

Abstract
Objective:
The present study examined forgiveness of others, self-forgiveness, sleep, and health in a nationally representative sample of United States adults. It was hypothesised that sleep would mediate the associations of forgiveness of others and self-forgiveness with health.
Design:
A nationally representative survey of 1,423 United States adults.
Main Outcome Measures:
Measures included forgiveness of others, self-forgiveness, sleep quantity, sleep quality, psychological distress, life satisfaction, and self-rated physical health.
Results:
Forgiveness of others (Beta = .20, p < .001) and self-forgiveness (Beta = .11, p < .01) were associated with sleep and forgiveness of others (Beta = .24, p < .001) and self-forgiveness (Beta = .27, p < .001) were associated with health. Sleep was associated with health (Beta = .45, p < .001) and also acted as a mediator of the associations of forgiveness of others (Beta = .09, p < .01) and self-forgiveness (Beta = .05, p < .01) with health.
Conclusions:
Forgiveness of others and self-forgiveness may attenuate emotions such as anger, regret, and rumination and to provide a buffer between one’s own and others’ offenses occurring during the day and offer a restful mental state that supports sound sleep which, in turn, is associated with better health.
Keywords: forgiveness of others, self-forgiveness, sleep, health, mediation
The present study examines how two dimensions of forgiveness, forgiveness of others and self-forgiveness, interface with the sleep and health relationship. Research on sleep and health has a long and rich history and evidence supports the notion that sleep is a critical factor in support of good health (Luyster, Strollo, Zee, & Walsh, 2012). Moreover, sleep deficiency is a growing issue in society that is related to impaired immune system functioning and increased risk for cardiovascular disease, diabetes, obesity, and cancer (Luyster et al., 2012). A contributor to sleep deficiency is stress, (Åkerstedt, 2006) thus, it is important to understand how people cope with stress in order to promote good sleep. Because of their stress-reducing properties, (Toussaint, Webb, & Hirsch, 2017; Worthington & Scherer, 2004) forgiveness of others and self-forgiveness might serve as coping styles that support good sleep and consequently promote good health. Research has shown that forgiveness of others and self-forgiveness are important factors in health (Cheadle & Toussaint, 2015), but much less research has focused on how forgiveness of others and self-forgiveness might be related to sleep and how this relationship might support health. The present study, therefore, aims to examine relationships of forgiveness of others and self-forgiveness with sleep and further aims to understand to what extent sleep might serve as an explanatory mechanism of the forgiveness and health relationship.
Forgiveness
Forgiveness of others entails reducing negative and increasing positive thoughts, feelings, and behaviours toward an offender (Berry, Worthington, O’Connor, Parrott III, & Wade, 2005). Similarly, self-forgiveness involves reducing self-condemning feelings and behaviours such as shame, guilt, blame, and rumination and increasing a more compassionate, loving, and accepting view of oneself (Worthington, 2013). Individuals who demonstrate tendencies toward forgiving others or oneself across time and place are considered high on the trait of forgiveness of others or self-forgiveness. State forgiveness of others and state self-forgiveness are often described as being the result of a process of working toward forgiving others or oneself. States are distinctly different constructs than traits, and states involve starting points, processes/steps, and outcomes. In the present study, the focus was on forgiveness of others and self-forgiveness as personality characteristics because traits influence health and health-related outcomes more consistently and more extensively than states (Low et al., 2011; Pressman & Cohen, 2005).
Forgiveness and Health
Both forgiveness of others and self-forgiveness are important in promoting good health. Forgiveness of others and self-forgiveness are both associated with improved mental and physical health, less pain, and better neurologic, physiologic, and immune function (Toussaint, Worthington Jr., & Williams, 2015). Forgiveness has been shown to be associated with less psychological distress and increased forgiveness is associated with reduced stress-related disorders (Toussaint, Shields, Dorn, & Slavich, 2016). Importantly, forgiveness is also related to greater life satisfaction (Kaleta & Mróz, 2018). In addition, forgiveness is positively correlated with better physical health, health behaviours, and with physiological properties indicative of better health, including fewer health symptoms, improved cardiovascular responses to stress, decreased diagnosis of cardiovascular diseases, and lower mortality rates (Friedberg, Suchday, & Shelov, 2007; Krause & Hayward, 2013; Lawler et al., 2003; Lawler et al., 2005; Seawell, Toussaint, & Cheadle, 2014; Toussaint & Cheadle, 2009; Toussaint, Owen, & Cheadle, 2012; Waltman et al., 2009; Webb, Hirsch, Visser, & Brewer, 2013). These associations are likely mediated by psychosocial factors. For instance, Lawler et al. (2005) examined four separate mediators of the forgiveness and health connection including spirituality, social skills, negative affect, and stress. Results of this early investigation found that spirituality and social skills were partial mediators of the state forgiveness and health association, but they fully mediated the trait forgiveness and health association. Negative affect and stress were full mediators of state and trait forgiveness and their associations with health. More recent work confirms that reduced stress and negative affect, as well as, health behaviours, and physiological processes are important mediators of the forgiveness and health association (Cheadle & Toussaint, 2015; Toussaint et al., 2012). Of all the health-related mechanisms that have been examined as explanatory factors of the forgiveness and health association, sleep has not yet been given full consideration as a mediating variable.
Sleep and Health
Like forgiveness, sleep is an important component of good overall health and well-being. High quality sleep has been shown to be associated with healthy weight maintenance, an improved immune system, improved learning and memory, and reductions in depressive symptoms (Besedovsky, Lange, & Born, 2012; Chaput & Tremblay, 2012; Gangwisch et al., 2010; Stickgold, 2005). Poor quality sleep has been shown to be associated with poor health outcomes including cardiovascular disease, cancer, mortality, depression, obesity, and suicidal thoughts and behaviours (Beccuti & Pannain, 2011; Cappuccio, Cooper, D’Elia, Strazzullo, & Miller, 2011; Cappuccio, D’Elia, Strazzullo, & Miller, 2010; Li, Wu, Gan, Qu, & Lu, 2016; Pigeon, Pinquart, & Conner, 2012). Overall, research shows that both forgiveness and sleep are connected to good health, but the interplay of forgiveness and sleep in promoting good health has not been examined.
