

Abstract
Background
Many women would like to avoid pharmacological or invasive methods of pain management in labour and this may contribute towards the popularity of complementary methods of pain management. This review examined evidence about the use of acupuncture and acupressure for pain management in labour. This is an update of a review last published in 2011.
Objectives
To examine the effects of acupuncture and acupressure for pain management in labour.
Search methods
For this update, we searched Cochrane Pregnancy and Childbirth’s Trials Register, (25 February 2019), the Cochrane Central Register of Controlled Trials (the Cochrane Library 2019, Issue 1), MEDLINE (1966 to February 2019), CINAHL (1980 to February 2019), ClinicalTrials.gov (February 2019), the WHO International Clinical Trials Registry Platfory (ICTRP) (February 2019) and reference lists of included studies.
Selection criteria
Published and unpublished randomised controlled trials (RCTs) comparing acupuncture or acupressure with placebo, no treatment or other non‐pharmacological forms of pain management in labour. We included all women whether nulliparous or multiparous, and in spontaneous or induced labour.
We included studies reported in abstract form if there was sufficient information to permit assessment of risk of bias. Trials using a cluster‐RCT design were eligible for inclusion, but quasi‐RCTs or cross‐over studies were not.
Data collection and analysis
Two review authors independently assessed trials for inclusion and risk of bias, extracted data and checked them for accuracy. We assessed the certainty of the evidence using the GRADE approach.
Main results
We included 28 trials with data reporting on 3960 women. Thirteen trials reported on acupuncture and 15 trials reported on acupressure. No study was at a low risk of bias on all domains. Pain intensity was generally measured on a visual analogue scale (VAS) of 0 to 10 or 0 to 100 with low scores indicating less pain.
Acupuncture versus sham acupuncture
Acupuncture may make little or no difference to the intensity of pain felt by women when compared with sham acupuncture (mean difference (MD) ‐4.42, 95% confidence interval (CI) ‐12.94 to 4.09, 2 trials, 325 women, low‐certainty evidence). Acupuncture may increase satisfaction with pain relief compared to sham acupuncture (risk ratio (RR) 2.38, 95% CI 1.78 to 3.19, 1 trial, 150 women, moderate‐certainty evidence), and probably reduces the use of pharmacological analgesia (RR 0.75, 95% CI 0.63 to 0.89, 2 trials, 261 women, moderate‐certainty evidence). Acupuncture may have no effect on assisted vaginal birth (very low‐certainty evidence), and probably little to no effect on caesarean section (low‐certainty evidence).
Acupuncture compared to usual care
We are uncertain if acupuncture reduces pain intensity compared to usual care because the evidence was found to be very low certainty (standardised mean difference (SMD) ‐1.31, 95% CI ‐2.14 to ‐0.49, 4 trials, 495 women, I2 = 93%). Acupuncture may have little to no effect on satisfaction with pain relief (low‐certainty evidence). We are uncertain if acupuncture reduces the use of pharmacological analgesia because the evidence was found to be very low certainty (average RR 0.72, 95% CI 0.60 to 0.85, 6 trials, 1059 women, I2 = 70%). Acupuncture probably has little to no effect on assisted vaginal birth (low‐certainty evidence) or caesarean section (low‐certainty evidence).
Acupuncture compared to no treatment
One trial compared acupuncture to no treatment. We are uncertain if acupuncture reduces pain intensity (MD ‐1.16, 95% CI ‐1.51 to ‐0.81, 163 women, very low‐certainty evidence), assisted vaginal birth or caesarean section because the evidence was found to be very low certainty.
Acupuncture compared to sterile water injection
We are uncertain if acupuncture has any effect on use of pharmacological analgesia, assisted vaginal birth or caesarean section because the evidence was found to be very low certainty.
Acupressure compared to a sham control
We are uncertain if acupressure reduces pain intensity in labour (MD ‐1.93, 95% CI ‐3.31 to ‐0.55, 6 trials, 472 women) or assisted vaginal birth because the evidence was found to be very low certainty. Acupressure may have little to no effect on use of pharmacological analgesia (low‐certainty evidence). Acupressure probably reduces the caesarean section rate (RR 0.44, 95% CI 0.27 to 0.71, 4 trials, 313 women, moderate‐certainty evidence).
Acupressure compared to usual care
We are uncertain if acupressure reduces pain intensity in labour (SMD ‐1.07, 95% CI ‐1.45 to ‐0.69, 8 trials, 620 women) or increases satisfaction with pain relief (MD 1.05, 95% CI 0.75 to 1.35, 1 trial, 105 women) because the evidence was found to be very low certainty. Acupressure may have little to no effect on caesarean section (low‐certainty evidence).
Acupressure compared to a combined control
Acupressure probably slightly reduces the intensity of pain during labour compared with the combined control (measured on a scale of 0 to 10 with low scores indicating less pain) (SMD ‐0.42, 95% CI ‐0.65 to ‐0.18, 2 trials, 322 women, moderate‐certainty evidence). We are uncertain if acupressure has any effect on the use of pharmacological analgesia (RR 0.94, 95% CI 0.71 to 1.25, 1 trial, 212 women), satisfaction with childbirth, assisted vaginal birth or caesarean section because the certainty of the evidence was all very low.
No studies were found that reported on sense of control in labour and only one reported on satisfaction with the childbirth experience.
Authors' conclusions
Acupuncture in comparison to sham acupuncture may increase satisfaction with pain management and reduce use of pharmacological analgesia. Acupressure in comparison to a combined control and usual care may reduce pain intensity. However, for other comparisons of acupuncture and acupressure, we are uncertain about the effects on pain intensity and satisfaction with pain relief due to very low‐certainty evidence. Acupuncture may have little to no effect on the rates of caesarean or assisted vaginal birth. Acupressure probably reduces the need for caesarean section in comparison to a sham control. There is a need for further high‐quality research that include sham controls and comparisons to usual care and report on the outcomes of sense of control in labour, satisfaction with the childbirth experience or satisfaction with pain relief.
Keywords: Female; Humans; Pregnancy; Acupressure; Acupressure/methods; Acupuncture Therapy; Acupuncture Therapy/methods; Analgesia, Obstetrical; Analgesia, Obstetrical/methods; Labor Pain; Labor Pain/therapy; Pain Management; Pain Management/methods; Randomized Controlled Trials as Topic
Plain language summary
Acupuncture or acupressure for relieving pain during labour
We examined the evidence from randomised controlled trials on the use of acupuncture or acupressure in helping women to manage pain during labour. This is an update of a review last published in 2011.
What is the issue?
The pain women experience during labour can be intense, with body tension, anxiety and fear making it worse. Pain is caused by contractions of the uterus, the opening of the cervix and, in the late first and second stages, by stretching of the vagina and pelvic floor as the baby moves down the birth canal. Effective, satisfactory pain management needs to be individualised for each woman. Women may also use strategies to try to break the fear‐tension‐pain cycle and work with the pain. Working with the pain involves offering women support and encouragement, finding comfortable positions, immersion in water and self‐help techniques.
Many women would like to go through labour without using drugs. Women may turn to acupuncture or acupressure to help reduce their pain and improve management of the pain.
Why is this important?
Acupuncture has a long history of use in Asia, including China, Korea and Japan. Technical needling skills are needed to apply the needles at the correct points. Acupressure also has its origins in early China. To apply acupressure, the therapist uses their hands and fingers to activate the same points as in acupuncture. Sometimes only a few points are needed to alleviate pain or bring about a feeling of relaxation. Other times a combination of points may be required for greater effect. Some forms of acupressure are applied by trained health professionals, while others can be applied by the individual as a form of self‐massage.
What evidence did we find?
Our updated search in February 2019 identified 17 new trials.
This review now includes 28 trials reporting on 3960 women, with 27 trials contributing results. The trials compared acupuncture or acupressure with sham treatment as placebo, no treatment or usual care for pain management during labour. Thirteen trials reported on acupuncture and 15 trials reported on acupressure. For 18 of the 27 trials women were in spontaneous labour. In other studies labour may have been induced.
Eight studies applied individualised traditional Chinese medicine while set acupuncture points were used in the majority of studies. We noted wide variation in how stimulation was applied (manually or with electro‐stimulation), duration of needling, number of points used, and depth of needling. It is unclear how representative the trial treatments were of acupuncture in practice.
Most comparisons suggest a small beneficial effect from acupuncture, though the supporting evidence was limited. We are uncertain if acupuncture reduces the intensity of pain when compared with sham acupuncture (2 trials, 325 women), usual care (4 trials, 495 women) and no treatment (1 trial, 163 women). The certainty of the evidence was low or very low. Acupuncture may increase satisfaction with pain relief compared to sham acupuncture (one trial, moderate‐certainty evidence). It slightly reduced the use of pharmacological analgesia compared to sham acupuncture (2 trials, 261 women, moderate‐certainty evidence). Use of acupressure was associated with a reduction in pain intensity in labour when compared to a combined control (2 trials, 322 women, moderate‐certainty evidence). Acupuncture did not appear to have any effect on the need for assisted vaginal births or caesarean births, but acupressure reduced the rate of caesarean section when compared to sham acupressure.
What does this mean?
Acupuncture may increase satisfaction with pain relief and reduce use of pharmacological pain relief. Acupressure may help relieve pain during labour, although the pain reduction may not be large. However, for other comparisons of acupuncture and acupressure, we are uncertain about the effects on pain intensity and satisfaction with pain relief due to very low‐certainty evidence. Acupuncture or acupressure may have little to no effect on assisted vaginal birth, but women having acupressure maybe less likely to need a caesarean section. Studies were conducted in different countries, which may reflect the different styles of applying acupuncture. A weakness of a number of trials continues to be that very few outcomes were measured and no safety outcomes were reported. More high‐quality research is needed.
Summary of findings
Summary of findings for the main comparison. Acupuncture compared to sham control for pain management in labour.
| Acupuncture compared to sham control for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupuncture Comparison: sham control | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with sham control | Risk with acupuncture | |||||
| Pain intensity
assessed with VAS scales 1‐100. Lower scores indicate less pain intensity |
The mean pain intensity ranged across control groups from 52.94 to 91.4 | The mean pain intensity score in the intervention group was 4.42 lower (12.94 lower to 4.09 higher) | 325 (2 RCTs) | ⊕⊕⊝⊝ LOW 1 2 | ||
| Satisfaction with pain relief in labour assessed with: number of women stating they were satisfied with their pain relief. | Study population | RR 2.38 (1.78 to 3.19) | 150 (1 RCT) | ⊕⊕⊕⊝ MODERATE3 | ||
| 387 per 1000 | 920 per 1000 (688 to 1000) | |||||
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth experience ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Use of pharmacological analgesia | Study population | RR 0.75 (0.63 to 0.89) | 261 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 767 per 1000 | 576 per 1000 (483 to 683) | |||||
| Assisted vaginal birth | Study population | RR 1.10 (0.41 to 2.97) | 261 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 4 5 6 | ||
| 163 per 1000 | 179 per 1000 (67 to 483) | |||||
| Caesarean section | Study population | RR 1.11 (0.49 to 2.48) | 411 (3 RCTs) | ⊕⊕⊝⊝ LOW7, 8 | ||
| 49 per 1000 | 54 per 1000 (24 to 122) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded one level due to serious risk of bias: one study high or unclear risk of bias on six domains.
2 Downgraded one level due to serious inconsistency: substantial heterogeneity present I2 = 87%
3 Downgraded one level due to serious imprecision: small sample size (150)
4 Downgraded one level due to serious risk of bias: one study did not blind participants to group allocation. Should not affect sham arm outcome but blinding integrity not reported.
5 Downgraded one level due to serious inconsistency: substantial heterogeneity present I2 = 72%
6 Downgraded one level for imprecision due to small sample size and wide confidence intervals crossing the line of no effect
7 Downgraded one level for imprecision due to small number of events and wide confidence intervals crossing the line of no effect
8 Downgraded one level due to serious risk of bias: one study did not blind participants to group allocation and two studies at high risk of other bias
Summary of findings 2. Acupuncture compared to usual care for pain management in labour.
| Acupuncture compared to usual care for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupuncture Comparison: care | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with usual care | Risk with acupuncture | |||||
| Pain intensity
assessed with VAS or NRS: lower scores indicate less pain
Scale from: 0 to 10 Mix of NRS and VAS scales so analysed using SMD |
The mean pain intensity score in the intervention group was 1.31 standard deviations lower (2.14 lower to 0.49 lower) | 495 (4 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | |||
| Satisfaction with pain relief in labour assessed with: number of women who reported satisfaction with pain relief | Study population | RR 1.07 (0.96 to 1.20) | 343 (2 RCTs) | ⊕⊕⊝⊝ LOW 3 | ||
| 787 per 1000 | 843 per 1000 (756 to 945) | |||||
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth experience ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Use of pharmacological analgesia | Study population | RR 0.72 (0.60 to 0.85) | 1059 (6 RCTs) | ⊕⊝⊝⊝ VERY LOW 4 5 | ||
| 833 per 1000 | 600 per 1000 (500 to 708) | |||||
| Assisted vaginal birth | Study population | RR 0.93 (0.70 to 1.24) | 1217 (6 RCTs) | ⊕⊕⊝⊝ LOW 6 8 | ||
| 127 per 1000 | 118 per 1000 (89 to 158) | |||||
| Caesarean section | Study population | RR 0.72 (0.47 to 1.09) | 861 (5 RCTs) | ⊕⊕⊝⊝ LOW 7 8 | ||
| 116 per 1000 | 83 per 1000 (54 to 126) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; NRS: numeric rating scale; SMD: SMD: standardised mean difference; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded two levels for very serious risk of bias: two of the three studies had high risk of performance bias and this was likely to influence a self‐reported outcome.
2 Downgraded two levels for very serious inconsistency: considerable heterogeneity present (I2 = 93%) not explained by subgroup analysis.
3 Downgraded two levels for very serious risk of bias: both studies had unclear or high risk of bias related to blinding and this was likely to influence a self‐reported outcome
4 Downgraded two levels for very serious risk of bias: all studies had unclear or high risk of performance bias and this was likely to influence the need for additional analgesia.
5 Downgraded one level for serious inconsistency: substantial heterogeneity (I2 = 70%) which is not explained by subgroups.
6 Downgraded one level for serious risk of bias: five of six studies at unclear or high risk of bias in both performance and detection bias. This may have influenced the outcome.
7 Downgraded one level for serious risk of bias: three of four studies at high or unclear risk of bias in both performance and detection bias. This may have influenced the outcome.
8 Downgraded one level for imprecision due to wide confidence intervals.
Summary of findings 3. Acupuncture compared to no treatment for pain management in labour.
| Acupuncture compared to no treatment for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupuncture Comparison: no treatment | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with no treatment | Risk with acupuncture | |||||
| Pain intensity Lower scores indicate less pain. |
The mean pain intensity in the control group was 7.92 | The mean pain intensity score in the intervention groups was 1.16 lower (1.51 lower to 0.81 lower) | ‐ | 163 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 2 | |
| Satisfaction with pain relief ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth experience ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Use of pharmacological pain relief ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Assisted vaginal birth | Study population | RR 0.49 (0.18 to 1.38) | 163 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 3 | ||
| 123 per 1000 | 60 per 1000 (22 to 170) | |||||
| Caesarean section | Study population | RR 0.76 (0.35 to 1.63) | 163 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 3 | ||
| 160 per 1000 | 122 per 1000 (56 to 262) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded by two levels for very serious risk of bias: high risk of bias in one domain (blinding for a subjective outcome) and unclear risk of bias in four domains.
2 Downgraded one level for serious imprecision due to a single study providing data with a small sample size (163)
3 Downgraded two levels for very serious imprecision due to a single study, with few events, small sample size and wide confidence intervals providing data
Summary of findings 4. Acupuncture compared to water injection for pain management in labour.
| Acupuncture compared to water injection for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupuncture Comparison: water injection | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with water injection | Risk with acupuncture | |||||
| Pain intensity ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with pain relief ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth experience ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Use of pharmacological analgesia | Study population | RR 0.84 (0.54 to 1.30) | 128 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 2 | ||
| 424 per 1000 | 356 per 1000 (229 to 552) | |||||
| Assisted vaginal birth | Study population | RR 1.60 (0.47 to 5.39) | 128 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 2 | ||
| 61 per 1000 | 97 per 1000 (28 to 327) | |||||
| Caesarean section | Study population | RR 1.33 (0.37 to 4.73) | 128 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 2 | ||
| 61 per 1000 | 81 per 1000 (22 to 287) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded two levels due to very serious risk of bias: high or unclear risk of bias in both blinding performance and detection bias
2 Downgraded two levels due to very serious imprecision: small study (128) with few events and wide confidence intervals crossing the line of no effect
Summary of findings 5. Acupressure compared to sham control for pain management in labour.
| Acupressure compared to sham control for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupressure Comparison: sham control | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with sham control | Risk with acupressure | |||||
| Pain intensity as measured by a 10 cm visual analogue scale. Lower scores indicate less pain |
The mean pain intensity in the control groups was 8.35 | The mean pain intensity score in the intervention group was 1.93 lower (3.31 lower to 0.55 lower) | 472 (6 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | ||
| Satisfaction with pain relief ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth experience ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Use of pharmacological analgesia | Study population | RR 0.54 (0.20 to 1.43) | 75 (1 RCT) | ⊕⊕⊝⊝ LOW 3 | ||
| 256 per 1000 | 138 per 1000 (51 to 367) | |||||
| Assisted vaginal birth | Study population | RR 3.00 (0.13 to 71.92) | 100 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 4 5 | ||
| 0 per 1000 | 0 per 1000 (0 to 0) | |||||
| Caesarean section | Study population | RR 0.44 (0.27 to 0.71) | 313 (4 RCTs) | ⊕⊕⊕⊝ MODERATE 6 | ||
| 308 per 1000 | 136 per 1000 (83 to 219) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded one level for serious risk of bias: majority of studies have unclear risk of bias in at least three domains.
2 Downgraded two levels for very serious inconsistency: considerable heterogeneity (I2 = 94%)
3 Downgraded two levels for very serious imprecision: very small sample size (75), small number of events and very wide confidence intervals
4 Downgraded one level for serious risk of bias: single study has high risk of performance bias and an unclear risk of allocation bias
5 Downgraded two levels for very serious imprecision: small sample size (100) and very wide confidence interval and small number of events
6 Downgraded one level for serious risk of bias: all studies have unclear risk of bias in at least three domains. Two studies have high or unclear risk of bias relating to performance bias
Summary of findings 6. Acupressure compared to usual care for pain management in labour.
| Acupressure compared to usual care for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupressure Comparison: usual care | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with usual care | Risk with acupressure | |||||
| Pain intensity as measured by numeric rating scale (NRS) and visual analogue scale (VAS). Lower scores indicate less pain. |
The mean pain intensity was 8.44 | The mean pain intensity score in the intervention group was 1.07 standard deviations lower (1.45 lower to 0.69 lower). | 620 (8 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | The use of acupressure would result in a pain score approximately 2 cm lower on a 10 cm VAS or 2 points on a numeric rating scale compared to usual care. | |
| Satisfaction with pain relief assessed with: higher score indicate greater satisfaction with pain relief. Scale from: 0 to 3 | The mean satisfaction score with pain relief in the control group was 1.6 | The mean satisfaction with pain relief score was 1.05 higher (0.75 higher to 1.35 higher) | 105 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 3 4 | ||
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth experience ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Use of pharmacological pain relief ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Assisted vaginal birth ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Caesarean section | Study population | RR 0.82 (0.54 to 1.23) | 391 (4 RCTs) | ⊕⊕⊝⊝ LOW 5 6 | ||
| 241 per 1000 | 198 per 1000 (130 to 296) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; NRS: numeric rating scale; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded one level due to serious risk of bias: majority of included studies have high or unclear risk of bias relating to performance and detection bias
2 Downgraded two levels due to very serious inconsistency: considerable heterogeneity (I2 = 75%)
3 Downgraded two levels due to very serious risk of bias: single study at high risk of bias for selection, performance and detection bias. Very likely to have influenced the outcome
4 Downgraded one level due to serious imprecision: small sample size (105)
5 Downgraded one level due to serious risk of bias: two of the four studies included were at high risk of performance and detection bias, two studies were at high or unclear risk of selection bias and three at high or unclear risk of incomplete outcome data
6 Downgraded one level due to serious imprecision: wide confidence intervals incorporating both benefit and harm
Summary of findings 7. Acupressure compared to combined control for pain management in labour.
| Acupressure compared to combined control for pain management in labour | ||||||
| Patient or population: pain management in labour Setting: hospital Intervention: acupressure Comparison: combined control | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with combined control | Risk with acupressure | |||||
| Pain intensity One study used VAS pain score on scale 1 ‐ 100 mm One study used VAS pain score on scale 1 ‐ 10 mm ‐ the mean score of pre‐ and post‐intervention difference in pain perception measured by VAS was taken in three phases, latent, active and transitional |
The mean pain intensity score in the intervention group was 0.42 standard deviations lower (0.65 lower to 0.18 lower) | 322 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | |||
| Satisfaction with pain relief ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Sense of control in labour ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Satisfaction with childbirth assessed with: greater score indicates greater satisfaction Scale from: 0 to 100 | The mean satisfaction score with childbirth in the control group was 80.2 | The mean satisfaction score in the intervention group was 4.8 higher (2.29 lower to 11.89 higher) | ‐ | 212 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2 3 | |
| Use of pharmacological analgesia | Study population | RR 0.94 (0.71 to 1.25) | 212 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2 4 | ||
| 525 per 1000 | 493 per 1000 (373 to 656) | |||||
| Assisted vaginal birth | Study population | RR 0.81 (0.39 to 1.67) | 212 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2 4 | ||
| 156 per 1000 | 126 per 1000 (61 to 261) | |||||
| Caesarean section | Study population | RR 0.48 (0.22 to 1.04) | 212 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2 4 | ||
| 206 per 1000 | 99 per 1000 (45 to 214) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded one level due to serious risk of bias: both studies have unclear risk of bias for performance bias, possible effect on this outcome
2 Downgraded one level due to serious risk of bias: single study has unclear risk of performance bias, likely to effect this outcome
3 Downgraded two levels due to very serious imprecision: wide confidence interval greater than 0.25 on either side of the line of no effect and small sample size
4 Downgraded two levels for very serious imprecision: wide confidence interval encompassing both benefit and harm and small sample size
Background
This review is one in a series of Cochrane Reviews examining pain management in labour. An earlier version of this review contributed to an overview of systematic reviews of pain management for women in labour (Jones 2012) and shared a generic protocol (Jones 2011). This review is an update of a review last published in 2011 (Smith 2011b).
Description of the condition
Labour presents a physiological and psychological challenge for women. As labour becomes more imminent, this can be a time of conflicting emotions: fear and apprehension can be coupled with excitement and happiness. Tension, anxiety and fear are factors contributing towards women's perception of pain and may also affect their labour and birth experience. Pain associated with labour has been described as one of the most intense forms of pain that can be experienced (Melzack 1984), although conversely some women do not experience intense pain during labour. Labour involves three stages, relating to dilation of the cervix, birth of the baby and delivery of the placenta. The latent phase is the early part of labour where there are irregular contractions and the cervix is softening and beginning to dilate. The first stage of labour consists of regular contractions with increasing strength and frequency accompanied by more significant cervical dilation of at least 4 cm to 6 cm. Transition may be observable anywhere between 7 cm to 8 cm and full dilation. The second stage of labour commences from full cervical dilation to the birth of the baby. The third stage of labour involves expulsion of the placenta.
Pain experienced by women in labour is caused by uterine contractions, the dilatation of the cervix and, in the late first stage and second stage, by stretching of the vagina and pelvic floor to accommodate the baby. There are different philosophies of pain management, which involve strategies to prevent what has been described as the fear‐tension‐pain cycle (Dick‐Read 2004; Dowswell 2009). Dick‐Read 2004 an advocate of 'natural childbirth', suggested that fear and anxiety can produce muscle tension, resulting in an increased perception of pain. The gate control theory of pain, first proposed by Melzack and Wall in 1965, suggests that pain can be offset by other 'larger' or overriding sensations, such as rubbing or pressing on an injury to reduce pain sensation (Melzack 1965). Melzack and colleagues further proposed the neuromatrix theory of pain, which introduces the notion that pain is multidimensional, and that pain intensity is influenced by many factors, including sensory, emotional and cognitive processes, including experiences and memory (Melzack 2004). In labour, the theory of pain incorporates elements of the gate control theory, but also past experiences, cultural factors, emotional state, cognitive input, stress regulation and immune systems, as well as immediate sensory input (Trout 2004). However, the complete removal of pain does not necessarily mean a more satisfying birth experience for women (Dickenson 2003). A follow‐up study at five years after birth found those women who had epidurals were less positive about the birth five years later (Maimburg 2016). The literature suggests that satisfaction with childbirth is significantly linked with women's sense of agency and participation in decision‐making during pregnancy and birth (Hodnett 2002; Hollins Martin 2013; Hotelling 2013; Howarth 2010). Effective and satisfactory pain management needs to be individualised for each woman, and may be influenced by two paradigms, working with pain, or pain relief (Leap 2010). The working with pain paradigm includes the belief that there are long‐term benefits to promoting normal birth, and that pain and women's agency plays an important role in this process. With a focus on women's natural hormonal mediation of labour, the working with pain approach offers support and encouragement to women, advocates the use of immersion in water, comfortable positions and self‐help techniques to cope with normal labour pain and facilitate the normal hormones of labour. The pain relief paradigm is characterised by the belief that no woman need suffer pain in labour and women are offered a variety of pharmacological pain relief.
The two concepts of efficacy and effectiveness are also important to consider when evaluating research outcomes for labour pain management. Efficacy trials are designed to show the extent to which a specific treatment or component of an intervention is effective under ideal experimental circumstances, and often use a placebo or sham comparison. Commonly, pain scales are used to assess the effectiveness of acupuncture or acupressure interventions, especially when evaluating treatments providing 'pain relief'. The most commonly used scale is the visual analogue scale (VAS), which assesses reduction in pain scores out of 10 or 100, in response to the intervention. However, effectiveness trials are designed to assess the effect of the whole therapy in a general population, and are often compared to usual care. When considering the 'working with pain paradigm', the effectiveness of an intervention may be indicated by a reduction of pharmacological pain medication, and satisfaction scores, and may not necessarily be reflected in pain scores (MacPherson 2008).
Description of the intervention
Acupuncture has a long history of use in Asia, including China, Japan, Korea and Taiwan. Traditional Chinese medicine (TCM), with acupuncture as one of the major modalities, describes a state of health maintained by a balance of energy or Qi in the body. Acupuncture performed within the context of TCM is a complex intervention involving not only technical needling skill but development of a therapeutic relationship, formulation of a diagnosis, provision of lifestyle advice, and often administering co‐interventions such as gua sha (scrapping), tuina (massage), moxibustion (a type of Chinese medicine which involves burning a herb close to the skin) or electrical stimulation. In clinical practice, use of co‐interventions is not uncommon although acupuncture is the primary focus. Acupuncture involves the insertion of fine needles into different parts of the body to correct the imbalance of energy in the body. TCM and classical acupuncture explain disease and physiological function based on theoretical concepts of Yin and Yang and the Five Elements (Beinfield 1991; Hicks 2011; Maciocia 2015). Five element acupuncture is based on the classical Chinese medicine texts and has been developed for application in a Western context with different diagnosis and treatment protocols to those used in Asia (Hicks 2011).A Westernised medical application of acupuncture involves the use of acupuncture using trigger points, segmental points and commonly used formula points. Auricular therapy, a form of Western acupuncture, involves the use of the ear to make a diagnosis and subsequent needling to points on the ear. Medical acupuncture may involve the application of acupuncture based on the principles of neurophysiology and anatomy, rather than TCM principles and philosophy. The style and approach of acupuncture characterises the acupuncture point selection and related treatment parameters administered in clinical practice and research.
Acupressure has its origins in early China (Beinfield 1991), and is based on the same paradigm as described for acupuncture. When acupressure is applied, the therapist uses their hands and fingers to activate the same points as applied by acupuncture. Sometimes only a few points need touch applied to alleviate pain, or bring about a feeling of relaxation. In other circumstances a combinations of points will be used to achieve a greater effect. There are several forms of acupressure, which draw on the same knowledge and philosophical system as other forms of traditional Asian medicine. Some of these systems are applied by trained health professionals and others can be applied by the individual by pressing or activating the points.
The use of complementary and alternative medicine (CAM) including acupuncture and acupressure has become popular with consumers worldwide. Studies suggest that between 36% and 62% of adults in industrialised nations use some form of CAM to prevent or treat health‐related problems (Barnes 2004). Complementary therapies are more commonly used by women of reproductive age, with almost half (49%) reporting use (Eisenberg 1998). In a recent Australian study, women were reported to be the highest users of CAM, and that a significant proportion of women are using these therapies during pregnancy (Steel 2014). A review of 14 studies with large sample sizes (N > 200) on the use of CAM in pregnancy identified a prevalence rate ranging from 1% to 87% (with nine falling between 20% and 60%) (Adams 2009). The review identified use of various complementary therapies including acupuncture and acupressure, aromatherapy, massage, yoga, homeopathy and chiropractic care. The review also showed many pregnant women had used more than one complementary product or service (Adams 2009). Many women would like to avoid pharmacological or invasive methods of pain relief in labour and this may contribute towards the popularity of complementary methods of pain management (Steel 2014). A recent Australian study also showed that women and partners who were taught a variety of complementary therapy techniques in an antenatal education class, used between three and four different therapies for pain management during labour (Levett 2016b).
How the intervention might work
Acupuncture has been used to treat a number of painful conditions, and several theories have been presented as to how acupuncture may work. It has been proposed that acupuncture may modify the perception of pain, or alter physiological functions (Stux 1995). Since the majority of acupuncture points are either connected to, or located near neural structures this suggests that acupuncture stimulates the nervous system (Zullo 2017). From a Western acupuncture perspective, points selected are based according to the innervation of the target organ, e.g. the uterus. Activation of muscle afferents at this segmental level transmits signals in the spinal cord and in the central nervous system. During needle stimulation of common acupuncture points for pain, signals are transmitted to the spinal cord, and via afferent pathways to the midbrain. The perception of pain emerges from the resulting flow and integration of this information among specific brain areas via neurochemical and hormonal changes, and may lead to a change in the perception of pain. Another theory suggests that acupuncture stimulates the body to produce endorphins, which reduce pain (Pomeranz 1989). Other pain‐relieving substances called opioids may be released into the body during acupuncture treatment (Ng 1992). Both segmental and central mechanisms of acupuncture are likely to be involved in the total effect of acupuncture (Stener‐Victorin 2006).
In a meta‐analysis by Chae 2013, authors reviewed 28 fMRI (functional magnetic resonance imaging) studies of acupuncture and touch stimulation, and found that acupuncture stimulation showed common patterns of activation and deactivation in the brain, and that touch showed these same patterns, but was not significant. The deactivation patterns seen in the studies correlated with areas of the brain associated with lower pain and anxiety perception, as well as overlapping with the area of the brain known as the ‘pain matrix’ in the brain. Research by Anderson 2012 suggests that acupuncture works by regulating the interaction of the two branches of the autonomic nervous system, sympathetic and parasympathetic.
Why it is important to do this review
There is interest by women to use additional forms of care to assist with their pain management in labour. It is important to examine the efficacy, effectiveness and safety of under‐evaluated forms of treatment to enable women, health providers and policy makers to make informed decisions about care. A number of clinical trials and a review of current reviews (Levett 2014) have been performed to study the efficacy of acupuncture for pain in labour although it remains uncertain whether the existing evidence is rigorous enough to reach a definitive conclusion.
This review is one in a series of Cochrane Reviews examining pain management in labour. An earlier version of this review contributed to an overview of systematic reviews of pain management for women in labour (Jones 2012) and shared a generic protocol (Jones 2011). This review is an update of a review last published in 2011 (Smith 2011b).
Objectives
To examine the effects of acupuncture and acupressure for pain management in labour.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) only. We included studies reported in abstract form if there was sufficient information to permit assessment of risk of bias. Cluster‐trials were eligible for inclusion, but none were identified. Cross‐over trials and quasi‐randomised trials were not eligible for inclusion.
Types of participants
Labouring women either in spontaneous or induced labour, irrespective of parity and pre‐term or post date status. We included studies of women with singleton or multiple pregnancies.
Types of interventions
The previous version of this review (Smith 2011b) contributed to an overview of systematic reviews of interventions for pain management in labour (Jones 2012), and shared a generic protocol (Jones 2011). To avoid duplication, the different methods of pain management were listed in a specific order, from one to 15. Individual reviews focusing on particular interventions included comparisons with only the intervention above it on the list. The list is as follows.
Placebo/no treatment
Hypnosis (Madden 2016)
Biofeedback (Barragán 2011)
Intracutaneous or subcutaneous sterile water injection (Derry 2012)
Immersion in water (Cluett 2018)
Aromatherapy (Smith 2011a)
Relaxation techniques (yoga, music, audio) (Smith 2018a)
Acupuncture or acupressure (this review)
Manual methods (massage, reflexology) (Smith 2018b)
Transcutaneous electrical nerve stimulation (TENS) (Dowswell 2009)
Inhaled analgesia
Opioids (Smith 2018c)
Non‐opioid drugs (Othman 2012)
Local anaesthetic nerve blocks
Epidural (including combined spinal‐epidural) (Anim‐Somuah 2018; Simmons 2012)
Accordingly, this review includes comparisons of any type of acupuncture or acupressure compared with any other type of acupuncture or acupressure, as well as any type of acupuncture or acupressure compared with: 1. placebo/no treatment; 2. hypnosis; 3. biofeedback; 4. intracutaneous or subcutaneous sterile water injection; 5. immersion in water; 6. aromatherapy; 7. relaxation techniques (yoga, music, audio).
Types of outcome measures
Primary outcomes
Effects of interventions
Pain intensity (as defined by trialists)
Satisfaction with pain relief (as defined by trialists)
Sense of control in labour (as defined by trialists)
Satisfaction with childbirth experience
Use of pharmacological pain relief
Safety of interventions
Effect (negative) on mother/baby interaction
Breastfeeding (at specified time points)
Assisted vaginal birth
Caesarean section
Side effects (for mother and baby; review specific)
Admission to special care baby unit/neonatal intensive care unit (as defined by trialists)
Apgar score less than seven at five minutes
Poor infant outcomes at long‐term follow‐up (as defined by trialists)
Other outcomes
Cost (as defined by trialists)
Secondary outcomes
Maternal
Length of labour; mode of birth; need for augmentation with oxytocin; perineal trauma (defined as episiotomy and incidence of second‐ or third‐degree tear); maternal blood loss (postpartum haemorrhage defined as greater than 500 mL); relaxation; anxiety.
Neonatal
Need for mechanical ventilation; neonatal encephalopathy.
Search methods for identification of studies
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Electronic searches
For this update, we searched Cochrane Pregnancy and Childbirth’s Trials Register by contacting their Information Specialist (25 February 2019).
The Register is a database containing over 25,000 reports of controlled trials in the field of pregnancy and childbirth. It represents over 30 years of searching. For full current search methods used to populate Pregnancy and Childbirth’s Trials Register including the detailed search strategies for CENTRAL, MEDLINE, Embase and CINAHL; the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service, please follow this link.
Briefly, Cochrane Pregnancy and Childbirth’s Trials Register is maintained by their Information Specialist and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE (Ovid);
weekly searches of Embase (Ovid);
monthly searches of CINAHL (EBSCO);
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Search results are screened by two people and the full text of all relevant trial reports identified through the searching activities described above is reviewed. Based on the intervention described, each trial report is assigned a number that corresponds to a specific Pregnancy and Childbirth review topic (or topics), and is then added to the Register. The Information Specialist searches the Register for each review using this topic number rather than keywords. This results in a more specific search set that has been fully accounted for in the relevant review sections (Included studies; Excluded studies; Studies awaiting classification; Ongoing studies).
In addition, we searched the Cochrane Central Register of Controlled Trials (the Cochrane Library 2019, Issue 1), MEDLINE (1966 to 25 Febriuary 2019), and CINAHL (1980 to 25 February 2019) using a combination of subject headings and text words. See Appendix 1.
We also searched ClinicalTrials.gov (25 February 2019) and the WHO International Clinical Trials Registry Platfory (ICTRP) (25 February 2019) for unpublished, planned and ongoing trial reports using the search methods detailed in Appendix 2.
