

Abstract
Objective
To investigate the association between maternal employment and childhood overweight in low- and middle-income countries (LMIC).
Design/Setting
We utilized cross-sectional data from forty-five Demographic and Health Surveys from 2010 to 2016 (n 268 763). Mothers were categorized as formally employed, informally employed or non-employed. We used country-specific logistic regression models to investigate the association between maternal employment and childhood overweight (BMI Z-score>2) and assessed heterogeneity in the association by maternal education with the inclusion of an interaction term. We used meta-analysis to pool the associations across countries. Sensitivity analyses included modelling BMI Z-score and normal weight (weight-for-age Z-score≥−2 to <2) as outcomes.
Subjects
Participants included children 0–5 years old and their mothers (aged 18–49 years).
Results
In most countries, neither formal nor informal employment was associated with childhood overweight. However, children of employed mothers, compared with children of non-employed mothers, had higher BMI Z-score and higher odds of normal weight. In countries where the association varied by education, children of formally employed women with high education, compared with children of non-employed women with high education, had higher odds of overweight (pooled OR=1·2; 95 % CI 1·0, 1·4).
Conclusions
We find no clear association between employment and child overweight. However, maternal employment is associated with a modestly higher BMI Z-score and normal weight, suggesting that employment is currently associated with beneficial effects on children’s weight status in most LMIC.
Keywords: Maternal employment, Childhood overweight, BMI Z-score, Low- and middle-income countries, Nutrition transition
Longitudinal studies from the USA and Canada have demonstrated an association between maternal employment and increased risk of childhood overweight( 1 – 4 ). Moreover, increasing maternal employment between 1968 and 2001 has been estimated to account for 10 % of the overall increase in overweight prevalence among children during this time period( 5 ). Maternal employment has also increased in low- and middle-income countries (LMIC). Over the past two decades, women’s participation in the labour force has increased by 15 percentage points and, on average, 50 % of women in LMIC are currently employed( 6 – 8 ). This increase coincides with an increase in childhood overweight in LMIC. Between 1990 and 2010, overweight prevalence among children aged 0–5 years increased from 4 to 6 %( 9 ). It is hypothesized that initially maternal employment in LMIC may be protective against undernutrition, since additional income may be allocated towards meeting children’s basic energy needs( 10 ). Although maternal employment can have positive impacts on households, as the economies in LMIC develop, there may also be unintended consequences for childhood obesity risk in LMIC, paralleling those observed in high-income countries.
Prior research provides some hypotheses on the mechanisms of the maternal employment–childhood overweight association. For example, one study indicated that the presence of a working mother was associated with increases in daily food intakes and total weekly expenditures( 11 ). However, as LMIC undergo their nutrition transitions and food environments and preferences change, lower- and middle-income households may use their income earned from employment to purchase energy-dense foods, which could increase the risk for childhood overweight( 12 , 13 ). Du et al. demonstrated that there is a positive income elasticity (i.e. the quantity demanded of a good, relative to change in income) for high-fat and animal-source foods, suggesting that high-fat and animal-source foods are increasingly consumed among low-income groups in LMIC as country-level gross domestic product (GDP) increases( 14 ). Similarly, portion sizes and the purchase of ultra-processed foods have increased and traditional diets are being supplemented with liberal amounts of oils( 15 ). Maternal employment may also have effects on maternal time allocation that could increase child overweight risk( 11 , 16 ). For example, working mothers may alter their preference towards more easily prepared foods or breast-feed for a shorter period of time( 11 , 17 ). Despite evidence suggesting that there are plausible mechanisms through which maternal employment could now be associated with child overweight in LMIC, only one prior study examines this relationship. Results from a small sample (forty-three children) in South Africa, an upper middle-income economy, suggested that children of working mothers had an eighteenfold higher odds of being overweight( 18 ).
The primary aim of the present study was to address key gaps in the literature by testing the hypothesis that maternal employment is associated with higher odds of overweight among children aged 0–5 years in LMIC, using the most recent data available from forty-five countries. Evaluating overweight risk among young children is important for several reasons. First, although the current public health burden of overweight among children aged 0–5 years in LMIC is lower than in high-income countries, overweight prevalence in this age group has increased by 65 % in the past 20 years and is expected to increase further( 9 , 19 – 22 ). Second, size tends to track through the life course as infants defined as obese or who are at the highest end of the distribution for BMI are more likely to be obese at later life stages( 22 – 27 ). Childhood overweight also has adverse consequences on adulthood cardiometabolic morbidity( 22 , 23 , 28 ). The secondary aim of the present study was to assess heterogeneity in the association between employment and childhood overweight by maternal education level, as prior literature suggests that the relationship between maternal employment and child nutritional status varies by maternal education and that women with higher educational attainment more often participate in formal sector employment( 1 , 4 , 29 , 30 ). A better understanding of the relationship between maternal employment and childhood overweight in LMIC is critical given the long-term adverse health consequences associated with childhood overweight and the potential need for additional policies designed to support women in the workplace( 22 , 23 , 28 ).
Methods
Data source and population
We utilized cross-sectional data from the Demographic and Health Surveys (DHS). The DHS are standardized, allowing for cross-country comparisons, and employ a multistage cluster sample design that is nationally representative( 31 ).
We utilized one survey per country from forty-five LMIC that met the following inclusion criteria: (i) it was the most recent survey administered between 2010 and June 2016; (ii) women were queried on their employment status; and (iii) the survey contained child anthropometrics. Four countries that had data available between 2010 and June 2016 were excluded because they did not have child anthropometrics. We included women, aged 18–49 years, who had at least one child aged 0–5 years (~45 % had one child, ~55 % had two or more children). Children residing outside the household were excluded (n 14 832 (3·5 %) across all forty-five countries). Our final analytic sample included 268 763 children from 121 917 mothers.
Our sample was limited to 0–5-year-old children, since: (i) this is the age range for which DHS routinely collects child anthropometry; and (ii) evaluating overweight risk among young children is important because childhood overweight has adverse consequences on risk of overweight and cardiometabolic morbidity at later life stages( 22 , 23 , 28 ).
Dependent variables
Overweight or obese (henceforth referred to as ‘overweight’), defined as BMI Z-score >2, served as our primary dependent variable( 32 ). Overweight was defined based on the age- and sex-specific 2006 WHO Child Growth Standards( 33 ). Individual-level weight (in kilograms) and length/height (length if the child was <2 years old; measured in centimetres) were measured by trained technicians( 34 ).
Primary independent variable
We modelled maternal employment as a three-category variable, namely formally employed, informally employed or non-employed, based on research indicating that: (i) many women employed in LMIC are engaged in informal employment; (ii) wages are more than 50 % lower in the informal sector; and (iii) the maternal employment–overweight relationship varies by the number of hours women work( 1 , 29 , 30 , 35 ). We describe women not participating in the labour force as ‘non-employed’ because this term includes persons who choose to not seek employment; ‘unemployed’ was not used because the term describes persons without jobs who are actively seeking employment( 36 ).
Employment type was defined based on the following four indicators: (i) employment status in the last 12 months (employed, non-employed); (ii) aggregate occupation category (skilled, unskilled; see online supplementary material, Supplemental Table 1); (iii) type of earnings (cash only, cash and in-kind, in-kind only, unpaid); and (iv) seasonality of employment (all year, seasonal/occasional employment). Formal employment included the following combinations: (i) employed, skilled occupation, cash-only earnings, employed all year; (ii) employed, skilled occupation, cash-only earnings, seasonal/occasional employment; and (iii) employed, unskilled occupation, cash-only earnings, employed all year. Other employed women were categorized as informally employed (see Supplemental Table 1).
Confounders and effect measure modifiers
We identified confounding factors a priori using a directed acyclic graph, which is a causal diagram used to characterize the relationship among variables thought to influence the primary independent and the dependent variables based on both theorized and documented relationships (see Fig. 1)( 37 ). In all models, confounders included maternal age (years), marital status (married or living together v. single, widowed, divorced), number of household members (a continuous variable), child’s age (months), child’s sex, and living with ones’ mother, mother-in-law or sister (as a proxy variable for childcare support).
Fig. 1.

Directed acyclic graph for the association between maternal employment and childhood overweight:  , exposure;
, exposure;  , outcome;
, outcome;  , adjusted variable;
, adjusted variable;  , unobserved (latent) variable;
, unobserved (latent) variable;  , other variable;
, other variable;  , causal path. Birth order was highly collinear with child’s age. Therefore, we controlled for child’s age in our primary models.
, causal path. Birth order was highly collinear with child’s age. Therefore, we controlled for child’s age in our primary models.