Forgiveness and Sleep
Though much extant research links forgiveness to other health behaviours and outcomes (Cheadle & Toussaint, 2015), research examining the connections between forgiveness and sleep is scant. That which has been done is limited by small, unrepresentative samples. Only a handful of studies exist that have even briefly considered sleep and forgiveness. In two different studies, one with a sample of 81 middle-aged adults (Mage = 43) (Lawler et al., 2005) and one with a sample of 80 middle-aged adults (Mage = 42) (Lawler-Row, 2010), both trait and state forgiveness of others were correlated with sleep quality (rs ≈ .40). Another study of 277 Midwestern Catholic college students showed smaller correlations (rs ≈ .15) between both trait and state forgiveness of others and sleep quality and daytime wakefulness, but no correlation between trait and state forgiveness and sleep interference (Stoia-Caraballo et al., 2008). In another study of 268 pregnant Iranian women (Mage = 23), forgiveness of others was inversely related (r = −.26) to poor sleep quality (Shirazi, Fardin, Arab, Sanagoue, & Alisofi, 2016). Furthermore, clinical mindfulness-based interventions (MBIs), which have been shown to increase the tendency to forgive following a conflict (Taylor et al., 2016), have also been shown to improve symptoms of insomnia (Wang et al., 2018), suggesting a possible link between forgiveness and sleep. In summary, in generally small and unrepresentative samples, both trait and state forgiveness of others appear to be related to sleep quality, but no known research has examined state or trait self-forgiveness and sleep outcomes.
Conceptual Model.
The present study was based on an integrated model of the above empirical literature with conceptual models of forgiveness, sleep, and health. One conceptualization (Stoia-Caraballo et al., 2008) of the potential forgiveness and sleep relationship suggests that forgiveness of others will improve sleep outcomes because it reduces anger and rumination, and this is consistent with models and evidence showing that anger, rumination, and emotional dysregulation interfere with sleep (Ballesio, Ottaviani, & Lombardo, 2018; Gruber & Cassoff, 2014; Hisler & Krizan, 2017; Stoia-Caraballo et al., 2008). Additionally, forgiveness of others may relate to better sleep because it reduces interpersonal distress resulting from interpersonal conflicts (Gunn, Troxel, Hall, & Buysse, 2014), resulting in activation of brain areas involved in theory of mind and empathy, such as the precuneus, right inferior parietal regions, and the dorsolateral prefrontal cortex (Ricciardi et al., 2013). These are readily identifiable mechanisms and models motivating the hypothesis that forgiveness of others is related to better sleep (Forgiveness 2192 Sleep). Though there is no empirical literature on self-forgiveness and sleep, self-forgiveness has been hypothesised to function in a similarly healthy way by reducing anger toward the self and associated self-focused rumination, emotional dysregulation, and distress (Toussaint et al., 2017; Worthington, 2013).
Sleep can be considered under the broad category of health behaviours (Perry, Patil, & Presley-Cantrell, 2013), and theoretical and empirical work posit health behaviours as a mechanism linking forgiveness to health (Forgiveness 2192 Health Behaviour 2192 Health)(Toussaint & Webb, 2005; Webb et al., 2013). That is, forgiveness could be related to better mental and physical health because forgiveness promotes healthy behaviour. Considering sleep as a health behaviour (Perry et al., 2013), it is a viable assertion that forgiveness is related to health because it promotes a key health behaviour -- sleep. As such, both empirical evidence and conceptual models support the hypothesis that forgiveness will be beneficially related to sleep, and in turn, that sleep will be beneficially related to health (Forgiveness 2192 Sleep 2192 Health), thereby explaining some part of the association of forgiveness and health. This model is illustrated in Figure 1. However, this hypothesis has not been explicitly tested with respect to the interplay between all three constructs of forgiveness, sleep, and health, and specifically with self-forgiveness (vs. forgiveness of others).
Figure 1.
Conceptual model for the proposed associations of forgiveness, sleep, and health.
Present Study
The purpose of the present study was to examine the associations of forgiveness of others and self-forgiveness with sleep and health in a nationally representative sample of United States adults. Forgiveness of others and self-forgiveness have been related to a variety of health outcomes, but the connections of forgiveness of others and self-forgiveness with sleep have been little tested. Furthermore, sleep is known to be an important correlate and predictor of health, and the potential benefits of forgiveness of others and self-forgiveness for sleep might translate to improved health. For this reason, it is important to examine not only the association between forgiveness of others and self-forgiveness and sleep but also to examine the extent to sleep mediates the association between forgiveness of others and self-forgiveness and health. We expected that forgiveness of others and self-forgiveness would be positively related to sleep quantity, sleep quality, and overall health. We further expected that sleep would, in turn, be associated with better health and function to explain some part of the associations of forgiveness of others and self-forgiveness with health.
Method
Participants & Procedure
Data for this study were obtained from a long-running national survey. The survey is administered by the Survey Research Center at the University of Michigan and has run continuously since 1946. The main focus of the survey is American consumer attitudes. Fifty core questions assess personal finances, business conditions, and buying conditions. This study added items on the survey to collect data on additional psychosocial (e.g., forgiveness, self-esteem, perceived socio-economic status,) and health variables (e.g., distress, life-satisfaction, physical health, activity limitations, chronic health conditions). The survey has been used in numerous published studies and reports, but none have examined the present model of forgiveness, sleep, and health. Participants were a randomly selected and nationally representative sample of 1,423 United States adults interviewed by telephone. A sample of this size provides power equal to or greater than .97 for associations ≥ .10 using a two-tailed test at p < .05. Thus, all tests were adequately powered (Cohen, 1992). Interviews were conducted by telephone interviewers with a minimum of a high school diploma who were formally trained using extensive (400+ page) training manuals and simulations. The mean and median interview length was 35 and 34 minutes, respectively. Minimum interview length was 14 minutes and maximum was 115 minutes. The standard deviation was 12 minutes. Supervisory quality control teams oversee data collection, and rigorous data checking standards are employed. The representativeness of the sample derives from the random-digit dialing procedure used to contact participants (Waksberg, 1978), and the survey represents the adult United States population residing in the 48 contiguous states. Each month 300 new participants are recruited to the study. The present sample was an aggregate of five consecutive months of interviews and monthly response rates ranged from 69 to 71%.
