

Abstract
The prevalence of obesity in Asia is of epidemic proportions, with an estimated 1 billion overweight/obese individuals in the region. The majority of patients with type 2 diabetes mellitus (T2DM) are overweight/obese, which increases the risk of cardiorenal outcomes in these patients; hence, sustained reductions in body weight and visceral adiposity are important management goals. However, most of the glucose-lowering therapies such as insulin, sulfonylureas, glinides, and thiazolidinediones induce weight gain, which makes the management of overweight/obese T2DM patients challenging. Sodium-glucose cotransporter-2 (SGLT-2) inhibitors are the only oral glucose-lowering agents that have been shown to reduce body weight and visceral adiposity. In addition, SGLT-2 inhibitors therapy reduces ectopic fat deposition and improves adipose tissue function and weight-related quality of life. In this article, we aim to consolidate the existing literature on the effects of SGLT-2 inhibitors in Asian patients with T2DM and to produce clinical recommendations on their use in overweight or obese patients with T2DM. Recommendations from international and regional guidelines, as well as published data from clinical trials in Asian populations and cardiovascular outcomes trials are reviewed. Based on the available data, SGLT-2 inhibitors represent an evidence-based therapeutic option for the management of overweight/obese patients with T2DM.
Keywords: Diabetes mellitus, type 2; Obesity; Sodium-glucose transporter 2 inhibitors
INTRODUCTION
Obesity is a serious global health concern and is a major contributing factor to the development of type 2 diabetes mellitus (T2DM). The pathophysiology of obesity and T2DM is closely linked with insulin resistance, which plays a key role in the dysregulation of glucose, lipid, and protein metabolism [1]. The chronic positive net energy balance increases adiposity and circulating levels of free fatty acids (FFAs), which accelerate the development of T2DM through impaired hepatic and peripheral glucose metabolism, reduced insulin clearance, impaired pancreatic β-cell function, ectopic fat deposition, and activation of pro-inflammatory pathways [2,3].
The measures of abdominal adiposity, such as waist circumference (WC), correlate with insulin resistance and markers of cardiovascular disease (CVD) better than body mass index (BMI) does [4,5]. Asian populations have higher abdominal obesity for the same BMI compared with their Caucasian counterparts, partly explaining the higher insulin resistance and excessive risk of T2DM and CVD among Asian populations [6,7]. Sniderman et al. [8] proposed that the superficial subcutaneous fat compartment is less developed, with a reduced storage capacity, in South Asians compared with Caucasians, which results in the preferential distribution of fat in visceral or deep subcutaneous depots. The underlying reason for this less developed superficial subcutaneous compartment has been suggested to be the heat stress or the chronic energy deficiency from malnutrition in the evolutionary past, resulting in a preference for the highly vascular visceral adipose tissue with high lipolytic activity [8,9]. The harmful effects of higher abdominal obesity in Asians are well recognized, and the World Health Organization (WHO)'s expert committee has recommended a lower BMI level as an actionable cutoff for the risk of T2DM and CVD in Asians (23 kg/m2 vs. 25 kg/m2 in Caucasians) [10]. For WC, the WHO provided gender-specific cutoff points for the risk of metabolic complications: 94 cm (men) and 80 cm (women) for increased risk, and 102 cm (men) and 88 cm (women) for the substantially increased risk [11]. Population and geography-specific WC cutoffs are provided by the International Diabetes Federation and these are lower for Asian men compared with their Caucasian counterparts: 90 cm (men) and 80 cm (women) for South Asian, Chinese, and Japanese populations versus 94 cm (men) and 80 cm (women) for Caucasians [12]. In Korea, the appropriate WC cutoff for the risk of metabolic syndrome was determined to be 90 cm in men and 85 cm in women [13].
It has been well recognized that weight reduction is a key strategy in the management of obese patients with T2DM. However, most of the glucose-lowering therapies, including insulin, sulfonylureas (SUs), glinides, and thiazolidinediones (TZDs), induce weight gain. The recently introduced glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium- glucose cotransporter-2 (SGLT-2) inhibitors have been shown to reduce body weight and have become the preferred agents for the management of overweight/obese patients with T2DM [14,15]. Previously, we reviewed the effects of SGLT-2 inhibitors on various cardiovascular (CV) risk factors, and developed expert recommendations on the clinical use of SGLT-2 inhibitors in Asian T2DM patients with CVD or multiple risk factors [16]. In the present article, we aim to review and consolidate the existing literature on the effects of SGLT-2 inhibitors on body weight and adiposity in Asian patients with T2DM. We then produced a series of clinical recommendations on the use of SGLT-2 inhibitors in overweight/obese patients with T2DM.
EPIDEMIOLOGY AND ASSOCIATED COMPLICATIONS OF OVERWEIGHT/OBESITY AND T2DM IN ASIA
The worldwide prevalence of overweight adults aged >18 years is estimated to be about 1.9 billion (39% of adults worldwide), and that of obesity is approximately 650 million (13% of adults worldwide) [17,18]. Data from the Global Burden of Disease Study show that high BMI accounts for 4 million deaths annually, of which more than two-thirds are due to CVD [19]. In addition, high BMI contributes to 120 million disability-adjusted life-years. Of note, about 34% of high BMI-related deaths and 32% of disability-adjusted life-years occur in individuals with BMI 25 to 30 kg/m2.
In the Asia Pacific region, an estimated 1 billion people (40.9%) are overweight/obese (2013 data; using BMI cutoff of 25 kg/m2 for overweight and 30 kg/m2 for obesity) [20]. The Global Burden of Disease Study reported region-wise prevalence estimates for overweight and obese adults. Within Asia Pacific, the prevalence of overweight and obesity is as follows: Australasia 68.6% (men) and 56.7% (women), East Asia 28.0% (men) and 27.1% (women), Southeast Asia 22.1% (men) and 28.3% (women), South Asia 20.2% (men) and 22.5% (women), and high-income Asian countries (Brunei, Japan, Singapore, and South Korea) 31.7% (men) and 20.6% (women) [19]. Also, the region accounts for about 56.7% of the global diabetes prevalence, with 158.8 million (9.5%) and 82 million (8.5%) adults with diabetes in the Western Pacific and Southeast Asia regions, respectively [21]. Over 85% of all T2DM patients are either overweight or obese, rendering a vast majority of T2DM patients at high risk of CV morbidity and mortality [22]. In the Joint Asia Diabetes Evaluation (JADE) program involving 3,687 patients from nine Asian countries, 30.1% (range, 20.8% to 38.7%) of patients with T2DM had a BMI of ≥27.5 kg/m2 and 53.5% (range, 19.4% to 76.4%) had abdominal obesity (WC ≥80 cm in women or ≥90 cm in men) [23]. Data from the Korea National Health and Nutrition Examination Survey, a nationally representative survey of the Korean population, showed that 50.4% of Korean patients with T2DM were obese (BMI ≥25 kg/m2) and 47.8% have abdominal obesity (WC ≥85 cm in women or ≥90 cm in men) [24].
Obesity increases the risk of hypertension, dyslipidemia, and coronary heart diseases in patients with T2DM. In addition, obesity and T2DM are chronic inflammatory states that further increase the risk of CV and cerebrovascular complications [25,26,27]. A pooled data analysis of 33 cohort studies (n=310,283; mean follow-up 6.9 years) by the Asia Pacific Cohort Studies Collaboration (APCSC) showed that each 2-units' decrease in BMI is associated with a 12% lower risk of ischemic stroke and 11% lower risk of ischemic heart disease [28]. Another pooled data analysis by APCSC involving six cohort studies in adults aged ≥20 years (n=45,988; mean follow-up 6.1 years) revealed that each standard deviation increase in BMI, WC, and the waist-to-hip ratio increases the risk of ischemic heart disease by 17% to 36% [29]. Also, metabolic syndrome is independently associated with ischemic heart disease and ischemic stroke [30].
A U-shaped relationship has been reported between BMI and mortality due to heart failure (HF), with a >60% higher risk of HF mortality in both underweight and obese individuals compared with healthy-weight individuals [31]. A pooled analysis of the Framingham Heart, Framingham Offspring, Chicago Heart Association Detection Project in Industry, and Atherosclerosis Risk In Communities (ARIC) studies evaluated the risk of incident HF in individuals with or without hypertension, obesity, or diabetes. Men and women without hypertension, obesity, or diabetes at the age of 45 years have 73% and 85% lower risk of incident HF compared with those with all three risk factors, respectively. In addition, individuals without any of the three risk factors at the age of 45 years live 3 to 15 years longer, free of HF, than those with one, two, or all three risk factors [32].
Furthermore, obesity is independently associated with the development and progression of chronic kidney disease (CKD) [33]. Results from the Renal and Vascular End-Stage Disease (PREVEND) study showed that obesity and central fat distribution are associated with a 1.7-fold higher risk of microalbuminuria and 2.7-fold higher risk of decreased glomerular filtration rate [34]. Similarly, a multinational, observational study of 20,828 outpatients with hypertension from 26 countries in Europe, North and Latin America, the Middle East, and Asia, showed that abnormal WC is associated with microalbuminuria, independent of BMI [35]. A retrospective analysis of National Diabetes Audit data (United Kingdom) showed that patients with T2DM and severe kidney disease (estimated glomerular filtration rate [eGFR] <30 mL/min/1.73 m2) are up to 1.75 times more likely to be obese compared with those with normal kidney function [36]. Furthermore, the risk of CKD (eGFR <60 mL/min/1.73 m2) is increased by 55% in the presence of metabolic syndrome [37].
The chronic elevation of circulatory FFAs and reduced FFA oxidation in obese individuals lead to ectopic fat deposition in non-adipose tissues, such as liver, skeletal muscle, heart, and pancreatic β-cells. Non-alcoholic fatty liver disease (NAFLD) is frequently reported in obese T2DM patients, which may increase the risk of non-alcoholic steatohepatitis, cirrhosis, and hepatocellular cancer [38].
There is a positive association between the presence of diabetes and high BMI (>25 kg/m2) and the incidence of cancer. Pearson-Stuttard et al. [39] analyzed the incidence of malignancies attributable to diabetes and high BMI as a combined risk factor, across 175 countries. Overall, 5.7% of all incident cancers are attributable to the combined effects of diabetes and high BMI as independent risk factors [39]. Of these 804,100 cancer cases, 23.8% occurred in East and Southeast Asia. Among the specific cancer types, 24.5% of liver cancer and 38.4% of endometrial cancer cases are attributable to these risk factors [39].
Furthermore, obstructive sleep apnea is prevalent in patients with abdominal obesity and may adversely affect glucose control in patients with T2DM [40].
CURRENT GUIDELINES FOR THE MANAGEMENT OF OVERWEIGHT/OBESE PATIENTS WITH T2DM
The clinical practice guidelines from Asian countries for the management of T2DM recommend a weight loss goal of 5% to 10% to improve glycemic control, blood pressure, lipid profile and quality of life (QoL) in overweight/obese patients with T2DM [41,42,43,44,45]. Similarly, guidelines from Western countries recommend a weight loss goal of 5% to 15% in these patients [14,46,47].
For the management of hyperglycemia in overweight/obese patients with T2DM, the guidelines recommend the use of glucose-lowering drugs (GLDs) that promote weight loss or that are weight-neutral [15,48]. Insulin secretagogues, such as SUs, and glinides have been shown to increase body weight in T2DM patients [49,50]. TZDs are associated with weight gain in the range of 3.6 kg (at 3 years) to 4.8 kg (at 5 years) in large randomized controlled trials [51,52]. Several meta-analyses investigating the effect of oral GLDs on body weight showed that the addition of SUs, TZDs, and glinides to metformin is associated with significant weight gain in patients with T2DM (range, 1 to 5 kg) [53,54]. Conversely, metformin, α-glucosidase inhibitors, and dipeptidyl peptidase-4 (DPP-4) inhibitors have a neutral effect on body weight [54,55,56]. Currently, GLDs that promote weight loss include SGLT-2 inhibitors and GLP-1 RAs. The 2018 guidelines from the American Diabetes Association and the European Association for the Study of Diabetes provided a treatment algorithm for patients with a compelling need to minimize weight gain or promote weight loss, and recommended either GLP-1 RAs or SGLT-2 inhibitors as the preferred choice of therapy after metformin [57].
Methods
An expert panel comprising 12 endocrinology experts from China, Hong Kong, India, Indonesia, Malaysia, the Philippines, Singapore, South Korea, Taiwan, Thailand, and Vietnam met four times (Bangkok, November 2017; Shanghai, March 2018; Orlando, June 2018; Kuala Lumpur, November 2018) to review the clinical evidence and develop clinical recommendations on the use of SGLT-2 inhibitors in overweight/obese Asian patients with T2DM. A literature search was conducted in the MEDLINE database using the search string: (“canagliflozin” OR “dapagliflozin” OR “empagliflozin” OR “ipragliflozin” OR “luseogliflozin” OR “tofogliflozin”) AND “type 2 diabetes.” The panel critically analyzed the studies of SGLT-2 inhibitors conducted in Asia as well as recommendations from international and regional guidelines. Following discussions, the group reached consensus on a series of recommendations supported by scientific evidence and experts' clinical opinion.
ROLE OF SGLT-2 INHIBITORS IN MANAGING OVERWEIGHT/OBESE PATIENTS WITH T2DM: AN ASIAN PERSPECTIVE
SGLT-2 inhibitors selectively and reversibly inhibit SGLT-2 transporters in the proximal convoluted tubule, preventing the renal reabsorption of glucose, thereby increasing urinary glucose excretion. The glucose-lowering effects of SGLT-2 inhibitors are independent of insulin function; hence, they are effective at all stages of T2DM [58]. The glycemic efficacy and safety of SGLT-2 inhibitors as monotherapy or in combination with other GLDs are well established. Results from three CV outcomes trials (EMPA-REG OUTCOME, CANVAS, DECLARE-TIMI 58) showed beneficial effects of SGLT-2 inhibitors in reducing the risk of CV outcomes in patients with T2DM [59,60,61].
