

Abstract
Many natural coumarins and their chemically synthesized analogs and derivatives exert diverse properties, such as anticancer, antioxidant, anti-inflammatory, or anticoagulant, with the latter being of the utmost importance. The widely used warfarin, acenocoumarol, and phenprocoumon exert anticoagulant properties by inhibiting the vitamin K epoxide reductase complex. In this interdisciplinary review, we present biochemical principles of the coagulation processes and possible methods for their tuning based on the use of coumarins. We also summarize chemical methods of synthesis of coumarins and discuss structures and properties of those that have been used for a long time, as well as newly synthesized compounds. Brief information on the clinical use of coumarins and other anticoagulant drugs is given, including the severe effects of overdosing and methods for reversing their action.
Keywords: coumarins, coumarin derivatives, oral anticoagulants, cardiovascular diseases, vitamin K, vitamin K antagonists
1. Blood Coagulation: A Process Dependent on Vitamin K Wanted or Dreadful
Diseases that attack the blood circulation system in humans are the most fatal, next to cancer, on all continents except Africa. There are numerous types of these diseases, including hemophilia, angina and myocardial infarction, stroke, hypertensive heart disease, rheumatic heart disease, cardiomyopathy, heart arrhythmia, and several others. Despite their variety, the risk factors are very common in developed countries and include high blood pressure, smoking, lack of exercise, diabetes, obesity, poor diet, high blood cholesterol, and overuse of alcohol [1]; therefore, tens of millions of people worldwide suffer from cardiovascular diseases. Nonetheless, in some countries proper education and a healthier lifestyle deliver optimistic results, i.e., reduced numbers of fatalities. Some of the aforementioned diseases are related to a blood coagulation phenomenon. The blood is capable of repairing traumatic injury and stopping bleeding due to a coagulation process that leads to formation of clots. Poor, inefficient coagulation is a rare genetic disorder (called hemophilia), in which blood does not clot normally due to an insufficient level of blood-clotting proteins (clotting factors). A hemophilia patient can bleed for a long time even from a small cut, but a significant threat comes from bleeding inside the body (joint, muscle and sub-, internal, and intracranial bleedings), which can be fatal due to the damage done to organs and tissues. The main treatment for severe hemophilia involves intravenously receiving a replacement of the specific clotting factor, either to combat an ongoing bleeding episode, or to prevent bleeding episodes on a regular basis. Replacement of the clotting factor is achieved from donated blood, but recombinant clotting factors are also available. It should also be noted that the coagulation factors dependent on vitamin K (1) (for the vitamin K characteristics see Figure 1) are synthesized in the liver, and therefore liver-related diseases can result in lower blood levels of vitamin K-dependent clotting factors, with concomitant susceptibility for uncontrolled bleeding.
Figure 1.

Chemical structures of vitamin K (1). (1a) K1; (1b and 1c) K2; and (1d) K3.
The first experiments that showed decreased vitamin K activity with the use of an anticoagulant compound (so it acts as a vitamin K antagonist, VKA) were done in 1954 [2]. The mechanism of action of VKAs is based on the inhibition of a vitamin K epoxide reductase (VKOR, see Section 2 and Section 4). The VKAs interact with widely used drugs, for example, with barbiturates, carbamazepines, rifampicin, nafcillin, and dikloksacilin. Long-term smoking, alcohol abuse or certain dietary components [3] can also negatively affect the VKAs’ action [4]. Derivatives of coumarin (2 in Figure 2) and 4-hydroxycoumarin (3 in Figure 2) are important orally administered anticoagulants, which antagonize VKOR and prevent recycling of vitamin K.
Figure 2.

Structures of coumarin and 4-hydroxycoumarin.
In contrast to hemophilia, there are diseases (in their chronic or acute forms), in which coagulation is too strong, and therefore there is too much clotting. In the most dangerous instances, acute forms (strokes) develop, which are caused by heart, brain, or blood vessel defects. In chronic, less dangerous cases, the symptoms of excessive clotting can be, to a certain extent, neutralized with anticoagulants. These drugs are also prescribed to prevent blood clots in people who have replacement heart valves, people with an irregular heartbeat, or those who had a heart attack, stroke, or a prior blood clot in the deep veins of the arms or legs. Venous thromboembolic (VTE) disease is the third, most common cardiovascular disease with an annual incidence of 100 to 200 per 100,000 inhabitants [5]. It can be fatal in its acute phase or can lead to chronic disease and disability, but it can also often be prevented [6]. Acute incidents of VTE must be treated with anticoagulants as soon as possible [7], but the drugs are also given in a long-term regime (minimum three months) to prevent the return of the disease [8,9]. For this purpose, the most frequently used drugs are VKAs, although the introduction of non-VKA oral anticoagulants (NOAC) such as dabigatran (4 in Figure 3) which is a direct inhibitor of thrombin; and rivaroxaban (5 in Figure 3), apixaban (6 in Figure 3), or edoxaban (7 in Figure 3) which are direct inhibitors of coagulation factor X, should be endorsed. The latter do not require frequent monitoring of blood coagulation parameters but can still cause bleeding and often require assessment of kidney function, especially in patients with kidney problems [10,11,12,13].
Figure 3.

Structures of selected non-VKA oral anticoagulants (NOAC).
There is also a much related and equally dangerous disease which is pulmonary embolism (PE), and in patients with its high and medium clinical probability, an immediate parenteral anticoagulation should be initiated [14]. In addition, patients with atrial fibrillation (AF), who have one high risk factor or two or more moderate risk factors for stroke, must be considered for chronic anticoagulation. In 2010, the number of people with AF worldwide was estimated at 20.9 million men and 12.6 million women [15]. In many cases, AF becomes fatal due to cerebral stroke, the risk of which can be significantly reduced by an anticoagulation treatment. The chronic treatment with VKAs is recommended for patients after implantation of artificial heart valves and with moderate or severe mitral valve stenosis [16,17,18]. Currently, developed NOACs should not be administered to this group of patients. In addition, pregnancy excludes NOACs, whereas VKAs can be used during the second and third trimester (until the 36th week) in women needing a low dose of the drugs (warfarin < 5 mg/day, see Section 5.1 and acenocoumarol < 2 mg/day) [19].
The risk of VKA-related major bleeding increases significantly if the international normalized ratio (INR) of the prothrombin time exceeds 4.5 and boosts exponentially above 6.0. Clinical problems in maintaining INR during treatment result from narrow therapeutic indices of these drugs, i.e., a situation where small differences in dose or concentration in the blood can lead to dose and blood concentration dependency, serious therapeutic failures, or adverse drug reactions. Thus, for a large number of patients, either ineffectiveness of therapy or increased risk of bleeding are noted, the latter mainly from the gastrointestinal tract [20,21,22]. Intracranial and intraarticular bleeding, epistaxis, and hematoma are also often observed [20]. For warfarin overdose related bleeding, vitamin K is a reversal agent, although it does not bring rapid effects, because it only facilitates synthesis of vitamin K-dependent clotting factors. To reverse dabigatran (a nonvitamin K anticoagulant), a monoclonal antibody fragment is used, whereas recombinant modified human activated factor X helps to neutralize the side effects of apixaban and rivaroxaban. It should be noted, that NOACs therapeutic indices are much improved as compared with VKAs because they do not require permanent dose control and interact less with other drugs and food. However, important contraindications for NOACs, i.e., renal failure, artificial heart valves, moderate or severe mitral valve stenosis, pregnancy, and therapy costs, force the use of VKAs, mostly warfarin or acenocoumarol [23].
Whereas there are four main groups of drugs that inhibit blood clotting, i.e., vitamin K antagonists, indirect and direct inhibitors of thrombin activity, and direct inhibitors of the clotting factor Xa activity, this review is focused on the anticoagulation properties of several natural coumarins (isolated mostly from plant extracts) and their chemically synthesized analogs, which act as vitamin K antagonists.
2. Coagulation Pathways
The function of the coagulation processes is to keep hemostasis, which is blockage of bleeding, either internal or external. This is a very complicated phenomenon which takes place with the participation of many proteins. Primary hemostasis is an aggregation of platelets that form a plug at the surface of exposed endothelial cells. This process is supported by secondary hemostasis (coagulation cascade), where the platelet plug is stabilized with a fibrin lattice.
The coagulation cascade process includes two separate pathways, extrinsic and intrinsic, which converge at a specific point, leading to fibrin activation. The intrinsic pathway is activated by damage inside the vascular system, and is triggered by platelets, exposed endothelium (the inner cellular lining of blood vessels and lymphatics), chemicals, or collagen. This pathway develops with the participation of several proteins, i.e., factors I, II, IX, X, XI, and XII, namely fibrinogen, prothrombin, Christmas factor, Stuart–Prower factor, plasma thromboplastin, and Hageman factor, respectively. It begins with the activation of factor XII (a zymogen, inactivated serine protease), which upon contact with endothelial collagen (exposed when the endothelium gets damaged) converts into factor XIIa (activated serine protease). Within this cascade, factor XIIa acts as a catalyst to activate factor XI to factor XIa, which then activates factor IX to factor IXa, at the end of the sequence which allowing conversion of factor X into factor Xa. The extrinsic pathway consists of factors I, II, VII, and X. Once the blood vessel gets damaged, the endothelial cells release a tissue factor, which activates factor VII (called stable factor, or proconvertin) to factor VIIa, and the latter activates factor X into factor Xa. At this point, the extrinsic and intrinsic pathways merge and factor Xa and factor Va activate factor II to IIa (prothrombin to thrombin), which eventually converts fibrinogen to fibrin. The fibrin subunits aggregate to form fibrin strands, and factor XIII uses them to form the aforementioned fibrin lattice.
Various substances are required for the proper functioning of the coagulation cascade. In a certain step, the intermediate complexes of factors Xa and IXa utilize the terminal γ-carboxyl groups (introduced at the side chain of glutamate residues) to interact with the phospholipid surfaces expressed by platelets, and this interaction is necessary for the clot formation to commence. The immature clotting factors are decorated with these additional γ-carboxyl groups upon action of hepatic γ-glutamylcarboxylase (GGCX), for which vitamin K is an essential factor. In this process, vitamin K gets oxidized to form vitamin K epoxide, which is reduced back to its active form with vitamin K epoxide reductase (vitamin K oxide reductase, VKOR, EC 1.17.4.4). Thus, VKOR is a pharmacologically important target for anticoagulant drugs, because if the enzyme gets inhibited, increasing deficiency of the active vitamin K prevents blood clotting. For that purpose, over the years, the most popular have been and still are two drugs, i.e., heparin (polysaccharide of 3000 to 30,000 Da molecular weight, delivered by injection) and warfarin (Coumadin, a coumarin derivative, administered orally). These drugs, although effective, also often cause severe side effects, including critical bleedings, however, there are several reversal agents available for the patients suffering from taking warfarin. On the one hand, the low platelet levels caused by heparin use can cause new clots in the blood vessels and this can lead to a stroke or heart attack. On the other hand, warfarin relatively easily makes the blood “too thin” and this can increase the risk of brain hemorrhage, a type of stroke caused by bleeding in the brain. In addition to those devastating effects, the use of anticoagulants can result in many less harsh side effects such as passing blood in the urine, severe bruising, prolonged nosebleeds, bleeding gums, or heavy periods in women. Speaking a bit in advance, recently developed oral anticoagulants (called “blood thinners”), i.e., dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis), surpass heparin and warfarin in reduced risk of stroke, but also can cause bleeding. Thus, there is an ongoing search for new effective anticoagulants with less severe side effects.
3. Members of the Vitamin K Family
Vitamin K is a group of structurally similar, fat-soluble vitamins, required not only for blood coagulation but also to control the binding of calcium. Deficiency of vitamin K (1) can lead to osteoporosis and can result in calcification of arteries and other soft tissues. The vitamin K family (Figure 1) includes vitamin K1 (1a in Figure 1) and a set of isoprenoid 3-substituted derivatives of 2-methyl-1,4-naphthoquinone, called vitamin K2 (1b in Figure 1). Vitamin K1 is known as phylloquinone and is present in the highest amounts in green leafy vegetables. Bacteria in gastrointestinal microbiota can convert K1 into more “unsaturated” vitamin K2 (menaquinone), with MK-4 (1b in Figure 1) (menaquinone vitamin K with four unsaturated bonds in the side chain) being the most common type in animal tissues. Interestingly, due to the frequent elongation of the isoprenoid side chain, a range of vitamin K2 congeners (1c in Figure 1) (MKn, n = 1–13, K2 vitamers) is produced. Synthetic vitamin K3 (1d in Figure 1) (menadione) without the side chain in the 3-position cannot exert all the functions of the K vitamins. However, it is metabolized to yield menaquinones, and hence should be called a provitamin.
Upon the entering into the coagulation process, the “idle”, 1,4-naphthoquinone form of vitamin K (1 in Scheme 1, R represents a partially unsaturated hydrocarbon chain) is transformed to the active, hydroquinone form (8 in Scheme 1, a reduced derivative). The reduced intermediate (8 in Scheme 1) participates in post-translational modification of specific glutamate residues (Glu) into γ-carboxylated species (Gla), which are required for the activity of vitamin K-dependent proteins (VKDP) [24]. The coagulation factors II, VII, IX, and X, all require the Gla units for proper work and in their shortage they cannot bind Ca2+ ions or create the enzymatic complexes on the surface of cell membranes [25,26]. The carboxylation is performed by GGCX, which also utilizes CO2, and O2. In this process, the reduced derivative (8 in Scheme 1) is oxidized into vitamin K 2,3-epoxide (9 in Scheme 1) (other modified proteins, which also contain Gla residues, are anticoagulant protein C, protein S, and protein Z which selectively inactivate or facilitate inactivation of factors Va, VIIIa, or Xa). The epoxide (9 in Scheme 1) must be reduced back to the reduced derivative (8 in Scheme 1) before it can re-enter the path, and this conversion is executed by VKOR [27,28].
Scheme 1.

