

Abstract
Introduction:
High blood pressure or hypertension is one of the chronic diseases causing other serious diseases and syndromes. Active involvement of the patient in the management of the disease is crucial in improving self-care and clinical outcomes. Mobile technology is nowadays used widely to improve the self-care process in people with chronic diseases such as hypertension.
Aim:
The objective of this study was to provide an overview of the existing research evaluating the impact of mobile applications on the self-care of patients with hypertension.
Methods:
The Scopus and PubMed databases were investigated using a comprehensive search strategy from the beginning of 2010 to 2019. All controlled clinical trial studies as well as quasi-experimental studies used mobile as a device for improving the self-care and conducted on patients with hypertension were included in the study. The studies were reviewed by two independent individuals.
Results:
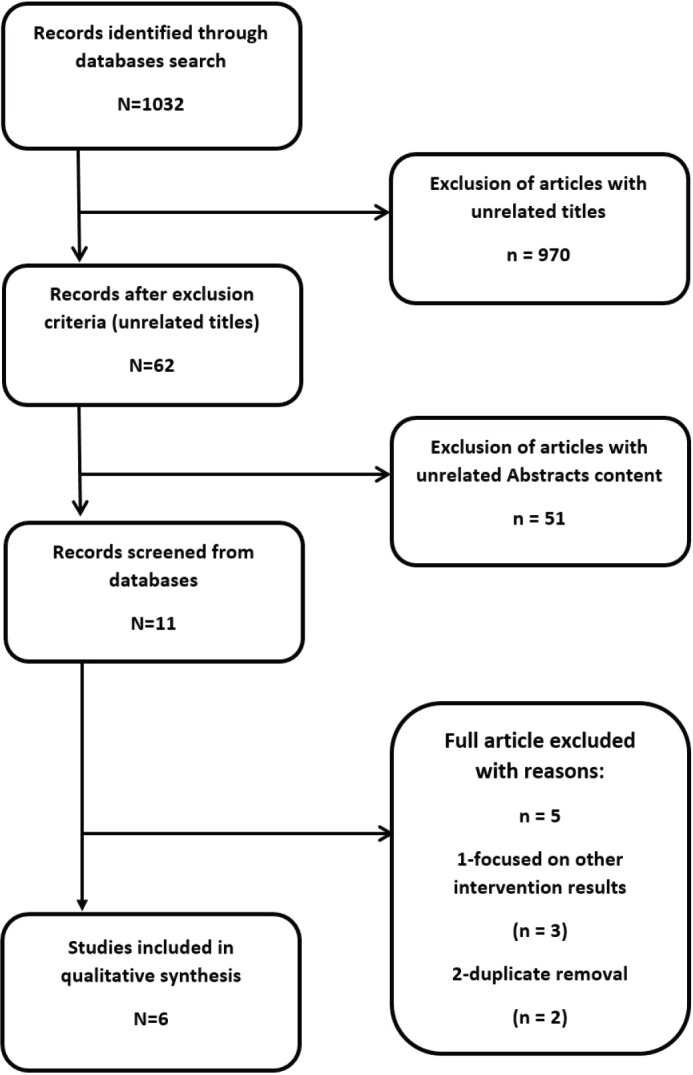
Out of 1032 studies found, 6 studies were finally reviewed after applying the inclusion criteria. Out of 6 studies reviewed, three studies confirmed the effect of using mobile applications on lowering blood pressure. Other studies reported a decline in blood pressure, while statistically significant were not shown.
Conclusion:
The results showed that mobile apps have positive potential on improving the self-care behavior of patients with hypertension, but the evidences presenting their impact are varied. Different reports for efficiency of mobile phone apps for the self-care modification was due to diverse condition of studies for mobile intervention on the patients with hypertension.
