

Abstract
Background
An increasing shortage of skilled personnel, including medical personnel, has been reported in many postindustrial economies. Persisting and growing trends in absenteeism and incapacity to work due to mental disorders are concerning and have increased political, economic, and scientific interest in better understanding and management of determinants related to the work environment and health.
Objective
This study protocol describes an integrated approach of social research methods to explore determinants of work-related stress in general practice teams as an example for micro, small, and medium-sized enterprises (SMEs).
Methods
The methods applied will allow an in-depth exploration of work practices and experiences relating to psychological well-being in general practice teams. An ethnographic approach will be used to develop an in-depth understanding of the drivers of work-related stress in general practice teams. We will combine participating observation and individual interviews with five to seven general practitioners (GPs), and five to seven focus group discussions with the nonphysician staff (3-4 participants per group) in approximately four GP group practices and one single practice in Germany. Data collection and analysis will follow a grounded theory approach.
Results
The Ethics Committee of the Medical Faculty, University Hospital of Tuebingen, Germany, has approved this study (reference number: 640/2017BO2). Recruitment has commenced with study completion anticipated in mid-2020.
Conclusions
The data from this project will be used in follow-up projects to develop and test an intervention to reduce and prevent work-related stress in GP practices and other SMEs.
International Registered Report Identifier (IRRID)
DERR1-10.2196/15809
Keywords: occupational health, work-related stress, small and medium-sized enterprises, general practice teams, ethnography, method triangulation, grounded theory
Introduction
Background
This study protocol describes an integrated approach of social research methods to explore work-related stress [1] in the primary care setting as an example for micro, small, and medium-sized enterprises (SMEs). We focus on general practice teams because they are particularly challenged by an increasingly complex, intense, and responsible working environment [2].
An increasing shortage of skilled medical personnel, including general practitioners (GPs) and physician’s assistants, has been reported in many postindustrial economies, such as the United States [3], Canada [4], the United Kingdom [5], and Germany [6]. This development has been linked to demographic change in these societies and other macroeconomic, political, and structural processes (eg, digitalization), which results in changing and challenging working environments that affect the mental health and well-being of employers and employees in all economic branches [7]. Managing economic and human resources are integral components of organizational and institutional development. A shortage of staff, together with a persisting and growing trend in absenteeism [8] and incapacity to work, has initiated political, economic, and scientific interest in better understanding and management of work-related stressors or psychosocial risks [9,10] and resources [11,12].
A European survey with a focus on workplace risks collected responses from approximately 50,000 enterprises, including questions on psychosocial risks and their management [7]. The results show that the proportion of establishments having an action plan to prevent work-related stress ranges from 60% in the United Kingdom to 8% in the Czech Republic (Germany: 20%) [13]. Compared with larger companies, SMEs with fewer than 250 employees have tighter financial and human resources; hence, health and safety can be of low priority, particularly affecting issues concerned with mental health [14]. However, enterprises in the nonfinancial business economy (eg, manufacturing, construction) account for 99.8% (Germany: 99.5%) of all enterprises across all European Union (EU) countries, including Norway and Switzerland, and 66.3% (Germany: 62.9%) of total employment [15], emphasizing the pivotal importance of ensuring health and safety for personnel working in smaller businesses.
Primary care practices are established microenterprises that have to be maintained and developed to be economically viable. Usually organized as single or group practices with independent practice owners, these microenterprises face increasing financial competition from new emerging health business models, such as large group practices or medical care centers in which a growing number of physicians are no longer self-employed [16,17]. Similar to other SMEs [18,19], many GPs close to retirement have difficulties finding successors, which has been related to a variety of factors, including relatively little recognition for GPs compared with specialists and increasingly unmanageable workloads [20]. This can jeopardize the existence of the entire business, which is concerning because the provision of regional health care is put at risk, with the availability of primary care in rural areas particularly affected [21,22].
Theoretical and Legal Frameworks Concerning Work-Related Stress
Although the proportion of physically strenuous work has been declining in many economically developed countries, growing job insecurity accompanied by high demands on employees’ flexibility and mobility have resulted in a shift from a hazardous physical environment to a more challenging and stressful psychosocial working environment [23]. Several relevant theoretical models have explained the development of work-related stress, such as the job demand-control model [24], the job demand-control-support model [25], the effort-reward-imbalance model [26], and the concept of organizational justice [27]. These models relate potentially harmful (eg, high workload and low scope of decision making) and beneficial working conditions (eg, social support and recognition, financial rewards, job security, organizational justice, or good leadership quality) to both physical and mental health (eg, cardiovascular diseases, depression) and health-related behaviors (eg, smoking and drinking) [7,9,28]. Therefore, these models play an important role in the development of concepts improving occupational health because they allow for the evaluation of measures preventing work-related stress.
From a legal perspective, the EU Agency for Safety and Health at Work provides guidelines for the improvement of working conditions implemented in European Health and Safety legislation based on Article 153 of the Lisbon Treaty [10,29]. Existing recommendations and guidelines concerning psychosocial factors in the working environment address both potentially harmful and protective dimensions [10,30-33]:
Work content (eg, job autonomy, completeness of tasks, variability of tasks, required qualification);
Work organization (eg, working time arrangements, possibility or need for communication or cooperation and delegation, working procedures, interruptions during specific tasks);
Social relations (eg, relationships between subordinates and leading personnel, hierarchies, leadership and managerial abilities);
Working environment (eg, workplace design and equipment) or working conditions (eg, noise, lighting); and
New forms of work (eg, increasing mobility, flexible and temporary working arrangements, telework, decreasing differentiation between work and leisure).
Work-Related Stress in Primary Care Practices
Higher levels of work-related stress have been reported in the health care setting compared with other economic sectors. Health care staff are exposed to a variety of well-established predictors of chronic stress, including high expectations in the workplace accompanied by insufficient resources (eg, time and personnel) and a lack of monetary, social, and work-related recognition [11,34]. A comparative study investigating work stress in primary care physicians across three different health care systems showed that the highest levels of physician work stress—due to effort and lack of rewards—were reported by German GPs, followed by physicians in the United States and the United Kingdom [35]. The study also highlighted the importance of work-related rewards (salary, career opportunities, and recognition) compared with other factors promoting or preventing work-related stress. Further research from England [36] and Germany [37,38] demonstrated a relatively high prevalence of psychological distress, perceived chronic stress, and burnout among workers in general practices compared with the general population.
