

Abstract
Well-known global health priorities (malaria, pneumonia, sepsis, diarrhea, human immunodeficiency virus [HIV], tuberculosis, trauma), although very different threats to an individual’s health, share a common consequence: Development of acute, life-threatening illness. In the developed world, such illness is routinely treated in an intensive care unit (ICU) by highly specialized physicians, nurses and support staff. This model of intensive care is spreading rapidly to low and middle income countries and as it spreads, challenges and limitations to this model arise [1].
Keywords: Critical Illness, Knowledge Translation, Quality Improvement Intervention, Stress Ulcer Prophylaxis, Surgical Safety Checklist
Introduction: Global Burden of Critical Illness
Well-known global health priorities (malaria, pneumonia, sepsis, diarrhea, human immunodeficiency virus [HIV], tuberculosis, trauma), although very different threats to an individual’s health, share a common consequence: Development of acute, life-threatening illness. In the developed world, such illness is routinely treated in an intensive care unit (ICU) by highly specialized physicians, nurses and support staff. This model of intensive care is spreading rapidly to low and middle income countries and as it spreads, challenges and limitations to this model arise [1].
With an estimated $1000–20,000 per quality-adjusted life year (QALY) gained, critical care support for potentially reversible acute medical or surgical illness should be one of the most cost-effective health care interventions [2, 3]. Unfortunately, incomplete knowledge of the best practices by front-line clinicians and delayed, error-prone care delivery processes are ubiquitous threats to patient safety and commonly offset the potential benefits of critical care support. This is particularly important early in the course of critical illness, when errors and delays in appropriate care often lead to costly complications and poor outcomes, even in advanced hospital settings. In resource-poor settings, inadequate human resources and training present additional barriers to safe and effective use of life-saving procedures. Simple interventions, such as early recognition and treatment of cardio-respiratory failure, low tidal volume mechanical ventilation, early appropriate antimicrobial treatment, physical therapy, deep vein thrombosis and stress ulcer prophylaxis, require little specialized equipment but are crucial to successful outcome of critically ill patients [4]. Accordingly, these interventions have to be systematically implemented without omission or delay. This seemingly simple and straightforward task has proven to be an enormous challenge and nothing but a distant dream in hospitals worldwide.
Why are Errors and Complications so Prevalent in Acute Care Settings?
Although medical technologies and knowledge are continuously improving, there is overwhelming evidence of persistent error [5] and poor real-world compliance with evidence-based practices in acute care hospitals [6–8]. Critically ill patients are particularly prone to medical errors because of inherent complexity involving multiple organ systems and the immediacy of the decision-making required. Errors of omission are as common as those of commission with cumulative failures in a multi-step process encumbering exponentially on a patient’s outcome, inevitably leading to development of costly complications (Table 1).
Table 1.
The chance for omission or error increases exponentially with the number of steps in a complex multi-step process emphasizing the need for very high reliability in each step. Adapted from [49] with permission
| Probability of Success for Each Step in the Process | ||||
|---|---|---|---|---|
| Number of Steps | 0.95 | 0.990 | 0.999 | 0.999999 |
| 1 | 0.95 | 0.990 | 0.999 | 0.9999 |
| 25 | 0.28 | 0.78 | 0.98 | 0.998 |
| 50 | 0.08 | 0.61 | 0.95 | 0.995 |
| 100 | 0.006 | 0.37 | 0.90 | 0.990 |
Within the interdisciplinary nature of intensive care, clinicians permanently face multitasking and interruptions. Data overload, meaningless complexity, interruptions, administrative burden, ineffective regulatory requirements, and fragmented provider-based (rather than patient-based) care are some of the most important barriers to error prevention in hospital environments. Care delivery is further impaired by poor communication, inadequate structure, staffing issues and wrong incentives. These errors persist not because physicians and nurses are ignorant, but because the current systems of care make it very difficult to implement the right decisions [9].