Based on prior literature suggesting that (i) the employment–nutritional status relationship varies by maternal educational attainment and (ii) education may be a determinant of participation in formal v. informal sector employment, we tested for effect modification by maternal education by including an interaction term( 1 , 4 , 29 , 30 , 38 ). We hypothesized a priori that within the formal or informal sector, better-educated, more skilled mothers are likely to have higher-skilled occupations that contribute to their sense of self-worth, improve decision-making power and increase their efficiency of time use, which could facilitate high-education mothers, compared with low-education mothers, differentially prioritizing health and nutrition( 39 , 40 ). Less-educated mothers likely have lower-skilled jobs, within the formal or informal sector, and co-workers who may be less knowledgeable about health-promoting nutrition practices and therefore less likely to share ideas regarding nutrition. Additionally, mothers with lower educational attainment may enter the workforce out of necessity, whereas mothers with higher educational attainment may do so voluntarily. This is generally consistent with Goldin’s hypothesis, which proposes a U-shaped relationship between country level of economic development, coinciding with an increase in average educational attainment, and labour force participation( 41 ). Goldin’s hypothesis suggests that women’s participation is highest in low-income countries, where average educational attainment is lower and women work out of necessity. In lower middle-income countries, female labour force participation is lower; the bottom of the U-shape occurs in countries with incomes of about $US 2500 per capita (in 1980) and is thought to be due in part to relatively lower wages for agriculture-based jobs in these countries. In these contexts, the opportunity costs of employment may not outweigh the perceived benefits of remaining at home. As economic development continues to increase (i.e. countries transition to upper middle-income or high-income), education levels rise and women re-enter the work force to take advantage of relatively skilled jobs as they emerge. Across all LMIC in this sample, approximately 50 % of women had less than a primary level of school completed. Therefore, education was modelled as a binary variable, with low education defined as less than a primary level of education completed and high education defined as at least primary school completed.
We hypothesized that the employment–overweight association would vary by countries’ stage in the nutrition transition because the socio-economic gradient of overweight prevalence shifts as countries economically develop( 42 ). We explored differences in the country-level associations by log(GDP per capita), adjusted for purchasing power parity and percentage urban, both theorized drivers of the nutrition transition( 12 ). These data were obtained from the World Development Indicators database, corresponding to the survey year( 43 ). GDP per capita was log-transformed to reflect the expected influence of a percentage increase (e.g. 10 %), rather than an absolute dollar increase (e.g. $US 10). Percentage urban was defined as the number of people living in urban areas divided by the total population.
Statistical analyses
Within-country analyses
We employed separate multivariable logistic regression models for each country to test the association between maternal employment and childhood overweight. Taylor-series linearized se accounted for the clustered design and we utilized DHS sampling weights to account for differential probability of selection and response.
With the inclusion of an interaction term, we tested for effect modification in the maternal employment–child overweight association by maternal educational attainment in our primary models, using a post hoc Wald test. We retained the interaction term only if it was statistically significant (n 7). In countries where the association did not vary by education (n 38), education was included as a confounder.
Between-country analyses
After obtaining disaggregated estimates for each country, coefficients for the employment–overweight associations were entered into a meta-analysis to obtain OR pooled across countries. Random-effects meta-analysis, used to generate pooled OR (POR), is the statistical combination of the estimates from separate countries (i.e. it utilizes the country-specific β coefficient) and assumes that the magnitude of the association between employment and overweight may differ by country. We estimated POR for three subgroups: (i) children in countries where the association did not vary by maternal education; (ii) children of women with low educational attainment in countries where the association varied by maternal education; and (iii) children of women with high educational attainment in countries where the association varied by education. Additionally, country-specific β coefficients were entered into a random-effects meta-regression in order to assess whether the association between employment and child overweight varied by country-level log(GDP) and percentage urban( 44 ).
Sensitivity analyses
Sensitivity analyses included modelling BMI Z-score (measured continuously) and at-risk-of-overweight (BMI Z-score>1) as the outcomes. We also modelled underweight (weight-for-age Z-score (WAZ)<−2) and normal weight (defined both as WAZ ≥−2 to <2 and BMI Z-score ≥−2 to <2) as outcomes to assess whether the results were consistent with the outcome of overweight. Additional robustness checks included: (i) excluding wasted children (BMI Z-score<−2) from the analysis; (ii) stratifying results based on child’s age (≤24 months v. >24 months); (iii) controlling for birth order; and (iv) controlling for maternal BMI. We also assessed our results when including current breast-feeding status (yes/no) as a covariate, which we hypothesize could influence mothers’ entry into the workforce. We was set α to 0·05 for main effects and to 0·10 for interaction terms( 45 , 46 ). Analyses were performed using the statistical software package Stata version 14.1.
Results
Overall, 23 % of mothers were formally employed and 32 % of mothers were informally employed. The mean age for children was 1·9 (sd 1·4) years and 47 % had a mother with at least a primary level of education (Table 1). Most formally employed women (61 %) had a high level of education, compared with 32 % of informally employed women and 50 % of non-employed women (see online supplementary material, Supplemental Table 2). Children of formally and informally employed women had a similar prevalence of overweight (6 %), but prevalence rates across countries were wide-ranging (Table 1).
Table 1.
Demographic characteristics of children in selected low- and middle-income countries*
| Overweight†,‡ | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Maternal age (years) | Mother with at least primary education | Child’s age (years) | Birth order | Formal employment | Informal employment | ||||||||
| Country (year) | N | Mean | sd | n | % | Mean | sd | Mean | sd | n | % | n | % |
| Armenia (2010)§ | 1328 | 26·9 | 4·8 | 1229 | 95 | 1·9 | 1·4 | 1·8 | 0·9 | 29 | 15 | 4 | 9·6 |
| Bangladesh (2014) | 6439 | 26·0 | 5·6 | 4443 | 67 | 2·0 | 1·4 | 2·3 | 1·5 | 15 | 0·97 | 7 | 2·5 |
| Burkina Faso (2010) | 6455 | 29·4 | 6·8 | 468 | 7·1 | 2·0 | 1·4 | 3·9 | 2·4 | 35 | 3·8 | 175 | 3·9 |
