

Abstract
Background
Escalating awareness of the magnitude of the challenge posed by low levels of physical activity in people with chronic obstructive pulmonary disease (COPD) highlights the need for interventions to increase physical activity participation. The widely‐accepted benefits of physical activity, coupled with the increasing availability of wearable monitoring devices to objectively measure participation, has led to a dramatic rise in the number and variety of studies that aimed to improve the physical activity of people with COPD. However, little was known about the relative efficacy of interventions tested so far.
Objectives
In people with COPD, which interventions are effective at improving objectively‐assessed physical activity?
Search methods
We identified trials from the Cochrane Airways Trials Register Register, which contains records identified from bibliographic databases including the Cochrane Central Register of Controlled Trials, MEDLINE, Embase, CINAHL, AMED, and PsycINFO. We also searched PEDro, ClinicalTrials.gov, the World Health Organization International Clinical Trials Registry Platform portal and the Australian New Zealand Clinical Trials Registry (from inception to June 2019). We checked reference lists of all primary studies and review articles for additional references, as well as respiratory journals and respiratory meeting abstracts, to identify relevant studies.
Selection criteria
We included randomised controlled trials of interventions that used objective measures for the assessment of physical activity in people with COPD. Trials compared an intervention with no intervention or a sham/placebo intervention, an intervention in addition to another standard intervention common to both groups, or two different interventions.
Data collection and analysis
We used standard methods recommended by Cochrane. Subgroup analyses were possible for supervised compared to unsupervised pulmonary rehabilitation programmes in clinically‐stable COPD for a range of physical activity outcomes. Secondary outcomes were health‐related quality of life, exercise capacity, adverse events and adherence. Insufficient data were available to perform prespecified subgroup analyses by duration of intervention or disease severity. We undertook sensitivity analyses by removing studies that were at high or unclear risk of bias for the domains of blinding and incomplete outcome data.
Main results
We included 76 studies with 8018 participants. Most studies were funded by government bodies, although some were sponsored by equipment or drug manufacturers. Only 38 studies had physical activity as a primary outcome. A diverse range of interventions have been assessed, primarily in single studies, but improvements have not been systematically demonstrated following any particular interventions. Where improvements were demonstrated, results were confined to single studies, or data for maintained improvement were not provided. Step count was the most frequently reported outcome, but it was commonly assessed using devices with documented inaccuracy for this variable.
Compared to no intervention, the mean difference (MD) in time in moderate‐ to vigorous‐intensity physical activity (MVPA) following pulmonary rehabilitation was four minutes per day (95% confidence interval (CI) −2 to 9; 3 studies, 190 participants; low‐certainty evidence). An improvement was demonstrated following high‐intensity interval exercise training (6 minutes per day, 95% CI 4 to 8; 2 studies, 275 participants; moderate‐certainty evidence). One study demonstrated an improvement following six months of physical activity counselling (MD 11 minutes per day, 95% CI 7 to 15; 1 study, 280 participants; moderate‐certainty evidence), but we found mixed results for the addition of physical activity counselling to pulmonary rehabilitation. There was an improvement following three to four weeks of pharmacological treatment with long‐acting muscarinic antagonist and long‐acting beta2‐agonist (LAMA/LABA) compared to placebo (MD 10 minutes per day, 95% CI 4 to 15; 2 studies, 423 participants; high‐certainty evidence). These interventions also demonstrated improvements in other measures of physical activity.
Other interventions included self‐management strategies, nutritional supplementation, supplemental oxygen, endobronchial valve surgery, non‐invasive ventilation, neuromuscular electrical stimulation and inspiratory muscle training.
Authors' conclusions
A diverse range of interventions have been assessed, primarily in single studies. Improvements in physical activity have not been systematically demonstrated following any particular intervention. There was limited evidence for improvement in physical activity with strategies including exercise training, physical activity counselling and pharmacological management. The optimal timing, components, duration and models for interventions are still unclear. Assessment of quality was limited by a lack of methodological detail. There was scant evidence for a continued effect over time following completion of interventions, a likely requirement for meaningful health benefits for people with COPD.
Plain language summary
What are the most effective ways to encourage people with chronic obstructive pulmonary disease (COPD) to be more physically active?
Background
Being physically active is important for everyone's health. It can be particularly difficult for people with COPD and we do not know the best way to improve physical activity.
Study characteristics
This review includes 76 studies involving 8018 people with COPD (published before 27 June 2019). Most studies were funded by government bodies, although some were sponsored by equipment or drug manufacturers. Many strategies have been developed and different studies have measured physical activity in lots of different ways. This means that it was hard to compare and combine their findings. It was also hard to tell exactly what was involved in some of the interventions, and therefore which components were important for improving physical activity.
Key results
Some studies looked at current interventions for people with COPD, including pulmonary rehabilitation and different types of exercise training as well as self‐management and education. Other studies have looked at special types of nutritional supplements, oxygen therapy, surgery, muscle stimulation and singing.
Some strategies that did work involved exercise training, physical activity counselling and COPD medications. Some studies showed that people did an extra 6 to 24 minutes of at least moderate‐intensity physical activity, as well as walking for longer or taking more steps each day. However, we are still uncertain about when or how these approaches should be used. Only a few studies followed people up after the intervention finished. It is not clear exactly what needs to be done to improve physical activity in the long term, which is what may be required for health benefits.
Quality of the evidence
The quality of evidence was generally low, due to difficulties working out exactly what people did in the studies, and also because there were lots of single studies (some quite small) looking at different types of interventions. This means that it was difficult to generalise these findings to all people with COPD.
Summary of findings
Summary of findings for the main comparison. Pulmonary rehabilitation/exercise training versus no intervention.
|
Population: people with COPD, clinical stability Intervention: pulmonary rehabilitation/exercise training Comparisons: intervention versus no intervention Outcome: time in physical activity (of at least moderate intensity) at end intervention | ||||||
| Interventions | Outcome | Illustrative comparative risks* [mean difference (95% CI) unless indicated] | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| No intervention | Pulmonary rehabilitation/exercise training | |||||
| Pulmonary rehabilitation vs. no intervention (8 to 10 weeks) |
Time/change in time in MVPA | The mean change in time ranged from −1 to 6 minutes per day, mean time 27 minutes per day | The mean difference was 4 (−2 to 9) minutes per day | 190 participants (3 studies; Analysis 1.2) | ⊕⊕⊝⊝ lowa | Baseline values: De Roos 2017 no intervention mean 11 (SD 10), pulmonary rehabilitation 12 (11); Wootton 2017 no intervention 46 (39), pulmonary rehabilitation 54 (43) |
| High‐intensity interval training vs. no intervention (8 to 12 weeks) |
Time in MVPA | The mean time ranged from 12 to 14 minutes per day | The mean difference was 6 (4 to 8) minutes per day | 275 participants (2 studies; Analysis 1.9) | ⊕⊕⊕⊝ moderateb |
‐ |
| Maintenance (telerehabilitation) following high‐intensity interval training vs. no intervention (12 months) |
Time in moderate intensity physical activity | The mean time was 11 minutes per day | The mean difference was 7 (4 to 10) minutes per day | 97 participants (1 study; Vasilopoulou 2017; Table 2) | ⊕⊕⊕⊝ moderateb |
‐ |
| Maintenance (centre‐based) following high intensity interval training vs. no intervention (12 months) |
The mean difference was 11 (8 to 14) minutes per day | 100 participants (1 study; Vasilopoulou 2017; Table 2) | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MVPA: moderate‐to‐vigorous physical activity; SD: standard deviation | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
aDowngraded one level for high risk of performance bias. Downgraded one level for imprecision as CI does not exclude possibility of no effect. bDowngraded one level for high risk of performance bias.
1.2. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 2 time/change in time in moderate‐to‐vigorous intensity physical activity (minutes per day); Intervention: pulmonary rehabilitation/exercise training.
1.9. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 9 time in moderate‐to‐vigorous intensity physical activity (minutes per day); Intervention: high‐intensity interval training.
1. Physical activity outcomes.
| Study |
Comparison (setting, if known) Clinical stability unless indicated |
Timepoint (end intervention unless indicated) | Outcome (minutes unless indicated) | Intervention group | Comparison group | Between‐group MD (95% CI) where available unless indicated | ||
| n | mean (95% CI) unless indicated | n | mean (95% CI) unless indicated | |||||
| Altenburg 2015 | Physical activity counselling vs. no intervention (primary care) | 12 weeks | ∆ step count (n) | 22 | median 537 (IQR −611 to 1740) | 18 | median 431 (IQR −899 to 749) | P = 0.48* |
| ∆ "daily physical activity" (n) | median 1408 (IQR −2165 to 3304) | median 528 (IQR −966 to 2179) | P = 0.35* | |||||
| follow‐up (12 months post‐intervention) | ∆ step count (n) | 20 | median 157 (IQR −1679 to 994) | 18 | median 48 (IQR −1004 to 885) | P = 0.90* | ||
| ∆ "daily physical activity" (n) | median 353 (IQR −1518 to 3038) | median −576 (IQR −2517 to 1008) | P = 0.26* | |||||
| Physical activity counselling vs. no intervention (secondary care) | 12 weeks | ∆ step count (n) | 21 | median 1002 (IQR −612 to 3077) | 22 | median −814 (IQR −2827 to 1063) | P = 0.007* | |
| ∆ "daily physical activity" (n) | median 1575 (IQR −752 to 3864) | median −1041 (IQR −1971 to 1031) | P = 0.007* | |||||
| follow‐up (12 months post‐intervention) | ∆ step count (n) | 20 | median 1128 (IQR −1322 to 2707) | 19 | median −217 (IQR −1951 to 1147) | P = 0.15* | ||
| ∆ "daily physical activity" (n) | median 1798 (IQR −1994 to 3128) | median −718 (IQR −1812 to 512) | P = 0.11* | |||||
| Physical activity counselling with PR vs. PR | 12 weeks | ∆ step count (n) | 22 | median 547 (IQR 187 to 1323) | 15 | median −211 (IQR −1337 to 1038) | P = 0.03* | |
| ∆ "daily physical activity" (n) | median 1302 (IQR −173 to 1922) | median −849 (IQR −2223 to 961) | P = 0.03* | |||||
| follow‐up (12 months post‐intervention) | ∆ step count (n) | 10 | median −569 (IQR −2512 to 1551) | 13 | median −1137 (IQR −2376 to 1427) | P = 0.58* | ||
| ∆ "daily physical activity" (n) | median −213 (IQR −4525 to 2274) | median −1827 (IQR −3540 to 629) | P = 0.97* | |||||
| Physical activity counselling vs. no intervention (primary care) SUBGROUP: ≥ 10,000 steps per day (baseline) |
12 weeks | ∆ step count (n) | median 675 (IQR 4 to 1853) | median 342 (IQR −955 to 658) | P = 0.20* | |||
| ∆ "daily physical activity" (n) | median 1807 (IQR 164 to 3720) | median 519 (IQR −1089 to 1709] | P = 0.11* | |||||
| follow‐up (12 months post‐intervention) | ∆ step count (n) | median 201 (IQR −693 to 1170) | median 38 (IQR −1071 to 821) | P = 0.55* | ||||
| ∆ "daily physical activity" (n) | median 525 (IQR −545 to 3078) | median −726 (IQR −2954 to 711) | P = 0.06* | |||||
| Physical activity counselling vs. no intervention (secondary care) SUBGROUP: ≤ 10,000 steps per day (baseline) |
12 weeks | ∆ step count (n) | median 1289 (IQR −183 to 3107) | median 34 (IQR −1707 to 1095) | P = 0.02* | |||
| ∆ "daily physical activity" (n) | median 1763 (IQR −763 to 3913) | median −925 (IQR −1452 to 1052) | P = 0.03* | |||||
| follow‐up (12 months post‐intervention) | ∆ step count (n) | median 1436 (IQR −1492 to 2722) | median 0 (IQR −1825 to 1103) | P = 0.12* | ||||
| ∆ "daily physical activity" (n) | median 1928 (IQR −1140 to 3320) | median −526 (IQR −1657 to 435) | P = 0.078* | |||||
| Physical activity counselling with PR vs. PR SUBGROUP: ≤ 10,000 steps per day (baseline) |
12 weeks | ∆ step count (n) | median 547 (IQR 187 to 1323) | median −198 (IQR −1403 to 1051) | P = 0.04* | |||
| ∆ "daily physical activity" (n) | median 1302 (IQR −173 to 1922) | median −843 (IQR −1737 to 1329) | P = 0.052* | |||||
| follow‐up (12 months post intervention) | ∆ step count (n) | median −569 (IQR −1770 to 2170) | median −759 (IQR −2027 to 1641) | P = 0.78* | ||||
| ∆ "daily physical activity" (n) | median −213 (IQR −4525 to 2274) | median −644 (IQR −3706 to 844) | P = 0.91* | |||||
| Beeh 2014 | LAMA vs. placebo | 3 weeks | ∆ step count (n) | 51 | median 69 (IQR −834 to 1262) | 53 | median 125 (IQR −1180 to 1249) | P = 0.73 |
| ∆ MVPA time | median 1 (IQR −22 to 25) | median −6 (IQR −21 to 15) | P = 0.11 | |||||
| ∆ PAL | median 0.00 (IQR −0.08 to 0.09) | median −0.01 (IQR −0.09 to 0.09) | P = 0.95 | |||||
| ∆ active EE (kcal) | median 10 (−131 to 116) | median −44 (IQR −122 to 40) | P = 0.11 | |||||
| Bender 2016 | Physical activity counselling with pedometer vs. pedometer | 12 weeks | step count (n) | 49 | x | 50 | x | x |
| Benzo 2016 | Self‐management (health coaching) with PR referral vs. PR referral | 12 months | ∆ PAL | 108 | mean −0.10 | 106 | mean 0.01 | P = not significant* |
| step count (n) | only baseline values reported | only baseline values reported | "We did not find a difference in any physical activity outcome between the intervention and control arms at any time point"* | |||||
| time sedentary | ||||||||
| LIPA time | ||||||||
| MPA time | ||||||||
| VPA time | ||||||||
| resting metabolic rate (calories per 24 hours) | ||||||||
| total EE (calories per 24 hours) | ||||||||
| Blumenthal 2014 | Self‐management vs. education and symptom management | 16 weeks | activity time | 162 | mean 13 (SE 1) | 164 | mean 11 (SE 1) | P = 0.045* |
| MPA time | mean 6 (SE 0.4) | mean 5.5 (SE 0.4) | 0.5 (−0.6 to 1.6) | |||||
| total EE ("caloric expenditure") | mean 3605 (SE 211) | mean 3113 (SE 212) | P = 0.022* | |||||
| Borges 2014 | Exercise training (whole‐body resistance training) vs. no intervention (inpatient) | 4‐week follow‐up | time lying | 15 | mean 224 (SD 131) | 14 | mean 203 (SD 140) | 21 (−78 to 120) |
| time sitting | mean 287 (122) | mean 298 (SD 107) | −11 (−94 to 72) | |||||
| time standing | mean 168 (104) | mean 153 (SD 94) | 15 (−57 to 87) | |||||
| time walking | mean 31 (21) | mean 50 (SD 35) | −19 (−40 to 2) | |||||
| Breyer 2010 | Nordic walking with education vs. education | 12 weeks | ∆ time sitting | 30 | mean −128 (SD 15) | 30 | "Controls did not show any significant change in their daily physical activities at any time point" | P = 0.014* |
| ∆ time standing | mean 129 (SD 26) | x | ||||||
| ∆ time walking | mean 15 (SD 20) | P = 0.034* | ||||||
| follow‐up (3 months post‐intervention) | ∆ time sitting | mean −120 (SD 32) | P < 0.05* | |||||
| ∆ time standing | mean 133 (SD 14) | P < 0.05* | ||||||
| ∆ time walking | mean 13 (SD 2) | x | ||||||
| follow‐up (6 months post‐intervention) | time sitting | mean 233 (SD 172) | mean 342 (SD 126) | P < 0.01* | ||||
| time standing | mean 320 (SD 178) | mean 220 (SD 130) | P = 0.16 | |||||
| time walking | mean 56 (SD 38) | mean 32 (SD 25) | P < 0.01 | |||||
| Chaplin 2017 | Web‐based PR vs. centre‐based PR | 7 weeks | step count (n) | 20 | x | 34 | x | P = 0.37* |
| "20 min bouts of purposeful activity" (n) | mean change 10% | x | P = 0.26* | |||||
| Charususin 2018 | Inspiratory muscle training with PR vs. sham with PR | 12 weeks (total n = 150) | step count (n) | x | mean 3958 (SD 2253) | x | mean 4506 (SD 1899) | −206 (−923 to 512)* |
| Curtis 2016 | ACE inhibitor with PR vs. placebo with PR | 10 weeks | ∆ step count (n) | 18 | mean −382 (SD 2082) | 22 | mean 561 (SD 2528) | −943 (−2372 to 486) |
| ∆ PAL | mean −0.06 (SD 0.16) | mean 0.04 (SD 0.15) | −0.10 (−0.20 to −0.00) | |||||
| Demeyer 2017 | Physical activity counselling vs. no intervention | 12 weeks | ∆ time walking | 140 | 7 (1 to 13) | 140 | −10 (−14 to −6) | 17 (10 to 24) |
| ∆ intensity movement (m/s2) | 0.06 (0.02 to 0.10) | −0.03 (−0.06 to −0.00) | 0.09 (0.04 to 0.14) | |||||
| ∆ MVPA time | 8 (5 to 12) | −3 (−6 to 0.2) | 11 (7 to 15) | |||||
| Duiverman 2008 | Non‐invasive ventilation with PR vs. PR | 12 weeks | step count (n) | 24 | median 2799 (IQR 891 to 6135) | 32 | median 2093 (IQR 914 to 3155) | median 1269 (IQR 242 to 2296)* |
| Felcar 2018 | Water‐based exercise training vs. land‐based exercise training | 6 months | active (n) (> 7500 steps per day) | 20 | baseline 4 end intervention 10 |
16 | baseline 4 end intervention 5 |
x |
| Hartman 2016 | Endobronchial valve surgery vs. no intervention | 6 months post‐surgery | ∆ step count (n) | 19 | 1252 (545 to 1960) | 24 | −148 (−512 to 216) | 1400 (655 to 2145) |
| ∆ time walking (%) | 1 (0 to 2) | 0 (−1 to 0) | 1 (0 to 2) | |||||
| ∆ time sitting (%) | 0 (−3 to 3) | 2 (1 to 3) | −2 (−5 to 1) | |||||
| ∆ time inactive | −1 (−3 to 1) | 0 (−1 to 1) | −1 (−3 to 1) | |||||
| ∆ intensity movement (g) | 0.01 (0.00 to 0.01) | 0.00 (−0.01 to 0.00) | 0.01 (0.00 to 0.02) | |||||
| Hornikx 2015 | Physical activity counselling vs. no intervention | 4 weeks | ∆ step count (n) | 12 | 984 (217 to 1752) | 14 | 1013 (307 to 1719) | −29 (−969 to 911) |
| ∆ time walking | 13 (3 to 23) | 13 (5 to 21) | 0 (−12 to 12) | |||||
| ∆ intensity movement (m/s2) | 0.06 (0.03 to 0.09) | 0.08 (−0.05 to 0.11) | −0.02 (−0.06 to 0.02) | |||||
| Jolly 2018 | Self‐management vs. no intervention | 12 months | MVPA time a week | 179 | mean 347 (SD 277) | 232 | mean 316 (SD 256) | 12 (−21 to 45)* |
| Kanabar 2015 | Self‐management (SPACE) vs. no intervention (post‐admission) | 7 days | ∆ step count (n) | 15 | −208 (−1146 to 730) | 10 | −518 (−2572 to 1536) | 310 (−1665 to 2285) |
| ∆ time sedentary | −14 (−71 to 43) | −18 (−87 to 51) | 4 (−75 to 83) | |||||
| ∆time in "physical activity" | −1 (−14 to 12) | −16 (−66 to 34) | 15 (−30 to 60) | |||||
| ∆ MPA time | −1 (−14 to 12) | −14 (−61 to 33) | 13 (−30 to 56) | |||||
| ∆ VPA time | 0 (−1 to 1) | −2 (−61 to 2) | 2 (−1 to 5) | |||||
| ∆ total EE (kcal) | −128 (−236 to −20) | −98 (−292 to 96) | −30 (−225 to 165) | |||||
| ∆ active EE (kcal) | −12 (−77 to 53) | −97 (−310 to 116) | 85 (−108 to 278) | |||||
| Kawagoshi 2015 | Physical activity counselling with PR vs. PR | 12 months | ∆ time sitting | 12 | 59 (−6 to 124) | 15 | 6 (−44 to 56) | 53 (−21 to 127) |
| ∆ time standing | 43 (24 to 60) | 31 (5 to 57) | 11 (−18 to 40) | |||||
| ∆ time walking | 51 (10 to 92) | 12 (−2 to 27) | 39 (1 to 78) | |||||
| ∆ time lying | −53 (−96 to −10) | −29 (−60 to 2) | −24 (−72 to 24) | |||||
| ∆ frequency postural changes: total (n) | 40 (−2 to 82) | 19 (−5 to 43) | 21 (−23 to 65) | |||||
| ∆ frequency postural changes: getting up (n) | 0 (−16 to 16) | 6 (−11 to 23) | −6 (−27 to 15) | |||||
| ∆ frequency postural changes: standing up (n) | 43 (5 to 81) | 14 (−5 to 33) | 29 (−9 to 67) | |||||
| Larson 2014 | Exercise‐specific self‐efficacy training with upper‐body resistance training vs. upper‐body resistance training | 4 months | time sedentary | 15 | mean 602 (SD 112) | 20 | mean 577 (SD 107) | 25 (−49 to 99) |
| time sedentary (% monitored time) | mean 70 (SD 10) | mean 70 (SD 9) | 0 (−6 to 6) | |||||
| MVPA time | mean 6 (SD 6) | mean 4 (SD 3) | 2 (−1 to 5) | |||||
| Upper‐body resistance training with health education vs. health education | time sedentary | 20 | mean 577 (SD 107) | 14 | mean 634 (SD 114) | −57 (−133 to 19) | ||
| time sedentary (% monitored time) | mean 70 (SD 9) | mean 70 (SD 9) | −2 (−8 to 4) | |||||
| MVPA time | mean 4 (SD 3) | mean 3 (SD 2) | 1 (−1 to 3) | |||||
| Loeckx 2018 | Physical activity counselling with PR vs. PR | 12 weeks | ∆ step count (n) | 25 | x | 25 | x | MD 1319 (SE 571), P = 0.02* |
| ∆ MVPA time | MD 8 (SE 4), P = 0.11* | |||||||
| 9 months (follow‐up) | ∆ step count (n) | MD 1348 (SE 628), P = 0.03* | ||||||
| ∆ MVPA time | MD 13 (SE 5), P = 0.02* | |||||||
| Lord 2012 | Singing vs. sham | 8 weeks | ∆ step count (n) | 13 | −763 (−1758 to 232) | 11 | 1011 (337 to 1685) | −1774 (−2848 to −700) |
| ∆ time sedentary | −36 (−113 to 41) | −27 (−72 to 18) | −9 (−88 to 71) | |||||
| ∆ “physical activity duration” | −93 (−224 to 38) | 50 (22 to 77) | −142 (−263 to −22) | |||||
| ∆ "activity‐related" EE (kJ) | −144 (−408 to 119) | 229 (131 to 327) | −373 (−625 to −121) | |||||
| Louvaris 2016 | High‐intensity interval training vs. no intervention | 12 weeks | step count (n) | 85 | mean 5136 (SD 2866) | 43 | mean 3453 (SD 2493) | 1683 (721 to 2646) |
| vector magnitude units (n) | mean 495 (SD 213) | mean 406 (SD 205) | 89 (13 to 165) | |||||
| "sedentarism" (%) (< 5000 steps per day) | baseline 69 end intervention 48 |
baseline 68 end intervention 69 |
x | |||||
| Magnussen 2017 | LAMA vs. placebo | 3 weeks | ∆ step count (n) | 14 | median 177 (IQR −222 to 1038) | 15 | median 86 (IQR −366 to 1000) | P = 0.63 |
| ∆ MVPA time | median −2 (IQR −12 to 26] | median −4 (IQR −16 to 19) | P = 0.51 | |||||
| ∆ PAL | median 0.01 (IQR −0.03 to 0.07] | median 0.01 (IQR −0.06 to 0.04) | P = 0.71 | |||||
| ∆ active EE (kcal) | median 43 (IQR −25 to 153) | median 17 (IQR −69 to 50) | P = 0.51 | |||||
| Mantoani 2018 | Physical activity counselling with PR vs. PR | 12 weeks | ∆ step count (n) | 22 | mean 1251 (SD 2408) | 22 | mean −410 (SD 1118) | 1661 (552 to 2770) |
| Mendoza 2015 | Pedometer with physical activity counselling vs. physical activity counselling | 12 weeks | ∆ step count (n) | 50 | mean 3080 (SD 3255) | 47 | mean 138 (SD 1950) | 2942 (1881 to 4003) |
| Mitchell 2013 | Self‐management (SPACE) vs. no intervention | 6 weeks | ∆ step count (n) | 52 | 333 (−85 to 751) | 65 | −214 (−566 to 138) | 547 (12 to 1082) |
| ∆ time sedentary | −10 (−53 to 33) | 13 (−21 to 47) | −23 (−77 to 31) | |||||
| ∆ total EE (kcal) | −4 (−105 to 97) | −20 (−83 to 43) | 16 (−100 to 132) | |||||
| time in bouts (data from graph) | median 142 (95% CI 91 to 190) | median 96 (95% CI 56 to 135) | P = 0.215* | |||||
| Nakamura 2016 | LAMA (aclidinium bromide) vs. LAMA (tiotropium) | 8 weeks | "physical activity with sedentary time" | 22 | x | 22 | x | P = 0.385* |
| NCT00144326 | LAMA vs. placebo | 12 weeks | not defined | 123 | x | 125 | x | "increase of activity in tiotropium relative to placebo from 7.9% to 12.23%" "the majority of the mean values over time in the tiotropium group are larger than those in the placebo group" |
| NCT01351792 | ICS (beclomethasone) with LABA (formoterol) vs. ICS (budesonide) with LABA (formoterol) | 16 weeks (4‐week run‐in, 12 week intervention) | step count (n) | 30 | mean 3826 (SD 2097) | 29 | mean 3510 (SD 2409) | 316 (−838 to 1470) |
| Ng 2015 | Four‐wheeled walker vs. no intervention | 4 weeks | step count (n) | 8 | mean 6465 (SD 4541) minimum 3039, maximum 16,558 |
9 | mean 2384 (SD 1319) minimum 574, maximum 4453 |
4081 (818 to 7344) N.B. no baseline assessment; likely imbalance, data skewed |
| Nolan 2017 | Physical activity counselling with PR vs. PR | 8 weeks (mid‐intervention, post‐PR) | ∆ step count (n) (SenseWear) | 63 | median 272 (IQR −342 to 782) | 59 | median 155 (IQR −438 to 867) | P = 0.99* |
| ∆ step count (n) (pedometer) | median 727 (IQR −1493 to 3119) | median 892 (IQR −1187 to 2534) | P = 0.55* | |||||
| ∆ MVPA time | median 11 (IQR −1 to 33) | median 11 (IQR −2 to 28) | P = 0.62* | |||||
| 6 months | ∆ step count (n) (SenseWear) | 56 | median −263 (IQR −778 to 197) | 57 | median −461 (IQR −1168 to −62) | P = 0.09* | ||
| ∆ step count (n) (pedometer) | median 116 (IQR −1698 to 3200) | median 481 (IQR −1931 to 1781) | P = 0.85* | |||||
| ∆ MVPA time | median 2 (IQR −12 to 25) | median 12 (IQR −7 to 31) | P = 0.16* | |||||
| ∆ LIPA time | 44 | median 13 (IQR −38 to 33) | 49 | median 0 (IQR −62 to 36) | P = 0.60* | |||
| ∆ time sedentary | median 2 (IQR −38 to 62) | median 22 (IQR −36 to 81) | P = 0.31 | |||||
| O'Neill 2018 | Physical activity counselling vs. PR | 12 weeks physical activity counselling, 6 weeks PR | ∆ MVPA time | 14 | 7 (−10 to 24) | 12 | 1 (−3 to 5) | 6 (−10 to 22) |
| ∆ MVPA bouts (n) | 0.5 (0.2 to 1.1) | −0.03 (−0.1 to 0.05) | 0.5 (0.3 to 0.8) | |||||
| ∆ MVPA time in bouts | 9 (−4 to 22) | −0.4 (−1 to 1) | 10 (−2 to 21) | |||||
| Orme 2018 | Feedback and education vs. no intervention; Education vs. no intervention; Feedback with education vs. education (post‐admission) | 14 days | ∆ step count (n) | no group data presented | ||||
| "stationary" time | ||||||||
| "light activity" time | ||||||||
| MVPA time | ||||||||
| Ogasawara 2018 | Enriched nutritional supplement with inpatient PR vs. nutritional supplement with inpatient PR | hospital discharge | ∆ step count | 24 | mean 1900 (SD 2110) | 21 | mean 1700 (SD 1694) | 200 (−913 to 1313) |
| ∆ EE (kcal) | mean 1521 (SD 285) | mean 1441 (SD 235) | 80 (−72 to 232) | |||||
| Priori 2017 | Physical activity counselling vs. no intervention | 4 weeks (mid intervention) | % ∆ MPA time | 10 | mean 19 (SD 30) | 8 | mean −5 (SD 13) | 2 (4 to 45) |
| 8 weeks | mean 20 (SD 29) | mean −12 (SD 22) | 32 (8 to 55) | |||||
| Probst 2011 | Exercise training (callisthenics) vs. exercise training (endurance and strength training) | 12 weeks (data from graph) | step count (n) | 20 | mean 4235 (SD 822) | 20 | mean 4198 (SD 680) | "There were no significant inter‐group differences in any variable"* |
| time walking | mean 43 (SD 26) | mean 53 (SD 39) | ||||||
| time standing | mean 231 (SD 123) | mean 243 (SD 106) | ||||||
| time sitting | mean 334 (SD 126) | mean 318 (SD 108) | ||||||
| time lying | mean 115 (SD 89) | mean 100 (SD 78) | ||||||
| MVPA time | mean 55 (SD 15) | mean 75 (SD 19) | ||||||
| active EE (kcal) | mean 335 (SD 104) | mean 389 (SD 119) | ||||||
| total EE (kcal) | mean 1362 (SD 186) | mean 1318 (SD 113) | ||||||
| Saini 2017 | Physical activity counselling vs. no intervention | 8 weeks (total n = 28) | % ∆ MPA time | x | mean −9 (SD 24) | x | mean −21 (SD 21) | P = 0.116* |
| Sandland 2008 | Supplemental oxygen vs. placebo (air) | 8 weeks | % ∆ "domestic activity counts" | 10 | mean 7 (SD 54) | 10 | mean −8 (SD 19) | 15 (−21 to 51) |
| Sena 2013 | Exercise training (eccentric cycle training) vs. exercise training (concentric cycle training) |
10 weeks | "physical activity levels" | 8 | x | 8 | x | "unchanged"* |
| Singh 1998 | Aware of purpose of pedometer with PR vs. unaware of purpose of pedometer with PR | 7 days | step count (n) | 10 | mean 4098 | 9 | mean 3679 | MD 419 "no significant difference between groups"* |
| Steele 2019 | Adherence intervention vs. PR | 6 months (follow‐up) | step count (n) | 32 | mean 5045 (SD 3147) | 31 | mean 5204 (SD 3261) | −159 (−1742 to 1424) |
| peak performance | mean 56 (SD 19) | mean 56 (SD 19) | 0 (−9 to 9) | |||||
| time inactive (%) | mean 68 (SD 15) | mean 70 (SD 13) | −2 (−9 to 5) | |||||
| Tabak 2014a | Physical activity counselling with optional supervised exercise vs. optional supervised exercise | 4 weeks | step count (n) | 13 | mean 5603 (SD 3475) | 16 | mean 4617 (SD 3460) | 986 (−1553 to 3525) |
| Tahirah 2015 | Exercise training (progressive walking and functional‐resistance exercises) vs. no intervention (inpatient) | hospital discharge | step count (n) | 17 | median 4215 (IQR 2133 to 6693) | 17 | median 2198 (IQR 1242 to 4857) | P = 0.07** |
| Troosters 2014 | LAMA with behavioural management vs. placebo with behavioural management | 6 months | step count (n) | 221 | mean 6485 | 205 | mean 6122 | x |
| MVPA time | mean 72 | mean 64 | MD 8 | |||||
| LIPA time | mean 111 (SD 82) | mean 101 (SD 80) | 10 (−6 to 26) | |||||
| inactive (%) (< 6000 steps per day) | mean 40 | mean 43 | OR 0.86 (95% CI 0.57 to 1.30) P = 0.477* | |||||
| Tsai 2016 | PR (telerehabilitation) vs. no intervention | 8 weeks | ∆ PAL | 19 | −0.03 (−0.1 to 0.02) | 17 | −0.02 (−0.1 to 0.1) | 0.08 (−0.1 to 0.1) |
| Vasilopoulou 2017 | Maintenance (telerehabilitation) following HIIT vs. no intervention | 12 months (data from graph) | time sedentary | 47 | mean 584 (SD 98) | 50 | mean 615 (SD 76) | −31 (−66 to 4) |
| LIPA time | mean 157 (SD 44) | mean 113 (SD 44) | 44 (27 to 62) | |||||
| MPA time | mean 18 (SD 6) | mean 11 (SD 7) | 7 (4 to 10) | |||||
| "lifestyle" physical activity time | mean 41 (SD 16) | mean 34 (SD 16) | 7 (1 to 13) | |||||
| Maintenance (centre‐based) following HIIT vs. no intervention | time sedentary | 50 | mean 551 (SD 83) | 50 | 615 (SD 76) | −64 (−95 to −33) | ||
| LIPA time | mean 159 (SD 43) | 113 (SD 44) | 46 (29 to 63) | |||||
| MPA time | mean 22 (SD 7) | 11 (SD 7) | 11 (8 to 14) | |||||
| "lifestyle" physical activity time | mean 52 (SD 17) | 34 (SD 16) | 18 (12 to 25) | |||||
| Maintenance (telerehabilitation) vs. maintenance (centre‐based) following HIIT | time sedentary | 47 | mean 584 (SD 98) | 50 | mean 551 (SD 83) | 33 (−3 to 69) | ||
| LIPA time | mean 157 (SD 44) | mean 159 (SD 43) | −2 (−19 to 15) | |||||
| MPA time | mean 18 (SD 6) | mean 22 (SD 7) | −4 (−7 to −1) | |||||
| "lifestyle" physical activity time | mean 41 (SD 16) | mean 52 (SD 17) | −11 (−18 to −4) | |||||
| Watz 2017 | LAMA/LABA vs. placebo | 4 weeks | inactive (%) (< 6000 steps per day) | 127 | mean 41 | 123 | mean 55 | OR 0.27 (95% CI 0.1 to 0.5)* |
| Widyastuti 2018 | Physical activity counselling vs. PR | 6 weeks | step count (n) | 18 | mean 6021 (SD 2549) | 18 | mean 6113 (SD 2403) | −92 (−1710 to 1526) |
| Wootton 2017 | Ground‐based walking vs. no intervention | 8 weeks | time sedentary (% awake time) | 62 | mean 69 (SD 10) | 39 | mean 68 (SD 10) | −2 (−6 to 2)* |
| LIPA time (% awake time) | mean 25 (SD 7) | mean 25 (SD 7) | 1 (−2 to 4)* | |||||
| MPA time (% awake time) | mean 7 (SD 5) | mean 7 (SD 5) | 1 (−2 to 4)* | |||||
| VPA time (% awake time) | mean 0 (SD 0) | mean 0 (SD 0) | 0 (0 to 0)* | |||||
| Physical activity counselling with pedometer vs. no intervention (following ground‐based walking training) | 12 months | ∆ total EE (kcal) | 23 | −75 (−156 to 6) | 20 | −80 (−166 to 5) | 17 (−131 to 164)* | |
| ∆ step count (n) | −157 (−753 to 439) | −1051 (−1687 to −424) | −617 (−1669 to 453)* | |||||
| ∆ time sedentary | −9 (−34 to 17) | −13 (−40 to 14) | −8 (−50 to 33)* | |||||
| ∆ LIPA time | 8 (−19 to 35) | −16 (−44 to 13) | −27 (−70 to 14)* | |||||
| ∆ MPA time | −11 (−23 to 1) | −1 (−13 to 12) | 20 (−1 to 41)* | |||||
| ∆VPA time | 0 (−1 to 1) | 0 (−1 to 1) | 0 (0 to 1)* | |||||
* from paper ** from author x data not provided Data are per day unless indicated
ACE: angiotensin‐converting enzyme; ∆ change from baseline; cpm: counts per minute; "daily physical activity": step count + metabolic equivalents; EE: energy expenditure; ICS: inhaled corticosteroid; LABA: long‐acting beta2 agonist; LAMA: long‐acting muscarinic antagonist; LIPA: light‐intensity physical activity; MD: mean difference; METs: metabolic equivalents; MPA: moderate‐intensity physical activity; MVPA: moderate‐to‐vigorous intensity physical activity; n: number of participants; OR: odds ratio; PAL: physical activity level; PR: pulmonary rehabilitation; SPACE: self‐management programme of activity, coping and education; SD: standard deviation; VPA: vigorous‐intensity physical activity
Summary of findings 2. Comparison of types of pulmonary rehabilitation/exercise training.
|
Population: people with COPD, clinical stability Intervention: pulmonary rehabilitation/exercise training Comparisons: intervention vs. another intervention Outcome: time in physical activity (of at least moderate intensity) at end intervention | ||||||
| Interventions | Outcome | Illustrative comparative risks* [mean difference (95% CI) unless indicated] | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Comparator | Intervention of interest | |||||
| Home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation (8 weeks) |
Change in time in MVPA | The mean change in time in the centre‐based group was 5 minutes per day | The mean difference was 6 (−19 to 31) minutes per day | 58 participants (1 study; Analysis 4.2) | ⊕⊕⊝⊝ lowa | Baseline values: centre‐based median 79 (IQR 24 to 136), home‐based median 68 (IQR 29 to 121) |
| Calisthenics vs. exercise training (12 weeks) |
Time in MVPA | The mean time in the exercise training group was 75 minutes per day | "no significant inter‐group differences in any variable" | 40 participants (1 study; Probst 2011; Table 2) | ⊕⊕⊝⊝ lowb | ‐ |
| Physical activity counselling vs. pulmonary rehabilitation (6 to 12 weeks) |
Change in time in MVPA | The mean change in time in the pulmonary rehabilitation group was 1 (−3 to 5) minutes per day | The mean difference was 6 (−10 to 22) minutes per day | 26 participants (1 study; O'Neill 2018; Table 2) | ⊕⊕⊝⊝ lowa | Baseline values: pulmonary rehabilitation mean 15 (SD 5), physical activity counselling mean 14 (SD 15) |
| Telerehabilitation maintenance programme vs. centre‐based maintenance programme (following high‐intensity interval training, 12 months) |
Time in moderate‐intensity physical activity | The mean time in the centre‐based group was 22 minutes per day | The mean difference was −4 (−7 to −1) minutes per day | 97 participants (1 study; Vasilopoulou 2017; Table 2) | ⊕⊕⊕⊝ moderatec |
‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; IQR: interquartile range; MVPA: moderate‐to‐vigorous physical activity; SD: standard deviation | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
aDowngraded one level for high risk of performance bias. Downgraded one level for imprecision as CI does not exclude possibility of no effect.
bDowngraded one level for unclear risk of selection, performance, detection, attrition and other potential bias. Downgraded one level for imprecision as CI does not exclude possibility of no effect. cDowngraded one level for high risk of performance bias.
4.2. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 2 change in time in moderate‐to‐vigorous intensity physical activity (minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
Summary of findings 3. Physical activity counselling.
|
Population: people with COPD, clinical stability Intervention: physical activity counselling Comparisons: intervention vs. no intervention, intervention in addition to a standard intervention common to both groups Outcome: time in physical activity (of at least moderate intensity) at end intervention | ||||||
| Interventions | Outcome | Illustrative comparative risks* [mean difference (95% CI) unless indicated] | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Comparator | Intervention of interest | |||||
| Comparison: intervention vs. no intervention | ||||||
| Physical activity counselling vs. no intervention (12 weeks) |
Change in time in MVPA | The mean change in time was −3 (−0.6 to 0.2) minutes per day | The mean difference was 11 (7 to 15) minutes per day | 280 participants (1 study; Demeyer 2017; Table 2) | ⊕⊕⊕⊝ moderatea |
Baseline values: no intervention median 15 (IQR 5 to 35), intervention median 14 (IQR 5 to 26) |
| Physical activity counselling vs. no intervention (following pulmonary rehabilitation, 12 months) |
Change in time in moderate intensity physical activity | The mean change was −1 (−13 to 12) minutes per day | The mean difference was 20 (−1 to 41) minutes per day | 43 participants (1 study; Wootton 2017; Table 2) | ⊕⊕⊝⊝ lowb | Baseline values: no intervention mean 51 (SD 49), intervention mean 59 (SD 52) |
| Comparison: intervention in addition to a standard intervention common to both groups | ||||||
| Physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation (6 months) |
Time in MVPA | The mean time in the pulmonary rehabilitation group was 28 minutes per day | The mean difference was 24 (2 to 45) minutes per day | 26 participants (1 study; Analysis 3.21) | ⊕⊕⊕⊝ moderatec |
P = 0.03 |
| Change in time in MVPA | The median change in time in the pulmonary rehabilitation group was 12 minutes per day | The median change in time was 2 (−12 to 25) minutes per day | 113 participants (1 study; Nolan 2017; Table 2) | ⊕⊕⊝⊝ lowd | P = 0.16 Baseline values: no intervention median 47 (IQR 18 to 103), intervention median 45 (IQR 20 to 81) |
|
| Physical activity counselling with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation (6 months) |
Change in time in MVPA | The mean change in time in the pulmonary rehabilitation group was 0 minutes per day | The mean difference was −6 (−16 to 3) minutes per day | 50 participants (1 study; Analysis 3.25) | ⊕⊝⊝⊝ very lowe | Baseline values: no intervention median 29 (IQR 17 to 44), intervention median 33 (IQR 16 to 47) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; IQR: interquartile range; MVPA: moderate‐to‐vigorous physical activity; SD: standard deviation | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
aDowngraded one level for high risk of performance bias and detection bias. bDowngraded one level for high risk of performance bias. Downgraded one level for imprecision as CI does not exclude possibility of no effect. cDowngraded one level for high risk of performance, detection and reporting bias. dDowngraded one level for high risk of performance bias. Downgraded one level for imprecision as results do not exclude possibility of no effect. eDowngraded one level for unclear risk of selection, reporting and other bias. Downgraded one level for imprecision as CI does not exclude possibility of no effect.
3.21. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 21 time in moderate‐to‐vigorous intensity physical activity (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
3.25. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 25 change in time in moderate‐to‐vigorous intensity physical activity (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
Summary of findings 4. Self‐management.
|
Population: people with COPD, clinical stability Intervention: self‐management Comparisons: intervention vs. no intervention, intervention in addition to a standard intervention common to both groups, intervention vs. another intervention Outcome: time in physical activity (of at least moderate intensity) at end intervention | ||||||
| Interventions | Outcome | Illustrative comparative risks* [mean difference (95% CI) unless indicated] | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Comparator | Intervention of interest | |||||
| Comparison: intervention vs. no intervention | ||||||
| Self‐management vs. no intervention (12 months) |
Time in MVPA | The mean time was 316 minutes a week | The mean difference was 12 (−21 to 45) minutes a week | 411 participants (1 study; Jolly 2018; Table 2) | ⊕⊕⊝⊝ lowa | P = 0.48 |
| Comparison: intervention in addition to a standard intervention common to both groups | ||||||
| Self‐efficacy training with upper limb exercise vs. education with upper limb exercise (16 weeks) |
Time in moderate‐intensity physical activity | The mean time in the education and upper‐limb exercise group was 4 minutes per day | The mean difference was 2 (−1 to 5) minutes per day | 35 participants (1 study; Larson 2014; Table 2) |
⊕⊕⊝⊝ lowa | ‐ |
| Comparison: intervention vs. another intervention | ||||||
| Self‐management vs. education and symptom monitoring (16 weeks) |
Time in moderate‐intensity physical activity | The mean time in the self‐management group was 6 minutes per day | The mean difference was 1 (−1 to 2) minutes per day | 326 participants (1 study; Blumenthal 2014; Table 2) | ⊕⊕⊝⊝ lowa | ‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MVPA: moderate‐to‐vigorous physical activity | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
aDowngraded one level for high risk of performance bias. Downgraded one level for imprecision as CI does not exclude possibility of no effect.
Summary of findings 5. Pharmacological interventions.
|
Population: people with COPD, clinical stability Intervention: pharmacological interventions Comparisons: intervention vs. placebo, intervention in addition to a standard intervention common to both groups Outcome: time in physical activity (of at least moderate intensity) at end intervention | ||||||
| Interventions | Outcome | Illustrative comparative risks* [mean difference (95% CI) unless indicated] | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Comparator | Intervention of interest | |||||
| Comparison: intervention vs. sham/placebo intervention | ||||||
| LAMA vs. placebo (3 weeks) |
Change in time in MVPA | The median change in time was −6 minutes per day | The median change in time was −1 (IQR −17 to 24) minutes per day | 131 participants (2 studies; Beeh 2014; Magnussen 2017; Table 2) | ⊕⊕⊕⊝ moderatea |
P = 0.07 Baseline values: Beeh 2014 placebo median 73 (IQR 38 to 135), LAMA median 74 (IQR 32 to 132) Magnussen 2017 placebo mean 88 (SD 65), intervention mean 57 (SD 32) |
| LAMA/LABA vs. placebo (3 to 4 weeks) |
Change in time in MVPA | The mean change in time ranged from −16 to −1 minutes per day | The mean difference was 10 (4 to 15) minutes per day | 423 participants (2 studies; Analysis 2.3) | ⊕⊕⊕⊕ high |
Baseline values: Watz 2016 placebo mean 130, LAMA/LABA mean 125 |
| Comparison: intervention in addition to a standard intervention common to both groups | ||||||
| LAMA with behaviour modification vs. placebo with behaviour modification (12 weeks to 6 months) |
Time in MVPA | The mean time was 64 minutes per day | The mean difference was 8 minutes per day | 426 participants (1 study; Troosters 2014; Table 2) | ⊕⊕⊕⊝ moderateb |
P = "not statistically significantly different" |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; IQR: interquartile range; LABA: long‐acting beta2 agonist; LAMA: long‐acting muscarinic antagonist; MVPA: moderate‐to‐vigorous physical activity; SD: standard deviation | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
aDowngraded one level for imprecision as results do not exclude possibility of no effect. bDowngraded one level for imprecision as no formal analysis of difference presented.
2.3. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 3 change in time in moderate‐to‐vigorous intensity physical activity (minutes per day): Intervention: LAMA/LABA.
Background
Description of the condition
Chronic obstructive pulmonary disease (COPD) is a common, treatable but incurable obstructive lung disease defined by persistent airflow limitation. Diagnosis is confirmed by spirometry in the clinical context of a person presenting with dyspnoea, chronic cough or sputum production, and a history of risk factor exposure (GOLD 2019). Development of COPD is primarily attributable to an enhanced chronic inflammatory airway response to noxious particles or gases, and is strongly linked to a history of smoking. However, there are a number of other risk factors including exposure to air pollution, occupational exposures, genetics, chronic asthma, history of severe childhood respiratory infections and low socioeconomic status (GOLD 2019). Systemic effects, including systemic inflammation and muscle dysfunction, and comorbid conditions, including cardiovascular disease, anxiety and depression, are commonly associated with COPD (Choudhury 2014). Prevalence studies suggest that COPD affects upwards of 384 million people (Adeloye 2015) and is the third leading cause of death worldwide (WHO 2017). Associated with advancing age (Anton 2016), and in the context of the fastest rate of population growth occurring in people over 65 years of age (UN 2015), COPD poses a substantial and growing economic and social burden globally (GOLD 2019).
Description of the intervention
We define the term ‘physical activity’ as any bodily movement produced by skeletal muscles that results in energy expenditure (Casperson 1985). It is a complex behaviour traditionally described according to type, intensity and duration, and incorporates a subset of undertakings including exercise, occupational and household activities. Public health promotion for regular participation in physical activity typically recommends a minimum of 150 minutes a week of at least moderate‐intensity activity as ‘sufficient’ for health benefits across the adult population (U.S. Department of Health and Human Services 2018). These benefits include reduced risk of all‐cause mortality, coronary heart disease, hypertension, stroke, metabolic syndrome, type 2 diabetes and depression (Lee 2012).
Participation in regular physical activity is also endorsed for people with COPD (GOLD 2019). Low levels of physical activity are one of the main risk factors for development of cardiovascular, metabolic and musculoskeletal comorbid conditions in people with COPD, and is observed across the disease spectrum (Van Remoortel 2014). Recent studies show that physical activity is reduced in smokers prior to diagnosis (Furlanetto 2014) and in people with a recent diagnosis and mild COPD before symptom onset (Johnson‐Warrington 2014). Physical activity participation is not clearly related to other clinical characteristics including impaired exercise capacity (Fastenau 2013; Gagnon 2015; Van Remoortel 2013; Watz 2009), but is reduced compared to healthy peers (Pitta 2005; Vorrink 2011) and to people with other chronic conditions (Arne 2009). It is further compromised during and after hospitalisation for an acute exacerbation (Pitta 2006a) and with increasing disease severity (Shrikrishna 2012; Troosters 2010; Waschki 2015). In people with COPD, low levels of participation in physical activity have been independently associated with poor outcomes, including increased risks of hospitalisation and mortality (Garcia‐Aymerich 2006; Garcia‐Rio 2012; Vaes 2014; Waschki 2011).
Much attention has been given to the development of physical activity interventions that incorporate strategies specifically designed to promote the adoption and maintenance of active lifestyles in the general population (Marcus 2006). Such interventions may be provided by a broad range of healthcare professionals and be delivered in a variety of ways (for example, in person, by internet or telephone).
How the intervention might work
Evidence suggests that people with COPD avoid participation in physical activity due to the perception of breathlessness, resulting from inefficiencies related to gas trapping and lung hyperinflation. A vicious circle is perpetuated, where muscle deconditioning results from avoiding activities that involve physical exertion and exacerbate symptoms, further compromising physical capacity to engage in activity (O’Donnell 2014). It is theorised that targeted interventions may be able to interrupt this cycle and increase participation in physical activity at a range of intensities that are associated with health benefits. The dual role of low physical activity levels as both a cause and consequence in chronic disease identifies physical activity as a potentially modifiable target that could affect health‐related quality of life and disease trajectory (Esteban 2010; Vaes 2014; Watz 2014a). Whether improvements in physical activity can ameliorate these effects in COPD is unknown.
Many physical and physiological disease features also appear to influence participation in physical activity by people with COPD. However, the quality of association between such features, including lung function, systemic inflammation, body composition, comorbidities and psychosocial factors, and physical activity participation is variable (Gimeno‐Santos 2011). Additional considerations, including fatigue (Andersson 2015), balance (Iwakura 2016), and seasonal and environmental factors (Alahmari 2015; Sewell 2010) may also impact on physical activity participation in this group. The broad range of strategies considered to date to address low levels of physical activity in people with COPD (for instance, exercise training, nutritional interventions and behavioural strategies) reflect the complexity of this issue.
There is evidence for a relationship between physical activity and rate of acute exacerbations (Esteban 2014) and therefore targeting improvements in physical activity in people with COPD may be an important therapeutic goal (Langer 2016; Singh 2016). However, achieving consistent improvements in participation and convincing evidence for the positive impact on health outcomes remain elusive.
Why it is important to do this review
Escalating awareness of the magnitude of the challenge posed by low levels of physical activity in people with COPD at all points in the disease course highlights the need for interventions to increase physical activity participation by people with COPD. The widely‐accepted benefits of physical activity, coupled with the increasing availability of wearable monitoring devices to objectively measure participation, has led to a dramatic rise in the number and variety of studies that aim to improve physical activity levels in people with COPD. However, little is known about the range of interventions tested so far, partly attributable to the complexities of data analysis and the challenge of rapidly evolving technology, and the relationship between effects on physical activity and other outcomes including exercise capacity and health‐related quality of life. This Cochrane Review aims to evaluate the efficacy of existing interventions to increase physical activity in people with COPD, and to signpost directions for future work.
Objectives
In people with COPD, which interventions are effective at improving objectively‐assessed physical activity?
Methods
Criteria for considering studies for this review
Types of studies
We include randomised controlled trials (RCTs) of any intervention where objectively‐assessed physical activity or sedentary behaviour was a measured outcome in people with COPD, as previous consensus statements (Watz 2014a) and systematic reviews (Dhillon 2015; Gimeno‐Santos 2011) have failed to identify subjective tools that accurately reflect this in people with COPD.
We include studies reported as full‐text articles, those published as abstract only and unpublished data. Physical activity could be either a primary or a secondary outcome of the study. We include cross‐over trials where pre‐cross‐over data were available from study authors.
Types of participants
We include adults (18 years of age and over) with a diagnosis of COPD according to established criteria, regardless of disease severity. We planned to include studies that incorporated a mix of diagnostic groups, only if we could obtain data on any of the review outcomes separately for people with COPD.
Types of interventions
We include trials that objectively assessed physical activity as an outcome. These trials compared an intervention versus no intervention or a sham/placebo intervention, compared an intervention in addition to another standard intervention common to both groups or to a different intervention. Interventions could be supervised or unsupervised. Interventions could include, but were not limited to, physical activity counselling, education programmes and self‐management strategies. Studies including exercise training undertaken as a stand‐alone intervention or as part of a comprehensive pulmonary rehabilitation programme incorporating other components targeting chronic disease self‐management (Hill 2013) were considered together. We analysed studies that included pulmonary rehabilitation (as defined by authors) separately from studies that did not include pulmonary rehabilitation. We also included studies in which both groups received pulmonary rehabilitation and which assessed the inclusion of an additional specific physical activity intervention in one group.
Comparisons
One or more interventions versus no intervention
One or more interventions versus sham/placebo intervention
One or more interventions in addition to a standard intervention common to both groups
One or more interventions versus a different intervention
Types of outcome measures
Primary outcomes
Studies had to include variable(s) that reflected participation in physical activity or sedentary behaviour, as measured objectively using a pedometer, accelerometer or activity monitor. Outcomes of interest included but were not limited to step count, activity counts, energy expenditure and physical activity time (different intensities, range of thresholds used). Primary time points were at baseline (prior to start) and at the time of intervention completion; we used change in physical activity from baseline for analysis where possible. We also categorised any follow‐up measurements reported following intervention completion as either short‐term (within one month), medium‐term (between one and six months) or long‐term (longer than six months). We sought raw data from the study authors where possible to facilitate comparisons.
Secondary outcomes
Health‐related quality of life (measured using either a generic or disease‐specific tool)
Exercise capacity: measured using a laboratory or field exercise test, e.g. cardiopulmonary exercise test, six‐minute walk test (6MWT)
Adverse events, e.g. musculoskeletal injury
Adherence to intervention
Search methods for identification of studies
Electronic searches
We identified studies from the Cochrane Airways Trials Register, which is maintained by the Information Specialist for the Group. The Cochrane Airways Trials Register contains studies identified from several sources:
Monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL), through the Cochrane Register of Studies Online (crso.cochrane.org);
Weekly searches of MEDLINE Ovid SP 1946 to June 2019;
Weekly searches of Embase Ovid SP 1974 to June 2019;
Monthly searches of PsycINFO Ovid SP 1967 to June 2019;
Monthly searches of Cumulative Index to Nursing and Allied Health Literature (CINAHL EBSCO), 1937 to June 2019;
Monthly searches of Allied and Complementary Medicine (AMED EBSCO), all years to June 2019;
Handsearches of the proceedings of major respiratory conferences.
Studies contained in the Trials Register are identified through search strategies based on the scope of Cochrane Airways. Details of these strategies, as well as a list of handsearched conference proceedings, are in Appendix 1. See Appendix 2 and Appendix 3 for search terms used to identify studies for this review.
We also searched Physiotherapy Evidence Database (PEDro), www.clinicaltrials.gov, the WHO ICTRP portal (www.who.int/ictrp/en/) and the Australian New Zealand Clinical Trials Registry (www.anzctr.org.au/). We searched all databases from their inception to June 2019, and imposed no restriction on language of publication.
Searching other resources
We checked reference lists of all primary studies and review articles for additional references. We searched relevant manufacturers' websites for trial information.
We searched for errata or retractions from included studies published in full text on PubMed (www.ncbi.nlm.nih.gov/pubmed) on 12 July 2019.
Data collection and analysis
Selection of studies
Two review authors (AB and NC) independently screened titles and abstracts for inclusion of all the potentially eligible studies we identified from the search, and coded them as either 'retrieve' (eligible or potentially eligible/unclear) or 'do not retrieve'. We retrieved the full‐text study reports/publications and two review authors (AB and NC) independently screened the full‐text articles and identified studies for inclusion, recording reasons for exclusion of the ineligible studies. We resolved any disagreement through discussion or, if required, we consulted a third review author (AH). We identified and excluded duplicates and collated multiple reports of the same study so that each study rather than each report was the unit of interest in the review. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram and Characteristics of excluded studies tables (Moher 2009).
Data extraction and management
We used a data collection form that was piloted on at least one study included in the review, to record study characteristics and outcome data. Two review authors (AB and NC) independently extracted the following study characteristics from included studies:
Methods: study design, duration of study, study locations, study setting, date of study;
Participants: number, mean age, age range, gender, severity of condition, diagnostic criteria, baseline lung function, smoking history, inclusion criteria, exclusion criteria, withdrawals;
Interventions: intervention, comparison, concomitant interventions;
Measurement tool;
Outcomes: primary and secondary outcomes specified and collected (at baseline and at the time of intervention completion) and follow‐up measurements at any other time points noted;
Notes: funding for trial, declared conflicts of interest by trial authors.
We resolved disagreements by reaching consensus, or by involving a third review author (AH or MA). We noted in the Characteristics of included studies table if the included studies did not report outcome data in a useable way. We contacted study authors to verify extracted data when necessary and we provided details of missing data when possible. One review author (AB) transferred data into the Review Manager 5 (RevMan 5) file (Review Manager 2014). We double‐checked that the review author had entered data correctly by comparing data presented in the systematic review with data provided in the study reports. A second review author (NC) spot‐checked study characteristics for accuracy against the trial report.
Where meta‐analyses of physical activity outcome were possible, we included figures in the review.
Assessment of risk of bias in included studies
Two review authors (AB and NC) independently assessed risks of bias for each included RCT, using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017). We resolved disagreements by discussion or by involving another review author (AH or MA). Where conflicts of interest were present, an independent co‐author conducted the assessment. We assessed risks of bias according to the following domains:
Random sequence generation;
Allocation concealment;
Blinding of participants and personnel;
Blinding of outcome assessment;
Incomplete outcome data;
Selective outcome reporting;
Other potential bias.
For the 'blinding of outcome assessment' domain, we rated both primary and secondary outcomes as ‘objective’ for objectively‐measured outcomes and ‘other’ for those outcomes with greater potential to be affected by lack of blinding (e.g. quality of life questionnaires).
We graded each potential source of bias as either high, low or unclear, and provided an extract from the study report together with a justification for our judgement. We resolved discrepancies by consensus. We summarised the 'Risk of bias' judgements across different studies for each of the domains listed and summarised results in a ’Risk of bias' table. When considering treatment effects, we took into account the risks of bias for studies that contributed to this outcome.
Assessment of bias in conducting the systematic review
We conducted the review according to this published protocol and have reported any deviations from it in the Differences between protocol and review section of the review.
Measures of treatment effect
We analysed all the data reported for each outcome, irrespective of dropout rate or use of intention‐to‐treat analysis.
We undertook meta‐analyses only when this was meaningful, i.e. if treatments, participants and the underlying clinical question were similar enough for pooling to make clinical sense.
We intended to analyse dichotomous data as odds ratios (ORs) and 95% confidence intervals (CIs) but no data were available. For continuous data we calculated mean differences (MDs: same metric scale). To retain the units of measurement, we did not express any data as standardised mean differences (SMDs: different metric scales) with 95% CIs. We narratively described skewed data reported as medians and interquartile ranges.
Where multiple arms were reported in a single trial, we included only the relevant arms. We had intended to halve the control group to avoid double‐counting in the event that we combined two comparisons (e.g. drug A versus placebo and drug B versus placebo) in the same meta‐analysis, but this approach was not required.
Unit of analysis issues
Where studies randomly allocated individual participants to study groups, we considered the participant as the unit of analysis. We only included cross‐over trials where data were available prior to cross‐over, due to the potential carry‐over effects of behavioural interventions. We had intended to consider the cluster as the unit of analysis for cluster‐randomised studies, but this approach was not required.
Dealing with missing data
In the event of missing data, we contacted investigators or study sponsors to verify key study characteristics and to obtain missing numerical outcome data when possible, e.g. when a study was reported only as an abstract. If this was not possible, we had intended to analyse the impact of including studies with missing data that may be related to the intervention by performing a sensitivity analysis, but this approach was not required.
Assessment of heterogeneity
We used the I2 statistic to measure heterogeneity among the trials in each analysis. Where we identified it, we considered statistical heterogeneity to be substantial if I2 was greater than 50% (Deeks 2017), and explored possible causes using prespecified subgroup analyses.
Assessment of reporting biases
We had intended to create a funnel plot to explore possible small‐study and publication biases if we could pool more than 10 included trials, but this was not possible.
Data synthesis
We performed a pooled quantitative synthesis where the trials were clinically homogeneous. We pooled data using a random‐effects model to incorporate between‐study heterogeneity into the meta‐analysis. Where the trials were clinically heterogeneous, we performed a narrative synthesis. For instance, we analysed data for different types of interventions separately, and data for studies starting in the period following acute exacerbation separately from those in stable disease.
'Summary of findings' table
We created 'Summary of findings' tables using the following outcomes:
time spent in moderate or moderate‐to‐vigorous physical activity at end intervention in participants with clinically‐stable COPD.
We used the five Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of a body of evidence as it related to studies that contributed data to the meta‐analyses for prespecified outcomes. We used methods and recommendations described in Section 8.5 (Higgins 2017) and Chapter 12 (Schünemann 2017) of the Cochrane Handbook for Systematic Reviews of Interventions, and we used the GRADEpro Guideline Development Tool software (GRADEpro GDT 2014). We justified all decisions to downgrade or upgrade the quality of the evidence using footnotes, and we provide comments to aid the reader's understanding of the review where necessary. We did not include data from studies published only in abstract form or on clinical trial registries, due to inadequate assessment of risks of bias.
Subgroup analysis and investigation of heterogeneity
We planned to perform the following subgroup analyses.
Duration of intervention (≤ 3 months versus > 3 months);
Supervision of intervention (yes or no);
Disease severity (mild disease, defined as forced expiratory volume in one second (FEV1) % predicted ≥ 80%, forced expiratory ratio (FER) < 0.7, compared with other classifications).
We used physical activity as the outcome for subgroup analyses.
We used the formal test for subgroup interactions in Review Manager 5 (RevMan 5) (Review Manager 2014).
Sensitivity analysis
We examined the effects of methodological quality on the pooled estimate by removing studies that were at high or unclear risk of bias for the domains of blinding and incomplete outcome data. We had also intended to examine the effects of measurement device on the pooled estimate by removing studies that used pedometers, as previous studies suggest that these might be less accurate in detecting steps in people with COPD (Pitta 2006b).
Results
Description of studies
Details are available in the Characteristics of included studies and Characteristics of excluded studies tables.
Results of the search
The search yielded 3233 citations and ended with 76 studies included from 179 citations. These included 12 abstracts (see Figure 1).
1.

Study flow diagram.
Eighty‐four studies are currently underway and pending study completion/publication (see Ongoing studies).
Included studies
Of the 76 studies included, 24 studies compared an intervention to promote physical activity versus no intervention (comparison 1). These included pulmonary rehabilitation/exercise training (Borges 2014; De Roos 2017; Egan 2010; Louvaris 2016, Tahirah 2015; Tsai 2016; Vasilopoulou 2017; Wootton 2017), physical activity counselling (Altenburg 2015; Arbillaga‐Etxarri 2018; Demeyer 2017; Hornikx 2015; Hospes 2009; Orme 2018; Priori 2017; Saini 2017; Wootton 2017), self‐management (Jolly 2018; Kanabar 2015; Mitchell 2013; Tabak 2014b), nutritional supplementation (Goris 2003), gait aid (Ng 2015) and endobronchial valve surgery (Hartman 2016).
There were 10 studies that compared an intervention to promote physical activity to sham/placebo (comparison 2). These included self‐management (Schuz 2015), pharmaceutical interventions (Beeh 2014;Magnussen 2017;NCT00144326; Watz 2016;Watz 2017), nutritional supplementation (Dal Negro 2012), supplemental oxygen (Sandland 2008), singing (Lord 2012) and neuromuscular electrical stimulation (Maddocks 2016).
There were 31 studies that compared an intervention to promote physical activity in addition to an intervention common to both groups (comparison 3). These included pulmonary rehabilitation/exercise training (Breyer 2010; Effing 2011; Larson 2014; Troosters 2018; Varas 2018), physical activity counselling (Altenburg 2015; Bender 2016; Cruz 2016; De Blok 2006; Kawagoshi 2015; Loeckx 2018; Mantoani 2018; Mendoza 2015; Moy 2015a; Nguyen 2009; Nolan 2017; Orme 2018; Singh 1998; Tabak 2014a; Vorrink 2016; Wan 2017), self‐management (Benzo 2016; Larson 2014), pharmaceutical interventions (Curtis 2016; Troosters 2014; Troosters 2018), nutritional supplementation (Ogasawara 2018; Van de Bool 2017) supplemental oxygen (Alison 2019), non‐invasive ventilation (Duiverman 2008) and inspiratory muscle training (Charususin 2018).
Sixteen studies compared two interventions to increase physical activity with each other (comparison 4). These studies included alternative models of or alternatives to pulmonary rehabilitation/exercise training (Chaplin 2017; Felcar 2018; Gamper 2019; Holland 2017; O'Neill 2018; Polkey 2018; Probst 2011; Rinaldo 2017; Sena 2013; Steele 2019; Vasilopoulou 2017; Widyastuti 2018), self‐management (Blumenthal 2014), pharmaceutical interventions (Nakamura 2016; NCT01351792) and a lightweight cylinder for supplemental oxygen (Casaburi 2012).
Of studies with more than two groups, four contributed to more than one comparison (Altenburg 2015; Larson 2014; Orme 2018; Vasilopoulou 2017).
The total number of participants involved in the included studies was 8018. The sample sizes ranged from eight participants (Nguyen 2009; Priori 2017; Sena 2013) to 289 participants (Jolly 2018). The mean age of participants was 66 years and mean FEV1 54% predicted. On average, groups comprised 63% men, but details relating to the sex of participants were not reported in four abstracts (Egan 2010; Nakamura 2016; Priori 2017; Sena 2013), three papers (Larson 2014; Lord 2012; Polkey 2018) and two clinical trial registries (NCT00144326; NCT01351792). Interventions were provided in person and by telephone call, smart phone app, website, device or printed information. Study duration ranged from one day (surgical procedure) to 12 months, with follow‐up provided in 11 studies (ranging from seven days to 12 months post‐intervention). Three studies assessed interventions provided during inpatient admissions for acute exacerbation of COPD (AECOPD) and five studies in the post‐admission phase. Of the 76 studies included, 38 had assessed physical activity as a primary outcome. Details are available in the Characteristics of included studies table.
Excluded studies
We excluded most of these 134 studies (n = 84) due to physical activity not being objectively assessed. We report reasons for exclusion in the Characteristics of excluded studies table.
Risk of bias in included studies
Overall, the domains with the highest risks of bias were performance bias, as the method of delivery of some interventions precluded participant blinding, and reporting bias. Domains with the lowest risks of bias were detection bias, as objective assessment of physical activity was an inclusion criterion, and selection bias, as most studies did report the method of random sequence generation (Figure 2).
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
For random sequence generation, 48 studies had a low risk of bias. Insufficient information was available to inform a decision for 17 studies (Bender 2016; Burtin 2015; Casaburi 2012; De Blok 2006; Gamper 2019; Hartman 2016; Hornikx 2015; Hospes 2009; Kawagoshi 2015; Magnussen 2017; Orme 2018; Polkey 2018; Probst 2011; Sandland 2008; Troosters 2014; Watz 2017; Widyastuti 2018), nine abstracts (Egan 2010; Kanabar 2015; Loeckx 2018; Mantoani 2018; Nakamura 2016; Ng 2015; Priori 2017; Saini 2017; Singh 1998) and studies from two clinical trial registries (NCT00144326; NCT01351792).
For allocation concealment, one study was assessed at high risk of bias (Altenburg 2015) and 28 at low risk of bias. Insufficient information was available to inform a decision in 36 studies (Beeh 2014; Bender 2016; Benzo 2016; Blumenthal 2014; Breyer 2010; Casaburi 2012; Curtis 2016; De Blok 2006; Duiverman 2008; Effing 2011; Gamper 2019; Goris 2003; Hartman 2016; Hornikx 2015; Hospes 2009; Kawagoshi 2015; Larson 2014; Magnussen 2017; Mendoza 2015; Moy 2015a; Nolan 2017; Ogasawara 2018; Orme 2018; Polkey 2018; Probst 2011; Rinaldo 2017; Sandland 2008; Steele 2019; Troosters 2014; Tsai 2016; Varas 2018; Vasilopoulou 2017; Vorrink 2016; Watz 2016; Watz 2017; Widyastuti 2018), nine abstracts (Egan 2010; Kanabar 2015; Loeckx 2018; Mantoani 2018; Nakamura 2016; Ng 2015; Priori 2017; Saini 2017; Singh 1998) and studies from two clinical trial registries (NCT00144326; NCT01351792).
Blinding
We assessed performance bias separately for participants and personnel.
Participants
We rated the risk of performance bias as high in 47 studies, in some cases due to the nature of the intervention precluding participant blinding. Most pharmaceutical interventions were able to blind participants and were assessed as being at low risk of performance bias (Beeh 2014; Curtis 2016; Magnussen 2017; NCT01351792; Troosters 2014; Watz 2016; Watz 2017), apart from the high risk assessment for Nakamura 2016 (lack of blinding) and unclear risk for NCT00144326 and Troosters 2018 (insufficient information). Similarly, studies involving nutritional supplementation were also able to blind participants and were assessed at low risk (Dal Negro 2012; Van de Bool 2017), apart from the high risk assessment for Ogasawara 2018 (lack of blinding) and unclear risk for Goris 2003 (insufficient information).
Other studies assessed as low risk were Alison 2019,Burtin 2015,Charususin 2018, Curtis 2016, Larson 2014, Maddocks 2016, Sandland 2008 and Varas 2018. Other studies with unclear risk due to insufficient information were Arbillaga‐Etxarri 2018,Cruz 2016,Loeckx 2018, NCT00144326, Probst 2011,Rinaldo 2017,Saini 2017, Schuz 2015,Sena 2013,Singh 1998, and Tahirah 2015.
Personnel
We judged most studies (n = 45) to be subject to unclear risk due to insufficient information. Studies at low risk (n = 12) included pharmacological interventions (Beeh 2014; Magnussen 2017; NCT01351792; Watz 2016; Watz 2017), supplemental oxygen (Alison 2019; Sandland 2008) and nutritional supplementation (Van de Bool 2017), as well as studies involving an intervention in addition to pulmonary rehabilitation programs (Burtin 2015; Charususin 2018; Nolan 2017) and one physical activity counselling study (De Blok 2006). There were 19 studies assessed at high risk which was primarily attributable to personnel awareness of group allocation during the study (Altenburg 2015; Arbillaga‐Etxarri 2018; Borges 2014; Casaburi 2012; Cruz 2016; Duiverman 2008; Felcar 2018; Gamper 2019; Maddocks 2016; Mantoani 2018; Moy 2015a; Nakamura 2016; Ogasawara 2018; Polkey 2018; Steele 2019; Tabak 2014b; Tahirah 2015; Varas 2018; Vasilopoulou 2017).
We assessed detection bias separately for outcomes that were or were not objectively assessed.
Objective outcomes
In line with the inclusion criteria, all studies objectively assessed physical activity. Most (n = 64) were therefore classified as low risk of detection bias. Studies at unclear risk were Altenburg 2015, Bender 2016, De Blok 2006, Gamper 2019,Loeckx 2018,Ogasawara 2018,Priori 2017, Saini 2017, Tabak 2014a, Tabak 2014b, Varas 2018 and Widyastuti 2018, as there was insufficient information to make an assessment.
Other outcomes
We rated 35 studies at low risk of detection bias (Alison 2019; Arbillaga‐Etxarri 2018; Beeh 2014; Blumenthal 2014; Borges 2014; Burtin 2015; Casaburi 2012; Chaplin 2017; Charususin 2018; Curtis 2016; Felcar 2018; Goris 2003; Jolly 2018; Larson 2014; Louvaris 2016; Magnussen 2017; Mendoza 2015; Mitchell 2013; NCT01351792; Nguyen 2009; Nolan 2017; O'Neill 2018; Priori 2017; Schuz 2015; Sena 2013; Singh 1998; Steele 2019; Tahirah 2015; Troosters 2014; Tsai 2016; Varas 2018; Vorrink 2016; Wan 2017; Watz 2017; Wootton 2017). We judged 12 studies to be at high risk (Altenburg 2015; Cruz 2016; Demeyer 2017; De Roos 2017; Duiverman 2008; Mantoani 2018; Moy 2015a; Orme 2018; Ogasawara 2018; Polkey 2018; Tabak 2014b; Widyastuti 2018), due to lack of assessor blinding. Insufficient information was available to inform a decision on the remaining 29 studies.
Incomplete outcome data
We rated most studies (n = 46) at low risk of attrition bias. We assessed 14 studies (Altenburg 2015; Benzo 2016; Borges 2014; Dal Negro 2012; Duiverman 2008; Felcar 2018; Goris 2003; Jolly 2018; Louvaris 2016; Probst 2011; Sandland 2008; Steele 2019; Vasilopoulou 2017; Wootton 2017) and 10 abstracts (Egan 2010; Kanabar 2015; Loeckx 2018; Mantoani 2018; Mitchell 2013; Ng 2015; Priori 2017; Saini 2017; Singh 1998; Tahirah 2015) to be at unclear risk.
We judged four studies to have a high risk of bias where attrition was unevenly distributed between groups (Tabak 2014b), documented but not detailed (Bender 2016), specifically addressed by authors (Vorrink 2016) or clearly related to the intervention (Hartman 2016).
Selective reporting
Most studies (n = 58) had a registered or published trial protocol which facilitated assessment for risk of reporting bias, except for 11 studies (Altenburg 2015; Dal Negro 2012; De Blok 2006; Goris 2003; Hospes 2009; Kawagoshi 2015; Probst 2011; Rinaldo 2017; Varas 2018; Vorrink 2016; Widyastuti 2018) and seven abstracts (Kanabar 2015; Loeckx 2018; Nakamura 2016; Ng 2015; Saini 2017; Priori 2017; Sena 2013).
We rated 12 studies at low risk (Alison 2019; Arbillaga‐Etxarri 2018; Beeh 2014; Charususin 2018; De Roos 2017; Gamper 2019; Maddocks 2016; Magnussen 2017; Ogasawara 2018; Rinaldo 2017; Troosters 2018; Watz 2016).
We judged 25 studies (Altenburg 2015; Bender 2016; Benzo 2016; Blumenthal 2014; Borges 2014; Breyer 2010; Burtin 2015; Chaplin 2017; Cruz 2016; Dal Negro 2012; Demeyer 2017; Duiverman 2008; Effing 2011; Hartman 2016; Hornikx 2015; Lord 2012; Louvaris 2016; Nguyen 2009; Orme 2018; Polkey 2018; Schuz 2015; Tabak 2014a; Tabak 2014b; Vasilopoulou 2017; Wan 2017), two abstracts (Kanabar 2015; Nakamura 2016) and one clinical trial registry study (NCT01351792) to be at high risk. This was primarily due to discrepancies between trial registration and publications (including identification of primary and secondary outcomes), as well as between the way that outcomes were prespecified to be analysed and actually reported. Thirty‐six studies were at unclear risk of reporting bias.
Other potential sources of bias
We rated most studies (n = 55) as being at unclear risk, or at low risk (n = 18; Alison 2019; Altenburg 2015; Beeh 2014; Curtis 2016; De Blok 2006; Hartman 2016; Holland 2017; Hospes 2009; Jolly 2018; Kanabar 2015; Kawagoshi 2015; Magnussen 2017; Mendoza 2015; Nolan 2017; Schuz 2015; Tsai 2016; Wan 2017; Watz 2016) from other potential sources of bias. We deemed three studies to be at high risk from other potential sources of bias (methodological concerns, Bender 2016, Nguyen 2009; lack of physical activity data by group, Orme 2018).
Effects of interventions
See: Table 1; Table 3; Table 4; Table 5; Table 6
Structure of the analysis
After examining the data, we found that the included studies examined a wide range of interventions (Table 7) across the four defined comparisons (intervention versus no intervention; intervention versus placebo/sham; intervention with common intervention versus common intervention; intervention versus intervention).
2. Overview of results.
| Comparison | Description of intervention(s) | OUTCOMES | ||||
| Physical activity | Health‐related quality of life | Exercise capacity | Adherence | Adverse events | ||
| TYPE OF INTERVENTION: Pulmonary rehabilitation/exercise training | ||||||
| Clinically stable | ||||||
| Intervention vs. no intervention | Pulmonary rehabilitation vs. no intervention | De Roos 2017 | Y | Y | Y | N |
| Egan 2010 | Y | Y | N | N | ||
| Tsai 2016 | Y | Y | Y | Y | ||
| Wootton 2017 | Y | Y | Y | Y | ||
| High‐intensity interval training vs. no intervention | Louvaris 2016 | Y | Y | N | N | |
| Vasilopoulou 2017 | Y | Y | Y | Y | ||
| Vasilopoulou 2017 | ||||||
| Maintenance (telerehabilitation) following high‐intensity interval training vs. no intervention | ||||||
| Maintenance (centre‐based) following high‐intensity interval training vs. no intervention | ||||||
| Intervention in addition to an intervention common to both groups | Nordic walking with education vs. education | Breyer 2010 | Y | Y | Y | Y |
| Structure exercise training (COPE‐active) with self‐management vs. self management | Effing 2011 | Y | Y | Y | Y | |
| Upper limb exercises with education vs. education | Larson 2014 | N | N | N | N | |
| Exercise training and LABA with LAMA and behavioural modification vs. LAMA and behavioural modification | Troosters 2018 | Y | Y | Y | Y | |
| Exercise training with LAMA/LABA and behavioural modification vs. LAMA/LABA and behavioural modification | ||||||
| Exercise training and LAMA/LABA with behavioural modification vs. placebo with behavioural modification | ||||||
| Exercise training and physical activity counselling with pedometer vs. pedometer | Varas 2018 | Y | Y | Y | N | |
| Intervention vs. intervention | Web‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | Chaplin 2017 | Y | Y | N | Y |
| Exercise training (eccentric cycle training) vs. exercise training (concentric cycle training) | Sena 2013 | N | Y | N | N | |
| Home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | Holland 2017 | Y | Y | Y | Y | |
| Water‐based exercise training vs. land‐based exercise training | Felcar 2018 | Y | Y | Y | Y | |
| Tai Chi vs. pulmonary rehabilitation | Polkey 2018 | Y | Y | Y | Y | |
| Exercise training (callisthenics) vs. exercise training (endurance and strength training) | Probst 2011 | Y | Y | Y | N | |
| Exercise training (outdoor walking) vs. exercise training (cycle ergometry) | Gamper 2019 | Y | Y | N | Y | |
| physical activity counselling vs. pulmonary rehabilitation | Widyastuti 2018 | Y | Y | N | N | |
| O'Neill 2018 | Y | Y | Y | Y | ||
| Exercise training with tapering supervision vs. supervised exercise training | Rinaldo 2017 | Y | Y | Y | N | |
| Adherence intervention vs. pulmonary rehabilitation | Steele 2019 | Y | Y | Y | N | |
| Maintenance following high‐intensity interval training: telerehabilitation vs. centre‐based | Vasilopoulou 2017 | Y | Y | Y | N | |
| Acute | ||||||
| Intervention vs. no intervention | Exercise training vs. no intervention | Tahirah 2015 | N | Y | Y | N |
| Borges 2014 | Y | Y | Y | Y | ||
| TYPE OF INTERVENTION: Physical activity counselling | ||||||
| Clinically stable | ||||||
| Intervention vs. no intervention | Physical activity counselling vs. no intervention | Priori 2017 | N | N | Y | N |
| Hospes 2009 | Y | Y | N | Y | ||
| Altenburg 2015 | Y | Y | N | Y | ||
| Demeyer 2017 | Y | Y | Y | Y | ||
| Arbillaga‐Etxarri 2018 | Y | Y | Y | Y | ||
| Saini 2017 | N | N | N | N | ||
| Wootton 2017 | Y | Y | Y | Y | ||
| Intervention in addition to an intervention common to both groups | Physical activity counselling with optional supervised exercise vs. optional supervised exercise | Tabak 2014a | Y | N | Y | N |
| Vorrink 2016 | Y | Y | Y | N | ||
| Pedometer with physical activity counselling vs. physical activity counselling | Mendoza 2015 | Y | Y | Y | N | |
| Physical activity counselling with pedometer vs. pedometer | Bender 2016 | Y | N | N | Y | |
| Wan 2017 | N | Y | Y | Y | ||
| Nguyen 2009 | Y | Y | Y | Y | ||
| Moy 2015a | Y | N | Y | Y | ||
| Pedometer with pulmonary rehabilitation: aware vs. unaware of purpose of pedometer | Singh 1998 | N | N | N | N | |
| Physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | Mantoani 2018 | Y | Y | N | N | |
| De Blok 2006 | Y | Y | Y | N | ||
| Altenburg 2015 | Y | Y | N | N | ||
| Cruz 2016 | Y | Y | Y | N | ||
| Nolan 2017 | Y | Y | Y | Y | ||
| Kawagoshi 2015 | Y | Y | Y | Y | ||
| Loeckx 2018 | Y | Y | N | N | ||
| Physical activity counselling with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation | Burtin 2015 | Y | Y | Y | N | |
| Acute | ||||||
| Intervention vs. no intervention | Physical activity counselling vs. no intervention | Hornikx 2015 | Y | Y | N | Y |
| Feedback and education vs. no intervention | Orme 2018 | Y | N | Y | Y | |
| Education vs. no intervention | ||||||
| Intervention in addition to an intervention common to both groups | Feedback with education vs. education | |||||
| TYPE OF INTERVENTION: Self‐management | ||||||
| Clinically stable | ||||||
| Intervention vs. no intervention | Self‐management vs. no intervention | Mitchell 2013 | Y | Y | N | Y |
| Tabak 2014b | Y | Y | Y | N | ||
| Jolly 2018 | Y | N | Y | Y | ||
| Intervention vs. sham/placebo intervention | Self‐management (health mentoring) vs. sham | Schuz 2015 | Y | N | Y | Y |
| Intervention in addition to an intervention common to both groups | Self‐efficacy training with upper limb exercises vs. education with upper limb exercises | Larson 2014 | N | N | N | N |
| Intervention vs. intervention | Self‐management (coping skills training) vs. education and symptom monitoring | Blumenthal 2014 | Y | Y | Y | Y |
| Acute | ||||||
| Intervention vs. no intervention | Self‐management (SPACE) vs. no intervention | Kanabar 2015 | N | Y | N | N |
| Intervention in addition to an intervention common to both groups | Self‐management (health coaching) with pulmonary rehabilitation referral vs. pulmonary rehabilitation referral | Benzo 2016 | Y | N | Y | Y |
| TYPE OF INTERVENTION: Pharmacological treatments | ||||||
| Clinically stable | ||||||
| Intervention vs. sham/placebo intervention | LAMA vs. placebo | Beeh 2014 | N | Y | N | Y |
| Magnussen 2017 | Y | N | N | Y | ||
| NCT00144326 | Y | Y | N | Y | ||
| LAMA/LABA vs. placebo | Watz 2016 | N | N | Y | Y | |
| Watz 2017 | N | Y | N | Y | ||
| Intervention in addition to an intervention common to both groups | LAMA with behavioural modification vs. placebo with behavioural modification | Troosters 2014 | N | N | Y | Y |
| Troosters 2018 | Y | Y | Y | Y | ||
| LAMA/LABA with behavioural modification vs. placebo with behavioural modification | Troosters 2018 | Y | Y | Y | Y | |
| LABA with LAMA and behavioural modification vs. LAMA and behavioural modification | ||||||
| ACE inhibitor with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation | Curtis 2016 | Y | Y | Y | Y | |
| Intervention vs. intervention | ICS and LABA vs. ICS and LABA | NCT01351792 | Y | N | N | Y |
| LAMA vs. LAMA | Nakamura 2016 | Y | N | Y | Y | |
| TYPE OF INTERVENTION: Nutritional supplementation | ||||||
| Clinically stable | ||||||
| Intervention vs. no intervention | Nutritional supplement vs. no intervention | Goris 2003 | N | N | Y | N |
| Intervention vs. sham/placebo intervention | Nutritional supplement vs. placebo | Dal Negro 2012 | Y | N | N | N |
| Intervention in addition to an intervention common to both groups | Nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation | Van de Bool 2017 | Y | Y | Y | Y |
| Nutritional supplement with physical activity counselling vs. physical activity counselling | ||||||
| Acute | ||||||
| Intervention in addition to an intervention common to both groups | Enriched nutritional supplement with inpatient pulmonary rehabilitation vs. nutritional supplement with inpatient pulmonary rehabilitation | Ogasawara 2018 | Y | N | N | N |
| TYPE OF INTERVENTION: Supplemental oxygen | ||||||
| Clinically stable | ||||||
| Intervention vs. sham/placebo intervention | Supplemental oxygen vs. placebo (air) | Sandland 2008 | Y | Y | Y | Y |
| Intervention in addition to an intervention common to both groups | Supplemental oxygen with exercise training vs. sham with exercise training | Alison 2019 | Y | Y | Y | Y |
| Intervention vs. intervention | Supplemental oxygen (lightweight ambulatory) vs. supplemental oxygen (E‐cylinder) | Casaburi 2012 | N | N | Y | Y |
| TYPE OF INTERVENTION: Other interventions | ||||||
| Clinically stable | ||||||
| Intervention vs. no intervention | Four‐wheeled walker vs. no intervention | Ng 2015 | Y | N | N | N |
| Endobronchial valve surgery vs. no intervention | Hartman 2016 | Y | Y | N | Y | |
| Intervention vs. sham/placebo intervention | Singing vs. sham | Lord 2012 | Y | Y | Y | N |
| Neuromuscular electrical stimulation vs. placebo | Maddocks 2016 | Y | Y | Y | Y | |
| Intervention in addition to an intervention common to both groups | Non‐invasive ventilation with pulmonary rehabilitation vs. pulmonary rehabilitation | Duiverman 2008 | Y | Y | Y | Y |
| Inspiratory muscle training with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | Charususin 2018 | Y | Y | Y | N | |
ACE: angiotensin‐converting enzyme; ICS: inhaled corticosteroid; LABA: long‐acting beta2 agonist; LAMA: long‐acting muscarinic antagonist; SPACE: self‐management programme of activity, coping and education
We present results for the primary outcome of physical activity here. We present results for secondary outcomes in Appendix 4 (health‐related quality of life), Appendix 5 (exercise capacity), Appendix 6 (adherence) and Appendix 7 (adverse events).
We present results by type of intervention, with precise comparison by clinical setting (clinically‐stable disease, acute exacerbation). We define the following types of intervention to aid the reader in finding relevant data:
pulmonary rehabilitation/exercise training;
physical activity counselling;
self‐management;
pharmacological;
nutritional supplementation;
supplemental oxygen;
other interventions.
INTERVENTION: Pulmonary rehabilitation/exercise training
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Pulmonary rehabilitation versus no intervention
No clear improvement in physical activity was demonstrated following pulmonary rehabilitation compared to no intervention, with a single variable showing an increase. The mean difference (MD) in step count was 208 steps (95% confidence interval (CI) −165 to 581; 3 studies, 180 participants; low‐certainty evidence; Analysis 1.1; Figure 3).
1.1. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 1 change in step count (steps per day); Intervention: pulmonary rehabilitation/exercise training.
3.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.1: Physical activity: change in step count (steps per day)
The mean difference in time in moderate‐to‐vigorous intensity physical activity (MVPA) was 4 minutes (95% CI −2 to 9; 3 studies, 190 participants; low‐certainty evidence; Analysis 1.2; Figure 4).
4.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.2: Physical activity: change in time in moderate‐to‐vigorous intensity physical activity (minutes per day)
The mean difference in time in light‐intensity physical activity (LIPA) was −2 minutes (95% CI −28 to 25; 3 studies, 182 participants; low‐certainty evidence; Analysis 1.3; Figure 5), with substantial heterogeneity evident (I2 = 77%) .
1.3. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 3 change in time in light‐intensity physical activity (minutes per day); Intervention: pulmonary rehabilitation/exercise training.
5.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.4: Physical activity: change in time in light‐intensity physical activity (minutes per day)
The mean difference in total energy expenditure was −42 kcal (95% CI −90 to 7; 2 studies, 144 participants; low‐certainty evidence; Analysis 1.4; Figure 6).
1.4. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 4 change in total energy expenditure (kcal); Intervention: pulmonary rehabilitation/exercise training.
6.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.3: Physical activity: change in total energy expenditure (kcal)
The mean difference in physical activity level (PAL) was 0.1 (95% CI −0.1 to 0.1; Tsai 2016, 36 participants; low‐certainty evidence; Table 2) following telerehabilitation, consisting of pulmonary rehabilitation delivered by videoconferencing into the home. The only clear improvement in physical activity following pulmonary rehabilitation was a greater increase in total time spent in physical activity (MD 23 minutes, 95% CI 6 to 40; 2 studies, 88 participants; low‐certainty evidence; Analysis 1.5; Figure 7).
1.5. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 5 change in time in physical activity (total; minutes per day); Intervention: pulmonary rehabilitation/exercise training.
7.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.6: Physical activity: change in time in physical activity (total, minutes per day)
The mean difference in change in sedentary time was 17 minutes (95% CI −27 to 60; 2 studies, 137 participants; low‐certainty evidence; Analysis 1.6; Figure 8) following pulmonary rehabilitation compared to no intervention.
1.6. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 6 change in sedentary time (minutes per day); Intervention: pulmonary rehabilitation/exercise training.
8.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.5: Physical activity: change in sedentary time (minutes per day)
High‐intensity interval training versus no intervention
Improvements in physical activity were demonstrated following high‐intensity interval training compared to no intervention in two studies from the same research team. Improvements in time in 'lifestyle' physical activity (MD 9 minutes, 95% CI 4 to 15; Analysis 1.7; Figure 9), in LIPA (MD 28 minutes, 95% CI 16 to 41; Analysis 1.8; Figure 10), in MVPA (MD 6 minutes, 95% CI 4 to 8; Analysis 1.9; Figure 11) and sedentary (MD −34 minutes, 95% CI −56 to −13; Analysis 1.10; Figure 12) were demonstrated at end intervention (2 studies, 275 participants; moderate‐certainty evidence).
1.7. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 7 time in "lifestyle" physical activity (minutes per day); Intervention: high‐intensity interval training.
9.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome: 1.8 Physical activity: time in "lifestyle" physical activity (minutes per day)
1.8. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 8 time in light‐intensity physical activity (minutes per day); Intervention: high‐intensity interval training.
10.

Forest plot of comparison: 1 Intervention vs. no intervention
Outcome: 1.7 Physical activity: time in light‐intensity physical activity (minutes per day)
11.
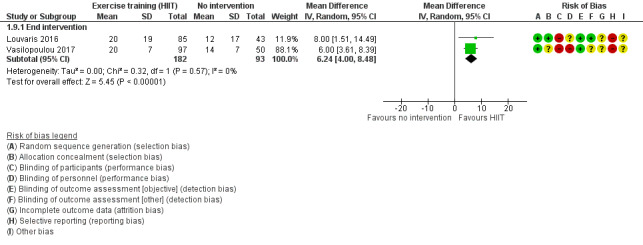
Forest plot of comparison 1: Intervention vs. vs. no intervention
Outcome 1.9: Physical activity: time in MVPA (minutes per day)
1.10. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 10 sedentary time (minutes per day); Intervention: high‐intensity interval training.
12.

