 authors are employees of industry, with an additional 3 authors having ties to industry (e.g. consultant, investigator). The study was sponsored by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomly assigned [to treatment] according to a centralized randomisation table" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information on how allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: This was an open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "centrally assessed by a blinded dermatologist expert panel...Dermatologists from the panel were not investigators in the study and were totally blinded regarding treatment allocation" Comment: Blinding was appropriate |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: Reasons for attrition were not provided |
| Selective reporting (reporting bias) | Low risk | Comment: Efficacy outcomes stated in trial protocol reported in publication. NCT00808366 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Lu 2005.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcome: Yes Duration of follow‐up: At 12 weeks Time points of measurements: 12 weeks Location: China (city/institution not stated) |
|
| Participants | Total n: 120 Age: 18 ‐ 65 years of age Sex: Unknown Inclusion criteria: 18 ‐ 65 years of age, with mycologically (KOH and culture) confirmed dermatophyte onychomycosis involving > 25% of at least 1 great toenail Exclusion criteria: Unknown Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophyte Number of people lost to follow‐up: n = 3, treatment unknown Trial duration: unknown |
|
| Interventions | Drug in study arm 1: 0% terbinafine HCl lacquer once daily for 12 weeks, n = unknown Drug in study arm 2: 1% terbinafine HCl lacquer once daily for 6 weeks, n = unknown Drug in study arm 3: 1% terbinafine HCl lacquer once daily for 12 weeks, n = unknown Drug in study arm 4: 5% terbinafine HCl lacquer once daily for 6 weeks, n = unknown Drug in study arm 5: 5% terbinafine HCl lacquer once daily for 12 weeks, n = unknown Drug in study arm 6: 10% terbinafine HCl lacquer once daily for 6 weeks, n = unknown Drug in study arm 7: 10% terbinafine HCl lacquer once daily for 12 weeks, n = unknown Drug in study arm 8: ciclopirox 8% lacquer once daily for 12 weeks, n = unknown |
|
| Outcomes | Mycological outcomes: negative KOH and negative culture at 12 weeks Clinical success (negative KOH, negative culture, new unaffected nail length ≥ 3mm) at 12 weeks Adverse events: reported |
|
| Notes | Conference abstract. All 3 authors are affiliated with industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information was available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information was available |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: Three patients were not included in the efficacy analysis, no reasons or treatment groups provided |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Multiple intervention trial however, outcomes for all interventions reported separately |
Montana 1994.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparisons for outcomes: No Duration of follow‐up: At 2 months Time points of measurements: Months 6, 12 and 14 Location: unknown |
|
| Participants | Total n: 20 Age: 18 to 75 years Sex: Unknown Inclusion criteria: Participants selected for the study were men and nonpregnant, nonlactating women between the ages of 18 and 75 with a clinical and mycologic diagnosis of distal subungual onychomycosis. A target toenail was chosen and was required to have at least 25% healthy nail. Exclusion criteria: People with psoriasis, lichen planus, or other diseases that may affect the nails or people with significant systemic disease were excluded. Other exclusion criteria included known hypersensitivity to any of the ingredients of the medications, use of a topical antifungal medication within 1 month, or systemic medication within 3 months prior to screening Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of participants lost to follow‐up: lack of efficacy of drug: n = 1, nondermatophyte infection (treatment failed): n = 1; study arm unknown Trial duration: unknown |
|
| Interventions | Treatment duration: twice daily for 12 months Drug in study arm 1: Active Group fungoid tincture (triacetin, cetylpyridinium chloride and chloroxylenol), n = 10. Drug in study arm 2: Vehicle, n = 10 |
|
| Outcomes | Mycological cure (KOH and culture) at months 6, 12 and 14 Adverse events: reported |
|
| Notes | Quote: "This study was supported by a research grant from [industry], which supplied all test materials." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Neither the investigator nor the patients knew the type of medication that each patient received" Comment: Appears to be blinded, but no indication if treatments looked identical |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method or who performed assessments |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "Two patients did not complete the study for reasons unrelated to the drug trial. They were replaced by two additional patients. One patient dropped out due to lack of efficacy of the drug. One of the patients...had a nondermatophyte infection" Comment: Treatment allocation of participants who did not complete the study not specified |
| Selective reporting (reporting bias) | High risk | Comment: Clinical outcomes are not defined clearly or reported. Study pre‐dates trial registry in the USA |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
NCT01080079.
| Methods | RCT (parallel) Study design: Single blind (participant) Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 11 months Time points of measurements: Month 11 Location: University of Alabama at Birmingham, Birmingham, Alabama, United States; International Clinical Research, LLC, Sanford, Florida, United States; Gwinnett Clinical Research Center, Inc., Snellville, Georgia, United States; Oregon Dermatology and Research Center, Portland, Oregon, United States; Temple University School of Podiatric Medicine, Philadelphia, Pennsylvania, United States; Tennessee Clinical Research Center, Nashville, Tennessee, United States; Endeavor Clinical Trials, PA, San Antonio, Texas, United States; Mediprobe Research Inc., London, Ontario, Canada; Lynderm Research Inc., Markham, Ontario, Canada |
|
| Participants | Total n: 168 Age: 18 ‐ 69 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Clinical diagnosis of distal subungual onychomycosis of at least 1 great toenail with 25% ‐ 65% nail involvement inclusive, positive KOH microscopy and culture for a dermatophyte, nail plate ≤ 3 mm thick. Willingness to refrain from using any nail polish products, oral and topical antifungals (except as provided by the investigator for active tinea pedis), and avoid pregnancy Exclusion criteria: Proximal subungual or white superficial onychomycosis, lunula involvement, psoriasis, eczema, tinea pedis, lichen planus, nail abnormalities, dermatophytoma or spikes, uncontrolled diabetes mellitus or diabetes requiring pharmaceutical therapy, peripheral vascular disease, immunosuppression, topical antifungals or corticosteroids in preceding 2 weeks, systemic corticosteroids within 30 days, systemic antifungals within 120 days, pregnant or nursing women, inappropriate birth control, pacemaker or automatic implantable cardioverter/defibrillator, implantable electronic devices Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophytes Number of people lost to follow‐up: Unknown Trial duration: May 2010 ‐ June 2012 |
|
| Interventions | Drug in study arm 1: terbinafine hydrochloride gel 4% with iontophoresis, n = unknown Drug in study arm 2: placebo with iontophoresis, n = unknown |
|
| Outcomes | Clinical and microbiological improvement at 11 months Adverse events: not reported |
|
| Notes | Commercial sponsor. Industry funding. Last update posted on clinicaltrials.gov: October 19, 2012 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information in trial registry |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | High risk | Quote: "Clinical and microbiological improvement in nails" Comment: Outcomes provided in clinical trial register (e.g. clinical improvement in nails) not defined |
| Other bias | Unclear risk | Comment: There are no results to assess |
NCT01145807.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 12 weeks Time points of measurements: Week 48, 52, and 60 Location: Academic Dermatology Associates, Alberquerque, New Mexico, United States |
|
| Participants | Total n: 738 Age: 18 ‐ 75 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Clinical diagnosis of distal subungual onychomycosis of at least 1 great toenail with 25% ‐ 65% nail involvement inclusive, positive KOH microscopy and culture for a dermatophyte, culture for a dermatophyte, or culture of dermatophyte/nondermatophyte. Target nail must have capacity for growth as determined by a history of nail cutting. Willingness to refrain from using any nail polish products and willingness to refrain from pedicures for duration of study Exclusion criteria: Use of an investigational drug within 1 month of study, pregnancy or planning to become pregnant, lactation, hypersensitivity to terbinafine, inability to self‐apply study medication, symptomatic tinea pedis requiring treatment, oral terbinafine within 6 months of study start, oral antifungals within 3 months, topical antifungals within 1 month of study start for toes or feet, nail dystrophy interfering with the assessment of clear nail, superficial white or proximal subungual onychomycosis, non‐dermatophyte‐only infections, matrix involvement, nail plate thickness > 2 mm, yellow streaks or dermatophytoma, history of peripheral arterial disease or diabetes mellitus, ALT or AST levels > 2 times the upper limit of normal without clinical reason Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophytes or mixed dermatophytes‐nondermatophyte Number of people lost to follow‐up: Unknown Trial duration: April 2010 ‐ August 2012 |
|
| Interventions | Treatment duration: Twice daily to all nails for 48 weeks Drug in study arm 1: TDT 067 terbinafine in transfersome spray, n = unknown Drug in study arm 2: Sham comparator, transfersome spray, n = unknown Drug in study arm 3: Placebo comparator, non‐transfersome spray, n = unknown |
|
| Outcomes | Complete cure at weeks 48, 52, 60 Mycologic cure at weeks 48, 52, 60 Effective treatment at weeks 48, 52, 60 Adverse events: not reported |
|
| Notes | Commercial sponsor. Industry funding. Last update posted on clinicaltrials.gov: August 1, 2012 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information in trial registry |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | High risk | Comment: Outcomes provided in clinical trial register (e.g. complete cure, effective treatment rate) not defined |
| Other bias | Unclear risk | Comment: Multiple treatment arm study, but there are no results to assess |
NCT01246518.
| Methods | RCT (parallel) Study design: Open Sample size calculation: Unknown Diagnosis mycology: Culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 9 and 3 months Time points of measurements: 12 months Location: 15 sites, Sweden (cities/institutions unknown) |
|
| Participants | Total n: 250 Age: 18 ‐ 70 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Clinical diagnosis of distal subungual onychomycosis (DSO) of at least 1 great toenail affecting 25% ‐ 75% nail, positive culture for a dermatophyte Exclusion criteria: Proximal subungual onychomycosis, DSO of both great toenails where unaffected proximal nail is less than 2 mm, spikes, dermatophytoma, oral and topical antifungal use within 3 and 1 month of screening, respectively, signs of severe peripheral circulatory insufficiency, immunosuppression, participation in a clinical trial during the previous 4 weeks, known allergies to treatment products, pre‐menopausal women who are pregnant or nursing, not surgically sterile, or not practicing acceptable birth control Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophytes Number of people lost to follow‐up: Unknown Trial duration: December 2010 ‐ October 2012 |
|
| Interventions | Drug in study arm 1: MOB015 once a day for 3 months, n = unknown Drug in study arm 2: MOB015 once a day for 9 months, n = unknown |
|
| Outcomes | Mycologic cure (negative microscopy and culture) at 12 months Proportion of participants with negative culture, negative microscopy, and complete cure at 1, 3, 6, 9, and 12 months Adverse events: not reported |
|
| Notes | Industry provided financial support. Last update posted on clinicaltrials.gov: 25 October 2012; Email correspondence: Data are not available. Phase 3 trials with this agent are ongoing, NCT02859519 and NCT02866032 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "randomisation using the method of randomly permuted blocks." Comment: Method of randomisation appropriate |
| Allocation concealment (selection bias) | Low risk | Email response: "randomisation lists will be prepared by [a third party]...group will be allocated in the web‐based e‐CRF provided by [the third party]" Comment: Allocation concealment appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: Open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: Open‐label study |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | High risk | Comment: Outcome (complete cure) provided in clinical trial register not defined |
| Other bias | Unclear risk | Comment: Not a multiple treatment arm study, but there are no results to assess |
NCT01400594.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: Unknown Time points of measurements: Week 48 Locations: 37 sites in the United States (Birmingham, Alabama, 3 sites: Total Skin and Beauty Dermatology Center; Radiant Research, Inc; UAB Department of Dermatology, University of Alabama; Clinical Research Advantage, Inc., Glendale, Arizona; Radiant Research, Inc., Tucson, Arizona; Diagnamics, Inc. Encinatas, California; Radiant Research, Inc., Denver, Colorado; Center for Clinical and Cosmetic Research, Aventura, Florida; Marta Rendon, MD, Skin Care Research, Inc., Boca Raton, Florida; Pab Clinical Research, Brandon, Florida; Dermatology Research Institute, Coral Gables, Florida; Ameriderm Research, Jacksonville, Florida; Lake Washington Foot & Ankle Center, Melbourne, Florida; Florida Academic Dermatology Center; Miami, Florida; Ameriderm Research, Ormond Beach, Florida; Leavitt Medical Associates of FL, Ormond Beach, Florida; Radiant Research, Inc., Pinellas Park, Florida; Radiant Research, Inc., Atlanta, Georgia; Radiant Research, Inc., Chicago, Illinois; Dawes Fretzin Clinical Research Group, LLC, Indianapolis, Indiana; Derm Research, LLC, Louisville, Kentucky; William P Coleman III, MD, Metairie, Louisiana; Callender center for Clinical Research, Glenn Dale, Maryland; Assoc Foot Clinic & Surgery Specialists, Flint, Michigan; Silverton Skin Institute, Grand Blanc, Michigan; University of Minnesota, Minnesota Clinical Study Center, Fridley, Minnesota; Radiant Research, St. Louis, Missouri; Radiant Research, Inc., Akron, Ohio; Group Health Associates, Tri‐Health, Cincinnati, Ohio; Central Sooner Research, Norman, Oklahoma; Society Hill Dermatology, Philadelphia, Pennsylvania; University of Pittsburg Medical Center, Department of Dermatology, Pittsburgh, Pennsylvania; Radiant Research, Inc., Anderson, South Carolina; Radiant Research, Inc., Dallas, Texas; Radiant Research, Inc., San Antonio, Texas; Coastal Podiatry Group, Virginia Beach, Virginia) |
|
| Participants | Total n: 182 Age: 18 ‐ 70 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Clinical diagnosis of distal subungual onychomycosis of at least 1 great toenail, positive KOH microscopy and culture for a dermatophyte, good general health, willingness to refrain from using lotion, cream, liquid, or polish on treated nails, willingness to refrain from pedicures, acceptable birth control Exclusion criteria: Inability to self‐apply test product onto toenails, use of topical antifungals within last month, uncontrolled diabetes, fingernail onychomycosis, confirmed non‐dermatophyte infection of target toenail, structural deformities of target toenail, history of severe or chronic immunosuppression, any systemic or dermatologic disorder such as severe eczema or atopic dermatitis, psoriasis of the toenails, hypersensitivity or allergy to topical preparations or adhesive dressings Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophytes Number of people lost to follow‐up: Unknown Trial duration: July 2011 ‐ January 2013 |
|
| Interventions | Treatment duration: applied to all toenails for 48 weeks Drug in study arm 1: HTU‐520 patch (terbinafine hydrochloride patch), n = unknown Drug in study arm 2: Placebo patch, n = unknown |
|
| Outcomes | Complete cure (mycological cure and clinical cure) at week 48 Adverse events: not reported |
|
| Notes | Commercial sponsor. Industry funding.Last update posted on clinicaltrials.gov: 4 June 2015 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information in trial registry |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | High risk | Comment: Outcome provided in clinical trial register not defined (e.g. clinical cure, mycological cure) |
| Other bias | Unclear risk | Comment: Not a multiple treatment study, but there are no results to assess |
NCT02022215.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 4 weeks Time points of measurements: Weeks 48, 52 Location: 31 cities in the United States (Birmingham, Alabama; Encinitas, California; San Diego, California; San Francisco, California; Santa Rosa, California; Denver, Colorado; Miami, Florida; Miramar, Florida; Newnan, Georgia; Boise, Idaho; Evansville, Indiana; Baltimore, Maryland; Ann Arbor, Michigan; Clinton Twp, Michigan; Fridley, Minnesota; Albuquerque, New Mexico; New York, New York; Rochester, New York; Cincinnati, Ohio; Portland, Oregon; Mount Pleasant, South Carolina; Knoxville, Tennessee; Nashville, Tennessee; Austin, Texas; College Station, Texas; Dallas, Texas; San Antonio, Texas; Salt Lake City, Utah; Lynchburg, Virginia; Norfolk, Virginia; Spokane, Washington) (institutions unknown) |
|
| Participants | Total n: 304 Age: 18 ‐ 70 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Men and women aged 18 ‐ 70 years with clinically‐diagnosed mild‐to‐moderate distal subungual onychomycosis of the target nail, with positive KOH and positive culture for a dermatophyte. Appropriate birth control required and good general health as determined by the investigator Exclusion criteria: Uncontrolled diabetes, fingernail onychomycosis, prior antifungal drug use with failure to complete washout, history of HIV, hepatitis B or C, diagnosis of psoriasis or history of psoriasis, participation in a trial within 30 days or concurrently, pregnancy/lactation Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophytes Number of people lost to follow‐up: Unknown Trial duration: December 19, 2013 ‐ March 1, 2016 |
|
| Interventions | Treatment duration: applied once daily for 48 weeks Drug in study arm 1: ME1111 solution, low strength, n = unknown Drug in study arm 2: ME1111 solution, high strength, n = unknown Drug in study arm 3: Vehicle solution, n = unknown |
|
| Outcomes | Complete cure at week 52 Complete or almost complete cure rate (5% or less clinical involvement of target great toenail and mycologic cure) at week 52 Number of adverse events up to week 48, week 52 Local tolerability assessments up to week 48, week 52 Adverse events: not reported |
|
| Notes | Commercial sponsor. Industry funding. Last update posted on clinicaltrials.gov: 23 March 2017 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information in trial registry |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register comprehensive and well‐defined |
| Other bias | Unclear risk | Comment: Multiple treatment arm study, but there are no results to assess |
NCT02343627.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparisons for outcomes: Unknown Duration of follow‐up: 300 days Time points of measurements: Days 28, 60, 90, 180, 270, and 360 Location: United States (city/institution unknown) |
|
| Participants | Total n: 47 Age: 18 ‐ 65 years of age Sex: 41 men (NVXT, n = 30) and 6 women (NVXT, n = 5) Inclusion criteria: Men and women 18 ‐ 65 years of age with clinically‐diagnosed mild‐to‐moderate onychomycosis of at least 1 toenail, 10% ‐ 50% nail involvement without involvement of 1 of the lunular proximal regions, with positive KOH and positive culture for a dermatophyte. No current topical or systemic antifungal therapy Exclusion criteria: Nail or anatomical abnormalities of the toe that may interfere with evaluations or dosing compliance Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow‐up: NVXT solution, n = 12; vehicle, n = 1; reasons not provided Trial duration: December 2014 ‐ January 2016 |
|
| Interventions | Treatment duration: applied once daily for 60 days Drug in study arm 1: NVXT solution, n = 35 Drug in study arm 2: Placebo solution, n = 12 |
|
| Outcomes | Negative fungal culture at 28, 60, 90, 180, 270, and 360 days Mycologic cure (negative KOH and culture) at 90, 180, 270, and 360 days Complete cure (0% nail involvement and mycologic cure) at 90, 180, 270, and 360 days Therapeutic success (mycologic cure and ≤ 5% nail involvement or 50% improvement) at 90, 180, 270, and 360 days Clinical cure (0% nail involvement) at 360 days Nail involvement (%) at 360 days Nail condition/appearance using subjective scale at 90, 180, 270, and 360 days Adverse events and application site reactions: reported |
|
| Notes | Commercial sponsor. Industry funding.Last update posted on clinicaltrials.gov: 22 August 2018 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information in trial registry |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register comprehensive and well‐defined |
| Other bias | Unclear risk | Comment: Not a multiple treatment arm study, but there are no results to assess |
NCT02933879.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparison for outcomes: Yes Duration of follow‐up: 365 days Time points of measurement: At days 141, 281, 365 Location: Novum Pharmaceutical Research Services (Novum), Pittsburgh, Pennsylvania, United States |
|
| Participants | Total n: 184 Age: Mean 51.8 ± 14.2 years Sex: Study arm 1: 43 men, 21 women; Study arm 2: 45 men, 17 women; Study arm 3: 37 men, 21 women Inclusion criteria: Men and women 18 years and older with a clinical diagnosis of mild‐to‐moderate onychomycosis of the target toenail (defined as 1 of the infected great toenails with 10% ‐ 35% nail involvement). Onset of clinical signs < 2 years before screening, positive KOH microscopy and positive culture for a dermatophyte, at least 5 mm clear nail between proximal nail fold and deepest extent of onychomycosis, no lunula involvement. Exclusion criteria: Women who are pregnant, lactating or likely to become pregnant during the study, people with proximal onychomycosis, dermatophytomas, fungal spikes, limited lateral onychomycosis, white superficial onychomycosis, significant nail dystrophy, total dystrophy, history of current diabetes or peripheral vascular disease or both, distal nail plate thickness > 3 mm, no new nail growth requiring trimming in the last 2 months for target nail, previous treatment for onychomycosis in the last 12 months that was unresponsive to treatment, non‐dermatophyte infections, history of nail trauma, current or history of psoriasis or lichen planus within the previous 12 months, immunocompromised, use of topical antifungals, immunomodulators, or systemic corticosteroids on the feet within 4 weeks of baseline and use of topical corticosteroids on the feet within 2 weeks of baseline, use of systemic antifungals for onychomycosis or any antifungals with known activity against dermatophytes within the previous 24 weeks Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow‐up: Study arm 1, n = 16; Study arm 2, n = 14; Study arm 3, n = 17 Trial duration: March 21, 2016 ‐ June 21, 2018 |
|
| Interventions | Treatment duration: Treatment daily for 8 weeks or 2 x 8‐week periods separated by 32‐week rest Drug in study arm 1: NVXT topical solution daily for 8 weeks, n = 64 Drug in study arm 2: NVXT topical solution daily for 2 x 8‐week periods, separated by 32 weeks, n = 62. Drug in study arm 3: Placebo topical daily for 2 x 8‐week periods, separated by 32 weeks, n = 58 |
|
| Outcomes | Mycological cure (negative KOH and negative culture) at days 141 and 365 Clinical cure (0% nail involvement) at days 141, 281, and 365 Complete cure (clinical and mycological cure) at days 141 and 365 Almost complete cure (≤ 5% nail involvement and mycological cure) at days 141 and 365 Almost clinical cure (≤ 5% nail involvement) at days 141, 281, and 365 Adverse events: reported |
|
| Notes | Industry provided financial support. Actual study completion date 21 June 2018 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomisation will be generated in blocks of 3" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "the clinical packaging company will hold the randomisation scheme until database lock." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "The study product will be packaged and blinded by an independent clinical packaging company... The bottles used for all three study products are identical in size, shape and colour. A standard label overlay will be used and there is no difference in odour of the products. Therefore, all three products are indistinguishable." Comment: Blinding was appropriate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The study product will be packaged and blinded by an independent clinical packaging company... The bottles used for all three study products are identical in size, shape and colour. A standard label overlay will be used and there is no difference in odour of the products. Therefore, all three products are indistinguishable." Comment: Blinding was appropriate |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: Trial record provides number of people lost to follow‐up but does not provide reasons for discontinuation. Number of people lost is similar among study arms |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes are explicit and results are posted in trial registry for outcomes identified in protocol provided as a link in trial registry |
| Other bias | High risk | Comment: Multiple intervention trial, but some outcomes are not reported separately for all interventions |
NCT03141840.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: Unknown Big toenail specified: Yes Statistical comparison for outcome: Unknown Duration of follow‐up: 12 months Time points of measurements: At months 3, 6 and 12 months Location: Fotcompaniet Stockholm, Stockholm, Sweden |
|
| Participants | Total n: 69 Age: 18 years and older Sex: Men and women (ratio unknown) Inclusion criteria: Provision of written informed consent, men and women above age 18 weighing over 40 kg, present with distal lateral subungual onychomycosis of any of the big toenails due to dermatophytes, the onychomycosis should involve < 50% of the nail bed and may not have reached the cuticle Exclusion criteria: Unable to come for study visits, known allergy to any of the components in ABL01, not willing to participate in the trial or not able to understand the content of the trial, present with proximal subungual onychomycosis or superficial onychomycosis, present with distal lateral subungual onychomycosis of other nails than the big toe, > 50% of the nailbed affected by onychomycosis or the cuticles infected, known conditions (like psoriasis) that cause abnormal nail appearance, nail damage caused by trauma, pressure or other mechanical reasons, currently on immunosuppressive therapy, showing signs of poor peripheral blood circulation, used another topical antifungal treatment within 1 month of screening, used a systemic antifungal treatment within 3 months of screening, participated in any other clinical onychomycosis trial in the previous 3 months Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown Trial duration: Auguts 14, 2017 ‐ February 8, 2019 |
|
| Interventions | Treatment duration: Once weekly for 6 months to 12 months Intervention in study arm 1: ABL01, n = unknown Intervention in study arm 2: Placebo, n = unknown |
|
| Outcomes | Clinical improvement (reduction of 40% in infected nail area) at 6 months Clinical improvement (reduction of 80% in infected nail area) at 12 months Mycological cure (negative test for dermatophytes) at 12 months Adverse events: not reported Participant questionnaire on ease of treatment |
|
| Notes | Completed February 2019, Last update posted 20 February 2019 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Study subjects are randomly assigned to treatment or placebo groups by a predetermined algorithm using sealed envelopes." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: "Sealed envelopes were supplied by the sponsor which specified the code indicating the device a patient received...[Investigators] were not involved in the randomisation procedure, this was handled by the sponsor." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Email response: "Placebo and active devices were labelled and packaged identically...supplied by the sponsor." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Email response: "The patient opened [and used] the device package at home....no devices present [in the clinic]." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information provided in protocol |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register are clearly defined |
| Other bias | Unclear risk | Comment: Not a multiple treatment arm study, but there are no results to assess |
NCT03289871.