Recent studies investigating psychosocial risks or work-related stressors [9,10] in the primary care setting have included specifically the profession of physician’s assistants. A recent systematic literature review highlighting career and job satisfaction in relation to burnout in physician’s assistants summarized several work-related factors unique to the profession, including the practice setting, team dynamics, and career flexibility [39]. The authors concluded that there is a lack of high-quality studies investigating occupational well-being in health care teams. The number of studies addressing the primary care environment was relatively low (7 of 37), highlighting the lack of research in this area. However, we have identified studies from Germany that provide further evidence for the relationship between psychosocial working conditions and the well-being of physician’s assistants [40-44].
Most studies to date have applied either quantitative (eg, cross-sectional research) or qualitative approaches (eg, interviews or focus group discussions). Participatory observation, an ethnographic approach, has also been applied in the health care setting to, for example, examine interprofessional communication within a clinical setting [45] or research complex interactions between doctors and nurses working in intensive care [46]. We identified very few studies in a medical setting in which ethnographic and other qualitative methods were applied in combination [46-49] to achieve a deeper understanding of aspects and circumstances related to occupational health. Furthermore, none of these were conducted in the general practice setting including both doctors and physician’s assistants, although the majority of patients (>65% in Germany and >95% the Netherlands) are treated by their GP before they see a specialist [50]. Therefore, a better understanding of occupational health and safety of health care personnel outside the hospital setting is of importance to mitigate and manage health system challenges at the local level (eg, dealing with multimorbidity, chronic disease, geriatric conditions, obesity, tobacco and alcohol consumption, provision of a family health strategy and prevention programs), which are key tasks of personnel working in the primary care setting.
Aims and Research Questions
This protocol is for a study that is part of the research collaboration IMPROVEjob funded by the German Federal Ministry of Education and Research (BMBF 01GL1751 A, B, C, and 01GL1851D) [51,52]. Researchers from four universities and six disciplines—occupational medicine, primary care, psychosomatic medicine, operations research, health promotion, and epidemiology—will collaborate within four consecutive work packages (see Multimedia Appendix 1). Within the research collaboration, we aim to develop a deeper understanding of factors related to the development and occurrence of work-related stress in primary care teams.
The focus of this protocol is related exclusively to the integrated qualitative approach that will be applied in work package 1. Modifiable, setting-specific factors considered relevant in this context are lack of leadership (eg, inexplicit description of responsibilities, poor prioritization), inefficient work processes (eg, long waiting times for patients, high frequency of interruptions), lack of communication (eg, within the practice team or with patients), insufficient implementation of occupational health and safety measures, and lack of occupational health promotion. The following questions will guide the analysis:
How is work organized within GP practice teams?
Which work-related resources and stressors are specific to the primary care setting?
Within the research collaboration IMPROVEjob, the findings will inform the development of a participatory intervention for the prevention of work-related stress within primary care teams (work package 2). Applying a cluster randomized controlled trial, the effect of the intervention will be assessed (work package 3) measuring the primary outcome “job satisfaction” and several secondary outcomes before and after the implementation of the intervention comparing possible changes between the intervention and the control group [53]. Finally, options for the transfer of the results into other medical practices and SMEs of other economic branches will be evaluated (work package 4).
Methods
Qualitative Methods
For the last three decades, qualitative methods have become an integral part of health-related and health services research. They provide tools for a comprehensive understanding of complex environmental, social, and cultural relationships within a particular setting. Ethnographic research design has been established in other disciplines but has yet found little application in research related to occupational health and safety. The study design conforms to the consolidated criteria for reporting qualitative research (COREQ) [54].
Study Design: Ethnography and Grounded Theory
An ethnographic technique will be used, including participatory observation accompanied by interviews with the practice owners and focus group discussions with the physician’s assistants. Observation will be guided by a theoretical framework developed through a transdisciplinary process [55,56] by the IMPROVEjob-Consortium based on occupational health and safety guidelines [10,30-33], while also considering life course-specific aspects relevant in the working environment (eg, professional training, pregnancy, dealing with illness and/or care, retirement). We will accompany different GP practice teams over a sustained period. This will allow the mapping of everyday work practices in relation to stressors [9,10] and resources [11,12] as they occur. Based on the observations, we will be able to capture aspects which the participants themselves are either not aware of or are unlikely to disclose in an interview situation, such as different forms of verbal and nonverbal communication (eg, gestures or impromptu responses to routine or nonroutine situations), as well as the dependency between work processes and work environment.
To further enrich the observational data, we will conduct a variety of interviews with the practice teams. Because we will experience teamwork and collaboration between the entire practice staff through observation, we decided to discuss additionally occurring aspects and themes separately with doctors and physician’s assistants acknowledging their different roles. This will create an atmosphere as unaffected as possible by structures of hierarchy and dependency. These qualitative interviews will be performed either as single interviews used mainly to collect the practice owners’ individual stories about everyday working life [57], or as focus group discussions [58] to capture the physician’s assistants perspective on how work is organized within the team and which work-related stressors [9,10] and resources [11,12] affect their daily routines [58].
The analysis of all data will follow a grounded theory approach, which is suitable for less-studied and complex research questions comprising the construction, modification, and evaluation of knowledge created through the reciprocal relationship between researchers and participants [59]. Grounded theory provides a systematic method to address initially unstructured data from different collection methods. Data collection and analysis are carried out alternatingly, allowing for the continuous development of emerging codes and themes until no new conceptual insights occur, and theoretical saturation is reached [59,60]. We will apply a triangulation of methods [60] (observation, individual interviews, and focus group discussions) to compare different perspectives (researcher, GPs, and physician’s assistants). Using these methods in combination, we expect to uncover different and potentially hidden work practices and interactions within the observed practice teams to understand, conceptualize, and evaluate how these relate to work-related resources and stressors relevant to the primary care setting.
Participatory Approach: Advisory Board and Research Support Group
To further ensure scientific rigor, an advisory board will offer guidance and support throughout the study. Members with a scientific and/or professional background in occupational health and safety, work design, or occupational health promotion, as well as scientists from two institutes of general medicine, will provide primarily theoretical and methodological expertise. The research support group, including GP practice staff (doctors and physician’s assistants), will provide advice on the practicalities of applying the ethnographic approach in the general practice setting; furthermore, they will take part in the validation of the emerging codes and themes throughout the analysis to improve the rigor and reliability of the results providing communicative validation [60]. A summary of the methods is displayed in Figure 1.
Figure 1.