Vitamin K cycle.
4. Vitamin K Oxide Reductase, VKOR
VKOR is an integral membrane protein which crosses the endoplasmic reticulum (ER) membrane three times (Figure 4). It has been proposed that for the enzyme to be active, the disulfide bridge (spanning cysteines 132 and 135) in the active site needs to be reduced. During each catalytic cycle, the two sulfhydryl groups are oxidized back to a disulfide bond, while two –SH hydrogen atoms and the oxygen atom (eliminated from the epoxide moiety) form a water molecule (for more detailed mechanism see [29]). VKOR is inhibited by warfarin and other coumarin derivatives. The active site and the proposed warfarin binding site (tyrosine 139) are both located in the third transmembrane helix, i.e., the first one from the C-terminus. Unfortunately, for a number of patients, coumarin-based drugs are ineffective, or their efficacy is much reduced. Table 1 shows mutations identified in VKOR being attributed to this coumarin resistance (CMRES) phenomenon.
Figure 4.

Topology of the VKOR protein, the amino terminus resides in the ER lumen and the carboxy terminus resides in the cytoplasm [30].
Table 1.
Amino acid mutations in VKOR related to CMRES (based on https://www.uniprot.org/uniprot/Q9BQB6) [31].
| Position of Amino Acid Residue | Mutation |
|---|---|
| 26 | A → T |
| 29 | V → L |
| 36 | D → G |
| 36 | D → Y |
| 45 | V → A |
| 52 | S → W |
| 56 | S → F |
| 58 | R → G |
| 59 | W → C |
| 59 | W → L |
| 66 | V → G |
| 66 | V → M |
| 71 | G → A |
| 77 | N → S |
| 77 | N → Y |
| 123 | I → N |
| 128 | L → R |
In addition to the identification of naturally existing mutations, mutagenesis studies were performed which showed the amino acid residues vital for the VKOR activity or strength of the coumarin inhibitory effect (Table 2).
Table 2.
Amino acid residues vital for the VKOR functioning or strength of the coumarin inhibitory effect (based on https://www.uniprot.org/uniprot/Q9BQB6) [32,33].
| Position of Amino Acid Residue | Mutation | Enzyme Activity | Coumarin Inhibitory Effect |
|---|---|---|---|
| 16 | C → A or S | Reduced by about 80% | |
| 35 | R → P | Nearly abolished | |
| 43 | C → A or S | Reduced | |
| 51 | C → A or S | Reduced | |
| 56 | S → P | Nearly abolished | |
| 57 | S → A | Nearly abolished | |
| 85 | C → A | Reduced by about 25% | |
| 85 | C → S | Reduced by about 75% | |
| 96 | C → A or S | Reduced by about 70% | |
| 98 | R → D or E | Reduced by about 80%. | Decreased |
| 98 | R → K | No effect | Decreased |
| 120 | L → Q | Decreased moderately. | Decreased |
| 128 | L → Q or S | Decreased by about 80%. | Decreased |
| 132 | C → S | Nearly abolished | |
| 135 | C → S | Nearly abolished | |
| 139 | Y → C, G or S | Decreased moderately | Strongly decreased |
| 139 | Y → F | No effect | Strongly decreased |
One can conclude that a better understanding of the vitamin K cycle and active complexes of VKOR is necessary to improve selectivity and efficacy of coumarin-based drugs [34,35]. These efforts must be accompanied by synthesis and testing of new members of this family.
5. Coumarins: Synthesis, Structures, and Properties
Coumarins, i.e., derivatives of benzo-α-pyrone (coumarin, 2H-chromen-2-one) (2 in Figure 2), belong to a family of benzopyrones which also contains compounds with a benzo-γ-pyrone skeleton (chromone, 4H-chromen-4-one) (10 in Figure 5) [36].
Figure 5.
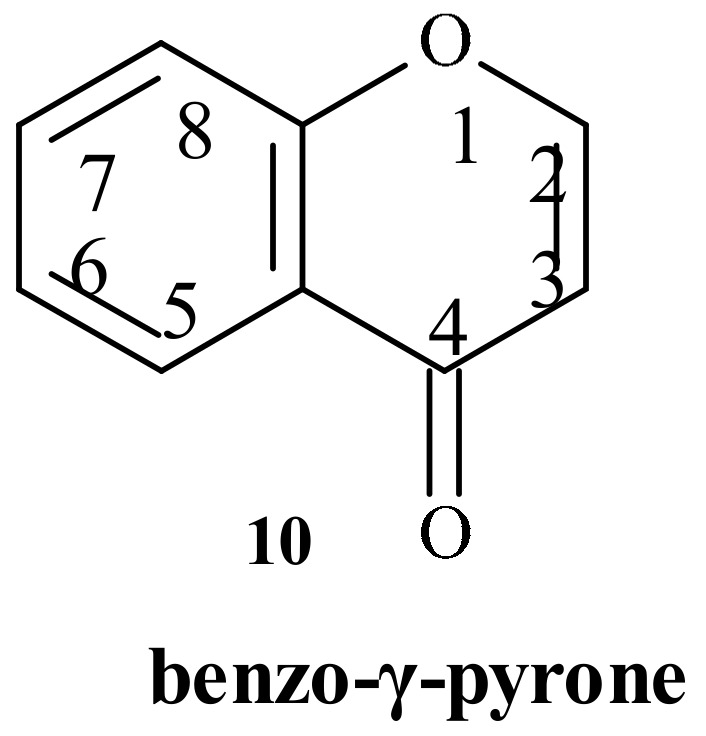
Structure of chromone.
The latter are often synthesized in so-called Simonis chromone cyclization (Scheme 2), the reaction of phenols and β-ketoesters driven by the presence of phosphorus pentoxide. Although this reaction is, to a certain extent, similar to the Pechmann synthesis of coumarins [37] (catalyzed by acids, vide infra), the different outcome results from the initial activation of the ketone moiety in the β-ketoester by P2O5 followed by a reaction with the phenol hydroxyl group and not with arene group.
Scheme 2.