| Methods | RCT (parallel) Study design: Open label Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: None Time points of measurements: Days 0, 14, 28, 56, 112, 168 Location: Hospital Habib Thameur, Tunis, Tunisia; Principal Instruction Military Hospital, Tunis, Tunisia |
|
| Participants | Total n: 112 Age: 18+ years of age Sex: Men and women (ratio unknown) Inclusion criteria: Ability to operate medical device, 18 years of age and older with superficial onychomycosis on at least 1 great toenail or light‐to‐moderate disto‐lateral onychomycosis without matrix involvement, confirmed with KOH staining, no systemic antifungal within 6 months of study and no topical antifungal within 3 months of study, use of contraception since at least 12 weeks before study until 1 month after the study. Exclusion criteria: Enrolment in another clinical trial, pregnant, nursing, or women planning to become pregnant, allergy to product constituents, serious or progressive disease such as diabetes, peripheral circulatory disease, HIV, psoriasis, lichen planus, immunosuppression, other cutaneous disease on the nails Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown Trial duration: January 2015 ‐ November 2015 |
|
| Interventions | Intervention arm 1: Excilor medical device, twice a day for 6 months, n = 56 Intervention arm 2: Amorolfine 5% nail lacquer, once a week for 6 months, n = 56 |
|
| Outcomes | Percentage of healthy nail as assessed using digital photography versus baseline at days 14, 28, 56, and 112 Clinical efficacy assessed on a 5‐point scale for onycholysis, nail dystrophy, nail discolouration, nail thickening at days 0, 14, 28, 56, 112, 168 Negative fungal culture at day 0, 168 Evaluation of product tolerance at days 14, 28, 56, and 112 Quality of life using NailQoL questionnaire at days 0, 14, 28, 56, 112, 168 Subjective evaluation with participant questionnaire at days 0, 14, 28, 56, 112, 168 Adverse events: not reported |
|
| Notes | Industry funded. Last update clinicaltrials.gov posted: 21 September 2017. Completed, no results posted | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information in trial registry |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Masking: None (Open Label)" Comment: It is likely that participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Masking: None (Open Label)" Comment: It is likely that outcome assessment was not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information in trial registry |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes provided in clinical trial register comprehensive and well‐defined |
| Other bias | Unclear risk | Comment: Not a multiple treatment arm study, but there are no results to assess |
Nijenhuis‐Rosien 2019.
| Methods | RCT (parallel) Study design: Quadruple blind Sample size calculation: Yes Diagnosis mycology: Microscopy, culture, and PCR Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: 1 year Time points of measurement: At weeks 30 and 52 Location: Innofeet, Zwole, The Netherlands |
|
| Participants | Total n: 63 Age: Median (IQR) Laser = 70.5 (60.7, 73.8); Sham = 66.3 (60.9, 71.1) Sex: Laser, 12 women and 20 men; Sham, 9 women and 22 men Inclusion criteria: Type 1 or type 2 diabetes, over 18 years old, clinical suspicion with microbiologic confirmation of onychomycosis, participant is at risk for diabetic foot ulcers defines as Simms score 1, 2 Exclusion criteria: People without the microbiological confirmation of fungal nail infection, Sims classification of 0 or 3, people with an active or history of a diabetic foot ulcer, people who used systemic or topical anti fungal agents during the preceding 3 months, people with ischaemic rest pain, people with ankle brachial index < 0.9, people with a documented toe pressure below 50 mmHg, people receiving dialysis, severe renal insufficiency (eGFR below 30 ml/min), people with an insufficient knowledge of the Dutch language to understand requirements of the study, people with a dark skin colour (Fitspatrick 4 and 5), people who use immunosuppressive medication, people suffering from nail psoriasis, lichen planus, or other abnormalities that could result in clinically abnormal toenails, and a history of epilepsy Disease duration: Unknown Comparable at baseline: Unknown Causative species: T. rubrum most common, in 78% of laser participants and 71% of sham participants. Other dermatophytes and non‐dermatophyte moulds present Number of people lost to follow‐up: None Trial duration: March 2015 ‐ July 2016 |
|
| Interventions | Treatment duration: Participants are treated with laser session in weeks 0, 2, 4, and 12 Intervention in study arm 1: Nd:YAG laser pulse therapy (1064 nm), n = 32 Intervention in study arm 2: Sham treatment, n=31 |
|
| Outcomes | Complete cure (completely normal nail or, negative mycological results where < 5% target nail affected) at 52 weeks Microbiologic cure at 52 weeks Recurrence (same causative species at baseline and week 52, with negative mycology at week 30) Adverse events: reported |
|
| Notes | Not industry funded, foundation grant‐funded. One of the employers of the lead author had a stake in a medical device supply company that includes the device in the current study, but the lead author has no stake in this company. All other authors have no conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation was done in blocks (5 blocks of 10 and 1 block of 14) by a third party using sealed, non‐transparent envelopes." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "The investigators, patients, outcome assessors, and statistician were blinded for allocation." Comment: Randomisation was performed by a third party and not study investigators. Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "patients were blinded by inserting a hanging barrier (a plain cloth) between the patients' head and his or her feet. In addition, a blinded laser safety goggle was worn by the subjects. During the procedure, the laser was actually turned on but blasted in a fireproof dish, which was placed next to the foot. The procedural sounds and lights during the laser application and sham procedure were identical." "No participant reported knowing about his or her treatment group." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: Personnel performing treatment were different from study investigators, outcome assessors, and the statistician. Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes reported in published trial protocol are explicit. The same outcomes are specified and reported verbatim in the publication. NCT01996995 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Parekh 2017.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparisons for outcomes: Yes Duration of follow‐up: None Time points of measurements: 6 months Location: Apollo Clinic Bangalore, India |
|
| Participants | Total n: 10 with onychomycosis Age: 18 years of age and older Sex: 20 men and 8 women were initially randomised, sex ratio in final group unknown Inclusion criteria: Men and women, age 18 and older, diagnosed severe or very severe onychomycosis, confirmed with positive KOH smear, positive culture for a dermatophyte, and presence of live spores Exclusion criteria: Oral or topical tinea treatments 1 week prior to screening, consumption of any drug 1 week prior to, or during, the study that was judged to compromise the study, history of allergy or intolerance to any drug, pregnancy or lactation, participation in a clinical trial within the previous 30 days Disease duration: Unknown Comparable at baseline: Yes Causative species: dermatophytes Number of people lost to follow‐up: None Trial duration: March 27, 2010 ‐ January 31, 2011 |
|
| Interventions | Drug in study arm 1: Calmagen® lotion twice daily for 12 weeks, followed by once daily for an additional 12 weeks, n = 5 Drug in study arm 2: Placebo lotion twice daily for 12 weeks, followed by once daily for an additional 12 weeks, n = 5 |
|
| Outcomes | Mycological cure: KOH, culture, and live spore counts at 6 months Clinical cure: IGA response of cleared or excellent at 6 months Reduction in severity score of symptoms using SCIO at 6 months Improvement assessed by photographs at 6 months Adverse events: reported |
|
| Notes | 2 of 6 authors own stock in parent company of treatment. No other competing interests listed. The study was sponsored by industry. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomised...in a 1:1 ratio, according to a computer‐generated list by block randomisation" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "The study coordinator kept one set of sealed envelopes containing the treatment codes" Comment: Treatment allocation was likely concealed as a centralised co‐ordinator controlled the randomisation table |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "All patients and the investigator involved in conducting the study were blinded to treatment codes." Comment: It is likely that blinding was maintained |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: The investigator assessed clinical endpoints and was blinded to treatment codes. It is likely that blinding was maintained |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: No participants withdrew from the study. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Addition of secondary outcome in the publication that was not included in the trial registry "IGA response". CTRI/2012/03/002522 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, with all outcomes reported for interventions |
Paul 2013.
| Methods | RCT (parallel) Study design: Open Sample size calculation: Yes Diagnosis mycology: Culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: Unknown Time points of measurements: Weeks 3, 11, 32, and 48 Location: 17 centres in France and Tunisia (cities/institutions unknown) |
|
| Participants | Total n: 142 Age: Mean ± SD (range) amorolfine (AMO) 47.1 ± 15.2 years (20 ‐ 84), sequential treatment (SEQ) 47.1 ± 13.8 years (21 ‐ 76), total 47.1 ± 14.4 years (20 ‐ 84) Sex: AMO: men 32/71 (45.1%), women 39/71 (54.9%). SEQ men 32/71 (45.1%), women 39/71 (54.9%). Total men 64/142 (45.1%), women 78/142 (54.9%) Inclusion criteria: Aged 18 – 70 years with distal‐lateral or lateral subungual onychomycosis caused by T. rubrum were included. They had to have onychomycosis affecting at least 1 big toenail without matrix involvement and showing between 25% and 60% of clinically infected nail area and with at least 2 mm of unaffected proximal target nail area. Eligible participants were required to have a dermatophyte identified by mycological culture. Systemic or topical antifungal therapy had to be stopped at least 3 months before randomisation Exclusion criteria: People with > 3 affected nails; people with psoriasis, lichen planus or other abnormalities that could result in clinically abnormal toenail(s); people with moccasin‐type tinea pedis, and those with known sensitivity to study treatments. Women were excluded if they were pregnant, breast‐feeding or planning a pregnancy during the course of the study Disease duration: Unknown Comparable at baseline: The baseline demographic characteristics and mycological results were similar between groups at inclusion Causative species: Onychomycosis caused by T. rubrum were included Number of people lost to follow‐up; AMO (n = 19): Randomisation error (n = 1), unauthorised concomitant treatment (n = 2), non‐respect of period between visits (n = 10), observance issues (n = 8), non‐assessment of the main efficacy criterion (n = 5). SEQ (n = 10): non‐respect of period between visits (n = 4), observance issues (n = 5), non‐assessment of the main efficacy criterion (n = 2). It was possible for more than 1 reason to be attributed to each participant Trial duration: August 2009 ‐ August 2011 |
|
| Interventions | Treatment duration: 36 weeks Drug in study arm 1: Sequential (SEQ) treatment with chemical nail avulsion with RV4104A ointment for 3 weeks followed by ciclopirox cream for 8 weeks and ciclopirox nail lacquer for 25 weeks (SEQ group), n = 71 Drug in study arm 2: Amorolfine nail lacquer (twice weekly for 36 weeks, AMO), n = 71 |
|
| Outcomes | Mycological cure (KOH and culture) Complete cure (the combination of clinical cure and negative mycology) at weeks 3, 11, 32, and 48 Clinical cure (disappearance of all lesions on each nail or residual disease of no more than 10% of the original total diseased surface) at weeks 3, 11, 32, and 48 Adverse events: reported |
|
| Notes | 3 of 16 authors are employees of industry, while the remaining authors do not state the presence or absence of conflicts. The study was sponsored by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "A centralized randomisation table (block of 2) was established by the Clinical Pharmacy Department...Patients were randomly assigned to one of the 2 parallel treatment arms" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "The treatment was allocated by means of sequentially numbered containers to each patient by the investigator, according to the randomisation list." Comment: Treatment allocation was likely concealed as a third party controlled randomisation table |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Investigator and patient were not blinded to treatment assignment." Comment: Participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Identification of dermatophytes...by two independent and experienced operators who were blinded with respect to the assigned treatment" Comment: Mycological cure was evaluator‐blinded. Clinical outcomes were not evaluator‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Primary outcome not defined in protocol ("efficacy"), with outcomes defined in publication. Secondary outcomes identified in the protocol are reported in the publication. NCT01014637 |
| Other bias | Low risk | Comment: Not a multiple intervention trial; all outcomes reported for interventions |
Romero‐Cerecero 2008.
| Methods | RCT (parallel) Study design: Double blind Sample size calculations: No Diagnosis mycology: Direct examination Big toenail specified: No Statistical comparison for outcomes: Yes Duration of follow‐up: Unknown Time points of measurements: Months 1, 2 and 3 Location: unknown |
|
| Participants | Total n: 110 Age: Mean ± SD (range): A. pichinchensis 44.6 ± 11.9 years, ciclopirox 46.5 ± 12.2 years, (18‐56). Sex: A. pichinchensis: men 14/55 (25.4%), women 41/55 (74.5%). Ciclopirox: men 18/55 (32.7%), women 37/55 (67.2%) Inclusion criteria: People with tinea pedis, with diagnosis of diabetes, as well as pregnant woman or women who were breast‐feeding, or patients who had received treatment for onychomycosis 1 month prior to study initiation, and those allergic to ciclopirox, were not included Exclusion criteria: Noncompliance with the treatment was identified or due to the presence of intense side effects Disease duration: Disease evolution ≤ 1 year A. pich 20/55 (36.3%) ciclopirox 13/55 (23.6%) 2 – 5 years A. pich 23/55 (41.8%) ciclopirox 22/55 (40.1%) > 5 years A. pich 5/55 (9.2%) ciclopirox 8/55 (14.5%) ≥ 10 years A. pich 7/55 (12.7%) ciclopirox 12/55 (21.8%) Comparable at baseline: Personal characteristics (concerning family and disease) of participants did not show differences between the groups Statistical analysis did not evidence inter‐group differences; under basal conditions, we observed that only nail colour alteration was higher in the experimental group Causative species: Most frequently isolated pathogen agent (80%) was T. rubrum Number of people lost to follow‐up: Experimental n = 6, control n = 8 Trial duration: unknown |
|
| Interventions | Treatment Duration: 6 months, three times a week for the first month, twice weekly for the second month, once weekly for the remaining 4 months Drug in study arm 1: A. pichinchensis extract (10%), n = 55 Drug in study arm 2: 8% ciclopirox (control), n = 55 |
|
| Outcomes | Mycological effectiveness (KOH microscopy) at months 1, 2 and 3 Clinical effectiveness (signs or symptoms were found on affected nails) at months 1, 2 and 3 Adverse events: reported |
|
| Notes | Public funding for study. Authors do not state presence or absence of conflicts of interest and are affiliated with academic and public research institutions | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Experimental and control treatments were distributed (in agreement with a table with randomised numbers) to patients consenting..." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: The party that carried out randomisation and treatment allotment is not explicitly stated in the article |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "the flask containing experimental treatment had a similar presentation to that of the control treatment", "the control group received an identical flask" Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for patients discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial, all outcomes reported for interventions |
Romero‐Cerecero 2009.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH Big toenail specified: No Statistical comparisons to outcomes: Yes Duration of follow‐up: Unknown Time points of measurements: Months 1, 2, 3, 4, 5 and 6 Location: Mexico (city/institution unknown) |
|
| Participants | Total n: 122 Age: Median (range): 47 years, (19 and 65). Sex: Men 28/122 (23%), women 94/122 (77%) Inclusion criteria: A diagnosis of mild or moderate onychomycosis aged 19 – 65 years Exclusion criteria: Pregnant or breastfeeding, with diabetes mellitus or another serious disease, as well as people who received treatment for this disease at least 1 month prior to the date of study inclusion, or with a history of sensitivity to topically administrated drugs Disease duration: Unknown Comparable at baseline: Distribution of these variables between both groups was similar, and no significant differences were detected Causative species: Unknown Number of people lost to follow‐up: Group 1 n = 7, group 2 n = 12 Trial duration: unknown |
|
| Interventions | Treatment duration: 6 months Drug in study arm 1: 12.6% Ageratina pichinchensis standardised extract (in a nail lacquer solution), n = 62 Drug in study arm 2: 16.8% Ageratina pichinchensis standardised extract (in a nail lacquer solution), n = 60 |
|
| Outcomes | Mycological diagnosis (microscopy) at months 1, 2, 3, 4, 5 and 6 Adverse events: reported |
|
| Notes | Public funding for the study. Authors do not state presence of absence of conflicts of interest and are affiliated with academic and public research institutions | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Based on a table with randomised numbers, two groups were organized" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: The party that carried out randomisation and treatment allotment is not explicitly stated in the article |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "the medicaments (in a 3‐mL flask presentation with a spiral cover that contained a brush for administration on nails) were packed and labelled in identical form" Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial, and all outcomes reported for interventions |
Schalka 2012.
| Methods | RCT (parallel) Study design: Single blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toe specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 5 and 180 days Time points of measurements: Days 60, 120 and 180 Location: unknown |
|
| Participants | Total n: 41 Age: Average (range): Group 1 41.2 years (18 ‐ 63), Group 2 41.2 years (19 ‐ 65) Sex: Group 1: men 5/20 (25%), women 15/20 (75%). Group 2: men 1/21 (5%), women 20/21 (95%) Inclusion criteria: Men and women, 18 ‐ 65 years of age with distal or lateral subungual onychomycosis of the first right or left toe, between 10% ‐ 50% involvement of the nail plate and without matrix involvement Exclusion criteria: Unknown Disease duration: Average, median ± SD (range): Group 1: 22.3 months, 12 ± 26.7 months (6 ‐ 120); Group 2: 18.2 months, 12 ± 17.5 months (3 ‐ 84) Comparable at baseline: The presence of fungus on the baseline evaluation was similar in both treatment groups. When analysing the results in terms of the population evaluated we noticed a homogeneous distribution between the 2 groups, in terms of sex, age, involved area, proportion of affected nail, time of evolution and previous treatments, this way reducing the interference of these characteristics on the interpretation of the results Causative species: Predominance of the Trichophyton genus, the Trichophyton rubrum and Trichophyton mentagrophytes being represented, respectively, in 55.0% and 30% of the people that used the posology of once a week (group I), and in 61.9% and 19% of those of the 3/2/1 regimen (Group 2). The other species identified were Scytalidium dimidiatum and Candida albicans with a frequency of < 10% Number of participants lost to follow‐up: 0 Trial duration: unknown |
|
| Interventions | Drug in study arm 1: Ciclopirox nail lacquer daily for 6 months, n = 20 Drug in study arm 2: Ciclopirox nail lacquer 3/2/1 (3 x a week in the first month, twice weekly for the second month and weekly till the end of the sixth month), n = 21 |
|
| Outcomes | Mycological cure (negative culture) at days 60, 120 and 180 Therapeutic success (negative culture and clinical improvement > 90% of the healthy nail) at days 60, 120 and 180 Clinical improvement (negative culture and improvement between 50% and 90% of the affected nail and the percentage of improvement of the extension of the affected nail) at days 60, 120 and 180 Adverse events: reported |
|
| Notes | All 3 authors have ties to industry (e.g. consultant, speaker). Grant for performing the study were received from industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly assigned" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: This is a single‐blind study comparing 2 different regimens of the same therapeutic agent. Participants were aware of treatment |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: It is possible that outcome assessors were blinded (single‐blind study). This is not explicitly stated in the article |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: All participants completed the study |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Not a multiple intervention trial, with all outcomes reported for interventions |
Sigurgeirsson 2016.