| Burundi (2010) | 3385 | 30·3 | 6·7 | 754 | 22 | 1·9 | 1·4 | 3·8 | 2·4 | 5 | 3·9 | 133 | 4·3 |
| Cambodia (2014) | 4314 | 28·6 | 5·9 | 1914 | 44 | 1·9 | 1·4 | 2·2 | 1·5 | 54 | 3·0 | 26 | 1·8 |
| Cameroon (2015) | 4944 | 28·4 | 6·6 | 2377 | 48 | 1·9 | 1·4 | 3·7 | 2·4 | 129 | 8·6 | 205 | 9·1 |
| Chad (2014) | 9873 | 28·4 | 6·6 | 1450 | 15 | 2·0 | 1·4 | 4·4 | 2·6 | 40 | 3·7 | 170 | 4·3 |
| Colombia (2010)║ | 15 369 | 28·0 | 6·6 | 11 733 | 86 | 2·0 | 1·4 | 2·3 | 1·6 | 255 | 5·2 | 200 | 5·9 |
| Comoros (2012) | 2226 | 30·0 | 6·6 | 791 | 34 | 1·9 | 1·4 | 3·6 | 2·4 | 45 | 10 | 49 | 11 |
| Congo (2011) | 4289 | 28·8 | 6·7 | 2550 | 70 | 1·8 | 1·4 | 3·2 | 2·0 | 66 | 4·2 | 44 | 4·3 |
| Côte d’Ivoire (2012) | 3110 | 29·0 | 6·8 | 460 | 16 | 1·8 | 1·4 | 3·6 | 2·3 | 32 | 4·0 | 63 | 4·5 |
| DRC (2014) | 7988 | 29·5 | 6·7 | 3627 | 46 | 2·0 | 1·4 | 4·0 | 2·5 | 72 | 6·2 | 279 | 5·4 |
| DR (2013) | 3050 | 27·5 | 6·1 | 2254 | 76 | 1·9 | 1·4 | 2·3 | 1·4 | 116 | 8·7 | 24 | 8·5 |
| Egypt (2014) | 14 267 | 28·6 | 5·5 | 10 989 | 77 | 1·9 | 1·4 | 2·4 | 1·4 | 308 | 20 | 75 | 21 |
| Ethiopia (2011) | 9527 | 29·3 | 6·5 | 518 | 5·2 | 2·0 | 1·4 | 4·0 | 2·6 | 38 | 3·1 | 93 | 2·3 |
| Gabon (2012) | 3229 | 29·4 | 6·8 | 1945 | 73 | 1·8 | 1·4 | 3·3 | 2·2 | 70 | 7·5 | 43 | 9·7 |
| Gambia (2013) | 3097 | 29·3 | 6·6 | 927 | 31 | 1·8 | 1·4 | 3·7 | 2·3 | 40 | 5·3 | 25 | 2·5 |
| Ghana (2014) | 2604 | 30·8 | 6·7 | 1462 | 58 | 1·9 | 1·4 | 3·3 | 2·1 | 52 | 4·5 | 20 | 2·1 |
| Guinea (2012) | 2973 | 29·1 | 7·1 | 337 | 11 | 2·0 | 1·4 | 3·8 | 2·3 | 39 | 5·5 | 82 | 4·8 |
| Haiti (2012) | 3932 | 29·7 | 7·0 | 1528 | 41 | 1·8 | 1·4 | 3·1 | 2·3 | 42 | 3·8 | 59 | 5·0 |
| Honduras (2012) | 9531 | 27·9 | 6·5 | 5801 | 65 | 2·0 | 1·4 | 2·7 | 2·0 | 186 | 6·9 | 78 | 5·0 |
| Kenya (2014) | 8806 | 28·9 | 6·3 | 4683 | 58 | 2·0 | 1·4 | 3·3 | 2·3 | 170 | 6·5 | 139 | 4·7 |
| Kyrgyz Republic (2012)§ | 3989 | 28·8 | 6·0 | 3267 | 88 | 1·9 | 1·4 | 2·4 | 1·4 | 62 | 8·5 | 9 | 7·2 |
| Lesotho (2014) | 1239 | 27·7 | 6·5 | 950 | 78 | 1·8 | 1·4 | 2·4 | 1·6 | 28 | 9·6 | 16 | 8·6 |
| Liberia (2013) | 3110 | 29·0 | 7·1 | 823 | 31 | 1·9 | 1·4 | 3·6 | 2·3 | 36 | 4·9 | 33 | 3·6 |
| Malawi (2010) | 4518 | 28·5 | 6·6 | 1039 | 23 | 2·0 | 1·4 | 3·6 | 2·3 | 83 | 13 | 338 | 13 |
| Mali (2013) | 3666 | 29·0 | 6·7 | 340 | 9·2 | 2·0 | 1·4 | 3·8 | 2·3 | 14 | 3·3 | 33 | 3·0 |
| Mozambique (2011) | 9237 | 29·1 | 7·1 | 1553 | 16 | 1·9 | 1·4 | 3·7 | 2·3 | 87 | 11 | 411 | 11 |
| Namibia (2013) | 1734 | 29·6 | 7·0 | 1214 | 76 | 1·7 | 1·4 | 2·9 | 2·0 | 37 | 7·1 | 7 | 4·6 |
| Nepal (2011) | 2252 | 26·9 | 6·0 | 880 | 38 | 2·0 | 1·4 | 2·6 | 1·8 | 4 | 1·8 | 21 | 1·4 |
| Niger (2012) | 4838 | 29·3 | 6·7 | 270 | 5·3 | 2·0 | 1·4 | 4·6 | 2·7 | 18 | 3·3 | 24 | 3·1 |
| Nigeria (2013) | 24 755 | 29·6 | 6·8 | 11 736 | 47 | 2·0 | 1·4 | 3·9 | 2·5 | 674 | 5·0 | 281 | 6·4 |
| Pakistan (2013) | 3225 | 29·2 | 6·0 | 1308 | 38 | 2·0 | 1·4 | 3·5 | 2·4 | 12 | 2·3 | 23 | 4·4 |
| Peru (2012)¶ | 9030 | 29·9 | 6·9 | 6691 | 81 | 2·0 | 1·4 | 2·6 | 1·8 | 328 | 8·5 | 82 | 4·8 |
| Rwanda (2014) | 3529 | 30·4 | 6·3 | 1236 | 35 | 1·9 | 1·4 | 3·0 | 2·1 | 78 | 14 | 280 | 10 |
| Senegal (2014) | 5937 | 29·9 | 6·8 | 713 | 13 | 1·9 | 1·4 | 3·6 | 2·3 | 30 | 1·9 | 21 | 1·4 |
| Sierra Leone (2013) | 4197 | 29·7 | 7·1 | 847 | 20 | 1·9 | 1·4 | 3·7 | 2·3 | 89 | 13 | 309 | 11 |
| Tajikistan (2012) | 4541 | 27·9 | 5·6 | 4466 | 95 | 1·9 | 1·4 | 2·5 | 1·6 | 50 | 11 | 64 | 8·3 |
| Tanzania (2010) | 6709 | 29·4 | 6·8 | 4053 | 60 | 1·9 | 1·4 | 3·8 | 2·4 | 67 | 7·0 | 347 | 6·8 |
| Timor-Leste (2010) | 7275 | 31·4 | 7·0 | 3720 | 51 | 2·1 | 1·4 | 4·1 | 2·5 | 38 | 8·7 | 130 | 5·7 |
| Togo (2014) | 3136 | 30·3 | 6·8 | 899 | 30 | 1·9 | 1·4 | 3·5 | 2·2 | 40 | 2·6 | 21 | 2·1 |
| Uganda (2011) | 2022 | 28·9 | 6·8 | 665 | 33 | 1·9 | 1·4 | 4·2 | 2·7 | 41 | 6·8 | 50 | 5·0 |
| Yemen (2013) | 13713 | 29·2 | 6·6 | 6090 | 45 | 2·0 | 1·4 | 3·9 | 2·7 | 5 | 1·1 | 16 | 1·9 |
| Zambia (2014) | 11 138 | 29·1 | 6·9 | 5368 | 49 | 2·0 | 1·4 | 3·8 | 2·4 | 139 | 7·5 | 360 | 7·8 |
| Zimbabwe (2011) | 4237 | 27·7 | 6·3 | 3587 | 85 | 1·7 | 1·4 | 2·6 | 1·7 | 39 | 6·8 | 69 | 6·2 |
| Total | 268 763 | 29·1 | 6·7 | 123 955 | 47 | 1·9 | 1·4 | 3·5 | 2·4 | 3837 | 6·1 | 4938 | 5·9 |
DRC, Democratic Republic of Congo; DR, Dominican Republic.
Total and country-specific sample sizes are unweighted. The numbers of observations and percentages, and means and sd in the case of child’s age, were estimated using the country-specific sample weight.
Overweight (BMI Z-score>2) was defined based on the 2006 WHO Child Growth Standards( 33 ).
Type of employment was based on four indicators: (i) employment during the last 12 months (yes, no); (ii) aggregate occupation category (skilled, unskilled); (iii) type of earnings (cash only, cash and in-kind, in-kind only, unpaid); and (iv) seasonality of employment (all year, seasonally, occasionally).
Maternal education level was dichotomized as less than secondary level of education and at least secondary level of education based on the high percentage (90 %) of women with at least secondary level of education completed.
Employment type was based on employment status, occupation category and earnings only because seasonality of employment was not queried in this survey.
Employment type was based on employment status, type of earnings and seasonality only because occupation type was not queried in this survey.
Formal employment was associated with higher odds of childhood overweight in three countries (Egypt, Ghana, Kenya) and lower odds of overweight in three other countries (Nigeria, Pakistan, Yemen; Figs. 2 and 3). Informal employment was associated with higher odds of overweight in five countries (Cameroon, Chad, Colombia, Egypt, Haiti) and lower odds in another five countries (Peru, Rwanda, Sierra Leonne, Timor-Leste, Yemen; Figs. 2 and 3). When pooling estimates across all forty-five LMIC, neither formal employment (POR=0·99; 95 % CI 0·89, 1·1) nor informal employment (POR=0·99; 95 % CI 0·89, 1·1), compared with non-employment, was associated with child overweight (Table 2). Like estimates pooled across all LMIC, in countries where the association did not vary by education, neither formal nor informal employment was associated with childhood overweight (formal: POR=1·0; 95 % CI 0·9, 1·1; informal: POR=0·97; 95 % CI 0·88, 1·1).
Fig. 2.

Forest plots showing the relationship between maternal employment (a, formal employment; b, informal employment) and childhood overweight in thirty-eight low- and middle-income countries where the association did not vary by maternal education. The study-specific OR and 95 % CI are represented by the black diamond and horizontal line, respectively; the area of the grey square is proportional to the specific-study weight to the overall meta-analysis. The centre of the open diamond represents the pooled OR and its width represents the pooled 95 % CI. Country-specific OR ratios are estimated using logistic regression. Pooled OR are generated using meta-analysis and pool estimates across countries. Childhood overweight is defined as BMI Z-score >2 based on the 2006 WHO Child Growth Standards( 33 ). Models were adjusted for maternal age (years), marital status (married, not married), number of household members, child’s age (months), child’s sex, substitute childcare provider (yes, no) and maternal education (less than primary education, at least primary education completed)
Fig. 3.