Forest plot of comparison 1: Intervention vs. no intervention
Outcome 1.10: Physical activity: sedentary time (minutes per day)
Additionally, improvements in step count (MD 1683 steps, 95% CI 721 to 2646) and vector magnitude units (VMU) (MD 89, 95% CI 13 to 165) were demonstrated following a 12‐week intervention (moderate‐certainty evidence; Louvaris 2016; 128 participants; Table 2).
Maintenance (telerehabilitation) following high‐intensity interval training versus no intervention
Increased time in LIPA (MD 44 minutes, 95% CI 27 to 62), moderate‐intensity (MD 7 minutes, 95% CI 4 to 10) and "lifestyle" physical activity (MD 7 minutes, 95% CI 1 to 13) were demonstrated following a 12‐month telerehabilitation maintenance programme compared to no intervention (moderate‐certainty evidence; Vasilopoulou 2017, 97 participants; Table 2). The mean difference in change in sedentary time was −31 minutes (95% CI −66 to 4; low‐certainty evidence; Vasilopoulou 2017, 97 participants; Table 2) at end intervention.
Maintenance (centre‐based) following high‐intensity interval training versus no intervention
Increased time in LIPA (MD 46 minutes, 95% CI 29 to 63), moderate‐intensity (MD 11 minutes, 95% CI 8 to 14) and "lifestyle" physical activity (MD 18 minutes, 95% CI 12 to 25) were demonstrated following a 12‐month centre‐based maintenance programme compared to no intervention. An improvement in sedentary time (MD −64 minutes, 95% CI −95 to −33; moderate‐certainty evidence; Vasilopoulou 2017, 100 participants; Table 2) was also demonstrated at end intervention.
COMPARISON: Intervention versus sham intervention
No studies presented data for this comparison.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
A range of interventions have been tested in single studies such that meta‐analysis was not possible.
Nordic walking with education versus education
Increased movement intensity was demonstrated following a 12‐week Nordic walking programme with education compared to education alone (MD 0.51 m/s2, 95% CI 0.27 to 0.75) and maintained at nine‐month follow‐up (MD 0.42 m/s2, 95% CI 0.21 to 0.63; Breyer 2010, 60 participants; low‐certainty evidence; Analysis 3.1). However, it was the only fully‐reported physical activity variable in this study and no data were available for time sitting, standing and walking in the education group (Breyer 2010; Table 2).
3.1. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 1 movement intensity (m/s2); Interventions: nordic walking with education vs. education.
Structured exercise training (COPE‐active) with self‐management versus self‐management
The mean difference in step count was 565 steps (95% CI −354 to 1484) after seven months of an 11‐month structured exercise training programme (COPE‐active) with self‐management compared to self‐management. An increase in step count was demonstrated at end intervention (MD 1178 steps, 95% CI 260 to 2096) and this improvement was maintained at 24‐month follow‐up (MD 1193 steps, 95% CI 226 to 2160; Effing 2011, 110 participants; low‐certainty evidence; Analysis 3.2).
3.2. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 2 change in step count (steps per day); Interventions: exercise training (COPE‐active) with self‐management vs. self management.
Upper‐limb exercise with education versus education
The mean difference in time in LIPA was 3 minutes (95% CI −31 to 38) at end intervention and 14 minutes (95% CI −36 to 64) at 12‐month follow‐up after a four‐month study of upper‐limb exercise with education compared to education alone (Larson 2014, 34 participants; low‐certainty evidence; Analysis 3.3).
3.3. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 3 change in time in light‐intensity physical activity (minutes per day); Interventions: upper body resistance training with health education vs. health education.
The mean difference in time spent in moderate‐intensity physical activity was 1 minute (95% CI −1 to 3), sedentary time was −57 minutes (95% CI −133 to 19) and proportion of time spent sedentary was −2% (95% CI −8 to 4) at end intervention (Larson 2014, 34 participants; low‐certainty evidence; Table 2).
Exercise training and long‐acting muscarinic antagonist/long‐acting beta agonist (LAMA/LABA) with behaviour modification versus placebo with behaviour modification
The mean difference in step count was −328 steps (95% CI −1214 to 558) after eight weeks and −541 steps (95% CI −1433 to 350) at end intervention following a 12‐week study for exercise training and LAMA/LABA with behavioural modification compared to placebo with behavioural modification (Troosters 2018; 8 weeks: 124 participants; 12 weeks: 112 participants; moderate‐certainty evidence; Analysis 3.4). The mean difference in walking time was −3 minutes (95% CI −13 to 6) after eight weeks and −6 minutes (95% CI −15 to 4) at end intervention (Troosters 2018; 8 weeks: 124 participants; 12 weeks: 112 participants; moderate‐certainty evidence; Analysis 3.5). The mean difference in walking intensity was −0.03 m/s2 (95% CI −0.11 to 0.05) after eight weeks and −0.02 (95% CI −0.10 to 0.06) at end intervention (Troosters 2018; 8 weeks: 124 participants; 12 weeks: 112 participants; moderate‐certainty evidence; Analysis 3.6).
3.4. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 4 step count (steps per day); Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification.
3.5. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 5 time walking (minutes per day); Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification.
3.6. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 6 walking intensity (m/s2); Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification.
Exercise training and LABA with LAMA and behaviour modification versus LAMA and behaviour modification
The mean difference in step count was −82 steps (95% CI −968 to 803) after eight weeks and 404 steps (95% CI −474 to 1281) at end intervention following a 12‐week study for exercise training and LABA with LAMA and behaviour modification compared to LAMA and behaviour modification (Troosters 2018; 8 weeks: 124 participants; 12 weeks: 114 participants; moderate‐certainty evidence; Analysis 3.7). The mean difference in walking time was −1 minute (95% CI −10 to 9) after eight weeks and 3 minutes (95% CI −6 to 13) at end intervention (Troosters 2018; 8 weeks: 124 participants; 12 weeks: 114 participants; moderate‐certainty evidence; Analysis 3.8). The mean difference in walking intensity was −0.05 m/s2 (95% CI −0.13 to 0.03) after eight weeks and 0.04 m/s2 (95% CI −0.04 to 0.12) at end intervention (Troosters 2018; 8 weeks: 124 participants; 12 weeks: 113 participants; moderate‐certainty evidence; Analysis 3.9).
3.7. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 7 step count (steps per day); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
3.8. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 8 time walking (minutes per day); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
3.9. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 9 walking intensity (m/s2); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
Exercise training with LAMA/LABA and behaviour modification versus LAMA/LABA and behaviour modification
The mean difference in step count was −554 steps (95% CI −1432 to 325) after eight weeks and −837 steps (95% CI −1708 to 33) at end intervention following a 12‐week study for exercise training with LAMA/LABA and behaviour modification compared to LAMA/LABA and behaviour modification (Troosters 2018; 8 weeks: 126 participants; 12 weeks: 117 participants; moderate‐certainty evidence; Analysis 3.10).
3.10. Analysis.
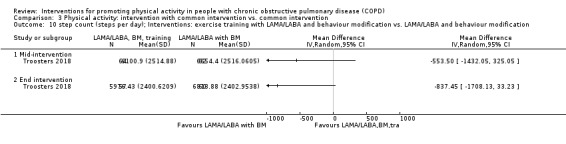
Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 10 step count (steps per day); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification.
The mean difference in walking time was −4 minutes (95% CI −14 to 5) after eight weeks and −8 minutes (95% CI −18 to 1) at end intervention (Troosters 2018; 8 weeks: 126 participants; 12 weeks: 117 participants; moderate‐certainty evidence; Analysis 3.11).
3.11. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 11 time walking (minutes per day); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification.
Walking intensity was lower in the group without exercise training (−0.09 m/s2, 95% CI −0.17 to −0.01) after eight weeks. The mean difference in walking intensity was −0.04 m/s2 (95% CI −0.12 to 0.04) at end intervention (Troosters 2018; 8 weeks: 126 participants; 12 weeks: 115 participants; moderate‐certainty evidence; Analysis 3.12).
3.12. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 12 walking intensity (m/s2); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification.
Exercise training and physical activity counselling with pedometer versus pedometer alone
An increase in step count (MD 3174 steps, 95% CI 1453 to 4895) was demonstrated following an eight‐week exercise training and physical activity counselling (in‐person) programme with pedometer compared to pedometer alone. This improvement was maintained at three‐month (MD 3841 steps, 95% CI 2225 to 5457) and 12‐month follow‐up (MD 2547 steps, 95% CI 927 to 4167; Varas 2018, 33 participants; moderate‐quality evidence; Analysis 3.13).
3.13. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 13 change in step count (steps per day); Interventions: exercise training and physical activity counselling with pedometer vs. pedometer.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Web‐based pulmonary rehabilitation versus centre‐based pulmonary rehabilitation
No data were presented in a seven‐week study of web‐based pulmonary rehabilitation compared to a centre‐based program (Chaplin 2017, 54 participants; very low‐certainty evidence; Table 2).
Exercise training (eccentric cycle training) versus exercise training (concentric cycle training)
No data were presented in a 10‐week study of eccentric cycle training compared to concentric training (Sena 2013, 16 participants; very low‐certainty evidence; Table 2).
Home‐based pulmonary rehabilitation versus centre‐based pulmonary rehabilitation
Similar results were demonstrated for change in step count (Analysis 4.1), time in MVPA (Analysis 4.2), number of MVPA bouts (Analysis 4.3), time in MVPA bouts (Analysis 4.4), sedentary time (Analysis 4.5), sedentary awake time (Analysis 4.6), number of sedentary bouts (Analysis 4.7), time in sedentary bouts (Analysis 4.8), METs (Analysis 4.9) and total energy expenditure (Analysis 4.10) at end intervention and 14‐month follow‐up in an equivalence study comparing an eight‐week home‐based pulmonary rehabilitation programme with a centre‐based programme (Holland 2017, 58 participants; low‐certainty evidence).
4.1. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 1 change in step count (steps per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.3. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 3 change in number of bouts of moderate‐to‐vigorous intensity physical activity; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.4. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 4 change in time in bouts of moderate‐to‐vigorous intensity physical activity(minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.5. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 5 change in sedentary time (minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.6. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 6 change in sedentary time (awake; minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.7. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 7 change in number of sedentary bouts; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.8. Analysis.
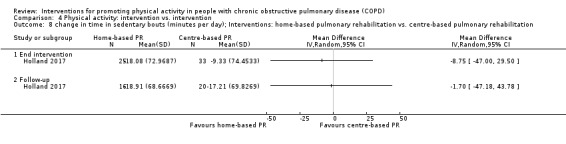
Comparison 4 Physical activity: intervention vs. intervention, Outcome 8 change in time in sedentary bouts (minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.9. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 9 change in METs; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
4.10. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 10 change in total energy expenditure (kcal); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
Water‐based exercise training versus land‐based exercise training
The mean difference in step count was 676 steps (95% CI −645 to 1997; Analysis 4.11) and total energy expenditure was 39 kcal (95% CI −14 to 92; Felcar 2018, Analysis 4.12). Ten participants in the water‐based group and five participants in the land‐based group were classified as "active" following a six‐month study of water‐based exercise training compared to a land‐based programme (Felcar 2018, 36 participants; low‐certainty evidence; Table 2).
4.11. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 11 change in step count (steps per day); Interventions: water‐based exercise training vs. land‐based exercise training.
4.12. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 12 change in total energy expenditure (kcal); Interventions: water‐based exercise training vs. land‐based exercise training.
Tai Chi versus pulmonary rehabilitation
An increase in step count was demonstrated in the Tai Chi group (MD 1349 steps, 95% CI 93 to 2605; Polkey 2018, 110 participants; moderate‐certainty evidence; Analysis 4.13) following 22 weeks in a 24‐week study of Tai Chi compared to pulmonary rehabilitation.
4.13. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 13 step count (steps per day); Interventions: Tai Chi vs. pulmonary rehabilitation.
Calisthenics versus exercise training
"No significant differences" in step count, MVPA time, time walking, time standing, time sitting, time lying, active energy expenditure or total energy expenditure were reported following a 12‐week callisthenics and breathing exercises programme compared to exercise training (Probst 2011, 40 participants; low‐certainty evidence Table 2).
Exercise training (outdoor walking) versus exercise training (cycle ergometry)
The mean difference in step count was −928 steps (95% CI −2515 to 659) following a three‐week study comparing outdoor walking and cycle ergometry. The mean difference in step count was −267 steps (95% CI −1622 to 1088) at three‐month follow up (Gamper 2019, 16 participants; low‐certainty evidence; Analysis 4.14).
4.14. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 14 step count (steps per day); Interventions: outdoor walking vs. cycle ergometry.
Physical activity counselling versus pulmonary rehabilitation
The mean difference in step count was −92 steps (95% CI −1710 to 1526; Widyastuti 2018, 36 participants; low‐certainty evidence; Table 2) following a six‐week physical activity counselling intervention (in‐person) compared to pulmonary rehabilitation.
The mean difference in step count was 1291 steps (95% CI −749 to 333) at end intervention following a 12‐week physical activity counselling intervention (in‐person) compared to six weeks of pulmonary rehabilitation. The mean difference in step count was 347 steps (95% CI −2216 to 2910) at three‐month follow‐up (O'Neill 2018, 26 participants; low‐certainty evidence; Analysis 4.15).
4.15. Analysis.
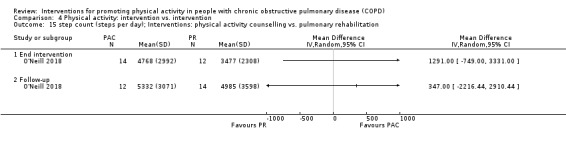
Comparison 4 Physical activity: intervention vs. intervention, Outcome 15 step count (steps per day); Interventions: physical activity counselling vs. pulmonary rehabilitation.
An improvement in number in MVPA bouts was demonstrated in the physical activity counselling group (MD 0.5, 95% CI 0.3 to 0.8).
The mean difference in time in MVPA was 6 minutes (95% CI −10 to 22) and time in MVPA bouts was 10 minutes (95% CI −2 to 21) at end intervention (O'Neill 2018, 26 participants; low‐certainty evidence; Table 2).
Exercise training with tapering supervision versus exercise training
The mean difference in total energy expenditure was 520 kcal (95% CI −105 to 1145) at end intervention and 400 kcal (95% CI −109 to 909) at 42‐week follow‐up after a 28‐week study of exercise training with tapered supervision compared to supervised exercise training (Rinaldo 2017, 24 participants; moderate‐certainty evidence; Analysis 4.16).
4.16. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 16 total energy expenditure (kcal); Interventions: exercise training with tapered supervision vs. supervised exercise training.
Adherence intervention versus pulmonary rehabilitation
The mean difference in step count was −159 steps (95% CI −1742 to 1424), time inactive was −2% (95% CI −9 to 5) and peak performance was 0 (95% CI −9 to 9) following six months of an adherence intervention compared to eight weeks of pulmonary rehabilitation (Steele 2019, 63 participants; low‐certainty evidence; Table 2).
Maintenance following high‐intensity interval training: telerehabilitation versus centre‐based programme
Less time was spent in lifestyle (MD −11 minutes, 95% CI −18 to −4) and moderate‐intensity physical activity (MD −4 minutes, 95% CI −7 to −1) in the telerehabilitation group compared to a centre‐based group following a 12‐month study of maintenance after eight weeks of high‐intensity interval exercise training.
The mean difference in time in LIPA was −2 minutes (95% CI −19 to 15) and sedentary time was 33 minutes (95% CI −3 to 69; Vasilopoulou 2017, 100 participants; moderate‐quality evidence; Table 2).
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Inpatient exercise training versus no intervention
No clear improvement in physical activity was demonstrated following two inpatient exercise‐training interventions.
The median step count for the exercise training group was 4215 steps (interquartile range (IQR) 2133 to 6693) compared to no intervention (median 2198 steps (IQR 1242 to 4857; P = 0.07; low‐certainty evidence; Tahirah 2015, 34 participants; Table 2) at discharge following inpatient walking and functional‐resistance training compared to no intervention.
The mean difference for time in standing was 15 minutes (95% CI −57 to 87), sitting was −11 minutes (95% CI −94 to 72), walking was −19 minutes (95% CI −40 to 2) and lying was 21 minutes (95% CI −78 to 120; low‐certainty evidence; Borges 2014, 29 participants; Table 2) four weeks after discharge following inpatient resistance training compared to no intervention.
INTERVENTION: Physical activity counselling
See Table 4.
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Physical activity counselling versus no intervention
We were unable to pool studies for quantitative synthesis due to data type (Altenburg 2015) and heterogeneous interventions (Arbillaga‐Etxarri 2018; Demeyer 2017; Hospes 2009; Priori 2017; Saini 2017; Wootton 2017; see Characteristics of included studies).
An increased proportion of time spent in moderate‐intensity physical activity (MD 32%, 95% CI 8 to 55; Priori 2017, 18 participants; very low‐certainty evidence; Table 2) was demonstrated following an eight‐week study of an automated coaching intervention compared to no intervention.
The same 12‐week in‐person intervention was used in three studies (two within this comparison). The mean difference in step count in one study was 1700 steps (95% CI −678 to 4078; Hospes 2009, 35 participants; low‐certainty evidence; Analysis 1.11) compared to no intervention. In a subsequent study, the median change in step count in participants recruited from primary care was 537 steps (IQR −611 to 1740) in the physical activity counselling group and 431 steps (IQR −899 to 749) in the no‐intervention group at end intervention (P = 0.48). The median change in step count was 157 steps (IQR −1679 to 994) in the physical activity counselling group and 48 steps (IQR −1004 to 885) in the no‐intervention group (P = 0.90) at 12‐month follow‐up (Altenburg 2015; 12 weeks: 40 participants; 12 months: 38 participants; low‐certainty evidence; Table 2). A greater median change in step count in participants recruited from secondary care was demonstrated in the physical activity counselling group (1002 steps, IQR −612 to 3077) compared to the no‐intervention group (−814 steps, IQR −2827 to 1063) at end intervention (P = 0.007). The median change in step count was 1128 steps (IQR −1322 to 2707) in the physical activity counselling group and −217 steps (IQR −1951 to 1147) in the no‐intervention group (P = 0.15) at 12‐month follow‐up (Altenburg 2015; 12 weeks: 43 participants; 12 months: 39 participants; low‐certainty evidence; Table 2). Participants in secondary care had more severe disease, as indicated by a lower baseline FEV1 (Characteristics of included studies). Subgroup analyses for participants with ≤ 10,000 steps per day at baseline revealed a similar pattern (Altenburg 2015; Table 2).
1.11. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 11 step count (steps per day); Intervention: physical activity counselling.
An increase in the mean difference for step count was 1548 steps (95% CI 1045 to 2051; Demeyer 2017; 280 participants; moderate‐certainty evidence; Analysis 1.11) following a 12‐week telecoaching intervention compared to no intervention. Improvements in walking time (MD 17 minutes, 95% CI 10 to 24), movement intensity (MD 0.09 m/s2, 95% CI 0.04 to 0.14) and MVPA time (MD 11 minutes, 95% CI 7 to 15) were also demonstrated (Demeyer 2017, 280 participants; moderate‐certainty evidence; Table 2).
The mean difference in step count was 177 steps (95% CI −828 to 1182; Arbillaga‐Etxarri 2018, 280 participants; low‐certainty evidence; Analysis 1.11) following a 12‐month Urban Training intervention compared to no intervention.
The mean difference in change in proportion of time in moderate‐intensity physical activity was −9% (standard deviation (SD) 24) in the physical activity counselling group and −21% (SD 21) in the no‐intervention group (P = 0.116) following an eight‐week physical activity counselling intervention compared to no intervention (Saini 2017, 28 participants; very low‐certainty evidence; Table 2).
The mean difference in step count was −617 steps (95% CI −1669 to 453), time in LIPA was −27 min (95% CI −70 to 14), time in moderate‐intensity physical activity was 20 minutes (95% CI −1 to 41), time in vigorous‐intensity physical activity was 0 minutes (95% CI 0 to 1) and energy expenditure wads 17 kcal (95% CI −131 to 164) following 12 months of physical activity counselling compared to no intervention, which was completion of phase 2 of a 14‐month study that all participants began with eight weeks of ground‐based walking training (Wootton 2017, 43 participants; low‐certainty evidence; Table 2).
COMPARISON: Intervention versus sham intervention
No studies presented data for this comparison.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Physical activity counselling with optional supervised exercise versus optional supervised exercise
The mean difference in step count was 986 steps (95% CI −1553 to 3525; Tabak 2014a, 29 participants; low‐certainty evidence; Table 2) following a three‐week physical activity counselling intervention (telecoaching) with optional supervised exercise compared to optional supervised exercise.
The mean difference in step count was 240 steps (95% CI −417 to 897) at end intervention and −77 steps (95% CI −763 to 609) at 12‐month follow‐up of a study of a six‐month physical activity counselling intervention (text message) following pulmonary rehabilitation with optional supervised exercise compared to optional supervised exercise (Vorrink 2016, 132 participants; low‐certainty evidence; Analysis 3.14). The mean difference in METs was −0.08 (95% CI −0.22 to 0.06) at end intervention and 0.05 (95% CI −0.10 to 0.20) at 12‐month follow‐up (Vorrink 2016, 121 participants; low‐certainty evidence; Analysis 3.15).
3.14. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 14 change in step count (weekday, steps per day); Interventions: physical activity counselling with optional supervised exercise vs. optional supervised exercise.
3.15. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 15 METs; Interventions: physical activity counselling with optional supervised exercise vs. optional supervised exercise.
Pedometer with physical activity counselling versus physical activity counselling
An increase in step count was demonstrated (MD 2942 steps, 95% CI 1881 to 4003; Mendoza 2015, 97 participants; moderate‐certainty evidence; Table 2) following a 12‐week study of pedometer use with physical activity counselling (in‐person) compared to physical activity counselling alone.
Physical activity counselling with pedometer versus pedometer
No data were presented for step count (completer data only) in a 12‐week study of a physical activity counselling intervention (phone call) with pedometer compared to pedometer alone (Bender 2016, 99 participants; very low‐certainty; Table 2).
The mean difference in step count was −75 steps (95% CI −1002 to 852; Wan 2017, 109 participants; low‐certainty evidence; Analysis 3.16) following a 12‐week physical activity counselling intervention (web‐based) with pedometer compared to pedometer alone.
3.16. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 16 step count (steps per day); Interventions: physical activity counselling with pedometer vs. pedometer.
The mean difference in step count was 1427 steps (95% CI −1482 to 4336) after 12 weeks and −63 steps (95% CI −3080 to 2754) following a six‐month physical activity counselling intervention (text message, coached) with pedometer compared to pedometer alone (Nguyen 2009, 17 participants; low‐certainty evidence; Analysis 3.16.
The mean difference in active time was 6 minutes (95% CI −2 to 13) after 12 weeks and −0 minutes (95% CI −7 to 7) at end intervention (Nguyen 2009, 17 participants; low‐certainty evidence; Analysis 3.17.
3.17. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 17 time active (minutes per day); Interventions: physical activity counselling (app) with pedometer vs. pedometer.
The mean difference in inactive time was −4 minutes (95% CI −15 to 8) after 12 weeks and 0 minutes (95% CI −12 to 1) at end intervention (Nguyen 2009, 17 participants; low‐certainty evidence; Analysis 3.18).
3.18. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 18 time inactive (minutes per day); Interventions: physical activity counselling (app) with pedometer vs. pedometer.
The mean difference in peak performance was 0 steps/min (95% CI −15 to 15) after 12 weeks and −12 steps/min (95% CI −27 to 3) at end intervention (Nguyen 2009, 17 participants; low‐certainty evidence; Analysis 3.19).
3.19. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 19 peak performance (steps per minute); Interventions: physical activity counselling (app) with pedometer vs. pedometer.
An increase in step count was demonstrated after four months (MD 793 steps, 95% CI 236 to 1350; 201 participants) but not at end intervention (MD 107 steps, 95% CI −498 to 712; Moy 2015a, 238 participants; low‐certainty evidence; Analysis 3.16) following a 12‐month physical activity counselling intervention (web‐based) with pedometer compared to pedometer alone.
Pedometer during pulmonary rehabilitation
The mean difference in step count was 419 steps in a seven‐day study of pedometer use during pulmonary rehabilitation with awareness of the purpose of the pedometer compared to lack of awareness (Singh 1998, 19 participants; very low‐certainty evidence; Table 2).
Physical activity counselling with pulmonary rehabilitation versus pulmonary rehabilitation
An increase in step count was demonstrated (MD 1661 steps, 95% CI 552 to 2770; Mantoani 2018, 44 participants; very low‐certainty evidence; Table 2) following a 12‐week physical activity counselling intervention (web‐based) with pulmonary rehabilitation compared to pulmonary rehabilitation.
The addition of the same 12‐week physical activity counselling intervention (in‐person) had mixed results in two studies where participants in both groups received pulmonary rehabilitation.
The mean difference in step count was 680 steps (95% CI −1105 to 2465; De Blok 2006, 16 participants; low‐certainty evidence; Analysis 3.20) following a 12‐week study of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation alone. In a subsequent study, a greater median change in step count was demonstrated in the physical activity counselling and pulmonary rehabilitation group (547 steps, IQR 187 to 1323) compared to the pulmonary rehabilitation group (−211 steps, IQR −1337 to 1038) at end intervention (P = 0.03). The median change in step count was −569 steps (IQR −2512 to 1551) in the physical activity counselling and pulmonary rehabilitation group, and −1137 steps (IQR −2376 to 1427) in the pulmonary rehabilitation group (P = 0.58) at 12‐month follow‐up (Altenburg 2015; 12 weeks: 37 participants; 12 months: 23 participants; low‐certainty evidence; Table 2).
3.20. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 20 step count (steps per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
Longer studies have also had contradictory findings.
An increase in step count was demonstrated (MD 4010 steps, 95% CI 1407 to 6613) at 12 weeks and end intervention (MD 3267 steps, 95% CI 589 to 5944; Cruz 2016, 26 participants; moderate‐certainty evidence; Analysis 3.20) following a six‐month study of a physical activity counselling intervention (in‐person) with 12 weeks of pulmonary rehabilitation compared to 12 weeks of pulmonary rehabilitation. An increase in MVPA time was demonstrated (MD 31 minutes, 95% CI 10 to 52) at 12 weeks and end intervention (MD 24 minutes, 95% CI 2 to 45; Cruz 2016, 26 participants; moderate‐certainty evidence; Analysis 3.21). An increase in total physical activity time was demonstrated (MD 68 minutes, 95% CI 18 to 117) at 12 weeks and end intervention (MD 66 minutes, 95% CI 10 to 122; Cruz 2016, 26 participants; moderate‐certainty evidence; Analysis 3.22). An improvement in sedentary time was demonstrated at 12 weeks (MD −90 minutes, 95% CI −159 to −20). The mean difference in sedentary time was 12 minutes (95% CI −73 to 97) at end intervention; Cruz 2016, 26 participants; moderate‐certainty evidence; Analysis 3.23).
3.22. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 22 time in physical activity (total, minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
3.23. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 23 time sedentary (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
The median difference in accelerometer‐assessed step count was 272 steps (IQR −342 to 782) in the physical activity counselling with pulmonary rehabilitation group and 155 steps (IQR −438 to 867) in the pulmonary rehabilitation group (P = 0.99) following a study of a six‐month in‐person physical activity counselling intervention with eight weeks of pulmonary rehabilitation compared to eight weeks of pulmonary rehabilitation alone. The median difference in pedometer‐assessed step count was 727 steps (IQR −1493 to 3119) in the physical activity counselling with pulmonary rehabilitation group and 892 steps (IQR −1187 to 2534) in the pulmonary rehabilitation group (P = 0.55) at end intervention. The median difference in MVPA time was 11 minutes (IQR −1 to 33) in the physical activity counselling with pulmonary rehabilitation group and 11 minutes (IQR −2 to 28) in the pulmonary rehabilitation group (P = 0.62) at end intervention (Nolan 2017, 122 participants; low‐certainty evidence; Table 2).
An improvement in change in walking time was demonstrated (MD 39 minutes, 95% CI 1 to 78) following a 12‐month study of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation alone. The mean difference in standing time was 11 minutes (95% CI −18 to 40), lying time was −24 minutes (95% CI −72 to 24), frequency of postural changes was 21 (95% CI −23 to 65) and sitting time was 53 minutes (95% CI −21 to 127) at end intervention (Kawagoshi 2015, 27 participants; low‐certainty evidence; Table 2).
An improvement in change in step count was demonstrated (MD 1319 steps, standard error (SE) 571, P = 0.02) at end intervention and nine‐month follow‐up (MD 1348 steps, SE 628, P = 0.03) following 12 weeks of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation after all participants undertook 12 weeks of pulmonary rehabilitation. The mean difference in change in MVPA time was 8 minutes (SE 4) (P = 0.11) at end intervention and an improvement in change in MVPA time was demonstrated at nine‐month follow‐up (MD 13 minutes, (SE 5), P = 0.02; Loeckx 2018, 50 participants; very low‐certainty evidence; Table 2).
Physical activity counselling with pulmonary rehabilitation versus sham intervention with pulmonary rehabilitation
The mean difference in step count was 182 steps (95% CI −812 to 1176) after 12 weeks and −532 steps (95% CI −1584 to 520) following a six‐month study of a physical activity counselling intervention (in‐person) with pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation (Burtin 2015; 12 weeks: 61 participants; 6 months: 50 participants; very low‐certainty evidence; Analysis 3.24). The mean difference in time in MVPA was MD −1 minute (95% CI −13 to 12) after 12 weeks and −7 minutes (95% CI −16 to 3) at end intervention (Burtin 2015; 12 weeks: 61 participants; 6 months: 50 participants; very low‐certainty evidence; Analysis 3.25). The mean difference in walking time was −3 minutes (95% CI −12 to 7) after 12 weeks and −1 minute (95% CI −18 to 16) at end intervention (Burtin 2015; 12 weeks: 61 participants; 6 months: 50 participants; very low‐certainty evidence; Analysis 3.26). The mean difference in total physical activity time was −12 minutes (95% CI −39 to 15) after 12 weeks and −34 minutes (95% CI −48 to −20) at end intervention (Burtin 2015; 12 weeks: 61 participants; 6 months: 50 participants; very low‐certainty evidence; Analysis 3.27).
3.24. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 24 change in step count (steps per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.26. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 26 change in time walking (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.27. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 27 change in time in physical activity (total, minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
COMPARISON: Intervention versus intervention
No studies presented data for this comparison.
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Two studies have evaluated physical activity counselling following hospital admission for AECOPD.
Physical activity counselling versus no intervention
The mean difference in step count was −29 steps (95% CI −969 to 911), walking time was 0 minutes (95% CI −12 to 12) and walking intensity was −0.02 m/s2 (95% CI −0.06 to 0.02; Hornikx 2015, 26 participants; low‐certainty evidence; Table 2) after a four‐week study comparing physical activity counselling to no intervention following hospital admission for AECOPD.
Feedback and education versus no intervention; education versus no intervention
No data were presented for a 14‐day study of feedback and education compared to no intervention (14 participants) or education compared to no intervention (9 participants) following hospital admission for AECOPD (Orme 2018; very low‐certainty evidence; Table 2).
COMPARISON: Intervention versus standard common intervention (acute exacerbation of COPD)
Feedback with education versus education
No data were presented in a 14‐day study of feedback with education compared to education (Orme 2018; 11 participants; very low‐certainty evidence; Table 2).
INTERVENTION: Self‐management
See Table 5.
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Self‐management versus no intervention
An increase in step count was demonstrated (MD 547 steps, 95% CI 12 to 1082) following a six‐week SPACE programme compared to no intervention. The mean difference in sedentary time was −23 minutes (95% CI −77 to 31). The median time in bouts of physical activity was 142 minutes (95% CI 91 to 190) in the self‐management group and 96 minutes (95% CI 56 to 135) in the no‐intervention group at end intervention (P = 0.215). The mean difference in total energy expenditure was 16 kcal (95% CI −100 to 132) at end intervention (Mitchell 2013, 117 participants; very low‐certainty evidence; Table 2).
Improvement in 'IMA' (time integral of the modulus of accelerometer output) was demonstrated (MD 176 cpm, 95% CI 53 to 298) after four weeks and at end intervention (MD 176 cpm, 95% CI 51 to 301) following a 12‐week self‐management intervention compared to no intervention (Tabak 2014b, 20 participants; moderate‐certainty evidence; Analysis 1.12).
1.12. Analysis.
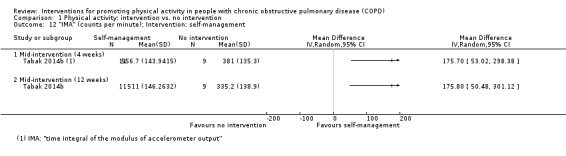
Comparison 1 Physical activity: intervention vs. no intervention, Outcome 12 "IMA" (counts per minute); Intervention: self‐management.
The mean difference in time in MVPA was 12 minutes (95% CI −21 to 45) at 12 months following a six‐month self‐management programme compared to no intervention (Jolly 2018, 411 participants; moderate‐certainty evidence; Table 2).
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Health mentoring versus sham intervention
The mean difference in step count was 61 steps (95% CI −951 to 1073) following a 12‐month study of phone call‐based health mentoring compared to a sham intervention (Schuz 2015, 120 participants; low‐certainty evidence; Analysis 2.1).
2.1. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 1 step count (steps per day); Intervention: self‐management (health mentoring).
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Self‐efficacy training with upper‐limb exercise versus education with upper‐limb exercise
An increase in time in LIPA was demonstrated (MD 43 minutes, 95% CI 15 to 71) at end intervention and the mean difference was 32 minutes (95% CI −18 to 82) at 12‐month follow‐up after a four‐month study of self‐efficacy training with upper‐limb exercise compared to upper‐limb exercise alone (Larson 2014, 35 participants; low‐certainty evidence; Analysis 3.28). The mean difference in time spent in moderate‐intensity physical activity was 2 minutes (95% CI −1 to 5), sedentary time was 25 minutes (95% CI −49 to 99) and the proportion of time spent sedentary was 0% (95% CI −6 to 6) at end intervention (Larson 2014, 35 participants; low‐certainty evidence; Table 2).
3.28. Analysis.
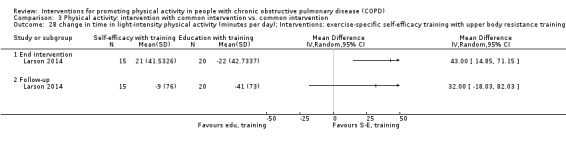
Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 28 change in time in light‐intensity physical activity (minutes per day); Interventions: exercise‐specific self‐efficacy training with upper body resistance training vs. upper body resistance training.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Self‐management versus education and symptom monitoring
An increase in physical activity was demonstrated in the self‐management group (mean 13 minutes (SE 1)) compared to the education and symptom‐monitoring group (mean 11 minutes (SE 1); P = 0.045) following 16 weeks of self‐management compared to education and symptom monitoring. An increase in total energy expenditure was also demonstrated in the self‐management group (MD 3605 (SE 211)) compared to the education and symptom‐monitoring group (MD 3113 (SE 212); P = 0.022) at end intervention. The mean difference in time in moderate‐intensity physical activity was 0.5 minutes (95% CI −0.6 to 1.6) at end intervention (Blumenthal 2014, 326 participants; low‐certainty evidence; Table 2).
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Self‐management versus no intervention
The mean difference in step count was 310 steps (95% CI −1665 to 2285), time in physical activity was 15 minutes (95% CI −30 to 60), time in moderate‐intensity physical activity was 13 minutes (95% CI −30 to 56), time in vigorous‐intensity physical activity was 2 minutes (95% CI −1 to 5), sedentary time was 4 minutes (95% CI −75 to 83), active energy expenditure was 85 kcal (95% CI −108 to 278), and total energy expenditure was −30 kcal (95% CI −225 to 165) following a seven‐day post‐admission self‐management programme of activity, coping and education (SPACE) compared to no intervention (Kanabar 2015, 25 participants; very low‐certainty evidence; Table 2).
COMPARISON: Intervention versus standard common intervention (acute exacerbation of COPD)
Health coaching with pulmonary rehabilitation referral versus pulmonary‐rehabilitation referral
No data were presented in a 12‐month post‐admission study of the addition of health coaching to pulmonary‐rehabilitation referral compared to pulmonary‐rehabilitation referral alone (Benzo 2016, 214 participants; very low‐certainty evidence; Table 2).
INTERVENTION: Pharmacological treatments
See Table 6.
COMPARISON: Intervention versus no intervention
No studies presented data for this comparison.
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
LAMA versus placebo
Two three‐week studies examined the impact of a long‐acting muscarinic antagonist (LAMA) compared to placebo. Individual‐level pre‐cross‐over data were obtained directly from the authors and used for combined analysis. The median change in step count was 104 steps (IQR −603 to 1228) in the LAMA group and 113 steps (IQR −936 to 1216) in the placebo group (P = 0.64) at end intervention. The median change in time in MVPA was −1 minute (IQR −17 to 24) in the LAMA group and −6 minutes (IQR −18 to 15) in the placebo group (P = 0.07) at end intervention. The median change in active energy expenditure was 15 kcal (IQR −103 to 117) in the LAMA group and −24 kcal (IQR −104 to 43) in the placebo group (P = 0.08) at end intervention. The median change in PAL was 0.00 (IQR −0.07 to 0.09) in the LAMA group and −0.01 (IQR −0.06 to 0.09) in the placebo group (P = 0.80) at end intervention (Beeh 2014; Magnussen 2017; 133 participants; moderate‐certainty evidence; Table 2).
No data were presented in another 12‐week study comparing LAMA with placebo (NCT00144326, 250 participants; very low‐certainty evidence; Table 2).
LAMA/LABA versus placebo
Two short‐term studies have assessed the effect of LAMA/long‐acting beta2 agonist (LABA); three weeks of indacaterol/glycopyrronium 110/50 μg once daily, Watz 2016; four weeks of aclidinium bromide/formoterol fumarate 400/12 μg twice daily, Watz 2017) compared to placebo. Meta‐analyses demonstrated improvements in step count (MD 531 steps, 95% CI 167 to 895; 2 studies, 426 participants; high‐certainty evidence; Analysis 2.2; Figure 13), time in MVPA (MD 10 minutes, 95% 4 to 15; 2 studies, 423 participants; high‐certainty evidence; Analysis 2.3; Figure 14) and active energy expenditure (MD 44 kcal, 95% CI 18 to 70; 2 studies, 423 participants; high‐certainty evidence; Analysis 2.4; Figure 15). Some heterogeneity was evident for step count (I2 = 27%), but not for other outcomes. Additionally, a reduced odds ratio (OR) was demonstrated for being classified as 'inactive' post‐intervention (OR 0.27, 95% CI 0.1 to 0.5; Watz 2017, 250 participants; high‐certainty evidence; Table 2).
2.2. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 2 change in step count (steps per day); Intervention: LAMA/LABA.
13.

Forest plot of comparison 2: Intervention vs. placebo
Outcome 2.2: Physical activity: change in step count (steps per day)
14.

Forest plot of comparison 2: Intervention vs. placebo
Outcome 2.3: Physical activity: change in time in moderate‐to‐vigorous intensity physical activity (minutes per day)
2.4. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 4 change in active energy expenditure (kcal); Intervention: LAMA/LABA.
15.

Forest plot of comparison 2: Intervention vs. placebo
Outcome 2.4: Physical activity: change in active energy expenditure (kcal)
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
LAMA with behaviour modification versus placebo with behaviour modification
The mean difference in time in MVPA was 8 minutes (95% CI −184 to 202), time in LIPA was 10 minutes (95% CI −6 to 26), odds ratio for being classified as 'inactive' post‐intervention 0.86 (95% CI 0.57 to 1.30; P = 0.477) following a six‐month study of LAMA compared to placebo (Troosters 2014, 426 participants; moderate‐certainty evidence; Table 2).
The mean difference in step count was −245 steps (95% CI −1146 to 655) after eight weeks. A deterioration in step count was demonstrated in the intervention group (MD −945 steps, 95% CI −1836 to −54) at end intervention following a 12‐week study for LAMA compared to placebo (Troosters 2018; 8 weeks: 120 participants; 12 weeks: 111 participants; moderate‐certainty evidence; Analysis 3.29). The mean difference in walking time was −3 minutes (95% CI −12 to 7) after eight weeks and −9 minutes (95% CI −20 to 2) at end intervention (Troosters 2018; 8 weeks: 120 participants; 12 weeks: 112 participants; moderate‐certainty evidence; Analysis 3.30). The mean difference in walking intensity was 0.02 m/s2 (95% CI −0.06 to 0.10) after eight weeks and −0.06 m/s2 (95% CI −0.14 to 0.02) at end intervention (Troosters 2018; 8 weeks: 120 participants; 12 weeks: 110 participants; moderate‐certainty evidence; Analysis 3.31).
3.29. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 29 step count (steps per day); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification.
3.30. Analysis.
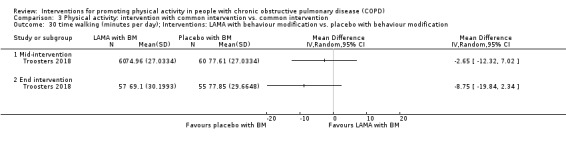
Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 30 time walking (minutes per day); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification.
3.31. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 31 walking intensity (m/s2); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification.
LAMA/LABA with behaviour modification versus placebo with behaviour modification
The mean difference in step count was 226 steps (95% CI −668 to 1119) after eight weeks and 296 steps (95% CI −585 to 1177) at end intervention following a 12‐week study of LAMA/LABA compared to placebo (Troosters 2018; 8 weeks: 122 participants; 12 weeks: 115 participants; moderate‐certainty evidence; Analysis 3.32. The mean difference in walking time was 1 minute (95% CI −8 to 11) after eight weeks and 3 minutes (95% CI −7 to 12) at end intervention (Troosters 2018; 8 weeks: 122 participants; 12 weeks: 115 participants; moderate‐certainty evidence; Analysis 3.33). The mean difference in walking intensity was 0.06 m/s2 (95% CI −0.02 to 0.14) after eight weeks and 0.02 m/s2 (95% CI −0.06 to 0.10) at end intervention (Troosters 2018: 8 weeks: 120 participants; 12 weeks: 112 participants; moderate‐certainty evidence; Analysis 3.34).
3.32. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 32 step count (steps per day); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
3.33. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 33 time walking (minutes per day); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
3.34. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 34 walking intensity (m/s2); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
LABA with LAMA and behaviour modification versus LAMA and behaviour modification
The mean difference in step count was 471 steps (95% CI −422 to 1364) after eight weeks and 1241 steps (95% CI 370 to 2112) at end intervention following a 12‐week study of LABA with LAMA and behaviour modification compared to LAMA and behaviour modification (Troosters 2018; 8 weeks: 122 participants; 12 weeks: 116 participants; moderate‐certainty evidence; Analysis 3.35). The mean difference in walking time was 4 minutes (5%CI −6 to 13) after eight weeks and 11 minutes (95% CI 2 to 21) at end intervention (Troosters 2018; 8 weeks: 122 participants; 12 weeks: 117 participants; moderate‐certainty evidence; Analysis 3.36). The mean difference in walking intensity was 0.04 m/s2 (95% CI −0.04 to 0.12) after eight weeks and 0.08 m/s2 (95% CI −0.00 to 0.16) at end intervention (Troosters 2018; 8 weeks: 122 participants; 12 weeks: 114 participants; moderate‐certainty evidence; Analysis 3.37).
3.35. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 35 step count (steps per day); Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
3.36. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 36 time walking (minutes per day); Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
3.37. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 37 walking intensity (m/s2); Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
Angiotensin‐converting enzyme (ACE) inhibitor with pulmonary rehabilitation versus placebo with pulmonary rehabilitation
The mean difference in change in step count was −943 steps (95% CI −2372 to 486) following a 10‐week study of an ACE inhibitor and pulmonary rehabilitation compared to a placebo and pulmonary rehabilitation. A deterioration in PAL was demonstrated in the ACE inhibitor group (MD −0.10, 95% CI −0.20 to −0.00; Curtis 2016, 40 participants; moderate‐certainty evidence; Table 2).
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Inhaled corticosteroid and LABA versus inhaled corticosteroid and LABA
The mean difference in step count was 316 steps (95% CI −838 to 1470) following a 12‐week study of inhaled corticosteroid (beclomethasone) and LABA compared to inhaled corticosteroid (budesonide) and LABA (NCT01351792, 59 participants; very low‐certainty evidence; Table 2).
LAMA versus LAMA
No data were presented in an eight‐week study of LAMA (aclidinium bromide) compared to LAMA (tiotropium; Nakamura 2016, 44 participants; very low‐certainty evidence; Table 2).
INTERVENTION: Nutritional supplementation
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Nutritional supplement versus no intervention
The mean difference in PAL was 0.02 (95% CI −0.04 to 0.08) after four weeks and 0.06 (95% CI −0.12 to 0.24) after 12 weeks following pulmonary rehabilitation or hospital admission for nutritional supplementation compared to no intervention (Goris 2003: 4 weeks: 20 participants; 12 weeks: 19 participants; moderate‐certainty evidence; Analysis 1.13). The mean difference in total energy expenditure was −0.6 MJ (95% CI −3.59 to 2.29) after four weeks and 0.5 MJ (95% CI −1.39 to 2.39) after 12 weeks (Goris 2003; 4 weeks: 20 participants; 12 weeks: 19 participants; moderate‐certainty evidence; Analysis 1.14).
1.13. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 13 physical activity level; Intervention: nutritional supplement.
1.14. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 14 total energy expenditure (MJ); Intervention: nutritional supplement.
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Nutritional supplement versus placebo
The mean difference in step count was 228 steps (95% CI −69 to 525) after four weeks of a 12‐week study of essential amino acid supplementation compared to placebo. An increase in step count (MD 577 steps, 95% CI 341 to 813) was demonstrated at end intervention (Dal Negro 2012, 88 participants; low‐certainty evidence; Analysis 2.5). An increase in energy expenditure for ambulation was demonstrated after four weeks (MD 0.6 kcal/step/FFM kg, 95% CI 0.3 to 1.0) and at end intervention (MD 2.3 kcal/step/FFM kg; 95% CI 1.8 to 2.8; Dal Negro 2012, 88 participants; low‐certainty evidence; Analysis 2.6).
2.5. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 5 step count (steps per day); Intervention: nutritional supplement.
2.6. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 6 energy expenditure for ambulation (kcal/step/FFM kg); Intervention: nutritional supplement.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Nutritional supplement and pulmonary rehabilitation versus placebo and pulmonary rehabilitation
The mean difference in change in step count was 719 steps (95% CI −635 to 2073) after four months of a 15‐month study of nutritional supplementation and pulmonary rehabilitation compared to a placebo and pulmonary rehabilitation in people with low muscle mass. An increase in step count was demonstrated (MD 1030 steps, 95% CI 101 to 1959) after eight months. The mean difference in step count was 796 steps (95% CI −201 to 1793; Van de Bool 2017, 61 participants; moderate‐certainty evidence; Analysis 3.38) at 15‐month follow‐up.
3.38. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 38 change in step count (steps per day); Interventions: nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation.
COMPARISON: Intervention versus intervention
No studies presented data for this comparison.
COMPARISON: Intervention versus standard common intervention (acute exacerbation of COPD)
Enriched nutritional supplement and inpatient pulmonary rehabilitation versus nutritional supplement and inpatient pulmonary rehabilitation
The mean difference in step count was 200 steps (95% CI −913 to 1313) following eicosapentaenoic acid‐enriched nutritional supplement and inpatient pulmonary rehabilitation compared to an unenriched nutritional supplement and inpatient pulmonary rehabilitation during hospital admission for an acute exacerbation of COPD. The mean difference in energy expenditure was 80 kcal (95% CI −72 to 232; Ogasawara 2018, 45 participants; low‐certainty evidence; Table 2).
INTERVENTION: Supplemental oxygen
COMPARISON: Intervention versus no intervention
No studies presented data for this comparison.
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Supplemental oxygen versus placebo
The mean difference in "domestic activity counts" was 15 (95% CI −21 to 51) following an eight‐week study of supplemental oxygen following pulmonary rehabilitation compared to placebo (Sandland 2008, 20 participants; moderate‐certainty evidence; Table 2).
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Supplemental oxygen and pulmonary rehabilitation versus sham and pulmonary rehabilitation
The mean difference in change in step count was 340 steps (95% CI −145 to 825) following eight weeks of supplemental oxygen and pulmonary rehabilitation compared to sham and pulmonary rehabilitation in people with desaturation on the six‐minute walk test (6MWT). The mean difference in change in step count was −316 steps (95% CI −865 to 233; Analysis 3.39) at six‐month follow‐up. The mean change in time in moderate‐intensity physical activity was 3 minutes (95% CI −5 to 11) at end intervention and −2 minutes (95% CI −11 to 7; Analysis 3.40) at follow‐up. The mean change in time in vigorous‐intensity physical activity was −1 minute (95% CI −3 to 1) at end intervention and −1 minute (95% CI −3 to 1; Analysis 3.41) at follow‐up. The mean change in LIPA time was −6 minutes (95% CI −35 to 23) at end intervention and −9 minutes (95% CI −41 to 23; Analysis 3.42) at follow‐up. The mean change in total energy expenditure was −59 kcal (95% CI −166 to 48) at end intervention and −4 kcal (95% CI −127 to 199; Analysis 3.43) at follow‐up. The mean change in sedentary time was 17 minutes (95% CI −28 to 62) at end intervention and 29 minutes (95% CI −25 to 75; Analysis 3.44) at follow‐up (Alison 2019: 8 weeks: 87 participants; 6 months: 65 participants; moderate‐certainty evidence).
3.39. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 39 change in step count (steps per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.40. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 40 change in time in moderate‐intensity physical activity (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.41. Analysis.
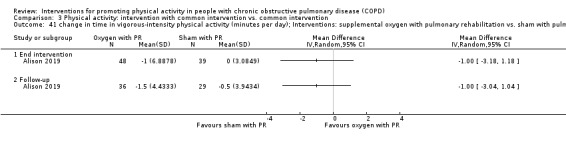
Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 41 change in time in vigorous‐intensity physical activity (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.42. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 42 change in time in light‐intensity physical activity (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.43. Analysis.
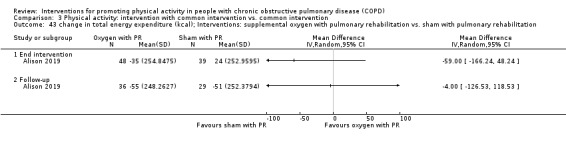
Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 43 change in total energy expenditure (kcal); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
3.44. Analysis.

Comparison 3 Physical activity: intervention with common intervention vs. common intervention, Outcome 44 change in sedentary time (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Lightweight versus standard oxygen‐cylinder use
The mean difference in "mid‐day activity" was 34 VMU/min (95% CI −23 to 91) following a six‐month study of lightweight ambulatory supplemental oxygen compared to supplemental oxygen with E‐cylinder (Casaburi 2012, 17 participants; low‐certainty evidence; Analysis 4.17).
4.17. Analysis.

Comparison 4 Physical activity: intervention vs. intervention, Outcome 17 mid day activity (vector magnitude units per minute); Interventions: supplemental oxygen (lightweight ambulatory) vs. supplemental oxygen (E‐cylinder).
INTERVENTION: Other interventions
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Four‐wheeled walker versus no intervention
An increase in step count (MD 4081 steps, 95% CI 818 to 7344) was demonstrated over four weeks following pulmonary rehabilitation using a four‐wheeled walker compared to no intervention (Ng 2015, 17 participants; very low‐certainty evidence; Table 2).
Endobronchial valve surgery versus no intervention
An increase in step count (MD 1400 steps, 95% CI 655 to 2145), proportion of time walking MD 1% (95% CI 0 to 2) and movement intensity (MD 0.01 m/s2, 95% CI 0.00 to 0.02) were demonstrated six months after endobronchial valve surgery compared to no intervention. The mean difference in the proportion of time sitting was −2% (95% CI −5 to 1) and time inactive was −1 minute (95% CI −3 to 1) after six months (Hartman 2016, 43 participants; moderate‐certainty evidence; Table 2).
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Singing versus sham intervention
A deterioration in step count (MD −1774 steps, 95% CI −2848 to −700) and activity‐related energy expenditure (MD −373 kJ, 95% CI −625 to −121) were demonstrated in the intervention group following an eight‐week singing intervention compared to a sham intervention. The mean difference in time in physical activity was −142 minutes (95% CI −263 to −22) and sedentary time was −9 minutes (95% CI −88 to 71) at end intervention (Lord 2012, 24 participants; low‐certainty evidence; Table 2).
Neuromuscular electrical stimulation versus placebo
The mean difference in step count was 36 steps (95% CI −446 to 518) at end intervention and −160 steps (95% CI −692 to 372) at 12‐week follow‐up after a six‐week neuromuscular electrical stimulation (NMES) programme compared to placebo (Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 2.7). The mean difference in change in number of up/down transitions was −5 (95% CI −12 to 3) at end intervention and −3 (95% CI −12 to 6) at 12‐week follow‐up (Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 2.8). The mean difference in upright time was 0.5 hours (95% CI −0.4 to 1.3) at end intervention and −0.4 (95% CI −1.2 to 0.4) at 12‐week follow‐up (Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 2.9).
2.7. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 7 change in step count (steps per day); Intervention: neuromuscular electrical stimulation.
2.8. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 8 change in up/down transitions (number); Intervention: neuromuscular electrical stimulation.
2.9. Analysis.

Comparison 2 Physical activity: intervention vs. placebo/sham, Outcome 9 change in time upright (hours); Intervention: neuromuscular electrical stimulation.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Non‐invasive ventilation with pulmonary rehabilitation versus pulmonary rehabilitation
An increase in step count was demonstrated (MD 1269 steps, 95% CI 242 to 2296; Duiverman 2008, 56 participants; moderate‐certainty evidence; Table 2) following a 12‐week study of non‐invasive ventilation with pulmonary rehabilitation compared to pulmonary rehabilitation in people with hypercapnia.
Inspiratory muscle training and pulmonary rehabilitation versus sham and pulmonary rehabilitation
The mean difference in step count was −206 steps (95% CI −923 to 512; Charususin 2018, 150 participants; moderate‐certainty evidence; Table 2) following a 12‐week study of the addition of inspiratory muscle training to pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation in people with inspiratory muscle weakness.
COMPARISON: Intervention versus intervention
No studies presented data for this comparison
Subgroup analysis and investigation of heterogeneity
Insufficient data were available to perform subgroup analyses according to disease severity or duration of intervention.
Subgroup analyses were possible for supervised versus unsupervised pulmonary rehabilitation programmes in clinically‐stable COPD for the following physical activity outcomes: step count; total energy expenditure; LIPA time; and total sedentary time.
Pulmonary rehabilitation: supervised versus unsupervised
The mean difference in step count in the supervised subgroup was 69 steps (95% CI −386 to 524; 2 studies, 144 participants) and unsupervised subgroup was 494 steps (95% CI −158 to 1146; Tsai 2016, 36 participants; low‐certainty evidence; test for subgroup differences: P = 0.29; Analysis 1.15).
1.15. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 15 subgroup analysis (supervised vs. unsupervised); change in step count (steps per day); Intervention: pulmonary rehabilitation/exercise training.
There was a significant difference (P = 0.02) between the supervised (MD 10 minutes, 95% CI −9 to 29; 2 studies, 146 participants) and unsupervised subgroups (MD −44 minutes, 95% CI −87 to −1; Tsai 2016, 36 participants; Analysis 1.16), but there was substantial heterogeneity within the supervised subgroup (I2 = 64%) and between subgroups (I2 = 80%).
1.16. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 16 supgroup analysis (supervised vs. unsupervised); change in time in light‐intensity physical activity (minutes per day); Intervention: pulmonary rehabilitation/exercise training.
The mean difference in total energy expenditure in the supervised subgroup was −47 kcal (95% CI −99 to 5; Wootton 2017, 108 participants) and in the unsupervised subgroup was −5 kcal (95% CI −139 to 129; Tsai 2016, 36 participants; low‐certainty evidence; test for subgroup differences: P = 0.57; Analysis 1.17).
1.17. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 17 subgroup analysis (supervised vs. unsupervised); change in total energy expenditure (kcal); Intervention: pulmonary rehabilitation/exercise training.
The mean difference in total sedentary time in the supervised subgroup was 3 minutes (95% CI −49 to 55; Wootton 2017, 101 participants) and in the unsupervised subgroup was 50 minutes (95% CI −31 to 131; Tsai 2016, 36 participants; low‐certainty evidence; test for subgroup differences: P = 0.34; Analysis 1.18).
1.18. Analysis.

Comparison 1 Physical activity: intervention vs. no intervention, Outcome 18 subgroup analysis (supervised vs. unsupervised); change in sedentary time (minutes per day); Intervention: pulmonary rehabilitation/exercise training.
Sensitivity analysis
We considered physical activity as the appropriate outcome for sensitivity analyses, as it was the prespecified primary outcome for the review. Insufficient data were available to perform sensitivity analyses to examine the effects of the measurement device on the pooled estimate by removing studies that used pedometers. Sensitivity analyses for missing data were not required.
We planned to examine the effects of methodological quality on the pooled estimate by removing studies that were at high or unclear risk of bias for the domains of blinding and incomplete outcome data.
Sensitivity analyses could be considered for three comparisons in clinically‐stable COPD: pulmonary rehabilitation versus no intervention; high‐intensity interval training versus no intervention; and LAMA/LABA versus placebo.
Pulmonary rehabilitation versus placebo
For change in step count, sensitivity analyses for blinding were not possible as all three included studies were at high/unclear risk of bias for the domain of blinding of participants and at low risk of bias for the domain of blinding of personnel (Egan 2010; Tsai 2016; Wootton 2017). Following the removal of the two studies at unclear risk of bias for the domain of incomplete outcome data (Egan 2010; Wootton 2017), the mean difference was 494 steps (95% CI −158 to 1146; Tsai 2016; 36 participants; low‐certainty evidence; Analysis 1.1).
For total physical activity time, sensitivity analyses for were not possible as both included studies were at high/unclear risk of bias for the domains of blinding of participants and personnel (Egan 2010; De Roos 2017). Following removal of the one study at unclear risk of bias for the domain of incomplete outcome data (Egan 2010), an improvement in total physical activity time was also demonstrated (MD 25 min, 95% CI 8 to 43; De Roos 2017, 45 participants; moderate‐certainty evidence; Analysis 1.5).
Sensitivity analyses were not possible for blinding of participants and personnel for time in MVPA (Analysis 1.2), time in LIPA (Analysis 1.3), total energy expenditure (Analysis 1.4) or total sedentary time (Analysis 1.6), as all included studies were at high/unclear risk of bias for these domains (De Roos 2017; Tsai 2016; Wootton 2017). Following the removal of the one study at unclear risk of bias for the domain of incomplete outcome data (Wootton 2017), the mean difference in time in MVPA was 5 minutes (95% CI −1 to 11; 2 studies; 81 participants; low‐certainty evidence; Analysis 1.2), the mean difference in time in LIPA was −9 minutes (95% CI −70 to 52; 2 studies; 81 participants; low‐certainty evidence; Analysis 1.3), the mean difference in total energy expenditure was −5 kcal (95% CI – 139 to 129; Tsai 2016; 36 participants; low‐certainty evidence; Analysis 1.4) and the mean difference in total sedentary time was – 50 minutes (95% CI –31 to 131; Tsai 2016; 36 participants; low‐certainty evidence; Analysis 1.6).
High‐intensity interval training versus placebo
Sensitivity analyses were not possible for blinding of participants and personnel or incomplete outcome data for time in “lifestyle” physical activity (Analysis 1.7), time in LIPA (Analysis 1.8), time in MVPA (Analysis 1.9) or sedentary time (Analysis 1.10), as both included studies were at high/unclear risk of bias for these domains (Louvaris 2016; Vasilopoulou 2017).
LAMA/LABA versus placebo
Sensitivity analyses were not possible for blinding of participants and personnel or incomplete outcome data for change in step count (Analysis 2.2), time in MVPA (Analysis 2.3) or active energy expenditure (Analysis 2.4), as both included studies were at low risk of bias for these domains (Watz 2016; Watz 2017).
Discussion
This review has synthesised the available evidence for interventions that have measured physical activity and sedentary behaviour in people with COPD. The complexity of a behaviour like physical activity (Casperson 1985) was reflected in the wide range of interventions that have been used to date (Table 7).
Summary of main results
Pulmonary rehabilitation/exercise training
Despite documented deterioration in physical activity associated with acute exacerbations of COPD (Pitta 2006a), there has been limited work targeting participation for people with COPD at this vulnerable time. To date, no improvements in physical activity have been demonstrated following inpatient exercise training (Borges 2014; Tahirah 2015), enriched nutritional supplementation during inpatient pulmonary rehabilitation (Ogasawara 2018), short‐term self‐management post‐discharge (Kanabar 2015; Orme 2018) or long‐term health coaching (Benzo 2016). This remains a key area of interest for future work.
Pulmonary rehabilitation represents the most widely‐studied intervention to improve physical activity to date. Findings in this review were consistent with clinically‐important and consistent improvements in health‐related quality of life and exercise capacity previously demonstrated across multiple trials (McCarthy 2015). However, translation of these benefits into improvement in physical activity was not clearly demonstrated. The appeal of using an existing intervention framework in an attempt to improve physical activity is clear. However, the addition of specific strategies underpinned by theoretical constructs to support behaviour change for physical activity is likely to be required. Meta‐analyses revealed only an increase in total physical activity time following pulmonary rehabilitation, which was not undesirable, but not consistent with the increased intensity required to meet physical activity recommendations for improving health (WHO 2010).
Specific treatments for components of COPD have been added to pulmonary rehabilitation in attempts to improve physical activity with varying success. No clear benefits for physical activity were evident with the addition of inspiratory muscle training in people with inspiratory muscle weakness (Charususin 2018), and results numerically favoured the placebo group in a study looking at the addition of an ACE‐inhibitor (Curtis 2016), although the confidence interval was wide. No clear benefit of supplemental oxygen was demonstrated in participants who desaturated during 6MWT (Alison 2019). However, increased step count was demonstrated following the addition of non‐invasive ventilation in people with hypercapnia (Duiverman 2008) and nutritional supplementation in people with low muscle mass (Van de Bool 2017).
Alternatives to pulmonary rehabilitation/exercise training programmes have been investigated in a range of single studies, including home‐based pulmonary rehabilitation (Holland 2017), water‐based exercise training (Felcar 2018), low‐intensity exercise training (Probst 2011), an exercise‐training programme with tapering supervision (Rinaldo 2017), outdoor walking (Gamper 2019), and an adherence intervention (Steele 2019), without improvements demonstrated. Improvement in physical activity has been demonstrated in a study of Tai Chi compared to pulmonary rehabilitation and was accompanied by improvements in health‐related quality of life and exercise capacity (Polkey 2018). Two studies assessed the impact of adding alternative models of exercise interventions to other components of pulmonary rehabilitation programmes (Nordic walking, COPE‐active) and also demonstrated improved physical activity alongside improved clinical outcomes (Breyer 2010; Effing 2011). At this stage, it appears that there are other exercise‐based interventions that may be equally (if not more) effective in improving physical activity compared to conventional pulmonary rehabilitation/exercise training programmes.
Use of a high‐intensity interval training protocol delivered improvements in physical activity in association with health‐related quality of life and exercise capacity at programme completion in two studies from the same group (Louvaris 2016; Vasilopoulou 2017). Mechanisms for these observed changes are yet to be clarified, longer‐term outcomes have not been demonstrated and results need to be replicated in other studies prior to recommendations for clinical practice.
The only study that has looked at two models of maintenance exercise programmes following high‐intensity interval training demonstrated that both telerehabilitation and centre‐based programmes were superior to usual care across a range of physical activity variables; these findings were mirrored by improvements in health‐related quality of life and exercise capacity. Comparing telerehabilitation and centre‐based maintenance to each other, there were no differences in health‐related quality of life, exercise capacity, time spent in light‐intensity physical activity or sedentary time, but lifestyle and moderate‐intensity physical activity were better in the centre‐based group (Vasilopoulou 2017). These results indicate a direction for the development of effective and sustainable interventions.
Physical activity counselling
Improvements in physical activity following physical activity counselling were inconsistently demonstrated, with a wide range of programme durations, participant interfaces and intervention components used (Arbillaga‐Etxarri 2018; Demeyer 2017; Hornikx 2015; Tabak 2014a; Vorrink 2016; Wootton 2017). The identification of effective components of interventions was complex. In some cases, clues to successful implementation were evident where the same intervention applied in different populations demonstrated (short‐term) improvements in step count that were mirrored by improvements in other outcomes in people with more severe disease (Altenburg 2015; Hospes 2009). Several features were shared with other successful interventions (Demeyer 2017; Vorrink 2016), where participants received direct feedback from a step counter, tracking of participation in activity as well as individual goal‐setting that was regularly revised. This was supported by some evidence specifically for the addition of a pedometer to physical activity counselling to increase step count (Mendoza 2015); however, evidence for the addition of physical activity counselling to use of a pedometer was less clear (Bender 2016; Moy 2015a; Nguyen 2009; Wan 2017). The components associated with success to date were not clearly linked to models of delivery or uniformly accompanied by improvements in health‐related quality of life or exercise capacity or both, but offer may merit further exploration.
Physical activity counselling and pulmonary rehabilitation/exercise training
Direct comparison of physical activity counselling with pulmonary rehabilitation was only undertaken in two studies. Whilst one compared interventions of equal duration (six weeks; Widyastuti 2018), the other compared a longer counselling programme (12 weeks) to pulmonary rehabilitation (six weeks; O'Neill 2018). The addition of physical activity counselling to pulmonary rehabilitation has been the subject of numerous studies. However, meta‐analyses were not possible due to diversity in trial designs. Whilst negative studies showed a lack of improvement in physical activity and clinical outcomes (Burtin 2015; De Blok 2006; Nolan 2017), positive results for physical activity were variably accompanied by improvements in health‐related quality of life and exercise capacity (Loeckx 2018; Mantoani 2018) or unaccompanied by these (Altenburg 2015; Cruz 2016; Kawagoshi 2015), maintained at follow‐up (Cruz 2016; Loeckx 2018) or not maintained (Altenburg 2015). One study has demonstrated that the combined addition of physical activity counselling and exercise training to use of a pedometer resulted in improvements in step count, health‐related quality of life and exercise capacity that were maintained at 12‐month follow‐up (Varas 2018), which provided a constructive indicator for programme development, suggesting that multifaceted interventions may be required for long‐term success.
Self‐management
Several shorter‐term self‐management interventions demonstrated some improvements in physical activity at end intervention compared to no intervention (Mitchell 2013; Tabak 2014b), as did education‐based alternatives (Blumenthal 2014; Larson 2014). These improvements were not seen in longer studies (Jolly 2018; Schuz 2015), which may reflect the challenge of longer‐term maintenance of this type of behaviour change.
Pharmacological treatments
There was mostly a lack of evidence for improvements in physical activity following LAMA treatment (Beeh 2014; Magnussen 2017). However, there was some evidence for a short‐term increase in step count and active energy expenditure following LAMA/LABA combination treatment (Watz 2016; Watz 2017). In the multiple comparisons of one study in which all groups received behaviour modification, no comprehensive improvements in physical activity were demonstrated with the addition of LAMA, LAMA/LABA or exercise training in any combination over 12 weeks (Troosters 2018). These results suggest that meaningful change in and long‐term adoption of regular participation in physical activity will require specific strategies targeting the behaviour of interest.
Endobronchial valve surgery
In one study assessing people six months after endobronchial valve surgery, expected improvement in exercise capacity was accompanied by improvement in a range of physical activity measures, but not measures of inactivity (Hartman 2016), which adds further evidence to the concept that improving physical capacity does not naturally result in comprehensive behaviour change.
Overall completeness and applicability of evidence
Study design
Of the 76 studies included, only 38 had physical activity as a primary outcome. In the context of the myriad of disparate interventions included in this review preventing meta‐analyses for most comparisons, findings were largely presented from individual studies. As a result, whether studies were sufficiently powered presents an important consideration.
Additionally, protocols for activity monitor‐wearing time resulted in fewer participants completing physical activity outcome assessments than health‐related quality of life or exercise‐capacity measures. Only 17 studies assessed physical activity after a post‐intervention follow‐up period, of which four studies demonstrated maintained improvements, so there was very limited information about the continued effect over time following interventions.
Methodology
A lack of comprehensive descriptions of interventions, particularly for physical activity counselling and exercise‐training interventions, and a paucity of data for adherence also made it difficult to know whether interventions were delivered as intended and therefore limited the identification of effective treatment components. The evolution of behaviour change theory and identification of critical components deployed in the development of interventions post‐dates some of this work (Michie 2013); future studies should provide sufficient detail to enable replication and implementation.
Devices
Rapid technological developments have led to a broad and ever‐growing range of tools being used within this field of practice. The most commonly‐used device to date (SenseWear Armband, 19 studies) is now obsolete, and the inaccuracy of step‐count data from this device has been documented (Lee 2015). Financial considerations will inevitably factor into decisions about device selection, both in research settings and in clinical practice. However, the accuracy of data generated by different devices in people with COPD warrants consideration. Although we could not conduct sensitivity analyses as planned according to pedometer use, it is worth noting that a quarter of the studies in this review (15 studies) assessed step count using pedometers, despite evidence for poor accuracy at slower gait speeds (Furlanetto 2010). The impact of device selection on step count was highlighted in the results of Nolan 2017, who demonstrated different results for pedometer‐assessed step count compared to another device.
Outcomes
Step count was the most commonly‐assessed outcome (54 studies), followed by MVPA time (23 studies), sedentary time (12 studies) and LIPA time (10 studies). One challenge with synthesis of these variables was the variety and, in many cases, lack of specification of threshold values used to define intensity of activity. A range of wearing protocols were used and details about data handling were not routinely specified. In some cases, it appeared that post‐intervention physical activity was assessed prior to completion (i.e. whilst participants were still undertaking the intervention).
Due to the small number of interventions that improved physical activity, it was not possible to evaluate whether improvements in physical activity were consistently accompanied by improvements in our secondary outcomes of health‐related quality of life or exercise capacity.
Other factors
To date, there has not been widespread regard for personal factors beyond disease, physical or physiological features. Given the complexity of physical activity behaviour, factors such as motivation, readiness to change and self‐efficacy are also likely to contribute to capacity to change physical activity, and therefore should be integrated into future design of interventions (Trost 2002).
Certainty of the evidence
In assessments of the quality of the evidence, most results were of low certainty, which was largely attributable to performance bias and imprecision. As expected, inclusion of studies that assessed physical activity objectively largely resulted in low risk of detection bias for physical activity outcomes. However, it is interesting to note that there were still instances where use of a device was subject to bias where participants were required to self‐report daily measures. The nature of many interventions, including exercise training and physical activity counselling, will inevitably limit the capacity to blind participants to group allocation. This places more importance on the role of blinding outcome assessors for other outcomes such as exercise capacity. It is therefore concerning that we rated only 33 studies at low risk of bias for this domain. Another common observation was the frequency with which physical activity outcomes were not identified or were reported in a different manner to prespecified protocols.
Potential biases in the review process
Data extraction and 'Risk of bias' assessments were undertaken independently by two review authors, with clarification sought from other co‐authors as required. The inclusion of data published only in conference abstracts ensured that we included all available data in the review. We sought additional information from 29 study authors to maximise accuracy of 'Risk of bias' assessment and data for inclusion, 21 of whom provided information (Characteristics of included studies).
Characteristics of the available data limited the application of prespecified analyses in this review, but it is likely that future versions will encompass these.
Use of cross‐over study designs provides a challenge to inclusion where behavioural components to interventions are delivered. Despite the best efforts of co‐operating authors, there were studies from which we could not obtain data that may have influenced estimates.
Cochrane Reviews often define study inclusion and exclusion criteria based on interventions; however, this review defined study criteria based on an outcome (objectively‐assessed physical activity). In this relatively new field of measurement of this complex behaviour, it is as yet unclear which interventions clearly demonstrate benefit, and therefore inclusion of any approach was intended to inform a comprehensive review of available data.
Agreements and disagreements with other studies or reviews
Previously, the two most comprehensive reviews of interventions to promote physical activity in people with COPD were conducted by Mantoani 2016 (to March 2015; 60 studies), and Lahham 2016 (to May 2016; 37 studies). Consistent with this review, both reviews noted poor quality of available evidence. Study inclusion criteria for our review restricted studies to those assessing physical activity objectively and to RCTs, where both previous reviews had included subjective assessment and Mantoani 2016 included non‐randomised, cohort and experimental designs. Previous observations about duration of pulmonary rehabilitation/exercise training relating to increased physical activity could not be substantiated in this review, however preliminary evidence for combined interventions (e.g. physical activity counselling and pulmonary rehabilitation/exercise training) was confirmed by these results. However, preservation of the original units of outcomes for analysis (e.g. number of steps, time in physical activity rather than effect sizes), rigour of inclusion criteria, a rapidly‐evolving area of clinical interest and concomitant increase in the number of papers have resulted in a unique body of evidence for the current review.
Authors' conclusions
Implications for practice.
Awareness is rapidly progressing of the importance of increasing physical activity and decreasing sedentary behaviour for health outcomes. This is reflected in our understanding of the magnitude of the challenge for people with COPD to achieve the necessary behaviour changes. A diverse range of interventions have been assessed, mostly in single studies, but improvements have not been systematically demonstrated following any particular interventions. There was limited evidence for improvement in physical activity with strategies including exercise training, physical activity counselling, self‐management, pharmacological interventions and endobronchial valve surgery, and in specific subgroups following nutritional supplementation and non‐invasive ventilation. Where improvements were demonstrated in activity of at least moderate intensity, as recommended by guidelines (U.S. Department of Health and Human Services 2018), they were of relatively small magnitude. Compared to no intervention, high‐intensity interval training did demonstrate an improvement of six minutes per day (Table 1) and physical activity counselling did demonstrate an improvement of 11 minutes per day (Table 4) after eight‐ to 12‐week studies. Similarly, three to four weeks of LAMA/LABA resulted in an improvement of 10 minutes per day (Table 6). The greatest improvement was 24 minutes per day after a six‐month study of physical activity counselling in addition to pulmonary rehabilitation in one study of 26 participants; this finding is at odds with similar studies (Table 4). These improvements were mirrored in the assessment of other physical activity outcomes.
Overall, assessment of quality was limited by a lack of methodological detail. The optimal timing, components, duration and models for interventions are still unclear. There was scant evidence for a continued effect over time following completion of interventions, a likely requirement for meaningful health benefits for people with COPD.
Implications for research.
This review does not indicate one clear path forward, but does signal that optimisation of pharmacological management and physical function, as well as compliance with COPD care guidelines, may have an additional role in conjunction with physical activity counselling strategies. Future research should consider the design of interventions that are based on behaviour change constructs, with follow‐up of physical activity outcomes after programme completion. Physical activity variables should be prospectively identified (ideally in a trial registry or published protocol) and reported accordingly. Outcomes should be selected according to intervention objectives, and consideration should be given to opportunities to inform longer‐term cardiometabolic risk factor mitigation. Device outputs should align with the outcomes of interest (for example, using a validated device for step count in an intervention targeting increasing walking towards a step count goal) and wear‐time protocols optimised to ensure data accuracy. A comprehensive description of intervention design and delivery, as well as physical activity data processing details, will be essential to move this field forward, particularly in the context of technological advancements.
Acknowledgements
We thank Elizabeth Stovold from the Cochrane Airways Group for her help with developing the search strategy.
We based the Background and Methods sections of this review on a standard template used by Cochrane Airways.
The authors and Airways Editorial Team are grateful to the following peer and consumer reviewers for their time and comments:
Andy Coles (consumer reviewer); Dr Kylie Hill, Curtin University, Australia; Marlies Zwerink, Medisch Spectrum Twente, the Netherlands; Dr Rachael Evans, University of Leicester, UK.
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding to the Cochrane Airways Group. The views and opinions expressed therein are those of the protocol authors and do not necessarily reflect those of the Systematic Reviews Programme, the NIHR, the NHS, or the Department of Health.
Angela Burge was the recipient of the Lung Foundation Australia/Cochrane Airways Australia Scholarship (2018).
We thank all authors who responded to requests for additional information, particularly Henrik Watz.
Appendices
Appendix 1. Sources and search methods for the Cochrane Airways Trials Register
Electronic searches: core databases
| Database | Dates searched | Frequency of search |
| CENTRAL (via the Cochrane Register of Studies (CRS)) | From inception | Monthly |
| MEDLINE (Ovid SP) | 1946 onwards | Weekly |
| EMBASE (Ovid SP) | 1974 onwards | Weekly |
| PsycINFO (Ovid SP) | 1967 onwards | Monthly |
| CINAHL (EBSCO) | 1937 onwards | Monthly |
| AMED (EBSCO) | From inception | Monthly |
Handsearches: core respiratory conference abstracts
| Conference | Years searched |
| American Academy of Allergy, Asthma and Immunology (AAAAI) | 2001 onwards |
| American Thoracic Society (ATS) | 2001 onwards |
| Asia Pacific Society of Respirology (APSR) | 2004 onwards |
| British Thoracic Society Winter Meeting (BTS) | 2000 onwards |
| Chest Meeting | 2003 onwards |
| European Respiratory Society (ERS) | 1992 onwards |
| International Primary Care Respiratory Group Congress (IPCRG) | 2002 onwards |
| Thoracic Society of Australia and New Zealand (TSANZ) | 1989 onwards |
MEDLINE search strategy
COPD search
1. Lung Diseases, Obstructive/
2. exp Pulmonary Disease, Chronic Obstructive/
3. emphysema$.mp.
4. (chronic$ adj3 bronchiti$).mp.
5. (obstruct$ adj3 (pulmonary or lung$ or airway$ or airflow$ or bronch$ or respirat$)).mp.
6. COPD.mp.
7. COAD.mp.
8. COBD.mp.
9. AECB.mp.
10. or/1‐9
Filter to identify RCTs
1. exp "clinical trial [publication type]"/
2. (randomised or randomised).ab,ti.
3. placebo.ab,ti.
4. dt.fs.
5. randomly.ab,ti.
6. trial.ab,ti.
7. groups.ab,ti.
8. or/1‐7
9. Animals/
10. Humans/
11. 9 not (9 and 10)
12. 8 not 11
(The MEDLINE strategy and RCT filter (Lefebvre 2011) are adapted to identify trials in other electronic databases.)
Appendix 2. Search strategy to identify relevant trials from the Cochrane Airways Trials Register and CENTRAL
Searched through the Cochrane Register of Studies (CRS)
#1 MeSH DESCRIPTOR Pulmonary Disease, Chronic Obstructive Explode All
#2 MeSH DESCRIPTOR Bronchitis, Chronic
#3 (obstruct*) near3 (pulmonary or lung* or airway* or airflow* or bronch* or respirat*)
#4 COPD:MISC1
#5 (COPD OR COAD OR COBD OR AECOPD):TI,AB,KW
#6 #1 OR #2 OR #3 OR #4 OR #5
#7 MeSH DESCRIPTOR Motor Activity
#8 MeSH DESCRIPTOR Exercise Test
#9 MeSH DESCRIPTOR Ergometry
#10 MeSH DESCRIPTOR Activities of Daily Living Explode All
#11 MeSH DESCRIPTOR Energy Metabolism
#12 MeSH DESCRIPTOR Exercise Tolerance
#13 MeSH DESCRIPTOR Walking
#14 MeSH DESCRIPTOR Monitoring, Ambulatory
#15 MeSH DESCRIPTOR Actigraphy
#16 MeSH DESCRIPTOR Physical Fitness
#17 physical* NEXT activity*
#18 pedometer*
#19 accelerometer*
#20 activity NEXT monitor*
#21 step* NEXT count*
#22 activity NEAR3 (monitor* or count* or level*)
#23 energy NEXT expenditure
#24 walking NEAR distance*
#25 (physical* OR activity or exercise* or rehabilitat* or life‐style*) NEAR3 (counselling* or feedback* or program* or coach* or increase* or improve* or modif* or promot* or advice*)
#26 #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25
#27 #6 and #26
[in search line #4, MISC1 denotes the field in the record where the reference has been coded for condition, in this case, COPD]
Appendix 3. Search strategy for ClinicalTrials.gov and the WHO trials portal
| Field | Search terms |
| Condition | COPD |
| Intervention | physical activity OR pedometer OR accelerometer OR step count OR activity monitor OR walking |
| Study type | Interventional |
Appendix 4. Secondary outcome: health‐related quality of life
Health‐related quality of life (HRQOL) was reported in 65 studies.
INTERVENTION: Pulmonary rehabilitation/exercise training
COMPARISON: Intervention versus no intervention (clinically stable COPD)
Pulmonary rehabilitation versus no intervention
Improvements in HRQOL were demonstrated following pulmonary rehabilitation compared to no intervention. A reduction in St George's Respiratory Questionnaire (SGRQ) total score (MD −9, 95% CI −14 to −4; 2 studies, 144 participants; moderate‐certainty evidence; Analysis 5.1) was demonstrated, and substantial heterogeneity (I2 = 61%) was evident. Reductions in SGRQ activity (MD −6, 95% CI −10 to −2) and impacts domain scores (MD −6, 95% CI −11 to −1) were demonstrated following ground‐based walking training compared to no intervention. The mean difference in the symptoms domain was −2 (95% CI −8 to 4; Wootton 2017, 101 participants; low‐certainty evidence; Analysis 5.2). An improvement in Chronic Respiratory Disease Questionnaire (CRQ) total score was demonstrated (MD 1.7, 95% CI 2.6 to 10.9; 3 studies, 182 participants; moderate‐certainty evidence; Analysis 5.3). Improvements in CRQ dyspnoea (MD 1.7, 95% CI 0.02 to 3.4) and emotional function domain scores (MD 2.4, 95% CI 0.5 to 4.4) were demonstrated (3 studies, 182 participants; moderate‐certainty evidence; Analysis 5.3). The mean difference in the fatigue domain score was 1.3 (95% CI −0.2 to 2.8) and mastery domain score was 0.6 (95% CI −0.5 to 1.7; 3 studies, 182 participants; low‐certainty evidence; Analysis 5.3). The mean difference in change in COPD Assessment Test (CAT) score was −0.3 (95% CI −7 to 0; Tsai 2016, 36 participants; low‐certainty evidence; Table 20) following telerehabilitation compared to no intervention.
5.1. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 1 change in SGRQ total score; Intervention: pulmonary rehabilitation/exercise training.
5.2. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 2 change in SGRQ domain scores. Intervention: pulmonary rehabilitation/exercise training (ground‐based walking).
5.3. Analysis.
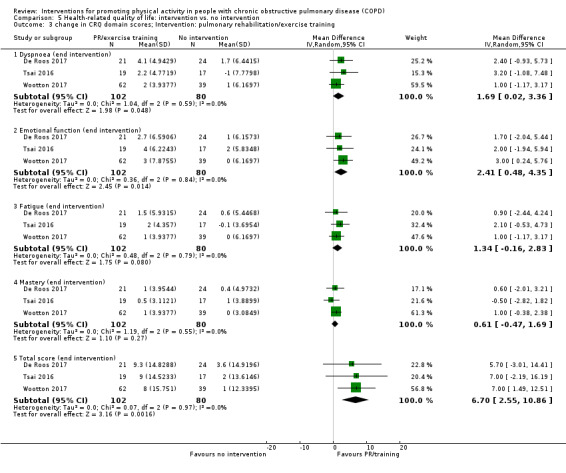
Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 3 change in CRQ domain scores; Intervention: pulmonary rehabilitation/exercise training.
3. Health‐related quality of life outcomes.
| Study |
Comparison (setting, if known) Clinical stability unless indicated |
Timepoint (end intervention unless indicated) | Outcome (score unless indicated) | Intervention group | Comparison group | Between‐group MD (95% CI) where available unless indicated | ||
| n | mean (95% CI) unless indicated | n | mean (95% CI) unless indicated | |||||
| Altenburg 2015 | Physical activity counselling vs. no intervention (primary care) | 12 weeks | ∆ CRQ total | 22 | median 2 (IQR −3 to 7) | 18 | median 5 (IQR −3 to 15) | P = 0.398* |
| ∆ CCQ total | median −0.1 (IQR −0.4 to 0.1) | median −0.1 (IQR −0.4 to 0.3) | P = 0.606* | |||||
| follow‐up (12 months post‐intervention) | ∆ CRQ total | 20 | median 2 (IQR −3 to 14) | 18 | median 13 (IQR −1 to 15) | P = 0.278* | ||
| ∆ CCQ total | median −0.1 (IQR −0.5 to 0.3) | median −0.2 (IQR −0.5 to 0.1) | P = 0.536* | |||||
| Physical activity counselling vs. no intervention (secondary care) | 12 weeks | ∆ CRQ total | 21 | median 2 (IQR −6 to 11) | 22 | median −9 (IQR −14 to 1) | P = 0.006* | |
| ∆ CCQ total | median 0.0 (IQR −0.6 to 0.4) | median 0.1 (IQR −0.2 to 0.5) | P = 0.529* | |||||
| follow‐up (12 months post‐intervention) | ∆ CRQ total | 20 | median 6 (IQR −4 to 10) | 19 | median 1 (IQR −9 to 1) | P = 0.311* | ||
| ∆ CCQ total | median −0.1 (IQR −0.5 to 0.2) | median 0.2 (IQR −0.3 to 0.5) | P = 0.220* | |||||
| Physical activity counselling with PR vs. PR | 12 weeks | ∆ CRQ total | 22 | median 13 (IQR 3 to 20) | 15 | median 8 (IQR 2 to 21) | P = 0.910* | |
| ∆ CCQ total | median −1 (IQR −1 to 0.2) | median −0.2 (IQR −1 to 0.0) | P = 0.345* | |||||
| follow‐up (12 months post‐intervention) | ∆ CRQ total | 10 | median −7 (IQR −16 to 1) | 13 | median −5 (IQR −14 to 2) | P = 0.344* | ||
| ∆ CCQ total | median 0.4 (IQR 0.1 to 1) | median 0.3 (IQR −0.2 to 0.7) | P = 0.368* | |||||
| Arbillaga‐Etxarri 2018 | Urban Training™ vs. no intervention | 12 months | CCQ total | 132 | mean 1 (SD 1) | 148 | mean 1 (SD 1) | 0.1 (−0.3 to 0.1)* |
| CAT | mean 11 (7) | mean 11 (7) | 0.1 (−1.1 to 1.2)* | |||||
| Bender 2016 | Physical activity counselling with pedometer vs. pedometer | 12 weeks | ∆ CAT | 49 | x | 50 | x | x |
| ∆ SGRQ | ||||||||
| Blumenthal 2014 | Self‐management vs. education and symptom monitoring | 16 weeks | PQLS | 162 | mean 83 (SE 1) | 164 | mean 81 (SE 1) | P = 0.04* |
| SGRQ | mean 44 (SE 1) | mean 42 (SE 1) | P = 0.068* | |||||
| Chaplin 2017 | Web‐based PR vs. centre‐based PR | 7 weeks | ∆ CRQ dyspnoea domain | 22 | 0.7 (0.2 to 1.2) | 40 | 0.8 (0.8 to 0.8) | −0.1 (−0.7 to 0.5) |
| Charususin 2018 | Inspiratory muscle training with PR vs. sham with PR | 12 weeks (total n = 150) | CRQ dyspnoea domain | x | mean 20 (SD 6) | x | mean 19 (SD 7) | 0.4 (−1.1 to 2.0)* |
| CRQ emotional function domain | mean 35 (SD 9) | mean 35 (SD 8) | −0.4 (−2.4 to 1.6)* | |||||
| CRQ mastery domain | mean 21 (SD 5) | mean 19 (SD 5) | 0.01 (−1.2 to 1.2)* | |||||
| CRQ fatigue domain | mean 19 (SD 5) | mean 18 (SD 5) | 0.4 (−0.8 to 1.6)* | |||||
| CRQ total | mean 94 (SD 23) | mean 92 (SD 22) | −1.0 (−5.2 to 3.9)* | |||||
| Curtis 2016 | ACE inhibitor with PR vs. placebo with PR | 10 weeks | ∆ CAT | 31 | mean 1 (SD 4) | 34 | mean −1 (SD 3) | 2 (0 to 4) |
| Dal Negro 2012 | Nutritional supplementation vs. placebo | 12 weeks | SGRQ total | 44 | mean 69 (SD 10) | 44 | mean 73 (SD 7) | P < 0.001* |
| Demeyer 2017 | Physical activity counselling vs. no intervention | 12 weeks | ∆ CAT** | 140 | 0 (−1 to 1) | 139 | 1 (0 to 2) | −1 (−2 to 1)** |
| Duiverman 2008 | Non‐invasive ventilation with PR vs. PR | 12 weeks | MRF total (%) | 24 | mean 45 (SD 22) | 32 | mean 52 (SD 24) | −10 (−18 to 1)* |
| MRF daily activities domain (%) | mean 53 (SD 29) | mean 57 (SD 27) | −5 (−17 to 6)* | |||||
| MRF cognition domain (%) | mean 28 (SD 25) | mean 41 (SD 38) | −22 (−35 to −9)* | |||||
| MRF invalidity domain (%) | mean 57 (SD 33) | mean 62 (SD 36) | −6 (−19 to 7)* | |||||
| SRI respiratory complaints domain (%) | mean 58 (SD 13) | mean 52 (SD 17) | 6 (−1 to 12)* | |||||
| SRI physical functioning domain (%) | mean 41 (SD 21) | mean 42 (SD 18) | −2 (−10 to 5)* | |||||
| SRI attendant symptoms and sleep domain (%) | mean 71 (SD 16) | mean 60 (SD 20) | 7 (−1 to 15)* | |||||
| SRI social relationships domain (%) | mean 65 (SD 13) | mean 66 (SD 14) | 1 (−6 to 8)* | |||||
| SRI anxiety domain (%) | mean 63 (SD 17) | mean 57 (SD 22) | 3 (−5 to 11)* | |||||
| SRI well‐being domain (%) | mean 68 (SD 14) | mean 59 (SD 19) | 4 (−3 to 11)* | |||||
| SRI social functioning domain (%) | mean 54 (SD 16) | mean 54 (SD 18) | 1 (−6 to 9)* | |||||
| SRI summary (%) | mean 60 (SD 11) | mean 56 (SD 15) | 3 (−2 to 8)* | |||||
| Hartman 2016 | Endobronchial valve surgery vs. no intervention | 6 months post‐surgery | ∆ SGRQ total | 19 | mean −16 (SD 16) | 24 | mean −3 (SD 9) | MD −13 (SD 4), P = 0.0005* |
| Hornikx 2015 | Physical activity counselling vs. no intervention | 4 weeks | ∆ CAT | 12 | median −3 (IQR −10 to 1) | 15 | median −5 (IQR −7 to 1) | P = 0.78 |
| Loeckx 2018 | Physical activity counselling with PR vs. PR | 12 weeks | ∆ CRQ dyspnoea domain | 25 | x | 25 | x | MD 3 (SE 1), P = 0.04* |
| 9 months (follow‐up) | MD 3 (SE 2), P = 0.08* | |||||||
| Lord 2012 | Singing vs. sham | 8 weeks | ∆ CAT | 13 | −1 (−6 to 4) | 11 | 1 (−3 to 5) | −2 (−7 to 4) |
| Louvaris 2016 | High‐intensity interval training vs. no intervention | 12 weeks | CRQ total | 85 | mean 98.4 (SD 21.6) | 43 | mean 89.1 (SD 26.1) | 9.3 (0.3 to 18.4) |
| CCQ total | mean 2 (SD 1) | mean 2 (SD 1) | −1 (−1 to −0) | |||||
| Magnussen 2017 | LAMA vs. placebo | 3 weeks | ∆ CAT | 15 | −2 (−4 to 0) | 15 | −1 (−2 to 1) | 1 (−1 to 4)** |
| Mantoani 2018 | Physical activity counselling with PR vs. PR | 12 weeks | CAT | 22 | median 16 (IQR 8 to 20) | 22 | x | x |
| Mendoza 2015 | Pedometer with physical activity counselling vs. physical activity counselling | 12 weeks | ∆ SGRQ total | 50 | −9 (−12 to −5) | 47 | −4 (−7 to −1) | −5 (−10 to −0.4) |
| ∆ CAT | −4 (−5 to −2) | −1 (−3 to 1) | −3 (−5 to −1) | |||||
| Nakamura 2016 | LAMA (aclidinium bromide) vs. LAMA (tiotropium) | 8 weeks | SGRQ activity domain | 22 | x | 22 | x | P < 0.05* |
| NCT00144326 | LAMA vs. placebo | 12 weeks | CRQ | 123 | x | 125 | x | "no significant differences between treatments and the improvement was less than 0.5" |
| NCT01351792 | ICS (beclomethasone) with LABA (formoterol) vs. ICS (budesonide) with LABA (formoterol) | 16 weeks (4‐week run‐in, 12‐week intervention) | ∆ CCQ | 30 | mean 0.1 (SD 0.5) | 29 | mean 0.1 (SD 0.5) | 0.01 (−0.24 to 0.26) |
| Nolan 2017 | Physical activity counselling with PR vs. PR | 8 weeks (mid‐intervention, post‐PR) | ∆ CRQ fatigue domain | 63 | median 2.0 (IQR 0 to 5.0) | 59 | median 4.0 (IQR 2.0 to 6.0) | P = 0.008* |
| ∆ CRQ emotional function domain | 3.1 (1.9 to 4.4) | 5.3 (3.3 to 7.3) | −2.2 (−4.5 to 0.1) | |||||
| ∆ CRQ mastery domain | 1.8 (1.0 to 2.7) | 3.4 (2.1 to 4.7) | −1.6 (−3.1 to −0.1) | |||||
| ∆ CRQ total | median 11 (IQR 3 to 20) | median 20 (IQR 8 to 27) | P = 0.008* | |||||
| 6 months | ∆ CRQ fatigue domain | 56 | 1 (−0.3 to 2) | 57 | 2 (0.7 to 3.4) | −1.0 (−2.8 to 0.8) | ||
| ∆ CRQ emotion domain | median 0.5 (IQR −3 to 4) | 2 (−1 to 6) | P = 0.12* | |||||
| ∆ CRQ mastery | median 0.5 (IQR −1 to 3) | 2 (−2 to 5) | P = 0.29* | |||||
| ∆ CRQ total | median 3 (IQR −8 to 16) | 10 (−2 to 19) | P = 0.07* | |||||
| O'Neill 2018 | Physical activity counselling vs. PR | 12 weeks physical activity counselling, 6 weeks PR | ∆ CAT | 17 | 0.6 (95% CI −3.3 to 4.6) | 19 | −0.4 (−3.5 to 2.7) | 1.1 (−3.6 to 5.7) |
| ∆ EQ5D index | 18 | −0.0 (95% CI −0.1 to 0.1) | 0.1 (0.0 to 0.2) | −0.10 (−0.22 to 0.01) | ||||
| ∆ EQ5D visual analogue scale | 2.6 (95% CI −14.9 to 20.1) | 13.3 (−0.9 to 27.4) | −10.7 (−31.7 to 10.3) | |||||
| Orme 2018 | Feedback and education vs. no intervention | 14 days | CAT | 8 | 22 (5) | 6 | 24 (11) | −2 (−12 to 7) |
| Education vs. no intervention | 3 | 23 (14) | 6 | 24 (11) | −1 (−19 to 17) | |||
| Feedback with education vs. education | 8 | 22 (5) | 3 | 23 (14) | −1 (−17 to 15) | |||
| Ogasawara 2018 | Enriched nutritional supplement with inpatient PR vs. nutritional supplement with inpatient PR | hospital discharge | CAT | 24 | median 10 (range 2 to 27) | 21 | 10 (3 to 28) | P = 0.75* |
| Probst 2011 | Exercise training (callisthenics) vs. exercise training (endurance and strength training) | 12 weeks | SGRQ | 20 | mean 47 (SD 12) | 20 | mean 39 (SD 21) | P = 0.37* |
| Sandland 2008 | Supplemental oxygen vs. placebo (air) | 8 weeks | CRQ dyspnoea domain | 10 | median 2.2 (IQR 1.8 to 3) | 10 | median 2.5 (IQR 1.5 to 3.2) | P > 0.05* |
| CRQ emotional function domain | median 4.8 (IQR 3.2 to 5.7) | median 3.8 (IQR 2.6 to 5.6) | ||||||
| CRQ mastery domain | median 5.1 (IQR 3.2 to 5.9) | median 3.6 (IQR 2.3 to 5.0) | ||||||
| CRQ fatigue domain | median 3.4 (IQR 2.8 to 4.8) | median 3.3 (IQR 1.8 to 4.3) | ||||||
| SF36 | x | x | "no significant changes in the SF36"* | |||||
| Schuz 2015 | Self‐management (health mentoring) vs. sham | 6 months (mid‐intervention)** | SGRQ total | 59 | median 39 (IQR 23 to 54) | 81 | median 37 (IQR 29 to 58) | P = 0.439* |
| SGRQ symptoms domain | median 54 (IQR 32 to 79) | median 51 (IQR 37 to 72) | P = 0.226* | |||||
| SGRQ activities domain | median 54 (IQR 31 to 79) | median 55 (IQR 42 to 73) | P = 0.901* | |||||
| SGRQ impacts domain | median 26 (IQR 14 to 43) | median 27 (IQR 12 to 44) | P = 0.188* | |||||
| SF36 physical function domain | median 39 (IQR 30 to 47) | 82 | median 36 (IQR 26 to 47) | P = 0.212* | ||||
| SF36 role physical domain | median 46 (IQR 40 to 53) | median 46 (IQR 39 to 53) | P = 0.166* | |||||
| SF36 bodily pain domain | median 52 (IQR 38 to 63) | median 51 (IQR 38 to 63) | P = 0.205* | |||||
| SF36 general health domain | median 37 (IQR 30 to 44) | median 37 (IQR 29 to 46) | P = 0.696* | |||||
| SF36 vitality domain | median 47 (IQR 41 to 53) | median 47 (IQR 41 to 53) | P = 0.586* | |||||
| SF36 social functioning domain | median 52 (IQR 41 to 57) | median 52 (IQR 41 to 57) | P = 0.137* | |||||
| SF36 role emotional domain | median 47 (IQR 40to 55) | median 47 (IQR 40 to 55) | P = 0.088* | |||||
| SF36 mental health domain | median 50 (IQR 41 to 58) | median 50 (IQR 41 to 58) | P = 0.808* | |||||
| SF36 physical component | median 41 (IQR 33 to 48) | median 38 (IQR 32 to 47) | P = 0.917* | |||||
| SF36 mental component | median 52 (IQR 43 to 58) | median 50 (IQR 40 to 58) | P = 0.222* | |||||
| 12 months** | SGRQ total | 65 | median 42 (IQR 27 to 56) | 79 | median 41 (IQR 26 to 52) | P = 0.484* | ||
| SGRQ symptoms domain | median 57 (IQR 33 to 71) | median 47 (IQR 35 to 69) | P = 0.253* | |||||
| SGRQ activity domain | median 60 (IQR 42 to 73) | median 55 (IQR 42 to 70) | P = 0.468* | |||||
| SGRQ impacts domain | median 30 (IQR 13 to 40) | median 26 (IQR 14 to 41) | P = 0.669* | |||||
| SF36 physical function domain | 63 | median 36 (IQR 28 to 45) | median 36 (IQR 30 to 45) | P = 0.599* | ||||
| SF36 role physical domain | median 44 (IQR 39 to 51) | median 46 (IQR 40 to 53) | P = 0.354* | |||||
| SF36 bodily pain domain | median 52 (IQR 42 to 63) | median 47 (IQR 38 to 63) | P = 0.392* | |||||
| SF36 general health domain | median 36 (IQR 31 to 46) | median 38 (IQR 31 to 46) | P = 0.476* | |||||
| SF36 vitality domain | median 47 (IQR 38 to 56) | median 50 (IQR 44 to 56) | P = 0.560* | |||||
| SF36 social functioning domain | median 52 (IQR 41 to 57) | median 52 (IQR 41 to 57) | P = 0.812* | |||||
| SF36 role emotional domain | median 53 (IQR 37 to 55) | median 50 (IQR 40 to 55) | P = 0.993* | |||||
| SF36 mental health domain | median 50 (IQR 44 to 58) | median 50 (IQR 41 to 58) | P = 0.690* | |||||
| SF36 physical component | median 40 (IQR 29 to 47) | median 39 (IQR 32 to 46) | P = 0.998* | |||||
| SF36 mental component | median 52 (IQR 44 to 60) | median 52 (IQR 42 to 59) | P = 0.941* | |||||
| Steele 2019 | Adherence intervention vs. PR | 6 months (follow‐up) | SF36 physical component | 32 | mean 31 (SD 8) | 31 | mean 31 (SD 10) | 0 (−4 to 5) |
| SF36 mental component | mean 52 (SD 12) | mean 52 (SD 10) | 0 (−6 to 6) | |||||
| CCQ | mean 3 (SD 1) | mean 3 (SD 1) | 0.1 (−0.5 to 0.7) | |||||
| Tabak 2014a | Physical activity counselling with optional supervised exercise vs. optional supervised exercise | 4 weeks | ∆ CCQ total | 14 | −0.3 (−0.6 to −0.01) | 15 | 0 (−0.3 to 0.3) | −0.3 (−0.7 to 0.1)* |
| Tsai 2016 | PR (telerehabilitation) vs. no intervention | 8 weeks | ∆ CAT | 19 | −1 (−4 to 2) | 17 | 3 (1 to 5) | −3 (−7 to 0)* |
| Vasilopoulou 2017 | Maintenance (telerehabilitation) vs. no intervention | 12 months | SGRQ total | 47 | mean 38 (SD 21) | 50 | mean 50 (SD 18) | −12 (−19 to −4) |
| CAT | mean 13 (SD 7) | mean 21 (SD 7) | −8 (−11 to −5) | |||||
| Maintenance (centre‐based) vs. no intervention | SGRQ total | 50 | mean 34 (SD 17) | 50 | mean 50 (SD 18) | −16 (−23 to −10) | ||
| CAT | mean 12 (SD 6) | mean 21 (SD 7) | −9 (−12 to −7) | |||||
| Maintenance (telerehabilitation) vs. maintenance (centre‐based) | SGRQ total | 47 | mean 38 (SD 21) | 50 | mean 34 (SD 17) | 5 (−3 to 12) | ||
| CAT | mean 13 (SD 7) | mean 12 (SD 6) | 1 (−2 to 4) | |||||
| Widyastuti 2018 | Physical activity counselling vs. PR | 6 weeks | CAT | 18 | mean 11 (SD 5) | 18 | mean 9 (SD 3) | 2 (−1 to 4) |
* from paper ** from author x data not provided
ACE: angiotensin‐converting enzyme; CAT: COPD assessment test; ∆: change from baseline; CCQ: clinical COPD questionnaire; CRQ: chronic respiratory disease questionnaire; EQ5D: EuroQol 5 dimensions questionnaire; ICS: inhaled corticosteroid; IQR: interquartile range; LAMA: long‐acting muscarinic antagonist; MRF: Maugeri respiratory failure questionnaire; MD: mean differences; n: number of participants; PQLS: pulmonary‐specific quality of life scale; RAND36: Dutch translation of SF36 questionnaire; SF36: Medical Outcomes Survey 36‐item short‐form health survey questionnaire; SGRQ: St George's respiratory questionnaire; SRI: severe respiratory insufficiency questionnaire
High‐intensity interval training versus no intervention
Improvements in HRQOL were demonstrated following high‐intensity interval training compared to no intervention. An improvement in CAT total score was demonstrated (MD −3.2, 95% CI −4.8 to −1.5; 2 studies, 275 participants; moderate‐certainty evidence; Analysis 5.4). Improvements in CRQ (MD 9.3, 95% CI 0.3 to 18.4) and Clinical COPD Questionnaire (CCQ) total scores (MD −1, 95% CI −1 to −0.2; Louvaris 2016, 128 participants; moderate‐certainty evidence; Table 20) were also demonstrated following a 12‐week high‐intensity interval training intervention compared to no intervention.
5.4. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 4 CAT score; Intervention: high‐intensity interval training.
Maintenance (telerehabilitation) following high‐intensity interval training versus no intervention
Improved SGRQ total (MD −12, 95% CI −19 to −4) and CAT scores (MD −8, 95% CI −11 to −5; Vasilopoulou 2017, 97 participants; moderate‐certainty evidence; Table 20) were demonstrated following a 12‐month telerehabilitation maintenance programme compared to no intervention.
Maintenance (centre‐based) following high‐intensity interval training versus no intervention
Improved SGRQ total (MD −16, 95% CI −23 to −10) and CAT scores (MD −9, 95% CI −12 to −7; Vasilopoulou 2017, 100 participants; moderate‐certainty evidence; Table 20) were demonstrated following a 12‐month centre‐based maintenance compared to no intervention.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Nordic walking with education versus education
Improvements in HRQOL were demonstrated following a 12‐week Nordic walking programme with education compared to education alone. However, only results for Medical Outcomes Survey 36‐item short‐form health survey questionnaire (SF36) physical‐component and mental‐component scores where participants had a baseline score less than 50 were presented. Improved physical component scores (MD 10, 95% CI 5 to 14) at end intervention and six‐month follow‐up (MD 13, 95% CI 9 to 17) were demonstrated. The mean difference was 14 (95% CI −14 to 41; Breyer 2010, 53 participants; low‐certainty evidence; Analysis 7.1) at nine‐month follow‐up. The mean difference in mental component score was 6 (95% CI −3 to 14) at end intervention. Improvements were demonstrated at six‐month (MD 7, 95% CI 0 to 13) and nine‐month follow‐up (MD 8, 95% CI 1 to 14; Breyer 2010, 53 participants; low‐certainty evidence; Analysis 7.1).
7.1. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 1 SF36 component scores (score < 50); Interventions: Nordic walking with education vs. education.
Structured exercise training (COPE‐active) with self‐management versus self‐management
The mean difference in CRQ dyspnoea domain score was 0.3 (95% CI −0.0 to 0.68), emotional function domain score was 0.0 (95% CI −0.3 to 0.4), fatigue domain score was 0.1 (95% CI −0.3 to 0.6) and mastery domain score was −0.0 (95% CI −0.3 to 0.3; Effing 2011, 131 participants; low‐certainty evidence; Analysis 7.2) after seven months of an 11‐month structured exercise training programme with self‐management compared to self‐management alone. The mean difference in dyspnoea domain score was 0.3 (95% CI −0.0 to 0.7), emotional function domain score was 0.1 (95% CI −0.2 to 0.4), fatigue domain score was 0.1 (95% CI −0.3 to 0.5) and mastery domain score was 0.1 (95% CI −0.3 to 0.5; Effing 2011, 139 participants; low‐certainty‐evidence; Analysis 7.2) at end intervention. An improvement in the dyspnoea domain score (MD 0.4, 95% CI 0.0 to 0.8) was demonstrated at 18‐month follow‐up. The mean difference in emotional function domain score was 0.2 (95% CI −0.2 to 0.5), fatigue domain score was 0.1 (95% CI −0.3 to 0.6) and mastery domain score was 0.2 (95% CI −0.2 to 0.5; Effing 2011, 131 participants; low‐certainty evidence; Analysis 7.2) at 18‐month follow‐up. The mean difference in dyspnoea domain score was 0.3 (95% CI −0.1 to 0.7), emotional function domain score was 0.2 (95% CI −0.1 to 0.5), fatigue domain score was −0.0 (95% CI−0.4 to 0.4) and mastery domain score was 0.3 (95% CI −0.1 to 0.6; Effing 2011, 125 participants; low‐certainty evidence; Analysis 7.2) at 24‐month follow‐up.
7.2. Analysis.
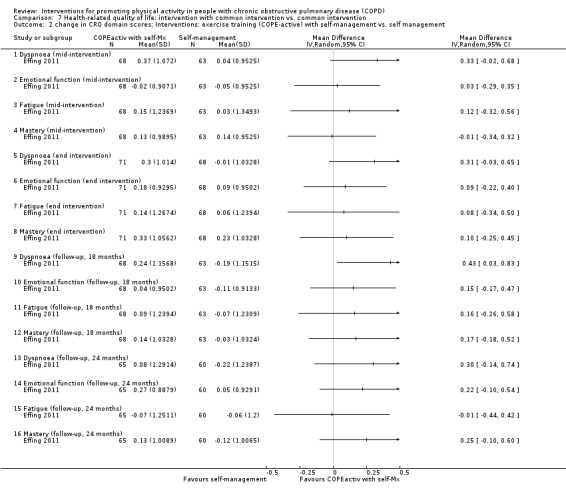
Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 2 change in CRQ domain scores; Interventions: exercise training (COPE‐active) with self‐management vs. self management.
The mean difference in CCQ symptoms domain score was 0.0 (95% CI −0.0 to 0.0) after seven months of an 11‐month structured exercise training programme with self‐management compared to self‐management alone. A deterioration in the functional state domain score (MD 0.1, 95% CI 0.0 to 0.1) and improvement in the mental state domain score (MD −0.14, 95% CI −0.19 to −0.09) were demonstrated in the intervention group after seven months. The mean difference in total score was −0.0 (95% CI −0.1 to 0.0; Effing 2011, 127 participants; low‐certainty evidence; Analysis 7.3) after seven months. The mean difference in symptom domain score was 0.1 (95% CI −0.3 to 0.4), functional state domain score was −0.1 (95% CI −0.4 to 0.2), mental state domain score was −0.0 (95% CI −0.4 to 0.3) and total score was −0.0 (95% CI −0.3 to 0.2; Effing 2011, 136 participants; low‐certainty evidence; Analysis 7.3) at end intervention. The mean difference in symptom domain score was 0.2 (95% CI −0.1 to 0.6), functional state domain score was 0.1 (95% CI −0.3 to 0.4), mental state domain score was −0.1 (95% CI −0.4 to 0.3) and total score was 0.1 (95% CI −0.2 to 0.4; Effing 2011, 129 participants; low‐certainty evidence; Analysis 7.3) at 18‐month follow‐up. The mean difference in symptom domain score was 0.3 (95% CI −0.1 to 0.7), functional state domain score was 0.2 (95% CI −0.2 to 0.5), mental state domain score was 0.0 (95% CI −0.4 to 0.4) and total score was 0.2 (95% CI −0.1 to 0.4; Effing 2011, 123 participants; low‐certainty evidence; Analysis 7.3) at 24‐month follow‐up.
7.3. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 3 change in CCQ domain scores; Interventions: exercise training (COPE‐active) with self‐management vs. self management.
Exercise training and LAMA/LABA with behaviour modification versus placebo with behaviour modification
Improvements in CRQ dyspnoea (MD 0.3, 95% CI 0.0 to 0.6) and fatigue domain scores (MD 0.5, 95% CI 0.2 to 0.8) were demonstrated after nine weeks of the 12‐week PHYSACTO study for exercise training and LAMA/LABA with behaviour modification compared to placebo with behaviour modification. The mean difference in emotional function domain score was 0.3 (95% CI 0.1 to 0.6) and mastery domain score was 0.3 (95% CI 0.0 to 0.6; Troosters 2018, 134 participants; moderate‐certainty evidence; Analysis 7.4) after nine weeks. Improvements in CRQ dyspnoea (MD MD 0.4, 95% CI 0.1 to 0.7) and fatigue domain scores (MD 0.5, 95% CI 0.2 to 0.8) were also demonstrated at end intervention. The mean difference in emotional function domain score was 0.2 (95% CI −0.1 to 0.5) and mastery domain score was 0.2 (95% CI −0.2 to 0.5; Troosters 2018, 131 participants; moderate‐certainty evidence; Analysis 7.4) at end intervention.
7.4. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 4 CRQ domain scores; Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification.
Exercise training and LABA with LAMA and behaviour modification versus LAMA and behaviour modification
An improvement in CRQ mastery domain score (MD 0.3, 95% CI 0.0 to 0.6) was demonstrated after nine weeks of the 12‐week PHYSACTO study for exercise training and LABA with LAMA and behaviour modification compared to LAMA and behaviour modification. The mean difference in the dyspnoea domain score was 0.1 (95% CI −0.2 to 0.4), emotional function domain score was 0.3 (95% CI −0.0 to 0.5) and fatigue domain score was 0.2 (95% CI −0.1 to 0.5; Troosters 2018, 136 participants; moderate‐certainty evidence; Analysis 7.5) after nine weeks. Improvements in CRQ dyspnoea (MD 0.3, 95% CI 0.0 to 0.6), fatigue (MD 0.3, 95% CI 0.0 to 0.6) and mastery domain scores (MD 0.4, 95% CI 0.1 to 0.8) were demonstrated at end intervention. The mean difference in the emotional function domain score was 0.2 (95% CI −0.1 to 0.4; Troosters 2018 132 participants; moderate‐certainty evidence; Analysis 7.5) at end intervention.
7.5. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 5 CRQ domain scores; Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
Exercise training with LAMA/LABA and behaviour modification versus LAMA/LABA and behaviour modification
The mean difference in CRQ dyspnoea domain score was −0.1 (95% CI −0.4 to 0.2), emotional function domain score was 0.1 (95% CI −0.2 to 0.3), mastery was domain score 0.1 (95% CI −0.2 to 0.4) and fatigue domain score was 0.1 (95% CI −0.2 to 0.4; Troosters 2018, 140 participants; moderate‐certainty evidence; Analysis 7.6) after nine weeks of the 12‐week PHYSACTO study for exercise training with LAMA/LABA and behaviour modification compared to LAMA/LABA and behaviour modification. The mean difference in CRQ dyspnoea domain score was 0.1 (95% CI −0.2 to 0.4), emotional function domain score was −0.1 (95% CI −0.3 to 0.2), mastery domain score was 0.0 (95% CI −0.3 to 0.4) and fatigue domain score was 0.1 (95% CI −0.2 to 0.4; Troosters 2018, 138 participants; moderate‐certainty evidence; Analysis 7.6) at end intervention.
7.6. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 6 CRQ domain scores; Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification.
Exercise training and physical activity counselling with pedometer versus pedometer
Improvements in change in the SGRQ symptoms domain score (MD −8, 95% CI −14 to −1), impacts domain score (MD −7, 95% CI −11 to −4) and total score (MD −5, 95% CI −8 to −3) were demonstrated following an eight‐week study of a physical activity counselling and exercise training programme with pedometer compared to pedometer alone. The mean difference in change in the activity domain score was −4 (95% CI −9 to 1.0; Varas 2018, 33 participants; low‐certainty evidence; Analysis 7.7) at end intervention.
7.7. Analysis.
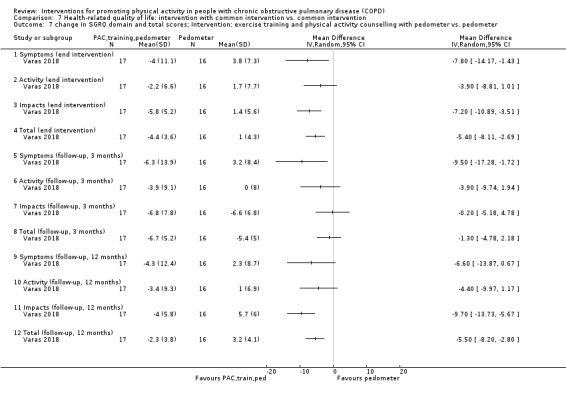
Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 7 change in SGRQ domain and total scores; Intervention: exercise training and physical activity counselling with pedometer vs. pedometer.
Improvements in change in the SGRQ symptoms domain score (MD −10, 95% CI −17 to −2) and total score (MD −1, 95% CI −5 to 2) were demonstrated at 12‐week follow‐up. The mean difference in change in the activity domain score was −4 (95% CI −10 to 2) and impacts domain score was −0 (95% CI −5 to 5; Varas 2018, 33 participants; low‐certainty evidence; Analysis 7.7) at 12‐week follow‐up.
Improvements in change in the SGRQ impacts domain score (MD −10, 95% CI −14 to −6) and total score (MD −6, 95% CI −8 to −3) were demonstrated at 12‐month follow‐up. The mean difference in change in the symptoms domain score was −7 (95% CI −14 to 1) and activity domain score was −4 (95% CI −10 to 1; Varas 2018, 33 participants; low‐certainty evidence; Analysis 7.7) at 12‐month follow‐up.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Web‐based pulmonary rehabilitation versus centre‐based pulmonary rehabilitation
The mean difference in CRQ dyspnoea domain score was −0.1 (95% CI −0.7 to 0.5; Chaplin 2017; 62 participants; low‐certainty evidence Table 20) following a seven‐week study of web‐based pulmonary rehabilitation compared to a centre‐based programme.
Home‐based pulmonary rehabilitation versus centre‐based pulmonary rehabilitation
The mean difference in CRQ dyspnoea domain score was 1.6 (95% CI −0.3 to 3.4), emotional function domain score was 0.8 (95% CI −1.4 to 3.1), fatigue domain score was 0.8 (95% CI −0.6 to 2.3) and mastery domain score was 0.4 (95% CI −1.0 to 1.8; Holland 2017, 148 participants; low‐certainty evidence; Analysis 10.1) following an equivalence study comparing an eight‐week home‐based pulmonary rehabilitation programme with a centre‐based programme. The mean difference in dyspnoea domain score was 0.1 (95% CI −2.0 to 2.1), emotional function domain score was 0.5 (95% CI −1.9 to 3.0), fatigue domain score was −0.3 (95% CI −1.8 to 1.3) and mastery domain score was 0.7 (95% CI −0.9 to 2.2; Holland 2017, 148 participants; low‐certainty evidence; Analysis 10.1) at 12‐month follow‐up.
10.1. Analysis.