| Methods | RCT (parallel) Study design: Single blind Sample size calculator: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons to outcomes: Yes Duration of follow‐up: At 7 days post‐final treatment Time points of measurements: Week 12 Location: Reykjavik, Iceland (institution name unknown) |
|
| Participants | Total n: 50 Age: Mean, median ± SD (min‐max, median): amorolfine 5% NL 53.7, 55.5 ± 12.5 (29 ‐ 73), amorolfine 5% NL+cosmetic nail varnish 55.1, 58.0 ± 12.0 (29 ‐ 71), total 54.4, 57.0 ± 12.1 (29 ‐ 73) Sex: Amorofline 5%‐NL: men 20/24 (83.3%), women 4/24 (16.7%). Amorofline 5%‐NL+Cosmetic varnish: men 19/26 (73.1%), women 7/26 (26.9%). Total: men 39/50 (78.0%), women 11/50 (22%) Inclusion criteria: Aged ≥ 18 years with at least 1 big toenail affected by mild‐to‐moderate distal subungual onychomycosis (confirmed by direct microscopic examination and positive mycological culture for dermatophytes or yeast). Participants had a maximum of 50% nail distal edge involved without matrix involvement and no dermatophytoma or subungual hyperkeratosis > 2 mm Exclusion criteria: People with lichen planus, eczema, psoriasis, or other abnormalities of the nail unit Disease duration: < 1 year: Amorolfine 5% NL 2/24 (8.3%), amorolfine 5% NL+cosmetic nail varnish 2/26 (7.7%), total 4/50 (8.0%). 1 ‐ 5 years: amorolfine 5% NL 10/24 (41.7%), amorolfine 5% NL+cosmetic nail varnish 5/26 (19.2%), total 15/50 (30.0%). > 5 years: amorolfine 5% NL 12/24 (50.0%), amorolfine 5% NL+cosmetic nail varnish 19/26 (73.1%), total 31/50 (62.0%) Comparable at baseline: Both groups were comparable in terms of dermographic characteristics Causative Species: Dermatophytes or yeast Number of people lost to follow‐up: n = 1 in each group Trial duration: February 2014 ‐ January 2016 |
|
| Interventions | Treatment duration: once weekly for 12 weeks Drug in study arm 1: Amorolfine 5% NL (alone), n = 24 Drug in study arm 2: Amorolfine 5% NL+a cosmetic nail varnish (applied 24 hours later), n = 26 |
|
| Outcomes | Mycological cure (culture) at week 12 Adverse events: reported |
|
| Notes | 3 of 5 authors are employees of industry. The remaining 2 authors received payment to conduct the study. The study was sponsored by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A randomisation list was generated using the Ranuni routine of the statistical analysis system and a kit number was assigned." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information on how allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: This is an investigator‐blinded study. Participants and personnel were aware of treatment |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "To maintain blinding, the person dispensing the study drug and the subject were instructed not to discuss the study treatments with the evaluating investigator." Comment: It is likely that investigators remained blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | Low risk | Comment: Efficacy outcomes stated in trial protocol reported in publication. NCT02321098 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, with all outcomes reported for interventions |
Stein 2014.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 4 weeks Time points of measurements: Week 52 Location: United States (city/institution unknown) |
|
| Participants | Total n: 334 Age: 18 ‐ 70 years of age, inclusive Sex: Men and women (ratio unknown) Inclusion criteria: Adult men and women, any race, 18 ‐ 70 years of age with a clinical diagnosis of mild‐to‐moderate distal subungual onychomycosis, 25% ‐ 50% nail involvement and positive KOH and culture. Participants had to be free of disease that in the investigator's opinion might interfere with study evaluations or jeopardise patient safety Exclusion criteria: History of intolerance or hypersensitivity to imidazole compounds or the inactive components of the solution. Current or recent participation in another investigational medication or device study Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of participants lost to follow‐up: Unknown Trial duration: unknown |
|
| Interventions | Drug in study arm 1: Luliconazole solution, 10% once daily for 48 weeks, n = unknown Drug in study arm 2: Vehicle solution, once daily for 48 weeks, n = unknown Drug in study arm 3: Luliconazole solution, 10% once daily for 12 weeks, followed by once weekly for 36 weeks, n = unknown Drug in study arm 4: Vehicle solution, 10% once daily for 12 weeks, followed by once weekly for 36 weeks, n = unknown |
|
| Outcomes | Complete cure at week 52 Adverse events: reported |
|
| Notes | Conference abstract of interim results so demographics limited. 1 of 6 authors has industry affiliation. Study supported by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients have been randomised" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: No information was available |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: No information was available |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: No information was available |
| Selective reporting (reporting bias) | Low risk | Comment: Efficacy outcomes stated in trial protocol also stated in abstract. NCT01431820 |
| Other bias | Unclear risk | Comment: Multiple treatment arms, but interim abstract of study's progress and no results to assess |
Syed 1998.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 16 and 36 weeks Time points of measurements: Weeks 8, 16 and 24 Location: unknown |
|
| Participants | Total n: 60 Age: Mean: treatment 27.5, control 26.9, (18 ‐ 60) Sex: Treatment: men 32/50 (64%), women 18/50 (36%), control: men 6/10 (60%), women 4/10 (40%) Inclusion criteria: Fungal infections on at least 1 big toenail with more than 25% involvement of the entire nail bed Exclusion criteria: Included onychomycosis caused by moulds, bacteria, and/or Candida spp., absence of a dermatophyte, a history or presence of psoriasis, any serious concurrent disease, hypersensitivity to azole or benzylamine derivatives, or concomitant therapy with drugs that might affect the bioavailability of benzylamines. People were also excluded if they had used any topical antifungal compound within 2 weeks, had received any systemic antifungal therapy < 3 months before the enrolment, or were pregnant or nursing mothers Disease duration: 4 to 24 months. Comparable at baseline: Statistically, participants who received active or placebo preparations were similar in age, race, number, and area of toenail infection Causative species; Active cream: T. rubrum 47/50 (94%), T. tonsurans 2/50 (4%), T. mentagrophytes 1/50 (2%). Placebo: T. rubrum 7/10 (70%), T. tonsurans 1/10 (10%), T. mentagrophytes 2/10 (20%) Number of participants lost to follow‐up: None Trial duration: unknown |
|
| Interventions | Treatment duration: twice daily for 7 days Drug in study arm 1: Butenafine hydrochloride (2%) and urea (20%), n = 50 Drug in study arm 2: Placebo, n = 10 |
|
| Outcomes | Complete cure (negative fungal culture on fresh specimen, no growth of dermatophytes in culture medium, progressive growth of normal nail and resolution of all clinical symptoms) at weeks 8, 16 and 24 Adverse events: reported |
|
| Notes | Authors have no obvious conflicts from academic affiliations. No statements of presence or absence of conflicts of interest are provided | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly allocated" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Butenafine hydrochloride (2%) and urea (20%) incorporated by weight into a cream and matching placebo were prepared at a department of health approved pharmaceutical laboratory. Trial samples were packed in pre‐coded 25‐g tubes...and coded medication was randomly allocated to each subject for one week" Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: All participants who were enrolled completed the study |
| Selective reporting (reporting bias) | Low risk | Comment: Outcomes specified in Method reported in Results. Study pre‐dates trial registry in the USA |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Syed 1999.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 36 weeks Time points of measurements: Weeks 8, 24 and 36 Location: unknown |
|
| Participants | Total n: 60 Age: Mean (range): active 29.6, placebo 29.7, total 29.6, (18 ‐ 80) Sex: Active: men 24/40 (60%), female 16/40 (40%). Placebo: men 15/20 (75%), women 5/20 (25%). Total: men 31/60 (52%), women 29/60 (48%) Inclusion criteria: Aged 18 – 80 years (mean 29.6) with at least 25% involvement of fungal infection of 1 of the large toenails and clinical diagnosis of distal subungual onychomycosis (confirmed mycologically by 30% KOH wet mount and positive culture for dermatophytes) entered the study Exclusion criteria: Screened at baseline, were onychomycosis caused by moulds, bacteria or Candida spp., a history of psoriasis, any serious concurrent disease, hypersensitivity to Melaleuca alternifolia oil, azole or benzylamine derivatives and concomitant therapy with drugs appearing to affect the bioavailability of benzylamines. Another exclusion criterion was absence of dermatophyte; thus, people who had received systemic antifungal treatment within the previous 3 months or who were using topical treatment during the 2 weeks preceding the study period were not enrolled. Pregnant and lactating women were not recruited Disease duration: Active: 14.3 months, placebo: 15.0 months, total: 6 ‐ 36 months. 29 participants (48.3%) had suffered from nail disease for < 1 year; 51.7% for 1 ‐ 3 years Comparable at baseline: Statistically both groups were comparable in age, race, number and area of toenail infection Causative species: T. rubrum: active 38/40 (95%), placebo 18/20 (90%).T. tonsurans, active 1/40 (2.5%), placebo 2/20 (10%). T. mentagrophytes: active 1/40 (2.5%), placebo 0/20 (0%) Number of people lost to follow‐up: None Trial duration: unknown |
|
| Interventions | Treatment duration: 8 weeks max, 3 times a day, with occlusive dressing Drug in study arm 1: 2% butenafine hydrochloride and 5% Melaleuca alternifolia oil, n = 40 Drug in study arm 2: Placebo (containing Melaleuca alternifolia oil), n = 20 |
|
| Outcomes | Mycological cure (KOH and culture) Clinical success (100% remission or 90% to 99% improvement in treated toenail) at weeks 8, 24 and 36 Overall cure (resolution of all clinical symptoms with respect to global assessment together with mycological cure and progressive growth of normal nail) at weeks 8, 24 and 36 Adverse events: reported |
|
| Notes | Authors have no obvious conflicts from academic affiliations. No statements of presence or absence of conflicts of interest are provided | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly assigned" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "A cream incorporating 2% butenafine hydrochloride and 5% Melaleuca alternifolia oil incorporated by weight and a matching placebo also containing Melaleuca alternifolia oil were prepared at an officially approved pharmaceutical laboratory. Test samples were packed in pre‐coded 40‐g tubes...and pre‐coded trial preparations... were randomly allocated to each patient for one week" Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: All participants who were enrolled completed the study |
| Selective reporting (reporting bias) | High risk | Comment: Not all efficacy outcomes stated in the Methods were reported in the Results |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Toledo‐Bahena 2014.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow up: At 6 months, efficacy measured at 180 and 360 days Time points of measurement: Days 180 and 360 Location: United States and Mexico (cities/institutions unknown) |
|
| Participants | Total n: 187 Age: Mean age ± SD (range): vehicle 43.6 ± 9.0 years (18 ‐ 62), 2.5% tavaborole 44.3 ± 9.8 years (25 ‐ 62), 5.0% tavaborole 39.6 ± 12.2 years (21 ‐ 64), 7.5% tavaborole 43.1 ± 12.1 years (18 ‐ 65) Sex: Vehicle: men 37/63 (58.7%), women 26/63 (41.3%). 2.5% Tavaborole: men 19/33 (57.6%), women 14/33 (42.4%). 5.0% Tavaborole: men 19/31 (61.3%), women 12/31 (38.7%). 7.5% Tavaborole: men 38/60 (63.3%), women 22/60 (36.7%) Inclusion criteria: Adults 18 ‐ 65 years of age with onychomycosis involving 20% ‐ 60% of at least 1 great toenail based on visual inspection and confirmed by positive KOH wet mount or positive fungal culture or both for a dermatophyte. The combined thickness of the affected distal nail plate and hyperkeratotic nail bed must have been < 3 mm. Enrolled participants were required to have normal or clinically non‐significant laboratory findings at screening Exclusion criteria: A history of failed topical antifungal therapy for onychomycosis; anatomic abnormalities of the toe or nail; chronic moccasin‐type tinea pedis; concurrent lichen planus; and current or historical evidence of psoriasis. Also excluded were individuals with diabetes mellitus requiring treatment other than diet and exercise and those with a history of significant internal disease. Concurrent use of topical anti‐inflammatories, topical antifungals applied to feet (except in the case of tinea pedis), topical or systematic antifungals, corticosteroids, and immunomodulators was not permitted. People who had undergone appropriate washout of these medications prior to baseline were permitted to participate. Debridement of the nails was not permissible during the study Disease duration: Unknown Comparable at baseline: The treatment groups in each of the studies were demographically similar Causative species: Dermatophytes Number of participants lost to follow‐up: (by email response) Total n = 119; vehicle N = 26 (lack of efficacy/worsening of condition n = 18; participant request n = 2; lost to follow‐up n = 6); tavaborole 2.5% n = 10 (lack of efficacy/worsening of condition n = 5; lost to follow‐up n = 5); tavaborole 5.0% n = 10 (lack of efficacy/worsening of condition n = 3; lost to follow‐up n = 7); tavaborole 7.5% n = 22 (lack of efficacy/worsening of condition n = 7; adverse event n = 1; participant request n = 4; lost to follow‐up n = 9; death n=1) Trial duration: unknown |
|
| Interventions | Treatment duration: Once daily for 3 months; then 3 times a week for 3 months Drug in study arm 1: Vehicle, n = 63 Drug in study arm 2: 2.5% tavaborole, n = 33 Drug in study arm 3: 5.0% tavaborole, n = 31 Drug in study arm 4: 7.5% tavaborole, n = 60 |
|
| Outcomes | Mycological cure (KOH and culture) at days 180 and 360 Treatment response (success or failure) at days 180 and 360 Mycological response (negative dermatophyte culture) at days 180 and 360 Complete response (ISGA score of clear, negative fungal culture and a negative KOH and the TGT) at days 180 and 360 Adverse events: reported |
|
| Notes | 2 of 8 authors are employees of industry, with the remaining 6 authors reporting ties to industry (e.g. consultant, investigator, speaker). Funded by industry. Disclosures accompanied by a quote: "The authors were fully responsible for the content, editorial decisions, and opinions expressed in the current article. No author received an honorarium related to the development of this manuscript." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Email response: "A computer generated set of random numbers starting with 101 were blocked in groups of 6 ...The randomisation list was securely retained by (the labelling and packaging contractor) and (the) selected clinical data management and biostatistician contractor...After meeting all qualification (baseline) criteria, the subject was assigned to a test agent treatment using the next sequential test agent number." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Email response: "The randomisation list was securely retained by (the labelling and packaging contractor) and [the] selected clinical data management and biostatistician contractor." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Email response: "Subjects, investigators, and research staff were blinded to the subject treatment assigned during the study." "(Tavaborole) Solution and Solution Vehicle were packaged in (identical) 15 mL bottles." Comment: Blinding was adequate |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Email response: "Subjects, investigators, and research staff were blinded to the subject treatment assigned during the study." Comment: Site investigators evaluated efficacy and were blinded to subject treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: The ITT population was clearly specified and used for analyses. Attrition data not included in publication but obtained through email request |
| Selective reporting (reporting bias) | High risk | Comment: Primary outcomes in protocol used as outcome for publication. Secondary measures differ between the protocol and publication. NCT00679965 |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Tschen 2013.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 4 weeks Time points of measurements: Weeks 4, 8, 12, 16, 24, 28, 32, 36 and 40 Location: Mexico ‐ Hosptial Dr. Ángel Leaño / Zapopan, Jalisco; Hospital Ignacio Morones Prieto SLP/SLP, SLP; Hospital General de México/DF; Unidad de Investigación en Salud/Chihuahua; Hospital Central Militar/DF; Instituto Dermatólogico de Jalisco/Guadalajara; Centro de Dermatología de Monterrey/Monterrey Nuevo León; Hospital Universitario /Monterrey Nuevo León; Hospital regional # 1 ISSSTE Mérida/ Mérida, Yucatán; MIRC/OCA Hospital/Monterrey Nuevo León; Clinical Research Institute/DF |
|
| Participants | Total n: 135 Age: Mean, median (range): efinaconazole 10% with semiocclusion 43.1, 44.5 years (19 ‐ 64), efinaconazole 10% 42.7, 39.0 years (20 ‐ 63), efinaconazole 5% 41.6, 40.5 years (20 ‐ 63), vehicle 44.2, 47.0 years (25 ‐ 62), total 42.8, 42.0 years (19 ‐ 64) Sex: Efinaconazole 10% with semiocclusion: men 16/36 (44.4%), women 20/36 (55.6%). Efinaconazole 10%: men 18/39 (46.2%), women 21/39 (53.8%). Efinaconazole 5%: men 19/38 (50%), women 19/38 (50%). Vehicle: men 9/22 (40.9%), women 13/22 (59.1%). Total: men 62/135 (45.9%), women 73/135 (54.1%) Inclusion criteria: Age of 18 to 65 years and a clinical diagnosis of DLSO affecting at least 1 great toenail. Mild‐to‐moderate disease was defined as clinical involvement of 20% to 50% of the target toenail, without dermatophytomas or matrix (lunula) involvement. The target toenail had an uninfected length ≥ 3 mm (from the proximal nail fold), thickness ≤ 3 mm, and evidence of toenail growth, positive KOH microscopy and culture of a dermatophyte or mixed dermatophyte/Candida ≤ 42 days before baseline visit. Women of childbearing potential had to be using effective birth control Exclusion criteria: A history of immunosuppression or clinical signs or both, indicative of possible immunosuppression, known HIV infection, or uncontrolled diabetes. Additional exclusion criteria included presence of toenail infection other than dermatophytes and Candida, severe moccasin‐type tinea pedis at the screening or baseline visits, any disease/condition that might have caused toenail abnormalities or interfered with the evaluation, and previous target toenail surgery. People were not excluded for concomitant drugs that inhibit cytochrome P450 3A4 Disease duration: Unknown Comparable at baseline: Yes Causative species: dermatophyte or mixed dermatophyte/Candida Number of participants lost to follow‐up: Lost to follow‐up (n = 8, 5.9%), participant request (n = 3, 2.2%) and AEs (n = 3, 2.2%). Reasons for discontinuation‐efinaconazole with semi‐occlusion: lost to follow‐up n = 4 Trial duration: October 2007 ‐ February 2009 |
|
| Interventions | Treatment duration: once daily for 36 weeks Drug in study arm 1: Efinaconazole 10% with semi‐occlusion, n = 36 Drug in study arm 2: Efinaconzole 10%, n = 39 Drug in study arm 3: Efinaconazole 5%, n = 38 Drug in study arm 4: Vehicle, n = 22 |
|
| Outcomes | Mycological cure (KOH and culture) Clinical efficacy (an affected target toenail area of < 20%) at weeks 24, 36 and FU Complete cure (0% clinical involvement of the target nail in addition to a mycological cure) at weeks 24, 36 and FU Effective treatment (mycological cure and either an affected target toenail area of 0% or > 3 mm proximal nail growth from baseline in the unaffected target toenail) at weeks 24, 36 and FU Adverse events: reported |
|
| Notes | 4 of 6 authors are employees of industry, while the remaining 2 have ties to industry (e.g. investigator). The study was funded by industry. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Subjects were randomised according to a computer‐generated randomisation schedule." Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Low risk | Quote: "After the completion of the study and after the database was locked, the code was provided to data management for identification of the drug assignment for each subject." Comment: Allocation concealment was appropriate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Email response: "While the study drugs were provided as identical solutions packaged in identical bottles, the study personnel who dispensed the medications would have known which subjects were assigned to the occlusive treatment arm; subjects within this treatment arm similarly would have known their test article assignment. Therefore, to maintain the integrity of the blind, the study staff at each site took precautions to ensure that the investigator did not have access to the study drug, study drug labelling, or any item that identified individual study drug assignments except in the event of a medical emergency." Comment: Assessed as low risk. Only 1 of 4 treatment arms was known, and the control group remained unknown to all personnel |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | See response above Email response: "all sponsor and contract research organization personnel who entered, analysed, or otherwise managed subject‐specific data were blinded throughout the study." Comment: Blinding was adequate |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Trial protocol reports one primary and one secondary outcome. Publication does not differentiate primary and secondary outcomes and includes additional outcomes. NCT00777868 |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Waibel 2013.
| Methods | RCT (parallel) Study design: Open Sample size calculation: No Diagnosis mycology: PAS stain and culture Big toenail specified: No Statistical comparisons for outcomes: No Duration of follow‐up: At 1, 3 and 6 months Time points of measurements: Months 1, 3 and 6 Location: unknown |
|
| Participants | Total n: 21 Age: Average (range): 1064 nm 55.6 years (41 ‐ 68) BBL 58.3 years (33 ‐ 79) 1319 nm 58.9 years (31 ‐ 83) Sex: 1064 nm: men 7/7 (100%), women 0/7 (0%). BBL: men 3/7 (43%), women 4/7 (57%). 1319 nm: men 4/7 (57%), 3/7 (43%). Total: 14 men, 7 women Inclusion criteria: People with both PAS positive and positive fungal culture results. Exclusion criteria: People with a mixed infection or who were pregnant Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of participants lost to follow‐up: None Trial duration: unknown |
|
| Interventions | Treatment Duration: weekly for 4 weeks Treatment in study arm 1: 1064 nm laser, n = 7 Treatment in study arm 2: 1319 nm laser, n = 7 Treatment in study arm 3: BroadBand Light from a filtered flash lamp, n = 7 |
|
| Outcomes | Mycological cure (culture)
Clinical endpoint (negative culture) Adverse events: reported |
|
| Notes | 2 of 3 authors state no relevant conflicts to disclose. 1 author has industry ties and is a "co‐inventor of intellectual property...and may gain royalties from future commercialisation of the technology" | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned to one of three treatment groups" Comment: Method of randomisation not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information was available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: Open trial |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: Open trial |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 21 participants entered the study and 21 completed the study |
| Selective reporting (reporting bias) | Unclear risk | Comment: Review authors were unable to find a clinical trial register entry for this study |
| Other bias | Low risk | Comment: Multiple intervention trial, but outcomes for all interventions reported separately |
Watanabe 2017.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Yes Diagnosis mycology: KOH and LAMP Big toenail specified: Yes Statistical comparisons for outcomes: Yes Duration of follow‐up: At 52 weeks Time points of measurements: Weeks 4, 48 and 52 Location: Japan (cities/institutions unknown) |
|
| Participants | Total n: 293 Age: Mean, median (range): luliconazole 56.9, 59.0 years (24 ‐ 79), vehicle 58.9, 62.0 years (21 ‐ 78), total 57.6, 60.0 years (21 ‐ 79) Sex: Luliconazole: men 129/194 (66.5%), women 65/194 (33.5%). Vehicle: men 76/99 (76.8%), women 23/99 (23.2%). Total: men 205/293 (70.0%), women 88/293 (30.0%) Inclusion criteria: The participants had to: (i) be at least 20 years of age but < 80 years; (ii) have distal lateral subungual onychomycosis involving either the left or the right great toenail; (iii) have positive KOH test results under direct microscopy, and positive detection of T. rubrum or T. mentagrophytes by the LAMP method; (iv) have onychomycosis‐related clinical involvement affecting 20% – 50% of the nail, with a nail thickness of < 3 mm; and (v) provide written informed consent Exclusion criteria: (i) had a history of hypersensitivity to an antifungal agent; (ii) had a history of outpatient treatment for contact dermatitis caused by a topical agent; (iii) had a history of narcotic/drug abuse or alcohol addiction or both; (iv) had severe heart, liver, kidney, lung or blood disease(s) or diabetes; (v) showed disease involvement near the proximal nail fold; (vi) had longitudinal streaks or a spike; (vii) had abnormal conditions in the target toenail that may affect evaluation of drug efficacy; (viii) were unlikely to obtain natural growth of the nail; (ix) had used an oral/injectable antifungal agent within 36 weeks before the start of this study (at baseline); (x) had applied a topical antifungal agent to the nail within 4 weeks before the start of this study (at baseline); (xi) were using or scheduled to use an adrenocortical hormone preparation, immunosuppressant, anti‐cancer drug, skin emollient or anti‐keratosis agent; (xii) were pregnant or suspected of being pregnant, were nursing or wished to become pregnant during the study period; or (xiii) were judged by the physicians in charge of the study to be ineligible to participate Disease duration: Unknown Comparable at baseline: Analysis of the participant disposition showed no significant differences between the 2 groups in any of the relevant demographic factors Causative species: Trichophyton rubrum: luliconazole 148/194 (76.3%); vehicle 76/99 (76.8%); total 224/293 (76.5%). T. mentagrophytes: luliconazole 46/194 (23.7%); vehicle 23/99 (23.2%); total 69/293 (23.5%) Number of people lost to follow‐up: Poor response to study drug or worsening of symptoms: luliconazole n = 4, vehicle n = 2. Development of adverse events: luliconazole n = 12, vehicle n = 2. Worsening of complications: luliconazole n = 1. Observation/laboratory tests could not be performed: luliconazole n = 3, vehicle n = 2. Non‐compliance (use of prohibited concomitant drug): luliconazole n = 1. 1 participant in the luliconazole group displayed 2 reasons simultaneously: poor response to study drug or worsening of symptoms and development of adverse events. Trial duration: April 2012 ‐ January 2014 |
|
| Interventions | Treatment duration: Once daily for 48 weeks Drug in study arm 1: Luliconazole 5% nail solution, n = 194 Drug in study arm 2: Vehicle, n = 99 |
|
| Outcomes | Mycological cure (KOH) at weeks 4, 48 and 52 Complete cure (0% clinical involvement of the nail with negative results on direct microscopy) at week 48 Adverse events: reported |
|
| Notes | 2 of 3 authors are employees of industry. The study was funded by industry | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomised...using the permuted block method with six subjects per block" Comment: Specific randomisation method that is suitable was specified |
| Allocation concealment (selection bias) | Unclear risk | Quote: "allocation of the study drug was entrusted to a third party not involved in evaluating the study results" Comment: Unclear if allocation was withheld from study personnel |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: Blinded, but unclear if study drugs looked identical |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: Blinded, but no specific mention of outcome assessor blinding method |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Reasons for participants discontinuing the study were provided for each treatment group. The ITT population was clearly specified |
| Selective reporting (reporting bias) | High risk | Comment: Trial protocol reports one outcome, complete cure, without a definition. The publication defines complete cure and includes additional secondary endpoints. NCT01431820 |
| Other bias | Low risk | Comment: Not a multiple intervention trial, with all outcomes reported for interventions |
AEs: adverse events; DLSO: distal lateral subungual onychomycosis; FU: follow‐up; ISGA: Investigator's Static Global Assessment; ITT: intention to treat; KOH: potassium hydroxide; LAMP: loop‐mediated isothermal amplification; PAS: periodic acid‐Schiff; PCR: polymerase chain reaction; RCT: randomised controlled trial; SCIO: scoring clinical index for onychomycosis; TEAEs: treatment‐emergent adverse events; TGT: target great toenail.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abd El‐Aal 2019 | Paediatric and adult patient population |
| Anonymous 2000 | Not a RCT |
| Anonymous 2015 | Not a RCT |
| Bassiri‐Jahromi 2012 | Not toenails alone |
| Bergstrom 2009 | Not a RCT |
| Botter 1971 | Not a RCT |
| Canavan 2018 | Not a RCT |
| Chan 2005 | Duration less than 12 weeks |
| Dina 2017 | Not a RCT |
| El‐Tatawy 2015 | Not toenails alone |
| Emtestam 2012 | Not toenails alone |
| Fredriksson 1974 | Not a RCT |
| Furtado 2005 | Not a RCT |
| Gilaberte 2017 | Not toenails alone |
| Gupta 2005 | Ineligible treatment |
| Halmy 2005 | Not toenails alone |
| Harris 2010 | Within‐participant design |
| Hay 1988 | Not a RCT |
| Jimenez‐Faraj 2018 | Duration less than 12 weeks |
| Kamalam 1980 | Not onychomycosis |
| Kim 2016a | Nail as unit of analysis |
| Kim 2016b | Not toenails alone |
| Krasaeath 2016 | Not a RCT |
| Landsman 2010 | Nail as unit of analysis |
| Landsman 2012 | Nail as unit of analysis |
| Lauharanta 1992 | Not toenails alone |
| Li 2014 | Not toenails alone |
| Lu 2016 | Nail as unit of analysis |
| Mahgoub 1975 | Not toenails alone |
| Malay 2009 | Nail as unit of analysis |
| Many 1964 | Not toenails alone |
| Mensing 1992 | Duration less than 12 weeks |
| Menéndez 2011 | Not toenails alone |
| Meyerson 1992 | Not a RCT |
| Morgado 2017 | Not a RCT |
| NCT03094468 | Paediatric and adult patient population |
| Oberste‐Lehn 1974 | Ineligible treatment |
| Ortiz 2014 | Within‐participant design |
| Rand 1996 | Not a RCT |
| Reinel 1992 | Nail as unit of analysis |
| Schaller 2017 | Within‐participant design |
| Schlockermann 1957 | Ineligible treatment |
| Shemer 2016 | Not a RCT |
| Sigurgeirsson 2010 | Prophylaxis |
| Sotiriou 2010 | Not a RCT |
| Souza 2014 | Not a RCT |
| Tardivo 2015 | Not a RCT |
| Tietz 2013 | Not toenails alone |
| Zaug 1995 | Not a RCT |
| Zhang 2012a | Not toenails alone |
| Zhou 2016 | Not toenails alone |
RCT: randomised controlled trial.