The “Checklist Manifesto”: Role of Checklists in Enhancing Patient Safety and Prevention of Medical Error [10]
Studies of human error have identified the key role of cognitive ergonomics and human factors engineering in designing improved care delivery processes and devices [8, 9]. Embracing a safety culture, limiting the number of steps (‘less is more’), enhancing and prompting clear prioritized information, patient- and family-centered care delivery (integration of values, beliefs and advanced directives), improved communication and coordination (hand-offs, physician extenders) are all needed for safe and efficient critical care delivery. Considering the exponential spreading of medical knowledge, it appears obvious that clinician memory cannot store and retrieve all of it, particularly during acute care support [9]. Medical textbooks and current guidelines provided by major scientific societies display exhaustive information for best practice, but may be complex to use as an efficient decision support at the point-of-care [11].
Multiple tools have recently been developed, tested and validated to enhance both efficiency and fidelity of acute care delivery. These include: Multidisciplinary rounds, daily goals of care sheets, smart alarms, dashboards and decision supports. Analogous to the complex industry environment (e. g., aviation, nuclear power plants), simplified checklists and care ‘bundles’ have been recently introduced on a large scale in various medical settings (Table 2) [12, 13].
Table 2.
Representative examples of the use of checklists in various acute care environments
| Settings | Checklist | Author, year [5] | Aim |
|---|---|---|---|
| Operating room | Anesthesia crisis management manual | Runciman, 2005 [36] | 24 specific anesthesia crisis management sub-algorithms |
| Sepsis during anesthesia management checklist | Myburgh, 2005 [50] | Provide a structured approach for the management of sepsis occurring in association with anesthesia | |
| Cesarean delivery anesthesia | Hart, 2005 [51] | Improving anesthesia preparation for caesarean delivery | |
| The WHO surgical safety checklist | Haynes, 2009 [52] | Address key safety steps during perioperative care to reduce rates of death and complications | |
| SURPASS checklist | De Vries, 2009 [53] | SURgical Patient Safety System: Address surgical errors and adverse events during daily clinical practice, from admission to discharge | |
| Obstetric safe surgery checklist | Rao, 2010 [54] | WHO surgical safety checklist adapted to obstetric specificities | |
| Operating room crisis checklists | Ziewacz, 2011 [55] | Improving care during 12 of the most common operating room crises | |
| Surgical safety | Bliss, 2012 [56] | Implementation of comprehensive surgical checklist | |
| Intensive care unit | Diagnosis of brain death | Young, 1991 [57] | Proper assessment and documentation to the declaration of brain death |
| Intensive care delirium screening checklist | Bergeron, 2001 [58] | Quickly identify delirious patient, with earlier diagnosis, earlier intervention and better care | |
| Improving communication in the ICU | Pronovost, 2003 [15] | Daily goals implementation improve understanding of goals of care and overall patient outcomes | |
| Room opening checklist | Quinio, 2003 [59] | Improve adequacy of room’s equipment endowment | |
| Weaning from mechanical ventilation in intensive care patients | Walsh, 2004 [60] | Checklist of metabolic, cardiorespiratory and neurological criteria that suggested that patients should start the weaning process (successful weaning from ventilator prediction) | |
| Catheter-related bloodstream infection (CR-BSI) multifaceted interventions | Berenholtz, 2004 [61] | Eliminate CR-BSIs with staff education, procedure cart, catheter removal daily prompting, evidence-based guidelines checklist | |
| Improving care for the ventilated patient | Berenholtz, 2004 [62] | Daily rounding checklist to improve mechanically ventilated patient outcome | |
| Withdrawal of life support (WOLS) standardized process | Hall, 2004 [63] | Improve conduct of end-of-life care | |
| Catheter-related bloodstream infections | Pronovost, 2006 [12] | Evidence-based intervention to reduce the incidence of infection |
Table 2.