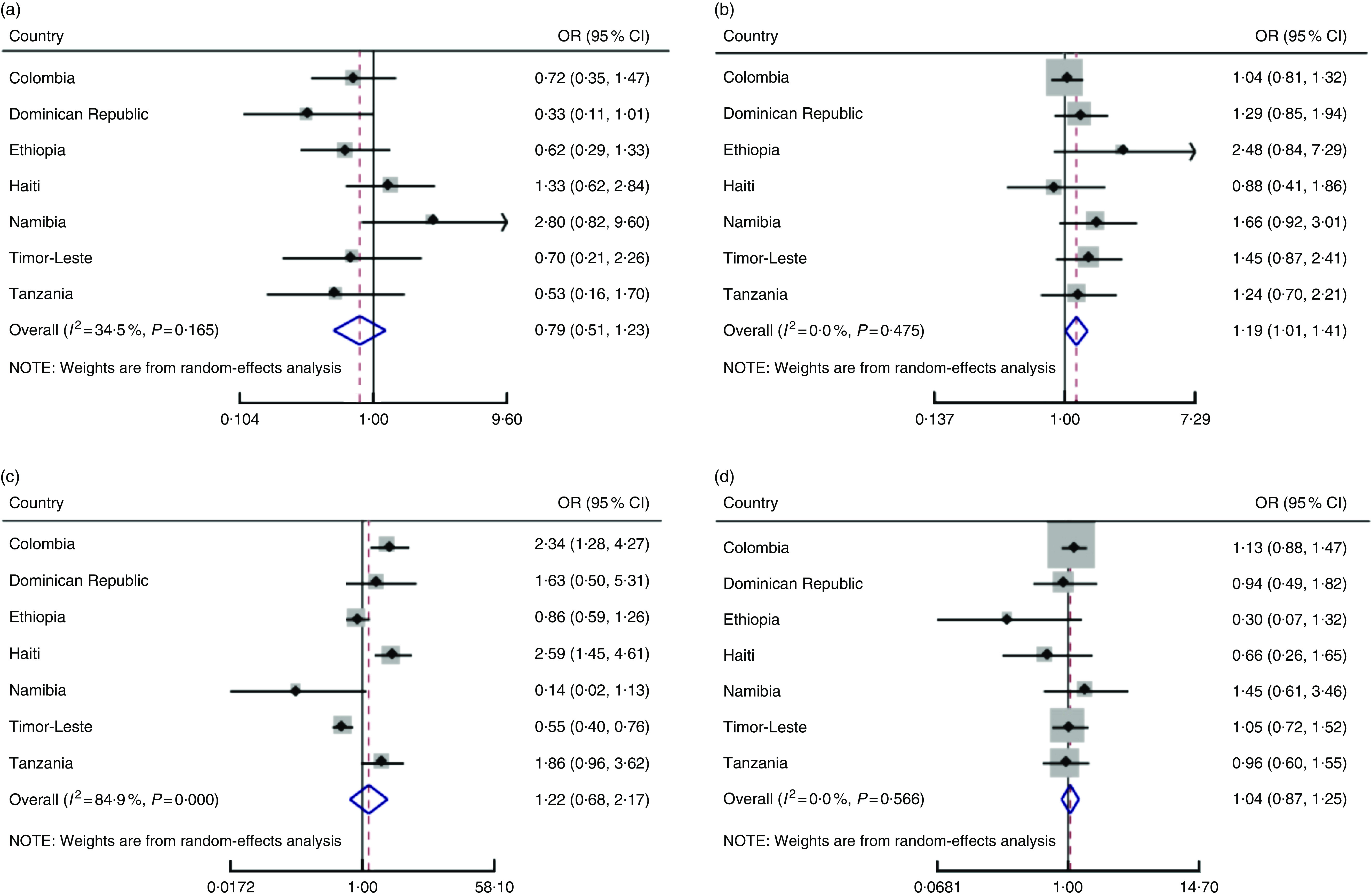
Forest plots showing the relationship between maternal employment and childhood overweight in seven low- and middle-income countries where the association varied by maternal education (a, formal employment, low education; b, formal employment, high education; c, informal employment, low education; d, informal employment, high education). The study-specific OR and 95 % CI are represented by the black diamond and horizontal line, respectively; the area of the grey square is proportional to the specific-study weight to the overall meta-analysis. The centre of the open diamond and the vertical dashed line represent the pooled OR; the width of the open diamond represent represents the pooled 95 % CI. Country-specific OR are estimated using logistic regression. Pooled OR ratios are generated using meta-analysis and pool estimates across countries. Childhood overweight is defined as BMI Z-score >2 based on the 2006 WHO Child Growth Standards( 33 ). Models were adjusted for maternal age (years), marital status (married, not married), number of household members, child’s age (months), child’s sex and substitute childcare provider (yes, no). Models include an employment×education interaction term (less primary education, at least primary education completed)
Table 2.
Pooled OR for the relationship between formal and informal maternal employment and childhood overweight in selected low- and middle-income countries*
| N 268 763† | ||
|---|---|---|
| Pooled OR | 95 % CI | |
| Formal employment‡,§ | ||
| All low- and middle-income countries | 0·99 | 0·89, 1·1 |
| Countries where the association did not vary by education | 1·0 | 0·90, 1·1 |
| Countries where the association varied by education: low education║ | 0·79 | 0·51, 1·2 |
| Countries where the association varied by education: high education║ | 1·2 | 1·0, 1·4 |
| Informal employment‡,§ | ||
| All low- and middle-income countries | 0·99 | 0·89, 1·1 |
| Countries where the association did not vary by education | 0·97 | 0·88, 1·1 |
| Countries where the association varied by education: low education║ | 1·2 | 0·68, 2·2 |
| Countries where the association varied by education: high education║ | 1·0 | 0·87, 1·3 |
Pooled OR are generated using meta-analysis and pool estimates across country subgroups. Childhood overweight is defined as BMI Z-score>2 based on the 2006 WHO Child Growth Standards( 33 ). Models are adjusted for maternal age (years), marital status (married, not married), number of household members, child’s age (months), child’s sex and proxy substitute childcare provider (yes, no). Models which did not retain the employment×education interaction term are also adjusted for maternal education (less than primary education, at least primary education).
Total sample size is unweighted.
The following strata experienced small cell sizes, resulting in observations being omitted from the model: Armenia (childcare proxy n 1); Bangladesh (marital status n 79); Burundi (childcare proxy n 8); Ghana (childcare proxy n 19); Mali (childcare proxy n 14); Nepal (childcare proxy n 18, marital status n 4); Pakistan (childcare proxy n 26); Tajikistan (childcare proxy n 12); Uganda (childcare proxy n 24).
Type of employment was based on four indicators: (i) employment during the last 12 months (yes, no); (ii) aggregate occupation category (skilled, unskilled); (iii) type of earnings (cash only, cash and in-kind, in-kind only, unpaid); and (iv) seasonality of employment (all year, seasonally, occasionally).
The employment×education interaction term was retained in the following countries: Colombia, Dominican Republic, Ethiopia, Haiti, Namibia, Tanzania and Timor-Leste. The relative difference in the employment–overweight association, comparing mothers with high and those with low education, is: for formal employment, POR=1·7 (95 % CI 0·97, 2·9); for informal employment, POR=0·71 (95 % CI 0·33, 1·5).
Heterogeneity by maternal level of education
The association between employment and child overweight varied by maternal education in seven LMIC (Table 2 and Fig. 3). Children of formally employed women with high education had higher odds of overweight compared with children of non-employed women with high education (POR=1·2; 95 % CI 1·0, 1·4). Additionally, maternal education modified the magnitude of the relationship between formal employment and childhood overweight. The combination of high education and formal employment (v. high education and non-employment) was associated with larger odds of childhood overweight, compared with the analogous combination of low education and formal employment (v. low education and non-employment; POR for difference in the associations=1·7; 95 % CI 0·97, 2·9; P=0·063).
Informal employment was not associated with overweight among children of women with low or high education (low education: POR=1·2; 95 % CI 0·68, 2·2; high education: POR=1·0; 95 % CI 0·87, 1·3). The magnitude of the association between informal employment and overweight was not different among children of women with high v. low education.
The meta-regression results indicated that neither the formal employment–overweight nor the informal employment–overweight association differed by log(GDP) or urbanization (Table 3 and online supplementary material, Supplemental Figs 1 and 2).
Table 3.
Meta-regression results for the association between formal and informal maternal employment and childhood overweight by log(GDP) and percentage urban in selected low- and middle-income countries*
| Log(GDP)† | Percentage urban†,‡ | |||
|---|---|---|---|---|
| β | 95 % CI | β | 95 % CI | |
| Formal employment§ | ||||
| All low- and middle-income countries | −0·083 | −0·21, 0·046 | −0·0025 | −0·0086, 0·0037 |
| Countries where the association did not vary by education | −0·084 | −0·22, 0·050 | −0·0023 | −0·0088, 0·0043 |
| Countries where the association varied by education: low education║ | −0·014 | −0·70, 0·67 | −0·0017 | −0·032, 0·028 |
| Countries where the association varied by education: high education║ | −0·081 | −0·35, 0·19 | −0·0064 | −0·017, 0·0045 |
| Informal employment§ | ||||
| All low- and middle-income countries | 0·0045 | −0·14, 0·15 | 0·0021 | −0·0047, 0·0089 |
| Countries where the association did not vary by education | −0·042 | −0·18, 0·096 | −0·0029 | −0·0094, 0·0036 |
| Countries where the association varied by education: low education║ | 0·083 | −0·88, 1·0 | 0·017 | −0·015, 0·050 |
| Countries where the association varied by education: high education║ | 0·11 | −0·15, 0·37 | 0·0028 | −0·0076, 0·013 |
Log(GDP), gross domestic product per capita, adjusted for purchasing power.