Characteristics of studies awaiting assessment [ordered by study ID]
Anonymous 2002.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Bagatell 1977.
| Methods | RCT: unknown Study design: Double blind Diagnosis mycology: KOH and culture Big toenail specified: Unknown if finger‐, toenails, or both Duration of follow‐up: 12 weeks Time points of measurements: 12 and 24 weeks Location: unknown |
| Participants | Total n: Unknown Age: Unknown Sex: Unknown Inclusion/exclusion criteria: Unknown Number of participants lost to follow‐up: 1 Trial duration: unknown |
| Interventions | Treatment duration: 12 weeks for double‐blind; single‐blind for weeks 12 ‐ 24 where placebo received active treatment Drug in study arm 1: Fluorouracil 1% in propylene glycol solution, n = unknown Drug in study arm 2: Placebo solution (propylene glycol), n = unknown |
| Outcomes | Clinical response and laboratory results Adverse events: not reported |
| Notes | Letter to the editor. Cannot assess eligibility as letter does not state whether study investigates fingernail, toenails, or both |
Barquero 2007.
| Methods | RCT: unknown Study design: Double blind Diagnosis mycology: culture Big toenail specified: No Duration of follow‐up: monthly Time points of measurements: monthly Location: Nicaragua (city/institution unknown) |
| Participants | Total n: 24 Age: Unknown Sex: Unknown Inclusion/exclusion criteria: Unknown Number of participants lost to follow‐up: none Trial duration: unknown |
| Interventions | Treatment duration: unknown Drug in study arm 1: terbinafine 1% gel, n = 16 Drug in study arm 2: placebo gel, n = 8 |
| Outcomes | Success or cure: continuous increase of normal nail bed until a normal nail replaced the infected nail Failure: inability, after 2 months, to increase the length of normal nail bed as compared to initial visit Adverse events: not reported |
| Notes | Conference abstract. Cannot assess eligibility as age of participants and whether randomisation occurred is not stated |
Butareva 1986.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Emokpare 1977.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English |
EUCTR2008‐002427‐90.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: Unknown Big toenail specified: No Statistical comparison for outcome: Unknown Duration of follow‐up: Unknown Time points of measurement: 6 or 9 months Location: France (city/institution unknown) |
| Participants | Total n: 300 Age: 18 ‐ 64 years old Sex: Men and women (ratio unknown) Inclusion criteria: Men and women, 18 ‐ 64 years of age, affiliated to a French social security scheme or benefiting from such a scheme, presenting with nail onychomycosis without matrix involvement of a finger or toe that has not yet been treated with an antimycotic Exclusion criteria: Disease or condition requiring immunosuppressive therapy, known allergies or contraindications to investigative products, 2+ fingers or toes affected, oral mycotic treatment, inability to consent, ineffective contraception, assessed as unlikely to comply with study requirements Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown Trial duration: unknown |
| Interventions | Treatment duration: FIngers for 6 months and toes for 9 months Drug in study arm 1: amorolfine, generic 5%, film‐forming solution, n = unknown Drug in study arm 2: Loceryl®, amorolfine 5%, n = unknown. |
| Outcomes | Clinical and mycological efficacy following 6 months (fingers) or 9 months (toes) Adverse events: not reported |
| Notes | Method of diagnosing onychomycosis not specified |
George 1991.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Abstract and full text not available |
Grant 1974.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Abstract and full text not available |
JPRN‐JapicCTI‐101143.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: Direct microscopy Big toenail specified: Unknown if finger‐, toenails, or both Statistical comparison for outcome: Unknown Duration of follow‐up: Unknown Time points of measurements: Unknown Location: Japan (city/institution unknown) |
| Participants | Total n: Unknown Age: 20 ‐ 79 years old Sex: Unknown. Inclusion criteria: People with turbidity on the nails. People with dermatophytes on the nails by direct microscopy. People with dermatophytes of the nails aged 20 ‐ 79 years old, both genders eligible Exclusion criteria: People who used antifungal agents of oral preparations and injections within 36 weeks before consent acquisition, were used up to the test site and the surrounding first joint within 4 weeks before consent acquisition. People who used external antifungal agent containing terbinafine hydrochloride within 12 weeks before consent acquisition Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of participants lost to follow‐up: Unknown Trial duration: unknown |
| Interventions | Treatment duration: Once a day for an unknown amount of time Drug in study arm 1: HTU‐520 (patch containing terbinafine hydrochloride), n = unknown Drug in study arm 2: HTU‐520 placebo applied once a day, n = unknown |
| Outcomes | Efficacy Adverse events: not reported |
| Notes | Cannot assess eligibility as does not state whether study investigates fingernail, toenails, or both |
Klima 1976.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Kull 1972.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Mathur 1973.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Abstract and full text not available |
NCT00253305.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: Unknown Time points of measurements: Unknown Location: United States (University of Alabama at Birmingham, Birmingham, Alabama; Genova Clinical Research, Inc., Tucson, Arizona; Greater Miami Skin and Laser Center, Miami Beach, Florida; Washington University, St. Louis, Missouri; Northwest Cutaneous Research, Portland, Oregon) |
| Participants | Total n: 75 Age: 18 ‐ 65 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Clinical diagnosis of distal subungual onychomycosis of one great toenail with 20% ‐ 65% nail involvement inclusive, positive KOH microscopy and culture for a dermatophyte, 2 mm clear nail proximally, women post‐menopausal or agree to appropriate contraceptives Exclusion criteria: Infecting organisms other than dermatophytes, proximal subungual onychomycosis, spikes of disease extending to nail matrix, 5+ infected nails, confounding problems/abnormalities of target nail, screening lab values more than 20% of normal, hypersensitivity to test materials, systemic medications, poor history of compliance Disease duration: Unknown Comparable at baseline: Unknown Causative species: dermatophytes Number of people lost to follow‐up: Unknown Trial duration: start September 2005, completion date unknown |
| Interventions | Treatment duration: Twice daily to all nails for 48 weeks Drug in study arm 1: Organogel of naftifine, 2% Drug in study arm 2: Organogel of terbinafine, 2% Drug in study arm 3: Organogel of naftifine, 6% Drug in study arm 4: Organogel of terbinafine, 6% |
| Outcomes | Quantitative improvement in toenail appearance KOH and culture Time to achieve 90% and 100% clearance of fungus from the nail Treatment success Mycological success Adverse events: not reported |
| Notes | Length of study unknown |
NCT02549001.
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: Culture and KOH Big toenail specified: Yes Statistical comparison for outcome: Unknown Duration of follow‐up: Unknown Time point of measurement: At week 60 Location: multiple locations in Belgium, Bulgaria, Czechia, Germany, Greece, Hungary, Iceland, Latvia, Lithuania, Poland, Russian Federation, Slovakia, and Sweden (cities/institutions unknown) |
| Participants | Total n: 980 Age: 12 years and older Sex: Unknown Inclusion criteria: Written informed consent, people aged 12 years and older of any race, male or female, people with onychomycosis involving ≥ 20% to ≤ 50% of target big toenail, people with a positive KOH examination and culture positive for dermatophyte Exclusion criteria: Presence of 'yellow spikes' on the target nail, presence of dermatophytoma on the target nail, presence of nail thickness exceeding 2 mm, people with proximal subungual involvement, people with severe plantar or moccasin tinea pedis, people with nail abnormalities due to other conditions, people with life expectancy < 2 years, chemotherapy, immunosuppressive therapy in the 12 weeks prior to screening visit (V1), systemic corticosteroids, antimetabolites and immune‐stimulants therapy in the 4 weeks prior to Screening visit (V1), HIV infection or any other immunodeficiency, alcohol or substance abuse, people with history of allergic reactions to terbinafine or its excipients, women who are pregnant, nursing an infant, or planning a pregnancy during the study period Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown Trial duration: August 20, 2015 ‐ September 17, 2018 |
| Interventions | Treatment duration: For 60 weeks
Drug in study arm 1: Drug: P‐3058 10%, n = unknown Drug in study arm 2: Vehicle of P‐3058 10%, n = unknown Drug in study arm 3: Amorolfine 5% (active comparator), n = unknown |
| Outcomes | Mycological cure (KOH and culture) at week 60 Complete cure at week 60 Adverse events: not reported |
| Notes | Industry provided financial support. Last participant completed 17 September 2018. Unknown if under 18 years of age and over 18 years of age will be reported separately |
Park 2017.
| Methods | RCT (parallel) Study design: Evaluator‐blind Sample size calculation: Yes Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparisons for outcomes: Yes Duration of follow‐up: None Time points of measurements: weeks 4, 8, 12, 16 Location: Department of Dermatology, Chung‐Ang University Hospital, Seoul, Korea |
| Participants | Total n: 128 Age: > 19 years of age Sex: Men and women (ratio unknown) Inclusion criteria: Men and women over 19 years of age, with onychomycosis confirmed with positive KOH smear Exclusion criteria: History of photosensitivity, allergic reaction to amorolfine, other prediagnosed nail disorders such as nail psoriasis, breastfeeding/pregnancy, or undergoing topical/systemic antifungal agent or laser treatments within 12 weeks before the study Disease duration: Unknown Comparable at baseline: Yes Causative species: dermatophytes Number of people lost to follow‐up: None Participant enrollment: May 2014 ‐ March 2015 |
| Interventions | Treatment in study arm 1: 1064‐nm Nd:YAG laser treatment, once every 4 weeks for 4 treatments, and concurrent amorolfine 5% nail lacquer once a week for 16 weeks, n = 64 Drug in study arm 2: 5% amorolfine nail lacquer once a week for 16 weeks, n = 64 |
| Outcomes | Mycological cure: negative KOH and culture at 16 weeks Cumulative cure: clinically normal nail or negative mycology with < 10% nail plate involvement at 16 weeks Change in lesion‐free area (%) from baseline at 16 weeks Participant satisfaction on a 5‐point Likert scale at 16 weeks Adverse events: reported |
| Notes | Toenails alone unknown |
Ramm 1994.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Abstract and full text not available |
Rüping 1993a.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Rüping 1993b.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Abstract and full text not available |
Schubert 1973.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Weuta 1972.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable |
Xu 2017.
| Methods | ‐ |
| Participants | ‐ |
| Interventions | ‐ |
| Outcomes | ‐ |
| Notes | Article not in English and unavailable. To be assessed for inclusion/exclusion in an update to the review. Added to review as part of updated literature search during review process |
Yao 2016.
| Methods | RCT: Yes Study design: unknown Diagnosis mycology: Unknown Big toenail specified: No Duration of follow‐up: 9 months Time points of measurements: 13 months Location: unknown |
| Participants | Total n: 60 Age: exact ages unknown, described as "middle and aged" Sex: Unknown Inclusion/exclusion criteria: Unknown Number of participants lost to follow‐up: Unknown Trial duration: unknown |
| Interventions | Treatment duration: 4 months Treatment in study arm 1: Fufang Tujin Piding topical twice daily with 1064‐nm Nd:YAG laser once weekly, n = 30 Treatment in study arm 2: 1064‐nm Nd:YAG laser once weekly, n = 30 |
| Outcomes | Clinical efficacy 9 months following treatment Mycological efficacy 9 months following treatment Adverse events: not reported |
| Notes | Conference abstract. Cannot assess eligibility as does not state whether study investigates fingernail, toenails, or both and does not state how onychomycosis was diagnosed |
KOH: potassium hydroxide.
Characteristics of ongoing studies [ordered by study ID]
ACTRN12618000131257.
| Trial name or title | Phase 1, first in human (FIH), randomised, double‐blind, placebo‐controlled multiple ascending dose study in healthy volunteers with mild‐to‐moderate onychomycosis |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and/or culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 52 weeks Time points of measurement: 3, 6, 12 months |
| Participants | Total n: 48 Age: 18 ‐ 65 years old Sex: Men and women (ratio unknown) Inclusion criteria: Men and women, 18 to 65 years of age inclusive, diagnosed with onychomycosis of the great toenail, involving at least 20%, but not more than 70% of nail involvement, confirmed by mycological staining or culture or both, thickness of distal nail plate < 3 mm, medically healthy, negative urine drug screen/alcohol breath test at screening and day 1, BMI of 17.5 ‐ 35 inclusive, use of double barrier contraception during the study and for 1 month (women) and 3 months (men) after the study or surgical sterilisation at least 6 months prior to screening or abstinence, men must not donate sperm for at least 3 months after the last drug dose, partners of all participants must use contraception, not be pregnant, or be post‐menopausal Exclusion criteria: History of allergy to any of the excipients in HXP124, positive test for HIV, hepatitis B surface antigen, hepatitis C antibodies, underlying conditions that prevent compliance (investigator's discretion), pregnancy or lactation, unwillingness to refrain from nail cosmetics during study, administration of another trial's product within 30 days of study, diabetes mellitus requiring treatment other than diet/exercise, not adhering to washout periods or concurrent use during study of topical antifungals applied to feet (washout: 4 weeks) apart from that for tinea pedis or anti‐inflammatories, corticosteroids, and topical immunomodulators (washouts: 2 weeks), not adhering to washout periods or concurrent use during study of systemic corticosteroids (washout: 2 weeks) or systemic antifungals with known activity against dermatophytes (washout: 12 weeks), use of systemic immunomodulators in the past 4 weeks, nail or anatomic abnormalities of the toe Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: once daily for 42 days Cohort 1: HXP124, 5 mg/mL, n = 4; Placebo, n = 2 Cohort 2: HXP124, 10 mg/mL, n = 4; Placebo, n = 2 Cohort 3: HXP124, 20 mg/mL, n = 4; Placebo, n = 2 Cohort 4: HXP124, n = 24; Placebo, n = 6 (dose for cohort 4 depends on results in cohorts 1 ‐ 3) |
| Outcomes | Mycological cure: negative KOH and culture at days 14, 42, 63, and 84 following the first dose Clinical appearance (photographs), including length and surface area of clear nail growth at days 7, 14, 42, 63, 84 following the first dose, plus day 365 for cohort 4 Safety and tolerability: vital signs and adverse events prior to first dose, and 0.5, 1, 3, 5, 7, 10, 15, and 24 hours, and day 3, 7, 14, 42, 63, and 84 following dosing, plus day 365 for cohort 4; physical exam and ECG prior to first dose, and 24 hours (exam only), day 3, 7, 14, 42, 63, and 84 after dosing; pain, erythema, and irritation assessment prior to first dose, and 60 mins, 4 hours (cohort 4), 7 and 24 hours (cohorts 1 ‐ 3), and on day 3, 7, 14, 42, 63, and 84 after first dose; blood collected prior to first dose and on day 7, 14, 42, 63, and 84 after first dose Pharmacokinetic parameters: Blood samples collected prior to first dose, and 0.5, 1, 3, 5, 7, 10, 15, and 24 hours (cohorts 1 ‐ 3) and day 3, 7, 14, and 42 following the first dose Adverse events: not reported |
| Starting date | Date of first participant enrolment 22 January 2018 |
| Contact information | Liisa Bevan, Linear Clinical Research Australia lbevan@linear.org.au |
| Location | QEII Medical Centre, Nedlands, WA, Australia |
| Notes | Recruiting, Estimated study completion 19 May 2019, Last updated on 14 February 2018 |
ChiCTR‐INR‐17013504.
| Trial name or title | 2940‐nm Er:YAG fractional laser combined with amorolfine hydrochloride and amorolfine hydrochloride for treating onychomycosis: a prospective, randomised, controlled, evaluator‐blinded, parallel‐group clinical trial |
| Methods | RCT (parallel) Study design: Single blind Sample size calculation: Unknown Diagnosis mycology: microscopy Big toenail specified: No Statistical comparisons for outcomes: Unknown Duration of follow‐up: 12 weeks Time points of measurement: 12 weeks |
| Participants | Total n: 266 Age: 18 ‐ 65 years old Sex: Men and women (ratio unknown) Inclusion criteria: Men and women, 18 to 65 years of age, diagnosed with onychomycosis, confirmed by clinical symptoms and positive fungal microscopy, an onychomycosis severity index score of > 1, and effective contraception for women of childbearing age during the trial period Exclusion criteria: Known history of allergy to romero liniment, severe immunosuppression or use of systemic glucocorticoids and immunosuppressive agents within 3 months, severe heart, liver, or kidney disease, severe neurological or mental illness, poorly‐controlled diabetes, antifungal use within last 3 months, women planning to conceive or unwilling to use contraception, history or drug abuse, clinical trial participation within 3 months Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown |
| Interventions | Intervention in study arm 1: 2940‐nm Er:YAG fractional laser combined with amorolfine hydrochloride, n = 133 Intervention in study arm 2: amorolfine hydrochloride, n = 133 |
| Outcomes | Mycological cure at 12 weeks Adverse events: not reported |
| Starting date | 01 January 2018 |
| Contact information | Sun Yat‐sen Memorial Hospital of Sun Yat‐sen University |
| Location | Sun Yat‐sen Memorial Hospital of Sun Yat‐sen University, Guangzhou, Guangdong, China |
| Notes | Ongoing. Estimated study completion December 2019, Last update 23 November 2017 |
DRKS00007709.
| Trial name or title | Treatment of onychomycosis with a short‐pulsed Nd:YAG laser (1064 nm) |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: Culture and PCR Big toenail specified: No Statistical comparisons for outcome: Unknown Duration of follow‐up: At 3 months Time points of measurements: Month 3 |
| Participants | Total n: 15 Age: 18 ‐ 90 years old Sex: Unknown Inclusion criteria: Both genders, aged 18 ‐ 90 years old with onychomycosis of toenail, positive fungal culture, positive PCR, legal age and written agreement Exclusion criteria: Oral or topical anti‐fungal agents in the preceding 6 months, non‐compliance, pregnancy, women of childbearing age or lactation and use of a legal carer Disease duration: Unknown Comparable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: Laser treated 4 times for 4 ‐ 6 weeks and applied once daily creme for 12 months Treatment in study arm 1: Short‐pulsed Nd:YAG Laser‐treatment and amorolfin creme, study control, n = unknown Drug in study arm 2: Amorolfin creme, study duration and control, n = unknown |
| Outcomes | Clinical cure at month 3 Mycological cure (fungal culture and PCR) at month 3 Adverse events: not reported |
| Starting date | Date of registration in DRKS: 20 January 2015 |
| Contact information | Address: Laserklinik Karlsruhe Kaiserstrasse 104 76133 Karlsruhe Germany Primary sponsor URL: www.raulin‐und‐kollegen.de |
| Location | Laserklinik Karlsruhe Kaiserstrasse 104 76133 Karlsruhe Germany |
| Notes | Investigator‐initiated trial, no commercial funding |
EUCTR2016‐001204‐39.
| Trial name or title | A multi‐centre, randomised, two‐armed, parallel group and evaluator‐blinded study of efficacy and safety of topical MOB015B in the treatment of mild‐to‐moderate distal subungual onychomycosis (DSO) |
| Methods | RCT Study design: Single blind Sample size calculation: Unknown Diagnosis mycology: Culture Big toenail specified: Yes Statistical comparisons for outcome: Unknown Duration of follow‐up: Unknown Time points of measurements: Visit 1 ‐ 7 |
| Participants | Total n: 406 Age: n = 366 18 ‐ 64 years old; n = 40; > 65 years old Sex: Unknown Inclusion criteria: Men or women 18 – 75 years of age (inclusive) at the time of Informed consent, DSO of at least one of the great toenail(s) affecting 20% to 60% of the target nail, positive culture for dermatophytes, signed written informed consent (ICF) prior to any study‐related activity Exclusion criteria: PSO, DSO of both great toenails where involvement has extended into the proximal portion of the target nail (unaffected proximal nail is < 3 mm), target toenail thickness more than 3 mm, 'spike' of onychomycosis extending to eponychium of the target toenail, presence of dermatophytoma (defined as thick masses of fungal hyphae and necrotic keratin between the nail plate and nail bed) on the target nail, other conditions than DSO known to cause abnormal nail appearance, presence of toenail infection other than dermatophytes, previous target toenail surgery with any residual disfigurement, topical treatment of the nails with other antifungal medication or medical device within 6 weeks before Screening/Visit 1, systemic use of antifungal treatment within 6 months before Screening/Visit 1, severe moccasin tinea pedis, signs of severe peripheral circulatory insufficiency, uncontrolled diabetes mellitus (blood glucose not adjusted to stable levels despite antidiabetic therapy and/or careful medical monitoring by the family physician/specialist is not ensured), known immunodeficiency, i.e. congenital immunodeficiency, acquired immunodeficiency (e.g. HIV, some bone marrow diseases, extreme diets), iatrogenic by immunosuppressive drugs like cytostatics or by radiation therapy or immunomodulatory medications (e.g. TNF inhibitors), participation in another clinical trial with an investigational drug or device during the previous 3 months before Baseline/Visit 2, known allergy to any of the tested treatment products, a positive pregnancy test indicating pregnancy in a woman of childbearing potential at Baseline/ Visit 2, women who are pregnant or breastfeeding, pre‐menopausal (last menstruation ≤ 1 year prior to screening) sexually active women who: are of childbearing potential and are not practising an acceptable method of birth control, or do not plan to continue practising an acceptable method of birth control throughout the trial, people previously randomised in this study, history of, or current drug or alcohol abuse, psychiatric condition that might limit the participation in the study and/or that lead to the assumption that the person’s ability to completely understand the consequences of consent is missing, close affiliation with the investigator (e.g. a close relative) or persons working at a study site, or person who is an employee of the sponsor’s company, people who are institutionalised because of legal or regulatory order, any diseases or circumstances in which the person should not participate in the study in the opinion of the investigator Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: Applied for 52 weeks Drug in study arm 1: MOB015B (terbinafine‐hydrochloride 10%), n = unknown Drug in study arm 2: MICLAST® (Ciclopirox 80 mg/g), n = unknown |
| Outcomes | Complete cure (culture and KOH) at week 52 Mycological cure (culture and KOH) at visit 3, 4, 5, 6 and 7 'Completely clear' or 'almost clear' (0% ‐ 10% clinical disease involvement of the target nail) at visit 3, 4, 5, 6 and 7 Adverse events: not reported |
| Starting date | 15 September 2016 |
| Contact information | Name of organisation: Moberg Pharma AB (publ) Address: Gustavslundsvägen 42, 5tr., Bromma, 16751, Sweden Phone: +46852230711 Fax number: +4687352029 Email: christin.strid@mobergpharma.se |
| Location | Sweden (city/institution unknown) |
| Notes | Industry‐sponsored trial Email response: The study has not been completed yet |
EUCTR2016‐003784‐19.
| Trial name or title | Phase III, multicentre, randomised, double‐blind, parallel‐group, clinical trial to evaluate the efficacy and safety of a new medicated nail lacquer for the treatment of toenail fungal infection |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 52 weeks Time points of measurements: At week 48 and 52 |
| Participants | Total n: 360 Age: 18 ‐ 70 Sex: Men and women (ratio unknown) Inclusion criteria: Adults 18 ‐ 70 years of age diagnosed with mild‐to‐moderate dermatophyte onychomycosis (20% ‐ 60% inclusive nail involvement) of at least one big toenail with no lunula involvement. Dermatophytes confirmed with positive KOH and positive culture Exclusion criteria: Allergy to medications used, life expectancy < 2 years at screening, pregnancy or breastfeeding, unwillingness to stop nail polish, unwillingness to use contraception, systemic antifungal use 6 months prior to screening, topical antifungal use 4 weeks prior to screening, chemotherapy or immunosuppressive therapy in the 12 weeks prior to screening, systemic glucocorticoids, antimetabolites, or immunostimulants in the 4 weeks prior to screening or the need for any of these. Presence of psoriasis, uncontrolled diabetes mellitus, suspicion or evidence of severe liver or kidney disease, alcohol or substance abuse, AIDS or any other immunodeficiency. Onychomycosis caused by yeasts or non‐dermatophyte moulds, mucocutaneous candidiasis, white superficial onychomycosis, proximal subungual involvement, yellow spikes on nails. Recurrent erysipela at screening, any other medical condition that the investigator determines contraindicates participation. Participation in any clinical investigation with medicine within the last 6 months prior to screening Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: 48 weeks Drug in study arm 1: RJ‐0265 cutaneous liquid, n = unknown Drug in study arm 2: Ciclopirox 8%, n = unknown Drug in study arm 3: Placebo liquid, n = unknown |
| Outcomes | Complete cure at week 52 Clinical success, responder, and improvement at week 52 Negative culture at week 52 Negative KOH at week 52 Adverse events over 52 weeks Growth rate of healthy nail at 52 weeks Time in months to complete cure or clinical success |
| Starting date | Unknown |
| Contact information | Name: Jordi Picas Email: Jordi.Picas@reigjofre.com Laboratorio Reig Jofre, SA Spain |
| Location | Laboratorio Reig Jofre, SA, Sant Joan Despi, Barcelona, Spain |
| Notes | Industry‐sponsored trial. Study record updated 20 June 2017, status is ongoing |
JapicCTI‐183840.