Products of cyclization according to Simonis (2-substituted chromone derivatives) and Pechmann (4-substituted coumarin derivatives).
Compounds possessing these structural motifs are not sporadic in nature [38] and have been found in citrus fruits, vegetables (tomatoes, broccoli, paprika), legumes, celeriacs, cinnamon, peppermint, green tea, lovage, papilionaceous plants, as well as in nuts and coffee. A high concentration of coumarins was detected in the essential oils cassia, cinnamon bark, and lavender oil. Coumarin was isolated in the nineteenth century from seeds of a tree Dipteryx odorata (commonly known as “cumaru” or “kumaru”) [39,40]. Coumarins decorated with various substituents are secondary metabolites [41] and possess numerous applications. For example, novobiocin (isolated from Streptomyces niveus, 11 in Figure 6) and clorobiocin (12 in Figure 6) are natural antimicrobial compounds [42]. Aside of anticoagulant properties, different coumarins exert antiviral [43,44,45] antioxidant [46] or antidepressant [47] activity, but also inhibit acetylcholinesterase (involved in Alzheimer’s disease) [48], aromatase (a target in breast cancer therapy) [49], and squalene-hopene cyclase (cholesterol lowering and antitrypanosomal drugs) [50]. They also exert antifungal [51] and anticancer activities [52]. Certain compounds derived from 4-hydroxycoumarin (3 in Figure 2) protect liver cells from damage by peroxides [53]. Some coumarins have found applications in perfumery [54], but also as dyes in laser technology [55], fluorescent indicators [56], nonlinear optical chromophores, fluorescent whiteners, material for optical recording, and solar energy collectors [57].
Figure 6.

Chemical structures of novobiocin and clorobiocin.
There are three main subtypes of useful, coumarin-related three-ring compounds presented in Figure 7, i.e., furanocoumarins (e.g., psoralen type, 13 in Figure 7, or angelicin type, 14 in Figure 7), and pyranocoumarins (15 in Figure 7), but they will not be discussed in this review.
Figure 7.

Furanocoumarins and pyranocoumarins.
The most popular methods for synthesis of coumarins are Pechmann [37,58] and Knoevenagel condensations [59]. There is also synthetically important intramolecular Wittig reaction [60], which is based on reactive carbonylmethylene(triphenyl) phosphorane intermediates obtained from either salicylaldehydes [61,62] or o-quinones [63,64] using phosphorus ylides of general formula Ph3P = CH-CO-Lg (Lg = a leaving group, for example, imidazole-1-yl, ethoxyl). Further available methods include, among others, Perkin [65], Reformatsky [66], and Kostanecki–Robinson [67] reactions.
The most commonly used synthetic route for the preparation of 4-substituted derivatives is Pechmann condensation, which utilizes simple substrates and offers high yields of products. According to this method, the appropriately substituted phenol and β-ketoester react in the presence of catalyst (concentrated H2SO4, trifluoroacetic acid, ZrCl2, TiCl4, AlCl3, etc.). It is assumed in [68] that in the first step the transesterification produces an aryl ester (Scheme 3, path A), in which the β-keto group is protonated. The intermediate rapidly cyclizes through an intramolecular condensation (a SEAr type reaction) followed by dehydration. However, there are NMR studies that have concluded that the sequence of events is different, i.e., the condensation begins with the activation of the β-keto group (protonation or complexation with a Lewis acid, path B) followed by electrophilic aromatic substitution, cyclization, and final dehydration [69]. It was found that the reaction can be promoted not only by homogenous catalysts, but also by convenient reusable or magnetically recoverable particles [70,71,72] or ionic liquids [73] carrying protic or Lewis acids. Kinetics and mechanistic aspects of their use have been investigated [74]. It was shown that the reaction dramatically speeds up (2 to 10 min instead of 24 h, 60% to 80% yield) if microwave irradiation is applied, even in a household microwave oven [75]. Ultrasonic irradiation also accelerates syntheses and provides the products in good yield [71,76,77]. The properties of many catalysts have been discussed in recently published reviews [78,79].
Scheme 3.

Mechanistic paths that are supposed to operate in Pechmann synthesis of coumarin derivatives.
The Knoevenagel condensation produces 3-substituted coumarins from 2-hydroxybenzaldehydes and 1,3-dicarbonyl compounds. In addition, other compounds containing active methylene group, for example, ROC(O)-CH2-X, where X = CN, Cl, Ar, or SO2R can be used [80]. This approach allows for having CN, COOH, COOR, or the aryl group at position 3. Typically used basic catalysts include proline, lysine, DBU, and piperidine. Similar to the Pechmann reaction, microwave or ultrasonic irradiation give better results than the temperature driven process (for details see [79]).
3,4-Substituted coumarins (Scheme 4, 16) can been prepared by other methods involving the formation of a 3-4 carbon-carbon bond [81]. For example, the Kostanecki–Robinson reaction of o-hydroxyarylalkyl ketones with an acid anhydride and the sodium salt of an acid produces coumarins by the formation of the 3-4 carbon-carbon bond after enolization of the ester (this step is marked by the red rectangular in Scheme 4), but chromones (4H-1-benzopyran-4-ones) can be the major products via the ketone enolate, and yields can be variable [82,83,84,85,86].
Scheme 4.

Mechanism of the Kostanecki–Robinson reaction.
A method that avoids the chromone byproducts of the Kostanecki–Robinson reaction is based on the treatment of methyl ester of 2-alkanoyloxybenzoic acids with metallic sodium [87,88] or bases [89,90,91,92]. Coumarins also have been prepared in good yields by a ring-closing metathesis reaction (3-4 bond formation) [93,94] but this reaction is not ideal in respect to the carbon atom economy and requires a ruthenium catalyst. Dittmer and co-workers showed the synthesis of coumarins by the cyclization triggered by lithium telluride (Scheme 5) [95]. Interestingly, sodium telluride is much less effective.
Scheme 5.

One-pot synthesis of coumarin via the tellurium-triggered cyclization.
In 1974, Klutchko [96] and coworkers showed a convenient and efficient method of synthesis of coumarin derivatives utilizing a hydrolytically promoted ring opening/ring closure reaction of chromone-3-carboxylic esters, with the key rotation step being indicated in Scheme 6 with the contour arrow. In 2017 Abdou published a comprehensive review on methods of synthesis, tautomeric structures and biological properties of 3-acetyl derivatives of 4-hydroxycoumarin (3a in Scheme 6) [97].
Scheme 6.

The mechanism of base promoted transformation of a chromone ester derivative into the corresponding coumarin derivative.
5.1. Warfarin: Stereochemistry and Metabolism
Although warfarin (4-hydroxy-3-(3-oxo-1-phenylbutyl) coumarin (17 in Scheme 7), 4-hydroxy-3-(3-oxo-1-phenylbutyl)-2H-1-benzopyran-2-one) was isolated (from spoiled sweet clover) by Karl Paul Link in 1939, it is still the most often prescribed anticoagulant worldwide [98]. Thus, it deserves a few comments. The lethal dose of warfarin in rats has been found to be between 0.125 and 0.25 mg/kg/day. The drug is administered as a racemate substance, whereas the S-warfarin has two to five times greater anticoagulation potency than the R counterpart. Warfarin’s maximum concentration in plasma is observed after ca. 90 min and its half-life of 36 to 42 h is usually noted [99]. The enantiomers of warfarin are metabolized mostly in the liver. Primarily, the oxidation reaction by various isoforms of cytochrome P450 takes place, but also reduction reactions can occur in the side chain ketone to yield enantiomeric alcohols. (Scheme 8). In rats, the enantiomers are metabolized by cytochrome p450 monooxygenases CYP 1A1, 2B1, 2C6, 2C11, and 3A2. In humans, S-warfarin is metabolized to 7-hydroxywarfarin (a major metabolite) and to 6-hydroxywarfarin (a minor one) by CYP 2C9. The R-enantiomer is metabolized to 6-, 8-, or 10-hydroxywarfarin derivatives by CYP 1A2, 2C19, or 3A4, respectively [100]. However, these hydroxylation processes are often affected by other factors, for example, by the coenzyme Q10 [101].
Scheme 7.

Tautomer substructures of warfarin (17), whose combination generates 40 distinct tautomeric forms.
Scheme 8.