Keywords: Mobile apps, hypertension, remote health, self-care, patient behavior
1. INTRODUCTION
At the present time, obesity, hypertension and type II diabetes are considered as major problems and the prevalence of these diseases is rapidly increasing in developing countries. The four major chronic diseases (cardiovascular disease, cancer, chronic respiratory disease and diabetes) account for 82% of deaths. A total of 17.7 million people die due to cardiovascular disease, 8.8 million die due to cancer, 3.9 million die due to respiratory diseases and 1.6 million die due to diabetes each year. Thus, identifying the best method to reduce the burden of care provided for patients with these chronic diseases is critical (1). Hypertension can have a great impact on health. It causes chronic kidney disease and cardiovascular disease and can lead to problems such as heart attacks, stroke, kidney failure, blindness, rupture of blood vessels and cognitive disorders (2-4). Hypertension is defined systolic blood pressure of 130 mm Hg or higher and diastolic blood pressure of 80 mm Hg or higher (5). Hypertension is also one of the preventable risk factors for disability and early mortality in the world. It is usually silent until one of its consequences occurs in the person, but controlling it can prevent potentially serious consequences (3, 6, 7).
Reports suggest that 972 million adults or 26.4% of the population were affected by hypertension by 2000. Reports released by various countries show that its rate has been rising in low- and middle-income countries since 2000, while its rate has followed a steady or declining trend in high-income countries. This number is projected to reach 1.56 billion by 2025. It is predicted that the prevalence of hypertension to increase to 1.56 billion people by 2025. Its prevalence among Iranian population aged above 17 years has been reported to be over 20% (3, 4, 8). Improved living conditions and treatment methods have increased life expectancy in people with chronic diseases such as hypertension. However, without effective management, the quality of life in these people might be low. Hence, empowering and making these people involved in managing their treatment is vital (9, 10). Thus, effective management of blood pressure is largely dependent on the patient’s self-care; sine a person plays a major role in his or her daily decision-making and behavior in management of this disease. Self-care skills in chronic conditions include adherence to medication use, diet, self-care, self-care of key parameters such as blood pressure, and coping skills for better management of anger or stress in life and disease (11). In fact, patient involvement in the treatment process can improve outcomes, improve care, and cut the costs. Timely access to information, assessment, and appropriate treatment can challenge the treatment team and people with chronic diseases (9, 10). Various tools are used as strategies to improve the treatment of a number of chronic diseases, most of which have focused on educating the patient and encouraging them to be involved more in their health. Therefore, the patient himself or herself plays a major role in his or her treatment (11).
Empowering patients with information and communication technology (ICT) may be a good strategy to facilitate fair and high quality health cares for patients with chronic diseases. Telehealth Technologies provide efficient service to any point in the world. Telehealth is increasingly being used to bridge the gap between professional health care and patient self-care. These services in regions with limited resources can be used effectively to link primary care providers or specialists for counseling or education to the patient (1).
Nowadays, with the growth of technology, self-care devices are being used increasingly. One of the tools have been used widely in recent years is the use of mobile phones. Studies conducted in recent years have focused more on the use of mobile messaging capabilities, but more emphasis is nowadays is on the use of mobile application capabilities. Mobile phones have become an appropriate opportunity for self-care purposes due to their adaptability to different communities and their interactive nature. The use of smartphones is increasing due to the global trend of lower prices for these devices. Reports suggest that smartphones and tablets have become the most popular and widely used type of mobile phones. At the present time, out of 6 billion phone subscriptions in the world, only 17% are non-smartphones (9, 12).
The World Health Organization (WHO, 2011) defines mobile health (mHealth) as “medical and health practices supported by mobile devices such as mobile phones, patient monitoring devices, personal digital assistants (PDAs) and other wireless devices (8).
Studies in recent years have reported the positive impact of using mobile capabilities on self-care in patients with hypertension (5, 13). Some studies have also questioned the efficacy of using this technology in these patients (14). Considering the importance of the hypertension issue and the potential capabilities of the mobile device for self-care, the effect of using this device on blood pressure control was investigated. This study reviews systematically the studies published since 2010 on the use of mobile devices for the purpose of self-care in people with hypertension.
2. METHODS
Identification of studies
A systematic review study was conducted by searching the Scopus and PubMed databases using a combination of the concepts of “mobile”, “software”, “self-care” and “hypertension”. The searched terms that correspond to the concepts listed are shown in Table 1.