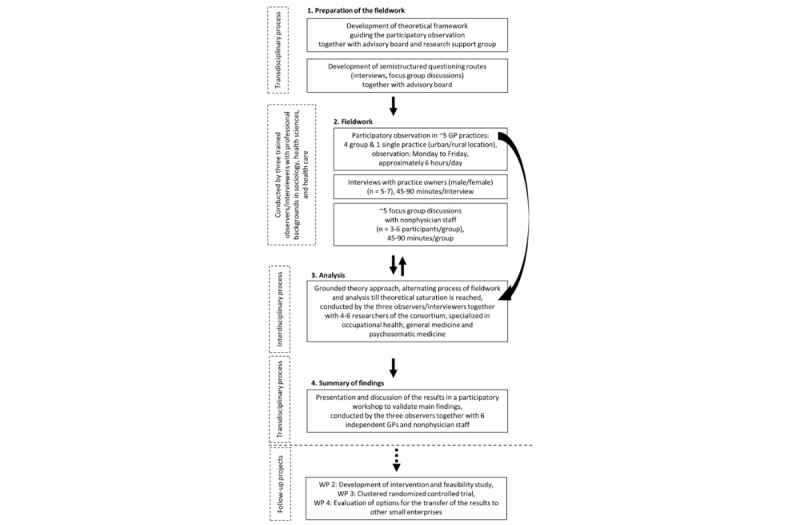
Flowchart of the methods that will be applied in work package 1.
Setting and Inclusion Criteria
To capture a variety of primary care settings, we plan to recruit approximately five practices (expected number of practices until theoretical saturation is reached): one single and four group practices in three urban and two rather rural areas, managed by male and/or female practice owners (purposive sampling). Prior research has shown that workload, income, and practice patterns differ frequently to the disadvantage of primary care physicians managing single practices [37] in rural areas [61,62]. Moreover, there is evidence that leadership styles can differ between men and women [63]. Leadership styles have also been related to job satisfaction; for example, transformational leadership has been shown to impact positively on workplace empowerment in the hospital setting, which increased the job satisfaction of nurses and promoted better safety outcomes for both staff and patients [64]. Furthermore, some national [65] and international [66,67] research has shown differences in job satisfaction between male and female GPs, with women being generally more satisfied at work [68]. However, for the perception of chronic stress and burnout, younger, female GPs working part-time have been reported to be more affected than their male colleagues [37,38].
Recruitment
Access to GP practices is planned through selective sampling via the network of GPs of the Institute for General Medicine, University Hospital Essen (IFAM, Germany). This network is representative of the primary care setting in Germany [69]. All participating practices in this network are located in urban and rural areas of North-Rhine-Westphalia (largest cities: Cologne, Duesseldorf, Dortmund, Essen), one of the most densely populated districts in Germany (population in 2017: 524 per square kilometer) [70]. Suitable GP practices will be invited via post and contacted by telephone if they agree to participate. During the phone call, practice owners will receive detailed information on the study and a schedule for the participatory observation (one working week: Monday to Friday), and the times for the interviews with the practice owners and the focus group discussions will be decided.
Preparation of the Field Work
In preparation for the fieldwork, all observers and interviewers will participate in a two-day methods course, which will include theoretical background on grounded theory and practical exercises concerning fieldwork and analysis. Each of the three female observers (with professional backgrounds in sociology, health sciences, and health care) will conduct a two-day trial observation in different GP practices to gain first impressions of the setting, its facilities, and organizational structures. The researchers will also have the opportunity to explore their role in the field and develop a feeling for suitable points of observation where they will attract as little attention as possible.
Data Collection and Sample Size
Data collection will take place in approximately five GP practices until theoretical saturation is achieved [71].
Participatory Observation
To allowing for comprehensive coverage during opening hours over the course of a workweek (Monday to Friday), each practice will be visited daily and in turn by two observers. According to previous studies [45,72], the observation time per person will be 2 to 4 hours to ensure the quality of the fieldwork. In agreement with the practice owners and the patients involved, the observers will attend as many situations and procedures as possible in areas such as reception, the waiting area, the kitchen, and in functional rooms (eg, laboratory, consultation room). Although the researchers will be in continuous contact with practice staff and patients, their aim is not to intervene actively in acute or sensitive events to avoid the disruption of procedures. If possible and appropriate, field notes will be taken, including the documentation of spontaneously occurring conversations with practice staff.
Interviews and Focus Group Discussions
All interviews and focus group discussions will follow up aspects that occurred over the course of the observations and will elaborate on particular situations, experiences, attitudes, and ambiguities. For both the interviews and discussions, we developed a semistructured questioning route including an introduction (short thematic intro, information on recording and data protection) and questions related to work content, work organization, social and working environment, as well as new forms of work [10,30-33]. Using a semistructured topic guide will provide the appropriate flexibility to guide the course of the interview. The researchers can clarify questions or can adapt the focus of the interview to further explore topics and phenomena that reoccur in different general practices. Depending on the availability of the practice staff, all individual interviews with the practice owners (approximately 5-7) and discussions (approximately 5, with 3-6 participants per discussion) are planned to last between 45 and 90 minutes. In agreement with the participants, all interviews and discussions will take place in the GP practices and will be digitally recorded, ensuring accuracy and completeness.
Data Management and Analysis
Observation protocols, complemented by material including spontaneous informal discussions with primary care staff and field notes, will be written by the participating researchers during or immediately following the fieldwork [73]. The transcription of the interviews and focus group discussions will be carried out by a professional company according to a simplified system whereby transcription is word-for-word, but not phonetic [74]. Quality checks, depersonalization, and pseudonymization of all data sources will be done by the team conducting the fieldwork. To facilitate the linkage and classification of all data sources, the software MAXQDA 2018 [75] will be used to organize the observational protocols, interviews, focus group transcripts, and emerging memos.
Data analysis will apply a grounded theory approach including open, axial, and selective coding as well as constant comparison of all material to develop codes, work out the relationships between the codes, and establish a narrative around selected core themes [76]. The analysis will be conducted by the investigators carrying out the fieldwork supported by an interdisciplinary team of researchers from the IMPROVEjob collaboration with expertise in general, psychosomatic, and occupational medicine.
Ethical Considerations
Individual declarations of informed written consent will need to be signed by all participating practice staff; each team member will have the opportunity to ask questions and revoke their participation at any time over the course of the study. Data management and storage will be subject to the EU General Data Protection Regulation. The data will be available only to persons involved in this research. Ethical approval for this study was obtained from the Ethics Committee of the Medical Faculty, University Hospital of Tuebingen, Germany (reference number: 640/2017BO2). This study complies with the Declaration of Helsinki, World Medical Association (1964), last revised October 2013 [77].