In the DECLARE-TIMI 58 trial, dapagliflozin treatment reduced the body weight by −1.8 kg compared with placebo at the median follow-up of 4.2 years [60]. Similar results are reported with empagliflozin and canagliflozin in the EMPA-REG OUTCOME and CANVAS trials respectively [59,61]. In all three cardiovascular outcome trials (CVOTs) the beneficial CV effects of SGLT-2 inhibitors were consistent across BMI subgroups (<30 or ≥30 kg/m2). Furthermore, in a meta-analysis of 55 randomized controlled trials, SGLT-2 inhibitor treatment was associated with a consistent and significant reduction in body weight with a dose-dependent response observed for dapagliflozin [62]. A recent, single-center real-world study from India including 486 patients with T2DM reported a mean weight loss of 3.2 and 3.9 kg with SGLT-2 inhibitor therapy at 6 and 12 months, respectively [63].
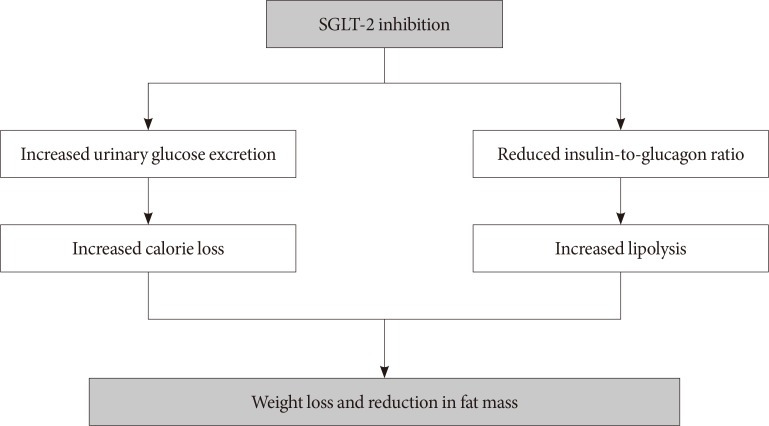
These effects of SGLT-2 inhibitors on body weight are of particular significance for overweight/obese patients with T2DM, in whom consistent weight loss and reduction in fat mass are critical for effective management (Fig. 1). In the following sections, we summarize the effects of SGLT-2 inhibitors on body weight, fat mass, and adipose tissue function in Asian T2DM patients.
Fig. 1. Proposed mechanisms of effects of sodium-glucose cotransporter-2 (SGLT-2) inhibitors on body weight and fat mass.
Effects on body weight in patients with T2DM
In Western populations, SGLT-2 inhibitor treatment induces a weight loss as monotherapy (weighted mean difference vs. placebo: −1.74 kg; 95% confidence interval [CI], −2.03 to −1.45) and as combination therapy (weighted mean difference vs. other GLDs: −1.80 kg; 95% CI, −3.50 to −0.11 kg) [64]. Similar results are observed in Asian patients with T2DM. Treatment with SGLT-2 inhibitors resulted in a significant reduction in body weight, ranging from −0.5 to −3.9 kg (study duration range, 8 to 104 weeks). The effect of SGLT-2 inhibitors on body weight in Asian patients with T2DM is summarized in Table 1 [65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106].
Table 1. Effect of SGLT-2 inhibitors on body weight and waist circumference in Asian patients with T2DM.
| Study | Design and population | Intervention | Effect on body weight | Effect on waist circumference |
|---|---|---|---|---|
| Monotherapy | ||||
| Inagaki et al. (2013) [79] | Phase II, 12-wk randomized study; Japanese T2DM (n=383) | Canagliflozin (50, 100, 200, or 300 mg); placebo | −1.98 kg (50 mg); −2.51 kg (100 mg); −2.39 kg (200 mg); −3.19 kg (300 mg); −0.78 kg (placebo) | −1.59 cm (50 mg), −1.81 cm (100 mg), −1.83 cm (200 mg), −2.21 cm (300 mg); −0.59 cm (placebo) |
| Inagaki et al. (2014) [73] | Phase III, 24-wk double-blind randomized study; Japanese T2DM (n=272) | Canagliflozin (100, 200 mg); placebo | −3.76% (100 mg), −4.02% (200 mg); −0.76% (placebo) | −2.21 cm (100 mg); −2.82 cm (200 mg); −1.03 cm (placebo) |
| Kaku et al. (2013) [80] | Phase II, 12-wk randomized study; Japanese T2DM (n=279) | Dapagliflozin (1, 2.5, 5, or 10 mg/day); placebo | −1.25 kg (1 mg); −1.24 kg (2.5 mg); −2.06 kg (5 mg); −1.91 kg (10 mg); −0.05 (placebo) | - |
| Ji et al. (2014) [74] | Phase III, 24-wk double-blind randomized study; drug-naïve Asian T2DM (n=393) | Dapagliflozin (5 or 10 mg); placebo | −1.64 kg (5 mg); −2.25 kg (10 mg); −0.27 kg (placebo) | −2.77 cm (5 mg); −2.20 cm (10 mg); −0.72 cm (placebo) |
| Kaku et al. (2014) [81] | Phase III, 24-wk double-blind randomized study; Japanese T2DM (n=261) | Dapagliflozin (5 or 10 mg); placebo | −2.13 kg (5 mg); −2.22 kg (10 mg); −0.84 kg (placebo) | - |
| Kadowaki et al. (2014) [82] | Phase II, 12-wk randomized study; Japanese T2DM (n=547) | Empagliflozin (5, 10, 25, or 50 mg); placebo | −2.5 kg (5 mg); −2.6 kg (10 mg); −2.9 kg (25 mg); −3.1 kg (50 mg); −0.9 kg (placebo) | −2.4 cm (5 mg); −2.3 cm (10 mg); −2.6 cm (25 mg); −2.6 cm (50 mg); −1.3 cm (placebo) |
| Kadowaki et al. (2015) [75] | 40-wk extension study; Japanese T2DM (n=532) | Empagliflozin (10, 25 mg) | −3.1 kg (10 mg); −3.1 kg (25 mg) | −2.8 cm (10 mg); −2.8 cm (25 mg) |
| Kashiwagi et al. (2014) [66] | Phase II, 12-wk randomized study; Japanese T2DM (n=361) | Ipragliflozin (12.5, 25, 50, or 100 mg/day); placebo | −1.46 kg (12.5 mg); −1.69 kg (25 mg); −1.81 kg (50 mg); −2.1 kg (100 mg); −0.39 kg (placebo) | - |
| Kashiwagi et al. (2015) [83] | Phase III, 16-wk double-blind randomized study; Japanese T2DM (n=131) | Ipragliflozin (50 mg); placebo | −2.31 kg (50 mg); −1.03 kg (placebo) | −1.61 cm (50 mg); −0.41 cm (placebo) |
| Seino et al. (2015) [67] | 52-wk open-label study; Japanese T2DM (n=299) | Luseogliflozin (2.5 mg, option to uptitrate to 5 mg) | 12 wk: −1.77 kg (2.5/5 mg) 24 wk: −1.91 kg (2.5/5 mg) 36 wk: −2.35 kg (2.5/5 mg) 52 wk: −2.68 kg (2.5/5 mg) | - |
| Hirose et al. (2016) [84] | 8-wk open-label study (n=17) | Tofogliflozin (20 mg) | −1.1 kg (20 mg) | - |
| Kaku et al. (2014) [65] | Phase II/III, 24-wk double-blind randomized study; Japanese T2DM (n=235) | Tofogliflozin (10, 20, or 40 mg); placebo | −2.23 kg (10 mg); −2.85 kg (20 mg); −2.97 kg (40 mg); −0.36 kg (placebo) | −2.42 cm (10 mg); −2.47 cm (20 mg); −2.27 cm (40 mg); 0.02 cm (placebo) |
| Add-on to oral antidiabetic agents | ||||
| Ji et al. (2015) [85] | Phase III, 18-wk double-blind randomized study; Asian T2DM (n=678) | Canagliflozin (100, 300 mg)+Met or SU+Met; placebo | −1.9 kg (100 mg); –2.1 kg (300 mg); –0.5 kg (placebo) | - |
| Inagaki et al. (2015) [72] | 52-wk open-label randomized study; Japanese T2DM (n=1,299) | Canagliflozin (100, 200 mg); other GLDs | −4.42% (100 mg); −4.70% (200 mg); −2.94% (100 mg+SU); −3.51% (200 mg+SU); −3.97% (100 mg+glinide); −4.37% (200 mg+glinide); −4.03% (100 mg+α-GI); −4.98% (200 mg+α-GI); −4.42% (100 mg+BG); −5.54% (200 mg+BG); −3.37% (100 mg+TZD); −3.43% (200 mg+TZD); −4.00% (100 mg+DPP-4i); −4.37% (200 mg+DPP-4i) | −2.76 cm (100 mg); −3.34 cm (200 mg); −1.96 cm (100 mg+SU); −1.72 cm (200 mg+SU); −2.93 cm (100 mg+glinide); −3.24 cm (200 mg+glinide); −2.27 cm (100 mg+α-GI); −2.57 (200 mg+α-GI); −3.40 cm (100 mg+BG); −3.82 cm (200 mg+BG); −3.12 cm (100 mg+TZD); −2.64 cm (200 mg+TZD); −3.34 cm (100 mg+DPP-4i); −2.37 cm (200 mg+DPP-4i) |
| Kadowaki et al. (2017) [86] | Phase III, 24-wk double-blind randomized study; Japanese T2DM (n=138) | Canagliflozin (100 mg); teneligliptin; placebo | −2.29 kg (100 mg+teneligliptin); −0.78 kg (placebo+teneligliptin) | - |
| Kadowaki et al. (2018) [87] | 52-wk open-label study; Japanese T2DM (n=153) | Canagliflozin (100 mg); teneligliptin | −2.86 kg (100 mg+teneligliptin) | - |
| Harashima et al. (2018) [68] | Phase IV, 52-wk open-label; Japanese T2DM (n=71) | Canagliflozin (100 mg); liraglutide | −3.29 kg (100 mg+liraglutide) | −3.39 cm (100 mg+liraglutide) |
| Kaku et al. (2014) [81] | Phase III, 52-wk open-label study; Japanese T2DM (n=728) | Dapagliflozin (5 mg, option to uptitrate to 10 mg); other GLDs | −2.6 kg (monotherapy); −2.1 kg (combination therapy) | −2.1 cm (monotherapy); −2.0 cm (combination therapy) |
| Yang et al. (2016) [78] | Phase III, 24-wk randomized doubleblind study; Asian T2DM (n=444) | Dapagliflozin (5, 10 mg); Met; placebo | −1.8 kg (5 mg+Met); −2.6 kg (10 mg+Met); −0.7 kg (placebo+Met) | −1.96 cm (5 mg+Met); −2.15 cm (10 mg+Met); −0.39 cm (placebo+Met) |
| Araki et al. (2015) [88] | Phase III, 52-wk randomized study; Japanese T2DM (n=1,160) | Empagliflozin (10, 25 mg); other GLDs | SU: −2.3 kg (10 mg+SU); −2.8 kg (25 mg+SU) BG: −3.9 kg (10 mg+BG); −3.4 kg (25 mg+BG) TZD: −2.6 kg (10 mg+TZD); −2.8 kg (25 mg+TZD) α-GI: −3.8 kg (10 mg+α-GI); −3.4 kg (25 mg+α-GI) DPP-4i: −2.9 kg (10 mg+DPP-4i); −2.8 kg (25 mg+DPP-4i) Glinide: −2.6 kg (10 mg+glinide); −3.1 kg (25 mg+glinide) | - |
| Kashiwagi et al. (2015) [89] | Phase III, 24-wk randomized study; Japanese T2DM (n=168) | Ipragliflozin (50 mg); Met; placebo | −2.33 kg (50 mg+Met); −0.63 kg (placebo+Met) | −2.39 cm (50 mg+Met); −0.48 cm (placebo+Met) |
| Lu et al. (2016) [76] | Phase III, 24-wk randomized doubleblind study; Asian T2DM (n=171) | Ipragliflozin (50 mg); Met; placebo | −2.93 kg (50 mg+Met); −1.70 kg (placebo+Met) | −1.72 cm (50 mg+Met); −0.85 cm (placebo+Met) |
| Kashiwagi et al. (2015) [90] | Phase III, 24-wk randomized doubleblind study; Japanese T2DM (n=152) | Ipragliflozin (50 mg); pioglitazone; placebo | −2.29 kg (50 mg+pioglitazone); 0.51 kg (placebo+pioglitazone) | −1.82 cm (50 mg+pioglitazone); 0.14 cm (placebo+pioglitazone) |
| Kashiwagi et al. (2015) [91] | Phase III, 24-wk randomized doubleblind study; Japanese T2DM (n=243) | Ipragliflozin (50, 100 mg); SU; placebo | −2.33 kg (50 mg+SU); −0.88 kg (placebo+SU) | −1.61 cm (50 mg+SU); −0.87 cm (placebo+SU) |
| Seino et al. (2018) [69] | 52-wk, open-label study; Japanese T2DM (n=76) | Luseogliflozin (2.5 mg, option to uptitrate to 5 mg); liraglutide | 12 wk: −1.65 kg (2.5/5 mg+GLP-RA) 12 wk: −2.52 kg (2.5/5 mg+GLP-RA) 36 wk: −2.86 kg (2.5/5 mg+GLP-RA) 52 wk: −2.71 kg (2.5/5 mg+GLP-RA) | 12 wk: −1.39 cm (2.5/5 mg+GLP-RA) 12 wk: −2.63 cm (2.5/5 mg+GLP-RA) 36 wk: −3.09 cm (2.5/5 mg+GLP-RA) 52 wk: −2.86 cm (2.5/5 mg+GLP-RA) |
| Ikeda et al. (2015) [92] | Phase II, 12-wk randomized, doubleblind study (n=398) | Tofogliflozin (2.5, 5, 10, 20, or 40 mg); Met; placebo | −1.56 kg (2.5 mg+Met); −1.85 kg (5 mg+Met); −2.24 kg (10 mg+Met); −2.55 kg (20 mg+Met); −2.82 kg (40 mg+Met); −0.74 kg (placebo+Met) | - |
| Add-on to insulin | ||||
| Inagaki et al. (2016) [93] | Phase IV, 16-wk double-blind randomized study; Japanese T2DM (n=146) | Canagliflozin (100 mg); insulin; placebo | −1.49 kg (100 mg+insulin); 0.15 kg (placebo+insulin) | - |
| Inagaki et al. (2018) [94] | Phase IV, 52-wk (16-wk double-blind randomized placebocontrolled study+36wk open-label extension); Japanese T2DM (n=146) | Canagliflozin (100 mg); insulin; placebo | −0.99 kg (placebo+insulin → 100 mg+insulin); −1.52 kg (100 mg+insulin → 100 mg+insulin) | - |
| Araki et al. (2016) [70] | Phase IV, 16-wk double-blind randomized placebo-controlled study; Japanese T2DM (n=182) | Dapagliflozin (5 mg); insulin; placebo | −0.55 kg (5 mg+insulin); 0.66 kg (placebo+insulin) | Placebo-corrected mean reduction: −1.00 cm |