Table 1. The words searched based on search strategy concepts.
| Concept of searched words | |||
|---|---|---|---|
| Mobile | Software | Self-care | Hypertension |
| Hand held computer | App | Self-management | Blood pressure |
| mHealth | Application | Self-care | BP |
| Mobile | Game | Self-administration | Hypertension |
| PDA | Software | Self-monitoring | HTN |
| Personal Digital Assistant | Soft-ware | Patient participation | |
| Phone | Consumer participation | ||
| Smartphone | |||
| Tablet | |||
Using the term mesh, the search results were very high, so the conjunction words of “AND” and “OR” were used to improve the search strategy. Table 2 summarizes the search strategy of the databases.
Table 2. Details of search strategy in databases.
| Database | Timespan | Search fields | Reference Type | Language | Returns |
|---|---|---|---|---|---|
| PubMed | 2010–2019 | Title/Abstract | All Reference | English | 71 |
| Scopus | 2010–2019 | Title/Abstract | All Reference | English | 961 |
Inclusion and exclusion criteria
All of the studies found by searching in database were entered into Endnotes X7 software and each study was evaluated by two researchers based on inclusion and exclusion criteria. Inclusion criteria included: English-language articles published between 2010 and June 2019, studies conducted with controlled, randomized, and observation design as well as interventional studies, using mobile as a self-care device for patients with hypertension. Exclusion criteria included: Any intervention other than the mobile phone. Finally, related studies were tagged and included into the study for review of their full text. PRISMA Diagram in Figure 1 illustrates this procedure.
Figure 1. Flow diagram of literature search and selection process (adapted from Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA]).
The final studies were independently reviewed by two researchers using a data extraction form designed to review the studies of this research and included the following items: a) Author name; b) Year of publication; c) Population size in both intervention and control groups; d) The country where the study was conducted; e) Study title; f) Type of study; g) Type of intervention; h) Goal of the intervention; and I) Statistical information related to the study results.
3. RESULTS
Search in PubMed and Scopus databases between the years 2010 and June 2019 resulted in finding 5 studies eligible to be included into this study. The results are fully shown in Table 3. The mean duration of follow-up and evaluation of study participants was 5 months. The included studies generally examined the following items.
Table 3. Summary of interventions and outcome characteristics of included articles.
| Author | Study type | Follow-up period | Target population | Number of participants | Intervention type | Comparison strategy (intervention vs control) | Goal of intervention | Result |
|---|---|---|---|---|---|---|---|---|
| Morawski et al (15) -United States -2018 |
Randomized controlled clinical trial | 3 months | People with uncontrolled hypertension who take between 1 and 3 antihypertensive medications. | 411 patients (209 in the intervention group and 202 in the control group) aged 18 to 75 years | Using the Smartphone Medisafe application to improve medication use and blood pressure control | Lack of receiving any intervention | Assisting people in self-monitoring and adherence to prescribed treatments | Significant improvement in medication adherence was observed, but there was no significant difference between the intervention and the control group in systolic blood pressure. |
| Kim et al (11) -United States -2016 |
Randomized controlled clinical trial | 2 months | People with hypertension who take at least one or more antihypertensive medications. | 95 patients (52 in the intervention group and 43 in the control group) with a mean age of 57 years | Using a wireless monitoring system and HealthyCircles application for self-management of the disease | Receiving services through in-person referring to service center | Positive behavioral change, adherence to medication orders and improving blood pressure | There was a significant decrease in smoking in the intervention group compared to the control group. However, changes in systolic and diastolic blood pressure, adherence to medication orders, and alcohol consumption were not statistically significant. |
| Bengtsson et al (16) -Sweden -2015 |
Before and after clinical trial | 6 months | People over 30 who were under treatment for hypertension. | 51 patients (50 in intervention group and 51 in control group) | Using a mobile web application for self-care and patient encouragement | The routine treatment process | Improving blood pressure changes through self-care | There was a significant reduction in blood pressure levels after the intervention compared to before the intervention. |
| Chandler et al(14) -Spain -2019 |
Randomized clinical trial | 9 months | People with hypertension who are under medication treatment | 54 people (26 in intervention group and 28 in ESC group) | Using the SMASH system including mobile application adapted to Android and iOS and GSM system as well as a Bluetooth for monitoring blood pressure | Receiving educational sms that sometimes contain instructive video links. | Improve blood pressure and adherence to medication orders | Significant improvement in blood pressure was observed in the SMASH group compared to the ESC group, but the changes in adherence to medication orders were not significant. |