Biotransformation of acenocoumarol in human.
Heteroatoms present in the warfarin molecule allow for the existence of many tautomeric forms. In 2015, Marc C. Nicklaus (Center for Cancer Research, NIH, Frederick, MD) wrote that warfarin “can exist in solution in 40 distinct tautomeric forms through both prototropic tautomerism and ring−chain tautomerism” [102]. However, 1H and 13C NMR analyses revealed that the drug exists mainly as a 70% SR’/28% SS’ mixture of the cyclic hemiketal diastereomers or their enantiomers RS’/RR’, along with a small portion of an open-chain form (Scheme 7).
5.2. Analogs of Warfarin
This section begins with dicoumarol (18 in Figure 8, 3,3′-methylenebis(4-hydroxy-2H-chromen-2-one), which barely is a structural analog of warfarin (17 in Scheme 7). Nonetheless, it is an important predecessor of warfarin, which was employed as an anticoagulant drug until the mid-1950s. Its structure, containing a coumarin motif, was determined by Stahman, in 1941 [88]. Dicoumarol was tested as an anticoagulant agent after the discovery of the cause of sickness and death in cattle. In the 1920s, on the Northern Plains of America, previously healthy cattle began dying of internal bleeding with no obvious reason. Due to the lack of a pathogenic organism or nutritional deficiency as suspects responsible for the bleeding, the diet of the livestock was analyzed. It was, then, found that wet hay became infected by molds such as Penicillium nigricans and Penicillium jensi, which produced dicoumarol, a metabolite responsible for the disease. In 1945, Karl Link proposed the idea of using a dicoumarol as a rodenticide, but it acted too slowly. After experiments with 150 naturally occurring coumarin derivatives, one compound, later named warfarin, was found to be remarkably active. Initially it was advertised as rodenticide, but after the transition to clinical application in 1955, warfarin was given to President Dwight Eisenhower suffering from a myocardial infarction.
Figure 8.

4-Hydroxy-coumarin drugs. (18) dicoumarol; (19) acenocoumarol; and (20) phenprocoumon.
Warfarin exerts high anticoagulation potency and offers high water solubility and good pharmacokinetic profile (good oral bioavailability and efficient absorption from the digestive tract), however, 4-hydroxy-coumarin derivatives (Figure 8), such as acenocoumarol ((R,S)-4-hydroxy-3-[1-(4-nitrophenyl)-3-oxobutyl]-2H-1-benzopiran-2-one, 19 in Figure 8) or synthetic phenprocoumon (Marcoumar, ((R,S)-4-hydroxy-3-(1-phenylpropyl)-2H-chromen-2-one, 20 in Figure 8) have also been used for the prevention and treatment of thromboembolism [103].
Acenocoumarol acts rapidly and the maximum concentration in plasma is achieved in about 2 h. Whereas an 8 to 11 h half-life time is typically noted, prothrombin time returns to normal 24 to 48 h after the end of the drug intake. In animals and humans, the drug causes no gastrointestinal problems if administered doses are in a normal therapeutic range [104]. Acenocoumarol is metabolized in humans on two paths which involve reduction or oxidation. The reduction converts the nitro group into an amine substituent, or the ketone group into a hydroxyl moiety. Oxidation of acenocoumarol leads to 6- and 7-hydroxy metabolites (Scheme 8).
The anticoagulation effect of phenprocoumon (20 in Figure 8) is connected with a significantly decreased concentration of factor VII and a less decreased concentration of factor V [105].
Other examples of 4-hydroxycoumarin derivatives which antagonize VKOR are those bearing at the position 3 substituted pyridyl (21 in Figure 9), pyrimidinyl (22 in Figure 9), and 3-pyrazolyl (23 in Figure 9) moieties. Comparative in vivo measurements (clotting time (CT) and prothrombin time (PT)) with warfarin as a reference showed that the pyrazolyl derivative bearing –(C=S)-NHPh attached to the nitrogen atom N1 (23a in Figure 9, Ar = 3-pyridyl)) was the most active (19.4%). The pyrazolyl derivative 23b in Figure 9, with Ar = 3,4,5-trimethoxyphenyl was inactive (see Figure 9) [106].
Figure 9.

The examples of 4-hydroxycoumarin derivatives, which antagonize VKOR.
Garazd et al. synthesized several 5-hydroxy- and 7-hydroxy-3,4-cycloannelated coumarin D-glucopyranosides (by condensation of potassium salts of hydroxycoumarins and acetobromosugars) [107]. Compared with the parent coumarins, their glycosides (Figure 10) are very soluble in water.
Figure 10.

5-Hydroxy- and 7-hydroxy-3,4-cycloannelated coumarin D-glucopyranosides.
Compound 24 in Figure 10 was only slightly active. Interestingly, compounds 25 and 26a in Figure 10 over a dose range 0.10–0.30 mg/kg showed hemostatic activity. Compound 24a in Figure 10 at 0.1 mg/kg showed the anticoagulant activity similar to heparin. Compound 25a in Figure 10 (at 0.3 mg/kg; structurally similar to hemostatic 26a in Figure 10, bearing Xylp instead of Arap) and compound 26 in Figure 10 (at 0.25 mg/kg; structurally similar to hemostatic 25 in Figure 10, bearing Arap instead of Glup) were slightly more active than heparin, with CT extended by ca. 6% and 20%, respectively.
The anticoagulant effect accompanied by antihypertensive activity was noted for methylated coumarins bearing an alkylaminohydroxypropoxy side chain at position 4 (27 in Figure 11). These derivatives caused a significant increase in bleeding and clotting time in rats as compared with the reference warfarin. The mechanism of their dual activity has not been identified [108].
Figure 11.

Methylated coumarins with an alkylaminohydroxypropoxy side chain.
Kasperkiewicz and coworkers synthesized new 3-methylidene-4-oxo-coumarin derivatives (28A in Scheme 9) which could adopt tautomeric forms (B and C in Scheme 9), however, X-ray studies revealed the presence of only A and B structures (Scheme 9), with the ring motifs formed by weak hydrogen bonds [109]. The latter tautomer has hydroxyl and imine functions (Scheme 9) and is somewhat similar to the warfarin molecule. The carbonyl-amine structures of analogs bearing in the C-3 position either 2,4- or 3,4-dimethoxybenzylamine moiety (29 and 30, respectively) are shown in Figure 12.
Scheme 9.

Possible tautomeric forms of 28 bearing the 3,4,5-trimethoxybenzylamine (28A) or 3,4,5-trimethoxybenzylimine moiety (28B and 28C).
Figure 12.

Coumarin derivatives 29–30 with two OMe groups in the benzylamine moiety.
The compounds 28–30 (in Scheme 9 and Figure 12) were docked to the vitamin K epoxide reductase complex (subunit 1) and human serum albumin (HSA) to assess their possible anticoagulant effect in comparison to the warfarin enantiomers [109].
Concomitantly with synthetic efforts, new coumarin derivatives were isolated from natural sources. Six new 4-hydroxycoumarin derivatives (some with a rare polycyclic pyrano[3-2c]carbon skeleton) and a few psoralene derivatives were isolated from an Ainsliaea fragrans herb (31–40, Figure 13) [110]. Preliminary studies have showed that compound 35 (Figure 13) was a potent anticoagulant with neither hepatic nor renal significant toxicity.
Figure 13.

Coumarin related compounds isolated from Ainsliaea fragrans.
Golfakhrabadi and coworkers isolated two coumarins, suberosin (41 in Figure 14) and suberenol (42 in Figure 14), from Ferulago carduchorum. These compounds prolonged the prothrombin time at doses of 3 and 6 mg/kg for suberenol, and at dose 6 mg/kg for suberosin [111].
Figure 14.

Structures of suberosin (41) and suberenol (42).
Bang and coworkers synthesized a series of new conjugates of phenolic acids and coumarin starting from 7-(2-bromoethoxy) coumarin derivatives. For several ether and ester derivatives, the anticoagulant activity was assessed by measurement of the prothrombin time. For the most active two compounds 43 and 44 (Figure 15), PT = 10.88 and 13.10 s were noted, so these compounds are 1.5 times more active than warfarin [112].
Figure 15.

Structure of anticoagulants 43 and 44.
Prashantha and coworkers synthesized ten novel coumarins by condensation of 4-hydroxy-coumarin or 7-hydroxy-, 4-methyl-coumarin with acylated amines but none of them showed significant anticoagulant activity and only four compounds were moderately active [113]. The longest clotting time (140 sec) was found for compound 45 (Figure 16), but it is much less than for warfarin (320 s).
Figure 16.

Structure of compound 45.
Many coumarin derivatives are present in natural extracts. Using three solvents (MeOH, EtOH, and water) and microwave assisted extraction at various temperatures, Channabasava prepared nine partially purified extracts from an Indian plant Sonchus oleraceus, in which the presence of coumarin components was confirmed by tests with ferric chloride/nitric acid (FeCl3/HNO3), and 1N sodium hydroxide (NaOH) solution. The extracts were subjected to APTT and PT anticoagulation assays and strong anticoagulant properties (concentration dependent clotting times for APTT 90 to 220 s and PT 40 to 180 s) were observed for one of the methanolic extracts [114]. However, the active compounds remain unidentified.
Shimizu and coworkers prepared an ethanolic extract from a Japanese plant Angelica shikokiana, which, additionally to the earlier reported anti-inflammatory, antioxidant, and antilipase activities, also had interesting antiplatelet and anticoagulant activities. Three coumarin related compounds, i.e., hyuganin C (Figure 17, 46), isoepoxypteryxin, and isopterixin were isolated and hyuganin C had a moderate anticoagulant activity as well as a moderate antiplatelet activity against ADP-induced platelet aggregation [115].
Figure 17.