| Araki et al. (2017) [71] | 36-wk open-label extension of Araki et al. 2016 [70] (n=175) | Dapagliflozin (5 mg); insulin | −1.5 kg (5 mg+insulin → 5 mg+insulin); −1.37 kg (placebo+insulin → 100 mg+insulin) | −1.4 cm (5 mg+insulin → 5 mg+insulin); −0.9 cm (placebo+insulin → 100 mg+insulin) |
| Yang et al. (2018) [95] | Phase III, 24-wk randomized doubleblind study; Asian T2DM (n=272) | Dapagliflozin (10 mg); insulin; placebo | −1.00 kg (10 mg+insulin); 0.37 kg (placebo+insulin) | −0.70 cm (10 mg+insulin); 0.00 cm (placebo+insulin) |
| Ishihara et al. (2016) [96] | Phase IV, 16-wk double-blind randomized placebo-controlled study; Japanese T2DM (n=262) | Ipragliflozin (50 mg); insulin; placebo | −1.09 kg (10 mg+insulin); −0.05 kg (placebo+insulin) | −1.36 cm (10 mg+insulin); −0.84 cm (placebo+insulin) |
| Seino et al. (2018) [77] | Phase IV, 52-wk (16-wk double-blind randomized placebo-controlled study+36-wk openlabel extension); Japanese T2DM (n=233) | Luseogliflozin (2.5 mg); insulin; placebo | −1.32 kg (2.5 mg+insulin); −0.05 kg (placebo+insulin) | −1.16 cm (2.5 mg+insulin); 0.04 cm (placebo+insulin) |
| Terauchi et al. (2017) [97] | Phase IV, 16-wk double-blind randomized placebo-controlled study; Japanese T2DM (n=211) | Tofogliflozin (20 mg); insulin; placebo | −1.34 kg (20 mg+insulin); 0.03 kg (placebo+insulin) | - |
| Terauchi et al. (2018) [98] | 36-wk open-label extension of Terauchi et al. (2017) [97] (n=210) | Tofogliflozin (20 mg); insulin | −1.52 kg (20 mg+insulin → 20 mg+insulin); −2.13 kg (placebo+insulin → 20 mg+insulin) | - |
| Suzuki et al. (2016) [99] | 24-wk randomized active-controlled study; Japanese T2DM (n=53) | Tofogliflozin (20 mg); insulin; insulin glargine | 0.6 kg (insulin); −2.9 kg (20 mg+insulin); −3.4 kg (20 mg+insulin glargine) | - |
| Pooled analyses | ||||
| John et al. (2016) [100] | Pooled data from four 26-wk placebo-controlled studies (n=2,313) and a 104-wk active-controlled study (n=1,450) in T2DM patients in hot climate countries | Canagliflozin (100, 300 mg); placebo; glim+Met; canagliflozin (100, 300 mg)+Met | Placebo-controlled trials Hot climate subset: −1.9 kg (100 mg); −2.4 (300 mg); −0.3 kg (placebo) Other climate subset: −2.8 kg (100 mg); −3.4 kg (300 mg); −0.7 kg (placebo) Active-controlled trials Hot climate subset: −2.6 kg (100 mg+Met); −2.8 (300 mg+Met); +1.3 (glim+Met) Other climate subset: −3.9 kg (100 mg+Met); −3.9 (300 mg+Met); 0.6 (glim+Met) | - |
| Yang et al. (2017) [101] | Pooled data from eight Phase IIb/III double-blind placebo-controlled trials of up to 24 wk (n=1,453) | Dapagliflozin (5, 10 mg); placebo | −1.9 kg (5 mg); −2.4 kg (10 mg); −0.6 kg (placebo) | - |
| Yoon et al. (2016) [102] | Pooled data from four Phase III trials up to 24 wk (n=1,326) | Empagliflozin (10, 25 mg); placebo, other GLDs | Pooled data: −1.6 kg (10 mg); −1.8 kg (10 mg) Monotherapy: −1.7 kg (10 mg); −2.1 kg (25 mg) Met: −1.4 kg (10 mg+Met); −1.5 kg (10 mg+Met) Met+SU: −1.5 kg (10 mg+Met+SU); −1.9 kg (10 mg+Met+SU) Pioglitazone: −2.0 kg (10 mg+pioglitazone); −1.7 kg (10 mg+pioglitazone) | |
| Prasanna Kumar et al. (2016) [103] | Pooled subgroup analysis of patients enrolled from India (n=124) in four randomized Phase III trials | Canagliflozin (100, 300 mg); placebo; other GLDs | Overall population: −2.6 (100 mg); −3.3 (300 mg) Indian subgroup: −1.7 (100 mg); −2.2 (300 mg) | |
| Seino et al. (2015) [104] | Pooled analysis of two 52-wk studies; Japanese T2DM (n=708) | Luseogliflozin (2.5 mg); other GLDs | SU: −2.23 kg (2.5 mg+SU) BG: −2.86 kg (2.5 mg+BG) DPP-4i: −1.96 kg (2.5 mg+DPP-4i) TZD: −2.32 kg (2.5 mg+TZD) Glinide: −2.88 kg (2.5 mg+glinide) α-GI: −2.80 kg (2.5 mg+α-GI) SU+placebo (24 wk): 0.16 kg (placebo+SU) | |
| Post-marketing study | ||||
| Utsunomiya et al. (2017) [105] | 1-yr prospective, observational, postmarketing study (n=1,424) | Tofogliflozin | −1.18 kg (4 wk); −1.81 kg (12 wk); −2.01 kg (24 wk); −1.72 kg (36 wk); −2.55 (52 wk) | |
| Nakamura et al. (2018) [106] | 24-mo post-marketing surveillance study (n=8,757) | Ipragliflozin | −1.32 kg (1 mo); −2.16 kg (3 mo); −2.45 kg (6 mo); −2.81 kg (12 mo); −3.11 (24 mo) |
SGLT-2, sodium glucose cotransporter-2; T2DM, type 2 diabetes mellitus; GLD, glucose-lowering drug; SU, sulfonylurea; α-GI, alpha glucosidase inhibitor; BG, biguanide; TZD, thiazolidinedione; DPP-4i, dipeptidyl peptidase-4 inhibitor; Met, metformin; GLP-RA, glucagon-like peptide-1 receptor agonist; glim, glimepiride.
As monotherapy in treatment-naïve Asian and Japanese patients with T2DM, consistent reduction in body weight is observed with dapagliflozin (range, −1.24 to −2.25 kg), canagliflozin (range, −1.98 to −3.19 kg), and empagliflozin treatments (range, −2.5 to −3.1 kg) (study duration up to 24 weeks) (Table 1). Similar effects are observed with ipragliflozin, luseogliflozin, and tofogliflozin, with body weight reductions ranging from −1.1 to −2.97 kg (study duration of 8 to 52 weeks) (Table 1) [65,66,67].
The reduction in body weight is also reported when SGLT-2 inhibitors are used in combination with other oral GLDs (range, −1.56 to −3.9 kg; study duration up to 52 weeks) (Table 1). Two studies reported on the effects of canagliflozin and luseogliflozin as an add-on to GLP-1 RAs in Japanese patients with T2DM. Addition of canagliflozin 100 mg to GLP-1 RAs resulted in a body weight reduction of −3.29 kg (4.46%) at 52 weeks [68]. Luseogliflozin as an add-on to liraglutide was associated with significant weight loss (−2.71 kg), with 33.9% of patients achieving a ≥5% reduction at 52 weeks [69]. Furthermore, the 28-week DURATION-8 trial demonstrated comparable effects of an SGLT-2 inhibitor (dapagliflozin) and GLP-1 RA (exenatide) on body weight (−2.22 kg vs. −1.56 kg, respectively), whereas an additive effect was observed with combination therapy (−3.55 kg). As GLP-1 RAs also exert weight-lowering effects, these results indicate additive effects of SGLT-2 inhibitors and GLP-1 RAs on weight reduction.
The weight-lowering effects of SGLT-2 inhibitors are consistent even when used as an add-on to insulin therapy. In studies with follow-up of up to 52 weeks, weight reduction with SGLT-2 inhibitor treatment ranged from −0.5 to −3.4 kg [70].
Effect on abdominal adiposity
In Western populations, SGLT-2 inhibitor treatment reduces WC by about −1.20 cm (weighted mean difference vs. placebo; 95% CI, −2.00 to −0.43) [107]. Similar results are observed in Asian patients with T2DM. Across the studies in patients with T2DM, treatment with SGLT-2 inhibitors reduced WC as monotherapy (range, −1.59 to −2.82 cm), or in combination with other oral GLDs (range, −1.39 to −3.82 cm) or in combination with insulin (range, −0.7 to −1.4 cm) [65,70,71,72,73,74,75,76,77,78,108]. Table 1 summarizes the effects of SGLT-2 inhibitors on WC in Asian T2DM patients.
In addition, Ohta et al. [109] evaluated the effects of ipragliflozin on intrahepatic lipid content and subcutaneous and visceral fat volume in Japanese T2DM patients. Treatment with ipragliflozin for 24 weeks was associated with significant reductions in subcutaneous and visceral fat volume, intrahepatic lipid content and fat mass, and appendicular skeletal mass indices. In another 12-month study in obese Japanese T2DM patients (n=20), treatment with ipragliflozin significantly reduced both visceral and subcutaneous fat volume at 3 months; the reduction in subcutaneous fat volume remained significant at 12 months follow-up [110]. The PRIME-V study compared the effects of ipragliflozin and metformin, as an add-on to DPP-4 inhibitor, on visceral fat reduction in Japanese patients with T2DM. Treatment with ipragliflozin in combination with DPP-4 inhibitor was associated with significant reductions in visceral fat area (P=0.04), subcutaneous fat area (P=0.004), total fat area (P=0.004), and WC (P=0.001), compared with metformin+DPP-4 inhibitor [111].
Furthermore, a 16-week study in Japanese patients with T2DM showed that the decrease in total fat mass accounts for 71% of total body weight reduction induced by SGLT-2 inhibitor treatment, with the remainder due to loss in water volume (22%) [112]. Another study revealed that SGLT-2 inhibitor-induced weight loss is not associated with reduction in the muscle mass [113]. In this study, 6-month treatment with dapagliflozin resulted in a significant reduction in body weight and total fat mass, with no significant effect on skeletal muscle mass and psoas muscle index.
Effect on adipose tissue function
Few studies have assessed the effects of SGLT-2 inhibitors on the adipose tissue in obese Asian patients with T2DM. In a 12-week study of dapagliflozin in obese patients with T2DM, there was a significant increase in the plasma adiponectin and decrease in high-sensitivity C-reactive protein levels but no significant changes in plasminogen activator inhibitor-1 levels [114].
Effect on ectopic fat
Obesity results in ectopic fat deposition which leads to impaired insulin sensitivity, non-alcoholic steatohepatitis, impaired insulin secretion, and diastolic dysfunction [115,116]. The prospective, open-label, randomized E-LIFT study (effect of empagliflozin on liver fat content in patients with T2DM), examined the effect of empagliflozin (10 mg/day as add-on to the standard therapy) on liver fat content (using magnetic resonance imaging-derived proton density fat fraction [MRI-PDFF]) in patients with T2DM and NAFLD. At 20 weeks, treatment with empagliflozin significantly reduced liver fat content (mean MRI-PDFF difference: −4.0%; P<0.0001) and serum alanine aminotransferase levels (−10.9 IU/L; P=0.005), compared with the control group [117]. Another open-label randomized study compared the effects of ipragliflozin and pioglitazone on liver fat content (change in liver-to-spleen [L/S] ratio on computed tomography scan) in patients with T2DM and NAFLD [118]. At 24 weeks, treatment with either ipragliflozin or pioglitazone improved liver fat content, with no significant difference between the two groups (L/S ratio increased by 0.22 in ipragliflozin vs. 0.21 in pioglitazone; P=0.90). In addition, both treatments reduced the levels of serum aspartate transaminase and alanine transaminase [118].