| Lee et al (1) -Vietnam -2018 |
Before and after clinical trial | 3 months | People with hypertension | 234 patients (36 in intervention group and 198 in control group) | Using a self-care mobile application and holding two distance sessions for educating patients | The routine treatment process | Improving the blood pressure | A significant decrease in blood pressure was observed in the intervention group compared to the control group. |
| Zha et al (5) -unites states -2019 |
Randomized controlled clinical trial | 6 months | Hypertension patients with low income | 25 people (12 in the intervention group and 13 in the control group) | Use blood pressure and heart rate measuring device (BP7 iHealth) connected to your mobile phone via Bluetooth. | Receiving standard cares | Improving blood pressure, adherence to blood pressure monitoring and medication orders | Reduction in blood pressure and improvement in adherence to continuous monitoring of blood pressure and adherence to medication orders were not significant. Among the life quality level factors, only the score of general health showed significant improvement |
Blood pressure
Out of 6 studies reviewed, three studies confirmed the effect of using mobile applications on lowering blood pressure. Another study reported a decline in the blood pressure, but it was not statistically significant.
Adherence to medication orders
Out of 6 studies reviewed, 4 studies examined the effect of using mobile applications on improving the adherence to medication orders, which 3 studies reported improvement as a result of adherence to medication orders (5, 11, 14). However, only one study reported this effect significant (16).
High-risk behaviors and improved quality of life
Out of the 5 studies reviewed, one study examined the effect of using mobile applications in reducing high-risk behaviors. In this study, it was reported that the use of mobile applications has a significant effect on reducing smoking (11). However, this effect on reducing alcohol consumption was not statistically significant. Another study examined the effect of mobile use on improving quality of life, which this effect was significant only on general mental health.
4. DISCUSSION
Given the risk of hypertension as one of the leading causes of death in the world, the use of new methods such as new technologies, is required to improve screening, diagnosis and control of hypertension in the community. The widespread availability of smartphones and mobile health applications has created a new perspective for the continuous monitoring of hypertension. The aim of this systematic review was to provide evidence of the effectiveness and usability of mobile and tablet applications for self-care and lowering blood pressure in patients. The results of this study are similar to the results of other studies evaluated the impact of mobile (17, 18, 19). Although some systematic review studies have shown the significant effects of using mobile technology in the management and control of diseases including hypertension (18, 19), this effect is not significant for all diseases and for all age groups (20).
Main results
The results of the reviewed studies showed that the effect of using mobile applications on self-care and hypotension in patients with hypertension was not significant. Although most studies have evaluated the use of mobile applications positive in lowering blood pressure levels, only three studies showed their significant effect on reducing the blood pressure (1, 14, 16). Studies also showed that the positive effect of using mobile applications on adherence to medication orders was not statistically significant, but different factors can influence the results of this study.
Economic status of communities
The inclusion criterion of most studies that could influence the results was the need to have a smartphone for research participants, which is not possible for all people in poor communities. Only one of the studies examined the intervention in these communities (5).
Method of measuring blood pressure
In the reviewed studies, the blood pressure was measured and reported by the participants themselves. Although in all studies, the treatment team taught the way of measuring and reporting the blood pressure for the participants, any errors in measuring and reporting their blood pressure can affect the outcome of these studies. It is recommended to use digital blood pressure monitors which is able to send information electronically to prevent any error from the entry of information.
Study length
Duration of patients following-up is an effective factor influenced the results of such studies, which was 5 months on average in the studies reviewed in this systematic review. As self-management and behavioral change are time-consuming, it seems that more studies with longer follow-up to be necessary. More time is also needed for studies to ensure the measured blood pressure and to ensure consistency of results.