Comparison 10 Health‐related quality of life: intervention vs. intervention, Outcome 1 change in CRQ domains; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
Water‐based exercise training versus land‐based exercise training
The mean difference in change in CRQ dyspnoea domain score was −2.0 (95% CI −7.8 to 3.8), emotional function domain score was −2.0 (95% CI −9.7 to 5.7), fatigue domain score was −1.0 (95% CI −5.1 to 3.1), mastery domain score was −2.0 (95% CI −6.8 to 2.8) and total score was −6.0 (95% CI −23.8 to 11.8; Felcar 2018, 36 participants; low‐certainty evidence; Analysis 10.2) after 12 weeks of a six‐month study comparing water‐based exercise training to a land‐based programme. The mean difference in change in CRQ dyspnoea domain score was −1.0 (95% CI −7.8 to 5.8), emotional function domain score was −2.0 (95% CI −8.7 to 4.7), fatigue domain score was 2.0 (95% CI −2.4 to 6.4), mastery domain score was 0.0 (95% CI −5.2 to 5.2) and total score was −1.0 (95% CI −20.1 to 18.1; Felcar 2018, 36 participants; low‐certainty evidence; Analysis 10.2) at end intervention.
10.2. Analysis.

Comparison 10 Health‐related quality of life: intervention vs. intervention, Outcome 2 change in CRQ domains; Interventions: water‐based exercise training vs. land‐based exercise training.
Tai Chi versus pulmonary rehabilitation
The mean difference in SGRQ symptoms domain score was 0 (95% CI −5 to 6), activity domain score was 1 (95% CI −6 to 7), impacts domain score was 2 (95% CI −3 to 7) and total score was 2 (95% CI −3 to 6; Polkey 2018, 110 participants; low‐certainty evidence; Analysis 10.3) after two weeks in a 24‐week study of Tai Chi compared to pulmonary rehabilitation. Improvements in SGRQ symptoms (MD 6, 95% CI 0 to 11) and impacts domain scores (MD 4, 95% CI 1 to 7) were demonstrated after 14 weeks. The mean difference in activity domain score was −1 (95% CI −6 to 5) and total score was 3 (95% CI −1 to 6; Polkey 2018, 110 participants; low‐certainty evidence; Analysis 10.3) after 14 weeks. The mean difference in SGRQ symptoms domain score was −2 (95% CI −7 to 2), activity domain score was −9 (95% CI −15 to −3), impacts domain score was 1 (95% CI −1 to 4) and total score was −2 (95% CI −6 to 1; Polkey 2018, 110 participants; low‐certainty evidence; Analysis 10.3) at end intervention.
10.3. Analysis.

Comparison 10 Health‐related quality of life: intervention vs. intervention, Outcome 3 SGRQ domain and total scores; Interventions: Tai Chi vs. pulmonary rehabilitation.
Calisthenics versus exercise training
The mean SGRQ total scores were 47 (SD 12) following a callisthenics and breathing exercises programme compared to 39 (SD 21) after exercise training following a 12‐week study (P = 0.37; Probst 2011, 40 participants; low‐certainty evidence; Table 20) following a 12‐week callisthenics and breathing exercises programme compared to exercise training.
Exercise training (outdoor walking) versus exercise training (cycle ergometry)
Improvement in CRQ total scores (MD 16, 95% CI 2 to 30) at end intervention and at three‐month follow‐up (MD 17, 95% CI 0.1 to 34; Gamper 2019, 16 participants; moderate‐certainty evidence; Analysis 10.4) were demonstrated following a three‐week study comparing outdoor walking and cycle ergometry.
10.4. Analysis.

Comparison 10 Health‐related quality of life: intervention vs. intervention, Outcome 4 CRQ total score; Interventions: outdoor walking vs. cycle ergometry.
Physical activity counselling versus pulmonary rehabilitation
The mean difference in CAT score was 2 (95% CI −1 to 4; Widyastuti 2018; 36 participants; low‐certainty evidence; Table 20) following a six‐week study comparing a physical activity counselling intervention to pulmonary rehabilitation.
The mean difference in change in CAT score was 1 (95% CI −4 to 6), EuroQol 5 dimensions questionnaire (EQ5D) index score was −0.1 (95% CI −0.2 to 0.0) and visual analogue score was −11 (95% CI −32 to 10; O'Neill 2018, 37 participants; low‐certainty evidence; Table 20) following a 12‐week physical activity counselling intervention (in‐person) compared to six weeks of pulmonary rehabilitation.
Exercise training with tapering supervision versus exercise training
The mean difference in Maugeri Respiratory Failure questionnaire score was −1.3 (95% CI −4.2 to 1.6) at end intervention and −2.0 (95% CI −4.7 to 0.7; Rinaldo 2017, 24 participants; moderate‐certainty evidence; Analysis 10.5) at 42‐week follow‐up after a 28‐week study of exercise training with tapered supervision compared to supervised exercise training.
10.5. Analysis.

Comparison 10 Health‐related quality of life: intervention vs. intervention, Outcome 5 Maugeri Respiratory Failure questionnaire; Interventions: exercise training with tapered supervision vs. supervised exercise training.
Adherence intervention versus pulmonary rehabilitation
The mean difference in SF36 physical component score was 0 (95% CI −4 to 5), SF36 mental component score was 0 (95% CI −6 to 6) and CCQ total score was 0.1 (95% CI −0.5 to 0.7; Steele 2019; 63 participants; low‐certainty evidence; Table 20) following six months of an adherence intervention compared to eight weeks of pulmonary rehabilitation.
Maintenance following high‐intensity interval training: telerehabilitation versus centre‐based programme
The mean difference in change in SGRQ total score was 5 (95% CI −3 to 12) and CAT score was 1 (95% CI −2 to 4; Vasilopoulou 2017, 97 participants; low‐certainty evidence; Table 20) following 12 months of telerehabilitation compared to a centre‐based maintenance programme.
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Inpatient exercise training versus no intervention
The mean difference in change in SGRQ symptoms domain score was 6% (95% CI −3 to 14), activity domain score was −4% (95% CI −17 to 8), impacts domain score was −10% (95% CI −32 to 12) and total score was −8% (95% CI −20 to 4; Borges 2014, 29 participants; low‐certainty evidence; Analysis 5.5) at discharge following inpatient resistance training compared to no intervention. The mean difference in SGRQ symptoms domain score was 1% (95% CI −13 to 14), activity domain score was 0.4% (95% CI −18 to 19), impacts domain score was −16% (95% CI −44 to 12) and total score was −6% (95% CI −24 to 13; 1 study; 29 participants; low‐certainty evidence; Analysis 5.5) four weeks after discharge.
5.5. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 5 SGRQ domain scores (%change); Intervention: exercise training [inpatient].
INTERVENTION: Physical activity counselling
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Physical activity counselling versus no intervention
The same 12‐week intervention has been used in three studies (two within this comparison).
The mean difference in SGRQ symptoms domain score was −7 (95% CI −22 to 8), activity domain score was −2 (95% CI −14 to 11), impacts domain score was −4 (95% CI −15 to 6) and total score was −4 (95% CI −14 to 6; Hospes 2009, 35 participants; low‐certainty evidence; Analysis 5.6) following one study when compared to no intervention. The mean difference in CCQ symptoms domain score was −0.6 (95% CI −1.4 to 0.2), functional state domain score was −0.3 (95% CI −0.9 to 0.3), mental state domain score was −0.3 (95% CI −0.8 to 0.2) and total score was −4.0 (95% CI −1.0 to 0.2; Hospes 2009, 35 participants; low‐certainty evidence; Analysis 5.7) at end intervention.
5.6. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 6 SGRQ domain scores; Intervention: physical activity counselling.
5.7. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 7 CCQ domain scores: Intervention: physical activity counselling.
The median change in CRQ total score in participants recruited from primary care was 2 (IQR −3 to 7) in the physical activity counselling group compared to 5 (IQR −3 to 15) in the no‐intervention group (P = 0.398; Altenburg 2015; 40 participants; low‐certainty evidence, Table 20) at end intervention. The median change in CRQ total score in participants recruited from primary care was 2 (IQR −3 to 14) in the physical activity counselling group compared to 13 (IQR −1 to 15) in the no‐intervention group (P = 0.278; Altenburg 2015, 38 participants; low‐certainty evidence, Table 20) at 12‐month follow‐up. The median change in CCQ total score in participants recruited from primary care was −0.1 (IQR −0.4 to 0.1) in the physical activity counselling group compared to −0.1 (IQR −0.4 to 0.3) in the no‐intervention group (P = 0.606; Altenburg 2015, 40 participants; low‐certainty evidence, Table 20) at end intervention. The median change in CCQ total score in participants recruited from primary care was −0.1 (IQR −0.5 to 0.3) in the physical activity counselling group compared to −0.2 (IQR −0.5 to 0.1) in the no‐intervention group (P = 0.536; Altenburg 2015, 38 participants; low‐certainty evidence, Table 20) at 12‐month follow‐up. The median change in CRQ total score in participants recruited from secondary care was 2 (IQR −6 to 11) in the physical activity counselling group compared to −9 (IQR −14 to 1) in the no‐intervention group (P = 0.006; Altenburg 2015, 43 participants; low‐certainty evidence; Table 20) at end intervention. The median change in CRQ total score in participants recruited from secondary care was 6 (IQR −4 to 10) in the physical activity counselling group compared to 1 (IQR −9 to 1) in the no‐intervention group (P = 0.311; Altenburg 2015, 39 participants; low‐certainty evidence; Table 20) at 12‐month follow‐up. The median change in CCQ total score in participants recruited from secondary care was 0 (IQR −0.6 to 0.4) in the physical activity counselling group compared to 0.1 (IQR −0.2 to 0.5) in the no‐intervention group (P = 0.529; Altenburg 2015, 43 participants; low‐certainty evidence; Table 20) at end intervention. The median change in CCQ total score in participants recruited from secondary care was −0.1 (IQR −0.5 to 0.2) in the physical activity counselling group compared to 0.2 (IQR −0.3 to 0.5) in the no‐intervention group (P = 0.220; Altenburg 2015, 39 participants; low‐certainty evidence, Table 20) at 12‐month follow‐up.
Improvements in CCQ functional (MD −0.21, 95% CI −0.42 to −0.01) and mental state domain scores (MD −0.23, 95% CI −0.45 to −0.01) were demonstrated following a 12‐week study comparing a telecoaching intervention to no intervention. The mean difference in symptoms domain score was −0.07 (95% CI −0.27 to 0.12; Demeyer 2017, 278 participants; moderate‐certainty evidence; Analysis 5.8. The mean difference in CAT score was −1 (95% CI −2 to 1; Demeyer 2017, 279 participants; low‐certainty evidence; Table 20).
5.8. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 8 change in CCQ domain scores; Intervention: physical activity counselling (telecoaching).
The mean difference in CCQ total score was 0.1 (95% CI −0.3 to 0.1) and CAT score was 0.1 (95% CI −1.1 to 1.2; Arbillaga‐Etxarri 2018, 280 participants; low‐certainty evidence; Table 20) following a 12‐month study comparing an Urban Training intervention to no intervention.
The mean difference in CRQ dyspnoea domain score was 0 (95% CI −2 to 2; 96 participants), emotional function domain score was 0 (95% CI −2 to 2), fatigue domain score was 0 (95% CI −1 to 1), mastery domain score was −1 (95% CI −2 to 1) and total score was −2 (95% CI −8 to 4; Wootton 2017, 98 participants; low‐certainty evidence; Analysis 5.9) following 12 months of physical activity counselling compared to no intervention, which was completion of phase 2 of a 14‐month study in which all participants began with eight weeks of ground‐based walking training. An improvement in SGRQ impacts domain score (MD −5, 95% CI −9 to −0.01) was demonstrated at end intervention. The mean difference in symptoms domain score was 1 (95% CI −9 to 11), activity domain score was −2 (95% CI −9 to 5) and total score was −3 (95% CI −8 to 2; Wootton 2017, 95 participants; low‐certainty evidence; Analysis 5.10) at end intervention.
5.9. Analysis.
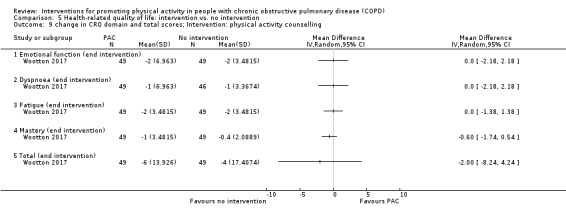
Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 9 change in CRQ domain and total scores; Intervention: physical activity counselling.
5.10. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 10 change in SGRQ domain and total scores; Intervention: physical activity counselling.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Physical activity counselling with optional supervised exercise versus optional supervised exercise
The mean difference in CCQ total score was −0.3 (95% CI −0.7 to 0.1; Tabak 2014a, 29 participants; low‐certainty evidence; Table 20) following a three‐week study comparing a telecoaching intervention with optional supervised exercise to optional supervised exercise.
The mean difference in CRQ dyspnoea domain score was 0.2 (95% CI −0.5 to 0.8), emotional function domain score was −0.1 (95% CI −0.3 to 0.1), fatigue domain score was 0.1 (95% CI −0.2 to 0.4) and mastery domain score was 0.0 (95% CI −0.2 to 0.3; Vorrink 2016, 139 participants; low‐certainty evidence; Analysis 7.8) after 12 weeks of a six‐month text message‐based physical activity counselling intervention following pulmonary rehabilitation with optional supervised exercise compared to optional supervised exercise. Improvement in CRQ fatigue domain score (MD −0.3, 95% CI −0.6 to −0.0) was demonstrated after six months. The mean difference in CRQ dyspnoea domain score was 0.2 (95% CI −0.1 to 0.6), emotional function domain score was −0.1 (95% CI −0.3 to 0.1), fatigue domain score was −0.3 (95% CI −0.6 to −0.0) and mastery domain score was −0.2 (95% CI −0.4 to 0.1; Vorrink 2016, 132 participants; low‐certainty evidence; Analysis 7.8) after six months. The mean difference in CRQ dyspnoea domain score was −0.1 (95% CI −0.4 to 0.3), emotional function domain score was −0.1 (95% CI −0.3 to 0.1), fatigue domain score was −0.0 (95% CI −0.3 to 0.3) and mastery domain score was 0.1 (95% CI −0.1 to 0.4; Vorrink 2016, 121 participants; low‐certainty evidence; Analysis 7.8) at end intervention.
7.8. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 8 change in CRQ domain scores; Interventions: physical activity counselling (app) with optional supervised exercise vs. optional supervised exercise.
Pedometer with physical activity counselling versus physical activity counselling
Improvements in SGRQ total score (MD −5, 95% CI −10 to −0.4) and CAT score (MD −3, 95% CI −5 to −1; Mendoza 2015, 97 participants; moderate‐certainty evidence; Table 20) were demonstrated following a 12‐week study of pedometer use with physical activity counselling compared to physical activity counselling.
Physical activity counselling with pedometer versus pedometer
No data were presented for SGRQ and CAT scores (completer data only) in a 12‐week study of a phone‐call physical activity counselling intervention with pedometer compared to pedometer alone (Bender 2016, 99 participants; very low‐certainty evidence; Table 20).
The mean difference in change in SGRQ total score was −0.2 (95% CI −5 to 4; Wan 2017, 109 participants; low‐certainty evidence; Analysis 7.9) following a 12‐week intervention looking at the addition of physical activity counselling to use of a pedometer. The mean difference in change in SGRQ total score was −1.1 (95% CI −4 to 2; Moy 2015a, 238 participants; low‐certainty evidence; Analysis 7.9) following a 12‐month intervention looking at the addition of physical activity counselling to use of a pedometer.
7.9. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 9 change in SGRQ total score; Interventions: physical activity counselling with pedometer vs. pedometer.
An improvement in SGRQ total score (MD −15, 95% CI −29 to −2) was demonstrated after three months of a six‐month study of a physical activity counselling intervention with pedometer compared to pedometer. The mean difference in SGRQ total score was −4 (95% CI −17 to 10; Nguyen 2009, 17 participants; low‐certainty evidence; Analysis 7.10) at end intervention. The mean difference in SF36 physical component score was 3.5 (95% CI −3.2 to 10.2) and mental component score was −8.3 (95% CI −19.4 to 2.8; Nguyen 2009, 17 participants; low‐certainty evidence; Analysis 7.11) at end intervention.
7.10. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 10 SGRQ total: Interventions: physical activity counselling (app) with pedometer vs. pedometer.
7.11. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 11 SF36: Interventions: physical activity counselling (app) with pedometer vs. pedometer.
An improvement in SGRQ symptoms domain score (MD −5, 95% CI −10 to −1; 224 participants) was demonstrated after four months of a 12‐month study of a physical activity counselling intervention with pedometer compared to pedometer. The mean difference in SGRQ symptoms domain score was −1 (95% CI −5 to 4; Moy 2015a, 238 participants; low‐certainty evidence; Analysis 7.12) at end intervention. The mean difference in SGRQ impacts domain score was −3 (95% CI −7 to 0) and activity was −1 (95% CI −4 to 3; 224 participants) after four months. The mean difference in SGRQ impacts domain score was −2 (95% CI −6 to 1) and activity was −0 (95% CI −4 to 4; Moy 2015a, 238 participants; low‐certainty evidence; Analysis 7.12) at end intervention.
7.12. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 12 change in SGRQ domain scores; Interventions: physical activity counselling (web‐based) with pedometer vs. pedometer.
Physical activity counselling with pulmonary rehabilitation versus pulmonary rehabilitation
No data were available for change in CAT score in the comparison group following a 12‐week web‐based physical activity counselling intervention with pulmonary rehabilitation compared to pulmonary rehabilitation (Mantoani 2018; 44 participants; very low‐certainty evidence; Table 20).
The addition of the same 12‐week physical activity counselling intervention had mixed results in two studies where participants in both groups received pulmonary rehabilitation. A deterioration in SGRQ symptoms domain scores (MD 17, 95% CI 3 to 32) was demonstrated at end intervention. The mean difference in the activity domain score was 11 (95% CI −8 to 30) and impacts domain score was 10 (95% CI −7 to 27; De Blok 2006, 16 participants; low‐certainty evidence; Analysis 7.13). A deterioration in RAND36 general health perception domain score (MD −13.7, 95% CI −24.9 to −2.5) was demonstrated at end intervention. The mean difference in the physical function domain score was −5.6 (95% CI −26.5 to 15.3), vitality was 3.1 (95% CI −12.1 to 18.3), bodily pain domain score was 1.5 (95% CI −26.6 to 29.6) and health status domain score was 3.1 (95% CI −29.8 to 36.0; De Blok 2006, 16 participants; low‐certainty evidence; Analysis 7.14). In a subsequent study, the median difference in change in CRQ total score was 13 (IQR 3 to 20) in the physical activity counselling and pulmonary rehabilitation group compared to 8 (IQR 2 to 21) in the pulmonary rehabilitation group (P = 0.910; Altenburg 2015, 37 participants; low‐certainty evidence; Table 20) at end intervention. The median difference in change in CRQ total score was −7 (IQR −16 to 1) in the physical activity counselling and pulmonary rehabilitation group compared to −5 (IQR −14 to 2) in the pulmonary rehabilitation group (P = 0.344; Altenburg 2015, 23 participants; low‐certainty evidence; Table 20) at 12‐month follow‐up. The median difference in change in CCQ total score was −1 (IQR −1 to 0.2) in the physical activity counselling and pulmonary rehabilitation group compared to −0.2 (IQR −1 to 0) in the pulmonary rehabilitation group (P = 0.345; Altenburg 2015; 37 participants; low‐certainty evidence; Table 20) at end intervention. The median difference in change in CCQ total score was 0.4 (IQR 0.1 to 1) in the physical activity counselling and pulmonary rehabilitation group compared to 0.3 (IQR −0.2 to 0.7) in the pulmonary rehabilitation group (P = 0.368; Altenburg 2015, 23 participants; low‐certainty evidence; Table 20) at 12‐month follow‐up.
7.13. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 13 SGRQ domain scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
7.14. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 14 RAND36 domain scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
Longer studies have also had contradictory findings.
The mean difference in change in CRQ dyspnoea domain scores was −1.9 (95% CI −4.0 to 0.2; 122 participants) after eight weeks (following pulmonary rehabilitation) and −1.9 (95% CI −4.3 to 0.5; Nolan 2017, 113 participants; low‐certainty evidence; Analysis 7.15) at end intervention following a six‐month in‐person physical activity counselling intervention with eight weeks of pulmonary rehabilitation compared to eight weeks of pulmonary rehabilitation. The mean difference in change in the emotional function domain score was −2.2 (95% CI −4.5 to 0.1; Nolan 2017, 122 participants; low‐certainty evidence; Table 20) at eight weeks. An improvement in the median difference in change in fatigue domain score (2, IQR 0 to 5) was demonstrated in the physical activity counselling and pulmonary rehabilitation group compared to the pulmonary rehabilitation group (4, IQR 2 to 6; P = 0.008; Nolan 2017, 122 participants; low‐certainty evidence; Table 20) at eight weeks. An improvement in the change in mastery domain score (MD −1.6, 95% CI −3.1 to −0.1; Nolan 2017, 122 participants; low‐certainty evidence; Table 20) was demonstrated at eight weeks. An improvement in the median difference in change in total score (11, IQR 3 to 20) was demonstrated in the physical activity counselling and pulmonary rehabilitation group compared to the pulmonary rehabilitation group (20, IQR 8 to 27; P = 0.008; Nolan 2017, 122 participants; low‐certainty evidence; Table 20) at eight weeks. The median difference in change in the emotional function domain score was 0.5 (IQR −3 to 4) was demonstrated in the physical activity counselling and pulmonary rehabilitation group compared to the pulmonary rehabilitation group (2, IQR −1 to 6; P = 0.12). The mean difference in change in the fatigue domain score was −1.0 (95% CI −2.8 to 0.8). The median difference in change in the mastery domain score was 0.5 (IQR −1 to 3) compared to the pulmonary rehabilitation group (2, IQR −2 to 5; P = 0.29). The median difference in change in the total score was 3 (IQR −8 to 16) compared to the pulmonary rehabilitation group (10, IQR −2 to 19; P = 0.07; Nolan 2017, 113 participants; low‐certainty evidence; Table 20) at end intervention.
7.15. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 15 change in CRQ dyspnoea domain score; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
The mean difference in SGRQ symptoms domain score was −4 (95% CI −19 to 12), activity domain score was −1 (95% CI −17 to 16), impacts domain score was −4 (95% CI −14 to 5) and total score was −3 (95% CI −14 to 8; Cruz 2016, 26 participants; low‐certainty evidence; Analysis 7.16) after 12 weeks (following pulmonary rehabilitation) of a six‐month physical activity counselling intervention with 12 weeks of pulmonary rehabilitation compared to 12 weeks of pulmonary rehabilitation. The mean difference in SGRQ symptoms domain score was −7 (95% CI −24 to 10), activity domain score was 2 (95% CI −11 to 15), impacts domain score was −5 (95% CI −14 to 4) and total score was −3 (95% CI −13 to 7; Cruz 2016, 26 participants; low‐certainty evidence; Analysis 7.16) at end intervention.
7.16. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 16 SGRQ scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
The mean difference in CRQ dyspnoea domain score was 0.0 (95% CI −6.5 to 6.5), emotional function domain score was −1.0 (95% CI −6.3 to 4.3), fatigue domain score was 1.0 (95% CI −2.4 to 4.4), mastery domain score was −2.0 (95% CI −6.6 to 2.6) and total score was −2.0 (95% CI −16.4 to 12.4; Kawagoshi 2015, 27 participants; low‐certainty evidence; Analysis 7.17) following a 12‐month study of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation.
7.17. Analysis.
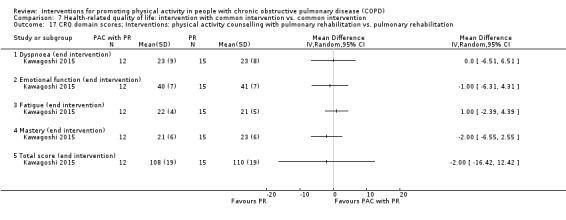
Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 17 CRQ domain scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
An improvement in change in CRQ dyspnoea domain score (MD 3, SE 1, P = 0.04) was demonstrated following 12 weeks of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation after all participants undertook 12 weeks of pulmonary rehabilitation. An improvement in change in CRQ dyspnoea domain score (MD 3, SE 2, P = 0.08) was also demonstrated at nine‐month follow‐up (Loeckx 2018; 50 participants; very low‐certainty evidence; Table 20).
Physical activity counselling and pulmonary rehabilitation versus sham intervention and pulmonary rehabilitation
The mean difference in CRQ total score was 4.0 (95% CI −3.2 to 11.2) after 12 weeks and 2.0 (95% CI −7.7 to 11.7; Burtin 2015, 50 participants; low‐certainty evidence; Analysis 7.18) following a six‐month study of physical activity counselling with pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation.
7.18. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 18 change in CRQ total score; Interventions: physical activity counselling with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation.
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Feedback and education versus no intervention; Education versus no intervention
The mean difference in CAT score was −2 (95% CI −12 to 7; Orme 2018, 14 participants; low‐certainty evidence; Table 20) following 14 days of feedback and education compared to no intervention following hospital admission for AECOPD. The mean difference in CAT score was −1 (95% CI −19 to 17; Orme 2018, 9 participants; low‐certainty evidence; Table 20) following 14 days of education compared to no intervention following hospital admission for AECOPD.
Physical activity counselling versus no intervention
The median difference in change in CAT score was −3 (IQR −10 to 1) in the physical activity counselling group and −5 (IQR −7 to 1; P = 0.78; Hornikx 2015, 27 participants; low‐certainty evidence; Table 20) in the no‐intervention group following a four‐week study comparing physical activity counselling to no intervention following hospital admission for AECOPD.
COMPARISON: Intervention versus standard common intervention (acute exacerbation of COPD)
Feedback with education versus education
The mean difference in CAT score was −1 (95% CI −17 to 15; Orme 2018, 11 participants; low‐certainty evidence; Table 20) following 14 days of feedback with education compared to education following hospital admission for AECOPD.
INTERVENTION: Self‐management
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Self‐management versus no intervention
Improvements in the mean difference for CRQ emotional function (MD 0.4, 95% CI 0.1 to 0.7) and mastery domain scores (MD 0.3, 95% CI −0.1 to 0.6) were demonstrated following a six‐week SPACE programme compared to no intervention. The mean difference in the dyspnoea domain score was 0.3 (95% CI −0.1 to 0.6) and mastery domain score was 0.3 (95% CI −0.1 to 0.6; Mitchell 2013, 155 participants; low‐certainty evidence; Analysis 5.11) at end intervention. The mean difference in the dyspnoea domain score was 0.2 (95% CI −0.2 to 0.6), emotional function domain score was 0.4 (95% CI −0.0 to 0.7), fatigue domain score was 0.3 (95% CI −0.0 to 0.6) and mastery domain score was 0.3 (95% CI −0.1 to 0.6; Mitchell 2013, 84 participants; low‐certainty evidence; Analysis 5.11) at six‐month follow‐up.
5.11. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 11 change in CRQ domain scores; Intervention: self‐management (SPACE).
The mean difference in CCQ total score was −0.4 (95% CI −0.9 to 0.1) after four weeks and −0.5 (95% CI −1.2 to 0.2; Tabak 2014b, 20 participants; low‐certainty evidence; Analysis 5.12) following a 12‐week self‐management intervention compared to no intervention. An improvement in EQ5D index score (MD 0.09, 95% CI 0.01 to 0.17) was demonstrated after four weeks. The mean difference in EQ5D index score was 0.17 (95% CI −0.07 to 0.41; Tabak 2014b, 20 participants; low‐certainty evidence; Analysis 5.13) at end intervention. The mean difference in EQ5D visual analogue scale score was 3.8 (95% CI −8.6 to 16.2) after four weeks and 9.9 (95% CI 0.7 to 19.1; Tabak 2014b, 20 participants; low‐certainty evidence; Analysis 5.14) at end intervention.
5.12. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 12 CCQ total score; Intervention: self‐management.
5.13. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 13 EQ5D index score; Intervention: self‐management.
5.14. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 14 EQ5D visual analogue scale score; Intervention: self‐management.
The mean difference in SGRQ symptoms domain score was 0 (95% CI −27 to 27; 507 participants), activity domain score was −2 (95% CI −6 to 2; 481 participants), impacts domain score was −2 (95% CI −5 to 1; 488 participants) and total score was −1.9 (95% CI −5.0 to 1.2; Jolly 2018, 459 participants; low‐certainty evidence; Analysis 5.15) following a six‐month self‐management programme compared to no intervention. The mean difference in SGRQ symptoms domain score was −1 (95% CI −5 to 3; 503 participants), activity domain score was −6, 95% CI −10 to −2; 484 participants) and impacts domain score was −3 (95% CI −6 to −0; 486 participants) at 12‐month follow‐up. An improvement in total score (MD −3.0, 95% CI −6.0 to −0.1; Jolly 2018, 473 participants; low‐certainty evidence; Analysis 5.15) was demonstrated at 12‐month follow‐up. The mean difference in EQ5D index score was 0.01 (95% CI −0.02 to 0.04; Jolly 2018, 516 participants; low‐certainty evidence; Analysis 5.16) following a six‐month self‐management programme compared to no intervention. The mean difference in EQ5D index score was 0.01 (95% CI −0.02 to 0.04; 505 participants; Jolly 2018; Analysis 5.16) at 12‐month follow‐up.
5.15. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 15 SGRQ domain scores; Intervention: self‐management (telephone health coaching).
5.16. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 16 EQ5D score; Intervention: self‐management (telephone health coaching).
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Health mentoring versus sham intervention
Similar effects for SF36 and SGRQ total and domain scores were demonstrated after six months and following a 12‐month study of phone call‐based health mentoring compared to a sham intervention (Schuz 2015; 6 months: 140 participants; 12 months: 142 participants; low‐certainty evidence; Table 20).
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Self‐management versus education and symptom monitoring
Improvements in SF36 domain scores were demonstrated for mental health (MD 3.3, 95% CI 0.5 to 6.1), role emotional (MD 12.1, 95% CI 4.6 to 19.6), vitality (MD 5.6, 95% CI 2.6 to 8.7) and social functioning (MD 5.3, 95% CI 0.9 to 9.7) following 16 weeks of self‐management compared to education and symptom monitoring. The mean difference in the pain domain score was −0.1 (95% CI −4.1 to 3.9), role physical domain score was 3.9 (95% CI −3.3 to 11.1), general health domain score was 1.9 (95% CI −1.2 to 5.0) and physical functioning domain score was 1.9 (95% CI −1.2 to 5.0; Blumenthal 2014, 326 participants, low‐certainty evidence; Analysis 10.6) at end intervention. Improvement in the pulmonary‐specific quality of life scale was demonstrated in the self‐management group (mean 83, SE 1) compared to the education and symptom‐monitoring group (mean 81, SE 1; P = 0.04; Blumenthal 2014; 326 participants; low‐certainty evidence; Table 20) at end intervention. The mean SGRQ total score was 44 (SE 1) in the self‐management group and 42 (SE 1; P = 0.068; Blumenthal 2014, 326 participants; low‐certainty evidence; Table 20) in the education and symptom monitoring group at end intervention.
10.6. Analysis.
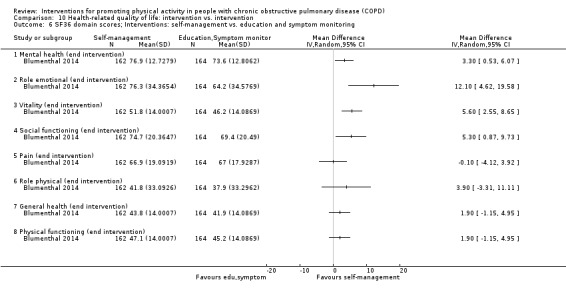
Comparison 10 Health‐related quality of life: intervention vs. intervention, Outcome 6 SF36 domain scores; Interventions: self‐management vs. education and symptom monitoring.
COMPARISON: Intervention versus standard common intervention (acute exacerbations of COPD)
Health coaching with pulmonary rehabilitation referral versus pulmonary rehabilitation referral
Improvements in CRQ physical function (MD 0.3, 95% CI 0.1 to 0.6) and emotional function domain scores (MD 0.4, 95% CI 0.1 to 0.7; Benzo 2016, 215 participants; moderate‐certainty evidence; Analysis 7.19) were demonstrated at six months post‐admission with the addition of health coaching to pulmonary rehabilitation referral compared to pulmonary rehabilitation referral. Improvements in CRQ physical function (MD 0.3, 95% CI 0.0 to 0.6) and emotional function domain scores (MD 0.3, 95% CI 0.0 to 0.5; Benzo 2016, 215 participants; moderate‐certainty evidence; Analysis 7.19) were demonstrated at end intervention.
7.19. Analysis.
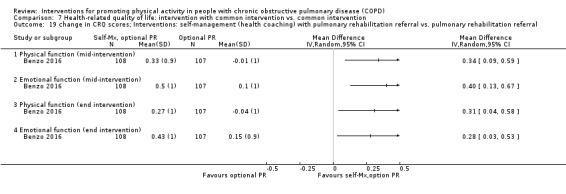
Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 19 change in CRQ scores; Interventions: self‐management (health coaching) with pulmonary rehabilitation referral vs. pulmonary rehabilitation referral.
INTERVENTION: Pharmacological treatment
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
LAMA versus placebo
The mean difference in CAT score was 1 (95% CI −1 to 4; Magnussen 2017, 30 participants; moderate‐certainty evidence; Table 20) following a three‐week study of LAMA compared to placebo.
Data were not presented in another 12‐week study comparing LAMA with placebo, but reported that the effect was similar in both groups (NCT00144326, 248 participants; very low‐certainty evidence; Table 20).
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
LAMA with behaviour modification versus placebo with behaviour modification
The mean difference in CRQ dyspnoea domain score was 0.2 (95% CI −0.1 to 0.5), emotional function domain score was 0.1 (95% CI −0.2 to 0.3), fatigue domain score was 0.3 (95% CI −0.1 to 0.6) and mastery domain score was 0.0 (95% CI −0.3 to 0.3; Troosters 2018, 132 participants; moderate‐certainty evidence; Analysis 7.20) after nine weeks of the 12‐week PHYSACTO study for LAMA with behaviour modification compared to placebo with behaviour modification. The mean difference in CRQ dyspnoea domain score was 0.1 (95% CI −0.2 to 0.4), emotional function domain score was 0.0 (95% CI −0.3 to 0.3), fatigue domain score was 0.2 (95% CI −0.1 to 0.5) and mastery domain score was −0.2 (95% CI −0.6 to 0.1; Troosters 2018, 129 participants; moderate‐certainty evidence; Analysis 7.20) at end intervention.
7.20. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 20 CRQ domain scores; Interventions: LAMA with behaviour modification vs. placebo with behaviour modification.
LAMA/LABA with behaviour modification versus placebo with behaviour modification
Improvements in CRQ dyspnoea (MD 0.4, 95% CI 0.1 to 0.7) and fatigue domain scores (MD 0.4, 95% CI 0.1 to 0.6) were demonstrated after nine weeks of the 12‐week PHYSACTO study for LAMA/LABA with behaviour modification compared to placebo with behaviour modification. The mean difference in emotional function domain score was 0.2 (95% CI −0.0 to 0.5) and mastery domain score was 0.2 (95% CI −0.1 to 0.5; Troosters 2018, 136 participants; moderate‐certainty evidence; Analysis 7.21) after nine weeks. The mean difference in CRQ dyspnoea domain score was 0.1 (95% CI −0.2 to 0.5), emotional function domain score was 0.2 (95% CI −0.0 to 0.5), fatigue domain score was 0.3 (95% CI 0.1 to 0.6) and mastery domain score was 0.1 (95% CI −0.2 to 0.5; Troosters 2018, 135 participants; moderate‐certainty evidence; Analysis 7.21) at end intervention.
7.21. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 21 CRQ domain scores; Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
LABA with LAMA and behaviour modification versus LAMA and behaviour modification
The mean difference in CRQ dyspnoea domain score was 0.2 (95% CI −0.1 to 0.5), emotional function domain score was 0.2 (95% CI −0.1 to 0.4), fatigue domain score was 0.1 (95% CI −0.2 to 0.4) and mastery domain score was 0.2 (95% CI −0.1 to 0.5; Troosters 2018, 138 participants; moderate‐certainty evidence; Analysis 7.22) after nine weeks of the 12‐week PHYSACTO study for LABA with LAMA and behaviour modification compared to LAMA and behaviour modification. An improvement in CRQ mastery domain score (MD 0.4, 95% CI 0.1 to 0.7) was demonstrated at end intervention. The mean difference for the dyspnoea domain score was 0.2 (95% CI −0.1 to 0.5), emotional function domain score was 0.2 (95% CI −0.1 to 0.5) and fatigue domain score was 0.2 (95% CI −0.1 to 0.5; Troosters 2018, 136 participants; moderate‐certainty evidence; Analysis 7.22) at end intervention.
7.22. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 22 CRQ domain scores; Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
Angiotensin‐converting enzyme (ACE) inhibitor with pulmonary rehabilitation versus placebo with pulmonary rehabilitation
The mean difference in change in SGRQ symptom score was −2 (95% CI −8 to 4), activity domain score was −2 (95% CI −9 to 5), impacts domain score was −1 (95% CI −6 to 4) and total score was −2 (95% CI −6 to 2; Curtis 2016, 65 participants; moderate‐certainty evidence; Analysis 7.23) following a 10‐week study of an ACE inhibitor and pulmonary rehabilitation compared to a placebo and pulmonary rehabilitation. The mean difference in change in CAT score was 2 (95% CI 0 to 4; Curtis 2016; 65 participants; moderate‐certainty evidence; Table 20) at end intervention.
7.23. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 23 change in SGRQ domain and total scores; Interventions: ACE inhibitor with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Inhaled corticosteroid and LABA versus inhaled corticosteroid and LABA
The mean difference for change in CCQ total score was 0.01 (95% CI −0.24 to 0.26; NCT01351792, 59 participants; very low‐certainty evidence; Table 20) following a 12‐week study of inhaled corticosteroid (beclomethasone) and LABA compared to inhaled corticosteroid (budesonide) and LABA.
LAMA versus LAMA
No data were presented in an eight‐week study comparing LAMA (aclidinium bromide) and LAMA (tiotropium; Nakamura 2016; 44 participants; very low‐certainty evidence; Table 20).
INTERVENTION: Nutritional supplementation
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Nutritional supplement versus placebo
The mean SGRQ total score was 69 (SD 10) in the nutritional‐supplement group compared to 73 (SD 7; P < 0.001; Dal Negro 2012; 88 participants; moderate‐certainty evidence; Table 20) in the placebo group following a 12‐week study of nutritional supplement (essential amino acids) compared to placebo.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Nutritional supplement with physical activity counselling versus physical activity counselling
The mean difference in change in SGRQ total score was 2 (95% CI −3 to 7) at end intervention and −3 (95% CI −9 to 4; Van de Bool 2017, 61 participants; moderate‐certainty evidence; Analysis 7.24) at three‐month follow‐up after a 12‐month study of nutritional supplementation and physical activity counselling compared to physical activity counselling in people with low muscle mass. The mean difference in change in EQ5D index score was 0.1 (95% CI −0.0 to 0.2) at end intervention. An improvement in change in EQ5D index score (MD 0.1, 95% CI 0.0 to 0.1; Van de Bool 2017, 61 participants; moderate‐certainty evidence; Analysis 7.25) was demonstrated at three‐month follow‐up.
7.24. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 24 change in SGRQ total score; Interventions: nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation.
7.25. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 25 change in EQ5D; Interventions: nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation.
COMPARISON: Intervention versus standard common intervention (acute exacerbation of COPD)
Enriched nutritional supplement with inpatient pulmonary rehabilitation versus nutritional supplement with inpatient pulmonary rehabilitation
The median CAT score was 10 for both groups following eicosapentaenoic acid‐enriched nutritional supplement and inpatient pulmonary rehabilitation compared with an unenriched nutritional supplement and inpatient pulmonary rehabilitation during hospital admission for an acute exacerbation of COPD (P = 0.75; Ogasawara 2018, 45 participants; low‐certainty evidence; Table 20).
INTERVENTION: Supplemental oxygen
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Supplemental oxygen versus placebo
The median CRQ dyspnoea domain score was 2.2 (IQR 1.8 to 3) in the supplemental oxygen group compared to 2.5 (IQR 1.5 to 3.2; P > 0.05) in the placebo group following an eight‐week study of supplemental oxygen following pulmonary rehabilitation compared to placebo. The median emotional function domain score was 4.8 (IQR 3.2 to 5.7) in the supplemental oxygen group compared to 3.8 (IQR 2.6 to 5.6; P > 0.05) in the placebo group at end intervention. The median mastery domain score was 5.1 (IQR 3.2 to 5.9) in the supplemental oxygen group compared to 3.6 (IQR 2.3 to 5.0; P > 0.05) in the placebo group at end intervention. The median fatigue domain score was 3.4 (IQR 2.8 to 4.8) in the supplemental oxygen group compared to 3.3 (IQR 1.8 to 4.3; P > 0.05; Sandland 2008, 20 participants; moderate‐certainty evidence; Table 20) in the placebo group at end intervention.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Supplemental oxygen and pulmonary rehabilitation versus sham and pulmonary rehabilitation
The mean difference in CRQ dyspnoea domain score was 0.1 (95% CI −0.3 to 0.5), emotional function domain score was 0.2 (95% CI −0.2 to 0.6), fatigue was domain score 0.1 (95% CI −0.3 to 0.5), mastery was domain score −0.1 (95% CI −0.34 to 0.2) and total score was 0.0 (95% CI −3 to 3; Alison 2019, 96 participants; moderate‐certainty evidence; Analysis 7.26) following eight weeks of supplemental oxygen and pulmonary rehabilitation compared to sham and pulmonary rehabilitation. The mean difference in CRQ dyspnoea domain score was 0 (95% CI −0.4 to 0.4), emotional function domain score was −0.1 (95% CI −0.5 to 0.3), fatigue domain score was 0.0 (95% CI −0.4 to 0.4), mastery domain score was 0.2 (95% CI −0.2 to 0.6) and total score was −0.1 (95% CI −0.5 to 0.3; Alison 2019, 78 participants; moderate‐certainty evidence; Analysis 7.26) at six‐month follow‐up.
7.26. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 26 change in CRQ domain scores; Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation.
INTERVENTION: Other interventions
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Four‐wheeled walker versus no intervention
The mean difference in CRQ dyspnoea domain score was 0.4 (95% CI −0.4 to 1.2), emotional function domain score was 0.5 (95% CI −0.6 to 1.6), fatigue domain score was 0.9 (95% CI −0.4 to 2.2) and mastery domain score was 0.9 (95% CI −0.4 to 2.2; Ng 2015, 17 participants; very low‐certainty evidence; Analysis 5.17) over four weeks following pulmonary rehabilitation using a four‐wheeled walker compared to no intervention.
5.17. Analysis.

Comparison 5 Health‐related quality of life: intervention vs. no intervention, Outcome 17 CRQ domain scores; Intervention: four‐wheeled walker.
Endobronchial valve surgery versus no intervention
The mean difference in SGRQ total score was −13 (SD 4, P = 0.0005; Hartman 2016, 43 participants; moderate‐certainty evidence; Table 20) six months following endobronchial valve surgery compared to no intervention.
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Singing versus sham intervention
An improvement in the SF36 physical component score (15.4, 95% CI 2.9 to 27.9) was demonstrated following an eight‐week singing intervention compared to a sham intervention. The mean difference in SF36 mental component score was 5.0 (95% CI −9.8 to 19.8; Lord 2012, 24 participants; low‐certainty evidence; Analysis 6.1) at end intervention. The mean difference in CAT score was −2 (95% CI −7 to 4; Lord 2012, 24 participants; low‐certainty evidence; Table 20).
6.1. Analysis.

Comparison 6 Health‐related quality of life: intervention vs. placebo/sham, Outcome 1 change in SF36 component scores; Intervention: singing.
Neuromuscular electrical stimulation versus placebo
The mean difference in change in CRQ total score was −0.2 (95% CI −2.0 to 1.6) at end intervention and −0.3 (95% CI −1.8 to 1.1; Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 6.2) at 12‐week follow‐up after a six‐week neuromuscular electrical stimulation (NMES) programme compared to placebo. The mean difference in change in SGRQ total score was −0.3 (95% CI −5 to 4) at end intervention and 3 (95% CI −3 to 10; Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 6.3) at 12‐week follow‐up. The mean difference in change in EQ5D index score was 0 (95% CI −1.0 to 1.0) at end intervention and 0.1 (95% CI −0.1 to 0.2; Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 6.4) at 12‐week follow‐up. The mean difference in change in EQ5D visual analogue scale score was 6 (95% CI −3 to 15) at end intervention and −5 (95% CI −15 to 6; Maddocks 2016, 52 participants; low‐certainty evidence; Analysis 6.5) at 12‐week follow‐up.
6.2. Analysis.
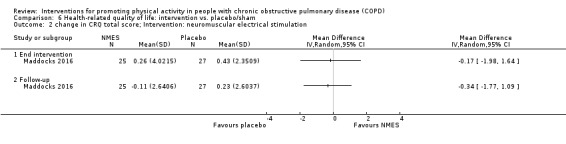
Comparison 6 Health‐related quality of life: intervention vs. placebo/sham, Outcome 2 change in CRQ total score; Intervention: neuromuscular electrical stimulation.
6.3. Analysis.

Comparison 6 Health‐related quality of life: intervention vs. placebo/sham, Outcome 3 change in SGRQ total score; Intervention: neuromuscular electrical stimulation.
6.4. Analysis.

Comparison 6 Health‐related quality of life: intervention vs. placebo/sham, Outcome 4 change in EQ5D index score; Intervention: neuromuscular electrical stimulation.
6.5. Analysis.
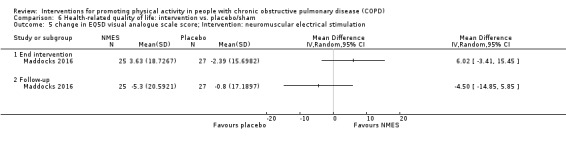
Comparison 6 Health‐related quality of life: intervention vs. placebo/sham, Outcome 5 change in EQ5D visual analogue scale score; Intervention: neuromuscular electrical stimulation.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Inspiratory muscle training and pulmonary rehabilitation versus sham and pulmonary rehabilitation
The mean difference in CRQ dyspnoea domain score was 0.4 (95% CI −1.1 to 2.0), emotional function domain score was −0.4 (95% CI −2.4 to 1.6), fatigue domain score was 0.4 (95% CI −0.8 to 1.6), mastery domain score was 0.0 (95% CI −1.2 to 1.2) and total score was −1.0 ( 95% CI −5.2 to 3.9; Charususin 2018, 150 participants; moderate‐certainty evidence; Table 20) following a 12‐week study of the addition of inspiratory muscle training to pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation.
Non‐invasive ventilation with pulmonary rehabilitation versus pulmonary rehabilitation
The mean difference in CRQ dyspnoea domain score was −0.4 (95% CI −3.6 to 2.8), emotional function domain score was 3.5 (95% CI −0.2 to 7.2), fatigue domain score was 3.4 (95% CI 0.8 to 6.0) and mastery domain score was 2.2 (95% CI −0.2 to 4.6; Duiverman 2008, 56 participants; low‐certainty evidence; Analysis 7.27) following a 12‐week study of the addition of non‐invasive ventilation with pulmonary rehabilitation compared to pulmonary rehabilitation. Improvement in the Maugeri Respiratory Failure questionnaire (MD −22%, 95% CI −35 to −9) was demonstrated at end intervention. The mean difference in daily activities domain score was −5% (95% CI −17 to 6), invalidity domain score was −6% (95% CI −19 to 7) and total score was −10% (95% CI −18 to 1; 56 participants; Duiverman 2008; Table 20) at end intervention. Similar effects for the Severe Respiratory Insufficiency questionnaire scores were demonstrated in both groups (Duiverman 2008, 56 participants; low‐certainty evidence; Table 20) at end intervention.
7.27. Analysis.

Comparison 7 Health‐related quality of life: intervention with common intervention vs. common intervention, Outcome 27 CRQ domain scores; Interventions: non‐invasive ventilation with pulmonary rehabilitation vs. pulmonary rehabilitation.
Appendix 5. Secondary outcome: exercise capacity
Exercise capacity was assessed in 56 studies.
INTERVENTION: Pulmonary rehabilitation/exercise training
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Pulmonary rehabilitation versus no intervention
Improvements in exercise capacity were demonstrated following pulmonary rehabilitation compared to no intervention. The mean difference in 6MWD was 29 metres (95% CI 14 to 44; 3 studies, 182 participants; moderate‐certainty evidence; Analysis 9.1) at end intervention. The mean difference in the distance walked during an incremental shuttle walk test (ISWD) was 19 metres (95% CI 2 to 36; 3 studies, 180 participants; moderate‐certainty evidence; Analysis 9.2) with some heterogeneity (I2 = 24%) evident. The mean difference in time walked during an endurance shuttle walk test (ESWT) was 238 seconds (95% CI 148 to 328; 2 studies, 137 participants; moderate‐certainty evidence; Analysis 9.3) at end intervention.
9.1. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 1 change in 6MWD (metres); Intervention: pulmonary rehabilitation/exercise training.
9.2. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 2 change in ISWD (metres); Intervention: pulmonary rehabilitation/exercise training.
9.3. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 3 change in ESWT (seconds); Intervention: pulmonary rehabilitation/exercise training.
High‐intensity interval training versus no intervention
Improvements in exercise capacity were demonstrated following high intensity interval training compared to no intervention. The mean difference in 6MWD was 47 metres (95% CI 25 to 68; 2 studies, 275 participants; moderate‐certainty evidence; Analysis 9.4) at end intervention. The mean difference in peak work rate was 15 watts (95% CI 9 to 22; 2 studies, 275 participants; moderate‐certainty evidence; Analysis 9.5) at end intervention. Additionally, an improvement in peak oxygen uptake (MD 2.3 mL/min/kg, 95% CI 0.8 to 3.8; Louvaris 2016, 128 participants; moderate‐certainty evidence; Table 21) was demonstrated following a 12‐week intervention.
9.4. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 4 6MWD (metres); Intervention: high‐intensity interval training.
9.5. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 5 work rate (watts); Intervention: high‐intensity interval training.
4. Exercise capacity outcomes.
| Study |
Comparison (setting, if known) Clinical stability unless indicated |
Time point (end intervention unless indicated) | Outcome | Intervention group | Comparison group | Between‐group MD (95% CI) where available unless indicated | ||
| n | mean (95% CI) unless indicated | n | mean (95% CI) unless indicated | |||||
| Altenburg 2015 | Physical activity counselling vs. no intervention (primary care) | 12 weeks | ∆ 6MWD (m) | 22 | median 10 (IQR −7 to 38) | 18 | median 3 (IQR −18 to 22) | P = 0.291* |
| follow‐up (12 months post‐intervention) | 20 | median 20 (IQR 8 to 54) | 18 | median 13 (IQR −2 to 38) | P = 0.313* | |||
| Physical activity counselling vs. no intervention (secondary care) | 12 weeks | 21 | median 23 (IQR 0 to 51) | 22 | median 4 (IQR −32 to 27) | P = 0.049* | ||
| follow‐up (12 months post intervention) | 20 | median 25 (IQR 4 to 52) | 19 | median 17 (IQR −9 to 57) | P = 0.555* | |||
| Physical activity counselling with PR vs. PR | 12 weeks | 22 | median 17 (IQR −27 to 42) | 15 | median 25 (IQR −15 to 60) | P = 0.605* | ||
| follow‐up (12 months post intervention) | 10 | median 7 (IQR −32 to 51) | 13 | median 10 (IQR −15 to 87) | P = 0.503* | |||
| Arbillaga‐Etxarri 2018 | Urban Training™ vs. no intervention | 12 months | 6MWD (m) | 132 | 488 (106) | 148 | 493 (90) | −2 (−11 to 8)* |
| Beeh 2014 | LAMA vs. placebo | 3 weeks | ∆ endurance time (sec)** | 54 | median 26 (IQR −106 to 117) | 54 | median −16 (IQR −109 to 18) | P = 0.093* |
| Blumenthal 2014 | Self‐management vs. education and symptom monitoring | 16 weeks | 6MWD (m) | 162 | mean 361 (SE 3) | 164 | mean 351 (SE 3) | P = 0.03* |
| Chaplin 2017 | Web‐based PR vs. centre‐based PR | 7 weeks | ∆ ESWT (sec) | 22 | 189 (95 to 283) | 40 | 185 (105 to 264) | 5 (−112 to 121) |
| Charususin 2018 | Inspiratory muscle training with PR vs. sham with PR | 12 weeks | 6MWD (m) n = 169 |
x | mean 388 (SD 113) | x | mean 407 (SD 105) | 1 (−13 to 15)* |
| endurance time (sec) n = 139 |
mean 496 (SD 309) | mean 466 (SD 292) | 98 (17 to 179)* | |||||
| peak work rate (W) n = 92 | mean 64 (SD 26) | mean 59 (SD 22) | 5.2 (−0.4 to 10.8)* | |||||
| VO2peak (mL/min) n = 92 | mean 1048 (SD 313) | mean 966 (SD 323) | 0.01 (−0.1 to 0.1)* | |||||
| VEpeak (L/min) n = 92 | mean 37 (SD 11) | mean 39 (SD 15) | −1 (−3 to 2)* | |||||
| Curtis 2016 | ACE inhibitor with PR vs. placebo with PR | 10 weeks | ∆ peak work rate (W) | 31 | 1 (−2 to 4) | 34 | 9 (5 to 13) | −8 (−13 to −3) |
| ∆ VO2peak (mL/min/kg) | 0.3 (−0.4 to 1.1) | 1.4 (0.8 to 2.0) | −1.0 (−2.0 to −0.1) | |||||
| ∆ VE/VCO2 slope | −0.9 (−2.1 to 0.4) | −1.3 (−3.2 to 0.7) | 0.4 (−2.0 to 2.8) | |||||
| ∆ oxygen uptake efficiency slope (ml/min) | 29 (−109 to 167) | 151 (40 to 261) | −122 (−292 to 49) | |||||
| De Blok 2006 | Physical activity counselling with PR vs. PR | 9 weeks | 2‐min step test (n steps) | 8 | 57 (32 to 82) | 8 | 55 (37 to 73) | 2 (−24 to 28) |
| Demeyer 2017 | Physical activity counselling vs. no intervention | 12 weeks | ∆ 6MWD (m) | 131 | mean 12 (SD 44) | 136 | mean −1 (SD 44) | 13 (2 to 23) |
| Duiverman 2008 | Non‐invasive ventilation with PR vs. PR | 12 weeks | ESWT (sec) | 24 | median 475 (IQR 295 to 1010) | 32 | 449 (213 to 1042) | 103 (−69 to 276)* |
| 6MWD (m) | mean 340 (SD 119) | mean 325 (SD 108) | 2 (−19 to 23)* | |||||
| VO2peak (mL/min/kg) | mean 9.8 (SD 2.9) | mean 9.5 (SD 3.0) | 0.3 (−0.9 to 1.4)* | |||||
| Gamper 2019 | Exercise training (outdoor walking) vs. exercise training (cycle ergometry) | 3 weeks | 6MWD (m) | 8 | mean 285 (SD 72) | 8 | mean 440 (SD 49) | −155 (−215 to −95) |
| Hartman 2016 | Endobronchial valve surgery vs. no intervention | 6 months post‐surgery | ∆ 6MWD (m) | 19 | mean 84 (SD 62) | 24 | mean −20 (SD 35) | MD 104 (SD 165)* |
| Hornikx 2015 | Physical activity counselling vs. no intervention | 4 weeks | ∆ 6MWD (m) | 12 | mean 67 (SD 84) | 15 | mean 64 (SD 59) | 3 (−53 to 59) |
| Hospes 2009 | Physical activity counselling vs. no intervention | 12 weeks | 6MWD (m) | 18 | mean 387 (SD 47) | 17 | mean 361 (SD SD 67) | 26 (−12 to 64) |
| Kanabar 2015 | Self‐management vs. no intervention (post‐admission) | 7 days | ∆ ISWD (m) | 15 | mean 46 (SD 32) | 10 | mean 44 (SD SD 99) | 2 (−62 to 66) |
| ∆ ESWT (sec) | mean 369 (SD 355) | mean 290 (SD SD 379) | 80 (−216 to 375) | |||||
| Kawagoshi 2015 | Physical activity counselling with PR vs. PR | 12 months | 6MWD (m) | 12 | mean 445 (SD 138) | 15 | mean 467 (SD SD 151) | −22 (−131 to 87) |
| Loeckx 2018 | Physical activity counselling with PR vs. PR | 12 weeks | ∆ 6MWD (m) | 25 | x | 25 | x | MD 8 (SE 14), P = 0.59* |
| ∆ endurance time (sec) | MD −80 (SE 71), P = 0.26* | |||||||
| 9 months (follow‐up) | ∆ 6MWD (m) | MD 2 (SE 16), P = 0.90* | ||||||
| ∆ endurance time (sec) | MD 153 (SE 79), P = 0.06* | |||||||
| Lord 2012 | Singing vs. sham | 8 weeks | ∆ ISWD (m) | 13 | −7 (−35 to 21) | 11 | 15 (−11 to 40) | −22 (−56 to 12) |
| Louvaris 2016 | High‐intensity interval training vs. no intervention | 12 weeks | VO2peak (mL/min/kg) | 85 | mean 17.8 (SD 4) | 43 | mean 15.5 (SD 4.1) | 2.3 (0.8 to 3.8) |
| Mantoani 2018 | Physical activity counselling with PR vs. PR | 12 weeks | ∆ESWT (sec) | 22 | 99 (37 to 161) | 22 | 3 (−34 to 40) | 96 (28 to 164) |
| Mendoza 2015 | Pedometer with PAI vs. PAI | 12 weeks | ∆6MWD (m) | 50 | mean 12 (SD 35) | 47 | mean −1 (SD 24) | 13 (1 to 25) |
| NCT00144326 | LAMA vs. placebo | 12 weeks | 6MWD (m) | 123 | x | 125 | x | "trend favouring tiotropium" |
| Nguyen 2009 | Physical activity counselling with pedometer vs. pedometer | 6 months | peak work rate (W) | 9 | mean 49 (SD 24) | 8 | mean 49 (SD 28) | 0 (−25 to 25) |
| Nolan 2017 | Pedometer with PR vs. PR | 8 weeks (mid‐intervention, post‐PR) | ∆ ISWD (m) | 63 | median 60 (IQR 20 to 90) | 59 | median 50 (IQR 10 to 90) | P = 0.83* |
| 6 months | 56 | median 30 (IQR 0 to 70) | 57 | median 10 (IQR −30 to 70) | P = 0.25* | |||
| O'Neill 2018 | Physical activity counselling vs. PR | 12 weeks physical activity counselling, 6 weeks PR | ∆ ISWD (m) | 16 | −12 (−60 to 36) | 17 | −8 (−44 to 28) | −4 (−60 to 51) |
| Probst 2011 | Exercise training (callisthenics) vs. exercise training (endurance and strength training) | 12 weeks | peak work load (W) | 20 | mean 30 (SD 30) | 20 | mean 48 (SD 30) | P = 0.04* |
| endurance time (min) | mean 8 (SD 7) | mean 17 (SD 24) | P = 0.08* | |||||
| 6MWD (m) | mean 424 (SD 114) | mean 483 (SD 89) | P = 0.30* | |||||
| Sandland 2008 | Supplemental oxygen vs. placebo (air) | 8 weeks | ISWD (m) | 10 | mean 251 (SD 136) | 10 | mean 211 (SD 99) | 40 (−64 to 144) |
| ESWT (sec) | mean 340 (SD 336) | mean 170 (SD 98) | 170 (−47 to 387) | |||||
| Sena 2013 | Exercise training (eccentric cycle training) vs. exercise training (concentric cycle training) | 10 weeks | ∆ peak work rate (W) | 8 | 9 (3 to 15) | 8 | 12 (5 to 19) | −3 (−11 to 5) |
| Steele 2019 | Adherence intervention vs. PR | 6 months (follow‐up) | 6MWD (m) | 32 | mean 320 (SD 134) | 31 | mean 315 (SD 116) | 5 (−57 to 67) |
| Tabak 2014b | Self‐management vs. no intervention | 12 weeks (mid‐intervention) | 6MWD (m) | 11 | mean 412 (SE 39) | 9 | mean 312 (SE 44) | 100 (−15 to 215) |
| Tahirah 2015 | Exercise training (progressive walking and functional‐resistance exercises) vs. no intervention (inpatient) | hospital discharge | 2‐min walk distance (m) | 16 | mean 162 (SD 38) | 16 | mean 146 (SD 4) | 13 (3 to 23)* |
| Van de Bool 2017 | Nutritional supplementation with PR vs. placebo with PR | 4 months (end intervention) | 6MWD (m) | 38 | mean 500 (SD 111) | 35 | mean 492 (SD 101) | MD −4 (SD 12)* |
| endurance time (sec) | mean 467 (SD 339) | mean 482 (SD 372) | MD −110 (SD 70)* | |||||
| 12 months (end maintenance) | ∆ endurance time (sec) | 32 | mean 107 (SD 63) | 29 | mean 200 (SD 65) | MD −93 (SD 90)* | ||
| Vasilopoulou 2017 | Maintenance (telerehabilitation) vs. no intervention | 12 months | 6MWD (m) | 47 | mean 420 (SD 75) | 50 | mean 340 (SD 110) | 80 (43 to 118) |
| peak work rate (W) | mean 76 (SD 35) | mean 58 (SD 24) | 18 (6 to 30) | |||||
| Maintenance (centre‐based) vs. no intervention | 6MWD (m) | 50 | mean 428 (SD 63) | 50 | mean 340 (SD 110) | 88 (52 to 123) | ||
| peak work rate (W) | mean 79 (SD 31) | mean 58 (SD 24) | 21 (10 to 32) | |||||
| Maintenance (telerehabilitation) vs. maintenance (centre‐based) | 6MWD (m) | 47 | mean 420 (SD 75) | 50 | mean 428 (SD 63) | −7 (−35 to 20) | ||
| peak work rate (W) | mean 76 (SD 35) | mean 79 (SD 31) | −3 (−16 to 10) | |||||
| Wan 2017 | Physical activity counselling with pedometer vs. pedometer | 12 weeks | ∆ 6MWD (m) | 57 | mean −1 (SD 56) | 52 | mean 4 (SD 47) | P = 0.72* |
| Watz 2017 | LAMA/LABA vs. placebo | 8 weeks (4 weeks medication only, 4 weeks medication and behavioural intervention) | endurance time (sec) | 127 | 51 (15 to 86) | 123 | −5 (−40 to 31) | LSMD 55 (95% CI 6 to 105)* |
| Widyastuti 2018 | Physical activity counselling vs. PR | 6 weeks | 6MWD (m) | 18 | mean 242 (SD 79) | 18 | mean 267 (SD 47) | −25 (−68 to 18) |
| Wootton 2017 | Physical activity counselling with pedometer vs. no intervention (following ground‐based walking training) | 12 months | ∆ 6MWD (m) | 35 | −23 (−41 to −5) | 36 | −39 (−59 to −18) | −16 (−46 to 15)* |
| ∆ ISWD (m) | 28 | −37 (−60 to −14) | −8 (−34 to 17) | 23 (−13 to 60)* | ||||
| ∆ ESWT (sec) | 29 | −110 (−232 to 12) | −168 (−303 to −33) | −54 (−245 to 137)* | ||||
* from paper x data not provided
ACE: angiotensin‐converting enzyme; ∆: change from baseline; ESWT: time walked during an endurance shuttle walk test; ISWD: distance walked during an incremental shuttle walk test; IQR: interquartile range; LSMD: least squares mean difference; m: metres; D: mean difference; n: number of participants; sec: seconds; SPACE: self‐management programme of activity, coping and education; 6MWD distance walked on six‐minute walk test; SD: standard deviation; VO2peak: peak oxygen uptake
Maintenance (telerehabilitation) following high‐intensity interval training versus no intervention
Improvements in 6MWD (MD 80 metres, 95% CI 43 to 118) and peak work rate (MD 18 watts, 95% CI 6 to 30; Vasilopoulou 2017, 97 participants; moderate‐certainty evidence; Table 21) were demonstrated following a 12‐month telerehabilitation maintenance programme compared to no intervention.
Maintenance (centre‐based) following high intensity interval training versus no intervention
Improvements in 6MWD (MD 88 metres, 95% CI 52 to 123) and peak work rate (MD 21 watts, 95% CI 10 to 32; Vasilopoulou 2017, 100 participants; moderate‐certainty evidence; Table 21) were demonstrated following a 12‐month centre‐based maintenance programme compared to no intervention.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Nordic walking with education versus education
An improvement in 6MWD (MD 98 metres, 95% CI 24 to 172) was demonstrated following a 12‐week Nordic walking programme with education compared to education. This improvement was maintained at six‐month (MD 103 metres, 95% CI 32 to 174) and nine‐month (MD 97 metres, 95% CI 23 to 171; Breyer 2010, 60 participants; moderate‐certainty evidence; Analysis 11.1) follow‐up.
11.1. Analysis.
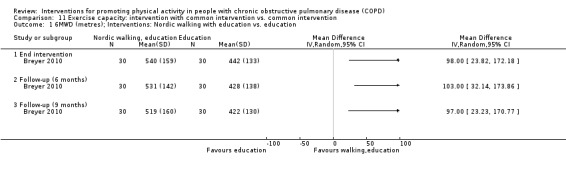
Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 1 6MWD (metres); Interventions: Nordic walking with education vs. education.
Structured exercise training with self‐management versus self‐management
The mean difference in ISWD was 24 metres (95% CI −2 to 51; 128 participants) after seven months of an 11‐month structured exercise training programme with self‐management compared to self‐management. An improvement in ISWD (MD 35 metres, 95% CI 8 to 63; 135 participants) was demonstrated at end intervention. The mean difference in ISWD was 23 metres (95% CI −5 to 51; 126 participants) after 18‐month follow‐up and 12 metres (95% CI −16 to 41; Effing 2011, 119 participants; low‐certainty evidence; Analysis 11.2) at 24‐month follow‐up. The mean difference for ESWT was 122 seconds (95% CI −49 to 293; 128 participants) after seven months and 142 seconds (95% CI −33 to 316; 134 participants) following an 11‐month structured exercise training programme with self‐management compared to self‐management. The mean difference in ISWD was 85 seconds (95% CI −111 to 281; 126 participants) after 18‐month follow‐up and 52 seconds (95% CI −143 to 247; Effing 2011, 119 participants; low‐certainty evidence; Analysis 11.3) at 24‐month follow‐up.
11.2. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 2 change in ISWD (metres); Interventions: exercise training (COPE‐active) with self‐management vs. self management.
11.3. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 3 change in ESWT (seconds); Interventions: exercise training (COPE‐active) with self‐management vs. self management.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
LAMA/LABA with exercise training with behaviour modification versus placebo with behaviour modification
An improvement in 6MWD (MD 27 metres, 95% CI 8 to 47; 123 participants) was demonstrated after eight weeks of the 12‐week PHYSACTO study for LAMA/LABA with exercise training compared to placebo. The mean difference in 6MWD was 14 metres (95% CI −8 to 36; Troosters 2018, 118 participants; moderate‐certainty evidence; Analysis 11.4) at end intervention. An improvement in ESWT was demonstrated after eight weeks (MD 112 seconds, 95% CI 52 to 171; 135 participants) and at end intervention (MD 81 seconds, 95% CI 21 to 141; Troosters 2018, 128 participants; high‐certainty evidence; Analysis 11.5).
11.4. Analysis.
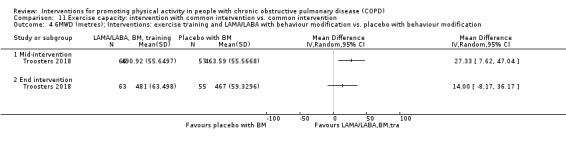
Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 4 6MWD (metres); Interventions: exercise training and LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
11.5. Analysis.
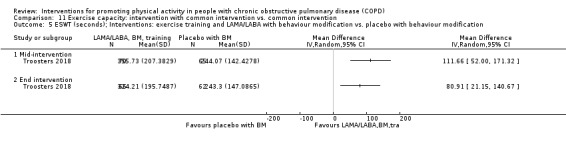
Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 5 ESWT (seconds); Interventions: exercise training and LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
LAMA/LABA with exercise training with behaviour modification versus LAMA with behaviour modification
An improvement in 6MWD (MD 32 metres, 95% CI 13 to 51; 128 participants) was demonstrated after eight weeks of the 12‐week PHYSACTO study for LAMA/LABA with exercise training compared to LAMA. The mean difference in 6MWD was 21 metres (95% CI −1 to 43; Troosters 2018, 123 participants; moderate‐certainty evidence; Analysis 11.6) at end intervention. An improvement in ESWT was demonstrated after eight weeks (MD 102 seconds, 95% CI 41 to 162; 137 participants) and at end intervention (MD 69 seconds, 95% CI 8 to 129; Troosters 2018, 130 participants; high‐certainty evidence; Analysis 11.7).
11.6. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 6 6MWD (metres); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
11.7. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 7 ESWT (seconds); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification.
LAMA/LABA with exercise training with behaviour modification versus LAMA/LABA with behaviour modification
The mean difference in 6MWD was 6 metres (95% CI −12 to 25; 137 participants) after eight weeks and was 2 metres (95% CI −19 to 23; Troosters 2018, 133 participants; moderate‐certainty evidence; Analysis 11.8) following the 12‐week PHYSACTO study for LAMA/LABA with exercise training compared to LAMA/LABA. The mean difference in ESWT was 40 seconds (95% CI −24 to 105; 142 participants) after eight weeks and was 22 seconds (95% CI −42 to 85; Troosters 2018, 137 participants; moderate‐certainty evidence; Analysis 11.9) at end intervention.
11.8. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 8 6MWD (metres); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification.
11.9. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 9 ESWT (seconds); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification.
Exercise training with physical activity counselling with pedometer versus pedometer
An improvement in ESWT (MD 7 seconds, 95% CI 4 to 10) was demonstrated following an eight‐week physical activity counselling and exercise training programme with pedometer compared to pedometer. This improvement was maintained at 12‐week (MD 8 seconds, 95% CI 5 to 12) and 12‐month follow‐up (MD 8 seconds, 95% CI 4 to 11; Varas 2018, 33 participants; moderate‐certainty evidence; Analysis 11.10).
11.10. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 10 change in ESWT (seconds); Intervention: physical activity counselling and exercise training with pedometer vs. pedometer.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Web‐based pulmonary rehabilitation versus centre‐based pulmonary rehabilitation
The mean difference in ESWT was 5 seconds (95% CI −112 to 121; Chaplin 2017, 62 participants; low‐certainty evidence; Table 21) following a seven‐week study of web‐based pulmonary rehabilitation compared to a centre‐based programme.
Exercise training (eccentric cycle training) versus exercise training (concentric cycle training)
The mean difference in peak work rate was −3 watts (95% CI −11 to 5; Sena 2013m 16 participants; very low‐certainty evidence; Table 21) following a 10‐week study of eccentric cycle training compared to concentric training.
Home‐based pulmonary rehabilitation versus centre‐based pulmonary rehabilitation
The mean difference in 6MWD was 19 metres (95% CI −3 to 40) at end intervention and −5 metres (95% CI −29 to 19; Holland 2017, 148 participants; low‐certainty evidence; Analysis 12.1) at 14‐month follow‐up after an equivalence study comparing an eight‐week home‐based pulmonary rehabilitation programme with a centre‐based programme.
12.1. Analysis.

Comparison 12 Exercise capacity: intervention vs. intervention, Outcome 1 change in 6MWD (metres); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation.
Water‐based exercise training versus land‐based exercise training
The mean difference in change in 6MWD was 14 metres (95% CI −41 to 13; Felcar 2018, 36 participants; low‐certainty evidence; Analysis 12.2) following a six‐month study of water‐based exercise training compared to a land‐based programme. The mean difference in change in ISWD was −52 metres (95% CI −107 to 3; Felcar 2018, 36 participants; low‐certainty evidence; Analysis 12.3) at end intervention. The mean difference in change in VO2max was −1.2 mL/min (95% CI −2.6 to 0.2; Felcar 2018, 36 participants; low‐certainty evidence; Analysis 12.4) at end intervention.
12.2. Analysis.

Comparison 12 Exercise capacity: intervention vs. intervention, Outcome 2 change in 6MWD (metres); Interventions: water‐based exercise training vs. land‐based exercise training.
12.3. Analysis.
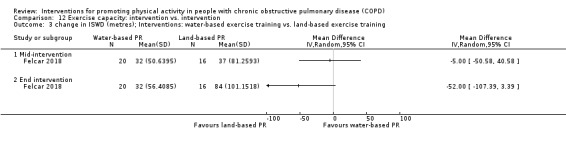
Comparison 12 Exercise capacity: intervention vs. intervention, Outcome 3 change in ISWD (metres); Interventions: water‐based exercise training vs. land‐based exercise training.
12.4. Analysis.

Comparison 12 Exercise capacity: intervention vs. intervention, Outcome 4 change in VO2max (ml/min); Interventions: water‐based exercise training vs. land‐based exercise training.
Tai Chi versus pulmonary rehabilitation
The mean difference in 6MWD was 20 metres (95% CI −3 to 43) after two weeks and 16 metres (95% CI −7 to 39) after 14 weeks of a 24‐week study of Tai Chi compared to pulmonary rehabilitation. An improvement in 6MWD (MD 41 metres, 95% CI 18 to 64; Polkey 2018, 110 participants; low‐certainty evidence; Analysis 12.5) was demonstrated at end intervention.
12.5. Analysis.

Comparison 12 Exercise capacity: intervention vs. intervention, Outcome 5 6MWD (metres); Interventions: Tai Chi vs. pulmonary rehabilitation.
Calisthenics versus exercise training
The mean difference in peak work load was 30 watts (SD 30) in the callisthenics group and 48 watts (SD 30) in the exercise training group (P = 0.04). The mean difference in cycle endurance time was 8 minutes (SD 7) in the callisthenics group and 17 minutes (SD 24) in the exercise training group (P = 0.08). The mean difference in 6MWD was 424 metres (SD 114) in the callisthenics group and 483 metres (SD 89) in the exercise training group (P = 0.30; Probst 2011, 40 participants; low‐certainty evidence; Table 21) following a 12‐week callisthenics and breathing exercises programme compared to exercise training.
Exercise training (outdoor walking) versus exercise training (cycle ergometry)
An improvement in 6MWD (MD −155 metres, 95% CI −215 to −95; Gamper 2019, 16 participants; moderate‐certainty evidence; Table 21) was demonstrated in the cycle ergometry group following a three‐week study comparing outdoor walking and cycle ergometry.
Physical activity counselling versus pulmonary rehabilitation
The mean difference in 6MWD was −25 metres (95% CI −68 to 18; Widyastuti 2018, 36 participants; low‐certainty evidence; Table 21) following a six‐week physical activity counselling intervention compared to pulmonary rehabilitation.
The mean difference in ISWD was −4 metres (95% CI −60 to 51; O'Neill 2018, 33 participants; low‐certainty evidence; Table 21) following a 12‐week physical activity counselling programme compared to a six‐week pulmonary rehabilitation programme.
Exercise training with tapering supervision versus exercise training
The mean difference in 6MWD was 60 metres (95% CI −14 to 134) at end intervention and 97 metres (95% CI −7 to 201; Rinaldo 2017, 24 participants; moderate‐certainty evidence; Analysis 12.6) at 42‐week follow‐up after a 28‐week study of exercise training with tapered supervision compared to supervised exercise training.
12.6. Analysis.

Comparison 12 Exercise capacity: intervention vs. intervention, Outcome 6 6MWD (metres); Interventions: exercise training with tapered supervision vs. supervised exercise training.
Adherence intervention versus pulmonary rehabilitation
The mean difference in 6MWD was 5 metres (95% CI −57 to 67; Steele 2019, 63 participants; low‐certainty evidence; Table 21) following six months of an adherence intervention compared to eight weeks of pulmonary rehabilitation.
Maintenance following high‐intensity interval training: telerehabilitation versus centre‐based programme
The mean difference in change in 6MWD was −7 metres (95% CI −35 to 20) and peak work rate was −3 watts (95% CI −16 to 10; Vasilopoulou 2017; 97 participants; low‐certainty evidence; Table 21) following 12 months of telerehabilitation compared to a centre‐based maintenance programme.
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Inpatient exercise training versus no intervention
Improvements in exercise capacity at time of hospital discharge were demonstrated following two inpatient training interventions compared to no intervention.
An improvement in two‐minute walk distance (MD 13 metres, 95% CI 3 to 23; Tahirah 2015, 32 participants; very low‐certainty evidence; Table 21) was demonstrated at discharge following inpatient walking and functional‐resistance training compared to no intervention.
An improvement in 6MWD (MD 94 metres, 95% CI 24 to 164) was demonstrated at discharge following inpatient resistance training compared to no intervention. The mean difference was 56 metres (95% CI −50 to 162; Borges 2014, 29 participants; low‐certainty evidence; Analysis 9.8) at four‐week follow‐up.
9.8. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 8 6MWD (metres); Intervention: exercise training [inpatient].
INTERVENTION: Physical activity counselling
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Physical activity counselling versus no intervention
The same 12‐week intervention has been used in three studies (two within this comparison). The mean difference in 6MWD was 26 metres (95% CI −12 to 64; Hospes 2009, 35 participants; low‐certainty evidence; Table 21) in one study when compared to no intervention. In a subsequent study, the median difference in change in 6MWD in participants recruited from primary care was 10 metres (IQR −7 to 38) in the physical activity counselling group compared to 3 metres (IQR −18 to 22) in the no‐intervention group (P = 0.291; 40 participants) at end intervention. The median difference in change in 6MWD in participants recruited from primary care was 20 metres (IQR 8 to 54) in the physical activity counselling group compared to 13 metres (IQR −2 to 38) in the no‐intervention group (P = 0.313; Altenburg 2015, 38 participants; low‐certainty evidence; Table 21) at 12‐month follow‐up. The median difference in change in 6MWD in participants recruited from secondary care was greater (23 metres, IQR 0 to 51) in the physical activity counselling group compared to 4 metres (IQR −32 to 27) in the no‐intervention group (P = 0.049; 43 participants) at end intervention. The median difference in change in 6MWD in participants recruited from secondary care was 25 metres (IQR 4 to 52) in the physical activity counselling group compared to 17 metres (IQR −9 to 57) in the no‐intervention group (P = 0.555; Altenburg 2015, 39 participants; low‐certainty evidence; Table 21) at 12‐month follow‐up.
The mean difference in 6MWD was 13 metres (95% CI 2 to 23; Demeyer 2017, 267 participants; moderate‐certainty evidence; Table 21) was demonstrated following a 12‐week telecoaching intervention compared to no intervention.
The mean difference in 6MWD was −2 metres (95% CI −11 to 8; Arbillaga‐Etxarri 2018, 280 participants; low‐certainty evidence; Table 21) following a 12‐month Urban Training intervention compared to no intervention.
The mean difference in 6MWD was −16 metres (95% CI −46 to 15; 71 participants), ISWD was 23 metres (95% CI −13 to 60; 64 participants) and ESWT was −54 seconds (95% CI −245 to 137; Wootton 2017, 65 participants; low‐certainty evidence; Table 21) following 12 months of physical activity counselling compared to no intervention, which was completion of phase 2 of a 14‐month study that all participants began with eight weeks of ground‐based walking training.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Physical activity counselling with optional supervised exercise versus optional supervised exercise
The mean difference in 6MWD was 8 metres (95% CI −18 to 34; 139 participants) after 12 weeks, 10 metres (95% CI −17 to 37; 132 participants) after six months and 10 metres (95% CI −18 to 38; Vorrink 2016, 121 participants; low‐certainty evidence; Analysis 11.11) following a study of a 12‐month text message‐based physical activity counselling intervention following pulmonary rehabilitation with optional supervised exercise compared to optional supervised exercise.
11.11. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 11 6MWD (metres); Interventions: physical activity counselling (app) with optional supervised exercise vs. optional supervised exercise.
Pedometer with physical activity counselling versus physical activity counselling
An improvement in 6MWD (MD 13 metres, 95% CI 1 to 25; Mendoza 2015, 97 participants; moderate‐certainty evidence; Table 21) was demonstrated following a 12‐week study of pedometer use with physical activity counselling compared to physical activity counselling.
Physical activity counselling with pedometer versus pedometer
The mean difference in change in 6MWD was −1 metre (SD 56) in the physical activity counselling with pedometer group and 4 metres (SD 47) in the pedometer group (P = 0.72; Wan 2017, 109 participants; low‐certainty evidence; Table 21) following a 12‐week web‐based intervention with pedometer compared to pedometer.
The mean difference in 6MWD was −5 metres (95% CI −116 to 106) after 12 weeks and −23 metres (95% CI −134 to 88; Nguyen 2009, 17 participants Analysis 11.12) following a six‐month study of physical activity counselling intervention with pedometer compared to pedometer. The mean difference in peak work rate was 0 watts (95% CI −25 to 25; Nguyen 2009; 17 participants; low‐certainty evidence; Table 21) at end intervention.
11.12. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 12 6MWD (metres); Interventions: physical activity counselling (app) with pedometer vs. pedometer.
Physical activity counselling with pulmonary rehabilitation versus pulmonary rehabilitation
An improvement in ESWT (MD 96 seconds, 95% CI 28 to 164; Mantoani 2018, 44 participants; very low‐certainty evidence; Table 21) was demonstrated following a 12‐week physical activity counselling intervention with pulmonary rehabilitation.
The addition of the same 12‐week intervention did not result in improved exercise capacity in two studies where participants in both groups received pulmonary rehabilitation. The mean difference in two‐minute step test was 2 steps (95% CI −24 to 28; De Blok 2006, 16 participants; low‐certainty evidence; Table 21) in one study. In a subsequent study, the median difference in 6MWD was 17 m (IQR −27 to 42) in the physical activity counselling and pulmonary rehabilitation group compared to 25 (IQR −15 to 60) in the pulmonary rehabilitation group at end intervention. The median difference in 6MWD was 7 m (IQR −32 to 51) in the physical activity counselling and pulmonary rehabilitation group compared to 10 metres (IQR −15 to 87; P = 0.503; Altenburg 2015, 23 participants; low‐certainty evidence; Table 21) in the pulmonary rehabilitation group at 12‐month follow‐up.
The median difference in change in ISWD was 60 metres (IQR 20 to 90) in the physical activity counselling and pulmonary rehabilitation group compared to 50 metres (IQR 10 to 90; P = 0.83; Nolan 2017, 122 participants) in the pulmonary rehabilitation group at eight weeks (following pulmonary rehabilitation) in a study of a six‐month in‐person physical activity counselling intervention with eight weeks of pulmonary rehabilitation compared to eight weeks of pulmonary rehabilitation. The median difference in change in ISWD was 30 metres (IQR 0 to 70) in the physical activity counselling and pulmonary rehabilitation group compared to 10 metres (IQR −30 to 70; P = 0.25; Nolan 2017, 113 participants; low‐certainty evidence; Table 21) in the pulmonary rehabilitation group at end intervention.
The mean difference in 6MWD was 18 metres (95% CI −22 to 59) after 12 weeks and 21 metres (95% CI −11 to 53; Cruz 2016, 26 participants; low‐certainty evidence; Analysis 11.13) following a six‐month study of physical activity counselling intervention with 12 weeks of pulmonary rehabilitation compared to 12 weeks of pulmonary rehabilitation.
11.13. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 13 6MWD (metres); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation.
The mean difference in 6MWD was −22 metres (95% CI −131 to 87; Kawagoshi 2015, 27 participants; low‐certainty evidence; Table 21) following a 12‐month study of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation
The mean difference in change in 6MWD was 8 metres (SE 14, P = 0.59) at end intervention and 2 metres (SE 16, P = 0.90; Loeckx 2018, 50 participants; very low‐certainty evidence; Table 21) at nine‐month follow‐up after a study of 12 weeks of physical activity counselling with pulmonary rehabilitation compared to pulmonary rehabilitation after all participants undertook 12 weeks of pulmonary rehabilitation. The mean difference in change in ESWT was −80 seconds (SE 71, P = 0.26) at end intervention and 153 seconds (SE 79, P = 0.06; Loeckx 2018, 50 participants; very low‐certainty evidence; Table 21) at nine‐month follow‐up.
Physical activity counselling using step‐tracking with pulmonary rehabilitation versus sham intervention with pulmonary rehabilitation
The mean difference in change in 6MWD was 11 metres (95% CI −22 to 44; 67 participants) after 12 weeks and 7 metres (95% CI −38 to 52; Burtin 2015, 50 participants; low‐certainty evidence; Analysis 11.14) following a six‐month study of physical activity counselling with pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation.
11.14. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 14 change in 6MWD (metres); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation.
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Physical activity counselling versus no intervention
The mean difference in change in 6MWD was 3 metres (95% CI −53 to 59; Hornikx 2015, 27 participants; low‐certainty evidence; Table 21) following a four‐week study comparing physical activity counselling to no intervention following hospital admission for AECOPD.
INTERVENTION: Self‐management
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Self‐management versus no intervention
The mean difference in ISWD was 16 metres (95% CI −2 to 34; 155 participants) at end intervention and 16 metres (95% CI −5 to 37; Mitchell 2013, 184 participants; low‐certainty evidence; Analysis 9.6) at six‐month follow‐up after a six‐week SPACE programme compared to no intervention. An improvement in ESWT (MD 118 seconds, 95% CI 14 to 221; 155 participants) was demonstrated at end intervention and at six‐month follow‐up (MD 184 seconds, 95% CI 73 to 294; Mitchell 2013, 184 participants; moderate‐certainty evidence; Analysis 9.7).
9.6. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 6 change in ISWD (metres); Intervention: self‐management (SPACE).
9.7. Analysis.