During fieldwork, all patients and other visitors will be informed about our study at the patient registration desk of the respective practice where a sign will refer to our study and the observing researchers. As working procedures involving patients are of interest only in terms of how work is organized and communicated within the GP team (eg, doctor-patient relationship), patients will be asked by the GP or physician’s assistant whether they agree to the observers being present in the treatment areas, and the observers will sign a declaration of confidentiality. However, we will neither collect nor analyze any patient-related information because this study focuses exclusively on the collaboration within the practice teams. All data sources will undergo the process of pseudonymization.
Results
Recruitment has commenced, and study completion is anticipated in mid-2020. On behalf of the IMPROVEjob-Consortium, the findings of this qualitative study (work package 1) will be disseminated via peer-reviewed publications, conferences, and workshops. The results will inform subsequent subprojects (work package 2-4) of the IMPROVEjob-project, including the development and evaluation of a participatory intervention for the prevention of work-related stress within primary care teams as an example for other SMEs.
Discussion
Principal Findings
This study protocol describes an integrated qualitative approach of social research methods to explore drivers of work-related stress in the primary care setting as an example for SMEs, including microenterprises. Criteria to ensure quality have been established, including persistent observation, member checks, and triangulation [60,78,79]. The triangulation of methods applied in this study will allow an in-depth exploration of work practices and experiences in relation to psychological well-being from different perspectives over a sustained period across a variety of GP practice teams, providing particular insight into values and ideas that are inherently difficult to capture (eg, team spirit, attitudes concerning patient care, workplace atmosphere). This is relevant because there is little research to date that applies a comprehensive approach to the study of work-related stress in SMEs such as GP practices. Reducing and preventing work-related stress is an important dimension in protecting the health and safety of employees as well as reducing illness-related costs.
Benefits of Transdisciplinary Research
The combination of scientific and practical expertise is a central prerequisite for transdisciplinary cooperation [55,56]. Transdisciplinary research networks thrive when an interdisciplinary academic and a practical consensus results in the integration of research ideas and results throughout the entire research process so that jointly developed knowledge and products can be shared with and used by the target audience. It is expected that the entire IMPROVEjob-project will have a positive effect on the prevention of work-related stress in not only the primary care setting. Other SMEs might benefit from the results learned from the experiences in the GP practices, which may eventually contribute to the promotion of psychosocial aspects of work-related health in other smaller businesses.
Limitations
From a practical and operational point of view, the recruitment of GPs for research has been shown to be challenging. This has been related to a variety of factors, including the high workload of GPs, skepticism in the applicability of the results, the feeling of being monitored and judged [80], and the sensitivity of the working environment regarding patient confidentiality and data security [81]. Furthermore, the ethnographic approach is prone to disrupting the usual working environment; researchers engage in participatory observation over a sustained period of time [82], which may cause an additional and unusual form of stress. Conducting this study within the collaborative research network, IMPROVEjob will provide resources to mitigate or overcome some of the challenges described. Over the course of the entire IMPROVEjob-project, the interdisciplinary research group will work closely together with the study’s target group of GP practice teams. For this subproject, the practitioners of the research support group will provide practical insight into the primary care setting, which will support the researchers with the familiarization of the setting, the recruitment of participating practices, as well as the organization and execution of the ethnographic fieldwork. The researchers will be invited into different GP practices and accompany the team for a week; therefore, we expect all participants (researchers, GPs, and physician’s assistants) to become familiar with this research approach so, ideally, it will cause as little disruption as possible.
Conclusion
It is expected that the entire IMPROVEjob-project will have a positive effect on the prevention of work-related stress inside and outside the primary care setting. Other SMEs might benefit from the results learned from the experiences in the GP practices, which may eventually contribute to the promotion of psychosocial aspects of occupational health in other small businesses.
Acknowledgments
Monika A Rieger, Birgitta Weltermann, Christine Kersting, Christine Preiser, Brigitte Werners, Florian Junne, Anne Herrmann-Werner, Claudia Pieper, Claudia Ose, and Karl-Heinz Jöckel wrote the funding application for the IMPROVEjob research collaboration. Birgitta Weltermann provided particular expertise on primary care and Monika A Rieger on occupational health. Thanks to all current and former members of the IMPROVEjob-Consortium (see Multimedia Appendix 2), including researchers from the University Hospitals Tuebingen, Bonn and Essen, and the Ruhr-University Bochum, Germany. Authors ER, SE, CP, ET, and MAR wrote this paper on behalf of the IMPROVEjob-Consortium.
The members of the IMPROVEjob-Consortium are as follows: MA Rieger; E Rind; A Siegel; S Burgess; E Tsarouha; F Junne; T Seifried-Dübon; F Stuber; A Herrmann-Werner; S Zipfel; B Weltermann; A Dreher; K Linden; B Werners; J Block; K-H Jöckel; C Pieper; A-L Eilerts; C Kersting; S Emerich; L Imhoff (Koppka); M Grot; C Ose; M Brinkmann; V Schröder; J-M Bois; M Hippler; S Kasten; L Degen; and A Wagner.
This work is supported by the German Federal Ministry of Education and Research (grant number FKZ 01GL1751A). In addition, the institutions’ own resources are used: the work of the Institute of Occupational and Social Medicine and Health Services Research Tuebingen is supported by an unrestricted grant of the Employers’ Association of the Metal and Electric Industry Baden-Wuerttemberg (Suedwestmetall). We gratefully acknowledge support by the German Research Foundation and the Open Access Publishing Fund of the University of Tuebingen.
Abbreviations
- EU
European Union
- GP
general practitioner
- IFAM
Insitut für Allgemeinmedizin, Universitätsklinikum Essen (Institute for General Medicine, University Hospital Essen)
- SME
small and medium-sized enterprise
Appendix
Evidence based for teams: aims of the transdisciplinary research consortium IMPROVEjob.
Current and former members of the IMPROVEjob-Consortium.
Review and proof ethics-English.
Review and proof ethics-German.
Review and proof of major funding - English.
Original peer review from the Federal Ministry of Education and Research - German.
Original peer review from the Federal Ministry of Education and Research - English.
Footnotes
Authors' Contributions: MR and CP developed the detailed qualitative research protocol. ER, ET, and SE contributed to the subsequent refinement of the analysis plan. MR, ER, SE, and ET were involved in obtaining approval from the Ethics Committee of the Medical Faculty, University Hospital of Tuebingen. ER is the primary investigator and drafted this study protocol with contributions from SE. All authors provided critical feedback on the manuscript and read and approved the final version.