Table 1 provides a summary of socio-demographic characteristics of the sample. Participant sex was 55% female. Race characteristics were 79% white, 10% black, 6% Hispanic, and 5% other races/ethnicities. Regarding marital status participants were 57% married, 17% separated/divorced, 6% widowed, and 20% never married. Participants were an average age of 44 (Mdn = 43; range = 18 – 93), with an average of 14 years of education, and the average range of household income was $40,000 - $49,999. Survey protocol and informed consent procedures were approved by the Institutional Review Board, and all subjects gave informed consent.
Table 1.
Sample Demographics
| Variable | M (SD) or percent distribution |
|---|---|
| Age | 44 (16) years |
| Gender | 55% female; 45% male |
| Race/ethnicity | 79% white, 10% black, 6% Hispanic, 5% other |
| Marital status | 57% married, 17% separated/divorced, 6% widowed, 20% never married |
| Education | 14 (3) years |
| Household income | $40,000-$49,999 |
Measures
Forgiveness.
Trait forgiveness of others and self-forgiveness scales were used (Musick, 2004; Musick & Williams, 1999; Webb, Toussaint, Kalpakjian, & Tate, 2010). These brief scales were originally built based on items from existing scales (Gorsuch & Hao, 1993; Idler et al., 2003; Mauger et al., 1992; Watson, Hood, Morris, & Hall, 1985; Watson, Morris, & Hood Jr, 1987). Forgiveness of others was a five-item index where three items were responded to on a 1 (never) to 5 (very often) scale and two items were responded to on a 1 (strongly agree) to 5 (strongly disagree) scale. A sample item is, “I have forgiven those who have hurt me.” Self-forgiveness was a two-item index where both items were responded to on a 1 (strongly agree) to 5 (strongly disagree) scale. A sample item is, “I find it hard to forgive myself for some of the things I have done wrong.” Items for respective scales were averaged and scored so that higher values represented higher levels of the construct. The forgiveness of others and self-forgiveness scales have been used in previous research and shown acceptable reliability (Musick, 2004; Musick & Williams, 1999; Webb et al., 2010). Internal consistency of the scales for the present study was .72 and .67, respectively.
Sleep.
Two items were used as global assessments of perceived sleep. Perceived sleep quantity was assessed using the item, “During the past 30 days, excluding naps, how many hours of actual sleep did you get at night on average?” This was an open-ended response format and the observed range of responses was one to twelve hours. Perceived sleep quality was assessed using the item, “During the past 30 days, how would you rate your sleep quality overall?” Responses were made on a 1 (very good) to 4 (very bad) response scale. This item was reverse scored so that higher values represented higher levels of sleep quality. Sleep quality and quantity assessments were based on a subset of two items from the Pittsburgh Sleep Quality Index (PSQI), which assesses self-reported sleep quality and quantity over the past 30 days (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). The PSQI has been found to be a reliable and valid measure of sleep quality and quantity in participants (Carpenter & Andrykowski, 1998; Mollayeva et al., 2016). Indeed, several studies have effectively assessed self-reported sleep using one or two questions about sleep quantity (Ikehara et al., 2009; Kakizaki et al., 2008; McElroy et al., 2006; Patel et al., 2004) or a single-item to assess sleep quality (Hublin, Partinen, Koskenvuo, & Kaprio, 2007; Verkasalo et al., 2005), similar to the present measures.
Health.
Health was assessed in a multidimensional fashion. Mental health was assessed using the K-6 index of psychological distress (Kessler et al., 2010). This is a six-item measure of non-specific distress experienced in the past 30 days intended for use in the general population. Items tap feelings of nervousness, restlessness, hopelessness, worthlessness, etc. and are responded to on a 1 (never) to 5 (very often) frequency scale. This scale has been used extensively in epidemiological and psychiatric research and has excellent psychometric properties. Items were averaged and scored so that higher values represented higher levels of the construct. The internal consistency of the scale in the present study was .83. Life satisfaction was assessed with the item, “Please think about your life as a whole. How satisfied are you with it? This item was responded to on a 1 (completely satisfied) to 5 (not at all satisfied) response scale. Physical health was assessed with the item, “Overall, how would you rate your health at the present time?” This item was responded to on a 1 (excellent) to 5 (poor) response scale. Single-item measures of life satisfaction and physical health are widely used in epidemiological research and have been shown to have acceptable reliability and validity (Bowling, 2005; Cheung & Lucas, 2014). Life-satisfaction and physical health items were reverse scored so that higher values represented higher levels of the construct.
Socio-demographics.
Socio-demographic variables measured included: sex, age, education, household income (13 categories, e.g., $30,000 – $34,999), race (i.e., White, Black, Hispanic, and other races/ethnicities), and marital status (i.e., married, separated/divorced, widowed, and never married).
Analyses
Descriptive statistics were computed, and Pearson correlations were run to examine bivariate correlations among the variables. To assess the suitability of the data for factor analyses Kaiser-Meyer-Olkin (KMO) test of sampling adequacy and Bartlett’s test of sphericity were examined. KMO values above .6 and significance (p < .05) of Bartlett’s test of sphericity indicate that the data are suitable for factor analysis (Tabachnick & Fidell, 2013). Measurement models examined the fit of the sleep and health variables to a single- versus two-factor model. Structural latent variable models were then used to test study hypotheses and examine the associations between forgiveness, sleep, and health. Bootstrapping methods were used to estimate indirect effects. As suggested by Kline (Kline, 2015), fit statistics used to evaluate measurement and structural models were chi-square, confirmatory fit index (CFI), and root mean square error of approximation (RMSEA). Models were adjusted for effects of sex, age, education, household income, race, and marital status. Statistical significance was set at p < .05. In the structural equation model five structural paths were key to testing our hypotheses, so we used a Bonferroni adjustment of .05/5 to arrive at p < .01 as our significance level for the structural model.