Structure of hyuganin C 46.
An extract obtained from a Melilotus officinalis plant used in a volume of 25, 50, and 75 μL showed a dose dependent prothrombin time of treated blood of 46 s, 140 s, and no-clot effect, respectively [116]. The extract was fractionated by column chromatography and anticoagulant activity was assessed for nine fractions, in which several coumarins were identified as: dicoumarol (18 in Figure 8), 2-hydroxy-4-methylene-5-oxo-2,3-dihydrofurane[2-3a][1]benzopyrane, 2-hydroxy-5-methylene-6-oxo-2H,6H,-3,4-dihydropyronal[3,2-C][1]benzopyranone, 2-hydroxy-5-oxo-3,4-dihydrofuran[3-2a][1]benzopyrone, 2-hydroxy-5-oxo-3,4 dihydropyronal[3,2-C][1]benzopyrane, as well as 6-amino-, 6-cyano-, 6-carboxy-, and 4-hydroxycoumarin. However, their overall concentration was relatively low.
In Artemisia dracunculus leaf extract (collected from the Sarajevo district) five coumarin derivatives were identified (Table 3) and anticoagulation tests were done, which showed their dose dependent activity [117].
Table 3.
Coumarin derivatives identified in Artemisia dracunculus.
| Coumarin Derivatives | Structures |
|---|---|
| 7,8-Dihydroxy-6-methoxy-coumarin |
|
| Umbeliferone |
|
| 3-Hydroxycoumarin |