Continuation
| Settings | Checklist | Author, year [5] | Aim |
|---|---|---|---|
| Intensive care unit | Daily quality rounding checklist | DuBose, 2008 [21] | Increase compliance to prophylactic measures relative to main ICU complications |
| Improving compliance to protocols and objectives in ICU | Byrnes, 2009 [20] | Mandatory verbal review of checklist to improve consideration and implementation of ICU best practices | |
| Checklist for lung injury prevention (CLIP) | Lee, 2012 [64] | Improving early recognition and utilization of good practices for patients at high-risk for ALI/ARDS | |
| Emergency department | Trauma patient pre-transfer checklist | Harahill, 1990 [65] | Checklist to promptly prepare patient for transfer |
| Sepsis treatment checklist | Djogovic, 2012 [66] | Optimize sepsis care in emergency departments | |
| Other acute care settings | Checklists and reminders | Wolff, 2004 [67] | Checklists and reminders in clinical care pathways for inpatients admitted for acute myocardial infarction or stroke (key best practices) |
| WHO patient care checklist: new influenza A (H1N1) | WHO, 2009 [68] | Highlights areas of care for the management of new influenza A (H1N1) |
Worldwide implementation of a relatively simple World Health Organization (WHO) surgical safety checklist led to improved outcomes across three continents [14]. Protocolized procedure bundles have similarly lead to the dramatic reduction in vascular device complications across multiple institutions [12]. The introduction of “goals of care sheet” [15] and checklist prompting during daily rounds [16] have both led to substantial improvements in efficiency and reliability of daily plan of care, and were associated with decreased complications.
In order to be helpful at the point-of-care, checklists and algorithms need to focus on brief prioritized information [17, 18]. Checklist effectiveness also relies on an appropriate display [19] and depends on the integration of the tool into bedside practice. This is often achieved using verbal prompting by the team leader or another designated clinician [20, 21]. Standardized processes spur teams to interact and communicate to find the best strategy in ensuring compliance with each care component [22].
‘Golden Hours’: The Importance of Error-free Care Early in the Course of Acute Critical Illness
The burden of medical error, omission and waste are especially exacerbated during the early course of critical illness when timely and efficient intervention are of paramount importance for patient outcome. The consequences of inadequate care delivery at the onset of acute critical illness are elegantly summarized in the words of one of the fathers of critical care support, the late Peter Safar: “The most sophisticated intensive care becomes unnecessarily expensive terminal care …” [23].
This intuitive concept, renowned as the ‘Golden Hour’, has informed trauma care since the second half of the 20th century [24, 25], but has yet to be widely adopted in most other critical care conditions. The non-linear trajectory and time-sensitive nature of acute critical illness is characteristic of the complex systems [26]. During the vulnerable period immediately prior to ‘phase transition’, seemingly minor errors, omissions or delays can profoundly alter the patient trajectory. Simple interventions (fluid bolus, oxygen, transfusion, thrombolytic reperfusion), while beneficial during early hours of critical illness may lose effectiveness or even become harmful later in the course of critical illness (after the ‘phase transition’) [27]. The importance of timely recognition and appropriate treatment of acute critical illness is nicely illustrated in Fig. 1, showing the importance of minute delays in the rapid application of basic critical care support to patients in shock [28]. More recently, a multicenter quality improvement intervention targeting patients with severe sepsis in the emergency department showed that rapid implementation of early bundle elements (i. e., appropriate empiric antimicrobials, fluid bolus, lactate) was associated with aborted progression of organ failures making the patients “ineligible” for subsequent bundle elements (inotropes, steroids, transfusions, low tidal volume ventilation for ARDS) [29].
Fig. 1.


Golden hours: Importance of minor delays in applying rapid interventions to acutely ill patients in shock. From [28] with permission
Regardless of how advanced hospital settings are, expected advantages of critical care support will be impaired if front-line clinicians fail to apply best practices in a timely manner. Therefore, avoiding diagnostic errors and therapeutic delays during these first minutes and hours of the care process (‘golden hours’) is necessary to prevent costly complications, preventable death and disability [16, 30].
Despite the notion of the importance of ‘golden hours, Table 2 shows that the most acute care checklists are concerned with day-to-day care and procedure management. The critical, early period that often occurs outside of the ICU (in the emergency department, hospital ward or recovery room) is largely ignored and checklist use anecdotal. This gap is particularly deep in non-surgical settings where checklists and algorithms generally do not address early recognition and treatment of acute illness, apart from cardiopulmonary resuscitation (CPR) [31], which is often too late!
Structured Approach to Early Recognition and Treatment of Acute Critical Illness
The traditional linear approach, from history and examination to diagnosis and treatment, too often leads to delays in appropriate care and an alternative, iterative approach of addressing life-threatening physiologic disturbances and reviewing the response concurrently with the identification and treatment of underlying condition has been recommended (Fig. 2) [32, 33].
Fig. 2.