Results
Descriptive statistics and bivariate correlations for the main study variables are provided in Table 2. As hypothesised, forgiveness of others and self-forgiveness were significantly (p < .001) positively correlated, respectively, with sleep quantity (r = .12, r = .12), sleep quality (r = .16, r = .22), life satisfaction (r = .23, r = .24), and physical health (r = .25, r = .14) and inversely associated with psychological distress (r = −.41, r = −.40). Also as hypothesised, sleep quantity and more so sleep quality were significantly (p < .001) inversely associated, respectively, with psychological distress (r = −.20, r = −.39) and positively associated with life satisfaction (r =.16, r = .24) and physical health (r = .16, r = .27). Forgiveness of others and self-forgiveness were positively correlated (r = .38, p < .001), sleep quantity and sleep quality were positively correlated (r = .38, p < .001), and psychological distress was inversely correlated with life satisfaction (r = −.37, p < .001) and physical health (r = −.37, p < .001) while the latter two variables were positively correlated (r = .31, p < .001).
Table 2.
Bivariate Correlations for Study Variables
| M | SD | 1. | 2. | 3. | 4. | 5. | 6. | |
|---|---|---|---|---|---|---|---|---|
| 1. Forgiveness of others | 3.98 | 1.20 | -- | |||||
| 2. Self-forgiveness | 4.02 | .76 | .38 | -- | ||||
| 3. Sleep quantity | 6.65 | 1.36 | .12 | .12 | -- | |||
| 4. Sleep quality | 3.06 | .74 | .16 | .22 | .38 | -- | ||
| 5. Psychological distress | 2.23 | .80 | −.41 | −.40 | −.20 | −.39 | -- | |
| 6. Life satisfaction | 3.67 | .89 | .23 | .24 | .16 | .24 | −.37 | -- |
| 7. Physical health | 3.60 | 1.01 | .25 | .14 | .16 | .27 | −.37 | .31 |
Note. All correlation coefficients significant at p < .001
Both KMO (.72) and Bartlett’s test of sphericity (χ2 (10) = 899.82, p < .001) indicated that the data were suitable for factor analysis. Using confirmatory factor analysis, a measurement model was specified with two factors. Sleep quantity and sleep quality loaded on a latent sleep variable and psychological distress, life satisfaction, and physical health loaded on a latent health variable. No observed variable covariances were allowed, but a latent sleep-health covariance was allowed. Standardised loadings of the observed variables sleep quantity and sleep quality on the latent sleep variable were .45 and .86, respectively, and standardised loadings of the observed variables on the latent health variable were −.76, .50, and .50 for psychological distress, life satisfaction, and physical health, respectively, and all loadings on both latent variables were significant at p < .001. The fit of this model was χ2 = 7.28, p = .12, CFI = 1.00, RMSEA = .03, 95% C.I. = .00 - .05. The two-factor model showed significantly improved fit compared to a one-factor model Δχ2 = 84.26, p < .001, where all observed variables were specified to load on one latent variable. As a result, sleep and health were shown to be associated (r = .62, p < .001) but independent constructs in this study and they were treated as such in subsequent structural models.
To examine the main hypotheses in this study, a latent structural model was specified to test the extent to which forgiveness of others and self-forgiveness was associated with sleep and health and to examine the extent to which sleep mediated the associations of forgiveness of others and self-forgiveness with health. Figure 2 shows the structural model. Direct and indirect (through sleep) associations of forgiveness of others and self-forgiveness with health were specified. As hypothesised, analyses revealed that both forgiveness of others (β = .20, p < .001) and self-forgiveness (β = .11, p < .001) had direct associations with sleep, and forgiveness of others (β = .24, p < .001) and self-forgiveness (β = .27, p < .001) had direct associations with health. The association between forgiveness of others and sleep was stronger than the association between self-forgiveness and sleep (Δχ2 = 7.77, p < .01), and the associations between forgiveness of others and self-forgiveness with health were not different in magnitude (Δχ2 = .24, p = .62). Also as hypothesised, sleep had a direct association with health (β = .45, p < .001). The indirect associations of forgiveness of others (β = .09, p < .01) and self-forgiveness (β = .05, p < .01) with health through sleep were both statistically significant, confirming the mediation hypothesis. The partial mediation model fit the data acceptably χ2 = 164.80, p < .001, CFI = .95, RMSEA = .06, 95% C.I. = .05 - .07, and testing full mediation by removing the direct effect of either forgiveness of others, Δχ2 = 53.69, p < .001, or self-forgiveness, Δχ2 = 72.59, p < .001, resulted in significantly worse model fit. All models controlled the effects of age, race, education, income, marital status, and gender.
Figure 2.