|
| Scopoletin |
|
| 6,7-Dihydroxycoumarin |
|
6. Summary
In this review, we described more than fifty coumarin derivatives of either natural or synthetic origin. The selection was based on their ability to inhibit a vitamin K epoxide reductase complex, which is a feature beneficial for patients suffering from too strong blood coagulation. Because of very complex biochemical relations governing the processes of clotting and enzymatic removal of clots (briefly presented in Section 2), inhibition of VKOR must be considered a relatively unsafe treatment with a substantial risk of even fatal side effects. Unfortunately, for a number of patients the already developed coumarin-based drugs are ineffective or their efficacy is much reduced because of mutations in the VKOR protein (for details see Section 4). Thus, an intensive search for new compounds is being carried out worldwide. In our review, we tried to compare the activity of new compounds possessing anticoagulant properties with known coumarin drugs, although crude or fractionated extracts from plants, which have been known for a wide spectrum of activity, were often reported. In many instances the active ingredients remain unidentified. The analysis of structures of those already characterized allowed us to conclude that coumarin derivatives bearing a methoxy or hydroxy group in positions C-3 or C-6 are often potent anticoagulants. Unfortunately, there are still no rules linking their structural features with the mechanism(s) of their action.
Funding
This work was supported by grant no. 503/3-066-02/503-31-001 from the Medical University of Lodz, Poland (to E. Budzisz) and by grant no. 506/1136 from the University of Lodz, Poland (to M.B. Ponczek).
Conflicts of Interest
The authors declare no conflict of interest.
References
- 1.Andersson T., Magnuson A., Bryngelsson I.L., Frøbert O., Henriksson K.M., Edvardsson N., Poçi D. All-cause mortality in 272,186 patients hospitalized with incident atrial fibrillation 1995–2008: A Swedish nationwide long-term case - control study. Eur. Heart J. 2013;34:1061–1067. doi: 10.1093/eurheartj/ehs469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Crowther M.A., Warkentin T.E. Bleeding risk and the management of bleeding complications in patients undergoing anticoagulant therapy: Focus on new anticoagulant agents. Blood. 2008;111:4871–4879. doi: 10.1182/blood-2007-10-120543. [DOI] [PubMed] [Google Scholar]
- 3.Ask the expert: Common Questions about Alcohol and Blood Thinners. [(accessed on 16 December 2019)]; Available online: https://www.healthline.com/health/high-cholesterol/alcohol-blood-thinners-ate.
- 4.Cropp J.S., Bussey H.I. A review of enzyme induction of warfarin metabolism with recommendations for patient management. Pharmacotherapy. 1997;17:917–928. [PubMed] [Google Scholar]
- 5.Heit J.A. The epidemiology of venous thromboembolism in the community. Arterioscler. Thromb. Vasc. Biol. 2008;28:370–372. doi: 10.1161/ATVBAHA.108.162545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Klok F.A., van Kralingen K.W., van Dijk A.P., Heyning F.H., Vliegen H.W., Kaptein A.A., Huisman M.V. Quality of life in long-term survivors of acute pulmonary embolism. Chest. 2010;138:1432–1440. doi: 10.1378/chest.09-2482. [DOI] [PubMed] [Google Scholar]
- 7.Konstantinides S.V., Torbicki A., Agnelli G., Danchin N., Fitzmaurice D., Galiè N., Gibbs J.S., Huisman M.V., Humbert M., Kucher N., et al. ESC guidelines for the diagnosis and management of acute pulmonary embolism in 2014. Working Group of the European Society of Cardiology (ESC) for the diagnosis and management of acute pulmonary embolism. Eur. Heart J. 2014;35:3033–3069. doi: 10.1093/eurheartj/ehu283. [DOI] [PubMed] [Google Scholar]
- 8.Agnelli G., Prandoni P., Becattini C., Silingardi M., Taliani M.R., Miccio M., Imberti D., Poggio R., Ageno W., Pogliani E., et al. Extended oral anticoagulant therapy after a first episode of pulmonary embolism. Ann. Intern. Med. 2003;139:19–25. doi: 10.7326/0003-4819-139-1-200307010-00008. [DOI] [PubMed] [Google Scholar]
- 9.Campbel I.A., Bentley D.P., Prescott R.J., Routledge P.A., Shetty H.G., Williamson I.J. Anticoagulation for three versus six months in patients with deep vein thrombosis or pulmonary embolism, or both: Randomised trial. BMJ. 2007;334:674. doi: 10.1136/bmj.39098.583356.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schulman S., Kakkar A.K., Goldhaber S.Z., Schellong S., Eriksson H., Mismetti P., Christiansen A.V., Friedman J., Le Maulf F., Peter N., et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129:764–772. doi: 10.1161/CIRCULATIONAHA.113.004450. [DOI] [PubMed] [Google Scholar]
- 11.Buller H.R., Prins M.H., Lensin A.W., Prins M.H., Lensin A.W., Decousus H., Jacobson B.F., Minar E., Chlumsky J., Verhamme P., et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N. Engl. J. Med. 2012;366:1287–1297. doi: 10.1056/NEJMoa1113572. [DOI] [PubMed] [Google Scholar]
- 12.Agnelli G., Buller H.R., Cohen A., Curto M., Gallus A.S., Johnson M., Masiukiewicz U., Pak R., Thompson J., Raskob G.E., et al. Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 2013;369:799–808. doi: 10.1056/NEJMoa1302507. [DOI] [PubMed] [Google Scholar]
- 13.Buller H.R., Decousus H., Grosso M.A., Mercuri M., Middeldorp S., Prins M.H., Raskob G.E., Schellong S.M., Schwocho L., Segers A., et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N. Engl. J. Med. 2013;369:1406–1415. doi: 10.1056/NEJMoa1306638. [DOI] [PubMed] [Google Scholar]
- 14.Brandjes D.P., Heijboer H., Buller H.R., de Rijk M., Jagt H., ten Cate J.W. Acenocoumarol and heparin compared with acenocoumarol alone in the initial treatment of proximal-vein thrombosis. N. Engl. J. Med. 1992;327:1485–1489. doi: 10.1056/NEJM199211193272103. [DOI] [PubMed] [Google Scholar]
- 15.Chugh S.S., Havmoeller R., Narayanan K., Singh D., Rienstra M., Benjamin E.J., Gillum R.F., Kim Y.H., McAnulty J.H., Jr., Zheng Z.J., et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation. 2014;129:837–847. doi: 10.1161/CIRCULATIONAHA.113.005119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Baumgartner H., Falk V., Bax J.J., De Bonis M., Hamm C., Holm P.J., Iung B., Lancellotti P., Lansac E., Rodrigez Muñoz D., et al. ESC/EACTS Guidelines for themanagement of valvular heart disease. The Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur. Heart. J. 2017;38:2739–2791. doi: 10.1093/eurheartj/ehx391. [DOI] [PubMed] [Google Scholar]
- 17.Cannegieter S.C., Rosendaal F.R., Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation. 1994;89:635–641. doi: 10.1161/01.CIR.89.2.635. [DOI] [PubMed] [Google Scholar]
- 18.Mok C.K., Boey J., Wang R., Chan T.K., Cheung K.L., Lee P.K., Chow J., Ng R.P., Tse T.F. Warfarin versus dipyridamole-aspirin and pentoxifylline-aspirin for the prevention of prosthetic heart valve thromboembolism: A prospective randomized clinical trial. Circulation. 1985;72:1059–1063. doi: 10.1161/01.CIR.72.5.1059. [DOI] [PubMed] [Google Scholar]
- 19.Regitz-Zagrosek V., Roos-Hesselink J.W., Bauersachs J., Blomström-Lundqvist C., Cífková R., Ferreira R., Foidart J.M., Gibbs J.S., Gohlke-Baerwolf C., Gorenek B., et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur. Heart J. 2018;39:3165–3241. doi: 10.1093/eurheartj/ehy340. [DOI] [PubMed] [Google Scholar]
- 20.Piccini J., Garg J., Patel M., Lokhnygina Y., Goodman S., Becker R., Berkowitz S.D., Breithardt G., Hacke W., Halperin J.L., et al. Management of major bleeding events in patients treated with rivaroxaban versus warfarin: Results from the ROCKET-AF trial. Eur. Heart J. 2014;35:1873–1880. doi: 10.1093/eurheartj/ehu083. [DOI] [PubMed] [Google Scholar]
- 21.Connolly S.J., Ezekowitz M.D., Yusuf S., Eikelboom J., Oldgren J., Parekh A., Pogue J., Reilly P.A., Themeles E., Varrone J., et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009;361:1139–1151. doi: 10.1056/NEJMoa0905561. [DOI] [PubMed] [Google Scholar]
- 22.Granger C.B., Alexander J.H., McMurray J.J., Lopes R.D., Hylek E.M., Hanna M., Al-Khalidi H.R., Ansell J., Atar D., Avezum A., et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011;365:981–992. doi: 10.1056/NEJMoa1107039. [DOI] [PubMed] [Google Scholar]
- 23.Kirchhof P., Benussi S., Kotecha D., Ahlsson A., Atar D., Casadei B., Castella M., Diener H.C., Heidbuchel H., Hendriks J., et al. ESC guidelines for the treatment of atrial fibrillation in 2016, developed in collaboration with EACTS. Working Group of the European Society of Cardiology (ESC) for treatment of atrial fibrillation. Eur. Heart. J. 2016;37:2893–2962. doi: 10.1093/eurheartj/ehw210. [DOI] [PubMed] [Google Scholar]
- 24.Ferland G. Vitamin K. In: Erdman J.W. Jr., Macdonald I.A., Zeisel S.H., editors. Present Knowledge in Nutrition. 10th ed. Wiley-Blackwell; Ames, IA, USA: 2012. pp. 230–247. [Google Scholar]
- 25.Stepien E., Wypasek E., Branicka A., Undas A. Optimalisation of treatment with vitamin K antagonists-the role of gene polymorphisms. Cardiol. Pol. 2010;68:S428–S435. [PubMed] [Google Scholar]
- 26.Natarajan S., Ponde C.K., Rajani R.M., Jijina F., Gursahani R., Dhairyawan P.P., Ashavaid T.F. Effect of CYP2C9 and VKORC1 genetic variations on warfarin dose requirements in Indian patients. Pharmacol. Rep. 2013;65:1375–1382. doi: 10.1016/S1734-1140(13)71496-8. [DOI] [PubMed] [Google Scholar]
- 27.Rishavy M.A., Hallgren K.W., Wilson L.A., Usubalieva A., Runge K.W., Berkner K.L. The vitamin K oxidoreductase is a multimer that efficiently reduces vitamin K epoxide to hydroquinone to allow vitamin K-dependent protein carboxylation. J. Biol. Chem. 2013;288:31556–31566. doi: 10.1074/jbc.M113.497297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tie J.K., Jin D.Y., Straight D.L., Stafford D.W. Functional study of the vitamin K cycle in mammalian cells. Blood. 2011;117:2967–2974. doi: 10.1182/blood-2010-08-304303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rishavy M.A., Usubalieva A., Hallgren K.W., Berkner K.L. Novel Insight into the Mechanism of the Vitamin K Oxidoreductase (VKOR) J. Biol. Chem. 2011;286:7267–7278. doi: 10.1074/jbc.M110.172213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sttaford D.W. The vitamin K cycle. J. Thromb. Haemost. 2005;3:1873–1878. doi: 10.1111/j.1538-7836.2005.01419.x. [DOI] [PubMed] [Google Scholar]