Searching other resources
We searched the reference lists of all included studies.
We did not apply any language or date restrictions.
Data collection and analysis
For methods used in the previous version of this review, seeSmith 2011b.
For this update, the following methods were used for assessing the 79 reports that were identified as a result of the updated search and we also reassessed the five trial reports in the Studies awaiting classification and the two in Ongoing studies sections of Smith 2011b.
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Selection of studies
Two review authors independently assessed for inclusion all the potential studies identified as a result of the search strategy. We resolved any disagreement through discussion or, if required, we consulted the third review author.
Data extraction and management
We designed a form to extract data. For eligible studies, two review authors extracted the data using the agreed form. We resolved discrepancies through discussion or, if required, we consulted the third review author. Data were entered into Review Manager software (RevMan 2014) and checked for accuracy.
When information regarding any of the above was unclear, we contacted authors of the original reports to provide further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Any disagreement was resolved by discussion or by involving a third assessor.
(1) Random sequence generation (checking for possible selection bias)
We described for each included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias when it was unclear, or there was insufficient reporting.
(2) Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias or there was insufficient reporting.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
We described for each included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded, or if we judged that the lack of blinding unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high or unclear risk of bias for participants;
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
We described for each included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we planned to re‐include missing data in the analyses which we undertook.
We assessed methods as:
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not pre‐specified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for each included study any important concerns we had about other possible sources of bias.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). With reference to (1) to (6) above, we planned to assess the likely magnitude and direction of the bias and whether we considered it is likely to impact on the findings. In future updates, we will explore the impact of the level of bias through undertaking sensitivity analyses ‐ seeSensitivity analysis.
Assessment of the certainty of the evidence using the GRADE approach
For this update, the certainty of the evidence was assessed using the GRADE approach as outlined in the GRADE Handbook in order to assess the certainty of the body of evidence relating to the following outcomes for the main comparisons: acupuncture compared to sham control; acupuncture compared to usual care; acupuncture compared to no treatment; acupuncture compared to water injection; acupressure compared to sham control; acupressure compared to usual care; acupressure compared to combined control.
Pain intensity (as defined by trialists)
Satisfaction with pain relief (as defined by trialists)
Sense of control in labour (as defined by trialists)
Satisfaction with childbirth experience
Use of pharmacological pain relief
Assisted vaginal birth
Caesarean section
These outcomes have been included in our 'Summary of findings' tables (Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7).
We used the GRADEpro Guideline Development Tool to import data from Review Manager 5.3 (RevMan 2014) in order to create 'Summary of findings’ tables. A summary of the intervention effect and a measure of certainty for each of the above outcomes was produced using the GRADE approach. The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the certainty of the body of evidence for each outcome. The evidence can be downgraded from 'high certainty' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates or potential publication bias.
Assessment of the quality of the acupuncture intervention delivered
We assessed the quality of the acupuncture or acupressure intervention in published journal articles using the NICMAN scale (Smith 2017). The NICMAN scale was developed to assess the quality of the acupuncture delivered in a clinical trial, and is designed to be used in combination with the STRICTA reporting guidelines (MacPherson 2010). This scale assesses and scores the following: the rationale behind the point selection, the qualifications and experience of the practitioner delivering the intervention, the adequacy of the number of treatment sessions, and the reporting of vital components of the acupuncture practice itself such as needle depth, diameter and stimulation. Higher scores indicate improved quality of the acupuncture intervention delivered, but there is no cut‐off for a 'high' versus 'low' quality score on the NICMAN scale. Each trial was independently scored out of 23 by two review authors (CS, KL, MA). Any discrepancies were resolved by discussion. If this was not reached a third review author (KL, CS or MA) decided on the final score.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented results as summary risk ratio with 95% confidence intervals.
Continuous data
We used the mean difference if outcomes were measured in the same way between trials. We used the standardised mean difference to combine trials that measured the same outcome, but used different methods.
Unit of analysis issues
Cluster‐randomised trials
If we had identified cluster‐randomised trials, we planned to include them in the analyses along with individually‐randomised trials. If such trials are identified in future updates of the review, we will adjust their sample sizes using the methods described in the Cochrane Handbook for Systematic Reviews of Interventions using an estimate of the intra‐cluster correlation co‐efficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population. If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐randomised trials and individually‐randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely. We will also acknowledge heterogeneity in the randomisation unit and perform a sensitivity analysis to investigate the effects of the randomisation unit.
Cross‐over trials
Cross‐over trials are not a suitable design for trials looking at interventions in labour and have been excluded.
Other unit of analysis issues
If we had identified trials with multiple arms, we planned that data from both treatment arms would be combined into one group. For studies with a sham control and no treatment control group, the shared intervention was divided evenly between groups and the weighting adjusted as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Dealing with missing data
For included studies, levels of attrition were noted. In future updates, if more eligible studies are included, the impact of including studies with high levels of missing data in the overall assessment of treatment effect will be explored by using sensitivity analysis.
For all outcomes, analyses were carried out, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the Tau², I² and Chi² statistics. We regarded heterogeneity as substantial if the I² was greater than 30% and either the Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. In future updates, if we identify substantial heterogeneity (above 30%), we plan to explore it by pre‐specified subgroup analysis.
Assessment of reporting biases
In future updates, if there are 10 or more studies in the meta‐analysis we will investigate reporting biases (such as publication bias) using funnel plots. We will assess funnel plot asymmetry visually. If asymmetry is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials were examining the same intervention, and the trials’ populations and methods were judged sufficiently similar.
If there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary, if an average treatment effect across trials was considered clinically meaningful. The random‐effects summary was treated as the average range of possible treatment effects and we discussed the clinical implications of treatment effects differing between trials. If the average treatment effect was not clinically meaningful, we did not combine trials. Where we used random‐effects analyses, the results were presented as the average treatment effect with 95% confidence intervals, and the estimates of Tau² and I².
Subgroup analysis and investigation of heterogeneity
Had we identified substantial heterogeneity, we planned to investigate it using subgroup analyses and sensitivity analyses. However, there were too few data included in any one comparison to carry out meaningful subgroup analysis.
In future updates, if possible we will carry out the following subgroup analyses for primary outcomes.
Spontaneous labour versus induced labour
Nulliparous versus multiparous
Term versus preterm
Continuous support in labour versus no continuous support
We will assess subgroup differences by interaction tests available within RevMan. We will report the results of subgroup analyses quoting the Chi² statistic and P value, and the interaction test I² value.
We did carry out subgroup analysis by type of acupuncture: manual acupuncture versus electro‐acupuncture, but there was not enough data in any one subgroup to demonstrate any differential effects.
Sensitivity analysis
Where subgroup analysis failed to explain the heterogeneity, we planned to analyse the data using the random‐effects model. A priori, we planned to perform sensitivity analyses on results to look at the possible contribution of: (1) differences in methodological quality, with trials of high quality (low risk of bias) compared to all trials; and (2) publication bias by country. If publication bias was present we planned to undertake a sensitivity analysis excluding trials from countries where there was a greater publication bias.
Results
Description of studies
Results of the search
See Figure 1.
1.
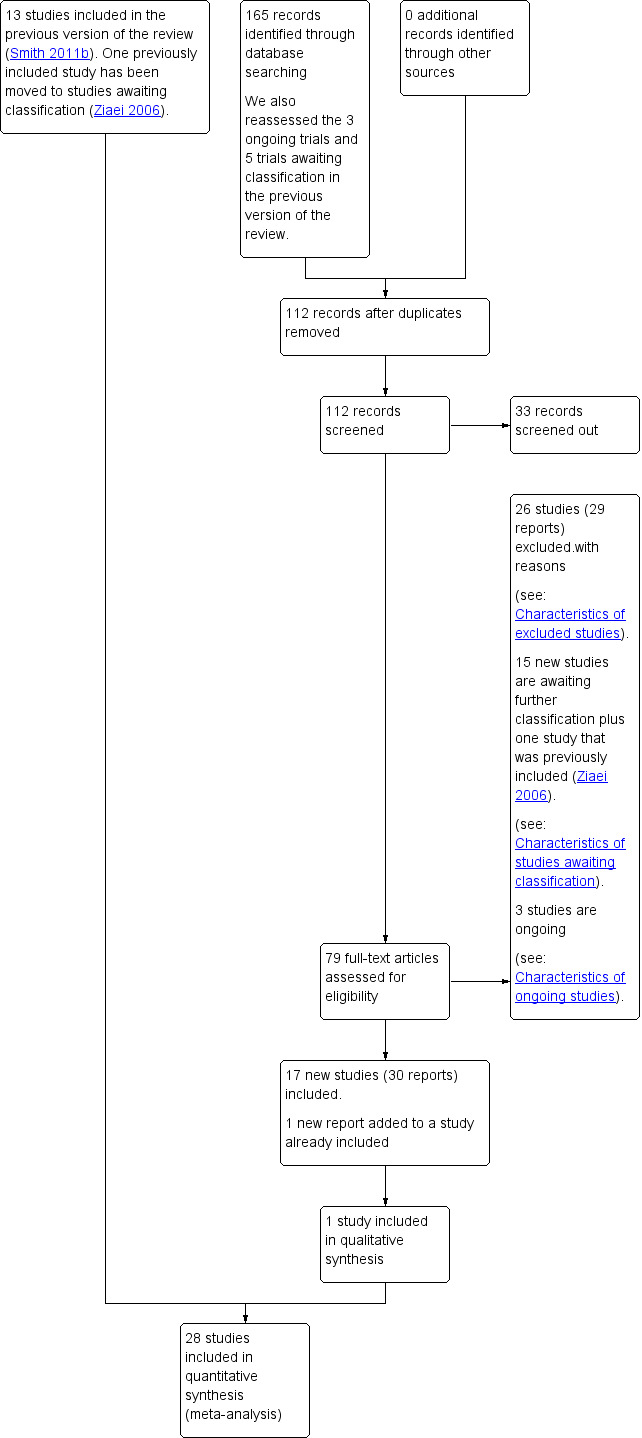
Study flow diagram.
For this update, we assessed 165 new records from the search. We also reassessed five studies that were awaiting classification and three ongoing studies from the previous version of the review. We had 112 records after removal of duplicates. From these, we screened out 33, leaving us with 79 trial reports to assess. Of these, we included 17 new studies (30 reports), added an additional report to an already included study, and excluded 26 (29 reports) Fifteen new studies are awaiting further classification (Studies awaiting classification) and three are ongoing (Ongoing studies).
One study (Ziaei 2006) had been previously included in a previous update (Smith 2011b). In this update it was moved to Studies awaiting classification due to having an unclear risk of bias across all domains and the authors had not responded to requests for further information.
The review included 28 trials of 3960 women, with data contributing to data and analysis from 27 trials of 3930 women.
Included studies
Study design
All studies were parallel design. Eleven studies had two groups (Calik 2014; Hamidzadeh 2012; Hamlaci 2017; Hantoushzadeh 2007; Kashanian 2010; Lee 2004; Martensson 2008; Nesheim 2003; Sehhatie‐Shafaie 2013; Skilnand 2002; Tjung 2008). Fourteen studies had three groups (Borup 2009; Chung 2003; Dabiri 2014; Dong 2015; Hjelmstedt 2010; Kordi 2010; Ma 2011; Mafetoni 2016; Mafetoni 2016a; Mansouri 2018; Ozgoli 2016; Qu 2007; Salehian 2011; Vixner 2014), and three studies had four arms (Huang 2008; Mackenzie 2011; Ramnero 2002). Comparative and control groups varied. Thirteen studies used placebo or sham controls (Chung 2003; Dabiri 2014; Hantoushzadeh 2007; Hjelmstedt 2010; Kashanian 2010; Kordi 2010; Lee 2004; Ma 2011; Mackenzie 2011; Mafetoni 2016; Skilnand 2002; Sehhatie‐Shafaie 2013; Skilnand 2002). Placebo, sham, or minimal acupuncture techniques varied between invasive and non‐invasive techniques. Comparison with usual care comprised of medication used in four studies (Borup 2009; Huang 2008; Tjung 2008; Vixner 2014). Other control groups included unspecified care or usual care in five studies (Dong 2015; Hjelmstedt 2010; Mafetoni 2016a; Nesheim 2003; Ramnero 2002). Huang 2008 used transcutaneous electrical nerve stimulation (TENS) and a breathing group; Martensson 2008 used sterile water injections, and comparison with no intervention was reported in two studies (Calik 2014; Qu 2007). Ozgoli 2016 used two active groups and a usual care group.
Sample sizes
Studies included in the review had sample sizes ranging from 30 (Mafetoni 2016a) to 607 (Borup 2009).
Study location and sources of women
Nine studies were undertaken in Iran (Dabiri 2014; Hamidzadeh 2012; Hantoushzadeh 2007; Kashanian 2010; Kordi 2010; Mansouri 2018; Ozgoli 2016; Salehian 2011; Sehhatie‐Shafaie 2013), four studies were undertaken in China (Dong 2015; Huang 2008; Ma 2011; Qu 2007), three studies undertaken in Sweden (Martensson 2008; Ramnero 2002; Vixner 2014), two each in Norway (Nesheim 2003; Skilnand 2002), Brazil (Mafetoni 2016; Mafetoni 2016a), and Turkey (Calik 2014; Hamlaci 2017), and one study each in Denmark (Borup 2009), India (Hjelmstedt 2010), Korea (Lee 2004) Phillipines (Tjung 2008); Taiwan (Chung 2003) and the UK (Mackenzie 2011).
Participants
Seventeen studies recruited both nulliparous and multiparous women (Borup 2009; Chung 2003; Dabiri 2014; Dong 2015; Hamidzadeh 2012; Hamlaci 2017; Kordi 2010; Lee 2004; Ma 2011; Mafetoni 2016; Mafetoni 2016a; Martensson 2008; Nesheim 2003; Ramnero 2002; Sehhatie‐Shafaie 2013; Skilnand 2002; Vixner 2014). Nulliparous only women were recruited in eight studies (Calik 2014; Hantoushzadeh 2007; Hjelmstedt 2010; Kashanian 2010; Mackenzie 2011; Mansouri 2018; Ozgoli 2016; Salehian 2011). Parous women only were recruited in two studies (Huang 2008; Qu 2007). It was unclear in one study (Tjung 2008). Women were recruited in spontaneous labour in 19 studies (Calik 2014; Chung 2003; Dabiri 2014; Hamidzadeh 2012; Hamlaci 2017; Hantoushzadeh 2007; Kordi 2010; Mafetoni 2016; Mafetoni 2016a; Martensson 2008; Mansouri 2018; Nesheim 2003; Ozgoli 2016; Qu 2007; Ramnero 2002; Sehhatie‐Shafaie 2013; Skilnand 2002; Tjung 2008; Vixner 2014). Two studies recruited women in both spontaneous and induced labour (Borup 2009; Hjelmstedt 2010), and one study reported on only induced labour (Mackenzie 2011). Reporting on the onset of labour was unclear in six studies (Dong 2015; Huang 2008; Kashanian 2010; Lee 2004; Ma 2011; Salehian 2011).
The intervention was administered at term for the majority of trials studies except Huang 2008 where details were not reported. There were no studies specifically for pre‐term labour.
We included labouring women either in spontaneous or induced labour, irrespective of parity and pre‐term or post date status. We included women with singleton or multiple pregnancies.
Types of intervention
Fifteen studies used acupressure (Calik 2014; Chung 2003; Dabiri 2014; Hamidzadeh 2012; Hamlaci 2017; Hjelmstedt 2010; Kashanian 2010; Kordi 2010; Lee 2004; Mafetoni 2016; Mafetoni 2016a; Mansouri 2018; Ozgoli 2016; Salehian 2011; Sehhatie‐Shafaie 2013) and 13 studies used acupuncture (Borup 2009; Dong 2015; Hantoushzadeh 2007; Huang 2008; Ma 2011; Mackenzie 2011; Martensson 2008; Nesheim 2003; Qu 2007; Ramnero 2002; Skilnand 2002; Tjung 2008; Vixner 2014) (includes manual and electro‐acupuncture). Acupuncture and acupressure varied in point selection, frequency of treatment and number of treatments, with commonly used points included SP6, LI4, BL23, BL32, HT7, GB34, LR3, ST36, PC6, BL67. A fixed set of acupuncture points only were administered in four studies (Dong 2015; Ma 2011; Mackenzie 2011; Qu 2007). A fixed set of acupressure points was used in 15 studies (Calik 2014; Chung 2003; Dabiri 2014; Hamidzadeh 2012; Hamlaci 2017; Hjelmstedt 2010; Kashanian 2010; Kordi 2010; Lee 2004; Mafetoni 2016; Mafetoni 2016a; Mansouri 2018; Ozgoli 2016; Salehian 2011; Sehhatie‐Shafaie 2013). Individualised treatment was administered in eight studies (Borup 2009; Hantoushzadeh 2007; Huang 2008; Martensson 2008; Nesheim 2003; Ramnero 2002; Skilnand 2002; Vixner 2014). Auriculotherapy, ear acupressure was used in one trial (Mafetoni 2016a). SeeCharacteristics of included studies.
Outcome measures
Pain intensity during labour was measured by visual analogue scale (VAS) in 25 studies (Borup 2009; Calik 2014; Chung 2003; Dabiri 2014; Dong 2015; Hamidzadeh 2012; Hamlaci 2017; Hantoushzadeh 2007; Hjelmstedt 2010; Huang 2008; Kashanian 2010; Kordi 2010; Lee 2004; Ma 2011; Mackenzie 2011; Mafetoni 2016; Mafetoni 2016a; Martensson 2008; Mansouri 2018; Nesheim 2003; Salehian 2011; Sehhatie‐Shafaie 2013; Skilnand 2002; Tjung 2008;Vixner 2014) and by a 0 to 10 numeric rating scale (NRS) in three studies (Ozgoli 2016; Qu 2007; Ramnero 2002). Two studies (Calik 2014; Vixner 2014) did not report pain intensity outcome data in a format that allowed them to be included in the meta‐analysis, so these were reported narratively. When pain intensity scores were given at multiple time points, the last time point was used. Standardised mean difference (SMD) was used when combining VAS and NRS pain scores. Use of pharmacological analgesia was reported by 26 studies.
Length of labour was reported in eight studies (Dong 2015; Hamidzadeh 2012; Hamlaci 2017; Kashanian 2010; Lee 2004; Ma 2011; Salehian 2011; Vixner 2014), and mode of birth (spontaneous vaginal birth, assisted vaginal birth or caesarean section) was reported by 16 studies (Borup 2009; Calik 2014; Hamidzadeh 2012; Hantoushzadeh 2007; Hjelmstedt 2010; Huang 2008; Kashanian 2010; Mackenzie 2011; Martensson 2008; Mafetoni 2016a; Nesheim 2003; Ozgoli 2016; Ramnero 2002; Skilnand 2002; Tjung 2008; Vixner 2014). Maternal outcomes (satisfaction, sense of control, anxiety, childbirth experience and acceptability of the intervention) were reported in 12 studies (Borup 2009; Chung 2003; Hamidzadeh 2012; Hantoushzadeh 2007; Hjelmstedt 2010; Huang 2008; Lee 2004; Martensson 2008; Ozgoli 2016; Qu 2007; Ramnero 2002; Vixner 2014), and clinical outcomes were reported in the majority of studies, however some are reported narratively as they were presented in a format that was not consistent with the review (Qu 2007).
Satisfaction with pain relief or satisfaction with childbirth was reported either via a Likert scale or via a Yes/No response to a question relating to sufficient pain relief. To provide a dichotomous outcome for satisfaction when recorded via a Likert scale we combined the two most favourable categories (e.g. very satisfied and satisfied or very good and good) as a 'Yes' response, while neutral or negative categories were characterised as a 'No' response.
Dates of trials
The majority of the trials took place between the year 1999 to 2013: Borup 2009 (2002‐2004), Calik 2014 (2009‐2010), Dabiri 2014 (2011‐2012), Dong 2015 (2012‐2013), Hamidzadeh 2012 (2006), Hamlaci 2017 (2012), Hantoushzadeh 2007 (2005), Hjelmstedt 2010 (2007‐2008), Huang 2008 (2004‐2005), Kashanian 2010 (2007), Lee 2004 (2002), Mackenzie 2011 (2005‐2009), Mafetoni 2016 (2013), Ozgoli 2016 (2008), Qu 2007 (2004‐2005), Ramnero 2002 (1999‐2000), Salehian 2011 (2008‐2009), Sehhatie‐Shafaie 2013 (2012), Skilnand 2002 (1998‐1999), Vixner 2014 (2008‐2011), Mansouri 2018 (2017), Tjung 2008 (2007‐2008). Five studies did not report the study duration (Chung 2003; Kordi 2010; Ma 2011; Martensson 2008; Nesheim 2003).
Funding
Twelve studies reported funding sources. Borup 2009 was funded by the Asse and Ejnar Danielsen's Foundation, Kgs, Lyngby, Dnemark; Knowledge and Research Cener for Alternative medicine, Aarhus, Denmark; Sophus Jacobsen Foundation, Capenhagen, Denmar; The Danish Midwifery Organisation, Copenhangen, Denmark; Lundbeck Foundation, Copenhagen, Denmark; Mads Clausens Foundation, Nordborg, Denmark; Hede Nielsen Foundation, Horsens, Denmark; The Research Fund at Aarhus University Hosptial, Aarhus, Denmark; Else and Mogens Wedell‐Wedellsborgs Foundation, Copenhagen, Denmark; and King Christian the 10th Foundation, Copenhagen, Denmark; Hantoushzadeh 2007 was funded by the Vali Asr Research Centre for Reproductive Health; Hjelmstedt 2010 was funded by Osher Center for Integrative Medicine, Karolinska Institutet and the Centre for Health Care Science, Karolinska Institutet; Huang 2008 was funded by the National Traditional Chinese Medicine Administration of Traditional Chinese Medicine Science and Techology Research Special TCM Clinical Research Fund (04‐05LQ04); Kashanian 2010 was funded by Iran University of Medical Sciences; Ma 2011 was funded by the State Administration of Traditional Chinese Medicine; National Science Foundation of China; and E‐institutes of Shanghai Municipal Education Commission. Mackenzie 2011 was funded by a grant from the Oxfordshire Health Services Research Committee and the Uterine Contractility Trust fund, held by the Oxford Radcliffe NHS Trust. Martensson 2008 was funded by grants from Skaraborg Institute for Reseach and Development, Barnets, Lychopenning, The Swedish Association of Midwives, Hegu Svenska AB and the University of Skövde; Qu 2007 was funded by the Innovation Research Foundation by government of Heilongjiang Privince, China; Ramnero 2002 was funded by grants from Örebro Council Research Committee and Centre for Nursing Science, Örebro University Hospital; Sehhatie‐Shafaie 2013 was funded by Tabriz University of Medical Sciences. Vixner 2014 was funded by grants from the Centre for Clinical Research Dalarna, Karolinska Institutet, Uppsala‐Örebro Regional Research Council, University of Skövde, FOU Fyrbodal, Magnus Bergvall. Stiftelse, and Dalarna University, Sweden.
Declarations of interest
Seven studies reported no conflict of interest (Hjelmstedt 2010; Ma 2011; Mackenzie 2011; Mansouri 2018; Ozgoli 2016; Sehhatie‐Shafaie 2013; Vixner 2014). One study (Mackenzie 2011) stated that one trial author provides legal opinion on litigation cases. In the remaining 21 studies, there was no clear conflict of interest reported.
Quality of acupuncture
All 15 studies of acupuncture were assessed using the NICMAN Scale (Smith 2017). The NICMAN Scale uses an 11‐item scale to review the quality of acupuncture studies. We now include this and report on studies of acupuncture using this scale. The items include: clear description of the population; intervention; comparator; outcome; appropriateness of study design for question; inclusion of a differential diagnosis; selection of acupuncture points consistent with treatment principles; description of needles, needling depth, stimulation, and sensation; point location description and justification according to texts; treatments administered; and the qualifications of the person administering the treatments (Table 8).
1. NICMAN Score (Acupuncture studies only).
| Study ID | Total NICMAN Score | P | I | C | O | Study design | Differential diagnosis | Point selection | Needling parameters | Acupuncture point location | Treatment dosage | Therapist qualifications |
| Borup 2009 | 19 | 2 | 2 | 2 | 2 | 3 | 0 | 2 | 1 | 1 | 2 | 2 |
| Dong 2015 | 15 | 2 | 2 | 2 | 2 | 3 | 0 | 0 | 1 | 1 | 2 | 0 |
| Hantoushzadeh 2007 | 20 | 2 | 2 | 2 | 2 | 3 | 1 | 2 | 2 | 2 | 2 | 0 |
| Huang 2008 | 16 | 2 | 2 | 2 | 2 | 3 | 2 | 2 | 0 | 0 | 1 | 0 |
| Ma 2011 | 17 | 2 | 2 | 2 | 2 | 3 | 0 | 2 | 2 | 2 | 2 | 0 |
| MacKenzie 2011 | 19 | 2 | 2 | 2 | 2 | 3 | 0 | 2 | 1 | 2 | 1 | 2 |
| Martensson 2008 | 16 | 2 | 2 | 2 | 2 | 3 | 0 | 1 | 1 | 0 | 2 | 1 |
| Nesheim 2003 | 16 | 2 | 2 | 2 | 2 | 3 | 2 | 0 | 2 | 0 | 1 | 0 |
| Qu 2007 | 13 | 2 | 2 | 2 | 2 | 3 | 0 | 0 | 1 | 0 | 1 | 0 |
| Ramnero 2002 | 17 | 2 | 2 | 2 | 2 | 3 | 1 | 1 | 1 | 2 | 1 | 0 |
| Skilnand 2002 | 18 | 2 | 2 | 2 | 2 | 3 | 0 | 2 | 2 | 2 | 1 | 0 |
| Tjung 2008 | 17 | 2 | 2 | 2 | 2 | 3 | 0 | 0 | 1 | 2 | 1 | 2 |
| Vixner 2014 | 18 | 2 | 2 | 2 | 2 | 3 | 1 | 2 | 1 | 2 | 1 | 0 |
The studies that ranked the highest on the NICMAN Scale were Borup 2009 and Mackenzie 2011, each with a score of 90.5%. The study that ranked the lowest was Mansouri 2018 with a score of 47%. The other studies received scores between these figures: Hantoushzadeh 2007 received a score of 87.0%; Ma 2011 scored 81%; Ramnero 2002 scored 74%; Skilnand 2002 and Vixner 2014 both scored 78.3%. Dong 2015 received a score of 71.4%, and Huang 2008, Martensson 2008 and Nesheim 2003 each scored 70.0%.
In reviewing individual items on the NICMAN Scale, all studies scored at the highest level (2 out of 2 or 3 out of 3) for reporting of clear description of the population; intervention; comparator; outcome; and appropriateness of study design for question. Seven studies reported on the inclusion of a differential diagnosis, and scored 2 (Huang 2008; Nesheim 2003), 1 (Hantoushzadeh 2007; Skilnand 2002; Vixner 2014) or 0 (Martensson 2008; Skilnand 2002) for selection and justification of acupuncture points consistent with treatment principles, seven studies scored 2 (Borup 2009; Hantoushzadeh 2007; Huang 2008; Ma 2011; Mackenzie 2011; Skilnand 2002; Vixner 2014), two studies scored 1 (Martensson 2008; Ramnero 2002) and three studies scored 0 (Dong 2015; Nesheim 2003; Qu 2007; for description and justification of needles type and consistency, needling depth, stimulation and justification, and sensation, four studies scored 2 (Hantoushzadeh 2007; Ma 2011; Nesheim 2003; Skilnand 2002), eight studies scored 1 (Borup 2009; Dong 2015; Mackenzie 2011; Martensson 2008; Qu 2007; Ramnero 2002; Tjung 2008; Vixner 2014), and two studies scored 0 (Huang 2008; Mansouri 2018); for reporting of point location description and justification according to texts, seven studies scored 2 (Hantoushzadeh 2007; Ma 2011; Mackenzie 2011; Ramnero 2002; Skilnand 2002; Tjung 2008; Vixner 2014), two scored 1 (Borup 2009; Dong 2015) and five scored 0 (Huang 2008; Martensson 2008; Mansouri 2018; Nesheim 2003; Qu 2007; with regard to reporting of treatments administered during labour and justified, five scored 2 Borup 2009; Dong 2015; Hantoushzadeh 2007; Ma 2011; Martensson 2008), nine scored 1 (Huang 2008; Mackenzie 2011; Mansouri 2018; Nesheim 2003; Qu 2007; Ramnero 2002; Skilnand 2002; Tjung 2008; Vixner 2014), and none scored 0; and for qualifications of the person administering the treatments meeting World Health Organization guidelines (generally a member of a recognised acupuncture association or > 200 hours training), three studies scored 2 (Borup 2009; Mackenzie 2011; Tjung 2008), one study scored 1 (Martensson 2008), and the remainder scored 0 (Dong 2015; Hantoushzadeh 2007; Huang 2008; Ma 2011; Mansouri 2018; Nesheim 2003; Qu 2007; Ramnero 2002; Skilnand 2002; Vixner 2014).
Excluded studies
We excluded 34 trials;seeCharacteristics of excluded studies. Many studies did not meet the inclusion criteria based on the criteria for interventions: for example, the use of point injection therapy (Zhang 2000), or ice massage (Hajiamini 2012; Kaviani 2012). We excluded eight studies due to insufficient reporting of randomisation (Aghdam 2012; Bo 2006; Deepak 2013; Li 2006; Peng 2010; Ternov 1998; Wang 1994; Zhu 2013), and we were unable to ascertain true randomisation status from the author. The study design was unclear or did not meet the criteria for inclusion in seven studies (Deen 1985; Kermani 2015; Levett 2016a; Mucuk 2014; Sebastian 2014; Vixner 2017; Wu 2017). No clinically relevant outcomes were measured in nine trials (Asadi 2015; Can 2015; Li 1996; Mollart 2013; Moradi 2014; Nistler 2010; Shalev 1991; Shang 1995). One study was reported as an abstract only, with insufficient reporting to determine inclusion (Park 2003). Seven studies did not assess pain in labour (Alsharnoubi 2015; Haghighi 2016; Liu 2012; Liu 2015a; Liu 2015b; Masoudi 2014; Samadi 2018).
Risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved any disagreements by discussion or by involving another review author.
SeeFigure 2 and Figure 3 for a graphical summary of the 'Risk of bias' assessments by authors of the included studies based on the six risk of bias domains. No study was at a low risk of bias on all domains.
2.
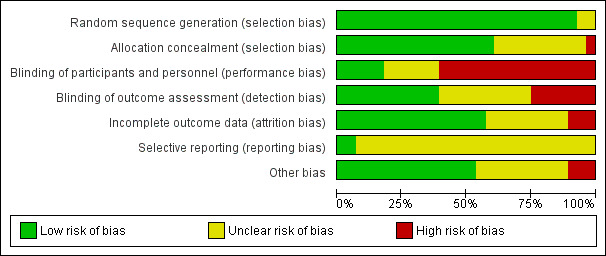
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
3.
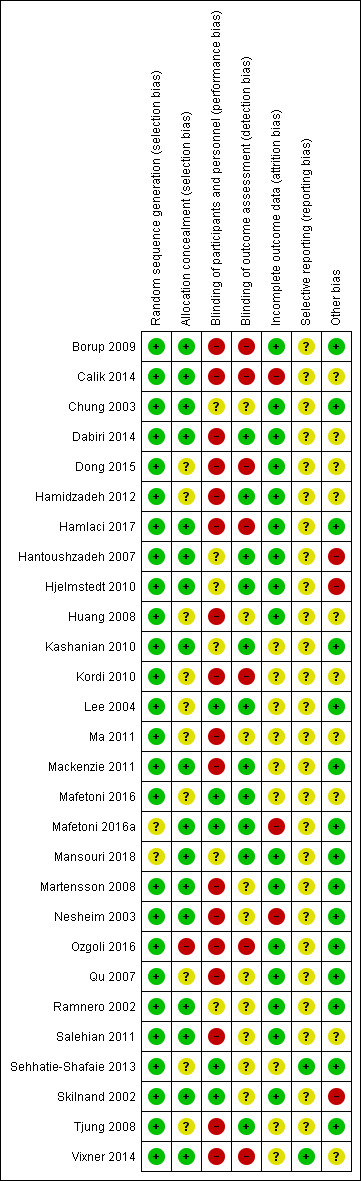
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Allocation
Method of allocation
All trials were assessed in terms of methods by which participants were allocation to intervention and control or sham groups. Seventeen trials reported the sequence was computer generated (Borup 2009; Calik 2014; Hamidzadeh 2012; Hantoushzadeh 2007; Hjelmstedt 2010; Huang 2008; Kashanian 2010; Kordi 2010; Ma 2011; Mackenzie 2011; Mafetoni 2016; Martensson 2008; Nesheim 2003; Ozgoli 2016; Salehian 2011; Sehhatie‐Shafaie 2013; Vixner 2014). The sequence was by lot drawing in six trials (Dabiri 2014; Dong 2015; Hamlaci 2017; Qu 2007; Skilnand 2002; Tjung 2008), coin tossing in one trial (Chung 2003), random number tables in one trial (Lee 2004), and shuffling cards in one trial (Ramnero 2002). The method of allocation generation was unclear in two studies (Mansouri 2018; Mafetoni 2016a).
Allocation concealment
Following adequate allocation to groups, allocation concealment was assessed for all studies. We assessed the methods used to prevent investigators' foreknowledge of group allocation, from evidence from the studies, extracted independently by two review authors. Where it was unclear, or not reported, we contacted the study author for clarification. Allocation concealment was described as low risk in 17 trials. Sealed envelopes were used in 15 trials (Calik 2014; Dabiri 2014; Hamlaci 2017; Hantoushzadeh 2007; Hjelmstedt 2010; Kashanian 2010; Mackenzie 2011; Martensson 2008; Mafetoni 2016a; Mansouri 2018; Nesheim 2003; Ramnero 2002; Salehian 2011; Skilnand 2002; Vixner 2014), central randomisation in one trial (Borup 2009) and sequential numbers in one trial (Chung 2003). One trial was at high risk due to no concealment (Ozgoli 2016). Ten trials were assessed at unclear risk in nine trials mainly due to method of concealment not being described (Dong 2015; Hamidzadeh 2012; Huang 2008; Kordi 2010; Lee 2004; Ma 2011; Mafetoni 2016; Qu 2007; Sehhatie‐Shafaie 2013; Tjung 2008).
Blinding
Blinding of participants and personnel (performance bias)
Participants (both participants and personnel) were largely aware of whether they had been assigned to acupuncture or acupressure or control. Some studies included sham controls, in an attempt to blind participants. Five trials were assessed at a low risk of bias (Lee 2004; Mafetoni 2016;Mafetoni 2016a; Sehhatie‐Shafaie 2013; Skilnand 2002). Blinding was assessed at high risk in 17 trials (Borup 2009, Calik 2014, Dabiri 2014; Dong 2015; Hamidzadeh 2012; Hamlaci 2017; Huang 2008; Kordi 2010; Ma 2011; Mackenzie 2011; Martensson 2008; Nesheim 2003; Ozgoli 2016; Qu 2007; Salehian 2011; Tjung 2008; Vixner 2014). The risk of blinding was unclear in six trials due to poor reporting (Chung 2003; Hantoushzadeh 2007; Hjelmstedt 2010; Kashanian 2010; Mansouri 2018; Ramnero 2002). We contacted study authors to clarify where possible.
Blinding of outcome assessment
We rated trials as having low risk of bias when researchers described blinded assessment of outcomes. Blinding was assessed at high risk, that is, assessment was largely done by the investigator, in seven trials (Borup 2009; Calik 2014; Dong 2015; Hamlaci 2017; Kordi 2010; Ozgoli 2016; Vixner 2014); 11 trials were at a low risk of bias, where assessment was performed by an independent person (Dabiri 2014; Hamidzadeh 2012; Hantoushzadeh 2007; Hjelmstedt 2010; Kashanian 2010; Lee 2004; Mackenzie 2011; Mafetoni 2016; Mafetoni 2016a; Mansouri 2018; Tjung 2008). Ten studies were at unclear risk of bias due to lack of reporting (Chung 2003; Huang 2008; Ma 2011; Martensson 2008; Nesheim 2003; Qu 2007; Ramnero 2002; Salehian 2011; Sehhatie‐Shafaie 2013; Skilnand 2002).
Incomplete outcome data
Outcome reporting, and risk of attrition, was assessed at a low risk of bias in 16 trials (Borup 2009; Chung 2003; Dabiri 2014; Dong 2015; Hamidzadeh 2012; Hamlaci 2017; Hantoushzadeh 2007; Hjelmstedt 2010; Huang 2008; Mansouri 2018; Martensson 2008;; Ozgoli 2016; Qu 2007; Ramnero 2002; Salehian 2011; Skilnand 2002), where missing data were clearly accounted for and dropout rates were low. Nine trials were at unclear risk (Kashanian 2010; Kordi 2010; Lee 2004; Ma 2011; Mackenzie 2011; Mafetoni 2016; Sehhatie‐Shafaie 2013; Tjung 2008; Vixner 2014), and three trials were assessed at high risk (Calik 2014; Mafetoni 2016a; Nesheim 2003) due to imbalance in dropout between groups and high attrition.
Selective reporting
Every effort was made to minimise the impact of reporting biases by undertaking comprehensive searches of multiple sources to identify unpublished material including protocols of randomised trials in English and Chinese. Although the study protocol was not available for most of the included studies, many showed consistency between results and methods sections. However, the risk of bias from selective reporting was determined to be unclear in 23 trials due to the absence of a study protocol, except for two trials assessed at low risk (Sehhatie‐Shafaie 2013; Vixner 2014).
Other potential sources of bias
The risk of bias from other sources of bias was rated as high risk in three trials due to lower pain scores in the control group prior to the commencement of the intervention, (Hantoushzadeh 2007); significant difference in baseline characteristics between groups (Hjelmstedt 2010; Skilnand 2002). Fifteen trials were assessed at, low risk (Borup 2009; Chung 2003; Hamlaci 2017; Kashanian 2010; Lee 2004; Mackenzie 2011; Mafetoni 2016a; Mansouri 2018; Martensson 2008; Nesheim 2003; Ozgoli 2016; Qu 2007; Ramnero 2002; Sehhatie‐Shafaie 2013; Tjung 2008) and unclear reporting in nine trials (Calik 2014; Dabiri 2014; Dong 2015; Hamidzadeh 2012; Huang 2008; Kordi 2010; Ma 2011; Mafetoni 2016; Salehian 2011; Vixner 2014).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7
This review included 27 trials of 3930 women in the meta‐analysis.
Data were not reported in a form that could be included in the meta‐analysis from Qu 2007 study and results are reported descriptively.
1) Acupuncture versus sham control
Five trials with 642 women reported on this comparison. No trial reported on the primary outcomes of: sense of control in labour, satisfaction with childbirth.
Primary outcomes
1.1) Outcome: pain intensity
Two trials assessed pain along a visual analogue scale (VAS) scale, a lower score indicated less pain. Data on this outcome were available from two trials and 325 women, (Analysis 1.1). Due to significant heterogeneity a random‐effects model was applied. Acupuncture may have little effect on reducing the intensity of pain felt by women when compared with sham acupuncture, (mean difference (MD) ‐4.42, 95% confidence interval (CI) ‐12.94 to 4.09, low‐certainty evidence).
1.1. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 1 Pain intensity.
1.2) Outcome: satisfaction with pain relief in labour
Satisfaction was assessed using a four‐point rating scale from very good to weak. Acupuncture probably improves satisfaction with pain relief in labour compared with control, (risk ratio (RR) 2.38, 95% CI 1.78 to 3.19, 1 trial, 150 women, moderate‐certainty evidence; Analysis 1.2).
1.2. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 2 Satisfaction with pain relief in labour.
1.3) Outcome: use of pharmacological analgesia
There was evidence of reduced use of pharmacological analgesia from manual acupuncture (RR 0.75, 95% CI 0.63 to 0.89, 2 trials, 261 women, moderate‐certainty evidence; Analysis 1.3).
1.3. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 3 Use of pharmacological analgesia.
1.4) Outcome: assisted vaginal birth
It is uncertain whether manual acupuncture reduces assisted vaginal birth when compared with sham acupuncture because the certainty of the evidence was found to be very low, with concerns due to imprecision, inconsistency of results and study limitations (RR 1.10, 95% CI 0.41 to 2.97, 2 trials, 261 women, very low‐certainty evidence), there was substantial heterogeneity I2 72% and a random‐effects model was applied; Analysis 1.4).
1.4. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 4 Assisted vaginal birth.
1.5) Outcome: caesarean section
There was no evidence of an effect for acupuncture in reducing caesarean section when compared with sham acupuncture (RR 1.11, 95% CI 0.49 to 2.48, 3 trials, 411 women, low‐certainty evidence;Analysis 1.5).
1.5. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 5 Caesarean section.
1.6) Outcome: Apgar score less than seven at five minutes
Two trials reported on this outcome. In the Mackenzie 2011 trial there were no babies with an Apgar score less than seven at five minutes. Skilnand 2002 reported on one event in the control group. The results are therefore unclear with so little data being provided for this outcome.
Secondary outcomes
1.7) Outcome: length of labour
The findings do not tell us whether acupuncture reduces the length of labour when compared with a sham control because the evidence was assessed to be of low certainty (MD ‐37.41 minutes, 95% CI ‐96.37 to 21.55; 1 trial, 175 women; Analysis 1.7).
1.7. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 7 Length of labour ‐ total.
1.8) Outcome: spontaneous vaginal birth
There was no evidence of an effect for acupuncture in increasing spontaneous vaginal birth when compared with sham acupuncture based on low‐certainty evidence (average RR 0.98, 95% CI 0.86 to 1.12, 3 trials, 411 women). There was significant heterogeneity between trials I2 = 64% and a random‐effects model was applied (Analysis 1.8).
1.8. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 8 Spontaneous vaginal birth.
1.9) Outcome: augmentation with oxytocin
There was significant heterogeneity between trials and so the results from the studies were not combined. The trial by Skilnand 2002 found reduced augmentation with synthetic oxytocin in the acupuncture group (RR 0.40, 95% CI 0.23 to 0.69), Hantoushzadeh 2007 found no evidence of a difference between groups (RR 0.93, 95% CI 0.85 to 1.02). The heterogeneity maybe explained by the length of time that the intervention was delivered which varied from two hours and until the time of delivery.
Subgroup analysis
There were not enough data relating to manual or electro‐acupuncture to demonstrate any differential effect according to type of acupuncture.
2) Acupuncture versus usual care
Ten trials with 1622 women had data suitable for inclusion in the meta‐analysis. One study (Vixner 2014) has outcomes reported narratively. No trial reported on the primary outcomes of: sense of control in labour, satisfaction with childbirth.
Primary outcomes
2.1) Outcome: pain intensity
Four trials, 495 women reported on this outcome (Analysis 2.1). Pain intensity was assessed with VAS or numeric rating scale (NRS): lower scores indicate less pain. We are uncertain if acupuncture reduces the pain intensity when compared with the control, there was significant heterogeneity and a random‐effects model was applied and the evidence was assessed as being very low certainty (standardised mean difference (SMD) ‐1.31, 95% CI ‐2.14 to ‐0.49, I2 = 93%, very low‐certainty evidence).
2.1. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 1 Pain intensity.
Vixner 2014 found that there were no differences between acupuncture groups (manual or electro acupuncture) and usual care when a simple non‐interaction model was used. When an interaction model was used there was evidence of an interaction between time and treatment group (P = 0.03), at 120 minutes manual acupuncture had lower pain scores than electro acupuncture, at 270 minutes manual acupuncture had lower pain scores than electro acupuncture and at 360 minutes usual care had lower pain scores than manual acupuncture.
2.2) Outcome: satisfaction with pain relief in labour
Two trials reported on this outcome assessed as the number who self reported satisfaction with pain relief.
Manual or electro acupuncture may have little effect on satisfaction with pain relief during labour (RR 1.07, 95% CI 0.96 to 1.20, 343 women, low‐certainty evidence; Analysis 2.2).
2.2. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 2 Satisfaction with pain relief in labour.
2.3) Outcome: use of pharmacological analgesia
Six trials and 1059 women reported on this outcome (Analysis 2.3). The findings do not tell us whether acupuncture may reduce use of pharmacological analgesia compared to a control because the evidence was assessed as very low certainty (average RR 0.72, 95% CI 0.60 to 0.85), there was significant heterogeneity (I2 = 70%) and a random‐effects analysis was undertaken.
2.3. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 3 Use of pharmacological analgesia.
2.4) Outcome: assisted vaginal birth
Six trials and 1217 women reported on this outcome. Acupuncture may make little difference to reducing assisted vaginal birth (RR 0.93, 95% CI 0.70 to 1.24, low‐certainty evidence;Analysis 2.4) (manual acupuncture (RR 0.87, 95% CI 0.64 to 1.17, 6 trials, 1089 women) or electro‐acupuncture (RR 1.60, 95% CI 0.64 to 4.04, 1 trial, 128 women).
2.4. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 4 Assisted vaginal birth.
2.5) Outcome: caesarean section
Five trials and 861 women reported on caesarean section. Acupuncture may make little difference to reducing caesarean section (RR 0.72, 95% CI 0.47 to 1.09, low‐certainty evidence; Analysis 2.5) (manual acupuncture (RR 0.78, 95% CI 0.50 to 1.24, 4 trials, 683 women), electro‐acupuncture (RR 0.46, 95% CI 0.16 to 1.28, 2 trials 178 women).
2.5. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 5 Caesarean section.
2.6) Outcome: Apgar score less than seven at five minutes
Six trials, 1061 women reported on this outcome. There was no evidence of harm from acupuncture (RR 0.99, 95% CI 0.28 to 3.47, very low‐certainty evidence; Analysis 2.6).
2.6. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 6 Apgar score < 7 at 5 minutes.
Secondary outcomes
2.7) Outcome: length of labour
Acupuncture may make no difference to reducing the length of labour in minutes (MD ‐13.89, 95% CI ‐28.93, 1.14, 3 trials, 608 women; Analysis 2.7), (manual acupuncture (MD 4.00, 95% CI ‐142.47 to 150.47, 1 trial, 124 women); electro‐acupuncture (MD ‐14.08, 95% CI ‐29.20 to 1.03, 3 trials, 484 women)).
2.7. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 7 Length of labour ‐ total.
2.8) Outcome: spontaneous vaginal birth
Four trials and 449 women reported on this outcome. Acupuncture probably makes little difference to rates of spontaneous vaginal birth (RR 0.98, 95% CI 0.89 to 1.08; Analysis 2.8), manual acupuncture (RR 0.96, 95% CI 0.85 to 1.10, 3 trials, 271 women), electro‐acupuncture (RR 0.99, 95% CI 0.86 to 1.14, 2 trials, 178 women).
2.8. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 8 Spontaneous vaginal birth.
2.9) Outcome: augmentation with oxytocin
Four trials and 813 women reported on this outcome. Acupuncture probably makes little difference to rates of augmentation compared with the control (RR 0.88, 95% CI 0.77 to 1.02; Analysis 2.9), manual acupuncture (RR 0.92, 95% CI 0.78 to 1.09, 3 trials, 635 women), electro‐acupuncture (RR 0.78, 95% CI 0.59 to 1.03, 2 trials, 178 women), although the CIs cross one and so a possible increase cannot be ruled out.
2.9. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 9 Augmentation with oxytocin.
2.10) Outcome: perineal trauma
One trial of 253 women reported on this outcome. The three‐arm study included electro and manual acupuncture and may make little difference to reducing perineal trauma (RR 0.49, 95% CI 0.19 to 1.26; Analysis 2.10).
2.10. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 10 Perineal trauma.
2.11) Outcome: maternal blood loss > 500 mL
One trial of 253 women reported on this outcome. The three arm study included electro and manual acupuncture and may reduce the rate of postpartum haemorrhage for women receiving the intervention (RR 0.30, 95% CI 0.11 to 0.78; Analysis 2.11).
2.11. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 11 Maternal blood loss > 500 mL.
2.12) Outcome: relaxation
We are uncertain whether manual acupuncture increases relaxation (MD ‐0.90, 95% CI ‐1.62 to ‐0.18, 90 women; Analysis 2.12).
2.12. Analysis.