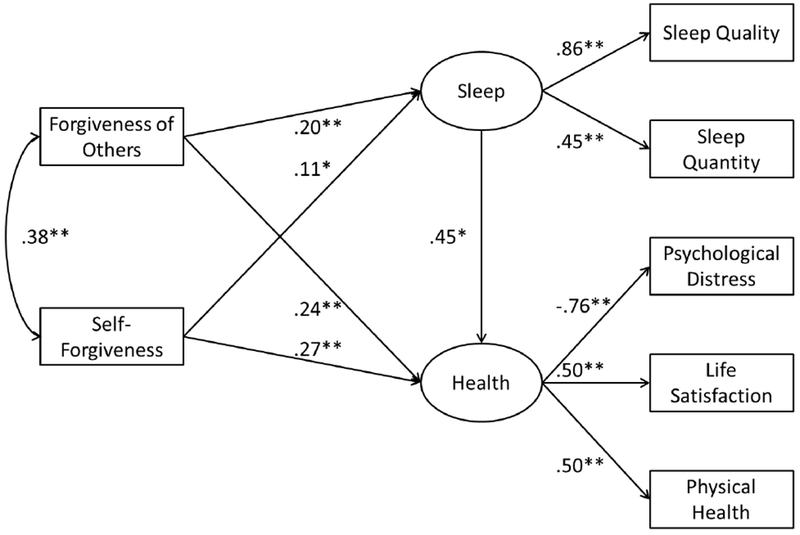
Structural latent variable model for the associations of forgiveness of others and self-forgiveness with health through the mediating mechanism of sleep. All standardised coefficients are adjusted for effects of sex, age, education, household income, race, and marital status. χ2 = 164.80, p < .001, CFI = .95, RMSEA = .06, 95% C.I. = .05 - .07. * p < .01, ** p < .001
Discussion
As hypothesised, forgiveness of others and self-forgiveness were related to both improved sleep and health. This confirms previous research on forgiveness of others and sleep (Lawler-Row, 2010; Lawler et al., 2005; Shirazi et al., 2016; Stoia-Caraballo et al., 2008), and on forgiveness of others and self-forgiveness and health (Toussaint et al., 2015). Also as expected, sleep was positively related to health confirming much previous research (Luyster et al., 2012), and sleep acted as a mediating mechanism between associations of forgiveness of others with health and self-forgiveness with health. To our knowledge, this represents the first study to document associations between forgiveness of others, self-forgiveness, sleep, and health in a nationally representative sample of United States adults.
Sleep served as a mediator or explanatory mechanism of the forgiveness and health association. Considerable research has been amassed over the last couple of decades suggesting that forgiveness is an important trait and state related to better health and well-being (Toussaint et al., 2015) and yet a full understanding of why eludes researchers. Though psychosocial variables (e.g., self-esteem, rumination, stress, appraisals) are certain to play a role, health behaviours and health-related functions such as sleep have gone relatively unexamined. As such, the present study provides a step forward in understanding why forgiveness promotes health. Because forgiveness is associated with better sleep, it capitalises on the powerful role that sleep plays in good health. If forgiveness of others and self-forgiveness can help people cope with the day’s psychological and emotional burdens in a way that frees one’s mind and promotes a more restful mental state for sleep, then they support the health-related process of sleep in meaningful ways. Forgiveness of others and self-forgiveness serve powerful roles as coping mechanisms (Toussaint et al., 2017; Worthington & Scherer, 2004) that may help individuals leave the past day’s regrets and offenses in the past and offer an important buffer between the events of the waking day and the onset and maintenance of sound sleep.
It is interesting to note the difference in the size of the associations of forgiveness of others and self-forgiveness with sleep and health. Although recent meta-analyses would suggest that self-forgiveness is more strongly related to health than forgiveness of others, (Davis et al., 2015), forgiveness of others and self-forgiveness showed similar associations with health in the present study. On the other hand, forgiveness of others was more strongly related to sleep than self-forgiveness. The reasons for this are not clear, especially because one would expect that personality characteristics that are equally tied to health would similarly connect to health-related behaviours. Nonetheless, consider the harmful connections between rumination, negative affect, and sleep (Thomsen, Mehlsen, Christensen, & Zachariae, 2003). It may be that offenses committed by others activate ruminative tendencies and negative affect to a greater degree than offenses committed by oneself and it is the underlying effect of stimulating rumination and negative affect that intrudes on sleep. This indirect connection between forgiveness of others, through rumination, and sleep has been demonstrated (Stoia-Caraballo et al., 2008), but no comparative analyses have borne out if this is true for self-forgiveness and sleep associations and, if so, if these indirect effects are similar in magnitude.
Limitations & Future Directions
A couple of limitations are important to note. First, this is a cross-sectional study wherein causality cannot be determined. Future studies that could evaluate the fit of alternative causal models would be welcome. For instance, perhaps forgiveness promotes better health and improved health is what allows for better sleep. As forgiveness was measured as a trait, it would be unlikely that either sleep or health would influence it, but that is not to exclude the possibility the sleep and health could influence states of forgiveness. Longitudinal designs will be needed to resolve these questions. Second, this was an epidemiological study and although that afforded a large, representative sample, it did not offer space for extensive measurement of any one given construct. Consequently, the measures used in the present study are global assessments and more comprehensive and in-depth measurement would be welcome. Reliability estimates for forgiveness of others and self-forgiveness were .72 and .67, respectively. Although these values are acceptable (Clark & Watson, 1995; Hair, Black, Babin, Anderson, & Tatham, 2006), especially for scales that have only a few items, it should be noted that measurement error attenuates the magnitude of associations between variables and is a limitation of our study. Sleep measures in particular may have attenuated the true associations identified in the present analyses as measurement error in the mediator can have important effects (Hoyle & Kenny, 1999).
Our data also limited the conclusions we could draw in other ways. We could not test potential additional relationships and mechanisms of demonstrated relationships. In particular, we speculated that other psychosocial factors and processes such as stress and rumination may be involved in the association of forgiveness and sleep, however, we were unable to test these associations. In addition, although the present study is the only known population-based study of forgiveness, sleep, and health, it is exclusively the United States population under study. Different populations and cultures have considerably different understandings of both forgiveness and sleep. For instance, researchers have coined the term “collectivistic forgiveness” to represent the type of forgiveness that is more fitting to people in Eastern, more collectivistic cultures (Hook, Worthington, Utsey, Davis, & Burnette, 2012). Likewise, cultures vary substantially in their understanding, expectations, and behaviours regarding sleep (National Sleep Foundation, 2013). It would be useful to examine how cultural differences might affect the forgiveness, sleep, and health equation.
Conclusions
A key part of maintaining good health is sufficient good quality sleep and it is important to identify factors that promote it. The present study offers the first known examination of how forgiveness may be related to good sleep and health. The present findings show that forgiveness of others and self-forgiveness are both related to better sleep and sleep is, in turn, related to better health. Because forgiveness of others and self-forgiveness offer an effective means of coping with one’s own or others’ offenses they may lift the burden of anger, regret, and rumination that all too commonly interfere with a good night’s sleep. In doing so, forgiveness of others and self-forgiveness tap the powerful, life-sustaining, health maintaining, and vitality enhancing benefits of a good night’s sleep.