Furthermore, in two 12-week pilot studies, luseogliflozin and ipragliflozin reduced the epicardial fat volume in overweight/ obese patients with T2DM [119,120].
Effect on weight loss-related QoL and treatment satisfaction
Overweight and obesity negatively affect the patient QoL. A placebo-controlled study in patients with T2DM (n=180) evaluated the effect of dapagliflozin on weight change- and health-related quality of life (HRQoL), using the Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes Weight Questionnaire-9 (SHIELD-WQ-9) survey [121]. Treatment with dapagliflozin was associated with improvement in most of the HRQoL domains at week 24, 50, and 102, and these changes correlated with the weight loss. Similarly, in a study assessing the treatment satisfaction in overweight patients with T2DM (n=221) using the Oral Hypoglycemic Agent-Questionnaire (OHA-Q) version 2, treatment with dapagliflozin was associated with a significant improvement in patient-reported treatment satisfaction [122]. Changes in the OHA-Q total score correlated with changes in body weight and glycosylated hemoglobin. Similar results were observed in a pooled analysis of four randomized controlled trials of canagliflozin [123]. A higher proportion of patients receiving canagliflozin reported interest in continuing treatment upon study completion.
RELATIONSHIP BETWEEN SGLT-2 INHIBITOR-INDUCED WEIGHT LOSS AND IMPROVEMENT OF HYPERGLYCEMIA AND CARDIOVASCULAR OUTCOMES
Weight loss might contribute to the CV benefits observed with SGLT-2 inhibitors in multiple trials. The randomized Look AHEAD trial studied the impact of weight loss on the primary prevention of CV outcomes in overweight/obese patients with T2DM [124]. The trial compared the efficacy of intensive lifestyle intervention with diabetes support and education in 5,145 adults with T2DM and a mean BMI of 36.0 kg/m2. After a median follow-up of 9.6 years, lifestyle intervention resulted in a significant weight loss (−8.7% at 1 year, and −6.0% at the end of study) but did not show a beneficial effect on mortality and CV outcomes [124]. However, a recent analysis from the study revealed a significant association between magnitude of weight loss and long-term risk of CV outcomes. Participants from both intensive lifestyle intervention and diabetes support and education groups who achieved a weight loss of >10% had a significantly lower risk of CV outcomes (composite of CV death, myocardial infarction, stroke, or angina hospitalization; hazard ratio, 0.79; 95% CI, 0.64 to 0.98) [125]. In addition, weight loss in the intensive lifestyle intervention group was associated with improved glycemic control, QoL, physical functioning and mobility, and reduced risk of CKD, sleep apnea, urinary incontinence, and depression [126,127,128,129,130,131,132]. In other studies, weight loss interventions such as anti-obesity drugs (orlistat, rimonabant, and sibutramine) and bariatric surgery have been shown to improve CV risk factors (T2DM, hypertension, and hyperlipidemia) in people with obesity [133,134,135].
The mechanism of SGLT-2 inhibitor-induced weight reduction is likely due to calorie loss and diuresis induced by urinary glucose excretion. A study to quantify the effect of SGLT-2 inhibitor-induced calorie loss on body weight showed a difference in the observed and expected weight loss based on urinary energy loss [136]. Over 90 weeks, the mean urinary energy loss with empagliflozin treatment was 206 kcal/day, which was expected to result in a weight loss of −11.3 kg (assuming no compensatory changes in energy intake), in contrast with the actual weight loss of −3.2 kg (29% of the predicted weight loss). This difference in the calorie-to-weight loss was higher in leaner patients (lower BMI) and those with higher eGFR [136]. Considering that the resting and postprandial energy expenditures were unaltered after chronic SGLT-2 inhibitor treatment [137], the difference in the calorie-to-weight loss was attributable to an adaptive increase in calorie intake after 10 weeks of treatment. In addition, the calorie deficit induced by glycosuria leads to a shift in substrate utilization from glucose to lipids, resulting in increased lipolysis and FFA oxidation. Of note, more than two-thirds of SGLT-2 inhibitor-induced weight loss is attributable to a reduction in fat mass [58,138,139]. Furthermore, recent studies have shown that SLGT-2 is expressed in the pancreatic alpha cells, and its inhibition triggers secretion of glucagon directly. Altered (reduced) insulin-to-glucagon ratio simulates “starvation” state leading to increased lipolysis and mobilization of FFAs [140,141]. In addition, studies on diet-induced obese rodent models suggested that SGLT-2 inhibition increases fat utilization (oxidation) and browning of white adipose tissue, reduces hepatic fat content, and attenuates obesity-induced inflammation and insulin resistance [142,143,144].
The role of weight loss induced by SGLT-2 inhibitors should be considered in combination with their other effects, which include: (1) diuretic and natriuretic effects and reduction in cardiac preload; (2) shift in cardiac energy substrate from fat and glucose oxidation to more efficient ketone bodies; (3) reduced epicardial fat volume leading to a decrease in cardiac fibrosis and enhanced contractility; (4) increase in hematocrit; and (5) renoprotective effects [58,139,145,146]. In addition, SGLT-2 inhibitors have been shown to enhance utilization of FFAs and improve adipose tissue function. These effects may lead to a reduction in inflammation, improvements in insulin resistance, glycemic control, and blood pressure control.
CONCLUSIONS
Management of overweight/obese patients with T2DM poses a challenge to clinicians because of there being fewer therapeutic options available for both glycemic control and weight reduction. Some of the older, established GLDs induce weight gain as a side effect. SGLT-2 inhibitors are novel oral GLDs that promote weight loss, decrease adiposity, and improve CV outcomes. As most of the T2DM patients are overweight/obese and at high risk of CVD, SGLT-2 inhibitors offer an effective therapeutic option for the management of these patients, particularly in the Asian region, which has a high burden of abdominal adiposity and CVD. Based on the current evidence on SGLT-2 inhibitors in the Asian population, results from the large CVOTs, and clinical experience, a series of clinical recommendations have been developed (Table 2).
Table 2. Clinical recommendations on the use of SGLT-2 inhibitors for the management of Asian patients with T2DM and abdominal obesity.
| Clinical recommendations |
|---|
| Overweight/obesity burden and associated complications in Asian patients with T2DM |
| • Overweight/obesity is a major driver of the increasing prevalence of T2DM in Asia, and most of the patients with T2DM are overweight/ obese. |
| • Asian populations have higher abdominal adiposity for any given BMI compared with their Caucasian counterparts. |
| • Visceral or abdominal adiposity is strongly associated with risk of adverse CV outcomes and has been shown to be superior to BMI in predicting CVD risk. |
| • Overweight/obesity in patients with T2DM independently increases the risk of hypertension, dyslipidemia, and CHD; it is also associated with other complications such as ectopic fat deposition (e.g., NAFLD). |
| Weight loss as an essential management goal in overweight/obese patients with T2DM |
| • Weight loss is an important management goal in patients with T2DM, who are overweight/obese. |
| • Lifestyle modification (diet, physical activity, and behavioral therapy) designed to achieve and maintain weight loss should be prescribed for patients with T2DM who are overweight/obese. |
| • Limited glucose-lowering pharmacological therapies are available that promote weight loss in T2DM. |
| • In overweight/obese patients with T2DM, use of glucose-lowering medications that promote weight loss or are weight neutral is recommended. |
| ∘ Use of medications that are associated with weight gain should be minimized in overweight/obese patients with T2DM. |
| Role of SGLT-2 inhibitors in the management of Asian patients with T2DM and abdominal obesity |
| • SGLT-2 inhibitor is recommended to promote weight loss and reduction in visceral adiposity in Asian patients with T2DM and abdominal obesity. |
| • SGLT-2 inhibitors promote weight loss in Asian patients with T2DM as monotherapy or in combination with other GLDs. |
| ∘ More than two-thirds of SGLT-2 inhibitor-induced weight loss is attributable to a reduction in body fat mass. |
| • SGLT-2 inhibitor treatment reduces WC (a measure of abdominal or visceral adiposity) and ectopic fat deposition in non-adipose tissues, and improves adipose tissue function, HRQoL, and patient-reported treatment satisfaction. |
SGLT-2, sodium glucose cotransporter-2; T2DM, type 2 diabetes mellitus; BMI, body mass index; CV, cardiovascular; CVD, cardiovascular disease; CHD, coronary heart disease; NAFLD, non-alcoholic fatty liver disease; GLD, glucose-lowering drug; WC, waist circumference; HRQoL, health-related quality of life.
ACKNOWLEDGMENTS
None.
Footnotes
CONFLICTS OF INTEREST: The development of these expert recommendations was supported by an unrestricted educational grant from AstraZeneca Ltd, who had no influence on the content. All authors have read, approved, and take full responsibility for the accuracy of the content.
Wayne Huey-Herng Sheu has been advisor and/or speaker for AstraZeneca, Bayer HealthCare, Boehringer Ingelheim Pharmaceuticals, Daiichi-Sankyo, Eli Lilly and Company, Merck Sharp & Dohme, Mitsubishi Tanabe Pharma Corporation, Novartis Pharmaceuticals, Novo Nordisk, Pfizer, Sanofi, and Takeda Pharmaceutical Company.
Chan Siew Pheng has received honoraria as speaker and advisor for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Merck Sharp & Dohme, Novartis, Novo Nordisk, Sanofi, and Servier.
Bien J. Matawaran has received honoraria and CME grants from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck, Multicare, Merck Sharp & Dohme, NatraPharm, Novartis, Novo Nordisk, Pfizer, Sanofi, Servier, and Torrent Pharma.
Chaicharn Deerochanawong has received honoraria as the speaker or advisor or research grants from AstraZeneca, Boehringer Ingelheim, Janssen, Bayer, Eli Lilly, Abbott, Novartis, Pfizer, Merck Sharp & Dohme, Novo Nordisk, Sanofi, and Takeda.
Ambrish Mithal has received honoraria as speaker and advisor from AstraZeneca, Abbott, Boehringer Ingelheim, Cipla, Dr. Reddy's, Eli Lilly, Glenmark, GlaxoSmithKline, Ipca Laboratories, Janssen, Lupin, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, Sanofi, Serdia Servier, Sun Pharma, Torrent, Wockhardt and Zydus Nutrition.
Juliana Chan is the Chief Executive Officer (on probono basis) of Asia Diabetes Foundation, a charitable foundation established under The Chinese University of Hong Kong Foundation for developing the JADE Technology. She has received honoraria and traveling support for consultancy or giving lectures and her affiliated institutions have received research and educational grants from Amgen, Ascencia, AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Daiichi-Sankyo, Eli Lilly, GlaxoSmithKline, Medtronic, Merck Serono, Merck Sharp & Dohme, Novo Nordisk, Pfizer, and Sanofi. Ketut Suastika has received honoraria as a speaker or advisor from AstraZeneca, Boehringer Ingelheim, Merck Sharp & Dohme, Novo Nordisk, Sanofi, Merck, and Servier.
Chin Meng Khoo has received honoraria as a speaker or advisor from AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Sanofi.
Nguyen Huu Man has no disclosures.
Ji Linong is a member of the DISCOVER Scientific Committee and received support from AstraZeneca to attend DISCOVER planning and update meetings. He has also received honoraria from Eli Lilly, Bristol-Myers Squibb, Novartis, Novo Nordisk, Bayer, Merck Sharp & Dohme, Takeda, Sanofi, Roche, Boehringer Ingelheim, and AstraZeneca; research support from Roche, Sanofi, Merck Sharp & Dohme, AstraZeneca, Novartis, Eli Lilly, and Bristol-Myers Squibb.
Andrea Luk is a member of advisory boards for AstraZeneca, Boehringer Ingelheim, Sanofi, and Amgen. She has received research grants from Boehringer Ingelheim, Merck Sharp & Dohme, Sanofi, and Amgen; and travel grants from AstraZeneca, Boehringer Ingelheim, Merck Sharp & Dohme, Novartis, Novo Nordisk, and Sanofi.
Kun-Ho Yoon has received honoraria as a speaker or advisor from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceutical, Merck Sharp & Dohme, Novo Nordisk, Sanofi, and Takeda; research support from AstraZeneca and Takeda.
Medical writing assistance was provided by Syed Abdul Haseeb (MS, CMPP) of MediTech Media, Asia Pacific, and was funded by AstraZeneca Ltd.