β coefficients were generated using meta-regression and pool estimates across country subgroups. Models were adjusted for maternal age (years), marital status (married, not married), number of household members, child’s age (months), child’s sex and substitute childcare provider (yes, no). Models which did not retain the employment ×education interaction term were also adjusted for maternal education (less than primary level of education, at least primary level of education).
Log(GDP) and percentage urban were obtained from the World Development Indicators database( 43 ) and correspond to the survey year used.
Percentage urban was defined as the number of people living in urban areas divided by the total population.
Type of employment was based on four indicators: (i) employment during the last 12 months (yes, no); (ii) aggregate occupation category (skilled, unskilled); (iii) type of earnings (cash only, cash and in-kind, in-kind only, unpaid), and (iv) seasonality of employment (all year, seasonally/occasionally).
The employment×education interaction term was retained in the following countries: Colombia, Dominican Republic, Ethiopia, Haiti, Namibia, Tanzania and Timor-Leste.
Sensitivity analyses
Results were substantively similar in magnitude and direction when including current breast-feeding status as a confounder (online supplementary material, Supplemental Table 3), when excluding wasted children (Supplemental Table 4), when controlling for maternal BMI (Supplemental Table 5) and when controlling for birth order (Supplemental Table 6). However, when controlling for maternal BMI, the association between formal employment (compared with non-employment) and overweight among children of women with high education was no longer significant (POR=1·1; 95 % CI 0·97, 1·4).
When stratifying results by child’s age, results were unchanged in countries where the employment–overweight association did not vary by education. In countries where the association varied by education, children aged >24 months of formally employed women with high education had higher odds of overweight (POR=1·3; 95 % CI 1·0, 1·7), compared with children aged >24 months of non-employed women with high education (online supplementary material, Supplemental Table 7). The point estimate for the analogous association among children ≤24 months of age was somewhat lower, but in the same direction (POR=1·1; 95 % CI 0·80, 1·6).
Results were unchanged when modelling at-risk-of-overweight as the outcome (Table 4). Notably, children of formally employed mothers, compared with non-employed, had lower odds of underweight (POR=0·83; 95 % CI 0·76, 0·90; Table 4). Correspondingly, children of formally employed mothers had higher odds of normal weight when defined based on WAZ (POR=1·2; 95 % CI 1·1, 1·3; Table 4). The point estimate was in the same direction when normal weight was defined based on BMI Z-score (POR=1·1; 95 % CI 0·98, 1·2). Informal employment was not associated with underweight, although the point estimates went in the same direction as those for formal employment, in countries where the employment–overweight association varied by education (low education: POR=0·91; 95 % CI 0·70, 1·2; high education: POR=0·91; 95 % CI 0·60, 1·4). Informal employment was associated with normal weight when defined based on BMI Z-score (POR=1·1; 95 % CI 1·0, 1·2). The point estimate went in the same direction when normal weight was defined based on WAZ (POR=1·0; 95 % CI 0·92, 1·1). Finally, children of formally employed mothers, compared with children of non-employed mothers, had a higher BMI Z-score (pooled β=0·042; 95 % CI 0·002, 0·082; Table 5). The point estimate for the relationship between informal employment and BMI Z-score followed a similar positive trend (pooled β=0·033; 95 % CI −0·010, 0·076).
Table 4.
Pooled OR for the relationship between maternal employment and childhood underweight, normal weight and at-risk-of-overweight in selected low- and middle-income countries*
| N 268 763† | ||||||||
|---|---|---|---|---|---|---|---|---|
| Underweight: WAZ<−2 | Normal weight: WAZ≥−2 to <2 | Normal weight: BMI Z-score≥−2 to <2 | At-risk-of-overweight: BMI Z-score>1 | |||||
| Pooled OR | 95 % CI | Pooled OR | 95 % CI | Pooled OR | 95 % CI | Pooled OR | 95 % CI | |
| Formal employment‡ | ||||||||
| All low- and middle-income countries | 0·83 | 0·76, 0·90 | 1·2 | 1·1, 1·3 | 1·1 | 0·98, 1·2 | 1·0 | 0·96, 1·1 |
| Countries where the association did not vary by education | 0·83 | 0·75, 0·91 | 1·2 | 1·1, 1·3 | 1·0 | 0·98, 1·1 | 1·0 | 0·96, 1·1 |
| Countries where the association varied by education: low education§ | 0·83 | 0·66, 0·99 | 1·2 | 0·97, 1·4 | 1·2 | 0·85, 1·7 | 0·99 | 0·83, 1·2 |
| Countries where the association varied by education: high education§ | 0·78 | 0·66, 0·91 | 1·1 | 0·88, 1·4 | 0·92 | 0·79, 1·1 | 1·2 | 1·0, 1·3 |
| Informal employment‡ | ||||||||
| All low- and middle-income countries | 1·0 | 0·97, 1·1 | 1·0 | 0·92, 1·1 | 1·1 | 1·0, 1·1 | 1·0 | 0·94, 1·1 |
| Countries where the association did not vary by education | 1·1 | 0·98, 1·2 | 1·0 | 0·89, 1·2 | 1·1 | 1·1, 1·2 | 1·0 | 0·93, 1·1 |
| Countries where the association varied by education: low education§ | 0·91 | 0·70, 1·2 | 0·96 | 0·79, 1·2 | 0·93 | 0·77, 1·1 | 1·1 | 0·81, 1·4 |
| Countries where the association varied by education: high education§ | 0·91 | 0·60, 1·4 | 0·86 | 0·73, 1·0 | 0·97 | 0·73, 1·3 | 1·0 | 0·90, 1·2 |
WAZ, weight-for-age Z-score.
Pooled OR were generated using meta-analysis and pool estimates across country subgroups. Weight status was defined based on the 2006 WHO Child Growth Standards( 33 ). Models were adjusted for maternal age (years), marital status (married, not married), number of household members, child’s age (months), child’s sex and proxy substitute childcare provider (yes, no). Models which did not retain the employment×education interaction term were also adjusted for maternal education (less than primary education, at least primary education).
Total sample size is unweighted.
Type of employment was based on four indicators: (i) employment during the last 12 months (yes, no); (ii) aggregate occupation category (skilled, unskilled); (iii) type of earnings (cash only, cash and in-kind, in-kind only, unpaid); and (iv) seasonality of employment (all year, seasonally, occasionally).
The employment×education interaction term was retained in the following countries: Colombia, Dominican Republic, Ethiopia, Haiti, Namibia, Tanzania and Timor-Leste.
Table 5.