Comparison 2 Acupuncture versus usual care, Outcome 12 Relaxation.
Subgroup analysis
There were not enough data relating to manual or electro‐acupuncture to demonstrate any differential effect according to type of acupuncture.
3 Acupuncture versus no treatment
One trial of 163 women reported on this comparison. No trial reported on the primary outcomes of: sense of control in labour, satisfaction with childbirth and satisfaction with pain relief.
Primary outcomes
3.1) Outcome: pain intensity
One trial of electro‐acupuncture assessed pain along a VAS scale where a lower score indicated less pain. It is uncertain whether electro‐acupuncture reduces pain intensity compared to the control based on a single trial providing very low‐certainty evidence (MD ‐1.16, 95% CI ‐1.51 to ‐0.81, 163 women, very low‐certainty evidence; Analysis 3.1).
3.1. Analysis.

Comparison 3 Acupuncture versus no treatment, Outcome 1 Pain intensity.
Data were not reported in a form that could be included in the meta‐analysis from the Qu 2007 study. The electro‐acupuncture group reported a lower intensity of pain compared with the control group (26 participants, one trial Qu 2007 study (P = 0.018)).
3.2) Outcome: assisted vaginal birth
It is uncertain whether electro‐acupuncture reduces assisted vaginal birth compared to the control based on a single trial providing very low‐certainty evidence (RR 0.49, 95% CI 0.18 to 1.38, 163 women, very low‐certainty evidence; Analysis 3.2).
3.2. Analysis.

Comparison 3 Acupuncture versus no treatment, Outcome 2 Assisted vaginal birth.
3.3) Outcome: caesarean section
It is uncertain whether electro‐acupuncture reduces caesarean section compared to the control based on a single trial providing very low‐certainty evidence (RR 0.76, 95% CI 0.35 to 1.63, 163 women, very low‐certainty evidence; Analysis 3.3).
3.3. Analysis.

Comparison 3 Acupuncture versus no treatment, Outcome 3 Caesarean section.
4) Acupuncture versus water injection
One trial of manual acupuncture with 128 women reported on this comparison. No trial reported on the primary outcomes of: pain intensity, sense of control in labour, satisfaction with childbirth.
Primary outcomes
4.1) Outcome: satisfaction with pain relief
Data from Martensson 2008 were not included in the meta‐analysis. This study assessed pain along a VAS scale where a lower score indicated less pain. Acupuncture may improve satisfaction with pain relief in labour (MD 18.60, 95% CI 11.54 to 25.66, 128 women).
4.2) Outcome: use of pharmacological analgesia
It is uncertain whether acupuncture reduces the use of pharmacological analgesia because the evidence was based on a single trial of very low‐certainty evidence (RR 0.84, 95% CI 0.54 to 1.30, 1 trial, 128 women, very low‐certainty evidence; Analysis 4.1).
4.1. Analysis.

Comparison 4 Acupuncture versus water injection, Outcome 1 Use of pharmacological analgesia.
4.3) Outcome: assisted vaginal birth
It is uncertain whether acupuncture reduces assisted vaginal birth because the evidence was based on a single trial of very low‐certainty evidence (RR 1.60, 95% CI 0.47 to 5.39, 1 trial, 128 women, very low‐certainty evidence; Analysis 4.2).
4.2. Analysis.

Comparison 4 Acupuncture versus water injection, Outcome 2 Assisted vaginal birth.
4.4) Outcome: caesarean section
It is uncertain whether acupuncture reduces caesarean section because the evidence was based on a single trial of very low certainty (RR 1.33, 95% CI 0.37 to 4.73, 1 trial, 128 women, Analysis 4.3).
4.3. Analysis.

Comparison 4 Acupuncture versus water injection, Outcome 3 Caesarean section.
Secondary outcomes
4.5) Outcome: augmentation with oxytocin
It is uncertain whether acupuncture reduces augmentation because the evidence was based on a single trial of very low‐certainty evidence (RR 1.16, 95% CI 0.85 to 1.58, 1 trial, 128 women; Analysis 4.4).
4.4. Analysis.

Comparison 4 Acupuncture versus water injection, Outcome 4 Augmentation with oxytocin.
4.6) Outcome: relaxation
Relaxation was assessed along a VAS scale where a score of 0 indicated totally relaxed and 100 feeling very tense. Acupuncture may improve women's sense of relaxation (MD 12.60, 95% CI 4.75 to 20.45, 1 trial, 128 women; Analysis 4.5).
4.5. Analysis.

Comparison 4 Acupuncture versus water injection, Outcome 5 Relaxation.
5) Acupressure versus sham control
Seven trials of 547 women reported on this comparison. No trial reported on the primary outcomes of: sense of control in labour, satisfaction with childbirth and satisfaction with pain relief.
Primary outcome
5.1) Outcome: pain intensity
Pain intensity was assessed using a VAS where a low score indicated less pain. We are uncertain if acupressure reduces pain intensity in labour because there was significant heterogeneity and the evidence was assessed as very low certainty (MD ‐1.93, 95% CI ‐3.31 to ‐0.55, 6 trials, 472 women; Analysis 5.1). The heterogeneity may be explained by the timing of the observation of pain at various stages during the first stage of labour.
5.1. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 1 Pain intensity.
5.2) Outcome: use of pharmacological analgesia
Acupressure may make little difference in the use of pharmacological analgesia between groups (RR 0.54, 95% CI 0.20 to 1.43, 1 trial, 75 women, low‐certainty evidence; Analysis 5.2).
5.2. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 2 Use of pharmacological analgesia.
5.3) Outcome: assisted vaginal birth
We are uncertain if acupressure reduces assisted vaginal birth because the evidence was assessed as very low certainty (RR 3.00, 95% CI 0.13 to 71.92, 100 women, 1 trial, very low‐certainty evidence; Analysis 5.3).
5.3. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 3 Assisted vaginal birth.
5.4) Outcome: caesarean section
Acupressure probably reduces the caesarean section rate compared to sham control (RR 0.44, 95% CI 0.27 to 0.71, 4 trials, 313 women, moderate‐certainty evidence; Analysis 5.4).
5.4. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 4 Caesarean section.
5.5) Outcome: Apgar scores less than seven at five minutes
Due to the small number of events we are uncertain if acupressure reduces the Apgar score (RR 0.33, 95% CI 0.01 to 7.99, 220 women, 2 trials; Analysis 5.5). Mafetoni 2016a reported Apgar scores as a mean and standard deviation at one and five minutes and there were no differences between groups.
5.5. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 5 Apgar score < 7 at 5 minutes.
Secondary outcomes
5.6) Length of labour
Acupuressure may reduce the length of labour in the acupressure group (minutes) (SMD ‐0.91, 95% CI ‐1.26 to ‐0.57, 4 trials, 399 women; Analysis 5.6). However, there was significant heterogeneity I2 = 63% and a random‐effects model was applied, which was reduced with the SMD. Data from Mafetoni 2016a were not in a form that could be included in the analysis.
5.6. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 6 Length of labour.
5.7) Outcome: spontaneous vaginal birth
There was no evidence of differences between groups (RR 1.04, 95% CI 0.92 to 1.18, 115 women, 2 trials; Analysis 5.7).
5.7. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 7 Spontaneous vaginal birth.
5.8) Outcome: augmentation with oxytocin
Acupressure may reduce augmentation, although the results were based on only two small trials (RR 0.65, 95% CI 0.46 to 0.91, 135 women, 2 trials; Analysis 5.8).
5.8. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 8 Augmentation with oxytocin.
5.9) Anxiety
Acupressure may reduce anxiety, but again the results were based on only one small trial (MD ‐1.40, 95% CI ‐2.51 to ‐0.29, 1 trial, 75 women; Analysis 5.9).
5.9. Analysis.

Comparison 5 Acupressure versus sham control, Outcome 9 Anxiety.
6) Acupressure versus usual care
Nine trials of 995 women reported data suitable for inclusion in the meta‐analysis. Calik 2014 reported data with medians and mean rank and this was reported narratively. No trial reported on the primary outcomes of: sense of control in labour, satisfaction with childbirth and satisfaction with pain relief.
Primary outcomes
6.1) Outcome: pain intensity
Pain was assessed using a VAS or NRS where a low score indicated less pain. We are uncertain if acupressure reduces pain intensity in labour because the evidence was assessed as very low certainty (SMD ‐1.07, 95% CI ‐1.45 to ‐0.69, 8 trials, 620 women, very low‐certainty evidence; Analysis 6.1). There was significant heterogeneity I2 75% explained by the Ozgoli 2016 trial.
6.1. Analysis.