Conflicts of Interest: None declared.
References
- 1.World Health Organization. [2019-10-28]. Stress at the workplace https://www.who.int/occupational_health/topics/stressatwp/en/
- 2.Baird B, Charles A, Honeyman M, Maguire D, Das P. The King's Fund. 2016. [2019-07-06]. Understanding pressures in general practice https://www.kingsfund.org.uk/publications/pressures-in-general-practice.
- 3.Dall T, West T, Chakrabarti R, Reynolds R, Iacobucci W. 2019 Update-The Complexities of Physician Supply and Demand: Projections from 2017 - 2032. Final Report. Washington, DC: Association of American Medical Colleges; 2019. Apr, [2019-11-12]. https://aamc-black.global.ssl.fastly.net/production/media/filer_public/31/13/3113ee5c-a038-4c16-89af-294a69826650/2019_update_-_the_complexities_of_physician_supply_and_demand_-_projections_from_2017-2032.pdf. [Google Scholar]
- 4.Hedden L, Barer ML, McGrail K, Law M, Bourgeault IL. In British Columbia, the supply of primary care physicians grew, but their rate of clinical activity declined. Health Aff (Millwood) 2017 Nov 19;36(11):1904–1911. doi: 10.1377/hlthaff.2017.0014. [DOI] [PubMed] [Google Scholar]
- 5.Barber S, Brettell R, Perera-Salazar R, Greenhalgh T, Harrington R. UK medical students' attitudes towards their future careers and general practice: a cross-sectional survey and qualitative analysis of an Oxford cohort. BMC Med Educ. 2018 Jul 04;18(1):160. doi: 10.1186/s12909-018-1197-z. https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-018-1197-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ulrich L, Pham TT, Gerlach FM, Erler A. [Family health teams in Ontario: ideas for Germany from a Canadian primary care model] Gesundheitswesen. 2019 Jun;81(6):492–497. doi: 10.1055/s-0043-111406. [DOI] [PubMed] [Google Scholar]
- 7.European Agency for Safety and Health at Work . Management of Psychosocial Risks in European Workplaces - Evidence from the Second European Survey of Enterprises on New and Emerging Risks (ESENER-2) Luxembourg: Publications Office of the European Union; 2018. [2019-05-17]. https://osha.europa.eu/en/tools-and-publications/publications/management-psychosocial-risks-european-workplaces-evidence/view. [Google Scholar]
- 8.World Health Organization. [2019-02-13]. Absenteeism from work due to illness, days per employee per year: 1970-2015 https://gateway.euro.who.int/en/indicators/hfa_411-2700-absenteeism-from-work-due-to-illness-days-per-employee-per-year/visualizations/#id=19398&tab=table.
- 9.European Agency for Safety and Health at Work. [2019-10-28]. Psychosocial risks and stress at work https://osha.europa.eu/en/themes/psychosocial-risks-and-stress.
- 10.Eurofound and European Agency for Safety and Health at Work . Psychosocial Risks in Europe: Prevalence and Strategies for Prevention. Luxembourg: Publications Office of the European Union; 2014. [2019-05-27]. https://osha.europa.eu/en/publications/reports/psychosocial-risks-eu-prevalence-strategies-prevention/view. [Google Scholar]
- 11.Bakker AB, Hakanen JJ, Demerouti E, Xanthopoulou D. Job resources boost work engagement, particularly when job demands are high. J Educ Psychol. 2007;99(2):274–284. doi: 10.1037/0022-0663.99.2.274. [DOI] [Google Scholar]
- 12.Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001 Jun;86(3):499–512. doi: 10.1037/0021-9010.86.3.499. [DOI] [PubMed] [Google Scholar]
- 13.European Agency for Safety and Health at Work. 2014. [2015-06-15]. ESENER-2: survey and statistics https://osha.europa.eu/en/surveys-and-statistics-osh/esener/2014.
- 14.European Agency for Safety and Health at Work . Promoting Health and Safety in European Small and Medum-Sized Enterprises (SMEs) Luxembourg: Office for Official Publications of the European Communities; 2005. [2019-05-27]. https://osha.europa.eu/en/tools-and-publications/publications/reports/ag05001. [Google Scholar]
- 15.Eurostat. 2018. [2019-02-13]. Statistics on small and medium-sized enterprises https://ec.europa.eu/eurostat/statistics-explained/index.php/Statistics_on_small_and_medium-sized_enterprises.
- 16.Schweizerische Ärztezeitung. 2006. Finanzierung von Arztpraxen [Financial aspects concerning general practices] https://saez.ch/journalfile/view/article/ezm_saez/de/saez.2006.12132/9eec91c64c95827bdd30ae118095d55f249ba3f4/saez_2006_12132.pdf/rsrc/jf.
- 17.Hohner H. Inhaberzentrierte Kleinunternehmen in organisationspsychologischer Perspektive - Das Beispiel Arztpraxis [Owner-centred small businesses from an organisational-psychological perspective - using general practices as an example]. Berichte aus dem Bereich. 1994. [2019-06-21]. https://www.ewi-psy.fu-berlin.de/einrichtungen/arbeitsbereiche/arbpsych/media/publikationen/forschungsberichte/fb_05.pdf.
- 18.Andric M, Bird M, Christen A, Gachet E, Halter F, Kissling S, Schenk R, Zellweger T. Company Succession in Practice: The Challenge of Generation Change. Zurich, Switzerland: Investment Solutions & Products; 2016. [2019-04-28]. https://www.alexandria.unisg.ch/248569/1/__SV-MONK_UNISG-Rfolder%24_FHalter_Desktop_2016-CS%28Unternehmensnachfolge%29_2016_EN_final.pdf. [Google Scholar]
- 19.Schwartz M. Generationenwechsel im Mittelstand: Bis 2019 werden 240.000 Nachfolger gesucht [Generation change in medium-sized businesses: 240,000 successors to be sought by 2019] KfW Research Fokus Volkswirtschaft. 2018;197:1–8. https://www.kfw.de/PDF/Download-Center/Konzernthemen/Research/PDF-Dokumente-Fokus-Volkswirtschaft/Fokus-2018/Fokus-Nr.-197-Januar-2018-Generationenwechsel.pdf. [Google Scholar]
- 20.National Health Executive. 2015. Jan 02, [2019-02-19]. Why don't doctors want to become GPs anymore? http://www.nationalhealthexecutive.com/Comment/why-dont-doctors-want-to-become-gps-anymore.