Adjusted linear regression for the relationship between formal and informal maternal employment and child BMI Z-score in selected low- and middle-income countries*
| Mean BMI Z-score | Formal employment† | Informal employment† | ||||||
|---|---|---|---|---|---|---|---|---|
| Country | Year | N | β | sd ‡ | β | 95 % CI‡ | β | 95 % CI‡ |
| Armenia§ | 2010 | 1329 | 0·7 | 1·6 | −0·21 | −0·54, 0·12 | −0·51 | −1·1, 0·062 |
| Bangladesh | 2014 | 6518 | −0·7 | 1·2 | −0·095 | −0·18, −0·0067 | −0·14 | −0·33, 0·048 |
| Burkina Faso | 2010 | 6455 | −0·5 | 1·5 | 0·091 | −0·042, 0·22 | 0·024 | −0·084, 0·13 |
| Burundi | 2010 | 3393 | −0·0 | 1·2 | 0·043 | −0·19, 0·28 | 0·034 | −0·17, 0·23 |
| Cambodia | 2014 | 4314 | −0·5 | 1·2 | 0·13 | 0·023, 0·24 | 0·043 | −0·078, 0·16 |
| Cameroon | 2011 | 4944 | 0·3 | 1·4 | 0·14 | 0·0019, 0·27 | 0·14 | 0·025, 0·26 |
| Chad | 2014 | 9873 | −0·4 | 1·4 | 0·29 | 0·17, 0·40 | 0·28 | 0·20, 0·37 |
| Colombia║,¶ | 2010 | 15 369 | 0·4 | 1·0 | 0·020 | −0·095, 0·13 | 0·17 | 0·048, 0·29 |
| Comoros | 2012 | 2226 | 0·0 | 1·8 | −0·23 | −0·52, 0·063 | −0·14 | −0·43, 0·16 |
| Congo | 2011 | 4289 | −0·1 | 1·2 | −0·011 | −0·15, 0·13 | −0·12 | −0·28, 0·042 |
| Côte d’Ivoire | 2012 | 3110 | −0·1 | 1·3 | 0·028 | −0·15, 0·21 | 0·17 | 0·022, 0·31 |
| DRC | 2014 | 7988 | −0·0 | 1·4 | 0·11 | −0·070, 0·28 | −0·039 | −0·18, 0·11 |
| DR | 2013 | 3050 | 0·3 | 1·2 | −0·11 | −0·34, 0·12 | 0·12 | −0·22, 0·46 |
| Egypt | 2014 | 14 267 | 0·4 | 1·8 | 0·16 | 0·028, 0·30 | 0·49 | 0·22, 0·76 |
| Ethiopia¶ | 2011 | 9527 | −0·3 | 1·3 | 0·11 | −0·029, 0·25 | 0·0031 | −0·088, 0·094 |
| Gabon | 2012 | 3229 | 0·3 | 1·3 | −0·13 | −0·28, 0·0092 | 0·077 | −0·086, 0·24 |
| Gambia | 2013 | 3097 | −0·5 | 1·4 | 0·15 | −0·067, 0·37 | 0·042 | −0·11, 0·19 |
| Ghana | 2014 | 2623 | −0·2 | 1·1 | 0·17 | 0·0016, 0·34 | 0·16 | −0·0013, 0·32 |
| Guinea | 2012 | 2973 | −0·2 | 1·4 | 0·00099 | −0·23, 0·24 | 0·084 | −0·098, 0·27 |
| Haiti¶ | 2012 | 3932 | −0·1 | 1·2 | 0·072 | −0·085, 0·23 | 0·11 | −0·041, 0·25 |
| Honduras | 2012 | 9531 | 0·4 | 1·0 | 0·13 | 0·068, 0·20 | 0·12 | 0·044, 0·19 |
| Kenya | 2014 | 8806 | 0·1 | 1·2 | 0·26 | 0·16, 0·36 | 0·16 | 0·074, 0·25 |
| Kyrgyz Republlic§ | 2012 | 3989 | 0·5 | 1·3 | −0·076 | −0·22, 0·065 | −0·18 | −0·42, 0·057 |
| Lesotho | 2014 | 1239 | 0·4 | 1·3 | 0·0039 | −0·24, 0·25 | −0·16 | −0·39, 0·068 |
| Liberia | 2013 | 3110 | −0·1 | 1·3 | −0·074 | −0·24, 0·094 | −0·026 | −0·16, 0·11 |
| Malawi | 2010 | 4518 | 0·5 | 1·4 | 0·011 | −0·17, 0·20 | 0·045 | −0·073, 0·16 |
| Mali | 2013 | 3680 | −0·4 | 1·5 | 0·15 | −0·024, 0·32 | 0·14 | 0·0035, 0·27 |
| Mozambique | 2011 | 9237 | 0·3 | 1·5 | 0·084 | −0·067, 0·23 | −0·047 | −0·15, 0·057 |
| Namibia¶ | 2013 | 1734 | −0·1 | 1·4 | 0·055 | −0·38, 0·49 | 0·31 | −0·069, 0·69 |
| Nepal | 2011 | 2274 | −0·5 | 1·2 | 0·15 | −0·12, 0·42 | −0·059 | −0·21, 0·092 |
| Niger | 2012 | 4838 | −0·7 | 1·5 | 0·22 | 0·066, 0·38 | 0·10 | −0·049, 0·24 |
| Nigeria | 2013 | 24 755 | −0·5 | 1·7 | −0·089 | −0·17, −0·0074 | 0·10 | 0·0015, 0·20 |
| Pakistan | 2013 | 3251 | −0·3 | 1·5 | −0·084 | −0·25, 0·085 | −0·14 | −0·37, 0·086 |
| Peru** | 2012 | 9030 | 0·6 | 1·0 | −0·039 | −0·12, 0·038 | −0·17 | −0·25, −0·096 |
| Rwanda | 2014 | 3529 | 0·6 | 1·2 | −0·28 | −0·48, −0·083 | −0·30 | −0·48, −0·13 |
| Senegal | 2014 | 5937 | −0·3 | 1·1 | 0·10 | −0·0032, 0·21 | 0·10 | −0·0075, 0·21 |
| Sierra Leone | 2013 | 4197 | 0·2 | 1·7 | −0·15 | −0·38, 0·089 | −0·079 | −0·26, 0·10 |
| Tajikistan | 2012 | 4553 | −0·1 | 1·6 | 0·098 | −0·078, 0·27 | 0·026 | −0·13, 0·18 |
| Tanzania¶ | 2010 | 6709 | 0·2 | 1·3 | 0·34 | 0·043, 0·64 | 0·40 | 0·21, 0·59 |
| Timor-Leste¶ | 2010 | 7275 | −0·5 | 1·7 | −0·11 | −0·52, 0·31 | −0·30 | −0·44, −0·17 |
| Togo | 2014 | 3136 | −0·2 | 1·1 | 0·12 | −0·022, 0·26 | 0·047 | −0·098, 0·19 |
| Uganda | 2011 | 2046 | 0·1 | 1·3 | 0·23 | 0·037, 0·42 | 0·087 | −0·091, 0·26 |
| Yemen | 2013 | 13 713 | −0·7 | 1·4 | −0·11 | −0·27, 0·054 | 0·032 | −0·084, 0·15 |
| Zambia | 2014 | 11 138 | 0·2 | 1·4 | −0·12 | −0·22, −0·025 | −0·069 | −0·14, 0·0065 |
| Zimbabwe | 2011 | 4237 | 0·3 | 1·2 | 0·028 | −0·11, 0·17 | 0·026 | −0·075, 0·13 |
| Total/pooled β | 268 968 | −0·065 | 1·4 | 0·042 | 0·0020, 0·082 | 0·033 | −0·010, 0·076 | |
DRC, Democratic Republic of Congo, DR, Dominican Republic.
Country-specific β coefficients are estimated using linear regression. All models were adjusted for maternal age (years), marital status (married, not married), number of household members, child’s age (months), child’s sex and proxy substitute childcare provider (yes, no). Models which did not retain the employment ×education interaction term were also adjusted for maternal education (less than primary level of education, at least primary level of education). Pooled coefficients are generated using meta-analysis and pool estimates across all low- and middle-income countries.
Type of employment was based on four indicators: (i) employment during the last 12 months (yes, no); (ii) aggregate occupation category (skilled, unskilled, unemployed); (iii) type of earnings (cash only, cash and in-kind, in-kind only, unpaid); and (iv) seasonality of employment (all year, seasonally/occasionally).
Small cell sizes resulted in missingness in some overweight models. These observations were retained in the above models where BMI Z-score was the outcome: Armenia (childcare proxy n 1); Bangladesh (marital status n 79); Burundi (childcare proxy n 8); Ghana (childcare proxy n 19); Mali (childcare proxy n 14); Nepal (childcare proxy n 18, marital status n 4); Pakistan (childcare proxy n 26); Tajikistan (childcare proxy n 12); Uganda (childcare proxy n 24).
Maternal education level was dichotomized as less than secondary level of education and at least secondary level of education.
Employment type based on employment status, occupation and earnings only because seasonality of employment was not queried in this survey.
Includes employment×education interaction term.
Employment type based on employment status, type of earnings and seasonality only because occupation type was not queried in this survey.
Discussion
The present study leveraged data from forty-five countries to investigate whether there was any association between maternal employment and childhood overweight in LMIC. As environments change, it is important to better understand the benefits, as well as any unintended consequences, of maternal employment on children’s weight status given the potential need for additional policies and programmes to support women in the workplace and prevent childhood overweight. In most countries, we did not observe an association between formal or informal employment and childhood overweight. However, children of employed mothers had a modestly higher BMI Z-score, higher odds of normal weight and lower odds of underweight. The employment–overweight association varied by maternal education level in seven countries. In these countries, children of formally employed women with high education had higher odds of overweight compared with children of non-employed women with high education.
Contrary to results from South Africa and high-income countries, we found that neither formal nor informal maternal employment was associated with risk for childhood overweight in most countries( 1 – 4 , 18 ). The low prevalence of overweight in some strata (e.g. children of informally employed women) is one plausible reason that we found a null association in most LMIC. However, several other factors may help explain these null findings. In multigenerational households where grandmothers are in part responsible for meal preparation, eating patterns at home may not change even if the mother is employed. Also, young children may have limited access to energy-dense foods in these contexts. Alternatively, children still have a negative BMI Z-score on average (BMI Z-score: −0·065); in contexts where the BMI Z-score is still negative on average, earned income may be going towards goods that are currently associated with healthy weight gain in LMIC. Correspondingly, energy needs of children aged 0–5 years are relatively high, due to growth( 47 ). Subsequently, increases in household food expenditures may result in only modest shifts in energy balance.