Acknowledgments
This study was supported in part by the Fetzer Institute as part of the John Templeton Foundation’s campaign for forgiveness research, and by grant T32-MH16806 from the National Institute of Mental Health, and by a Faculty Research Grant from the Office of the Vice President for Research at the University of Michigan.
References
- Åkerstedt T (2006). Psychosocial stress and impaired sleep. [journal article]. Scandinavian Journal of Work, Environment and Health(6), 493–501. doi: 10.5271/sjweh.1054 [DOI] [PubMed] [Google Scholar]
- Ballesio A, Ottaviani C, & Lombardo C (2018). Poor cognitive inhibition predicts rumination about insomnia in a clinical sample. Behavioral Sleep Medicine, 1–10. doi: 10.1080/15402002.2018.1461103 [DOI] [PubMed] [Google Scholar]
- Beccuti G, & Pannain S (2011). Sleep and obesity. Curr Opin Clin Nutr Metab Care, 14(4), 402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berry JW, Worthington EL, O’Connor LE, Parrott L III, & Wade NG (2005). Forgivingness, vengeful rumination, and affective traits. Journal of Personality, 73(1), 183–225. doi: 10.1111/j.1467-6494.2004.00308.x [DOI] [PubMed] [Google Scholar]
- Besedovsky L, Lange T, & Born J (2012). Sleep and immune function. Pflugers Archiv. European Journal of Physiology, 463(1), 121–137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowling A (2005). Just one question: If one question works, why ask several? Journal of Epidemiology and Community Health, 59(5), 342–345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF, Monk TH, Berman SR, & Kupfer DJ (1989). The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213. doi: 10.1016/0165-1781(89)90047-4 [DOI] [PubMed] [Google Scholar]
- Cappuccio FP, Cooper D, D’Elia L, Strazzullo P, & Miller MA (2011). Sleep duration predicts cardiovascular outcomes: A systematic review and meta-analysis of prospective studies. European Heart Journal, 32(12), 1484–1492. [DOI] [PubMed] [Google Scholar]
- Cappuccio FP, D’Elia L, Strazzullo P, & Miller MA (2010). Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep, 33(5), 585–592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter JS, & Andrykowski MA (1998). Psychometric evaluation of the Pittsburgh Sleep Quality Index. Journal of Psychosomatic Research, 45(1), 5–13. doi: 10.1016/S0022-3999(97)00298-5 [DOI] [PubMed] [Google Scholar]
- Chaput J-P, & Tremblay A (2012). Adequate sleep to improve the treatment of obesity. Canadian Medical Association Journal, 184(18), 1975–1976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheadle ACD, & Toussaint LL (2015). Forgiveness and physical health in healthy populations In Toussaint LL, Worthington EL Jr. & Williams DR (Eds.), Forgiveness and health: Scientific evidence and theories relating forgiveness to better health (pp. 91–106). New York: Springer. [Google Scholar]
- Cheung F, & Lucas RE (2014). Assessing the validity of single-item life satisfaction measures: Results from three large samples. Quality of Life Research, 23(10), 2809–2818. doi: 10.1007/s11136-014-0726-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark LA, & Watson D (1995). Constructing validity: Basic issues in objective scale development. Psychological Assessment, 7(3), 309–319. doi: 10.1037/1040-3590.7.3.309 [DOI] [Google Scholar]
- Cohen J (1992). A power primer. Psychological Bulletin, 112(1), 155–159. [DOI] [PubMed] [Google Scholar]
- Davis DE, Ho MY, Griffin BJ, Bell C, Hook JN, Van Tongeren DR, … Westbrook CJ (2015). Forgiving the self and physical and mental health correlates: A meta-analytic review. Journal of Counseling Psychology, 62(2), 329–335. doi: 10.1037/cou0000063 [DOI] [PubMed] [Google Scholar]
- Friedberg JP, Suchday S, & Shelov DV (2007). The impact of forgiveness on cardiovascular reactivity and recovery. International Journal of Psychophysiology, 65(2), 87–94. doi: 10.1016/j.ijpsycho.2007.03.006 [DOI] [PubMed] [Google Scholar]
- Gangwisch JE, Babiss LA, Malaspina D, Turner BJ, Zammit GK, & Posner K (2010). Earlier parental set bedtimes as a protective factor against depression and suicidal ideation. Sleep, 33(1), 97–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorsuch RL, & Hao JY (1993). Forgiveness: An exploratory factor analysis and its relationships to religious variables. Review of Religious Research, 34, 333–347. [Google Scholar]
- Gruber R, & Cassoff J (2014). The interplay between sleep and emotion regulation: Conceptual framework empirical evidence and future directions. Current Psychiatry Reports, 16(11), 500. doi: 10.1007/s11920-014-0500-x [DOI] [PubMed] [Google Scholar]
- Gunn HE, Troxel WM, Hall MH, & Buysse DJ (2014). Interpersonal distress is associated with sleep and arousal in insomnia and good sleepers. Journal of Psychosomatic Research, 76(3), 242–248. doi: 10.1016/j.jpsychores.2013.11.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hair J, Black W, Babin B, Anderson R, & Tatham R (2006). Multivariate data analysis (6 ed.). Uppersaddle River, N.J.: Prentice Hall. [Google Scholar]
- Hisler G, & Krizan Z (2017). Anger tendencies and sleep: Poor anger control is associated with objectively measured sleep disruption. Journal of Research in Personality, 71, 17–26. doi: 10.1016/j.jrp.2017.08.009 [DOI] [Google Scholar]
- Hook JN, Worthington EL, Utsey SO, Davis DE, & Burnette JL (2012). Collectivistic self-construal and forgiveness. Counseling and Values, 57(1), 109–124. doi: 10.1002/j.2161-007X.2012.00012.x [DOI] [Google Scholar]