Comparison 6 Acupressure versus usual care, Outcome 1 Pain intensity.
Calik 2014 recorded pain intensity measures at five time points and found that there were significant differences between the groups in subjective labour pain scores in favour of acupressure at all time points except time point 4 (P < 0.001).
6.2) Outcome: satisfaction with pain relief
Satisfaction was assessed from women's views indicating a score of 0 was not effective to 3 = very effective. We are uncertain if acupressure increases satisfaction with pain relief because the evidence was assessed as very low certainty (MD 1.05, 95% CI 0.75 to 1.35, 1 trial, 105 women, very low‐certainty evidence).
6.3) Outcome: caesarean section
Acupressure may make little difference to caesarean section (RR 0.82, 95% CI 0.54 to 1.23, 4 trials, 391 women, low‐certainty evidence; Analysis 6.3).
6.3. Analysis.

Comparison 6 Acupressure versus usual care, Outcome 3 Caesarean section.
6.4) Apgar scores less than seven at five minutes
Two trials Calik 2014 and Ozgoli 2016 reported data that could not be included in the meta‐analysis.
Secondary outcomes
6.5 Length of labour
Acupressure may make little difference to the length of labour in minutes (MD ‐16.23, 95% CI ‐79.64 to 47.18, 1 trial, 44 women; Analysis 6.4). The data from the Salehian 2011 trial were not included as this reported on the first and second stage of labour only. Data from Calik 2014 were excluded due to the unclear reporting of total duration of labour.
6.4. Analysis.

Comparison 6 Acupressure versus usual care, Outcome 4 Length of labour.
6.6 Spontaneous vaginal birth
Acupressure may make little difference to rates of vaginal birth (RR 1.04, 95% CI 0.90 to 1.21, 3 trials, 220 women; Analysis 6.5).
6.5. Analysis.

Comparison 6 Acupressure versus usual care, Outcome 5 Spontaneous vaginal birth.
6.7 Augmentation with oxytocin
There was no evidence of a difference between groups (RR 2.00, 95% CI 0.39 to 10.31, 1 trial, 15 women; Analysis 6.6).
6.6. Analysis.

Comparison 6 Acupressure versus usual care, Outcome 6 Augmentation with oxytocin.
7) Acupressure versus combined control (placebo and no treatment)
Two trials of 322 women reported on this comparison. No trial reported on the primary outcomes of: sense of control in labour and satisfaction with pain relief.
Primary outcomes
7.1) Outcome: pain intensity
Pain was assessed using a VAS scale where a low score indicated less pain. Acupressure probably slightly reduces the intensity of pain during labour compared with the combined control (SMD ‐0.42, 95% CI ‐0.65 to ‐0.18, 2 trials, 322 women, moderate‐certainty evidence; Analysis 7.1).
7.1. Analysis.

Comparison 7 Acupressure versus combined control, Outcome 1 Pain intensity.
7.2) Outcome: satisfaction with childbirth
Satisfaction was assessed using a VAS scale with a low score indicating very bad and a high score very good. One trial, 212 women reported on this outcome. The results are very low certainty and so we are uncertain whether acupressure has any effect on satisfaction with childbirth (MD 4.80, 95% CI ‐2.25 to 11.85, 1 trial, 212 women; Analysis 7.2).
7.2. Analysis.

Comparison 7 Acupressure versus combined control, Outcome 2 Satisfaction with childbirth.
7.3) Use of pharmacological analgesia
It is uncertain whether acupressure reduces use of pharmacological analgesia because the evidence was based on a single trial of very low certainty (RR 0.94, 95% CI 0.71 to 1.25, 1 trial, 212 women, very low‐certainty evidence; Analysis 7.3).
7.3. Analysis.

Comparison 7 Acupressure versus combined control, Outcome 3 Use of pharmacological analgesia.
7.4) Outcome: assisted vaginal birth
It is uncertain whether acupressure reduces assisted vaginal birth because the evidence was based on a single trial of very low certainty (RR 0.81, 95% CI 0.39 to 1.67, 1 trial, 212 women, very low‐certainty evidence; Analysis 7.4).
7.4. Analysis.

Comparison 7 Acupressure versus combined control, Outcome 4 Assisted vaginal birth.
7.5) Caesarean section
It is uncertain whether acupressure reduces caesarean section because the evidence was based on a single trial of very low certainty (RR 0.48, 95% CI 0.22 to 1.04, 1 trial, 212 women, very low‐certainty evidence; Analysis 7.5).
7.5. Analysis.

Comparison 7 Acupressure versus combined control, Outcome 5 Caesarean section.
Secondary outcomes
7.6) Outcome: augmentation with oxytocin
Acupressure may make little difference to augmentation with oxytocin (RR 1.01, 95% CI 0.77 to 1.31, 1 trial, 212 women, low‐certainty evidence; Analysis 7.6).
7.6. Analysis.

Comparison 7 Acupressure versus combined control, Outcome 6 Augmentation with oxytocin.
Sensitivity analysis
It was proposed to undertake a sensitivity analysis on the results to look at the possible contribution of: (1) differences in methodological quality, with trials of high quality (low risk of bias) compared to all trials; and (2) publication bias by country. This was not done due to the small number of trials overall. There were no trials of high quality; there were also too few trials within comparisons to make comparisons to examine the influence of publication bias. Where there was heterogeneity, we applied a random‐effects model.
Subgroup analysis
We were only able to analyse data according to the subgroup of manual versus electro‐acupuncture, but there were not enough data to demonstrate any differences between these two subgroups. For other pre‐specified subgroups, we did not undertake subgroup analysis, based on insufficient reporting of trials with the variables of interest by outcome.
Discussion
Summary of main results
The review included 28 trials of 3960 women, with data contributing to data and analysis from 27 trials of 3930 women. The evidence suggests a limited benefit from acupuncture and acupressure in relation to the primary outcomes of less intense pain, and increased maternal satisfaction from acupuncture.
Acupuncture compared to sham control
Acupuncture may make little or no difference to the intensity of pain felt by women when compared with sham acupuncture (low‐certainty evidence), but probably increases satisfaction with pain relief and probably reduces the use of pharmacological analgesia (moderate‐certainty evidence). Acupuncture may have no effect on assisted vaginal birth (very low‐certainty evidence), and probably little to no effect on caesarean section (low‐certainty evidence).
Acupuncture compared to usual care
We are uncertain if acupuncture reduces pain intensity compared to usual care. Acupuncture may have little to no effect on satisfaction with pain relief (low‐certainty evidence). We are uncertain if acupuncture reduces the use of pharmacological analgesia (very low‐certainty evidence). Acupuncture probably has little to no effect on assisted vaginal birth (low‐certainty evidence) or caesarean section (low‐certainty evidence).
Acupuncture compared to no treatment
One trial compared acupuncture to no treatment. We are uncertain if acupuncture reduces pain intensity, assisted vaginal birth or caesarean section because the evidence was found to be of very low certainty.
Acupuncture compared to sterile water injection
We are uncertain if acupuncture has any effect on use of pharmacological analgesia, assisted vaginal birth or caesarean section because the evidence was found to be of very low certainty.
Acupressure compared to a sham control
We are uncertain if acupressure reduces pain intensity in labour (very low‐certainty evidence), or assisted vaginal birth (very low‐certainty evidence). Acupressure probably reduces the caesarean section rate compared to sham control (moderate‐certainty evidence). Acupressure may have little to no effect on use of pharmacological analgesia (low‐certainty evidence).
Acupressure compared to usual care
We are uncertain if acupressure reduces pain intensity in labour (very low‐certainty evidence) or increases satisfaction with pain relief (very low‐certainty evidence). Acupressure may have little to no effect on caesarean section (low‐certainty evidence).
Acupressure compared to a combined control
Acupressure probably slightly reduces the intensity of pain during labour group compared with the combined control (moderate‐certainty evidence). We are uncertain if acupressure has any effect on the use of pharmacological analgesia, satisfaction with childbirth, assisted vaginal birth or caesarean section because the certainty of the evidence was all very low.
Currently there are a small number of trials included within each comparison, and this limits the power of the review to detect meaningful differences between groups and analyses, suggesting any limited benefits should be interpreted with caution.
For both primary and secondary outcomes the evidence was moderate to very low certainty using the GRADE framework and the results were heterogenous. Many of the comparisons are characterised as having significant clinical and substantial or considerable statistical heterogeneity. This may relate to the intervention regarding dosing characteristics and the heterogeneity of the controls. Within comparisons we presented data by mode of acupuncture stimulation (manual, electro‐acupuncture). Although the comparisons between acupuncture and the different control groups are not all consistent in their findings, most comparisons suggest a beneficial effect from acupuncture, though the potential for bias exists. Due to small numbers of studies we have been unable to identify treatment‐dose parameters that may moderate and influence the treatment outcomes.
Additional sources of bias have been highlighted throughout the review but the role of participants' expectations and their often unblinded status may also play a role. In trials where there was no blinding, the expectation effects may be greater and contribute a larger placebo effect. The sham controlled trials in this review show an overall small benefit from acupuncture compared with this control, however there is high heterogeneity and different controls may differ in the degree of how inert or credible they are, or whether there is a placebo effect. Addressing this is a priority for future studies.
Overall completeness and applicability of evidence
There remain relatively few trials of acupuncture and acupressure that assess the role of these interventions in the management of pain relief in labour. The completeness and applicability of the evidence is limited from the 28 included trials, with no trial at a low risk of bias on all domains. A weakness of a number of trials continues to be the inclusion of few outcomes and omission of safety clinical outcomes.
Trials recruited low‐risk nulliparous and multiparous women at term, mostly in spontaneous labour. Studies were conducted in different countries and consequently this reflects the different styles of acupuncture administered in the studies. There are many styles of acupuncture, including individualised traditional Chinese medicine, as illustrated by eight trials administering individualised treatment (Borup 2009; Hantoushzadeh 2007; Huang 2008; Martensson 2008; Nesheim 2003; Ramnero 2002; Skilnand 2002; Vixner 2014) and those using standardised acupuncture points as used in the majority of trials in this review. The systematic review documented wide variation in the mode of stimulation, duration of needling, number of points used, depth of needling and duration of the trial. It is unclear how representative the treatment protocols used in the research are generalisable to acupuncture as it is usually practiced. There was insufficient reporting of the rationale of the acupuncture used in the research setting. The variation may also reflect the context in which acupuncture is practiced.
Quality of the evidence
The risk of bias (Figure 2; Figure 3) demonstrates that acupuncture has not been consistently subjected to rigorous study protocols. The quality of reporting was poor in the majority of trials. The risk of bias was mostly low in respect to randomisation. No one trial was rated at a low risk of bias on all domains. Rates of follow‐up were high in the majority of trials with only a small number of trials reporting a small loss of participants. For many studies blinding of participants and the practitioner was not possible, and reporting indicated that the outcomes could have been influenced by a lack of blinding and consequently were rated at a high risk of bias. The small number of studies within comparisons and lack of high‐quality trials suggest there remains insufficient evidence of a consistent treatment effect from acupuncture. We contacted the chief investigators of some studies to provide additional methodological and statistical information; however, we obtained only a few responses (Chung 2003; Huang 2008; Kashanian 2010).
The certainty of evidence was affected by unexplained substantial heterogeneity in some comparisons arising from both the heterogeneity of the clinical interventions and study designs. The small number of studies within comparisons, small samples sizes and lack of high‐quality trials prevented further investigation of the heterogeneity and the impact on treatment effects. The certainty of evidence was downgraded due the high levels of heterogeneity, small studies, and high risk of bias on one or more domains. We were unable to examine the effect of study quality using a sensitivity analysis due to few studies at a low risk of bias. The quality of reporting remains poor in many studies.
The certainty of evidence overall using GRADE was very low to moderate (Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7).
Quality of acupuncture
The quality of acupuncture that was administered was assessed using the newly published 'Reliability of the NICMAN Scale: An Instrument to Assess the Quality of Acupuncture Administered in Clinical Trials' (Smith 2017). All studies of acupuncture were scored on an 11‐point scale that evaluated reported populations and study design, as well as the quality of reporting of the methods of acupuncture used, justification according to texts and evidence, and qualifications of those administering treatment (see Description of studies). The administration of acupuncture in the context of labour pain was assessed as an "acute condition" where few acupuncture treatments would normally be administered. In this context, studies scored high and provided evidence to support the assessment of quality. The rationale for the selection of points was generally well‐justified. However, reporting of details of the acupuncturist delivering the treatment was generally poorly reported and assessed as unclear, or was considered insufficient. The variation in the duration, frequency and selection of acupuncture points suggests that the acupuncture may not have been therapeutically effective and in some cases may not represent best clinical practice.
Potential biases in the review process
We attempted to minimise publication bias. Our search was comprehensive and we included studies identified in languages other than English. However, we cannot rule out the possibility that some studies have been missed. We excluded cross‐over trials from this review owing to lack of clarity regarding the appropriate period of washout for acupuncture trials. Two review authors assessed the eligibility of trials, carried out data extraction and assessed the risk of bias. We are aware that some literature on acupuncture may not be published in mainstream journals and therefore may be excluded from the main databases.
Agreements and disagreements with other studies or reviews
There is one other systematic review of acupuncture to manage pain in labour (Cho 2010) that included trials for which we were unable to ascertain the randomisation details, or we excluded because the trials did not meet the eligibility criteria. Our findings and conclusions concerning the role of acupuncture for pain relief in labour are similar to Cho 2010. Our results differ to those presented in a systematic review of non pharmacological interventions based on endogenous mechanism of action and compared with usual care (Chaillet 2014). This review classified acupuncture and acupressure through a diffuse noxious inhibitory control stimulating an endorphinergic system response. The review detailed different eligibility criteria and direct comparisons can not be made but the review found that acupuncture and acupressure compared to usual care was associated with reduced augmentation of epidural analgesia, labour pain and a better experience with childbirth. A number of clinical trials have been performed to study the efficacy of acupuncture for pain in labour although it remains uncertain whether the existing evidence is rigorous enough to reach a definitive conclusion. In a narrative review of three systematic reviews (Levett 2014), the authors note that the study questions and methods to address these differed, and attention should be paid to the matching of question to study design. Overall, there was evidence of a beneficial effect of acupuncture and acupressure in the systematic reviews in terms of pain scores, use of pharmacological analgesia and satisfaction when appropriate study designs were considered in the context of the clinical question.
Authors' conclusions
Implications for practice.
Acupuncture in comparison to sham acupuncture may increase satisfaction with pain management and reduce use of pharmacological analgesia. Acupressure in comparison to a combined control may reduce pain intensity. However, for other comparisons of acupuncture and acupressure, we are uncertain about the effects on pain intensity and satisfaction with pain relief due to very low‐certainty evidence. Acupuncture may have little to no effect on the rates of caesarean or assisted vaginal birth. Acupressure probably reduces the need for caesarean section. There is a need for further high‐quality research that include sham controls and comparisons with usual care and report on the outcomes of sense of control in labour, satisfaction with the childbirth experience or satisfaction with pain relief.
Implications for research.
Further randomised controlled trials of acupuncture and acupressure for pain management in labour are needed. Further randomised trials should include clinically‐relevant outcomes such as those described in this review. There is a need for improving the quality of future trials to minimise the risk of bias. Our review has indicated significant variation in the dosing of the acupuncture and acupressure administered in the clinical trial. Future research would benefit from greater justification of the treatment regimen being administered and the rationale for the choice in the dosing characteristics of the intervention. Greater compliance with reporting standards of future trials is needed. In particular, consideration should be given in the analysis and reporting on the person providing the intervention: for example, their training, length of experience and relationship to the woman. In addition, further research is required which includes data measuring neonatal outcomes and the effects on analgesia requirements in institutions with and without an 'on demand' epidural service. A cost‐benefit analysis should be incorporated into the design of future studies.
Future studies may need to consider the use of both effectiveness designs using medication, or other forms of usual care, and efficacy designs using placebo controls.
What's new
| Date | Event | Description |
|---|---|---|
| 10 February 2020 | Amended | Corrected typo in the Plain language summary heading. |
History
Protocol first published: Issue 6, 2011 Review first published: Issue 7, 2011
| Date | Event | Description |
|---|---|---|
| 25 February 2019 | New search has been performed | Search identified new studies. A total of 17 new studies included. One previously included study from the last update has been moved to studies awaiting classification (Ziaei 2006). Seven 'Summary of findings' tables have been incorporated. |
| 25 February 2019 | New citation required but conclusions have not changed | Acupuncture and acupressure may be helpful, further research is needed. |
| 1 July 2011 | Amended | We deleted "however, there was significant heterogeneity" from the Results section within the Abstract because, according to Analysis 1.5, assisted vaginal birth, there was no significant heterogeneity. |
Notes
This new review is one of three which, collectively, update the previous review on a range of complementary therapies (Smith 2006). This review includes only trials of acupuncture or acupressure.
Acknowledgements
The review authors would like to acknowledge the Pregnancy and Childbirth team for assistance with the preparation of the original review and its update, including the Information Specialist for assistance in developing the search strategy, the editors, co‐editors and other staff within the team. We also acknowledge the contributions from colleagues with translations in the previous versions of this review including Chinese to English translation assistance provided by Song Mei Wu, and Huijuan Cao for her assistance with seeking clarification from authors in China.
As part of the pre‐publication editorial process, this review has been commented on by four peers (an editor and three referees who are external to the editorial team) and the Group's Statistical Adviser. The authors are grateful to the following peer reviewers for their time and comments: Terje Alraek, Kristiania University College/National Research Center in Complementary and Alternative Medicine, Institute of Health Sciences/Department of Community Medicine, Faculty of Health Sciences, Oslo, Norway/UiT The Arctic University of Norway, Tromsø, Norway; Joanne C Mockler, Monash Health and Monash University, Melbourne, Australia and one other referee.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Appendices
Appendix 1. Search strategies for CENTRAL, MEDLINE and CINAHL
Authors wrote and ran the following searches:
a) Cochrane Central Register of Controlled Trials (the Cochrane Library 2019, Issue 1)
#1 (labor)
#2 (childbirth):ti,ab,kw
#3 (labor):ti,ab,kw or (Childbirth):ti,ab,kw or (pain* manag*):ti,ab,kw or (Pain* labo*r):ti,ab,kw or (contraction*):ti,ab,kw in Clinical Trials
#4 (#1 OR #2 OR #3)
#5 (Acupuncture):ti,ab,kw or (meridian*):ti,ab,kw and (therapy):au
#6 MeSH descriptor Acupuncture explode all trees
#7 MeSH descriptor Acupressure explode all trees
#8 MeSH descriptor Acupressure, this term only
#9 MeSH descriptor Acupuncture, this term only
#10 MeSH descriptor Acupuncture Analgesia, this term only
#11 MeSH descriptor Acupuncture, Ear, this term only
#12 MeSH descriptor Meridians explode all trees
#13 MeSH descriptor Acupuncture Points, this term only
#14 MeSH descriptor Moxibustion, this term only
#15 needling in Clinical Trials
#16 (needling):ti,ab,kw in Clinical Trials
#17 (acu NEXT point*):ti,ab,kw in Clinical Trials
#18 (shu*):ti,ab,kw in Clinical Trials
#19 (acupoint*):ti,ab,kw in Clinical Trials
#20 (shiatsu):ti,ab,kw or (tui na):ti,ab,kw in Clinical Trials
#21 (acupuncture):ti,ab,kw in Clinical Trials
#22 (acupressure):ti,ab,kw in Clinical Trials
#23 (electro NEXT acupuncture):ti,ab,kw in Clinical Trials
#24 (meridian):ti,ab,kw in Clinical Trials
#25(mox*):ti,ab,kw in Clinical Trials
#26 (#5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25)
#27 (#4 AND #26)
b) MEDLINE (1966 to February 2019) – 60 studies identified, 42 not relevant
S17 S4 AND S13 AND S16
S16 S14 OR S15
S15 TI randomised OR TI randomised OR TI randomly
S14 TI randomi*ed controlled trial OR TI controlled clinical trial OR TI trial
S13 S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12
S12 TI needl* OR TI tui na OR TI shiatsu
S11 TI mox* OR TI needling OR TI shu
S10 TI meridian OR TI channel OR TI pathway
S9 (MM "Acupuncture") OR "acupuncture" OR (MM "Acupuncture Therapy+") OR (MM "Acupuncture, Ear") OR (MM "Acupuncture Points") OR (MM "Acupuncture Analgesia")
S8 TI auricular acupuncture OR TI ear acupuncture OR TI acu‐point
S7 TI acupuncture analgesia OR TI acupuncture therapy OR TI acupoint
S6 TI electroacupuncture OR TI electro acupuncture OR TI electro‐acupuncture S5 TI acupuncture OR TI acupressure OR TI acup*
S4 S1 OR S2 OR S3
S3 TI childbirth OR TI child birth OR TI birth
S2 (MM "Labor Pain") OR "labo*r"
S1 TI labo*r OR TI matern* OR TI obstetri*
c) CINAHL (1980 to February 2019) – 41 studies identified, 24 not relevant
S19 S4 AND S5 AND S12
S18 S4 AND S12 AND S16
S17 S4 AND S5 AND S12 AND S16
S16 S13 OR S14 OR S15
S15 TI placebo OR TI placebo* OR TI control*
S14 TI RCT OR TI random* control* trial* OR TI random* allocat*
S13 TI clinical trials OR TI clinical trial* OR TI randomi?ed controlled trial
S12 S6 OR S7 OR S8 OR S9 OR S10 OR S11
S11 TI acu point OR TI acu‐point OR TI acupoint*
S10 TI mox* OR TI needl* OR TI acupoint*
S9 TI pathway OR TI channel therapy
S8 TI meridian OR TI meridian therapy OR TI channel
S7 TI electroacupuncture OR TI electro acupuncture OR TI electro‐acupuncture
S6 TI acup* OR TI acupuncture OR TI acupressure
S5 TI pain manag* OR TI pain* manag* OR TI pain
S4 S1 OR S2 OR S3
S3 TI obstetri* OR TI maternity OR TI mater*
S2 TI childbirth OR TI birth OR TI child birth
S1 TI labour OR TI ( labor and birth ) OR TI labor
Appendix 2. Search methods used for ClinicalTrials.gov and ICTRP
ClinicalTrials.gov
Advanced search
1) Study type: Interventional studies
Intevention/treatment: acupuncture
Condition: labor pain
2) Study type: Interventional studies
Intevention/treatment: acupressure
Condition: labor pain
ICTRP
acupuncture AND labour
acupuncture AND labor
acupressure AND labour
acupressure AND labor
Data and analyses
Comparison 1. Acupuncture versus sham control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain intensity | 2 | 325 | Mean Difference (IV, Random, 95% CI) | ‐4.42 [‐12.94, 4.09] |
| 1.1 Manual acupuncture | 1 | 150 | Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐3.58, 2.98] |
| 1.2 Electro‐acupuncture | 1 | 175 | Mean Difference (IV, Random, 95% CI) | ‐9.0 [‐14.08, ‐3.92] |
| 2 Satisfaction with pain relief in labour | 1 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.38 [1.78, 3.19] |
| 2.1 Manual acupuncture | 1 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.38 [1.78, 3.19] |
| 3 Use of pharmacological analgesia | 2 | 261 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.63, 0.89] |
| 3.1 Manual acupuncture | 2 | 261 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.63, 0.89] |
| 4 Assisted vaginal birth | 2 | 261 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.41, 2.97] |
| 4.1 Manual acupuncture | 2 | 261 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.41, 2.97] |
| 5 Caesarean section | 3 | 411 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.49, 2.48] |
| 5.1 Manual acupuncture | 3 | 411 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.49, 2.48] |
| 6 Apgar score < 7 at 5 minutes | 2 | 261 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.01, 7.79] |
| 6.1 Manual acupuncture | 2 | 261 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.01, 7.79] |
| 7 Length of labour ‐ total | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Electro‐acupuncture | 1 | 175 | Mean Difference (IV, Fixed, 95% CI) | ‐37.41 [‐96.37, 21.55] |
| 8 Spontaneous vaginal birth | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 8.1 Manual acupuncture | 3 | 411 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.86, 1.12] |
| 9 Augmentation with oxytocin | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.1 Manual acupuncture | 2 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
1.6. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 6 Apgar score < 7 at 5 minutes.
1.9. Analysis.

Comparison 1 Acupuncture versus sham control, Outcome 9 Augmentation with oxytocin.
Comparison 2. Acupuncture versus usual care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain intensity | 4 | 495 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.31 [‐2.14, ‐0.49] |
| 1.1 Manual acupuncture | 2 | 270 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.89 [‐2.36, 0.58] |
| 1.2 Electro‐acupuncture | 2 | 225 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.79 [‐3.37, ‐0.21] |
| 2 Satisfaction with pain relief in labour | 2 | 343 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.96, 1.20] |
| 2.1 Manual acupuncture | 2 | 215 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.95, 1.23] |
| 2.2 Electro‐acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.87, 1.30] |
| 3 Use of pharmacological analgesia | 6 | 1059 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.60, 0.85] |
| 3.1 Manual acupuncture | 5 | 884 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.60, 0.82] |
| 3.2 Electro‐acupuncture | 2 | 175 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.01, 8.16] |
| 4 Assisted vaginal birth | 6 | 1217 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.70, 1.24] |
| 4.1 Manual acupuncture | 6 | 1089 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.64, 1.17] |
| 4.2 Electro‐acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.60 [0.64, 4.04] |
| 5 Caesarean section | 5 | 861 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.47, 1.09] |
| 5.1 Manual acupuncture | 4 | 683 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.50, 1.24] |
| 5.2 Electro‐acupuncture | 2 | 178 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.46 [0.16, 1.28] |
| 6 Apgar score < 7 at 5 minutes | 6 | 1061 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.28, 3.47] |
| 6.1 Manual acupuncture | 5 | 883 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.18, 3.10] |
| 6.2 Electro‐acupuncture | 2 | 178 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.39 [0.12, 48.61] |
| 7 Length of labour ‐ total | 3 | 608 | Mean Difference (IV, Fixed, 95% CI) | ‐13.89 [‐28.93, 1.14] |
| 7.1 Manual acupuncture | 1 | 124 | Mean Difference (IV, Fixed, 95% CI) | 4.0 [‐142.47, 150.47] |
| 7.2 Electro‐acupuncture | 3 | 484 | Mean Difference (IV, Fixed, 95% CI) | ‐14.08 [‐29.20, 1.03] |
| 8 Spontaneous vaginal birth | 4 | 449 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.89, 1.08] |
| 8.1 Manual acupuncture | 3 | 271 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.85, 1.10] |
| 8.2 Electro‐acupuncture | 2 | 178 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.86, 1.14] |
| 9 Augmentation with oxytocin | 4 | 813 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.77, 1.02] |
| 9.1 Manual acupuncture | 3 | 635 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.78, 1.09] |
| 9.2 Electro‐acupuncture | 2 | 178 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.59, 1.03] |
| 10 Perineal trauma | 1 | 253 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.19, 1.26] |
| 10.1 Manual acupuncture | 1 | 125 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.13, 1.92] |
| 10.2 Electro‐acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.12, 1.79] |
| 11 Maternal blood loss > 500 mL | 1 | 253 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.11, 0.78] |
| 11.1 Manual acupuncture | 1 | 125 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.40 [0.11, 1.43] |
| 11.2 Electro‐acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.04, 0.93] |
| 12 Relaxation | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 12.1 Manual acupuncture | 1 | 90 | Mean Difference (IV, Fixed, 95% CI) | ‐0.90 [‐1.62, ‐0.18] |
Comparison 3. Acupuncture versus no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain intensity | 1 | 163 | Mean Difference (IV, Fixed, 95% CI) | ‐1.16 [‐1.51, ‐0.81] |
| 1.1 Electro‐acupuncture | 1 | 163 | Mean Difference (IV, Fixed, 95% CI) | ‐1.16 [‐1.51, ‐0.81] |
| 2 Assisted vaginal birth | 1 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.18, 1.38] |
| 2.1 Electro‐acupuncture | 1 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.18, 1.38] |
| 3 Caesarean section | 1 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.35, 1.63] |
| 3.1 Electro‐acupuncture | 1 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.35, 1.63] |
Comparison 4. Acupuncture versus water injection.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Use of pharmacological analgesia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Manual acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.84 [0.54, 1.30] |
| 2 Assisted vaginal birth | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Manual acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.60 [0.47, 5.39] |
| 3 Caesarean section | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Manual acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [0.37, 4.73] |
| 4 Augmentation with oxytocin | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.1 Manual acupuncture | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.16 [0.85, 1.58] |
| 5 Relaxation | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 Manual acupuncture | 1 | 128 | Mean Difference (IV, Fixed, 95% CI) | 12.60 [4.75, 20.45] |
Comparison 5. Acupressure versus sham control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain intensity | 6 | 472 | Mean Difference (IV, Random, 95% CI) | ‐1.93 [‐3.31, ‐0.55] |
| 2 Use of pharmacological analgesia | 1 | 75 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.20, 1.43] |
| 3 Assisted vaginal birth | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.13, 71.92] |
| 4 Caesarean section | 4 | 313 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.44 [0.27, 0.71] |
| 5 Apgar score < 7 at 5 minutes | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.99] |
| 6 Length of labour | 4 | 399 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.91 [‐1.26, ‐0.57] |
| 6.1 Length of labour | 4 | 399 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.91 [‐1.26, ‐0.57] |
| 7 Spontaneous vaginal birth | 2 | 115 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.92, 1.18] |
| 8 Augmentation with oxytocin | 2 | 135 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.46, 0.91] |
| 9 Anxiety | 1 | 75 | Mean Difference (IV, Fixed, 95% CI) | ‐1.40 [‐2.51, ‐0.29] |
Comparison 6. Acupressure versus usual care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain intensity | 8 | 620 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.07 [‐1.45, ‐0.69] |
| 2 Satisfaction with pain relief | 1 | 105 | Mean Difference (IV, Fixed, 95% CI) | 1.05 [0.75, 1.35] |
| 3 Caesarean section | 4 | 391 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.54, 1.23] |
| 4 Length of labour | 1 | 44 | Mean Difference (IV, Random, 95% CI) | ‐16.23 [‐79.64, 47.18] |
| 5 Spontaneous vaginal birth | 3 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.90, 1.21] |
| 6 Augmentation with oxytocin | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.0 [0.39, 10.31] |
6.2. Analysis.