Comparison 9 Exercise capacity: intervention vs. no intervention, Outcome 7 change in ESWT (seconds); Intervention: self‐management (SPACE).
The mean difference in 6MWD was 100 metres (95% CI −15 to 215; Tabak 2014b, 20 participants; low‐certainty evidence; Table 21) following a 12‐week self‐management intervention compared to no intervention.
COMPARISON: Intervention versus intervention (clinically‐stable COPD)
Self‐management versus education and symptom monitoring
A mean improvement in 6MWD (361 metres, SE 3) was demonstrated in the self‐management group compared to 351 metres (SE 3) in the education and symptom‐monitoring group (P = 0.03; Blumenthal 2014, 326 participants; moderate‐certainty evidence; Table 21) following 16 weeks of self‐management compared to education and symptom monitoring.
COMPARISON: Intervention versus no intervention (acute exacerbation of COPD)
Self‐management versus no intervention
The mean difference in ISWD was 2 metres (95% CI −62 to 66) and ESWT was 80 seconds (95% CI −216 to 375; Kanabar 2015, 25 participants; very low‐certainty evidence; Table 21) following a seven‐day post‐admission self‐management programme compared to no intervention.
INTERVENTION: Pharmacological treatments
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
LAMA versus placebo
The median difference in change in cycle endurance time was 26 seconds (IQR −106 to 117) in the LAMA group compared to −16 seconds (IQR −109 to 18) in the placebo group (P = 0.093; Beeh 2014, 108 participants; moderate‐certainty evidence; Table 21) following a three‐week study of LAMA compared to placebo.
Data were not presented in another 12‐week study comparing LAMA with placebo but reported that results favoured the intervention group (NCT00144326, 248 participants; very low‐certainty evidence; Table 21).
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
LAMA with behaviour modification versus placebo with behaviour modification
The mean difference in 6MWD was −5 metres (95% CI −25 to 15; 119 participants) after eight weeks, and was −7 metres (95% CI −29 to 15; Troosters 2018, 115 participants; moderate‐certainty evidence; Analysis 11.15) following the 12‐week PHYSACTO study for LAMA with behaviour modification compared to placebo with behaviour modification. The mean difference in ESWT was 10 seconds (95% CI −39 to 60; 132 participants) after eight weeks and 12 seconds (95% CI −40 to 65; Troosters 2018, 126 participants; moderate‐certainty evidence; Analysis 11.16) at end intervention.
11.15. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 15 6MWD (metres); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification.
11.16. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 16 ESWT (seconds); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification.
LAMA/LABA with behaviour modification versus placebo with behaviour modification
An improvement in cycle endurance time (least squares MD 55 seconds, 95% CI 6 to 105; Watz 2017, 250 participants; moderate‐certainty evidence; Table 21) was demonstrated following eight weeks of LAMA/LABA with four weeks of behavioural modification.
An improvement in 6MWD (MD 21 metres, 95% CI 2 to 40; 128 participants) was demonstrated after eight weeks of the 12‐week PHYSACTO study for LAMA/LABA with behaviour modification compared to placebo with behaviour modification. The mean difference was 12 metres (95% CI −9 to 33; Troosters 2018, 125 participants; moderate‐certainty evidence; Analysis 11.17) at end intervention. An improvement in ESWT was demonstrated after eight weeks (MD 71 seconds, 95% CI 16 to 126; 137 participants) and at end intervention (MD 59 seconds, 95% CI 3 to 115; Troosters 2018, 133 participants; high‐certainty evidence; Analysis 11.18).
11.17. Analysis.
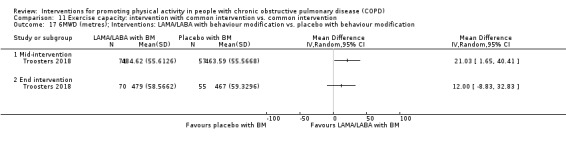
Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 17 6MWD (metres); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
11.18. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 18 ESWT (s); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification.
LABA with LAMA and behaviour modification versus LAMA and behaviour modification
An improvement in 6MWD (MD 26 metres, 95% CI 7 to 45; 133 participants) was demonstrated after eight weeks of the 12‐week PHYSACTO study for LABA with LAMA and behaviour modification compared to LAMA and behaviour modification. The mean difference was 19 metres (95% CI −2 to 40; Troosters 2018, 130 participants; moderate‐certainty evidence; Analysis 11.19) at end intervention. An improvement in ESWT (MD 61 seconds, 95% CI 6 to 117; 139 participants) was demonstrated after eight weeks. The mean difference was 47 seconds (95% CI −10 to 104; Troosters 2018, 135 participants; moderate‐certainty evidence; Analysis 11.20).
11.19. Analysis.
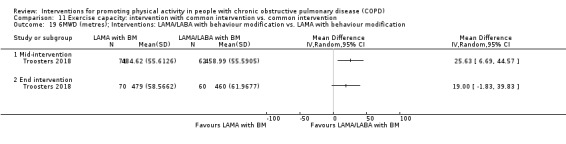
Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 19 6MWD (metres); Interventions: LAMA/LABA with behaviour modification vs. LAMA with behaviour modification.
11.20. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 20 ESWT (seconds); Interventions: LAMA/LABA with behaviour modification vs. LAMA with behaviour modification.
Angiotensin‐converting enzyme (ACE) inhibitor with pulmonary rehabilitation versus placebo with pulmonary rehabilitation
A reduction in change in peak work rate (MD −8 watts, 95% CI −13 to −3) and peak oxygen uptake (MD −1.0 mL/min/kg, 95% CI −2.0 to −0.1) were demonstrated following a 10‐week study of an ACE inhibitor with pulmonary rehabilitation compared to a placebo with pulmonary rehabilitation.The mean difference in change in oxygen uptake efficiency was 0.4 (95% CI −2.0 to 2.8) and oxygen uptake efficiency slope was −122 mL/min (95% CI −292 to 49; Curtis 2016, 65 participants; moderate‐certainty evidence; Table 21) at end intervention.
INTERVENTION: Nutritional supplementation
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Nutritional supplement with pulmonary rehabilitation versus placebo with pulmonary rehabilitation
The mean difference in 6MWD was −4 metres (SD 12) and cycle endurance time was −110 seconds (SD 70; Van de Bool 2017, 73 participants; moderate‐certainty evidence; Table 21) following a four‐month study of nutritional supplementation with pulmonary rehabilitation compared to a placebo with pulmonary rehabilitation.
Nutritional supplement with physical activity counselling versus physical activity counselling
The mean difference in change in endurance time was −93 seconds (SD 90; Van de Bool 2017, 61 participants; moderate‐certainty evidence; Table 21) following stage 2 of a 15‐month study after eight months of nutritional supplementation with physical activity counselling compared to physical activity counselling in people with low muscle mass.
INTERVENTION: Supplemental oxygen
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Lightweight versus standard oxygen‐cylinder use
The mean difference in ISWD was 40 metres (95% CI −64 to 144) and ESWT was 170 seconds (95% CI −47 to 387; Sandland 2008, 20 participants; moderate‐certainty evidence; Table 21) following an eight‐week study of supplemental oxygen following pulmonary rehabilitation compared to placebo.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Supplemental oxygen with pulmonary rehabilitation versus sham intervention with pulmonary rehabilitation
The mean difference in change in ISWD was 5 metres (95% CI −14 to 24; 94 participants) at end intervention and 9 metres (95% CI −12 to 30; Alison 2019, 75 participants; moderate‐certainty evidence; Analysis 11.21) at six‐month follow‐up after eight weeks of supplemental oxygen with pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation. The mean difference in change in ESWT was 15 seconds (95% CI −102 to 132; 95 participants) at end intervention and −15 seconds (95% CI −143 to 113; Alison 2019, 74 participants; moderate‐certainty evidence; Analysis 11.22) at six‐month follow‐up.
11.21. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 21 change in ISWD (metres); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation.
11.22. Analysis.

Comparison 11 Exercise capacity: intervention with common intervention vs. common intervention, Outcome 22 change in ESWT (seconds); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation.
INTERVENTION: Other interventions
COMPARISON: Intervention versus no intervention (clinically‐stable COPD)
Endobronchial valve surgery versus no intervention
Results for 6MWD favoured the intervention group six months after endobronchial valve surgery compared to no intervention (MD 104 metres, SD 165; Hartman 2016; 43 participants; Table 21).
COMPARISON: Intervention versus sham intervention (clinically‐stable COPD)
Singing versus sham intervention
Results for ISWD favoured the intervention group following an eight‐week singing intervention compared to a sham intervention (MD −22 metres, 95% CI −56 to 12; Lord 2012; 24 participants; Table 21).
Neuromuscular electrical stimulation versus placebo
Improvement in change in 6MWD was demonstrated following a six‐week neuromuscular electrical stimulation (NMES) programme compared to placebo, with results favouring the intervention group at 12‐week follow‐up (6 weeks: MD 36 metres, 95% CI 12 to 60; 12 weeks: MD 7 metres, 95% CI −32 to 46; Maddocks 2016, 52 participants; Analysis 8.1).
8.1. Analysis.