- 31.Watzka M., Geisen C., Bevans C.G., Sittinger K., Spohn G., Rost S., Seifried E., Muller C.R., Oldenburg J. Thirteen novel VKORC1 mutations associated with oral anticoagulant resistance: Insights into improved patient diagnosis and treatment. J. Thromb. Haemost. 2011;9:109–118. doi: 10.1111/j.1538-7836.2010.04095.x. [DOI] [PubMed] [Google Scholar]
- 32.Rost S., Fregin A., Hunerberg M., Bevans C.G., Muller C.R., Oldenburg J. Site-directed mutagenesis of coumarin-type anticoagulant-sensitive VKORC1: Evidence that highly conserved amino acids define structural requirements for enzymatic activity and inhibition by warfarin. Thromb. Haemost. 2005;94:780–786. doi: 10.1160/TH05-02-0082. [DOI] [PubMed] [Google Scholar]
- 33.Pelz H.J., Rost S., Hunerberg M., Fregin A., Heiberg A.C., Baert K., MacNicoll A.D., Prescott C.V., Walker A.S., Oldenburg J., et al. The genetic basis of resistance to anticoagulants in rodents. Genetics. 2005;170:1839–1847. doi: 10.1534/genetics.104.040360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rost S., Fregin A., Ivaskevicius V., Conzelmann E., Hörtnagel K., Pelz H.J., Lappegard K., Seifried E., Scharrer I., Tuddenham E.G., et al. Mutations in VKORC1 cause warfarin resistance and multiple coagulation factor deficiency type 2. Nature. 2004;427:537–541. doi: 10.1038/nature02214. [DOI] [PubMed] [Google Scholar]
- 35.The personalized medicine report. [(accessed on 16 August 2016)]; Available online: http://www.personalizedmedicinecoalition.org/Userfiles/PMC-Corporate/file/pmc_personalized_medicine_tests.pdf.
- 36.Lacy A., O’ Kennedy R. Studies on Coumarins and Coumarin-Related Compounds to Determine their Therapeutic Role in the Treatment of Cancer. Curr. Pharm. Des. 2004;10:3797–3811. doi: 10.2174/1381612043382693. [DOI] [PubMed] [Google Scholar]
- 37.Pechmann V.H., Duisberg C. Neue Bildungsweise der Cumarine. Synthese des Daphnetins. Chem. Ber. 1884;17:929–979. doi: 10.1002/cber.188401701248. [DOI] [Google Scholar]
- 38.Murray R.D.H. Naturally occurring plant coumarins. Prog. Chem. Org. Nat. Prod. 2002;83:1–119. [Google Scholar]
- 39.Haskins F.A., Gorz H.J. Glucosides of Coumarinic and o-Coumarinic Acids in the Tonka Bean. Science. 1963;139:496–497. doi: 10.1126/science.139.3554.496. [DOI] [PubMed] [Google Scholar]
- 40.Stefanachi A., Leonetti F., Pisani L., Catto M., Carotti A. Coumarin: A Natural, Privileged and Versatile Scaffold for Bioactive Compounds. Molecules. 2018;23:250. doi: 10.3390/molecules23020250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Skoczyńska A., Pastuszko A., Budzisz E. Coumarins – properties and application in cosmetology and medicine. Pol. J. Cosmetol. 2014;17:2–13. [Google Scholar]
- 42.Bourgaud F., Hehn A., Larbat R., Doerper S., Gontier E., Kellner S., Matern U. Biosynthesis of coumarins in plants: A major pathway still to be unravelled for cytochrome P450 enzymes. Phytochem. Rev. 2006;5:293–308. doi: 10.1007/s11101-006-9040-2. [DOI] [Google Scholar]
- 43.Hariprassad V., Talele T.T., Kulkarni V.M. Design and synthesis of a novel series of nonpeptidic HIV-1 protease inhibitors. Pharm. Pharmacol. Commun. 1998;4:365–372. [Google Scholar]
- 44.Kaye P.T., Musa M.A., Nichinda A.T., Nocanda X.W. Novel Heterocyclic Analogues of the HIV-1 Protease Inhibitor, Ritonavir. Synth. Commun. 2004;34:2575–2589. doi: 10.1081/SCC-200025617. [DOI] [Google Scholar]
- 45.Tang J., Jones S.A., Jeffrey J.L., Miranda S.R., Galardi C.M., Irlbeck D.M., Brown K.W., McDanal C.B., Johns B.A. Discovery of a novel and potent class of anti-HIV-1 maturation inhibitors with improved virology profile against gag polymorphisms. Bioorg. Med. Chem. Lett. 2017;27:2689–2694. doi: 10.1016/j.bmcl.2017.04.042. [DOI] [PubMed] [Google Scholar]
- 46.Xi G.L., Liu Z.Q. Coumarin-Fused Coumarin: Antioxidant Story from N,N-Dimethylamino and Hydroxyl Groups. J. Agric. Food Chemistry. 2015;63:3516–3523. doi: 10.1021/acs.jafc.5b00399. [DOI] [PubMed] [Google Scholar]
- 47.Sashidhara K.V., Kumar A., Chatterjee M., Rao K.B., Singh S., Verma A.K., Palit G. Discovery and synthesis of novel 3-phenylcoumarin derivatives as antidepressant agents. Bioorg. Med. Chem. Lett. 2011;21:1937–1941. doi: 10.1016/j.bmcl.2011.02.040. [DOI] [PubMed] [Google Scholar]
- 48.Rollinger J.M., Hornick A., Langer T., Stuppner H., Prast H. Acetylcholinesterase inhibitory activity of scopolin and scopoletin discovered by virtual screening of natural products. J. Med. Chem. 2004;47:6248–6254. doi: 10.1021/jm049655r. [DOI] [PubMed] [Google Scholar]
- 49.Chen S., Cho M., Karlsberg K., Zhou D., Yuan Y.C. Biochemical and biological characterization of a novel anti-aromatase coumarin derivative. J. Biol. Chem. 2004;279:48071–48078. doi: 10.1074/jbc.M406847200. [DOI] [PubMed] [Google Scholar]
- 50.Cravotto G., Balliano G., Robaldo B., Oliaro-Bosso S., Chimichi S., Boccalini M. Farnesyloxycoumarins, a new class of squalene-hopene cyclase inhibitors. Bioorg. Med. Chem. Lett. 2004;14:1931–1934. doi: 10.1016/j.bmcl.2004.01.085. [DOI] [PubMed] [Google Scholar]
- 51.Sardari S., Nishibe S., Daneshtalab M. Coumarins, the bioactive structures with antifungal property. Stud. Nat. Prod. Chem. 2000;23:335–393. [Google Scholar]
- 52.Klenkar J., Molnar M. Natural and synthetic coumarins as potential anticancer agents. J. Chem. Pharm. Res. 2015;7:1223–1238. [Google Scholar]
- 53.Refouvelet B., Guyon C., Jacquot Y., Girard C., Fein H., Bevalot F., Robert J.-F., Heyd B., Mantion G., Richert L., et al. Synthesis of 4-hydroxycoumarin and 2,4-quinolinediol derivatives and evaluation of their effects on the viability of HepG2 cells and human hepatocytes culture. Eur. J. Med. Chem. 2004;39:931–937. doi: 10.1016/j.ejmech.2004.07.006. [DOI] [PubMed] [Google Scholar]
- 54.Clark G.S. Coumarin. An aroma chemical profile. Perfum. Flavor. 1995;20:23–34. [Google Scholar]
- 55.Sekar N. Coumarin dyes in laser technology. Colourage. 2003;50:55–56. [Google Scholar]
- 56.Brun M.-P., Bischoff L., Garbay C. A very short route to enantiomerically pure coumarin-bearing fluorescent amino acids. Angew. Chem. Int. Ed. 2004;43:3432–3436. doi: 10.1002/anie.200454116. [DOI] [PubMed] [Google Scholar]
- 57.Nian L., Zhang W., Zhu N., Liu L., Xie Z., Wu H., Wurthner F., Ma Y. Photoconductive Cathode Interlayer for Highly Efficient Inverted Polymer Solar. Cells. 2015;137:6995–6998. doi: 10.1021/jacs.5b02168. [DOI] [PubMed] [Google Scholar]
- 58.Panetta A., Rapoport H. New syntheses of coumarins. J. Org. Chem. 1982;47:946–950. doi: 10.1021/jo00345a009. [DOI] [Google Scholar]
- 59.Jones F., Piermatti O., Pizzo F. Simple and Efficient One-Pot Preparation of 3-Substituted Coumarins in Water. Heterocycles. 1996;43:1257–1266. [Google Scholar]
- 60.Maercker A. The Wittig Reaction. Org. React. 1965;14:270–291. [Google Scholar]
- 61.Mali R.S., Tilve S.G. Useful Synthesis of Coumestans. Synth. Commun. 1990;20:1781–1791. doi: 10.1080/00397919008053103. [DOI] [Google Scholar]
- 62.Upadhyay P.K., Kumar P. A novel synthesis of coumarins employing triphenyl(α-carboxymethylene)- phosphorane imidazolide as a C-2 synthon. Tetrahedron Lett. 2009;50:236–238. doi: 10.1016/j.tetlet.2008.10.133. [DOI] [Google Scholar]
- 63.Nicolaides D.N., Adamopoulos S.G., Lefkaditis D.A., Litinas K.E. Reactions of ortho-Quinones with Ethoxycarbonylmethylene(triphenyl)-phosphorane. Trapping of the ortho- Quinone Methanide Intermediates. J. Chem. Soc. Perkin Trans. 1990;1:2127–2132. doi: 10.1039/p19900002127. [DOI] [Google Scholar]
- 64.Nicolaides D.N., Gautam D.R., Litinas K.E., Papamehael T. Synthesis of some 3,4-dihydro-2H-benzo[f]pyrano[2,3-h]chromen-6-one derivatives. J. Chem. Soc. Perkin Trans. 2002;1:1455–1460. doi: 10.1039/b202640f. [DOI] [Google Scholar]
- 65.Perkin W.H. On propionic coumarin and some of its derivatives. J. Chem. Soc. 1875;28:10–11. doi: 10.1039/JS8752800010. [DOI] [Google Scholar]
- 66.Shriner R.L. The Reformatsky Reaction. Org. React. 1942;1:15–46. [Google Scholar]
- 67.Kostanecki S., Różycki A. A formation of chromone derivatives. Ber. Dtsch. Chem. Ges. 1901;34:102–112. [Google Scholar]
- 68.Heravi M.M., Khaghaninejad S., Mostofi M. Pechmann reaction in the synthesis of coumarin derivatives. J. Adv. Heterocycl. Chem. 2014;112:1–50. [Google Scholar]
- 69.Tyndall S., Fai W.K., VanAlstine-Parris M.A. Insight into the Mechanism of the Pechmann Condensation Reaction Using NMR. J. Org. Chem. 2015;80:8951–8953. doi: 10.1021/acs.joc.5b01802. [DOI] [PubMed] [Google Scholar]
- 70.Khalafi-Nezhad A., Haghighi S.M., Panahi F. Nano-TiO2 on dodecylsulfated silica: As an efficient heterogeneous Lewis acid-surfactant combined catalyst (HLASC) for reaction in aqueous media. ACS Sustain. Chem. Eng. 2013;1:1015–1023. doi: 10.1021/sc4000913. [DOI] [Google Scholar]
- 71.Khaligh N.G. Ultrasound-assisted one-pot synthesis of substituted coumarins catalyzed by poly(4-vinylpyridinium) hydrogen sulfate as an efficient and reusable solid acid catalyst. Ultrason. Sonochem. 2013;20:1062–1068. doi: 10.1016/j.ultsonch.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 72.Jadhav N.H., Sakate S.S., Rasal N.K., Shinde D.R., Pawar R.A. Heterogeneously catalyzed Pechmann condensation employing the tailored Zn0.925Ti0.075O NPs: Synthesis of coumarin. ACS Omega. 2019;4:8522–8527. doi: 10.1021/acsomega.9b00257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Shirini F., Yahyazadeh A., Mohammadi K. A solvent-free synthesis of coumarins using 1,3-disulfonic acid imidazolium hydrogen sulfate as a reusable and effective ionic liquid catalyst. Res. Chem. Intermed. 2015;41:6207–6218. doi: 10.1007/s11164-014-1733-3. [DOI] [Google Scholar]
- 74.EL-Dafrawy S.M., Hassan S.M., Farag M. Kinetics and mechanism of Pechmann condensation reaction over sulphated zirconia-supported zinc oxide. J. Mater. Res. Technol. 2020;9:13–21. doi: 10.1016/j.jmrt.2019.09.063. [DOI] [Google Scholar]