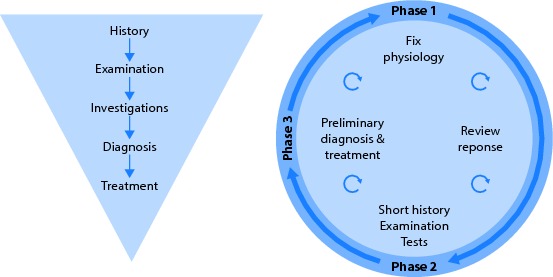

Contrasting linear vs. iterative approach to initial management of acutely ill patients, adapted from the ESICM PACT module on Clinical Examination [32]
Accurate diagnosis is often elusive during the early stages of critical illness in which vastly different underlying conditions may trigger similar and/or interrelated physiologic disturbances leading to a limited number of acute presentations (Box 1) [34]. The timely and appropriate management of these key presentations followed by syndromic diagnoses (shock, respiratory failure, increased intracranial pressure, acute coronary syndrome, etc.), often without full understanding of the underlying condition, constitutes the basics of the acute care of critically ill patients. Keeping in mind the challenges clinicians are facing during early stages of acute critical illness, and the fact that experienced specialist help is often delayed, it is not difficult to imagine the advantages of a systematic and disciplined method that can consistently combine and articulate key diagnostic and therapeutic interventions [35]. Of note, even experienced clinicians are prone to making basic errors during emergency situations exposing patients to harm and clinicians to litigation [36].
Box 1: Common Presentations of Life-threatening Conditions
Shortness of breath
Hypotension
Chest pain
Arrhythmia
Altered mental state
Abdominal pain
Sepsis
Gastrointestinal bleeding
Trauma
Intoxication/overdose
Postoperative
One of the first examples to the systematic and standardized approach to life-threatening illness is the development of the mnemonic ‘ABC’ by the late Dr. Safar and colleagues in the early 1960 s in order to standardize the immediate care of patients with cardiac arrest [37]. In the 1970 s, Dr. Styner extended the context of the initial ABC approach for the evaluation of critically injured trauma patients and formed the basis of the Advanced Trauma Life Support courses [38]. The ABCDE approach has been implemented into trauma settings successfully for many years. Box 2 provides an example of the ABCDE checklist suitable for various acute care environments.
Box 2: Example of an ABCDE checklist
| A |
Airway compromise Stridor Wheezing |
| B |
Poor air entry Crackles Work of breathing |
| C |
1EKG monitor Weak pulse Mottling |
| D |
2AVPU Seizure Focal deficit |
| E |
Abdominal distension Bleeding 3Skin |
1 Sinus, bradycardia, supraventricular tachycardia, ventricular tachycardia, ventricular fibrillation, ST changes
2 Alert, verbal responsive, pain responsive, unresponsive
3 Edema, rash, jaundice, wound
The advantage of the structured approach to life-threatening emergencies has been elegantly demonstrated in a recent study [18]. In this study, the use of checklists by operating room teams markedly decreased critical omissions (23 % vs. 6 %, p < 0.001) in a high fidelity simulation of 106 surgical crises scenarios. Unfortunately, apart from CPR, which is too late, a similar checklist approach is largely missing during golden hours outside operating room and trauma settings [36].
Figure 3 outlines the key elements of a structured approach to acute life-threatening illness or injury: Primary survey to address immediate life-threats (need for CPR, ABCDE bundle) followed by secondary survey to assess each organ system, identify relevant syndromes and, in parallel, initiate emergent therapies.
Fig. 3.


Outline of the structured approach to early recognition and treatment of acute illness. ABG: arterial blood gases; CBC: complete blood count; COPD: chronic obstructive pulmonary disease; CPR: cardiopulmonary resuscitation; CT: computed tomography; DNR: do-not-resuscitate; ECG: electrocardiography; HR: heart rate; ICU: intensive care unit; RR: respiratory rate; SpO2: peripheral oxygen saturation; Temp: body temperature; UOP: urine output; US: ultrasound
Emerging Technologies: Information Displays, Cloud Computing and Mobile Devices
The advances in information technology, medical informatics and human factors engineering, have provided a tremendous opportunity for the development of novel and user-friendly checklists and decision support tools that can be widely applied in a complex and busy acute care settings [9]. To be successful, these applications need to reduce information overload and the potential for error, facilitate adherence to practice guidelines and enable clear communication and collaborative decision making between all members of health care team, patients and families. To facilitate high quality, high value health care behaviors, information display and functionality need to be designed using cognitive ergonomic principles and integrated into the clinician workflow in a manner that facilitates, rather than disrupts, care delivery.