Differences in the work and home environments in most LMIC, compared with higher-income contexts like South Africa or the USA, also offer possible explanations for our findings. Informal employment may afford flexibility in hours and allow children in LMIC to accompany their mother to work. This is in stark contrast to the formal labour market in the USA, which demands longer working hours and offers childcare arrangements that are less flexible. Evidence also suggests that increased screen time among children is a key mechanism of the employment–childhood overweight association in the USA( 4 ). Screen time promotes sedentary behaviour, but also increases children’s exposure to food-related advertisements; however, children in LMIC are subject to less screen time than children in the USA( 4 , 48 ).
At the same time, we found that formal employment and (to a lesser degree) informal employment, compared with non-employment, are associated with beneficial effects on children’s weight status as maternal employment was associated with a higher BMI Z-score, paired with higher odds of normal weight and lower odds of underweight. In this sample, a higher BMI Z-score seems to be a positive change to average weight status. However, we expect that over time there will be increases in women’s labour force participation in LMIC and in the future, there will be a rightward shift in the BMI distribution among children, like we have seen in adults in these contexts( 49 ). In a well-nourished population, a positive association between maternal employment and BMI Z-score could have unintended consequences for childhood obesity risk. Having followed a similar pattern in the USA, it is estimated that maternal employment contributed to approximately 10 % of the overall increase in childhood overweight( 5 ).
Among children of women with high education, we found that formal employment, compared with non-employment, was associated with higher odds of overweight (POR=1·2; 95 % CI 1·0, 1·4). Formally employed mothers may have additional time constraints compared with their non-employed counterparts, which could lead to higher odds of childhood overweight. Descriptive data from the Philippines suggest that employed mothers, compared with non-employed mothers, spend 3.2 h less per day on childcare and evidence suggests that unsupervised children consume more energy, as compared with supervised children, which would be expected to ultimately affect child weight status( 11 , 50 ). Formally employed, more highly educated women are among the wealthiest women in many LMIC (Supplemental Table 2). In countries at an earlier phase of the nutrition transition (e.g. Ethiopia, Tanzania), we might expect that wealthier women are able to use their earned income from employment to increase their purchase of energy-dense foods( 10 , 11 ). Comparatively, in countries further along in the nutrition transition (i.e. upper middle-income), energy-dense foods may be affordable and accessible to almost everyone, including lower-income women. The transformation of the food and built environments as LMIC undergo their nutrition transition, such as the spread of supermarkets and availability of ultra-processed foods, may provide an enabling environment for the hypothesized changes among children of formally employed women with high education( 51 – 53 ).
We additionally found that the formal employment effect differed by maternal education level (high v. low education: POR=1·7; 95 % CI 0·97, 2·9; P=0·063). Although contrary to our hypothesis that higher maternal education (v. lower education) within the formal or informal sector would be associated with lower odds of child overweight, our findings are similar to US-based studies which find that the risk of child overweight associated with employment is greater for more highly educated women than it is for less-educated women( 1 , 4 ). More highly educated formally employed women are more likely to be shifting into full-time employment, as those types of jobs emerge in the formal labour sector in LMIC( 41 ). Therefore, highly educated, formally employed women may be working longer hours, resulting in increased time constraints. We speculate that these women may spend less time preparing meals or caring for their child, which could lead to increased childhood overweight through increased reliance on ready-prepared foods which tend to be more energy-dense( 54 ). It also may be difficult to find caregivers who have knowledge and skills equal to those of more highly educated mothers( 17 ). Women with relatively low education in the formal sector may be employed in positions that are lower paying and entail longer hours (e.g. factory work or shift work), compared with women with a high education (e.g. teacher). For these women with low education, more nominal increases in income may not afford substantive increases in household food expenditures and, in particular, may not allow mothers to increase their purchase of energy-dense foods( 29 ).
The limitations of our study should be noted. Our findings may not be generalizable to older aged children and adolescents and children who are not living in the same residence as their mother. Similarly, countries retained for these analyses may not be representative of other LMIC which no longer participate in DHS, such as upper middle-income countries that now administer their own survey (e.g. Mexico). This sample includes mostly low-income countries (n 24), which may limit our ability to observe variation in the association by country-level factors. We cannot infer causality and unmeasured or residual confounding is possible with the use of cross-sectional data. Countries are likely at different stages of their nutrition transitions, but we have aimed to keep samples comparable by selecting countries with a recent DHS (2010–2016) and we allow for different relationships in each country by starting with disaggregated estimates. Finally, non-employed women who choose to not seek employment are likely different from non-employed women who are actively seeking employment, and those differences could affect child overweight risk. However, we cannot distinguish between these two types of women in the DHS.
Despite some limitations, a key strength of the present study is utilizing data from forty-five countries to gain a better understanding of the maternal employment–childhood overweight relationship as countries undergo their nutrition transition. Moreover, these results have several implications for public health. These findings suggest that countries should continue to monitor child overweight prevalence in relation to maternal employment status. There may also be an opportunity to prevent future increases in childhood overweight like those observed in the USA. Countries could consider implementing policies which both support women’s employment and may prevent childhood overweight; as more women are expected to enter the formal labour force in LMIC, such policies might include subsidized childcare, with provisions for providing healthy food, or include programmes modelled after Head Start which has had beneficial effects on children’s BMI in the USA( 55 ).
Conclusions
Utilizing nationally representative data, we did not observe an association between formal or informal employment and overweight in most LMIC. Yet, overall, our results indicate that employment is associated with a modestly higher BMI Z-score, higher odds of normal weight and lower odds of underweight, suggesting that maternal employment is currently associated with beneficial effects on children’s weight status in LMIC. As countries undergo their nutrition transitions and BMI Z-scores increase among children on average, it will be important to continue to monitor trends of childhood overweight in relation to maternal employment to both support women in the workforce and mitigate future risk of overweight among children in LMIC.
Acknowledgements
Financial support: This work was supported by the National Institutes of Health, Clinical Research and Endocrinology Training Grant in Epidemiology in Diabetes (grant number T32DK062707). The National Institutes of Health had no role in the design, analysis or writing of this article. Conflict of interest: The authors do not have any conflicts of interest to disclose. Authorship: The authors contributed as follows: V.M.O. and J.C.J-.S. conceptualized the research question and analysis plan; V.M.O. analysed the data; V.M.O. drafted the manuscript with critical input from N.T.M., S.N.B., K.M.P., P.J.S. and J.C.J-.S.; all authors reviewed and approved the final manuscript. Ethics of human subject participation: The Johns Hopkins Institutional Review Board deemed that this analysis of de-identified secondary data was not human subjects research.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980017001720.
click here to view supplementary material
References
- 1. Anderson PM, Butcher KF & Levine PB (2003) Maternal employment and overweight children. J Health Econ 22, 477–504. [DOI] [PubMed] [Google Scholar]
- 2. Phipps SA, Lethbridge L & Burton P (2006) Long-run consequences of parental paid work hours for child overweight status in Canada. Soc Sci Med 62, 977–986. [DOI] [PubMed] [Google Scholar]
- 3. Chia YF (2008) Maternal labour supply and childhood obesity in Canada: evidence from the NLSCY. Can J Econ 41, 217–242. [Google Scholar]
- 4. Fertig A, Glomm G & Tchernis R (2009) The connection between maternal employment and childhood obesity: inspecting the mechanisms. Rev Econ Househ 7, 227–255. [Google Scholar]
- 5. Courtemanche C (2014) Longer hours and larger waistlines? The relationship between work hours and obesity. http://ssrn.com/abstract=975099 (accessed May 2016).