Comparison 8 Exercise capacity: intervention vs. placebo/sham, Outcome 1 change in 6MWD (metres); Intervention; neuromuscular electrical stimulation.
COMPARISON: Intervention versus standard common intervention (clinically‐stable COPD)
Inspiratory muscle training with pulmonary rehabilitation versus sham with pulmonary rehabilitation
An improvement in cycle endurance time (MD 98 seconds, 95% CI 17 to 179; Charususin 2018, 139 participants; high‐certainty evidence; Table 21) was demonstrated following a 12‐week study of the addition of inspiratory muscle training to pulmonary rehabilitation compared to a sham intervention with pulmonary rehabilitation. The mean difference in 6MWD was 1 metre (95% CI −13 to 15, 169 participants), peak work rate was 5.2 watts (95% CI −0.4 to 10.8) and VO2max was 0.01 mL/min (95% CI −0.1 to 0.1; Charususin 2018, 92 participants; moderate‐certainty evidence; Table 21).
Non‐invasive ventilation with pulmonary rehabilitation versus pulmonary rehabilitation
The mean difference in 6MWD was 2 metres (95% CI −19 to 23), ESWT was 103 seconds (95% CI −69 to 276) and peak oxygen uptake was 0.3 mL/min/kg (95% CI −0.9 to 1.4; Duiverman 2008, 56 participants; low‐certainty evidence; Table 21) following a 12‐week study of non‐invasive positive pressure ventilation with pulmonary rehabilitation compared to pulmonary rehabilitation.
Appendix 6. Secondary outcome: adherence
Overall, adherence was inconsistently defined and variably reported using a range of variables. Available information is presented in Characteristics of included studies and Table 22. Documentation was provided in 51 studies.
5. Adherence.
| Study | Comparison (setting); Clinical stability unless indicated | Data regarding adherence |
| Alison 2019 | Supplemental oxygen with exercise training vs. sham with exercise training | Attended ≥ 16 sessions; oxygen 48 participants; sham 41 participants |
| Arbillaga‐Etxarri 2018 | Urban Training™ vs. no intervention | Urban training (132 participants)
|
| Benzo 2016 | Self‐management (health coaching) with PR referral vs. PR referral | Attendance at PR:
85% of participants completed self‐management intervention (≥ 15 of 21 calls) |
| Blumenthal 2014 | Self‐management (coping skills training) vs. education and symptom monitoring | Both groups: median number of completed sessions 14 (100%) |
| Borges 2014 | Exercise training (whole‐body resistance training) vs. no intervention (inpatient) | Attendance: 5.6 sessions (95%); Intensity (weight load): increase 9.7% |
| Breyer 2010 | Exercise training (Nordic walking) with education vs. education | "All patients achieved the preset goal for maximum heart rate to ensure training efficiency (> 75% of the initial maximum heart rate)… none of the patients had any difficulties in performing Nordic Walking adequately" |
| Burtin 2015 | Physical activity counselling with PR vs. sham with PR | PR: "did not systematically record adherence"; Physical activity counselling/sham (8 scheduled sessions): 82% attendance |
| Casaburi 2012 | Supplemental oxygen (lightweight ambulatory) vs. supplemental oxygen (E‐cylinder) | Oxygen use: lightweight ambulatory 8.9 (4.8) hours per day; E‐cylinder 16.9 (3.9) hours per day |
| Charususin 2018 | Inspiratory muscle training with PR vs. sham with PR | Completed prescribed sessions of inspiratory muscle training: inspiratory muscle training 79 (4)%; PR 81 (4)% Intensity (inspiratory muscle training load relative to baseline Pimax): 47 (2)% Week 1; 84 (4)% Week 12 |
| Cruz 2016 | Physical activity counselling with PR vs. PR | "All participants received allocated intervention" |
| Curtis 2016 | ACE inhibitor with PR vs. placebo with PR |
|
| De Blok 2006 | Physical activity counselling with PR vs. PR | Physical activity counselling: individual exercise counselling 4 sessions attended, diary‐recorded daily step counts 96% |
| De Roos 2017 | Exercise training vs. no intervention | Exercise training attendance 18.2 (1.1) of 20 scheduled sessions, home‐based walking 8.6 (0.4) sessions |
| Demeyer 2017 | Physical activity counselling vs. no intervention | PAC median 6 (IQR 4 to 9) contacts (range 0 to 25) |
| Duiverman 2008 | Non‐invasive ventilation with PR vs. PR | PR
NIPPV
|
| Effing 2011 | Exercise training (COPE‐active) with self‐management vs. self management | COPE‐active 56 (73%) participants completed (not defined) |
| Felcar 2018 | Water‐based exercise training vs. land‐based exercise training | "All studied patients completed 60 sessions" |
| Goris 2003 | Nutritional supplement vs. no intervention | Adherence: nutritional supplement 95 (6)% Month 1; 89 (14)% Month 3 |
| Holland 2017 | Home‐based PR vs. centre‐based PR |
|
| Jolly 2018 | Self‐management vs. no intervention | Self‐management 999 (86%) of 1156 calls, participated in all 4 scheduled calls 218 (75%) of 289 participants |
| Kawagoshi 2015 | Physical activity counselling with PR vs. PR | Days of home‐based PR: 239 (25) days a year, 65 (7)%, 4 days a week Days of pedometer wear: 293 (49) days a year, 80 (13)% |
| Lord 2012 | Singing vs. sham | Attendance: singing 14.5 of 16 scheduled sessions; sham 7 of 8 scheduled sessions |
| Maddocks 2016 | NMES vs. placebo | Intervention: 42 sessions (1260 minutes)
|
| Mendoza 2015 | Pedometer with physical activity counselling vs. physical activity counselling | Physical activity counselling and pedometer strong correlations between diary and device memory step count (r2 Month 1 0.996, Month 2 0.999, Month 3 0.975) "suggesting a high degree of compliance with the program." |
| Moy 2015a | Physical activity counselling with pedometer vs. pedometer | Valid step‐count data
Physical activity counselling with pedometer:
|
| Nakamura 2016 | LAMA (aclidinium bromide) vs. LAMA (tiotropium) | Adherence (both groups) "estimated to be 100% during study period" |
| Nguyen 2009 | Physical activity counselling with pedometer vs. pedometer | Exercise and symptom data submitted: PAC with pedometer 87%; pedometer 66% |
| Nolan 2017 | Physical activity counselling with PR vs. PR | Physical activity counselling with PR (revised step‐count goal, 5% increments, 8 possible occasions) did not occur 5 (10) occasions |
| O'Neill 2018 | Physical activity counselling vs.PR |
Attended 75% sessions: 100%; mean 11.8 (SD 0.6) of 12 planned consultations
Attended 75% sessions: 70% (9 of 13 participants); mean 10.5 (SD 1.2) of 12 planned classes |
| Orme 2018 | Feedback and education vs. no intervention; Education vs. no intervention; Feedback with education vs. education (post‐admission) |
Intervention delivery: feedback and education 21 (95%) sessions ; education 1 session not delivered |
| Polkey 2018 | Tai Chi vs. PR | "Both groups had high compliance in terms of attendance rate (present days/total expected days)" Tai Chi 91 (1)%; PR 87 (2)% |
| Priori 2017 | Physical activity counselling vs. no intervention | Days accessed website: Physical activity counselling 87 (15)% |
| Probst 2011 | Exercise training (callisthenics) vs. exercise training (endurance and strength training) | Attendance (32 planned sessions): callisthenics 19 (61%) sessions; endurance and strength training 20 (63%) sessions |
| Rinaldo 2017 | Exercise training with tapered supervision vs. supervised exercise training | Attendance: exercise training with tapered supervision 100%; supervised exercise training 87% |
| Sandland 2008 | Supplemental oxygen vs. placebo (air) | Number of cylinders used: oxygen 20.2 (13.7); placebo 10.7 (4.9); P < 0.002 |
| Schuz 2015 | Self‐management (health mentoring) vs. sham | Attendance: phone contacts median 9.5 of 16 planned sessions (range 1 to 21) |
| Steele 2019 | Adherence intervention vs. PR | Attended ≥ 80% sessions: Adherence intervention: 80% (37 of 46 allocated participants); PR: 57% (25 of 44 allocated participants) |
| Tabak 2014a | Physical activity counselling with optional supervised exercise vs. optional supervised exercise | Physical activity counselling activity coach: 86% "complied" [time activity coach was worn], wear time 17.5 (2.2) days (109% of prescribed), 588 (101) min per day Physical activity counselling diary: 1 participant "complied" (completed diary every day), 1 participant did not use the web portal, 1 participant used web portal for 4 days; completed 17.3 (7.8) times a patient (58% of prescribed) |
| Tabak 2014b | Self‐management vs. no intervention | Web portal: 86% of days Triage diary: most used module (median 83%) Exercise: 127 exercise schemes performed of 569 schemes prescribed (median 21%) Activity coach‐module: used for 299 days (132 days in monitoring mode, 167 days in feedback mode), "rarely used outside of the measurement weeks" |
| Varas 2018 | Physical activity counselling and exercise training with pedometer vs. pedometer |
"2 (participants) were excluded for non‐compliance during the intervention phase" Author correspondence states "non‐compliance of the program was established previously, before starting the study, by considering none achieving the individual target of steps/week for three consecutive weeks" |
| Vasilopoulou 2017 | Maintenance (telerehabilitation) vs. no intervention; Maintenance (centre‐based) vs. no intervention; Maintenance (telerehabilitation) vs. maintenance (centre‐based) following high‐intensity interval training |
"Adherence to the home‐based maintenance tele‐rehabilitation and hospital‐based, outpatient, maintenance programmes were assessed by the adherence rate (actual number of sessions/total expected number of session×100). Adherence to measurements of vital signs, home exercises, responses to questionnaires and daily steps were recorded for each participant by the number of registrations entered divided by the number of those recommended." "Overall compliance rate" (twice‐weekly supervised exercise training sessions): telerehabilitation 93.5%; centre‐based 91% |
| Vorrink 2016 | Physical activity counselling with optional supervised exercise vs. optional supervised exercise | App accessed: PAC with optional supervised exercise 89 (19)% days, accessed app and personal physical activity goal obtained 34 (16)% days |
| Wan 2017 | Physical activity counselling with pedometer vs. pedometer | Pedometer
Website use: Physical activity counselling and pedometer > 4 logins a month "suggests good adherence to the requested weekly logins" (data not shown) |
| Watz 2016 | LAMA/LABA vs. placebo | Combined treatment periods 1 and 2: LAMA/LABA 99.5%; placebo 99.6% |
| Wootton 2017 | Exercise training (ground‐based walking) vs. no intervention | Attendance: 18 (6) of 24 scheduled sessions; Progression (duration): 76 (84%) participants |
| Physical activity counselling with pedometer vs. no intervention (following ground‐based walking) | % Adherence (number of walks reported divided by the number of prescribed walks) Physical activity counselling: 8 months mean 52 (SD 17); 14 months 52 (55) No intervention: 8 months mean 92 (SD 38); 14 months 77 (54) |
Data are mean or mean (SD) unless indicated ACE: angiotensin‐converting enzyme; COPD: chronic obstructive pulmonary disease; LABA: long‐acting beta2‐agonist; LAMA: long‐acting muscarinic antagonist; min: minutes; n: number; Pimax: maximal inspiratory mouth pressure
In studies including pulmonary rehabilitation or exercise training, adherence was primarily reported as programme attendance, which was highly variable ranging from 48% to > 90% (Alison 2019; Benzo 2016; Curtis 2016; Cruz 2016; De Roos 2017; Felcar 2018; Kawagoshi 2015; O'Neill 2018; Polkey 2018; Steele 2019; Tahirah 2015; Troosters 2018). Some studies also reported progression of training intensity or duration (Borges 2014; Duiverman 2008; Tsai 2016; Wootton 2017) or programme completion (Effing 2011; Holland 2017). Breyer 2010 did not report attendance or programme completion, but did report training intensity according to prespecified criteria. Burtin 2015 reported as a study limitation that programme attendance was not recorded in their study.
Exclusions for non‐compliance and dropouts were also reported (Van de Bool 2017; Varas 2018). Vasilopoulou 2017 did not describe adherence to the initial eight‐week pulmonary rehabilitation programme but did present a high (> 90%) "overall compliance rate" for the 12‐month home‐based telerehabilitation maintenance period.
For physical activity counselling interventions delivered in‐person, high levels of adherence were demonstrated (≥ 74%) as assessed by programme attendance/completion (Benzo 2016; Burtin 2015;De Blok 2006; Demeyer 2017; O'Neill 2018; Orme 2018). One study reported poor adherence with a prespecified progression protocol for revision of step‐count goals (did not occur mean 5 (SD 10) of eight planned occasions; Nolan 2017).
For physical activity counselling interventions delivered remotely or indirectly, methods for assessment and results for adherence varied widely as given in participant self‐report (Arbillaga‐Etxarri 2018), completion of diaries/access of online repositories (Mendoza 2015; Moy 2015a; Nguyen 2009; Priori 2017; Tabak 2014b; Vorrink 2016; Wan 2017), and device‐wearing time (Tabak 2014a).
In studies including self‐management, deteriorating levels of adherence were demonstrated over time. Adherence (assessed by completion according to prespecified attendance/delivery criteria) was 86% over 12 weeks (Troosters 2018), 75% over six months (Jolly 2018), and lower again over 12 months (median 9.5 of 16 planned calls (Schuz 2015)).
Adherence was not consistently assessed for pharmacological interventions, but available data generally demonstrated high levels of adherence (Curtis 2016; Nakamura 2016; Troosters 2014; Troosters 2018; Watz 2016).
High levels of adherence were demonstrated as assessed by: nutritional supplement consumption (Goris 2003); supplemental oxygen use (Casaburi 2012; Sandland 2008); completion according to prescribed number of sessions of inspiratory muscle training (80%; Charususin 2018); non‐invasive ventilation use (96%; Duiverman 2008); and singing/sham programme attendance (91%/88%; Lord 2012). A similar number of sessions and session duration of neuromuscular electrical stimulation and placebo were reported (Maddocks 2016).
Appendix 7. Secondary outcome: adverse events
Overall, adverse events were inconsistently defined and not clearly reported, especially for the number of events versus the number of affected participants. Available information is presented in Characteristics of included studies and Table 23. Adverse events were described in 47 studies. Nine studies stated that no adverse events occurred (Alison 2019; Bender 2016; Breyer 2010; Effing 2011; Gamper 2019; Holland 2017; O'Neill 2018; Vasilopoulou 2017; Wootton 2017). Two studies described monitoring for adverse events, but did not present any results (Altenburg 2015; Chaplin 2017).
6. Adverse events.
| Study |
Comparison (setting), if known] Clinical stability unless indicated |
Data regarding adverse events |
| Alison 2019 | Supplemental oxygen with exercise training vs. sham with exercise training | AE: incidence and severity similar in both groups
|
| Altenburg 2015 | Physical activity counselling vs. no intervention (primary care, secondary care); Physical activity counselling with PR vs. PR |
Monitoring for AEs described, no results presented: "WA had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any AEs" |
| Arbillaga‐Etxarri 2018 | Urban Training™ vs. no intervention | Participants experiencing any AE: Urban Training 99 (77%) of 128 participants; no intervention 103 (73%) of 142 participants; P = 0.363
|
| Beeh 2014 | LAMA vs. placebo | SAEs: none; AEs leading to discontinuation: LAMA 4 events in 57 participants; placebo 1 event in 53 participants |
| Bender 2016 | Physical activity counselling with pedometer vs. pedometer | "No withdrawals due to AEs" |
| Benzo 2016 | Self‐management (health coaching) with PR referral vs. PR referral | "Reasons for not completing the intervention were death during the study period (n = 3)" (108 participants) |
| Blumenthal 2014 | Self‐management (coping‐skills training) vs. education and symptom monitoring | Education and symptom monitoring: 3 participants died during the intervention period |
| Borges 2014 | Exercise training (whole‐body resistance training) vs. no intervention (inpatient) | "No patients exhibited clinical deterioration except oxygen desaturation (oxygen saturation by pulse oximeter <88%) and increased dyspnoea, which were reversed with oxygen or increasing supplemental oxygen" |
| Breyer 2010 | Nordic walking with education vs. education | "No (serious) AEs were reported" |
| Casaburi 2012 | Supplemental oxygen (lightweight ambulatory) vs. supplemental oxygen (E‐cylinder) | AEs: lightweight ambulatory 1 death (sudden) in 11 participants; E‐cylinder 1 death (congestive heart failure) in 11 participants |
| Chaplin 2017 | Web‐based PR vs. centre‐based PR | Monitoring for AEs described, no results presented: "Any SAEs were reported to the sponsor. A SAE was defined as an acute exacerbation of their COPD that resulted in a hospital admission" |
| Curtis 2016 | ACE inhibitor with PR vs. placebo with PR | AECOPD or AE: no difference between groups
|
| Demeyer 2017 | Physical activity counselling vs. no intervention | Respiratory AEs (≥ 1 AECOPD): physical activity counselling 43 (27%) of 159 participants; no intervention 48 (30%) of 159 participants; P = 0.54; 5 participants required hospitalisation Musculoskeletal AEs (back pain, knee pain, rib fracture): physical activity counselling 11 events; no intervention 2 events; P = 0.01; none caused study discontinuation 8 other AEs (not study‐related: cardiovascular problems, melanoma, urinary problems, gastrointestinal problems) |
| Duiverman 2008 | Non‐invasive ventilation with PR vs. PR | Respiratory AEs: Non‐invasive ventilation 1 death ("progressive respiratory failure due to COPD exacerbation") in 24 participants Musculoskeletal AEs: Non‐invasive ventilation 1 withdrawal ("rheumatic complaints") |
| Effing 2011 | Exercise training (COPE‐active) with self‐management vs. self management | AEs: none reported |
| Felcar 2018 | Water‐based exercise training vs. land‐based exercise training | Participant discontinuations due to "health problems"
|
| Gamper 2019 | Exercise training (outdoor walking) vs. exercise training (cycle ergometry) | During rehabilitation: no AE During follow‐up: ergometry 3 participants AECOPD Walking: unable to use HR monitor as planned, required chest strap; difficult for 70% of participants; resolved using modified Borg scale to guide training intensity |
| Hartman 2016 | Endobronchial valve surgery vs. no intervention | AEs: endobronchial valve surgery 1 death, 8 valves removed in 19 participants |
| Holland 2017 | Home‐based PR vs. centre‐based PR | AEs: none |
| Hornikx 2015 | Physical activity counselling vs. no intervention | Respiratory AEs
|
| Hospes 2009 | Physical activity counselling vs. no intervention | AEs: no intervention 1 death in 17 participants |
| Jolly 2018 | Self‐management vs. no intervention | SAEs: self‐management 24 of 179 participants; no intervention 20 of 232 participants
|
| Kawagoshi 2015 | Physical activity counselling with PR vs. PR | AEs: Physical activity counselling with PR 1 death in 12 participants; PR 1 death in 15 participants |
| Maddocks 2016 | NMES vs. placebo | Similar between groups; AE: NMES 5 (20%) participants; placebo 9 (33%) participants
|
| Magnussen 2017 | LAMA vs. placebo | SAEs: none; AEs: were all "mild or moderate", not study‐related, no withdrawals |
| Mitchell 2013 | Self‐management (SPACE) vs. no intervention | AEs: SPACE five participants with comorbidities, one participant with "worsening of COPD" in 89 participants; no intervention five participants with comorbidities, one death in 95 participants |
| Moy 2015a | Physical activity counselling with pedometer vs. pedometer | Musculoskeletal AEs ("mild / minor"):
Deaths:
Four‐month data
12‐month data "no differences between groups with respect to pulmonary, cardiac or other adverse events"
|
| Nakamura 2016 | LAMA (aclidinium bromide) vs. LAMA (tiotropium) | AEs: aclidinium bromide 9 events in 22 participants; tiotropium 7 events in 22 participants |
| NCT00144326 | LAMA vs. placebo |
“No relevant issues concerning safety were found” Any AE: LAMA 44 (36%) participants, placebo 56 (44%) participants
Most were mild (72 participants, 29%) or moderate (47 participants, 19%) Concerning drug‐related AEs: LAMA 1 (1%) participant; placebo 4 participants SAE: 5 participants (2%) in screening period, 1 died
|
| NCT01351792 | ICS (beclomethasone) with LABA (formoterol) vs. ICS (budesonide) with LABA (formoterol) | TEAEs: beclomethasone with formoterol 18 events in 10 participants (33%); budesonide with formoterol 32 events in 15 participants (52%), 1 AECOPD (only severe event) Adverse drug reactions: beclomethasone with formoterol 5 events in 3 participants (10%); budesonide with formoterol 3 events in 3 participants (10%) AEs leading to study discontinuation: beclomethasone with formoterol 3 events in 3 participants (10%); budesonide with formoterol 5 events in 3 participants (10%) "No relevant differences between groups were observed in the proportion of patients with TEAEs, SAEs, adverse drug reactions, severe AEs and AEs leading to discontinuation" |
| Nguyen 2009 | Physical activity counselling with pedometer vs. pedometer | AEs: Physical activity counselling with pedometer "greater number (of AEs)... two falls and three AECOPD" (9 participants) |
| Nolan 2017 | Physical activity counselling with PR vs. PR |
|
| O'Neill 2018 | Physical activity counselling vs. PR | Study‐related and unexpected AEs; no withdrawals
|
| Orme 2018 | Feedback and education vs. no intervention; Education vs. no intervention; Feedback with education vs. education (post‐admission) |
Hospital admissions (at least 1 overnight stay, not study‐related): education 2 admissions in 6 participants (1 respiratory, 1 non‐respiratory) Hospital re‐admissions for AECOPD (not considered AE, withdrawn from study): education and feedback 3 admissions in 8 participants; no intervention 1 admission in 6 participants No deaths |
| Polkey 2018 | Tai Chi vs. PR | AEs: "No difference in AEs was observed between the groups" (undefined); Tai Chi 2 events in 60 participants; PR 2 events in 60 participants Reasons for hospitalisation (SAE) P = 0.769
|
| Sandland 2008 | Supplemental oxygen vs. placebo (air) | AEs: 1 death during walking test at baseline assessment |
| Schuz 2015 | Self‐management (health mentoring) vs. sham | AEs: self‐management 2 deaths in 47 participants; sham 2 deaths in 73 participants Respiratory AEs (at least 1 admission for COPD): self‐management 11 (12.2%) participants; sham 5 (5.4%) participants; P = 0.11 |
| Troosters 2014 | LAMA (tiotropium) with behavioural management vs. placebo with behavioural management |
"No SAEs were considered related to study drug and patients recovered from all events"; no deaths TEAEs
|
| Troosters 2018 | LAMA vs. placebo; LAMA/LABA vs. placebo; LAMA/LABA and exercise training vs. placebo; LAMA/LABA vs. LAMA; LAMA/LABA and exercise training vs. LAMA; LAMA/LABA and exercise training vs. LAMA/LABA N.B. all groups received behavioural modification |
Any AE: placebo 46 events in 60 participants; LAMA 51 events in 76 participants; LAMA/LABA 44 events in 76 participants; LAMA/LABA and exercise training 49 events in 76 participants TEAE: placebo 4 events; LAMA 6 events; LAMA/LABA 3 events; LAMA/LABA and exercise training 2 events Severe AE: placebo 5 events; LAMA 10 events; LAMA/LABA 3 events LAMA/LABA and exercise training 8 events "Specific AEs with incidence > 2%"
|
| Vasilopoulou 2017 | Maintenance (telerehabilitation) vs. no intervention; Maintenance (centre‐based) vs. no intervention; Maintenance (telerehabilitation) vs. maintenance (centre‐based) |
AEs: none reported |
| Wan 2017 | Physical activity counselling with pedometer vs. pedometer | SAEs (not study‐related: abdominal pain, anxiety, mental health crisis, headache, congestion, ear pain, rash, skin abscess, kidney problems, toe fracture, car accident): Physical activity counselling with pedometer 14 events in 9 of 57 participants; pedometer 10 events in 8 of 52 participants; P = 0.54 Respiratory AEs: Physical activity counselling with pedometer 15 events in 13 participants; pedometer 9 events in 8 participants; P = 0.29 |
| Watz 2016 | LAMA/LABA vs. placebo | All TEAEs: LAMA/LABA 73 events in 44 of 193 participants (4 participants discontinued); placebo 48 events in 43 of 188 participants (2 participants discontinued) Suspected‐related TEAEs: LAMA/LABA 12 events in 11 participants; placebo 4 events in 4 participants
Serious TEAEs: LAMA/LABA 4 participants, 1 death (not study‐related: suspected myocardial infarction); placebo 2 participants |
| Watz 2017 | LAMA/LABA vs. placebo | TEAEs: LAMA/LABA 42.5%, placebo 45.1% SAEs leading to discontinuation: LAMA/LABA 1.5%, placebo 2.3% AEs leading to discontinuation: LAMA/LABA 3%, placebo 4.5% Events reported by > 5% of participants: nasopharyngitis (LAMA/LABA 10.4%; placebo 9.8%), headache (LAMA/LABA 3.0%; placebo 9.0%) |
| Wootton 2017 | Exercise training (ground‐based walking) vs. no intervention | AEs: none reported |
| Physical activity counselling with pedometer vs. no intervention (following ground‐based walking) | "No AEs were reported during the study" |
ACE: angiotensin‐converting enzyme; AE: adverse event; AECOPD: acute exacerbation of COPD; COPD: chronic obstructive pulmonary disease; ICS: inhaled corticosteroid; LABA: long‐acting beta2‐agonist; LAMA: long‐acting muscarinic antagonist; n: number; NMES: neuromuscular electrical stimulation; OR: odds ratio; PR: pulmonary rehabilitation; SAE: serious adverse event; SPACE: self‐management programme of activity, coping and education; TEAE: treatment‐emergent adverse event
In studies including pulmonary rehabilitation or exercise training, reports of adverse events were largely similar for deaths and reasons for discontinuation (Felcar 2018; Kawagoshi 2015; Nolan 2017, Polkey 2018), other than Benzo 2016 where all three deaths occurred in the intervention group, but were unlikely to be related to the intervention. Of note was the less frequent report of "orthopaedic complications" in the water‐based training group of Felcar 2018 compared to land‐based exercise training.
In studies including physical activity counselling, reports of adverse events were largely similar between groups (Hornikx 2015; Hospes 2009; Nguyen 2009; Orme 2018; Wan 2017). "Musculoskeletal events" were more commonly reported in the intervention groups compared to usual care (Arbillaga‐Etxarri 2018; Demeyer 2017) and pedometer‐only group (Moy 2015a), with no difference in other categories of adverse events.
In studies including self‐management, one six‐week study reported one death in the usual‐care group (Mitchell 2013). In one six‐month study with 12‐month follow‐up, serious adverse events were commonly reported in both groups and the five deaths in the intervention group were deemed to be unrelated to the intervention (Jolly 2018), while two deaths in each group were reported over 12 months by Schuz 2015.
Adverse events were reported by all pharmacological studies and were generally balanced between groups (Curtis 2016; Magnussen 2017;Nakamura 2016;NCT00144326; NCT01351792; Troosters 2014; Troosters 2018; Watz 2017). In two studies, a slightly higher proportion of adverse events were seen in the intervention group compared to placebo (LAMA: Beeh 2014; LAMA/LABA: Watz 2016).
In one study of endobronchial valve surgery, one death and removal of eight valves were reported (Hartman 2016). Where reported, there were no differences of note related to the intervention in studies of neuromuscular electrical stimulation (Maddocks 2016), nutritional supplementation (Van de Bool 2017) or supplemental oxygen (Casaburi 2012; Sandland 2008).
Data and analyses
Comparison 1. Physical activity: intervention vs. no intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in step count (steps per day); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 End intervention | 3 | 180 | Mean Difference (IV, Random, 95% CI) | 208.24 [‐164.91, 581.39] |
| 2 time/change in time in moderate‐to‐vigorous intensity physical activity (minutes per day); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 End intervention | 3 | 190 | Mean Difference (IV, Random, 95% CI) | 3.62 [‐1.90, 9.14] |
| 3 change in time in light‐intensity physical activity (minutes per day); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 End intervention | 3 | 182 | Mean Difference (IV, Random, 95% CI) | ‐1.87 [‐28.35, 24.61] |
| 4 change in total energy expenditure (kcal); Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 End intervention | 2 | 144 | Mean Difference (IV, Random, 95% CI) | ‐41.54 [‐89.97, 6.90] |
| 5 change in time in physical activity (total; minutes per day); Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 End intervention | 2 | 88 | Mean Difference (IV, Random, 95% CI) | 23.01 [6.12, 39.90] |
| 6 change in sedentary time (minutes per day); Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 End intervention | 2 | 137 | Mean Difference (IV, Random, 95% CI) | 16.56 [‐27.06, 60.18] |
| 7 time in "lifestyle" physical activity (minutes per day); Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 7.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | 9.40 [3.87, 14.93] |
| 8 time in light‐intensity physical activity (minutes per day); Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | 28.12 [15.64, 40.60] |
| 9 time in moderate‐to‐vigorous intensity physical activity (minutes per day); Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 9.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | 6.24 [4.00, 8.48] |
| 10 sedentary time (minutes per day); Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 10.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | ‐34.25 [‐55.90, ‐12.60] |
| 11 step count (steps per day); Intervention: physical activity counselling | 3 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11.1 Step count: in‐person (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 Change in step count: telecoaching (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.3 Step count: 'Urban Training' (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 "IMA" (counts per minute); Intervention: self‐management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Mid‐intervention (4 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.2 Mid‐intervention (12 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 physical activity level; Intervention: nutritional supplement | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 total energy expenditure (MJ); Intervention: nutritional supplement | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 subgroup analysis (supervised vs. unsupervised); change in step count (steps per day); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 15.1 Supervised pulmonary rehabilitation/exercise training | 2 | 144 | Mean Difference (IV, Random, 95% CI) | 68.86 [‐386.29, 524.01] |
| 15.2 Unsupervised pulmonary rehabilitation/exercise training | 1 | 36 | Mean Difference (IV, Random, 95% CI) | 494.0 [‐157.70, 1145.70] |
| 16 supgroup analysis (supervised vs. unsupervised); change in time in light‐intensity physical activity (minutes per day); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 16.1 Supervised pulmonary rehabilitation/exercise training | 2 | 146 | Mean Difference (IV, Random, 95% CI) | 9.87 [‐9.22, 28.96] |
| 16.2 Unupervised pulmonary rehabilitation/exercise training | 1 | 36 | Mean Difference (IV, Random, 95% CI) | ‐44.0 [‐87.04, ‐0.96] |
| 17 subgroup analysis (supervised vs. unsupervised); change in total energy expenditure (kcal); Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Supervised pulmonary rehabilitation/exercise training | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 Unsupervised pulmonary rehabilitation/exercise training | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 subgroup analysis (supervised vs. unsupervised); change in sedentary time (minutes per day); Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Supervised pulmonary rehabilitation/exercise training | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 Unsupervised pulmonary rehabilitation/exercise training | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 2. Physical activity: intervention vs. placebo/sham.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 step count (steps per day); Intervention: self‐management (health mentoring) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in step count (steps per day); Intervention: LAMA/LABA | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 End intervention | 2 | 426 | Mean Difference (IV, Random, 95% CI) | 531.30 [167.10, 895.49] |
| 3 change in time in moderate‐to‐vigorous intensity physical activity (minutes per day): Intervention: LAMA/LABA | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 End intervention | 2 | 423 | Mean Difference (IV, Random, 95% CI) | 9.74 [4.23, 15.24] |
| 4 change in active energy expenditure (kcal); Intervention: LAMA/LABA | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 End intervention | 2 | 423 | Mean Difference (IV, Random, 95% CI) | 43.89 [17.92, 69.86] |
| 5 step count (steps per day); Intervention: nutritional supplement | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 energy expenditure for ambulation (kcal/step/FFM kg); Intervention: nutritional supplement | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 change in step count (steps per day); Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 change in up/down transitions (number); Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 change in time upright (hours); Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 3. Physical activity: intervention with common intervention vs. common intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 movement intensity (m/s2); Interventions: nordic walking with education vs. education | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Follow‐up (6 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Follow‐up (9 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in step count (steps per day); Interventions: exercise training (COPE‐active) with self‐management vs. self management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Follow‐up (18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.4 Follow‐up (24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in time in light‐intensity physical activity (minutes per day); Interventions: upper body resistance training with health education vs. health education | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 step count (steps per day); Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 time walking (minutes per day); Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 walking intensity (m/s2); Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 step count (steps per day); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 time walking (minutes per day); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 walking intensity (m/s2); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 step count (steps per day); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 time walking (minutes per day); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 walking intensity (m/s2); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 change in step count (steps per day); Interventions: exercise training and physical activity counselling with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 Follow‐up (3 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.3 Follow‐up (12 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 change in step count (weekday, steps per day); Interventions: physical activity counselling with optional supervised exercise vs. optional supervised exercise | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.3 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 METs; Interventions: physical activity counselling with optional supervised exercise vs. optional supervised exercise | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.3 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 step count (steps per day); Interventions: physical activity counselling with pedometer vs. pedometer | 3 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Step count: web‐based (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 Step count: app (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.3 Step count: app (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.4 Change in step count: web‐based (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.5 Change in step count: web‐based (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 time active (minutes per day); Interventions: physical activity counselling (app) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 time inactive (minutes per day); Interventions: physical activity counselling (app) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 peak performance (steps per minute); Interventions: physical activity counselling (app) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 step count (steps per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 End intervention (7 days including PR) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 End intervention (6 days excluding PR) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.3 End intervention (4 days excluding PR) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.4 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.5 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 time in moderate‐to‐vigorous intensity physical activity (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 21.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 time in physical activity (total, minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 22.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 time sedentary (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 23.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 change in step count (steps per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 24.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25 change in time in moderate‐to‐vigorous intensity physical activity (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 25.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26 change in time walking (minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 26.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 change in time in physical activity (total, minutes per day); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 27.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 28 change in time in light‐intensity physical activity (minutes per day); Interventions: exercise‐specific self‐efficacy training with upper body resistance training vs. upper body resistance training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 28.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 28.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 29 step count (steps per day); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 29.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 29.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 30 time walking (minutes per day); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 30.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 30.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 31 walking intensity (m/s2); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 31.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 31.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 32 step count (steps per day); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 32.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 32.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 33 time walking (minutes per day); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 33.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 33.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 34 walking intensity (m/s2); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 34.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 34.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 35 step count (steps per day); Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 35.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 35.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 36 time walking (minutes per day); Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 36.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 36.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 37 walking intensity (m/s2); Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 37.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 37.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 38 change in step count (steps per day); Interventions: nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 38.1 End intervention (stage 1) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 38.2 End intervention (stage 2) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 38.3 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 39 change in step count (steps per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 39.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 39.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 40 change in time in moderate‐intensity physical activity (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 40.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 40.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 41 change in time in vigorous‐intensity physical activity (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 41.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 41.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 42 change in time in light‐intensity physical activity (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 42.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 42.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 43 change in total energy expenditure (kcal); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 43.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 43.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 44 change in sedentary time (minutes per day); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 44.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 44.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 4. Physical activity: intervention vs. intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in step count (steps per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in time in moderate‐to‐vigorous intensity physical activity (minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in number of bouts of moderate‐to‐vigorous intensity physical activity; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 change in time in bouts of moderate‐to‐vigorous intensity physical activity(minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 change in sedentary time (minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 change in sedentary time (awake; minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 change in number of sedentary bouts; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 change in time in sedentary bouts (minutes per day); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 change in METs; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 change in total energy expenditure (kcal); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 change in step count (steps per day); Interventions: water‐based exercise training vs. land‐based exercise training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 change in total energy expenditure (kcal); Interventions: water‐based exercise training vs. land‐based exercise training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 step count (steps per day); Interventions: Tai Chi vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Mid‐intervention (6 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 Mid‐intervention (22 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 step count (steps per day); Interventions: outdoor walking vs. cycle ergometry | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 step count (steps per day); Interventions: physical activity counselling vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 total energy expenditure (kcal); Interventions: exercise training with tapered supervision vs. supervised exercise training | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 16.1 End intervention | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 Follow‐up | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 mid day activity (vector magnitude units per minute); Interventions: supplemental oxygen (lightweight ambulatory) vs. supplemental oxygen (E‐cylinder) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 5. Health‐related quality of life: intervention vs. no intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in SGRQ total score; Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 End intervention | 2 | 144 | Mean Difference (IV, Random, 95% CI) | ‐8.79 [‐14.08, ‐3.51] |
| 2 change in SGRQ domain scores. Intervention: pulmonary rehabilitation/exercise training (ground‐based walking) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in CRQ domain scores; Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Dyspnoea (end intervention) | 3 | 182 | Mean Difference (IV, Random, 95% CI) | 1.69 [0.02, 3.36] |
| 3.2 Emotional function (end intervention) | 3 | 182 | Mean Difference (IV, Random, 95% CI) | 2.41 [0.48, 4.35] |
| 3.3 Fatigue (end intervention) | 3 | 182 | Mean Difference (IV, Random, 95% CI) | 1.34 [‐0.16, 2.83] |
| 3.4 Mastery (end intervention) | 3 | 182 | Mean Difference (IV, Random, 95% CI) | 0.61 [‐0.47, 1.69] |
| 3.5 Total score (end intervention) | 3 | 182 | Mean Difference (IV, Random, 95% CI) | 6.70 [2.55, 10.86] |
| 4 CAT score; Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | ‐3.15 [‐4.82, ‐1.47] |
| 5 SGRQ domain scores (%change); Intervention: exercise training [inpatient] | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.4 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.5 Symptoms (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.6 Activity (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.7 Impacts (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.8 Total score (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 SGRQ domain scores; Intervention: physical activity counselling | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.4 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 CCQ domain scores: Intervention: physical activity counselling | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Functional state (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 Mental state (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.4 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 change in CCQ domain scores; Intervention: physical activity counselling (telecoaching) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Functional state (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.3 Mental state (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 change in CRQ domain and total scores; Intervention: physical activity counselling | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.5 Total (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 change in SGRQ domain and total scores; Intervention: physical activity counselling | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.4 Total (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 change in CRQ domain scores; Intervention: self‐management (SPACE) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.5 Dyspnoea (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.6 Emotional domain (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.7 Fatigue (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.8 Mastery (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 CCQ total score; Intervention: self‐management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Mid‐intervention (4 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.2 Mid‐intervention (12 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 EQ5D index score; Intervention: self‐management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Mid‐intervention (4 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 Mid‐intervention (12 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 EQ5D visual analogue scale score; Intervention: self‐management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Mid‐intervention (4 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Mid‐intervention (12 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 SGRQ domain scores; Intervention: self‐management (telephone health coaching) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.4 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.5 Symptoms (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.6 Activity (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.7 Impacts (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.8 Total score (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 EQ5D score; Intervention: self‐management (telephone health coaching) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 CRQ domain scores; Intervention: four‐wheeled walker | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 6. Health‐related quality of life: intervention vs. placebo/sham.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in SF36 component scores; Intervention: singing | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Physical component (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Mental component (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in CRQ total score; Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in SGRQ total score; Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 change in EQ5D index score; Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 change in EQ5D visual analogue scale score; Intervention: neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 7. Health‐related quality of life: intervention with common intervention vs. common intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SF36 component scores (score < 50); Interventions: Nordic walking with education vs. education | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Physical component score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Physical component score (follow‐up, 6 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Physical component score (follow‐up, 9 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.4 Mental component score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.5 Mental component score (follow‐up, 6 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.6 Mental component score (follow‐up, 9 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in CRQ domain scores; Interventions: exercise training (COPE‐active) with self‐management vs. self management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.6 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.7 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.9 Dyspnoea (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.10 Emotional function (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.11 Fatigue (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.12 Mastery (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.13 Dyspnoea (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.14 Emotional function (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.15 Fatigue (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.16 Mastery (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in CCQ domain scores; Interventions: exercise training (COPE‐active) with self‐management vs. self management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Symptoms (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Functional state (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Mental state (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 Total (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.5 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.6 Functional state (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.7 Mental state (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.8 Total (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.9 Symptoms (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.10 Functional state (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.11 Mental state (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.12 Total (follow‐up, 18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.13 Symptoms (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.14 Functional state (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.15 Mental state (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.16 Total (follow‐up, 24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 CRQ domain scores; Interventions: LAMA/LABA and exercise training with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.6 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 CRQ domain scores; Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.6 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 CRQ domain scores; Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.3 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.6 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 change in SGRQ domain and total scores; Intervention: exercise training and physical activity counselling with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.4 Total (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.5 Symptoms (follow‐up, 3 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.6 Activity (follow‐up, 3 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.7 Impacts (follow‐up, 3 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.8 Total (follow‐up, 3 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.9 Symptoms (follow‐up, 12 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.10 Activity (follow‐up, 12 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.11 Impacts (follow‐up, 12 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.12 Total (follow‐up, 12 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 change in CRQ domain scores; Interventions: physical activity counselling (app) with optional supervised exercise vs. optional supervised exercise | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Dyspnoea (12 weeks, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Emotional function (12 weeks, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.3 Fatigue (12 weeks, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.4 Mastery (12 weeks, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.5 Dyspnoea (6 months, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.6 Emotional function (6 months, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.7 Fatigue (6 months, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.8 Mastery (6 months, mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.9 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.10 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.11 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.12 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 change in SGRQ total score; Interventions: physical activity counselling with pedometer vs. pedometer | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 web‐based (12 weeks, end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 web‐based (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.3 web‐based (12 months, end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 SGRQ total: Interventions: physical activity counselling (app) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 SF36: Interventions: physical activity counselling (app) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Physical component score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 Mental component score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 change in SGRQ domain scores; Interventions: physical activity counselling (web‐based) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Symptoms (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.2 Impacts (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.3 Activities (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.4 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.5 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.6 Activities (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 SGRQ domain scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.3 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 RAND36 domain scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Physical function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Vitality (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.3 Bodily pain (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.4 General health perception (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.5 Health status (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 change in CRQ dyspnoea domain score; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 Mid‐intervention (end PR) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 SGRQ scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Symptoms (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 Activity (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.3 Impacts (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.4 Total score (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.5 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.6 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.7 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.8 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 CRQ domain scores; Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.5 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 change in CRQ total score; Interventions: physical activity counselling with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 change in CRQ scores; Interventions: self‐management (health coaching) with pulmonary rehabilitation referral vs. pulmonary rehabilitation referral | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Physical function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.3 Physical function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.4 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 CRQ domain scores; Interventions: LAMA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.3 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.6 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 CRQ domain scores; Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 21.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.3 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.6 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 CRQ domain scores; Interventions: LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 22.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.2 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.3 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.5 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.6 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.8 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 change in SGRQ domain and total scores; Interventions: ACE inhibitor with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 23.1 Symptoms (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.2 Activity (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.3 Impacts (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.4 Total (end intervention) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 change in SGRQ total score; Interventions: nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 24.1 End intervention (stage 2) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25 change in EQ5D; Interventions: nutritional supplement with pulmonary rehabilitation vs. placebo with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 25.1 End intervention (stage 2) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26 change in CRQ domain scores; Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 26.1 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.5 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.6 Dyspnoea (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.7 Emotional function (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.8 Fatigue (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.9 Mastery (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.10 Total score (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 CRQ domain scores; Interventions: non‐invasive ventilation with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 27.1 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.5 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 8. Exercise capacity: intervention vs. placebo/sham.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in 6MWD (metres); Intervention; neuromuscular electrical stimulation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 9. Exercise capacity: intervention vs. no intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in 6MWD (metres); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 End intervention | 3 | 182 | Mean Difference (IV, Random, 95% CI) | 29.06 [14.38, 43.75] |
| 2 change in ISWD (metres); Intervention: pulmonary rehabilitation/exercise training | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 End intervention | 3 | 180 | Mean Difference (IV, Random, 95% CI) | 19.02 [2.20, 35.85] |
| 3 change in ESWT (seconds); Intervention: pulmonary rehabilitation/exercise training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 End intervention | 2 | 137 | Mean Difference (IV, Random, 95% CI) | 237.87 [147.59, 328.16] |
| 4 6MWD (metres); Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | 46.55 [24.66, 68.45] |
| 5 work rate (watts); Intervention: high‐intensity interval training | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 End intervention | 2 | 275 | Mean Difference (IV, Random, 95% CI) | 15.47 [8.76, 22.17] |
| 6 change in ISWD (metres); Intervention: self‐management (SPACE) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 change in ESWT (seconds); Intervention: self‐management (SPACE) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 6MWD (metres); Intervention: exercise training [inpatient] | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 10. Health‐related quality of life: intervention vs. intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in CRQ domains; Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.4 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.5 Dyspnoea (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.6 Emotional function (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.7 Fatigue (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.8 Mastery (follow‐up) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in CRQ domains; Interventions: water‐based exercise training vs. land‐based exercise training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Dyspnoea (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Emotional function (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Fatigue (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.4 Mastery (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.5 Total score (mid‐intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.6 Dyspnoea (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.7 Emotional function (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.8 Fatigue (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.9 Mastery (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.10 Total score (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 SGRQ domain and total scores; Interventions: Tai Chi vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Symptoms (mid‐intervention, 2 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Activity (mid‐intervention, 2 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Impacts (mid‐intervention, 2 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 Total (mid‐intervention, 2 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.5 Symptoms (mid‐intervention, 14 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.6 Activity (mid‐intervention, 14 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.7 Impacts (mid‐intervention, 14 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.8 Total (mid‐intervention, 14 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.9 Symptoms (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.10 Activity (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.11 Impacts (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.12 Total (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 CRQ total score; Interventions: outdoor walking vs. cycle ergometry | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Maugeri Respiratory Failure questionnaire; Interventions: exercise training with tapered supervision vs. supervised exercise training | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 End intervention | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Follow‐up | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 SF36 domain scores; Interventions: self‐management vs. education and symptom monitoring | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Mental health (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Role emotional (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.3 Vitality (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.4 Social functioning (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.5 Pain (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.6 Role physical (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.7 General health (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.8 Physical functioning (end intervention) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 11. Exercise capacity: intervention with common intervention vs. common intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 6MWD (metres); Interventions: Nordic walking with education vs. education | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Follow‐up (6 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Follow‐up (9 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in ISWD (metres); Interventions: exercise training (COPE‐active) with self‐management vs. self management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Follow‐up (18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.4 Follow‐up (24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in ESWT (seconds); Interventions: exercise training (COPE‐active) with self‐management vs. self management | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Follow‐up (18 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 Follow‐up (24 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 6MWD (metres); Interventions: exercise training and LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 ESWT (seconds); Interventions: exercise training and LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 6MWD (metres); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 ESWT (seconds); Interventions: exercise training and LABA with LAMA and behaviour modification vs. LAMA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 6MWD (metres); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 ESWT (seconds); Interventions: exercise training with LAMA/LABA and behaviour modification vs. LAMA/LABA and behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 change in ESWT (seconds); Intervention: physical activity counselling and exercise training with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Follow‐up (3 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Follow‐up (12 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 6MWD (metres); Interventions: physical activity counselling (app) with optional supervised exercise vs. optional supervised exercise | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Mid‐intervention (12 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 Mid‐intervention (6 months) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.3 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 6MWD (metres); Interventions: physical activity counselling (app) with pedometer vs. pedometer | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 6MWD (metres); Interventions: physical activity counselling with pulmonary rehabilitation vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 change in 6MWD (metres); Interventions: physical activity counselling with pulmonary rehabilitation vs. sham with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 6MWD (metres); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 ESWT (seconds); Interventions: LAMA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 6MWD (metres); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 ESWT (s); Interventions: LAMA/LABA with behaviour modification vs. placebo with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 6MWD (metres); Interventions: LAMA/LABA with behaviour modification vs. LAMA with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 ESWT (seconds); Interventions: LAMA/LABA with behaviour modification vs. LAMA with behaviour modification | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 change in ISWD (metres); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 21.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 change in ESWT (seconds); Interventions: supplemental oxygen with pulmonary rehabilitation vs. sham intervention with pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 22.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 12. Exercise capacity: intervention vs. intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 change in 6MWD (metres); Interventions: home‐based pulmonary rehabilitation vs. centre‐based pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 change in 6MWD (metres); Interventions: water‐based exercise training vs. land‐based exercise training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 change in ISWD (metres); Interventions: water‐based exercise training vs. land‐based exercise training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 change in VO2max (ml/min); Interventions: water‐based exercise training vs. land‐based exercise training | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Mid‐intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 6MWD (metres); Interventions: Tai Chi vs. pulmonary rehabilitation | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Mid‐intervention (2 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Mid‐intervention (14 weeks) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 End intervention | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 6MWD (metres); Interventions: exercise training with tapered supervision vs. supervised exercise training | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 End intervention | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Follow‐up | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Alison 2019.
| Methods | DESIGN 2 groups DATES January 2013 to January 2017 SETTING PR, 7 metropolitan hospitals (Australia) SAMPLE SIZE ESWT, CRQ "For the physical activity outcome, 82 participants will be sufficient to provide 80% power to detect as significant, at the (two‐sided) 5% level, a minimum of 1845 step difference in the mean steps per day between the groups, assuming SD 2968" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS (TOTAL n = 111)
AGE mean 69 (SD 7) years; SEX 30 (52%) male; FEV1 mean 47 (SD 17)% predicted
AGE mean 69 (SD 8) years; SEX 31 (59%) male; FEV1 mean 45 (SD 16)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP 6 months SUPERVISION yes COMMON INTERVENTION exercise training DURATION 8 weeks SETTING supervised outpatient group CONTACT 3 sessions a week (minimum 20 sessions) AEROBIC TRAINING treadmill walking, stationary cycling
STRENGTH TRAINING, OTHER COMPONENTS, EDUCATION nil INTERVENTION supplemental oxygen, 5 litres a minute from oxygen concentrator SHAM intranasal air, 5 litres a minute from modified oxygen concentrator |
|
| Outcomes | DEVICE SenseWear
ASSESSMENT TIME POINTS
PRIMARY OUTCOMES
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "The study was funded by a National Health and Medical Research Council, Australia, project grant APP1019989. Funding information for this article has been deposited with the Crossref Funder Registry." CONFLICT OF INTEREST statement provided CONTACT Jenny Alison jennifer.alison@sydney.edu.au University of Sydney (Australia) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Sequence generation will be determined using a computerised random number generator" |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation concealment will be achieved by the use of a central telephone randomisation system coordinated through the NHMRC Clinical Trials Centre at The University of Sydney" |
| Blinding of participants (performance bias) | Low risk | Quote: "blinding of participants, therapists and assessors" |
| Blinding of personnel (performance bias) | Low risk | Quote: "blinding of participants, therapists and assessors" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Quote: "blinding of participants, therapists and assessors" |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Quote: "blinding of participants, therapists and assessors" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT figure provided |
| Selective reporting (reporting bias) | Low risk | Registry, published protocol and paper in agreement Paper additionally reports all CRQ domains, adherence, adverse events and intervention fidelity |
| Other bias | Low risk | Prospective registration |
Altenburg 2015.
| Methods | DESIGN 2 groups (3 subgroups according to location of recruitment)
DATES November 2006 to November 2010 SETTING general practice, outpatient hospital clinics, PR centre (The Netherlands) SAMPLE SIZE calculation based on step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS of subgroups (not provided by intervention groups)
AGE median 65 (IQR 58 to 72) years; SEX 32 (66%) male; FEV1 median 78 (IQR 66 to 95)% predicted
AGE median 68 (IQR 61 to 72) years; SEX 34 (74%) male; FEV1 median 58 (IQR 40 to 69)% predicted
AGE median 54 (IQR 50 to 63) years; SEX 36 (59%) male; FEV1 median 43 (IQR 28 to 58)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP 12 months post‐intervention SUPERVISION yes INTERVENTION PAC (in‐person, as in De Blok 2006, Hospes 2009) INTERFACE 5 individual sessions ACTIVITY lifestyle physical activity (e.g. walking, cycling, stair‐climbing, gardening) STEP‐TRACKING pedometer (direct feedback) RECORD diary: daily step count, other activities (e.g. cycle, swim) GOALS “Maximal” step count goal, end intervention: set personal “physical activity norm” (between mean and maximal step count) goal EDUCATION/RESOURCES NO INTERVENTION "care appropriate to their health status" SUBGROUP PR DURATION 9 weeks SETTING centre‐based outpatient group CONTACT 3 sessions per week, one to two hours AEROBIC TRAINING "cycling, walking, swimming & sports" STRENGTH TRAINING nil OTHER COMPONENTS "psychological and/or nutritional support as needed" EDUCATION "educational courses" |
|
| Outcomes | DEVICE Digiwalker SW‐2000 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was supported by an unrestricted grant from Boehringer Ingelheim B.V. and by the University Medical Centre Groningen" CONFLICT OF INTEREST statement provided CONTACT Wytske Altenburg w.a.altenburg@umcg.nl University of Groningen (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was computerized" |
| Allocation concealment (selection bias) | High risk | Quote: "Allocation was open to the researcher, counsellor and patient" |
| Blinding of participants (performance bias) | High risk | Quote: "Allocation was open to the researcher, counsellor and patient" |
| Blinding of personnel (performance bias) | High risk | Quote: "Allocation was open to the researcher, counsellor and patient" |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: step count was reported by participants |
| Blinding of outcome assessment [other] (detection bias) | High risk | Quote: "Allocation was open to the researcher, counsellor and patient" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow chart provided but not specified by group according to site of recruitment (as data are presented) N.B. high number of dropouts (45% from the counselling arm of the study) in the pulmonary rehabilitation group |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOMES Paper: additional outcomes reported
Registry: 3 months for intervention group, 6 months for both groups (additional follow‐up time points not reported) SECONDARY OUTCOMES Registry: upper limb, lower limb and respiratory muscle strength; COPD‐related costs (not reported) Paper: SF36 (described in Methods, not reported) |
| Other bias | Low risk | N/A |
Arbillaga‐Etxarri 2018.
| Methods | DESIGN 2 groups DATES October 2013 to January 2016 SETTING 33 primary care centres and hospitals from 5 seaside municipalities (Spain) SAMPLE SIZE calculation based on step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA registry
BASELINE CHARACTERISTICS
AGE mean 69 (SD 9) years SEX 170 (84%) male; FEV1 mean 56 (SD 17)% predicted
AGE mean 69 (SD 8) years; SEX 176 (86%) male; FEV1 mean 57 (SD 18)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 months FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (Urban Training) INTERFACE
ACTIVITY walking (trail of intensity as in baseline dyspnoea and 6MWD) STEP‐TRACKING pedometer (direct feedback) RECORD personalised calendar GOALS
EDUCATION/RESOURCES
NO INTERVENTION brochure with recommendation to complete MPA ≥ 30 minutes, ≥ 5 days per week |
|
| Outcomes | DEVICE Dynaport MoveMonitor (centre of lower back with an elastic strap)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Judith Garcia‐Aymerich judith.garcia@isglobal.org ISGlobal, Barcelona (Spain) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A statistician blinded to study objectives and not involved in any study procedure or analysis created the randomisation sequence using Stata 12.0 (StataCorp, College Station, TX, USA) software" |
| Allocation concealment (selection bias) | Low risk | Quote: "At the second study visit, a physiotherapist allocated patients to the corresponding group using a secured computer file, where allocations were ordered according to the randomisation sequence and only available one at a time" |
| Blinding of participants (performance bias) | Unclear risk | Unable to blind participants to intervention BUT Quote: "Patients were not aware of the existence of the alternative group…" Quote: "We implemented diverse measures to avoid contamination (i.e., that participants did not receive the intervention to which they were randomised)" |
| Blinding of personnel (performance bias) | High risk | Quote: "The physiotherapists who administered the intervention and knew the allocated groups" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "outcome examiners and data analysts remained blinded to the allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow chart provided |
| Selective reporting (reporting bias) | Low risk | As per registry |
| Other bias | Unclear risk | Original estimated enrolment (July 2013) n = 600; Actual enrolment (April 2016) n = 412 |
Beeh 2014.
| Methods | DESIGN cross‐over trial (only pre‐cross‐over data used), 2 groups DATES November 2011 to June 2012 SETTING 14 sites (Germany, Spain, UK) SAMPLE SIZE calculation based on endurance time (cycle ergometry) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
MEDICATIONS
BASELINE CHARACTERISTICS
AGE mean 61 (SD 8) years; SEX 35 (61%) male; FEV1 mean 57 (SD 12)% predicted
AGE mean 59 (SD 8) years SEX 42 (76%) male; FEV1 mean 56 (SD 12)% predicted |
|
| Interventions | DURATION OF INTERVENTION 3 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION LAMA (aclidinium bromide, 400 μg) twice daily (09:00, 21:00 ± 1 hour) with a dry powder inhaler (Genuair®/Pressair®) PLACEBO twice daily (09:00, 21:00 ± 1 hour) with a dry powder inhaler (Genuair®/Pressair®) |
|
| Outcomes | DEVICE SenseWear Pro3 (software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was supported by Almirall S.A., Barcelona, Spain, and Forest Laboratories LLC, a subsidiary of Actavis, New York, NY, USA. The study sponsors (Almirall S.A., Barcelona, Spain, and Forest Laboratories LLC, a subsidiary of Actavis, New York, NY, USA) were responsible for the conception and design of the study, collection of the data, and data analysis. The sponsors placed no restrictions on statements made in the final version of the manuscript or on the decision to submit the manuscript for publication." CONFLICT OF INTEREST statement provided CONTACT Henrik Watz H.Watz@pulmoresearch.de German Center for Lung Research, Grosshansdorf (Germany) Additional data provided: as in Almirall |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed according to unique patient identification numbers and a computer‐generated random allocation sequence" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | Low risk | Quote: "Patients and investigators were blinded to treatment allocation throughout the study" |
| Blinding of personnel (performance bias) | Low risk | Quote: "Patients and investigators were blinded to treatment allocation throughout the study" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity, exercise capacity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Low risk | Paper: physical activity (additional outcome) |
| Other bias | Low risk | N/A |
Bender 2016.
| Methods | DESIGN 2 groups DATES May 2013 to September 2014 SETTING pulmonary outpatient clinics (USA) SAMPLE SIZE "As this was a pilot study, the study was not powered" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 65 (SD 8) years; SEX 25 (44%) male; FEV1 post‐bronchodilator mean 56 (SD 12)% predicted
AGE mean 66 (SD 8) years; SEX 23 (40%) male; FEV1 post‐bronchodilator mean 52 (SD 12)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION PAC (wellness coaching) INTERFACE
ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD diary: daily step count GOALS personally meaningful activity goal; increase 15% steps a month EDUCATION/RESOURCES nil INTERVENTION pedometer INTERFACE 5 phone calls (fortnightly, report step count) ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD Diary: daily step count GOALS, EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE Omron pedometer
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was funded by a grant from GlaxoSmithKline." CONFLICT OF INTEREST "DS is an employee of GlaxoSmithKline and holds stock/shares in GlaxoSmithKline. AE, now an employee of PAREXEL International, was an employee of GlaxoSmithKline at the time the study was conducted and holds stock/shares in GlaxoSmithKline. SS was an employee of GlaxoSmithKline at the time the study was conducted and holds stock/shares in GlaxoSmithKline. All other authors have confirmed that they have no conflict of interest related to this manuscript." CONTACT Bruce Bender BenderB@njhealth.org National Jewish Health, Denver (US) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomized" insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Insufficient information |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: step count was reported by participants |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Insufficient information |
| Incomplete outcome data (attrition bias) All outcomes | High risk | No participant flow diagram provided Total number randomised provided; no details re exclusion or attrition Quote: "Forty‐nine of 57 patients in the Goal group and 50 of the 58 in the Control group completed the study and provided a Week 12 mean steps/day assessment forming the Completer population" |
| Selective reporting (reporting bias) | High risk | No trial registry Paper:
|
| Other bias | High risk |
|
Benzo 2016.
| Methods | DESIGN 2 groups DATES September 2010 to July 2016 SETTING 2 hospitals (USA) SAMPLE SIZE calculation based on readmission rates |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 68 (SD 9) years; SEX 52 (48%) male; FEV1 mean 41 (SD 17)% predicted
AGE mean 68 (SD 9) years; SEX 51 (48%) male; FEV1 mean 40 (SD 17)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 months FOLLOW‐UP no SUPERVISION no INTERVENTION self‐management (health coaching) INTERFACE
ACTIVITY Stamina InMotion Elliptical Trainer (provided) STEP‐TRACKING, RECORD nil GOALS 20 minutes a day (intensity not prescribed) EDUCATION/RESOURCES
OPTIONAL PR "Referred for conventional PR" care according to GOLD guidelines |
|
| Outcomes | DEVICE Sensewear armband (model and software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Roberto Benzo benzo.roberto@mayo.edu Mayo Clinic, Minnesota (US) Additional information requested |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "We randomly assigned subjects using an online, computer‐generated, simple binomial randomization program to one of the two groups, stratified by center" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | CONSORT diagram provided 3 people died but full count in the analysis? Quote: "Patients with missing or unknown outcomes were excluded from this analysis… Intent‐to‐treat analyses were also run to account for the missing values (almost none for the primary outcome). Patients with missing values were considered to have died or to have had COPD hospitalisation in these analyses. Because there were very few missing values and results from intent‐to‐treat analyses were similar to the original analyses, no imputations were done." |
| Selective reporting (reporting bias) | High risk | Discrepancy with study dates
PRIMARY OUTCOME
SECONDARY OUTCOMES
N.B. selective reporting of CRQ domains |
| Other bias | Unclear risk |
|
Blumenthal 2014.
| Methods | DESIGN 2 groups DATES January 2009 to May 2013 SETTING Duke University Medical Center and Ohio State University (USA) SAMPLE SIZE "based on two primary outcomes: (1) combined death and hospitalizations/COPD‐related physician visits and (2) QoL (mental health and physical functioning) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 8) years; SEX 101 (62%) male; FEV1 mean 45 (SD 17)% predicted
AGE mean 67 (SD 9) years; SEX 98 (60%) male; FEV1 mean 46 (SD 17)% predicted |
|
| Interventions | DURATION OF INTERVENTION 16 weeks FOLLOW‐UP annual follow‐up intervals for up to 4 years SUPERVISION no INTERVENTION telephone‐based enhanced coping‐skills training (CST) SETTING home‐based CONTACT telephone calls Weeks 1 to 12: 1 session a week, 30 minutes Weeks 13 and 14: 2 bi‐weekly “booster sessions“ CONTENT coping skills for symptom management
INTERVENTION usual care plus education and symptom monitoring SETTING home‐based CONTACT telephone calls
CONTENT assess health status, providing support, COPD education |
|
| Outcomes | DEVICE accelerometer (Kenz Lifecorder Plus NL‐216) (hip)
ASSESSMENT TIME POINTS
PRIMARY OUTCOMES
SECONDARY OUTCOME
|
|
| Notes |
FUNDING “This research was supported by Grant No. HL 065503 from the National Institutes of Health, Bethesda, Maryland” CONFLICT OF INTEREST not stated CONTACT James Blumenthal Blume003@mc.duke.edu |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Randomization was performed centrally by computer" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Insufficient information |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Blinded outcomes assessor |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk |
|
| Other bias | Unclear risk |
PROTOCOL “600 COPD patients and their respective caregivers” REPORTED ON REGISTRY “746 participants (patients and caregivers) were consented… of these, 326 patients were randomized and participated in the study intervention along with 252 consented participants who acted as a caregiver; in total 578 participants (patients and caregivers) were involved with the study intervention” |
Borges 2014.
| Methods | DESIGN 2 groups DATES April 2009 to October 2010 SETTING hospital (Brazil) SAMPLE SIZE calculation based on quadriceps strength |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 64 (SD 13) years SEX 8 (53%) male FEV1 mean 42 (SD 14)% predicted
AGE mean 68 (SD 9) years; SEX 10 (71%) male; FEV1 mean 39 (SD 16)% predicted |
|
| Interventions | DURATION OF INTERVENTION duration of hospital admission FOLLOW‐UP 4 weeks SUPERVISED yes INTERVENTION exercise training (whole‐body resistance training) DURATION during admission SETTING individual sessions CONTACT began Day 3 until discharge ≥ 3 sessions AEROBIC TRAINING nil STRENGTH TRAINING upper and lower limbs (2 sets, 8 repetitions)
OTHER COMPONENTS, EDUCATION nil N.B. MONITORING
NO INTERVENTION Normal daily care
No exercise programme or recommendation to exercise after hospital discharge |
|
| Outcomes | DEVICE Dynaport MoveMonitor
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Rodrigo Borges rodrigounopar@yahoo.com.br University of Sao Paulo, Sao Paulo (Brazil) Additional data provided: 6MWD; time lying, sitting, standing and walking |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The randomization sequence was computer generated by 1 investigator who was not involved in the study" |
| Allocation concealment (selection bias) | Low risk | Quote: "allocation was concealed in sequentially numbered, sealed, opaque envelopes" |
| Blinding of participants (performance bias) | High risk | Unable to be blinded to the intervention |
| Blinding of personnel (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "evaluations were performed by a blinded evaluator" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow diagram provided Randomised n = 46, "completed" n = 29: Quote: "Despite anticipating a patient attrition rate of 40%, it was necessary to randomise more 4 patients to obtain the calculated sample size" "we had a 37% loss to follow‐up that can be considered large and probably reflects the patients’ severity because 35% of patients were referred to the ICU. Another reason for the loss during follow up was the high rate of early discharge... In addition, there was a greater loss to follow‐up in the CG because 2 patients died for reasons unrelated to COPD (rupture of aortic aneurysm, sepsis of abdominal origin) and 2 patients refused to attend the hospital 1 month after discharge" |
| Selective reporting (reporting bias) | High risk | SECONDARY OUTCOMES Paper: exercise capacity, HRQOL, systemic inflammatory mediators, arterial blood gases (baseline), lung function, length of stay, number of sessions, adherence to sessions (additional outcomes reported) |
| Other bias | Unclear risk | Retrospectively registered
Participants performed exercises with NIV in 35% of the sessions because of dyspnoea (Borg ≥ 6). |
Breyer 2010.
| Methods | DESIGN 2 groups DATES March 2006 to March 2007 SETTING (Austria) SAMPLE SIZE "The present study was the first to investigate the effect of Nordic Walking on the physical activity of COPD patients. Therefore, we were unable to reliably estimate the effect size and variances prior to the study." |
|
| Participants | "All patients were retired at time of inclusion or on sick leave" INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 62 (SD 9) years; SEX 14 (47%) male; FEV1 mean 48 (SD 19)% predicted
AGE mean 59 (SD 8) years; SEX 13 (43%) male; FEV1 mean 47 (SD 16)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP 6 months SUPERVISION yes INTERVENTION exercise training (Nordic walking) SETTING "mostly performed outdoors", group CONTACT 3 sessions a week AEROBIC TRAINING Nordic walking “bearable dyspnoea, optimal oxygen saturation”
STRENGTH TRAINING, OTHER COMPONENTS nil INTERVENTION education Weekly session: pulmonary pathophysiology, management of breathlessness and exacerbations, clearance of pulmonary secretions, smoking cessation, medication, nutrition |
|
| Outcomes | DEVICE DynaPort Activity Monitor (box on a waist belt, leg sensor: left upper leg)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Marie Breyer marie.breyer@gmx.at Otto Wagner Hospital, Vienna (Austria) Additional information requested |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation to either the Nordic Walking or the control group was done by a computer‐generated algorithm maintained by SPSS version 15.01" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT flow diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOME Registry: 6MWD (secondary outcome in paper) Paper
SECONDARY OUTCOMES Paper: SF36 (additional outcome reported) |
| Other bias | Unclear risk | Retrospectively registered No information as to whether participants had completed PR or whether they undertook PR during the follow‐up period which may have influenced results. |
Burtin 2015.
| Methods | DESIGN 2 groups DATES April 2009 to December 2010 SETTING hospital outpatient PR (Belgium) SAMPLE SIZE calculation based on daily walking time |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 7) years; SEX 34 (86%) male; FEV1 mean 45 (SD 14)% predicted
AGE mean 67 (SD 8) years; SEX 32 (79%) male; FEV1 mean 46 (SD 18)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION yes COMMON INTERVENTION PR SETTING centre‐based outpatient group CONTACT 60 sessions (1 week break for evaluation at Month 3)
AEROBIC TRAINING cycling exercise, treadmill walking, stair climbing, arm ergometry
STRENGTH TRAINING upper and lower limbs (3 sets, 8 repetitions)
OTHER COMPONENTS individual appointments with other healthcare providers as needed (pulmonologist, psychologist, occupational therapist, dietician, social worker, respiratory nurse) EDUCATION programme topics: understanding their disease, role of exercise training, dealing with breathlessness, adequate inhaler use, advice on how to adapt daily life activities, psychological aspects, nutritional aspects, social and financial aspects INTERVENTION PAC (in‐person) INTERFACE 8 individual sessions ACTIVITY not specified STEP‐TRACKING Sensewear Pro armband (no direct feedback) GOALS feedback provided during sessions RECORD, EDUCATION/RESOURCES nil SHAM INTERFACE 8 individual sessions STEP‐TRACKING Sensewear Pro armband (no direct feedback) ACTIVITY, RECORD, GOALS, EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE Dynaport Minimod1 (McRoberts) (lower back at the height of the second lumbar vertebra): time walking, step count Sensewear Pro (software version not reported) (upper arm): time in mild (2 to 3.6 METs) physical activity, MVPA (≥ 3.6 METs)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Thierry Troosters thierry.troosters@kuleuven.be KU Leuven (Belgium) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "This study is a two‐armed randomized controlled trial" Comment: insufficient information |
| Allocation concealment (selection bias) | Low risk | Quote: "Group allocation will be performed using sealed opaque envelopes in random block sizes (unknown by the investigators) after stratification for daily number of steps at baseline" |
| Blinding of participants (performance bias) | Low risk | Comment: Not possible to blind participants to the intervention BUT ‘sham attention’ provided to control group Quote: "Patients in the control group received a sham attention program. Duration and timing of the individualized sessions were similar to the intervention group, but the general health status of the patient and the progression during training was discussed during the conversations. Intermediate evaluation of physical activity was performed, but no structured feedback was provided" |
| Blinding of personnel (performance bias) | Low risk | Quote: "The multidisciplinary team providing pulmonary rehabilitation was also blinded to group allocation" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "all tests were performed by experienced health professionals that were blinded to group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | SECONDARY OUTCOMES
|
| Other bias | Unclear risk |
|
Casaburi 2012.
| Methods | DESIGN 2 groups DATES not reported SETTING 5 sites of the COPD Clinical Research Network (USA) SAMPLE SIZE calculation based on oxygen use |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 67 (SD 8) years; SEX 6 (55%) male; FEV1 mean 37 (SD 13)% predicted
AGE mean 67 (SD 10) years SEX 8 (73%) male; FEV1 mean 30 (SD 8)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION clinical co‐ordinator: education session focused on increasing LTOT understanding and encouraging ambulation instructed to use supplemental oxygen 24 hours a day INTERVENTION supplemental oxygen (lightweight ambulatory) INTERVENTION supplemental oxygen (E‐cylinder) |
|
| Outcomes | DEVICE RT3 (tri‐axial accelerometer) (waist belt)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Richard Casaburi casaburi@ucla.edu Harbor‐UCLA Medical Center, California (USA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were then randomized (stratified by enrollment site) to either continued E‐cylinder use or lightweight device use" Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of personnel (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow chart provided |
| Selective reporting (reporting bias) | Unclear risk | PRIMARY OUTCOME Paper: average oxygen use per hour, variability in oxygen use pattern over the course of the day (additional outcomes reported) SECONDARY OUTCOMES Registry: spirometry (Month 3, Month 6), haemoglobin level, functional exercise capacity, body weight, health status, ambulatory status, survival, number of exacerbations, physician office visits, hospitalisations, exercise endurance (not reported) |
| Other bias | Unclear risk |
|
Chaplin 2017.
| Methods | DESIGN 2 groups DATES May 2013 to July 2015 SETTING PR at university hospitals, primary care and rehabilitation services (UK) SAMPLE SIZE "The study will aim to recruit as many suitable patients as are referred to the PR service within the operational phase. One of the main objectives of this feasibility study is to provide data on recruitment and to enable an accurate estimation of sample size for a planned RCT. Based on calculations from previous studies carried out in the PR service, we anticipate a recruitment rate of around 100 patients during our operational phase. This feasibility study will enable us to estimate the required sample size for the subsequent RCT based on a realistic recruitment strategy." |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 10) years; SEX 38 (75%) male; FEV1 mean 59 (SD 29)% predicted
AGE mean 66 (SD 8) years SEX 33 (64%) male FEV1 mean 55 (SD 21)% predicted |
|
| Interventions | DURATION OF INTERVENTION web‐based: predicted to be 6 to 7 weeks, mean 11 weeks observed; centre‐based: 7 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION web‐based PR SETTING home CONTACT
AEROBIC TRAINING “encouraged to exercise on a daily basis” walking
STRENGTH TRAINING upper and lower limbs, hand‐held weights
OTHER COMPONENTS
EDUCATION individualised web page featuring a personalised action plan and educational content based on SPACE for COPD manual, work through content at their own pace INTERVENTION centre‐based PR SETTING outpatient group
CONTACT twice a week, exercise 60 min, education 60 min AEROBIC TRAINING
STRENGTH TRAINING upper and lower limbs, dumbbells, Borg scale rating of perceived exertion (rating 13 – 15)
OTHER COMPONENTS
EDUCATION variety of relevant self‐management topics: medication, relaxation skills, chest clearance, breathlessness management and energy conservation |
|
| Outcomes | DEVICE Sensewear armband (model and software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Emma Chaplin emma.chaplin@uhl‐tr.nhs.uk University Hospitals Of Leicester NHS Trust, Leicester (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation to treatment group allocation will be a 1:1 ratio to either group and will use internet based ‘Sealed Envelope’ randomisation codes where treatment group allocation is sent by automated email to the research physiotherapist" |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisation to treatment group allocation will be a 1:1 ratio to either group and will use internet based ‘Sealed Envelope’ randomisation codes where treatment group allocation is sent by automated email to the research physiotherapist" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "clinical measures... were conducted by a research physiotherapist who was blinded to treatment group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOME Registry: ISWD; Paper: only baseline ISWD data reported N.B. paper: "physical activity data are to be presented in future publications" |
| Other bias | Unclear risk |
REGISTRY 06/05/2015: The following changes were made to the trial record... The target number of participants was changed from 100 to 120 however 100 participants specified in the protocol and 103 people were randomised
REGISTRY "We anticipate that it will take approximately 6 to 7 weeks to work through the online programme". PROTOCOL "We anticipate from our work… that it will take approximately 6 weeks to work through the online programme". PAPER METHODS "It was anticipated from previous work that it would take ∼6– 8 weeks to work through the online programme" PAPER RESULTS "The average number of weeks to complete the website was 11±4"
Could this have been a reason for higher drop‐out rate? Not mentioned in Discussion ABSTRACT "Dropout rates were higher in the web‐based programme (57% vs 23%)." PAPER METHODS "7 weeks (4 weeks supervised; 3 weeks unsupervised)… Patients were classed as a completer if they had reached stage 3 or above of the web programme, achieving 75% of the programme which is standard in clinical practice for those attending classes".
REGISTRY Follow Up Length: 3 months PAPER METHODS "Clinical measures were performed at baseline and repeated again at the discharge assessment following completion of either rehabilitation programme (usually ∼6–7 weeks after starting the programme)"
PROTOCOL "patients’ ability to exercise safely will be monitored." PAPER METHODS "Non‐clinical outcomes included a web‐usage audit for the internet‐based programme, recruitment rates, eligibility and patient preference as well as dropout and completion rates in both treatment groups. Any serious adverse events were reported to the sponsor. A serious adverse event was defined as an acute exacerbation of their COPD that resulted in a hospital admission. In order to assess the patients’ ability to exercise safely, an exercise safety quiz was completed online before being able to progress onto stage 2 of the programme which involved exercising. Patients were then monitored online and through the weekly contacts." |
Charususin 2018.
| Methods | DESIGN two groups DATES February 2012 to October 2016 SETTING hospitals (Belgium, Germany, The Netherlands, Canada) SAMPLE SIZE calculation based on 6MWD |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 8) years; SEX 52 (47%) male; FEV1 mean 40 (SD 15)% predicted
AGE mean 65 (SD 7) years; SEX 43 (39%) male; FEV1 mean 43 (SD 17)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION PR SETTING centre‐based outpatient group CONTACT 3 to 5 sessions a week, 1 hour (20 sessions Germany, 36 sessions other centres) AEROBIC TRAINING cycling exercise, treadmill walking, stair climbing, arm ergometry
STRENGTH TRAINING upper and lower limbs, Borg Scale dyspnoea and rating of perceived exertion
OTHER COMPONENTS inspiratory muscle training as by group allocation EDUCATION nil INTERVENTION inspiratory muscle training Powerbreathe KH1 device ‘resistance training’ at high intensity (≥ 50% Pimax) 21 min: 6 cycles of 30 breaths; cycle: approx 3.5 min of resistive breathing, 1 min rest; 2 cycles, 3 sessions a day SHAM Powerbreathe KH1 device ‘endurance training’ at a low training intensity (≤ 10% Pimax) 21 min: 6 cycles of 30 breaths; cycle: approx 3.5 min of resistive breathing, 1 min rest; 3 cycles, 2 sessions a day |
|
| Outcomes | DEVICE Dynaport Minimod
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "HaB International (Southam, UK) and McRoberts (The Hague, The Netherlands) provided equipment for testing and training in this study on loan... Disclaimer: None of the sponsors had any role in the preparation of the trial design, patient recruitment, data collection, data analysis, interpretation of the data, approval of the report or the decision to submit this manuscript for publication." CONFLICT OF INTEREST "AM acknowledges a previous (now expired) beneficial interest in the POWERbreathe inspiratory muscle trainers in the form of a share of royalty income to the University of Birmingham, and a potential share of royalty income to Brunel University. In the past, she has also provided consultancy services to POWERbreathe International, but no longer does so. She is named on two patents relating to POWERbreathe products, including the device used in the present study, as well as being the author of two books on inspiratory muscle training. FM reports research support from Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Grifols and Novartis, advisory board participation for Boehringer Ingelheim and GlaxoSmithKline, and speaking engagements for Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Grifols and Novartis." CONTACT Daniel Langer daniel.langer@kuleuven.be KU Leuven (Belgium) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Group allocation will be performed by simple randomisation using sealed opaque envelopes in random block sizes of four and six (order unknown to investigators)" |
| Allocation concealment (selection bias) | Low risk | Quote: "Group allocation will be performed by simple randomisation using sealed opaque envelopes in random block sizes of four and six (order unknown to investigators)" |
| Blinding of participants (performance bias) | Low risk | Quote: "(sham) intervention described to patients as ‘endurance training’ at a low training intensity" |
| Blinding of personnel (performance bias) | Low risk | Quote: "Physiotherapists providing this intervention will be blinded to group allocation of patients" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity and exercise capacity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL: Quote: "all tests will be performed by experienced investigators who are blinded to group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Low risk | Protocol: anxiety and depression (not reported) |
| Other bias | Unclear risk | Quote: "data were analysed using a modified intention‐to‐treat approach... we did not consider patients who had missing outcome data due to loss to follow‐up in the analysis. Consequently, no imputation for missing data was performed and a so‐called ‘complete/available case analysis’ was performed" Quote: "Interactions between centres and between‐group post‐treatment differences in PImax, progression of exercise training intensity, endurance cycling time and 6MWD were observed." Quote: "One of the centres offering a 36 session programme (32% of total inclusions) consistently exceeded between group differences in the centre offering 20 sessions (36% of total inclusions). In other centres offering 36 sessions (32% of total inclusions), between‐group differences in these outcomes were consistently smaller than in the centre offering a lower training volume" Quote: "The sham intervention... might even have constituted an endurance‐type training stimulus for these patients in addition to the endurance‐type training stimulus provided by the exercise training sessions" |
Cruz 2016.
| Methods | DESIGN 2 groups DATES April to July 2014 SETTING 3 primary care centres, district hospital (Portugal) SAMPLE SIZE calculation based on MVPA time |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 69 (SD 8) years; SEX 13 (81%) male; FEV1 mean 66 (SD 21)% predicted
AGE mean 64 (SD 8) years; SEX 14 (88%) male; FEV1 mean 68 (SD 20)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION yes COMMON INTERVENTION PR SETTING outpatient group CONTACT 3 sessions a week, 1 hour AEROBIC TRAINING walking, 20 minutes, modified Borg Scale dyspnoea and fatigue (rating 4 to 6)
STRENGTH TRAINING upper and lower limbs, 15 minutes (2 sets, 10 repetitions)
OTHER COMPONENTS
EDUCATION one session per week, 90 minutes
INTERVENTION PAC INTERFACE
ACTIVITY walking STEP‐TRACKING pedometer Yamax Power Walker EX‐510 (direct feedback) RECORD diary: daily step count, short‐term step count goals GOALS ≥ 800 steps if previous goal met EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE AGT3X+ (Actilife v6.10.4)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Alda Marques amarques@ua.pt University of Aveiro, Aveiro (Portugal) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "This was a randomised controlled trial. Patients were randomly assigned…using a computer‐generated schedule in random blocks of two" |
| Allocation concealment (selection bias) | Low risk | Quote: "One researcher kept the allocation sequence in sealed opaque envelopes, drew the envelopes and scheduled patients" |
| Blinding of participants (performance bias) | Unclear risk | Quote: "Patients knew about the existence of two groups but not the differences between interventions" |
| Blinding of personnel (performance bias) | High risk | Quote: "All measures were administrated in a face‐to‐face interview conducted by the same researchers who implemented the intervention. Thus, assessor blinding was not possible" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity: Quote: "all measures were administrated in a face‐to‐face interview conducted by the same researchers who implemented the intervention. Thus, assessor blinding was not possible" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOMES Registry: time spent in different postures (not reported) SECONDARY OUTCOMES Registry: patients' perspectives post intervention, change in number and duration of respiratory exacerbations and hospitalisations (not reported) Paper: upper‐limb isometric muscle strength, behavioural regulations in exercise (additional outcomes) |
| Other bias | Unclear risk | Both groups underwent 12 weeks of PR between April and July 2014. The intervention group also received an additional 12 weeks of physical activity‐focused behavioural intervention
|
Curtis 2016.
| Methods | DESIGN 2 groups DATES December 2012 to March 2015 SETTING Royal Brompton Hospital, London (UK) SAMPLE SIZE calculation based on peak workload (incremental cycle ergometry) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA (PAPER)
EXCLUSION CRITERIA (REGISTRY)
BASELINE CHARACTERISTICS
AGE mean 66 (SD 10) years; SEX 14 (45%) male; FEV1 mean 48 (SD 23)% predicted
AGE mean 68 (SD 7) years; SEX 20 (59%) male; FEV1 mean 52 (SD 20)% predicted |
|
| Interventions | DURATION OF INTERVENTION AND FOLLOW‐UP 10 weeks (PR 8 weeks) SUPERVISION no COMMON INTERVENTION PR DURATION 8 weeks SETTING multidisciplinary outpatient group: goal‐setting and progressive approach, continuous reassessment to allow progression as tolerated CONTACT 3 exercise sessions a week (2 supervised) 1 hour exercise, 1 hour education AEROBIC TRAINING treadmill and cycle exercise; intensity 60% to 80% predicted VO2 peak STRENGTH TRAINING upper and lower limb, weights, progression as tolerated OTHER COMPONENTS 1 unsupervised home‐based exercise session EDUCATION self‐management topics including exercise, medication use, diet, coping strategies, increasing physical activity, recognising and managing infections INTERVENTION ACE inhibitor (10 mg enalapril) once daily Started treatment 1 week before PR PLACEBO (microcrystalline cellulose) once daily Started treatment 1 week before PR |
|
| Outcomes | DEVICE SenseWear Pro Armband (professional version 7.0) (body of the triceps muscle of right arm)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes |
FUNDING "Supported by the Medical Research Council (grant reference MR/J000620/1), which provided the salary for K.J.C. The salary of M.I.P. is partly funded by the National Institute for Health Research (NIHR) Biomedical Research Unit. H.M. is partly funded by the NIHR University College London Hospitals Biomedical Research Centre. W.D.‐C.M. is funded by a NIHR Clinical Scientist Award (CS/7/007), a NIHR Clinical Trials Fellowship (NIHR‐CTF‐01‐12‐04), a Medical Research Council New Investigator Grant (G1002113), and the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for NW London." CONFLICT OF INTEREST provided CONTACT Nicholas S Hopkinson n.hopkinson@ic.ac.uk Imperial College, London (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomly allocated… using block randomization and a block size of four. Randomization was performed by Imperial College Trials Unit" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | Low risk | Quote: "Both subjects and the assessor were blind to treatment allocation" |
| Blinding of personnel (performance bias) | Unclear risk | Insufficient information |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Quote: "Both subjects and the assessor were blind to treatment allocation" |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Quote: "Both subjects and the assessor were blind to treatment allocation"Quote: |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | 6MWD listed as secondary outcome in the registry; not reported in the paper |
| Other bias | Low risk | Quote: “Analysis was performed on a per protocol basis” Comment: Prospectively registered |
Dal Negro 2012.
| Methods | DESIGN 2 groups DATES not reported SETTING outpatients..."regularly attending our units" (Italy) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 75 (SD 5) years; SEX 32 (73%) male; FEV1 mean 0.8 (SD 0.4) litres per second
AGE mean 73 (SD 8) years; SEX 29 (66%) male; FEV1 mean 0.8 (SD 0.2) litres per second |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION essential amino acids supplement, oral mixture (4 grams, Aminotrofic) dose at 10:00 and 17:00 PLACEBO isocaloric undistinguishable dose oral mixture dose at 10:00 and 17:00 |
|
| Outcomes | DEVICE SenseWear Armband Pro3 (software version not reported) (upper right arm)
ASSESSMENT TIME POINTS
PRIMARY/SECONDARY OUTCOMES
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement not provided CONTACT R Dal Negro rdalnegro@ulss22.ven.it Federica Boschi federica boschi@unipv.it Universita degli Studi di Pavia, Pavia (Italy) Additional data requested |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Eight‐eight outpatients…were selected from those regularly attending our units and enrolled… randomisation table" |
| Allocation concealment (selection bias) | Low risk | Quote: "investigators were blinded to the randomisation table, the code assignments…as subjects were enrolled, they were assigned a progressive number" |
| Blinding of participants (performance bias) | Low risk | Quote: "indistinguishable dose of placebo" |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "double‐blind… investigators were blinded to…the procedure" Comment: not clear if this refers to personnel or outcome assessors |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL: Quote: "double‐blind… investigators were blinded to…the procedure" Comment: not clear if this refers to personnel or outcome assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | No trial registry; results presented as in Methods Unclear whether some results represent change from baseline or post‐intervention values |
| Other bias | Unclear risk | Unclear relationship with other publication (Dal Negro 2010) |
De Blok 2006.
| Methods | DESIGN 2 groups DATES not reported SETTING PR (The Netherlands) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 10) years; SEX 5 (50%) male; FEV1 mean 52 (SD 22)% predicted
AGE mean 63 (SD 12) years; SEX 4 (36%) male; FEV1 mean 43 (SD 13)% predicted |
|
| Interventions | DURATION OF INTERVENTION 9 weeks FOLLOW‐UP no SUPERVISION yes COMMON INTERVENTION PR DURATION 9 weeks SETTING centre‐based outpatient group CONTACT not stated EXERCISE TRAINING “according to evidence‐based guidelines” OTHER COMPONENTS dietary intervention EDUCATION psycho‐educational modules INTERVENTION PAC (in‐person, Altenburg 2015, Hospes 2009) INTERFACE 4 individual sessions ACTIVITY lifestyle physical activity (e.g. walking, cycling, stair‐climbing, gardening) STEP‐TRACKING pedometer (direct feedback) RECORD diary: daily step count, other activities (e.g. cycle, swim) GOALS “maximal” step‐count goal, end intervention: set personal “physical activity norm” (between mean and maximal step count) goal EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE Yamax Digi‐Walker SW‐200 (pedometer) (belt or waistband)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement not provided CONTACT Mathieu HG de Greef M.de.Greef@ppsw.rug.nl University of Groningen (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients who were referred for pulmonary rehabilitation were randomly assigned" Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Low risk | Quote: "clinical staff…blinded for group assignment" |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: unclear if step count was reported by participants |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods |
| Other bias | Low risk | N/A |
De Roos 2017.
| Methods | DESIGN 2 groups DATES not reported SETTING primary physiotherapy care centres (The Netherlands) SAMPLE SIZE calculation based on walking time |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 69 (SD 10) years; SEX 8 (31%) male; FEV1 mean 68 (SD 8)% predicted
AGE mean 71 (SD 9) years; SEX 10 (38%) male; FEV1 mean 65 (SD 10)% predicted |
|
| Interventions | DURATION OF INTERVENTION 10 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION exercise training SETTING group‐based circuit training in primary physiotherapy care centres CONTACT 2 sessions a week, 1 hour AEROBIC TRAINING 10 minutes treadmill walking, 10 minutes cycling STRENGTH TRAINING extremity resistance exercises OTHER COMPONENTS unsupervised home exercise programme once a week (≥ 30 minutes) “Emphasis on continuity rather than increasing training intensity and goal setting” EDUCATION 5 minutes a week: exercise compliance, importance of staying active in daily life "further details on onset intensity, frequency, duration and progression of the workload are described in Appendix A, see online supplementary material" (not available in online supp) NO INTERVENTION standard medical care from their general physician, self‐referral consultation in case of worsening symptoms |
|
| Outcomes | DEVICE Personal activity monitor (uniaxial accelerometer) (waist) Quantifies amount of motion in vertical plane with EE ≥ 0.8 METs
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "Eight activity monitors were provided without charge by PAM. PAM had no involvement in the study." CONFLICT OF INTEREST statement provided CONTACT Pieter de Roos pieterderoos@chello.nl, p.deroos@hotmail.com Physiotherapy Centre De Oppers (The Netherlands) Additional information provided: confirmed threshold for MPA |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Allocation was randomised… All possible sequences in permuted blocks of four with two intervention and two control tickets were created and placed at random in sequentially numbered order by an individual not affiliated to the study" |
| Allocation concealment (selection bias) | Low risk | Quote: "concealed using opaque sealed envelopes… At intake and under the supervision of the physiotherapist in the primary care centre, participants were instructed to open the first envelope" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to intervention |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "there was an inevitable lack of blinding of the physiotherapists" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity: Quote: "due to the setting of the research, the outcome assessor was not blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT flow diagram provided |
| Selective reporting (reporting bias) | Low risk | Results presented as in Methods |
| Other bias | Unclear risk | Clinical trial registration number NL24766.018.08. but unable to locate Email confirmation from author that trial was registered as per Dutch regulations, unable to access in English |
Demeyer 2017.
| Methods | DESIGN 2 groups DATES May 2014 to March 2015 SETTING centres across Europe (Belgium, Greece, UK, Switzerland, The Netherlands) SAMPLE SIZE calculation based on step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 8) years; SEX 111 (65%) male; FEV1 mean 55 (SD 20)% predicted
AGE mean 67 (SD 8) years; SEX 108 (63%) male; FEV1 mean 57 (SD 21)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION physical activity intervention INTERFACE semi‐automated telecoaching
ACTIVITY "favourite activities" STEP‐TRACKING Step counter (Fitbug Air©; direct feedback) RECORD Fitbug sends step count to app GOALS
EDUCATION/RESOURCES Home exercise booklet NO INTERVENTION Individual in‐person discussion (5 to 10 minutes at Visit 2) Standard leaflet explaining the importance of physical activity in COPD and information about physical activity recommendations |
|
| Outcomes | DEVICES (waist) Dynaport MoveMonitor: time walking, walking intensity Actigraph GT3x (software version not reported): step count, MVPA time
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "Swisscom AG who provided 30 sim cards and data usage of up to 1 GB per month" CONFLICT OF INTEREST statement provided CONTACT Heleen Demeyer heleen.demeyer@kuleuven.be KU Leuven (Belgium) Additional information provided: physical activity, HRQOL, exercise capacity |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The random sequence was generated with varying block sizes of 4, 6 or 8 and stratified by centre using a statistical software (STATA V.12.0, StataCorp, College Station, Texas, USA)" |
| Allocation concealment (selection bias) | Low risk | Quote: "Investigators obtained group allocation using an online system that ensured concealment of random allocation" |
| Blinding of participants (performance bias) | High risk | Quote: "Neither patients nor investigators were blinded to treatment allocation" |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "Neither patients nor investigators were blinded to treatment allocation" Comment: Not clear if this also refers to personnel responsible for implementation |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity: Quote: "neither patients nor investigators were blinded to treatment allocation... nevertheless, we do acknowledge the lack of blinding could have minimally influenced the 6MWD results" Comment: infers 'investigators' refers to assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | SECONDARY OUTCOMES Registry: Proportion of patients showing an increase in physical activity > 20%; Paper: "for responder analysis a clinically significant increase in step count was defined as ≥ 1000 steps" Registry: anxiety and depression, PROactive instrument, satisfaction, compliance (not reported) Paper: time walking, walking intensity, sedentarism (defined as step count < 5000), AECOPD in the last 12 months (additional outcomes reported) |
| Other bias | Unclear risk | Sample size calculation
|
Duiverman 2008.
| Methods | DESIGN 2 groups DATES November 2004 SETTING 9 rehabilitation centres (The Netherlands) SAMPLE SIZE calculation based on CRQ |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 63 (SD 10) years; SEX 18 (58%) male; FEV1 not reported
AGE mean 61 (SD 7) years; SEX 17 (49%) male; FEV1 not reported |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION yes COMMON INTERVENTION PR SETTING in‐hospital or outpatient (depending on travel distance to centre) CONTACT 3 sessions a week, 1 hour AEROBIC TRAINING Weeks 3 to 12:
STRENGTH TRAINING upper and lower limbs OTHER COMPONENTS
EDUCATION group sessions: disease, treatment strategies, medication, coping, role of rehabilitation, how to recognise an exacerbation, breathing exercises INTERVENTION NIPPV (nocturnal, spontaneous/timed mode, nasal or full face mask) In the hospital within a week after the baseline measurements (before starting PR) Maximal tolerated inspiratory airway pressure, titrated for optimal correction of nocturnal ABG In‐hospital practice period until ≥ 6 hours sleep |
|
| Outcomes | DEVICE Digiwalker SW‐200 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOME
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT ML Duiverman m.l.duiverman@int.umcg.nl University Medical Center Groningen (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation was computerised and performed by an independent statistician" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of personnel (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity and exercise capacity (cycle ergometry) |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity (6MWD, ESWT): Quote: "Masking: None (Open Label)" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow diagram provided: differential attrition noted Quote: "In the NIPPV + PR group, seven patients did not complete the study. Five patients could not adapt to the NIPPV (16%), one patient withdrew because of rheumatic complaints and one patient died of progressive respiratory failure due to a COPD exacerbation after 69 days on NIPPV, despite initial blood gas improvements... In the PR group, three patients (9%) did not complete the study because of non‐compliance" |
| Selective reporting (reporting bias) | High risk | Registry: polysomnography, baseline dyspnoea index, exercise capacity, electromyography, respiratory muscle strength (not reported) Paper: additional outcomes, step count, HRQOL (Maugeri Respiratory Failure questionnaire, Severe Respiratory Insufficiency questionnaire), anxiety and depression, dyspnoea, arterial blood gases, treatment compliance (additional outcomes) |
| Other bias | Unclear risk |
|
Effing 2011.
| Methods | DESIGN 2 groups DATES November 2004 to July 2008 SETTING hospital outpatient pulmonary clinic (The Netherlands) SAMPLE SIZE calculation based on ISWD |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 63 (SD 8) years; SEX 42 (54%) male; FEV1 mean 50 (SD 14)% predicted
AGE mean 64 (SD 8) years; SEX 44 (58%) male; FEV1 mean 51 (SD 17)% predicted |
|
| Interventions | DURATION OF INTERVENTION 11 months FOLLOW‐UP yes SUPERVISION yes COMMON INTERVENTION self‐management 4 sessions (2 hours) follow‐up phone calls allowed to attend regular, non‐COPEactive physiotherapy sessions if this was prescribed as part of regular care INTERVENTION exercise training (COPE‐active) Programme development: problematic activities incorporated (bicycling, walking, climbing stairs, and lifting weights) SETTING exercise training in private physiotherapy practices, small groups (2 to 3 participants) CONTACT
AEROBIC TRAINING bicycling, walking, climbing stairs
STRENGTH TRAINING upper and lower extremities
OTHER COMPONENTS
EDUCATION nil N.B. n = 25 (33%) received non‐standardised physiotherapy |
|
| Outcomes | DEVICE Yamax Digi‐Walker SW200 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement provided CONTACT Tanja Effing tanja.effing@health.sa.gov.au University of South Australia, Adelaide (Australia) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomised into two study groups, using a minimisation programme" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOMES Registry: duration and severity of exacerbations measured by daily diaries (not reported) SECONDARY OUTCOMES Registry: Social Support List, self‐efficacy list, EQ5D (not reported) |
| Other bias | Unclear risk |
|
Egan 2010.
| Methods | DESIGN 2 groups DATES June 2007 to July 2010 SETTING PR (UK) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS not reported
|
|
| Interventions | DURATION OF INTERVENTION 7 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION PR SETTING centre‐based outpatient group CONTACT 2 sessions a week, 1 hour exercise, 1 hour education AEROBIC TRAINING exercise bike
STRENGTH TRAINING light dumbbells and body resistance
OTHER COMPONENTS
EDUCATION
|
|
| Outcomes | DEVICE SenseWear Pro (software version 6.0) (right triceps)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement provided CONTACT Richard Costello rcostello@rcsi.ie Beaumont Hospital, Dublin (Ireland) Additional information provided: confirmed methodology as per 2012 publication, results as in abstract (no group comparison in paper) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "prospective single‐blinded randomised controlled study" (abstract) Quote: "random allocation to parallel assignment"(registry) |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: Quote: "assessor blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Total number randomised and group numbers provided; no details re attrition or exclusion |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information (abstract only) |
| Other bias | Unclear risk | Only PR group data subsequently published |
Felcar 2018.
| Methods | DESIGN 2 groups DATES July 2010 to October 2014 SETTING university‐based outpatient clinic (Brazil) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA (REGISTRY)
INCLUSION CRITERIA (PAPER)
EXCLUSION CRITERIA (REGISTRY)
EXCLUSION CRITERIA (PAPER)
BASELINE CHARACTERISTICS
AGE mean 69 (SD 9) years; SEX 14 (41%) male; FEV1 mean 48 (SD 17)% predicted
AGE mean 68 (SD 8) years; SEX 9 (25%) male; FEV1 mean 46 (SD 14)% predicted |
|
| Interventions | DURATION OF INTERVENTION AND FOLLOW‐UP 6 months FOLLOW‐UP no SUPERVISION yes INTERVENTION water‐based exercise training SETTING outpatient group; heated pool (33 oC), 1 metre depth; up to 4 participants CONTACT 60 sessions, 1 hour
AEROBIC TRAINING high‐intensity, individualised training load, revised weekly
STRENGTH TRAINING (3 sets, 8 repetitions)
OTHER COMPONENTS nil EDUCATION 8 group sessions held every 2 weeks, 15 minutes: disease features and treatment, such as physical training, energy conservation techniques, symptoms, nutrition INTERVENTION land‐based exercise training SETTING centre‐based outpatient group CONTACT 60 sessions, 1 hour
AEROBIC TRAINING high‐intensity, individualised training load
STRENGTH TRAINING upper and lower limbs
OTHER COMPONENTS nil EDUCATION 8 group sessions held every 2 weeks, 15 minutes: disease features and treatment, such as physical training, energy conservation techniques, symptoms, nutrition |
|
| Outcomes | DEVICE Power Walker‐PW610: monitor set individually taking into consideration body weight and step length (measured in a 10‐metre walk at usual speed)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Fabio Pitta fabiopitta@uol.com.br Universidade Estadual de Londrina, Parana (Brazil) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation was performed in two stages: generation of numbers (table of random numbers)" |
| Allocation concealment (selection bias) | Low risk | Quote: "blind allocation (opaque and sealed envelopes)" |
| Blinding of participants (performance bias) | High risk | Quote: "Due to the characteristics of the intervention, it was not possible to blind participants and therapists who applied the training" |
| Blinding of personnel (performance bias) | High risk | Quote: "Due to the characteristics of the intervention, it was not possible to blind participants and therapists who applied the training" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "outcome assessors were not informed about the allocation of patients in the respective groups" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | Registry (Time Frame: 4 years) SECONDARY OUTCOMES Registry: static balance, timed up and go test (not reported) Paper: spirometry, peripheral and respiratory muscle strength, anthropometry, dyspnoea, anxiety and depression (additional outcomes) |
| Other bias | Unclear risk | Registry
|
Gamper 2019.
| Methods | DESIGN 2 groups DATES screened for inclusion July to December 2016 SETTING Rehabilitation Center, Walenstadtberg (Switzerland) SAMPLE SIZE "aim to... estimate the required sample size for a RCT" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 7) years; SEX 5 (63%) male; FEV1 not reported
AGE mean 63 (SD 9) years; SEX 5 (63%) male; FEV1 not reported |
|
| Interventions | DURATION OF INTERVENTION 3 weeks FOLLOW‐UP 3 months SUPERVISION yes COMMON INTERVENTION exercise training DURATION 3 weeks SETTING inpatient (commence Day 3 of admission), supervised CONTACT 6 sessions a week, 30 minutes AEROBIC TRAINING voluntary exhaustion, 8 to 12 minutes
INTERVENTION outdoor walking
INTERVENTION cycle ergometer
|
|
| Outcomes | DEVICE Fitbit One (Fitbit Inc., San Francisco, CA, USA)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was financially supported by Valens Clinics". CONFLICT OF INTEREST "The authors state that they have no financial, consulting or personal relationships to people or organizations that could influence the authors’ work. There are no conflicts of interests". CONTACT Esther Gamper esther.gamper@rheinburg.ch Zurich University of Applied Science, Winterthur (Switzerland) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "concealed block randomization procedure" Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Quote: "concealed block randomization procedure" Comment: insufficient information |
| Blinding of participants (performance bias) | High risk | REGISTRY Blinding: Open (masking not used) |
| Blinding of personnel (performance bias) | High risk | REGISTRY Blinding: Open (masking not used) |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Insufficient information (?participant diary to self‐report) |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Blinded assessor for 6MWT, otherwise assessor unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Low risk | Registry and paper in agreement |
| Other bias | Unclear risk | Retrospective registration |
Goris 2003.
| Methods | DESIGN 2 groups DATES not reported SETTING hospital and pulmonary rehabilitation centre (The Netherlands) SAMPLE SIZE calculation based on BMI |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