- 21.Hissbach J, Zimmermann S, Hampe W. Student selection cannot resolve the lack of general practitioners and country doctors. GMS J Med Educ. 2017;34(2):Doc16. doi: 10.3205/zma001093. doi: 10.3205/zma001093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kesternich I, Schumacher H, Winter J, Fischer MR, Holzer M. Student characteristics, professional preferences, and admission to medical school. GMS J Med Educ. 2017;34(1):Doc5. doi: 10.3205/zma001082. doi: 10.3205/zma001082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Siegrist J, Li J. Work stress and the development of chronic diseases. Int J Environ Res Public Health. 2018 Mar 16;15(3):pii: E536. doi: 10.3390/ijerph15030536. http://www.mdpi.com/resolver?pii=ijerph15030536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Karasek R, Theorell T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life. New York: Basic Books, Inc; 1990. [Google Scholar]
- 25.Johnson JV, Hall EM. Job strain, work place social support, and cardiovascular disease: a cross-sectional study of a random sample of the Swedish working population. Am J Public Health. 1988 Oct;78(10):1336–1342. doi: 10.2105/ajph.78.10.1336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Siegrist J. Effort-reward imbalance at work and health. In: Siegrist J, editor. Historical and Current Perspectives on Stress and Health. Bingley, UK: Emerald Group Publishing Limited; 2002. pp. 261–291. [Google Scholar]
- 27.Greenberg J. Taxonomy of Organizational Justice Theories. Acad Manage Rev. 1987;12(1):9–22. [Google Scholar]
- 28.Junne F, Rieger M, Michaelis M, Nikendei C, Gündel H, Zipfel S, Rothermund E. Psychische Belastungsfaktoren in der Arbeitswelt: Modelle und Prävention [Psychological stress factors in the work environment: models and prevention] Psychother Psychosom Med Psychol. 2017;67(3-4):161–173. doi: 10.1055/s-0043-103270. [DOI] [PubMed] [Google Scholar]
- 29.Panizza R. Fact Sheets on the European Union. 2018. [2019-02-13]. The Treaty of Lisbon http://www.europarl.europa.eu/factsheets/en/sheet/5/the-treaty-of-lisbon.
- 30.Gemeinsame Deutsche Arbeitsschutzstrategie (GDA) Occupational Safety and Health in Practice. Recommendations for implementing psychosoical risk assessement. Berlin: Management of the GDA Mental Health Working Programme; 2014. [2019-10-28]. https://tinyurl.com/tg224n2. [Google Scholar]
- 31.Bundesanstalt für Arbeitsschutz und Arbeitsmedizin . Psychische Gesundheit in der Arbeitswelt-Wissenschaftliche Standortbestimmung. Forschung Projekt F 2353 [Mental health in the work environment - a scientific assessment] Dortmund: Bundesanstalt für Arbeitsschutz und Arbeitsmedizin; 2017. [2019-05-27]. https://www.baua.de/DE/Angebote/Publikationen/Berichte/Psychische-Gesundheit.pdf?__blob=publicationFile. [Google Scholar]
- 32.GDA-Arbeitsprogramm Psyche . Arbeitsschutz in der Praxis. Psychische Arbeitsbelastung und Gesundheit. Artikelnummer: A097 [Occupational health and safety in practice. Psychological stress and health] Berlin: Gemeinsame Deutsche Arbeitsschutzstrategie; 2017. [2019-05-27]. https://www.gda-psyche.de/SharedDocs/Publikationen/DE/psychische-arbeitsbelastung-und-gesundheit.pdf?__blob=publicationFile&v=1. [Google Scholar]
- 33.Gemeinsame Deutsche Arbeitsschutzstrategie . Leitlinie Beratung und Überwachung bei psychischer Belastung am Arbeitsplatz [Guideline: counselling and monitoring of mental stress at the workplace] Berlin: Geschäftsstelle der Nationalen Arbeitsschutzkonferenz, c/o Bundesanstalt für Arbeitsschutz und Arbeitsmedizin; 2018. [2019-05-27]. http://www.gda-portal.de/DE/Downloads/pdf/Leitlinie-Psych-Belastung.pdf?__blob=publicationFile&v=5. [Google Scholar]
- 34.Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev. 2015;(4):CD002892. doi: 10.1002/14651858.CD002892.pub5. http://europepmc.org/abstract/MED/25847433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Siegrist J, Shackelton R, Link C, Marceau L, von dem Knesebeck O, McKinlay J. Work stress of primary care physicians in the US, UK and German health care systems. Soc Sci Med. 2010;71(2):298–304. doi: 10.1016/j.socscimed.2010.03.043. http://europepmc.org/abstract/MED/20494505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Calnan M, Wainwright D, Forsythe M, Wall B, Almond S. Mental health and stress in the workplace: the case of general practice in the UK. Soc Sci Med. 2001;52(4):499–507. doi: 10.1016/s0277-9536(00)00155-6. [DOI] [PubMed] [Google Scholar]
- 37.Dreher A, Theune M, Kersting C, Geiser F, Weltermann B. Prevalence of burnout among German general practitioners: comparison of physicians working in solo and group practices. PLoS One. 2019;14(2):e0211223. doi: 10.1371/journal.pone.0211223. http://dx.plos.org/10.1371/journal.pone.0211223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Viehmann A, Kersting C, Thielmann A, Weltermann B. Prevalence of chronic stress in general practitioners and practice assistants: personal, practice and regional characteristics. PLoS One. 2017;12(5):e0176658. doi: 10.1371/journal.pone.0176658. http://dx.plos.org/10.1371/journal.pone.0176658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Essary A, Bernard KS, Coplan B, Dehn R, Forister JG, Smith NE, Valentin LV. NAM Perspectives. Washington, DC: National Academy of Medicine; 2018. [2019-02-13]. Burnout and job and career satisfaction in the physician assistant profession: a review of the literature. Discussion paper https://nam.edu/wp-content/uploads/2018/11/Burnout-and-Satisfaction-in-the-PA-Profession.pdf. [Google Scholar]