Education-based self-care
Self-care in hypertension is directly associated with health literacy and patient education (21). Hence, providing education for patients in the areas of diet (low salt), exercise, lifestyle change, and so on needs to be prioritized.
Adherence to medication orders
One of the most important self-care feedbacks is the timely taking of hypertension medications. Majority of the conducted studies have also emphasized adherence to medication orders. Most applications used different functional combinations to improve adherence to medication orders. Therefore, it can be stated that adherence to medication order is the most important self-care outcome in hypertension patients. It is better that the device recording the changes of blood pressure to be equipped with alert and reminder systems to improve taking the medications, since timely and correctly taking of medications by patients directly associated with blood pressure regulation and disease management.
Usability
The measurement applications and devices used in studies and the ease of working with them can also influence the results (9). Out of the 6 studies reviewed, only two studies investigated the usability of applications and the selections of applications with the least usability. In similar studies that assessed users’ satisfaction, participants were generally satisfied with the use of applications for self-care (22). Due to old age of people with hypertension and the importance of ease of working with mobile devices and applications, usability issue can play an important role in the effectiveness of an application.
Limitations: This research suffered from several limitations. The main limitation of this study was the low number of studies conducted in this regard. Meta-analysis was also not possible due to the design of the studied studies. Non-English studies were also not included in this study. Differences in objectives, study design, and study results also made it difficult to compare the studies appropriately.
Author’s contribution:
Each author gave substantial contribution in acquisition, analysis and data interpretation. Each author had a part in preparing article for drafting and revising it critically for important intellectual content. Each author gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of interest:
There are no conflict of interest.
Financial support:
Nil.
REFERENCES
- 1.Lee HY, Kim JY, Na KY, Park HY, Han J, Pak Y, et al. The role of telehealth counselling with mobile self-monitoring on blood pressure reduction among overseas Koreans with high blood pressure in Vietnam. J Telemed Telecare. 2019;25(4):241–248. doi: 10.1177/1357633X18780559. [DOI] [PubMed] [Google Scholar]
- 2.Nerenberg KA, Zarnke KB, Leung AA, Dasgupta K, Butalia S, Mc- Brien K, et al. Hypertension Canada’s 2018 guidelines for diagnosis, risk assessment, prevention, and treatment of hypertension in adults and children. Canadian Journal of Cardiology. 2018;34(5):506–525. doi: 10.1016/j.cjca.2018.02.022. [DOI] [PubMed] [Google Scholar]
- 3.Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134(6):441–450. doi: 10.1161/CIRCULATIONAHA.115.018912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mirzaei M, Moayedallaie S, Jabbari L, Mohammadi M. Prevalence of hypertension in Iran 1980-2012: a systematic review. The Journal of Tehran University Heart Center. 2016;11(4):159. [PMC free article] [PubMed] [Google Scholar]
- 5.Zha P, Qureshi R, Porter S, Chao YY, Pacquiao D, Chase S, et al. Utilizing a Mobile Health Intervention to Manage Hypertension in an Underserved Community. Western Journal of Nursing Research. 2019 doi: 10.1177/0193945919847937. [DOI] [PubMed] [Google Scholar]
- 6.Wright JM, Musini VM, Gill R. First line drugs for hypertension. Cochrane Database of systematic reviews. 2018(4) doi: 10.1002/14651858.CD001841.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Daskalopoulou SS, Rabi DM, Zarnke KB, Dasgupta K, Nerenberg K, Cloutier L, et al. The 2015 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Canadian Journal of Cardiology. 2015;31(5):549–568. doi: 10.1016/j.cjca.2015.02.016. [DOI] [PubMed] [Google Scholar]