"None of the patients participated in an outpatient or home‐based PR programme" BASELINE CHARACTERISTICS
AGE mean 61 (SD 12) years; SEX 6 (55%) male; FEV1 mean 40 (SD 13)% predicted
AGE mean 62 (SD 10) years; SEX 6 (67%) male; FEV1 mean 40 (SD 16)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION nutritional supplement(energy dense) 3 125 ml Respifor (sip‐feed, Nutricia, The Netherlands) morning, afternoon and evening (daily) provided 2.38 MJ a day (20% protein, 20% fat, 60% carbohydrate) NO INTERVENTION nutritional advice from a dietitian on how to increase their energy intake |
|
| Outcomes | DEVICE Tracmor (triaxial accelerometer) (belt at the back of the waist)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement not provided CONTACT Marja Vermeeren vermeeren.marja@zonnet.nl University Hospital Maastricht (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The patients were then at random assigned (with a randomisation table) to the intervention group or to the control group" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | Unclear risk | Not specified |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity (energy expenditure) |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as per methods |
| Other bias | Unclear risk | Quote: "Depleted COPD patients (n=20) were studied 1 and 3 months after discharge from the university hospital… or from the pulmonary rehabilitation centre" Comment: participants post‐admission might respond differently to people who have just completed PR |
Hartman 2016.
| Methods | DESIGN cross‐over trial (only pre‐cross‐over data used), 2 groups DATES May 2011 to May 2013 SETTING hospital (The Netherlands) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 59 (SD 10) years; SEX 6 (32%) male; FEV1 mean 32 (SD 8)% predicted
AGE mean 59 (SD 8) years; SEX 4 (17%) male; FEV1 mean 30 (SD 7)% predicted |
|
| Interventions | DURATION OF INTERVENTION surgery FOLLOW‐UP 6 months SUPERVISION yes INTERVENTION endobronchial valve surgery |
|
| Outcomes | DEVICE Dynaport MoveMonitor (around the waist at the lower back)
ASSESSMENT TIME POINTS
PRIMARY/SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST "NHT and JH have no conflicts of interest, KK received travel grants and a speakers fee from PulmonX, DJS is a physician advisor to PulmonX, received travel grants and lecture fees for educational and scientific meetings from PulmonX and participates in other clinical trials funded by PulmonX. All authors had complete access to the data, reviewed and approved the manuscript. PulmonX was not involved at any stage during the trial." CONTACT Jorine Hartman j.hartman@umcg.nl University Medical Center Groningen (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "A randomized controlled crossover trial" Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "Masking/Blinding: none" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: Quote: "Masking/Blinding: none" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Participant flow diagram provided Attrition in intervention group attributable to group allocation (8 participants had valves removed and not included at 6‐month assessment) |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOMES
Registry: FVC, FEV1, 6MWD (secondary outcomes in paper) Manuscript: daily physical activity (not in registry) SECONDARY OUTCOMES Paper: SGRQ, dyspneoa (additional outcomes) |
| Other bias | Low risk | N/A |
Holland 2017.
| Methods | DESIGN 2 groups DATES October 2011 to September 2014 SETTING 2 hospital‐based outpatient PR programmes (Australia) SAMPLE SIZE calculation based on CRQ and 6MWD |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 69 (SD 13) years; SEX 48 (60%) male; FEV1 mean 52 (SD 19)% predicted
AGE mean 69 (SD 10) years; SEX 51 (60%) male; FEV1 mean 49 (SD 19)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP 12 months SUPERVISION No INTERVENTION home‐based PR SETTING home CONTACT
AEROBIC TRAINING
STRENGTH TRAINING functional activities and equipment accessible in home, including sit‐to‐stand from a dining chair, step ups on an internal or external step, and water bottles for upper limb weights OTHER COMPONENTS
EDUCATION
INTERVENTION centre‐based PR SETTING outpatient group CONTACT 2 sessions a week AEROBIC TRAINING ≥ 30 minutes
STRENGTH TRAINING functional activities such as stair climbing and sit‐to‐stand practice, as well as free weights for the upper limbs OTHER COMPONENTS Unsupervised home exercise programme 3 sessions a week EDUCATION Self‐management training: structured (lecture‐based) and unstructured disease management education and goal setting (management of exacerbations, understanding medications, ongoing participation in exercise) |
|
| Outcomes | DEVICE SenseWear Armband (software version 7.0) (left upper arm)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Anne Holland A.Holland@alfred.org.au Alfred Health, Melbourne (Australia) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A randomised, controlled equivalence trial… using a computer generated sequence… generated by an individual unrelated to the study" |
| Allocation concealment (selection bias) | Low risk | Quote: "randomised to treatment groups… using a computer generated sequence that was concealed using opaque envelopes" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "All subsequent assessments were performed by an individual blinded to group allocation, who had no involvement in provision of either intervention. The success of assessor blinding was evaluated after the 12‐month assessment by asking the assessor to nominate the group to which they thought the participant had been assigned…At the end of the trial, the assessors correctly identified group allocation for 52% of participants (κ=0.26), demonstrating the success of blinding" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | SECONDARY OUTCOMES Protocol: Spirometry will be repeated at 12 months (only baseline reported) |
| Other bias | Low risk | Quote: "We made every attempt to assess all participants at all time points, even if they were unwell or had not completed the programme. This may have affected the overall magnitude of benefit, but is reflective of the real world challenges of pulmonary rehabilitation" "Importantly, the programme completion rate in the centre‐based group was low, which may not reflect completion rates in all real world centre‐based services and may limit the generalisability of results" |
Hornikx 2015.
| Methods | DESIGN 2 groups DATES March 2013 to April 2014 SETTING hospital (Belgium) SAMPLE SIZE calculation based on walking time |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 66 (SD 7) years; SEX 8 (53%) male; FEV1 mean 38 (17%)% predicted
AGE mean 68 (SD 6) years; SEX 9 (60%) male; FEV1 mean 48 (18%)% predicted |
|
| Interventions | DURATION OF INTERVENTION 4 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION PAC INTERFACE 3 phone calls a week ACTIVITY not specified STEP‐TRACKING pedometer (direct feedback) GOALS progress report with tips to increase physical activity posted Week 2 and Week 4 RECORD, EDUCATION/RESOURCES nil NO INTERVENTION provided with advice about increasing physical activity during the hospital stay from a physiotherapist |
|
| Outcomes | DEVICE Dynaport MoveMonitor (lower back at the height of the second lumbar vertebra)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Thierry Troosters thierry.troosters@kuleuven.be KU Leuven (Belgium) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Eligible patients were randomized" Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOMES Registry: step count Paper: step count, time walking (used for sample size calculation), walking intensity SECONDARY OUTCOMES Paper: spirometry, peripheral muscle strength, dyspnoea, CAT (additional outcomes reported) Paper: hospital readmission, medications, PR enrolment (results presented, not in methods) |
| Other bias | Unclear risk | Quote: "By executing this study, we experienced that including patients after an exacerbation of COPD is very difficult. After 1 year, only 30 patients agreed to participate in the study. Intermediate analyses did not reveal better improvements in physical activity in the group that received maximal counselling and real‐time feedback compared to usual care. Based on these conclusions and the fact that the study was very time consuming for the researcher, we decided not to continue with the study" |
Hospes 2009.
| Methods | DESIGN 2 groups DATES not reported SETTING hospital pulmonary outpatient clinic (The Netherlands) SAMPLE SIZE "a power analysis was calculated" (outcome not stated) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 63 (SD 9) years; SEX 10 (50%) male; FEV1 mean 68 (SD 18)% predicted
AGE mean 61 (SD 9) years; SEX 11 (58%) male; FEV1 mean 62 (SD 14)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION pac (in‐person, Altenburg 2015, De Blok 2006) INTERFACE 5 individual sessions ACTIVITY lifestyle physical activity (e.g. walking, cycling, stair‐climbing, gardening) STEP‐TRACKING pedometer (direct feedback) RECORD Diary: daily step count, other activities (e.g. cycle, swim) GOALS “maximal” step count goal, end intervention: set personal “physical activity norm” (between mean and maximal step count) goal EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE Digiwalker SW‐2000 (pedometer)
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING "This study was supported by a research grant from Boehringer Ingelheim B.V. The funding source(s) had no involvement in the study." CONFLICT OF INTEREST "Herewith we state that none of the authors had any actual or potential conflict of interest including any financial, personal or other relationships with other people or organizations within 3 years of beginning the submitted work that could inappropriately influence, or be perceived to influence, their work." CONTACT Linda Bossenbroek l.bossenbroek@umcg.nl University Medical Center Groningen (The Netherlands) Additional information requested. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned…" Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity: unclear if step count was reported by participants |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods apart from subgroups for step count in Results (justification presented in Discussion) |
| Other bias | Low risk | N/A |
Jolly 2018.
| Methods | DESIGN 2 groups DATES March 2014 to December 2016 SETTING 71 general practices (UK) SAMPLE SIZE calculation based on SGRQ |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
N.B. use of population descriptor as 'mild' refers to mMRC grade FEV1 ≥ 80% predicted: 89 of 289 (31%) participants in intervention group and 104 of 288 (36%) participants in no‐intervention group so does not meet review definition for subgroup analyses BASELINE CHARACTERISTICS
AGE mean 71 (SD 9) years, SEX 183 (63%) male; FEV1 mean 71 (SD 19)% predicted
AGE mean 70 (SD 8) years; SEX 183 (64%) male; FEV1 mean 72 (SD 19)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION no INTERVENTION self‐management (telephone health coaching) INTERFACE telephone by a nurse with
STEP‐TRACKING pedometer RECORD self‐monitoring diary EDUCATION/RESOURCES
|
|
| Outcomes | DEVICE GENEActiv [non‐dominant wrist]
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Kate Jolly c.b.jolly@bham.ac.uk University of Birmingham, Birmingham (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "individually randomised in a 1:1 ratio to the telephone health coaching or usual care group stratified by centre. The allocation was made using a web‐based programme hosted by the Primary Care Clinical Research and Trials Unit, University of Birmingham. Centre specific randomisation lists were produced by a statistician at the trials unit" |
| Allocation concealment (selection bias) | Low risk | Quote: "Only the Primary Care Clinical Research and Trials Unit had access to the allocation sequence. Patients were informed of their allocation at the end of the recruitment appointment" |
| Blinding of participants (performance bias) | High risk | Quote: "Patients… were not masked to treatment allocation" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL: Quote: "data were entered into the study database by researchers at the University of Birmingham who were masked to the treatment allocation" (postal responses) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | PRIMARY OUTCOME (SGRQ) Registry: 6 and 12 months; Paper: 12 months only SECONDARY OUTCOMES Registry: none specified |
| Other bias | Low risk | N/A |
Kanabar 2015.
| Methods | DESIGN 2 groups DATES not reported (abstract only) SETTING "following discharge from a respiratory‐related admission" (UK) SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION/EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS
AGE mean 68 (SD 9) years; SEX 7 (47%) male; FEV1 mean 36 (SD 12)% predicted
AGE mean 67 (SD 4) years; SEX 4 (40%) male; FEV1 mean 48 (SD 13)% predicted |
|
| Interventions | DURATION OF INTERVENTION 7 days FOLLOW‐UP no SUPERVISION no INTERVENTION self‐management (SPACE) (as in Mitchell 2013) brief physical activity advice in the form of a self‐management manual |
|
| Outcomes | DEVICE SenseWear armband Pro3 (software version not reported)
ASSESSMENT TIME POINTS daily for 7 days OUTCOMES
|
|
| Notes | FUNDING, CONFLICT OF INTEREST not reported (abstract only) CONTACT Sally Singh sally.singh@uhl‐tr.nhs.uk University Hospitals Of Leicester NHS Trust, Leicester (UK) Additional information provided: group demographics, physical activity and exercise outcomes |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomised controlled trial" Comment: Insufficient information (abstract only) |
| Allocation concealment (selection bias) | Unclear risk | Not specified (abstract only) |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified (abstract only) |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Exercise capacity: not specified (abstract only) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Total number randomised and group numbers provided; no details re attrition or exclusion (abstract only) |
| Selective reporting (reporting bias) | High risk | Paper:
|
| Other bias | Low risk | N/A |
Kawagoshi 2015.
| Methods | DESIGN 2 groups DATES not reported SETTING (Japan) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 64 (SD 8) years; SEX 16 (83%) male; FEV1 mean 58 (SD 23)% predicted
AGE mean 75 (SD 9) years; SEX 19 (93%) male; FEV1 mean 61 (SD 21)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 months FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION PR SETTING home CONTACT
AEROBIC TRAINING daily, ≥ 15 minutes, level walking
STRENGTH TRAINING upper and lower limbs, daily OTHER COMPONENTS
EDUCATION monthly, 45 minutes: equipment use, nutrition, stress management, relaxation techniques, home exercises, the benefits of pulmonary rehabilitation INTERVENTION PAC INTERFACE monthly (or fortnightly) individual session ACTIVITY not specified STEP‐TRACKING Pedometer Kens Lifecorder EX (no direct feedback) GOALS 8000 steps a day
RECORD, EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE Activity Monitoring and Evaluation System (A‐MES tri‐axial accelerometer) (attached on thigh and chest in clothing pockets)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement provided CONTACT Atsuyoshi Kawagoshi acr00009@med.city.akita.akita.jp Akita City Hospital, Akita (Japan) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The patients were randomly assigned to one of two groups" Comment: Not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Quote: "Patients were not blinded to the randomization" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods |
| Other bias | Low risk | N/A |
Larson 2014.
| Methods | DESIGN 3 groups (2 comparisons)
DATES not reported SETTING (USA) SAMPLE SIZE calculation based on LIPA time |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 71 (SD 8) years; *SEX not reported; FEV1 mean 61 (SD 20)% predicted
AGE mean 72 (SD 9) years; *SEX not reported; FEV1 mean 54 (SD 17)% predicted
AGE mean 71 (SD 8) years; *SEX not reported; FEV1 mean 56 (SD 17)% predicted *"small proportion of women" |
|
| Interventions | DURATION OF INTERVENTION 4 months FOLLOW‐UP 12 months SUPERVISION yes INTERVENTION upper‐body resistance training SETTING outpatient group CONTACT 2 sessions a week, 90 minutes supervised upper‐limb training
AEROBIC TRAINING nil STRENGTH TRAINING cable cross‐over system: shoulder shrug, modified latissimus dorsi pulldown, overhead pulldown, front pulldown, front raise, upright row, biceps curl, triceps extension
INTERVENTION exercise‐specific self‐efficacy intervention general principles of exercise, coping with respiratory infections by modifying PA, overcoming barriers to exercise, establishing an active lifestyle INTERVENTION health education basic lung physiology, pathophysiology of COPD, commonly used medications, breathing techniques, healthy eating, relaxation, travel considerations, energy conservation, osteoarthritis, cardiovascular risk factors, cholesterol INTERVENTION gentle chair exercises stretching and toning exercises that were not aerobic |
|
| Outcomes | DEVICE Actigraph (model 7164) (software version not reported) (waist)
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Janet Larson janetlar@med.umich.edu University of Michigan (USA) Additional information requested. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was stratified by sex and disease severity (GOLD stages) using a customized computer program that blinded investigators to group assignment [software program (biased coin algorithm to ensure equivalent groups)" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "concealed allocation process" Comment: Not specified |
| Blinding of participants (performance bias) | Low risk | "All subjects were assigned to an active intervention without being told which intervention was the experimental intervention of interest. We explained that all three interventions were potentially beneficial and that we were comparing the effects of each" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | PRIMARY OUTCOMES Trial registry: not reported
Paper: physical activity (additional outcome) |
| Other bias | Unclear risk | Retrospectively registered in January 2010; study started September 2003, primary completion January 2009 |
Loeckx 2018.
| Methods | DESIGN 2 groups DATES, SETTING, SAMPLE SIZE not provided (abstract only) |
|
| Participants | INCLUSION CRITERIA "Patients with COPD enrolled in a conventional 6 month OP PRP were screened for eligibility. After 3 months of PR and one week of PA measurements" EXCLUSION CRITERIA not provided (abstract only)
AGE not reported; SEX 25 (50%) male; FEV1 mean 49 (SD 20)% predicted
|
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP 6 months SUPERVISION yes INTERVENTION PAC "Coaching through a semi‐automated telecoaching program consisting of a step counter and a project‐tailored smartphone application" (Demeyer 2017) INTERVENTION PR |
|
| Outcomes | DEVICE not reported (abstract only) ASSESSMENT TIME POINTS
PRIMARY/SECONDARY OUTCOMES
|
|
| Notes | FUNDING, CONFLICT OF INTEREST not provided (abstract only) CONTACT Matthias Loeckx matthias.loeckx@kuleuven.be KU Leuven (Belgium) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information (abstract only) |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information (abstract only) |
| Blinding of participants (performance bias) | Unclear risk | Insufficient information (abstract only) |
| Blinding of personnel (performance bias) | Unclear risk | Insufficient information (abstract only) |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Insufficient information (abstract only) |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Insufficient information (abstract only) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information (abstract only) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information (abstract only) |
| Other bias | Unclear risk | Insufficient information (abstract only) |
Lord 2012.
| Methods | DESIGN 2 groups DATES January 2009 to August 2009 SETTING respiratory clinics (UK) SAMPLE SIZE calculation based on SF36 |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS
AGE mean 69 (SD 11) years; SEX not reported; FEV1 mean 44 (SD 14)% predicted
AGE mean 68 (SD 9) years; SEX not reported; FEV1 mean 64 (SD 26)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION singing
SHAM film workshops
|
|
| Outcomes | DEVICE SenseWear Pro (software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Nicholas Hopkinson n.hopkinson@ic.ac.uk Imperial College, London (UK) Additional information requested |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "At the end of the baseline visit, patients were randomized to either the singing classes or the film workshops, using randomization in blocks of 4…The sequence was developed by NSH who was not involved with the day to day conduct of the trial" |
| Allocation concealment (selection bias) | Low risk | Quote: "consecutive sequentially numbered sealed envelopes" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "The co‐ordinators of each session were unaware of the tests measured at baseline" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: Quote: "Following attendance to either group for eight weeks, baseline measurements were again assessed by the same respiratory physiotherapists, who were blinded to treatment allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOME Registry: daily physical activity Paper: SF36 (not in registry) SECONDARY OUTCOMES Paper: control of breathing, qualitative assessments (additional outcomes reported) |
| Other bias | Unclear risk | Retrospectively registered |
Louvaris 2016.
| Methods | DESIGN 2 groups DATES October 2013 to July 2016 SETTING outpatient PR programme (Greece) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA (as in Nasis 2015)
EXCLUSION CRITERIA (as per Nasis 2015)
BASELINE CHARACTERISTICS
AGE mean 65 (SD 8) years; SEX 68 (80%) male; FEV1 mean 49 (SD 19)% predicted
AGE mean 67 (SD 8) years; SEX 36 (84%) male; FEV1 mean 45 (SD 19)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION exercise training (HIIT) SETTING centre‐based outpatient group CONTACT 3 sessions a week AEROBIC TRAINING cycling 45 minutes, alternating 30‐second exercise intervals with 30‐second rest periods
STRENGTH TRAINING upper and lower limbs
OTHER COMPONENTS nil EDUCATION education programme: breathing retraining, dietary advice |
|
| Outcomes | DEVICE Actigraph GT3X (ActiLife software (version 5.10.0)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Ioannis Vogiatzis gianvog@phed.uoa.gr Zafeiris Louvaris zafeiris.louvaris@kuleuven.be National and Kapodistrian University of Athens (Greece) Additional information provided:
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomised…in random block sizes of three and six." |
| Allocation concealment (selection bias) | Low risk | Quote: "sealed opaque envelopes" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Not specified (research letter only) |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity and exercise capacity (cycle ergometry) |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity (6MWD): Quote: "experienced, health professionals who were blinded to group allocation performed all categories of assessment" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No participant flow diagram (research letter only) Quote: "150 consecutive COPD patients were screened… Patients were randomised in a 2:1 ratio into the interval training group (n=85) or the usual care group (n=43)" Attrition and exclusions not reported. |
| Selective reporting (reporting bias) | High risk | Referral to trial registry is not study‐specific.
PRIMARY OUTCOMES Registry: PROactive tool (not reported) Paper: physical activity variables (daily activity levels amount and intensity, sedentarism, wear time, step count, VMU, time in sedentary, light, lifestyle and moderate activities) SECONDARY OUTCOME Registry: daily physical activity (number of steps, VMU per activity minute, walking intensity) Paper: spirometry, anthropometry, exercise capacity, muscle strength, dyspnoea, HRQOL (CAT, CCQ, CRQ), anxiety and depression (additional outomces reported) |
| Other bias | Unclear risk | Registry: no reference to HIIT protocol |
Maddocks 2016.
| Methods | DESIGN 2 groups DATES Screened between June 2012 and July 2014 SETTING multidisciplinary respiratory and palliative care meetings and across PR services, 3 National Health Service trusts, London, UK SAMPLE SIZE calculation based on 6MWD |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 70 (SD 11) years; SEX 11 (44%) male; FEV1 mean 31 (SD 11)% predicted
AGE mean 69 (SD 9) years; SEX 10 (37% male); FEV1 mean 31 (SD 13)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 weeks FOLLOW‐UP 6 weeks SUPERVISION no COMMMON INTERVENTION neuromuscular electrical stimulation
ADMINISTRATION self‐administered, 30 minutes daily frequency 50Hz, pulse width 350µs, duty cycle 11% to 50% (equivalent to 15% to 25% of maximum voluntary contraction) INSTRUCTION standardised 30 minutes face‐to‐face training, supervise first set‐up in hospital or home (participant preference)
INTERVENTION amplitude 0 to 120mA over 1000O proportion of active treatment duration: increase weekly from 11% to 25% to 50%, then constant PLACEBO amplitude 0 to 20mA "levels of stimulation detectable by the patient but not able to elicit a tetanic muscle contraction" |
|
| Outcomes | DEVICE activPAL (PAL Technologies,Glasgow, UK)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes |
FUNDING "The funder of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. This study was funded by National Institute for Health Research (NIHR; PDF‐2011‐04‐048). This study represents independent research supported by the UK Clinical Research Collaboration‐registered King’s Clinical Trials Unit at King’s Health Partners, and the NIHR/Wellcome Trust King’s Clinical Research Facility, which are part funded by the NIHR Biomedical Research Centre for Mental Health and the Dementia Unit at South London and Maudsley NHS Foundation Trust, King’s College London and the NIHR Evaluation, Trials and Studies Coordinating Centre. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health … MM is supported by an NIHR Post‐Doctoral Fellowship (PDF‐2011‐04‐048) and Clinical Trials Fellowship (CTF‐2013‐02‐009). CMN is supported by an NIHR Doctoral Fellowship (DRF‐2014‐07‐089). WD‐CM is supported by an NIHR Clinician Scientist Award, a Medical Research Council (UK) New Investigator Research Grant, an NIHR Clinical Trials Fellowship and by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Northwest London. MIP is supported by the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. IJH is an NIHR Senior Investigator and is supported by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for South London and Cicely Saunders International." CONFLICT OF INTEREST "MIP reports receiving personal or institutional payment for consultancy or for research from GlaxoSmithKline, Novartis, Lilly, Pfizer, AstraZeneca, Regeneron, and Biomarin. MM, CMN, WD‐CM, NH, and IJH report holding grants from the National Institute for Health Research during the conduct of the trial. All other authors declare no competing interests." CONTACT Matthew Maddocks matthew.maddocks@kcl.ac.uk Kings College, London (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Participants were randomly assigned (1:1) at the individual level, using an independent web‐based randomisation system within the independent UK Clinical Research Collaboration‐registered King’s Clinical Trials Unit (London, UK). Using a hybrid minimisation method, 20% of participants were entered using simple randomisation and 80% entered using computer‐generated probabilistic minimisation to balance three potential confounders" |
| Allocation concealment (selection bias) | Low risk | Quote: "Following randomisation to active or placebo NMES, the Clinical Trials Unit informed trial staff via secure email. The trial coordinator, who arranged subsequent masked assessment visits, was informed of trial entry but not group allocation" |
| Blinding of participants (performance bias) | Low risk | Quote: "Participants were not informed of group allocation" |
| Blinding of personnel (performance bias) | High risk | Quote: "Trial physiotherapists and nurses were informed of group allocation and selected an active or placebo NMES device accordingly" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Quote: "Two linked Good Clinical Practice compliant online data entry systems (InferMed, London, UK; MACRO version 4) were created to maintain blinding; the first was used by physiotherapists and nurses for data regarding compliance and safety, and the second was used by trial assessors for outcome data" "trial coordinator (masked to group allocation) undertook physical assessments; questionnaires were self‐completed independently by participants" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Low risk | Paper additionally reports 4‐metre gait speed and adverse events |
| Other bias | Unclear risk | Retrospectively registered Quote: "One participant from each group commenced pulmonary rehabilitation classes during the follow‐up period, with three cumulative attendances between the 6‐week and 12‐week assessments in the active group and two in the placebo group." |
Magnussen 2017.
| Methods | DESIGN cross‐over trial (only pre‐cross‐over data used), 2 groups DATES April 2014 to June 2015 SETTING 2 centres (Germany) SAMPLE SIZE "As this was a pilot study, no formal sample size calculation was performed" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
·MEDICATIONS
BASELINE CHARACTERISTICS
AGE mean 64 (SD 7) years; SEX 8 (53%) male; FEV1 median 1.4 (IQR 1.3 to 2.0) litres
AGE mean 65 (SD 8) years; SEX 7 (47%) male; FEV1 median 1.4 (IQR 0.9 to 1.8) litres |
|
| Interventions | DURATION OF INTERVENTION 3 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION LAMA (aclidinium bromide, 400 μg) twice daily (09:00, 21:00 ± 1 hour) with a dry‐powder inhaler (Genuair®/Pressair®) PLACEBO twice daily (09:00, 21:00 ± 1 hour) via a dry‐powder inhaler (Genuair®/Pressair®) |
|
| Outcomes | DEVICE SenseWear Pro3 (software version not reported)
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING "Support statement: This study was sponsored by Almirall S.A., Barcelona, Spain. Almirall S.A. were involved in the study design, collection, analysis, interpretation of data and development of this manuscript. Almirall S.A. and AstraZeneca Plc were involved in the review of the manuscript; the decision to submit the manuscript for publication was made jointly by the funders and authors. Funding information for this article has been deposited with the Crossref Funder Registry." CONFLICT OF INTEREST "Principal Investigators are NOT employed by the organization sponsoring the study. There IS an agreement between the Principal Investigator and the Sponsor (or its agents) that restricts the PI's rights to discuss or publish trial results after the trial is completed. Publication of the results by the Investigator will be subject to mutual agreement between the investigator and sponsor." (registry) CONTACT Henrik Watz H.Watz@pulmoresearch.de German Center for Lung Research, Grosshansdorf (Germany) Additional data provided: as in Almirall |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomized" Comment: insufficient information (research letter only) |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | Low risk | Quote: "Masking: Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor)" |
| Blinding of personnel (performance bias) | Low risk | Quote: "Masking: Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL: Quote: "Masking: Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor)" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No participant flow diagram (research letter only) |
| Selective reporting (reporting bias) | Low risk | Results presented as in registry |
| Other bias | Low risk | Quote: "per‐protocol population (all patients in the safety population who had no major protocol deviations)" |
Mantoani 2018.
| Methods | DESIGN 2 groups DATES February 2015 to March 2017 SETTING Community Treatment Centre and hospitals (UK) SAMPLE SIZE calculation based on "physical activity levels" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS (total n = 44) AGE mean 69 (SD 11) years; SEX 22 (50%) male; FEV1 mean 54 (SD 19)% predicted
|
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION PR DURATION 6 to 10 weeks SETTING outpatient group CONTACT 1 to 2 sessions a week, one hour AEROBIC TRAINING treadmill, cycle ergometer
STRENGTH TRAINING upper and lower limbs OTHER COMPONENTS, EDUCATION nil INTERVENTION PAC (web‐based human coaching) DURATION 12 weeks INTERFACE website ACTIVITY not specified STEP‐TRACKING Activity monitor (Tracmor D): (direct feedback, daily target) RECORD nil GOALS
EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE
ASSESSMENT TIME POINTS
PRIMARY
SECONDARY
|
|
| Notes | FUNDING "Sponsor: University of Edinburgh. Collaborator: Philips Healthcare" CONFLICT OF INTEREST not reported (abstract only) CONTACT not reported (abstract only) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomized controlled trial" Comment: Insufficient information (abstract only) |
| Allocation concealment (selection bias) | Unclear risk | Not specified (abstract only) |
| Blinding of participants (performance bias) | High risk | Quote: "None (Open Label)" |
| Blinding of personnel (performance bias) | High risk | Quote: "None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity: Quote: "None (Open Label)" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not specified (abstract only) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information (abstract only) |
| Other bias | Unclear risk |
|
Mendoza 2015.
| Methods | DESIGN 2 groups DATES January 2011 to April 2013 SETTING outpatient clinics at private and public hospitals, private clinics, public primary health centres (Chile) SAMPLE SIZE calculation based on step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 69 (SD 10) years; SEX 29 (56%) male; FEV1 mean 66 (SD 18)% predicted
AGE mean 68 (SD 8) years; SEX 33 (66%) male; FEV1 mean 66 (SD 21)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION PAC (in‐person) INTERFACE monthly individual session ACTIVITY walking RECORD diary: daily symptoms GOALS walk ≥ 30 minutes a day STEP‐TRACKING, EDUCATION/RESOURCES nil INTERVENTION pedometer INTERFACE monthly individual session ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD diary: daily step count, symptoms GOALS protocol‐driven (revised weekly)
EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE Tanita PD724 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Laura Mendoza lmendoza08@gmail.com Hospital Clínico Universidad de Chile, Santiago (Chile) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The study was a parallel group, assessor‐blind, randomised controlled trial… Consecutive patients who consented to participate were randomly assigned to one of two groups…by the investigators based on a random number sequence generated in Excel (Microsoft, Redmond, WA, USA) before enrolment commenced" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "assessor‐blind…Assessments were performed by investigators blinded to treatment allocation…All assessments were made by technicians of the pulmonary function laboratory at Hospital Clínico Universidad de Chile, who were blinded to the allocation of the patients" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | Paper: anthropometrics, spirometry, dyspnoea, using data from the participant diaries, the incidence of (AECOPD)…was determined (additional outcomes reported) |
| Other bias | Low risk | N/A |
Mitchell 2013.
| Methods | DESIGN 2 groups DATES December 2009 to April 2012 SETTING 30 primary care COPD registers (UK) SAMPLE SIZE calculation based on CRQ dyspnoea domain |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 69 (SD 8) years; SEX 54 (61%) male; FEV1 mean 56 (SD 17)% predicted
AGE mean 69 (SD 10) years; SEX 47 (50%) male; FEV1 mean 60 (SD 17)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 weeks FOLLOW‐UP 6 months SUPERVISION no INTERVENTION self‐management (SPACE) (as in Kanabar 2015)
NO INTERVENTION Managed within primary care, no PR during the study period |
|
| Outcomes | DEVICE SenseWear armband (software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Sally Singh sally.singh@uhl‐tr.nhs.uk University Hospitals Of Leicester NHS Trust, Leicester (UK) Additional data provided: group numbers |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Participants were assigned to either usual care or SPACE FOR COPD via a web‐based, concealed allocation programme, using simple randomisation codes prepared by the trial statistician" |
| Allocation concealment (selection bias) | Low risk | Quote: "concealed allocation programme" |
| Blinding of participants (performance bias) | High risk | Quote: "Lack of participant blinding may have increased motivation when receiving the treatment and attempts to satisfy the researchers might have increased the observed treatment effect in the intervention arm. We cannot, therefore, rule out the possible impact of attention" |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "Randomisation was conducted by the trial investigator responsible for administering the intervention" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "assessments at 6 weeks and 6 months were conducted by a member of the research team who was blind to randomisation allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | CONSORT diagram provided for all study participants but subgroup with physical activity data unclear |
| Selective reporting (reporting bias) | Unclear risk | SECONDARY OUTCOMES Registry: task completion, adherence, exacerbation rates (not reported) |
| Other bias | Unclear risk |
|
Moy 2015a.
| Methods | DESIGN 2 groups DATES December 2011 to January 2013 SETTING Veterans identified from a national database (USA, Puerto Rico) SAMPLE SIZE calculation based on SGRQ |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 67 (SD 9) years; SEX 146 (95%) male; FEV1 not assessed
AGE mean 66 (SD 9) years; SEX 77 (92%) male; FEV1 not assessed |
|
| Interventions | DURATION OF INTERVENTION 12 months FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION pedometer No instructions about exercise INTERFACE website ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD website: step count at least monthly GOALS, EDUCATION/RESOURCES nil INTERVENTION PAC (web‐based, as in Wan 2017) DURATION initial intensive 4‐month phase followed by an 8‐month maintenance phase INTERFACE website ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD website: step count at least weekly GOALS Website: display progress, protocol‐driven goal (revised weekly) EDUCATION/RESOURCES website: education and motivational content, community forum |
|
| Outcomes | DEVICE Omron HJ‐720 ITC (pedometer)
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Caroline Richardson caroli@umich.edu University of Michigan (USA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A random sample of 28,957 veterans (one‐half urban, one‐half rural) were sent a recruitment letter… Group assignment was computer generated" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to intervention. |
| Blinding of personnel (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL: Quote: "Masking: None (Open Label)" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | Paper: adherence, engagement, safety, dyspnoea (Methods: baseline, month 4, month 12; Results: baseline) (additional outcomes reported) |
| Other bias | Unclear risk |
|
Nakamura 2016.
| Methods | DESIGN 2 groups DATES not reported (abstract only) SETTING multicentre (Japan) SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS not reported
|
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION LAMA (aclidinium bromide, 400 μg) twice daily INTERVENTION LAMA (tiotropium, 18 μg) once daily |
|
| Outcomes | DEVICE GT3X‐BT (software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was funded by Kyorin Pharmaceutical Co., Ltd. (UMIN000020020)" CONFLICT OF INTEREST not reported (abstract only) CONTACT not provided |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomized" Comment: Insufficient information (abstract only) |
| Allocation concealment (selection bias) | Unclear risk | Not specified (abstract only) |
| Blinding of participants (performance bias) | High risk | Quote: "open‐label" |
| Blinding of personnel (performance bias) | High risk | Quote: "open‐label" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL: Quote: "open‐label" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Appears that all randomised participants completed the study |
| Selective reporting (reporting bias) | High risk | No registry available; abstract only No data presented that can be used for analysis; only between‐group P‐values provided |
| Other bias | Unclear risk | Abstract only |
NCT00144326.
| Methods | DESIGN 2 groups, phase 3 DATES September 2003 to October 2005 SETTING Canada, Germany, Spain SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS not reported
|
|
| Interventions | DURATION OF INTERVENTION AND FOLLOW‐UP 12 weeks SUPERVISION no INTERVENTION LAMA (tiotropium bromide, 18 mcg) oral inhalation capsules, once daily in the morning with HandiHaler PLACEBO oral inhalation capsules, once daily in the morning with HandiHaler |
|
| Outcomes | DEVICE Stayhealthy RT3 accelerometer
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING Boehringer Ingelheim CONFLICT OF INTEREST not stated CONTACT not stated |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | Unclear risk | Quote: "Double blind" Comment: unclear to whom this refers |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "Double blind" Comment: unclear to whom this refers |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Objectively assessed physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Quote: "Double blind" Comment: unclear to whom this refers |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No participant flow chart |
| Selective reporting (reporting bias) | Unclear risk | No data presented suitable for meta‐analysis |
| Other bias | Unclear risk | No participant features reported Not published in peer‐reviewed journal |
NCT01351792.
| Methods | DESIGN 2 groups DATES September 2011 to November 2012 SETTING 7 centres (The Netherlands) SAMPLE SIZE not reported |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS not reported
|
|
| Interventions | DURATION OF INTERVENTION 4‐week run‐in phase, 12 week intervention FOLLOW‐UP no SUPERVISION no COMMON RUN‐IN PHASE 4 weeks, Symbicort (200/6 µg/unit dose) 1 inhalation twice a day INTERVENTION Foster (beclomethasone dipropionate 100 µg plus formoterol 6 µg/unit dose), 2 inhalations twice a day INTERVENTION Symbicort (budesonide 200 μg plus formoterol fumarate 6 μg/actuation) |
|
| Outcomes | DEVICE pedometer ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOME
|
|
| Notes | FUNDING Chiesi Farmaceutici Parma (Italy) CONFLICT OF INTEREST CONTACT Chiesi Farmaceutici clinicaltrials_info@chiesi.com Eddi Bindi E.Bindi@chiesigroup.com Gabriele Nicolini g.nicolini@chiesigroup.com Marteen van den Berge m.van.den.berge@umcg.nl |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: “randomised” Comment: insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | Low risk | Quadruple (participant, care provider, investigator, outcomes assessor) (NCT) |
| Blinding of personnel (performance bias) | Low risk | Quadruple (participant, care provider, investigator, outcomes assessor) (NCT) |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Quadruple (participant, care provider, investigator, outcomes assessor) (NCT) |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Quadruple (participant, care provider, investigator, outcomes assessor) (NCT) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | EUCTR: target size n = 170 NCT: target size n = 130, actual recruitment n = 113 Study report: randomised Foster n = 31, symbicort n = 29 |
| Selective reporting (reporting bias) | High risk | Results not published in peer‐reviewed journal; only data available are from study report |
| Other bias | Unclear risk | Prospectively registered Quote: “prematurely ended; low number of evaluable patients (which was less than half of the planned number)” |
Ng 2015.
| Methods | DESIGN cross‐over trial (only pre‐cross‐over data used), 2 groups DATES not reported (abstract only) SETTING PR (country?) SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS (total n = 19) AGE mean 72 (SD 8) years; SEX 11 (58%) males; FEV1 mean 38 (SD 19)% predicted
|
|
| Interventions | DURATION OF INTERVENTION AND FOLLOW‐UP 4 weeks (only pre‐cross‐over data) FOLLOW‐UP no SUPERVISION no INTERVENTION four‐wheeled walker |
|
| Outcomes | DEVICE StepWatch
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Kylie Hill k.hill@curtin.edu.au Cindy Ng cindy.ng.l.w@sgh.com.sg Curtin University, Perth (Australia) Additional information provided: CRQ, physical activity pre‐cross‐over data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly allocated" Comment: Insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not specified
|
| Selective reporting (reporting bias) | Unclear risk | ActivPAL results provided in author correspondence but not presented otherwise |
| Other bias | Unclear risk | No baseline assessment |
Nguyen 2009.
| Methods | DESIGN 2 groups DATES October 2006 to April 2008 SETTING PR programmes SAMPLE SIZE feasibility study; no power calculation |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 72 (SD 9) years; SEX 3 (33%) male; FEV1 mean 47 (SD 19)% predicted
AGE mean 64 (SD 12) years; SEX 3 (38%) male; FEV1 mean 34 (SD 15)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (coached, app) INTERFACE
ACTIVITY Individual home exercise programme (as in exercise test performance, dyspnoea, community‐based facilities, preferred mode) STEP‐TRACKING pedometer (direct feedback) RECORD daily symptoms and exercise log via phone, transmitted real‐time to central server GOALS
EDUCATION/RESOURCES
INTERVENTION PAC (self‐managed, app) INTERFACE
ACTIVITY individual home exercise programme (as in exercise test performance, dyspnoea, community‐based facilities, preferred mode) STEP‐TRACKING pedometer (direct feedback) RECORD daily symptoms and exercise log by phone GOALS
EDUCATION/RESOURCES
|
|
| Outcomes | DEVICE Stepwatch 3 (right ankle)
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING reported "Omron Healthcare donated the pedometers" CONFLICT OF INTEREST statement provided CONTACT Huong Nguyen HQN@u.washington.edu University of Washington, Seattle (USA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A biostatistician who was not involved in the day‐to‐day study operations generated the randomization sequence" |
| Allocation concealment (selection bias) | Low risk | Quote: "A biostatistician who was not involved in the day‐to‐day study operations…placed the randomization in separate sealed opaque envelopes" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "the interventionist was not blind to group assignment" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity and exercise capacity (cycle ergometry) |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity (6MWD): Quote: "the outcome assessments were performed by a research assistant who was blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOME Registry: exercise behaviour (not defined) Paper: autonomous self‐regulation for exercise (additional outcome) SECONDARY OUTCOMES Registry: AECOPD (not reported) Paper: technical issues, beliefs and attitudes towards exercise and self care, validation of self‐reported exercise, intervention time and costs (additional outcomes) |
| Other bias | High risk |
|
Nolan 2017.
| Methods | DESIGN 2 groups DATES July 2012 to June 2014 SETTING hospital PR unit (UK) SAMPLE SIZE calculation based on time in moderate‐intensity physical activity |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 68 (SD 9) years; SEX 56 (74%) male; FEV1 mean 51 (SD 21)% predicted
AGE mean 68 (SD 8) years; SEX 54 (71%) male; FEV1 mean 51 (SD 22)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION no INTERVENTION PR DURATION 8 weeks SETTING outpatient group CONTACT 2 sessions a week (15 minutes warm‐up, 60 minutes exercise, 45 minutes education) AEROBIC TRAINING walking, aim 15 minutes continuously, Borg scale dyspnoea (rating 3 to 4)
STRENGTH TRAINING upper and lower limbs (2 sets, 10 repetitions)
OTHER COMPONENTS at least once a week, home‐based exercise session EDUCATION
INTERVENTION PAC (in‐person) INTERFACE 8 individual sessions (weekly during PR) ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD diary: daily step count GOALS
EDUCATION/RESOURCES nil |
|
| Outcomes | DEVICE SenseWear (Software version not reported) and Yamax DigiWalker CW700 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTERESTstatement provided CONTACT Claire Nolan c.nolan15@imperial.ac.uk Imperial College, London (UK) Additional information provided: confirmed distribution of variables precluding inclusion in meta‐analysis |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "parallel, two‐group, assessor‐blinded randomized controlled trial… following baseline assessment, participants were randomly allocated 1:1 to… the allocation sequence was computer generated and accessed by a researcher independent of (study processes)" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Quote: "It was not possible to conceal group allocation from participants" |
| Blinding of personnel (performance bias) | Low risk | Quote: "The clinical team delivering the PR program were blinded to the participants' group allocation" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "assessors blinded to group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | SECONDARY OUTCOMES
Registry: SF36 (not reported) Paper: accelerometer and pedometer step counts, adverse events, hospitalisations and deaths (additional outcomes) |
| Other bias | Low risk | N/A |
O'Neill 2018.
| Methods | DESIGN 2 groups DATES February 2014 to January 2016 SETTING PR within 2 Health and Social Care Trusts (Northern Ireland) SAMPLE SIZE "this study will inform a future large scale RCT" |
|
| Participants | INCLUSION CRITERIA (registry)
EXCLUSION CRITERIA (registry)
BASELINE CHARACTERISTICS
AGE mean 61 (SD 9); SEX 13 (57%) male; FEV1 mean 54 (SD 23)% predicted
AGE mean 67 (SD 8); SEX 11 (42%) male; FEV1 mean 57 (SD 24)% predicted |
|
| Interventions | DURATION OF INTERVENTION PAC 12 weeks, PR 6 weeks FOLLOW‐UP no SUPERVISION yes COMMON INTERVENTION participants given the Living Well With COPD for PR booklet INTERVENTION physical activity intervention DURATION 12 weeks INTERFACE weekly contact with the physiotherapist or nurse
ACTIVITY walking STEP‐TRACKING unsealed Yamax Digiwalker CW700 pedometers each day for motivation and feedback RECORD manual with weekly step diary GOALS COM‐B model of behaviour change (capability, opportunity, motivation, behaviour)
EDUCATION/RESOURCES during consultations clinicians focused on helping participants to build self‐efficacy, encouraging social support, providing disease‐specific education INTERVENTION pulmonary rehabilitation DURATION 6 weeks SETTING hospital or health‐centre outpatient departments CONTACT 2 x week, also given a booklet with exercises and encouraged to perform these independently on a third occasion AEROBIC TRAINING exercise component usually lasted for 1 hour, generally consisted of cardiovascular exercises STRENGTH TRAINING lower‐ and upper‐body strengthening exercises OTHER COMPONENTS A diary was used to record the exercises undertaken and the level of breathlessness measured with the BORG scale EDUCATION centre‐based disease‐specific education, at which time participants could engage in discussion and ask questions at least once weekly (30 – 60 minutes) |
|
| Outcomes | DEVICE ActigraphVR GT3X accelerometer, sealed Yamax Digiwalker CW700 pedometer worn around the waist for 7 days during all waking hours Only Actigraph data that contained a minimum of 5 days of 10 hours wear‐time were used for analysis Only sealed pedometer data that had a minimum of 5 days of 100 – 50,000 steps were used for analysis ASSESSMENT TIME POINTS 4 study visits for outcome assessment
PRIMARY OUTCOME / SECONDARY OUTCOMES
|
|
| Notes | FUNDING "The study was funded by the Northern Ireland Chest Heart and Stroke (NICHS). PhD student (O’Shea O) was funded by the Department of Employment and Learning. The study was sponsored by the Ulster University and the Western and Belfast Health and Social Care Trusts. The study was supported by the Northern Ireland Clinical Research Network (NICRN) Respiratory Health interest group." CONFLICT OF INTEREST "The authors have no conflicts of interest to declare." CONTACT Brenda O'Neill b.oneill@ulster.ac.uk Ulster University, Newtownabbey (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Participants were randomly assigned to two groups using computer‐generated block random numbers by a member of team not involved in any other aspect of the study in order to ensure allocation concealment" |
| Allocation concealment (selection bias) | Low risk | Quote: "The allocation was retained in sealed envelopes which were opened to reveal group allocation only after consent and after the completion of baseline assessment" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to intervention |
| Blinding of personnel (performance bias) | Unclear risk | Insufficient information |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Quote: "All data was collected by a trained independent assessor not involved in the delivery of either intervention; a physiotherapist and/or a research assistant" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Participants’ flow through the study is shown in Figure 1. Quote: "The patients were assessed and randomised to the PAI (n = 24) or PR (n = 26). One participant who was randomised to the PAI made a mistake and attended PR. Therefore, n = 27 attended PR and n = 23 attended the PAI. A further n = 1 participant randomised to PR was excluded from the analysis as subsequent information about their diagnosis revealed that the person did not meet the GOLD criteria for COPD; therefore, n = 49 have been included in the analysis: n = 23 PAI; n = 26 PR." |
| Selective reporting (reporting bias) | Unclear risk | Results reported as in Methods, apart from time points for assessment where follow‐up data not presented |
| Other bias | Unclear risk | Retrospectively registered |
Ogasawara 2018.
| Methods | DESIGN 2 groups DATES November 2014 to October 2017 SETTING single centre (Japan) SAMPLE SIZE calculation based on lean body mass index |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 77 (SD 10) years; SEX 21 (88%) male; FEV1 mean 64 (SD 25)% predicted
AGE mean 79 (7) years; SEX 20 (95%) male; FEV1 mean 68 (SD 35)% predicted |
|
| Interventions | DURATION OF INTERVENTION hospital length of stay FOLLOW‐UP no SUPERVISION yes COMMON INTERVENTION
INTERVENTION nutritional supplement with eicosapentaenoic acid (ProSure) 1 pack or can a day INTERVENTION nutritional supplement without eicosapentaenoic acid (ENSURE®) 1 pack or can a day |
|
| Outcomes | DEVICE pedometer (HJA‐401F, Omron) step length measured as 0.37 * height (cm) (input for device)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors" CONFLICT OF INTEREST "None of the authors declared a conflict of interest" CONTACT Takashi Ogasawara shikatarawasagao@gmail.com Hamamatsu Medical Centre, Shizuoka (Japan) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed using a computer‐generated randomization scheme with blocks of four" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | High risk | Quote: "open‐label" |
| Blinding of personnel (performance bias) | High risk | Quote: "open‐label" |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Quote: "open‐label" |
| Blinding of outcome assessment [other] (detection bias) | High risk | Quote: "open‐label" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT figure provided Quote: "In total, 50 eligible patients were enrolled in the study and evaluated prospectively (Fig. 1). One patient in the EPA group was excluded, because his body weight at the time of admission was erroneously input to the BIA, resulting in the BMI and LBMI being characterized as overweight. Three patients in the control group were also excluded because they could not continue taking ONS orally due to dysphagia or intubation, and one patient withdrew informed consent" |
| Selective reporting (reporting bias) | Low risk | Registry and paper in agreement |
| Other bias | Unclear risk | Prospectively registered Unable to access supplementary data: Quote: "Data not available / The authors do not have permission to share data" |
Orme 2018.
| Methods | DESIGN 3 groups (3 comparisons)
DATES February to June 2016 SETTING hospital (UK) SAMPLE SIZE "The study will aim to recruit as many patients as are admitted to hospital for an acute COPD exacerbation within the operational period. One of the main objectives of this feasibility study is to provide data on eligibility and recruitment and to enable an accurate estimation of the required sample size for a future trial based on a realistic recruitment plan." |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS AGE mean 71 (SD 20) years; SEX 10 (30%) male; FEV1 not reported
|
|
| Interventions | DURATION OF INTERVENTION 2 weeks following discharge from hospital FOLLOW‐UP no SUPERVISION no INTERVENTION feedback INTERFACE
ACTIVITY break up sedentary bouts STEP‐TRACKING inclinometer (direct haptic feedback: sedentary time > threshold) RECORD inclinometer sends data to app GOALS app: step count, sitting, standing, lying down, sit‐to‐stand transitions INTERVENTION education EDUCATION/RESOURCES verbal and written information: booklet Sit Less, Move More, Live Healthier adapted for COPD |
|
| Outcomes | DEVICE ActiGraph wGT3X‐BT (version 6.13.2; firmware 1.6.1) (waistband on the right anterior axillary line)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Mark Orme mark.orme@uhl‐tr.nhs.uk University Hospitals Of Leicester NHS Trust, Leicester (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Block randomization was conducted... by an individual independent of the research team" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "sequentially numbered sealed envelopes ... balanced combinations of group allocations within blocks will be conducted by a researcher at Loughborough University who is independent of the research team. This will ensure study team researchers will be blinded to group allocation prior to patients deciding whether to take part in the study. Owing to limited study team members and logistical barriers, study team researchers will be made aware of group allocation before consent. Patients will only be informed of their group allocation after providing informed consent" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL: Quote: "researchers will not be blinded to treatment allocation for qualitative interviews and study measurements" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | Registry: 20 metre gait analysis using foot‐worn inertial sensors (not reported) Registry and protocol: EQ5D, grip strength (not reported) Protocol:
Paper: PR attendance, information on the ownership and usage of computers and smartphones, index of multiple deprivation (additional outcomes reported) |
| Other bias | High risk | No physical activity data available per group Registry: changes made on 31 May 2016 (following completion of recruitment)
|
Polkey 2018.
| Methods | DESIGN 2 groups DATES December 2015 to August 2016 SETTING hospital (China) SAMPLE SIZE "In the absence of pilot data, a formal power calculation was not possible" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE, SEX not reported; FEV1 post‐bronchodilator mean 49 (SD 13)% predicted
AGE, SEX not reported; FEV1 post‐bronchodilator mean 47 (SD 15)% predicted |
|
| Interventions | DURATION OF INTERVENTION 2 weeks indacaterol, 12 weeks indacaterol and intervention FOLLOW‐UP 12 weeks indacaterol SUPERVISION yes INTERVENTION Tai Chi DURATION 12 weeks SETTING "big exercise hall" CONTACT 5 sessions a week, 1 hour TRAINING Yang style
OTHER COMPONENTS LABA (indacaterol, 150 ug per day) EDUCATION "educational input" INTERVENTION PR DURATION 12 weeks SETTING supervised, outpatient, group CONTACT 3 sessions a week, 1 hour AEROBIC TRAINING 50%
STRENGTH TRAINING 50% shoulder abduction, bicep curls, sit to stand, lunge walks with dumbbells
OTHER COMPONENTS LABA (indacaterol, 150 ug per day) EDUCATION "educational sessions" |
|
| Outcomes | DEVICE ActiGraph
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES (visits 2, 3, 6, 9)
|
|
| Notes |
FUNDING "The study was in part funded by Novartis China as an investigator‐initiated trial; the State Key Laboratory of Respiratory Disease (Guangzhou Medical University) was the sponsor. The study drug (indacaterol) was provided by Novartis China. Both the Key State Laboratory (Guangzhou) and the NIHR Respiratory Biomedical Unit provided in‐kind support, the latter through partial salary support of M. I. P. Space for the study was made available by the governors of Xing‐Ning People’s Hospital. Y.M. L. was also partially supported by the National Key Research and Development Program of China (Project No. 2016YFC1304200)." CONFLICT OF INTEREST "Financial/nonfinancial disclosures: None declared. Role of sponsors: Novartis China had no role in writing the manuscript or the decision to publish." CONTACT Yuan‐Ming Luo y.m.luo@vip.163.com State Key Laboratory of Respiratory Disease, Guangzhou (China) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Allocation: Randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to exercise intervention |
| Blinding of personnel (performance bias) | High risk | Quote: "None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity: Quote: "None (Open Label)" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOME Registry: only specified primary outcomes
Paper: SGRQ at Visits 2, 3, 6, 9 SECONDARY OUTCOMES not specified in registry Paper:
|
| Other bias | Unclear risk |
|
Priori 2017.
| Methods | DESIGN 2 groups DATES, SETTING, SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION/EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS (n = 21)
AGE mean 70 (SD 8) years; SEX not reported; FEV1 mean 44 (SD 14)% predicted
AGE mean 68 (SD 5) years; SEX not reported; FEV1 mean 43 (SD 12)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (automated coaching) INTERFACE automated coaching messages GOALS "weekly goals, daily feedback" ACTIVITY, STEP‐TRACKING, RECORD, EDUCATION/RESOURCES nil NO INTERVENTION"blinded to their physical activity" |
|
| Outcomes | DEVICE DirectLife (activity monitor)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING, CONFLICT OF INTEREST not reported (abstract only) 7 co‐authors on this abstract are employed by Philips (as in Saini abstract) also no disclaimer re Philips (funded as in Saini abstract?) CONTACT Rita Priori rita.priori@philips.com Phillips (The Netherlands) Additional information provided: confirmed this is a stand‐alone study |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomized" Comment: Insufficient information (abstract only) |
| Allocation concealment (selection bias) | Unclear risk | Not specified (abstract only) |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified (abstract only) |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: unclear if participant reported |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "21 patients were recruited… Ten IG… and 8 CG…patients completed the study" Comment: Insufficient information (abstract only) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information (abstract only) |
| Other bias | Unclear risk | Abstract only |
Probst 2011.
| Methods | DESIGN 2 groups DATES July 2006 to July 2009 SETTING University Hospital, Universidade Estadual de Londrina, Londrina, Parana (Brazil) SAMPLE SIZE post hoc power calculation… time spent in activities of intensity > 3 METs |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
MEDICATIONS "Pharmacologic treatment was not changed during the course of the study" BASELINE CHARACTERISTICS (n = 63)
AGE mean 65 (SD 10) years; SEX 11 (58%) male; FEV1 mean 39 (SD 14)% predicted
AGE mean 67 (SD 7) years; SEX 10 (50%) male; FEV1 mean 40 (SD 13)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION exercise training (calisthenics and breathing exercises) DURATION 12 weeks SETTING outpatient group CONTACT 3 sessions a week, 1 hour STRENGTH TRAINING
AEROBIC TRAINING, OTHER COMPONENTS, EDUCATION nil INTERVENTION exercise training (endurance and strength training) DURATION 12 weeks SETTING outpatient group CONTACT 3 sessions a week, 1 hour AEROBIC TRAINING
STRENGTH TRAINING quadriceps, biceps, triceps
OTHER COMPONENTS, EDUCATION nil |
|
| Outcomes | DEVICE DynaPort Activity Monitor (waist): time walking, standing, sitting, and lying SenseWear (upper‐posterior region of the right arm): step count, MVPA time, energy expenditure
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Fabio Pitta fabiopitta@uol.com.br Universidade Estadual de Londrina, Parana (Brazil) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomized trial" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | Unclear risk | Not specified |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity and exercise capacity (cycle ergometry) |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity (6MWD): not specified |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No participant flow diagram Group numbers prior to dropout not stated |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods (other than results for respiratory muscle force after intervention) |
| Other bias | Unclear risk | Post hoc power calculation identified in study limitations in Discussion |
Rinaldo 2017.
| Methods | DESIGN 2 groups DATES January 2013 to January 2014, followed up until November 2014 SETTING Fitness Centre of the Exercise and Sport Science School of Verona University (Italy) SAMPLE SIZE calculation based on 6MWD |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA Unstable cardiac disease, pneumonia, pulmonary embolism, pulmonary vascular disease, respiratory infections, lung cancer, thoracic malignancy, and bone fractures BASELINE CHARACTERISTICS
AGE mean 66 (SD 5) years; SEX 100% male; FEV1 mean 72 (SD 19)% predicted
AGE mean 66 (SD 4) years; SEX 100% male; FEV1 mean 60 (SD 24)% predicted |
|
| Interventions | DURATION OF INTERVENTION 28 weeks FOLLOW‐UP 14 weeks SUPERVISION no INTERVENTION exercise training with tapered supervision physical activity education programme approach, based on a periodically supervised protocol of different exercise modalities DURATION 28 weeks SETTING outpatient group CONTACT 60 minutes
AEROBIC/STRENGTH TRAINING
OTHER COMPONENTS nil EDUCATION "Participants also received brochures with information about the local physical activity facilities" INTERVENTION supervised exercise training training protocol was in line with published recommendations "The participants self‐monitored the intensity and duration of endurance and resistance exercises to avoid exertional dyspnoea" DURATION 28 weeks SETTING outpatient group CONTACT 3 times a week, 1 hour AEROBIC TRAINING cycling, treadmill walking or upper limb ergometer
STRENGTH TRAINING upper limb, lower limb, trunk; 4 sets
OTHER COMPONENTS flexibility and balance exercises EDUCATION "All participants were instructed to continue with their prescribed exercise program during the 14‐week follow‐up period." |
|
| Outcomes | DEVICE SenseWear (software version not reported)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "The authors received no financial support." CONFLICT OF INTEREST "The authors have no conflict to declare." CONTACT Giuseppe Coratella giuseppe.coratella@univr.it University of Verona (Italy) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a restricted block (size = 4) randomization, generated by free online software (www.randomization.com) was used to allocate the participants within the 2 groups" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "allocation and randomization were completed by one of the researchers without any contact or knowledge of the participants…. Thus, no allocation concealment mechanisms were necessary" |
| Blinding of participants (performance bias) | Unclear risk | Not specified |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Low risk | No trial registry; results presented as in Methods |
| Other bias | Unclear risk | only male participants |
Saini 2017.
| Methods | DATES, SETTING, SAMPLE SIZE not reported (abstract only) | |
| Participants | INCLUSION CRITERIA COPD patients
EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS (TOTAL n = 28) AGE mean 64 (SD 7) years; SEX 15 (54%) males; FEV1 not reported |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION online physical activity coaching system designed to support maintenance of physical activity at home after PR NO INTERVENTION |
|
| Outcomes | DEVICE Philips DirectLife activity monitor
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOME
|
|
| Notes | FUNDING This abstract is funded by Philips CONFLICT OF INTEREST None stated CONTACT Privender Saini privender.saini@philips.com Phillips (The Netherlands) NB. Abstract states that this study is ongoing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | Unclear risk | Insufficient information |
| Blinding of personnel (performance bias) | Unclear risk | Insufficient information |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Insufficient information |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Insufficient information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information |
| Other bias | Unclear risk | This abstract is funded by Philips |
Sandland 2008.
| Methods | DESIGN 2 groups DATES not reported SETTING hospital PR department (UK) SAMPLE SIZE calculation based on arbitrary activity counts |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS
AGE mean 71 (SD 4) years; SEX 6 (60%) male; FEV1 mean 43 (SD 16)% predicted
AGE mean 76 (SD 8) years; SEX 8 (80%) male; FEV1 mean 44 (SD 29)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP no SUPERVISION no COMMON INTERVENTION 2 litres a minute through nasal cannula backpack no limit on cylinder usage standard advice
INTERVENTION supplemental oxygen PLACEBO air |
|
| Outcomes | DEVICE Z80 32K VI (waist)
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING ACKNOWLEDGMENT: "The authors acknowledge Air Products for the supply of cylinders." CONFLICT OF INTEREST statement provided CONTACT Carolyn Sandland carolyn.sandland@uhl‐tr.nhs.uk University Hospitals Of Leicester NHS Trust, Leicester (UK) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomized to receive cylinder oxygen or cylinder air for 8 weeks. Prior to the study, a randomization list was prepared" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "prior to the study, a randomization list was prepared and transferred to sealed envelopes" |
| Blinding of participants (performance bias) | Low risk | Quote: "double‐blinded… the cylinders were prefllIed with oxygen or air and were disguised and only identifiable by a colour code" |
| Blinding of personnel (performance bias) | Low risk | Quote: "double‐blinded… the cylinders were prefllIed with oxygen or air and were disguised and only identifiable by a colour code" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | no participant flow diagram by group provided |
| Selective reporting (reporting bias) | Unclear risk | Results as in Methods except SF36 results not presented other than "there were no significant changes in the SF36" |
| Other bias | Unclear risk | Trial registration: National Research Register N0123109178. Unable to access |
Schuz 2015.
| Methods | DESIGN 2 groups DATES May 2008 to December 2010 SETTING 31 general practices in rural, remote and metropolitan areas (Australia) SAMPLE SIZE calculation based on SF36 |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS AGE mean 68 (SD 8) years; SEX 97 (53%) male; FEV1 mean 55 (SD 13)% predicted
|
|
| Interventions | DURATION OF INTERVENTION 12 months FOLLOW‐UP no SUPERVISION no INTERVENTION self‐management (health mentoring) Up to 16 phone calls, trained community nurses
SHAM Usual care as provided by GP Monthly “social” phone calls without specific advice or skills training |
|
| Outcomes | DEVICE ActiGraph GT1M
ASSESSMENT TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Julia Walters julia.walters@utas.edu.au University of Tasmania, Hobart (Australia) Additional data provided: step count, HRQOL |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "cluster randomized controlled trial… Participating practices were randomised using a code generated from a random numbers table" |
| Allocation concealment (selection bias) | Low risk | Quote: "concealment of allocation was provided by sequentially numbered opaque, sealed envelopes" |
| Blinding of participants (performance bias) | Unclear risk | Quote: "randomisation occurred at general practice level to avoid contamination between the intervention and control groups" |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "randomisation occurred at general practice level to avoid contamination between the intervention and control groups" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL: Quote: "blinded assessor" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | Registry (not in paper)
|
| Other bias | Low risk | N/A |
Sena 2013.
| Methods | DESIGN 2 groups DATES, SETTING, SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS not reported
|
|
| Interventions | DURATION OF INTERVENTION 10 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION exercise training (eccentric cycle training) SETTING outpatient CONTACT 3 sessions a week AEROBIC TRAINING high‐intensity: target 4 times 80% baseline concentric maximal work capacity STRENGTH TRAINING, OTHER COMPONENTS, EDUCATION nil INTERVENTION exercise training (concentric cycle training) SETTING outpatient CONTACT 3 sessions a week AEROBIC TRAINING high‐intensity: target 80% baseline concentric maximal work capacity STRENGTH TRAINING, OTHER COMPONENTS, EDUCATION nil |
|
| Outcomes | DEVICE SenseWear Pro3 (software version not reported)
TIME POINTS
OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement not provided (abstract only) CONTACT Riany Sena rianysena@yahoo.com.br McGill University Health Center, Montreal (Canada) Additional information provided: type of device, risk of bias assessment |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed by an investigator not involved in the study with variable block design (maximum size of 4) with equal allocation ratio (1:1), using a computer‐generated sequence (http://www.randomizer.org)" (correspondence) |
| Allocation concealment (selection bias) | Low risk | Quote: "The allocation sequence was placed in double‐sealed opaque envelopes. The trainer opened the appropriate envelope only once the baseline evaluation had been completed" (correspondence) |
| Blinding of participants (performance bias) | Unclear risk | Quote: "Given the kind of intervention, a blinded design was not possible for patients... (but) patients were unaware of our primary outcome... patients allotted to the (eccentric training) group exercised at a different time than did the patients in the (concentric training) group and were asked not to discuss their exercises with assessors and their peers" (correspondence) |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "Given the kind of intervention, a blinded design was not possible for patients and trainers... however, trainers were not involved in the data collection" (correspondence) |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity, exercise capacity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "We had a total of 4 dropouts. There were 11 participants in the eccentric group and 13 participants in the concentric group, but 10 participants in each group completed all the training sessions. For the final study, we did intention to treat analyses and included all 24 participants" (correspondence) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information (abstract only) |
| Other bias | Unclear risk | Abstract only |
Singh 1998.
| Methods | DESIGN 2 groups DATES not reported (abstract only) SETTING PR programme (UK) SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA not reported BASELINE CHARACTERISTICS
AGE mean 67 (SD 10) years; SEX 7 (78%) males; FEV1 mean 1.2 (SD 0.3) litres
AGE mean 71 (SD 9) years; SEX 8 (80%) males; FEV1 mean 1.1 (SD 0.4) litres |
|
| Interventions | DURATION OF INTERVENTION 1 week FOLLOW‐UP no SUPERVISION no INTERVENTION PR SETTING outpatient group INTERVENTION unaware of purpose of pedometer, no knowledge of the true purpose of the activity monitor INTERVENTION aware of purpose of pedometer, full knowledge of the purpose of the activity monitor |
|
| Outcomes | DEVICE Gaewiler Electronic (waist)
ASSESSMENT TIME POINTS daily for 7 days OUTCOMES
|
|
| Notes | FUNDING, CONFLECT OF INTEREST not reported (abstract only) CONTACT Sally Singh sally.singh@uhl‐tr.nhs.uk University Hospitals Of Leicester NHS Trust, Leicester (UK) Additional information requested. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomised into two groups" Comment: Insufficient information (abstract only) |
| Allocation concealment (selection bias) | Unclear risk | Not specified (abstract only) |
| Blinding of participants (performance bias) | Unclear risk | Quote: "Patients were randomised into two groups; Group 1, no knowledge of the true purpose of the activity monitor… group 2, full knowledge of the purpose of the activity monitor" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified (abstract only) |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not specified (abstract only) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information (abstract only) |
| Other bias | Unclear risk | Abstract only |
Steele 2019.
| Methods | DESIGN 2 groups DATES 2009 to 2012 SETTING VA Puget Sound Health Care System, Seattle (USA) SAMPLE SIZE calculation based on step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
AGE mean 67 (SD 10) years; SEX 100% male; FEV1 mean 32 (SD 14) % predicted
AGE mean 67 (SD 9) years; SEX 100% male; FEV1 mean 32 (SD 10)% predicted N.B. group numbers at 6 months not provided |
|
| Interventions | DURATION OF INTERVENTION 8 weeks PR, 6 months adherence intervention FOLLOW‐UP yes SUPERVISION no COMMON INTERVENTION exercise sessions SETTING outpatient AEROBIC AND STRENGTH TRAINING goal: treadmill walking 20 minutes
5 minutes warm‐up: upper‐ and lower‐extremity stretching 20 minutes NuStep Borg scale (rating 4 to 6) 5 minutes free arm weights 5 minutes arm ergometry 5 minutes cool‐down: upper‐ and lower‐extremity stretching INTERVENTION adherence intervention
DURATION 4 weeks SETTING outpatient CONTACT 4 hours CONTENT exercise and integrated self‐management education, home safety evaluation
DURATION 3 months SETTING home‐based CONTACT 1 phone call a week CONTENT
DURATION 2 months SETTING home‐based CONTACT 1 phone call a fortnight CONTENT as per stage 2
SETTING outpatient CONTACT 1 session per month CONTENT supervised exercise session INTERVENTION PR DURATION 8 weeks CONTACT 2 hours CONTENT exercise and self‐management instruction Following the 8‐week programme
|
|
| Outcomes | DEVICE Stepwatch Activity Monitor (Orthocare Innovations, LLC, Mountlake Terrace, WA) (above dominant ankle)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes |
FUNDING VA HSR&D, NRI 04–242 CONFLICT OF INTEREST "The authors declare no conflicts of interest" CONTACT Cynthia Dougherty cindyd@uw.edu University of Washington, Seattle (USA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomized … using a computerized adaptive treatment assignment algorithm" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding of participants (performance bias) | High risk | Quote: "Masking: none (open label)" |
| Blinding of personnel (performance bias) | High risk | Quote: "Masking: none (open label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Quote: "Post‐program measures were completed... by a team member blinded to group assignment" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | CONSORT diagram provided No details about attrition according to diagnosis group |
| Selective reporting (reporting bias) | Unclear risk | Primary outcomes Registry: 6MWD Paper: 6MWD and physical activity Secondary outcomes Registry: SF36 PCS Paper: SF36 PCS and MCS, clinical COPD questionnaire, Geriatric Depression Scale, cardiopulmonary function outcomes 12‐month outcomes not presented according to group allocation |
| Other bias | Unclear risk | Prospectively registered First Posted: April 30, 2007 Study Start Date: December 2007 Actual Primary Completion Date: December 2011 May 2007; Quote: "Improvement in functional capability, quality of life, self‐efficacy, cardiopulmonary function, gait & balance, mediating effects of self‐regulation model on functional capability, reduction in hospital admissions, outpatient visits & expenditures" August 30, 2010; Enrolment: 200; Revised to 82 February 7, 2012; Enrolment: 100 August 30, 2017; Enrolment: 90 |
Tabak 2014a.
| Methods | DESIGN 2 groups DATES October 2010 to April 2011 SETTING "recruited by a chest physician or nurse practitioner" (The Netherlands) SAMPLE SIZE feasibility (limited availability of activity coach) |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 65 (SD 9) years; SEX 8 (44%) male; FEV1 mean 49 (SD 17)% predicted
AGE mean 68 (SD 6) years; SEX 11 (67%) male; FEV1 mean 56 (SD 11)% predicted |
|
| Interventions | DURATION OF INTERVENTION 3 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (telerehabilitation) INTERFACE
ACTIVITY "Try to be active in such a way during the day that the displayed reference line is closely approached" STEP‐TRACKING Accelerometer (MTx‐W sensor) RECORD
GOALS
EDUCATION/RESOURCES
INTERVENTION optional supervised exercise SETTING optional, weekly, group sessions, local physiotherapy practices |
|
| Outcomes | DEVICE Yamax Digiwalker 200 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Monique Tabak m.tabak@rrd.nl Roessingh Research and Development, Roessinghsbleekweg (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "participants were randomly assigned…according to a computer‐generated randomization list" |
| Allocation concealment (selection bias) | Low risk | Quote: "participants were allocated in order of inclusion following the randomization list. Recruitment, randomization, and allocation were performed by different persons" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: unclear if step count was reported by participants |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL: not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | High risk | SECONDARY OUTCOMES Registry: distribution of activities throughout the day, correlation between pedometer and MTX‐W motion sensor (not reported) Paper: CCQ, dyspnoea, fatigue, number of visits to the web portal, time the activity sensor was worn, adherence (additional outcomes) |
| Other bias | Unclear risk | Physiotherapy‐supervised exercise training in both groups: participation only described at baseline |
Tabak 2014b.
| Methods | DESIGN 2 groups DATES December 2011 to July 2013 SETTING Medisch Spectrum Twente Hospital and primary care physiotherapy practices, Enschede (The Netherlands) SAMPLE SIZE Registry: n = 30 Paper: “sample size was based upon the estimated number of patients that could be included within the recruitment period and the availability of technology” |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA (registry)
BASELINE CHARACTERISTICS
AGE mean 64 (SD 9) years; SEX 6 (50%) male; FEV1 median 50 (IQR 33 to 62)% predicted
AGE mean 63 (SD 7) years; SEX 6 (50%) male; FEV1 median 36 (IQR 26 to 54)% predicted |
|
| Interventions | DURATION OF INTERVENTION 9 months FOLLOW‐UP no SUPERVISION no INTERVENTION “Condition Coach” technology‐supported care programme Pre‐program: 2 90‐minute self‐management teaching sessions given by a nurse practitioner
4 modules 1. Web‐based exercise programme: breathing exercises, relaxation, mobilisation, resistance and endurance training, mucus clearance created by physiotherapist; every exercise has description and movie care professionals could check progress on the web portal 2. Accelerometer‐based activity sensor and smartphone ambulant activity registration and display, real‐time feedback; goal: reference activity line motivational cues 3. Web‐based self‐management module: participants to treat exacerbations themselves; decision‐support system that automatically formed advice to start medication if worsening clinical condition 4. Teleconsultation module for communication with primary care physiotherapist NO INTERVENTION in case of impending AECOPD, contact medical doctor allowed to attend regular physiotherapy sessions if prescribed as part of usual care |
|
| Outcomes | DEVICE accelerometer‐based activity sensor (Inertia Technology, Enschede, The Netherlands)
ASSESSMENT TIME POINTS
PRIMARY OUTCOMES
SECONDARY OUTCOMES
|
|
| Notes | FUNDING “Financial support was provided by the NL Agency, a division of the Dutch Ministry of Economic Affairs (grant CALLOP9089).” CONFLICT OF INTEREST “The authors report no conflicts of interest in this work.” CONTACT Monique Tabak m.tabak@utwente.nl University of Twente, Drienerlolaan (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Patients were randomized using a computer‐generated randomization list (Blocked Stratified Randomization version 5; Steven Piantadosi), where randomization was applied in random blocks of two and four.” |
| Allocation concealment (selection bias) | Low risk | Quote:“Participants were allocated by a data manager in order of inclusion following the randomization list, placed in a sealed envelope.” |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to intervention |
| Blinding of personnel (performance bias) | High risk | Masking: None (registry) |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity (unclear if assessed during intervention) |
| Blinding of outcome assessment [other] (detection bias) | High risk | Masking: None (registry) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Flow chart provided and attrition documented Quote:“Although 101 patients fulfilled the COPE II study criteria, only 29 patients (29%) were able and willing to participate. The reason for not participating was that patients did not fulfill the additional criterion of having a computer with Internet access at home…. A large number of patients were not able or willing to continue study participation: 33% in the intervention group and 86% in the control group… Although some patients in the intervention group quit the physiotherapy modules (exercising and activity coach) due to weak (n=1, ,T1) or unstable condition (n=1, ,T2) and personal circumstances (n=2, ,T4), they persisted in using the web portal and triage diary till T4.” |
| Selective reporting (reporting bias) | High risk | Results only presented for T0, T1, T2 |
| Other bias | Unclear risk | SAMPLE SIZE Registry: n = 30 Paper: “sample size was based upon the estimated number of patients that could be included within the recruitment period and the availability of technology” |
Tahirah 2015.
| Methods | DESIGN 2 groups DATES not reported (abstract only) SETTING hospital (? Malaysia) SAMPLE SIZE not reported (abstract only) |
|
| Participants | INCLUSION CRITERIA (as in registry)
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 62 (SD 7) years; SEX 20 (100%) male; FEV1 mean 33 (SD 14)% predicted
AGE mean 66 (SD 8) years; SEX 17 (94%) male; FEV1 mean 34 (14)% predicted |
|
| Interventions | DURATION OF INTERVENTION length of stay FOLLOW‐UP no SUPERVISION yes INTERVENTION exercise training (progressive walking and functional resistance exercises) DURATION during admission for AECOPD SETTING inpatient CONTACT commenced within 48 hours of admission, until discharge
AEROBIC TRAINING walking
STRENGTH TRAINING functional resistance exercises
OTHER COMPONENTS afternoon session unsupervised EDUCATION nil NO INTERVENTION as per Malaysian COPD clinical practice guidelines usual physiotherapy care may comprise airway clearance (if required), strategies to minimise dyspnoea (e.g. pursed lip breathing and positioning), and encouragement to mobilise in the ward |
|
| Outcomes | DEVICE Stepwatch
ASSESSMENT TIME POINTS
PRIMARY OUTCOMES baseline and prior to discharge
SECONDARY OUTCOMES:
|
|
| Notes | FUNDING, CONFLICT OF INTEREST not reported (abstract only) CONTACT Fatim Tahirah fatim_mirza@uitm.edu.my Curtin University, Perth (Australia) Additional information provided: baseline characteristics, physical activity, exercise capacity |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomisation table created by computerised sequence generation" |
| Allocation concealment (selection bias) | Low risk | Quote: "sealed opaque envelopes" |
| Blinding of participants (performance bias) | Unclear risk | Quote: "Participants unable to be blinded to intervention but unaware of other treatment group’s intervention" |
| Blinding of personnel (performance bias) | High risk | Quote: "Not blinded: personnel" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | Exercise capacity: Quote: "assessor blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information (abstract only) |
| Selective reporting (reporting bias) | Unclear risk | Registry: sit to stand test (not reported) |
| Other bias | Unclear risk | Abstract only |
Troosters 2014.
| Methods | DESIGN 2 groups DATES April 2007 to July 2010 SETTING 70 centres in 10 countries SAMPLE SIZE calculation based on FEV1 area under the curve |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
MEDICATIONS
BASELINE CHARACTERISTICS
AGE mean 61 (SD 8) years; SEX 167 (70%) male; FEV1 post‐bronchodilator mean 66 (SD 8)% predicted
AGE mean 62 (SD 9) years; SEX 147 (67%) male; FEV1 post‐bronchodilator mean 66 (SD 8)% predicted |
|
| Interventions | DURATION OF INTERVENTION 24 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION behavioral modification INTERFACE monthly individual session ACTIVITY walking/cycling STEP‐TRACKING nil RECORD activity diary GOALS
EDUCATION/RESOURCES educational DVDs INTERVENTION LAMA (tiotropium, 18 μg) once daily self‐administered morning via HandiHaler PLACEBO once daily self‐administered morning via HandiHaler |
|
| Outcomes | DEVICE SenseWear Armband (software version 6.1) (right upper arm)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "The study was funded by Pfizer Inc and Boehringer Ingelheim Pharma GmbH & Co KG." CONFLICT OF INTEREST statement provided CONTACT Thierry Troosters thierry.troosters@kuleuven.be KU Leuven (Belgium) Additional information requested: unable to source from Pfizer |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomized, double‐blind, placebo‐controlled, multinational study" (protocol) |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | Low risk | Quote: "placebo" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified Quote: "double‐blind treatment phase" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | Protocol: LIPA time, patient diary (not reported) Paper: safety evaluation, adverse events, serous adverse events, AECOPD (additional outcomes reported) |
| Other bias | Unclear risk | Quote: "When this study was designed (in 2006/7), physical activity monitoring was in its infancy. We therefore did not include physical activity as a primary endpoint. Today there is more clarity on factors affecting the outcome of such monitoring, number of days of assessment needed, hours/day and validity of activity monitors in COPD. We measured physical activity using a validated activity monitor as an exploratory endpoint, which allowed for some flexibility in the analysis" |
Troosters 2018.
| Methods | DESIGN 4 groups N.B. all groups received 12 weeks behaviour modification (5 comparisons)
DATES March 2014 to October 2015 SETTING "17 academic institutes, 15 secondary care and 5 primary care centres" (Australia, New Zealand, the USA, Canada and Europe) SAMPLE SIZE calculation based on "EET for each arm compared to self‐management with placebo" "Comparisons between the three non‐placebo arms were also performed; however, the trial was not designed or powered for these comparisons" |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
FROM ONLINE SUPPLEMENT "Patients on continuous home oxygen were excluded from the study... Willingness to increase physical activity is not an inclusion criterion but patients have to be willing to take part in the 8‐week exercise training program (1 in 4 chance of being randomised to the treatment arm that includes exercise training) and take part in the behaviour‐change self‐management program." MEDICATIONS "Patients are permitted to continue with inhaled corticosteroids but not LAMAs, LABAs or short‐acting muscarinic antagonists during the trial, and all are provided with open‐label salbutamol for rescue medication use throughout the trial. Acute exacerbations can be treated as medically necessary." BASELINE CHARACTERISTICS
AGE mean 64 (SD 7) years; SEX 46 (71%) male; FEV1 post‐bronchodilator mean 56 (SD 14)% predicted
AGE mean 66 (SD 6) years; SEX 51 (76%) male; FEV1 post‐bronchodilator mean 57 (SD 13)% predicted
AGE mean 65 (SD 7) years; SEX 45 (63%) male; FEV1 post‐bronchodilator mean 59 (SD 11)% predicted
AGE mean 65 (SD 7) years; SEX 42 (60%) male; FEV1 post‐bronchodilator mean 57 (SD 13)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks (exercise training first 8 weeks) FOLLOW‐UP no SUPERVISION no INTERVENTION placebo once daily INTERVENTION LAMA (tiotropium 5 µg) once daily INTERVENTION LAMA/LABA (tiotropium+olodaterol 5/5 µg) once daily INTERVENTION LAMA/LABA (tiotropium+olodaterol 5/5 µg) once daily with exercise training INTERVENTION behaviour modification DURATION 12 weeks INTERFACE
ACTIVITY Not specified STEP‐TRACKING Pedometer OMRON HJ‐321 (direct feedback) RECORD "patient worksheet" GOALS
EDUCATION/RESOURCES
INTERVENTION high‐intensity whole‐body exercise training SETTING outpatient CONTACT 3 sessions per week AEROBIC TRAINING 30 minutes stationary leg cycling or treadmill walking
STRENGTH TRAINING upper and lower limbs, 45 minutes
OTHER COMPONENTS, EDUCATION nil |
|
| Outcomes | DEVICE MoveMonitor
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "Troosters: Funding This work was supported by Boehringer Ingelheim Pharma GmbH & Co. KG. Medical writing assistance was provided by Claire Scofield of Complete HealthVizion, which was contracted and compensated by Boehringer Pharma GmbH & Co. KG. The PROactive project is funded by the IMI‐JU (#115011). The PHYSACTO trial is an in‐kind contribution of the sponsor Boehringer Ingelheim to the PROactive project. In this project, the innovative patient‐reported outcome tool and the activity monitor were developed and validated. Bourbeau: The PROactive project is funded by the IMI‐JU grant number #115011. The PHYSACTO trial is an in‐kind contribution of the sponsor Boehringer Ingelheim to the PROactive project Acknowledgements Medical writing assistance was provided by Laura George, PhD, of Complete HealthVizion, which was contracted and compensated by Boehringer Ingelheim Pharma Inc." CONFLICT OF INTEREST "Competing interests JB has received grants from the Canadian Institute of Health Research R&D collaborative programme (AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Merck, Nycomed, Novartis), the Canadian Respiratory Research Network, the Respiratory Health Network of the FRQS and the Research Institute of the MUHC. KLL reports personal fees from the study sponsor for personnel training, as well as a grant from AbbVie and personal fees from Bayer, Janssen, Novartis, AbbVie, Mundipharma and Almirall. MS is employed by Respiplus, a non‐profit organisation that was contracted by the study sponsor to develop the educational component of the training programme. DDS, DE and AH are employees of Boehringer Ingelheim. FM has received grants from Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Nycomed and Pfizer, personal fees from Boehringer Ingelheim, GlaxoSmithKline and Novartis, and other financial support from GlaxoSmithKline. TT has received grants from the Innovative Medicines Initiative Joint Undertaking and speaker fees from Boehringer Ingelheim and GlaxoSmithKline. NL is employed by Evidera, a healthcare research firm that provides consulting and other research services to pharmaceutical and other organisations including the study sponsor. The authors meet the criteria for authorship as recommended by the International Committee of Medical Journal Editors. They take full responsibility for the scope, direction, content of, and editorial decisions relating to the manuscript, were involved in reviewing and revising the manuscript at all stages of development, and have approved the submitted manuscript. Troosters: Competing interests TT has received grants from the Innovative Medicines Initiative Joint Undertaking and speaker fees from Boehringer Ingelheim and GlaxoSmithKline. JB has received grants from the Canadian Institute of Health Research R&D collaborative programme (AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Merck, Nycomed, Novartis), the Canadian Respiratory Research Network, the Respiratory Health Network of the FRQS and the Research Institute of the MUHC. FM has received grants from Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Nycomed and Pfizer, personal fees from Boehringer Ingelheim, GlaxoSmithKline and Novartis, and other financial support from GlaxoSmithKline. NL is employed by Evidera, a healthcare research firm that provides consulting and other research services to pharmaceutical and other organisations including the study sponsor. DE, DDS, LK and AH are employees of Boehringer Ingelheim. DE, DDS and AH are employees of the sponsor and were involved in the design, implementation and interpretation of the study results, together with the investigators Registry: Principal Investigators are NOT employed by the organization sponsoring the study. There IS an agreement between Principal Investigators and the Sponsor (or its agents) that restricts the PI's rights to discuss or publish trial results after the trial is completed. Restriction Description: Boehringer Ingelheim (BI) acknowledges that investigators have the right to publish the study results. Investigators shall provide BI with a copy of any publication or presentation for review prior to any submission. Such review will be done with regard to proprietary information, information related to patentable inventions, medical, scientific, and statistical accuracy within 60 days. BI may request a delay of the publication in order to protect BI’s intellectual property rights." CONTACT Thierry Troosters thierry.troosters@kuleuven.be KU Leuven (Belgium) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation is performed using a pseudo‐random number generator and block randomisation is used to achieve balanced allocation" |
| Allocation concealment (selection bias) | Low risk | Quote: "Patients are assigned to treatment arms using a web‐based and telephone‐based response system, and provided with numbered medication boxes" |
| Blinding of participants (performance bias) | Unclear risk | Quote: "A double‐blind design is used for the groups receiving placebo & behaviour modification, (LAMA) & behaviour modification, and (LAMA/LABA) & behaviour modification" Quote: "It is not possible to blind the participants or staff against the group receiving (exercise training)" |
| Blinding of personnel (performance bias) | Unclear risk | Quote: "A double‐blind design is used for the groups receiving placebo+behaviour modification, tiotropium monotherapy+behaviour modification, and tiotropium +olodaterol+behaviour modification" Quote: "It is not possible to blind the participants or staff against the group receiving (exercise training)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: Quote: "A double‐blind design is used for the groups receiving placebo+behaviour modification, tiotropium monotherapy+behaviour modification, and tiotropium +olodaterol+behaviour modification" Quote: "It is not possible to blind the participants or staff against the group receiving (exercise training)" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Low risk | Paper: CRQ, dyspnoea, medication adherence (additional outcomes reported) |
| Other bias | Unclear risk | Registry: Study start March 2014 Study completion October 2015 Original entry: 3 arms Modifications made November 2016: four arms |
Tsai 2016.
| Methods | DESIGN 2 groups DATES not reported SETTING tertiary hospital PR programme (Australia) SAMPLE SIZE calculation based on ESWT |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 73 (8) years; SEX 12 (63%) male; FEV1 mean 60 (SD 23)% predicted
AGE mean 75 (SD 9) years; SEX 6 (35%) male; FEV1 mean 68 (SD 19)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP no SUPERVISION yes INTERVENTION PR (telerehabilitation) SETTING home (laptop computer with an in‐built camera), outpatient group (maximum 4 participants) CONTACT
AEROBIC TRAINING
STRENGTH TRAINING sit to stand, squats (3 sets, 10 repetitions) OTHER COMPONENTS, EDUCATION nil |
|
| Outcomes | DEVICE SenseWear (software version 8.0) (left upper arm)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement not provided CONTACT Ling Ling Tsai lingling.tsai@health.nsw.gov.au University of Sydney (Australia) Adiitional information provided: clarification for total energy expenditure units (kcal), thresholds for classification of physical activity according to intensity (light, moderate) and results for all time in physical activity greater than three METs (to enable inclusion in meta‐analysis). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "This study was a prospective, blinded (assessor and statistician) RCT. Participants were randomized by one of the investigators (L.L.Y.T.) using a computer‐generated sequence" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "concealed allocation" |
| Blinding of participants (performance bias) | High risk | Unable to blind participant to intervention. |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "this study was a prospective, blinded (assessor and statistician) RCT… measurements which were performed by a research assistant who was blind to group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | SECONDARY OUTCOMES Registry: satisfaction, semi‐structured interview post telerehabilitation (not reported in paper) |
| Other bias | Low risk | N/A |
Van de Bool 2017.
| Methods | DESIGN Stage 1 2 groups (intervention (nutritional supplement) with PR vs. PR) Stage 2 2 groups (intervention (nutritional supplement) with PAC vs. PAC) DATES September 2011 to April 2014 SETTING outpatient PR programme in 7 hospitals (The Netherlands) SAMPLE SIZE calculation based on peak torque |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 63 (SEM 1) years; SEX 18 (43%) male; FEV1 mean 57 (SEM 3)% predicted
AGE mean 62 (SEM 1) years; SEX 23 (59%) male; FEV1 mean 53 (SEM 3)% predicted |
|
| Interventions | DURATION OF INTERVENTION Phase 1: 4‐month nutritional intervention Phase 2: 8‐month maintenance phase FOLLOW‐UP Phase 3: up for 3 months, without any intervention in either group SUPERVISION no PHASE 1 COMMON INTERVENTION 4‐month outpatient centre‐based pulmonary rehabilitation
INTERVENTION protein, carbohydrates, fat and micronutrients, enriched with leucine, omega‐3 PUFA, and vitamin D (Nutricia NV, Zoetermeer, The Netherlands) PLACEBO flavoured non‐caloric cloudified aqueous solution, no active components PHASE 2 COMMON INTERVENTION Both groups received feedback on their physical activity behaviour twice, based on accelerometry INTERVENTION 1 oral nutritional supplement a day, four nutritional counselling sessions |
|
| Outcomes | DEVICE GT3X Actigraph accelerometer
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was financially supported by a Public–Private Consortium of Maastricht University/NUTRIM, CIRO+ BV Horn, Lung Foundation Netherlands (grant 3.4.09.003), and Nutricia Research." CONFLICT OF INTEREST "ER, FF and EW declare that they have no conflict of interest regarding the present manuscript. AvH is employed by Nutricia Research. CvdB and AS report grants from Netherlands Lung Foundation and Nutricia." Research, during the conduct of the study. AS is a member of International Scientific Advisory Board of Nutricia Advanced Medical Nutrition." CONTACT Annemie Schols a.schols@maastrichtuniversity.nl Maastricht University Medical Center, (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The randomization sequence was generated using the PLAN procedure of SAS statistical software (Enterprise Guide version 4.3) by a statistician from Nutricia Research who had no further involvement in the conduct of the study. The permuted block randomization was stratified for site, with a 1:1 allocation ratio" |
| Allocation concealment (selection bias) | Low risk | Quote: "All details of the randomization, including block size, were unknown to the investigator, site staff, and study staff, except for the statistician who was responsible for generating the randomization sequence, and the supplies manager who needed to be unblinded in order to label the study products and to create unblinding envelopes, etc" |
| Blinding of participants (performance bias) | Low risk | Quote: "The packaging of the test product and control product were identical in appearance. The study product was labelled using product numbers. Which product numbers corresponded to which treatment was only known to the statistician who was responsible for generating the randomization sequence and the clinical studies supplies manager" |
| Blinding of personnel (performance bias) | Low risk | Quote: "The packaging of the test product and control product were identical in appearance. The study product was labelled using product numbers. Which product numbers corresponded to which treatment was only known to the statistician who was responsible for generating the randomization sequence and the clinical studies supplies manager" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity and exercise capacity (cycle ergometry) |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | Exercise capacity (6MWD):"double blind" (paper), "triple blind"(registry) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided Quote: "Two of the 81 randomized patients did not start the treatment. During the PR, the drop‐out rate was 9.5% (four patients) in NUTRITION and 5.4% (two patients) in PLACEBO" |
| Selective reporting (reporting bias) | Unclear risk | PRIMARY OUTCOME Registry: skeletal muscle strength (baseline, 12 months) Paper: quadriceps muscle strength (baseline, 4 months) SECONDARY OUTCOMES Registry:
Paper:
|
| Other bias | Unclear risk | Quote "Patient inclusion was prematurely discontinued because the test product could not be produced within the appropriate quality specifications due to discontinuation of the supply of one of the ingredients, but justifiable based on other RCTs published in the meantime as argued in the discussion" |
Varas 2018.
| Methods | DESIGN 2 groups DATES not reported SETTING University (Spain) SAMPLE SIZE not reported |
|
| Participants | "Recruitment was conducted by the pulmonology consultants of the aforementioned hospitals, using an intentional system of consecutive series" INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 70 (SD 7) years; SEX 18 (86%) male; FEV1 mean 46 (SD 17)% predicted
AGE 65 (SD 9) years; SEX 13 (68%) male; FEV1 mean 52 (SD 16)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks FOLLOW‐UP 12 months SUPERVISION no INTERVENTION PAC and exercise training INTERFACE weekly phone call ACTIVITY walking 5 sessions a week, 30 to 60 minutes (15‐ to 20‐minute cycles) (as for ISWT) STEP‐TRACKING pedometer (direct feedback, control walking speed) RECORD diary: daily step count GOALS revised weekly, 10% to 20% increase EDUCATION/RESOURCES nil INTERVENTION pedometer ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) GOALS general recommendations to walk more every day EDUCATION/RESOURCES 5 group sessions of respiratory physiotherapy (ventilation techniques, bronchial clearance, thoracic mobilisation, education). "This initial intervention, considered as “standard care” in a PR programme, has shown no influence in the variables we analysed" (Spruit 2013) INTERFACE, RECORD nil |
|
| Outcomes | DEVICE OMRON Walking Style X Pocket HJ‐320e (pedometer) (waist, next to right hip)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Jordi Vilaró jordivc@blanquerna.url.edu Universidad Autónoma de Madrid (Spain) Additional information provided: 'Risk of bias' assessment |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were allocated to one of two groups (experimental or control) through simple randomization, using a system of random numbers generated by Microsoft® Excel 2010" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "The allocation sequence was concealed" (correspondence) |
| Blinding of participants (performance bias) | Low risk | Quote: "Participants were not aware of the interventions applied to the other group, and contact between the two groups was avoided at all times" |
| Blinding of personnel (performance bias) | High risk | Quote: "Correspondence between numerical codes and study group was only available to researchers in charge of the treatment, not to evaluators" |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: Quote: "obtained the data recorded in the memory of the device and the data collected by the patients every day in a diary. We confirmed that either data coincident or, we accepted when there was a variation lower than 10%" (correspondence) |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "correspondence between numerical codes and study group was only available to researchers in charge of the treatment, not to evaluators" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods |
| Other bias | Unclear risk |
|
Vasilopoulou 2017.
| Methods | DESIGN 3 groups, 2 phases
DATES not reported SETTING outpatient clinic (Greece) SAMPLE SIZE calculation based on number of hospitalisations for AECOPD |
|
| Participants | "The majority of patients were referred to the PR programme because of persistent respiratory symptoms, but also following hospitalisation for acute exacerbation of COPD (four patients in group A and six patients in group B). These patients were included in the study at least 8 weeks after the hospitalisation. None of these patients had previously participated in a PR programme." INCLUSION CRITERIA
Additional as per registry
EXCLUSION CRITERIA
Additional as in registry
BASELINE CHARACTERISTICS
AGE mean 67 (SD 10) years; SEX 44 (94%) male; FEV1 mean 50 (SD 22)% predicted
AGE mean 67 (SD 7) years; SEX 38 (76%) male; FEV1 mean 52 (SD 17)% predicted
AGE mean 64 (SD 8) years; SEX 37 (74%) male; FEV1 mean 52 (SD 21)% predicted |
|
| Interventions | DURATION OF INTERVENTION 14 months FOLLOW‐UP no SUPERVISION yes INTERVENTION exercise training (HIIT) DURATION 8 weeks SETTING centre‐based outpatient group CONTACT 3 sessions a week AEROBIC TRAINING cycling 45 minutes, alternating 30‐second exercise intervals with 30‐second rest periods
STRENGTH TRAINING upper and lower limbs, 15 minutes (3 sets, 10 repetitions) OTHER COMPONENTS advice from dietician EDUCATION instructions on breathing control, self‐management techniques INTERVENTION maintenance (telerehabilitation) DURATION 12 month SETTING home CONTACT 1 session a week, 1 hour (144 sessions) telephone or video conference (tablet) AEROBIC TRAINING individually‐tailored home‐based exercise programme: walking drills STRENGTH TRAINING upper and lower limbs, 3 sets, 10 to 12 repetitions OTHER COMPONENTS
EDUCATION individualised action plan, brochure of prescribed exercises, video demonstrations: home exercises, breathing retraining techniques, educational leaflets for COPD, instruction on management of anxiety and depression symptoms, dietary and self‐management advice INTERVENTION maintenance (centre‐based) DURATION 12 months SETTING outpatient group CONTACT 2 sessions a week (96 sessions) AEROBIC and STRENGTH TRAINING “exercise training” OTHER COMPONENTS nil EDUCATION physiotherapy, dietary and psychological advice |
|
| Outcomes | DEVICE Actigraph GT3X (ActiLife software version 5.10.0) (waist, above right hip)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME (12 months following completion of HIIT)
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Ioannis Vogiatzis gianvog@phed.uoa.gr, Maroula Vasilopoulou maroulavas@yahoo.gr National and Kapodistrian University of Athens (Greece) Additional results provided: scale for graph of time in moderate‐intensity physical activity |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomised into 3 groups using a set of computer‐generated random numbers" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | High risk | Quote: "Masking: None (Open Label)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Unclear risk | HRQOL and exercise capacity: Quote: "Masking: None (Open Label)" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | CONSORT diagram provided Quote: "During the 2‐month primary PR programme, three patients from group A were discontinued from the study because of transport barriers" |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOMES discrepancy between registry and paper Registry:
Methods and Results:
SECONDARY OUTCOMES Paper: cycle ergometry, adherence (additional outcomes) |
| Other bias | Unclear risk | Quote: "During the period spanning from December 2013 to July 2015, patients in groups A and B initially completed a multidisciplinary intense hospital‐based, outpatient, pulmonary rehabilitation programme lasting for 2 months, which was followed by a 12‐month maintenance rehabilitation programme... patients in group C followed the usual care treatment throughout the 14‐month period" Registry: First submitted: November 2015 Primary completion date: July 2015 (definition: final data collection date for primary outcome measure) Study completion date: July 2016 (definition: final data for the primary outcome measures, secondary outcome measures and adverse events (the last participant's last visit). |
Vorrink 2016.
| Methods | DESIGN 2 groups DATES not reported SETTING 32 physiotherapy practices (The Netherlands) SAMPLE SIZE calculation based on weekday step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 62 (SD 9) years; SEX 42 (50%) male; FEV1 mean 59 (SD 20)% predicted
AGE mean 63 (SD 8) years; SEX 36 (49%) male; FEV1 mean 63 (SD 15)% predicted |
|
| Interventions | DURATION OF INTERVENTION 6 months FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (app) INTERFACE
ACTIVITY not specified STEP‐TRACKING accelerometer (in smartphone, direct feedback) GOALS 30 intensive minutes a day
RECORD, EDUCATION/RESOURCES nil INTERVENTION optional supervised exercise SETTING optional, 1 to 2 sessions a week, group training sessions, local physiotherapy practices |
|
| Outcomes | DEVICE SenseWear Pro or MF‐SW mini armband (software version 7.1)
ASSESSMENT TIME POINTS
PRIMARY/SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Sigrid Vorrink sigrid.vorrink@hu.nl Utrecht University of Applied Sciences (The Netherlands) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "This was a multicentre, investigator‐blinded, randomised controlled trial…The patients included in the study were randomly assigned to the intervention or usual care group, independent of physiotherapy practice, based on a random number sequence generated in Excel (Microsoft, Redmond, WA, USA) before enrolment. These numbers ranged between 0 and 1. The values were categorised into 0 (usual care) and 1 (intervention), based on a 0.5 threshold. Subsequently, each newly recruited participant was given the first available number and enrolled in the corresponding group. Patients with and without long‐term physiotherapy after pulmonary rehabilitation…were separately randomised via stratification, because this was seen as a confounder" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "assessments were performed by two researchers that were blinded to the group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "Drop‐out in the intervention group was higher (39% in the intervention group versus 27% in the usual care group), and it was also higher among females. Initial worries about the telephone contract (linked to a personal bank account) and fear of losing the device were reasons for patients to drop out of the study. After the consent form was adjusted to state explicitly that there would not be any financial ramifications, the drop‐out rate decreased" |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods |
| Other bias | Unclear risk | Quote: "Patients with GOLD stage 4 disease were not included in the study, resulting in a sample not fully similar to other pulmonary rehabilitation studies. This was because their low physical activity level renders an intervention effect improbable" Quote: "The present study was set up in primary care and did not measure outcomes at the start of the pulmonary rehabilitation programme. This makes it difficult to compare the decline in physical activity with the potentially beneficial effects of the preceding pulmonary rehabilitation programme" Quote: "The intervention might have yielded different results in patients that did not complete a pulmonary rehabilitation programme. As there could be more room for improvement, physical activity levels could have increased. This has been shown in previous pedometer studies. Nevertheless, as the intervention was not successful in maintaining physical activity in patients after pulmonary rehabilitation, the question remains whether it is capable of improving physical activity in patients without pulmonary rehabilitation" |
Wan 2017.
| Methods | DESIGN 2 groups DATES April 2012 to August 2015 SETTING general pulmonary clinics (USA) SAMPLE SIZE calculation based on step count |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS
AGE mean 68 (SD 9) years; SEX 56 (98%) male; FEV1 mean 60 (SD 21)% predicted
AGE mean 69 (SD 8) years; SEX 51 (98%) male; FEV1 mean 66 (SD 22)% predicted |
|
| Interventions | DURATION OF INTERVENTION 12 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (web‐based, as per Moy 2015a) INTERFACE website ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD website: step count weekly GOALS website: display progress, protocol‐driven goal (revised weekly) minimum value of 3 possibilities: 1) 400 step increase from previous goal; 2) 400 step increase from 7‐day average; or 3) 10,000 steps EDUCATION/RESOURCES website: education and motivational content, community forum INTERVENTION pedometer No instructions about exercise INTERFACE website ACTIVITY walking STEP‐TRACKING pedometer (direct feedback) RECORD website: step count monthly GOALS nil EDUCATION/RESOURCES written materials about exercise at study entry |
|
| Outcomes | DEVICE Omron HJ‐720 ITC (pedometer)
ASSESSMENT TIME POINTS PRIMARY OUTCOME
SECONDARY OUTCOMES
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Marilyn Moy marilyn.moy@va.gov, Emily Wan emily.wan@channing.harvard.edu VA Boston Healthcare System (USA) Additional information provided: confirmed that data in text and Table 20 are SD (not standard errors) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Subjects were then randomized (1:1) by a computer algorithm" |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomization assignments were generated with random block sizes which were not disclosed to study staff. Assignments were communicated to study staff through the ESC website, and subjects were notified by telephone of their assignment groups" |
| Blinding of participants (performance bias) | High risk | Quote: "Due to the nature of the intervention, participant blinding was not possible" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "the research assistant conducting assessments at the study conclusion (3 months) was blinded to group assignment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | High risk | PRIMARY OUTCOME Registry: Originally 6MWD (January 2013) then changed to step count (March 2017) as in paper Between April 2012 and August 2015, 114 participants were enrolled and randomised SECONDARY OUTCOMES Paper: 6MWD, exercise adherence, HRQOL, dyspnoea, depression, COPD knowledge, exercise self‐efficacy, social support, motivation, confidence to exercise daily (additional outcomes reported) |
| Other bias | Low risk | N/A |
Watz 2016.
| Methods | DESIGN cross‐over trial (only pre‐cross‐over data used), 2 groups DATES April 2014 to February 2015 SETTING 30 secondary care/pulmonology practices (Germany) SAMPLE SIZE calculation based on physical activity |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
MEDICATIONS
BASELINE CHARACTERISTICS
AGE mean 64 (SD 8) years; SEX 64 (67%) male; FEV1 mean 63 (SD 10)% predicted
AGE mean 61 (SD 8) years; SEX 63 (64%) male; FEV1 mean 60 (SD 11)% predicted |
|
| Interventions | DURATION OF INTERVENTION 3 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION LAMA/LABA (indacaterol/glycopyrronium (QVA149) 110/50 μg) once daily Breezhaler® PLACEBO once daily Breezhaler® |
|
| Outcomes | DEVICE Sensewear (software version not reported)
TIME POINTS
PRIMARY OUTCOMES
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "This study was funded by Novartis Pharma GmbH. Employees of Novartis Pharma GmbH were involved in the design of the study and analysis, and interpretation of data and oversaw the collection of data. Two of the authors (CM and MB) are authors of the manuscript." CONFLICT OF INTEREST statement provided CONTACT Henrik Watz h.watz@pulmoresearch.de German Center for Lung Research, Grosshansdorf (Germany) Additional information provided: pre‐cross‐over results as per Novartis |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomised to one of two treatment sequences in a ratio of 1:1 using a randomisation number from a list generated by the study sponsor. This list was produced using a validated automated system." |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | Low risk | Quote: "Masking: Double (Participant, Care Provider)" |
| Blinding of personnel (performance bias) | Low risk | Quote: "Masking: Double (Participant, Care Provider)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Low risk | All data reported as in registry |
| Other bias | Low risk | N/A |
Watz 2017.
| Methods | DESIGN 2 groups (data from first 4 weeks only) DATES April 2015 to July 2016 SETTING 26 sites (Canada, Germany, Hungary, Spain) SAMPLE SIZE calculation based on spirometry |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
MEDICATIONS
BASELINE CHARACTERISTICS
AGE mean 63 (SD 8) years; SEX 82 (61%) male; FEV1 post‐bronchodilator mean 60 (SD 11)% predicted
AGE mean 62 (SD 8) years; SEX 80 (60%) male; FEV1 post‐bronchodilator mean 61 (SD 11)% predicted |
|
| Interventions | DURATION OF INTERVENTION 4 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION LAMA/LABA (aclidinium bromide/formoterol fumarate, 400/12 μg) dry‐powder inhaler twice daily (Genuair™/Pressair®) PLACEBO dry‐powder inhaler twice daily (Genuair™/Pressair®) |
|
| Outcomes | DEVICE DynaPort MoveMonitor
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING "Complete Medical Communications, Macclesfield, UK, for providing medical writing support, which was funded by AstraZeneca in accordance with Good Publication Practice (GPP3) guidelines. This study was sponsored by Menarini Group through its affiliate Berlin‐Chemie and AstraZeneca. Menarini Group and AstraZeneca were involved in the study design, collection, analysis, interpretation of data, and development of this manuscript. Menarini Group and AstraZeneca were also involved in the review of the manuscript." CONFLICT OF INTEREST statement provided CONTACT Henrik Watz h.watz@pulmoresearch.de German Center for Lung Research, Grosshansdorf (Germany) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Allocation: Randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | Low risk | Quote: "Masking: Double (Participant, Investigator)" |
| Blinding of personnel (performance bias) | Low risk | Quote: "Masking: Double (Participant, Investigator)" |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity, exercise capacity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | N/A |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participant flow diagram provided |
| Selective reporting (reporting bias) | Unclear risk | SECONDARY OUTCOMES Paper: additional outcomes
|
| Other bias | Unclear risk | Quote: "When considering the design of the ACTIVATE study and any impact this may have had on the results, it should be noted that statistical significance for the primary end point (trough FRC) was reached only after the use of a nonparametric test or after excluding four potential outliers (the sample size was too small to overcome random error in the presence of these extreme outliers). It was unexpected that the improvements in trough FRC did not reach statistical significance, given that previous evidence showed that aclidinium 400 μg improved trough FRC in patients with moderate‐to‐severe COPD, in addition to improvements in other lung hyperinflation end points both in patients with moderate‐to‐severe COPD and in patients with severe‐to‐very severe COPD. However, when considered collectively with the post‐dose data, this post‐hoc analysis supports the conclusion that AB/FF significantly reduced lung hyperinflation. In addition to this, the 2‐month study period of ACTIVATE is too short to show long‐term treatment effects on physical activity, considering that it can be challenging to encourage long‐term changes in physical activity in patients with COPD and that data for long‐term improvements of physical activity by bronchodilators are lacking." |
Widyastuti 2018.
| Methods | DESIGN 2 groups DATES October 2016 to January 2017 SETTING hospital outpatient clinic (Indonesia) SAMPLE SIZE calculation based on 6MWT |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
MEDICATION "Patients maintained their usual drug medication during the entire study" BASELINE CHARACTERISTICS (total n = 40)
AGE mean 68 (7) years; SEX 16 (89%) male; FEV1 mean 1.1 (SD 0.5) litres
AGE mean 61 (7) years; SEX 15 (83%) male; FEV1 mean 0.9 (SD 0.4) litres |
|
| Interventions | DURATION OF INTERVENTION 6 weeks FOLLOW‐UP no SUPERVISION no INTERVENTION PAC (in‐person) DURATION 6 weeks INTERFACE
ACTIVITY walking ≥ 30 minutes a day, fastest pace possible STEP‐TRACKING pedometer RECORD daily log book: step count, change in clinical condition GOALS aim > 6500 steps a day
EDUCATION/RESOURCES nil INTERVENTION exercise training DURATION 6 weeks SETTING centre‐based supervised outpatient CONTACT 3 sessions a week, 30 minutes AEROBIC TRAINING treadmill
OTHER COMPONENTS Encouraged to be more active at home (i.e. no goals)
STRENGTH TRAINING, EDUCATION nil |
|
| Outcomes | DEVICE Omron HJ 321 (pedometer)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING not reported CONFLICT OF INTEREST statement provided CONTACT Kiki Widyastuti dr.kikiwidy@gmail.com Dr Moewardi Hospital, Central Jawa (Indonesia) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants (performance bias) | High risk | Quote: "Patients were not blind to treatment" |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Unclear risk | Physical activity: unclear if step count data was reported by participants |
| Blinding of outcome assessment [other] (detection bias) | High risk | HRQOL and exercise capacity: Quote: "researchers evaluating results and patients were not blind to treatment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | CONSORT diagram provided |
| Selective reporting (reporting bias) | Unclear risk | No trial registry; results presented as in Methods |
| Other bias | Unclear risk | Quote: "During the first week, all patients were taught how to use pedometers in three face to face sessions with a researcher checking patients’ ability to use the device properly. After the training week, subjects were randomly assigned to two groups." Comment: unclear if this was the same week as baseline data collection |
Wootton 2017.
| Methods | DESIGN Phase 1 2 groups (intervention (supervised walking training) vs. no intervention) Phase 2 supervised walking training group from Phase 1 randomised into 2 groups (intervention (PAC and pedometer with walking) vs. intervention (walking)) DATES May 2009 to June 2012 SETTING 5 sites, outpatient PR, 2 metropolitan cities (Australia) SAMPLE SIZE Phase 1: calculation based on CRQ Phase 2: calculation based on total SGRQ score at the 14‐month assessment |
|
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS Phase 1
AGE mean 69 (SD 8) years; SEX 56 (59%) male; FEV1 mean 43 (SD 15)% predicted
AGE mean 68 (SD 9) years; SEX 28 (58%) male; FEV1 mean 43 (SD 15)% predicted Phase 2 (participants from the intervention group in phase 1)
AGE mean 70 (SD 7) years; SEX 25 (51%) male; FEV1 mean 43 (SD 15)% predicted
AGE mean 69 (SD 9) years; SEX 30 (65%) male; FEV1 mean 43 (SD 15)% predicted |
|
| Interventions | DURATION OF INTERVENTION 8 weeks exercise training, 12‐month maintenance period FOLLOW‐UP no SUPERVISION Phase 1 supervised, Phase 2 unsupervised Phase 1 INTERVENTION exercise training (ground‐based walking) with follow‐up advice SETTING centre‐based outpatient group, supervised CONTACT 3 sessions a week (20 sessions within 8 to 10 weeks) AEROBIC TRAINING walking, flat indoor track
STRENGTH TRAINING, OTHER COMPONENTS, EDUCATION nil
SETTING home‐based CONTACT telephone
AEROBIC TRAINING adjusted according to the number of steps achieved in the past 2 training sessions NO INTERVENTION medical management optimised at baseline, including individualised COPD action plan; "did not participate in any exercise training and were not given any instructions regarding exercise" Phase 2 Participants in the intervention group in phase 1 were asked to complete a further 12 months of home‐based walking SETTING home‐based ACTIVITY walk ≥ 3 days a week
RECORD weekly diary card (number of days, number of minutes walked) EDUCATION/RESOURCES written instructions, scoring system for self‐assessment of breathlessness and effort INTERVENTION PAC and pedometer INTERFACE
STEP‐TRACKING pedometer (G‐Sensor accelerometer, direct feedback) GOALS based on step count (immediate past 2 training sessions) |
|
| Outcomes | DEVICE SenseWear® Pro3 (software version 6.1)
ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
|
| Notes | FUNDING reported CONFLICT OF INTEREST statement provided CONTACT Sally Wootton sally.wootton@health.nsw.gov.au University of Sydney (Australia) Additional results provided: physical activity and exercise capacity |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "This study was a prospective, blinded (assessor and statistician), multicentre, randomised controlled trial with concealed allocation. Following baseline assessment participants were randomised via an independent telephone randomisation service using computerised random number generator sequencing to either the walking group or control group. Randomisation was stratified according to baseline lung function, SGRQ, 6MWD and study centre. Randomisation was biased towards the walking group with a 2:1 ratio for the purposes of a long‐term follow‐on study to 12 months." |
| Allocation concealment (selection bias) | Low risk | Quote: "concealed allocation… following baseline assessment participants were randomised via an independent telephone randomisation service" |
| Blinding of participants (performance bias) | High risk | Unable to blind participants to the intervention |
| Blinding of personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment [objective] (detection bias) | Low risk | Physical activity |
| Blinding of outcome assessment [other] (detection bias) | Low risk | HRQOL and exercise capacity: Quote: "assessor blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Lack of clarity on participant numbers |
| Selective reporting (reporting bias) | Unclear risk | Physical activity results not reported at 8 months (as in registry) |
| Other bias | Unclear risk | Quote: "Retrospectively registered" (as per www.anzctr.org.au) |
ACE: angiotensin‐converting enzyme; AECOPD: acute exacerbation of COPD; BMI: body mass index; CAT: COPD assessment test; CCQ: clinical COPD questionnaire; COPD: chronic obstructive pulmonary disease; COPEactive: community‐based physiotherapeutic exercise programme; cpm: counts per minute; CRQ: chronic respiratory disease questionnaire; CT: computerised tomography; ECG: electrocardiogram; EE: energy expenditure; ESWT: time walked on endurance shuttle walk test; EQ5D: EuroQol 5 dimensions questionnaire; FER: forced expiratory ratio; FEV1: forced expiratory volume in 1 second; FRC: functional residual capacity; GOLD: Global Initiative for Chronic Obstructive Lung Disease; HIIT: high‐intensity interval training; HRmax: maximum heart rate; HRQOL: health‐related quality of life; ICD‐10: International Statistical Classification of Diseases and Related Health Problems 10th Revision; ICS: inhaled corticosteroid; ISWD: distance walked on incremental shuttle walk test; ITT: intention‐to‐treat; IQR: interquartile range; LABA: long‐acting beta2 agonist; LAMA: long‐acting muscarinic antagonist; LIPA: light‐intensity physical activity; LTOT: long‐term oxygen therapy; MRC: Medical Research Council; METs: metabolic equivalents; min: minutes; MVPA: moderate‐to‐vigorous physical activity; n: number; NIPPV: non‐invasive positive pressure ventilation; 1RM: one repetition maximum; PAC: physical activity counselling; PaCO2: partial pressure of carbon dioxide; PAL: physical activity level; PaO2: partial pressure of oxygen; Pimax: maximal inspiratory pressure; PR: pulmonary rehabilitation; RAND‐36: Dutch version of SF36; RV: residual volume; sec: seconds; SF36: Medical Outcomes Survey 36‐item short‐form health survey questionnaire; SGRQ: St George's respiratory questionnaire; 6MWD: distance walked on six‐minute walk test; 6MWT: six‐minute walk test; SD: standard deviation; SEM: standard error of measurement; SPACE: self‐management programme of activity, coping and education; SpO2: peripheral oxygen saturation; TLC: total lung capacity; VMU: vector magnitude unit; Wmax: maximum work rate.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| ACTRN12611001034921 | study not completed/withdrawn from registry |