- Hoyle R, & Kenny D (1999). Sample size, reliability, and tests of statistical mediation In Hoyle R (Ed.), Statistical strategies for small sample research (pp. 195–222). Thousand Oaks, CA: Sage. [Google Scholar]
- Hublin C, Partinen M, Koskenvuo M, & Kaprio J (2007). Sleep and mortality: A population-based 22-year follow-up study. Sleep, 30(10), 1245–1253. doi: 10.1093/sleep/30.10.1245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Idler EL, Musick MA, Ellison CG, George LK, Krause N, Ory MG, … Williams DR (2003). Measuring multiple dimensions of religion and spirituality for health research: Conceptual background and findings from the 1998 general social survey. Research on Aging, 25(4), 327–365. [Google Scholar]
- Ikehara S, Iso H, Date C, Kikuchi S, Watanabe Y, Wada Y, … the JACC Study Group. (2009). Association of sleep duration with mortality from cardiovascular disease and other causes for japanese men and women: The JACC study. Sleep, 32(3), 295–301. doi: 10.1093/sleep/32.3.295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kakizaki M, Inoue K, Kuriyama S, Sone T, Matsuda-Ohmori K, Nakaya N, … Tsuji I (2008). Sleep duration and the risk of prostate cancer: The Ohsaki cohort study. British Journal of Cancer, 99, 176. doi: 10.1038/sj.bjc.6604425 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaleta K, & Mróz J (2018). Forgiveness and life satisfaction across different age groups in adults. Personality and Individual Differences, 120, 17–23. doi: 10.1016/j.paid.2017.08.008 [DOI] [Google Scholar]
- Kessler RC, Green JG, Gruber MJ, Sampson NA, Bromet E, Cuitan M, … Hu CY (2010). Screening for serious mental illness in the general population with the k6 screening scale: Results from the who world mental health (wmh) survey initiative. International Journal of Methods in Psychiatric Research, 19(S1), 4–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB (2015). Principles and practice of structural equation modeling. New York: Guilford Press. [Google Scholar]
- Krause N, & Hayward RD (2013). Self-forgiveness and mortality in late life. Social Indicators Research, 111(1), 361–373. doi: 10.1007/s11205-012-0010-3 [DOI] [Google Scholar]
- Lawler-Row KA (2010). Forgiveness as a mediator of the religiosity—health relationship. Psychology of Religion and Spirituality, 2(1), 1–16. [Google Scholar]
- Lawler KA, Younger JW, Piferi RL, Billington E, Jobe R, Edmondson K, & Jones WH (2003). A change of heart: Cardiovascular correlates of forgiveness in response to interpersonal conflict. Journal of Behavioral Medicine, 26(5), 373–393. doi: 10.1023/A:1025771716686 [DOI] [PubMed] [Google Scholar]
- Lawler KA, Younger JW, Piferi RL, Jobe RL, Edmondson KA, & Jones WH (2005). The unique effects of forgiveness on health: An exploration of pathways. Journal of Behavioral Medicine, 28(2), 157–167. doi: 10.1007/s10865-005-3665-2 [DOI] [PubMed] [Google Scholar]
- Li L, Wu C, Gan Y, Qu X, & Lu Z (2016). Insomnia and the risk of depression: A meta-analysis of prospective cohort studies. BMC Psychiatry, 16, 375. doi: 10.1186/s12888-016-1075-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Low CA, Bower JE, Moskowitz JT, Epel ES, Sheldon KM, Kashdan TB, & Steger MF (2011). Positive psychological states and biological processes In Sheldon KM, Kashdan TB & Steger MF (Eds.), Designing positive psychology: Taking stock and moving forward (pp. 41–50). New York: Oxford University Press. [Google Scholar]
- Luyster FS, Strollo JPJ, Zee PC, & Walsh JK (2012). Sleep: A health imperative. Sleep, 35(6), 727–734. doi: 10.5665/sleep.1846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mauger PA, Perry JE, Freeman T, Grove DC, McBride AG, & McKinney K (1992). The measurement of forgiveness: Preliminary research. Journal of Psychology and Christianity, 11(2), 170–180. [Google Scholar]
- McElroy JA, Newcomb PA, Titus-Ernstoff L, Trentham-Dietz AMY, Hampton JM, & Egan KM (2006). Duration of sleep and breast cancer risk in a large population-based case–control study. Journal of Sleep Research, 15(3), 241–249. doi: doi: 10.1111/j.1365-2869.2006.00523.x [DOI] [PubMed] [Google Scholar]
- Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, & Colantonio A (2016). The Pittsburgh Sleep Quality Index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Medicine Reviews, 25, 52–73. [DOI] [PubMed] [Google Scholar]
- Musick MA (2004). Multiple forms of forgiveness and their relationships with aging and religion In Schaie KW & Krause N (Eds.), Religious influences on health and well-being (pp. 204–214). New York: Springer Publishing Company. [Google Scholar]
- Musick MA, & Williams DR (1999). Forgiveness and well-being: Findings from a national sample Paper presented at the Annual meetings of the Gerontological Society of America, San Francisco, CA. [Google Scholar]
- National Sleep Foundation. (2013). International bedroom poll. Arlington, VA. [Google Scholar]
- Patel SR, Ayas NT, Malhotra MR, White DP, Schernhammer ES, Speizer FE, … Hu FB (2004). A prospective study of sleep duration and mortality risk in women. Sleep, 27(3), 440–444. doi: 10.1093/sleep/27.3.440 [DOI] [PubMed] [Google Scholar]
- Perry GS, Patil SP, & Presley-Cantrell LR (2013). Raising awareness of sleep as a healthy behavior. Preventing Chronic Disease, 10, 1–4. doi: 10.5888/pcd10.130081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pigeon WR, Pinquart M, & Conner K (2012). Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. The Journal of Clinical Psychiatry, 73(9), e1160–1167. doi: 10.4088/jcp.11r07586 [DOI] [PubMed] [Google Scholar]