- 8.Tabrizi JS, Sadeghi-Bazargani H, Farahbakhsh M, Nikniaz L, Nikniaz Z. Prevalence and associated factors of prehypertension and hypertension in Iranian Population: The Lifestyle Promotion Project (LPP) PloS one. 2016;11(10):e0165264. doi: 10.1371/journal.pone.0165264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Whitehead L, Seaton P. The effectiveness of self-management mobile phone and tablet apps in long-term condition management: a systematic review. Journal of medical Internet research. 2016;18(5):e97. doi: 10.2196/jmir.4883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kaplan AL, Cohen ER, Zimlichman E. Improving patient engagement in self-measured blood pressure monitoring using a mobile health technology. Health information science and systems. 2017;5(1):4. doi: 10.1007/s13755-017-0026-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kim JY, Wineinger NE, Steinhubl SR. The Influence of Wireless Self-Monitoring Program on the Relationship Between Patient Activation and Health Behaviors, Medication Adherence, and Blood Pressure Levels in Hypertensive Patients: A Substudy of a Randomized Controlled Trial. J Med Internet Res. 2016;18(6):e116. doi: 10.2196/jmir.5429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cui M, Wu X, Mao J, Wang X, Nie M. T2DM self-management via smartphone applications: a systematic review and meta-analysis. PloS one. 2016;11(11):e0166718. doi: 10.1371/journal.pone.0166718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Logan AG, Irvine MJ, McIsaac WJ, Tisler A, Rossos PG, Easty A, et al. Effect of home blood pressure telemonitoring with self-care support on uncontrolled systolic hypertension in diabetics. Hypertension. 2012;60(1):51–57. doi: 10.1161/HYPERTENSIONAHA.111.188409. [DOI] [PubMed] [Google Scholar]
- 14.Chandler J, Sox L, Kellam K, Feder L, Nemeth L, Treiber F. Impact of a Culturally Tailored mHealth Medication Regimen Self-Management Program upon Blood Pressure among Hypertensive Hispanic Adults. Int J Environ Res Public Health. 2019;16(7) doi: 10.3390/ijerph16071226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Morawski K, Ghazinouri R, Krumme A, Lauffenburger JC, Lu Z, Durfee E, et al. Association of a smartphone application with medication adherence and blood pressure control: The MedISAFE- BP randomized clinical trial. JAMA Internal Medicine. 2018;178(6):802–809. doi: 10.1001/jamainternmed.2018.0447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bengtsson U, Kjellgren K, Hallberg I, Lindwall M, Taft C. Improved Blood Pressure Control Using an Interactive Mobile Phone Support System. Journal of Clinical Hypertension. 2016;18(2):101–108. doi: 10.1111/jch.12682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bonoto BC, de AVE, Godói IP, de LLLP, Godman B, Bennie M, et al. Efficacy of Mobile Apps to Support the Care of Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR Mhealth Uhealth. 2017;5(3):e4. p2. doi: 10.2196/mhealth.6309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.McLean G, Band R, Saunderson K, Hanlon P, Murray E, Little P, et al. Digital interventions to promote self-management in adults with hypertension systematic review and meta-analysis. J Hypertens. 2016 Apr;34(4):600–612. doi: 10.1097/HJH.0000000000000859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liu S, Dunford SD, Leung YW, Brooks D, Thomas SG, Eysenbach G, et al. Reducing blood pressure with Internet-based interventions: a meta-analysis. Can J Cardiol. 2013 May;29(5):613–621. doi: 10.1016/j.cjca.2013.02.007. [DOI] [PubMed] [Google Scholar]
- 20.Kitt J, Fox R, Tucker K.L, et al. New Approaches in Hypertension Management: a Review of Current and Developing Technologies and Their Potential Impact on Hypertension Care. Curr Hypertens Rep. 2019;21(6):44–53. doi: 10.1007/s11906-019-0949-4. Available on . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Daniali S, Eslami A, Maracy M, Shahabi J, Mostafavi-Darani F. The impact of educational intervention on self-care behaviors in overweight hypertensive women: A randomized control trial. ARYA Atherosclerosis. 2017;13(1):20–28. [PMC free article] [PubMed] [Google Scholar]
- 22.Alessa T, Abdi S, Hawley MS, de Witte L. Mobile Apps to Support the Self-Management of Hypertension: Systematic Review of Effectiveness, Usability, and User Satisfaction. JMIR Mhealth Uhealth. 2018;6(7):e10723. doi: 10.2196/10723. [DOI] [PMC free article] [PubMed] [Google Scholar]