| Trial name or title | A phase 2, multicenter, randomised, double‐blind, vehicle‐controlled, parallel‐group study to investigate the efficacy and safety of ME1111 for 48 weeks of treatment in patients with mild‐to‐moderate onychomycosis |
| Methods | RCT (parallel) Study design: Unknown Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: Yes Statistical comparisons for outcomes: Unknown Duration of follow‐up: 4 weeks Time points of measurement: 52 weeks |
| Participants | Total n: 240 Age: 20 ‐ 70 years old Sex: Men and women (ratio unknown) Inclusion criteria: Men and women, 20 to 70 years of age inclusive, diagnosed with mild‐to‐moderate onychomycosis of at least 1 great toenail, with 20% ‐ 50% nail involvement confirmed by positive fungal microscopy and culture for a dermatophyte, no more than 6 affected toenails as determined by visual inspection Exclusion criteria: History of allergy to components of the solution product (including alcohol), underlying uncontrolled disease at discretion of investigator (e.g. cardiovascular disease, liver disease, pulmonary disease, blood disease, etc.), uncontrolled diabetes mellitus, any antifungal treatment, laser, or other therapy for onychomycosis within 24 weeks of study drug administration, unsuccessful attempts at previous antifungal treatment for onychomycosis, unwilling to refrain from topical antifungals for tinea pedis, nail or anatomic abnormalities, presence of history of psoriasis, chronic moccasin type tinea pedis, immunodeficiencies (HIV), women who are nursing, pregnant, planning pregnancy, or men with plans to have partners become pregnant Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown |
| Interventions | Drug in study arm 1: ME1111 solution, once a day for 48 weeks Drug in study arm 2: Vehicle solution, once a day for 48 weeks Drug in study arm 3: Efinaconazole, once a day for 48 weeks |
| Outcomes | Mycological cure at 12 weeks Adverse events: not reported |
| Starting date | February 2018, recruiting |
| Contact information | Meiji Seika Pharma Co. Ltd., clinical_trials@meiji.com |
| Location | Japan (city/institution unknown) |
| Notes | Ongoing, last updated 5 December 2018 |
NCT02644551.
| Trial name or title | The efficacy of CELEXT07 in the treatment of toenail onychomycosis: a phase 2, randomised, double‐blind study |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparison for outcome: Unknown Duration of follow‐up: Unknown Time points of measurement: At week 52 |
| Participants | Total n: 120 Age: 18 years and older Sex: Unknown Inclusion criteria: Age > 18, clinically diagnosed onychomycosis of the target nail, presence of mild‐to‐moderate onychomycosis, defined as 20% ‐ 50% of the area of the target nail being clinically affected, has a positive KOH examination from the target nails, has a positive dermatophyte culture from the target nail, written informed consent obtained, participant agreed to follow the protocol Exclusion criteria: Presence of any disease or condition that might cause nail abnormalities or may interfere with the evaluation of the study drug, use of any systemic antifungal therapy within 4 weeks prior to the Screening visit or non‐responsive to systemic antifungal therapy for onychomycosis, use of any prescription or over‐the‐counter topical antifungal therapy for the toenails within 4 weeks prior to the screening visit, woman who is pregnant, nursing an infant, or planning a pregnancy during the study period Inability to understand and comply with the instructions of the study, people less than age 18, individuals with known allergy/hypersensitivity to Thuja occidentalis, Chelidonium majus, Eucalyptus citriodora, Tea tree or Thymus vulgaris Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: Once daily for 52 weeks Drug in study arm 1: CELEXT07, n = unknown Drug in study arm 2: Vehicle solution, n = unknown Drug in study arm 3: Ciclopirox, n = unknown |
| Outcomes | Complete cure at week 52 Mycological cure (microscopy and culture) at week 52 Adverse events: not reported |
| Starting date | November 2016 |
| Contact information | Principal investigator: Céline Devaux, MD, FRCPC 9305‐9954 Quebec Inc Study director: Guy Chamberland, M.Sc., Ph.D. 9305‐9954 Quebec Inc Names: Wil Lee, DPM, AACFAS Address: Clinique podiatrique de Montréal Recruiting Montreal, Quebec, Canada, H1X 2B3 Phone: 514 254‐5000 Email: drwlee@hotmail.com Sponsors and Collaborators 9305‐9954 Quebec Inc |
| Location | Clinique podiatrique de Montréal, Montréal, Quebec, Canada |
| Notes | Study record updated 26 April 2017, status is recruiting |
NCT02812043.
| Trial name or title | Comparison of the efficacy and safety between long‐pulsed Nd:YAG, amorolfine and combination of long‐pulsed Nd:YAG and amorolfine in treating non‐dermatophyte and mixed‐infection onychomycosis |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: KOH and culture Big toenail specified: No Statistical comparisons for outcome: Unknown Duration of follow‐up: At 6 months Time point of measurement: Months 1, 2, 3, 4 and 6 |
| Participants | Total n: 60 Age: aged more than 18 years old Sex: Unknown Inclusion criteria: People aged more than 18 years old, diagnosed with non‐dermatophytes or mixed‐infection onychomycosis from both KOH examination and fungal cultured, without any prior anti‐fungal treatment within 6 months, no use of vasodilator drugs or isotretinoin within 6 months, willing to participate, and accepting the methods and risk Exclusion criteria: People with other medical dermatologic condition associated with onychomycosis such as psoriasis, paronychia etc, people on immunosuppressive drugs, or the immunocompromised host, people with severe vascular disease, such as severe DVT, or poor capillary refill time, people with onychomycosis which involved in nail matrix, pregnancy or lactation, problems in communication or difficulty travelling to the faculty for the checkup Disease duration: Unknown Comparable at baseline: Unknown Causative species: Non‐dermatophyte or mixed‐infection Number of people lost to follow up: Unknown |
| Interventions | Treatment duration: Laser had 2 passes each visit with 4‐week intervals, amorolfine was applied once a week for 6 months Drug in study arm 1: Amorolfine nail lacquer, n = unknown Drug in study arm 2: Long‐pulsed 1064nm, n = unknown Drug in study arm 3: Long‐pulsed 1064nm and amorolfine, n = unknown |
| Outcomes | Mycological cure (negative culture) at months 1, 2, 3, 4, and 6 Adverse events: not reported |
| Starting date | August 2016 |
| Contact information | Name: Charussri Leeyaphan, MD Department of Dermatology Siriraj Hospital Bangkoknoi, Bangkok, Thailand, 10700 Phone: 6624194333 Email: charussrilee@gmail.com Sponsors and Collaborators Mahidol University |
| Location | Department of Dermatology Siriraj Hospital, Bangkoknoi, Bangkok, Thailand |
| Notes | Supported by academic institution. Recruiting, estimated completion date December 2019. Last update 8 March 2019 |
NCT02859519.
| Trial name or title | A multi‐centre, double‐blind, randomised, vehicle‐controlled study of efficacy and safety of topical MOB015B in the treatment of mild‐to‐moderate distal subungual onychomycosis (DSO) |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: Unknown Diagnosis mycology: Culture Big toenail specified: Yes Statistical comparison for outcomes: Unknown Duration of follow‐up: Unknown Time points of measurements: Weeks 52 |
| Participants | Total n: Unknown Age: 12 ‐ 70 years old Sex: Unknown Inclusion criteria: Men or women 12 ‐ 70 years of age, DSO of at least 1 of the great toenail(s) affecting 20% to 50% of the target nail, positive culture for dermatophytes, written informed consent Exclusion criteria: PSO, DSO of both great toenails where involvement has extended into the proximal portion of the target nail (unaffected proximal nail is < 3 mm), target toenail thickness > 3 mm, 'Spike' of onychomycosis extending to eponychium of the target toenail, presence of dermatophytoma (defined as thick masses of fungal hyphae and necrotic keratin between the nail plate and nail bed) on the target nail, other conditions than DSO known to cause abnormal nail appearance, presence of toenail infection other than dermatophytes, previous target toenail surgery with any residual disfigurement, topical treatment of the nails with other antifungal medication within 1 month before Baseline/Visit 2, systemic use of antifungal treatment within 7 months before Baseline/Visit 2, severe moccasin tinea pedis, signs of severe peripheral circulatory insufficiency, uncontrolled diabetes mellitus, known immunodeficiency, participation in another clinical trial with an investigational drug or device during the previous 3 months before Baseline/Visit 2, known allergy to any of the tested treatment products, a positive pregnancy test at Baseline/Visit 2 indicating pregnancy in a woman of childbearing potential or a premenarche woman, women who are pregnant or breastfeeding, men who have female sexual partners of child‐bearing potential and sexually active women of child‐bearing potential who are not practising an acceptable method of birth control, or who will not remain abstinent through the trial, people previously randomised in this study, history of, or current drug or alcohol abuse, psychiatric condition that might limit the participation in the study and/or that lead to the assumption that the person's ability to completely understand the consequences of consent is missing, close affiliation with the investigator (e.g. a close relative) or persons working at a study site, or person who is an employee of the sponsor's company, people who are institutionalised because of legal or regulatory order, any diseases or circumstances in which the person should not participate in the study in the opinion of the investigator Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: For 52 weeks Drug in study arm 1: MOB015B, n = unknown Drug in study arm 2: MOB015B Vehicle, n = unknown |
| Outcomes | Complete cure at 52 weeks Adverse events: not reported |
| Starting date | October 2016 |
| Contact information | Name: Kjell Rensfeldt, MD Phone: +46 8 522 307 00 Email: kjell.rensfeldt@mobergpharma.se Name: Anna Hill, MSc Phone: +46 8 522 307 00 Email: anna.hill@mobergpharma.se USA and Canada Sponsors and Collaborators Moberg Pharma AB |
| Location | United States, multiple sites in California, Florida, Idaho, Illinois, Minnesota, New Jersey, Oregon, Texas, and Virginia Canada, multiple locations Cities/institutions unknown |
| Notes | Active, last update posted 22 October 2018. Estimated completion date February 2020 |
NCT02866032.
| Trial name or title | A multi‐centre, randomised, two‐armed, parallel group and evaluator‐blinded study of efficacy and safety of topical MOB015B in the treatment of mild‐to‐moderate Distal Subungual Onychomycosis (DSO) |
| Methods | RCT (parallel) Study design: Single blind Sample size calculation: Unknown Diagnosis mycology: Culture Big toenail specified: Yes Statistical comparison for outcomes: Unknown Duration of follow‐up: Unknown Time points of measurement: Weeks 52 |
| Participants | Total n: Unknown Age: 18 ‐ 70 years old Sex: Unknown Inclusion criteria: Men or women 18 ‐ 70 years of age, DSO of at least 1 of the great toenail(s) affecting 20% to 50% of the target nail, positive culture for dermatophytes, signed written informed consent Exclusion criteria: PSO, DSO of both great toenails where involvement has extended into the proximal portion of the target nail (unaffected proximal nail is < 3 mm), target toenail thickness more than 3 mm, 'Spike' of onychomycosis extending to eponychium of the target toenail, presence of dermatophytoma (defined as thick masses of fungal hyphae and necrotic keratin between the nail plate and nail bed) on the target nail, other conditions than DSO known to cause abnormal nail appearance, presence of toenail infection other than dermatophytes, previous target toenail surgery with any residual disfigurement, topical treatment of the nails with other antifungal medication or medical device within 1 month before Baseline/Visit 2, systemic use of antifungal treatment within 7 months before Baseline/Visit 2, severe moccasin tinea pedis, signs of severe peripheral circulatory insufficiency, uncontrolled diabetes mellitus, known immunodeficiency, participation in another clinical trial with an investigational drug or device during the previous 3 months before Baseline/Visit 2, known allergy to any of the tested treatment products, a positive pregnancy test indicating pregnancy in a woman of childbearing potential at Baseline/Visit 2, women who are pregnant or breastfeeding, pre‐menopausal (last menstruation ≤ 1 year prior to screening) sexually active women who are of childbearing potential and are not practising an acceptable method of birth control, or do not plan to continue practising an acceptable method of birth control throughout the trial, people previously randomised in this study History of, or current drug or alcohol abuse, psychiatric condition that might limit the participation in the study and/or that lead to the assumption that the person's ability to completely understand the consequences of consent is missing, close affiliation with the investigator (e.g. a close relative) or persons working at a study site, or person who is an employee of the sponsor's company, people who are institutionalised because of legal or regulatory order, any diseases or circumstances in which the person should not participate in the study in the opinion of the investigator Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophytes Number of people lost to follow up: Unknown |
| Interventions | Treatment duration: For 52 weeks Drugs in study arm 1: MOB015B, n = unknown Drugs in study arm 2: Ciclopirox 80 mg/g, n = unknown |
| Outcomes | Complete cure for 52 weeks Adverse events: not reported |
| Starting date | September 2016 |
| Contact information | Name: Kjell Rensfeldt, MD
Phone: +46 8 522 307 00
Email: kjell.rensfeldt@mobergpharma.se Name: Christin Strid, MSc Phone: +46 8 522 307 00 Email: christin.strid@mobergpharma.se Germany and Poland Sponsors and Collaborators Moberg Pharma AB |
| Location | Multiple locations in Germany, Poland, and the United Kingdom (cities/institutions unknown) |
| Notes | Active, last update posted 28 March 2019. Estimated completion date September 2020 |
NCT02961634.
| Trial name or title | Study efficacy and safety in comparative use of investigational product adjuvant treatment in onychomycosis |
| Methods | RCT (parallel) Study design: Single blind Sample size calculation: Unknown Diagnosis mycology: Culture Big toenail specified: No Statistical comparisons for outcome: Unknown Duration of follow‐up: Unknown Timr points for measurement: At days 45 and 90 |
| Participants | Total n: 46 Age: 18 ‐ 65 years old Sex: Unknown Inclusion criteria: Volunteers of both sexes, aged 18 ‐ 65 years, with onychomycosis confirmed by positive direct mycological nail of hands or feet, agreement to comply with the test procedures and attend the clinic on the days and times for certain applications or assessments or both, understand, consent and sign the "Instrument of Consent of Clarified" Exclusion criteria: Pregnancy or risk pregnancy/lactation, use of anti‐inflammatory/immunosuppressive drugs (in the last 30 days and during the study), concomitant nail pathologies (psoriasis, lichen planus, etc.), systemic conditions that may compromise the growth of the nail (vascular disease, diabetes, etc.), irritation. History of similar products to the investigational product, treatment with antifungal medication prior to the study (up to 12 weeks for systemic medications and topical medications for 4 weeks), other conditions considered by the investigator physician as reasonable for the disqualification of the individual's participation in the study Disease duration: Unknown Comaprable at baseline: Unknown Causative species: Unknown Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: Twice daily, morning and night for 30 days, ciclopirox every other day for 1 month, twice a week for a month and once a week for a month
Drug in study arm 1: Nailner 2 in 1 and Ciclopirox 8%, n = unknown Drug in study arm 2: Ciclopirox 8%, n = unknown |
| Outcomes | Mycological cure (culture) at days 45 and 90 Adverse events: not reported |
| Starting date | April 2017 |
| Contact information | Name: Ana Carolina Prazias Massei Phone: +55(16)3624‐4056 Email: carolina.prazias@mipbrasilfarma.com.br Sponsors and Collaborators MIP Brasil Indústria e Comércio de Produtos Farmacêuticos LTDA Buranello e Rodrigues Consultoria em Desenvolvimento Farmacêutico Ltda ME |
| Location | Unknown |
| Notes | Industry provided financial support. Study record updated 31 March 2017, status is not yet recruiting |
NCT03098342.
| Trial name or title | Comparison of efficacy and safety between methylene blue‐mediated photodynamic therapy and 5% amorolfine nail lacquer for toenail onychomycosis treatment in Asians |
| Methods | RCT (parallel) Study design: Single blind Sample size calculation: Unknown Diagnosis mycology: Culture, KOH, PAS and/or GMS Big toenail specified: Unknown Statistical comparisons for outcomes: Unknown Duration of follow‐up: 18 months. Time points of measurements: At weeks 2, 4, 6, 8, 10, 12, 20, 28, 36, 44, 52, 60, 68, 76 |
| Participants | Total n: 42 Age: 18 ‐ 90 years old Sex: Unknown Inclusion criteria: Adults, aged between 18 and 90 years, with distal and lateral subungual toenail onychomycosis diagnosed clinically and mycologically clinical signs of onychomycosis as following: discolouration, dystrophy of nail plate, subungual hyperkeratosis Onycholysis confirmed by: positive culture of dermatophyte or non‐dermatophyte (must be isolated from sequential specimens) and/or positive microscopic evidence, any of these methods, direct microscopy (KOH preparation), nail plate culture on Sabouraud's dextrose agar (SDA), histopathological examination of nail clippings using PAS staining (HPE‐PAS), histopathological examination of nail clippings using GMS staining (HPE‐GMS), polymerase chain reaction Exclusion criteria: Those with nail changes because of skin disease or associated systemic diseases, pregnancy or lactating women, those who are allergic to amorolfine, methylene blue, those who are photosensitive to visible light, those who had previously used anti‐fungal medications within 3 months for systemic and 1 month for topical therapy Disease duration: Unknown Comparable at baseline: Unknown Causative species: Dermatophyte Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: 6 treatments, 15 days between each sessions or lacquer applied daily Drug in study arm 1: Methylene blue‐mediated photodynamic therapy, n = unknown Drug in study arm 2: Amorolfine 5% nail lacquer, n = unknown |
| Outcomes | Onychomycosis severity index (OSI) change from baseline at weeks 2, 4, 6, 8, 10, 12, 20, 28, 36, 44, 52, 60, 68, and 76 Adverse events: not reported |
| Starting date | 1 June 2017 |
| Contact information | Name: Nutthamon Bowornsathitchai, M.D. Phone: 66818239488 Email: bee_o_bo@hotmail.com King Chulalongkorn Memorial Hospital Bangkok, Thailand, 10330 Sponsors and Collaborators Chulalongkorn University, King Chulalongkorn Memorial Hospital |
| Location | King Chulalongkorn Memorial Hospital Bangkok, Thailand |
| Notes | Study record updated 31 March 2017, status is not yet recruiting |
NCT03814343.
| Trial name or title | Comparison of effectiveness of topical amphotericin B in 30% dimethylsulphoxide (DMSO) and 30% DMSO in treating non‐dermatophytes onychomycosis: Randomised double‐blind controlled trial pilot study |
| Methods | RCT (parallel) Study design: Double blind Sample size calculation: No Diagnosis mycology: Culture Big toenail specified: Unknown Statistical comparisons for outcomes: Unknown Duration of follow‐up: 36 weeks Time points of measurements: At week 36 |
| Participants | Total n: 20 Age: 18 years and older. Sex: Men and women (ratio unknown) Inclusion criteria: Adults 18 years of age and older diagnosed with non‐dermatophyte onychomycosis and have not been treated with any oral/IV/topical antifungal therapy within 36 weeks before enrolled Exclusion criteria: People with dermatophyte onychomycosis, immunocompromisation, or concomitant nail diseases Disease duration: Unknown Comparable at baseline: Unknown Causative species: Non‐dermatophytes Number of people lost to follow‐up: Unknown |
| Interventions | Treatment duration: 12 weeks Drug in study arm 1: Amphotericin B in 30% DMSO, n = 10 Drug in study arm 2: Placebo (30% DMSO), n = 10 |
| Outcomes | Mycological cure at 36 weeks Clinical cure (complete clinical improvement or < 10% nail involvement) at 36 weeks Adverse events over 12 weeks Median time to mycological and clinical cure |
| Starting date | 15 January 2019 |
| Contact information | Name: Dr. Charussri Leeyaphan, M.D. Email: charussrilee@gmail.com Department of Dermatology, Siriraj Hospital Bangkoknoi, Bangkok, Thailand |
| Location | Department of Dermatology, Siriraj Hospital Bangkoknoi, Bangkok, Thailand |
| Notes | Study record updated 29 January 2019, status is recruiting |
BMI: body mass index; DSO: distal subungual onychomycosis; GMS: KOH: potassium hydroxide; PAS: periodic acid‐Schiff; PCR: polymerase chain reaction; PSO: proximal subungual onychomycosis; RCT: randomised controlled trial.
Differences between protocol and review
Types of interventions. The protocol did not include 'vehicle' as a comparator in the inclusion criteria. This was added to the intervention review. This was a simple oversight on the part of the authors, as vehicle should have been included in the protocol. Commonly, placebo and vehicle are used interchangeably but they are different. For reference, placebo has no pharmacological activity (e.g. sugar pill) whereas a vehicle is meant to be similar to the drug formulation in ingredients, with the exception that the active drug is not included in the vehicle.
Data collection and analysis. In the protocol, authors FS, DD, DL, and MP were designated as the individuals that would select studies, perform data extraction and management, and evaluate risks of bias. These authors were unavailable to continue working on the intervention review and were replaced with authors KF, RM, and SV.
Assessment of risk of bias in included studies. Assessment of other potential sources of bias was not included in the protocol and is assessed in the review. We assessed other bias in the review because it was included in the RevMan 'Risk of bias' tool. We used this domain to assess whether there was selective reporting of subgroups and whether multiple intervention trials reported outcomes for all study arms, as suggested in Chapter 16 of the Cochrane Handbook (Higgins 2011).
Measures of treatment effect. In the protocol, we stated that continuous outcomes would be analysed as a mean difference (MD) with a 95% CI. In the review, we did not do this because there were no continuous data to analyse. In the protocol, we stated that time to recurrence would be measured using the hazard ratio and standard errors collected from Cox proportional hazards models. In the review, we did not do this because time to recurrence data were not reported in included studies.
Unit of analysis issues. The protocol did not address studies with multiple intervention arms. We added to the review "Where studies had multiple intervention arms, all arms are mentioned in the Characteristics of included studies table." The protocol states, "The participant was the unit of analysis, with clinical trials designating one target toenail per participant as the unit of analysis. We did not consider nail data in clinical studies that used individual nails as the unit of analysis, including multiple toenails per participant in their data set." The review still states this, with the addition "The exception to this was in the case of studies where multiple toenails per participant were included if outcomes were reported per participant." This was done so that device studies, specifically laser, could be eligible for inclusion in the review.
Assessment of heterogeneity. We originally planned not to report meta‐analyses for comparisons where I2 is greater than 75%. We decided not to do this because I2 thresholds are guidelines and it was important to show all of the data. Instead, the large heterogeneity was explicitly addressed in the Results section for each comparison where it was present and explanations provided as to why the heterogeneity could have been large. Where possible, we performed a sensitivity analysis to determine if removing studies would affect the heterogeneity and this is also reported in the Results section. Lastly, we downgraded the quality of evidence for inconsistency when heterogeneity was large.