- Pressman SD, & Cohen S (2005). Does positive affect influence health? Psychological Bulletin, 131(6), 925–971. [DOI] [PubMed] [Google Scholar]
- Seawell A, Toussaint LL, & Cheadle ACD (2014). Prospective associations between unforgiveness and physical health and positive mediating mechanisms in a nationally representative sample of older adults. Psychology & Health, 29(4), 375–389. doi: 10.1080/08870446.2013.856434 [DOI] [PubMed] [Google Scholar]
- Shirazi M, Fardin MA, Arab A, Sanagoue G, & Alisofi AN (2016). The impact of positive psychological states in predicting sleep quality amongst pregnant women. Iranian Journal of Psychiatry and Behavioral Sciences, 10(4), 1–5. [Google Scholar]
- Stickgold R (2005). Sleep-dependent memory consolidation. Nature, 437(7063), 1272–1278. [DOI] [PubMed] [Google Scholar]
- Stoia-Caraballo R, Rye MS, Pan W, Kirschman KJB, Lutz-Zois C, & Lyons AM (2008). Negative affect and anger rumination as mediators between forgiveness and sleep quality. Journal of Behavioral Medicine, 31(6), 478–488. [DOI] [PubMed] [Google Scholar]
- Tabachnick B, & Fidell L (2013). Using multivariate statistics. Boston: Pearson. [Google Scholar]
- Taylor C, Harrison J, Haimovitz K, Oberle E, Thomson K, Schonert-Reichl K, & Roeser RW (2016). Examining ways that a mindfulness-based intervention reduces stress in public school teachers: A mixed-methods study. Mindfulness, 7(1), 115–129. doi: 10.1007/s12671-015-0425-4 [DOI] [Google Scholar]
- Thomsen DK, Mehlsen MY, Christensen S, & Zachariae R (2003). Rumination--relationship with negative mood and sleep quality. Personality and Individual Differences, 34(7), 1293–1301. doi: 10.1016/S0191-8869(02)00120-4 [DOI] [Google Scholar]
- Toussaint L, & Cheadle A (2009). Unforgiveness and the broken heart: Unforgiving tendencies, problems due to unforgiveness, and 12-month prevalence of cardiovascular health conditions In Evans MT & Walker ED (Eds.), Religion and psychology. New York: Nova Publishers. [Google Scholar]
- Toussaint L, Shields GS, Dorn G, & Slavich GM (2016). Effects of lifetime stress exposure on mental and physical health in young adulthood: How stress degrades and forgiveness protects health. Journal of Health Psychology, 21(6), 1004–1014. doi: 10.1177/1359105314544132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toussaint L, & Webb JR (2005). Theoretical and empirical connections between forgiveness and mental health and well-being In Worthington EL Jr. (Ed.), Handbook of forgiveness (pp. 349–362). New York, NY: Routledge. [Google Scholar]
- Toussaint L, Webb JR, & Hirsch JK (2017). Self-forgiveness and health: A stress-and-coping model In Woodyatt L, Worthington EL Jr. , Wenzel M & Griffin BJ (Eds.), Handbook of the psychology of self-forgiveness. New York, NY: Springer. [Google Scholar]
- Toussaint LL, Owen AD, & Cheadle A (2012). Forgive to live: Forgiveness, health, and longevity. Journal of Behavioral Medicine, 35(4), 375–386. doi: 10.1007/s10865-011-9362-4 [DOI] [PubMed] [Google Scholar]
- Toussaint LL, Worthington EL Jr., & Williams DR (2015). Forgiveness and health: Scientific evidence and theories relating forgiveness to better health. New York: Springer. [Google Scholar]
- Verkasalo PK, Lillberg K, Stevens RG, Hublin C, Partinen M, Koskenvuo M, & Kaprio J (2005). Sleep duration and breast cancer: A prospective cohort study. Cancer Research, 65(20), 9595–9600. doi: 10.1158/0008-5472.can-05-2138 [DOI] [PubMed] [Google Scholar]
- Waksberg J (1978). Sampling methods for random digit dialing. Journal of the American Statistical Association, 73(361), 40–46. doi: 10.1080/01621459.1978.10479995 [DOI] [PubMed] [Google Scholar]
- Waltman MA, Russell DC, Coyle CT, Enright RD, Holter AC, & M. Swoboda C (2009). The effects of a forgiveness intervention on patients with coronary artery disease. Psychology & Health, 24(1), 11–27. doi: 10.1080/08870440801975127 [DOI] [PubMed] [Google Scholar]
- Wang YY, Wang F, Zheng W, Zhang L, Ng CH, Ungvari GS, & Xiang YT (2018). Mindfulness-based interventions for insomnia: A meta-analysis of randomized controlled trials. Behavioral Sleep Medicine, 1–9. doi: 10.1080/15402002.2018.1518228 [DOI] [PubMed] [Google Scholar]
- Watson PJ, Hood RW, Morris RJ, & Hall JR (1985). Religiosity, sin and self-esteem. Journal of Psychology and Theology, 13, 116–128. [Google Scholar]
- Watson PJ, Morris RJ, & Hood RW Jr (1987). Antireligious humanistic values, guilt, and self esteem. Journal for the Scientific Study of Religion, 26, 535–546. [Google Scholar]
- Webb JR, Hirsch JK, Visser PL, & Brewer KG (2013). Forgiveness and health: Assessing the mediating effect of health behavior, social support, and interpersonal functioning. The Journal of Psychology, 147(5), 391–414. doi: 10.1080/00223980.2012.700964 [DOI] [PubMed] [Google Scholar]
- Webb JR, Toussaint L, Kalpakjian CZ, & Tate DG (2010). Forgiveness and health-related outcomes among people with spinal cord injury. Disability and Rehabilitation: An International, Multidisciplinary Journal, 32(5), 360–366. doi: 10.3109/09638280903166360 [DOI] [PubMed] [Google Scholar]
- Worthington EL Jr. (2013). Moving forward: Six steps to forgiving yourself and breaking free from the past. Colorado Springs, CO: WaterBrook. [Google Scholar]
- Worthington EL Jr, & Scherer M (2004). Forgiveness is an emotion-focused coping strategy that can reduce health risks and promote health resilience: Theory, review, and hypotheses. Psychology & Health, 19(3), 385–405. doi: 10.1080/0887044042000196674 [DOI] [Google Scholar]