- 40.Gavartina A, Zaroti S, Szecsenyi J, Miksch A, Ose D, Campbell SM, Goetz K. Practice assistants in primary care in Germany - associations with organizational attributes on job satisfaction. BMC Fam Pract. 2013 Aug 05;14:110. doi: 10.1186/1471-2296-14-110. https://bmcfampract.biomedcentral.com/articles/10.1186/1471-2296-14-110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Goetz K, Berger S, Gavartina A, Zaroti S, Szecsenyi J. How psychosocial factors affect well-being of practice assistants at work in general medical care?--a questionnaire survey. BMC Fam Pract. 2015 Nov 11;16:166. doi: 10.1186/s12875-015-0366-y. https://bmcfampract.biomedcentral.com/articles/10.1186/s12875-015-0366-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Goetz K, Campbell S, Broge B, Brodowski M, Steinhaeuser J, Wensing M, Szecsenyi J. Job satisfaction of practice assistants in general practice in Germany: an observational study. Fam Pract. 2013 Aug;30(4):411–417. doi: 10.1093/fampra/cmt015. [DOI] [PubMed] [Google Scholar]
- 43.Vu-Eickmann P, Li J, Müller A, Angerer P, Loerbroks A. Associations of psychosocial working conditions with health outcomes, quality of care and intentions to leave the profession: results from a cross-sectional study among physician assistants in Germany. Int Arch Occup Environ Health. 2018 Jul;91(5):643–654. doi: 10.1007/s00420-018-1309-4. [DOI] [PubMed] [Google Scholar]
- 44.Vu-Eickmann P, Loerbroks A. [Psychosocial working conditions of physician assistants: results from a qualitative study on occupational stress, resources, possible approaches to prevention and intervention needs] Z Evid Fortbild Qual Gesundhwes. 2017;126:43–51. doi: 10.1016/j.zefq.2017.06.005. [DOI] [PubMed] [Google Scholar]
- 45.Conn LG, Lingard L, Reeves S, Miller K, Russell A, Zwarenstein M. Communication channels in general internal medicine: a description of baseline patterns for improved interprofessional collaboration. Qual Health Res. 2009;19(7):943–953. doi: 10.1177/1049732309338282. [DOI] [PubMed] [Google Scholar]
- 46.Manias E, Street A. Nurse-doctor interactions during critical care ward rounds. J Clin Nurs. 2001;10(4):442–450. doi: 10.1046/j.1365-2702.2001.00504.x. [DOI] [PubMed] [Google Scholar]
- 47.Andersson A, Hallberg N, Timpka T. A model for interpreting work and information management in process-oriented healthcare organisations. Int J Med Inform. 2003;72(1-3):47–56. doi: 10.1016/j.ijmedinf.2003.09.001. [DOI] [PubMed] [Google Scholar]
- 48.Lewis K, Patel D, Yorston D, Charteris D. A qualitative study in the United Kingdom of factors influencing attendance by patients with diabetes at ophthalmic outpatient clinics. Ophthalmic Epidemiol. 2007;14(6):375–380. doi: 10.1080/09286580701375195. [DOI] [PubMed] [Google Scholar]
- 49.Schoot T, Proot I, Meulen RT, de Witte L. Actual interaction and client centeredness in home care. Clin Nurs Res. 2005;14(4):370–393. doi: 10.1177/1054773805280093. [DOI] [PubMed] [Google Scholar]
- 50.Linden M, Gothe H, Ormel J. Ländervergleich Deutschland/Niederlande: Der Hausarzt als Gatekeeper [Country comparison Germany/Netherlands: the general practitioner as gatekeeper] Dtsch Arztebl. 2004;101(39):A2600–A2602. https://www.aerzteblatt.de/archiv/43510/Laendervergleich-Deutschland-Niederlande-Der-Hausarzt-als-Gatekeeper. [Google Scholar]
- 51.Federal Ministry of Education and Research. 2017. [2019-06-08]. IMPROVEjob - Partizipative Intervention zur Verbesserung des psychischen Befindens von Arztpraxisteams: Ein Modell für Verhältnis- und Verhaltensprävention in KMU [IMPROVEjob - Participatory intervention to improve the psychological well-being in primary care practice teams: a model for structural and behavioural prevention in small and medium-sized enterprises] https://www.gesundheitsforschung-bmbf.de/de/improvejob-partizipative-intervention-zur-verbesserung-des-psychischen-befindens-von-6725.php.
- 52.IMPROVEjob-Consortium Transdisciplinary Research Collaboration IMPROVEjob [in German] 2019. [2019-06-08]. https://www.improvejob.de/
- 53.German Clinical Trials Register. 2019. [2019-10-28]. DRKS-ID: DRKS00012677-Participatory intervention to improve the psychological well-being in medical practice teams_ a model for structural and behavioral prevention in small and medium-sized enterprises https://www.drks.de/drks_web/setLocale_EN.do.
- 54.Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007 Dec;19(6):349–357. doi: 10.1093/intqhc/mzm042. http://intqhc.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=17872937. [DOI] [PubMed] [Google Scholar]
- 55.Defila R, Di Giulio A, Scheuermann M. Forschungsverbundmanagement - Handbuch für die Gestaltung inter- und transdisziplinärer Projekte [Management of Research Collaborations: Manual for the Design of Inter- and Transdisciplinary Projects] ETH Zürich: vdf Hochschulverlag AG; 2006. [Google Scholar]
- 56.Gibbons M, Nowotny H. The potential of transdisciplinarity. In: Gibbons M, Nowotny H, editors. Transdisciplinarity: Joint Problem Solving among Science, Technology, and Society: An Effective Way for Managing Complexity. Basel: Birkhaeuser Basel; 2001. pp. 67–80. [Google Scholar]
- 57.Britten N. Qualitative interviews in medical research. BMJ. 1995;311(6999):251–253. doi: 10.1136/bmj.311.6999.251. http://europepmc.org/abstract/MED/7627048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kitzinger J. Qualitative research. Introducing focus groups. BMJ. 1995;311(7000):299–302. doi: 10.1136/bmj.311.7000.299. http://europepmc.org/abstract/MED/7633241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Charmaz K. Constructing Grounded Theory. A Practical Guide Through Qualitative Analysis. 2nd Edition. Thousand Oaks, CA: SAGE Publications; 2014. [Google Scholar]
- 60.Al-Busaidi ZQ. Qualitative research and its uses in health care. Sultan Qaboos Univ Med J. 2008;8(1):11–19. http://europepmc.org/abstract/MED/21654952. [PMC free article] [PubMed] [Google Scholar]
- 61.Steinhaeuser J, Joos S, Szecsenyi J, Miksch A. A comparison of the workload of rural and urban primary care physicians in Germany: analysis of a questionnaire survey. BMC Fam Pract. 2011;12:112. doi: 10.1186/1471-2296-12-112. https://bmcfampract.biomedcentral.com/articles/10.1186/1471-2296-12-112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Weeks WB, Wallace AE. Rural-urban differences in primary care physicians' practice patterns, characteristics, and incomes. J Rural Health. 2008;24(2):161–170. doi: 10.1111/j.1748-0361.2008.00153.x. [DOI] [PubMed] [Google Scholar]