Data synthesis. There were no continuous data to analyse in this review. Thus we did not calculate mean differences (continuous data) using the inverse‐variance model. The protocol did not identify how studies with multiple interventions arms would be handled. We therefore added to the review "For studies with multiple intervention arms, the relevant interventions were identified. Where possible, intervention arms were combined so that a single comparison was included in the meta‐analysis. When this was not possible, the relevant intervention arms were used in the analysis and identified in the footnotes of the forest plot". We originally planned to conduct meta‐analyses for comparisons where there were at least three studies ("Where meta‐analysis is possible (e.g. at least three trials), we will conduct the analyses using a random‐effects model"). We instead conducted meta‐analyses for comparisons where there were at least two studies. This was done because there was a lack of studies for each treatment comparison. In the protocol, we state "If meta‐analysis is not possible due to the number of trials (less than three) or considerable heterogeneity (greater than 75%), we will assess the studies for the data collected qualitatively." In the review, we reported data qualitatively if the number of trials was fewer than two (see earlier in this section) and we reported meta‐analyses where heterogeneity was greater than 75% and discussed qualitatively (see 'Assessment of heterogeneity' in this section). There were no data for the 'Time to recurrence' outcome. Thus we did not summarise time to recurrence by calculating random‐effects estimates of the pooled hazard ratio using the generic inverse‐variance method.
Sensitivity analysis. The protocol states that we would perform sensitivity analyses to determine the impact of removing studies with missing data, to examine if they contributed to the risk of bias. We did not do this because studies in our analyses did not have missing data.
'Summary of findings' table. The protocol states that if further subgroup analyses merit their own 'Summary of findings' table, we will include further tables. There were no subgroup analyses that warranted a separate 'Summary of findings' table in the review. The protocol states that primary outcomes will be included in the 'Summary of findings' table. We also included the secondary outcomes, mycological cure and clinical cure, in the tables because this provides readers with a more complete understanding of the findings.
Contributions of authors
KF was the contact person with the editorial base. AKG, KF co‐ordinated contributions from the co‐authors and wrote the final draft of the review. KF, SV screened papers against eligibility criteria. KF, RM, SV obtained data on ongoing and unpublished studies. KF, RM appraised the quality of papers. KF, RM, SV extracted data for the review and sought additional information about papers. KF, RM, SV entered data into Review Manager 5. AKG, KF analysed and interpreted data. EV, KF worked on the Methods sections. AKG, KF drafted the clinical sections of the Background and responded to the clinical comments of the referees. EV, KF responded to the methodology and statistics comments of the referees. DJ was the consumer co‐author and checked the review for readability and clarity, as well as ensuring outcomes are relevant to consumers. AKG is the guarantor of the update.
Disclaimer
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the Cochrane Skin Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Sources of support
Internal sources
No sources of support supplied
External sources
-
The National Institute for Health Research (NIHR), UK.
The NIHR, UK, is the largest single funder of the Cochrane Skin Group.
Declarations of interest
Kelly Foley, Aditya Gupta, Rachel Mays, and Sarah Versteeg are employed by Mediprobe Research Inc. Mediprobe Research Inc. is not a commercial organisation, nor is it a contract research organisation.
In addition to Dr Gupta's dermatology practice, he conducts clinical trials and these are done through Dr AK Gupta Medicine Professional Corporation, previously known as Mediprobe Research. In Canada, all physicians work through Professional Corporations, and Dr Gupta does the same. Mediprobe Research is the name we continue to use because we have done so for years, but the official corporate entity is Dr AK Gupta Medicine Professional Corporation. We have not conducted clinical trials for tinea pedis in the past three years, and Dr Gupta is currently recruiting for two trials using topical treatments for onychomycosis for Valeant Canada and Moberg Pharma. Dr Gupta has received honoraria through his institution for educational presentations to physicians from Valeant Canada. Elmer Villanueva: nothing to declare. Denny John: nothing to declare.
Aditya Gupta, lead author on the protocol for this Cochrane Review, became conflicted in terms of Cochrane’s commercial sponsorship policy and has been replaced by Kelly Foley, as lead author. Kelly Foley has no relevant financial conflict of interest, and in the judgement of Cochrane Skin’s editorial team, she has made a contribution equal to Aditya Gupta, which justifies her position as first author. This change has been discussed with and approved by the Funding Arbiters.
New
References
References to studies included in this review
ACTRN12614000946617 {unpublished data only}
- ACTRN12614000946617. Kunzea oil for the management of fungal nail infection (toenail onychomycosis), a pilot randomised controlled trial. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=366923 (first received 4 September 2014). [CENTRAL: CN‐01831590]
ACTRN12614001238662 {unpublished data only}
- ACTRN12614001238662. Evaluation of mastic paint in the treatment of nail disorders (onycholysis, onychomycosis, onychorrhexis). www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12614001238662 (first received 26 November 2014).
Alberdi 2019 {published data only}
- Alberdi E, Gomez C. Efficiency of methylene blue‐mediated photodynamic therapy vs intense pulsed light in the treatment of onychomycosis in the toenails. Photodermatology, Photoimmunology, and Photomedicine 2019;35(2):69‐77. [CENTRAL: CN‐01951889] [DOI] [PubMed] [Google Scholar]
Amichai 2010 {published data only}
- Amichai B, Nitzan B, Mosckovitz R, Shemer A. Iontophoretic delivery of terbinafine in onychomycosis: a preliminary study. British Journal of Dermatology 2010;162(1):46‐50. [CENTRAL: CN‐00741789] [DOI] [PubMed] [Google Scholar]
Auvinen 2015 {published data only}
- Auvinen T, Tiihonen R, Soini M, Wangel M, Sipponen A, Jokinen JJ. Efficacy of topical resin lacquer, amorolfine and oral terbinafine for treating toenail onychomycosis: a prospective, randomized, controlled, investigator‐blinded, parallel‐group clinical trial. British Journal of Dermatology 2015;173(4):940‐8. [CENTRAL: CN‐01105172] [DOI] [PubMed] [Google Scholar]
Baran 2009 {published data only}
- Baran R, Tosti A, Hartmane I, Altmeyer P, Hercogova J, Koudelkova V, et al. An innovative water‐soluble biopolymer improves efficacy of ciclopirox nail lacquer in the management of onychomycosis. Journal of the European Academy of Dermatology and Venereology 2009;23(7):773‐81. [CENTRAL: CN‐00718755] [DOI] [PubMed] [Google Scholar]
- Piraccini BM, Tosti A. Ciclopirox hydroxypropyl chitosan: efficacy in mild‐to‐moderate onychomycosis. Skin Appendage Disorders 2019;5(1):13‐9. [CENTRAL: CN‐01611757] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bonhert 2019 {published data only}
- Bonhert K, Dorizas A, Sadick NS. Efficacy of combination therapy with efinaconazole 10% solution and 1064 nm Nd:YAG laser for treatment of toenail onychomycosis. Journal of Cosmetic and Laser Therapy 2019;21(3):179‐83. [CENTRAL: CN‐01629520] [DOI] [PubMed] [Google Scholar]
Buck 1994 {published data only}
- Buck DS, Nidorf DM, Addino JG. Comparison of two topical preparations for the treatment of onychomycosis: Melaleuca alternifolia (tea tree) oil and clotrimazole. Journal of Family Practice 1994;38(6):601‐5. [CENTRAL: CN‐00101608] [PubMed] [Google Scholar]
Eertmans 2018 {published data only}
- Eertmans F, Doss N, Rossel B, Adriaens E. Daily application of an aqueous, acidifying, peelable nail polish versus weekly amorolfine for topical onychomycosis treatment: a prospective, randomized, blinded trial. Dermatology and Therapy 2018;8(3):463‐73. [CENTRAL: CN‐01646389] [DOI] [PMC free article] [PubMed] [Google Scholar]
Elewski 2013a {published data only}
- Elewski BE, Ghannoum MA, Mayser P, Gupta AK, Korting HC, Shouey RJ, et al. Efficacy, safety and tolerability of topical terbinafine nail solution in patients with mild‐to‐moderate toenail onychomycosis: results from three randomized studies using double‐blind vehicle‐controlled and open‐label active‐controlled designs. Journal of the European Academy of Dermatology and Venereology 2013;27(3):287‐94. [PUBMED: 22181693] [DOI] [PubMed] [Google Scholar]
Elewski 2013b {published data only}
- Elewski BE, Ghannoum MA, Mayser P, Gupta AK, Korting HC, Shouey RJ, et al. Efficacy, safety and tolerability of topical terbinafine nail solution in patients with mild‐to‐moderate toenail onychomycosis: results from three randomized studies using double‐blind vehicle‐controlled and open‐label active‐controlled designs. Journal of the European Academy of Dermatology and Venereology 2013;27(3):287‐94. [PUBMED: 22181693] [DOI] [PubMed] [Google Scholar]
Elewski 2013c {published and unpublished data}
- Elewski BE, Rich P, Pollak R, Pariser DM, Watanabe S, Senda H, et al. Efinaconazole 10% solution in the treatment of toenail onychomycosis: two phase III multicenter, randomized, double‐blind studies (Erratum appears in Journal of the American Academy of Dermatology, 2014 Feb;70(2):399). Journal of the American Academy of Dermatology 2013;68(4):600‐8. [CENTRAL: CN‐00966732] [DOI] [PubMed] [Google Scholar]
- Gupta AK, Elewski BE, Sugarman JL, Ieda C, Kawabata H, Kang R, et al. The efficacy and safety of efinaconazole 10% solution for treatment of mild to moderate onychomycosis: a pooled analysis of two phase 3 randomized trials. Journal of Drugs in Dermatology 2014;13(7):815‐20. [CENTRAL: CN‐01041119] [PubMed] [Google Scholar]
Elewski 2013d {published and unpublished data}
- Elewski BE, Rich P, Pollak R, Pariser D M, Watanabe S, Senda H, et al. Efinaconazole 10% solution in the treatment of toenail onychomycosis: two phase III multicenter, randomized, double‐blind studies (Erratum appears in Journal of the American Academy of Dermatolology, 2014 Feb;70(2):399). Journal of the American Academy of Dermatology 2013;68(4):600‐8. [CENTRAL: CN‐00966732] [DOI] [PubMed] [Google Scholar]
- Gupta AK, Elewski BE, Sugarman JL, Ieda C, Kawabata H, Kang R, et al. The efficacy and safety of efinaconazole 10% solution for treatment of mild to moderate onychomycosis: a pooled analysis of two phase 3 randomized trials. Journal of Drugs in Dermatology 2014;13(7):815‐20. [CENTRAL: CN‐01041119] [PubMed] [Google Scholar]
Elewski 2015a {published data only}
- Elewski BE, Aly R, Baldwin SL, Gonzalez Soto RF, Rich P, Weisfeld M, et al. Efficacy and safety of tavaborole topical solution, 5%, a novel boron‐based antifungal agent, for the treatment of toenail onychomycosis: Results from 2 randomized phase‐III studies. Journal of the American Academy of Dermatology 2015;73(1):62‐9. [CENTRAL: CN‐01085211] [DOI] [PubMed] [Google Scholar]
- Gupta AK, Hall S, Zane LT, Lipner SR, Rich P. Evaluation of the efficacy and safety of tavaborole topical solution, 5%, in the treatment of onychomycosis of the toenail in adults: a pooled analysis of an 8‐week, post‐study follow‐up from two randomised phase 3 studies. Journal of Dermatological Treatment 2018;29(1):44‐8. [CENTRAL: CN‐01458612] [DOI] [PubMed] [Google Scholar]
- Pariser DM, Wendelken ME, Rycerz AM, Gellings Lowe N, Yost JM, Lipner SR. Planimetric post‐hoc analysis of women with onychomycosis from tavaborole 5% phase III studies: evidence of greater improvements in patients with >50% baseline infection. Journal of Drugs in Dermatology 2018;17(2):168‐72. [CENTRAL: CN‐01627312] [PubMed] [Google Scholar]
Elewski 2015b {published data only}
- Elewski BE, Aly R, Baldwin SL, Gonzalez Soto RF, Rich P, Weisfeld M, et al. Efficacy and safety of tavaborole topical solution, 5%, a novel boron‐based antifungal agent, for the treatment of toenail onychomycosis: Results from 2 randomized phase‐III studies. Journal of the American Academy of Dermatology 2015;73(1):62‐9. [CENTRAL: CN‐01085211] [DOI] [PubMed] [Google Scholar]
- Gupta AK, Hall S, Zane LT, Lipner SR, Rich P. Evaluation of the efficacy and safety of tavaborole topical solution, 5%, in the treatment of onychomycosis of the toenail in adults: a pooled analysis of an 8‐week, post‐study follow‐up from two randomised phase 3 studies. Journal of Dermatological Treatment 2018;29(1):44‐8. [CENTRAL: CN‐01458612] [DOI] [PubMed] [Google Scholar]
- Pariser DM, Wendelken ME, Rycerz AM, Gellings Lowe N, Yost JM, Lipner SR. Planimetric post‐hoc analysis of women with onychomycosis from tavaborole 5% phase III studies: evidence of greater improvements in patients with >50% baseline infection. Journal of Drugs in Dermatology 2018;17(2):168‐72. [CENTRAL: CN‐01627312] [PubMed] [Google Scholar]
EUCTR2005‐005905‐51 {unpublished data only}
- EUCTR2005‐005905‐51. A phase II, single‐centre, randomised, parallel‐group, clinical study to investigate the tolerability of double blind ciclopirox nail product compared to double blind placebo nail product compared to single blind mycoster in subjects with mild to moderate onychomycosis. www.clinicaltrialsregister.eu/ctr‐search/search?query=2005‐005905‐51 (first received 20 February 2006). [CENTRAL: CN‐01813729]
EUCTR2006‐000974‐54 {unpublished data only}
- EUCTR2006‐000974‐54. A multi‐centre, randomized, parallel groups, vehicle and active controlled study of amorolfine 4% and 10% nail lacquer new formulation in the topical treatment of distal and lateral subungual toenail onychomycosis. www.clinicaltrialsregister.eu/ctr‐search/search?query=eudract_number:2006‐000974‐54 (first received 28 February 2007). [CENTRAL: CN‐01835701]
EUCTR2006‐005895‐42 {unpublished data only}
- EUCTR2006‐005895‐42. A study to determine the safety and efficacy of a terbinafine topical formulation system in subjects with onychomycosis in laser treated toenails versus ciclopirox lacquer in intact toenails. www.clinicaltrialsregister.eu/ctr‐search/search?query=2006‐005895‐42 (first received 2 March 2009). [CENTRAL: CN‐01852085]
EUCTR2008‐003215‐13 {unpublished data only}
- EUCTR2008‐003215‐13. A double‐blind, randomized, multicenter, placebo‐controlled phase 3 trial to prove the superiority of bifonazole vs. placebo after 4 weeks of onychomycosis treatment (as a follow‐up of a 2 weeks treatment of non‐surgical nail ablation of diseased nail matrix with a 40% urea paste). www.clinicaltrialsregister.eu/ctr‐search/search?query=2008‐003215‐13 (first received 21 October 2008). [CENTRAL: CN‐01822662]
EUCTR2016‐001242‐25 {unpublished data only}
- EUCTR2016‐001242‐25. An early phase development, partly blinded, positive and vehicle controlled, randomized, non‐inferiority investigation of the pharmacokinetics, safety and efficacy of BB2603 cutaneous hand‐pump spray versus Lamisil® spray and versus BB2603 vehicle hand‐pump spray in subjects with onychomycosis and associated tinea pedis. www.clinicaltrialsregister.eu/ctr‐search/search?query=2016‐001242‐25 (first received 7 February 2017). [CENTRAL: CN‐01816797]
Gupta 2000a {published data only}
- Gupta AK, Fleckman P, Baran R. Ciclopirox nail lacquer topical solution 8% in the treatment of toenail onychomycosis. Journal of the American Academy of Dermatology 2000;43(4 Suppl):S70‐80. [CENTRAL: CN‐00602467] [DOI] [PubMed] [Google Scholar]
Gupta 2000b {published data only}
- Gupta AK, Fleckman P, Baran R. Ciclopirox nail lacquer topical solution 8% in the treatment of toenail onychomycosis. Journal of the American Academy of Dermatology 2000;43(4 Suppl):S70‐80. [CENTRAL: CN‐00602467] [DOI] [PubMed] [Google Scholar]
Gupta 2006 {published data only}
- Gupta A, Mo J, Lu M. A randomized, controlled, dose‐ranging study to assess the efficacy and safety of terbinafine HCl nail lacquer for onychomycosis. Journal of the American Academy of Dermatology 2006;54(3 Suppl):AB148. [CENTRAL: CN‐00602415] [Google Scholar]
Hartmane 2013 {published data only (unpublished sought but not used)}
- Hartmane I, Dervenice A, Mailland F, Mikazans I, Frisenda L, Caserini M. Evaluation of safety profile, pharmacokinetics, and clinical benefit of an innovative terbinafine transungual solution (P‐3058): A phase I study in patients with mild‐to‐moderate distal subungual onychomycosis. Journal of the American Academy of Dermatology 2013;68(4 S1):AB105. [Google Scholar]
Hollmig 2014 {published data only}
- Hollmig ST, Rahman Z, Henderson MT, Rotatori RM, Gladstone H, Tang JY. Lack of efficacy with 1064‐nm neodymium:yttrium‐aluminum‐garnet laser for the treatment of onychomycosis: a randomized, controlled trial. Journal of the American Academy of Dermatology 2014;70(5):911‐7. [CENTRAL: CN‐00988910] [DOI] [PubMed] [Google Scholar]
Ijzerman 2010 {published data only (unpublished sought but not used)}
- Ijzerman M, Baker J, Flack M, Robinson P. Forty‐two‐week safety study of topical nanoemulsion (NB‐002) for the treatment of mild to moderate distal subungual onychomycosis: a randomized, double‐blind, vehicle‐controlled trial. Journal of the American Academy of Dermatology 2010;62(3 Suppl):AB77. [CENTRAL: CN‐00843737] [Google Scholar]
Iorizzo 2016 {published data only}
- Iorizzo M, Hartmane I, Derveniece A, Mikazans I. Ciclopirox 8% HPCH nail lacquer in the treatment of mild‐to‐moderate onychomycosis: a randomized, amorolfine controlled study using a blinded evaluator. Skin Appendage Disorders 2016;1(3):134‐40. [PUBMED: 27171791] [DOI] [PMC free article] [PubMed] [Google Scholar]
Karsai 2017 {published data only}
- Karsai S, Jager M, Oesterhelt A, Weiss C, Schneider SW, Junger M, et al. Treating onychomycosis with the short‐pulsed 1064‐nm‐Nd: YAG laser: results of a prospective randomized controlled trial. Journal of the European Academy of Dermatology and Venereology 2017;31(1):175‐80. [CENTRAL: CN‐01285896] [DOI] [PubMed] [Google Scholar]
Koren 2018 {published data only}
- Koren A, Salameh F, Sprecher E, Artzi O. Laser‐assisted photodynamic therapy or laser‐assisted amorolfine lacquer delivery for treatment of toenail onychomycosis: an open‐label comparative study. Acta Dermato‐Venereologia 2018;98(4):467‐8. [CENTRAL: CN‐01643159] [DOI] [PubMed] [Google Scholar]
Kumar 2001 {published data only}
- Kumar SV, Kulkarni K. Clinical trial of nailcare capsule and creams in toenail tinea unguium infection. Bombay Hospital Journal 2001;43(4):519‐23. [CENTRAL: CN‐01094773] [Google Scholar]
Lahfa 2013 {published data only}
- Lahfa M, Bulai‐Livideanu C, Baran R, Ortonne J P, Richert B, Tosti A, et al. Efficacy, safety and tolerability of an optimized avulsion technique with onyster (40% urea ointment with plastic dressing) ointment compared to bifonazole‐urea ointment for removal of the clinically infected nail in toenail onychomycosis: a randomized evaluator‐blinded controlled study. Dermatology 2013;226(1):5‐12. [CENTRAL: CN‐00906754] [DOI] [PubMed] [Google Scholar]
Lu 2005 {published data only}
- Lu MQ, Mo J, Bonfrisco J. Randomized, double‐blind, parallel design trial to assess the efficacy and safety of terbinafine nail lacquer for the treatment of onychomycosis. Journal of the European Academy of Dermatology and Venereology 2005;19(Suppl 2):394‐5. [CENTRAL: CN‐00602518] [Google Scholar]
Montana 1994 {published data only}
- Montana JB, Scher RK. A double‐blind, vehicle‐controlled study of the safety and efficacy of fungoid tincture in patients with distal subungual onychomycosis of the toes. Cutis 1994;53(6):313‐6. [CENTRAL: CN‐00103913] [PubMed] [Google Scholar]
NCT01080079 {unpublished data only}
- NCT01080079. Efficacy and safety study of iontophoretic application of terbinafine gel in subjects with onychomycosis. clinicaltrials.gov/ct2/show/NCT01080079 (first received 3 March 2010). [CENTRAL: CN‐01528416]
NCT01145807 {unpublished data only}
- NCT01145807. A randomized, double‐blind, vehicle‐ and placebo‐controlled, multicenter trial in patients with mild to moderate distal subungual toenail onychomycosis to investigate the efficacy, tolerability, and safety of twice daily application of TDT 067 for 48 weeks. clinicaltrials.gov/ct2/show/NCT01145807 (first received 17 June 2010). [CENTRAL: CN‐01530110]
NCT01246518 {unpublished data only}
- NCT01246518. Efficacy and safety of two treatment regimens of topical MOB015 in adults with distal subungual onychomycosis. clinicaltrials.gov/ct2/show/NCT01246518 (first received 23 November 2010). [CENTRAL: CN‐01502004]
NCT01400594 {unpublished data only}
- NCT01400594. Safety and efficacy study of HTU‐520 in the treatment of distal subungual onychomycosis of the toenail. clinicaltrials.gov/ct2/show/study/NCT01400594 (first received 22 July 2011). [CENTRAL: CN‐01487713]
NCT02022215 {unpublished data only}
- NCT02022215. Efficacy and safety study of ME1111 in patients with onychomycosis. clinicaltrials.gov/ct2/show/NCT02022215 (first received 27 December 2013). [CENTRAL: CN‐01480021]
NCT02343627 {unpublished data only}
- NCT02343627. Safety and efficacy of NVXT solution in mild to moderate fungal infection of the toenail. clinicaltrials.gov/ct2/show/NCT02343627 (first received 22 January 2015). [CENTRAL: CN‐01575756]
NCT02933879 {unpublished data only}
- NCT02933879. Randomized, placebo‐controlled, double‐blind, parallel‐group, multi‐site phase 2b clinical study. www.clinicaltrials.gov/ct2/show/NCT02933879 (first received 14 October 2016). [CENTRAL: CN‐01521579]
NCT03141840 {unpublished data only}
- NCT03141840. Clinical trial of topical ABL01 treatment of onychomycosis. www.clinicaltrials.gov/ct2/show/NCT03141840 (first received 5 May 2017). [CENTRAL: CN‐01493896]
NCT03289871 {unpublished data only}
- NCT03289871. Clinical evaluation of the efficacy of a medical device in treatment of toenail onychomycosis. clinicaltrials.gov/ct2/show/record/NCT03289871 (first received 21 September 2017). [CENTRAL: CN‐01592803]
Nijenhuis‐Rosien 2019 {published data only (unpublished sought but not used)}