Comparison 6 Acupressure versus usual care, Outcome 2 Satisfaction with pain relief.
Comparison 7. Acupressure versus combined control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain intensity | 2 | 322 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.42 [‐0.65, ‐0.18] |
| 2 Satisfaction with childbirth | 1 | 212 | Mean Difference (IV, Fixed, 95% CI) | 4.80 [‐2.25, 11.85] |
| 3 Use of pharmacological analgesia | 1 | 212 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.71, 1.25] |
| 4 Assisted vaginal birth | 1 | 212 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.39, 1.67] |
| 5 Caesarean section | 1 | 212 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.22, 1.04] |
| 6 Augmentation with oxytocin | 1 | 212 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.77, 1.31] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Borup 2009.
| Methods | Randomised trial of acupuncture, TENS or traditional analgesics. | |
| Participants | 607 healthy, Danish‐speaking women in labour with a normal singleton pregnancy who were giving birth at term (37‐42 completed weeks) and with a fetus in cephalic presentation were eligible for the study. Women were recruited from a university hospital. Women were excluded if they had medical complications, or already received analgesics in labour. | |
| Interventions | Acupuncture group: acupuncture was administered by midwives who had completed a 5‐day course in Western techniques of obstetric acupuncture, and received at least 6 months' clinical training using acupuncture during labour. Treatment was individualised, according to location of pain and woman’s mobility, needles used of 3 depths 0.20 mm x 15 mm, 0.30 mm x 30 mm, 0.35 mm x 50 mm. Duration of needling 30‐120 minutes and could be repeated. Needles removed if woman uncomfortable or if obstetric pathology. Supplementary analgesics provided on request as per control group. Acupuncture points included BL 23, 24, 25, 26, 31‐34, 36, 60, CV20 and sishongong, ear points uterus, shenmen, endocrine, EX‐HN3 yintang, LR3, SP6, SP9, ST36, GB34, HT7, PC6, LI10,11, LU7, LI 4. Control group: traditional analgesics: women randomised to the traditional group could choose among all analgesic methods available (sterile water papules, nitrous oxide, warm tub bath, pethidine, and epidural analgesia). |
|
| Outcomes | Need for pharmacological pain relief, pain intensity, overall experience and satisfaction, duration of labour, use of oxytocin, mode of birth, postpartum haemorrhage, Apgar score, umbilical cord pH. | |
| Notes | Study duration: 1 March 2002 to 29 February 2004. Conflicts of interest: none stated. Employment declared in public health and research institutions. Funding: study sponsored by the Asse and Ejnar Danielsen's Foundation, Kgs, Lyngby, Dnemark; Knowledge and Research Cener for Alternative medicine, Aarhus, Denmark; Sophus Jacobsen Foundation, Capenhagen, Denmar; The Danish Midwifery Organisation, Copenhangen, Denmark; Lundbeck Foundation, Copenhagen, Denmark; Mads Clausens Foundation, Nordborg, Denmark; Hede Nielsen Foundation, Horsens, Denmark; The Research Fund at Aarhus University Hosptial, Aarhus, Denmark; Else and Mogens Wedell‐Wedellsborgs Foundation, Copenhagen, Denmark; and King Christian the 10th Foundation, Copenhagen, Denmark. Setting: maternity hospital. Country: Denmark. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated sequence, with randomisation in a ratio of 2:1. |
| Allocation concealment (selection bias) | Low risk | Central randomisation voice response. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Women, midwife acupuncturists were not blinded to their group allocation. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | It was unclear if the outcome assessor or analyst was blinded to group allocation. Outcomes would be recorded by staff providing care who would be aware of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data were missing from 8%, with the reasons similar between groups: no project midwife available, did not want the allocated treatment, rapid progression of labour, other reasons. |
| Selective reporting (reporting bias) | Unclear risk | The study protocol is not available but the study reports the expected outcomes. |
| Other bias | Low risk | The study appears free of other biases. |
Calik 2014.
| Methods | Parallel randomised controlled trial of 193 women. | |
| Participants | Women who would give birth at full term for the first time (between the 37th and 41st week of pregnancy), had 1 fetus with a weight of 2500 g to 4000 g according to ultrasound, had no pregnancy complications, were able to communicate effectively both orally and in written form, were primary school graduates or more, had no systemic or neurological disorder, had an intact membrane, were in the latent phase of labour (cervical opening 2 cm), had no damage, bruises or irritation at the SP6 acupoint, and had similar obstetric histories and socio‐demographic characteristics. | |
| Interventions | 1. The SP6 acupressure was applied 35 times during uterine contractions, 15 times at 2 cm to 3 cm of cervical dilation, and 10 times each at 5 cm to 6 cm and 8 cm to 9 cm of cervical dilation. Acupressure was applied by placing thumbs on both legs at the same time from the beginning to the end of the contraction. 2. Researcher provided the same care for the control group, but without the use of acupressure. |
|
| Outcomes | Labour pain and time of labour. Subjective pain was measured using the VAS at 5 time points. |
|
| Notes | Study duration: August 2009 to April 2010. Funding: not stated. Conflict of interest: not declared. Setting: maternity hospital. Country: Turkey. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | 2 part block randomisation sequence. |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes used. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Assessors unclear, not reported. Outcomes would be recorded by staff providing care who would be aware of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | High attrition rates. 93 women were excluded from the study for the following reasons: 41 women gave birth by caesarean, 19 had a prolonged labour, 9 developed fetal distress, 7 were taken to the obstetric table without 10 cm dilation or wanted to withdraw from the study, 13 women developed complications, and 4 were administered narcotic analgesics No ITT analysis, and data are not able to be re‐included. |
| Selective reporting (reporting bias) | Unclear risk | Protocol not available and limited outcomes were included in the study. |
| Other bias | Unclear risk | High attrition rates. No ITT. Unclear if researcher was also outcomes assessor. Researcher provided care for both groups. |
Chung 2003.
| Methods | Single‐blind, randomised controlled trial of acupressure, effleurage and a control group. It was not feasible for the participant and therapist to be blind to their group allocation. | |
| Participants | 127 women participated in the trial, during their first stage of labour. Participants needed to be between 37 and 42 weeks pregnant, a low‐risk pregnancy, singleton pregnancy and able to speak Chinese. Women who were induced with oxytocin, or received an epidural block or who planned a caesarean section were excluded from the study. The trial was undertaken in Taiwan; no other details were reported. | |
| Interventions | Trained midwives administered the acupressure to women. The intervention lasted 20 minutes, consisting of 5 minutes pressure to points LI4 and BL67. 5 cycles of acupressure were completed in 5 minutes, with each cycle comprising 10 seconds of sustained pressure and 2 seconds of rest without pressure. A protocol was established to control finger pressure, accuracy of points and accuracy of technique. For the effleurage group, the left and right upper arms were massaged for 10 minutes. In the control group, the midwife stayed with the participant for 20 minutes, taking notes or talking with the participant or family members. | |
| Outcomes | A VAS scale was used to measure the intensity of labour pain. This was administered before and after the intervention. Qualitative data were also collected on women's experience of labour pain 1‐2 hours after delivery. The frequency and intensity of uterine contractions were measured from electronic fetal monitors. | |
| Notes | Study duration: unclear. Funding: unclear. Conflict of interest: unclear. Setting: maternity setting. Country: China There was no power analysis. An ITT analysis was not performed. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Coin tossing. |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | The outcome assessors were blinded to women's group allocation but unclear for analyst. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 23 (18%) women withdrew from the study due to a need for a caesarean section, pain medication. The reason for attrition was similar across groups and due to the need for induction or pain relief. |
| Selective reporting (reporting bias) | Unclear risk | Unclear the study protocol was unavailable and limited outcomes were reported. |
| Other bias | Low risk | No other sources of bias detected. |
Dabiri 2014.
| Methods | 3‐arm parallel randomised controlled trial of 149 women. | |
| Participants | Singleton pregnant women at a gestational age of 37–42 weeks, cephalic presentation, 4 cm to 5 cm cervical dilatation with spontaneous onset of labour, and with no history of previous high‐risk pregnancy, caesarean section, cephalopelvic disproportion, or narcotic use within the past 8 hours were included in the study. | |
| Interventions | 1. In the acupressure group, a trained and registered midwife, certificated in the acupressure method, performed the treatment. Pressure was applied bilaterally within the contraction on Hegu point (LI4), Prior to applying pressure the patient was asked to take a deep breath then a rotational and vibration pressure was applied for 60 seconds, she then received a 60‐second rest, and pressure was repeated. This cycle continued for 30 minutes. Accurate location of the acupoint was confirmed when the participants felt heaviness, pressure, tingling, or numbness in the area or a pleasant feeling. If the participant reported feeling severe pain at the site of pressure, the pressure was stopped temporarily and commenced after a few minutes. The sign of the intensity of the pressure was partial discolouration of the nail bed to white 2. In the touching group, the same point was touched but with no pressure applied. The 30‐minute intervention time used is based on acupressure theory, which says the time needed to turn the energy in the body’s energy circuits is about 24 minutes. 3. Control. Received usual care |
|
| Outcomes | Pain intensity was measured using the VAS. Pain intensity was measured before and several times after the intervention at 30 minutes, 1 hour and every hour after intervention until the end of first stage of labour. |
|
| Notes | Study duration: October 2011 to April 2012. Funding: not stated. Conflict of interest: authors declared there are no conflicts of interest. Setting: maternity setting. Country: Iran. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Lot drawing. |
| Allocation concealment (selection bias) | Low risk | Concealed in envelope. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Control group received placebo, usual care not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Author clarification that outcome assessor was blinded to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Incomplete data accounted for. ITT analysis included. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available and limited relevant outcomes were reported. |
| Other bias | Unclear risk | Insufficient information to report. |
Dong 2015.
| Methods | 3‐arm parallel randomised controlled trial of 180 women. | |
| Participants | Women aged 20‐25, with a planned vaginal delivery, singleton pregnancy, 37‐42 weeks gestational age, fetus in vertex presentation, no obstetric or non‐obstetric complications, cervical dilation greater than or equal to 3 cm with regular contractions. | |
| Interventions | 2 experimental groups, 1 control: 1. EX‐B2, 2. SP6, 3. Control. An electro‐acupuncture device (HANS‐100B, China) provides electrical current with intensity range from 5 to 40 mA. The frequency of 100 Hz with a burst frequency of 2 Hz (dense‐dispersed waveform), pulse duration of 0.5 ms (ms) was used. In this study, the intensity of the current was set at 15 mA at the starting point of the active phase of labour and can be adjusted to higher intensity upon request. The device was run by experienced midwives who had been adequately trained in acupuncture before the study. 1. In EX‐B2 (Appointed Jiaji acupoints, approximately 1.7 cm lateral to the posterior median line, from tenth thoracic vertebral to third lumbar vertebral) group, 2 electrodes which connected to the device were attached on the bilateral EX‐B2 acupoints. 2. In SP6 (Sanyinjiao acupoints, 5 cm above medial malleolus in lower leg) group, 2 electrodes were attached on SP6 acupoints of both legs. 3. Routine intrapartum care |
|
| Outcomes | Primary: VAS: 0 cm to 10 cm scale. VAS scores were recorded during the last contraction before the intervention and then 30, 60, 120 minutes after the intervention in active phase of labour by the same trained midwife. VAS scores decreased > 3 at the last VAS measurement was considered effective. Secondary: duration of labour – active, second and third phases, oxytocin use, neonatal birthweight, Apgar scores 1 and 5 minutes. |
|
| Notes | Study duration: October 2012 to September 2013. Funding: not stated. Conflict of interest: authors state there is no conflicts of interest. Setting: maternity hospital. Country: China. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | By lottery method. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes assessor was treating clinician. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Describes attrition of participants. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available and limited study outcomes were reported. |
| Other bias | Unclear risk | Not sufficient information reported. |
Hamidzadeh 2012.
| Methods | Single‐blind placebo‐controlled trial of 120 women. | |
| Participants | Women have their 1st to 3rd pregnancy, no addiction to drugs, reading and writing literacy, > 37 weeks’ gestation, natural pregnancy, singleton, cephalic presentation, anterior position, spontaneous onset of labour, cervical dilation between 3 cm to 5 cm, 20‐40 years of age, no experience of acupressure, not damage, bruises, sensitivity or irritation at LI4 acupoint, no prior caesarean birth. | |
| Interventions | 1. At the beginning of the active phase of labour (3 cm to 4 cm dilatation of cervix with regular uterine contractions), women in the acupressure group (n = 50) received LI4 acupressure at the onset of the active phase for the duration of each uterine contraction over a period of 20 minutes. At onset of active phase of labour, women in acupressure group received simultaneous acupressure on both hands. 5 pressures on LI4 were applied per minute. Each period included 10 seconds of pressure and 2 seconds of rest. Done during each uterine contraction over a 20‐minute period. The ‘effect’ was confirmed by a feeling by the woman of warmth, weight, swelling and numbness. 2. Women in the control group received a touch on LI4 acupressure point without massage. |
|
| Outcomes | Labour pain was measured using the VAS before the intervention, immediately after the intervention, 20 and 60 minutes after, and then every subsequent hour until birth. Satisfaction with labour. Mode of birth. | |
| Notes | Study duration: September 2006 to December 2006. Funding: not stated. Conflict of interest: authors state there are no conflicts of interests. Setting: maternity hospital. Country: Iran. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified randomisation with a block size of 2. Stratified for nulliparous and multiparous women to select 50% each. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Imcomplete data addressed. |
| Selective reporting (reporting bias) | Unclear risk | No trial protocol available. Limited study outcomes were reported. |
| Other bias | Unclear risk | Trial seems free of other biases. |
Hamlaci 2017.
| Methods | Parallel randomised controlled trial of 44 women. | |
| Participants | Pregnant women between 37 and 40 weeks of gestation by ultrasonography, singleton pregnancy, fetal weight of 2500 g to 4000 g according to ultrasonography, had no complications during pregnancy (threatened abortion, hyperemesis gravidarum, etc), had no systemic diseases during pregnancy (gestational diabetes, hypertension, heart disease, etc), spontaneous onset of labour, cervical dilation less than 5 cm, and had planned a vaginal delivery. | |
| Interventions | 1. Study group: Point LI‐4 was located, then acupressure was applied when cervical dilatation reached 4 cm to 5 cm and again when dilation reached 7 cm to 8 cm. In the first and second applications, acupressure was applied to acupoint LI‐4 on both hands at the same time from the beginning to the end of the contraction. Acupressure was applied 16 times during uterine contraction, 8 times at 4 cm to 5 cm of cervical dilatation and 8 times at 7 cm to 8 cm cervical dilatation. Acupressure was applied by placing thumbs on both hands. The mean pressure applied was approximately 3 kg to 5 kg, and this amount was ascertained by the researcher. The first application took approximately 1 hour. The second application took 30 minutes. Acupressure was applied by the researcher in the pregnant woman’s room during labour. It was applied in the active phase of the birth and in the periods of increased labour pain intensity as the most important time for pain management. 2. Control group: pregnant women were given no acupressure or treatment other than routine care. Except for the acupressure practice given to the acupressure group, the researcher gave the participants in both groups equal care throughout the labour. |
|
| Outcomes | Pain as measured by VAS. | |
| Notes | Study duration: 1 June 2012 to 30 September 2012. Funding: not stated. Conflict of interest: authors state there are no conflicts of interest. Setting: maternity hospital. Country: Turkey. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Lottery method used. |
| Allocation concealment (selection bias) | Low risk | Sealed envelope. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Researcher also performed outcome assessment. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All outcome data accounted for. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available. Limited study outcomes were reported. |
| Other bias | Low risk | Nil. |
Hantoushzadeh 2007.
| Methods | Single‐blind randomised controlled trial of acupuncture versus placebo acupuncture using sham needling. Duation: February to September 2005. Setting: government general hospital, Tehran, Iran. |
|
| Participants | 150 women with a singleton pregnancy, at term (37 weeks), nulliparous, parturient and in spontaneous active labour. Exclusion criteria: presence of medical or surgical disease, indication for caesarean section, pace‐maker, emphysema, history of anticoagulation, HIV, HCV or HBV infection, pregnancy‐related complications, e.g. chorioamnionitis, placental abruption, placenta praevia and pre‐eclampsia/eclampsia, cervical dilation > 6 cm. | |
| Interventions | The study group received acupuncture administered by the study investigator, who was trained to practice acupuncture. Points were selected bilaterally according to parturient symptoms, and needles were inserted at 45 degree or perpendicularly with a depth that depended on the thickness of the subcutaneous fat. The selection of points was done according to acupuncture principles and was subject to variation from patient to patient. Needles were manually stimulated until the de chi sensation (sensation of warmth, numbness, tingling, or heaviness) was achieved. The needles were not taped and were removed either when delivery occurred or the patient herself asked to do so or when the effect terminated or there was no effect. The following points and there indication were reported as follows: LI4‐ analgesia, BL32‐back pain, BL60 back pain, SP6 severe pain during contractions, ST36 general pain, LR3 analgesia, GB34 cervical rigidity, HT7 anxiety, nervousness. The control group received minimal acupuncture which involved insertion of acupuncture needles away from true acupuncture points. Participants were not asked about de qi and the needles were manually stimulated for about 20 minutes. Both groups received care from health providers, routine analgesia was not available. |
|
| Outcomes | Pain scores measured using VAS scale 0‐100, at beginning, 30 minutes, 60 minutes, 120 minutes, then every hour until end of labour. Duration of active labour, amount of oxytocin used, vaginal birth, birthweight, Apgar score at 1 minute, acceptability of acupuncture. |
|
| Notes | Study duration: February 2005 to September 2005. Funding: Vali Asr Research Centre for Reproductive Health. Conflict of interest: not stated. Setting: maternity hospital. Country: Iran. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Partcipants blinded to group allocation (assessment of intact blinding not reported), administering clinician unblinded, care provider unclear. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5 losses in the acupuncture group: 3 caesarean section, 2 labour stopped. 1 loss in the control group caesarean section. No ITT. |
| Selective reporting (reporting bias) | Unclear risk | Protocol not available. |
| Other bias | High risk | Partcipants in the control group had significantly lower pain scores before intervention commenced. |
Hjelmstedt 2010.
| Methods | Parallel randomised controlled trial of acupressure compared with light touch or standard care. | |
| Participants | Public hospital in Trivandrum, India. 212 women randomised to the trial. Inclusion criteria: nulliparous, transferred to labour room, dilation 3 cm to 7 cm, healthy, uncomplicated pregnancy, term, live fetus, cephalic presentation. Exclusion criteria: hypertensive disorder, pre‐eclampsia, diabetes, neuropathic pain, multiparous, intrauterine death, multiple fetuses, breech presentation, gestation < 38 or > 42 weeks, dilation < 3 cm or > 7 cm, elective caesarean section, presence of pharmacological pain relief. |
|
| Interventions | Group 1: acupressure at acupoint SP6 bilaterally during contractions over a 30‐minute period. Treatment was not repeated after 2 hours if the woman was not in second stage or had not delivered. Intensity of pressure adapted to each woman's pain threshold. Group 2: (TG) receive light touch at SP6 bilaterally during contractions. Group 3: (SCG) standard care. Acupressure and touch was delivered by same person who had undergone 3 days of training by a certified acupressure therapist. |
|
| Outcomes | Participant’s self‐assessment of in‐labour pain via VAS pain scores, oxytocin augmentation, pharmacological pain relief, caesarean section, mode of birth, episiotomy, birthweight, birth length, Apgar (5 minutes). Retrospective ratings of labour pain, coping with labour pain and experience of childbirth. | |
| Notes | Trial duration: 1 September 2007 to 30 April 2008. Funding: Osher Center for Integrative Medicine, Karolinska Institutet and the Centre for Health Care Science, Karolinska Institutet. Conflict of interest: the authors state there are no conflicts of interest. Setting: maternity hospital. Country: India. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelope. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | It was unclear if the participant was blinded to light touch or acupressure, the clinician was not blinded to group allocation. It would have been and obvious to an observer.re the group 3. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The outcome assessor was blinded to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 women withdrew from the standard care group. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol unavailable. |
| Other bias | High risk | Baseline pain scores were significantly different between APG and SCG, and boarding on significance between APG and TG. Therefore scores were not used for a between group comparison, but were used for a within‐group comparison over time. |
Huang 2008.
| Methods | Single‐blind randomised controlled trial, 4‐arm study: 1) electro‐acupuncture group N = 82; TENS group N = 82; control group (breathing) N = 81; spinal‐epidural analgesia group N = 79. Unit of randomisation: 1:1:1:1. |
|
| Participants | Inclusion criteria: 324 primiparae women aged 22‐34 years, vaginal delivery, monocyesis, not cephalopelvic disproportion, no abnormal fetal position, no serious complications of pregnancy, agreement to labour analgesia. Exclusion criteria: not explicitly stated. |
|
| Interventions | 1) Electro‐acupuncture. Shi diagnosis labour pain mainly located in the lumbosacral and with bearing‐down sensation, sturdy body, desiring cold and fearing of warmth, good appetite, normal or dry stool, normal or less yellow urine, good sleep, normal red tongue with thin and whitish or slightly thicker tongue coating, wiry, drooling and strong pulse. Xu diagnosis: labour pain mainly located in the lower abdomen and distending, weak body, seeking warmth and fearing of cold, poor appetite, loose stool, clear abundant urine, increased nocturnal enuresis, worse sleep, easily waken up in the night, fatty and whitish tongue with teeth mark, thicken and greasy coating, deep and thin, weak pulse. Electro‐acupuncture group applied self‐developed acusector on selected acupoints according to syndrome differentiation, and needling and galvanism were combined on the acupoints. Main acupoints were ST36, CV3 and CV4. Additional points for Shi were BL32 and LR3) and for Xu were LI4 and SP6. Radio frequency electrodes (self‐developed, putting auricular needle in the centre of electrode plate with thumb‐tack needle) were inserted and connected to Han's acupoint nerve stimulator. Dilatational wave of 2Hz/100 Hz operated as a stimulator and the strength adjusted to the woman's tolerance level. 2) TENS group used Han's acupoint nerve stimulator and stimulated point with 2/100 Hz of dilatational wave. 3) Spinal‐epidural analgesia group received combined spinal and epidural block anaesthesia. 4) Advice on breathing during contraction and local massage during severe pain. |
|
| Outcomes | VAS scores of pain applied at pre‐pain, 30 minutes, 60 minutes, 120 minutes after pain analgesia, at the end of active stage (cervical dilation of 7 cm to 8 cm), complete dilation of cervix, second stage of labour, third stage of labour and 1 day after labour. 0‐no pain, 1‐mild pain, 10‐most severe and intolerable pain. Degree of satisfaction to labour analgesia 2 hours after delivery. Satisfied: pain completely relieved without evident discomfort. Relatively satisfied: pain relieved to some extent without evident discomfort. Unsatisfied: pain not relieved with evident discomfort. Mode of birth, maternal and labour complications. |
|
| Notes | Trial duration: April 2004 to February 2005. Funding: National Traditional Chinese Medicine Administration of Traditional Chinese Medicine Science and Techology Research Special TCM Clinical Research Fund (04‐05LQ04). Conflict of interest: not stated. Setting: delivery unit at the Beijing Gynaecology and Obstetrics Hospital. Country: China. Data from electro‐acupuncture and groups 3 and 4 were combined. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Unclear risk | No details reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No participant loss. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol unavailable. |
| Other bias | Unclear risk | Insufficient reporting. |
Kashanian 2010.
| Methods | Single‐blind randomised controlled trial of acupressure at SP6 or light touch control group. | |
| Participants | 120 women. Inclusion criteria: age: 18‐35 years, nulliparous, singleton, cephalic presentation, gestational age 37‐41 weeks, intact membranes, cervical dilation 3 cm to 4 cm, established contractions (> 3:10 minutes 45‐60 seconds duration). Exclusion criteria: any sedation during labour, abnormal or deceased fetus, fetal distress, meconium passage, previous hysterotomy or uterine scar, any medical or surgical complications of pregnancy, drug use except usual supplements, vaginal bleeding and high‐risk pregnancy. |
|
| Interventions | Acupressure, performed by investigator, at SP6 during contractions for a total acupressure time of 30 minutes. Control: touch at SP6, performed by same investigator, for same duration of time. |
|
| Outcomes | Severity of pain as measured by VAS, duration of active phase of labour, mode of birth, use of oxytocin, neonatal weight, and Apgar scores. | |
| Notes | Study duration: March to September 2007. Funding: the research was supported by Iran University. Conflict of interest: not stated. Setting: labour ward at Akbaradi teaching hospital, Iran. Country: Iran. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | 4 part block randomisation method (seems to be computer generated). |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | It was possible to blind participants. Treatment was known and administered by the investigator. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor was blinded to treatment group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No discussion of loss of participants at data collection points. No discussion of exclusions after randomisation but exclusion criteria of any sedation during labour or any sign of fetal distress could indicate exclusion after randomisation. |
| Selective reporting (reporting bias) | Unclear risk | The study protocol was unavailable. |
| Other bias | Low risk | No imbalances at randomisation. |
Kordi 2010.
| Methods | 3‐arm parallel randomised controlled trial of 83 women. | |
| Participants | Women with a gestational age between 38‐42 weeks, single fetus, cephalic presentation, intact membranes, lack of medical and midwifery diseases, cervical dilatation 3 cm to 4 cm. | |
| Interventions | 1. Acupressure at LI4 2. Touch at LI4 3. Usual care No further details available from translation. |
|
| Outcomes | VAS scale measuring intensity of labour pain (immediately, 30 minutes, 1 and 2 hours after the intervention during the first stage of labour), duration of uterine contractions (immediately, 30 minutes, 1, 2, 3 and 4 hours after the intervention). | |
| Notes | Study duration: not stated in translated data extraction. Funding: not stated in translated data extraction. Conflict of interest: not stated in translated data extraction. Setting: Omolbanin Maternity hospital Mashhad, Iran. Country: Iran. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were blinded. Personnel were not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessors were not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not described. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available. Limited relevant study outcomes were reported. |
| Other bias | Unclear risk | Unclear. |
Lee 2004.
| Methods | Single‐blind, randomised controlled trial of acupressure or touch control. | |
| Participants | 89 women were randomly allocated to the trial. Inclusion criteria for the study were: greater than 37 weeks pregnant, singleton pregnancy, planning a vaginal delivery and in good health. Women were recruited to the study from publicity materials in the outpatient department of a general hospital in Korea. | |
| Interventions | Women allocated to the intervention group received acupressure at SP6, or to the control group touch at SP6. The acupressure involved pressure at SP6 on both legs during a contraction during a 30‐minute time period during each contraction. The pressure applied was 2150 mmHg. The control group received touch with no pressure from the thumbs. | |
| Outcomes | Pain was measured along a VAS and assessed at entry, before the intervention was administered, after the intervention, and 30 and 60 minutes after the intervention. Other outcomes included duration of labour, use of pain relief, and maternal anxiety. | |
| Notes | Study duration: May 2002 to September 2002. Funding: not stated. Conflict of interest: not stated. Setting: delivery suite at a University Hospital. Country: Korea. No power analysis was reported. An ITT analysis was performed. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomisation sequence was generated from random‐number tables. |
| Allocation concealment (selection bias) | Unclear risk | Unclear. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The participants were blinded to group allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were blinded to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 14 (15%) women did not complete the study. Reasons given were caesarean section, withdrawal or incomplete data. No information was reported by group allocation. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol unavailable. All pre‐specified outcomes were reported. |
| Other bias | Low risk | No other bias detected. |
Ma 2011.
| Methods | 3‐arm placebo‐controlled randomised trial. | |
| Participants | 350 women in labour, aged 24 to 35 years old, with gestational age 38 to 41 completed weeks, who have had a trial labour indication, have never had prior acupuncture treatment, and have regular uterine contraction, cervical dilatation 2 cm to 3 cm and head presentation labour score > 10 were included. | |