- 6. Standing G (1996) Global feminization through flexible labor: a theme revisited. World Dev 27, 583–602. [Google Scholar]
- 7. Head S, Zweimueller S, Marchena C et al. (2014) Women’s Lives and Challenges: Equality and Empowerment Since 2000. Rockville, MD: ICF International. [Google Scholar]
- 8. Adair L, Guilkey D, Bisgrove E et al. (2002) Effect of childbearing on Filipino women’s work hours and earnings. J Popul Econ 15, 625–645. [Google Scholar]
- 9. de Onis M, Blossner M & Borghi E (2010) Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr 92, 1257–1264. [DOI] [PubMed] [Google Scholar]
- 10. Engle PL (1993) Influences of mothers’ and fathers’ income on children’s nutritional status in Guatemala. Soc Sci Med 37, 1303–1312. [DOI] [PubMed] [Google Scholar]
- 11. Popkin BM (1980) Time allocation of the mother and child nutrition. Ecol Food Nutr 9, 1–13. [DOI] [PubMed] [Google Scholar]
- 12. Popkin BM & Du S (2003) Dynamics of the nutrition transition toward the animal foods sector in China and its implications: a worried perspective. J Nutr 133, 11 Suppl. 2, 3898S–3906S. [DOI] [PubMed] [Google Scholar]
- 13. Drewnowski A (2000) Nutrition transition and global dietary trends. Nutrition 16, 486–487. [DOI] [PubMed] [Google Scholar]
- 14. Du S, Mroz TA, Zhai F et al. (2004) Rapid income growth adversely affects diet quality in China – particularly for the poor! Soc Sci Med 59, 1505–1515. [DOI] [PubMed] [Google Scholar]
- 15. Monteiro CA, Levy RB, Claro RM et al. (2011) Increasing consumption of ultra-processed foods and likely impact on human health: evidence from Brazil. Public Health Nutr 14, 5–13. [DOI] [PubMed] [Google Scholar]
- 16. Bamji MS & Thimayamma BVS (2000) Impact of women’s work on maternal and child nutrition. Ecol Food Nutr 39, 13–31. [Google Scholar]
- 17. Nair M, Ariana P & Webster P (2014) Impact of mothers’ employment on infant feeding and care: a qualitative study of the experiences of mothers employed through the Mahatma Gandhi National Rural Employment Guarantee Act. BMJ Open 4, e004434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Mamabolo RL, Alberts M, Steyn NP et al. (2005) Prevalence and determinants of stunting and overweight in 3-year-old black South African children residing in the Central Region of Limpopo Province, South Africa. Public Health Nutr 8, 501–508. [DOI] [PubMed] [Google Scholar]
- 19. Moss BG & Yeaton WH (2011) Young children’s weight trajectories and associated risk factors: results from the Early Childhood Longitudinal Study-Birth Cohort. Am J Health Promot 25, 190–198. [DOI] [PubMed] [Google Scholar]
- 20. Dubois L & Girard M (2006) Early determinants of overweight at 4.5 years in a population-based longitudinal study. Int J Obes (Lond) 30, 610–617. [DOI] [PubMed] [Google Scholar]
- 21. Pryor LE, Tremblay RE, Boivin M et al. (2011) Developmental trajectories of body mass index in early childhood and their risk factors: an 8-year longitudinal study. Arch Pediatr Adolesc Med 165, 906–912. [DOI] [PubMed] [Google Scholar]
- 22. Lourenço BH, Villamor E, Augusto RA et al. (2015) Influence of early life factors on body mass index trajectory during childhood: a population‐based longitudinal analysis in the Western Brazilian Amazon. Matern Child Nutr 11, 240–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Baird J, Fisher D, Lucas P et al. (2005) Being big or growing fast: systematic review of size and growth in infancy and later obesity. BMJ 331, 929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Binkin NJ, Yip R, Fleshood L et al. (1988) Birth weight and childhood growth. Pediatrics 82, 828–834. [PubMed] [Google Scholar]
- 25. Skilton MR, Siitonen N, Wurtz P et al. (2014) High birth weight is associated with obesity and increased carotid wall thickness in young adults: the cardiovascular risk in young Finns study. Arterioscler Thromb Vasc Biol 34, 1064–1068. [DOI] [PubMed] [Google Scholar]
- 26. Eyzaguirre F, Bancalari R, Román R et al. (2012) Prevalence of components of the metabolic syndrome according to birthweight among overweight and obese children and adolescents. J Pediatr Endocrinol 25, 51–56. [DOI] [PubMed] [Google Scholar]
- 27. Mehta SH, Kruger M & Sokol RJ (2011) Being too large for gestational age precedes childhood obesity in African Americans. Am J Obstet Gynecol 204, e261–e265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Reilly JJ & Kelly J (2011) Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes (Lond) 35, 891–898. [DOI] [PubMed] [Google Scholar]
- 29. Günther I & Launov A (2012) Informal employment in developing countries: opportunity or last resort? J Dev Econ 97, 88–98. [Google Scholar]
- 30. Fields G (2005) A guide to multisector labor market models. Paper prepared for the World Bank Labor Market Conference. http://siteresources.worldbank.org/SOCIALPROTECTION/Resources/SP-Discussion-papers/Labor-Market-DP/0505.pdf (accessed May 2016).
- 31. ICF Macro (2008) Demographic and Health Surveys: DHS Model Questionnaires. Calverton, MD: ICF Macro. [Google Scholar]
- 32. De Onis M & Lobstein T (2010) Defining obesity risk status in the general childhood population: which cut-offs should we use? Int J Pediatr Obes 5, 458–460. [DOI] [PubMed] [Google Scholar]
- 33. WHO Multicentre Growth Standards Working Group (2006) WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr 450, 76–85. [DOI] [PubMed] [Google Scholar]
- 34. ICF Macro (2009) Training Field Staff for DHS Surveys. Calverton, MD: ICF Macro. [Google Scholar]
- 35. Chen MA (2012) The Informal Economy: Definitions, Theories and Policies. Manchester: Women in Informal Economy Globalizing and Organizing. [Google Scholar]
- 36. Murphy KM & Topel R (1997) Unemployment and nonemployment. Am Econ Rev 87, 295–300. [Google Scholar]
- 37. Textor J, Hardt J & Knuppel S (2011) DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology 22, 745. [DOI] [PubMed] [Google Scholar]
- 38. Galobardes B, Morabia A & Bernstein MS (2000) The differential effect of education and occupation on body mass and overweight in a sample of working people of the general population. Ann Epidemiol 10, 532–537. [DOI] [PubMed] [Google Scholar]
- 39. Glewwe P (1999) Why does mother’s schooling raise child health in developing countries? Evidence from Morocco. J Hum Resour 34, 124–159. [Google Scholar]
- 40. Wachs TD (2008) Mechanisms linking parental education and stunting. Lancet 371, 280–281. [DOI] [PubMed] [Google Scholar]
- 41. Goldin C (1995) The U-shaped female labor force function in economic development and economic history. In Investment in Women’s Human Capital and Economic Development, pp. 61–90 [TP Schultz, editor]. Chicago, IL: University of Chicago Press. [Google Scholar]
- 42. Jones-Smith JC, Gordon-Larsen P, Siddiqi A et al. (2011) Cross-national comparisons of time trends in overweight inequality by socioeconomic status among women using repeated cross-sectional surveys from 37 developing countries, 1989–2007. Am J Epidemiol 173, 667–675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. The World Bank Group (2016) World Development Indicators. http://data.worldbank.org/data-catalog/world-development-indicators (accessed May 2016).
- 44. Thompson SG & Higgins J (2002) How should meta‐regression analyses be undertaken and interpreted? Stat Med 21, 1559–1573. [DOI] [PubMed] [Google Scholar]
- 45. Sterne JA, Cox D & Smith GD (2001) Sifting the evidence – what’s wrong with significance tests? Another comment on the role of statistical methods. BMJ 322, 226–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Jewell N (2004) Statistics for Epidemiology. Boca Raton, FL: Chapman & Hall/CRC. [Google Scholar]
- 47. Dewey K & Brown K (2003) Update on technical issues concerning complementary feeding of young children in developing countries and implications for intervention programs. Food Nutr Bull 24, 5–28. [DOI] [PubMed] [Google Scholar]
- 48. Gomez LF, Parra DC, Lobelo F et al. (2007) Television viewing and its association with overweight in Colombian children: results from the 2005 National Nutrition Survey: a cross sectional study. Int J Behav Nutr Phys Act 4, 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Popkin BM & Slining M (2013) New dynamics in global obesity facing low‐and middle‐income countries. Obes Rev 14, 11–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Klesges RC, Stein RJ, Eck LH et al. (1991) Parental influence on food selection in young children and its relationships to childhood obesity. Am J Clin Nutr 53, 859–864. [DOI] [PubMed] [Google Scholar]
- 51. Reardon T & Berdegue JA (2002) The rapid rise of supermarkets in Latin America: challenges and opportunities for development. Dev Policy Rev 20, 371–388. [Google Scholar]
- 52. Reardon T, Timmer CP, Barrett CB et al. (2003) The rise of supermarkets in Africa, Asia, and Latin America. Am J Agric Econ 85, 1140–1146. [Google Scholar]
- 53. Monteiro CA, Moubarac JC, Cannon G et al. (2013) Ultra‐processed products are becoming dominant in the global food system. Obes Rev 14, 21–28. [DOI] [PubMed] [Google Scholar]
- 54. Lin B-H & Guthrie JF (2012) Nutritional Quality of Food Prepared at Home and Away from Home, 1977–2008 . Washington, DC: US Department of Agriculture, Economic Research Service. [Google Scholar]
- 55. Lumeng JC, Kaciroti N, Sturza J et al. (2015) Changes in body mass index associated with Head Start participation. Pediatrics 135, e449–e456. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980017001720.
click here to view supplementary material