- Nijenhuis‐Rosien L, Kleefstra N, Dijk PR, Wolfhagen MJ, Groenier KH, Bilo HJ, et al. Laser therapy for onychomycosis in patients with diabetes at risk for foot ulcers: a randomised, quadruple‐blind, sham controlled trial (LASER‐1). Journal of the European Academy of Dermatology and Venereology 2019 Mar 28 [Epub ahead of print]. [CENTRAL: CN‐01940931; DOI: 10.1111/jdv.15601] [DOI] [PubMed]
- Nijenhuis‐Rosien L, Kleefstra N, Wolfhagen MJ, Groenier KH, Bilo HJ, Landman GW. Laser therapy for onychomycosis in patients with diabetes at risk for foot complications: study protocol for a randomised, double‐blind, controlled trial (LASER‐1). Trials 2015;16:108. [CENTRAL: CN‐01256326] [DOI] [PMC free article] [PubMed] [Google Scholar]
Parekh 2017 {published data only}
- Parekh M, Ramaiah G, Pashilkar P, Ramanujam R, Johnston P, Ilag LL. A pilot single centre, double blind, placebo controlled, randomized, parallel study of Calmagen® dermaceutical cream and lotion for the topical treatment of tinea and onychomycosis. BMC Complementary and Alternative Medicine 2017;17(1):464. [CENTRAL: CN‐01412779; PUBMED: 28923039] [DOI] [PMC free article] [PubMed] [Google Scholar]
Paul 2013 {published data only}
- Paul C, Coustou D, Lahfa M, Bulai‐Livideanu C, Doss N, Mokthar I, et al. A multicenter, randomized, open‐label, controlled study comparing the efficacy, safety and cost‐effectiveness of a sequential therapy with RV4104A ointment, ciclopiroxolamine cream and ciclopirox film‐forming solution with amorolfine nail lacquer alone in dermatophytic onychomycosis. Dermatology 2013;227(2):157‐64. [CENTRAL: CN‐01001997] [DOI] [PubMed] [Google Scholar]
Romero‐Cerecero 2008 {published data only}
- Romero‐Cerecero O, Zamilpa A, Jimenez‐Ferrer JE, Rojas‐Bribiesca G, Roman‐Ramos R, Tortoriello J. Double‐blind clinical trial for evaluating the effectiveness and tolerability of Ageratina pichinchensis extract on patients with mild to moderate onychomycosis. A comparative study with ciclopirox (Planta Med) 2008:October;74(12):1430‐1435. Planta Medica 2008;74(14):1767. [CENTRAL: CN‐00668953] [DOI] [PubMed] [Google Scholar]
Romero‐Cerecero 2009 {published data only}
- Romero‐Cerecero O, Roman‐Ramos R, Zamilpa A, Jimenez‐Ferrer JE, Rojas‐Bribiesca G, Tortoriello J. Clinical trial to compare the effectiveness of two concentrations of the Ageratina pichinchensis extract in the topical treatment of onychomycosis. Journal of Ethnopharmacology 2009;126(1):74‐8. [CENTRAL: CN‐00733423] [DOI] [PubMed] [Google Scholar]
Schalka 2012 {published data only}
- Schalka S, Nunes S, Gomes Neto A. Comparative clinical evaluation of efficacy and safety of a formulation containing ciclopirox 8% in the form of a therapeutic nail lacquer in two different posologies for the treatment of onychomycosis of the toes. Anais Brasileiros de Dermatologia 2012;87(1):19‐25. [CENTRAL: CN‐00895307] [DOI] [PubMed] [Google Scholar]
Sigurgeirsson 2016 {published data only}
- Sigurgeirsson B, Ghannoum MA, Osman‐Ponchet H, Kerrouche N, Sidou F. Application of cosmetic nail varnish does not affect the antifungal efficacy of amorolfine 5% nail lacquer in the treatment of distal subungual toenail onychomycosis: results of a randomised active‐controlled study and in vitro assays. Mycoses 2016;59(5):319‐26. [CENTRAL: CN‐01260064] [DOI] [PubMed] [Google Scholar]
Stein 2014 {published data only (unpublished sought but not used)}
- Stein L, Tavakkol A, Wiltz H, Noss M, Pollak R, Kempers S. A blinded review of the ongoing SOLUTION study, a phase 2b/3 study of 2 dosing regimens of a novel 10% luliconazole solution in patients with onychomycosis. Journal of the American Academy of Dermatology 2014;70(5 Suppl 1):AB88. [DOI: 10.1016/j.jaad.2014.01.367] [DOI] [Google Scholar]
Syed 1998 {published data only}
- Syed TA, Ahmadpour OA, Ahmad SA, Shamsi S. Management of toenail onychomycosis with 2% butenafine and 20% urea cream: a placebo‐controlled, double‐blind study. Journal of Dermatology 1998;25(10):648‐52. [CENTRAL: CN‐00157302] [DOI] [PubMed] [Google Scholar]
Syed 1999 {published data only}
- Syed TA, Qureshi ZA, Ali SM, Ahmad S, Ahmad SA. Treatment of toenail onychomycosis with 2% butenafine and 5% Melaleuca alternifolia (tea tree) oil in cream. Tropical Medicine & International Health 1999;4(4):284‐7. [CENTRAL: CN‐00164395] [DOI] [PubMed] [Google Scholar]
Toledo‐Bahena 2014 {published and unpublished data}
- Toledo‐Bahena ME, Bucko A, Ocampo‐Candiani J, Herz‐Ruelas ME, Jones TM, Jarratt M T, et al. The efficacy and safety of tavaborole, a novel, boron‐based pharmaceutical agent: phase 2 studies conducted for the topical treatment of toenail onychomycosis. Journal of Drugs in Dermatology 2014;13(9):1124‐32. [CENTRAL: CN‐01113743] [PubMed] [Google Scholar]
Tschen 2013 {published data only}
- Tschen EH, Bucko AD, Oizumi N, Kawabata H, Olin JT, Pillai R. Efinaconazole solution in the treatment of toenail onychomycosis: a phase 2, multicenter, randomized, double‐blind study. Journal of Drugs in Dermatology 2013;12(2):186‐92. [CENTRAL: CN‐01164712] [PubMed] [Google Scholar]
Waibel 2013 {published data only}
- Waibel J, Wulkan A J, Rudnick A. Prospective efficacy and safety evaluation of laser treatments with real‐time temperature feedback for fungal onychomycosis. Journal of Drugs in Dermatology 2013;12(11):1237‐42. [CENTRAL: CN‐00996765] [PubMed] [Google Scholar]
Watanabe 2017 {published data only}
- Watanabe S, Kishida H, Okubo A. Efficacy and safety of luliconazole 5% nail solution for the treatment of onychomycosis: A multicenter, double‐blind, randomized phase III study. Journal of Dermatology 2017;44(7):753‐9. [CENTRAL: CN‐01458932] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Abd El‐Aal 2019 {published data only}
- Abd El‐Aal EB, Abdo HM, Ibrahim SM, Eldestawy MT. Fractional carbon dioxide laser assisted delivery of topical tazarotene versus topical tioconazole in the treatment of onychomycosis. Journal of Dermatological Treatment 2019;30(3):277‐82. [PUBMED: 30081698] [DOI] [PubMed] [Google Scholar]
Anonymous 2000 {published data only}
- Anonymous. Ciclopirox (Penlac) nail lacquer for onychomycosis. Medical Letter on Drugs & Therapeutics 2000;42(1080):51‐2. [PUBMED: 10859733] [PubMed] [Google Scholar]
Anonymous 2015 {published data only}
- Anonymous. Tavaborole topical solution (Kerydin) for onychomycosis. Medical Letter on Drugs & Therapeutics 2015;57(1463):35‐6. [PUBMED: 25719999] [PubMed] [Google Scholar]
Bassiri‐Jahromi 2012 {published data only (unpublished sought but not used)}
- Bassiri‐Jahromi S, Ehsani AH, Mirshams‐Shahshahani M, Jamshidi B. A comparative evaluation of combination therapy of fluconazole 1% and urea 40% compared with fluconazole 1% alone in a nail lacquer for treatment of onychomycosis: therapeutic trial. Journal of Dermatological Treatment 2012;23(6):453‐6. [CENTRAL: CN‐00882643] [DOI] [PubMed] [Google Scholar]
Bergstrom 2009 {published data only}
- Bergstrom KG. Tea tree oil: Panacea or placebo?. Journal of Drugs in Dermatology 2009;8(5):494‐6. [PUBMED: 19537376] [PubMed] [Google Scholar]
Botter 1971 {published data only}
- Botter AA. Topical treatment of nail and skin infections with miconazole, a new broad‐spectrum antimycotic. Mykosen 1971;14(4):187‐91. [PUBMED: 4251820] [DOI] [PubMed] [Google Scholar]
Canavan 2018 {published data only}
- Canavan TN, Bevans SL, Cantrell WC, Wang C, Elewski BE. Single‐center, prospective, blinded study comparing the efficacy and compatibility of efinaconazole 10% solution in treating onychomycosis with and without concurrent nail polish use. Skin Appendage Disorders 2018;5(1):9‐12. [CENTRAL: CN‐01767497; PUBMED: 30643774] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chan 2005 {published data only}
- Chan TC, Czarniecki C, Burrows W, Bittker R, Stough DB, Lam GN, et al. EcoNail™ (5% econazole plus 18% SEPA®) nail lacquer in patients with severe onychomycosis: safety, local tolerability, and systemic exposure. Journal of Investigative Dermatology 2005;125(1):A4. [CENTRAL: CN‐00792736] [Google Scholar]
Dina 2017 {published data only}
- Dina A, Gomaa AH, Mohammed GF, Eyada MM, Sweify MA. Evaluation of the therapeutic efficacy of tea tree oil in treatment of onychomycosis. International Journal of Pharmacognosy and Phytochemical Research 2017;9(12):1414‐20. [CENTRAL: CN‐01466199] [Google Scholar]
El‐Tatawy 2015 {published data only (unpublished sought but not used)}
- El‐Tatawy RA, Abd El‐Naby NM, El‐Hawary EE, Talaat RA. A comparative clinical and mycological study of Nd‐YAG laser versus topical terbinafine in the treatment of onychomycosis. Journal of Dermatological Treatment 2015;26(5):461‐4. [CENTRAL: CN‐01129437] [DOI] [PubMed] [Google Scholar]
Emtestam 2012 {published data only (unpublished sought but not used)}
- Emtestam L, Kaaman T, Rensfeldt K. Treatment of distal subungual onychomycosis with a topical preparation of urea, propylene glycol and lactic acid: results of a 24‐week, double‐blind, placebo‐controlled study. Mycoses 2012;55(6):532‐40. [CENTRAL: CN‐00880045] [DOI] [PubMed] [Google Scholar]
Fredriksson 1974 {published data only}
- Fredriksson T. Topical treatment of superficial mycoses with clotrimazole. Postgraduate Medical Journal 1974;50 Suppl 1:62‐4. [CENTRAL: CN‐00012751] [PubMed] [Google Scholar]
Furtado 2005 {published data only}
- Furtado T, Adjadj L, Halmy K. Cost‐effectiveness analysis comparing amorolfine and ciclopirox in the treatment of onychomycosis without matrix involvement. Journal of the American Academy of Dermatology 2005;52:P124. [Google Scholar]
Gilaberte 2017 {published data only (unpublished sought but not used)}
- Gilaberte Y, Robres MP, Frias MP, Garcia‐Doval I, Rezuta A, Aspiroz C. Methyl aminolevulinate photodynamic therapy for onychomycosis: a multicentre, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology 2017;31:347‐54. [CENTRAL: CN‐01332762] [DOI] [PubMed] [Google Scholar]
Gupta 2005 {published data only}
- Gupta AK. Ciclopirox nail lacquer as an adjunct to oral terbinafine for toenail onychomycosis: interim results from a randomized controlled trial. Journal of the European Academy of Dermatology and Venereology 2005;19(Suppl 2):28‐9. [CENTRAL: CN‐00602229] [Google Scholar]
Halmy 2005 {published data only (unpublished sought but not used)}
- Halmy K. Experience with nail lacquers containing amorolfine 5% and ciclopirox 8% in patients with onychomycosis. Abstract P‐56. 85th BAD Annual Meeting 5‐8th July 2005, Glasgow, UK. British Journal of Dermatology 2005;153(Suppl 1):38. [CENTRAL: CN‐00527206] [Google Scholar]
Harris 2010 {published data only}
- Harris D, Gupta A, Pollak R, Goffe B, Lanzafame R. Pulsed infrared laser treatment for onychomycosis: Controlled, randomized, multi‐centered trial (n = 155). Lasers in Surgery and Medicine 2010;42:62. [Google Scholar]
Hay 1988 {published data only}
- Hay RJ, Roberts DT, Doherty VR, Richardson MD, Midgley G. The topical treatment of onychomycosis using a new combined urea/imidazole preparation. Clinical and Experimental Dermatology 1988;13(3):164‐7. [CENTRAL: CN‐00240760] [DOI] [PubMed] [Google Scholar]
Jimenez‐Faraj 2018 {published data only}
- Jimenez‐Faraj JE, Torres‐Oviedo JN, Fiores‐Acosta ME, Castillo‐Moreno CG, Argueta‐Cruz AK, Portillo‐Varela EC, et al. Comparison of therapy with 1% bifonazole plus 40% urea, monotherapy with 40% urea and placebo on patients with onychomycosis. Dermatologia Revista Mexicana 2018;62(1):11‐8. [CENTRAL: CN‐01464271] [Google Scholar]
Kamalam 1980 {published data only}
- Kamalam A, Thambiah AS. Clotrimazole and econazole in dermatophytoses (a double blind study). Mycoses 1980;23(12):707‐10. [CENTRAL: CN‐00024851] [DOI] [PubMed] [Google Scholar]
Kim 2016a {published data only}
- Kim MS, Jung JY, Cho EB, Park EJ, Kim KH, Kim KJ. The effectiveness of 1,064‐nm long‐pulsed Nd:YAG laser in the treatment of severe onychomycosis. Journal of Cosmetic and Laser Therapy 2016;18(6):317‐22. [CENTRAL: CN‐01208456] [DOI] [PubMed] [Google Scholar]
Kim 2016b {published data only (unpublished sought but not used)}
- Kim TI, Jeong KH, Suh DH, Lee SJ, Shin MK, Lee MH. A randomised comparative study of 1064 nm neodymium‐doped yttrium aluminum garnet (Nd:YAG) laser and topical antifungal treatment of onychomycosis. Mycoses 2016;59(12):803‐10. [CENTRAL: CN‐01248276] [DOI] [PubMed] [Google Scholar]
Krasaeath 2016 {published data only}
- Krasaeath R, Elizondo J. Topical antifungals for treatment of onychomycosis. American Family Physician 2016;94(9):734. [PUBMED: 27929250] [PubMed] [Google Scholar]
Landsman 2010 {published data only}
- Landsman AS, Robbins AH, Angelini PF, Wu CC, Cook J, Oster M, et al. Treatment of mild, moderate, and severe onychomycosis using 870‐ and 930‐nm light exposure. Journal of the American Podiatric Medical Association 2010;100(3):166‐77. [CENTRAL: CN‐00759930] [DOI] [PubMed] [Google Scholar]
Landsman 2012 {published data only}
- Landsman AS, Robbins AH. Treatment of mild, moderate, and severe onychomycosis using 870‐ and 930‐nm light exposure: some follow‐up observations at 270 days. Journal of the American Podiatric Medical Association 2012;102(2):169‐71. [CENTRAL: CN‐00903460] [DOI] [PubMed] [Google Scholar]
Lauharanta 1992 {published data only (unpublished sought but not used)}
- Lauharanta J. Comparative efficacy and safety of amorolfine nail lacquer 2% versus 5% once weekly. Clinical and Experimental Dermatology 1992;17(Suppl 1):41‐3. [CENTRAL: CN‐00089244] [DOI] [PubMed] [Google Scholar]
Li 2014 {published data only (unpublished sought but not used)}
- Li Y, Yu S, Xu J, Zhang R, Zhao J. Comparison of the efficacy of long‐pulsed Nd:YAG laser intervention for treatment of onychomycosis of toenails or fingernails. Journal of Drugs in Dermatology 2014;13(10):1258‐63. [CENTRAL: CN‐01110964] [PubMed] [Google Scholar]
Lu 2016 {published data only}
- Lu S, Zhang J, Liang Y, Li X, Cai W, Xi L. The efficacy of prognostic factors for long‐pulse neodymium: yttrium‐aluminum‐garnet laser treatment on onychomycosis: A pilot study. Annals of Dermatology 2016;28(3):406‐8. [PUBMED: 27274650] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mahgoub 1975 {published data only (unpublished sought but not used)}
- Mahgoub ES. Clinical trial with clotrimazole cream (Bay b 5097) in dermatophytosis and onychomycosis. Mycopathologia 1975;56(3):149‐52. [PUBMED: 128698] [DOI] [PubMed] [Google Scholar]
Malay 2009 {published data only}
- Malay DS, Yi S, Borowsky P, Downey MS, Mlodzienski AJ. Efficacy of debridement alone versus debridement combined with topical antifungal nail lacquer for the treatment of pedal onychomycosis: a randomized, controlled trial. Journal of Foot & Ankle Surgery 2009;48(3):294‐308. [CENTRAL: CN‐00705155] [DOI] [PubMed] [Google Scholar]
Many 1964 {published data only}
- Many H, Franklin CL, Derbes VJ. Candida albicans onychomycosis‐ a study of five modes of therapy. Dermatologia Tropica Et Ecologica Geographica 1964;3(1):17‐20. [CENTRAL: CN‐00446588] [PubMed] [Google Scholar]
Menéndez 2011 {published data only (unpublished sought but not used)}
- Menéndez S, Falcón L, Maqueira Y. Therapeutic efficacy of topical OLEOZON® in patients suffering from onychomycosis. Mycoses 2011;54(5):e272‐7. [PUBMED: 20492527] [DOI] [PubMed] [Google Scholar]
Mensing 1992 {published data only}
- Mensing H, Polak‐Wyss A, Splanemann V. Determination of the subungual antifungal activity of amorolfine after 1 month's treatment in patients with onychomycosis: comparison of two nail lacquer formulations. Clinical and Experimental Dermatology 1992;17(Suppl 1):29‐32. [CENTRAL: CN‐00089242] [DOI] [PubMed] [Google Scholar]
Meyerson 1992 {published data only}
- Meyerson MS, Scher RK, Hochman LG, Cohen JL, Pappert AS, Holwell JE. Open‐label study of the safety and efficacy of fungoid tincture in patients with distal subungual onychomycosis of the toes. Cutis 1992;49(5):359‐62. [CENTRAL: CN‐00269422] [PubMed] [Google Scholar]
Morgado 2017 {published data only}
- Morgado LF, Travolo AR, Muehlmann LA, Narcizo PS, Nunes RB, Pereira PA, et al. Photodynamic therapy treatment of onychomycosis with aluminium‐phthalocyanine chloride nanoemulsions: A proof of concept clinical trial. Journal of Photochemistry and Photobiology. B, Biology 2017;173:266‐70. [PUBMED: 28622558] [DOI] [PubMed] [Google Scholar]
NCT03094468 {unpublished data only}
- NCT03094468. Study to evaluate the efficacy and safety of P‐3058 nail solution in the treatment of onychomycosis. clinicaltrials.gov/ct2/show/NCT03094468 (first received 29 March 2017).
Oberste‐Lehn 1974 {published data only}
- Oberste‐Lehn H. Ideal properties of a modern antifungal agent‐‐the therapy of mycoses with clotrimazole. Postgraduate Medical Journal 1974;50(Suppl 1):51‐3. [PUBMED: 4282870] [PubMed] [Google Scholar]
Ortiz 2014 {published data only}
- Ortiz AE, Truong S, Serowka K, Kelly KM. A 1,320‐nm Nd: YAG laser for improving the appearance of onychomycosis. Dermatologic Surgery 2014;40(12):1356‐60. [CENTRAL: CN‐01037143] [DOI] [PubMed] [Google Scholar]
Rand 1996 {published data only}
- Rand S. Clinical trials of the new antifungal drug therapies. Journal of the American Academy of Dermatology 1996;34(5 Pt 1):863. [PUBMED: 8632094] [DOI] [PubMed] [Google Scholar]
Reinel 1992 {published data only}
- Reinel D, Clarke C. Comparative efficacy and safety of amorolfine nail lacquer 5% in onychomycosis, once‐weekly versus twice‐weekly. Clinical and Experimental Dermatology 1992;17(Suppl 1):44‐9. [CENTRAL: CN‐00089245] [DOI] [PubMed] [Google Scholar]
Schaller 2017 {published data only}
- Schaller M, Sigurgeirsson B, Sarkany M. Patient‐reported outcomes from two randomised studies comparing once‐weekly application of amorolfine 5% nail lacquer to other methods of topical treatment in distal and lateral subungual onychomycosis. Mycoses 2017;60(12):800‐7. [CENTRAL: CN‐01431814] [DOI] [PubMed] [Google Scholar]
Schlockermann 1957 {published data only}
- Schlockermann FW. Therapy of onychomycosis. Hautarzt 1957;8(6):270‐1. [PUBMED: 13448560] [PubMed] [Google Scholar]
Shemer 2016 {published data only}
- Shemer A, Gupta AK, Amichai B, Farhi R, Baran R, Daniel III CR, et al. An open comparative study of nail drilling as adjunctive treatment for toenail onychomycosis. Journal of Dermatological Treatment 2016;27(5):480‐3. [PUBMED: 27032812] [DOI] [PubMed] [Google Scholar]
Sigurgeirsson 2010 {published data only}
- Sigurgeirsson B, Olafsson JH, Steinsson JT, Kerrouche N, Sidou F. Efficacy of amorolfine nail lacquer for the prophylaxis of onychomycosis over 3 years. Journal of the European Academy of Dermatology and Venereology : JEADV 2010;24(8):910‐5. [CENTRAL: CN‐00772061] [DOI] [PubMed] [Google Scholar]
Sotiriou 2010 {published data only}
- Sotiriou E, Koussidou‐Eremonti T, Chaidemenos G, Apalla Z, Ioannides D. Photodynamic therapy for distal and lateral subungual toenail onychomycosis caused by Trichophyton rubrum: Preliminary results of a single‐centre open trial. Acta Dermato‐Venereologica 2010;90(2):216‐7. [PUBMED: 20169321] [DOI] [PubMed] [Google Scholar]
Souza 2014 {published data only}
- Souza LW, Souza SV, Botelho AC. Distal and lateral toenail onychomycosis caused by trichophyton rubrum: treatment with photodynamic therapy based on methylene blue dye. Anais Brasileiros de Dermatologia 2014;89(1):184‐6. [PUBMED: 24626676] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tardivo 2015 {published data only}
- Tardivo JP, Wainwright M, Baptista M. Small scale trial of photodynamic treatment of onychomycosis in Sao Paulo. Journal of Photochemistry and Photobiology. B, Biology 2015;150:66‐8. [PUBMED: 25835504] [DOI] [PubMed] [Google Scholar]
Tietz 2013 {published data only (unpublished sought but not used)}
- Tietz HJ, Hay R, Querner S, Delcker A, Kurka P, Merk HF. Efficacy of 4 weeks topical bifonazole treatment for onychomycosis after nail ablation with 40% urea: a double‐blind, randomized, placebo‐controlled multicenter study. Mycoses 2013;56(4):414‐21. [CENTRAL: CN‐00964322] [DOI] [PubMed] [Google Scholar]
Zaug 1995 {published data only}
- Zaug M. Amorolfine nail lacquer: Clinical experience in onychomycosis. Journal of the European Academy of Dermatology and Venereology 1995;4(Suppl 1):S23‐30. [CENTRAL: CN‐00174369] [Google Scholar]
Zhang 2012a {published data only (unpublished sought but not used)}
- Zhang RN, Wang DK, Zhuo FL, Duan XH, Zhang XY, Zhao JY. Long‐pulse Nd:YAG 1064‐nm laser treatment for onychomycosis. Chinese Medical Journal 2012;125(18):3288‐91. [CENTRAL: CN‐00967772] [PubMed] [Google Scholar]
Zhou 2016 {published data only (unpublished sought but not used)}
- Zhou BR, Lu Y, Permatasari F, Huang H, Li J, Liu J, et al. The efficacy of fractional carbon dioxide (CO2) laser combined with luliconazole 1% cream for the treatment of onychomycosis: A randomized, controlled trial. Medicine 2016;95(44):e5141. [CENTRAL: CN‐01306946] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
Anonymous 2002 {published data only}
- Anonymous. A frequently underestimated dermatomycosis. Long‐term therapeutic success with fungicidal effect. MMW Fortschritte der Medizin 2002;144(43):52‐3. [PUBMED: 12534020] [PubMed] [Google Scholar]
Bagatell 1977 {published data only}
- Bagatell FK. Topical therapy for onychomycosis. Archives of Dermatology 1977;113(3):378. [CENTRAL: CN‐00465913] [PubMed] [Google Scholar]
Barquero 2007 {published data only}
- Barquero N. Treatment of toenail DSO onychomycosis by T rubrum with topical 1% terbinafine gel. Journal of the American Academy of Dermatology 2007;56(2):AB113. [CENTRAL: CN‐00616061] [Google Scholar]
Butareva 1986 {published data only}
- Butareva TA, Kukushkin AM, Unzhakov VP, Nemkaeva RM. 8‐Hydroxyquinoline derivatives in the treatment of patients with onychomycoses. Vestnik Dermatologii i Venerologii 1986;12:50‐3. [PUBMED: 2951932] [PubMed] [Google Scholar]
Emokpare 1977 {published data only}
- Emokpare NA. Clinical evaluation of a new antifungal agent clotrimazole in dermatomycoses. Zeitschrift fur Arztliche Fortbildung (Jena) 1977;71(3):144‐6. [PUBMED: 139766] [PubMed] [Google Scholar]
EUCTR2008‐002427‐90 {unpublished data only}
- EUCTR2008‐002427‐90. Double‐blind study of the clinical and mycological equivalence of Loceryl® (Amorolfine, film‐forming solution at 5%) and its generic in the treatment of onychomycosis without the nail matrix [Etude en double aveugle de l’équivalence clinique et mycologique du Locéryl® (Amorolfine, solution filmogène à 5%) et de son générique dans le traitement des onychomycoses sans atteinte de la matrice unguéale]. www.clinicaltrialsregister.eu/ctr‐search/search?query=2008‐002427‐90 (first received 20 October 2008).