| Aksu 2006 | physical activity not objectively assessed outcome |
| Arnedillo 1998 | physical activity not objectively assessed outcome |
| Atkins 1984 | physical activity not objectively assessed outcome |
| Barnes‐Harris 2019 | physical activity not objectively assessed outcome |
| Bartlett 2017 | physical activity not objectively assessed outcome |
| Baumann 2006 | physical activity not objectively assessed outcome |
| Behnke 2000 | physical activity not objectively assessed outcome |
| Behnke 2005 | not randomised |
| Bernardi 2017 | not randomised |
| Bertici 2013 | not randomised |
| Biscione 2009 | physical activity not objectively assessed outcome |
| Bohning 1990 | physical activity not objectively assessed outcome |
| Boland 2015 | physical activity not objectively assessed outcome |
| Borges 2012 | observational |
| Bourbeau 2000 | physical activity not objectively assessed outcome |
| Budnevskiy 2015 | physical activity not objectively assessed outcome |
| Bunker 2012 | physical activity not objectively assessed outcome |
| Bustamante 2013 | tried to contact author: no physical activity data presented |
| Börekçi 2008 | physical activity not objectively assessed outcome |
| Camillo 2011 | physical activity not objectively assessed outcome |
| Cebollero 2018 | not randomised |
| Chen 2018 | physical activity not objectively assessed outcome |
| Corrado 1995 | physical activity not objectively assessed outcome |
| Coultas 2011 | physical activity not objectively assessed outcome |
| Coultas 2017 | physical activity not objectively assessed outcome |
| De Backer 2014 | physical activity not objectively assessed outcome |
| De Souza 2017 | physical activity not objectively assessed outcome |
| Deering 2011 | Quote: "a complete control group was not possible; therefore, the control group in the present study was monitored on 2 separate occasions 8 weeks apart, and then randomized to either the rehabilitation group or acupuncture and rehabilitation" |
| Durheim 2015 | no group comparison |
| Dyer 2011 | physical activity not objectively assessed outcome |
| EUCTR2016‐003675‐21‐ES | physical activity not objectively assessed outcome |
| Faulkner 2010 | physical activity not objectively assessed outcome |
| Fernandez 1998 | physical activity not objectively assessed outcome |
| Foy 2006 | attempted to contact author: no objective physical activity outcomes published |
| Friis 2017 | attempted to contact author: unable to obtain pre‐cross‐over data |
| Furness 2014 | physical activity not objectively assessed outcome |
| Garcia Aymerich 2016 | secondary analyses |
| Gohl 2004 | physical activity not objectively assessed outcome |
| Gohl 2006 | physical activity not objectively assessed outcome |
| Gomez 2006 | physical activity not objectively assessed outcome |
| Gosselink 1990 | physical activity not objectively assessed outcome |
| Grabenhorst 2013 | physical activity not objectively assessed outcome |
| Greulich 2013 | physical activity not objectively assessed outcome |
| Guell 2008 | physical activity not objectively assessed outcome |
| Gurgun 2011 | physical activity not objectively assessed outcome |
| Hartman 2012 | observational |
| Hataji 2017 | not randomised |
| Herrejon 2010 | physical activity not objectively assessed outcome |
| Hillegass 2012 | physical activity not objectively assessed outcome |
| Horton 2018 | physical activity not objectively assessed outcome |
| Ichinose 2017 | contacted author: unable to obtain pre‐cross‐over data |
| Ides 2012 | physical activity not objectively assessed outcome |
| Innocenti 2000 | physical activity not objectively assessed outcome |
| Johnson‐Warrington 2016 | physical activity not objectively assessed outcome |
| Jonsdottir 2015 | physical activity not objectively assessed outcome |
| Kato 2017 | attempted to contact author: no physical activity data for control group |
| Kim 2003 | physical activity not objectively assessed outcome |
| Kruis 2014 | physical activity not objectively assessed outcome |
| Langer 2018 | physical activity listed as objectively assessed outcome in registry, no results reported in paper |
| Larraz 2010 | physical activity not objectively assessed outcome |
| Lee 2007 | physical activity not objectively assessed outcome |
| Liang 2018 | physical activity not objectively assessed outcome |
| Liu 2019 | physical activity not objectively assessed outcome |
| Lum 2007 | physical activity not objectively assessed outcome |
| Mahesh 2017 | physical activity not objectively assessed outcome |
| Marques 2019 | not randomised |
| Martinez 2008 | physical activity not objectively assessed outcome |
| McGlone 2006 | observational |
| McMahon 2000 | attempted to contact author: unable to obtain pre‐cross‐over data |
| Mesquita 2017 | no group comparison |
| Moore 2009 | observational |
| Morris 2012 | not randomised |
| Moy 2009 | observational |
| Moy 2012 | observational |
| Murphy 2005 | physical activity not objectively assessed outcome |
| Nagata 2018 | attempted to contact author: unable to obtain pre‐cross‐over data |
| NCT00620022 | contacted author; unable to access pre‐cross‐over data from Novartis |
| NCT01012765 | author correspondence: pre‐cross‐over data not available |
| NCT01380652 | author correspondence: physical activity not objectively assessed outcome |
| NCT01486186 | physical activity not objectively assessed outcome |
| NCT01722370 | author correspondence: pre‐cross‐over data not available |
| NCT01854008 | physical activity not objectively assessed outcome |
| NCT01867970 | author correspondence: unable to obtain results just for participants with COPD |
| NCT01871025 | physical activity not objectively assessed outcome |
| NCT02100709 | study not completed/withdrawn from registry |
| NCT02172794 | physical activity not objectively assessed outcome |
| NCT02629965 | not randomised |
| NCT02656667 | physical activity not objectively assessed outcome |
| NCT03751670 | physical activity not objectively assessed outcome |
| NL1729 | author correspondence: study ceased soon after trial registration, no data |
| Norweg 2006 | physical activity not objectively assessed outcome |
| Nyberg 2017 | not randomised |
| Paneroni 2016 | physical activity not objectively assessed outcome |
| Pasqua 2010 | physical activity not objectively assessed outcome |
| Pinnock 2013 | physical activity not objectively assessed outcome |
| Pitta 2008 | observational |
| Pomidori 2012 | no group comparison |
| Raphael 2014 | physical activity not objectively assessed outcome |
| Ringbaek 2009 | physical activity not objectively assessed outcome |
| Robbins 2000 | physical activity not objectively assessed outcome |
| Rodriguez‐Trigo 2011 | physical activity not objectively assessed outcome |
| Romagnoli 2005 | physical activity not objectively assessed outcome |
| Roman 2013 | physical activity not objectively assessed outcome |
| Schacher 2006 | physical activity not objectively assessed outcome |
| Schönhofer 1997 | observational |
| Senthilnathan 2018 | physical activity not objectively assessed outcome |
| Sewell 2005 | physical activity not objectively assessed outcome |
| Sewell 2010 | no group comparison |
| Sirichana 2013 | no group comparison |
| Soicher 2009 | physical activity not objectively assessed outcome |
| Spencer 2012 | no group comparison |
| Steele 2008 | author correspondence: unable to obtain results just for participants with COPD |
| Strijbos 1991 | physical activity not objectively assessed outcome |
| Sutanto 2018 | physical activity not objectively assessed outcome |
| TCTR20170214002 | physical activity not objectively assessed outcome |
| Troosters 2010 | observational |
| Troosters 2011 | no group comparison |
| Tse 2013 | physical activity not objectively assessed outcome |
| Turnbull 2013 | attempted to contact author: unable to obtain results just for participants with COPD |
| Turner‐Lawlor 2005 | physical activity not objectively assessed outcome |
| U1111‐1169‐0718 | not randomised |
| UMIN000001833 | attempted to contact author: unable to determine if randomised |
| Valenson 2016 | not randomised |
| Voncken‐Brewster 2013 | physical activity not objectively assessed outcome |
| Wilson 2015 | physical activity not objectively assessed outcome |
| Zanini 2002 | physical activity not objectively assessed outcome |
Characteristics of ongoing studies [ordered by study ID]
ACTRN 12616000360415.
| Trial name or title | Telerehabilitation versus traditional centre‐based PR for people with chronic respiratory disease: protocol for a randomised controlled trial (REACH) |
| Methods | DESIGN 2 groups, equivalence trial; COMPARISON intervention vs. intervention; SETTING Alfred Health and Austin Health (metropolitan, Melbourne), Wimmera Health Care Group (regional, Horsham) (Australia); SAMPLE SIZE n = 142 (based on CRQ dyspnea domain) Selection bias: "Participants will be randomly allocated (1:1) …. A computer‐generated, block randomisation scheme will be used with stratification …. Sequence generation will be performed by an individual who is independent of the research team and randomisation will occur using an online database. The randomisation sequence will be concealed from investigators"; Performance bias: "Given the nature of the intervention (exercise training) participants will not be blinded to the intervention", also personnel; Detection bias: "assessor‐blinded" |
| Participants | Primary diagnosis of a chronic lung disease (COPD, bronchiectasis, asthma, ILD); age ≥ 40 years |
| Interventions | DURATION OF INTERVENTION 8 weeks COMMON COMPONENTS Protocol for exercise training prescription and progression Disease‐specific education and collaborative self‐management training
OTHER COMPONENTS encouraged to perform an additional 3 unsupervised sessions each week, home diary reviewed weekly; encouraged to continue with a regular exercise regimen following programme completion INTERVENTION Telerehabilitation SETTING home‐based, remotely supervised, groups of 4 to 6 participants
CONTACT
AEROBIC TRAINING cycle training, 30 minutes, ≥ 2 bouts
STRENGTH TRAINING use equipment readily available in the home environment
INTERVENTION Centre‐based PR SETTING outpatient, groups of 8 to 12 participants CONTACT 2 sessions a week AEROBIC TRAINING cycling and walking, 30 minutes, ≥ 2 bouts
STRENGTH TRAINING use equipment readily available in the home environment
|
| Outcomes | DEVICE GeneActiv (wrist), Wear instructions: 7 days ASSESSMENT TIME POINTS
PRIMARY OUTCOME HRQOL: CRQ dyspnoea domain SECONDARY OUTCOMES
SAFETY "The trial will be monitored by an independent Data Safety Monitoring Board (DSMB) comprising a respiratory physician and two clinical research physiotherapists, with consultation with a statistician as required. The DSMB will review data relating to the primary outcome (CRQ‐D) as well as 6MWD, endurance cycle time and Hospital Anxiety and Depression Scale scores. Data will be presented to the DSMB in a blinded fashion. The DSMB will initially review data at a time 6 months from the commencement of recruitment. Any serious adverse events will be notified immediately to the overseeing ethics committee (Alfred Health) and the relevant site governance committee, as well as to the DSMB. If there are concerns about the safety of participants, the DSMB will make a recommendation to the trial steering committee about continuing, stopping, or modifying the trial." |
| Starting date | Prospectively registered; recruitment commenced August 2016; last participant enrolment January 2019 |
| Contact information | Narelle Cox n.cox@latrobe.edu.au La Trobe University, Melbourne (Australia) |
| Notes | FUNDING "This study is funded by a National Health and Medical Research Council (NHMRC) project grant (GNT1101616). NSC is supported by an NHMRC Early Career Fellowship (GNT 1119970). The NHMRC will not interfere with the independence of the authors in regard to the conduct of the trial and will not delay or prevent publication of the study" N.B. will need data only for COPD participants for inclusion |
ACTRN12615000121561.
| Trial name or title | Effect of opioids on outcomes of PR: a randomised, double‐blind, multi‐site, parallel arm, fixed dose, placebo‐controlled trial of the effects of morphine on exercise capacity and other outcomes of PR in COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 260 (based on 6MWD) Selection bias: "schedules have been developed by an organisation not involved in this study... block randomisation schedule held by the Central Registry Clinical Trials Pharmacist"; Blinding: participants, personnel and outcome assessors |
| Participants | Diagnosis of COPD (post‐bronchodilator FER < 0.7); Age ≥ 18 years; modified MRC dyspnoea scale (score 3 or 4); Stable medications for breathlessness for 1 week; Eligible for PR as judged by the treating physician and the investigator |
| Interventions | DURATION OF INTERVENTION 8 weeks INTERVENTION morphine and PR oral sustained‐release morphine 20 mg in the morning and 2 capsules of blinded laxative INTERVENTION placebo and PR oral placebo capsule and 2 capsules of placebo laxative |
| Outcomes | DEVICE (accelerometer) PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; last participant enrolment September 2017; final recruitment n = 10; "stopped early: participant recruitment difficulties; data collected is being analysed" |
| Contact information | David Currow david.currow@health.sa.gov.au Flinders University, Adelaide (Australia) |
| Notes | FUNDING Commonwealth Department of Health |
ACTRN12616001534471.
| Trial name or title | A behaviour‐change intervention to reduce sedentary time in people with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. sham; SETTING PR waiting lists, Royal Prince Alfred Hospital and Prince of Wales Hospital, Sydney (Australia); SAMPLE SIZE n = 70 (based on sedentary time) |
| Participants | Diagnosis of COPD (FER < 0.7); clinically stable (no change in medication within 4 weeks); can mobilise independently with or without a walking aid; expected to wait ≥ 8 weeks for PR |
| Interventions | DURATION OF INTERVENTION 6 weeks INTERVENTION PAC (behaviour change) INTERFACE weekly
GOALS 2 target behaviours
ACTIVITY TRACKING Jawbone UP3 (wrist), all waking hours, real‐time feedback on prolonged bouts of sedentary time, vibrate after 30 minutes of sustained inactivity CONTENT
SHAM No instructions about physical activity or exercise CONTACT weekly phone calls, 15 minutes CONTENT Enquire about change in health status, directed to contact their local doctor if they have any health issues |
| Outcomes | DEVICE activPAL3, Wear instructions: 7 days, 24 hours a day (remove if skin irritation) ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: sedentary time, number of bouts of sedentary time (> 30 minutes), number of sit‐to‐stand transitions SECONDARY OUTCOMES
|
| Starting date | Anticipated to begin February 2017, complete March 2019 |
| Contact information | Zoe McKeough zoe.mckeough@sydney.edu.au University of Sydney (Australia) |
| Notes | FUNDING "This research study is supported by a Physiotherapy Research Foundation Seeding Grant (2016). The principal researcher Sonia Cheng is supported by a Better Breathing Foundation scholarship." CONFLICT OF INTEREST "The authors have no conflicts of interest." |
ACTRN12616001586404.
| Trial name or title | Effect of a PR programme of 8 weeks duration compared to 12 weeks on exercise capacity in people with COPD (PuRe Duration): a randomised controlled trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 68 (based on ESWT) Selection bias: "will be determined using a computer‐generated randomisation program with a minimisation algorithm... completed for each consenting participant by a person independent of the study"; Blinding: outcome assessor, data analysts |
| Participants | Diagnosis of COPD (FEV1 20% to 80% predicted, FER < 0.7); age 40 to 85 years; referred to PR |
| Interventions |
COMMON INTERVENTION PR SETTING outpatient, hospital CONTACT 2 sessions a week, 60 to 90 minutes AEROBIC TRAINING
STRENGTH TRAINING upper and lower limbs (3 sets, 8 to 10 repetitions) INTERVENTION PR (12 weeks) INTERVENTION PR (8 weeks) |
| Outcomes | DEVICE Actigraph and ActivPAL, Wear instructions: 1 week ASSESSMENT TIME POINTS
PRIMARY OUTCOME Exercise capacity: ESWT SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; first participant enrolment February 2017 |
| Contact information | Joshua Bishop joshua.bishop@sswahs.nsw.gov.au Balmain Hospital, Sydney (Australia) |
| Notes |
ACTRN12617000242325.
| Trial name or title | Does Tai Chi increase cerebral and peripheral oxygenation and do these changes relate to improved cognitive and physical performance in people with COPD? A randomised controlled trial |
| Methods | DESIGN 3 groups; COMPARISONS intervention vs. intervention, intervention vs. no intervention; SAMPLE SIZE n = 66 Selection bias: "sealed opaque envelope"; Blinding: outcome assessors, data analysts |
| Participants | Diagnosis of COPD (GOLD stage ≥ II: FEV1 < 80% predicted; FER < 0.7); age ≥ 55 years |
| Interventions | DURATION OF INTERVENTION 12 weeks COMMON INTERVENTION Exercise and Tai Chi groups SETTING outpatient, group of 4 to 6 participants CONTACT 2 sessions a week, 1 hour TRAINING warm up, exercise, cool down accelerometer (wrist) to record physical activity, exercise log book INTERVENTION Exercise (ergometer) modified Borg Scale (moderate intensity: rating 3 to 4) INTERVENTION Tai Chi (sun style) advised to practice daily at home NO INTERVENTION |
| Outcomes | DEVICE (accelerometer) PRIMARY OUTCOME Exercise capacity: CPET SECONDARY OUTCOMES
|
| Starting date | Prospectively registered February 2017; last data collection September 2018 |
| Contact information | Shirley Ngai shirley.ngai@polyu.edu.hk Hong Kong Polytechnic University (Hong Kong) |
| Notes | FUNDING Research Grants Council, University Grants Committee Secretariat |
ACTRN12617000499381.
| Trial name or title | Randomised controlled trial of a non‐pharmacological integrated care intervention to reduce breathlessness in patients with severe or very severe COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 94 (based on CRQ) Selection bias: "randomisation table created by computer software (i.e. computerised sequence generation)", "sealed opaque envelopes"; Blinding: personnel, outcome assessors |
| Participants | Diagnosis of COPD (GOLD moderate to very severe: FEV1 < 60% predicted; FER < 0.7); age ≥ 18 years; modified MRC dyspnoea scale (score ≥ 2); PR within 1 year or unwilling to attempt PR due to breathlessness |
| Interventions | DURATION OF INTERVENTION eight weeks INTERVENTION range of interventions to address breathlessness
NO INTERVENTION waitlist; basic information about COPD, assessment and correction of inhaler technique, action plan |
| Outcomes | DEVICE (pedometer), Wear instructions: 7 days PRIMARY OUTCOME HRQOL: CRQ mastery domain SECONDARY OUTCOMES
|
| Starting date | Retrospectively registered; first participant enrolment October 2016; registered April 2017; last data collection anticipated June 2021 |
| Contact information | John Wheatley john.wheatley@sydney.edu.au; Tracy Smith Tracy.Smith2@health.nsw.gov.au Westmead Hospital, Sydney (Australia) |
| Notes | FUNDING HCF Research Foundation |
ACTRN12617000653369.
| Trial name or title | Effect of cognitive behaviour therapy on anxiety, depression and breathlessness in patients with COPD: a randomised controlled trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 60 Selection bias: "computer‐generated randomisation table", "sealed opaque envelopes"; Blinding: personnel |
| Participants | Diagnosis of COPD (GOLD severe or very severe : FEV1 < 60% predicted; FER < 0.7); age ≥ 18 years; modified MRC dyspnoea scale (score ≥ 2); Completion of the Westmead Hospital Breathlessness Clinic within 9 months; HADS anxiety or depression score > 8 |
| Interventions | DURATION OF INTERVENTION 10 weeks INTERVENTION Cognitive behaviour therapy CONTACT individual weekly sessions, 1 hour, experienced clinical psychologist SETTING
COMPONENTS
NO INTERVENTION waitlist |
| Outcomes | DEVICE (pedometer) Wear instructions: 7 days ASSESSMENT TIME POINTS
PRIMARY OUTCOME HRQOL: CRQ SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; last participant enrolment anticipated September 2021 |
| Contact information | John Wheatley john.wheatley@sydney.edu.au Westmead Hospital, Sydney (Australia) |
| Notes |
ANZCTR12611000292976.
| Trial name or title | In people with COPD does PR combined with a cognitive behavioural therapy programme for the sensation of breathlessness (BREVE) compared to PR alone improve anxiety and functional exercise capacity at 1, 6 and 12 months? |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SETTING PR at Repatriation General Hospital, Adelaide (Australia); SAMPLE SIZE n = 120 |
| Participants | Diagnosis of COPD (FEV1 < 80% predicted, FER < 0.7); referred and intend to undertake PR |
| Interventions | DURATION OF INTERVENTION 8 weeks COMMON INTERVENTION PR 3 exercise sessions, 1 education session each week INTERVENTION cognitive behavioural therapy with PR INTERVENTION social interaction with PR |
| Outcomes | DEVICE Actigraph GT1X3e ASSESSMENT TIME POINTS
PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; first participant enrolment May 2011; last participant enrolment September 2013 |
| Contact information | Marie Williams marie.williams@unisa.edu.au University of South Australia (Australia) |
| Notes | Physical activity assessed but no results in abstract that can be used for meta‐analysis. Publication pending. |
Beekman 2014.
| Trial name or title | Exacerbations in patients with COPD receiving physical therapy: a cohort‐nested randomised controlled trial (protocol]) Reducing exacerbations in patients with COPD with physiotherapy (DO‐IT COPD) (registry) |
| Methods | DESIGN 2 groups, cohort‐nested; SETTING physical therapy practices, GPs and pulmonologists (southern districts, The Netherlands); SAMPLE SIZE n = 300 (based on exacerbation frequency) |
| Participants | Diagnosis of COPD (GOLD stage II to IV; post‐bronchodilator FEV1 < 80% predicted; FER < 0.7); age > 18 years; AECOPD within 56 days (defined as: unscheduled visit to general practitioner / pulmonologist, hospitalisation, course of antibiotics and/or prednisone); adequate and optimal medication (inhalation) regimen; eligible for reimbursement by health insurance companies for physical therapy (post‐bronchodilator Tiffeneau‐index < 0.6) |
| Interventions |
"The project in total will take 5 years. During the first 2 years of the project, COPD patients will be recruited at participating physiotherapy practices. The included patients will be assigned to one of two treatment arms, and followed for 2 years by means of the COPD electronic documentation system, clinical tests and questionnaires. Duration of the treatment in both the intervention and control group will be one year." INTERVENTION "early physical therapy" starting within 56 days of AECOPD DURATION 1 year SETTING outpatient, physiotherapy practices CONTACT 2 sessions a week, one hour AEROBIC TRAINING "high‐intensity"
STRENGTH TRAINING upper and lower limbs
OTHER COMPONENTS
INTERVENTION optional sham No or very low‐intensity exercise training (if the participant insists on training; ≤ 30 minutes once a week, ≤ 15% maximum; modified Borg scale dyspnoea and fatigue (rating ≤ 2) > 30 minutes of moderately‐intense physical activity ≥ 5 days a week |
| Outcomes | DEVICE Dynaport ASSESSMENT TIME POINTS
SECONDARY OUTCOMES
|
| Starting date | Trial registered August 2009; planned start January 2008; planned completion January 2013; protocol published 2014; registry amended March 2016 |
| Contact information | Emmylou Beekman e.beekman@maastrichtuniversity.nl Maastricht University (The Netherlands) |
| Notes |
ChiCTR1800017405.
| Trial name or title | Effects of PR prescription on COPD patients |
| Methods | DESIGN 5 groups; COMPARISONS intervention vs. intervention, intervention vs. no intervention; SAMPLE SIZE n = 100 Sequence generation: "a random sequence was generated by a simple random grouping method by a staff member who was not directly involved in the inclusion of the objects"; Allocation concealment: " opaque sealed envelope" |
| Participants | Diagnosis of COPD (GOLD); Age 40 to 80 years; clinically stable ≥ 4 weeks; Have not exercised regularly for ≥ 6 months before the study (≥ twice a week) |
| Interventions |
NO INTERVENTION Conventional treatment INTERVENTION Conventional treatment and walking INTERVENTION Conventional treatment and PR INTERVENTION Conventional treatment and upper‐ and lower‐extremities resistance movement INTERVENTION Conventional treatment and upper‐ and lower‐extremities resistance movement + PR |
| Outcomes | PRIMARY OUTCOME Exercise capacity: (not defined) SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; anticipated study completion November 2019 |
| Contact information | Peijun Li lpj0227@163.com Shanghai University of Sport; Xiaodan Liu hzhp403@126.com Shanghai University of Traditional Chinese Medicine (China) |
| Notes |
DRKS00004931.
| Trial name or title | "Medical Vulnerability": Impact of hospital room cooling on vulnerable patients with lung disease during periods of extreme weather (UCaHS) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 300 Blinding: none |
| Participants | Diagnosis of COPD, asthma, pneumonia, lung fibrosis, or pulmonary hypertension; age ≥ 18 years |
| Interventions |
INTERVENTION room with radiant cooling NO INTERVENTION room without radiant cooling |
| Outcomes | SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; first enrolment June 2014; recruitment ongoing (registry) |
| Contact information | Christian Witt christian.witt@charite.de Arbeitsbereich Ambulante Pneumologie der Charité Universitätsmedizin, Berlin (Germany) |
| Notes | FUNDING Deutsche Forschungsgemeinschaft N.B. will need data only for COPD participants for inclusion |
DRKS00010777.
| Trial name or title | The influence of the maintenance of physical activity on mental health of patients with occupational lung diseases after an inpatient rehabilitation in the BG clinic of Falkenstein |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 194 Blinding: none |
| Participants | Recognised occupational diseases; age 18 to 80 years |
| Interventions |
INTERVENTION behaviour‐oriented exercise intervention with inpatient rehabilitation 9 sessions, 45 minutes Influence the participant's attitude towards an active lifestyle with the help of motivational and volitional strategies e.g. action‐planning INTERVENTION inpatient rehabilitation |
| Outcomes | DEVICE ActiGraphGT3x+ TIME POINTS
PRIMARY OUTCOMES Physical activity: (not defined) SECONDARY OUTCOMES
|
| Starting date | Retrospective registration; first enrolment 2016; registered December 2017; recruiting complete, follow‐up continuing |
| Contact information | Petra Wagner petra.wagner@uni‐leipzig.de Universität Leipzig, Sportwissenschaftliche Fakultät, Institut für Gesundheitssport und Public Health (Germany) |
| Notes | FUNDING Deutsche Gesetzliche Unfallversicherung (Germany) N.B. will need data only for COPD participants for inclusion, also to confirm diagnosis |
EUCTR2006‐005534‐20‐GB.
| Trial name or title | Effect of Erdosteine on inflammatory and oxidative biomarkers in sputum and exhaled breath in patients with COPD |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. placebo; SAMPLE SIZE n = 32 Blinding: double |
| Participants | Diagnosis of COPD (GOLD moderate and severe; FER < 0.7, FEV1 < 15% reversibility after 200 µg salbutamol); smoking history (current or former) > 10 pack‐years; age 38 to 80 years; stable COPD (no chest infection requiring antibiotics or oral steroids or both within 2 months); BMI 19 to 32 kg/m2 |
| Interventions |
INTERVENTION Erdosteine (Erdotin) oral capsule PLACEBO |
| Outcomes | DEVICE (pedometer) SECONDARY OUTCOMES
|
| Starting date | Prospective registration; registered November 2007; first enrolment January 2008 |
| Contact information | Imperial College London (UK); no details provided |
| Notes | Unable to identify any publications N.B. will need pre‐cross‐over data for inclusion |
EUCTR2013‐003619‐24‐ES.
| Trial name or title | Benefits of liquid oxygen in COPD patients without evidence of domiciliary oxygen therapy, presenting desaturation on exertion |
| Methods | DESIGN 2 groups, cross‐over COMPARISON intervention vs, placebo; SAMPLE SIZE n = 112 |
| Participants | Diagnosis of COPD (GesEPOC Stadium II to IV/GOLD III to IV: FEV1 < 80%, FER < 0.7, TLC > 80% predicted); clinical stability for 1 month; optimised medical treatment; do not meet conventional criteria for LTOT (SEPAR Guide, GOLD); SpO2 < 88% on 6MWT; active life |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION Liquefied medicinal oxygen (Visionox ® device) Concentration number: 1 to 6 PLACEBO |
| Outcomes | DEVICE (accelerometer) ASSESSMENT TIME POINT End intervention: 12 weeks PRIMARY OUTCOME HRQOL: CAT SECONDARY OUTCOMEs
|
| Starting date | Prospective registration; global end of the trial February 2019 "prematurely ended" |
| Contact information | Maria Rosa Güell‐Rous mguellr@santpau.cat Grup ROV de la Societat Catalana de Pneumologia (Spain) |
| Notes | FUNDING Sociedad Española de Neumología y Cirugía Torácica (Spain) N.B. will need pre‐cross‐over data for inclusion |
EUCTR2016‐001238‐89‐ES.
| Trial name or title | Iron deficiency in patients with COPD: impact of topping with iron carboxymaltose. FACE study; Assessment in patients with ferinject and iron deficiency COPD to improve exercise tolerance |
| Methods | DESIGN 2 groups COMPARISON intervention vs. placebo Blinding: single |
| Participants | Diagnosis of COPD; age 45 to 80 years; clinically stable ≥ 8 weeks (no change in pharmacotherapy treatment since last antibiotics intake or systemic steroids or both for AECOPD) |
| Interventions |
INTERVENTION ferric carboxymaltose (Ferinject 50 mg/ml) solution for injection PLACEBO |
| Outcomes | DEVICE SenseWear Pro2, Wear instructions: 7 days ASSSESSMENT TIME POINT 4 weeks PRIMARY OUTCOME Exercise capacity: endurance time (cycle ergometer, 75%) SECONDARY OUTCOMES
|
| Starting date | Prospective registration; first enrolment June 2016; "data collection is anticipated to be completed by the end of 2019" |
| Contact information | Diego Rodriguez Chiaradía DARodriguez@parcdesalutmar.cat Consorci Mar Parc de Salut de Barcelona (Spain) |
| Notes |
EUCTR2016‐001805‐18‐SE.
| Trial name or title | A randomised, placebo‐controlled, blinded, cross‐over, pilot study to explore safety and efficacy of NBMI treatment of patients with mild, moderate and severe COPD |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. placebo; SAMPLE SIZE: n = 12 Blinding: "double blind" |
| Participants | Diagnosis of COPD (GOLD stages I to III; post‐bronchodilator FEV1 > 30% predicted, FER < 0.7); smoking history ≥ 10 pack‐years (ex‐smokers > 6 months); age 45 to 75 years; CAT score > 10; bronchitis with cough and sputum production during many days of the last month, and ≥ 3 months during the last year |
| Interventions | STUDY DURATION 14 days INTERVENTION Emeramide (NBMI) Capsule, oral PLACEBO |
| Outcomes | PRIMARY OUTCOME Adverse events: frequency and severity SECONDARY OUTCOMES
EXPLORATORY OUTCOME Physical activity: (not defined) |
| Starting date | Prospective registration; global end of the trial May 2018 |
| Contact information | Ragnar Klingberg ragnar.klingberg@emeramed.com NBMI Science AB, Stockholm (Sweden) |
| Notes | FUNDING NBMI Science AB N.B. will need pre‐cross‐over data |
Fastenau 2014.
| Trial name or title | Effectiveness of a physical exercise training programme COPD in primary care: a randomised controlled trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. sham; SETTING primary care, Limburg (The Netherlands); SAMPLE SIZE based on 6MWD |
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA Physical exercise training programme or rehabilitation therapy in the past year, respiratory tract infections ≤ 8 weeks, serious comorbid conditions which may interfere with exercise BASELINE CHARACTERISTICS
AGE mean 62 (SD 9) years; SEX 27 (59%) male; FEV1 mean 74 (SD 15) % predicted
AGE mean 63 (SD 11) years; SEX 17 (39%) male; FEV1 mean 74 (SD 12) % predicted |
| Interventions | DURATION OF INTERVENTION four months INTERVENTION exercise training SETTING physiotherapy practice CONTACT 2 supervised and 1 unsupervised training sessions a week
AEROBIC TRAINING endurance/interval treadmill training
STRENGTH TRAINING upper and lower limbs (2 to 3 sets, 8 to 12 repetitions)
OTHER COMPONENTS
SHAM "exercise training" SETTING physiotherapy practice CONTACT 1 session a week, 30 minutes TRAINING modified Borg scale dyspnoea and fatigue (rating ≤ 2) OTHER COMPONENTS
|
| Outcomes | DEVICE Dynaport, Wear instructions: 3 days and nights ASSESSMENT TIME POINTS
PRIMARY OUTCOME Exercise capacity: 6MWD (30 metre corridor was not always feasible, minimal corridor length 10 metres) SECONDARY OUTCOMES Physical activity: step count, MVPA time, time walking, time active, movement intensity during walking, PAL
|
| Starting date | Registered 2008, planned closing 2010, protocol published 2014, abstract published 2015 |
| Contact information | Annemieke Fastenau annemieke.fastenau@maastrichtuniversity.nl Maastricht University (The Netherlands) |
| Notes | FUNDING "The funding of this study is provided by the MUMC MOVE programme of Maastricht University, and an unconditional grant of Boehringer‐Ingelheim, the Netherlands" CONFLICT OF INTEREST "The authors declare that they have no competing interests." email correspondence with author: results are under preparation for publication and advised to use abstract and protocol only pending publication of results |
ISRCTN11017699.
| Trial name or title | Histological, cellular and molecular investigation of steroid responsiveness in COPD: the HISTORIC study |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 188 Blinding: double |
| Participants | Diagnosis of COPD (GOLD groups B to D); smoking history (current or former) ≥ 10 pack‐years; age ≥ 40 years; no AECOPD or any respiratory infection requiring medical attention or leading to a change in medication within 4 weeks; unchanged respiratory medication regimen within 8 weeks; ≥ 1 AECOPD in previous year |
| Interventions | DURATION OF INTERVENTION 12 months RUN‐IN PERIOD 6 weeks LAMA (aclidinium 400 mcg), LABA (formoterol 12 mcg) and ICS (budesonide 400 mcg), twice daily INTERVENTION ICS, LAMA, LABA (groups A1 and B1) INTERVENTION placbo, LAMA, LABA (groups A2 and B2) |
| Outcomes | ASSESSMENT TIME POINTS
SECONDARY OUTCOME MEASURES
|
| Starting date | Prospective registration; overall trial end April 2021 |
| Contact information | Daiana Stolz Daiana.Stolz@usb.ch University Hospital Basel (Switzerland) |
| Notes | FUNDING AstraZeneca |
ISRCTN13899108.
| Trial name or title | The effectiveness of a physical activity intervention versus PR on cardiovascular risk markers for individuals with COPD: a feasibility study (PARC) |
| Methods | DESIGN: 3 groups; COMPARISON intervention vs. intervention, intervention vs. no intervention; SAMPLE SIZE n = 60 Selection bias: www.sealedenvelope.com |
| Participants | Diagnosis of COPD; age 40 to 85 years |
| Interventions | DURATION OF INTERVENTION 6 weeks INTERVENTION PAC FitBit Charge 2 (heart rate and fitness wristband); tracks activity and exercise; send data to investigators (physical activity level, intensity, time) CONTACT send messages to participant through device FEEDBACK/GOAL SETTING target calculation: mean of the 4 most active days plus 500 steps
INTERVENTION PR SETTING outpatient, group CONTACT 2 sessions a week, 2 hours CONTENT exercise training and education NO INTERVENTION |
| Outcomes | DEVICE Actigraph; Wear instructions: 1 week SECONDARY OUTCOMES
|
| Starting date | Retrospectively registered; registered April 2019; study dates January 2018 to October 2020 |
| Contact information | Sally Singh sally.singh@uhl‐tr.nhs.uk Glenfield Hospital, Leicester (UK) |
| Notes | FUNDING National Centre for Sport and Exercise Medicine, Loughborough University; University Hospital Leicester NHS Trust (UK) |
ISRCTN15949009.
| Trial name or title | The role of nasal high‐flow to reduce 30‐day hospital readmissions following severe exacerbations of COPD: a mixed‐methods feasibility study: NHF Post‐AECOPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 80 |
| Participants | Emergency hospital admission with a primary diagnosis of AECOPD to St Thomas’ Hospital, London; smoking history ≥ 10 pack‐years; age 40 to 80 years; BMI ≤ 35 kg/m2; home environment safe for visits; live in catchment area |
| Interventions | "followed up for 30 days after hospital discharge" INTERVENTION nasal high‐flow device, daily NO INTERVENTION |
| Outcomes | DEVICE wrist‐worn physical activity monitor; Wear instructions: measured continuously for 30‐day follow‐up period SECONDARY OUTCOMES
|
| Starting date | Retrospectively registered; registered February 2019; study dates September 2018 to August 2021 |
| Contact information | Nicholas Hart Nicholas.hart@gstt.nhs.uk Rebecca D’Cruz Rebecca.DCruz@gstt.nhs.uk Guy’s and St Thomas’ NHS Foundation Trust (UK) |
| Notes | FUNDING National Institute for Health Research (UK) |
ISRCTN17942821.
| Trial name or title | A self‐management programme of activity coping and education ‐ SPACE for COPD(C) ‐ in primary care: the protocol for a pragmatic trial |
| Methods | DESIGN 2 groups COMPARISON intervention vs. no intervention; SETTING primary care, COPD registers, Respiratory Biomedical Research Unit at University Hospitals of Leicester (UK); SAMPLE SIZE n = 193 (based on CAT) |
| Participants | Diagnosis of COPD (GOLD) |
| Interventions | DURATION OF INTERVENTION 5 months INTERVENTION SPACE for COPD(C) SETTING group‐based, up to 10 participants, community venues, times and locations to suit participants CONTACT 6 sessions, 2 hours CONTENT
NO INTERVENTION "If referred to PR duing study, they will not be denied access to the programme; however, they will not be included in the final analysis due to use of 'intention‐to‐treat' analysis" |
| Outcomes | DEVICE SenseWear Armband [back of right arm], Wear instructions: seven days, 24 hours ASSESSMENT TIME POINTS
PRIMARY OUTCOME HRQOL: CAT SECONDARY OUTCOMES
|
| Starting date | Retrospective registration; start February 2015, end June 2017; preliminary results available October 2018 from trial registry; HRQOL and exercise capacity, not physical activity data |
| Contact information | Sally Singh Sally.Singh@uhl‐tr.nhs.uk University Hospital Leicester NHS Trust (UK) |
| Notes | FUNDING National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East Midlands (UK) |
ISRCTN19684749.
| Trial name or title | CELEB trial: Comparative effectiveness of lung volume reduction surgery for emphysema and bronchoscopic lung volume reduction with valve placement: a protocol for a randomised controlled trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SETTING outpatient clinics at hospital sites which have an established multidisciplinary team meeting dedicated to identifying suitable candidates for lung volume reduction (UK); SAMPLE SIZE n = 76 (based on BODE score) Random sequence (low risk): "If the person has a CV negative lobar target for treatment they will be immediately allocated randomly to one of the treatment arms, using an online system. Randomisation will be on a 1:1 basis based on a computer‐generated random sequence with random block sizes generated by Sealed Envelope (London, UK); Allocation concealment (high risk): Patients, the study coordinator and those providing clinical care will not be blinded to treatment allocation; Blinding of participants (high risk): unable to blind participants to intervention; Blinding of personnel (low risk): Investigators and all individuals involved in trial conduct or analysis remained blinded to the randomized treatment until after data lock; Detection bias (low risk): The primary endpoint measures will be performed by staff blinded to treatment allocation and patients will be asked not to reveal this in order to reduce bias." |
| Participants | Diagnosis of COPD (FEV1 < 60% predicted); significant hyperinflation (TLC > 100% predicted, RV > 170% predicted); ex‐smoker > 3 months; Age ≥ 18 years; modified MRC dyspnoea scale (score ≥ 3); CT scan: intact interlobar fissures (> 90%) and heterogeneous emphysema |
| Interventions |
INTERVENTION lung volume reduction surgery unilateral video‐assisted thoracoscopic surgery approach intended to remove the most emphysematous area of lung high dependency unit postoperatively, management will include attention to wound discomfort, management of chest drains and prompt mobilisation. INTERVENTION Bronchoscopic lung volume reduction with valve placement bronchoscopy; procedures including valve adjustment and replacement will be permitted to ensure treatment is optimised. |
| Outcomes | DEVICE DynaPort MoveMonitor, Wear instructions: 7 days ASSESSMENT TIME POINTS
PRIMARY OUTCOME Exercise capacity: ISWD SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; opened for recruitment in October 2016; overall trial end March 2020 |
| Contact information | Nicholas Hopkinson n.hopkinson@ic.ac.uk Imperial College, London (UK) |
| Notes | FUNDING "The study is funded by a grant to Royal Brompton and Harefield NHS Foundation Trust, from the NIHR, through the Research for Patient Benefit scheme (PB‐PG‐1014‐35051). Imperial College, London will support the reporting of this manuscript. Trial sponsor representative: Patrik Pettersson, Royal Brompton and Harefield NHS Foundation Trust (RB&HFT), Royal Brompton Hospital." CONFLICT OF INTEREST "Royal Brompton has received reimbursement of clinical trial expenses from PneumRx, PulmonX, Olympus, Uptake Medical, Holaira and Creo Medical" |
ISRCTN27860457.
| Trial name or title | ON‐EPIC Oral nitrate supplementation to enhance PR in COPD |
| Methods | DESIGN 2 groups, cross‐over (registry); COMPARISON intervention vs. intervention; SETTING Royal Brompton and Harefield NHS Foundation Trust (UK); SAMPLE SIZE total final enrolment n = 165 Blinding: double |
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS (n = 166, 122 completed) AGE mean 68 (SD 10) years; SEX not reported; FEV1 mean 49 (SD 17)% predicted |
| Interventions |
COMMON INTERVENTIONS
DURATION 8 weeks CONTACT 2 sessions a week CONTENT supervised, strength and endurance training, home exercise programme
INTERVENTION Nitrate‐rich beetroot juice (containing 12.9 mmol nitrate) with PR INTERVENTION Nitrate‐deplete beetroot juice with PR |
| Outcomes | ASSESSMENT TIME POINTS
PRIMARY OUTCOME Exercise capacity: ISWD SECONDARY OUTCOMES
|
| Starting date | Prospectively registered September 2014; study dates January 2015 to April 2018; intention to publish September 2019 |
| Contact information | Nicholas Hopkinson n.hopkinson@ic.ac.uk Imperial College, London (UK) |
| Notes | FUNDING The JP Moulton Medical Foundation (UK) N.B. need to confirm: objective assessment of physical activity for inclusion; if cross‐over study, will need pre‐cross‐over data |
ISRCTN45695543.
| Trial name or title | Training to Improve Dyspnoea (TIDe): a randomised controlled trial to investigate the use of high frequency airway oscillations as training to relieve dyspnoea in COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. sham; SAMPLE SIZE n = 106 (based on CRQ) Selection bias: "web‐based programme (www.sealedenvelope.com)", "randomisation will be allocated by an unblinded assessor and concealed from the patient and the outcome assessor"; Performance bias: "randomisation will be... concealed from the patient" ; Detection bias: "randomisation will be... concealed from the outcome assessor" |
| Participants | Diagnosis of COPD (FER < 0.7); modified MRC dyspnoea scale (score ≥ 2) |
| Interventions | DURATION OF INTERVENTION 8 weeks INTERVENTION Aerosure Medic (HFAO device) battery‐operated, dual‐action device providing oscillations at 25 Hz flow resistance from 0 to 50 cmH2O dependent on the participant’s flow rate inhale and exhale through a mouthpiece deeply for ≥ 5 minutes, 3 times a day SHAM device appears identical, valve is removed (no flow resistance or oscillations) inhale and exhale through a mouthpiece deeply for ≥ 5 minutes, 3 times a day |
| Outcomes | DEVICE ActiGraph GT3X (around the waist, above right hip), Wear instructions: 7 days ASSESSMENT TIME POINTS
PRIMARY OUTCOME HRQOL: CRQ dyspnoea domain SECONDARY OUTCOMES
EXPLORATORY Physical activity: (not defined) |
| Starting date | Retrospectively registered; study dates June 2017 to December 2020 |
| Contact information | Enya Daynes enya.daynes@uhl‐tr.nhs.uk Glenfield Hospital (UK) |
| Notes | FUNDING Actegy Ltd, Bracknell (UK) |
ISRCTN80279999.
| Trial name or title | Domiciliary application of non‐invasive positive pressure ventilation with average volume assured pressure support to subjects with COPD who remain hypercapnic following the application of non‐invasive positive pressure ventilation (NPPV) for an acute exacerbation: AVAPS‐COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 60 |
| Participants | Diagnosis of COPD (European Respiratory Society/American Thoracic Society); age 50 to 80 years; minimum of 48 hours without NPPV after using NPPV or invasive ventilation in hospital during AECOPD; persistent hypercapnia (PaCO2 ≥ 50 mmHg, < 65 mmHg; pH > 7.32; room air) |
| Interventions | DURATION OF INTERVENTION 1 year INTERVENTION Long‐term domiciliary non‐invasive positive pressure ventilation with average volume assured pressure support ventilatory support function that dynamically determines the pressure support level, which generates the target or control level of exhaled tidal volume by producing a gradual pressure change based on the preceding several breaths NO INTERVENTION |
| Outcomes | DEVICE Actiwatch ASSESSMENT TIME POINTS
SECONDARY OUTCOMES
|
| Starting date | Retrospectively registered; registered December 2008; first enrolment November 2008; trial end November 2010 |
| Contact information | JL Pepin JPepin@chu‐grenoble.fr Laboratoire Exploration Fonctionnelle Cardio‐Respiratoire, Grenoble (France) |
| Notes | FUNDING Respironics International, Inc. (France) email sent 23 August 2019 |
NCT01037387.
| Trial name or title | Effect of the noninvasive mechanical ventilation on the daily physical activity and the inflammatory biomarkers in stable patients with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 50 Blinding: none |
| Participants | Diagnosis of COPD (post‐bronchodilator FEV1 < 45% predicted, FER < 0.7 for ≥ 6 months); smoking history > 15 pack‐years; age 45 to 75 years; clinically stable ≥ 3 months; pharmacological treatment optimised within 2 years; baseline pH 7.35 to 7.45, PaCO2 > 45 mmHg (room air) |
| Interventions |
INTERVENTION nocturnal BiPAP (IPAP 10 to 20 cmH2O, EPAP 4 to 6 cmH2O) NO INTERVENTION |
| Outcomes | PRIMARY OUTCOME Physical activity: (not defined) SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start December 2009; estimated study completion June 2021 |
| Contact information | Francisco Garcia‐Rio fgr01m@gmail.com Hospital Universitario La Paz, Madrid (Spain) |
| Notes |
NCT01537627.
| Trial name or title | Effects of a long‐term physical training programme on pulmonary and systemic aspects in patients with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 82 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD (GOLD); age ≥ 40 years; clinical stability (absence of AECOPD for 3 months); absence of any unstable/severe cardiac, osteoarticular or neuromuscular disorders which could limit physical activities in daily life; no participation in PR within 1 year |
| Interventions | DURATION OF INTERVENTION 6 months INTERVENTION Low‐intensity training 3 sessions a week, 1 hour Calisthenic and breathing exercises; 7 different sets; progressive degrees of difficulty INTERVENTION High‐intensity training 3 sessions a week Aerobic exercises (treadmill and cyclo‐ergometer) ≥ 20 minutes
Resistive exercises upper and lower limbs (3 sets, 8 repetitions)
|
| Outcomes | PRIMARY (up to 4 years) Physical activity: time in activities ≥ moderate intensity SECONDARY (up to 4 years)
|
| Starting date | Retrospectively registered; first posted February 2012; study start November 2009; estimated study completion July 2018 |
| Contact information | Fabio Pitta fabiopitta@uol.com.br Hospital Universitário Norte do Paraná, Londrina (Brazil) |
| Notes | Sponsor: Universidade Estadual de Londrina |
NCT01539434.
| Trial name or title | Behavioural medicine intervention to maintain physical capacity and level of physical activity in patients with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 100 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD; age 40 to 80 years; participated in 12 weeks of physical training at Uppsala and Umeå university hospitals |
| Interventions |
INTERVENTION PAC personal meeting with the physiotherapist: advice about the value of physical activity, recommendations on how to be physically active. motivational interviewing telephone calls
NO INTERVENTION personal meeting with the physiotherapist: advice about the value of physical activity, recommendations on how to be physically active. |
| Outcomes | PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Actual study start September 2010; estimated study completion December 2020 |
| Contact information | Margareta Emtner margareta.emtner@neuro.uu.se Uppsala University, Sweden |
| Notes |
NCT01783808.
| Trial name or title | Effects on exercise capacity, physical activity and quality of life using ambulatory oxygen in patients with COPD who desaturate only during exercise |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 144 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD (post‐bronchodilator FEV1 < 80% predicted, FER < 0.7); non‐smoker (smoke‐free ≥ 6 months); age ≥ 18 years; no AECOPD within 4 weeks; PaO2 > 8 kilopascal at rest; SpO2 ≤ 88%, fall ≥ 4% during 6MWT (room air); SpO2 ≥ 92% during a walk test in self‐selected pace with supplemental oxygen |
| Interventions | DURATION OF INTERVENTION 6 months COMMON INTERVENTION PAC stimulated by a physiotherapist to be more physically active; “a behavioural medicine intervention” INTERVENTION supplemental oxygen during physical activity with PAC INTERVENTION PAC |
| Outcomes | DEVEICE (accelerometer) PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOME Physical activity: “physical activity level” OTHER OUTCOMES HRQOL: EQ5D, SGRQ, CAT |
| Starting date | Retrospective registration; actual study start November 2012; estimated study completion December 2020 |
| Contact information | Margareta Emtner margareta.emtner@neuro.uu.se Uppsala University (Sweden) |
| Notes | Collaborators: Umeå University, Karolinska Institutet, University of California, Los Angeles |
NCT01905982.
| Trial name or title | The effect of reflective breathing therapy compared with conventional breathing therapy on dyspnoea, activity and parasympathetic activities in patients with COPD III to IV |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 44 Blinding: none |
| Participants | Diagnosis of COPD (GOLD stage III and IV); age 50 to 75 years; inpatient rehabilitation |
| Interventions |
INTERVENTION Conventional breathing therapy, 4 sessions, 30 minutes INTERVENTION Reflectory breathing therapy, 2 sessions, 60 minutes |
| Outcomes | DEVICE Sensewear, Wear instruction: 48 hours post‐intervention SECONDARY OUTCOMES
|
| Starting date | Prospective registration; estimated study completion March 2020 |
| Contact information | Klaus Kennkklenn@schoen‐klinik.de Klinikum Berchtesgadener Land der Schön‐Kliniken (Germany) |
| Notes | N.B. will need pre‐cross‐over data for inclusion |
NCT01998724.
| Trial name or title | Long‐term Exercise After PR (LEAP): design and rationale of a randomised controlled trial of Tai Chi |
| Methods | DESIGN 3 groups, participants will be enrolled in cohorts; COMPARISON intervention vs. intervention, intervention vs. no intervention; SETTING PR at Beth Israel Deaconess Medical Center, VA Boston Healthcare System, Brigham and Women's Hospital, and Boston Medical Center, as well as referrals from other sites in Massachusetts (USA); SAMPLE SIZE n = 90 (based on 6MWD) |
| Participants | Diagnosis of COPD (FER < 0.7 or CT evidence of emphysema); age > 40 years; Completion of standard PR ≥ 8 weeks duration within 24 weeks |
| Interventions | DURATION OF INTERVENTION 24‐week intervention, 1 year follow‐up INTERVENTION Tai Chi CONTACT total 36 classes
CONTENT 5 formal movements
INTERVENTION Group walking CONTACT total 36 classes
CONTENT Same approximate amount of physical activity (low to moderate aerobic exercise with gentle stretching)
NO INTERVENTION "general recommendations for exercise at home" e.g. walking in the community, local gym, equipment at facility‐based PR programme reommend strength training 3 to 4 sessions a week, 20 minutes Participants are allowed to participate in the maintenance programmes of their usual PR programme |
| Outcomes | DEVICE Omron HJ‐720ITC (pedometer) (waist), Wear instructions: waking hours for 14 days, excluding periods of bathing or other water activities |
| Starting date | Retrospective registration; study start August 2012; first posted December 2013; final data collection for primary outcome measure June 2018 |
| Contact information | Marilyn Moy marilyn.moy@va.gov VA Boston Healthcare System (USA) |
| Notes | FUNDING "This study was supported by an award from the National Center for Complementary and Integrative Health, National Institutes of Health (Moy and Yeh, R01AT006358)." CONFLICT OF INTEREST "Peter Wayne is the founder and sole owner of the Tree of Life Tai Chi Center. Peter Wayne's interests were reviewed and are managed by the Brigham and Women's Hospital and Partners HealthCare in accordance with their conflict of interest policy." |
NCT02099799.
| Trial name or title | The effect of physical activity promotion on short‐ and long‐term outcomes in COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 185 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD (FER < 0.70 or chest CT evidence of emphysema); Age ≥ 40 years; Medical clearance to participate in an exercise programme; Active email account and can check email at least weekly; Access to a computer with Internet connection or willing to come to use study computers; Pedometer with > 90% accuracy compared to manual counts on short clinic walk |
| Interventions |
INTERVENTION Pedometer and PAC Website: feedback, goal setting, educational and motivational content and community forum NO INTERVENTION Verbal instructions and written materials about exercise |
| Outcomes | DEVICE (pedometer) PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Prospective registration; estimated study completion February 2020 |
| Contact information | Marilyn Moy marilyn.moy@va.gov VA Boston Healthcare System (USA) |
| Notes |
NCT02205242.
| Trial name or title | BACE Trial ‐ physical activity as a crucial patient‐reported outcome in COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. placebo Blinding: participant, care provider, investigator |
| Participants | Diagnosis of COPD (clinical history OR spirometry); smoking history ≥ 10 pack‐years; age ≥ 18 years; current hospitalisation for potential infectious AECOPD treated with standard therapy; history of at least 1 AECOPD during the last year (prior to the current hospital admission) with systemic steroids and or antibiotics, or both; ECG at admission |
| Interventions |
INTERVENTION Azithromycin (oral) n = 250 Day 1 to Day 3: 500 mg azithromycin once a day; Day 4 to Day 90: 250 mg azithromycin once every 2 days PLACEBO (oral) n = 250 Day 1 to Day 3: 500 mg placebo once a day; Day 4 to Day 90: 250 mg placebo once every 2 days |
| Outcomes | DEVICE Dynaport, Wear instructions: 7 days BOTH GROUPS physical activity assessed in subgroups (n = 30 each) Baseline (post‐discharge from hospital), 3 months, 9 months PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOME Physical activity: step count, time MVPA, time sedentary, time active |
| Starting date | Prospective registration; estimated study completion April 2018 |
| Contact information | Wim Janssens wim.janssens@uzleuven.be KU Leuven (Belgium) |
| Notes | Collaborator: Pro‐Active Medical Pty Ltd |
NCT02398643.
| Trial name or title | Examine the impact of early chronic disease management education following hospital discharge in acute exacerbation of COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 150 Blinding: none |
| Participants | Diagnosis of COPD; age 50 to 85 years; admitted to the pulmonary ward for AECOPD |
| Interventions |
INTERVENTION Early pulmonary education focused education sessions by Certified Respiratory Educator within 2 weeks of discharge NO INTERVENTION general education sessions by Certified Respiratory Educator within 1 month of discharge |
| Outcomes | DEVICE (accelerometer) (wrist or upper arm) ASSESSMENT TIME POINTS
SECONDARY
|
| Starting date | Prospectively registered; estimated study completion December 2019 |
| Contact information | Brandie Walker blthorla@ucalgary.ca Lisette Machado lmachado@ucalgary.ca University of Calgary (Canada) |
| Notes |
NCT02455206.
| Trial name or title | Effect of counselling during PR on self‐determined motivation towards physical activity in people with COPD – protocol of a mixed‐methods study |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SETTING outpatient PR, Canton Hospital Winterthur (Switzerland); SAMPLE SIZE n = 62 Blinding: single |
| Participants | Diagnosis of COPD (GOLD stages B to D); age 40 to 90 years |
| Interventions |
COMMON INTERVENTION Pneumofit (PR) DURATION 12 weeks SETTING outpatient CONTACT 3 sessions a week, 90 minutes (36 sessions) AEROBIC TRAINING cycle ergometer or treadmill
STRENGTH TRAINING seated
INTERVENTION PAC with PR CONTACT Week 12 of PR
CONTENT motivational interviewing techniques INTERVENTION PR |
| Outcomes | DEVICE SenseWear Pro (upper right arm wear); Wear instructions: 7 consecutive days (remove for bathing or showering) ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOMES
|
| Starting date | Prospectively registered May 2015; study start October 2015, final data collection for primary outcome measure January 2020 |
| Contact information | Anne‐Kathrin Rausch‐Osthoff rauh@zhaw.ch Zurich University of Applied Sciences (Switzerland) |
| Notes | FUNDING "This study is funded by the Swiss Lung Association. Funding includes devices (accelerometer) and some of the working hours." CONFLICT OF INTEREST "All authors declare that they have no competing interests." |
NCT02471235.
| Trial name or title | Short‐course PR and exacerbations and activity of COPD patients over 1 year |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention Blinding: none |
| Participants | INCLUSION CRITERIA
EXCLUSION CRITERIA
BASELINE CHARACTERISTICS (TOTAL n = 136; intervention n = 68, usual care n = 68) AGE mean 75 (SD 7) years; SEX 132 (97%) males; FEV1 mean 47 (SD 16)% predicted |
| Interventions | DURATION OF INTERVENTION 12 months INTERVENTION exercise training SETTING outpatient physiotherapy training CONTACT
NO INTERVENTION |
| Outcomes | DEVICE Actigraph GT3XP ASSESSMENT TIME POINT End intervention: 12 months SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start July 2015; study completion November 2018 |
| Contact information | Fanny Ko fannyko@cuhk.edu.hk The Chinese University of Hong Kong (Hong Kong) |
| Notes | Need physical activity data "At 12 months, there was no change in activity measured by steps per day between the IG and UG groups" [abstract] |
NCT02478359.
| Trial name or title | Patient‐centered physical activity coaching in COPD (Walk On!): a study protocol for a pragmatic randomised controlled trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; ; SETTING 14 hospitals, 16 medical services, Kaiser Permanente Southern California (USA); SAMPLE SIZE actual recruitment n = 2702 (composite primary outcome of all‐cause hospitalisations, emergency department visits, observational stays and death) |
| Participants | Any COPD‐related hospitalisation, emergency department visit or observational stay within 12 months; on at least a bronchodilator or steroid inhaler prior to the encounter or if not on an inhaler, previous COPD diagnosis; age > 40 years |
| Interventions | DURATION OF INTERVENTION 12 months INTERVENTION PAC 'Walk On!' Week 0 In‐person individual/group orientation visit
Month 1 ‘intensive’ weekly coaching phone calls
Months 2 to 12
NO INTERVENTION access to all health services e.g. primary, specialty care, PR, health education and lifestyle programmes No instructions to exercise only informed that their medical centre is participating in a study to improve outcomes for members with COPD |
| Outcomes | DEVICES
SECONDARY OUTCOMES
|
| Starting date | Study start June 2015; estimated study completion December 2018 |
| Contact information | Huong Nguyen Huong.Q2.Nguyen@kp.org Kaiser Permanente, Pasadena, California (USA) |
| Notes | FUNDING "Funding in part by the Patient‐Centered Outcomes Research Institute, PCORI 1403‐14117, 2015–2018 to Dr. Nguyen" |
NCT02557178.
| Trial name or title | Home‐based health management of COPD patients |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. no intervention ; SAMPLE SIZE n = 166 Blinding: none |
| Participants | Diagnosis of COPD (GOLD stage II, III or IV); smoking history (current of former) ≥ 10 pack‐years; age ≥ 40 years, hospitalised for AECOPD |
| Interventions |
INTERVENTION PAC: activity monitor plus health coaching Actigraph daily during weeks 1, 9, and 17; daily steps and activity will be measured Health coaching NO INTERVENTION |
| Outcomes | DEVICE SenseWear Pro PRIMARY OUTCOMES
|
| Starting date | Prospective registration; actual study completion March 2019 |
| Contact information | Sara Seifert, Minnesota Health Solutions (USA) |
| Notes | Collaborators: National Heart, Lung, and Blood Institute (NHLBI), Mayo Clinic, “Minnesota HealthSolutions Corporation (MHS) proposes to develop and evaluate a program to motivate and monitor people with COPD to complete home exercise as part of PR” N.B. will need pre‐cross‐over data for inclusion |
NCT02667171.
| Trial name or title | COPD online‐rehabilitation versus conventional COPD rehabilitation – rationale and design for a multicenter randomised controlled trial study protocol (CORe trial) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SETTING Respiratory and Physiotherapy Departments of 8 hospitals in the capital region of Denmark: Amager, Hvidovre, Bispebjerg, Frederiksberg, Herlev, Gentofte, Frederikssund and Hillerød University Hospitals, University of Copenhagen (Denmark); SAMPLE SIZE n = 134 (based on 6MWD) Blinding: assessor and data analyst blinded |
| Participants | Diagnosis of COPD (severe or very severe; FEV1 < 50% predicted ; FER < 0.7); modified MRC dyspnoea scale (score ≥ ) |
| Interventions |
COMMON COMPNENT life with COPD, participants topics, medication, daily activity, nutrition, smoking cessation, respiratory and relaxation exercises INTERVENTION online rehabilitation DURATION 10 weeks SETTING home‐based, web‐cam, group of 4 to 8 participants CONTACT 3 sessions a week, 1 hour EXERCISE TRAINING
EDUCATION 25 minutes INTERVENTION centre‐based rehabilitation DURATION 8 to 12 weeks SETTING outpatient, group CONTACT 2 sessions a week, 1 to 2 hours EXERCISE TRAINING 1 hour
EDUCATION 1 session a week, 90 minutes |
| Outcomes | DEVICE ActivPAL
ASSESSMENT TIME POINTS
PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Study start March 2016, scheduled to continue until December 2017 |
| Contact information | Henrik Hansen Henrik.hansen.09@regionh.dk; henrikhanseninfo@gmail.com University of Copenhagen, Copenhagen (Denmark) |
| Notes | FUNDING "This research project received specific grants from the Danish Lung Foundation (Charitable funding), Telemedical Center Regional Capital Copenhagen (governmental funding), TrygFonden foundation (Charitable funding). The Grants covers expenses conducting the trial, salary for project employed, and University fee for the PhD education for Henrik Hansen." CONFLICT OF INTEREST "The authors declare that they have no competing interests." |
NCT02691104.
| Trial name or title | Use of the SMART COPD physical activity app in PR: a randomised feasibility study |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 30 Blinding: none |
| Participants | Diagnosis of COPD; age ≥ 18 years; attending PR in Sheffield, Rotherham or Doncaster |
| Interventions |
INTERVENTION PAC (app) with PR and pedometer During PR: app and pedometer Post‐PR: app and pedometer
App and pedometer: set physical activity goals, monitor progress, provide feedback INTERVENTION PR and pedometer During PR: blinded pedometer Post‐PR (8 weeks): blinded pedometer |
| Outcomes | DEVICE Fitbit® Charge pedometer SECONDARY OUTCOMES
|
| Starting date | First posted February 2016; study start January 2016; actual study completion September 2018 |
| Contact information | Mark Hawley mark.hawley@sheffield.ac.uk University of Sheffield (UK) |
| Notes | Sponsor: Sheffield Teaching Hospitals NHS Foundation Trust Collaborators: University of Sheffield, National Institute for Health Research: CLAHRC YH, The Rotherham NHS Foundation Trust, Doncaster And Bassetlaw Hospitals NHS Foundation Trust |
NCT02702791.
| Trial name or title | Sustaining Training Effects through Physical activity (STEP): enhancing physical activity to achieve sustainable benefits in extrapulmonary consequences of COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 84 Blinding: none |
| Participants | Diagnosis of COPD (internationally‐accepted guidelines); smoking history (current or former) ≥ 10 pack‐years; age 40 to 80 years; completed 3 months of outpatient PR (Gasthuisberg University Hospital, Leuven, Belgium); ability to manage electronic devices (smartphone, step counter) |
| Interventions | DURATION OF INTERVENTION 6 months INTERVENTION PAC (tele‐coaching) with PR feasible goal‐setting and feedback to enhance participant's motivation and commitment Pedometer‐based goals and tele‐coaching support INTERVENTION PR general advices regarding physical activity |
| Outcomes | ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOMES
|
| Starting date | Retrospective registration; estimated study completion June 2018 |
| Contact information | Thierry Troosters Thierry.Troosters@kuleuven.be KU Leuven (Belgium) |
| Notes | Collaborator: Conselho Nacional de Desenvolvimento Científico e Tecnológico |
NCT02707770.
| Trial name or title | The role of ambulatory oxygen in improving the effectiveness of PR for COPD patients |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 20 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD; fulfil clinical criteria for PR; exercise‐induced desaturation (fall in SaO2 ≥ 4% to ≤ 90%, or any fall < 90%) and demonstrate improvement with ambulatory oxygen |
| Interventions |
INTERVENTION ambulatory oxygen with PR INTERVENTION placebo with PR |
| Outcomes | DEVICE (pedometer )ASSESSMENT TIME POINTS Baseline, 6 weeks, 14 weeks, 18 weeks PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Prospective registration; actual study completion December 2017 |
| Contact information | Vijayaragavan Padmanaban, Imperial College Healthcare NHS Trust (UK) |
| Notes | Collaborator: National Institute for Health Research (UK) |
NCT02720822.
| Trial name or title | Breathlessness, Exertion And Morphine Sulfate (BEAMS) study |
| Methods | DESIGN "A five stage, national, multi‐site, double‐blind, parallel arm, block randomised, placebo controlled, factorial, dose increment phase III study"; COMPARISON intervention vs. placebo; SETTING 19 centres (Australia); SAMPLE SIZE n = 171 PROTOCOL "The BEAMS study will be promoted to patients with COPD that interferes with ADLs through LungNet (Lung Foundation Australia) and the Primary Health Networks in each recruitment catchment area. Potentially eligible participants will be identified and approached by both primary and secondary care clinicians at participating sites across Australia who will then refer them to the research team. Research team attendance at relevant clinics and study advertisements will help to remind clinical staff of study recruitment and encourage patients to self‐refer. Permission will be sought from consultants in charge of the care of potential participants for research staff to approach them directly. Case identification in both inpatient units and outpatient clinics will also occur following case‐note review." Selection bias: "Randomisation will occur through the development of randomisation tables using random number tables generated by an independent provider", "Randomisation requests will take the form of receipt of a prescription for study medicines by site pharmacists. Site pharmacists will receive the next randomisation number available through telephone contact with the central registry"; Performance bias: "All research staff, treating clinicians and patients will remain blinded to the treatment allocation" |
| Participants | Diagnosis of COPD (post‐bronchodilator FER < 0.7); age ≥ 18 years; modified MRC dyspnoea scale (score 3 or 4); atable medications over prior week; respiratory physician‐confirmed optimisation of treatment; worst breathlessness intensity in the previous 24 hours was at least 3/10 |
| Interventions |
COMMON COMPONENTS Written advice detailing standard therapeutic strategies for managing breathlessness Battery‐operated, hand‐held fan and instructions for use throughout the study period as standard breathlessness management strategies INTERVENTION sustained‐release morphine sulfate 1 double‐blind capsule in the morning (8 mg, 16 mg, 24 mg or 32 mg) laxative (Docusate with senna) PLACEBO 1 double‐blind capsule in the morning, placebo laxative optional |
| Outcomes | DEVICE FitBit Charge HR ASSESSMENT TIME POINTS "weeks one and three of the study" OUTCOME MEASURES Physical activity: steps per day, "activity" SAFETY "Participant safety will remain of paramount importance throughout the study period. Rescue medication will therefore be available for participants for treatment of common opioid side effects including nausea and constipation. Opioid toxicity is defined by physician assessment of respiratory depression (≤10 breaths per minute), drowsiness, myoclonus, myosis or National Cancer Institute Common Terminology Criteria for Adverse Events version 4 (NCI CTCAEv4) grade ≥3 for cognitive impairment, confusion or somnolence. Signs suggestive of opioid toxicity will result in urgent physician assessment, investigation of contributing factors and treated with either opioid dose reduction or naloxone according to the severity of the toxicity and degree of respiratory compromise. Reasons for cessation of study drug or withdrawal from the study include treatment failure as defined by unacceptable side effects of NCI CTCAEv4 grade 3 that do not settle with symptomatic intervention or grade 4 or 5 harms. Participants may also be withdrawn if treatment is deemed ineffective by treating clinician, increasing breathlessness scores despite study treatment or withdrawal of participant consent." |
| Starting date | Study start August 2016, estimated primary completion June 2019 |
| Contact information | David Currow david.currow@flinders.edu.au Flinders University, Adelaide (Australia) |
| Notes | FUNDING "This study was funded by the National Health and Medical Research Council, Australia (Grant Number APP1065571) and sponsored by Flinders University, Adelaide, Australia. The funders and study sponsors had no role in the study design and will have no role in the data collection, analysis or dissemination of study results." CONFLICT OF INTEREST "DCC has received an unrestricted research grant from Mundipharma, is an unpaid member of an advisory board for Helsinn Pharmaceuticals and has consulted Mayne Pharma and received intellectual property payments from them. MJJ has received consulting payments from Mayne Pharma." |
NCT02864420.
| Trial name or title | Hospital‐level care at home for acutely ill adults: a pilot randomised controlled trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SETTING emergency departments, academic medical centre and community hospital (USA); SAMPLE SIZE "We had limited funding and could only continue our pilot for at most 2.25 months. Thus, irrespective of enrollment, we a priori planned to stop the pilot when funds were depleted." Selection bias: "Participants were randomized to usual care admission or home hospital admission by research study staff. Randomization was stratified by condition with randomly selected block sizes between 4 and 6", "allocation concealment via sealed envelopes"; Performance/detection bias: "Given the nature of the study, blinding of patients, study staff, and physicians was not possible" |
| Participants | Primary or possible diagnosis of any infection, heart failure exacerbation; AECOPD or asthma exacerbation; age ≥ 18 years; resides within 5‐mile radius; caregiver to stay for first 24 hours of admission; primary diagnosis of cellulitis, heart failure, complicated urinary tract infection, or pneumonia that requires inpatient admission |
| Interventions |
COMMON COMPONENTS minimum 1 daily visit from an attending general internist 2 daily visits from a home health registered nurse additional visits as needed Also tailored to participant need: medical meals, home health aide, social worker, physical therapist, occupational therapist All participants had continuous monitoring of heart rate, respiratory rate, telemetry, movement, falls, and sleep by a small skin patch (physIQ, Chicago, IL; VitalConnect, San Jose, CA). Monitoring was performed through machine‐based algorithms, and clinical staff reviewed alarms INTERVENTION "Home hospital" could provide oxygen therapy, respiratory therapies, intravenous medications via infusion pump, in‐home radiology, and point‐of‐care blood diagnostics Participants communicated with their home hospital team by telephone, encrypted video, and encrypted short message service physician available 24 hours a day NO INTERVENTION |
| Outcomes | DEVICE VitalConnect VitalPatch ASSESSMENT TIME POINTS
SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start September 2016 |
| Contact information | David Levine dmlevine@bwh.harvard.edu Brigham and Women's Hospital, Boston (USA) |
| Notes | FUNDING "Partners HealthCare Population Health Management provided funding support for the home hospital clinical program. Dr. Levine received funding support from an Institutional National Research Service Award from (T32HP10251) and the Ryoichi Sasakawa Fellowship Fund. The NIH had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; or the preparation, review, or approval of the manuscript." CONFLICT OF INTEREST "The authors declare that they do not have a conflict of interest." Author correspondence: "Please note that this was the pilot study of ˜20 patients. There are too few patients with COPD to make cuts in the data, sadly. Please note our larger study will be published soon." |
NCT02895152.
| Trial name or title | The role of activity monitors in improving physical activity in COPD patients participating in PR |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 20 Blinding: none |
| Participants | Diagnosis of COPD (FER < 0.7); optimised pharmacology intervention; referred for PR |
| Interventions | DURATION OF INTERVENTION 7 weeks INTERVENTION PAC with PR wear activity monitor: weekly feedback: amount of activity, steps taken, active minutes each day, wear time tailored advice on how to improve activity levels INTERVENTION PR wear activity monitor, no feedback |
| Outcomes | DEVICE "data recorded on the device, throughout study, up to seven weeks" ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
| Starting date | First posted September 2016; estimated study completion August 2017 |
| Contact information | Patricia Kelly patricia.kelly@srft.nhs.uk Glenn Cardwell glen.cardwell@srft.nhs.uk Natalie Garratt Natalie.Garratt@manchester.ac.uk Salford Royal NHS Foundation Trust, Greater Manchester (UK) |
| Notes |
NCT02917915.
| Trial name or title | The CaNadian Standardized Pulmonary Rehabilitation Efficacy Trial (CoNSPiRE) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 200 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD (post‐bronchodilator FER < 0.7); enrolled in PR within affiliated sites or satellite tele‐health programme; as part of standard rehabilitation referral procedures; ambulatory, no unstable cardiovascular disease |
| Interventions |
COMMON INTERVENTION PR DURATION 6 or 8 weeks SETTING centre‐based or tele‐rehabilitation CONTACT 2 days a week CONTENT 2 hours of exercise training (aerobic and resistance), 1 hour of education designed to promote self‐management INTERVENTION traditional educational approach with PR CONTACT
CONTENT exercise, anatomy, pulmonary diseases, healthier breathing, pulmonary medications, pulmonary devices, exercise action plan, allergies and pulmonary function tests, health and air quality, healthier eating, travel, stress management INTERVENTION new Canadian standardised educational approach with PR CONTACT
CONTENT exercise, living well with chronic lung disease, breathing management, conserving energy, pulmonary medications, inhaler devices, integrating exercise in your life, management of respiratory infections, management of aggravating environmental factors, management of stress and anxiety, nutrition, leisure and travel, getting a good night's sleep, enjoying intimacy, living in a smoke‐free environment, integrating long‐term oxygen into your life, keeping a healthy lifestyle |
| Outcomes | DEVICE Fitbit ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; first posted September 2016; actual study start January 2017; estimated study completion August 2019 |
| Contact information | Anne‐Marie Selzler aselzler@ualberta.ca; Michael K Stickland michael.stickland@ualberta.ca University of Alberta (Canada) |
| Notes | Collaborators: McGill University, University of Toronto, Université de Sherbrooke |
NCT02924870.
| Trial name or title | Long‐term effect of a health education programme on daily physical activity in patients with moderate‐to‐very severe COPD (EA‐EPOC) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 128 Blinding: none |
| Participants | Diagnosis of moderate‐to‐very severe COPD (GesEPOC criteria: FEV1 < 80% predicted, ≥ 3 months); smoking history (current or former) > 10 pack‐years; age > 35 years; hospital admission for AECOPD |
| Interventions |
INTERVENTION health education 2 nursing health education sessions, 15 and 30 days after discharge
NO INTERVENTION Treatment and follow‐up according to conventional clinical practice including recommendations on healthy habits and lifestyle |
| Outcomes | PRIMARY OUTCOME Physical activity: “physical activity level” SECONDARY OUTCOMES
|
| Starting date | Prospective registration; estimated study completion March 2020 |
| Contact information | Francisco Garcia‐Rio fgr01m@gmail.com Hospital Universitario La Paz, Madrid (Spain) |
| Notes |
NCT02956213.
| Trial name or title | Assessing the effect of different efficiency indoor air filters on respiratory symptoms in former smokers |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. sham; SAMPLE SIZE n = 52 Blinding: participant, investigator, outcomes assessor |
| Participants | Smoking history; does not currently smoke and no‐one currently smokes inside the home; history of AECOPD or development of respiratory symptoms with periods of high outdoor air pollution; age ≥ 40 years; access to Wi‐Fi, cell phone, tablet or personal computer |
| Interventions |
INTERVENTION portable HEPA air filtering device with MERV17 air filter SHAM portable air filtering device with basic carbon filter |
| Outcomes | ASSESSMENT TIME POINTS Baseline, 12 weeks, 3 months, 6 months PRIMARY OUTCOME HRQOL: SGRQ SECONDARY/OTHER OUTCOMES
|
| Starting date | Prospective registration; actual study completion June 2019 |
| Contact information | Denitza Blagev, Intermountain Medical Center, Salt Lake City, Utah (USA) |
| Notes | N.B. will need to confirm specific diagnosis of COPD for inclusion, also will need pre‐cross‐over data |
NCT02966561.
| Trial name or title | Pedometer‐based behavioural intervention for individuals with COPD to Stay Active After Rehabilitation (STAR) |
| Methods | DESIGN 2 groups COMPARISON intervention vs. placebo; SETTING PR clinic Bad Reichenhall (Germany); SAMPLE SIZE n = 502 |
| Participants | Primary reason for referral to PR: diagnosis of COPD (classifications A – D; post‐bronchodilator FER < 0.7); age ≥ 18 years |
| Interventions |
COMMON INTERVENTION DURATION 3 weeks, extension 1 to 2 weeks if required (centre average 25 days) SETTING inpatient PR AEROBIC TRAINING 4 to 5 sessions, 45 minutes STRENGTH TRAINING 3 sessions, 45 minutes OTHER COMPONENTS 7 sessions whole‐body vibration muscle training EDUCATION Structured COPD patient education
Intervention components addressing the promotion of physical activity INTERVENTION PAC: pedometer‐based behaviour change intervention SETTING open groups, 6 to 12 participants CONTACT 2 sessions, 45 minutes
CONTENT
PLACEBO “behavior placebo” "Playful" physical activity and revisions of information on physical activity (knowledge of exercise recommendations, knowledge of possibilities of self‐regulation of endurance‐training exercise intensity) as in standard education Booklet: looks identical to intervention group diary, contains a repetition of physical activity‐related information as for standard education |
| Outcomes | DEVICE Actigraph wGT3X‐BT
Sedentary < 100 counts, MVPA > 1952 counts a minute ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: time sedentary (< 100 cpm), MVPA time (> 1952 cpm) |
| Starting date | "recruitment starts in June 2016 and is likely to be finished in September 2017" |
| Contact information | Wolfgang Geidl wolfgang.geidl@fau.de Friedrich‐Alexander University, Erlangen (Germany) |
| Notes | FUNDING "This study is funded by the German Pension Insurance Association, Section Bavaria South (Deutsche Rentenversicherung Bayern Süd; Abteilung Rehabilitation und Sozialmedizin, Am Alten Viehmarkt 2, 84028 Landshut, Germany) (Reference number: 5.011‐6.031.115) (www.deutscherentenversicherung‐ bayernsued.de) which was not involved in the design of the study and collection, management, analysis, interpretation of data, in writing the manuscript, or the decision to submit the report for publication." CONFLICT OF INTEREST "The authors declare that they have no competing interests." |
NCT02999685.
| Trial name or title | Development and feasibility of a home PR program with health coaching |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 120 |
| Participants | Diagnosis of COPD (GOLD stage II to IV; "as documented by PFT"); smoking history (current or former) ≥10 pack‐years; age ≥ 40 years; eligible for PR |
| Interventions | DURATION OF INTERVENTION 8 weeks INTERVENTION home‐based PR with health coaching SETTING home INTERFACE
ACTIVITY
MONITORING
NO INTERVENTION |
| Outcomes | DEVICE Actigraph ASSESSMENT TIME POINTS
OUTCOME MEASURES
|
| Starting date | Estimated study completion June 2019 |
| Contact information | Roberto Benzo benzo.roberto@mayo.edu Mayo Clinic, Minnesota (USA) |
| Notes | FUNDING "Dr Kramer and Ms Seifert are affiliated with the Minnesota Health Solutions Corporation, Saint Paul, Minnesota. Dr Benzo, Ms Hoult, Ms Seifert, and Dr Kramer are supported by National Institutes of Health Grant SBIRHL 114162‐2 (to Ms Seifert [PI] and Dr Benzo [clinical trial PI]). Ms Seifert has disclosed a relationship with NovuHealth." CONFLICT OF INTEREST "The other authors have disclosed no conflicts of interest" |
NCT03073954.
| Trial name or title | The feasibility of working memory training in COPD patients and the efficacy on cognitive performance, self‐control and stress response |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 75 Blinding: participant, care provider, investigator, outcomes assessor |
| Participants | Diagnosis of COPD (GOLD); age ≥ 18 years; motivated as evaluated by the self‐determination questionnaire |
| Interventions |
COMMON COMPONENTS
INTERVENTION working memory training and healthy lifestyle coaching domain‐general cognitive working memory training programme training increases with difficulty if participants answer 2 subsequent questions correctly INTERVENTION sham working memory training and healthy lifestyle coaching training that does not increase in difficulty |
| Outcomes | DEVICE (accelerometer )PRIMARY OUTCOMES Adherence: training SECONDARY OUTCOMES
|
| Starting date | Prospective registration; estimated study completion July 2019 |
| Contact information | Sarah Mount sarah.mount@maastrichtuniversity.nl; Martijn van Beers Martijn.vanbeers@maastrichtuniversity.nl Maastricht University Medical Center, Limburg (The Netherlands) |
| Notes | Collaborator: Eatwell |
NCT03080662.
| Trial name or title | Impact of inspiratory muscle training on daily physical activity (INAF) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. sham; SAMPLE SIZE n = 20 Blinding: participant |
| Participants | Diagnosis of COPD; age 45 to 80 years; clinically stable ≥ 4 weeks; inspiratory muscle weakness (PImax < 70%); pulmonary hyperinflation (TLC > 120%) |
| Interventions | DURATION OF INTERVENTION 5 weeks INTERVENTION inspiratory muscle training OXYGEN DUAL Inspiratory valve with increase resistance INTERVENTION sham inspiratory muscle training Inspiratory valve without resistance |
| Outcomes | DEVICE (accelerometer) ASSESSMENT TIME POINTS
PRIMARY OUTCOME
|
| Starting date | Retrospective registration; estimated study completion March 2018 |
| Contact information | Diego Agustin Rodriguez DARodriguez@parcdesalutmar.cat Parc de Salut Mar, Hospital Del Mar (Spain) |
| Notes |
NCT03084874.
| Trial name or title | Efficacy of a coaching programme to promote physical activity and reduce sedentary behaviour after a COPD exacerbation that require hospitalisation |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 66 Blinding: participant, investigator, outcomes assessor |
| Participants | Diagnosis of COPD (post‐bronchodilator FER < 0.7); smoking history > 10 pack‐years; age > 40 years; hospitalisation due to AECOPD |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION PAC individualised physical activity and sedentary behaviour coaching motivational interview; usual exercise habits, possible barriers and facilitators, self‐efficacy and motivation progressive program with specific goals‐setting and self‐monitoring NO INTERVENTION |
| Outcomes | DEVICE (accelerometer) ASSESSMENT TIME POINTS
PRIMARY OUTCOME
SECONDARY OUTCOMES
|
| Starting date | First posted March 2017; estimated study start March 2017; estimated study completion December 2018 |
| Contact information | Maria A Ramon maramon@vhebron.net; Esther Rodriguez estherod@vhebron.net Hospital Universitari Vall d'Hebron Research Institute, Barcelona (Spain) |
| Notes | Collaborator: Spanish Society of Pneumology and Thoracic Surgery |
NCT03114241.
| Trial name or title | Long‐term effects of a 3‐month pedometer‐based programme to enhance physical activity in patients with severe COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 74 Blinding: none |
| Participants | Diagnosis of COPD (GOLD severe; FEV1 < 50%); age ≥ 40 years |
| Interventions | DURATION OF INTERVENTION 12 months INTERVENTION Pedometer and PAC 3 months coaching followed by 9 months (keep pedometer, encouraged to sustain an increased level of daily physical activity) “encouraged to be more active” Daily step count goal: 15% increase compared to baseline Monthly telephone calls: encourage compliance, motivate NO INTERVENTION |
| Outcomes | DEVICE SenseWear Pro (upper left arm); Wear instructions: 7 consecutive days ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOME HRQOL: CAT, SF36 |
| Starting date | Prospectively registered; actual study start May 2017; estimated study completion August 2019 |
| Contact information | Christian Clarenbach christian.clarenbach@usz.ch; Noriane Sievi noriane.sievi@usz.ch University of Zurich (Switzerland) |
| Notes |
NCT03127878.
| Trial name or title | Effects of upper‐limb endurance exercise training addition to a conventional high‐intensity exercise training programme on physical activity level and activities of daily living performance in patients with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 64 Blinding: none |
| Participants | Diagnosis of COPD (GOLD); age 40 to 95 years; absence of AECOPD in the previous month (clinical stability); absence of severe or non‐stable cardiac disease; no exercise training programme within 1 year |
| Interventions | DURATION OF INTERVENTION 3 months INTERVENTION High‐intensity endurance exercise of lower limb strengthening exercise of upper and lower limb INTERVENTION High‐intensity endurance exercise of upper and lower limb strengthening exercise of upper and lower limb |
| Outcomes | PRIMARY OUTCOME Physical activity: sedentary time (< 1.5 METs), active time (> 3 METs) SECONDARY OUTCOMES
|
| Starting date | Retrospective registration; first posted April 2017; actual study start January 2017; estimated study completion January 2020 |
| Contact information | Fabio Pitta fabiopitta@uol.com.br Universidade Estadual de Londrina (Brazil) |
| Notes | Collaborator: National Council for Scientific and Technological Development (Brazil) |
NCT03201198.
| Trial name or title | Active for life: COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. sham; SAMPLE SIZE n = 183 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD; Age ≥ 50 years; no AECOPD or major illnesses requiring hospitalisation within 8 weeks; no history of other major lung diseases as primary pulmonary problem, history of a recent heart attack or recent onset of chest pains with activity or increasing episodes of chest pain; no other health or mobility problems that limit physical activity; sedentary (< 30 minutes of moderate activity, 3 days a week) |
| Interventions | DURATION OF INTERVENTION
INTERVENTION "Active Life" focus on increasing light physical activity; encouraged to increase total PA by ≥ 60 minutes a day
SHAM chair exercises, behavioural relaxation and health education
|
| Outcomes | DEVICE ActivPal and Actigraph; Wear instructions: 1 week TIME POINTS
PRIMARY OUTCOME Physical activity: time in physical activity, time sedentary (ActivPal), time in light‐intensity physical activity, MVPA time (Actigraph) SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; actual study start July 2017; estimated study completion February 2022 |
| Contact information | She'Lon Tucker shehill@umich.edu; Ron Dechert rdechert@med.umich.edu, Janet Larson, School of Nursing, University of Michigan (USA) |
| Notes |
NCT03275116.
| Trial name or title | The effect of twice‐daily aclidinium bromide/formoterol fumarate 340/12 mcg vs. once‐daily tiotropium 'respimat' 5 mcg on static and dynamic hyperinflation in patients with COPD during 24 hours |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 49 Blinding: none |
| Participants | Diagnosis of COPD (moderate‐to‐very severe > 12 months before screening; post‐bronchodilator FEV1 < 80% predicted, FER < 0.7); smoking history (current or former) ≥ 10 pack‐years; age ≥ 40 years; modified MRC dyspnoea scale (score at least 2); entering PR at CIRO; severe static hyperinflation (RV > 150% predicted); co‐operative attitude and ability to use correctly the inhalers |
| Interventions | DURATION OF INTERVENTION 4 days INTERVENTION LAMA/LABA (Aclidinium Bromide/Formoterol Fumarate 340/12 mcg) twice daily INTERVENTION LAMA (Tiotropium 'Respimat' 5 mcg) once daily |
| Outcomes | DEVICE (accelerometer); Wear instructions: 4 days SECONDARY OUTCOME Physical activity: “Nighttime physical activity” (inverse surrogate for sleep quality) |
| Starting date | Restrospective registration; first posted September 2017; actual study start July 2017, estimated study completion November 2018 |
| Contact information | Lowie Vanfleteren lowievanfleteren@ciro‐horn.nl; Maud Koopman maudkoopman@ciro‐horn.nl CIRO, Horn (The Netherlands) |
| Notes | Sponsor: Maastricht University Medical Center Collaborators: AstraZeneca N.B. will need pre‐cross‐over data for inclusion, also clarification of physical activity |
NCT03280355.
| Trial name or title | The effects of singing training for patients with COPD |
| Methods | DESIGN 2 groups, cluster‐randomised; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 220 Blinding: investigator, outcomes assessor |
| Participants | Diagnosis of COPD; age ≥ 18 years; modified MRC scale (score at least 2); recommended for PR; sufficient mobility to attend |
| Interventions | DURATION OF INTERVENTION 10 weeks COMMON INTERVENTION PR SETTING outpatient, group CONTACT 2 sessions a week, 90 minutes (total 20 sessions) CONTENT supervised warm‐ups, aerobic and strength training, breathing exercises INTERVENTION singing training with PR technical instruction in order to achieve better respiratory control and primary muscular strength focus on techniques for efficient expiration focus on musical content and interpretation as well as interaction, the social aspects and joy of singing together. INTERVENTION PR |
| Outcomes | DEVICE (pedometer); Wear instructions: 1 week PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Retrospective registration; actual study start August 2017; first posted September 2017; estimated study completion November 2018 |
| Contact information | Mette Kaasgaard mk@clin.au.dk; Uffe Bodtger ubt@regionsjaelland.dk University of Aarhus (Denmark) |
| Notes |
NCT03321279.
| Trial name or title | Social incentives to increase mobility among hospitalised patients: the MOVE IT randomised trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 227 Blinding: investigator, outcomes assessor |
| Participants | Pneumonia, diabetes, congestive heart failure, COPD; age ≥ 18 years; admitted to medicine or oncology floor in the hospital |
| Interventions | DURATION OF INTERVENTION 12 weeks post‐discharge INTERVENTION pedometer with "social incentives" daily step counts Week 2 to Week 13 after hospital discharge weekly step goal: increases from baseline by 10% each week social incentive‐based gamification based on points and levels daily feedback for the step counts, weekly feedback for levels support partner will receive weekly reports INTERVENTION pedometer daily step counts Week 2 to Week 13 after hospital discharge |
| Outcomes | DEVICE pedometer (Nokia Steel) PRIMARY OUTCOME Physical activity: step count |
| Starting date | Prospectively registered; study start January 2018; estimated study completion October 2019 |
| Contact information | Ryan Greysen, Mitesh Patel, University of Pennsylvania (USA) |
| Notes | N.B. will need data only for participants with COPD |
NCT03359473.
| Trial name or title | A randomised, double‐blind (sponsor unblind), placebo‐controlled, multi‐centre phase IIa study to evaluate the safety and efficacy of 13 weeks of once daily oral dosing of the selective androgen receptor modulator (SARM) GSK2881078 in older men and post‐menopausal women with COPD and muscle weakness, participating in home exercise |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. placebo; SAMPLE SIZE n = 100 Blinding: participant, investigator |
| Participants | Diagnosis of COPD (American Thoracic Society/European Respiratory Society criteria: post‐bronchodilator FEV1 30% to 65% predicted, FER < 0.7); smoking history (current or former) ≥ 10 pack‐years; age 50 to 75 years; BMI 18 to 32 kg/m2; able to read and write in the language used for the diary and able to operate electronic device; if participating in a structured exercise programme must be willing to convert their current exercise programme to the study programme |
| Interventions |
INTERVENTION GSK2881078 Cohort 1 Males 2 mg capsules, once daily, oral administration PLACEBO Cohort 1 men 2 capsules of placebo once daily, oral administration INTERVENTION GSK2881078 Cohort 2 women 1 mg capsule, once daily, oral administration PLACEBO Cohort 2 women 2 capsules of placebo once daily, oral administration |
| Outcomes | DEVICE (accelerometer); Wear instructions: 1 week PRIMARY OUTCOME Adverse events and serious adverse events SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start February 2018; estimated study completion November 2019 |
| Contact information | |
| Notes | Sponsor: GlaxoSmithKline Collaborator: Parexel (USA, Germany, UK) |
NCT03513068.
| Trial name or title | Portable oxygen concentrator improvements to physical activity, oxygen usage, and quality of life in COPD patients using LTOT (POC‐STEP) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 190 Blinding: none |
| Participants | Diagnosis of COPD; age ≥ 40 years; qualifies for continuous LTOT, prescribed oxygen at ≤ 5 litres a minute; has not used a portable oxygen concentrator prior to enrolling in this study; able to tolerate pulsed oxygen therapy |
| Interventions |
INTERVENTION portable oxygen concentrator with LTOT INTERVENTION LTOT |
| Outcomes | DEVICE "Actigraphy" PRIMARY OUTCOME Physical activity: (not defined) SECONDARY OUTCOME HRQOL: SGRQ |
| Starting date | Prospectively registered; study start July 2018; estimated study completion February 2021 |
| Contact information | Cindy Wen cindy.wen@resmed.com ResMed (USA) |
| Notes | Collaborator: Inogen, Inc (USA) |
NCT03584269.
| Trial name or title | Non‐invasive ventilation and nocturnal alveolar hypoventilation in patients with COPD treated by long‐term oxygen therapy at home |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 38 Blinding: none |
| Participants | Diagnosis of COPD; age 18 to 85 years; LTOT |
| Interventions |
INTERVENTION non‐invasive ventilation (respiratory assistance by a facial mask without intubation or tracheotomy) with LTOT INTERVENTION LTOT |
| Outcomes | SECONDARY OUTCOMES
|
| Starting date | Actual study start June 2018; first posted July 2018; estimated study completion April 2020 |
| Contact information | Jean‐Louis Pépin JPepin@chu‐grenoble.fr Marjorie Dole mdole2@chu‐grenoble.fr University Hospital, Grenoble (France) |
| Notes | Collaborators: AGIR à Dom, ResMed |
NCT03584295.
| Trial name or title | A multicentre, randomised‐controlled trial of extracorporeal CO2 removal (ECCO2R) to facilitate early extubation compared to invasive mechanical ventilation in patients with severe AECOPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 202 Blinding: none |
| Participants | Known history of COPD; age 18 to 75 years; AECOPD requiring invasive mechanical ventilation; acute and potentially reversible cause of acute respiratory failure |
| Interventions |
INTERVENTION Extracorporeal carbon dioxide removal Invasive mechanical ventilation treated with vv‐ECCO2R (Extracorporeal carbon dioxide removal) to facilitate early extubation Standard configuration with either double lumen cannula (20 to 22 Fr) or 2 small single vessel cannulas (15 to 19 Fr), allowing a blood flow rate between 1 and 2 litres a minute INTERVENTION conventional care Invasive mechanical ventilation; attempt to extubate and switch to non‐invasive ventilation If extubation fails, tracheostomy can be performed according to treating physician |
| Outcomes | DEVICE Actigraph; Wear instructions: up to 60 days SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; estimated study start January 2019; estimated study completion July 2023 |
| Contact information | Christian Karagiannidis christian.karagiannidis@uni‐wh.de Anne Hage‐Hülsmann Anne.hage‐huelsmann@uni‐wh.de University of Witten/Herdecke (Germany) |
| Notes |
NCT03620630.
| Trial name or title | Evidence generation for the clinical efficacy and cost effectiveness of myCOPD in patients with mild and moderate newly‐diagnosed COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 60 Blinding: outcomes assessor |
| Participants | Diagnosis of COPD (mild or moderate; FEV1 > 50% predicted) or diagnosed within 12 months (FER < 0.7); smoking history (current or former); age 40 to 80 years; currently taking inhaled medications; access to the internet at home, use of mobile technology and the ability to operate a web platform in English |
| Interventions |
INTERVENTION "myCOPD" web‐based application designed to support people in long‐term management of COPD NO INTERVENTION |
| Outcomes | DEVICE FITBIT (pedometer)
PRIMARY OUTCOME HRQOL: CAT SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; actual study start November 2018; estimated study completion February 2019 |
| Contact information | Mal North mal.north@mymhealth.com Chloe Barker chloe.barker@mmhealth.com my mhealth Limited, Bournemouth (UK) |
| Notes | Collaborators: Innovate UK, Imperial College London, Hull and East Yorkshire Hospitals NHS Trust Hampshire Hospitals NHS Foundation Trust, Central London Community Healthcare NHS Trust |
NCT03654092.
| Trial name or title | Effects of a long‐term home‐based exercise training programme using minimal equipment vs. usual care in COPD patients: a study protocol for 2 multicentre randomised controlled trials (HOMEX‐1 and HOMEX‐2 trials) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention SETTING Canton of Zurich (Switzerland); SAMPLE SIZE n = 120 (based on CRQ dyspnoea domain) Blinding: none |
| Participants | Diagnosis of COPD (GOLD stages II to IV; post‐bronchodilation FEV1 < 80% predicted; FER < 0.7); age ≥ 40 years; no PR within 2 years |
| Interventions | DURATION OF INTERVENTION 12 months INTERVENTION home‐based exercise SETTING home CONTACT
TRAINING 6 days a week, 15 to 20 minutes, individualised and progressive strength‐training, 3 different levels CONTENT
NO INTERVENTION |
| Outcomes | DEVICE ActiGraph, Wear instructions: 1 week ASSESSMENT TIME POINTS
PRIMARY OUTCOME HRQOL: CRQ dyspnoea domain SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start October 2018; estimated primary completion October 2020 |
| Contact information | Anja Frei anja.frei@uzh.ch University of Zurich (Switzerland) |
| Notes | FUNDING "HOMEX‐2 is supported by LUNGE ZÜRICH, Switzerland.The funding bodies had/have no role in the design of the study, data collection, analysis and interpretation of data and in writing the manuscript." CONFLICT OF INTEREST "The authors declare that they have no competing or financial interests." N.B. physical activity not assessed in HOMEX‐1 |
NCT03655028.
| Trial name or title | Increasing physical activity in COPD through rhythmically‐enhanced music |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 170 Blinding: investigator, outcomes assessor |
| Participants | Diagnosis of COPD (FEV1 < 70% predicted, FER < 0.7); age ≥ 40 years; mean SpO2 88% at peak exercise (with or without oxygen supplementation); ability to hear music |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION home‐based exercise programme with rhythmically auditory stimulation‐enhanced music INTERVENTION home‐based exercise programme without music |
| Outcomes | DEVICE Actigraph (hip); Wear instructions: 1 week PRIMARY OUTCOME Exercise capacity: 6MWD SECONDARY OUTCOMES
|
| Starting date | Prospective recruitment; study start October 2018; estimated study completion September 2022 |
| Contact information | Susan A O'Connell Schnell susan.oconnell@va.gov Franco Laghi franco.laghi@va.gov Edward Hines Jr. VA Hospital, Illinois (USA) |
| Notes | Sponsor: VA Office of Research and Development |
NCT03660644.
| Trial name or title | Physical activity following PR in patients with COPD |
| Methods | DESIGN 2 groups, cluster; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 60 Blinding: outcomes assessor, "Physiotherapists will be aware of the allocation of the programmes (not possible to blind) as they will be involved with delivering information/training of intervention components. A researcher blinded to group allocation will perform quantitative analysis." |
| Participants | Diagnosis of COPD; age 30 to 100 years; enrolled in PR within Lincolnshire Community Health Services; for telephone interviews: access to a telephone |
| Interventions | DURATION OF INTERVENTION 12 months following PR INTERVENTION PAC
NO INTERVENTION |
| Outcomes | ASSESSMENT TIME POINTS
PRIMARY OUTCOME MEASURE Adherence : “acceptability” number of participants who comply with intervention SECONDARY OUTCOMES
|
| Starting date | Retrospectively registered; actual study start June 2018; first posted September 2018; estimated study completion October 2019 |
| Contact information | Hayley Robinson hrobinson@lincoln.ac.uk Arwel Jones ArJones@lincoln.ac.uk University of Lincoln (UK) |
| Notes | Collaborators: NHS PR clinics across Lincolnshire, United Kingdom, British Lung Foundation, University College, University of Oxford |
NCT03746873.
| Trial name or title | A web‐based self‐management intervention to increase level of physical activity and decrease use of health care for people with COPD in primary care: a protocol for a randomised controlled clinical trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 144 Blinding: none |
| Participants | Diagnosis of COPD (ICD‐10:J44:9); age ≥ 40 years; visit included primary care units due to COPD; have a smartphone, tablet or computer with access to internet |
| Interventions |
INTERVENTION PAC (COPD Web) with pedometer written information about the importance of physical activity website, self‐managed
INTERVENTION pedometer written information about the importance of physical activity |
| Outcomes | DEVICE DynaPort MiniMod; Wear instructions: 1 week ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: (not defined) SECONDARY OUTCOME HRQOL: CAT, CRQ |
| Starting date | Study start November 2018; estimated study completion March 2020 |
| Contact information | Tobias Stenlund tobias.stenlund@umu.se; Karin Wadell karin.wadell@umu.se Umeå University (Sweden) |
| Notes |
NCT03749655.
| Trial name or title | A feasibility study assessing the inclusion of physical activity promotion to standard care PR and cognitive behavioural therapy in patients with COPD who are anxious and depressed |
| Methods | DESIGN 2 groups; COMPARISON; intervention vs. intervention; SAMPLE SIZE n = 40 Blinding: single, principal investigator will be blinded from the randomisation as this member will conduct cognitive behavioural therapy |
| Participants | Diagnosis of COPD (obstructive spirometry); age ≥ 40 years; clinically stable; optimised medical therapy; HADS score ≥ 8 |
| Interventions | DURATION OF INTERVENTION 8 weeks INTERVENTION PAC with PR and cognitive behavioural therapy SETTING consultation sessions CONTACT 2 sessions a week (total 16 sessions) CONTENT
INTERVENTION PR and cognitive behavioural therapy |
| Outcomes | DEVICE (triaxial accelerometer); Wear instructions: 1 week ASSESSMENT TIME POINTS
PRIMARY OUTCOME Adherence: PAC
SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start November 2018; estimated study completion May 2020 |
| Contact information | Matthew Armstrong matthew.armstrong@northumbria.ac.uk Northumbria University; Karen Heslop‐Marshell Karen.Heslop@nuth.nhs.uk Newcastle Upon Tyne, Tyne And Wear (UK) |
| Notes |
NCT03750292.
| Trial name or title | Residential cleaning of indoor air to reduce acute exacerbations of COPD (CARE): a pilot randomised cross‐over trial |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. placebo; SAMPLE SIZE n = 20 Blinding: participant, investigator, outcomes assessor |
| Participants | Diagnosis of COPD (severe; FEV1 < 50% predicted); age ≥ 18 years; live in Monroe County; referred for PR; AECOPD within 1 year; standard‐sized windows in their bedroom and living room amenable to device installation; expect to sleep each night of the study (2 months of period 1, 2 months of period 2) in either their bedroom or living room ≥ 6 hours a night, no other air filtering devices |
| Interventions |
INTERVENTION HEPAirX air filter medical re‐circulating air cleaner 99.97% efficient filter for particles 0.3 µm in size PLACEBO provides only recirculation (without filtration or ventilation using outdoor air) and temperature control of room air |
| Outcomes | PRIMARY OUTCOMES
|
| Starting date | Retrospective registration; actual study start March 2019; first posted November 2018; estimated study completion October 2020 |
| Contact information | Daniel Croft daniel_croft@urmc.rochester.edu University of Rochester Medical Center, New York (USA) |
| Notes | N.B. will need pre‐cross‐over data for inclusion |
NCT03793192.
| Trial name or title | Promoting activity after COPD exacerbations: Aim 2 (PACE2) |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 64 Selection bias: "Allocation sequence will be concealed"; Blinding: outcomes assessor |
| Participants | Diagnosis of COPD (physician‐diagnosed); age ≥ 18 years; hospitalised as an inpatient, 23‐hour observation, or clinical decision unit; admitting respiratory conditions sensitive to the Centers for Medicare and Medicaid Services Hospital Readmission Reduction Program as listed (AECOPD, asthma/COPD overlap, decompensated heart failure, pneumonia, chronic airway disease) |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION PAC (PACE2) with pedometer
INTERVENTION pedometer |
| Outcomes | PRIMARY OUTCOME Physical activity: step count (averaged over 1 week, over time using repeated measures over 12 weeks) |
| Starting date | First posted January 2019; estimated study completion May 2022 |
| Contact information | Valentin Prieto‐Centurion, University of Illinois, Chicago (USA) |
| Notes |
NCT03794921.
| Trial name or title | Leveraging technology to address access and adherence to conventional hospital‐based PR in veterans with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 120 Blinding: outcomes assessor, "study staff communicating randomization assignments to subjects will be different from study staff conducting follow‐up outcome assessments" |
| Participants | Diagnosis of COPD (FER < 0.70 or chest CT evidence of emphysema or prior documentation of FER < 0.70 and clinical evidence of COPD defined as 10 pack‐year cigarette smoking history, dyspnoea or on bronchodilators); age ≥ 40 years; declined participation in conventional PR; medical clearance to participate in exercise; access to computer with Internet connection, a USB port or Bluetooth capability, and Windows XP/Vista/7/8/10 or higher, or Mac OSX 10.5 or higher operating system, or willing to come to VA Medical Center to use study computers; pedometer and accelerometer with > 90% accuracy compared to manual counts on short clinic walk |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION PAC (Every Step Counts)
NO INTERVENTION
|
| Outcomes | DEVICE (pedometer) PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; estimated start September 2019; estimated completion April 2024 |
| Contact information | Marilyn Moy Marilyn.Moy@va.gov; Eric Garshick Eric.Garshick@va.gov VA Boston Healthcare System (USA) |
| Notes | SPONSOR VA Office of Research and Development |
NCT03807310.
| Trial name or title | The effect of targeted nutrient supplementation on physical activity and HRQOL in advanced COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 166 Blinding: participant, investigator, outcomes assessor |
| Participants | Diagnosis of COPD (GOLD); age ≥ 18 years; medically stable; history of ≥ 2 moderate AECOPDs, ≥ 1 severe AECOPD (GOLD stage C and D) or FEV1 < 50% predicted and ≥ 1 moderate or severe AECOPD within 12 months |
| Interventions | DURATION OF INTERVENTION 12 months COMMON COMPONENT Counselling CONTACT once a month CONTENT healthy lifestyle (physical activity, smoking cessation, weight management) by motivational interviewing INTERVENTION Targeted nutrient supplement (once daily) with counselling INTERVENTION Placebo supplement (once daily) with counselling |
| Outcomes | DEVICE activPAL; Wear instructions: 1 week ASSESSMENT TIME POINTS
PRIMARY OUTCOMES
SECONDARY/OTHER OUTCOMES
|
| Starting date | First posted January 2019; estimated study completion May 2023 |
| Contact information | Rosanne Beijers r.beijers@maastrichtuniversity.nl; Harry Gosker h.gosker@maastrichtuniversity.nl Maastricht University Medical Center (The Netherlands) |
| Notes | Collaborator: Nutricia Research |
NCT03810755.
| Trial name or title | EfiKroniK research programme: effectiveness of physical exercise for people with chronic pathologies. Hybrid, clinical and implementation randomised trial |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 370 Blinding: care provider, outcomes assessor |
| Participants | Diagnosis of COPD; Age 18 to 75 years; BODE index (score 3 to 7); clinical stability (absence of exacerbation, antibiotic treatment, systemic corticosteroids or hospitalisation within 30 days); life expectancy > 2 years; colon, breast or lung solid cancers stage IV non‐small cell with standard first‐line chemotherapy treatment; malignant haemopathy with autologous transplant or lymphomas not localised, in treatment with immunotherapy; schizophrenia; adequate renal, hepatic and haematological function |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION "personalised exercise program" SETTING supervised nursing in primary and autonomous care afterwards, with support from community resources NO INTERVENTION |
| Outcomes | DEVICE Actigraph xGT3X‐BT (right iliac crest); Wear instructions: 1 week ASSESSMENT TIME POINTS
PRIMARY OUTCOMES
|
| Starting date | Retrospective registration; actual start January 2018; first posted January 2019; estimated study completion December 2020 |
| Contact information | Nere Mendizabal nere.mendizabalgallastegui@osakidetza.eus Primary Care Research Unit of Bizkaia, Bilbao (Spain) |
| Notes | SPONSOR Basque Health Service (Spain) N.B. will need COPD‐only data for inclusion in this review |
NCT03817294.
| Trial name or title | Personalised exercise training in COPD ‐ exploring the interaction between exercise physiology, exercise perception and training progression |
| Methods | DESIGN "pilot/feasibility study aiming to characterise exercise limitation at baseline and then conducting an abridged RCT with four training arms"; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 60 |
| Participants | Diagnosis of COPD (FEV1 < 80% predicted, FER < 0.7); age ≥ 40 years; MRC dyspnoea scale (score ≥ 3); stable dose of current regular medication within 4 weeks; clinically‐acceptable ECG at enrolment |
| Interventions |
INTERVENTION Eccentric cycling INTERVENTION Concentric cycling INTERVENTION Single‐leg cycling INTERVENTION Lower‐limb resistance training |
| Outcomes | DEVICE “seven‐day activity monitor” PRIMARY OUTCOME Adherence: training attendance SECONDARY OUTCOMES
|
| Starting date | Retrospectively registered; first posted January 2019; actual start October 2018; estimated study completion August 2019 |
| Contact information | Tom Ward t.ward@lboro.ac.uk Loughborough University (UK) |
| Notes |
NCT03869112.
| Trial name or title | The effectiveness of a physical activity intervention versus PR on cardiovascular risk markers for individuals with COPD: a feasibility study |
| Methods | DESIGN 3 groups; COMPARISONS intervention vs. intervention, intervention vs. no intervention; SAMPLE SIZE n = 60 |
| Participants | Diagnosis of COPD; age 40 to 85 years |
| Interventions | DURATION OF INTERVENTION 6 weeks INTERVENTION PAC SETTING home‐based, unsupervised CONTENT FitBit device: step targets (increase by 500 steps a week) INTERVENTION PR SETTING outpatient, supervised, group CONTENT exercise and education NO INTERVENTION |
| Outcomes | DEVICE Actigraph ASSESSMENT TIME POINTS
PRIMARY OUTCOMES
|
| Starting date | First posted March 2019; estimated study completion February 2020 |
| Contact information | Tareq Alotaibi T.alotaibi@lboro.ac.uk; David Stensel D.J.Stensel@lboro.ac.uk; Sally Singh sally.singh@uhl‐tr.nhs.uk University Hospitals of Leicester NHS Trust (UK) |
| Notes |
NCT03899558.
| Trial name or title | The role of humidified nasal high‐flow to reduce 30‐day hospital re‐admissions following severe exacerbations of COPD: a mixed‐methods feasibility study |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 80 Blinding: none |
| Participants | Emergency hospital admission with a primary diagnosis of AECOPD; smoking history ≥ 10 pack‐years; age 40 to 80 years; BMI ≤ 35kg/m2; to be discharged to home environment deemed safe to perform home assessments; live in the catchment area |
| Interventions | DURATION OF INTERVENTION hospital length of stay INTERVENTION Humidified nasal high‐flow device warmed, humidified air at flow rates of up to 60 litres a minute through a nasal cannula interface (intended delivery 30 litres a minute at 37 ºC if tolerated) NO INTERVENTION |
| Outcomes | DEVICE (triaxial accelerometer) (wrist) ASSESSMENT TIME POINTS Follow‐up: 30 days following discharge SECONDARY OUTCOMES
|
| Starting date | First posted April 2019; estimated study completion August 2021 |
| Contact information | Nicholas Hart nicholas.hart@gstt.nhs.uk; Rebecca D'Cruz rebecca.dcruz@gstt.nhs.uk Guy's and St Thomas' NHS Foundation Trust (UK) |
| Notes |
NL3827.
| Trial name or title | PRACTISS COPD; PR of COPD: a trial of sustained internet based self‐management support |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 100 Blinding: single |
| Participants | Pulmonologist‐diagnosed COPD (FER < 0.7); COPD most important limiting factor; PR completion |
| Interventions | DURATION OF INTERVENTION 1 year following PR INTERVENTION self‐management by internet "PatientCoach‐platform" Tools are available to guide discussion; participant determines goal, identifies barriers and plans for overcoming the barriers NO INTERVENTION |
| Outcomes | ASSESSMENT TIME POINTS
PRIMARY OUTCOME HRQOL: CRQ SECONDARY OUTCOMES
|
| Starting date | Study dates February 2013 to February 2015 |
| Contact information | Jacob Sont j.k.sont@lumc.nl Leids Universitair Medisch Centrum (The Netherlands) |
| Notes | FUNDING Netherlands Asthma Foundation Email sent to enquire regarding objective assessment of physical activity and availability of results |
NL5277.
| Trial name or title | Efficacy of a physical activity coaching system for patients with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 90 Blinding: none |
| Participants | Diagnosis of COPD (GOLD); age > 45 years; referred for PR; clinical stability within 4 weeks (pulmonary infections or AECOPD); absence of recent myocardial Infarction (within 3 months), unstable angina, other significant cardiac problems, resting systolic blood pressure > 180 mmHg, resting diastolic blood pressure > 100 mmHg or tachycardia; absence of significant orthopaedic, neurological, cognitive and/or psychiatric impairment restricting mobility; internet access at home |
| Interventions | DURATION OF INTERVENTION 8 weeks following inpatient PR INTERVENTION PAC Philips physical activity coaching system NO INTERVENTION wears activity monitor no coaching or insight into physical activity |
| Outcomes | ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: (not defined) |
| Starting date | Study dates April 2015 to March 2018 |
| Contact information | Marian Dekker marian.dekker@philips.com Philips Research |
| Notes | FUNDING Philips Research and CIRO+ expertise Center (The Netherlands) Email sent 23 August 2019 to ask about possible relationship with Priori 2017 or Saini 2017 |
RBR‐3zmh3r.
| Trial name or title | Effects of the inclusion of a functional circuit to aerobic and resistance training on functionality, physical activity in daily life and immuno‐metabolic response of patients with COPD: a randomised clinical trial with follow‐up |
| Methods | DESIGN 3 groups; COMPARISONS intervention vs. intervention, intervention vs. no intervention; SAMPLE SIZE n = 75 Blinding: none |
| Participants | Diagnosis of COPD (GOLD); age 18 to 100 years; clinically stable (no AECOPD or changes in medications within 30 days); non‐smokers; no home oxygen therapy; no pathological conditions that prevent physical activity, severe or unstable heart disease, other pathological condition that may influence the systemic inflammatory process; not participating in another systematic exercise programme |
| Interventions |
COMMON COMPONENT Aerobic training (treadmill)
INTERVENTION "GTF"
INTERVENTION "GTC" Aerobic training only NO INTERVENTION including respiratory physiotherapy techniques |
| Outcomes | OUTCOME MEASURES
|
| Starting date | Prospectively registered; planned last enrolment July 2019 |
| Contact information | Ercy Mara Cipulo Ramos ercy@fct.unesp.br; Fabiano Lima fabiano_ffl@hotmail.com Universidade Estadual Julio de Mesquita Filho, Presidente Prudente, São Paulo (Brazil) |
| Notes | FUNDING "Fundação de Amparo a Pesquisa do Estado de São Paulo (Brazil)" N.B. need to confirm objective assessment of physical activity for inclusion |
UMIN000027190.
| Trial name or title | The effect of the combination treatment with tiotropium and olodaterol compared to tiotropium on symptoms, respiratory functions and physical activity in maintenance‐naïve Japanese patients with COPD |
| Methods | DESIGN 2 groups; COMPARISON intervention vs. intervention; SAMPLE SIZE n = 80 Blinding: none |
| Participants | Diagnosis of COPD (FEV1 < 80% predicted, FER < 0.7); smoking history (current or former); age 40 to 85 years; maintenance treatment‐naïve |
| Interventions | DURATION OF INTERVENTION 12 weeks INTERVENTION LAMA/LABA (tiotropium and olodaterol) INTERVENTION LAMA (tiotropium) |
| Outcomes | DEVICE (triaxial accelerometer) ASSESSMENT TIME POINTS
SECONDARY OUTCOMES
|
| Starting date | Disclosure of study information April 2017; last follow‐up May 2019; recruitment status: no longer recruiting |
| Contact information | Koichiro Takahashi takahak@cc.saga‐u.ac.jp Division of Respiratory Medicine, Saga University (Japan) |
| Notes | FUNDING Nippon Boehringer Ingelheim Co, Ltd |
UMIN000031173.
| Trial name or title | Combined effect of progressive resistance training and physical activity counselling in patients with COPD: a randomised controlled cross‐over study |
| Methods | DESIGN 2 groups, cross‐over; COMPARISON intervention vs. no intervention; SAMPLE SIZE n = 15 Blinding: none |
| Participants | Diagnosis of COPD (GOLD); age 18 to 90 years |
| Interventions | DURATION OF INTERVENTION 8 weeks INTERVENTION exercise training and PAC CONTACT 1 session a week CONTENT
NO INTERVENTION |
| Outcomes | DEVICE (pedometer) ASSESSMENT TIME POINTS
PRIMARY OUTCOME Physical activity: step count SECONDARY OUTCOMES
|
| Starting date | Disclosure of study information February 2018; Recruitment status: completed |
| Contact information | Chiharu Fujisawa chiharu.fujisawa@shinkohp.or.jp Shinko Hospital Rehabilitation Center (Japan) |
| Notes | Funding: Japan Science and Technoligy Agency N.B. will need pre‐cross‐over data for inclusion |
UMIN000033093.
| Trial name or title | The effect of comprehensive respiratory rehabilitation using cloud system on exacerbation of patients with COPD at home |
| Methods | DESIGN 2 groups; COMPARISON intervention vs..no intervention; SAMPLE SIZE n = 50 Blinding: none |
| Participants | Diagnosis of COPD (Guidelines for Diagnosis and Treatment of COPD 4th Edition, Japan Respiratory Society); age ≥ 65 years; stable; attending Shinshu University Medical School Hospital for the purpose of diagnosis and treatment of COPD |
| Interventions |
INTERVENTION "comprehensive respiratory rehabilitation" SETTING home CONTACT multi‐occupational co‐operation tool CONTENT Exercise; physical activity instruction in daily life; education NO INTERVENTION |
| Outcomes | SECONDARY OUTCOME Physical activity |
| Starting date | Disclosure of the study information July 2018 |
| Contact information | Shohei Kawachi drodman@shinshu‐u.ac.jp Shinshu University Hospital Rehabilitation Department (Japan) |
| Notes | N.B. need to confirm objective assessment of physical activity for inclusion |
Zanaboni 2016.
| Trial name or title | Long‐term integrated telerehabilitation of COPD patients: a multicentre randomised controlled trial (iTrain) |
| Methods | DESIGN 3 groups; COMPARISONS intervention vs. intervention, intervention vs. no intervention; SETTING Australia, Denmark, Norway; SAMPLE SIZE n = 120 |
| Participants | Diagnosis of COPD (FEV1 < 80% predicted, FER < 0.7); age 40 to 80 years; ≥ 1 COPD‐related emergency department presentation or hospitalisation within 12 months |
| Interventions | STUDY DURATION two years "Any participant in the trial can undertake a traditional PR program at any time during the study period if it is considered clinically indicated by their usual treating team" INTERVENTION Telerehabilitation SETTING home CONTACT
AEROBIC TRAINING treadmill, ≥ 30 minutes
STRENGTH TRAINING 2 to 3 sessions a week INTERVENTION Unsupervised exercise training SETTING unsupervised, home TRAINING treadmill Individualised, prescribed as for telerehabilitation arm, no review or progression Record sessions in paper‐based diary NO INTERVENTION |
| Outcomes | DEVICE SenseWear Armband (software version 7.0) (left upper arm)
ASSESSMENT TIME POINTS
SECONDARY OUTCOMES
|
| Starting date | Prospectively registered; study start October 2014; final data collection for primary outcome measure December 2018 |
| Contact information | Paolo Zanaboni paolo.zanaboni@telemed.no University Hospital of North Norway, Tromsø (Norway) |
| Notes | FUNDING "This study was funded by the Research Council of Norway (Project Grant 228919/H10) and the Northern Norway Regional Health Authority (Project Grants HST1117‐13 and HST1118‐13)." CONFLICT OF INTEREST "The authors declare that they have no competing interests." |
AECOPD: acute exacerbation of COPD; BMI: body mass index; CAT: COPD assessement test; CCQ: clinical COPD questionnaire; COPD: chronic obstructive pulmonary disease; CPET: cardiopulmonary exercise test; CRQ: chronic respiratory disease questionnaire; CT: computerised tomography; ECG: electrocardiogram; EE: energy expenditure; EPAP: expiratory positive airway pressure; ESWT: time walked on endurance shuttle walk test; EQ5D: EuroQol 5 dimensions questionnaire; FER: forced expiratory ratio; FEV1: forced expiratory volume in one second; GOLD: Global Initiative for Chronic Obstructive Lung Disease; HRQOL: health‐related quality of life; ICD‐10: International Statistical Classification of Diseases and Related Health Problems 10th Revision; ICS: inhaled corticosteriod; ILD: intersitial lung disease; IPAP: inspiratory positive airway pressure; ISWD: distance walked on incremental shuttle walk test; LABA: long‐acting beta2 agonist; LAMA: long‐acting muscarinic antagonist; LIPA: light intensity physical activity; LTOT: long term oxygen therapy; MRC: Medical Research Council; METs: metabolic equivalents; MVPA: moderate to vigorous physical activity; 1RM: one repetition maximum; PAL: physical activity level; Pimax: maximal inspiratory pressure; PR: pulmonary rehabilitation; RV: residual volume; SAE: serious adverse event; SF36: Medical Outcomes Survey 36‐item short‐form health survey questionnaire; SGRQ: St George's respiratory questionnaire; SpO2: oxygen saturation; 6MWD: distance walked on six‐minute walk test; 6MWT: six‐minute walk test; TLC: total lung capacity; VO2: peak oxygen uptake
Differences between protocol and review
The protocol stated the intent to exclude cross‐over trials due to the potential carry‐over effects of behavioural interventions. However, where pre‐cross‐over data were available from study authors, we included them to maximise coverage of relevant data (Beeh 2014; Hartman 2016; Magnussen 2017; Ng 2015; Watz 2016).
After reviewing the body of literature generated by the search results, a comparison was evident that we had not prespecified in the protocol and facilitated the inclusion of additional data that could be particularly relevant for clinical decision‐making. This comparison was defined as one or more interventions to increase physical activity versus another intervention to increase physical activity (intervention versus intervention) and included data from nine studies (Chaplin 2017; Felcar 2018; Holland 2017; O'Neill 2018; Polkey 2018; Probst 2011; Rinaldo 2017; Sena 2013; Widyastuti 2018).
We undertook characterisation of interventions as 'pulmonary rehabilitation' or 'exercise training' as classification by authors, rather than according to the McCarthy 2015 definition as stated in the protocol, since sufficient detail was not available in all cases to make an independent determination.
We amended outcomes for the 'Summary of findings' tables to only include 'Time in moderate‐to‐vigorous physical activity' as the outcome with the most evidence for associations with improved health outcomes.
We made changes to the wording of Background and Methods for clarity, following the peer‐review process.
Contributions of authors
Angela Burge: initiation and writing of protocol and manuscript, data extraction and analysis.
Narelle Cox: protocol development and review, data extraction, manuscript review.
Michael Abramson: protocol development and review, data extraction and analysis, manuscript review.
Anne Holland: protocol development and review, data analysis, manuscript review.
Contributions of editorial team
Rebecca Fortescue (Co‐ordinating Editor, contact editor): edited the review; advised on methodology, interpretation and content.
Chris Cates (Co‐ordinating Editor): checked the data entry prior to the full write‐up of the review; approved the final review prior to publication.
Emma Dennett (Managing Editor): co‐ordinated the editorial process; advised on interpretation and content; edited the review.
Emma Jackson (Assistant Managing Editor): conducted peer review; obtained translations; edited the Plain Language Summary and reference sections of the protocol and the review.
Elizabeth Stovold (Information Specialist): designed the search strategy; ran the searches; edited the search methods section.
Sources of support
Internal sources
The authors declare that no such funding was received for this systematic review, Other.
External sources
National Health and Medical Research Council, Australia.
Declarations of interest
Angela Burge received a PhD stipend from the National Health and Medical Research Council (NHMRC), Australia. This Cochrane Review forms a part of those PhD studies. The National Health and Medical Research Council (NHMRC) supports the independent conduct and publication of this Cochrane Review.
Narelle Cox is the holder of a NHMRC Early Career Fellowship. She presented workshops relating to pulmonary rehabilitation at the 2018 National General Practitioners Meeting sponsored by Boeringher Ingelheim.
Michael Abramson holds investigator‐initiated grants from Pfizer and Boehringer‐Ingelheim for unrelated research, undertook unrelated consultancies for AstraZeneca and Sanofi, and received assistance with conference attendance from Boehringer‐Ingelheim and Sanofi.
Anne Holland has received fees from AstraZeneca and Boehringer Ingelheim for non‐promotional speaking engagements (unrelated to the present work).
Three review authors (AB, NC and AH) were co‐authors on an included study (Holland 2017), so an independent co‐author (MA) undertook the assessment of risks of bias.
New
References
References to studies included in this review
Alison 2019 {published data only}
- Alison JA, McKeough ZJ, Jenkins SC, Holland AE, Hill K, Morris NR, et al. A randomised controlled trial of supplemental oxygen versus medical air during exercise training in people with chronic obstructive pulmonary disease: supplemental oxygen in pulmonary rehabilitation trial (SuppORT) [protocol]. BMC Pulmonary Medicine 2016;1:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alison JA, McKeough ZJ, Leung RW, Holland AE, Hill K, Morris NR, et al. Oxygen compared to air during exercise training in COPD with exercise‐induced desaturation. European Respiratory Journal 2019;53:1802429. [DOI] [PubMed] [Google Scholar]
Altenburg 2015 {published data only}
- Altenburg W, Wempe J, Greef M, Hacken N, Kerstjens H. Short‐ and long‐term effects of a physical activity counselling program in COPD [abstract]. European Respiratory Journal 2014;44:3490. [Google Scholar]
- Altenburg WA, Hacken NH, Bossenbroek L, Kerstjens HA, Greef MH, Wempe JB. Short‐ and long‐term effects of a physical activity counselling programme in COPD: a randomized controlled trial. Respiratory Medicine 2015;109(1):112‐21. [DOI] [PubMed] [Google Scholar]
Arbillaga‐Etxarri 2018 {published data only}
- Arbillaga‐Etxarri A, Gimeno‐Santos E, Balcells E, Barberan‐Garcia A, Benet M, Celorrio N, et al. Effectiveness of an intervention of urban training in patients with COPD: a randomized controlled trial [abstract]. European Respiratory Journal 2017;50:OA513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arbillaga‐Etxarri A, Gimeno‐Santos E, Barberan‐Garcia A, Balcells E, Benet M, Borrell E, et al. Long‐term efficacy and effectiveness of a behavioural and community‐based exercise intervention (Urban Training™) to increase physical activity in patients with COPD. A randomised controlled trial. European Respiratory Journal 2018;52(4):1800063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arbillaga‐Etxarri A, Torrent‐Pallicer J, Gimeno‐Santos E, Barberan‐Garcia A, Delgado A, Balcells E, et al. Validation of walking trails for the urban training of chronic obstructive disease patients. PLoS ONE 2016;11(1):e0146705. [DOI] [PMC free article] [PubMed] [Google Scholar]
Beeh 2014 {published and unpublished data}
- Beeh KM, Watz H, Puente‐Maestu L, Teresa L, Jarreta D, Caracta C, et al. Aclidinium improves exercise endurance, dyspnea, lung hyperinflation, and physical activity in patients with COPD: a randomized, placebo‐controlled, crossover trial. BMC Pulmonary Medicine 2014;14(1):209. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bender 2016 {published data only}