| Interventions | Randomly assigned to receive 1. electroacupuncture (EA), 2. sham EA or 3. no acupuncture. Acupuncture was conducted at the end of the latency period of the first labour stage in all participants, when the dilatation of cervix was at 3 cm. Experimental intervention: EA: women received the electroacupuncture at the 1 acupoint, Sanyinjiao (SP6), at the end of the latent phase of the first labour stage (cervical dilation 2 cm to 4 cm). The inserted needle was stimulated with make‐and‐break waves (dense wave at 4Hz and disperse wave at 20Hz) and left for 30 minutes. Analgesia and safety indices were observed at 7 time points including before needle, needle retention for 15 minutes and 30 minutes, 1, 2, 3 and 4 hours after needle withdrawal. Oxytocin was administered when indicated during labour. Caesarean section was performed as needed based on the patient’s labour progression. Control/Comparison intervention: sham EA and no acupuncture. Sham EA: the procedure was identical to that used in the acupuncture group but without needle insertion into the skin. The needle operations were conducted out of the patient’s visual field. The electroacupuncture apparatus was within sight of the parturients, and the blinking of display lamp in the apparatus could lead parturients to believe that they were receiving electroacupuncture. A post‐examination was conducted for the patients blinding by asking whether they received the acupuncture. No acupuncture: for the control group, parturients were treated as regular parturients in labour. |
|
| Outcomes | Self‐rated analgesic effect (VAS: 0‐100). The duration and paralysis time of uterine contraction, uterine contraction regularity, degree of cervical extension, presentation of fetal descent, the condition of intrapartum haemorrhage and postpartum haemorrhage, labour manner, lochia, involution of uterus, milk secretion, neonate Apgar score and neonate body height and weight. | |
| Notes | Study duration: not stated. Funding: State Administration of Traditional Chinese Medicine; National Science Foundation of China; and E‐institutes of Shanghai Municipal Education Commission. Conflict of interest: authors state there are no conflicts of interest. Setting: maternity hospital. Country: China. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Unclear risk | Did not describe. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Does not describe. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Does not describe. |
| Selective reporting (reporting bias) | Unclear risk | No protocol provided. |
| Other bias | Unclear risk | No baseline imbalances. |
Mackenzie 2011.
| Methods | 4‐arm, single‐blind, placebo‐controlled randomised trial. | |
| Participants | Study reports on participants undergoing a medical induction of labour. 105 nulliparous, singleton pregnancy, fetal cephalic presentation, intact membranes, undergoing labour induction using vaginal prostaglandins, low amniotomy for prolonged gestation or mild hypertension. All groups: subsequent pain management including aromatherapy, TENS and parenteral opioids, and regional blockade was provided when requested or recommended by the attending midwife or obstetrician. |
|
| Interventions |
Experimental intervention Manual acupuncture – needles stimulated by hand for 30 minutes. Electro‐acupuncture – needles attached to an electrical stimulator and stimulated for 30 minutes. Commenced in both groups after medical induction initiated but before painful contractions started. Acupuncture provided by qualified registered acupuncturists. Needles inserted intramuscularly to depth of 15‐20 mm until unusual sensation (de qi) developed, needles remained inserted for 30‐60 minutes. Points used: LI 4, SP6, BL60 and BL67. Control/Comparison intervention Sham acupuncture – manual and electro 1:1 ratio – acupuncture stimulation not provided. Needles inserted adjacent to the specific acupuncture site – insufficient to provoke de qi sensation. Sham manual received no stimulation, sham electro were connected to the electrical stimulator but current not activated. Usual intrapartum care. |
|
| Outcomes | Primary outcome: rate of intrapartum epidural anaesthesia. Secondary outcomes: parenteral analgesia requirement, duration of labour, mode of birth, neonatal condition, postpartum haemorrhage. | |
| Notes | Study duration: August 2005 to February 2009. Funding: supported by a grant from the Oxfordshire Health Services Research Committee and the Uterine Contractility Trust fund, held by the Oxford Radcliffe NHS Trust. Conflict of interest: authors state there are no conflicts of interest, except 1 author (IM) who provides legal opinion in litigation cases at the request of claimants and defendants. Setting: John Radcliffe Hospital. Country: UK. Manual and electro‐acupuncture were combined in the analysis due to the reporting of data in the manuscript for some outcomes. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers. Variable block sizes used. |
| Allocation concealment (selection bias) | Low risk | Allocation concealment by sealed opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants blinded in 2 groups, except for the usual care group. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Does not describe. |
| Selective reporting (reporting bias) | Unclear risk | No published protocol. |
| Other bias | Low risk | No baseline imbalances. |
Mafetoni 2016.
| Methods | 3‐arm randomised controlled single‐blind pragmatic trial. | |
| Participants | Women of any age and parity, from 37 weeks' gestation, in spontaneous, induced, and/or augmented labour and > 4 cm dilated, 2‐3 contractions every 10 minutes, with undamaged skin at the bilateral SP6 point, fetus in cephalic vertex position with good vital signs. | |
| Interventions | Randomised to: 1. Acupressure SP6 (SP6) 2. Touch group ‐ touch at SP6 3. Placebo and control group (CG) |
|
| Outcomes | Pain intensity measured using VAS Caesarean section Length of labour |
|
| Notes | Study duration: January 2013 to August 2013. Funding: not stated. Conflict of interest: not stated. Setting: tertiary teaching hospital in Sao Paulo, Brazil. Country: Brazil. Data from groups 1 and 2 included in the analysis. Data from group 3 unclear from translation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Women were allocated through a computer‐generated sequential list of random numbers in blocks of 6, and participants were distributed in 3 groups. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participant in SP6G and TG were blinded. Participants in CG not blinded due to nature of trial. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor was also blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No losses to follow‐up. Analysis was ITT. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available, limited relevant study outcomes were reported. |
| Other bias | Unclear risk | Baseline imbalance between SP6 group and control group with mean number of pregnancies (P = 0.02). |
Mafetoni 2016a.
| Methods | 3‐ arm randomised controlled trial | |
| Participants | 30 women. Inclusion criteria: any parity, from 37 weeks' gestation, in spontaneous, induced, and/or augmented labour with dilation > 4 cm dilated, 2 or more contractions every 10 minutes, with intact skin in the auricle pavilion, with a living fetus in cephalic presentation with good vital signs. Exclusion criteria: dilation > 7 cm, severe pre‐eclampsia, placenta previa, previous caesarean section, immediate indication for caesarean section. |
|
| Interventions | Auriculotherapy with crystal beads on ear points Shenmen, uterus point, neurasthenia and endocrine point pressed for 1 minute. Control groups Auiculotherapy with glass beads placebo not manipulated Control group |
|
| Outcomes | Pain intensity measured on a VAS scale Caesarean section Apgar score at 1 and 5 minutes Length of labour Augmentation with oxytocin |
|
| Notes | Study duration April 2015 to August 2015 Funding: not reported. Conflict of interest: not reported Setting: tertiary teaching hospital Sao Paulo Country: Brazil |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | List of random numbers stated but method not stated. |
| Allocation concealment (selection bias) | Low risk | Opaque sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Treatment and placebo group blinded, control group not blind to group allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assesor was blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 10 women withdrawn whose delivery took place prior to last observation, 3 in treatment, 5 placebo and 2 control group. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available |
| Other bias | Low risk | No baseline differences. |
Mansouri 2018.
| Methods | 3‐armed randomised controlled trial of 165 randomised women | |
| Participants | Inclusion criteria: primiparous, gestational age ≥ 37 weeks, age of 18‐35 years, singleton fetus with vertex presentation, fetal weight of 2500 g to 4000 g, spontaneous vaginal delivery (4 cm to 5 cm cervical dilatation with at least 2 contractions of 20 seconds and more within 10 minutes), healthy skin in the pressure areas, no history of medical and obstetric problems, and pain intensity ≥ 50 mm based on VAS on admission. Exclusion criteria: 1) using any analgesics, 2) fast delivery, 3) emergency caesarean section, 4) abnormal fetal heartbeat, 5) lack of progress, and 6) unwillingness of the mother to continue participating in the study. |
|
| Interventions | Group 1 Acupressure on bladder points of BL5, BL8, BL9, and GV20. For the first stage of labor, simultaneous with the beginning of uterine contraction the parturient was placed in a semi‐sitting position with the head in body alignment. The researcher placed over the head of parturient and applied a fixed pressure with a thumb for 60 seconds on each of the BL5, BL8, BL9, and GV20 points. Therefore, the parturient felt the tai chi (heaviness, pressure, hotness, tingling, or numbness) at these points. The pressure was completed within 5 4‐minute cycles (i.e. total of 20 minutes) with intervals of 30 minutes. After the first stage of labour (10 cm cervical dilatation), a four‐minute pressure cycle was resumed on the points at the beginning of the second stage of labour (maternal exiting). Group 2 Pressure on gallbladder points of GB8, GB16, GB17, GB18, and GV20 60 sec of pressure was applied on each of the 5 GB8, GB16, GB17, GB18, and GV20 points (5‐min cycle) with the onset of uterine contraction in the first stage of labour. The pressure was carried out as 4 5‐minute cycles with 30‐minute intervals making a total of 20 minutes pressure. At the beginning of the second stage of labor, 60 seconds of pressure was applied to the points (5‐minute cycle). Group 3 Routine care unspecified. |
|
| Outcomes | VAS scale. | |
| Notes | Study duration May 2017 to November 2017 Funding: study formed part of a Masters Thesis. Conflict of interest: authors declare there are no conflicts of interest. Setting: Um Al‐Benin Specialized Women's Hospital, Mashad Country: Iran The 2 acupressure groups were combined in the analysis. Data reported at the end of second stage of labour when intervention finished |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Women allocate to the 3 groups through random allocation. ‘The first three participants were asked to take the papers randomly. Afterwards, the order of first three people was repeated for the rest of the participants’ |
| Allocation concealment (selection bias) | Low risk | Concealed in an envelope |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Similar pressure was applied to the 2 intervention groups. Women on the control group unblinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Binded research assistant collected outcome data. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 12 women were excluded from the analysis. 7 women in the intervention group stopped receiving the acupressure, 3 women had hypertonic contractions, 1 women had fetal distress and 1 women a lack of progress. Control group 1 women stopped receiving the intervention, one received narcotic pain relief. |
| Selective reporting (reporting bias) | Unclear risk | No reference to a protocol, limited study outcomes reported. |
| Other bias | Low risk | No imbalance at randomisation. |
Martensson 2008.
| Methods | Randomised controlled trial of acupuncture compared with sterile water injections. | |
| Participants | 128 women. Inclusion criteria were: 37‐42 weeks' gestation, spontaneous onset of labour, frequency of 3 contractions during 10 minutes and a requirement for pain relief. Exclusion criteria were: no opoid analgesics, acupuncture, TENS, or sterile water injection in the previous 10 hours, or had received paracervical nerve block, epidural or intrathecal analgesia or augmentation of labour. | |
| Interventions | Acupuncture group: all women were treated at GV20, LI4 and SP6. Local acupuncture points were selected individually depending on where the pain was perceived; the midwives could choose 4 to 7 points from BL23‐24, BL54, EX19, GB25‐29 and KI11. The acupuncture points were chosen both from recommendations in the literature and in cooperation with the midwives, the latter in an attempt to imitate normal clinical practice. The needles (Hegu AB, Landsbro, Sweden) were made of stainless steel (0.3030 or 0.3550 mm). After insertion, the needles were stimulated to evoke needle sensation (De Qi), a feeling of heaviness, numbness and distension, reflecting activation of muscle‐nerve afferents. The needles were left in place for 40 minutes, and were stimulated manually, as described, every 10 minutes. The first assessment after treatment took place 30 minutes after all the needles were in place. The treatment was repeated if necessary. Water injection group was given 48 subcutaneous injections of 0.5 mL sterile water. The injections were administered in the area where the woman felt pain; the injections could be repeated if necessary. A 2‐mL plastic syringe (B. Braun Omnifix†) with a thin needle (B. Braun Omnifix†; diameter: 0.40 mm, length: 20 mm) was used. The injections were administered during a contraction. The first assessment after treatment took place 30 minutes after all the injections were given. 40 midwives administered acupuncture and/or injections of sterile water. All midwives were equally trained in administration of acupuncture and injection of sterile water. All protocols were thoroughly standardised. |
|
| Outcomes | Pain and relaxation was assessed using a VAS immediately before and 30, 60, 90, 120, 150 and 180 minutes after treatment. The woman was asked to mark her degree of pain and relaxation on the 100‐mm line with the following endpoints: 0 = no pain at all and 100 = worst conceivable pain, and 0 = totally relaxed and 100 = very tense, for pain and relaxation, respectively. Obstetric outcomes were also assessed. After delivery, the woman was asked the extent to which the treatment had provided pain relief and relaxation, and if she would accept the same treatment during a future delivery. | |
| Notes | Study duration: not stated. Funding: grants from Skaraborg Institute for Reseach and Development, Barnets, Lychopenning, The Swedish Association of Midwives, Hegu Svenska AB and the University of Skövde. Conflict of interest: not stated. Setting: labour ward at Kärnsjukhuset in Skövde. Country: Sweden. Stratified by parity, randomisation in blocks of 10. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts defined as events after randomisation leading to no treatment or events after treatment, such as delivery or requirement for other methods of pain relief. Another midwife undertook women's assessment of pain and relaxation. The reasons for dropout were similar between groups; 16 women in the acupuncture group and 11 women in the injection group dropped out (total 17% dropout). |
| Selective reporting (reporting bias) | Unclear risk | Study protocol was not available. |
| Other bias | Low risk | There was a slight imbalance in age, there appears to be no other source of bias. |
Nesheim 2003.
| Methods | A single‐blind, controlled trial of acupuncture versus usual care. | |
| Participants | 198 women were enrolled into the trial of acupuncture versus usual care. Women were recruited to the trial who were at term, experiencing regular contractions and had an ability to speak Norwegian. Women were excluded if their labour was induced, planning a caesarean section, a plan to request an epidural block, medical reasons for an epidural, or experiencing any infectious diseases. | |
| Interventions | 8 midwives were educated and trained to practice acupuncture for the trial. All women received other analgesics on demand. The acupuncture points used were selected based on the participants' needs and included points BL32, GV20, BL60, BL62, HT7, LR3, GB34, CV4, LI10, LI11, BL23, BL27, 28, 32, LI4, SP6, PC6,7, ST36. De qi was obtained. Needles were left in place for 10‐20 minutes, or removed after the needling sensation was obtained, or taped and left in place. Women in the control group received conventional care. | |
| Outcomes | Clinical outcomes included use of meperidine, use of other analgesics, duration of labour, mode of birth and Apgar score. Participants also rated their pain relief along a VAS scale and asked to report any side effects from the treatment. | |
| Notes | Study duration: not stated. Funding: not stated. Conflict of interest: not stated. Setting: Ulleval University hospital, Oslo Norway. Country: Norway. A power analysis was undertaken. An ITT analysis was performed. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated. |
| Allocation concealment (selection bias) | Low risk | Adequate, sealed opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinician not blinded. Interventions were substantially different and obvious to an observer. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Inbalance in dropouts between groups; 6 dropouts, 1 dropout from acupuncture group. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol was unavailable. |
| Other bias | Low risk | Demographic baseline characteristics comparable between groups. |
Ozgoli 2016.
| Methods | Ranomised controlled trial of LI4 and BL32 acupressure compared with usual care. | |
| Participants | 105 primiparous women in active phase of first stage of labour. Inclusion criteria: age range of 19–35 years, term pregnancy (> 37 weeks of gestation), planned vaginal delivery without obstetrical or non‐obstetric complications, fetal vertex presentation, and being in active phase of first‐stage labour with cervical dilatation of ≥ 4 cm and presence of at least 3 uterine contractures within 10 minutes. Exclusion criteria: unwillingness to continue taking part in the study. |
|
| Interventions | Experimental intervention: Hegu LI4, n = 35 and BL32 acupressure: n = 35 Intervention applied at cervical dilation 4 cm to 5 cm, 6 cm to 7 cm, 8 cm to 10 cm during 6 uterine contractions. Pressure applied by the researcher until nail bed changed colour. Application of pressure stopped at the end of the contraction. Repeated for 6 contractions, following 6th contraction women gave assessment of pain Control group: usual care |
|
| Outcomes | Pain assessed by numerical rating scale. Type of delivery, Apgar score. | |
| Notes | Study duration: August to November 2008. Funding: none reported. Conflict of interest: none declared Setting: Shahid Akbarabadi Hospital (Tehran) Country: Iran Data from both acupuncture groups will be combined in the analysis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated: random allocation software |
| Allocation concealment (selection bias) | High risk | Open list no concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding, open‐label. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Data collected by the researcher administering the intervention |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 woman in the control group withdrew |
| Selective reporting (reporting bias) | Unclear risk | No protocol available. Dose of oxytocin that was administered in each subject for labour induction, pattern of uterus contractions, Bishop Score, frequency of pethidine administration were also recorded but not reported. |
| Other bias | Low risk | No evidence of other biases. |
Qu 2007.
| Methods | Randomised controlled trial of electro‐acupuncture or control (no pain relief). | |
| Participants | 36 study participants. Inclusion criteria: primiparous women, with a normal single pregnancy with spontaneous onset of labour, cephalic presentation, cervical dilation < 6 cm at admission, gestational age 37‐42 completed weeks. Exclusion criteria: diabetes, pre‐eclampsia, hypertension, kidney disease, thrombocytopenia, psychological distress or anorexia, infectious blood disease, atopic eczema or psoriasis. |
|
| Interventions | Acupuncture group: bilateral acupuncture points stimulation of points LI4 and SP6. Treatment started at beginning of active phase of first stage of labour. When de‐Qi achieved, needles retained for 2 minutes, then connected to electro‐acupuncture stimulator, at a frequency of 2‐100Hz, current: 14‐30mA. Stimulation increased gradually and needles removed after 20 minutes. When dilation reached 7 cm to 8 cm, procedure performed again. Control group: no pain relief. |
|
| Outcomes | Assessment of pain intensity and degree of relaxation throughout the labour. (Assessed hourly. Assessment tool 11‐point scale: 0 = painless and well relaxed; 10 = worst pain imaginable and very tense.) | |
| Notes | Study duration: August 2004 to May 2005. Funding: authors are funded by the Innovation Research Foundation by government of Heilongjiang Privince, China. Conflict of interest: not stated. Setting: affiliated hospital of Heilongjiang University of Chinese Medicine. Country: China. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Lot drawing. |
| Allocation concealment (selection bias) | Unclear risk | quote: "Neither the doctors, midwives, nor the primiparas could predict the group allocation.” |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Women and the study practitioner was not blind to the study groups. No other details reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 women excluded from the analysis, 2 acupuncture (no pain or relaxation data available), 1 woman from the control group (no spontaneous labour). |
| Selective reporting (reporting bias) | Unclear risk | Study protocol not available. |
| Other bias | Low risk | No imbalances at baselines, the study appears free of other biases. |
Ramnero 2002.
| Methods | Parallel single‐blind, randomised controlled trial of acupuncture. The trial was stratified by parity. Women received acupuncture or no acupuncture. | |
| Participants | 100 women were recruited. Randomisation took place in the delivery suite following admission. Inclusion criteria: 37+ weeks' gestation, spontaneous labour, cephalic presentation, cervical dilatation < 7 cm at admission. Exclusion criteria: diabetes, pre‐eclampsia, kidney disease, thrombocytopenia, psychological distress or anorexia, infectious blood disease, atopic eczema or psoriasis. | |
| Interventions | All women had access to conventional analgesia. 11 midwives completed a 4‐day course in acupuncture for labour pain. These midwives administered acupuncture to the treatment group. Acupuncture treatment was individualised with relaxing points combined with local and distal analgesic points. Needles were inserted at 45 or 90 degrees, stimulated manually until de qui (needling sensation) was obtained. Needles were left in situ and removed after 1‐3 hours. | |
| Outcomes | Pain intensity and degree of relaxation was assessed once every hour, prior to any analgesic and 15 minutes after. Other outcomes included the use of analgesics, augmentation of labour with oxytocin, duration of labour, outcome of birth, antepartum haemorrhage, Apgar scores, and infant birthweight. | |
| Notes | Study duration: April 1999 to June 2000. Funding: supported by grants from Örebro Council Research Committee and Centre for Nursing Science, Örebro University Hospital. Conflict of interest: not stated. Setting: recruited from the antenatal clinic. Country: Sweden. No sample‐size calculation was described. An ITT analysis was performed. Stratified for parity. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was generated by shuffling cards. |
| Allocation concealment (selection bias) | Low risk | Adequate, concealed in sealed, opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Women and the study practitioner were not blinded to the study groups. No other details reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10 (10%) were excluded from the analysis after not meeting the inclusion criteria (breech presentation, not in active labour, not in spontaneous labour, missing pain and relaxation data). 5 from each group relating to not in active labour, breech presentation, not in spontaneous labour, emergency caesarean section, no assessment of pain. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol unavailable. |
| Other bias | Low risk | Baseline characteristics comparable between groups, no other identifiable source of bias. |
Salehian 2011.
| Methods | 3‐arm randomised controlled trial. | |
| Participants | Primiparous women at the beginning of active phase of labour, gestational age between 38‐42 weeks, single pregnancy, cephalic presentation of the fetus, and in good health, not diagnosed with any specific diseases, dilation 4 cm and 2 or 3 uterine contractions every 10 minutes. | |
| Interventions | 1. Hoku (Hegu) point (LI4) acupressure 2. SanYinJiao (SP6) acupressure 3. Control group ‐ usual care |
|
| Outcomes | Labour pain (before and after the intervention at the stages of 4, 6, 8 and 10 cm cervical dilation), length of labour (in 2 stages: from 4 cm cervical dilation to 10 cm cervical dilatation, and 10 cm cervical dilatation to birth). | |
| Notes | Study duration: 2008 to 2009. Funding: not stated. Conflict of interest: not stated. Setting: Iran Hospital, Iranshahr, Iran. Country: Iran. Translated from Persian. Groups 1 and 2 were combined. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Created 2 blocks and assigned sample numbers equally to each group. |
| Allocation concealment (selection bias) | Low risk | Concealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Women and the study practitioner was not blinded to the study groups. No other details reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessor blinded according to author clarification. Analyst unclear. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Predefined outcomes in the methods have been reported on. |
| Selective reporting (reporting bias) | Unclear risk | Outcome measures addressed in the protocol has been reported in the paper but protocol has been registered retrospectively (IRCT138804232170N1). |
| Other bias | Unclear risk | Protocol states that this clinical trial was performed on 60 nulliparas women. Baseline differences not reported. |
Sehhatie‐Shafaie 2013.
| Methods | 2‐group parallel randomised controlled trial. | |
| Participants | 18 to 35 years old, gestational age 37 to 42 weeks (according to LMP or ultrasound in less than 12 weeks), singleton pregnancy, at least 4 cm dilation (entering the active phase of labour), viewing the head, intact amniotic sac at examination, or elapse of 6 hours after the rupture of the amniotic sac, spontaneous onset of uterine contraction, low risk pregnancy (such as the absence of chronic disease like heart disease, hypertension, lung disease, diabetes, anaemia, urinary tract infection, thyroid disease, and epilepsy, did not have abortion, dead fetus, bleeding or any abnormality when referring to the hospital), fetal weight of less than 4000 g (based on Johnson formula), absence of cephalopelvic disproportion during vaginal examination, height of more than 145 cm. No lesions in Sanyinjiao (SP6) and Hegu (LI4) points, no disabilities that lead to communication problems for the mother. | |
| Interventions | At 4 cm dilation, with the start of the contraction in the experimental group (SP6 and LI4), the research assistant applied vertical pressure with thumbs on the sanyinjiao (SP6) points of both inner ankles of the patient. With the start of the first contraction, pressure was applied gradually for 30 seconds on the above mentioned points. Then this pressure was slowly intensified to the extent that the patient felt tingling, numbness, heaviness, and strain in the surrounding area. The amount of applied pressure was identified by the research assistant’s thumb nail colour. When the thumb nail turned white the most pressure was applied. At this point the pressure was held for 1 minute and then it was gradually decreased. The points were free of pressure for 30 seconds. Then for 5 minutes the hegu (LI4) points on both hands were pressed during the contractions followed by the pressure on the sanyinjiao (SP6) points on the inner ankle for 5 minutes. This process continued for 20 minutes. Control group: pressure applied on ineffective areas of the legs and hands with the same timing and condition as the above and by the research assistant's thumb. The pressure in the control group was to the extent that the participants felt the first pain. |
|
| Outcomes | Primary: intensity of labour pain as assessed using VAS. Secondary: duration of labour. |
|
| Notes | Study duration: February 2012 to May 2012. Funding: Tabriz University of Medical Sciences funding. Conflict of interest: authors state there is no conflicts of interest. Setting: delivery room of Alavi and Sabalan Hospitals. Country: Iran. Clinical trials register: Iranian Registry of Clinical Trials IRCT201106143027N5. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated variable block design. |
| Allocation concealment (selection bias) | Unclear risk | Not described, but implied. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not described. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported as detailed on the Clinical trials register: Iranian Registry of Clinical Trials IRCT201106143027N5. No protocol available. |
| Other bias | Low risk | No significant baseline imbalances. |
Skilnand 2002.
| Methods | Single‐blind, randomised controlled trial of acupuncture versus minimal acupuncture. | |
| Participants | 210 women were recruited. Women with a singleton pregnancy, cephalic presentation, in spontaneous active labour met the inclusion criteria. 110 women refused to participate in the trial. | |
| Interventions | Real acupuncture followed a treatment protocol. The protocol specified obtaining the de qi sensation, needles were taped and left in place until delivery or until conventional analgesics were required. Acupuncture points included HT7, LU7, ST30, ST29, GB34, ST36, SP8, SP6, KI3, GB41, LR3, GV20, BL34, BL32, LI4, BL67, BL60. Minimal acupuncture involved the same procedure but needles were inserted away from the meridians. Some needles were removed after 20 minutes if insufficient pain relief was provided by the treatment and control interventions. Conventional pain relief was made available. Midwives providing the intervention had received formal training in acupuncture. | |
| Outcomes | Pain was assessed along a 10 cm VAS, recorded at 30 minutes, 1 and 2 hours after treatment, the need for conventional pain relief and use of oxytocin. | |
| Notes | Study duration: 13 months during 1998/1999. Funding: not stated. Conflict of interest: not stated. Setting: maternity ward. Country: Norway. No power analysis was reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was assigned by drawing lots. |
| Allocation concealment (selection bias) | Low risk | Adequate, randomisation concealed in sealed in opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Women were blinded to their group allocation and study personnel collecting data were unaware of women's study group allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 women were excluded from the control group because they delivered prior to the intervention being administered. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol unavailable. Limited study outcomes reported. |
| Other bias | High risk | There was an imbalance in parity at baseline. |
Tjung 2008.
| Methods | 2‐arm randomised controlled trial of electro‐acupuncture versus control (no medication). | |
| Participants | 50 women with a normal singleton pregnancy 37 to 42 weeks' gestation, in labour, cephalic presentation, intact membranes with a cervical dilatation of 4 cm to 5 cm, at least 50% effaced, and Universal Pain Assessment Tool (UPAT) score for pain intensity and relaxation of not more than 3. Exclusion criteria: diagnosis of hypertension, cardiovascular, pulmonary, renal, gastrointestinal, and hematological diseases, moderate to severe dermatologic conditions. |
|
| Interventions | The acupuncture points used were Hegu (LI‐4) and (SP‐6) bilaterally. Treatment was started at the beginning of the active phase (4‐5 cm cervical dilatation) in the first stage of labour. Stainless steel filiform needles (gauge 32: 0.25 mm diameter by 25 mm long) were inserted into the acupoints to depths of 15 mm (Hegu LI4), and 20 mm (SP6Sanyinjiao) and the needles were retained for 2 minutes. Then, the handles of the needles were connected to the electro‐acupuncture stimulation apparatus, at a frequency of 2‐100 Hz and electric current of 14‐30 mA (tolerable strength) with a dense‐and‐sparse wave form. The stimulation strength was increased gradually. The needles were removed after 20 minutes. All acupuncture procedures were done by the author, a certified acupuncturist with 2 years of training and 7 years in the practice of acupuncture. Conrol: no pain relief at the start of the active phase of labour. In both groups, patients with pain scale of > 7 were given 50 mg meperidine and 25 mg promethazine at 7 cm dilation |
|
| Outcomes | Pain score, use and dose of oxytocin. Apgar score and mode of birth. | |
| Notes | Study duration: between February 2007 and March 2008 Funding: not stated Conflict of interest: not stated Setting: Mary Chiles General Hospital Country: Phillipines |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The numbers 1‐50 were selected randomly by drawing of lots to be designated as belonging to Group A or B. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label trial no blinding of participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Independent assessor. An independent observer (same for both groups) was also asked to rate the patient using the same tool. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | There are data for 50 participants, but there is no mention of missing data or otherwise |
| Selective reporting (reporting bias) | Unclear risk | Not stated – no protocol referenced |