- 75.Singh V., Singh J., Kaur P., Kad G.L. Acceleration of the Pechmann reaction by microwave irradiation: Application to the preparation of coumarin. J. Chem. Research (S) 1997;2:58–59. doi: 10.1039/a605672e. [DOI] [Google Scholar]
- 76.Puri S., Kaur B., Parmar A., Kumar H. Ultrasound-promoted greener synthesis of 2H-chromen-2-ones catalyzed by copper perchlorate in solventless media. Ultrason. Sonochem. 2009;16:705–707. doi: 10.1016/j.ultsonch.2009.04.002. [DOI] [PubMed] [Google Scholar]
- 77.Prousis K.C., Avlonitis N., Heropoulos G.A., Calogeropoulou T. FeCl3-catalysed ultrasonic-assisted, solvent-free synthesis of 4-substituted coumarins. A useful complement to the Pechmann reaction. Ultrason. Sonochem. 2014;21:937–942. doi: 10.1016/j.ultsonch.2013.10.018. [DOI] [PubMed] [Google Scholar]
- 78.Zambare A.S., Khan F.A.K., Zambare S.P., Shinde S.D., Sangshetti J.N. Recent advances in the synthesis of coumarin derivatives via Pechmann condensation. Curr. Org. Chem. 2016;20:798–828. doi: 10.2174/1385272820666151026224227. [DOI] [Google Scholar]
- 79.Ansary I., Taher A. One-Pot Synthesis of Coumarin Derivatives. In: Rao V., Mans D., Rao L., editors. Phytochemicals in Human Health. IntechOpen; London, UK: 2019. pp. 1–34. [Google Scholar]
- 80.Sashidhara K.V., Kumar A., Kumar M., Sonkar R., Bhatia G., Khanna A.K. Novel coumarin derivatives as potential antidyslipidemic agents. Bioorg. Med. Chem. Lett. 2010;20:4248–4251. doi: 10.1016/j.bmcl.2010.05.023. [DOI] [PubMed] [Google Scholar]
- 81.Williams A.C., Camp N. In: Science of Synthesis: Houben-Weyl Methods of Molecular Transformations. Bellus D., Ley S.V., Noyori R., Regitz M., Schaumann E., Shinkai E., Thomas E.J., Trost B.M., Reider P.J., Thomas E.J., editors. Thieme; Stuttgart, Germany: 2004. pp. 347–438. [Google Scholar]
- 82.Baker W., Robinson R. CCLXVI.-Synthetical Experiments in the isoFlavone Group. Part, I. J. Chem. Soc. 1925;127:1981–1986. doi: 10.1039/CT9252701981. [DOI] [Google Scholar]
- 83.Baker W., Eastwood F.M. Colloidal phenoxides. Part, I. The relation between constitution and colloidal properties in benzo-γ-pyrones. J. Chem. Soc. 1929:2897–2907. doi: 10.1039/JR9290002897. [DOI] [Google Scholar]
- 84.Heilbron I.M., Hey D.H., Lythgoe B. Studies in the pyrone series. Part III. Influence of the phenyl group in Kostanecki reaction. J. Chem. Soc. 1936:295–300. doi: 10.1039/jr9360000295. [DOI] [Google Scholar]
- 85.Neelakantan S., Raman P.V., Tinabaye A. A new and convenient synthesis of 4-methyl-3-phenyl-coumarins and 3-phenylcoumarins. Indian J. Chem. Sect. B Org. Chem. Incl. Med. Chem. 1982;21:256–257. [Google Scholar]
- 86.Yamaguchi S., Saitoh M., Kawase Y. Some fatty acids having an O-heterocycle in their terminal positions. II. ω-(3-Coumarinyl)alkanoic acids and ω-(2-chromonyl)alkanoic acids. J. Heterocycl. Chem. 1991;28:125–127. doi: 10.1002/jhet.5570280122. [DOI] [Google Scholar]
- 87.Mentzer C., Meunier P., Antivitamins K.I. Hemorrhagic activity and nature of the heterocyclic ring. Bull. Soc. Chim. Fr. 1943;25:379–383. [Google Scholar]
- 88.Stahmann M.A., Wolff I., Link K.P. Studies on 4-Hydroxycoumarins. I. The Synthesis of 4-Hydroxycoumarins. J. Am. Chem. Soc. 1943;65:2285–2287. doi: 10.1021/ja01252a007. [DOI] [Google Scholar]
- 89.Silverman R.B. Model studies for a molecular mechanism of action of oral anticoagulants. J. Am. Chem. Soc. 1981;103:3910–3915. doi: 10.1021/ja00403a050. [DOI] [Google Scholar]
- 90.Gandhidasan R., Neelakantan S., Raman P.V., Sripathi S.K. A new one - step synthesis of 3-aryl-4-hydroxycoumarins. Indian J. Chem. Sect. B Org. Chem. Incl. Med. Chem. 1988;27:849. [Google Scholar]
- 91.Lokhande P.D., Ghiya B. Novel method in synthesis of 3-phenyl-4-styryl-hydroxycoumarin and 3-phenyl-4-hydroxycoumarins – formation of 3-phenylacetic acid benzisoxazole from 3-phenyl-4-hydroxycoumarin and NH2OH·HCl. J. Indian Chem. Soc. 1989;66:314–315. doi: 10.1002/chin.199004168. [DOI] [Google Scholar]
- 92.Da Re P., Sandri E. Über eine neue Synthese der 4-Hydroxy-cumarine. Chem. Ber. 1960;93:1085–1088. [Google Scholar]
- 93.Chatterjee A.K., Toste F.D., Goldberg S.D., Grubbs R.H. Synthesis of coumarins by ring-closing metathesis. Pure Appl. Chem. 2003;75:421–425. doi: 10.1351/pac200375040421. [DOI] [Google Scholar]
- 94.Nicolaou K.C., Pfefferkorn J.A., Roecker A.J., Cao G.-Q., Barluenga S., Mitchell H.J. Natural product-like combinational libraries based on privileged structures 2. Constructions of a 10,000-membered benzopyran library by directed split-and-pool chemistry using NanoKans and optical encoding. J. Am. Chem. Soc. 2000;122:9939–9953. doi: 10.1021/ja002033k. [DOI] [Google Scholar]
- 95.Ditmer D.C., Li Q., Avilov D.V. Synthesis of coumarins, 4-hydroxycoumarins, and 4-hydroxyquinolinones by tellurium-triggered cyclizations. J. Org. Chem. 2005;70:4682–4686. doi: 10.1021/jo050070u. [DOI] [PubMed] [Google Scholar]
- 96.Klutchko S., Shavel J., von Strandtmann M. Base Rearrangement of chromone-3-carboxylic esters to 3-acyl-4-hydroxycoumarins. J. Org. Chem. 1974;39:2436–2437. doi: 10.1021/jo00930a031. [DOI] [Google Scholar]
- 97.Abdou M.M. 3-Acetyl-4-hydroxycoumarin: Synthesis, reactions and applications. Arabian J. Chem. 2017;10:3664–3675. doi: 10.1016/j.arabjc.2014.04.005. [DOI] [Google Scholar]
- 98.Atrial Fibrillation and New Oral Anticoagulant Drugs. [(accessed on 10 March 2016)]; Available online: http://www.fda.gov/Drugs/NewsEvents/ucm405148.htm.
- 99.Hirsh J., Dalen J., Anderson D.R., Poller L., Bussey H., Ansell J., Deykin D. Oral anticoagulants: Mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 2001;119:8S–21S. doi: 10.1378/chest.119.1_suppl.8S. [DOI] [PubMed] [Google Scholar]
- 100.Inoue T., Nitta K., Sugihara K., Horie T., Kitamura S., Ohta S. CYP2C9-Catalyzed Metabolism of S-Warfarin to 7-Hydroxywarfarin in Vivo and in Vitro in Chimeric Mice with Humanized Liver. Drug. Metab. Dispos. 2008;36:2429–2433. doi: 10.1124/dmd.108.022830. [DOI] [PubMed] [Google Scholar]
- 101.Zhou Q., Zhou S., Chan E. Effect of Coenzyme Q10 on Warfarin Hydroxylation in Rat and Human Liver Microsomes. Curr. Drug Metab. 2005;6:67–81. doi: 10.2174/1389200053586091. [DOI] [PubMed] [Google Scholar]
- 102.Guasch L., Peach M.L., Nicklaus M.C. Tautomerism of Warfarin: Combined Chemoinformatics, Quantum Chemical, and NMR Investigation. J. Org. Chem. 2015;80:9900–9909. doi: 10.1021/acs.joc.5b01370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Borges F., Roleira F., Milhazes N., Santana L., Uriarte E. Simple Coumarins and Analogues in Medicinal Chemistry: Occurrence, Synthesis and Biological Activity. Curr. Med. Chem. 2005;12:887–916. doi: 10.2174/0929867053507315. [DOI] [PubMed] [Google Scholar]
- 104.Mayer G.A., Conell W.F. The Anticoagulant Effect of a New Coumarin Derivative—Sintrom (Geigy) and Its Control by Standardized Clotting Time. Can, Med. Assoc. J. 1957;76:272–278. [PMC free article] [PubMed] [Google Scholar]
- 105.Prior I.A.M. Anticoagulant Studies with “Marcoumar”, A New Coumarin Derivative. Br. Med. J. 1955;2:944–946. doi: 10.1136/bmj.2.4945.944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Abdelhafez O.M., Amin K.M., Batran R.Z., Maher T.J., Nada S.A. Sethumadhavan, S. Synthesis, anticoagulant and PIVKA-II induced by new 4-hydroxycoumarin derivatives. Bioorg. Med. Chem. 2010;18:3371–3378. doi: 10.1016/j.bmc.2010.04.009. [DOI] [PubMed] [Google Scholar]
- 107.Garazd Y.L., Kornienko E.M., Maloshtan L.N., Garazd M.M., Khilya V.P. Modified Coumarins. 17. Synthesis and Anticoagulant Activity of 3,4-Cycloannelated Coumarin D-Glycopyranosides. Chem. Nat. Comp. 2005;41:508–512. doi: 10.1007/s10600-005-0194-8. [DOI] [Google Scholar]
- 108.Thumber B.L., Vasoya V.G., Desai T.R., Naliapara Y.T., Shah K.V., Tirgar P.R. Anticoagulant activity of methylated coumarin derivatives. Pharm. Online 2. 2011:1010–1017. [Google Scholar]
- 109.Kasperkiewicz K., Malecka M., Ponczek M.B., Nowak P., Budzisz E. Design, synthesis, X-ray structures of the new coumarin derivatives and perspectives of binding them to albumin and vitamin K epoxide reductase complex subunit 1. Cryst. Growth Des. 2016;16:456–466. doi: 10.1021/acs.cgd.5b01456. [DOI] [Google Scholar]
- 110.Lei L., Xue Y., Liu Z., Peng S., He Y., Zhang Y., Fang R., Wang J.P., Luo Z.W., Yao G.M., et al. Coumarin derivatives from Ainsliaea fragrans and their anticoagulant activity. Sci. Rep. 2015;5:13544. doi: 10.1038/srep13544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Golfakhrabadi F., Abdollahi M., Ardakani M.R., Saeidnia S., Akbarzadeh T., Ahmadabadi A.N., Ebrahimi A., Yousefbeyk F., Hassanzadeh A., Khanavi M. Anticoagulant activity of isolated coumarins (suberosin and suberenol) and toxicity evaluation of Ferulago carduchorum in rats. Pharm. Biol. 2014;52:1335–1340. doi: 10.3109/13880209.2014.892140. [DOI] [PubMed] [Google Scholar]
- 112.Bang N.C., Abyshev A.Z., Ivkin D.Y. Synthesis and in vivo evaluation of new coumarin conjugates as potential indirect-action anticoagulants. Pharm. Chem. J. 2019;53:419–422. doi: 10.1007/s11094-019-02013-z. [DOI] [Google Scholar]
- 113.Venkatramaiah T., Prashantha Kumar B.R. Design, synthesis and anticoagulant activity of some novel coumarins. Asian J. Pharm. Anal. Med. Chem. 2018;6:105–122. [Google Scholar]
- 114.Govindappa M., Chandrashekhar N., Channabasava B.P. Anticoagulant activity of partially purified coumarin(s) extracts of Sonchus oleraceus. Adv. Med. Plant Res. 2015;3:87–91. [Google Scholar]
- 115.Mira A., Alkhiary W., Shimizu K. Antiplatelet and Anticoagulant Activities of Angelica shikokiana Extract and Its Isolated Compounds. Clin. Appl. Thromb/Hemost. 2017;23:91–99. doi: 10.1177/1076029615595879. [DOI] [PubMed] [Google Scholar]
- 116.Hashim F.J., Hussain S.M., Shawkat M.S. Separation, Characterization and Anticoagulant Activity of Coumarin and its Derivatives Extracted from Melilotus officinalis. Biosci. Biotech. Res. Asia. 2017;14 doi: 10.13005/bbra/2412. [DOI] [Google Scholar]
- 117.Durić K., Kovac Besovic E.E., Niksic H., Muratovic S., Sofic E. Anticoagulant activity of some Artemisia dracunculus leaf extracts. Bosn. J. Basic Med. Sci. 2015;15:9–14. doi: 10.17305/bjbms.2015.384. [DOI] [PMC free article] [PubMed] [Google Scholar]