References
- 1.Scheen AJ, Van Gaal LF. Combating the dual burden: therapeutic targeting of common pathways in obesity and type 2 diabetes. Lancet Diabetes Endocrinol. 2014;2:911–922. doi: 10.1016/S2213-8587(14)70004-X. [DOI] [PubMed] [Google Scholar]
- 2.Eckel RH, Kahn SE, Ferrannini E, Goldfine AB, Nathan DM, Schwartz MW, Smith RJ, Smith SR. Obesity and type 2 diabetes: what can be unified and what needs to be individualized? J Clin Endocrinol Metab. 2011;96:1654–1663. doi: 10.1210/jc.2011-0585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sears B, Perry M. The role of fatty acids in insulin resistance. Lipids Health Dis. 2015;14:121. doi: 10.1186/s12944-015-0123-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bodenant M, Kuulasmaa K, Wagner A, Kee F, Palmieri L, Ferrario MM, Montaye M, Amouyel P, Dallongeville J MORGAM Project. Measures of abdominal adiposity and the risk of stroke: the MOnica Risk, Genetics, Archiving and Monograph (MORGAM) study. Stroke. 2011;42:2872–2877. doi: 10.1161/STROKEAHA.111.614099. [DOI] [PubMed] [Google Scholar]
- 5.Casanueva FF, Moreno B, Rodriguez-Azeredo R, Massien C, Conthe P, Formiguera X, Barrios V, Balkau B. Relationship of abdominal obesity with cardiovascular disease, diabetes and hyperlipidaemia in Spain. Clin Endocrinol (Oxf) 2010;73:35–40. doi: 10.1111/j.1365-2265.2009.03727.x. [DOI] [PubMed] [Google Scholar]
- 6.Balkau B, Deanfield JE, Despres JP, Bassand JP, Fox KA, Smith SC, Jr, Barter P, Tan CE, van Gaal L, Wittchen HU, Massien C, Haffner SM. International Day for the Evaluation of Abdominal Obesity (IDEA): a study of waist circumference, cardiovascular disease, and diabetes mellitus in 168,000 primary care patients in 63 countries. Circulation. 2007;116:1942–1951. doi: 10.1161/CIRCULATIONAHA.106.676379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lim U, Ernst T, Buchthal SD, Latch M, Albright CL, Wilkens LR, Kolonel LN, Murphy SP, Chang L, Novotny R, Le Marchand L. Asian women have greater abdominal and visceral adiposity than Caucasian women with similar body mass index. Nutr Diabetes. 2011;1:e6. doi: 10.1038/nutd.2011.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sniderman AD, Bhopal R, Prabhakaran D, Sarrafzadegan N, Tchernof A. Why might South Asians be so susceptible to central obesity and its atherogenic consequences?: the adipose tissue overflow hypothesis. Int J Epidemiol. 2007;36:220–225. doi: 10.1093/ije/dyl245. [DOI] [PubMed] [Google Scholar]
- 9.Wells JC. Commentary: why are South Asians susceptible to central obesity?: the El Nino hypothesis. Int J Epidemiol. 2007;36:226–227. doi: 10.1093/ije/dyl287. [DOI] [PubMed] [Google Scholar]
- 10.WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157–163. doi: 10.1016/S0140-6736(03)15268-3. [DOI] [PubMed] [Google Scholar]
- 11.World Health Organization. Waist circumference and waist-hip ratio: report of a WHO expert consultation, Geneva, 8–11 December 2008. Geneva: World Health Organization; 2011. [Google Scholar]
- 12.International Diabetes Federation. The IDF consensus worldwide definition of the metabolic syndrome. [cited 2020 Jan 28]. Available from: https://www.idf.org/component/attachments/attachments.html?id=705&task=download.
- 13.Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, Kim DY, Kwon HS, Kim SR, Lee CB, Oh SJ, Park CY, Yoo HJ. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007;75:72–80. doi: 10.1016/j.diabres.2006.04.013. [DOI] [PubMed] [Google Scholar]
- 14.American Diabetes Association. Standards of medical care in diabetes: 2019. Diabetes Care. 2019;42(Suppl 1):S1–S193. doi: 10.2337/dc19-Sint01. [DOI] [PubMed] [Google Scholar]
- 15.Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, Dagogo-Jack S, DeFronzo RA, Einhorn D, Fonseca VA, Garber JR, Garvey WT, Grunberger G, Handelsman Y, Hirsch IB, Jellinger PS, McGill JB, Mechanick JI, Rosenblit PD, Umpierrez GE. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm: 2018 executive summary. Endocr Pract. 2018;24:91–120. doi: 10.4158/CS-2017-0153. [DOI] [PubMed] [Google Scholar]
- 16.Deerochanawong C, Chan SP, Matawaran BJ, Sheu WH, Chan J, Man NH, Suastika K, Khoo CM, Yoon KH, Luk A, Mithal A, Linong J. Use of sodium-glucose co-transporter-2 inhibitors in patients with type 2 diabetes mellitus and multiple cardiovascular risk factors: an Asian perspective and expert recommendations. Diabetes Obes Metab. 2019;21:2354–2367. doi: 10.1111/dom.13819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, Abraham JP, Abu-Rmeileh NM, Achoki T, AlBuhairan FS, Alemu ZA, Alfonso R, Ali MK, Ali R, Guzman NA, Ammar W, Anwari P, Banerjee A, Barquera S, Basu S, Bennett DA, Bhutta Z, Blore J, Cabral N, Nonato IC, Chang JC, Chowdhury R, Courville KJ, Criqui MH, Cundiff DK, Dabhadkar KC, Dandona L, Davis A, Dayama A, Dharmaratne SD, Ding EL, Durrani AM, Esteghamati A, Farzadfar F, Fay DF, Feigin VL, Flaxman A, Forouzanfar MH, Goto A, Green MA, Gupta R, Hafezi-Nejad N, Hankey GJ, Harewood HC, Havmoeller R, Hay S, Hernandez L, Husseini A, Idrisov BT, Ikeda N, Islami F, Jahangir E, Jassal SK, Jee SH, Jeffreys M, Jonas JB, Kabagambe EK, Khalifa SE, Kengne AP, Khader YS, Khang YH, Kim D, Kimokoti RW, Kinge JM, Kokubo Y, Kosen S, Kwan G, Lai T, Leinsalu M, Li Y, Liang X, Liu S, Logroscino G, Lotufo PA, Lu Y, Ma J, Mainoo NK, Mensah GA, Merriman TR, Mokdad AH, Moschandreas J, Naghavi M, Naheed A, Nand D, Narayan KM, Nelson EL, Neuhouser ML, Nisar MI, Ohkubo T, Oti SO, Pedroza A, Prabhakaran D, Roy N, Sampson U, Seo H, Sepanlou SG, Shibuya K, Shiri R, Shiue I, Singh GM, Singh JA, Skirbekk V, Stapelberg NJ, Sturua L, Sykes BL, Tobias M, Tran BX, Trasande L, Toyoshima H, van de Vijver S, Vasankari TJ, Veerman JL, Velasquez-Melendez G, Vlassov VV, Vollset SE, Vos T, Wang C, Wang X, Weiderpass E, Werdecker A, Wright JL, Yang YC, Yatsuya H, Yoon J, Yoon SJ, Zhao Y, Zhou M, Zhu S, Lopez AD, Murray CJ, Gakidou E. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi: 10.1016/S0140-6736(14)60460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.World Health Orgaization. Obesity and overweight. [updated 2018 Feb 16]. Available from: http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight.
- 19.GBD 2015 Obesity Collaborators. Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, Lee A, Marczak L, Mokdad AH, Moradi-Lakeh M, Naghavi M, Salama JS, Vos T, Abate KH, Abbafati C, Ahmed MB, Al-Aly Z, Alkerwi A, Al-Raddadi R, Amare AT, Amberbir A, Amegah AK, Amini E, Amrock SM, Anjana RM, Arnlov J, Asayesh H, Banerjee A, Barac A, Baye E, Bennett DA, Beyene AS, Biadgilign S, Biryukov S, Bjertness E, Boneya DJ, Campos-Nonato I, Carrero JJ, Cecilio P, Cercy K, Ciobanu LG, Cornaby L, Damtew SA, Dandona L, Dandona R, Dharmaratne SD, Duncan BB, Eshrati B, Esteghamati A, Feigin VL, Fernandes JC, Furst T, Gebrehiwot TT, Gold A, Gona PN, Goto A, Habtewold TD, Hadush KT, Hafezi-Nejad N, Hay SI, Horino M, Islami F, Kamal R, Kasaeian A, Katikireddi SV, Kengne AP, Kesavachandran CN, Khader YS, Khang YH, Khubchandani J, Kim D, Kim YJ, Kinfu Y, Kosen S, Ku T, Defo BK, Kumar GA, Larson HJ, Leinsalu M, Liang X, Lim SS, Liu P, Lopez AD, Lozano R, Majeed A, Malekzadeh R, Malta DC, Mazidi M, McAlinden C, McGarvey ST, Mengistu DT, Mensah GA, Mensink GBM, Mezgebe HB, Mirrakhimov EM, Mueller UO, Noubiap JJ, Obermeyer CM, Ogbo FA, Owolabi MO, Patton GC, Pourmalek F, Qorbani M, Rafay A, Rai RK, Ranabhat CL, Reinig N, Safiri S, Salomon JA, Sanabria JR, Santos IS, Sartorius B, Sawhney M, Schmidhuber J, Schutte AE, Schmidt MI, Sepanlou SG, Shamsizadeh M, Sheikhbahaei S, Shin MJ, Shiri R, Shiue I, Roba HS, Silva DAS, Silverberg JI, Singh JA, Stranges S, Swaminathan S, Tabares-Seisdedos R, Tadese F, Tedla BA, Tegegne BS, Terkawi AS, Thakur JS, Tonelli M, Topor-Madry R, Tyrovolas S, Ukwaja KN, Uthman OA, Vaezghasemi M, Vasankari T, Vlassov VV, Vollset SE, Weiderpass E, Werdecker A, Wesana J, Westerman R, Yano Y, Yonemoto N, Yonga G, Zaidi Z, Zenebe ZM, Zipkin B, Murray CJL. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27. doi: 10.1056/NEJMoa1614362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Helble M, Francisco K. The imminent obesity crisis in Asia and the Pacific: first cost estimates. Tokyo: Asian Development Bank Institute; 2017. [Google Scholar]
- 21.International Diabetes Federation. IDF diabetes atlas 8th edition. [cited 2020 Jan 28]. Available from: https://www.idf.org/component/attachments/attachments.html?id=1405&task=download.
- 22.Daousi C, Casson IF, Gill GV, MacFarlane IA, Wilding JP, Pinkney JH. Prevalence of obesity in type 2 diabetes in secondary care: association with cardiovascular risk factors. Postgrad Med J. 2006;82:280–284. doi: 10.1136/pmj.2005.039032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.So WY, Raboca J, Sobrepena L, Yoon KH, Deerochanawong C, Ho LT, Himathongkam T, Tong P, Lyubomirsky G, Ko G, Nan H, Chan J JADE Program Research Team. Comprehensive risk assessments of diabetic patients from seven Asian countries: the Joint Asia Diabetes Evaluation (JADE) program. J Diabetes. 2011;3:109–118. doi: 10.1111/j.1753-0407.2011.00115.x. [DOI] [PubMed] [Google Scholar]
- 24.Kim BY, Won JC, Lee JH, Kim HS, Park JH, Ha KH, Won KC, Kim DJ, Park KS. Diabetes fact sheets in Korea, 2018: an appraisal of current status. Diabetes Metab J. 2019;43:487–494. doi: 10.4093/dmj.2019.0067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ford ES. Body mass index, diabetes, and C-reactive protein among U.S. adults. Diabetes Care. 1999;22:1971–1977. doi: 10.2337/diacare.22.12.1971. [DOI] [PubMed] [Google Scholar]
- 26.Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002;347:1557–1565. doi: 10.1056/NEJMoa021993. [DOI] [PubMed] [Google Scholar]
- 27.van Dijk EJ, Prins ND, Vermeer SE, Vrooman HA, Hofman A, Koudstaal PJ, Breteler MM. C-reactive protein and cerebral small-vessel disease: the Rotterdam Scan Study. Circulation. 2005;112:900–905. doi: 10.1161/CIRCULATIONAHA.104.506337. [DOI] [PubMed] [Google Scholar]
- 28.Ni Mhurchu C, Rodgers A, Pan WH, Gu DF, Woodward M Asia Pacific Cohort Studies Collaboration. Body mass index and cardiovascular disease in the Asia-Pacific Region: an overview of 33 cohorts involving 310 000 participants. Int J Epidemiol. 2004;33:751–758. doi: 10.1093/ije/dyh163. [DOI] [PubMed] [Google Scholar]
- 29.Asia Pacific Cohort Studies Collaboration. Central obesity and risk of cardiovascular disease in the Asia Pacific Region. Asia Pac J Clin Nutr. 2006;15:287–292. [PubMed] [Google Scholar]
- 30.Iso H, Sato S, Kitamura A, Imano H, Kiyama M, Yamagishi K, Cui R, Tanigawa T, Shimamoto T. Metabolic syndrome and the risk of ischemic heart disease and stroke among Japanese men and women. Stroke. 2007;38:1744–1751. doi: 10.1161/STROKEAHA.106.469072. [DOI] [PubMed] [Google Scholar]
- 31.Huxley RR, Barzi F, Woo J, Giles G, Lam TH, Rahimi K, Konety S, Ohkubo T, Jee SH, Fang X, Woodward M Asia Pacific Cohort Studies Collaboration. A comparison of risk factors for mortality from heart failure in Asian and non-Asian populations: an overview of individual participant data from 32 prospective cohorts from the Asia-Pacific Region. BMC Cardiovasc Disord. 2014;14:61. doi: 10.1186/1471-2261-14-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ahmad FS, Ning H, Rich JD, Yancy CW, Lloyd-Jones DM, Wilkins JT. Hypertension, obesity, diabetes, and heart failure-free survival: the cardiovascular disease lifetime risk pooling project. JACC Heart Fail. 2016;4:911–919. doi: 10.1016/j.jchf.2016.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Maric-Bilkan C. Obesity and diabetic kidney disease. Med Clin North Am. 2013;97:59–74. doi: 10.1016/j.mcna.2012.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pinto-Sietsma SJ, Navis G, Janssen WM, de Zeeuw D, Gans RO, de Jong PF PREVEND Study Group. A central body fat distribution is related to renal function impairment, even in lean subjects. Am J Kidney Dis. 2003;41:733–741. doi: 10.1016/s0272-6386(03)00020-9. [DOI] [PubMed] [Google Scholar]
- 35.Thoenes M, Reil JC, Khan BV, Bramlage P, Volpe M, Kirch W, Bohm M. Abdominal obesity is associated with microalbuminuria and an elevated cardiovascular risk profile in patients with hypertension. Vasc Health Risk Manag. 2009;5:577–585. doi: 10.2147/vhrm.s5207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hill CJ, Cardwell CR, Maxwell AP, Young RJ, Matthews B, O'Donoghue DJ, Fogarty DG. Obesity and kidney disease in type 1 and 2 diabetes: an analysis of the National Diabetes Audit. QJM. 2013;106:933–942. doi: 10.1093/qjmed/hct123. [DOI] [PubMed] [Google Scholar]
- 37.Thomas G, Sehgal AR, Kashyap SR, Srinivas TR, Kirwan JP, Navaneethan SD. Metabolic syndrome and kidney disease: a systematic review and meta-analysis. Clin J Am Soc Nephrol. 2011;6:2364–2373. doi: 10.2215/CJN.02180311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Smith BW, Adams LA. Nonalcoholic fatty liver disease and diabetes mellitus: pathogenesis and treatment. Nat Rev Endocrinol. 2011;7:456–465. doi: 10.1038/nrendo.2011.72. [DOI] [PubMed] [Google Scholar]
- 39.Pearson-Stuttard J, Zhou B, Kontis V, Bentham J, Gunter MJ, Ezzati M. Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment. Lancet Diabetes Endocrinol. 2018;6:e6–e15. doi: 10.1016/S2213-8587(18)30150-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bonsignore MR, Borel AL, Machan E, Grunstein R. Sleep apnoea and metabolic dysfunction. Eur Respir Rev. 2013;22:353–364. doi: 10.1183/09059180.00003413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.The Diabetes Association of the Republic of China. DAROC Clinical Practice Guidelines for diabetes care 2018, Taiwan. [cited 2020 Jan 28]. Available from: http://www.endo-dm.org.tw/dia/direct/index.asp?BK_KIND=29¤t=2018%E7%B3%96%E5%B0%BF%E7%97%85%E8%87%A8%E5%BA%8A%E7%85%A7%E8%AD%B7%E6%8C%87%E5%BC%95+++++++++++++++++ [DOI] [PubMed]
- 42.Health Technology Assessment Section, Medical Development Division, Ministry of Health Malaysia. Clinical practice guidelines: management of type 2 diabetes mellitus. [cited 2020 Jan 28]. Available from: http://www.acadmed.org.my/view_file.cfm?fileid=763.