| Other bias | Low risk | None. No significant difference existed in age of patients, age of gestation, parity and birthweight of the baby between the 2 groups. |
Vixner 2014.
| Methods | 3‐armed, randomised controlled trial. | |
| Participants | 303 nulliparas, normal singleton pregnancies, cephalic presentation, 37 + 0 to 41 + 6 gestational age, expressed need for labour pain relief, admitted to delivery ward in active or latent phase of labour, spontaneous onset of labour. Sufficient Swedish for consent. | |
| Interventions | 1. Manual acupuncture: MA group ‐ needles were inserted and stimulated manually until DeQi achieved and thereafter stimulated at 10‐minute intervals. 2. Electro‐acupuncture: EA group, needles were inserted and first stimulated manually until DeQi achieved, then 8 of the local needles were connected to an electrical stimulator which was set at a high frequency (80 Hz) stimulation. The decision regarding which local needles were to be connected to the stimulator was made by the midwife. The woman adjusted the intensity of the electrical stimulation herself to a level just under the pain threshold. The remaining needles were stimulated manually every ten minutes by the midwife until DeQi was achieved. The women in the EA group received a combination of electrical and manual stimulation. MA or EA treatment was repeated after 2 hours, and thereafter made available on request. After the first treatment with acupuncture, women in the MA end EA groups had access to all the other pharmacological and non‐pharmacological methods of pain relief available on the delivery wards. After randomisation and when requesting pain relief, women in the MA and EA groups were treated with 13–21 needles, at 3 bilateral distal points and 4–8 bilateral local points, all within the same somatic area as the cervix and uterus. The local points were chosen with regard to the pain location. The needles were removed after 40 minutes. 3. Control group: usual care: women had access to all forms of pain relief with the exception of acupuncture, and the choice of which pain relief that was used was made by the woman and the midwife together. Pain relief included pharmacological analgesia (NO2, EDB, morphine), SWI, TENS. |
|
| Outcomes | Outcomes: primary: women’s self‐assessment of labour pain. Secondary: experience of relaxation, use of epidural analgesia, satisfaction with pain relief. Outcomes reported in trial design paper also include: labour outcomes: mode of birth, pain relief, augmentation of labour, duration of labour and perineal trauma. Negative side effects, experience of midwife support, pro‐inflammatory cytokines (IL‐1, IL‐6, hs‐CRP, TNF‐alpha). Memory of labour and pain and overall childbirth experience. Infant outcomes: Apgar score, pH, BE, neonatal transfer. |
|
| Notes | Study duration: November 2008 to October 2011. Funding: funded by grants from the Centre for Clinical Research Dalarna, Karolinska Institutet, Uppsala‐Örebro Regional Research Council, University of Skövde, FOU Fyrbodal, Magnus Bergvall. Stiftelse, and Dalarna University, Sweden. Conflict of interest: authors state there are no conflicts of interest. Setting: delivery wards at 2 Swedish hospitals. Country: Sweden. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation sequence. The randomisation was conducted in blocks with the length of 9, 12 and 15 which varied randomly. |
| Allocation concealment (selection bias) | Low risk | Opaque sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | MA group: 99 randomised – 16 did not receive MA; 19 did not receive MA according to study design (3 did not fulfilled inclusion criteria; 13 received < 7 needles; 9 had Rx < 40 minutes). N = 64 received MA according to study design. EA group: 103 randomised ‐ 16 did not receive EA; 35 did not receive MA according to study design (5 did not fulfilled inclusion criteria; 14 received < 7 needles; 16 had Rx < 40 minutes). N = 52 received MA according to study design. SC group: 101 randomised ‐ 18 did not receive SC; 8 did not receive SC according to study design (8 did not fulfilled inclusion criteria). N = 75 received SC according to study design MA group: ITT n = 83; PP n = 64 EA group: ITT n = 87; PP n = 52 SC group: ITT n = 83; PP n = 75 |
| Selective reporting (reporting bias) | Low risk | Trial protocol published. Some outcomes on blood sampling not reported. |
| Other bias | Unclear risk | No baseline imbalances. |
APG: acupressure group ITT: intention to treat LMP: last menstrual period SCG: standard care group SWI: sterile water injections TENS: transcutaneous electrical nerve stimulation TG: touch group VAS: visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aghdam 2012 | This study was not randomised. |
| Alsharnoubi 2015 | Outcome measures for this study did not match those of the review. No pain measures were recorded. |
| Asadi 2015 | Reports methods. |
| Bo 2006 | We were unable to establish study details to determine details of randomisation, blinding and data completeness. |
| Can 2015 | Study is investigating the effect of ice massage at acupoints. Study design is not consistent with review. |
| Deen 1985 | We were unable to establish study details to determine the exact study design. |
| Deepak 2013 | Study uses a quasi‐experimental study design. |
| Haghighi 2016 | Study assesses the effect of the intervention delivered postpartum. |
| Hajiamini 2012 | Study is investigating the effect of ice massage at acupoints. Study design is not consistent with review. |
| Kaviani 2012 | Study is investigating the effect of ice massage at acupoints. Study design is not consistent with review. |
| Kermani 2015 | Study uses pethidine as control group. |
| Levett 2016a | Study uses multiple techniques for pain management. Confounding effect of combination of techniques being evaluated. |
| Li 2006 | We were unable to confirm if the study was a randomised controlled trial following communication with the authors. |
| Li 1996 | This trial evaluated the effect of 2 acupuncture points on the strength and timing of uterine contractions following acupuncture. It did not report on any primary outcomes relevant to this review by study group. |
| Liu 2012 | Study is designed for length of labour, not for pain management in labour. |
| Liu 2015a | Control group uses epidural analgesia. Confounding effect of control intervention. |
| Liu 2015b | Uses sterile water injections at acupoints and then acupuncture. Confounding effect of SWI. |
| Masoudi 2014 | Intervention is care by a doula plus acupuncture. Outcome measure is anxiety not pain. Counfounding effect of other models of care. |
| Mollart 2013 | Study is for cervical ripening in preparation for labour, not pain management in labour. |
| Moradi 2014 | Outcome measures are fetal well‐being and anxiety, not pain management. Not consistent with review. |
| Mucuk 2014 | Study uses TENS machine. This is the subject of another review and is not covered by this one. |
| Nistler 2010 | Study involved osteopathic treatment and is not consistent with acupuncture/acupressure review. |
| Park 2003 | Only abstract published. Insufficient data reported to assess if eligibility criteria met. |
| Peng 2010 | Non randomised study. |
| Samadi 2018 | The trial assessed anxiety during labour. |
| Sebastian 2014 | We were unable to establish the study design quasi‐randomised or a controlled clinical trial. |
| Shalev 1991 | Twenty‐five women recruited during labour at a maternity hospital in Israel. Thirteen women randomised to receive electroacupuncture and 12 women received no analgesia at the start of the active phase of labour (cervical dilatation 4 cm, effacement 60%). The study reported on beta endorphin levels and did not report on any measures relevant to this review. |
| Shang 1995 | In this trial of 161 women, the effect of acupuncture on Hegu point was examined in relation to the length of the second stage of labour and the amount of postpartum bleeding. The study was excluded as it did not examine the effect on pain relief. |
| Ternov 1998 | We were unable to establish the study design quasi‐random or a controlled clinical trial. |
| Vixner 2017 | Cohort study |
| Wang 1994 | Not a randomised study. |
| Wu 2017 | Use of sterile injection confounded effects of the intervention. |
| Zhang 2000 | The evaluation of point injection therapy did not meet our eligibility criteria. |
| Zhu 2013 | Study does not use a randomised design. |
SWI: sterile water injections TENS: transcutaneous electrical nerve stimulation
Characteristics of studies awaiting assessment [ordered by study ID]
Akbarzadeh 2014.
| Methods | 3‐arm parallel randomised control trial of 150 women. |
| Participants | 18–35 years of age, term pregnancy, singleton pregnancy, and healthy fetal membranes, no history of medical, surgical, or mental problems, no pregnancy complications. The participants’ uterine contractions started spontaneously and, at admission, the contractions occurred every 5–10 minutes and cervical dilatation was 3 cm to 4 cm. |
| Interventions |
1. Acupressure: the participants were located in the appropriate position and BL32 acupoint was pressed. Pressure was applied by the beginning of contractions (3 to 4 cm cervical dilatation) and continued during the transitional phase of labour (7 cm to 8 cm cervical dilatation), up to the end of the first stage. When the contractions began, the point was pressed gently for 30 seconds. The researcher applied pressure by the right and the left thumbs was measured as 1405 and 1277 mmHg, respectively. The pressure was applied by the beginning and stopped at the end of the contractions. 2. Doula/supportive care: the doula (the researcher) was constantly beside the mother from maternity ward admission (beginning of the active phase of labour at 3 cm to 4 cm cervical dilatation) to the end of the second stage of labour. Supportive measures classified into psychological and emotional, educational, and physical categories were offered to the mother. Psychological and emotional support included touching, empathy, compassion, encouraging the mother to continue co‐operation in the labour process, reassurance, taking mother’s hands, maintaining eye contact, creating a sense of trust and confidence, continuous talking, and reduction of fear during labour. Educational support included informing the mother about the natural process of childbirth and answering her questions. Finally, physical support included cooling the mother, satisfying her hunger and thirst, and helping her change the positions in various stages of labour. These positions were as follows: the mothers followed activity positions, such as straddling a chair, leaning, tailor stretching, and lunging for 20 minutes at 3 cm to 8 cm dilatation. Then, they were required to follow relaxing positions, such as semi sitting and side‐lying for 10 minutes. At 8 cm to 10 cm dilatation, the mothers followed fetal head descent positions, such as dangling, squatting, and hands and knees. 3. Routine care. |
| Outcomes | VAS 10‐point scale following 30‐minute intervention, mode of birth. |
| Notes | Location: Iran. Setting: delivery ward. Authors were contacted seeking clarification of methods of randomisation, no response obtained. |
Akbarzadeh 2016.
| Methods | 3‐arm parallel randomised control trial of 150 women. |
| Participants | 18–35 years of age, term pregnancy, singleton pregnancy, and healthy fetal membranes, no history of medical, surgical, or mental problems, no pregnancy complications. The participants’ uterine contractions started spontaneously and, at admission, the contractions occurred every 5–10 minutes and cervical dilatation was 3 cm to 4 cm. |
| Interventions |
1. Acupressure: the participants were located in the appropriate position and BL32 acupoint was pressed. Pressure was applied by the beginning of contractions (3 cm to 4 cm cervical dilatation) and continued during the transitional phase of labour (7 cm to 8 cm cervical dilatation) up to the end of the first stage. when the contractions began, the point was pressed gently for 30 seconds. The researcher applied pressure by the right and the left thumbs was measured as 1405 and 1277 mmHg, respectively. The pressure was applied by the beginning and stopped at the end of the contractions. 2. Doula/supportive care: the doula (the researcher) was constantly beside the mother from maternity ward admission (beginning of the active phase of labour at 3 cm to 4 cm cervical dilatation) to the end of the second stage of labour. Supportive measures classified into psychological and emotional, educational, and physical categories were offered to the mother. Psychological and emotional support included touching, empathy, compassion, encouraging the mother to continue cooperation in the labour process, reassurance, taking mother’s hands, maintaining eye contact, creating a sense of trust and confidence, continuous talking, and reduction of fear during labour. Educational support included informing the mother about the natural process of childbirth and answering her questions. Finally, physical support included cooling the mother, satisfying her hunger and thirst, and helping her change the positions in various stages of labour. These positions were as follows: the mothers followed activity positions, such as straddling a chair, leaning, tailor stretching, and lunging for 20 minutes at 3 cm to 8 cm dilatation. Then, they were required to follow relaxing positions, such as semi sitting and side‐lying for 10 minutes. At 8 cm to 10 cm dilatation, the mothers followed fetal head descent positions, such as dangling, squatting, and hands and knees. 3. Routine care. |
| Outcomes | Length of labour, Apgar scores. The Apgar scores are reported as < 8. Not standard reporting. |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Fei 1985.
| Methods | Parallel randomised controlled trial of 200 women. |
| Participants | Women undergoing normal labour. |
| Interventions | Electro‐acupuncture with G6805 needles, with 3‐5 volt, 1500–3000 Hz. |
| Outcomes | Pain control, length of labour, Apgar scores. |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Heidari 2008.
| Methods | Randomised controlled trial of 128 women. |
| Participants | Pregnant women, nulliparous or multiparous (second pregnancy), 37 weeks, cephalic presentation, cervical dilatation of 3 cm, admitted to the hospital. |
| Interventions | 1. 30 minutes of acupressure on SP‐6 point (6 seconds constant pressure on uterine contractions to the point that participants have a little pain at the site and then 2 seconds of rest, moderate to severe pressure, average pressure was measured as pressure of 1600 mmHg of right thumb and 1300 mmHg of the left thumb; severe pressure was measured as pressure of 2000 mmHg of right thumb and 1800 mmHg of the left thumb). 2. 30 minutes of touch on SP‐6 point. |
| Outcomes | Apgar score at 1 minute and 5 minute, labour pain and pain intensity (VAS scale) before intervention, immediately after intervention, 30 minutes after intervention, and then every hour until the end of the first stage of labour. |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Jin 2011.
| Methods | Single‐blind parallel randomised controlled trial. |
| Participants | 174 cases of singleton primiparas. |
| Interventions | Moxibustion applied to an acupuncture point versus moxa to a non acupuncture point and no treatment. |
| Outcomes | Length of labour, Apgar scores. |
| Notes |
Okumus 2017.
| Methods | Randomised controlled trial of acupressure versus oxytocin |
| Participants | 100 women recruited from a private hospital in Turkey. Inclusion criteria: singleton pregnancy, primiparous, in active spontaneous labour. |
| Interventions | Acupressure at point SP6 versus oxytocin |
| Outcomes | Labour, pain, anxiety. length of labour. |
| Notes | Awaiting full text, conference abstract of poster findings only |
Pour 2012.
| Methods | Randomised controlled trial. |
| Participants | Singleton pregnancy, 38‐42 weeks, cephalic presentation, intact membranes, no disease or restrictions to perform acupressure and electrical stimulation of the skin (skin disorders such as eczema and skin infections) and heart disorders. |
| Interventions |
1. Acupressure group: cervical dilation 3 cm to 4 cm at the beginning of uterine contractions, a researcher massaged the SP6 area (4 fingers above the ankle) on both legs for half an hour. The pressure was ended when uterine contraction was finished. 2. TENS group: clinical Tens novin (model: NEWDYNE 40B) was used. In each leg, a pair of electrodes was placed in the SP6 area. In 3 cm to 4 cm cervical dilatation, skin needle‐like flow of electrical stimulation was maintained continuously and up to the patient's tolerance for half an hour (4 Hz frequency and length of 200 metres per second). This flow increased up to her tolerance each time she felt the flow rate reducing. 3. Control group. |
| Outcomes | Pain intensity (3 groups) and satisfaction of technique for its use in the next delivery (2 groups). |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Samadi 2010.
| Methods | 3‐armed randomised controlled trial. |
| Participants | The participants were 131 pregnant women between 38‐42 weeks of pregnancy and in labour. They were 18 to 35 years old; parity of 1 or 2; not using medications (psychotherapeutics, labour induction medications, chemical or natural pain killers) prior to the study; cervical dilatation of 3 cm to 5 cm; normal uterine contraction (20 seconds repeated every 5 minutes or less); body mass index less than 29; lack of medical or obstetrical problems such as uterine myomas, precancerous lesions, cephalopelvic disproportion, infertility or surgical operation on uterus or cervix, placenta previa, placental abruption, polyhydramnios or oligohydramnios, erythroblastosis fetalis, pre‐eclampsia, gestational diabetes, decreased fetal movements; no use of tobacco (e.g. smoking, hubble bubble, drugs) or alcohol and no verbal, auditory, or mental problems. Exclusion criteria: lack of consent; oxytocin dose in excess of routine requirements and any sign of fetal distress such as a heart rate of over 160 or less than 110 beats/minute, late decelerations, thick meconium staining and prolonged or precipitate labour, newborn weighing less than 2500 g or more than 4000 g. |
| Interventions | Acupressure on SP6 versus light touch at SP6 and usual care. |
| Outcomes | Labour pain intensity, labour duration and mode of birth. |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Su 2001.
| Methods | 4‐arm randomised controlled trial. |
| Participants | Women were full term (38‐42 weeks' gestation), primigravida, with singleton pregnancy, no cervical or obstetric diseases, healthy fetus, no cephalopelvic disproportion, no contraindications to vaginal delivery, no contraindications to spinal analgesia. |
| Interventions |
1. HANS group (group I): acupuncture at ZhiYang point and JiZhong point. Stimulated at 2/100Hz at 6‐second intervals. The stimulation is at 2Hz and 100 Hz for 0.6ms and 0.2ms, respectively. All titrated up to patient tolerance; usually at 8‐12 mA for ZhiYang, and 15‐25mA for JiZhong point. The acupuncture is done hourly for a total of 30 minutes. 2. Placebo + PCEA (group II): intradural inserted at L3‐5 with lidocaine 6 mL; PCA is given at 4 mL per press, and is subsequently locked for 15 minutes; max is 20 mL per hour. Baseline is given at 0.1 mL per hour. 3. HANS + PCEA (group III): acupuncture as per group I and PCEA as per group II. 4. Control; no intervention (group IV): no intervention. |
| Outcomes | Maternal parameters (blood pressure in kPa, heart rate in beats per minute, breathing in breaths per minute): every 30 minutes from start of stage I labour to completion of delivery. SpO2 – oximetry every half‐hourly; if lower than 90%, given oxygen. Uterine contractions and time of labour. Fetal heart rate every 15‐30 minutes measurement. VAS pain scoring of 0 to 10, measured at pre‐intervention, and every half‐hour post intervention. Neonatal Apgar (1 minute, 5 minute). Adverse events: blood pressure decrease, respiratory arrest, nausea, urinary retention, those requiring labour augmentation (Intravenous or surgical caesarean delivery). Volume of PCEA used and number of PCA presses. Postpartum haemorrhage (total during delivery and up to 2 hours after). |
| Notes | Translated from Chinese. |
Torkzahrani 2016.
| Methods | 3‐arm randomised controlled trial ‐ acupressure versus sham acupressure versus control. |
| Participants | 162 pregnant nulliparous women without any symptoms of labour from Shahid Akbar Abadi Hospital in Tehran, 2015. Inclusion criteria: gestational age of 39‐41 weeks ؛ nulliparous women؛ Bishop score < 4. Exclusion criteria: discontinuing of the study by mother request؛ taking chemical or herbal drugs. |
| Interventions |
1. Acupressure Acupressure was performed in the SP6, BL32, and BL60 at 39‐40 weeks of gestation in low‐risk participants. 30 minutes, twice per day. 2. Sham acupressure Pressure was applied to an ineffective point for 30 minutes 2 times a day 3. Control group No details in abstract or clinical trial registry. |
| Outcomes | Use of analgesics and oxytocin |
| Notes | Only English abstract available. Full text in Farsi |
Wan 2016.
| Methods | 2‐arm randomised controlled trial of acupressure and control (no details provided. |
| Participants | 120 primiparous women in labour 2 cm to 3 cm dilated |
| Interventions | Acupressure to points LI4, SP6, LR3, PC6, BL32, BL33. |
| Outcomes | Pain scores, mode of birth, length of labour. |
| Notes | English only abstract awaiting full text in Chinese. |
Wan 2018.
| Methods | 3‐arm randomised controlled trial of acupressure and music. |
| Participants | 241 pregnant women recruited from a maternity hospital in China. |
| Interventions | Acupressure versus music versus no treatment. |
| Outcomes | VAS (pain) (1, 4, 8, 16, 24 hours) Satisfaction for childbirth (2, 12, 24 hours post intervention) |
| Notes | The authors have been contacted for details on randomisation and for pain data that are presented in a graphical format only. |
Xu 2000.
| Methods | 2‐arm randomised controlled trial. |
| Participants | Inpatient hospital setting in Hebei, China. Described as normal labour women. |
| Interventions |
1. HANS + Diazepam group (group I): diazepam 10 mg intramuscular injection when cervical dilation of 3 cm. HANS acupuncture delivery system is used, after diazepam is given: 4 pads, each 5 cm‐square of electrode pads are placed on both sides of the T10 and L1/2 spine. Their position is adjusted again when cervical dilation is at 7 cm to 8 cm. 2. Control/Comparison intervention: diazepam only (group II): 10 mg of Intramuscular injection diazepam given when cervical dilation of 3 cm. |
| Outcomes | Pain score (taken when dilation 3 cm, 7 cm to 8 cm, and during labour):
Serum cortisol (taken when dilation 3 cm, 7 cm to 8 cm, and during labour). Serum Beta‐endorphin (taken when dilation 3 cm, 7 cm to 8 cm, and during labour), neonatal Apgar, neonatal blood gas, postpartum haemorrhage, labour time, caesarean section. |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Zhang 2002.
| Methods | 4‐arm randomised controlled trial. |
| Participants | Healthy, full‐term pregnancy, singleton, vertex presentation, primigravida, cervical dilation 2 cm to 3 cm. |
| Interventions |
1. Hans Acupoint Nerve stimulation (HANS): 4 cm x 9 cm electrode pads, placed on the Han’s acupoint area located at T10 to L3 region, and another at the S2 ‐ S4 region on the back. Current is 2/100Hz, alternating, and at 14 mA to 30 mA. 2. Diazepam: 10 mg IV (D). 3. Both Hans Acupoint Nerve stimulation (HANS + D). 4. Control group: (pads placed, but without any current); no intervention given. |
| Outcomes |
Primary VAS for pain measurement – pre intervention, post intervention (1 hour post), during first stage labour (or at cervical dilation 7 cm to 8 cm), during 2nd stage of labour. Secondary Labour progress time, postpartum haemorrhage, surgical augmentation, oxytocin, fetal heart rate, amniotic fluid testing, Apgar score, umbilical artery pH, neonatal respiratory distress, neonatal apnoea. |
| Notes | The authors were contacted for further information on the methodology of the study. To date no response has been received. |
Zhang 2006.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We have been unable to locate full‐text article. |
Ziaei 2006.
| Methods | Randomised controlled trial of acupuncture compared with placebo acupuncture and no intervention. |
| Participants | 90 women were recruited from a hospital in Tehran, Iran. Inclusion criteria: were normal singleton pregnancy of 37 weeks or longer and a spontaneous onset of labour, cephalic version, cervical dilatation of 3 cm to 6 cm. |
| Interventions |
Acupuncture (30 women): solid titanium needles GV20, Yingtang, ST36, SP6, LI4, CV2, 3. Needle insertion began when pre‐treatment pain score of 3 or higher was reached. A feeling of de qi was obtained. Needles left in place until delivery. Control group 1 (30 women): ‘pretend’ acupuncture, solid titanium needles of same type as intervention, inserted at 6 points normally used for vaccinations and other injections. Control group 2 (30 women): no intervention. |
| Outcomes | Pain intensity, relaxation, duration of labour, need for augmentation by oxytocin, caesarean section. |
| Notes | The authors were contacted for further information on the methodology of the study as randomisation status was unclear. To date (September 2017) no response has been received. |
PCEA: patient‐controlled epidural analgesia SpO2: capillary oxygen saturation TENS: transcutaneous electrical nerve stimulation VAS: visual analogue scale
Characteristics of ongoing studies [ordered by study ID]
Alimoradi 2018.
| Trial name or title | Comparing the effect of auricular and body acupressure on the pain and duration of the first stage of labour |
| Methods | |
| Participants | Primigravida women aged 19‐35 years. Low‐risk pregnancy: gestational age between 37‐42 weeks; singleton pregnancy; cephalic presentation; no prior medical or surgical complication; height more than 150 cm. Having 3 cm to 4 cm cervical dilatation. Exclusion criteria: having analgesic drugs 3 hours prior to or during intervention Induction or augmentation of labour |
| Interventions | 1‐ Auricular acupressure 2‐ body acupressure 3‐ control with routine care |
| Outcomes | Duration of first stage of labour, labour pain |
| Starting date | 11/3/2018 |
| Contact information | Zainab Alimoradi email zainabalimoradi.sbmu.ac.ir@gmail.com |
| Notes | Trial is recruiting |
Ozgoli 2018.
| Trial name or title | The effect of pressure on bile duct 21 on labour pain in primiparous women |
| Methods | Randomised controlled trial |
| Participants | Inclusion criteria: primiparous; age 18‐35 years; cephalic presentation; gestational age 37‐41 weeks; singleton; ability to read and write; tendency to use analgesia; active phase of labour. Exclusion criteria: not having willingness to work with researcher, planned caesarean section |
| Interventions | Pressure group on GB 21 Control group: pressure group on sham point |
| Outcomes | Severity of labour pain. Satisfaction of the treatment course |
| Starting date | 21/1/2018 |
| Contact information | Hamideh Torkiyan Shahid Beheshti University of Medical Sciences, iranifavahar@gmail.com |
| Notes | Trial has completed recruitment but is unpublished. |
Ranjkesh 2018.
| Trial name or title | The effect of LI4, H7 and SP6, Neima acupressure on the pain severity and duration of delivery in nulliparous women |
| Methods | Randomised controlled trial. |
| Participants | 144 pregnant women aged 19 to 35 years old, nulliparous gestational age between 42‐37 weeks, singleton and low‐risk pregnancies. Exclusion criteria: oxytocin administration for induction of labour, use of analgesic medications, unreliable embryonic cardiac rhythm. |
| Interventions | Acupressure applied to point SP6 in early labour, and from 8 cm, the points are changed to H7 and LI4 points. Control usual care plus aromatherapy. |
| Outcomes | Pain in labour. |
| Starting date | 21/1/2018. |
| Contact information | Fatemeh Ranjkesh email: franjkesh@qums.ac.ir |
| Notes | Trial recruiting |
Differences between protocol and review
2011 This updated review differs from the previously published Cochrane systematic review 'Complementary and alternative therapies for pain management in labour' (Smith 2006). This review has now been revised to three separate reviews.
2019 This updated review differs from the previous published Cochrane systematic review 'Acupuncture or acupressure for pain management in labour' (Smith 2011a, please see Other published versions of this review). Since the last review, a publication that describes the NICMAN scale, which uses an 11‐item scale to review the quality of acupuncture studies, has been published (Smith 2017). We now include this and report on studies of acupuncture using this scale. The items include: clear description of the population; intervention; comparator; outcome; appropriateness of study design for question; inclusion of a differential diagnosis; selection of acupuncture points consistent with treatment principles; description of needles, needling depth, stimulation, and sensation; point location description and justification according to texts; treatments administered; and the qualifications of the person administering the treatments.
Seven 'Summary of findings' tables have been incorporated in the current update (2017).
Contributions of authors
Caroline Smith and Carmel Collins conceptualised and wrote the protocol, reviewed trials, performed data extraction and jointly wrote the review and its subsequent updates.
Kate Levett reviewed trials, contacted primary authors, co‐ordinated translation and review of data extraction from translated papers, performed data extraction, contributed to the analysis, and jointly wrote the review and its update.
Mike Armour undertook checking of the data, contributed to the analysis and contributed to the writing of the update.
Hannah Dahlen performed data extraction, contributed to the discussion and conclusion.
Aidan Tan undertook Chinese translations, contacted primary authors, and undertook data extraction, and commented on the draft of the review.
Bita Mesgarpour undertook Persian translations, contacted primary authors, and undertook data extraction, and commented on the draft of the review.
Caroline Smith is the guarantor of the review.
Sources of support
Internal sources
Western Sydney University, Australia, Other.
The University of Adelaide, Adelaide, Australia.
Child Health Research Institute, Australia.
Child, Youth and Women's Health Services, Adelaide, Australia.
-
University of Notre Dame Australia, Other.
In kind
External sources
No sources of support supplied
Declarations of interest
Carmel Collins: none known.
Hannah Dahlen: none known.
Bita Mesgarpour: none known.
Aidan Tan: none known.
Mike Armour: is an acupuncturist, not currently in clinical practice and until recently was a director of an acupuncture and physiotherapy clinic. As a medical research institute, the National Institute of Complementary Medicine (NICM) receives research grants and donations from foundations, universities, government agencies and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the Institute. This systematic review was not specifically supported by donor or sponsor funding to NICM.
Caroline Smith: as a medical research institute, the National Institute of Complementary Medicine receives research grants and donations from foundations, universities, government agencies and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the Institute.
Kate Levett: is employed at The University of Notre Dame, School of Medicine, and as a medical school employee receives research grants and donations from Foundations, Government agencies and industry. Kate Levett offers private acupressure for labour and birth education classes in Sydney Australia; these classes include complementary therapy strategies for pain relief in labour.
Edited (no change to conclusions)
References
References to studies included in this review
Borup 2009 {published data only}
- Borup L, Wurlitzer W, Hedegaard M, Kesmodel US, Hvidman L. Acupuncture as pain relief during delivery: a randomized controlled trial. Birth 2009;36(1):5‐12. [DOI] [PubMed] [Google Scholar]
Calik 2014 {published data only}
- Calik KY, Komurcu N. Effects of SP6 acupuncture point stimulation on labor pain and duration of labor. Iranian Red Crescent Medical Journal 2014;16(10):e16461. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chung 2003 {published data only}
- Chung UL, Hung LC, Kuo SC, Huang CL. Effects of LI4 and BL67 acupressure on labor pain and uterine contractions in the first stage of labour. Journal of Nursing Research 2003;11(4):251‐60. [DOI] [PubMed] [Google Scholar]
Dabiri 2014 {published data only}
- Dabiri F, Shahi A. The effect of LI4 acupressure on labor pain intensity and duration of labor: A randomized controlled trial. Oman Medical Journal 2014;29(6):425‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dong 2015 {published data only}
- Dong C, Hu L, Liang F, Zhang S. Effects of electro‐acupuncture on labor pain management. Archives of Gynecology and Obstetrics 2015;291:531‐6. [DOI] [PubMed] [Google Scholar]
Hamidzadeh 2012 {published data only}
- Hamidzadeh A, Shahpourian F, Orak RJ. Effects of LI4 acupressure on labor pain in the first stage of labor. Koomesh 2011;12(2):196‐203. [DOI] [PubMed] [Google Scholar]
- Hamidzadeh A, Shahpourian F, Orak RJ, Montazeri AS, Khosravi A. Effects of LI4 acupressure on labor pain in the first stage of labor. Journal of Midwifery and Women's Health 2012;57(2):133‐8. [DOI] [PubMed] [Google Scholar]
- Hamizadeh A, IRCT138904104281N1. Effects of LI4 acupressure on labor pain in the first stage of labor. en.search.irct.ir/view/3532 (first received 26 August 2010). [IRCT138904104281N1]
Hamlaci 2017 {published data only}
- Hamlacı Y, Yazici S. The effect of acupressure applied to point LI4 on perceived labor pains. Holistic Nursing Practice 2017;31(3):167‐76. [DOI: ; PUBMED: 28406870] [DOI] [PubMed] [Google Scholar]
Hantoushzadeh 2007 {published data only}