- 63.Eagly AH, Johannesen-Schmidt MC, van Engen ML. Transformational, transactional, and laissez-faire leadership styles: a meta-analysis comparing women and men. Psychol Bull. 2003;129(4):569–591. doi: 10.1037/0033-2909.129.4.569. [DOI] [PubMed] [Google Scholar]
- 64.Boamah SA, Spence Laschinger HK, Wong C, Clarke S. Effect of transformational leadership on job satisfaction and patient safety outcomes. Nurs Outlook. 2018;66(2):180–189. doi: 10.1016/j.outlook.2017.10.004. [DOI] [PubMed] [Google Scholar]
- 65.Götz K, Broge B, Willms S, Joos S, Szecsenyi J. Die Arbeitszufriedenheit von Allgemeinmedizinern [Job satisfaction of general practitioners] Med Klin (Munich) 2010;105(11):767–771. doi: 10.1007/s00063-010-8881-z. [DOI] [PubMed] [Google Scholar]
- 66.Chambers R, Campbell I. Gender differences in general practitioners at work. Br J Gen Pract. 1996;46(406):291–293. https://bjgp.org/cgi/pmidlookup?view=long&pmid=8762745. [PMC free article] [PubMed] [Google Scholar]
- 67.Goetz K, Jossen M, Szecsenyi J, Rosemann T, Hahn K, Hess S. Job satisfaction of primary care physicians in Switzerland: an observational study. Fam Pract. 2016;33(5):498–503. doi: 10.1093/fampra/cmw047. [DOI] [PubMed] [Google Scholar]
- 68.Clark AE. Job satisfaction and gender: Why are women so happy at work? Labour Economics. 1997 Dec;4(4):341–372. doi: 10.1016/S0927-5371(97)00010-9. [DOI] [Google Scholar]
- 69.Viehmann A, Thielmann A, Gesenhues S, Weltermann B. Repräsentieren akademische Hausarztpraxen die hausärztliche Regelversorgung? Eine methodische Annäherung [Do Academic Family Practices Reflect Routine Primary Care? A Methodological Approach] Zeitschrift für Allgemeinmedizin (ZFA) 2014;90(9):354–359. doi: 10.3238/zfa.2014.0354–0359. [DOI] [Google Scholar]
- 70.DESTATIS Bevölkerung in Deutschland [Population in Germany] [2019-02-13]. Pressemitteilung Nr. 347 vom 14.09.2018 https://www.destatis.de/DE/PresseService/Presse/Pressemitteilungen/2018/09/PD18_347_12411.html.
- 71.Aldiabat KM, Le Navenec C-L. Data saturation: the mysterious step in grounded theory methodology. Qual Rep. 2018;23(1):245–261. https://nsuworks.nova.edu/cgi/viewcontent.cgi?article=2994&context=tqr. [Google Scholar]
- 72.Low LP, Chien WT, Lam LW, Wong KK. A qualitative study protocol of ageing carers' caregiving experiences and their planning for continuation of care for their immediate family members with intellectual disability. BMC Geriatr. 2017 Apr 07;17(1):81. doi: 10.1186/s12877-017-0473-9. https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-017-0473-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Emerson R, Fretz R, Shaw L. Writing Ethnographic Fieldnotes. Chicago, IL: University of Chicago Press; 2011. [Google Scholar]
- 74.Dresing T, Pehl T. Praxisbuch Interview, Transkription & Analyse. Anleitungen und Regelsysteme für qualitativ Forschende [Research in practice: interviews, transcription & analysis. Instructions and control systems for qualitative researchers] Marburg: dr dresing & pehl GmbH; 2018. [2019-03-04]. https://www.audiotranskription.de/Praxisbuch-Transkription.pdf. [Google Scholar]
- 75.MAXQDA. 2018. [2018-03-12]. The art of data analysis https://www.maxqda.com/how-to-analyse-qualitative-data.
- 76.Glaser B, Strauss A, Paul A. Grounded Theory: Strategien qualitativer Forschung [Grounded Theory: Strategies in Qualitative Research] Bern: Huber; 2010. [Google Scholar]
- 77.World Medical Association. 2018. Jul 09, [2019-07-19]. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
- 78.Mays N, Pope C. Qualitative research in health care. Assessing quality in qualitative research. BMJ. 2000;320(7226):50–52. doi: 10.1136/bmj.320.7226.50. http://europepmc.org/abstract/MED/10617534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Rölker-Denker L, Kowalski C, Ansmann L, Hahn U, Hammer A, Auer R, Kostuj T, Nöst S. [DNVF-Memorandum III - Methods for Health Services Research, Part 4 - Concept and Methods for Organizational Health Services Research. Chapter 2 - Methodological Approaches for Organizational Health Services Research: Measures, Data Sources, Data Collection and Data Analysis] Gesundheitswesen. 2019 Mar;81(3):e72–e81. doi: 10.1055/a-0862-0565. http://www.thieme-connect.com/DOI/DOI?10.1055/a-0862-0565. [DOI] [PubMed] [Google Scholar]
- 80.Rosemann T, Szecsenyi J. General practitioners' attitudes towards research in primary care: qualitative results of a cross sectional study. BMC Fam Pract. 2004;5(1):31. doi: 10.1186/1471-2296-5-31. https://bmcfampract.biomedcentral.com/articles/10.1186/1471-2296-5-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Asch S, Connor SE, Hamilton EG, Fox SA. Problems in recruiting community-based physicians for health services research. J Gen Intern Med. 2000 Aug;15(8):591–599. doi: 10.1046/j.1525-1497.2000.02329.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0884-8734&date=2000&volume=15&issue=8&spage=591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Kawulich B. Participant observation as a data collection method. Forum Qual Soc Res. 2005;6(2):Art 43. http://www.qualitative-research.net/index.php/fqs/article/view/466/996. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Evidence based for teams: aims of the transdisciplinary research consortium IMPROVEjob.
Current and former members of the IMPROVEjob-Consortium.
Review and proof ethics-English.
Review and proof ethics-German.
Review and proof of major funding - English.
Original peer review from the Federal Ministry of Education and Research - German.
Original peer review from the Federal Ministry of Education and Research - English.