- 43.Weng J, Ji L, Jia W, Lu J, Zhou Z, Zou D, Zhu D, Chen L, Chen L, Guo L, Guo X, Ji Q, Li Q, Li X, Liu J, Ran X, Shan Z, Shi L, Song G, Yang L, Yang Y, Yang W Chinese Diabetes Society. Standards of care for type 2 diabetes in China. Diabetes Metab Res Rev. 2016;32:442–458. doi: 10.1002/dmrr.2827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ministry of Health Singapore. Diabetes mellitus: MOH clinical practice guidelines. [cited 2020 Jan 28]. Available from: https://www.moh.gov.sg/docs/librariesprovider4/guidelines/cpg_diabetes-mellitus-booklet---jul-2014.pdf.
- 45.Kim MK, Ko SH, Kim BY, Kang ES, Noh J, Kim SK, Park SO, Hur KY, Chon S, Moon MK, Kim NH, Kim SY, Rhee SY, Lee KW, Kim JH, Rhee EJ, Chun S, Yu SH, Kim DJ, Kwon HS, Park KS Committee of Clinical Practice Guidelines, Korean Diabetes Association. 2019 Clinical practice guidelines for type 2 diabetes mellitus in Korea. Diabetes Metab J. 2019;43:398–406. doi: 10.4093/dmj.2019.0137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Garvey WT, Mechanick JI, Brett EM, Garber AJ, Hurley DL, Jastreboff AM, Nadolsky K, Pessah-Pollack R, Plodkowski R Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American Association of Clinical Endocrinologists and American College of endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22 Suppl 3:1–203. doi: 10.4158/EP161365.GL. [DOI] [PubMed] [Google Scholar]
- 47.Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, Hu FB, Hubbard VS, Jakicic JM, Kushner RF, Loria CM, Millen BE, Nonas CA, Pi-Sunyer FX, Stevens J, Stevens VJ, Wadden TA, Wolfe BM, Yanovski SZ American Heart Association Task Force on Practice Guidelines; Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. 2014;63(25 Pt B):2985–3023. doi: 10.1016/j.jacc.2013.11.004. [DOI] [PubMed] [Google Scholar]
- 48.Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR. Management of hyperglycaemia in type 2 diabetes, 2015: a patient-centred approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2015;58:429–442. doi: 10.1007/s00125-014-3460-0. [DOI] [PubMed] [Google Scholar]
- 49.Rosenstock J, Hassman DR, Madder RD, Brazinsky SA, Farrell J, Khutoryansky N, Hale PM Repaglinide Versus Nateglinide Comparison Study Group. Repaglinide versus nateglinide monotherapy: a randomized, multicenter study. Diabetes Care. 2004;27:1265–1270. doi: 10.2337/diacare.27.6.1265. [DOI] [PubMed] [Google Scholar]
- 50.Schernthaner G, Grimaldi A, Di Mario U, Drzewoski J, Kempler P, Kvapil M, Novials A, Rottiers R, Rutten GE, Shaw KM. GUIDE study: double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients. Eur J Clin Invest. 2004;34:535–542. doi: 10.1111/j.1365-2362.2004.01381.x. [DOI] [PubMed] [Google Scholar]
- 51.Dormandy JA, Charbonnel B, Eckland DJ, Erdmann E, Massi-Benedetti M, Moules IK, Skene AM, Tan MH, Lefebvre PJ, Murray GD, Standl E, Wilcox RG, Wilhelmsen L, Betteridge J, Birkeland K, Golay A, Heine RJ, Koranyi L, Laakso M, Mokan M, Norkus A, Pirags V, Podar T, Scheen A, Scherbaum W, Schernthaner G, Schmitz O, Skrha J, Smith U, Taton J PROactive Investigators. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomized controlled trial. Lancet. 2005;366:1279–1289. doi: 10.1016/S0140-6736(05)67528-9. [DOI] [PubMed] [Google Scholar]
- 52.Kahn SE, Haffner SM, Heise MA, Herman WH, Holman RR, Jones NP, Kravitz BG, Lachin JM, O'Neill MC, Zinman B, Viberti G ADOPT Study Group. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006;355:2427–2443. doi: 10.1056/NEJMoa066224. [DOI] [PubMed] [Google Scholar]
- 53.Bolen S, Feldman L, Vassy J, Wilson L, Yeh HC, Marinopoulos S, Wiley C, Selvin E, Wilson R, Bass EB, Brancati FL. Systematic review: comparative effectiveness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med. 2007;147:386–399. doi: 10.7326/0003-4819-147-6-200709180-00178. [DOI] [PubMed] [Google Scholar]
- 54.Phung OJ, Scholle JM, Talwar M, Coleman CI. Effect of noninsulin antidiabetic drugs added to metformin therapy on glycemic control, weight gain, and hypoglycemia in type 2 diabetes. JAMA. 2010;303:1410–1418. doi: 10.1001/jama.2010.405. [DOI] [PubMed] [Google Scholar]
- 55.Karagiannis T, Paschos P, Paletas K, Matthews DR, Tsapas A. Dipeptidyl peptidase-4 inhibitors for treatment of type 2 diabetes mellitus in the clinical setting: systematic review and meta-analysis. BMJ. 2012;344:e1369. doi: 10.1136/bmj.e1369. [DOI] [PubMed] [Google Scholar]
- 56.Saenz A, Fernandez-Esteban I, Mataix A, Ausejo M, Roque M, Moher D. Metformin monotherapy for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2005;(3):CD002966. doi: 10.1002/14651858.CD002966.pub3. [DOI] [PubMed] [Google Scholar]
- 57.Davies MJ, D'Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, Rossing P, Tsapas A, Wexler DJ, Buse JB. Management of hyperglycaemia in type 2 diabetes, 2018: a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2018;61:2461–2498. doi: 10.1007/s00125-018-4729-5. [DOI] [PubMed] [Google Scholar]
- 58.Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation. 2016;134:752–772. doi: 10.1161/CIRCULATIONAHA.116.021887. [DOI] [PubMed] [Google Scholar]
- 59.Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377:644–657. doi: 10.1056/NEJMoa1611925. [DOI] [PubMed] [Google Scholar]
- 60.Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS DECLARE-TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380:347–357. doi: 10.1056/NEJMoa1812389. [DOI] [PubMed] [Google Scholar]
- 61.Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–2128. doi: 10.1056/NEJMoa1504720. [DOI] [PubMed] [Google Scholar]
- 62.Cai X, Yang W, Gao X, Chen Y, Zhou L, Zhang S, Han X, Ji L. The association between the dosage of SGLT2 inhibitor and weight reduction in type 2 diabetes patients: a meta-analysis. Obesity (Silver Spring) 2018;26:70–80. doi: 10.1002/oby.22066. [DOI] [PubMed] [Google Scholar]
- 63.Gill HK, Kaur P, Mahendru S, Mithal A. Adverse effect profile and effectiveness of sodium glucose co-transporter 2 inhibitors (SGLT2i): a prospective real-world setting study. Indian J Endocrinol Metab. 2019;23:50–55. doi: 10.4103/ijem.IJEM_566_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Vasilakou D, Karagiannis T, Athanasiadou E, Mainou M, Liakos A, Bekiari E, Sarigianni M, Matthews DR, Tsapas A. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2013;159:262–274. doi: 10.7326/0003-4819-159-4-201308200-00007. [DOI] [PubMed] [Google Scholar]
- 65.Kaku K, Watada H, Iwamoto Y, Utsunomiya K, Terauchi Y, Tobe K, Tanizawa Y, Araki E, Ueda M, Suganami H, Watanabe D Tofogliflozin 003 Study Group. Efficacy and safety of monotherapy with the novel sodium/glucose cotransporter-2 inhibitor tofogliflozin in Japanese patients with type 2 diabetes mellitus: a combined Phase 2 and 3 randomized, placebo-controlled, double-blind, parallel-group comparative study. Cardiovasc Diabetol. 2014;13:65. doi: 10.1186/1475-2840-13-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kashiwagi A, Kazuta K, Yoshida S, Nagase I. Randomized, placebo-controlled, double-blind glycemic control trial of novel sodium-dependent glucose cotransporter 2 inhibitor ipragliflozin in Japanese patients with type 2 diabetes mellitus. J Diabetes Investig. 2014;5:382–391. doi: 10.1111/jdi.12156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Seino Y, Kaku K, Inagaki N, Haneda M, Sasaki T, Fukatsu A, Ubukata M, Sakai S, Samukawa Y. Fifty-two-week long-term clinical study of luseogliflozin as monotherapy in Japanese patients with type 2 diabetes mellitus inadequately controlled with diet and exercise. Endocr J. 2015;62:593–603. doi: 10.1507/endocrj.EJ15-0097. [DOI] [PubMed] [Google Scholar]
- 68.Harashima SI, Inagaki N, Kondo K, Maruyama N, Otsuka M, Kawaguchi Y, Watanabe Y. Efficacy and safety of canagliflozin as add-on therapy to a glucagon-like peptide-1 receptor agonist in Japanese patients with type 2 diabetes mellitus: a 52-week, open-label, phase IV study. Diabetes Obes Metab. 2018;20:1770–1775. doi: 10.1111/dom.13267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Seino Y, Yabe D, Sasaki T, Fukatsu A, Imazeki H, Ochiai H, Sakai S. Sodium-glucose cotransporter-2 inhibitor luseogliflozin added to glucagon-like peptide 1 receptor agonist liraglutide improves glycemic control with bodyweight and fat mass reductions in Japanese patients with type 2 diabetes: a 52-week, open-label, single-arm study. J Diabetes Investig. 2018;9:332–340. doi: 10.1111/jdi.12694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Araki E, Onishi Y, Asano M, Kim H, Ekholm E, Johnsson E, Yajima T. Efficacy and safety of dapagliflozin in addition to insulin therapy in Japanese patients with type 2 diabetes: results of the interim analysis of 16-week double-blind treatment period. J Diabetes Investig. 2016;7:555–564. doi: 10.1111/jdi.12453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Araki E, Onishi Y, Asano M, Kim H, Yajima T. Efficacy and safety of dapagliflozin over 1 year as add-on to insulin therapy in Japanese patients with type 2 diabetes: the DAISY (Dapagliflozin Added to patients under InSulin therapY) trial. Diabetes Obes Metab. 2017;19:562–570. doi: 10.1111/dom.12853. [DOI] [PubMed] [Google Scholar]
- 72.Inagaki N, Kondo K, Yoshinari T, Kuki H. Efficacy and safety of canagliflozin alone or as add-on to other oral antihyperglycemic drugs in Japanese patients with type 2 diabetes: a 52-week open-label study. J Diabetes Investig. 2015;6:210–218. doi: 10.1111/jdi.12266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Inagaki N, Kondo K, Yoshinari T, Takahashi N, Susuta Y, Kuki H. Efficacy and safety of canagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled with diet and exercise: a 24-week, randomized, double-blind, placebo-controlled, phase III study. Expert Opin Pharmacother. 2014;15:1501–1515. doi: 10.1517/14656566.2014.935764. [DOI] [PubMed] [Google Scholar]
- 74.Ji L, Ma J, Li H, Mansfield TA, T'joen CL, Iqbal N, Ptaszynska A, List JF. Dapagliflozin as monotherapy in drug-naive Asian patients with type 2 diabetes mellitus: a randomized, blinded, prospective phase III study. Clin Ther. 2014;36:84–100. doi: 10.1016/j.clinthera.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 75.Kadowaki T, Haneda M, Inagaki N, Terauchi Y, Taniguchi A, Koiwai K, Rattunde H, Woerle HJ, Broedl UC. Efficacy and safety of empagliflozin monotherapy for 52 weeks in Japanese patients with type 2 diabetes: a randomized, double-blind, parallel-group study. Adv Ther. 2015;32:306–318. doi: 10.1007/s12325-015-0198-0. [DOI] [PubMed] [Google Scholar]
- 76.Lu CH, Min KW, Chuang LM, Kokubo S, Yoshida S, Cha BS. Efficacy, safety, and tolerability of ipragliflozin in Asian patients with type 2 diabetes mellitus and inadequate glycemic control with metformin: results of a phase 3 randomized, placebo-controlled, double-blind, multicenter trial. J Diabetes Investig. 2016;7:366–373. doi: 10.1111/jdi.12422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Seino Y, Sasaki T, Fukatsu A, Imazeki H, Ochiai H, Sakai S. Efficacy and safety of luseogliflozin added to insulin therapy in Japanese patients with type 2 diabetes: a multicenter, 52-week, clinical study with a 16-week, double-blind period and a 36-week, open-label period. Curr Med Res Opin. 2018;34:981–994. doi: 10.1080/03007995.2018.1441816. [DOI] [PubMed] [Google Scholar]
- 78.Yang W, Han P, Min KW, Wang B, Mansfield T, T'Joen C, Iqbal N, Johnsson E, Ptaszynska A. Efficacy and safety of dapagliflozin in Asian patients with type 2 diabetes after metformin failure: a randomized controlled trial. J Diabetes. 2016;8:796–808. doi: 10.1111/1753-0407.12357. [DOI] [PubMed] [Google Scholar]