- Hantoushzadeh S, Alhusseini N, Lebaschi AH. The effects of acupuncture during labour on nulliparous women: a randomised controlled trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 2007;47(1):26‐30. [DOI] [PubMed] [Google Scholar]
Hjelmstedt 2010 {published data only}
- Hjelmstedt A, Shenoy S, Stener‐Victorin E, Lekander M, Bhat M, Balakumaran L, et al. Acupressure to reduce labour pain ‐ a randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2010;89(11):1453‐9. [DOI] [PubMed] [Google Scholar]
- Hjelmstedt A, Shenoy S, Stener‐Victorin E, Lekander M, Bhat M, Leena K Kb, et al. Acupressure to reduce labour pain ‐ a randomized controlled trial. International Journal of Gynecology & Obstetrics 2009;107(Suppl 2):S201. [Google Scholar]
Huang 2008 {published data only}
- Huang T, Yang Y, Huang X. Selection of acupoints and opportunity for acupuncture analgesia in delivery. Journal of Traditional Chinese Medicine 2008;49:625‐8. [Google Scholar]
Kashanian 2010 {published data only}
- Kashanian M, Shahali S. Effect of acupressure at the Sanyinjiao Point (SP6) on the process of active phase labor in nulliparas women. Journal of Babol University of Medical Sciences 2010;12(3):7‐11. [Google Scholar]
- Kashanian M, Shahali S. Effects of acupressure at the Sanyinjiao point (SP6) on the process of active phase of labor in nulliparous women. Journal of Maternal‐Fetal and Neonatal Medicine 2010;23(7):638‐41. [DOI] [PubMed] [Google Scholar]
Kordi 2010 {published data only}
- Kordi M, Firoozi M, Esmaili H. Effect of L14 acupressure on labor pain in the first stage of labor in nulliparous women. HAYAT 2010;6(3‐4):95‐101. [Google Scholar]
- Kordi M, Mashadi SR, Fadaee A, Esmaili H. [Effects of SP6 acupressure on reducing the labor pain during first stage of delivery]. Iranian Journal of Obstetrics, Gynecology and Infertility 2010;12(4):7‐12. [Google Scholar]
Lee 2004 {published data only}
- Lee MK. Effects of San‐Yin‐Jiao (SP6) acupressure on labor pain, delivery time in women during labor. Journal of Korean Academy of Nursing 2003;33(6):753‐61. [DOI] [PubMed] [Google Scholar]
- Lee MK, Chang SB, Kang D‐H. Effects of SP6 acupressure on labor pain and length of delivery time in women during labor. Journal of Alternative and Complementary Medicine 2004;10(6):959‐65. [DOI] [PubMed] [Google Scholar]
Ma 2011 {published data only}
- Ma SX, Wu FW, Cui JM, Jin ZH, Kong LJ. Effect on moxibustion at Sanyinjiao (SP 6) for uterine contraction pain in labor: a randomized controlled trial. Zhongguo Zhenjiu 2010;30(8):623‐6. [PubMed] [Google Scholar]
- Ma W, Bai W, Lin C, Zhou P, Xia L, Zhao C, et al. Effects of Sanyinjiao (SP6) with electroacupuncture on labour pain in women during labour. Complementary Therapies in Medicine 2011;19(Suppl 1):S13‐S18. [DOI] [PubMed] [Google Scholar]
- Ma WZ, Zhou PJ, Zhang Y, Yuan Y, Wu Y, Zhao CH, et al. Clinical observation on the effect of electroacupuncture of Sanyinjiao (SP 6) on labor. Acupuncture Research 2010;35(3):217‐21. [PubMed] [Google Scholar]
Mackenzie 2011 {published data only}
- MacKenzie IZ, NCT01165099. Acupuncture for pain relief during induced labour for nulliparae. clinicaltrials.gov/ct2/show/record/NCT01165099 (first received 19 July 2010). [NCT01165099]
- Mackenzie I, Xu J, Cusick C, Midwinter‐Morten H, Meacher H, Mollison J, et al. Acupuncture for pain relief during induced labour in nulliparae: a randomised controlled study. BJOG: an international journal of obstetrics and gynaecology 2011;118(4):440‐7. [DOI] [PubMed] [Google Scholar]
Mafetoni 2016 {published data only}
- Mafetoni RR, Shimo AK. Effects of acupressure on progress of labor and cesarean section rate: randomized clinical trial. Revista De Saude Publica 2015;49(1):1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mafetoni RR, Shimo AK. The effects of acupressure on labor pains during child birth: randomized clinical trial. Revista Latino‐Americana De Enfermagem 2016; Vol. 24:e2738. [DOI] [PMC free article] [PubMed]
Mafetoni 2016a {published data only}
- Mafetoni RR, Shimo AK. Effects of auriculotherapy on labour pain: a randomized clinical trial. Revista Da Escola De Enfermagem Da U S P 2016;50(5):726‐32. [DOI] [PubMed] [Google Scholar]
Mansouri 2018 {published data only (unpublished sought but not used)}
- Mansouri E, Kordi M, Aval SB, Shakeri MT, Mirteimouri M. Comparsion of pressure on Bladder‐GV20 and Gallbladder‐GV20 on labour pain intensity among the primiparous women: a randomized clinical trial. Evidence Based Care Journal 2018;8(3):7‐16. [Google Scholar]
Martensson 2008 {published data only}
- Martensson L, Stener‐Victorin E, Wallin G. Acupuncture versus subcutaneous injections of sterile water as treatment for labour pain. Acta Obstetricia et Gynecologica Scandinavica 2008;87(2):171‐7. [DOI] [PubMed] [Google Scholar]
Nesheim 2003 {published data only}
- Nesheim BI, Kinge R, Berg B, Alfredsson B, Allgot E, Hove G, et al. Acupuncture during labor can reduce the use of meperidine: a controlled clinical study. Clinical Journal of Pain 2003;19(3):187‐91. [DOI] [PubMed] [Google Scholar]
Ozgoli 2016 {published data only}
- Ozgoli G, Sedigh Mobarakabadi S, Heshmat R, Alavi Majd H, Sheikhan Z. Effect of LI4 and BL32 acupressure on labor pain and delivery outcome in the first stage of labor in primiparous women: A randomized controlled trial. Complementary Therapies in Medicine 2016;29:175‐80. [DOI] [PubMed] [Google Scholar]
- Ozgoli G, Sedigh S, Heshmat R, AlaviMajd H. Effect of right hand hegu acupressure on pain intensity of active phase of labor in primiparous women. Kowsar Medical Journal 2010;14(4):229‐34. [Google Scholar]
Qu 2007 {published data only}
- Qu F, Zhou J. Electro‐acupuncture in relieving labor pain. Evidence‐based Complementary and Alternative Medicine 2007;4(1):125‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramnero 2002 {published data only}
- Ramnero A, Hanson U, Kihlgren M. Acupuncture treatment during labour ‐ a randomised controlled trial. BJOG: an international journal of obstetrics and gynaecology 2002;109:637‐44. [PubMed] [Google Scholar]
Salehian 2011 {published data only}
- Mohamadinia N. Comparing Hoku point (LI4) acupressure and San‐Yin‐Jiao (SP6) acupressure on labor pain and length of delivery time in nulliparous women in Iran hospital 2008‐2009. Iranian Registry of Clinical Trials (IRCT) (http://www.irct.ir/) (accessed 6.01.2011).
- Salehian T, Dehcheshmaei FS, Pirak A, Kazemian A, Atarodi Z, Righi SD. Comparison of the effect of Hoku point (LI4) acupressure with that of San‐Yin‐Jiao (SP6) acupressure on labor pain and the length of delivery time in primiparous women. Scientific Journal of Kurdistan University of Medical Sciences 2011;16(1):64‐72. [Google Scholar]
Sehhatie‐Shafaie 2013 {published data only}
- Sehhatie‐Shafaie F, Kazemzadeh R, Amani F, Heshmat R. The effect of acupressure on sanyinjiao and hugo points on labor pain in nulliparous women: a randomized clinical trial. Journal of Caring Sciences 2013;2(2):123‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Skilnand 2002 {published data only}
- Skilnand E, Fossen D, Heiberg E. Acupuncture in the management of pain in labor. Acta Obstetricia et Gynecologica Scandinavica 2002;81:943‐8. [DOI] [PubMed] [Google Scholar]
Tjung 2008 {published data only}
- Tjung V, Solis SM, Servas AQ. Electro‐acupuncture in labor for pain relief and reduction of oxytocin use: a randomized controlled trial. Philippine Journal of Obstetrics & Gynecology 2008;32(4):156‐62. [Google Scholar]
Vixner 2014 {published data only}
- Martensson L, NCT01197950. Acupuncture to reduce labour pain. clinicaltrials.gov/ct2/show/record/NCT01197950 (first received 9 September 2010). [NCT01197950]
- Vixner L, Martensson L, Schytt E, Victorin ES. Manual and electroacupuncture for labour pain. Study design of a longitudinal randomized controlled trial. Journal of Alternative and Complementary Medicine (New York, N.Y.) 2013;19(7):A38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vixner L, Martensson LB, Schytt E. Acupuncture with manual and electrical stimulation for labour pain: A two month follow up of recollection of pain and birth experience. BMC Complementary and Alternative Medicine 2015;15(1):180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vixner L, Martensson LB, Stener‐Victorin E, Schytt E. Manual and electroacupuncture for labour pain: Study design of a longitudinal randomized controlled trial. Evidence‐based Complementary and Alternative Medicine 2012;2012:Article ID 943198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vixner L, Schytt E, Stener‐Victorin E, Waldenstrom U, Pettersson H, Martensson LB. Acupuncture with manual and electrical stimulation for labour pain: a longitudinal randomised controlled trial. BMC Complementary and Alternative Medicine 2014;14(1):187. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Aghdam 2012 {published data only}
- Aghdam SK, Daryabakhsh A. Effect of acupressure at Hugo point (LI4) on the process and outcomes of labor in nulliparous women. Iranian Journal of Obstetrics, Gynecology and Infertility 2012;15(27):14‐20. [Google Scholar]
Alsharnoubi 2015 {published data only}
- Alsharnoubi J, Khattab A, Elnoury A. Laser acupuncture effect on fetal well‐being during induction of labor. Lasers in Medical Science 2015;30(1):403‐6. [DOI] [PubMed] [Google Scholar]
Asadi 2015 {published data only}
- Asadi N, Maharlouei N, Khalili A, Darabi Y, Davoodi S, Raeisi Shahraki H, et al. Effects of LI‐4 and SP‐6 Acupuncture on labor pain, cortisol level and duration of labor. Journal of Acupuncture and Meridian Studies 2015;8(5):249‐54. [DOI] [PubMed] [Google Scholar]
Bo 2006 {published data only}
- Bo QX, Zhang JX. Observation on therapeutic effect of scalp acupuncture analgesia on labor. Zhongguo Zhenjiu 2006;26(9):659‐61. [PubMed] [Google Scholar]
Can 2015 {published data only}
- Can HO, Saruhan A. Evaluation of the effects of ice massage applied to large intestine 4 (hegu) on postpartum pain during the active phase of labor. Iranian Journal of Nursing and Midwifery Research 2015;20(1):129‐38. [PMC free article] [PubMed] [Google Scholar]
Deen 1985 {published data only}
- Deen P, Yuelam H. Use of acupuncture analgesia during childbirth. Journal of Traditional Chinese Medicine 1985;5(4):253‐5. [PubMed] [Google Scholar]
Deepak 2013 {published data only}
- Deepak AK, Chopra S. Effect of acupressure on intensity of labor pains and duration of first stage of labor among primigravida mothersEffect of acupressure on intensity of labor pains and duration of first stage of labor among primigravida mothers. Nursing and Midwifery Research Journal 2013;9(4):178‐86. [Google Scholar]
Haghighi 2016 {published data only}
- Haghighi NB, IRCT2016070428240N2. The effect of acupressure and touch point (SP6) on pain intensity after delivery 88 qualified mothers give birth on 22 Bahman hospital in Gonabad city. https://en.irct.ir/trial/22945 (22 August 2016).
Hajiamini 2012 {published data only}
- Hajiamini Z, Masoud SN, Ebadi A, Mahboubh A, Matin AA. Comparing the effects of ice massage and acupressure on labor pain reduction. Complementary Therapies in Clinical Practice 2012;18(3):169‐72. [DOI] [PubMed] [Google Scholar]
Kaviani 2012 {published data only}
- Kaviani M, Ashoori M, Azima S, RajaeiFard A, HadianFard MJ. Comparing the effect of two methods of acupressure and ice massage on the pain, anxiety levels and labor length in the point LI‐4. Journal of Shahid Sadoughi University of Medical Sciences 2012;20(2):220‐8. [Google Scholar]
Kermani 2015 {published data only}
- Kermani S, Derogar M, Moghadam MB, Bahri N, Mahmoudian AS, Mojtabavi SJ. Comparison of the effects of SP6 acupressure and use of pethidine on the intensity of labor pain in nulliparous women. Avicenna Journal of Phytomedicine 2015; Vol. 5, issue Suppl 1:23.
Levett 2016a {published data only}
- Levett KM, Smith CA, Bensoussan A, Dahlen HG. Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour. BMJ Open 2016;6(7):e010691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levett KM, Smith CA, Bensoussan A, Dahlen HG. The complementary therapies for labour and birth study making sense of labour and birth ‐ experiences of women, partners and midwives of a complementary medicine antenatal education course. Midwifery 2016;40:124‐31. [DOI] [PubMed] [Google Scholar]
- Levett KM, Smith CA, Dahlen HG, Bensoussan A. Complementary therapies for labour and birth: Results from a mixed methods study. Journal Paediatrics and Child Health 2014;50(Suppl 1):19. [Google Scholar]
Li 1996 {published data only}
- Li XH, Ma WZ. Effect of electro‐acupuncture Shenmen (Otopoint) and Hegu (LI4) on uterine contraction of parturients. Shanghai Journal of Acupuncture and Moxibustion 1996;15(4):14‐5. [Google Scholar]
Li 2006 {published data only}
- Li P, Liu X. Clinical and mechanism study on acupuncture for relieving the labour pain. Journal of Tianjin University of Traditional Chinese Medicine 2006;25(2):74‐6. [Google Scholar]
Liu 2012 {published data only}
- Liu YL, Jin ZG. Clinical observation of the impacts and safety of electroacupuncture at Sanyinjiao (SP 6) on labor. Chinese Acupuncture & Moxibustion 2012; Vol. 32, issue 5:409‐12. [PubMed]
Liu 2015a {published data only}
- Liu Y, Xu M, Che X, He J, Guo D, Zhao G, et al. Effect of direct current pulse stimulating acupoints of JiaJi (T10‐13) and Ciliao (BL 32) with Han's Acupoint Nerve Stimulator on labour pain in women: a randomized controlled clinical study. Journal of Traditional Chinese Medicine 2015;35(6):620‐5. [DOI] [PubMed] [Google Scholar]
Liu 2015b {published data only}
- Liu X, Wu L, Yi W. Clinical research of analgesic for labor with acupoint injection and electroacupuncture. Chinese Acupuncture & Moxibustion 2015;35(11):1155‐8. [PubMed] [Google Scholar]
Masoudi 2014 {published data only}
- Masoudi Z, Akbarzadeh M, Vaziri F, Zare N, Ramzi M. The effects of decreasing maternal anxiety on fetal oxygenation and nucleated red blood cells count in the cord blood. Iranian Journal of Pediatrics 2014;24(3):285‐92. [PMC free article] [PubMed] [Google Scholar]
Mollart 2013 {published data only}
- Mollart L. A randomized controlled trial of acupressure to assist spontaneous labour for women who are pregnant for the first time experiencing post‐date pregnancy: A pilot study. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=363555 (first received 6 February 2013).
Moradi 2014 {published data only}
- Moradi Z, Akbarzadeh M, Moradi P, Toosi M, Hadianfard MJ. The effect of acupressure at GB‐21 and SP‐6 acupoints on anxiety level and maternal‐fetal attachment in primiparous women: a randomized controlled clinical trial. Nursing and Midwifery Studies 2014;3(3):e19948. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mucuk 2014 {published data only}
- Mucuk S, Baser M. Effects of noninvasive electroacupuncture on labour pain and duration. Journal of Clinical Nursing 2014;23(11‐12):1603‐10. [DOI] [PubMed] [Google Scholar]
- Mucuk S, Baser M, Ozkan T. Effects of noninvasive electroacupuncture on labor pain, adrenocorticotropic hormone, and cortisol. Alternative Therapies in Health & Medicine 2013;19(3):26‐30. [PubMed] [Google Scholar]
Nistler 2010 {published data only}
- Nistler G, Deutschmann U, Lenz D, Schwerla F. Osteopathy as a therapy during pregnancy: A randomised controlled trial. International Journal of Osteopathic Medicine 2010;13(3):128. [Google Scholar]
Park 2003 {published data only}
- Park Y, Cho J, Kwon J, Ahn E, Lim J, Chang S. The effect of san‐yin‐jiao (SP‐6) acupressure on labor progression (abstract). American Journal of Obstetrics and Gynecology 2003;189(6):S209. [Google Scholar]
Peng 2010 {published data only}
- Peng T, Li XT, Zhou SF, Xiong Y, Kang Y, Cheng HD. Transcutaneous electrical nerve stimulation on acupoints relieves labor pain: a non‐randomized controlled study. Chinese Journal of Integrative Medicine 2010;16(3):234‐8. [DOI] [PubMed] [Google Scholar]
Samadi 2018 {published data only}
- Samadi P, Alipour Z, Lamyian M. The effect of acupressure at spleen 6 acupuncture point on the anxiety level and sedative and analgesics consumption of women during labor: a randomized, single‐blind clinical trial. Iranian Journal of Nursing and Midwifery Research 2018;23(2):87‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sebastian 2014 {published data only}
- Sebastian MK. Effect of acupressure on labour pain during first stage of labour among Primi mothers in a selected hospital of Delhi. Nursing Journal of India 2014;105(3):136‐9. [PubMed] [Google Scholar]
Shalev 1991 {published data only}
- Shalev E, Yanay N, Peleg D, Yagudin E. Electroacupuncture during labour and its effect on peripheral plasma beta‐endorphin concentration. American Journal of Acupuncture 1991;19(4):345‐8. [Google Scholar]
Shang 1995 {published data only}
- Shang LF, Liu JY, Li AX. Puncture the Hegu acupoint to accelerate the second stage of labor and to reduce the postpartum hemorrhage. Chinese Journal of Nursing 1995;30(9):537‐8. [PubMed] [Google Scholar]
Ternov 1998 {published data only}
- Ternov K, Nilsson M, Lofberg L, Algotsson L, Akeson J. Acupuncture for pain relief during childbirth. Acupuncture and Electro‐therapeutics 1998;23:19‐26. [DOI] [PubMed] [Google Scholar]
Vixner 2017 {published data only}
- Vixner L, Schytt E, Martensson LB. Associations between maternal characteristics and women's responses to acupuncture during labour: a secondary analysis from a randomised controlled trial. Acupuncture in Medicine 2017;35(3):180‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 1994 {published data only}
- Wang RY. Application of acupuncture‐combined with hypnotism in painless labor. Acupuncture Research 1994;19(1):180. [Google Scholar]
Wu 2017 {published data only}
- Wu L, Yin Y, Sun K, Hou H, Liu X, Yi W, et al. Effectiveness of acupuncture versus spinal‐epidural anesthesia on labor pain: a randomized controlled trial. Journal of Traditional Chinese Medicine 2017;37(5):629‐35. [PubMed] [Google Scholar]
Zhang 2000 {published data only}
- Zhang LJ. Point‐injection therapy for labor pains. Shanghai Journal of Acupuncture and Moxibustion 2000;19(2):10. [Google Scholar]
Zhu 2013 {published data only}
- Zhu HX, Yao Y, Wu YS, Liu Y, Yan LR, Su XJ. Influence of acupoint injection with small dose of fentanyl‐droperidol mixed liquor on labor analgesia and level of stress hormone in parturient. Chinese Acupuncture & Moxibustion 2013;33(4):342‐6. [PubMed] [Google Scholar]
References to studies awaiting assessment
Akbarzadeh 2014 {published data only}
- Akbarzadeh M, Masoudi Z, Hadianfard MJ, Kasraeian M, Zare N. Comparison of the effects of maternal supportive care and acupressure (BL32 acupoint) on pregnant women's pain intensity and delivery outcome. Journal of Pregnancy 2014;2014:Article ID: 129208. [DOI] [PMC free article] [PubMed] [Google Scholar]
Akbarzadeh 2016 {published data only}
- Akbarzadeh M, Masoudi Z, Zare N, Kasraeian M. Comparison of the effects of maternal supportive care and acupressure (at BL32 acupoint) on labor length and infant's Apgar score. Global Journal of Health Science 2016;8(3):236‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fei 1985 {published data only}
- Fei DE, Huang YL. Application of acupuncture analgesia in labor. Chinese Acupuncture & Moxibustion 1985;5(2):16‐7. [Google Scholar]
Heidari 2008 {published data only}
- Heidari P, Mojdeh F, Mazloom R, Tanbakoi K, Judaki K. Effect of acupressure on labor pain intensity. Hakim Research Journal 2008;11(2):39‐46. [Google Scholar]
Jin 2011 {published data only}
- Jin ZH, Zhang P, Ma SX. Effect of moxibustion at sanyinjiao (SP 6) on the process of childbirth: a randomized controlled study. Chinese Acupuncture & Moxibustion 2011;31(1):7‐10. [PubMed] [Google Scholar]
Okumus 2017 {published data only}
- Okumus F, Oncu‐Celik H. Acupressure on the sanyinjiao (SP6) versus synthetic oxytocin during labour. BMC Complementary and Alternative Medicine 2017;17(Suppl 1):317, Abstract no: P244. [Google Scholar]
Pour 2012 {published data only}
- Pour NH, Kaviani M, Razeghi M. Comparison of effect of transcutaneous electrical nerve stimulation and acupressure in decreasing labor pain in primiparous women. Iranian Journal of Obstetrics, Gynecology and Infertility 2012;15(12):27‐33. [Google Scholar]
Samadi 2010 {published data only}
- Samadi P, Lamiyan M, Heshmat R, Faghihzadeh S. Effect of acupressure at SP6 point on labor pain intensity. Journal of Hormozgan University of Medical Sciences 2010;14(1):55‐64. [Google Scholar]
Su 2001 {published data only}
- Su XJ. Clinical effect with Hans acupoint nerve stimulator (Hans) for reliving labour pain. Chinese Journal of Pain Medicine 2001;2:89. [Google Scholar]
Torkzahrani 2016 {published data only}
- Torkzahrani S, Mahmoudikohani F, Saatchi K, Sefidkar R, Banaei M. Effect of acupressure before the onset of labor on using analgesics and oxytocin during labor. Journal of Mazandaran University of Medical Sciences 2016;26(139):1‐9. [Google Scholar]
Wan 2016 {published data only}
- Wan Y, Li D. Clinical observation of analgesia in delivery treated with acupoint pressure therapy. Chinese Acupuncture & Moxibustion 2016;36(12):1243‐6. [DOI] [PubMed] [Google Scholar]
Wan 2018 {published data only}
- Wan Q, Wen FY. Effects of acupressure and music therapy on reducing labor pain. International Journal of Clinical and Experimental Medicine 2018;11(2):898‐903. [Google Scholar]
Xu 2000 {published data only}
- Xu CP. Combination of Hans and diazepam for labor analgesia: a basic and clinical study. Chinese Journal of Pain Medicine 2000;6(1):12. [Google Scholar]
Zhang 2002 {published data only}
- Zhang SY. Hans combined with diazepam for labor pain control. Chinese Journal of Pain Medicine 2002;8(2):101. [Google Scholar]
Zhang 2006 {published data only}
- Zhang N. The effect of electric acupuncture Hegu Acupuncture point with uterine contraction intensity of parturient. Chinese Journal of Information on Traditional Chinese Medicine 2006; Vol. 13, issue 11:79‐80.
Ziaei 2006 {published data only}
- Ziaei S, Hajipour L. Effect of acupuncture on labor. International Journal of Gynecology & Obstetrics 2006;92(1):71‐2. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Alimoradi 2018 {published data only}
- Alimoradi Z, IRCT20180218038789N1. Comparing the effect of auricular point acupressure and body acupressure on the pain score and the active phase duration of first stage of labor. https://en.irct.ir/trial/29707 (first received 4 March 2018).
Ozgoli 2018 {published data only}
- Ozgoli G, IRCT20100503003860N34. The effect of pressure on bile duct 21 on labor pain in primiparous women. https://en.irct.ir/trial/29423 (first received 17 April 2018).
Ranjkesh 2018 {published data only}
- Ranjkesh F, IRCT20171203037731N1. The effect of LI4, H7 and SP6, neima acupressure on the pain severity and duration of delivery in nulliparous women. https://en.irct.ir/trial/29263 (first received 6 June 2018).
Additional references
Adams 2009
- Adams J, Lui C‐W, Sibbritt D, Broom A, Wardle J, Homer C, et al. Women's use of complementary and alternative medicine during pregnancy: a critical review of the literature. Birth 2009;36(3):237‐45. [DOI] [PubMed] [Google Scholar]
Anderson 2012
- Anderson B, Nielsen A, McKee D, Jeffres A, Kligler B. Acupuncture and heart rate variability: a systems level approach to understanding mechanism. Explore: the Journal of Science and Healing 2012;8(2):99‐106. [DOI: 10.1016/j.explore.2011.12.002] [DOI] [PubMed] [Google Scholar]
Anim‐Somuah 2018
- Anim‐Somuah M, Smyth RM, Cyna AM, Cuthbert A. Epidural versus non‐epidural or no analgesia for pain management in labour. Cochrane Database of Systematic Reviews 2018, Issue 5. [DOI: 10.1002/14651858.CD000331.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Barnes 2004
- Barnes P, Powell‐Griner E, McFann K, Nahin R. Complementary and alternative medicine use among adults: United States. CDC Advance Data Report 2002:343. [PubMed]
Barragán 2011
- Barragán Loayza IM, Solà I, Juandó Prats C. Biofeedback for pain management during labour. Cochrane Database of Systematic Reviews 2011, Issue 6. [DOI: 10.1002/14651858.CD006168.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Beinfield 1991
- Beinfield H, Korngold E. Between Heaven and Earth : a Guide to Chinese Medicine (unabridged ed.). New York: Ballantine Books, 1991. [Google Scholar]
Chae 2013
- Chae Y, Chang DS, Lee SH, Jung WM, Lee IS, Jackson S, et al. Inserting needles into the body: a meta‐analysis of brain activity associated with acupuncture needle stimulation. Journal of Pain 2013;14(3):215‐22. [http://www.sciencedirect.com/science/article/pii/S1526590012009613] [DOI] [PubMed] [Google Scholar]
Chaillet 2014
- Chaillet N, Belaid L, Crochetière C, Roy L, Gagné GP, Moutquin JM, et al. Nonpharmacologic approaches for pain management during labor compared with usual care: a meta‐analysis. Birth 2014;41(2):122‐37. [DOI] [PubMed] [Google Scholar]
Cho 2010
- Cho SH, Lee H, Ernst E. Acupuncture for pain relief in labour: a systematic review and meta‐analysis. BJOG: an international journal of obstetrics and gynaecology 2010;117:907‐20. [DOI] [PubMed] [Google Scholar]
Cluett 2018
- Cluett ER, Burns E, Cuthbert A. Immersion in water during labour and birth. Cochrane Database of Systematic Reviews 2018, Issue 5. [DOI: 10.1002/14651858.CD000111.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Derry 2012
- Derry S, Straube S, Moore RA, Hancock H, Collins SL. Intracutaneous or subcutaneous sterile water injection compared with blinded controls for pain management in labour. Cochrane Database of Systematic Reviews 2012, Issue 1. [DOI: 10.1002/14651858.CD009107.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Dick‐Read 2004
- Dick‐Read G. Childbirth Without Fear: the Principles and Practice of Natural Childbirth. London: Pinter & Martin, 2004. [Google Scholar]
Dickenson 2003
- Dickinson JE, Paech MJ, McDonald SJ, Evans SF. Maternal satisfaction with childbirth and intrapartum analgesia in nulliparous labour. Australian & New Zealand Journal of Obstetrics & Gynaecology 2003;43(6):463‐8. [DOI] [PubMed] [Google Scholar]
Dowswell 2009
- Dowswell T, Bedwell C, Lavender T, Neilson JP. Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database of Systematic Reviews 2009, Issue 2. [DOI: 10.1002/14651858.CD007214.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Eisenberg 1998
- Eisenberg DA, Davis RB, Ettner SL, Appel S, Wilky S, Rompay M. Trends in alternative medicine use in the United States, 1990‐1997: results of a follow up national survey. JAMA 1998;280:1569‐75. [DOI] [PubMed] [Google Scholar]
Hicks 2011
- Hicks A, Hicks J, Mole P. Five Element Constitutional Acupuncture. Second Edition. London: Churchill Livingstone, 2011. [Google Scholar]
Higgins 2011
- Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hodnett 2002
- Hodnett ED. Pain and women's satisfaction with the experience of childbirth: A systematic review. American Journal of Obstetrics and Gynacology 2002;186(5):S160‐S172. [DOI] [PubMed] [Google Scholar]
Hollins Martin 2013
- Hollins Martin CJ, Robb Y. Women's views about the importance of education in preparation for childbirth. Nurse Education in Practice 2013;13(6):512‐8. [DOI] [PubMed] [Google Scholar]
Hotelling 2013
- Hotelling BA. The nocebo effect in childbirth classes. Jouranl of Perinatal Education 2013;22(2):120‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Howarth 2010
- Howarth AM, Swain N, Treharne GJ. A review of psychosocial predictors of outcomes in labour and childbirth. New Zealand College of Midwives Journal 2010;42:17‐20. [Google Scholar]
Jones 2011
- Jones L, Dou L, Dowswell T, Alfirevic Z, Neilson JP. Pain management for women in labour: generic protocol. Cochrane Database of Systematic Reviews 2011, Issue 6. [DOI: 10.1002/14651858.CD009167] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jones 2012
- Jones L, Othman M, Dowswell T, Alfirevic Z, Gates S, Newburn M, et al. Pain management for women in labour: an overview of systematic reviews. Cochrane Database of Systematic Reviews 2012, Issue 3. [DOI: 10.1002/14651858.CD009234.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Leap 2010
- Leap N, Dodwell M, Newburn M. Working with pain in labour: an overview of evidence. New Digest 2010;49:22‐6. [Google Scholar]
Levett 2014
- Levett K, Smith CA, Dahlen H, Bensoussan A. Acupuncture and acupressure for pain management in labour and birth: a critical narrative review of current systematic review evidence. Complementary Therapies in Medicine 2014;22:523‐40. [DOI] [PubMed] [Google Scholar]
Levett 2016b
- Levett KM, Dahlen HG, Bensoussan A, Smith CA. Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour. BMJ Open 2016;6(7):e010691. [DOI] [PMC free article] [PubMed] [Google Scholar]
Maciocia 2015
- Maciocia G. The Foundations of Chinese Medicine : a Comprehensive Text. Elesevier, 2015. [Google Scholar]
MacPherson 2008
- MacPherson H, Nahin R, Paterson C, Cassidy CM, Lewith GT, Hammerschlag R. Developments in acupuncture research: big‐picture perspectives from the leading edge. Journal of Alternative and Complementary Medicine 2008;14(7):883‐7. [DOI] [PubMed] [Google Scholar]
MacPherson 2010
- MacPherson H, Altman DG, Hammerschlag R, Li YP, WU TX, White A, et al. Revision of standards for reporting interventions in clinical trials of acupuncture. Chinede Journal of Integrative Medicine 2010;8(9):804‐18. [DOI] [PubMed] [Google Scholar]
Madden 2016
- Madden K, Middleton P, Cyna AM, Matthewson M, Jones L. Hypnosis for pain management during labour and childbirth. Cochrane Database of Systematic Reviews 2016, Issue 5. [DOI: 10.1002/14651858.CD009356.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Maimburg 2016
- Maimburg, RD, Vaeth M, Dahlen H. Women's experience of childbirth‐a five year follow up of the randomised controlled trial "Ready for Child Trial". Women and Birth 2016;5:450‐4. [DOI] [PubMed] [Google Scholar]
Melzack 1965
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965;150(3699):971‐9. [DOI] [PubMed] [Google Scholar]
Melzack 1984
- Melzack R. The myth of painless childbirth. Pain 1984;19:331‐7. [DOI] [PubMed] [Google Scholar]
Melzack 2004
- Melzack R, Katz J. The gate control theory: reaching for the brain. In: Craig KD, Hadjistravroploulos T editor(s). Pain: Psychological Perspectives. Lawrence Erlbaum Associates, 2004. [Google Scholar]
Ng 1992
- Ng LK, Katims JJ, Lee MH. Acupuncture, a neuromodulation technique for pain control. In: Aronoff GM editor(s). Evaluation and Treatment of Chronic Pain. 2nd Edition. Baltimore: Williams & Wilkins, 1992. [Google Scholar]
Othman 2012
- Othman M, Jones L, Neilson JP. Non‐opioid drugs for pain management in labour. Cochrane Database of Systematic Reviews 2012, Issue 7. [DOI: 10.1002/14651858.CD009223.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pomeranz 1989
- Pomeranz B, Stux G. Scientific Bases of Acupuncture. Berlin: Springer‐Verlag, 1989. [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Simmons 2012
- Simmons SW, Taghizadeh N, Dennis AT, Hughes D, Cyna AM. Combined spinal‐epidural versus epidural analgesia in labour. Cochrane Database of Systematic Reviews 2012, Issue 10. [DOI: 10.1002/14651858.CD003401.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2011a
- Smith CA, Collins CT, Crowther CA. Aromatherapy for pain management in labour. Cochrane Database of Systematic Reviews 2011, Issue 7. [DOI: 10.1002/14651858.CD009215] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2017
- Smith CA, Zaslawski CJ, Cochrane S, Zhu X, Zheng Z, Loyeung B, et al. Reliability of the NICMAN Scale: an instrument to assess the quality of acupuncture administered in clinical trials. Evidence‐Based Complementary and Alternative Medicine 2017;2017:Article ID:5694083. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2018a
- Smith CA, Levett KM, Collins CT, Armour M, Dahlen HG, Suganuma M. Relaxation techniques for pain management in labour. Cochrane Database of Systematic Reviews 2018, Issue 3. [DOI: 10.1002/14651858.CD009514.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2018b
- Smith CA, Levett KM, Collins CT, Dahlen HG, Ee CC, Suganuma M. Massage, reflexology and other manual methods for pain management in labour. Cochrane Database of Systematic Reviews 2018, Issue 3. [DOI: 10.1002/14651858.CD009290.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2018c
- Smith LA, Burns E, Cuthbert A. Parenteral opioids for maternal pain management in labour. Cochrane Database of Systematic Reviews 2018, Issue 6. [DOI: 10.1002/14651858.CD007396.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Steel 2014
- Steel A, Adams J, Sibbritt D, Broom A, Frawley J, Gallois C. The influence of complementary and alternative medicine use in pregnancy on labor pain management choices: results from a nationally representative sample of 1,835 women. Journal of Alternative and Complementary Medicine 2014;20(2):87‐97. [DOI] [PubMed] [Google Scholar]
Stener‐Victorin 2006
- Stener‐Victorin E, Fujisawa S, Kurosawa M. Ovarian blood flow responses to electroacupuncture stimulation depend on estrous cycle and frequency of stimulation in anesthetized rates. Journal of Applied Physiology 2006;101:84‐91. [DOI] [PubMed] [Google Scholar]
Stux 1995
- Stux G, Pomeranz B. Basics of Acupuncture. Berlin: Springer‐Verlag, 1995. [Google Scholar]
Trout 2004
- Trout KK. The neuromatrix theory of pain: implications for selected nonpharmacologic methods of pain relief for labor. Journal of Midwifery & Women's Health 2004;49(6):482‐8. [DOI] [PubMed] [Google Scholar]
Zullo 2017
- Zullo A, Mancini FP, Schleip R, Wearing S, Yahia L, Klingler W. The interplay between fascia, skeletal muscle, nerves, adipose tissue, inflammation and mechanical stress in musculo‐fascial regeneration. Journal of Gerontology and Geriatrics 217;65:271‐83. [Google Scholar]
References to other published versions of this review
Smith 2006
- Smith CA, Collins CT, Cyna AM, Crowther CA. Complementary and alternative therapies for pain management in labour. Cochrane Database of Systematic Reviews 2006, Issue 4. [DOI: 10.1002/14651858.CD003521.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2011b
- Smith CA, Collins CT, Crowther CA, Levett KM. Acupuncture or acupressure for pain management in labour. Cochrane Database of Systematic Reviews 2011, Issue 7. [DOI: 10.1002/14651858.CD009232] [DOI] [PubMed] [Google Scholar]