- Bender BG, Depew A, Emmett A, Goelz K, Make B, Sharma S, et al. A patient‐centered walking program for COPD. Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation 2016;3(4):769‐77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bender BG, Make BJ, Emmett A, Sharma S, Stempel D. Enhancing physical activity in patients with chronic obstructive pulmonary disease (COPD) through a program of patient selected goals [abstract]. American Journal of Respiratory and Critical Care Medicine 2015;191:A2458. [Google Scholar]
Benzo 2016 {published data only (unpublished sought but not used)}
- Benzo R, McEvoy C. Effect of health coaching delivered by a respiratory therapist or nurse on self‐management abilities in severe COPD: analysis of a large randomized study. Respiratory Care 2019;64(9):1065‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benzo R, Vickers K, Ernst D, Tucker S, McEvoy C, Lorig K. Development and feasibility of a self‐management intervention for chronic obstructive pulmonary disease delivered with motivational interviewing strategies. Journal of Cardiopulmonary Rehabilitation and Prevention 2013;33(2):113‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benzo R, Vickers K, Novotny PJ, Tucker S, Hoult J, Neuenfeldt P, et al. Health coaching and chronic obstructive pulmonary disease rehospitalization: a randomized study. American Journal of Respiratory and Critical Care Medicine 2016;194(6):672‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
Blumenthal 2014 {published data only}
- Blumenthal JA, Emery CF, Smith PJ, Keefe FJ, Welty‐Wolf K, Mabe S, et al. The effects of a telehealth coping skills intervention on outcomes in chronic obstructive pulmonary disease: primary results from the INSPIRE‐II study. Psychosomatic Medicine 2014;76(8):581‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blumenthal JA, Keefe FJ, Babyak MA, Fenwick CV, Johnson JM, Stott K, et al. Caregiver‐assisted coping skills training for patients with COPD: background, design, and methodological issues for the INSPIREII study. Clinical Trials 2009;6(2):172‐84. [DOI] [PMC free article] [PubMed] [Google Scholar]
Borges 2014 {published and unpublished data}
- Borges R, Carvalho CR. Effect of resistance training during hospitalization in the systemic inflammation, functional capacity and muscle strength in COPD patients [abstract]. European Respiratory Journal 2011;38:1890. [Google Scholar]
- Borges RC, Carvalho CR. Impact of resistance training in chronic obstructive pulmonary disease patients during periods of acute exacerbation. Archives of Physical Medicine and Rehabilitation 2014;95(9):1638‐45. [DOI] [PubMed] [Google Scholar]
Breyer 2010 {published data only (unpublished sought but not used)}
- Breyer MK, Breyer‐Kohansal R, Funk GC, Dornhofer N, Spruit MA, Wouters EF, et al. Nordic walking improves daily physical activities in COPD: a randomised controlled trial. Respiratory Research 2010;11:112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Breyer MK, Kohansal R, Burghuber OC, Hartl S. The effects of Nordic walking on exercise capacity and physical activity in daily life (AoDL) in COPD [abstract]. European Respiratory Journal 2008;32(Supp 52):1754. [Google Scholar]
Burtin 2015 {published data only}
- Burtin C, Lander D, Remoortel H, Gosselinki R, Decramer M, Janssens W, et al. Physical activity counseling and long‐term effects of pulmonary rehabilitation [abstract]. American Journal of Respiratory and Critical Care Medicine 2012;185:A3675. [Google Scholar]
- Burtin C, Langer D, Remoortel H, Demeyer H, Gosselink R, Decramer M, et al. Physical activity counselling during pulmonary rehabilitation in patients with COPD: a randomised controlled trial. PLOS One 2015;10(12):e0144989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burtin C, Langer D, Remoortel J, Demeyer H, Gosselink R, Decramer M, et al. Correction: Physical activity counselling during pulmonary rehabilitation in patients with COPD: a randomised controlled trial. PLOS One 2016;11(2):e0148705. [DOI] [PMC free article] [PubMed] [Google Scholar]
Casaburi 2012 {published data only}
- Casaburi R, Porszasz J, Hecht A, Tiep B, Albert RK, Anthonisen NR, et al: for the COPD Clinical Research Network. Influence of lightweight ambulatory oxygen on oxygen use and activity patterns of COPD patients receiving long‐term oxygen therapy. Journal of Chronic Obstructive Pulmonary Disease 2012;9(1):3‐11. [DOI] [PubMed] [Google Scholar]
Chaplin 2017 {published data only}
- Barnes A, Newby C, Chaplin E, Houchen‐Wolloff, Singh SJ. Purposeful physical activity in COPD patients comparing standard and web based pulmonary rehabilitation [abstract]. European Respiratory Journal 2016;48(Supp 60):PA2056. [Google Scholar]
- Chaplin E, Hewitt S, Apps L, Bankart J, Pulikottil‐Jacob R, Boyce S, et al. Interactive web‐based pulmonary rehabilitation programme: a randomised controlled feasibility trial. BMJ Open 2017;7(3):e013682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaplin E, Hewitt S, Apps L, Edwards K, Brough C, Glab A, et al. An interactive web‐based programme: a randomised controlled feasibility trial [abstract]. European Respiratory Journal 2016;48(Suppl 60):PA2064. [Google Scholar]
- Chaplin E, Hewitt S, Apps L, Edwards K, Brough C, Glab A, et al. The evaluation of an interactive web‐based pulmonary rehabilitation programme: protocol for the WEB SPACE for COPD feasibility study. BMJ Open 2015;5(8):e008055. [DOI] [PMC free article] [PubMed] [Google Scholar]
Charususin 2018 {published data only}
- Charususin N, Gosselink R, Decramer M, Demeyer H, McConnell A, Saey D, et al. Randomised controlled trial of adjunctive inspiratory muscle training for patients with COPD. Thorax 2018;73(10):942‐50. [DOI] [PubMed] [Google Scholar]
- Charususin N, Gosselink R, Decramer M, McConnell A, Saey D, Maltais F, et al. Inspiratory muscle training protocol for patients with chronic obstructive pulmonary disease (IMTCO study): A multicentre randomised controlled trial. BMJ Open 2013;3(8):e003101. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cruz 2016 {published data only}
- Cruz J, Brooks D, Marques A. Walk2Bactive: a randomised controlled trial of a physical activity‐focused behavioural intervention beyond pulmonary rehabilitation in chronic obstructive pulmonary disease. Chronic Respiratory Disease 2016;13(1):57‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
Curtis 2016 {published data only}
- Curtis KJ, Meyrick VM, Mehta B, Haji GS, Li K, Montgomery H, et al. Angiotensin‐converting enzyme inhibition as an adjunct to pulmonary rehabilitation in chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 2016;194(11):1349‐57. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dal Negro 2012 {published data only (unpublished sought but not used)}
- Dal Negro RW, Aquilani R, Bertacco S, Boschi F, Micheletto C, Tognella S. Comprehensive effects of supplemented essential amino acids in patients with severe COPD and sarcopenia. Monaldi Archives of Chest Disease 2010;73(1):25‐33. [DOI] [PubMed] [Google Scholar]
- Dal Negro RW, Testa A, Aquilani R, Tognella S, Pasini E, Barbieri A, et al. Essential amino acid supplementation in patients with severe COPD: a step towards home rehabilitation. Monaldi Archives of Chest Disease 2012;77(2):67‐75. [DOI] [PubMed] [Google Scholar]
De Blok 2006 {published data only}
- Blok BM, Greef MH, Hacken NH, Sprenger SR, Postema K, Wempe JB. The effects of a lifestyle physical activity counseling program with feedback of a pedometer during pulmonary rehabilitation in patients with COPD a pilot study [abstract]. European Respiratory Journal 2005;26(Suppl 49):548. [DOI] [PubMed] [Google Scholar]
- Blok BM, Greef MH, Hacken NH, Sprenger SR, Postema K, Wempe JB. The effects of a lifestyle physical activity counseling program with feedback of a pedometer during pulmonary rehabilitation in patients with COPD: a pilot study. Patient Education and Counseling 2006;61(1):48‐55. [DOI] [PubMed] [Google Scholar]
Demeyer 2017 {published and unpublished data}
- Demeyer H, Louvaris Z, Frei A, Rabinovich RA, Jong C, Gimeno‐Santos E, et al: on behalf of the Mr Papp PROactive study group and the PROactive consortium. Physical activity is increased by a 12‐week semiautomated telecoaching programme in patients with COPD: a multicentre randomised controlled trial. Thorax 2017;72(5):415‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Demeyer H, Louvaris Z, Tanner R, Rubio N, Frei A, Jong C, et al. Increasing physical activity in patients with COPD using a telecoaching program: a multicentre RCT [abstract]. European Respiratory Journal 2015;46:OA278. [Google Scholar]
- Loeckx M, Louvaris Z, Tanner R, Rubio N, Frej A, Jong C, et al. Contact time between patients with COPD and coach during an activity telecoaching intervention: Impact on the intervention effect [abstract]. European Respiratory Journal 2016;48(Suppl 60):OA4817. [Google Scholar]
- Loeckx M, Louvaris Z, Tanner RJ, Yerramasu C, Busching G, Frei A, et al. Compliance with a three month telecoaching program to enhance physical activity in patients with Chronic Obstructive Pulmonary Disease [abstract]. American Journal of Respiratory and Critical Care Medicine 2015;191:A2007. [Google Scholar]
- Loeckx M, Rabinovich RA, Demeyer H, Louvaris Z, Tanner R, Rubio N, et al. Smartphone‐based physical activity telecoaching in chronic obstructive pulmonary disease: mixed‐methods study on patient experiences and lessons for implementation. JMIR mHealth and uHealth 2018;6(2):e200. [DOI] [PMC free article] [PubMed] [Google Scholar]
De Roos 2017 {published and unpublished data}
- Roos P, Lucas C, Strijbos JH, Trijffel E. Effectiveness of a combined exercise training and home‐based walking programme on physical activity compared with standard medical care in moderate COPD: a randomised controlled trial. Physiotherapy 2017;104(1):116‐21. [DOI] [PubMed] [Google Scholar]
Duiverman 2008 {published data only}
- Duiverman ML, Bladder G, Wempe JB, Kerstjens HA, Zijlstra JG, Wijkstra PJ. Chronic ventilatory support improves the outcomes of rehabilitation in hypercapnic COPD patients [abstract]. American Thoracic Society International Conference; 2008 May 16‐21; Toronto. 2008:A557.
- Duiverman ML, Wempe JB, Bladder G, Jansen DF, Kerstjens HA, Zijlstra JG, et al. Nocturnal non‐invasive ventilation in addition to rehabilitation in hypercapnic patients with COPD. Thorax 2008;63(12):1052‐7. [DOI] [PubMed] [Google Scholar]
Effing 2011 {published data only}
- Effing T, Zielhuis G, Kerstjens H, Valk P, Palen J. Community based physiotherapeutic exercise in COPD self‐management: a randomised controlled trial. Respiratory Medicine 2011;105(3):418‐26. [DOI] [PubMed] [Google Scholar]
- Zwerink M, Effing T, Kerstjens HA, Valk P, Brusse‐Keizer M, Zielhuis G, et al. Cost‐effectiveness of a community‐based exercise programme in COPD self‐management. Journal of Chronic Obstructive Pulmonary Disease 2016;13(2):214‐23. [DOI] [PubMed] [Google Scholar]
- Zwerink M, Palen J, Kerstjens HA, Valk P, Brusse‐Keizer M, Zielhuis G, et al. A community‐based exercise programme in COPD self‐management: two years follow‐up of the COPD‐II study. Respiratory Medicine 2014;108(10):1481‐90. [DOI] [PubMed] [Google Scholar]
- Zwerink M, Palen J, Kerstjens HA, Valk P, Brusse‐Keizer M, Zielhuis G, et al. A community‐based exercise programme in COPD self‐management: two‐year follow‐up of the COPD‐II study [abstract]. European Respiratory Journal 2014;44:1711. [Google Scholar]
- Zwerink M, Palen J, Valk P, Brusse‐Keizer M, Effing T. Relationship between daily physical activity and exercise capacity in patients with COPD. Respiratory Medicine 2013;102(2):242‐8. [DOI] [PubMed] [Google Scholar]
Egan 2010 {published and unpublished data}
- Egan C, Costello R, Deering B, McCormack NM, Blake C. Physical activity in COPD patients following pulmonary rehabilitation [abstract]. European Respiratory Society 20th Annual Congress; 2010 Sep 18‐22; Barcelona. 2010:E3535.
- Egan C, Deering BM, Blake C, Fullen BM, McCormack NM, Spruit MA, et al. Short term and long term effects of pulmonary rehabilitation on physical activity in COPD. Respiratory Medicine 2012;106(12):1671‐9. [DOI] [PubMed] [Google Scholar]
Felcar 2018 {published data only}
- Felcar JM, Probst VS, Carvalho DR, Merli MF, Mesquita R, Vidotto LS, et al. Effects of exercise training in water and on land in patients with COPD: a randomised clinical trial. Physiotherapy 2018;104(4):408‐16. [DOI] [PubMed] [Google Scholar]
- Felcar JM, Probst VS, Carvalho DR, Merli MF, Mesquita RB, Vidotto LS, et al. Effects of exercise training in water and on land in patients with COPD [abstract]. European Respiratory Journal 2015;46(Suppl 59):PA2396. [Google Scholar]
Gamper 2019 {published data only}
- Gamper E, Schmidt U, Bansi J, Kool J. Outdoor walking training compared to cycle ergometer training in severe COPD: a randomized controlled feasibility trial. COPD: Journal of Chronic Obstructive Pulmonary Disease 2019;16(1):37‐44. [DOI] [PubMed] [Google Scholar]
Goris 2003 {published data only}
- Goris AH, Vermeeren MA, Wouters EF, Schols AM, Westerterp KR. Energy balance in depleted ambulatory patients with chronic obstructive pulmonary disease: the effect of physical activity and oral nutritional supplementation. British Journal of Nutrition 2003;89(5):725‐9. [DOI] [PubMed] [Google Scholar]
Hartman 2016 {published data only}
- Hartman JE, Klooster K, Slebos DJ, Hacken NH. Daily physical activity significantly improves after endobronchial valve treatment in patients with emphysema [abstract]. European Respiratory Journal 2015;46:OA1767. [Google Scholar]
- Hartman JE, Klooster K, Slebos DJ, Hacken NH. Improvement of physical activity after endobronchial valve treatment in emphysema patients. Respiratory Medicine 2016;117:116‐21. [DOI] [PubMed] [Google Scholar]
Holland 2017 {published data only}
- Holland AE, Mahal A, Hill CJ, Lee AL, Burge AT, Cox NS, et al. Home‐based rehabilitation for COPD using minimal resources: a randomised, controlled equivalence trial. Thorax 2017;72(1):57‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holland AE, Mahal A, Hill CJ, Lee AL, Burge AT, Cox NS, et al. Low cost home‐based pulmonary rehabilitation for chronic obstructive pulmonary disease: a randomized controlled equivalence trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2016;193:A2620. [Google Scholar]
- Holland AE, Mahal A, Hill CJ, Lee AL, Burge AT, Moore R, et al. Benefits and costs of home‐based pulmonary rehabilitation in chronic obstructive pulmonary disease ‐ a multi‐centre randomised controlled equivalence trial [protocol]. BMC Pulmonary Medicine 2013;13:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahham A, McDonald CF, Mahal A, Lee AL, Hill CJ, Burge AT, et al. Participation in physical activity during center and home‐based pulmonary rehabilitation for people with COPD: a secondary analysis of a randomized controlled trial. Journal of Cardiopulmonary Rehabilitation and Prevention 2019;39:E1‐4. [DOI] [PubMed] [Google Scholar]
- Liacos A, McDonald CF, Mahal A, Hill CJ, Lee AL, Burge AT, et al. The Pulmonary Rehabilitation Adapted Index of Self‐Efficacy (PRAISE) tool predicts reduction in sedentary time following pulmonary rehabilitation in people with chronic obstructive pulmonary disease (COPD). Physiotherapy 2019;105(1):90‐7. [DOI] [PubMed] [Google Scholar]
Hornikx 2015 {published data only}
- Hornikx M, Demeyer H, Camillo CA, Janssens W, Troosters T. The effects of a physical activity counseling program after an exacerbation in patients with chronic obstructive pulmonary disease: a randomized controlled pilot study. BMC Pulmonary Medicine 2015;15:136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hornikx M, Demeyer H, Camillo CA, Janssens W, Troosters T. The effects of physical activity coaching in patients with COPD after an acute exacerbation [abstract]. European Respiratory Journal 2014;44:1920. [Google Scholar]
Hospes 2009 {published data only (unpublished sought but not used)}
- Hospes G, Bossenbroek L, Hacken NH, Hengel P, Greef MH. Enhancement of daily physical activity increases physical fitness of outclinic COPD patients: results of an exercise counseling program. Patient Education and Counseling 2009;75(2):274‐8. [DOI] [PubMed] [Google Scholar]
- Hospes G, Hacken NH, Hengel P, Greef MH. Pedometer‐based exercise counseling in COPD [abstract]. American Thoracic Society International Conference; 2007 May 18‐23; San Francisco. 2007; Vol. 175:A601.
Jolly 2018 {published data only}
- Jolly K, Sidhu MS, Hewitt CA, Coventry PA, Daley A, Jordan R, et al. Self management of patients with mild COPD in primary care: randomised controlled trial. BMJ 2018;361:k2241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sidhu MS, Daley A, Jordan R, Coventry PA, Heneghan C, Jowett S, et al. Patient self‐management in primary care patients with mild COPD – protocol of a randomised controlled trial of telephone health coaching. BMC Pulmonary Medicine 2015;15(1):16. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kanabar 2015 {published and unpublished data}
- Kanabar P, Warrington V, Houchen‐Wolloff L, Singh SJ. Investigating the profile of physical activity in COPD patients 7 days post discharge from a respiratory‐related admission. Does brief advice have an effect? [abstract]. Thorax 2015;70(Suppl 3):A146. [Google Scholar]
Kawagoshi 2015 {published data only}
- Kawagoshi A, Kiyokawa N, Iwakura M, Okura K, Sugawara K, Takahashi H, Sakata S, Satake M, Shioya T. Effects of low‐intensity exercise and home‐based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with COPD [abstract]. European Respiratory Journal 2015;46:PA3563. [DOI] [PubMed] [Google Scholar]
- Kawagoshi A, Kiyokawa N, Sugawara K, Takahashi H, Sakata S, Satake M, et al. Effects of low‐intensity exercise and home‐based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with chronic obstructive pulmonary disease. Respiratory Medicine 2015;109(3):364‐71. [DOI] [PubMed] [Google Scholar]
Larson 2014 {published data only (unpublished sought but not used)}
- Covey MK, McAuley E, Kapella MC, Collins EG, Alex CG, Berbaum ML, et al. Upper‐body resistance training and self‐efficacy enhancement in COPD. Journal of Pulmonary and Respiratory Medicine 2012;Suppl 9:001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson JL, Covey MK, Kapella MC, Alex CG, McAuley E. Self‐efficacy enhancing intervention increases light physical activity in people with chronic obstructive pulmonary disease. International Journal of Chronic Obstructive Pulmonary Disease 2014;9:1081‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Loeckx 2018 {published data only}
- Loeckx M, Rodrigues F, Demeyer H, Janssens W, Troosters T. Improving physical activity to obtain sustainable benefits in extra‐pulmonary consequences of COPD after pulmonary rehabilitation: a randomized controlled trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A2452. [Google Scholar]
Lord 2012 {published data only (unpublished sought but not used)}
- Lord VM, Hume VJ, Kelly JL, Cave P, Silver J, Waldman M, et al. Effects of 'singing for breathing' in patients with chronic obstructive pulmonary disease (COPD) ‐ a randomized controlled trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2012;185:A5788. [Google Scholar]
- Lord VM, Hume VJ, Kelly JL, Cave P, Silver J, Waldman M, et al. Singing classes for chronic obstructive pulmonary disease: a randomized controlled trial. BMC Pulmonary Medicine 2012;12:69. [DOI] [PMC free article] [PubMed] [Google Scholar]
Louvaris 2016 {published and unpublished data}
- Kortianou E, Louvaris Z, Spetsioti S, Vasilopoulou M, Chynkiamis N, Nasis I, et al. High‐intensity interval exercise training improves daily physical activity levels in COPD [abstract]. European Respiratory Journal 2014;44(Suppl 58):1709. [Google Scholar]
- Louvaris Z, Spetsioti S, Kortianou EA, Vasilopoulou M, Nasis I, Kaltsakas G, et al. Aerobic interval training induces clinically meaningful effects in daily physical activity in COPD [abstract]. European Respiratory Journal 2016;48:PA2053. [DOI] [PubMed] [Google Scholar]
- Louvaris Z, Spetsioti S, Kortianou EA, Vasilopoulou M, Nasis I, Kaltsakas G, et al. Interval training induces clinically meaningful effects in daily activity levels in COPD. European Respiratory Journal 2016;48(2):567‐70. [DOI] [PubMed] [Google Scholar]
Maddocks 2016 {published data only}
- Maddocks M, Nolan CM, Man WD, Polkey MI, Hart N, Gao W, et al. Neuromuscular electrical stimulation to improve exercise capacity in patients with severe COPD: a randomised double‐blind, placebo‐controlled trial. Lancet Respiratory Medicine 2016;4(1):27‐36. [DOI] [PubMed] [Google Scholar]
Magnussen 2017 {published and unpublished data}
- Magnussen H, Arzt M, Andrea S, Plate T, Ribera A, Seoane B, et al. Aclidinium bromide improves symptoms and sleep quality in COPD: a pilot study. European Respiratory Journal 2017;49(6):1700485. [DOI] [PubMed] [Google Scholar]
- Magnussen H, Arzt M, Andreas S, Plate T, Ribera A, Seoane B, et al. The effect of aclidinium bromide 400µg on lung function, sleep quality and physical activity in patients with chronic obstructive pulmonary disease: results of a phase IV pilot study [abstract]. American Journal of Respiratory and Critical Care Medicine 2016;193:A6820. [Google Scholar]
- Magnussen H, Arzt M, Andreas S, Plate T, Ribera A, Seoane B, et al. The effect of aclidinium bromide 400µg on sleep quality in COPD: a pilot study [abstract]. European Respiratory Journal 2016;48:PA4051. [DOI] [PubMed] [Google Scholar]
Mantoani 2018 {published data only}
- Mantoani L, McKinstry B, McNarry S, Mullen S, Begg S, Saini P, et al. Physical activity enhancing programme (PAEP) in COPD – a randomised controlled trial [abstract]. European Respiratory Journal 2018;52(Suppl 62):OA1986. [Google Scholar]
Mendoza 2015 {published data only}
- Mendoza L, Aguilera M, Balmaceda N, Espinoza J, Horta P, Castro A, et al. Effect of a program of physical activity enhancement using pedometers in patients with chronic obstructive pulmonary disease [abstract]. American Journal of Respiratory and Critical Care Medicine 2013;187:A1360. [Google Scholar]
- Mendoza L, Aguilera M, Espinoza J, Balmaceda N, Horta P, Castro A, et al. Effects of a program of physical activity encouragement using pedometers in COPD patients [abstract]. European Respiratory Journal 2013;45(2):A570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendoza L, Horta P, Espinoza J, Aguilera M, Balmaceda N, Castro A, et al. Pedometers to enhance physical activity in COPD: a randomised controlled trial. European Respiratory Journal 2015;45(2):347‐54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mitchell 2013 {published and unpublished data}
- Mitchell KE, Johnson‐Warrington V, Apps LD, Bankart J, Sewell L, Williams JE, et al. A self‐management programme for COPD: a randomised controlled trial. European Respiratory Journal 2014;44(6):1538‐47. [DOI] [PubMed] [Google Scholar]
- Mitchell KE, Warrington V, Sewell L, Bankart J, Williams JE, Steiner MC, et al. A randomised controlled trial of a self‐management programme of activity coping and education ‐ SPACE for COPD: impact on physical activity at 6 weeks [abstract]. American Journal of Respiratory and Critical Care Medicine 2013;187:A5952. [Google Scholar]
- Mitchell‐Wagg K, Warrington V, Apps L, Sewell L, Bankart J, Steiner MC, et al. A self‐management programme of activity coping and education (SPACE) for COPD: results from a randomised controlled trial [abstract]. Thorax 2012;67(Suppl 2):A25. [Google Scholar]
- Wagg K, Warrington V, Apps L, Sewell L, Bankart J, Steiner M, et al. A self‐management programme of activity coping and education (SPACE) for COPD: 6 week results from a randomised controlled trial [abstract]. European Respiratory Journal 2012;40(Suppl 56):548s. [Google Scholar]
- Wagg K, Wilcock E, Williams J, Sewell L, Steiner MC, Morgan M, et al. Pulmonary rehabilitation using the space (a self management programme of activity, coping and education) manual at home: a randomised controlled trial [abstract]. Thorax 2009;64:A97. [Google Scholar]
Moy 2015a {published data only}
- Martinez CH, Moy ML, Nguyen HQ, Cohen M, Kadri R, Roman P, et al. Taking healthy steps: rationale, design and baseline characteristics of a randomized trial of a pedometer‐based internet‐mediated walking program in veterans with chronic obstructive pulmonary disease. BMC Pulmonary Medicine 2014;14:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moy ML, Collins RJ, Martinez CH, Kadri R, Roman P, Holleman RG, et al. An internet‐mediated pedometer‐based program improves health‐related quality‐of‐life domains and daily step counts in COPD: a randomized controlled trial. Chest 2015;148(1):128‐37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moy ML, Collins RJ, Martinez CH, Kadri R, Roman P, Holleman RG, et al. An internet‐mediated, pedometer‐based walking program improves HRQOL in veterans with COPD [abstract]. American Journal of Respiratory and Critical Care Medicine 2014;189:A3642. [Google Scholar]
- Moy ML, Martinez CH, Kadri R, Roman P, Holleman RG, Kim HM, et al. Long‐term effects of an internet‐mediated pedometer‐based walking program for chronic obstructive pulmonary disease: randomized controlled trial. Journal of Medical Internet Research 2016;18(8):e215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moy ML, Martinez CH, Kadri R, Roman P, Holleman RG, Kim HM, et al. Long‐term effects of an internet‐mediated pedometer‐based walking program in COPD: a randomized controlled trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2015;191:A2457. [Google Scholar]
Nakamura 2016 {published data only}
- Nakamura H, Mori Y, Nanki N, Kamei T. Clinical benefits of aclidinium bromide twice daily compared with tiotropium once daily in patients with moderate to severe chronic obstructive pulmonary disease [abstract]. American Journal of Respiratory and Critical Care Medicine 2017;195:A5471. [Google Scholar]
NCT00144326 {published data only}
- García Río F. A randomised, double‐blind, placebo‐controlled, 12 weeks trial to evaluate the effect of tiotropium inhalation capsules on the magnitude of exercise, measured using an accelerometer, in patients with chronic obstructive pulmonary disease. Boehringer Ingelheim Trial Results 2007; Vol. Trial number 205.269 (first received 5 September 2005).
NCT01351792 {published data only}
- NCT01351792. Multicentre, randomized research study to test the safety and efficacy of Foster® compared to Symbicort® on small airway function in patients with COPD. Chiesi Clinical Study Report (first received 11 May 2011). [Study number CCD‐1007‐PR‐0045]
Ng 2015 {published and unpublished data}
- Ng LW, Jenkins S, Cecins N, Eastwood P, Hill K. A wheeled walker improves physical activity in chronic obstructive pulmonary disease [abstract]. Physiotherapy 2015;101:eS1084. [Google Scholar]
- Ng LW, Jenkins S, Cecins N, Eastwood P, Hill K. The effect of using a wheeled walker on physical activity in people with COPD: preliminary data [abstract]. Respirology 2012;17(Suppl 1):60. [Google Scholar]
Nguyen 2009 {published data only}
- Estrada EL, Silva K, Medina E, Desai S, Fan VS, Nguyen HQ. Depression and anxiety are associated with COPD patients' lower confidence for increasing physical activity but not with their motivation [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A7066. [Google Scholar]
- Lee JS, Liu AI, Pounds D, Mahmud F, Flores C, Desai SA, et al. Characteristics of COPD patients who agree to participate in a pragmatic trial of physical activity coaching compared to non‐participants [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A2642. [Google Scholar]
- Mahmud F, Valmonte F, Medina E, Pounds D, Nguyen HQ. Real‐world implementation of a physical activity coaching program [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A2728. [Google Scholar]
- Nguyen HQ, Gill DP, Wolpin S, Steele BG, Benditt JO. Pilot study of a cell phone‐based exercise persistence intervention post‐rehabilitation for COPD. International Journal of Chronic Obstructive Pulmonary Disease 2009;4:301‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nolan 2017 {published and unpublished data}
- Nolan CM, Maddocks M, Canavan JL, Jones SE, Delogu V, Kaliaraju D, et al. Pedometer step count targets during pulmonary rehabilitation in chronic obstructive pulmonary disease: a randomized controlled trial. American Journal of Respiratory and Critical Care Medicine 2017;195(10):1344‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolan CM, Maddocks M, Canavan JL, Jones SE, Delogu V, Kaliaraju D, et al. Pedometer step count targets during pulmonary rehabilitation in chronic obstructive pulmonary disease: a randomized controlled trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2016;193:A7862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolan CM, Maddocks M, Canavan JL, Jones SE, Kon SS, Kaliaraju D, et al. Do pedometers maintain the benefits of pulmonary rehabilitation in COPD patients? [abstract]. European Respiratory Journal 2016;48:PA2058. [Google Scholar]
O'Neill 2018 {published data only}
- O'Neill B, O'Shea OM, McDonough SM, McGarvey L, Bradbury I, Arden MA, et al. Physical activity intervention versus pulmonary rehabilitation in COPD: the LIVELY COPD project [abstract]. Thorax 2016;71(Suppl 3):A20. [DOI] [PubMed] [Google Scholar]
- O’Neill B, O’Shea OM, McDonough SM, McGarvey L, Bradbury I, Arden MA, et al. Clinician‐facilitated physical activity intervention versus pulmonary rehabilitation for improving physical activity in COPD: a feasibility study. COPD: Journal of Chronic Obstructive Pulmonary Disease 2018;15(3):254‐64. [DOI] [PubMed] [Google Scholar]
Ogasawara 2018 {published data only}
- Ogasawara T, Marui S, Miura E, Sugiura M, Matsuyama W, Aoshima Y, et al. Effect of eicosapentaenoic acid on prevention of lean body mass depletion in patients with exacerbation of chronic obstructive pulmonary disease: a prospective randomized controlled trial. Clinical Nutrition ESPEN 2018;28:67‐73. [DOI] [PubMed] [Google Scholar]
Orme 2018 {published data only}
- Orme MW, Weedon AE, Esliger DW, Saukko PM, Morgan MD, Steiner MC, et al. Study protocol for Chronic Obstructive Pulmonary Disease‐Sitting and ExacerbAtions Trial (COPD‐SEAT): a randomised controlled feasibility trial of a home‐based self‐monitoring sedentary behaviour intervention [protocol]. BMJ Open 2016;6:e013014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orme MW, Weedon AE, Saukko PM, Esliger DW, Morgan MD, Steiner MC, et al. Findings of the Chronic Obstructive Pulmonary Disease ‐ Sitting and Exacerbations Trial (COPD‐SEAT) in reducing time using wearable and mobile technologies with educational support: randomized controlled feasibility trial. JMIR mHealth and uHealth 2018;6(4):e84. [DOI] [PMC free article] [PubMed] [Google Scholar]
Polkey 2018 {published data only}
- Polkey MI, Qiu ZH, Zhou L, Zhu MD, Wu YX, Chen YY, et al. Tai Chi and pulmonary rehabilitation compared for treatment‐naïve patients with COPD; a randomized controlled trial. Chest 2018;153(3):1116‐24. [DOI] [PubMed] [Google Scholar]
Priori 2017 {published and unpublished data}
- Priori R, Genugten L, Barretto C, Schonenberg H, Stut W, Miller B, et al. Automated coaching for physical activity in COPD patients: results from a pilot study [abstract]. European Respiratory Journal 2017;50:OA4868. [Google Scholar]
- Saini PK, Dekker M, Van Genugten, Prior R, Klee M. Online coaching for physical activity in COPD patients: user engagement and determinants [abstract]. European Respiratory Journal 2018;52:PA3644. [Google Scholar]
- Genugten L, Priori R, Barretto C, Schonenberg H, Dekker M, Klee M, et al. An online intervention to maintain physical activity levels in COPD patients after pulmonary rehabilitation [abstract]. Bulletin of the European Health Psychology Society 2016;18:635. [Google Scholar]
Probst 2011 {published data only}
- Probst VS, Kovelis D, Hernandes NA, Camillo CA, Cavalheri V, Pitta F. Effects of 2 exercise training programs on physical activity in daily life in patients with COPD. Respiratory Care 2011;56(11):1799‐807. [DOI] [PubMed] [Google Scholar]
Rinaldo 2017 {published data only}
- Rinaldo N, Bacchi E, Coratella G, Vitali F, Milanese C, Rossi A, et al. Effects of combined aerobic‐strength training vs fitness education program in COPD patients. International Journal of Sports Medicine 2017;38(13):1001‐8. [DOI] [PubMed] [Google Scholar]
Saini 2017 {published data only}
- Saini PK, Dekker M, Genugten L, Priori R, Klee M. Online coaching for physical activity in COPD patients: user engagement and determinants [abstract]. European Respiratory Journal 2018;52(Suppl 62):PA3644. [Google Scholar]
- Saini PK, Priori R, Barretto C, Delbressine J, Genugten L, Dekker M, et al. Activity maintenance after pulmonary rehabilitation ‐ first results of an online coaching program [abstract]. American Journal of Respiratory and Critical Care Medicine 2017;195:A4942. [Google Scholar]
- Genugten L, Prior R, Barretto C, Schonenberg H, Dekker M, Klee M, et al. An online intervention to maintain physical activity levels after pulmonary rehabilitation [abstract]. European Health Psychologist 2016; Vol. 18.
Sandland 2008 {published data only}
- Sandland CJ, Morgan MD, Singh SJ. Patterns of domestic activity and ambulatory oxygen usage in COPD. Chest 2008;134(4):753‐60. [DOI] [PubMed] [Google Scholar]
Schuz 2015 {published and unpublished data}
- Schuz N, Walters JA, Cameron‐Tucker H, Scott J, Wood‐Baker R, Walters EH. Patient anxiety and depression moderate the effects of increased self‐management knowledge on physical activity: a secondary analysis of a randomised controlled trail on health‐mentoring in COPD. Journal of Chronic Obstructive Pulmonary Disease 2015;12(5):502‐9. [DOI] [PubMed] [Google Scholar]
- Walters JA, Cameron‐Tucker H, Wills K, Schuz N, Scott J, Robinson A, et al. Effects of telephone health mentoring in community‐recruited chronic obstructive pulmonary disease on self‐management capacity, quality of life and psychological morbidity: a randomised controlled trial. BMJ Open 2013;3(9):e003097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walters JA, Wills K, Robinson A, Nelson M, Scott J, Turner P, et al. Effect of health‐mentoring to increase daily physical activity in chronic obstructive pulmonary disease (COPD) [abstract]. Respirology 2012;17:TP079. [Google Scholar]
Sena 2013 {published and unpublished data}
- Sena R, Baril J, Kapchinsky S, MacMillan NJ, Rocha DV, Ruddy R, et al. The effects of eccentric and concentric exercise training on muscle strength in COPD: preliminary results [abstract]. European Respiratory Journal 2012;40(Suppl 56):P482. [Google Scholar]
- Sena R, MacMillan NJ, Baril J, Rocha V, Richard R, Perrault H, et al. Short term effects of eccentric and concentric exercise training on strength muscle, exercise capacity and physical activity in patients with chronic obstructive pulmonary disease [abstract]. Canadian Respiratory Journal 2013;20(2):e36. [Google Scholar]
Singh 1998 {published data only (unpublished sought but not used)}
- Singh SJ, Curcio A, Williams J, Morgan MD, Jones P. Does wearing an activity monitor influence daily activity recorded in patients with COPD? [abstract]. Thorax 1998;53(Suppl 4):A24. [Google Scholar]
Steele 2019 {published data only}
- Kang Y, Steele BG, Burr RL, Dougherty CM. Mortality in advanced chronic obstructive pulmonary disease and heart failure following cardiopulmonary rehabilitation. Biological Research for Nursing 2018;20(4):429‐39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steele BG, Dougherty CM, Burr RL, Gylys‐Colwell I, Hunziker J. A feasibility trial of two rehabilitation models in severe cardiopulmonary illness. Rehabilitation Nursing 2019;44(3):130‐40. [DOI] [PubMed] [Google Scholar]
- Steele BG, Dougherty CM, Burr RL, Gylys‐Colwell I, Hunziker J. An intervention to enhance function in severe cardiopulmonary illness [abstract]. American Journal of Respiratory and Critical Care Medicine 2012;185:A4879. [Google Scholar]
Tabak 2014a {published data only}
- Tabak M, Vollenbroek‐Hutten MM, Valk PD, Palen H, Hermens HJ. A telerehabilitation intervention for patients with chronic obstructive pulmonary disease: a randomized controlled pilot trial. Clinical Rehabilitation 2014;28(6):582‐91. [DOI] [PubMed] [Google Scholar]
Tabak 2014b {published data only}
- Tabak M, Brusse‐Keizer M, Valk P, Hermens H, Vollenbroek‐Hutten M. A telehealth program for self‐management of COPD exacerbations and promotion of an active lifestyle: a pilot randomized controlled trial. International Journal of Chronic Obstructive Pulmonary Disease 2014;9:935‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tahirah 2015 {published and unpublished data}
- Tahirah F, Jenkins S, Othman SK, Ismail R, Ismail T, Hill K. A randomised controlled trial of individualised, progressed early exercise in patients hospitalised with an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) [abstract]. European Respiratory Journal 2015;46:PA743. [Google Scholar]
Troosters 2014 {published data only (unpublished sought but not used)}
- Sciurba FC, Siafakas NM, Troosters T, Klioze SS, Sutradhar SC, Weisman IM, et al. The efficacy and safety of tiotropium handihaler 18 micrograms once daily plus prn salbutamol versus placebo plus prn salbutamol in COPD subjects naive to maintenance therapy [abstract]. American Journal of Respiratory and Critical Care Medicine 2011;183:A1589. [Google Scholar]
- Troosters T, Sciurba FC, Decramer M, Siafakas NM, Klioze SS, Sutradhar SC, et al. Tiotropium in patients with moderate COPD naive to maintenance therapy: a randomised placebo‐controlled trial. Primary Care Respiratory Medicine 2014;24:14003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troosters T, Weisman I, Dobbels F, Giardino N, Valluri SR. Assessing the impact of tiotropium on lung function and physical activity in GOLD stage II COPD patients who are naïve to maintenance respiratory therapy: a study protocol. Open Respiratory Medicine Journal 2011;5:1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Troosters 2018 {published data only}
- Bourbeau J, Lavoie KL, Sedano M, Sousa D, Erzen D, Hamilton A, et al. Behaviour‐change intervention in a multicentre, randomised, placebo‐controlled COPD study: methodological considerations and implementation [protocol]. BMJ Open 2016;6:e010109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bourbeau J, Sedeno M, Li PZ, Troosters T, Hamilton A, Sousa D, et al. Impact of meeting behavioral targets in a self‐management behaviour‐modification program designed to improve physical activity in COPD patients [abstract]. European Respiratory Journal 2017;50:PA4899. [Google Scholar]
- Frith P, Troosters T, Bourbeau J, Maltais F, Leidy N, Erzen D, et al. Effect of tiotropium and olodaterol, alone and with exercise training, on exercise endurance in COPD [abstract]. Respirology 2017;22(Suppl 2):TO048. [Google Scholar]
- Frith P, Troosters T, Lavoie KL, Leidy N, Maltais F, Sedeno M, et al. Bronchodilator therapy and exercise added to self‐management behaviour‐modifications: effects on physical activity in COPD [abstract]. Respirology 2017;22(Suppl 2):TO129. [Google Scholar]
- Lavoie KL, Sedeno M, Li PZ, Troosters T, Hamilton A, Sousa D, et al. Effects of bronchodilator therapy and exercise with self‐management behaviour‐modification on psychological and cognitive outcomes in COPD [abstract]. European Respiratory Journal 2017;50:OA4669. [Google Scholar]
- Troosters T, Bourbeau J, Maltais F, Leidy N, Erzen D, Sousa D, et al. Effect of 8 and 12 weeks' once‐daily tiotropium and olodaterol alone and combined with exercise training, on exercise endurance during walking in patients with COPD [abstract]. European Respiratory Journal 2016;48:PA976. [Google Scholar]
- Troosters T, Bourbeau J, Maltais F, Leidy N, Erzen D, Sousa D, et al. Effect of 8 and 12 weeks' once‐daily tiotropium and olodaterol, alone and combined with exercise training, on exercise endurance during walking in patients with COPD [abstract]. Thorax 2016;71(Suppl 3):A21‐22. [Google Scholar]
- Troosters T, Bourbeau J, Maltais F, Leidy N, Erzen D, Sousa D, et al. Enhancing exercise tolerance and physical activity in COPD with combined pharmacological and non‐pharmacological interventions: PHYSACTO randomised, placebo‐controlled study design [protocol]. BMJ Open 2016;6:e010106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troosters T, Lavoie KL, Leidy N, Maltais F, Sedeno M, Janssens W, et al. Effects of bronchodilator therapy and exercise training, added to a self‐management behaviour‐modification programme, on physical activity in COPD [abstract]. European Respiratory Journal 2016;48:PA713. [Google Scholar]
- Troosters T, Lavoie KL, Leidy N, Maltais F, Sedeno M, Janssens W, et al. Effects of bronchodilator therapy and exercise training, added to a self‐management behaviour‐modification programme, on physical activity in COPD [abstract]. Pneumonologie 2017;71(S01):37. [Google Scholar]
- Troosters T, Maltais F, Leidy N, Lavoie KL, Sedeno M, Janssens A, et al. Effect of bronchodilation and exercise training with behavior modification on exercise tolerance and downstream effects on symptoms and physical activity in COPD. American Journal of Respiratory and Critical Care Medicine 2018;198(8):1021‐32. [DOI] [PubMed] [Google Scholar]
Tsai 2016 {published and unpublished data}
- Tsai LL, McNamara RJ, Moddel C, Alison JA, McKenzie D, McKeogh ZJ. Home‐based telerehabilitation via real‐time videoconferencing improves endurance exercise capacity in patients with COPD: the randomized controlled TeleR study. Respirology 2017;22(4):699‐707. [DOI] [PubMed] [Google Scholar]
- Tsai LL, McNamara RJ, Moddel C, Alison JA, McKenzie DK, McKeough ZJ. Home‐based telerehabilitation via real‐time videoconferencing improves endurance exercise capacity in patients with COPD: the randomized controlled TeleR sStudy [abstract]. Respirology 2016;21(S2):TP086. [DOI] [PubMed] [Google Scholar]
- Tsai LL, McNamara RJ, Moddel C, McKenzie D, Alison JA, McKeough ZJ. Telerehabilitation in people with chronic obstructive pulmonary disease (COPD): a randomised controlled trial [abstract]. European Respiratory Journal 2016;48(Suppl 60):PA2065. [Google Scholar]
Van de Bool 2017 {published data only}
- Beers M, Rutten‐van Molken MP, Bool C, Boland M, Kremers SP, Franssen FM, et al. Clinical outcome and cost‐effectiveness of 1‐year nutritional intervention program in COPD [abstract]. European Respiratory Journal 2018;52(Suppl 62):PA723. [Google Scholar]
- Beers M, Rutten‐van Molken MP, Bool C, Boland M, Kremers SP, Franssen FM, et al. Clinical outcome and cost‐effectiveness of a 1‐year nutritional intervention programme in COPD patients with low muscle mass: the randomized controlled NUTRAIN trial. Clinical Nutrition 2019;39(2):405‐13. [DOI] [PubMed] [Google Scholar]
- Bool C, Rutten EP, Helvoort A, Franssen FM, Wouters EF, Schols AM. A randomized clinical trial investigating the efficacy of targeted nutrition as adjunct to exercise training in COPD. Journal of Cachexia, Sarcopenia and Muscle 2017;8(5):748‐58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bool C, Helvoort A, Franssen FM, Wouters EF, Schols AM. Physiological effects of nutritional supplementation as adjunct to exercise training in COPD patients with low muscle mass. The double blind, placebo controlled multi‐centre NUTRAIN‐trial [abstract]. European Respiratory Journal 2016;48(Suppl 60):OA266. [Google Scholar]
Varas 2018 {published and unpublished data}
- Varas AB, Cordoba S, Rodriguez‐Andonaegui I, Rueda MR, Garcia‐Juez S, Vilaro J. Effectiveness of a community‐based exercise training programme to increase physical activity level in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Physiotherapy Research International 2018;23(4):e1740. [DOI] [PubMed] [Google Scholar]
Vasilopoulou 2017 {published and unpublished data}
- Vasilopoulou M, Papaioannou AI, Chynkiamis N, Vasilogiannakopoulou T, Spetsioti S, Louvaris Z, et al. Effectiveness of home telerehabilitation on functional capacity and daily physical activity in COPD patients [abstract]. European Respiratory Journal 2015;46:OA273. [Google Scholar]
- Vasilopoulou M, Papaioannou AI, Kaltsakas G, Louvaris Z, Chynkiamis N, Spetsioti S, et al. Home‐based maintenance tele‐rehabilitation reduces the risk of acute exacerbations of COPD, hospitalisations and emergency department visits. European Respiratory Journal 2017;49(5):pii:1602129. [DOI] [PubMed] [Google Scholar]
Vorrink 2016 {published data only}
- Vorrink S, Huisman C, Kort H, Troosters T, Lammers JW. Perceptions of patients with chronic obstructive pulmonary disease and their physiotherapists regarding the use of an ehealth intervention. JMIR Human Factors 2017;4(3):e20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vorrink SN, Kort HS, Troosters T, Zanen P, Lammers JL. Efficacy of an mHealth intervention to stimulate physical activity in COPD patients after pulmonary rehabilitation. European Respiratory Journal 2016;48(4):1019‐29. [DOI] [PubMed] [Google Scholar]
Wan 2017 {published and unpublished data}
- Kantorowski A, Wan ES, Homsy D, Kadri R, Richardson CR, Moy ML. Determinants and outcomes of change in physical activity in COPD. ERJ Open Research 2018;4(3):pii: 00054‐2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson SA, Shimada SL, Quigley KS, Moy ML. A web‐based physical activity intervention benefits persons with low self‐efficacy in COPD: results from a randomized controlled trial. Journal of Behavioral Medicine 2019;42(6):1082‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wan ES, Kantorowski A, Homsy D, Kadri R, Richardson CR, Mori D, et al. Self‐reported task‐oriented physical activity: a comparison with objective daily step count in COPD. Respiratory Medicine 2018;140:63‐70. [DOI] [PubMed] [Google Scholar]
- Wan ES, Kantorowski A, Homsy D, Teylan M, Kadri R, Richardson CR, et al. Promoting physical activity in COPD: insights from a randomized trial of a web‐based intervention and pedometer use. Respiratory Medicine 2017;130:102‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wan ES, Kantorowski A, Teylan M, Kadri R, Richardson CR, Garshick E, et al. Patterns of change in daily step count among COPD patients enrolled in a 3‐month physical activity intervention [abstract]. American Journal of Respiratory and Critical Care Medicine 2017;195:A4939. [Google Scholar]
Watz 2016 {published and unpublished data}
- Watz H, Mailaender C, Kirsten AM. Effects of indacaterol/glycopyrronium on lung function and physical activity in patients with moderate to severe COPD [abstract]. Thorax 2015;70:A146‐7. [Google Scholar]
- Watz H, Mailander C, Baier M, Kirsten AM. Effects of indacaterol/glycopyrronium (QVA149) on lung hyperinflation and physical activity in patients with moderate to severe COPD: a randomised, placebo‐controlled, crossover study (The MOVE Study). BMC Pulmonary Medicine 2016;16(1):95. [DOI] [PMC free article] [PubMed] [Google Scholar]
Watz 2017 {published data only}
- Watz H, Troosters T, Beeh KM, Garcia Aymerich J, Paggiaro P, Molins E, et al. ACTIVATE: effect of aclidinium/formoterol on physical activity in patients with COPD [abstract]. European Respiratory Journal 2017;60(Suppl 61):PA687. [Google Scholar]
- Watz H, Troosters T, Beeh KM, Garcia Aymerich J, Paggiaro P, Molins E, et al. Effect of aclidinium/formoterol on lung hyperinflation, exercise capacity and physical activity in patients with COPD: results from ACTIVATE, a phase IV study [abstract]. American Journal of Respiratory and Critical Care Medicine 2017;195:A3593. [Google Scholar]
- Watz H, Troosters T, Beeh KM, Garcia‐Aymerich J, Paggiaro P, Molins E, et al. ACTIVATE: the effect of aclidinium/formoterol on hyperinflation, exercise capacity and physical activity in patients with COPD. International Journal of Chronic Obstructive Pulmonary Disease 2017;12:2545‐58. [DOI] [PMC free article] [PubMed] [Google Scholar]
Widyastuti 2018 {published data only}
- Widyastuti K, Makhabah DN, Rima A, Sutanto YS, Suradi S, Ambrosino N. Home based pulmonary rehabilitation with pedometers in Indonesian COPD patients [abstract]. European Respiratory Journal 2017;50:PA777. [Google Scholar]
- Widyastuti K, Makhabah DN, Rima Setijadi A, Sutanto YS, Suradi S, Ambrosino N. Benefits and costs of home pedometer assisted physical activity in patients with COPD: a preliminary randomized controlled trial. Pulmonology 2018;24(4):211‐8. [DOI] [PubMed] [Google Scholar]
Wootton 2017 {published and unpublished data}
- Hill K, Wootton SL, Ng LW, Jenkins S, Cecins N, Straker L, et al. High‐intensity ground‐based walking does not change time spent in physical activity or sedentary behaviour in people with chronic obstructive pulmonary disease [abstract]. Respirology 2016;21(Suppl 2):TP083. [Google Scholar]
- Watts SL, Ng LW, McKeogh ZJ, Jenkins S, Hill K, Eastwood PR, et al. Effects of ground walking training in COPD: a randomized controlled trial [abstract]. Respirology 2013;18(Suppl 2):O064. [Google Scholar]
- Wootton SL, Hill K, Alison JA, Ng LW, Jenkins S, Eastwood PR, et al. Effects of ground‐based walking training on daily physical activity in people with COPD: a randomised controlled trial. Respiratory Medicine 2017;132:139‐45. [DOI] [PubMed] [Google Scholar]
- Wootton SL, Hill K, Alison JA, Ng LW, Jenkins S, Eastwood PR, et al. Effects of ongoing feedback during a 12‐month maintenance walking program on daily physical activity in people with COPD. Lung 2019;197(3):315‐9. [DOI] [PubMed] [Google Scholar]
- Wootton SL, Ng LW, McKeough ZJ, Jenkins S, Hill K, Eastwood PR, et al. Ground walking training in chronic obstructive pulmonary disease: a randomised controlled trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2014;189:A4162. [Google Scholar]
- Wootton SL, Ng LW, McKeough ZJ, Jenkins S, Hill K, Eastwood PR, et al. Ground‐based walking training improves quality of life and exercise capacity in COPD. European Respiratory Journal 2014;44(4):885‐94. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
ACTRN12611001034921 {published data only}
- ACTRN12611001034921. A randomised controlled clinical trial in adults with Chronic Obstructive Pulmonary Disease on the effect of telephone health‐mentoring, home‐based walking and rehabilitation compared with rehabilitation only on health‐related quality of life. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=343303 (first received 29 November 2011).
Aksu 2006 {published data only}
- Aksu B, Inanir M, Basyigit I, Dursun N, Yildiz F. Comparison of two different exercise programs in chronic obstructive pulmonary disease [abstract]. European Respiratory Journal 2006;28(Suppl 50):555s. [Google Scholar]
Arnedillo 1998 {published data only}
- Arnedillo A, Puente L, Mangas A, Leaan A. Comparison of two exercise training programmes in patients with chronic obstructive pulmonary disease [abstract]. Neumosur 1998;10(4):223‐9. [Google Scholar]
Atkins 1984 {published data only}
- Atkins CJ, Kaplan RM, Timms RM, Reinsch S, Lofback K. Behavioral exercise programs in the management of chronic obstructive pulmonary disease. Journal of Consulting and Clinical Psychology 1984;52(4):591‐603. [DOI] [PubMed] [Google Scholar]
Barnes‐Harris 2019 {published data only}
- Barnes‐Harris M, Allgar V, Booth S, Currow D, Hart S, Phillips J, et al. Battery operated fan and chronic breathlessness: does it help?. BMJ Supportive and Palliative Care 2019;May 8:pii: bmjspcare‐2018‐001749. [DOI] [PubMed] [Google Scholar]
Bartlett 2017 {published data only}
- Bartlett YK, Webb TL, Hawley MS. Using persuasive technology to increase physical activity in people with chronic obstructive pulmonary disease by encouraging regular walking: a mixed‐methods study exploring opinions and preferences. Journal of Medical Internet Research 2017;19(4):e124. [DOI] [PMC free article] [PubMed] [Google Scholar]
Baumann 2006 {published data only}
- Baumann HJ, Rummel K, Schmoller T, Meyer A. Efficacy of a long term ambulatory interdisciplinary rehabilitation (AIR) program in moderate to severe COPD [abstract]. European Respiratory Journal 2006;28(Suppl 50):555s. [Google Scholar]
Behnke 2000 {published data only}
- Behnke M. The effects of a home‐based exercise training programme in patients with chronic obstructive lung disease. Pneumologie 2000;53:2‐3. [PubMed] [Google Scholar]
Behnke 2005 {published data only}
- Behnke M, Wewel AR, Kirsten D, Jorres RA, Magnussen H. Exercise training raises daily activity stronger than predicted from exercise capacity in patients with COPD. Respiratory Medicine 2005;99(6):711‐7. [DOI] [PubMed] [Google Scholar]
Bernardi 2017 {published data only}
- Bernardi E, Merlo C, Bellotti F, Grazzi G, Cogo A. An exercise training program improves endothelial function in COPD patients [abstract]. European Respiratory Journal 2017;50(Suppl 61):OA1959. [Google Scholar]
Bertici 2013 {published data only}
- Bertici N, Fira‐Mladinescu O, Oancea C, Tudorache V. The usefulness of pedometry in patients with chronic obstructive pulmonary disease. Multidisciplinary Respiratory Medicine 2013;8(1):7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Biscione 2009 {published data only}
- Biscione G, Crigna G, Auciello L, Pasqua F, Cazzola M. Addition of tiotropium (T) to a regular treatment with long‐acting beta‐agonist + inhaled corticosteroid (LABA + ICS) in patients with severe to very‐severe COPD under in‐patient pulmonary rehabilitation program (PRP) [abstract]. European Respiratory Society 19th Annual Congress; 2009 Sep 12‐15; Vienna. 2009:P526.
Bohning 1990 {published data only}
- Bohning W, Wettengel R. Physical exercise training in COPD during a 4 ‐week rehabilitation programme [abstract]. European Respiratory Journal 1990;3(Suppl 10):212S. [Google Scholar]
Boland 2015 {published data only}
- Boland MR, Tsiachristas A, Rutten van Molken M. COPD performance indicators in an integrated care program and its impact on health outcomes: The Recode Cluster Randomized Trial [abstract]. Value in Health 2015;18(7):A505. [Google Scholar]
- Kruis AL, Boland MR, Assendelft WJ, Gussekloo J, Tsiachristas A, Stijnen T, et al. Effectiveness of integrated disease management for primary care chronic obstructive pulmonary disease patients: Results of cluster randomised trial. BMJ 2014;349(7976):g5392. [DOI] [PMC free article] [PubMed] [Google Scholar]
Börekçi 2008 {published data only}
- Börekçi S, Elci A, Ovayolu N, Elbeck O. Applicability and efficacy of the pulmonary rehabilitation program for COPD patients in a secondary‐care community hospital [Abstract]. American Thoracic Society International Conference; 2008 May 16‐21; Toronto. 2008; Vol. 5, issue 5:P416.
Borges 2012 {published data only}
- Borges RC, Carvalho CR. Physical activity in daily life in Brazilian COPD patients during and after exacerbation. Chronic Obstructive Pulmonary Disease 2012;9(6):596‐602. [DOI] [PubMed] [Google Scholar]
Bourbeau 2000 {published data only}
- Bourbeau J, Julien M, Rouleau M, Maltais F, Beaupre A, Begin R, et al. Impact of an integrated rehabilitative self‐management program on health status of COPD patients: a multicentre randomised clinical trial [abstract]. European Respiratory Journal 2000;16(Suppl 31):159s. [Google Scholar]
Budnevskiy 2015 {published data only}
- Budnevskiy AV, Chernov AV, Isaeva YV, Yu Malysh E. Clinical efficacy of pulmonary rehabilitation program in patients with chronic obstructive pulmonary disease and metabolic syndrome. Pulmonologiya 2015;25(4):447‐55. [Google Scholar]
Bunker 2012 {published data only}
- Bunker JM, Reddel HK, Dennis SM, Middleton S, Schayck C, Crockett AJ, et al. A pragmatic cluster randomized controlled trial of early intervention for chronic obstructive pulmonary disease by practice nurse‐general practitioner teams: study protocol. Implementation Science 2012;7:83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bustamante 2013 {published data only}
- Bustamante V, Lopez de Santamaria E, Marina N, Gorostiza A, Fernandez Z, Galdiz J. Neuromuscular magnetic stimulation of the quadriceps muscle after COPD exacerbations. European Respiratory Journal 2013;42:P3572. [Google Scholar]
Camillo 2011 {published data only}
- Camillo CA, Laburu V de M, Gonçalves NS, Cavalheri V, Tomasi FP, Hernandes NA, et al. Improvement of heart rate variability after exercise training and its predictors in COPD. Respiratory Medicine 2011;105(7):1054‐62. [DOI] [PubMed] [Google Scholar]
Cebollero 2018 {published data only}
- Cebollero P, Anton M, Hernandez M, Hueto J. Walking program for COPD patients: clinical impact after two years of follow‐up [Programa de paseos para pacientes con EPOC: impacto clínico tras 2 anos de seguimiento]. Archivos de Bronconeumología 2018;54(8):431‐3. [DOI] [PubMed] [Google Scholar]
- Hernandez Bonaga M, Zambom F, Cascante JA, Hueto J, Anton M, Cebollero Rivas P. Walking guide for COPD patients: a promoter of physical activity?. European Respiratory Journal 2014;44:p3681. [Google Scholar]
- Hernandez M, Zambom F, Cascante JA, Hueto J, Anton M, Cebollero P. Walking guide for COPD patients: can be used as a promoter of physical activity?. European Respiratory Journal 2013;42:p3703. [Google Scholar]
- Hernandez M, Zambom‐Ferraresi F, Milagros Anton M, Hueto J, Cascante J, Cebollero P. Short and long term effects of a physical activity programa in COPD patients. European Respiratory Journal 2015;46(Suppl 59):PA 2213. [Google Scholar]
Chen 2018 {published data only}
- Chen K‐Y, Hung M‐H, Chang M‐C, Kuo C, Lin C‐M, Chuang L‐P, et al. Four‐weeks remote pulmonary rehabilitation protocol with mobile apps of real‐time heart rate monitoring for gold category B/C/D‐A study design. Respirology 2018;23(Suppl 2):82. [Google Scholar]
Corrado 1995 {published data only}
- Corrado A, Gorini M, Paola E, Martorana P, Villella G, Augustynen A, et al. Effects of a short outpatient pulmonary rehabilitation program (PRP) in severe COPD patients with chronic respiratory insufficiency (CRI) [abstract]. European Respiratory Journal 1995;8(Suppl 19):126s. [Google Scholar]
Coultas 2011 {published data only}
- Coultas D, Sloan J, Wilson D. Pilot study of effectiveness of home rehabilitation for homebound patients with severe COPD [abstract]. European Respiratory Society 21st Annual Congress; 2011 Sep 24‐28; Amsterdam. 2011:881s.
Coultas 2017 {published data only}
- Ashmore J, Russo R, Peoples J, Sloan J, Jackson BE, Bae S, et al. Chronic obstructive pulmonary disease self‐management activation research trial (COPD‐SMART): design and methods. Contemporary Clinical Trials 2013;35(2):77‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coultas D, Russo R, Peoples J, Ashmore J, Sloan J, Jackson B, et al. A lifestyle physical activity intervention is associated with decline in health care utilization (HCU) among patients with COPD [abstract]. European Respiratory Journal 2014;44(Suppl 58):P611. [Google Scholar]
- Coultas DB, Jackson BE, Russo R, Peoples J, Singh KP, Sloan J, et al. Home‐based physical activity coaching, physical activity, and healthcare utilization in COPD: COPD‐SMART secondary outcomes. Annals of the American Thoracic Society 2018;15(4):470‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russo R, Coultas D, Ashmore J, Peoples J, Sloan J, Jackson BE, et al. Chronic obstructive pulmonary disease self‐management activation research trial (COPD‐SMART): results of recruitment and baseline patient characteristics. Contemporary Clinical Trials 2015;41C:192‐201. [DOI] [PMC free article] [PubMed] [Google Scholar]
De Backer 2014 {published data only}
- Backer W, Vos W, Holsbeke C, Vinchurkar S, Claes R, Hufkens A, et al. The effect of roflumilast in addition to LABA/LAMA/ICS treatment in COPD patients [abstract]. European Respiratory Journal 2014;44(2):527‐9. [DOI] [PubMed] [Google Scholar]
Deering 2011 {published data only}
- Deering BM, Fullen B, Egan C, McCormack N, Kelly E, Pender M, et al. Acupuncture as an adjunct to pulmonary rehabilitation. Journal of Cardiopulmonary Rehabilitation and Prevention 2011;31(6):392‐9. [DOI] [PubMed] [Google Scholar]
De Souza 2017 {published data only}
- Souza Y, Sliva KM, Condesso D, Figueira B, Alves RR, Costa CH, et al. Home‐based pulmonary rehabilitation intervention: does it maintain the benefits achieved during the outpatient program [abstract]. American Journal of Respiratory and Critical Care Medicine 2017;195:A941. [Google Scholar]
Durheim 2015 {published data only}
- Durheim MT, Smith PJ, Babyak MA, Mabe SK, Emery CF, Blumenthal JA, et al. Physical function as measured by 6‐minute walk distance or accelerometry predicts clinical outcomes in COPD patients independent of GOLD 2011 [abstract]. American Journal of Respiratory and Critical Care Medicine 2014;189:A6679. [Google Scholar]
- Durheim MT, Smith PJ, Babyak MA, Mabe SK, Martinu T, Welty‐Wolf KE, et al. Six‐minute‐walk distance and accelerometry predict outcomes in chronic obstructive pulmonary disease independent of Global Initiative for Chronic Obstructive Lung Disease 2011 Group. Annals of the American Thoracic Society 2015;12(3):349‐56. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dyer 2011 {published data only}
- Dyer F, Flude L, Bazari F, Jolley C, Englebretsen C, Lai D, et al. Non‐invasive ventilation (NIV) as an aid to rehabilitation in acute respiratory disease. BMC Pulmonary Medicine 2011;11:58. [DOI] [PMC free article] [PubMed] [Google Scholar]
EUCTR2016‐003675‐21‐ES {published data only}
- EUCTR2016‐003675‐21‐ES. A study to test different doses of Danirixin in patients with COPD. www.clinicaltrialsregister.eu/ctr‐search/trial/2016‐003675‐21/results (first received 18 April 2017).
Faulkner 2010 {published data only}
- Faulkner J, Walshaw E, Campbell J, Jones R, Taylor R, Price D, et al. The feasibility of recruiting patients with early COPD to a pilot trial assessing the effects of a physical activity intervention. Primary Care Respiratory Journal 2010;19(2):124‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fernandez 1998 {published data only}
- Fernandez J, Martin M, Moreno LF. Evaluation of a home‐based rehabilitation program controlled with pulse‐meter in COPD. Neumosur 1998;10(1):54‐5. [Google Scholar]
Foy 2006 {published data only}
- Foy CG, Wickley KL, Adair N, Lang W, Miller ME, Rejeski WJ, et al. The Reconditioning Exercise and Chronic Obstructive Pulmonary Disease Trial II (REACT II): Rationale and study design for a clinical trial of physical activity among individuals with chronic obstructive pulmonary disease. Contemporary Clinical Trials 2006;27(2):135‐46. [DOI] [PubMed] [Google Scholar]
Friis 2017 {published data only}
- Friis AL, Steenholt CB, Lokke A, Hansen M. Dietary beetroot juice ‐ effects on physical performance in COPD patients: a randomized controlled crossover trial. International Journal of Chronic Obstructive Pulmonary Disease 2017;12:1765‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Furness 2014 {published data only}
- Furness T, Joseph C, Naughton G, Welsh L, Lorenzen C. Benefits of whole‐body vibration to people with COPD: a community‐based efficacy trial. BMC Pulmonary Medicine 2014;14(1):38. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garcia Aymerich 2016 {published data only}
- Garcia Aymerich J, Puham M, Jongh C, Demeyer H, Erzen D, Gimeno Santos E, et al. Responsiveness of PROactive instruments to measure physical activity in COPD patients [abstract]. European Respiratory Journal 2016;48:PA1896. [Google Scholar]
Gohl 2004 {published data only}
- Gohl O, Linz H, Otte B, Schonleben T, Weineck J, Worth H. Benefits of a multicomponent outpatient rehabilitation program for patients with chronic obstructive pulmonary disease [abstract]. American Thoracic Society 100th International conference; 2004 May 21‐26; Orlando. 2004:D14.
- Gohl O, Linz H, Otte B, Schonleben T, Weineck J, Worth H. Effects of multicomponent outpatient rehabilitation program for patients with COPD [abstract]. European Respiratory Journal 2004;24(Suppl 48):208s. [Google Scholar]
Gohl 2006 {published data only}
- Gohl O, Schacher C, Grensemann S, Worth H. Effects of inspiratory muscle training with the RESPIFIT S in addition to an outpatient exercise training program for patients with COPD [abstract]. European Respiratory Journal 2006;28(Suppl 50):556s. [Google Scholar]
Gomez 2006 {published data only}
- Gomez A, Roman M, Larraz C, Esteva M, Mir I, Thomas V, et al. Efficacy of respiratory rehabilitation on patients with moderate COPD in primary care and maintenance of benefits at 2 years. Atencion Primaria / Sociedad Espanola de Medicina de Familia y Comunitaria 2006;38(4):230‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gosselink 1990 {published data only}
- Gosselink H, Keimpema A, Wagenaar R, Chadwick Straver R. The relative efficacy of a rehabilitation‐programme in COPD patients [abstract]. European Respiratory Journal 1990;10(Suppl 10):212S. [Google Scholar]
Grabenhorst 2013 {published data only}
- Grabenhorst M, Jehn M, Maldener N, Liebers U, Kohler F, Witt C. Telemedicine in patients with COPD: Feasibility and benefit of regular exercise testing via remote patient monitoring [abstract]. Pneumologie 2013;67:P377. [Google Scholar]
Greulich 2013 {published data only}
- Greulich T, Augsten M, Kehr K, Nell C, Koehler U, Werner J. A randomized clinical trial to assess the influence of a three months training program (individualized vs. non‐individualized) in patients with moderate to very severe COPD [abstract]. American Journal of Respiratory and Critical Care Medicine 2012;185:A4874. [Google Scholar]
- Greulich T, Kehr K, Nell C, Haid D, Koehler U, Koehler K, et al. A randomized clinical trial comparing the influence of two different training modalities (individualized vs. non‐individualized) in patients with moderate to very severe COPD [abstract]. American Journal of Respiratory and Critical Care Medicine 2013;187:A1801. [Google Scholar]
Guell 2008 {published data only}
- Guell MR, Lucas P, Galdiz JB, Montemayor T, Gonzalez‐Moro JM, Gorostiza A, et al. Home versus hospital‐based pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: a Spanish multicenter trial. Archivos de Bronconeumología 2008;44(10):512‐8. [PubMed] [Google Scholar]
- Guell R, Delucas P, Galdiz JB, Montemayor T, Rodriguez JM, Gorostiza A, et al. Effectiveness of a home based pulmonary rehabilitation program compared to a hospital based pulmonary rehabilitation program in COPD patients, a Spanish multicenter randomized trial [abstract]. European Respiratory Journal 2006;28(Supp 50):298s. [Google Scholar]
Gurgun 2011 {published data only}
- Gurgun A, Tuncel S, Korkmaz Ekren P, Deniz PS, Karapolat H, Kayahan B. Efficacy of an eight‐week pulmonary rehabilitation in COPD patients: an experience of a single center in Turkey [abstract]. American Journal of Respiratory and Critical Care Medicine 2011;183:A5049. [Google Scholar]
Hartman 2012 {published data only}
- Hartman JE, Boezen M, Heintzbergen S, Greef MH, Klooster K, Hacken NH, et al. Daily physical activity after bronchoscopic lung volume reduction: a pilot study. European Respiratory Journal 2012;40:1566‐7. [DOI] [PubMed] [Google Scholar]
Hataji 2017 {published data only}
- Hataji O, Nishii Y, Ito K, Sakaguchi T, Saiki H, Suzuki Y, et al. Smart watch‐based coaching with tiotropium and olodaterol ameliorates physical activity in patients with chronic obstructive pulmonary disease. Experimental and Therapeutic Medicine 2017;14(5):4061‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Herrejon 2010 {published data only}
- Herrejon A, Catalan P, Palop J, Inchaurraga I, Blanquer R, Lopez A, et al. Effect of 8‐week 320 mg Megestrol acetate daily administration In severe COPD and weight loss [abstract]. American Journal of Respiratory and Critical Care Medicine 2010;181:A4484. [Google Scholar]
Hillegass 2012 {published data only}
- Hillegass E, Hayes D, Sanders D, Owens T, Langbehn C, Johnson M, et al. Continuous versus pulsed oxygen: is there a difference with activity? A pilot study [abstract]. Chest 2012;142(4):802A. [Google Scholar]
Horton 2018 {published data only}
- Horton EJ, Mitchell KE, Johnson‐Warrington V, Apps LD, Sewell L, Morgan M, et al. Comparison of a structured home‐based rehabilitation programme withe conventional supervised pulmonary rehabilitation: a randomised non‐inferiority trial. Thorax 2018;73:29‐36. [DOI] [PubMed] [Google Scholar]
Ichinose 2017 {published data only}
- Ichinose M, Minakata Y, Motegi T, Ueki J, Gon Y, Seki T. Efficacy of tiotropium/olodaterol on lung volume, exercise capacity, and physical activityet al. International Journal of Chronic Obstructive Pulmonary Disease 2018;13:1407‐19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ichinose M, Minakata Y, Motegi T, Ueki J, Gon Y, Seki T, et al. Efficacy of tiotropium/olodaterol on lung hyperinflation, exercise capacity, and physical activity in Japanese patients with Chronic Obstructive Pulmonary Disease (VESUTO Study): a randomized crossover trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A4243. [Google Scholar]
- Ichinose M, Minakata Y, Motegi T, Ueki J, Seki T, Anzai T, et al. Study design of VESUTO: efficacy of tiotropium/olodaterol on lung hyperinflation, exercise capacity and physical activity in Japanese patients with chronic obstructive pulmonary disease. Advances in Therapy 2017;34(7):1622‐35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ichinose M, Minakata Y, Motegi T, Ueki J, Seki T, Anzai T, et al. Study design of VESUTO; study to evaluate the efficacy of tiotropium + olodaterol vs tiotropium on lung hyperinflation, exercise capacity, and physical activity in Japanese COPD patients [abstract]. Respirology 2016;21(S3):APSR6‐0457. [Google Scholar]
- Minakata Y, Motegi T, Ueki J, Gon Y, Seki T, Anzai T, et al. Efficacy of tiotropium/olodaterol on sedentary/active time in COPD patients: VESUTO study [abstract]. European Respiratory Journal 2018;52(Suppl 62):PA4390. [Google Scholar]
Ides 2012 {published data only}
- Ides KM, Backer L, Daems D, Boelen E, Leemans G, Vissers D, et al. Preliminary results of noninvasive ventilation during a pulmonary rehabilitation program in patients with COPD [abstract]. European Respiratory Journal 2012;50(Suppl 56):639s. [Google Scholar]
Innocenti 2000 {published data only}
- Innocenti F, Fabbri A, Guerrini M, Fonseca D, Lippi P. Results of an outpatient pulmonary rehabilitation program in patients with COPD [abstract]. European Respiratory Journal 2000;16(Suppl 31):46s. [Google Scholar]
Johnson‐Warrington 2016 {published data only}
- Johnson‐Warrington V, Rees K, Gedler C, Morgan MD, Singh SJ. Can a supported self‐management program for COPD upon hospital discharge reduce readmissions? A randomized controlled trial. International Journal of Chronic Obstructive Pulmonary Disease 2016;11:1161‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jonsdottir 2015 {published data only}
- Jonsdottir H, Amundadottir OR, Gudmundsson G, Halldorsdottir BS, Hrafnkelsson B, Ingadottir TS, et al. Effectiveness of a partnership‐based self‐management programme for patients with mild and moderate chronic obstructive pulmonary disease: a pragmatic randomized controlled trial. Journal of Advanced Nursing 2015;71(11):2634‐49. [DOI] [PubMed] [Google Scholar]
Kato 2017 {published data only}
- Kato D, Dobashi K, Fueki M, Tomioka S, Yamada H, Fueki N. Short‐term and long‐term effects of a self‐managed physical activity program using a pedometer for chronic respiratory disease: a randomized controlled trial. Journal of Physical Therapy Science 2017;89:807‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2003 {published data only}
- Kim DS, Na JO, Jegal YJ, Yoon SH, Shim TS, Lim CM, et al. Efficacy of home based pulmonary rehabilitation program for the patients with chronic lung diseases [abstract]. European Respiratory Journal 2003;22(Suppl 45):A1082. [Google Scholar]
Kruis 2014 {published data only}
- Kruis AL, Boland MR, Assendelft WJ, Gussekloo J, Tsiachristas A, Stijnen T, et al. Effectiveness of integrated disease management for primary care chronic obstructive pulmonary disease patients: Results of cluster randomised trial. BMJ Online 2014;349(7976):g5392. [DOI] [PMC free article] [PubMed] [Google Scholar]
Langer 2018 {published data only}
- Langer D, Ciavaglia C, Faisal A, Webb KA, Neder JA, Gosselink R, et al. Inspiratory muscle training reduces diaphragm activation and dyspnea during exercise in COPD. Journal of Applied Physiology 2018;125(2):381‐92. [DOI] [PubMed] [Google Scholar]
Larraz 2010 {published data only}
- Larraz C, Esteva M, Ripoll J, Mir I, Gómez A, Román M. Efficacy of a rehabilitation program on moderate COPD conducted in primary care and the maintenance of benefits during two years [abstract]. Primary Care Respiratory Journal 2010;19(2):A22. [Google Scholar]
Lee 2007 {published data only}
- Lee KH, Shin KC, Chung JH, Yu SK. Effects of self‐efficacy promoting pulmonary rehabilitation program for chronic obstructive pulmonary disease patients [abstract]. American Thoracic Society International Conference; 2007 May 18‐23; San Francisco. 2007:M60.
Liang 2018 {published data only}
- Liang J, Abramson M, Zwar N, Russell G, Holland A, Bonevski B, et al. An interdisciplinary model of care for the early detection and management of chronic obstructive pulmonary disease (COPD) in primary care‐the RADICALS trial [abstract]. Respirology 2016;21(Suppl 2):61. [Google Scholar]
- Liang J, Abramson MJ, Zwar NA, Russell GM, Holland AE, Bonevski M, et al. Diagnosing COPD and supporting smoking cessation in general practice: evidence–practice gaps. Medical Journal of Australia 2018;208(1):29‐34. [DOI] [PubMed] [Google Scholar]
Liu 2019 {published data only}
- Liu X, Li P, Xiao L, Lu Y, Li N, Wang Z, et al. Effects of home‐based prescribed pulmonary exercise by patients with chronic obstructive pulmonary disease: study protocol for a randomized controlled trial. Trials 2019;20(1):41. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lum 2007 {published data only}
- Lum CM, Woo J, Yeung F, Hui DS, Hui E. Semi‐supervised, domiciliary pulmonary rehabilitation programme: a controlled clinical trial. Hong Kong Medical Journal 2007;13(Suppl 5):42‐5. [Google Scholar]
Mahesh 2017 {published data only}
- Mahesh PA, Srikanth JN, Ananthakrishna MS, Parthasarathi G, Chaya SK, Rajgopal R, et al. Amelioration of quality of life and lung function of chronic obstructive pulmonary disease by pranic healing as adjuvant therapy: a randomised double blind placebo controlled pilot study. Australasian Medical Journal 2017;10(8):665‐73. [Google Scholar]
Marques 2019 {published data only}
- Marques A, Jacome C, Rebelo P, Paixao C, Oliveira A, Cruz J, et al. Improving access to community‐based pulmonary rehabilitation: 3R protocol for real‐world settings with cost‐benefit analysis. BMC Public Health 2019;19(1):676. [DOI] [PMC free article] [PubMed] [Google Scholar]
Martinez 2008 {published data only}
- Martinez G, Thogersen J, Brondum E, Ringaek T, Lange P. Effect of maintenance training after 7 weeks rehabilitation programme [abstract]. European Respiratory Society 18th Annual Congress; 2008 Oct 3‐7; Berlin. 2008:E2805.
McGlone 2006 {published data only}
- McGlone S, Venn A, Walters EH, Wood‐Baker R. Physical activity, spirometry and quality‐of‐life in chronic obstructive pulmonary disease. COPD 2006;3(2):83‐8. [DOI] [PubMed] [Google Scholar]
McMahon 2000 {published data only}
- McMahon S, Small T, Higgins BG, Corris PA. The use of a novel patient activity monitor to assess the therapeutic effect of adding salmeterol to regular therapy in patients with chronic obstructive pulmonary disease [abstract]. Thorax 2000;55(Suppl 3):A40. [Google Scholar]
Mesquita 2017 {published data only}
- Mesquita R, Meijer K, Pitta F, Azcuna H, Goertz YM, Essers JM, et al. Changes in physical activity and sedentary behaviour following pulmonary rehabilitation in patients with COPD. Respiratory Medicine 2017;126:122‐9. [DOI] [PubMed] [Google Scholar]
Moore 2009 {published data only}
- Moore R, Berlowitz D, Denehy L, Jackson B, McDonald CF. Comparison of pedometer and activity diary for measurement of physical activity in chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation and Prevention 2009;29(1):57‐61. [DOI] [PubMed] [Google Scholar]
Morris 2012 {published data only}
- Atkinson C, Seale H, Walsh J, Adams L, Morris NR. The addition of a pedometer‐guided intervention to pulmonary rehabilitation fails to improve physical activity levels in individuals with COPD [abstract]. Respirology 2012;17(Suppl 1):64. [Google Scholar]
- Morris NR, Atkinson C, Seale H, Walsh J. The addition of a pedometer guided intervention to pulmonary rehabilitation [abstract]. American Journal of Respiratory and Critical Care Medicine 2012;185:A2383. [Google Scholar]
Moy 2009 {published data only}
- Moy ML, Matthess K, Stolzmann K, Reilly J, Garshick E. Free‐living physical activity in COPD: assessment with accelerometer and activity checklist. Journal of Rehabilitation Research and Development 2009;46(2):277‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moy 2012 {published data only}
- Moy ML, Weston NA, Wilson EJ, Hess ML, Richardson CR. A pilot study of an Internet walking program and pedometer in COPD. Respiratory Medicine 2012;106(9):1342‐50. [DOI] [PubMed] [Google Scholar]
Murphy 2005 {published data only}
- Murphy MC, Campbell M, Saunders JE, Jackson B. A randomized trial to compare the outcomes of a pulmonary rehabilitation program (PRP) weekly maintenance and the Stanford Model Chronic Disease Self Management Program (CDSMP) in COPD [abstract]. American Thoracic Society International Conference; 2005 May 20‐25; San Diego. 2005:A26.
Nagata 2018 {published data only}
- Nagata K, Kikuchi T, Horie T, Shiraki A, Kitajima T, Kadowaki T, et al. Domiciliary high‐flow nasal cannula oxygen therapy for patients with stable hypercapnic Chronic Obstructive Pulmonary Disease. A multicenter randomized crossover trial. Annals of the American Thoracic Society 2018;15(4):422‐39. [DOI] [PubMed] [Google Scholar]
- Nagata K, Kikuchi T, Horie T, Shiraki A, Kitajima T, Kadowaki T, et al. Domiciliary high‐flow nasal cannula oxygen therapy for stable hypercapnic chronic obstructive pulmonary disease: a prospective, multicentre, randomised crossover trial [abstract]. European Respiratory Journal 2017;50:OA4428. [DOI] [PubMed] [Google Scholar]
NCT00620022 {published data only}
- O'Donnell D, Casaburi R, Vincken W, Puente‐Maestu L, Swales J, Lawrence D, et al. Effect of indacterol on exercise endurance and lung hyperinflation in COPD. Respiratory Medicine 2011;105(7):1030‐6. [DOI] [PubMed] [Google Scholar]
NCT01012765 {published data only}
- Watz H, Krippner F, Kirsten A, Magnussen H, Vogelmeier C. Effects of indacaterol on lung volumes and physical activity In moderate chronic obstructive pulmonary disease [abstract]. American Journal of Respiratory and Critical Care Medicine 2012;185:A2257. [Google Scholar]
- Watz H, Krippner F, Kirsten A, Magnussen, Vogelmeier C. Indacaterol improves lung hyperinflation and physical activity in patients with moderate chronic obstructive pulmonary disease ‐ a randomized, multicenter, double‐blind, placebo‐controlled study. BMC Pulmonary Medicine 2014;14(1):158. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT01380652 {published data only}
- NCT01380652. Effects of whole body vibration training on physical activity in Chronic Obstructive Pulmonary Disease (COPD) III/IV patients during a three‐week rehabilitation. clinicaltrials.gov/ct2/show/NCT01380652 (first received 27 June 2011).
NCT01486186 {published data only}
- Wang M, Li J, Li S, Wang H, Yu X, Zhang H. Effect of traditional Chinese medicine on outcomes in patients with mild/moderate chronic obstructive pulmonary disease: study protocol for a randomized placebo‐controlled trial. Trials 2012;13:109. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT01722370 {published data only}
- NCT01722370. Ambulatory oxygen effects on muscles in COPD (OM‐COPD). clinicaltrials.gov/ct2/show/NCT01722370 (first received 6 November 2012).
NCT01854008 {published data only}
- Pleguezuelos E, Pérez ME, Guirao L, Samitier B, Costea M, Ortega P, et al. Improving physical activity in patients with COPD with urban walking circuits. Respiratory Medicine 2013;107(12):1948‐56. [DOI] [PubMed] [Google Scholar]
- Pleguezuelos E, Pérez ME, Guirao L, Samitier B, Costea M, Ortega P, et al. Improving physical activity in patients with severe COPD with urban walking circuits. A randomised trial [abstract]. European Respiratory Society Annual Congress; 2013 September 7‐11; Barcelona. 2013; Vol. 42, issue Suppl 57:302s.
NCT01867970 {published data only}
- Weegen S, Verwey R, Spreeuwenberg M, Tange H, Weijden T, Witte L. It's LiFe! Mobile and web‐based monitoring and feedback tool embedded in primary care increases physical activity: a cluster randomized trial. Journal of Medical Internet Research 2015;17(7):e184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verwey R, Weegen S, Spreeuwenberg M, Tange H, Weijden T, Witte L. A monitoring and feedback tool embedded in a counselling protocol to increase physical activity of patients with COPD or type 2 diabetes in primary care: study protocol of a three‐arm cluster randomised controlled trial. BMC Family Practice 2014;15:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT01871025 {published data only}
- Rodriguez DA, Rodopin A, Guerrero M, Coll R, Huerta A, Soler N, et al. Impact of step exercises as an early intervention during COPD exaverbation [abstract]. European Respiratory Journal 2016;48:PA2061. [Google Scholar]
NCT02100709 {published data only}
- NCT02100709. The effect of NIV on QoL and exercise capacity in a COPD exercise rehabilitation program. clinicaltrials.gov/ct2/show/NCT02100709 (first received 27 March 2014).
NCT02172794 {published data only}
- NCT02172794. Tiotropium inhalation capsules and salmeterol inhalation aerosol on muscular efficiency and resting energy expenditure in patients with stable chronic obstructive pulmonary disease. clinicaltrials.gov/ct2/show/NCT02172794 (first received 24 June 2014).
NCT02629965 {published data only}
- NCT02629965. Comparing the efficacy of tiotropium + olodaterol fixed dose combination over tiotropium in improvement of lung hyperinflation, exercise capacity and physical activity in Japanese COPD patients. clinicaltrials.gov/ct2/show/NCT02629965 (first received 15 December 2015).
NCT02656667 {published data only}
- Vivodtzev I, Debigaré R, Gagnon P, Mainguy V, Saey D, Dubé A, et al. Functional and muscular effects of neuromuscular electrical stimulation in patients with severe COPD: a randomized clinical trial. Chest 2012;141(3):716‐25. [DOI: 10.1378/chest.11-0839; NCT02656667] [DOI] [PubMed] [Google Scholar]
NCT03751670 {published data only}
- NCT03751670. Pulmonary rehabilitation during acute exacerbations of Chronic Obstructive Pulmonary Disease: a mixed‐methods approach. clinicaltrials.gov/ct2/show/NCT03751670 (first received 23 November 2018).
NL1729 {published data only}
- NL1729. Effects of a phyisiotherapeutic exercise programme in patients with a combination of COPD and chronic heart failure: the CHEST‐study. www.trialregister.nl/trial/1729 (first received 2009).
Norweg 2006 {published data only}
- Norweg AM, Whiteson J, Malady R, Mola A, Rey M. The effectiveness of different combinations of pulmonary rehabilitation program components: a randomized controlled trial. Journal of Cardiopulmonary Rehabilitation 2006;26(2):120‐1. [DOI] [PubMed] [Google Scholar]
Nyberg 2017 {published data only}
- Nyberg A, Wadell K, Lindgren H, Tistad M. Internet‐based support for self‐management strategies for people with COPD‐protocol for a controlled pragmatic pilot trial of effectiveness and a process evaluation in primary healthcare. BMJ Open 2017;7(7):e016851. [DOI] [PMC free article] [PubMed] [Google Scholar]
Paneroni 2016 {published data only}
- Paneroni M, Scalvini S, Bernocchi P, Galli T, Baratti D, Rovere MT, et al. Home telerehabilitation maintenance program for patients affected by COPD and CHF [abstract]. European Respiratory Journal 2016;48(Suppl 60):OA268. [Google Scholar]
Pasqua 2010 {published data only}
- Pasqua F, Biscione G, Crigna G, Auciello L, Cazzola M. Combining triple therapy and pulmonary rehabilitation in patients with advanced COPD: A pilot study. Respiratory Medicine 2010;104(3):412‐7. [DOI] [PubMed] [Google Scholar]
Pinnock 2013 {published data only}
- Pinnock H, Hanley J, Lewis S, MacNee W, Pagliari C, Pol M, et al. The impact of a telemetric chronic obstructive pulmonary disease monitoring service: Randomised controlled trial with economic evaluation and nested qualitative study. Primary Care Respiratory Journal 2009;18(3):233‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pitta 2008 {published data only}
- Pitta F, Takaki MY, Oliveira NH, Sant'anna TJ, Fontana AD, Kovelis D, et al. Relationship between pulmonary function and physical activity in daily life in patients with COPD. Respiratory Medicine 2008;102(8):1203‐7. [DOI] [PubMed] [Google Scholar]
Pomidori 2012 {published data only}
- Pomidori L, Contoli M, Mandolesi G, Cogo A. A simple method for home exercise training in patients with chronic obstructive pulmonary disease: One‐year study. Journal of Cardiopulmonary Rehabilitation and Prevention 2012;32(1):53‐7. [DOI] [PubMed] [Google Scholar]
Raphael 2014 {published data only}
- Raphael Y, Maynard Da Silva K, Bessa EJ, Bartholo TP, Faria AC, Noronha Filho AJ, et al. Brazilian manual of home‐based pulmonary rehabilitation: does it maintain the benefits achieved during the outpatient program? [abstract]. American Journal of Respiratory and Critical Care Medicine 2014;189:A1913. [Google Scholar]
Ringbaek 2009 {published data only}
- Ringbaek T, Broendum E, Martinez G, Thoegersen J, Lange P. Effect of maintenance training after 7‐weeks rehabilitation programme on hospitalisation [abstract]. European Respiratory Society 19th Annual Congress; 2009 Sep 12‐15; Vienna. 2009:P576.
Robbins 2000 {published data only}
- Robbins R. More evidence for the short‐term beneficial effects of lung volume reduction surgery. Critical Care 2002;2(1):6379. [Google Scholar]
Rodriguez‐Trigo 2011 {published data only}
- Rodriguez‐Trigo G, Cejudo P, Puy C, Galdiz JB, Bdeir K, Gorostiza A, et al. Long term pulmonary rehabilitation programs for chronic obstructive pulmonary disease (COPD). Two years follow‐up [abstract]. European Respiratory Journal 2011;38(55):655s. [Google Scholar]
Romagnoli 2005 {published data only}
- Romagnoli M, Dell'Orso D, Lubello R, Lucic S, Lugli D, Bellantone T, et al. Repeated pulmonary rehabilitation program (PRP) in severe and disabled COPD patients [abstract]. European Respiratory Journal 2005;26(Supp 49):A542. [Google Scholar]
Roman 2013 {published data only}
- Roman M, Larraz C, Gomez A, Ripoll J, Mir I, Miranda EZ, et al. Efficacy of pulmonary rehabilitation in patients with moderate chronic obstructive pulmonary disease: a randomized controlled trial. BMC Family Practice 2013;14(1):21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schacher 2006 {published data only}
- Schacher C, Dhein Y, Schoeffski O, Worth H. Comparison of two different exercise programs in chronic obstructive pulmonary disease [abstract]. European Respiratory Journal 2006;28(Suppl 50):555s. [Google Scholar]
Schönhofer 1997 {published data only}
- Schönhofer B, Ardes P, Geibel M, Köhler D, Jones PW. Evaluation of a movement detector to measure daily activity in patients with chronic lung disease. European Respiratory Journal 1997;10(12):2814‐9. [DOI] [PubMed] [Google Scholar]
Senthilnathan 2018 {published data only}
- Senthilnathan CV, Abinaya P, Rajalaxmi V, Mohan Kumar G, Subramanian SS. Efficacy of physical training program on chronic obstructive pulmonary disease [abstract]. Biomedicine 2018;38(2):240. [Google Scholar]
Sewell 2005 {published data only}
- Sewell L, Singh SJ, Williams JE, Collier R, Morgan MD. Can individualized rehabilitation improve functional independence in elderly patients with COPD?. Chest 2005;128(3):1194‐200. [DOI] [PubMed] [Google Scholar]
- Sewell L, Singh SJ, Williams JE, Collier R, Morgan MD. Goal directed pulmonary rehabilitation does not significantly improve health status and domestic function. European Respiratory Journal 2001;18(Suppl 33):187s. [Google Scholar]
Sewell 2010 {published data only}
- Sewell L, Singh SJ, Williams JE, Morgan MD. Seasonal variations affect physical activity and pulmonary rehabilitation outcomes. Journal of Cardiopulmonary Rehabilitation and Prevention 2010;30(5):329‐33. [DOI] [PubMed] [Google Scholar]
Sirichana 2013 {published data only}
- Sirichana W, Moore‐Gillon CE, Patel MH, Taylor M, Storer TW, Cooperr CB. Daily physical activity in COPD: quantification by tri‐axial accelerometry [abstract]. American Journal of Respiratory and Critical Care Medicine 2013;187:A1361. [Google Scholar]
Soicher 2009 {published data only}
- Soicher JE. A longitudinal study of physical activity behaviour in chronic disease: the example of chronic obstructive pulmonary disease [dissertation]. Montreal: McGill University, Montreal, 2009. [Google Scholar]
Spencer 2012 {published data only}
- Spencer L, Mckeough Z, Alison J. Where are they now? Four years after the completion of a maintenance exercise programme in people with COPD [abstract]. Respirology 2012;17(Suppl 1):15. [Google Scholar]
Steele 2008 {published data only}
- Steele BG, Belza B, Cain KC, Coppersmith J, Lakshminarayan S, Howard J, et al. A randomized clinical trial of an activity and exercise adherence intervention in chronic pulmonary disease. Archives of Physical Medicine and Rehabilitation 2008;89(3):404‐12. [DOI] [PubMed] [Google Scholar]
- Steele BG, Belza B, Coppersmith J, Cain K, Howard J, Lakshminarayan S. Promoting activity and exercise in chronic lung disease: an intervention study [abstract]. American Journal of Respiratory and Critical Care Medicine 2005;191:A2007. [Google Scholar]
Strijbos 1991 {published data only}
- Strijbos JH, Koeter GH, Postma DS, Altena R. Reactivation of severe COPD patients. Long term results of a first line and a clinical rehabilitation program. Nederlands Tijdschrift Fysiotherapie 1991;101(4):105‐10. [Google Scholar]
Sutanto 2018 {published data only}
- Sutanto YS, Santi N, Makhabah DN, Aphridasari J, Kusumo H, Reviono R. Pedometer as a tool for quality of life improvement in COPD patients [abstract]. Respirology 2018;23(Suppl 2):244‐5. [Google Scholar]
TCTR20170214002 {published data only}
- TCTR20170214002. The effects of breathing with a positive expiratory pressure on physical activity in patients with Chronic Obstructive Pulmonary Disease. www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=2177 (first received 5 February 2017).
Troosters 2010 {published data only}
- Troosters T, Sciurba F, Battaglia S, Langer D, Valluri SR, Martino L, et al. Physical inactivity in patients with COPD, a controlled multi‐center pilot‐study. Respiratory Medicine 2010;104(7):1005‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Troosters 2011 {published data only}
- Troosters T, Sutradhar S, Sciurba FC, Klioze SS, Siafakas N, Yunis C, et al. Understanding physical activity in moderate COPD: results from a large, multicenter trial [abstract]. American Journal of Respiratory and Critical Care Medicine 2011;183:A3959. [Google Scholar]
Tse 2013 {published data only}
- Tse HN, Raiteri L, Wong KY, Yee KS, Ng LY, Wai KY, et al. High‐dose N‐acetylcysteine in stable COPD: the 1‐year, double‐blind, randomized, placebo‐controlled HIACE study. Chest 2013;144(1):106‐18. [DOI] [PubMed] [Google Scholar]
Turnbull 2013 {published data only}
- Turnbull J, McDonnell L, Bott J, Prevost T, Davidson C. Physical exercise and ambulatory oxygen device preference in patients' with exertional hypoxemia: a multicentre RCT [abstract]. European Respiratory Journal 2013;42(Suppl 57):772s. [Google Scholar]
- Turnbull J, McDonnell L, Osman L, Bott J, Prevost T, Davidson AC. Patient activity levels and oxygen device preference: an RCT comparing refillable cylinders (HomefillTM) with usual ambulatory device [abstract]. Thorax 2012;67(Suppl 2):A83. [Google Scholar]
Turner‐Lawlor 2005 {published data only}
- Turner‐Lawlor PJ, Shiels K, Griffiths TL. Randomized controlled trial of an 18 session pulmonary rehabilitation program delivered over 6 or 18 weeks, clinical outcomes [abstract]. American Thoracic Society International Conference; 2005 May 20‐25; San Diego. 2005:C87.
U1111‐1169‐0718 {published data only}
- U1111‐1169‐0718. Effect of training in vibrating platform in subjects with Chronic Obstructive Pulmonary Disease. www.ensaiosclinicos.gov.br/rg/RBR‐3kxkzn/ (first received 7 April 2015).
UMIN000001833 {published data only}
- Sakai K, Nakayama H, Hokari S, Suzuki R, Takiguchi A, Takada T, et al. The efficacy of the assistant use of short‐acting Beta2 stimulant procaterol on the daily activity in COPD patients: Niigata multicentre study [abstract]. European Respiratory Journal 2011;38:862. [Google Scholar]
Valenson 2016 {published data only}
- Valenson W, Valmonte F, Rodriguez O, Medina E, Lowrey M, Lew S, et al. Perceived barriers to physical activity in patients at high risk for COPD exacerbations. Chest 2016;150(4 Suppl 1):892A. [Google Scholar]
Voncken‐Brewster 2013 {published data only}
- Voncken‐Brewster V, Tange H, Vries H, Nagykaldi Z, Winkens B, Weijden T. A randomised controlled trial testing a web‐based, computer‐tailored self‐management intervention for people with or at risk for chronic obstructive pulmonary disease: a study protocol. BMC Public Health 2013;13:557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voncken‐Brewster V, Tange H, Vries H, Nagykaldi Z, Winkens B, Weijden T. A randomized controlled trial evaluating the effectiveness of a web‐based, computer‐tailored self‐management intervention for people with or at risk for COPD. International Journal of Chronic Obstructive Pulmonary Disease 2015;10:1061‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wilson 2015 {published data only}
- Wilson AM, Browne P, Olive S, Clark A, Galey P, Dix E, et al. The effects of maintenance schedules following pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a randomised controlled trial. BMJ Open 2015;5(3):e005921. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zanini 2002 {published data only}
- Zanini A, Giorgetti G, Facchetti C, Mazzucchelli G, Conti S, Lucioni A, et al. Efficacy of a rehabilitation program based on circuit training in COPD subjects: A preliminary report [abstract]. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A738. [Google Scholar]
References to ongoing studies
ACTRN12615000121561 {published data only}
- ACTRN12615000121561. Effect of opioids on outcomes of pulmonary rehabilitation. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=367581 (first received 12 January 2015).
ACTRN 12616000360415 {published data only}
- Cox NS, McDonald CF, Alison JA, Mahal A, Wootton R, Hill CJ, et al. Telerehabilitation versus traditional centre‐based pulmonary rehabilitation for people with chronic respiratory disease: protocol for a randomised controlled trial. BMC Pulmonary Medicine 2018;18:71. [DOI] [PMC free article] [PubMed] [Google Scholar]
ACTRN12616001534471 {published data only}
- ACTRN12616001534471. A behaviour‐change intervention to reduce sedentary time in people with chronic obstructive pulmonary disease. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=371728 (first received 3 Nov 2016).
- Cheng SW, Alison JA, Dennis S, Stamatakis E, Spencer LM, McNamara RJ, et al. A behaviour change intervention to reduce sedentary time in people with chronic obstructive pulmonary disease: a protocol for a randomised controlled trial. Journal of Physiotherapy 2017;63:182. [DOI] [PubMed] [Google Scholar]
ACTRN12616001586404 {published data only}
- ACTRN12616001586404. Effect of a pulmonary rehabilitation program of 8 weeks duration compared to 12 weeks on exercise capacity in people with chronic obstructive pulmonary disease (PuRe Duration): a randomised controlled trial. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=371612 (first received 16 November 2016).
ACTRN12617000242325 {published data only}
- ACTRN12617000242325. Tai Chi for people with chronic obstructive pulmonary disease (COPD). www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372216 (first received 16 February 2017).
ACTRN12617000499381 {published data only}
- ACTRN12617000499381. Non drug interventions to reduce breathlessness in patients with chronic obstructive pulmonary disease (emphysema). www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372467 (first received 6 April 2017).
ACTRN12617000653369 {published data only}
- ACTRN12617000653369. Effect of cognitive behaviour therapy on anxiety, depression and breathlessness in patients with chronic obstructive pulmonary disease. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372765 (first received 5 May 2017).
ANZCTR12611000292976 {published data only}
- ANZCTR12611000292976. Can changing the way people with chronic lung disease think about breathlessness improve and sustain health outcomes?. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=336473 (first received 17 March 2011).
- Williams MT, John D, Cafarella P, Frith P. No additional benefit for 6MWT or HADS in combining cognitive behavioural therapy and pulmonary rehabilitation [abstract]. Respirology 2017;22(S2):TO050. [Google Scholar]
- Williams MT, Paquet C, John D, Cafarella P, Frith P. No additional benefits for pulmonary rehabilitation including cognitive behavioural therapy [abstract]. Respirology 2018;23(S1):TO131. [Google Scholar]
Beekman 2014 {published data only}
- Beekman E, Mesters I, Hendriks EJ, Muris JW, Wesseling G, Evers SM, et al. Exacerbations in patients with chronic obstructive pulmonary disease receiving physical therapy: a cohort‐nested randomised controlled trial [protocol]. BMC Pulmonary Medicine 2014;14(1):71. [DOI] [PMC free article] [PubMed] [Google Scholar]
ChiCTR1800017405 {published data only}
- ChiCTR1800017405. Effects of pulmonary rehabilitation prescription on COPD patients. www.chictr.org.cn/showprojen.aspx?proj=28343 (first received 28 July 2018).
DRKS00004931 {published data only}
- DRKS00004931. "Medical Vulnerability" Impact of hospital room cooling in vulnerable patients with lung disease during periods of extreme weather (UCaHS). www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00004931 (first received 26 April 2013).
DRKS00010777 {published data only}
- DRKS00010777. The influence of the maintenance of physical activity on mental health of patients with occupational lung diseases after an inpatient rehabilitation in the BG clinic of Falkenstein. www.dguv.de/ifa/forschung/projektverzeichnis/ff‐fb0227‐2.jsp (first received 15 December 2017).
EUCTR2006‐005534‐20‐GB {published data only}
- EUCTR2006‐005534‐20‐GB. Effect of erdosteine on inflammatory and oxidative biomarkers in sputum and exhaled breath in patients with COPD. www.clinicaltrialsregister.eu/ctr‐search/trial/2006‐005534‐20/GB (first received 29 November 2007).
EUCTR2013‐003619‐24‐ES {published data only}
- EUCTR2013‐003619‐24‐ES. Benefits of liquid oxygen in chronic obstructive pulmonary disease (COPD) patients without evidence of domiciliary oxygen therapy, presenting desaturation on exertion. www.clinicaltrialsregister.eu/ctr‐search/trial/2013‐003619‐24/ES (first received 13 December 2013).
EUCTR2016‐001238‐89‐ES {published data only}
- EUCTR2016‐001238‐89‐ES. Impact of iron replacement in patients with chronic obstructive pulmonary disease. www.clinicaltrialsregister.eu/ctr‐search/trial/2016‐001238‐89/ES (first received 20 April 2016).
EUCTR2016‐001805‐18‐SE {published data only}
- EUCTR2016‐001805‐18‐SE. A pilot study to explore safety and efficacy of NBMI treatment compared to placebo in patients with chronic obstructive pulmonary disease. www.clinicaltrialsregister.eu/ctr‐search/trial/2016‐001805‐18/SE (first received 19 May 2016).
Fastenau 2014 {published data only}
- Fastenau A. Exercise training and physical activity in patients with mild to moderate COPD in primary care [thesis]. Maastricht: Maastricht University, Maastricht, 2015. [Google Scholar]
- Fastenau A, Muris JW, Bie RA, Hendriks EJ, Asijee GM, Beekman E, et al. Efficacy of a physical exercise training programme COPD in primary care: study protocol of a randomized controlled trial. BMC Public Health 2014;14:788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fastenau A, Schayck O, Winkens B, Gosselink R, Muris J. Effectiveness of a physical exercise training programme COPD in primary care: a randomized controlled trial [abstract]. European Respiratory Journal 2015;46:OA3287. [DOI] [PubMed] [Google Scholar]
ISRCTN11017699 {published data only}
- ISRCTN11017699. Investigation of steroid responsiveness in patients with chronic obstructive pulmonary disease. www.isrctn.com/ISRCTN11017699 (first received 15 November 2016).
ISRCTN13899108 {published data only}
- ISRCTN13899108. Can a physical activity programme or pulmonary rehabilitation reduce the risk of heart and circulation disease in people with COPD?. www.isrctn.com/ISRCTN13899108 (first received 5 April 2019).
ISRCTN15949009 {published data only}
- ISRCTN15949009. Humidified nasal high flow to improve clinical outcomes following severe exacerbations of chronic obstructive pulmonary disease. www.isrctn.com/ISRCTN15949009 (first received 19 February 2019).
ISRCTN17942821 {published data only}
- Bourne CL, Kanabar P, Mitchell K, Schreder S, Houchen‐Wolloff L, Bankart MJ, et al. A self‐management programme of activity coping and education ‐ SPACE for COPD(C) ‐ in primary care: the protocol for a pragmatic trial. BMJ Open 2017;7(7):e014463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN17942821. A self‐management programme of activity coping and education ‐ SPACE FOR COPD ‐ in primary care: a pragmatic trial. www.isrctn.com/ISRCTN17942821?q=&filters=conditionCategory:Respiratory,ageRange:All&sort=relevance&offset=1&totalResults=9&page=1&pageSize=10&searchType=basic‐search (first received 17 November 2014).
ISRCTN19684749 {published data only}
- Buttery S, Kemp SV, Shah PL, Waller D, Jordan S, Lee JT, et al. CELEB trial: Comparative effectiveness of lung volume reduction surgery for emphysema and bronchoscopic lung volume reduction with valve placement: a protocol for a randomised controlled trial. BMJ Open 2018;8:e021368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN19684749. CELEB: Lung volume reduction in COPD ‐ surgery vs endobronchial valves. www.isrctn.com/ISRCTN19684749?q=&filters=conditionCategory:Respiratory&sort=&offset=9&totalResults=657&page=1&pageSize=10&searchType=basic‐search (first received 23 May 2016).
ISRCTN27860457 {published data only}
- ISRCTN27860457. ON‐EPIC Oral nitrate supplementation to enhance pulmonary rehabilitation in chronic obstructive pulmonary disease. www.isrctn.com/ISRCTN27860457 (first received 22 September 2014).
- Pavitt M, Lewis AP, Buttery SC, Fernandez BO, Mikus‐Lelinska M, Feelisch M, et al. Dietary nitrate supplementation increases exercise endurance time in COPD patients using ambulatory oxygen [abstract]. European Respiratory Journal 2018;52(Suppl 62):PA4049. [Google Scholar]
- Pavitt M, Tanner RJ, Lewis AP, Buttery SC, Mehta B, Jefford H, et al. Dietary nitrate supplementation enhances the benefit of pulmonary rehabilitation in people with COPD [abstract]. European Respiratory Journal 2018;52(Suppl 62):PA4045. [Google Scholar]
- Pavitt MJ, Tanner RJ, Lewis AP, Buttery SC, Mehta B, Jefford H, et al. Oral dietary nitrate supplementation to enhance pulmonary rehabilitation in chronic obstructive pulmonary disease: a multi‐centre, double blind, placebo‐controlled, parallel group study [abstract]. Thorax 2018;73(Suppl 4):A3. [DOI] [PubMed] [Google Scholar]
ISRCTN45695543 {published data only}
- Daynes E, Greening N, Sidiqqui S, Singh SJ. A randomised controlled trial to investigate the use of high‐frequency airway oscillations as training to improve dyspnoea in COPD [protocol]. ERJ Open Research 2019;5:00064‐2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN45695543. Training to improve dyspnoea. www.isrctn.com/ISRCTN45695543 (first received 15 February 2017).
ISRCTN80279999 {published data only}
- ISRCTN80279999. Domiciliary application of non‐invasive positive pressure ventilation with average volume assured pressure support to subjects with chronic obstructive pulmonary disease (COPD) who remain hypercapnic following the application of non‐invasive positive pressure ventilation (NPPV) for an acute exacerbation. www.isrctn.com/ISRCTN80279999 (first received 11 December 2008).
NCT01037387 {published data only}
- NCT01037387. Effect of noninvasive ventilation on physical activity and inflammation in COPD patients. clinicaltrials.gov/ct2/show/NCT01037387 (first received 23 December 2009).
NCT01537627 {published data only}
- NCT01537627. Long‐term physical training in chronic obstructive pulmonary disease. clinicaltrials.gov/ct2/show/NCT01537627 (first received 23 February 2012).
NCT01539434 {published data only}
- NCT01539434. Behavioral intervention to maintain physical capacity and activity in patients with chronic obstructive pulmonary disease (COPD). clinicaltrials.gov/ct2/show/NCT01539434 (first received 27 February 2012).
NCT01783808 {published data only}
- NCT01783808. Intervention study to investigate supplemental oxygen in COPD. clinicaltrials.gov/ct2/show/NCT01783808 (first received 5 February 2013).
NCT01905982 {published data only}
- NCT01905982. The effect of reflective breathing therapy compared with conventional breathing therapy in patients with chronic obstructive pulmonary disease (COPD) III‐IV; part 2. clinicaltrials.gov/ct2/show/NCT01905982 (first received 23 July 2013).
NCT01998724 {published data only}
- Moy ML, Wayne PM, Litrownik D, Beach D, Klings ES, Davis RB, et al. Long‐term exercise after pulmonary rehabilitation (LEAP): design and rationale of a randomized controlled trial of Tai Chi. Contemporary Clinical Trials 2015;45(Part B):458‐67. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT02099799 {published data only}
- NCT02099799. The effect of physical activity promotion on short and long‐term outcomes in COPD (WEB). clinicaltrials.gov/ct2/show/NCT02099799 (first received 31 March 2014).
NCT02205242 {published data only}
- NCT02205242. BACE trial substudy 1 ‐ PROactive substudy. clinicaltrials.gov/ct2/show/NCT02205242 (first received 31 July 2014).
NCT02398643 {published data only}
- NCT02398643. Examine the impact of early education on COPD management. clinicaltrials.gov/ct2/show/NCT02398643 (first received 25 March 2015).
NCT02455206 {published data only}
- NCT02455206. Counseling during pulmonary rehabilitation. clinicaltrials.gov/ct2/show/NCT02455206 (first received 27 May 2015).
- Rausch‐Osthoff AK, Greco N, Schwank A, Beyer S, Gisi D, Scheermesser M, et al. Effect of counselling during pulmonary rehabilitation on self‐determined motivation towards physical activity in people with chronic obstructive pulmonary disease ‐ protocol of a mixed methods study. BMC Pulmonary Medicine 2017;17(1):115. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT02471235 {published data only}
- Ko FW, Chan K‐P, Tam W, Wong I, Chan TO, Ip A, et al. Short‐course pulmonary rehabilitation and exacerbations and activity of COPD patients over 1 year [abstract]. European Respiratory Journal 2018;52(Suppl 52):PA3353. [Google Scholar]
- NCT02471235. Short‐course out‐patient pulmonary rehabilitation and COPD exacerbations. clinicaltrials.gov/ct2/show/NCT02471235 (first received 15 June 2015).
NCT02478359 {published data only}
- Estrada EL, Silva K, Medina E, Desai S, Fan VS, Nguyen HQ. Depression and anxiety are associated with COPD patients' lower confidence for increasing physical activity but not with their motivation [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A7066. [Google Scholar]
- Lee JS, Liu AI, Pounds D, Mahmud F, Flores C, Desai SA, et al. Characteristics of COPD patients who agree to participate in a pragmatic trial of physical activity coaching compared to non‐participants [abstract]. American Journal of Respiratory and Critical Care Medicine 2018;197:A2642. [Google Scholar]
- NCT02478359. Walk on! Physical activity coaching. clinicaltrials.gov/ct2/show/NCT02478359 (first received 23 June 2015).
- Nguyen HQ, Bailey A, Coleman KJ, Desai S, Fan VS, Gould MK, et al. Patient‐centered physical activity coaching in COPD (Walk On!): a study protocol for a pragmatic randomized controlled trial. Contemporary Clinical Trials 2016;46:18‐29. [DOI] [PubMed] [Google Scholar]
- Valenson W, Valmonte F, Rodriguez O, Medina E, Lowrey M, Lew S, et al. Perceived barriers to physical activity in patients at high risk for COPD exacerbations [abstract]. Chest 2016;150(4 Suppl 1):892A. [Google Scholar]
NCT02557178 {published data only}
- NCT02557178. Home‐based health management of COPD patients. clinicaltrials.gov/ct2/show/NCT02557178 (first received 23 September 2015).
NCT02667171 {published data only}
- Hansen H, Bieler T, Beyer N, Godtfredsen N, Kallemose T, Frolich A. COPD online‐rehabilitation versus conventional COPD rehabilitation ‐ rationale and design for a multicenter randomized controlled trial study protocol (CORe trial). BMC Pulmonary Medicine 2017;17:140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02667171. COPD online rehabilitation (CORe) (CORe). clinicaltrials.gov/ct2/show/NCT02667171 (first received 28 January 2016).
NCT02691104 {published data only}
- NCT02691104. Use of the SMART COPD physical activity app in pulmonary rehabilitation. clinicaltrials.gov/ct2/show/NCT02691104 (first received 25 February 2016).
NCT02702791 {published data only}
- NCT02702791. Sustaining training effects through physical activity (STEP). clinicaltrials.gov/ct2/show/NCT02702791 (first received 9 March 2016).
NCT02707770 {published data only}
- NCT02707770. The role of ambulatory oxygen in improving the effectiveness of pulmonary rehabilitation for COPD patients. clinicaltrials.gov/ct2/show/NCT02707770 (first received 14 March 2016).
NCT02720822 {published data only}
- Currow D, Watts GJ, Johnson M, McDonald CF, Miners JO, Somogyi AA, et al. on behalf of the Australian National Palliative Care Clinical Studies Collaborative. A pragmatic, phase III, multisite, double‐blind, placebo‐controlled, parallel‐arm, dose increment randomised trial of regular, low‐dose extended‐release morphine for chronic breathlessness: breathlessness, exertion And morphine sulfate (BEAMS) study protocol. BMJ Open 2017;7(7):e018100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02720822. Breathlessness exertion and morphine sulphate (BEAMS). clinicaltrials.gov/ct2/show/NCT02720822 (first received 28 March 2016).
NCT02864420 {published data only}
- Levine DM, Ouchi K, Blanchfield B, Diamond K, Licurse A, Pu CT, et al. Hospital‐level care at home for acutely ill adults: a pilot randomized controlled trial. Journal of General Internal Medicine 2018;33(5):729‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02864420. Hospitalization at home: The acute care home hospital program for adults. clinicaltrials.gov/ct2/show/NCT02864420 (first received 12 August 2016).
NCT02895152 {published data only}
- NCT02895152. Activity monitor use in COPD patients undergoing rehabilitation. clinicaltrials.gov/ct2/show/NCT02895152 (first received 9 September 2016).
NCT02917915 {published data only}
- NCT02917915. The CaNadian Standardized Pulmonary Rehabilitation Efficacy trial (CoNSPiRE). clinicaltrials.gov/ct2/show/NCT02917915 (first received 28 September 2016).
- Selzler AM, Jourdain T, Sedeno M, Wald J, Janaudis‐Ferreira T, Goldstein R, et al. Development of the Canadian standardized pulmonary rehabilitation efficacy trial: a protocol update [abstract]. Canadian Journal of Respiratory Critical Care and Sleep Medicine 2017;1(3):170. [Google Scholar]
NCT02924870 {published data only}
- NCT02924870. Long‐term effect of an health education program on daily physical activity in patients with moderate to very severe chronic obstructive pulmonary disease (EA‐EPOC). clinicaltrials.gov/ct2/show/NCT02924870 (first received 5 October 2016).
NCT02956213 {published data only}
- NCT02956213. Indoor air quality and respiratory symptoms in former smokers. clinicaltrials.gov/ct2/show/NCT02956213 (first received 6 November 2016).
NCT02966561 {published data only}
- Geidl W, Semrau J, Streber R, Lehbert N, Wingart S, Tallner A, et al. Effects of a brief, pedometer‐based behavioral intervention for individuals with COPD during inpatient pulmonary rehabilitation on 6‐week and 6‐month objectively measured physical activity: study protocol for a randomized controlled trial. Trials 2017;18:396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02966561. Pedometer‐based behavioural intervention for individuals with COPD to stay active after rehabilitation (STAR). clinicaltrials.gov/ct2/show/NCT02966561 (first received 17 November 2016).
NCT02999685 {published data only}
- Benzo RP, Kramer KM, Hoult JP, Anderson PM, Begue IM, Seifert SJ. Development and feasibility of a home pulmonary rehabilitation program with health coaching. Respiratory Care 2018;63(2):131‐40. [DOI] [PubMed] [Google Scholar]
- NCT02999685. Home‐based health management of chronic obstructive lung Ddsease (COPD) patients. clinicaltrials.gov/ct2/show/NCT02999685 (first received 21 December 2016).
NCT03073954 {published data only}
- NCT03073954. Working memory training in COPD patients: the Cogtrain‐Trial. clinicaltrials.gov/ct2/show/NCT03073954 (first received 8 March 2017).
NCT03080662 {published data only}
- NCT03080662. Impact of inspiratory muscle training on daily physical activity (INAF). clinicaltrials.gov/ct2/show/NCT03080662 (first received 15 March 2017).
NCT03084874 {published data only}
- NCT03084874. Efficacy of a coaching program to promote physical activity and reduce sedentary behavior after a COPD hospitalization. clinicaltrials.gov/ct2/show/NCT03084874 (first received 21 March 2017).
NCT03114241 {published data only}
- NCT03114241. Long‐term effects of a 3‐month pedometer‐based program to enhance physical activity in patients with severe COPD. clinicaltrials.gov/ct2/show/NCT03114241 (first received 14 April 2017).
NCT03127878 {published data only}
- NCT03127878. Effects of upper‐limb training addition to a conventional ET program on PA level and ADL performance. clinicaltrials.gov/ct2/show/NCT03127878 (first received 25 April 2017).
NCT03201198 {published data only}
- NCT03201198. Active for life: chronic obstructive pulmonary disease (ActiveCOPD). clinicaltrials.gov/ct2/show/NCT03201198 (first received 28 June 2017).
NCT03275116 {published data only}
- NCT03275116. The effect of twice daily vs. once daily bronchodilation on hyperinflation in COPD patients during 24 hours (BOTH). clinicaltrials.gov/ct2/show/NCT03275116 (first received 7 September 2017).
NCT03280355 {published data only}
- NCT03280355. The effects of singing training for patients with chronic obstructive pulmonary disease. clinicaltrials.gov/ct2/show/NCT03280355 (first received 12 September 2017).
NCT03321279 {published data only}
- NCT03321279. Social incentives to increase mobility. clinicaltrials.gov/ct2/show/NCT03321279 (first received 25 October 2017).
NCT03359473 {published data only}
- NCT03359473. Study to evaluate the safety and efficacy of 13 weeks of the selective androgen receptor modulator (SARM) GSK2881078 in chronic obstructive pulmonary disease. clinicaltrials.gov/ct2/show/NCT03359473 (first received 2 December 2017).
NCT03513068 {published data only}
- NCT03513068. Portable oxygen concentrator improvements to physical activity, oxygen usage, and quality of life in chronic obstructive pulmonary disease patients using long‐term oxygen therapy (POC‐STEP). clinicaltrials.gov/ct2/show/NCT03513068 (first received 1 May 2018).
NCT03584269 {published data only}
- NCT03584269. Innovation in non invasive ventilation in COPD patients treated by long term oxygen therapy (INOV‐LTOT). clinicaltrials.gov/ct2/show/NCT03584269 (first received 12 July 2018).
NCT03584295 {published data only}
- NCT03584295. Early extubation by ECCO2R compared to IMV in patients with severe acute exacerbation of COPD (X‐COPD). clinicaltrials.gov/ct2/show/NCT03584269 (first received 12 July 2018).
NCT03620630 {published data only}
- NCT03620630. Clinical efficacy and cost effectiveness of MYCOPD in patients with mild and moderate newly diagnosed COPD (EARLY). clinicaltrials.gov/ct2/show/NCT03620630 (first received 8 August 2018).
NCT03654092 {published data only}
- Frei A, Radtke T, Lana KD, Braun J, Müller RM, Puhan MA. Effects of a long‐term home‐based exercise training programme using minimal equipment vs. usual care in COPD patients: a study protocol for two multicentre randomised controlled trials (HOMEX‐1 and HOMEX‐2 trials). BMC Pulmonary Medicine 2019;19:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT03655028 {published data only}
- NCT03655028. Increasing physical activity in COPD through rhythmically enhanced music. clinicaltrials.gov/ct2/show/NCT03655028 (first received 31 August 2018).
NCT03660644 {published data only}
- NCT03660644. Physical activity following pulmonary rehabilitation in COPD. clinicaltrials.gov/ct2/show/NCT03660644 (first received 6 September 2018).
NCT03746873 {published data only}
- NCT03746873. Increase level of physical activity and decrease use of health care for people with COPD. clinicaltrials.gov/ct2/show/NCT03746873 (first received 20 November 2018).
NCT03749655 {published data only}
- NCT03749655. Physical activity promotion added to standard care pulmonary rehabilitation and cognitive behavioural therapy. clinicaltrials.gov/ct2/show/NCT03749655 (first received 21 November 2018).
NCT03750292 {published data only}
- NCT03750292. Residential cleaning of indoor air to protect COPD patients (CARE). clinicaltrials.gov/ct2/show/NCT03750292 (first received 23 November 2018).
NCT03793192 {published data only}
- NCT03793192. Promoting activity after COPD exacerbations (aim 2, PACE2). clinicaltrials.gov/ct2/show/NCT03793192 (first received 4 January 2019).
NCT03794921 {published data only}
- NCT03794921. COPD access to pulmonary rehabilitation intervention (CAPRI). clinicaltrials.gov/ct2/show/NCT03794921 (first received 7 January 2019).
NCT03807310 {published data only}
- NCT03807310. Targeted nutrient supplement in COPD (NUTRECOVER‐trial). clinicaltrials.gov/ct2/show/NCT03807310 (first received 16 January 2019).
NCT03810755 {published data only}
- NCT03810755. EfiKroniK research program: physical exercise for people with chronic pathologies. clinicaltrials.gov/ct2/show/NCT03810755 (first received 22 January 2019).
NCT03817294 {published data only}
- NCT03817294. Personalised exercise training in COPD. clinicaltrials.gov/ct2/show/NCT03817294 (first received 25 January 2019).
NCT03869112 {published data only}
- NCT03869112. Physical activity intervention and cardiovascular risk markers in COPD (PARC). clinicaltrials.gov/ct2/show/NCT03869112 (first received 11 March 2019).
NCT03899558 {published data only}
- NCT03899558. The role of HNHF to improve clinical outcomes following severe AECOPD. clinicaltrials.gov/ct2/show/NCT03899558 (first received 2 April 2019).
NL3827 {published data only}
- NL3827. Pulmonary rehabilitation of COPD: a trial of sustained internet based self‐management support (PRACTISS COPD). www.trialregister.nl/trial/3827 (first received 27 May 2013).
NL5277 {published data only}
- NL5277. Efficacy of a physical activity coaching system for patients with COPD. www.trialregister.nl/trial/5277 (first received 30 October 2015).
RBR‐3zmh3r {published data only}
- RBR‐3zmh3r. Effects of the inclusion of a functional circuit to aerobic and resistance training on functionality, physical activity in daily life and inflammation of patients with chronic obstructive pulmonary disease. www.ensaiosclinicos.gov.br/rg/RBR‐3zmh3r/ (first received 7 March 2018).
UMIN000027190 {published data only}
- UMIN000027190. The effect of the combination treatment with tiotropium and olodaterol compared to tiotropium on symptoms, respiratory functions and physical activity in maintenance naive Japanese patient with COPD. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000031159 (first received 29 April 2017).
UMIN000031173 {published data only}
- UMIN000031173. Combined effect of progressive resistance training and physical activity counseling in patients with chronic obstructive pulmonary disease: a randomized controlled crossover study. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000035589 (first received 26 February 2018).
UMIN000033093 {published data only}
- UMIN000033093. The effect of comprehensive respiratory rehabilitation using cloud system on exacerbation of patients with chronic obstructive pulmonary disease at home. upload.umin.ac.jp/cgi‐open‐bin/ctr_e/ctr_view.cgi?recptno=R000037694 (first received 1 July 2018).
Zanaboni 2016 {published data only}
- Zanaboni P, Dinesen B, Hjalmarsen A, Hoaas H, Holland AE, Oliveira CC, et al. Long‐term integrated telerehabilitation of COPD patients: A multicentre randomised controlled trial (iTrain) [protocol]. BMC Pulmonary Medicine 2016;16(1):126. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Adeloye 2015
- Adeloye D, Chua S, Lee C, Basquill C, Papana A, Theodoratou E, et al. Global and regional estimates of COPD prevalence: systematic review and meta‐analysis. Journal of Global Health 2015;5(2):020415. [DOI] [PMC free article] [PubMed] [Google Scholar]
Alahmari 2015
- Alahmari AD, Mackay AJ, Patel AR, Kowlessar BS, Singh R, Brill SE, et al. Influence of weather and atmospheric pollution on physical activity in patients with COPD. Respiratory Research 2015;16:71. [DOI] [PMC free article] [PubMed] [Google Scholar]
Andersson 2015
- Andersson M, Stridsman C, Ronmark E, Lindberg A, Emtner M. Physical activity and fatigue in chronic obstructive pulmonary disease ‐ a population based study. Respiratory Medicine 2015;109(8):1048‐57. [DOI] [PubMed] [Google Scholar]
Anton 2016
- Anton A, Ratarasarn K. Pulmonary function testing and role of pulmonary rehabilitation in the elderly population with pulmonary diseases. Current Geriatric Reports 2016;5(2):117‐23. [Google Scholar]
Arne 2009
- Arne M, Janson C, Janson S, Boman G, Lindqvist U, Berne C, et al. Physical activity and quality of life in subjects with chronic obstructive pulmonary disease compared with rheumatoid arthritis and diabetes mellitus. Scandinavian Journal of Primary Health Care 2009;27(3):141‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Casperson 1985
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health‐related research. Public Health Reports 1985;100(2):126‐31. [PMC free article] [PubMed] [Google Scholar]
Choudhury 2014
- Choudhury G, Rabinovich R, MacNee W. Comorbidities and systemic effects of chronic obstructive pulmonary disease. Clinics in Chest Medicine 2014;35(1):101‐30. [DOI] [PubMed] [Google Scholar]
Deeks 2017
- Deeks JJ, Higgins JP, Altman DG, editor(s) on behalf of the Cochrane Statistical Methods Group. Chapter 9: Analysing data and undertaking metaanalyses. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Dhillon 2015
- Dhillon SS, Sima CA, Kirkham AR, Syed N, Camp PG. Physical activity measurement accuracy in individuals with chronic lung disease: a systematic review with meta‐analysis of method comparison studies. Archives of Physical Medicine and Rehabilitation 2015;96(11):2079‐88.e.10. [DOI] [PubMed] [Google Scholar]
Esteban 2010
- Esteban C, Quintana JM, Aburto M, Moraza J, Equrrola M, Pérez‐Izquierdo J, et al. Impact of changes in physical activity on health‐related quality of life among patients with COPD. European Respiratory Journal 2010;36(2):292‐300. [DOI] [PubMed] [Google Scholar]
Esteban 2014
- Esteban C, Arostequi I, Aburto M, Moraza J, Quintana JM, Aispiri S, et al. Influence of changes in physical activity on frequency of hospitalization in chronic obstructive pulmonary disease. Respirology 2014;19(3):330‐8. [DOI] [PubMed] [Google Scholar]
Fastenau 2013
- Fastenau A, Schayck OC, Gosselink R, Aretz KC, Muris JW. Discrepancy between functional exercise capacity and daily physical activity: a cross‐sectional study in patients with mild to moderate COPD. Primary Care Respiratory Journal 2013;22(4):425‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Furlanetto 2010
- Furlanetto KC, Bisca GW, Oldemberg N, Sant'Anna TJ, Morakami FK, Camillo CA, et al. Step counting and energy expenditure estimation in patients with chronic obstructive pulmonary disease and healthy elderly: accuracy of 2 motion sensors. Archives of Physical Medicine and Rehabilitation 2010;91(2):261‐7. [DOI] [PubMed] [Google Scholar]
Furlanetto 2014
- Furlanetto KC, Mantoani LC, Bisca G, Morita AA, Zabatiero J, Proença M, et al. Reduction of physical activity in daily life and its determinants in smokers without airflow obstruction. Respirology 2014;19(3):69‐75. [DOI] [PubMed] [Google Scholar]
Gagnon 2015
- Gagnon P, Casaburi R, Saey D, Porszasz J, Provencher S, Milot J, et al. Cluster analysis in patients with GOLD 1 chronic obstructive pulmonary disease. PLOS One 2015;10(4):e012362. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garcia‐Aymerich 2006
- Garcia‐Aymerich J, Lange P, Benet M, Schohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax 2006;61(9):772‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garcia‐Rio 2012
- Garcia‐Rio F, Rojo B, Casitas R, Lores V, Madero R, Romero D, et al. Prognostic value of the objective measurement of daily physical activity in patients with COPD. Chest 2012;142(2):338‐46. [DOI] [PubMed] [Google Scholar]
Gimeno‐Santos 2011
- Gimeno‐Santos E, Frei A, Dobbels F, Rüdell K, Puhan MA, Garcia‐Aymerich J, et al. Validity of instruments to measure physical activity may be questionable due to a lack of conceptual frameworks: a systematic review. Health and Quality of Life Outcomes 2011;9:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
GOLD 2019
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD 2019. goldcopd.org/ (accessed 7 August 2019).
GRADEpro GDT 2014 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 29 September 2016. Hamilton (ON): McMaster University (developed by Evidence Prime), 2014.
Higgins 2017
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Hill 2013
- Hill K, Vogiatzis I, Burtin C. The importance of components of pulmonary rehabilitation, other than exercise training, in COPD. European Respiratory Review 2013;22(129):405‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Iwakura 2016
- Iwakura M, Okura K, Shibata K, Kawagoshi A, Sugawara K, Takahashi H, et al. Relationship between balance and physical activity measured by an activity monitor in elderly COPD patients. International Journal of Chronic Obstructive Pulmonary Disease 2016;11:1505‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Johnson‐Warrington 2014
- Johnson‐Warrington V, Harrison S, Mitchell K, Steiner M, Morgan M, Singh S. Exercise capacity and physical activity in patients with COPD and healthy subjects classified as Medical Research Council dyspnoea scale grade 2. Journal of Cardiopulmonary Rehabilitation and Prevention 2014;34(2):150‐4. [DOI] [PubMed] [Google Scholar]
Lahham 2016
- Lahham A, McDonald CF, Holland AE. Exercise training alone or with the addition of activity counseling improves physical activity levels in COPD: a systematic review and meta‐analysis of randomized controlled trials. International Journal of COPD 2016;11:3121‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Langer 2016
- Langer D, Demeyer H. Interventions to modify physical activity in patients with COPD: where do we go from here?. European Respiratory Journal 2016;48(1):14‐7. [DOI] [PubMed] [Google Scholar]
Lee 2012
- Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non‐communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380(9838):219‐29. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lee 2015
- Lee JA, Laurson KR. Validity of the SenseWear armband step count measure during controlled and free‐living conditions. Journal of Exercise Science and Fitness 2015;13(1):16‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org. The Cochrane Collaboration.
Mantoani 2016
- Mantoani LC, Rubio N, McKinstry B, Macnee W, Rabinovich PA. Interventions to modify physical activity in patients with COPD: a systematic review. European Respiratory Journal 2016;48(1):69‐81. [DOI] [PubMed] [Google Scholar]
Marcus 2006
- Marcus BH, Williams DM, Dubbert PM, Sallis JF, King AC, Yancey AK, et al. Physical activity intervention studies: what we know and what we need to know. A scientific statement from the American Heart Association Council on Nutrition, Physical Activity and Metabolism. Circulation 2006;114(24):2739‐52. [DOI] [PubMed] [Google Scholar]
McCarthy 2015
- McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2015, Issue 2. [DOI: 10.1002/14651858.CD003793.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Michie 2013
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy of 93 hierarchically clustered techniques: building an international consensus for the reporting of behaviour change interventions. Annals of Behavioral Medicine 2013;46(1):81‐95. [DOI] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman D, PRISMA Group. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. PLOS Medicine 2009;6(7):e1000097. [DOI: 10.1371/journal.pmed.1000097] [DOI] [PMC free article] [PubMed] [Google Scholar]
Nasis 2015
- Nasis I, Kortianou E, Vasilopoulou Μ, Spetsioti S, Louvaris Z, Kaltsakas G, et al. Hemodynamic effects of high intensity interval training in COPD patients exhibiting exercise‐induced dynamic hyperinflation. Respiratory Physiology and Neurobiology 2015;217:8‐16. [DOI] [PubMed] [Google Scholar]
O’Donnell 2014
- O’Donnell DE, Laveneziana P, Webb K, Neder JA. Chronic obstructive pulmonary disease: clinical integrative physiology. Clinics in Chest Medicine 2014;35(1):51‐69. [DOI] [PubMed] [Google Scholar]
Pitta 2005
- Pitta F, Troosters T, Spruit M, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 2005;171(9):972‐7. [DOI] [PubMed] [Google Scholar]
Pitta 2006a
- Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Physical activity and hospitalisation for exacerbation of COPD. Chest 2006;129(3):536‐44. [DOI] [PubMed] [Google Scholar]
Pitta 2006b
- Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Quantifying physical activity in daily life with questionnaires and motion sensors in COPD. European Respiratory Journal 2006;27(5):1040‐55. [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schünemann 2017
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, Akl E, Guyatt GH on behalf of the Cochrane Applicability and Recommendations Methods Group. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Shrikrishna 2012
- Shrikrishna D, Patel M, Tabber RJ, Seymour JM, Connolly BA, Puthucheary ZA, et al. Quadriceps wasting and physical inactivity in patients with COPD. European Respiratory Journal 2012;40(5):1115‐22. [DOI] [PubMed] [Google Scholar]
Singh 2016
- Singh S. One step at a time: lifestyle physical activity interventions. Annals of the American Thoracic Society 2016;13(5):586‐7. [DOI] [PubMed] [Google Scholar]
Trost 2002
- Trost SG, Owen N, Cauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Medicine and Science in Sports and Exercise 2002;34(12):1996‐2001. [DOI] [PubMed] [Google Scholar]
U.S. Department of Health and Human Services 2018
- U.S. Department of Health and Human Services. Physical activity guidelines for Americans, 2nd edition. Washington, DC 2018.
UN 2015
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects. Key findings & advance tables. 2015 revision. population.un.org/wpp/Publications/Files/WPP2015_DataBooklet.pdf (accessed 31 March 2020).
Vaes 2014
- Vaes AW, Garcia‐Aymerich J, Marott JL, Benet M, Groenen MT, Schnohr P, et al. Changes in physical activity and all‐cause mortality in COPD. European Respiratory Journal 2014;44(5):1199‐209. [DOI] [PubMed] [Google Scholar]
Van Remoortel 2013
- Remoortel H, Hornikx M, Demeyer H, Langer D, Burtin C, Decramer M, et al. Daily physical activity in subjects with newly diagnosed COPD. Thorax 2013;68(10):962‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Van Remoortel 2014
- Remoortel H, Hornikx M, Langer D, Burtin C, Everaerts S, Verhamme P, et al. Risk factors and comorbidities in the preclinical stage of chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 2014;189(1):30‐8. [DOI] [PubMed] [Google Scholar]
Vorrink 2011
- Vorrink SN, Kort HS, Troosters T, Lammers JW. Level of daily physical activity in individuals with COPD compared to healthy controls. Respiratory Research 2011;12:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
Waschki 2011
- Waschki B, Kirsten A, Holz O, Mueller KC, Meyer T, Watz H, et al. Physical activity is the strongest predictor of all‐cause mortality in patients with COPD: a prospective cohort study. Chest 2011;140(2):331‐42. [DOI] [PubMed] [Google Scholar]
Waschki 2015
- Waschki B, Kirsten A, Holz O, Mueller KC, Schaper M, Sack AL, et al. Disease progression and changes in physical activity in patients with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 2015;192(3):295‐306. [DOI] [PubMed] [Google Scholar]
Watz 2009
- Watz H, Waschki B, Meyer T, Magnussen H. Physical activity in patient with COPD. European Respiratory Journal 2009;33(2):262‐72. [DOI] [PubMed] [Google Scholar]
Watz 2014a
- Watz H, Pitta F, Rochester CL, Garcia‐Aymerich J, ZuWallack R, Troosters T, et al. An official European Respiratory Society statement on physical activity in COPD. European Respiratory Journal 2014;44(6):1521‐37. [DOI] [PubMed] [Google Scholar]
WHO 2010
- World Health Organization. Global recommendations on physical activity for health. 2010. www.who.int/dietphysicalactivity/publications/9789241599979/en/ (accessed 29 September 2016). [PubMed]
WHO 2017
- World Health Organization. The top 10 causes of death (fact sheet 310). www.who.int/mediacentre/factsheets/fs310/en/ (accessed 30 March 2017).
References to other published versions of this review
Burge 2017
- Burge AT, Cox NS, Abramson MJ, Holland AE. Interventions for promoting physical activity in people with COPD. Cochrane Database of Systematic Reviews 2017, Issue 4. [DOI: 10.1002/14651858.CD012626] [DOI] [PMC free article] [PubMed] [Google Scholar]