- 79.Inagaki N, Kondo K, Yoshinari T, Maruyama N, Susuta Y, Kuki H. Efficacy and safety of canagliflozin in Japanese patients with type 2 diabetes: a randomized, double-blind, placebo-controlled, 12-week study. Diabetes Obes Metab. 2013;15:1136–1145. doi: 10.1111/dom.12149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kaku K, Inoue S, Matsuoka O, Kiyosue A, Azuma H, Hayashi N, Tokudome T, Langkilde AM, Parikh S. Efficacy and safety of dapagliflozin as a monotherapy for type 2 diabetes mellitus in Japanese patients with inadequate glycaemic control: a phase II multicentre, randomized, double-blind, placebo-controlled trial. Diabetes Obes Metab. 2013;15:432–440. doi: 10.1111/dom.12047. [DOI] [PubMed] [Google Scholar]
- 81.Kaku K, Kiyosue A, Inoue S, Ueda N, Tokudome T, Yang J, Langkilde AM. Efficacy and safety of dapagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled by diet and exercise. Diabetes Obes Metab. 2014;16:1102–1110. doi: 10.1111/dom.12325. [DOI] [PubMed] [Google Scholar]
- 82.Kadowaki T, Haneda M, Inagaki N, Terauchi Y, Taniguchi A, Koiwai K, Rattunde H, Woerle HJ, Broedl UC. Empagliflozin monotherapy in Japanese patients with type 2 diabetes mellitus: a randomized, 12-week, double-blind, placebo-controlled, phase II trial. Adv Ther. 2014;31:621–638. doi: 10.1007/s12325-014-0126-8. [DOI] [PubMed] [Google Scholar]
- 83.Kashiwagi A, Kazuta K, Takinami Y, Yoshida S, Utsuno A, Nagase I. Ipragliflozin improves glycemic control in Japanese patients with type 2 diabetes mellitus: the BRIGHTEN study. Diabetol Int. 2015;6:8–18. [Google Scholar]
- 84.Hirose S, Nakajima S, Iwahashi Y, Seo A, Takahashi T, Tamori Y. Impact of the 8-week administration of tofogliflozin for glycemic control and body composition in Japanese patients with type 2 diabetes mellitus. Intern Med. 2016;55:3239–3245. doi: 10.2169/internalmedicine.55.6367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Ji L, Han P, Liu Y, Yang G, Dieu van NK, Vijapurkar U, Qiu R, Meininger G. Canagliflozin in Asian patients with type 2 diabetes on metformin alone or metformin in combination with sulphonylurea. Diabetes Obes Metab. 2015;17:23–31. doi: 10.1111/dom.12385. [DOI] [PubMed] [Google Scholar]
- 86.Kadowaki T, Inagaki N, Kondo K, Nishimura K, Kaneko G, Maruyama N, Nakanishi N, Iijima H, Watanabe Y, Gouda M. Efficacy and safety of canagliflozin as add-on therapy to teneligliptin in Japanese patients with type 2 diabetes mellitus: results of a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Obes Metab. 2017;19:874–882. doi: 10.1111/dom.12898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Kadowaki T, Inagaki N, Kondo K, Nishimura K, Kaneko G, Maruyama N, Nakanishi N, Watanabe Y, Gouda M, Iijima H. Long-term safety and efficacy of canagliflozin as add-on therapy to teneligliptin in Japanese patients with type 2 diabetes. Diabetes Obes Metab. 2018;20:77–84. doi: 10.1111/dom.13038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Araki E, Tanizawa Y, Tanaka Y, Taniguchi A, Koiwai K, Kim G, Salsali A, Woerle HJ, Broedl UC. Long-term treatment with empagliflozin as add-on to oral antidiabetes therapy in Japanese patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2015;17:665–674. doi: 10.1111/dom.12464. [DOI] [PubMed] [Google Scholar]
- 89.Kashiwagi A, Kazuta K, Goto K, Yoshida S, Ueyama E, Utsuno A. Ipragliflozin in combination with metformin for the treatment of Japanese patients with type 2 diabetes: ILLUMINATE, a randomized, double-blind, placebo-controlled study. Diabetes Obes Metab. 2015;17:304–308. doi: 10.1111/dom.12331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Kashiwagi A, Shiga T, Akiyama N, Kazuta K, Utsuno A, Yoshida S, Ueyama E. Efficacy and safety of ipragliflozin as an add-on to pioglitazone in Japanese patients with inadequately controlled type 2 diabetes: a randomized, double-blind, placebo-controlled study (the SPOTLIGHT study) Diabetol Int. 2015;6:104–116. [Google Scholar]
- 91.Kashiwagi A, Akiyama N, Shiga T, Kazuta K, Utsuno A, Yoshida S, Ueyama E. Efficacy and safety of ipragliflozin as an add-on to a sulfonylurea in Japanese patients with inadequately controlled type 2 diabetes: results of the randomized, placebo-controlled, double-blind, phase III EMIT study. Diabetol Int. 2015;6:125–138. [Google Scholar]
- 92.Ikeda S, Takano Y, Cynshi O, Tanaka R, Christ AD, Boerlin V, Beyer U, Beck A, Ciorciaro C, Meyer M, Kadowaki T. A novel and selective sodium-glucose cotransporter-2 inhibitor, tofogliflozin, improves glycaemic control and lowers body weight in patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2015;17:984–993. doi: 10.1111/dom.12538. [DOI] [PubMed] [Google Scholar]
- 93.Inagaki N, Harashima S, Maruyama N, Kawaguchi Y, Goda M, Iijima H. Efficacy and safety of canagliflozin in combination with insulin: a double-blind, randomized, placebo-controlled study in Japanese patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2016;15:89. doi: 10.1186/s12933-016-0407-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Inagaki N, Harashima SI, Kaku K, Kondo K, Maruyama N, Otsuka M, Kawaguchi Y, Iijima H. Long-term efficacy and safety of canagliflozin in combination with insulin in Japanese patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2018;20:812–820. doi: 10.1111/dom.13152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Yang W, Ma J, Li Y, Li Y, Zhou Z, Kim JH, Zhao J, Ptaszynska A. Dapagliflozin as add-on therapy in Asian patients with type 2 diabetes inadequately controlled on insulin with or without oral antihyperglycemic drugs: a randomized controlled trial. J Diabetes. 2018;10:589–599. doi: 10.1111/1753-0407.12634. [DOI] [PubMed] [Google Scholar]
- 96.Ishihara H, Yamaguchi S, Nakao I, Okitsu A, Asahina S. Efficacy and safety of ipragliflozin as add-on therapy to insulin in Japanese patients with type 2 diabetes mellitus (IOLITE): a multi-centre, randomized, placebo-controlled, double-blind study. Diabetes Obes Metab. 2016;18:1207–1216. doi: 10.1111/dom.12745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Terauchi Y, Tamura M, Senda M, Gunji R, Kaku K. Efficacy and safety of tofogliflozin in Japanese patients with type 2 diabetes mellitus with inadequate glycaemic control on insulin therapy (J-STEP/INS): results of a 16-week randomized, double-blind, placebo-controlled multicentre trial. Diabetes Obes Metab. 2017;19:1397–1407. doi: 10.1111/dom.12957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Terauchi Y, Tamura M, Senda M, Gunji R, Kaku K. Long-term safety and efficacy of tofogliflozin as add-on to insulin in patients with type 2 diabetes: results from a 52-week, multicentre, randomized, double-blind, open-label extension, phase 4 study in Japan (J-STEP/INS) Diabetes Obes Metab. 2018;20:1176–1185. doi: 10.1111/dom.13213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Suzuki K, Mitsuma Y, Sato T, Anraku T, Hatta M. Comparison of combined tofogliflozin and glargine, tofogliflozin added to insulin, and insulin dose-increase therapy in uncontrolled type 2 diabetes. J Clin Med Res. 2016;8:805–814. doi: 10.14740/jocmr2741w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.John M, Cerdas S, Violante R, Deerochanawong C, Hassanein M, Slee A, Canovatchel W, Hamilton G. Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus living in hot climates. Int J Clin Pract. 2016;70:775–785. doi: 10.1111/ijcp.12868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Yang W, Ji L, Zhou Z, Cain VA, Johnsson KM, Sjostrom CD. Efficacy and safety of dapagliflozin in Asian patients: a pooled analysis. J Diabetes. 2017;9:787–799. doi: 10.1111/1753-0407.12484. [DOI] [PubMed] [Google Scholar]
- 102.Yoon KH, Nishimura R, Lee J, Crowe S, Salsali A, Hach T, Woerle HJ. Efficacy and safety of empagliflozin in patients with type 2 diabetes from Asian countries: pooled data from four phase III trials. Diabetes Obes Metab. 2016;18:1045–1049. doi: 10.1111/dom.12699. [DOI] [PubMed] [Google Scholar]
- 103.Prasanna Kumar KM, Mohan V, Sethi B, Gandhi P, Bantwal G, Xie J, Meininger G, Qiu R. Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus from India. Indian J Endocrinol Metab. 2016;20:372–380. doi: 10.4103/2230-8210.179996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Seino Y, Inagaki N, Haneda M, Kaku K, Sasaki T, Fukatsu A, Ubukata M, Sakai S, Samukawa Y. Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus. J Diabetes Investig. 2015;6:443–453. doi: 10.1111/jdi.12316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Utsunomiya K, Shimmoto N, Senda M, Kurihara Y, Gunji R, Fujii S, Kakiuchi S, Fujiwara H, Kameda H, Tamura M, Kaku K. Safety and effectiveness of tofogliflozin in elderly Japanese patients with type 2 diabetes mellitus: a post-marketing study (J-STEP/EL Study) J Diabetes Investig. 2017;8:766–775. doi: 10.1111/jdi.12626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Nakamura I, Maegawa H, Tobe K, Tabuchi H, Uno S. Safety and efficacy of ipragliflozin in Japanese patients with type 2 diabetes in real-world clinical practice: interim results of the STELLA-LONG TERM post-marketing surveillance study. Expert Opin Pharmacother. 2018;19:189–201. doi: 10.1080/14656566.2017.1408792. [DOI] [PubMed] [Google Scholar]
- 107.Musso G, Gambino R, Cassader M, Pagano G. A novel approach to control hyperglycemia in type 2 diabetes: sodium glucose co-transport (SGLT) inhibitors: systematic review and meta-analysis of randomized trials. Ann Med. 2012;44:375–393. doi: 10.3109/07853890.2011.560181. [DOI] [PubMed] [Google Scholar]
- 108.Kaku K, Maegawa H, Tanizawa Y, Kiyosue A, Ide Y, Tokudome T, Hoshino Y, Yang J, Langkilde AM. Dapagliflozin as monotherapy or combination therapy in Japanese patients with type 2 diabetes: an open-label study. Diabetes Ther. 2014;5:415–433. doi: 10.1007/s13300-014-0086-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Ohta A, Kato H, Ishii S, Sasaki Y, Nakamura Y, Nakagawa T, Nagai Y, Tanaka Y. Ipragliflozin, a sodium glucose co-transporter 2 inhibitor, reduces intrahepatic lipid content and abdominal visceral fat volume in patients with type 2 diabetes. Expert Opin Pharmacother. 2017;18:1433–1438. doi: 10.1080/14656566.2017.1363888. [DOI] [PubMed] [Google Scholar]
- 110.Nishio SI, Sekido T, Ohkubo Y, Oiwa A, Komatsu M. Long-term effects of ipragliflozin on adipose tissue in Japanese patients with obese type 2 diabetes. Shinshu Med J. 2018;66:29–37. [Google Scholar]
- 111.Koshizaka M, Ishikawa K, Ishibashi R, Maezawa Y, Sakamoto K, Uchida D, Nakamura S, Yamaga M, Yokoh H, Kobayashi A, Onishi S, Kobayashi K, Ogino J, Hashimoto N, Tokuyama H, Shimada F, Ohara E, Ishikawa T, Shoji M, Ide S, Ide K, Baba Y, Hattori A, Kitamoto T, Horikoshi T, Shimofusa R, Takahashi S, Nagashima K, Sato Y, Takemoto M, Newby LK, Yokote K PRIME-V Study Group. Comparing the effects of ipragliflozin versus metformin on visceral fat reduction and metabolic dysfunction in Japanese patients with type 2 diabetes treated with sitagliptin: a prospective, multicentre, open-label, blinded-endpoint, randomized controlled study (PRIME-V study) Diabetes Obes Metab. 2019;21:1990–1995. doi: 10.1111/dom.13750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Yamamoto C, Miyoshi H, Ono K, Sugawara H, Kameda R, Ichiyama M, Yamamoto K, Nomoto H, Nakamura A, Atsumi T. Ipragliflozin effectively reduced visceral fat in Japanese patients with type 2 diabetes under adequate diet therapy. Endocr J. 2016;63:589–596. doi: 10.1507/endocrj.EJ15-0749. [DOI] [PubMed] [Google Scholar]