George 1991 {published data only}
- George MA. A comparison of three treatments for fungal nail infection. British Journal of Podiatric Medicine 1991;46:134‐5. [CENTRAL: CN‐00252045] [Google Scholar]
Grant 1974 {published data only}
- Grant LV. A further look at the treatment of onychomycosis with topical glutaraldehyde. Journal of the American Podiatry Association 1974;64(3):158‐60. [CENTRAL: CN‐00250917] [DOI] [PubMed] [Google Scholar]
JPRN‐JapicCTI‐101143 {unpublished data only}
- JPRN‐JapicCTI‐101143. A placebo‐controlled, parallel group study of HTU‐520 in patients with onychomycosis. apps.who.int/trialsearch/Trial2.aspx?TrialID=JPRN‐JapicCTI‐101143 (first received 24 May 2010).
Klima 1976 {published data only}
- Klima J. A report on the clinical experiences from the comparison of the effectiveness of 0.2% and 0.5% solutions of the antimycotic agent VUFB 9244 (working name Jopargin). Ceskoslovenska Dermatologie 1976;51(6):404‐6. [PUBMED: 137783] [PubMed] [Google Scholar]
Kull 1972 {published data only}
- Kull E. Local treatment of skin and nail mycoses with Daktarin, a new broad‐spectrum antifungal agent. Testing results of a group of dermatologists in practice. Schweizerische Rundschau fur Medizin Praxis 1972;61(42):1308‐10. [PUBMED: 4263785] [PubMed] [Google Scholar]
Mathur 1973 {published data only}
- Mathur SM, Agarwal RK. Clinical trial of Jadit in superficial mycoses. Indian Journal of Dermatology, Venereology and Leprology 1973;39(6):266‐9. [PUBMED: 29139428] [PubMed] [Google Scholar]
NCT00253305 {unpublished data only}
- NCT00253305. Topical gel anti‐fungal agent for tinea unguium. clinicaltrials.gov/ct2/show/NCT00253305 (first received 15 November 2005).
NCT02549001 {unpublished data only}
- NCT02549001. Study to evaluate the efficacy and safety of P‐3058 10% nail solution in the treatment of toenail onychomycosis. www.clinicaltrials.gov/ct2/show/NCT02549001 (first received 14 September 2015).
Park 2017 {published data only}
- Park KY, Suh JH, Kim BJ, Kim MN, Hong CK. Randomized clinical trial to evaluate the efficacy and safety of combination therapy with short‐pulsed 1,064‐nm neodymium‐doped yttrium aluminium garnet laser and amorolfine nail lacquer for onychomycosis. Annals of Dermatology 2017;29(6):699‐705. [CENTRAL: CN‐01568577; PUBMED: 29200757] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramm 1994 {published data only}
- Ramm S. Loceryl nail lacquer ‐ a new treatment of onychomycosis [Loceryl nagellack ‐ neuer ansatz zur therapie der nagelmykose]. Aktuelle Dermatologie 1994;20(9/10):335‐7. [CENTRAL: CN‐00727297] [Google Scholar]
Rüping 1993a {published data only}
- Ruping KW, Haas PJ. Treatment onychomycoses‐‐bifonazole nail set in comparison with urea with ciclopiroxolamine formulation [Behandlung von onychomykosen‐‐bifonazol‐nagelset im vergleich zur harnstoffrezeptur mit ciclopiroxolamin]. Zeitschrift fur Arztliche Fortbildung 1993;87(5):425‐9. [CENTRAL: CN‐00094233] [PubMed] [Google Scholar]
Rüping 1993b {published data only}
- Rüping KW, Haas PJ. Treatment of onychomycoses. Zeitschrift für Allgemeinmedizin 1993;69(20‐21):568‐72. [CENTRAL: CN‐00257388] [Google Scholar]
Schubert 1973 {published data only}
- Schubert E. Clinical experience in the treatment of nail mycoses with the new antibiotic Bay b5097 (clotrimazol). Zeitschrift fur Hautkrankheiten 1973;48(21):887‐91. [PUBMED: 4273270] [PubMed] [Google Scholar]
Weuta 1972 {published data only}
- Weuta H. Clotrimazol cream and solution‐‐clinical assessment in an open trial. Arzneimittel‐Forschung 1972;22(8):1295‐9. [PUBMED: 4264179] [PubMed] [Google Scholar]
Xu 2017 {published data only}
- Xu TH, Su L, Huang D, Li YH, Gao XH, Chen HD. Clinical efficacy of 0.3‐ms pulsed 1,064 nm Nd:YAG laser for onychomycosis. Journal of Clinical Dermatology 2017;46(6):450‐4. [CENTRAL: CN‐01404845] [Google Scholar]
Yao 2016 {published data only}
- Yao Y, Wang XH. Clinical observation of the effects of focused ultrasound combined traditional Chinese medicine on neurodermatitis in middle and aged patients. Journal of the American Geriatrics Society 2016;64:S338. [Google Scholar]
References to ongoing studies
ACTRN12618000131257 {unpublished data only}
- ACTRN12618000131257. Phase I, first in human (FIH), randomised, double‐blind, placebo‐controlled multiple ascending dose study in healthy volunteers with mild to moderate onychomycosis. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=374039 (first received 30 January 2018).
ChiCTR‐INR‐17013504 {unpublished data only}
- ChiCTR‐INR‐17013504. 2940‐nm Er:YAG fractional laser combined with amorolfine hydrochloride and amorolfine hydrochloride for treating onychomycosis: a prospective, randomized, controlled, evaluator‐blinded, parallel‐group clinical trial. www.chictr.org.cn/showproj.aspx?proj=23130 (accessed 16 April 2018).
DRKS00007709 {unpublished data only}
- DRKS00007709. Treatment of onychomycosis with a short‐pulsed Nd:YAG Laser (1064nm). apps.who.int/trialsearch/Trial2.aspx?TrialID=DRKS00007709 (first received 20 January 2015).
EUCTR2016‐001204‐39 {unpublished data only}
- EUCTR2016‐001204‐39. A multi‐centre, randomized, two‐armed, parallel group and evaluator‐blinded study of efficacy and safety of topical MOB015B in the treatment of mild to moderate distal subungual onychomycosis (DSO). www.clinicaltrialsregister.eu/ctr‐search/search?query=2016‐001204‐39 (first received 15 September 2016).
EUCTR2016‐003784‐19 {unpublished data only}
- EUCTR2016‐003784‐19. Phase III, multicentre, randomised, double‐blind, parallel‐group, clinical trial to evaluate the efficacy and safety of a new medicated nail lacquer for the treatment of toenail fungal infection. www.clinicaltrialsregister.eu/ctr‐search/search?query=2016‐003784‐19 (first received 18 April 2017).
JapicCTI‐183840 {unpublished data only}
- JapicCTI‐183840. A phase II multicenter, randomized, double‐blind, vehicle‐controlled, parallel‐group study to investigate the efficacy and safety of ME1111 for 48 weeks of treatment in patients with mild to moderate onychomycosis. www.clinicaltrials.jp/user/showCteDetailE.jsp?japicId=JapicCTI‐183840 (first received 22 January 2018).
NCT02644551 {unpublished data only}
- NCT02644551. The efficacy of CELEXT07 in the treatment of toenail onychomycosis. www.clinicaltrials.gov/ct2/show/NCT02644551 (first received 1 January 2016).
NCT02812043 {unpublished data only}
- NCT02812043. Comparison between long‐pulsed Nd:YAG, amorolfine and combination treatment in treating non‐dermatophyte onychomycosis. www.clinicaltrials.gov/ct2/show/NCT02812043 (first received 23 June 2016).
NCT02859519 {unpublished data only}
- NCT02859519. A multi‐centre, double‐blind, randomized, vehicle‐controlled study of efficacy and safety of topical MOB015B in the treatment of mild to moderate distal subungual onychomycosis (DSO). www.clinicaltrials.gov/ct2/show/NCT02859519 (first received 9 August 2016).
NCT02866032 {unpublished data only}
- NCT02866032. Study to evaluate the efficacy and safety of topical MOB015B in the treatment of mild to moderate distal subungual onychomycosis (DSO). www.clinicaltrials.gov/ct2/show/NCT02866032 (first received 15 August 2016).
NCT02961634 {unpublished data only}
- NCT02961634. Study efficacy and safety in comparative use of investigational product adjuvant treatment in onychomycosis. www.clinicaltrials.gov/ct2/show/NCT02961634 (first received 11 November 2016).
NCT03098342 {unpublished data only}
- NCT03098342. Comparison of efficacy and safety between methylene blue‐mediated photodynamic therapy and 5% amorolfine nail lacquer for toenail onychomycosis treatment. www.clinicaltrials.gov/ct2/show/NCT03098342 (first received 31 March 2017).
NCT03814343 {unpublished data only}
- NCT03814343. Topical amphotericin B in 30% dimethylsulphoxide in treating of non‐dermatophytes onychomycosis. www.clinicaltrials.gov/ct2/show/NCT03814343 (first received 24 January 2019).
Additional references
Akkus 2017
- Akkus G, Evran M, Gungor D, Karakas M, Sert M, Tetiker T. Tinea pedis and onychomycosis frequency in diabetes mellitus patients and diabetic foot ulcers. A cross sectional‐observational study. Pakistan Journal of Medical Sciences 2016;32(4):891‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Anderson 1983
- Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983;220(4596):524–7. [PUBMED: 6836297 ] [DOI] [PubMed] [Google Scholar]
Baran 2008
- Baran R, Hay RJ, Garduno JI. Review of antifungal therapy, part II: treatment rationale, including specific patient populations. Journal of Dermatologic Treatment 2008;19(3):168‐75. [PUBMED: 18569273] [DOI] [PubMed] [Google Scholar]
Baran 2011
- Baran R. The nail in the elderly. Clinics in Dermatology 2011;29(1):54‐60. [PUBMED: 21146733] [DOI] [PubMed] [Google Scholar]
Barber 2006
- Barber K, Claveau J, Thomas R. Review of treatment for onychomycosis: consideration for special populations. Journal of Cutaenous Medicine and Surgery 2006;10(6 Suppl 2):S48‐53. [DOI: 10.2310/7750.2006.00054] [DOI] [Google Scholar]
Bristow 2014
- Bristow IR. The effectiveness of lasers in the treatment of onychomycosis: a systematic review. Journal of Foot and Ankle Research 2014;7:34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Centre for Evidence‐Based Medicine
- Centre for Evidence‐Based Medicine. Number needed to treat, 2014. www.cebm.net/number‐needed‐to‐treat‐nnt/ (accessed 9 September 2015).
Crowley 2015
- Crowley JJ, Weinberg JM, Wu JJ, Robertson AD, Voorhees AS, National Psoriasis Foundation. Treatment of nail psoriasis: best practice recommendations from the medical board of the National Psoriasis Foundation. JAMA Dermatology 2015;151(1):87‐94. [DOI] [PubMed] [Google Scholar]
CS‐COUSIN
- Cochrane Skin. Core Outcomes Set Initiative (CS‐COUSIN). skin.cochrane.org/core‐outcomes‐set‐initiative‐csg‐cousin (accessed 30 November 2018).
Dermik 2003
- Dermik Laboratories. Penlac Nail Lacquer (ciclopirox) Topical Solution 8% (Product insert). www.accessdata.fda.gov/drugsatfda_docs/label/2004/21022s004lbl.pdf (accessed 25 October 2018).
Dijkman 2009
- Dijkman B, Kooistra B, Bhandari M, for the Evidence‐Based Surgery Working Group. How to work with a subgroup analysis. Canadian Journal of Surgery 2009;52(6):515‐22. [PUBMED: 2792383] [PMC free article] [PubMed] [Google Scholar]
Dwan 2008
- Dwan K, Altman DG, Arnaiz JA, Bloom J, Chan A, Cronin E, et al. Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PLoS One 2008;3(8):e3081. [PUBMED: 18769481] [DOI] [PMC free article] [PubMed] [Google Scholar]
Döner 2011
- Döner N, Yasar S, Ekmekçi TR. Evaluation of obesity‐associated dermatoses in obese and overweight individuals [Obezite ile iliskili dermatozlarin obezlerde ve asiri kilolularda arastirilmasi]. Turkderm 2011;45(3):146‐51. [EMBASE: 2011536948] [Google Scholar]
Elewski 2016
- Elewski BE, Gupta AK, Rosen T, Caldwell BD, Pariser DM, Kircik L, et al. Onychomycosis: Does cure equate to treatment success?. Journal of Drugs in Dermatology 2016;15(5):626‐32. [PUBMED: 27168271] [PubMed] [Google Scholar]
Faergemann 2003
- Faergemann J, Baran R. Epidemiology, clinical presentation and diagnosis of onychomycosis. British Journal of Dermatology, Suppl 2003;149(65):1‐4. [EMBASE: 2003465096] [DOI] [PubMed] [Google Scholar]
Fukunaga 2013
- Fukunaga A, Washio K, Ogura K, Taguchi K, Chiyomaru K, Ohno Y, et al. Onychomycosis as a warning sign for peripheral arterial disease. Acta Dermatology Venereology 2013;93(6):747‐8. [DOI] [PubMed] [Google Scholar]
Galderma 2011
- Galderma. Loceryl Nail Lacquer (amorolfine) (Product insert). medicines.org.uk/emc/files/pil.1411.pdf (accessed 20 December 2019).
GRADEPro [Computer program]
- McMaster University. GRADEpro GDT. McMaster University, 2015.
Gupta 1994
- Gupta AK, Sauder DN, Shear NH. Antifungal agents: an overview. Part II. Journal of the American Academy of Dermatology 1994;30(6):911‐933. [EMBASE: 1994177736] [DOI] [PubMed] [Google Scholar]
Gupta 1997
- Gupta AK, Lynde CW, Jain HC, Sibbald RG, Elewski BE, Daniel CR 3rd, et al. A higher prevalence of onychomycosis in psoriatics compared with non‐psoriatics: a multicentre study. British Journal of Dermatology 1997;136(5):786‐9. [EMBASE: 1997197390] [PubMed] [Google Scholar]
Gupta 2000
- Gupta AK, Taborda P, Taborda V, Gilmour J, Rachlis A, Salit I, et al. Epidemiology and prevalence of onychomycosis in HIV‐positive individuals. International Journal of Dermatology 2000;39(10):746‐53. [EMBASE: 2000387514] [DOI] [PubMed] [Google Scholar]
Gupta 2012
- Gupta AK, Drummond‐Main C, Cooper EA, Brintnell W, Piraccini BM, Tosti A. Systematic review of nondermatophyte mold onychomycosis: diagnosis, clinical types, epidemiology, and treatment. Journal of the American Academy of Dermatology 2012;66(3):494‐502. [EMBASE: 2012113486] [DOI] [PubMed] [Google Scholar]
Gupta 2013
- Gupta AK, Paquet M, Simpson FC. Therapies for the treatment of onychomycosis. Clinics in Dermatology 2013;31(5):544‐54. [EMBASE: 2013610881] [DOI] [PubMed] [Google Scholar]
Gupta 2014a
- Gupta AK, Simpson FC. Investigational drugs for onychomycosis. Expert Opinion on Investigational Drugs 2014;23(1):97‐106. [EMBASE: 2013778604] [DOI] [PubMed] [Google Scholar]
Gupta 2014b
- Gupta AK, Daigle D, Foley KA. Topical therapy for toenail onychomycosis: an evidence‐based review. American Journal of Clinical Dermatology 2014;15(6):489‐502. [EMBASE: 25257931] [DOI] [PubMed] [Google Scholar]
Gupta 2015a
- Gupta AK, Sibbald RG, Andriessen A, Belley R, Boroditsky A, Botros M, et al. Toenail onychomycosis‐A Canadian approach with a new transungual treatment: Development of a clinical pathway. Journal of Cutaneous Medicine and Surgery 2015;19(5):440‐9. [PUBMED: 25857439] [DOI] [PubMed] [Google Scholar]
Gupta 2015b
- Gupta AK, Daigle D, Foley KA. Network meta‐analysis of onychomycosis treatments. Skin Appendage Disorders 2015;1(2):74‐81. [PUBMED: 27170937] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gupta 2016b
- Gupta AK, Simpson FC, Heller DF. The future of lasers in onychomycosis. Journal of Dermatological Treatment 2016;27(2):167‐72. [PUBMED: 26270468] [DOI] [PubMed] [Google Scholar]
Gupta 2017
- Gupta AK, Versteeg SG. A critical review of improvement rates for laser therapy used to treat toenail onychomycosis. Journal of the European Academy of Dermatology and Venereology 2017;31(7):1111‐8. [PUBMED: 28294418] [DOI] [PubMed] [Google Scholar]
Hay 2011
- Hay RJ, Baran R. Onychomycosis: a proposed revision of the clinical classification. Journal of the American Academy Dermatology 2011;65(6):1219‐27. [EMBASE: 2011628916] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Deeks JJ, Altman DJ. Chapter 16: Special topics in statistics. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2017
- Higgins JP, Altman DG, Sterne JA. editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Higgins 2019
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). The Cochrane Collaboration, 2019. Available from www.training.cochrane.org/handbook.
Lipner 2018
Lipner 2019
- Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. Journal of the American Academy of Dermatology 2019;80(4):853‐67. [PUBMED: 29959962] [DOI] [PubMed] [Google Scholar]
Ozkan 2013
- Ozkan F, Ozturk P, Ozyurt K, Inci MF, Kalender AM, Bakan B, et al. Frequency of peripheral arterial disease and venous insufficiency in toenail onychomycosis. Journal of Dermatology 2013;40(2):107‐10. [DOI] [PubMed] [Google Scholar]
Papini 2013
- Papini M, Cicoletti M, Fabrizi V, Landucci P. Skin and nail mycoses in patients with diabetic foot. Giornale Italiano di Dermatologia e Venereologia 2013;148(6):603‐8. [PubMed] [Google Scholar]
Piraccini 2008
- Piraccini BM, Rech G, Tosti A. Photodynamic therapy of onychomycosis caused by Trichophyton rubrum. Journal of the American Academy of Dermatology 2008;59(5 Suppl):S75‐6. [EMBASE: 2008471503] [DOI] [PubMed] [Google Scholar]
Piraccini 2010
- Piraccini BM, Sisti A, Tosti A. Long‐term follow‐up of toenail onychomycosis caused by dermatophytes after successful treatment with systemic antifungal agents. Journal of the American Academy of Dermatology 2010;62(3):411‐4. [PUBMED: 20159308] [DOI] [PubMed] [Google Scholar]
Reich 2011
- Reich A, Szepietowski JC. Health‐related quality of life in patients with nail disorders. American Journal of Clinical Dermatology 2011;12(5):313‐20. [EMBASE: 2011453579] [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rigopoulos 2017
- Rigopoulos D, Papanagiotou V, Daniel R 3rd, Piraccini BM. Onychomycosis in patients with nail psoriasis: a point to point discussion. Mycoses 2017;60(1):6‐10. [DOI] [PubMed] [Google Scholar]
Rock 2007
- Rock FL, Mao W, Yaremchuk A, Tukalo M, Crépin T, Zhou H, et al. An antifungal agent inhibits an aminoacyl‐tRNA synthetase by trapping tRNA in the editing site. Science 2007;213(5832):1759‐61. [EMBASE: 2007311724] [DOI] [PubMed] [Google Scholar]
Rosen 2015
- Rosen T, Fallon Friedlander S, Kircik L, Zirwas MJ, Stein Gold L, Bhatia N, et al. Onychomycosis: Epidemiology, diagnosis, and treatment in a changing landscape. Journal of Drugs in Dermatology 2015;14(3):223‐28. [PubMed] [Google Scholar]
Rossaneis 2013
- Rossaneis MA, Haddad MD, Mantovani MF, Marcon SS, Pissinati PS. Foot ulceration in patients with diabetes: a risk analysis. British Journal of Nursing 2017;26(6):S6‐S14. [DOI] [PubMed] [Google Scholar]
Ryan 2016a
- Ryan R, Hill S. How to GRADE the quality of the evidence. Cochrane Consumers and Communication Group. Version 3.0 December 2016. cccrg.cochrane.org/author‐resources.
Ryan 2016b
- Ryan R, Synnot A, Hill S. Describing results. Cochrane Consumer and Communications Group. Version 2.0 December 2016. cccrg.cochrane.org/author‐resources.
Schulz 2010
- Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c332. [PUBMED: 20332509] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sigurgeirsson 2002
- Sigurgeirsson B, Olafsson JH, Steinsson JB, Paul C, Billstein S, Evans EG. Long‐term effectiveness of treatment with terbinafine vs itraconazole in onychomycosis: a 5‐year blinded prospective follow‐up study. Archives of Dermatology 2002;138(3):353‐7. [DOI] [PubMed] [Google Scholar]
Sigurgeirsson 2014
- Siguregeirsson B, Baran R. The prevalence of onychomycosis in the global population: a literature study. Journal of the European Academy of Dermatology and Venereology 2014;28(11):1480‐91. [EMBASE: 24283696] [DOI] [PubMed] [Google Scholar]
Szepietowski 2006
- Szepietowski JC, Reich A, Garlowska E, Kulig M, Baran E. Factors influencing coexistence of toenail onychomycosis with tinea pedis and other dermatomycoses: a survey of 2761 patients. Archives of Dermatology 2006;42(10):1279‐84. [EMBASE: 2006511256] [DOI] [PubMed] [Google Scholar]
Tosti 1998
- Tosti A, Piraccini BM, Stinchi C, Colombo MD. Relapses of onychomycosis after successful treatment with systemic antifungals: a three‐year follow‐up. Dermatology (Basel, Switzerland) 1998;197(2):162‐6. [PUBMED: 9732167] [DOI] [PubMed] [Google Scholar]
U.S. FDA 2015
- U.S. Food, Drug Administration. Medical Devices and Clinical Trial Design for the Treatment or Improvement in the Appearance of Fungally‐Infected Nails ‐ Draft Guidance for Industry and FDA Staff 2015. www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM431312.pdf (accessed 12 October 2017).
Valeant 2004
- Valeant Bermuda. Penlac® Nail Lacquer (ciclopirox) Topical Solution, 8%. www.accessdata.fda.gov/drugsatfda_docs/label/2004/21022s004lbl.pdf (accessed 9 September 2015).
Ventura 2017
- Ventura A, Mazzeo M, Gaziano R, Galluzzo M, Bianchi L, Campione E. New insight into the pathogenesis of nail psoriasis and overview of treatment strategies. Drug Design, Development and Therapy 2017;11:2527‐35. [PUBMED: 28919705] [DOI] [PMC free article] [PubMed] [Google Scholar]
Welsh 2010
- Welsh O, Vera‐Cabrera L, Welsh E. Onychomycosis. Clinics in Dermatology 2010;28(2):151‐9. [EMBASE: 2010196893] [DOI] [PubMed] [Google Scholar]
Zaias 1972
- Zaias N. Onychomycosis. Archives of Dermatology 1972;105(2):263‐74. [EMBASE: 4258535] [PubMed] [Google Scholar]
References to other published versions of this review
Crawford 2007
- Crawford F, Hollis S. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database of Systematic Reviews 2007, Issue 3. [DOI: 10.1002/14651858.CD001434.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gupta 2016a
- Gupta AK, Simpson F, Daigle D, Villanueva E, John D, Foley K. Topical and device‐based treatments for fungal infections of the toenails. Cochrane Database of Systematic Reviews 2016, Issue 2. [DOI: 10.1002/14651858.CD012093] [DOI] [PMC free article] [PubMed] [Google Scholar]