- 113.Sugiyama S, Jinnouchi H, Kurinami N, Hieshima K, Yoshida A, Jinnouchi K, Nishimura H, Suzuki T, Miyamoto F, Kajiwara K, Jinnouchi T. Dapagliflozin reduces fat mass without affecting muscle mass in type 2 diabetes. J Atheroscler Thromb. 2018;25:467–476. doi: 10.5551/jat.40873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Okamoto A, Yokokawa H, Sanada H, Naito T. Changes in levels of biomarkers associated with adipocyte function and insulin and glucagon kinetics during treatment with dapagliflozin among obese type 2 diabetes mellitus patients. Drugs R D. 2016;16:255–261. doi: 10.1007/s40268-016-0137-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Roh E, Kim KM, Park KS, Kim YJ, Chun EJ, Choi SH, Park KS, Jang HC, Lim S. Comparison of pancreatic volume and fat amount linked with glucose homeostasis between healthy Caucasians and Koreans. Diabetes Obes Metab. 2018;20:2642–2652. doi: 10.1111/dom.13447. [DOI] [PubMed] [Google Scholar]
- 116.Snel M, Jonker JT, Schoones J, Lamb H, de Roos A, Pijl H, Smit JW, Meinders AE, Jazet IM. Ectopic fat and insulin resistance: pathophysiology and effect of diet and lifestyle interventions. Int J Endocrinol. 2012;2012:983814. doi: 10.1155/2012/983814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Kuchay MS, Krishan S, Mishra SK, Farooqui KJ, Singh MK, Wasir JS, Bansal B, Kaur P, Jevalikar G, Gill HK, Choudhary NS, Mithal A. Effect of empagliflozin on liver fat in patients with type 2 diabetes and nonalcoholic fatty liver disease: a randomized controlled trial (E-LIFT trial) Diabetes Care. 2018;41:1801–1808. doi: 10.2337/dc18-0165. [DOI] [PubMed] [Google Scholar]
- 118.Ito D, Shimizu S, Inoue K, Saito D, Yanagisawa M, Inukai K, Akiyama Y, Morimoto Y, Noda M, Shimada A. Comparison of ipragliflozin and pioglitazone effects on nonalcoholic fatty liver disease in patients with type 2 diabetes: a randomized, 24-week, open-label, active-controlled trial. Diabetes Care. 2017;40:1364–1372. doi: 10.2337/dc17-0518. [DOI] [PubMed] [Google Scholar]
- 119.Bouchi R, Terashima M, Sasahara Y, Asakawa M, Fukuda T, Takeuchi T, Nakano Y, Murakami M, Minami I, Izumiyama H, Hashimoto K, Yoshimoto T, Ogawa Y. Luseogliflozin reduces epicardial fat accumulation in patients with type 2 diabetes: a pilot study. Cardiovasc Diabetol. 2017;16:32. doi: 10.1186/s12933-017-0516-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Fukuda T, Bouchi R, Terashima M, Sasahara Y, Asakawa M, Takeuchi T, Nakano Y, Murakami M, Minami I, Izumiyama H, Hashimoto K, Yoshimoto T, Ogawa Y. Ipragliflozin reduces epicardial fat accumulation in non-obese type 2 diabetic patients with visceral obesity: a pilot study. Diabetes Ther. 2017;8:851–861. doi: 10.1007/s13300-017-0279-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Grandy S, Hashemi M, Langkilde AM, Parikh S, Sjostrom CD. Changes in weight loss-related quality of life among type 2 diabetes mellitus patients treated with dapagliflozin. Diabetes Obes Metab. 2014;16:645–650. doi: 10.1111/dom.12263. [DOI] [PubMed] [Google Scholar]
- 122.Nakajima H, Okada S, Mohri T, Kanda E, Inaba N, Hirasawa Y, Seino H, Kuroda H, Hiyoshi T, Niiya T, Ishii H. Dapagliflozin improves treatment satisfaction in overweight patients with type 2 diabetes mellitus: a patient reported outcome study (PRO study) Diabetol Metab Syndr. 2018;10:11. doi: 10.1186/s13098-018-0313-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Cai J, Delahanty LM, Akapame S, Slee A, Traina S. Impact of canagliflozin treatment on health-related quality of life among people with type 2 diabetes mellitus: a pooled analysis of patient-reported outcomes from randomized controlled trials. Patient. 2018;11:341–352. doi: 10.1007/s40271-017-0290-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Look AHEAD Research Group. Wing RR, Bolin P, Brancati FL, Bray GA, Clark JM, Coday M, Crow RS, Curtis JM, Egan CM, Espeland MA, Evans M, Foreyt JP, Ghazarian S, Gregg EW, Harrison B, Hazuda HP, Hill JO, Horton ES, Hubbard VS, Jakicic JM, Jeffery RW, Johnson KC, Kahn SE, Kitabchi AE, Knowler WC, Lewis CE, Maschak-Carey BJ, Montez MG, Murillo A, Nathan DM, Patricio J, Peters A, Pi-Sunyer X, Pownall H, Reboussin D, Regensteiner JG, Rickman AD, Ryan DH, Safford M, Wadden TA, Wagenknecht LE, West DS, Williamson DF, Yanovski SZ. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369:145–154. doi: 10.1056/NEJMoa1212914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Look AHEAD Research Group. Gregg EW, Jakicic JM, Blackburn G, Bloomquist P, Bray GA, Clark JM, Coday M, Curtis JM, Egan C, Evans M, Foreyt J, Foster G, Hazuda HP, Hill JO, Horton ES, Hubbard VS, Jeffery RW, Johnson KC, Kitabchi AE, Knowler WC, Kriska A, Lang W, Lewis CE, Montez MG, Nathan DM, Neiberg RH, Patricio J, Peters A, Pi-Sunyer X, Pownall H, Redmon B, Regensteiner J, Rejeski J, Ribisl PM, Safford M, Stewart K, Trence D, Wadden TA, Wing RR, Yanovski SZ. Association of the magnitude of weight loss and changes in physical fitness with long-term cardiovascular disease outcomes in overweight or obese people with type 2 diabetes: a post-hoc analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol. 2016;4:913–921. doi: 10.1016/S2213-8587(16)30162-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Faulconbridge LF, Wadden TA, Rubin RR, Wing RR, Walkup MP, Fabricatore AN, Coday M, Van Dorsten B, Mount DL, Ewing LJ Look AHEAD Research Group. One-year changes in symptoms of depression and weight in overweight/obese individuals with type 2 diabetes in the Look AHEAD study. Obesity (Silver Spring) 2012;20:783–793. doi: 10.1038/oby.2011.315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Foster GD, Borradaile KE, Sanders MH, Millman R, Zammit G, Newman AB, Wadden TA, Kelley D, Wing RR, Pi-Sunyer FX, Reboussin D, Kuna ST Sleep AHEAD Research Group of Look AHEAD Research Group. A randomized study on the effect of weight loss on obstructive sleep apnea among obese patients with type 2 diabetes: the Sleep AHEAD study. Arch Intern Med. 2009;169:1619–1626. doi: 10.1001/archinternmed.2009.266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Foy CG, Lewis CE, Hairston KG, Miller GD, Lang W, Jakicic JM, Rejeski WJ, Ribisl PM, Walkup MP, Wagenknecht LE Look AHEAD Research Group. Intensive lifestyle intervention improves physical function among obese adults with knee pain: findings from the Look AHEAD trial. Obesity (Silver Spring) 2011;19:83–93. doi: 10.1038/oby.2010.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Phelan S, Kanaya AM, Subak LL, Hogan PE, Espeland MA, Wing RR, Burgio KL, DiLillo V, Gorin AA, West DS, Brown JS Look AHEAD Research Group. Weight loss prevents urinary incontinence in women with type 2 diabetes: results from the Look AHEAD trial. J Urol. 2012;187:939–944. doi: 10.1016/j.juro.2011.10.139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Rejeski WJ, Ip EH, Bertoni AG, Bray GA, Evans G, Gregg EW, Zhang Q Look AHEAD Research Group. Lifestyle change and mobility in obese adults with type 2 diabetes. N Engl J Med. 2012;366:1209–1217. doi: 10.1056/NEJMoa1110294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Williamson DA, Rejeski J, Lang W, van Dorsten B, Fabricatore AN, Toledo K Look AHEAD Research Group. Impact of a weight management program on health-related quality of life in overweight adults with type 2 diabetes. Arch Intern Med. 2009;169:163–171. doi: 10.1001/archinternmed.2008.544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Look AHEAD Research Group. Effect of a long-term behavioural weight loss intervention on nephropathy in overweight or obese adults with type 2 diabetes: a secondary analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol. 2014;2:801–809. doi: 10.1016/S2213-8587(14)70156-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Aldekhail NM, Logue J, McLoone P, Morrison DS. Effect of orlistat on glycaemic control in overweight and obese patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2015;16:1071–1080. doi: 10.1111/obr.12318. [DOI] [PubMed] [Google Scholar]
- 134.Puzziferri N, Roshek TB, 3rd, Mayo HG, Gallagher R, Belle SH, Livingston EH. Long-term follow-up after bariatric surgery: a systematic review. JAMA. 2014;312:934–942. doi: 10.1001/jama.2014.10706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Zhou YH, Ma XQ, Wu C, Lu J, Zhang SS, Guo J, Wu SQ, Ye XF, Xu JF, He J. Effect of anti-obesity drug on cardiovascular risk factors: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2012;7:e39062. doi: 10.1371/journal.pone.0039062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Ferrannini G, Hach T, Crowe S, Sanghvi A, Hall KD, Ferrannini E. Energy balance after sodium-glucose cotransporter 2 inhibition. Diabetes Care. 2015;38:1730–1735. doi: 10.2337/dc15-0355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Ferrannini E, Muscelli E, Frascerra S, Baldi S, Mari A, Heise T, Broedl UC, Woerle HJ. Metabolic response to sodium-glucose cotransporter 2 inhibition in type 2 diabetic patients. J Clin Invest. 2014;124:499–508. doi: 10.1172/JCI72227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Daniele G, Xiong J, Solis-Herrera C, Merovci A, Eldor R, Tripathy D, DeFronzo RA, Norton L, Abdul-Ghani M. Dapagliflozin enhances fat oxidation and ketone production in patients with type 2 diabetes. Diabetes Care. 2016;39:2036–2041. doi: 10.2337/dc15-2688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Ferrannini E, Mark M, Mayoux E. CV protection in the EMPA-REG OUTCOME trial: a “thrifty substrate” hypothesis. Diabetes Care. 2016;39:1108–1114. doi: 10.2337/dc16-0330. [DOI] [PubMed] [Google Scholar]
- 140.Bonner C, Kerr-Conte J, Gmyr V, Queniat G, Moerman E, Thevenet J, Beaucamps C, Delalleau N, Popescu I, Malaisse WJ, Sener A, Deprez B, Abderrahmani A, Staels B, Pattou F. Inhibition of the glucose transporter SGLT2 with dapagliflozin in pancreatic alpha cells triggers glucagon secretion. Nat Med. 2015;21:512–517. doi: 10.1038/nm.3828. [DOI] [PubMed] [Google Scholar]
- 141.Lee PC, Ganguly S, Goh SY. Weight loss associated with sodium-glucose cotransporter-2 inhibition: a review of evidence and underlying mechanisms. Obes Rev. 2018;19:1630–1641. doi: 10.1111/obr.12755. [DOI] [PubMed] [Google Scholar]
- 142.Hawley SA, Ford RJ, Smith BK, Gowans GJ, Mancini SJ, Pitt RD, Day EA, Salt IP, Steinberg GR, Hardie DG. The Na+/glucose cotransporter inhibitor canagliflozin activates AMPK by inhibiting mitochondrial function and increasing cellular AMP levels. Diabetes. 2016;65:2784–2794. doi: 10.2337/db16-0058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Obata A, Kubota N, Kubota T, Iwamoto M, Sato H, Sakurai Y, Takamoto I, Katsuyama H, Suzuki Y, Fukazawa M, Ikeda S, Iwayama K, Tokuyama K, Ueki K, Kadowaki T. Tofogliflozin improves insulin resistance in skeletal muscle and accelerates lipolysis in adipose tissue in male mice. Endocrinology. 2016;157:1029–1042. doi: 10.1210/en.2015-1588. [DOI] [PubMed] [Google Scholar]
- 144.Xu L, Nagata N, Nagashimada M, Zhuge F, Ni Y, Chen G, Mayoux E, Kaneko S, Ota T. SGLT2 inhibition by empagliflozin promotes fat utilization and browning and attenuates inflammation and insulin resistance by polarizing M2 macrophages in diet-induced obese mice. EBioMedicine. 2017;20:137–149. doi: 10.1016/j.ebiom.2017.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Inzucchi SE, Zinman B, Wanner C, Ferrari R, Fitchett D, Hantel S, Espadero RM, Woerle HJ, Broedl UC, Johansen OE. SGLT-2 inhibitors and cardiovascular risk: proposed pathways and review of ongoing outcome trials. Diab Vasc Dis Res. 2015;12:90–100. doi: 10.1177/1479164114559852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Kimura G. Diuretic action of sodium-glucose cotransporter 2 inhibitors and its importance in the management of heart failure. Circ J. 2016;80:2277–2281. doi: 10.1253/circj.CJ-16-0780. [DOI] [PubMed] [Google Scholar]