Two years of provider surveys and field observation in medical and surgical ICUs of the Mayo Clinic have provided a robust framework for the prioritization of high value data for the management of critically ill patients [39]. The investigators identified no more than 50 data points that are commonly used by ICU experts. These 50 data points are prioritized on the novel user interface depending on the task at hand [40]. Knowledge translation is facilitated by smart alerts and real time access to evidence-based checklists. Collaborative workspace provides a shared view of the plan of care with patient specific tasks, status checks and reminders enabling the clear communication of the goals of care and their status to all members of the multidisciplinary team including the patient and family. Availability of key patient, process and outcome data in an electronic format provides easy access to scheduled and on demand reports of quality metrics and outcomes.
Using real-time data feeds and standardized patient care tasks in a simulated acute care environment, this novel interface was shown to have a significant advantage over the conventional electronic medical record in reducing provider cognitive load and errors [41]. Direct comparisons between electronic and paper checklists have not been done. Despite the potential pitfalls (need for additional training, reliable hardware, software and network) electronic checklists and decision supports offer some compelling advantages including, but not limited to, global access using mobile computing devices, standardized updates based on new knowledge and wide user feedback, versatile display capabilities (hyperlinks, videos and animations) which facilitate the processing of vast patient information and medical knowledge. In addition electronic tools obviate the need for paper products and its transport, thereby reducing associated cost and pollution.
Rapidly increasing access to mobile phones and cellular networks even in remote and resource-poor settings have recently enabled previously unimaginable, successful quality improvement interventions in rural Africa [42]. Cloud computing technology is also evolving swiftly, providing easy shared access to information with an almost unlimited/scalable storage capability increasing the ability for widespread knowledge translation. Using the approach outlined above and inspired by a surgical crisis checklist [17, 18], a multidisciplinary, international team of acute care clinicians is testing the effectiveness of electronic decision support (CERTAIN – Checklist for Early Recognition and Treatment of Acute Illness) in critical care environments across Eastern Europe, Asia, Africa and Central America [43, 44].
Implementing Checklists at the Bedside of Acutely Ill Patients
Regardless of the format (paper vs. electronic), checklist implementation often encounters cultural barriers, particularly among physicians. Perceptions on limitation of autonomous judgment, checklist dependency and questioning someone’s seniority, knowledge and skill pose significant challenges to the implementation process [45]. Clinicians are often worried about over-standardized care processes ignoring the critical illness complexity (‘cookbook medicine’). But despite these challenges, the checklist approach provides a framework to ensure the best care and a guardrail to avoid errors and omissions during diagnostic and therapeutic courses. Rather than replacing the bedside clinician, these tools are designed to help structure his/her reasoning (focus, precision, reminder, lucidity) and action in spite of facing fatigue and stressful conditions [46].
Assessing the information needs at the point of care is a key prerequisite for designing improved care delivery processes and devices that can fit in clinician workflow. PDSA (Plan-Do-Study-Act) cycles of field observation, surveys, interviews, workflow observations are necessary in order to meet the needs of frontline clinicians. Beta testing and validation of such tools in a simulated environment is essential before implementing them into clinical practice. Similar to any quality improvement projects, the checklist should be reviewed, refined and updated regularly. Senior leadership support is essential to overcome political barriers to the patient-centered (as opposed to the provider-centered) checklist processes. “The model for improvement” [47] is a powerful framework used by many health care organizations to accelerate the improvement of health care processes and outcomes [13, 48].
Conclusions
To fully realize the anticipated patient benefit while treating acute critical illness, clinicians ought to embrace systematic reasoning and a reliable approach to promote early recognition and ensure timely and appropriate treatment. In the current system, much of the effort in critical care is reactionary rather than proactive in implementing best practices aimed at preventing complications. A structured, reliable and error-free approach to the management of acutely ill or injured patients during the early, most vulnerable period is facilitated by point-of-care checklists and algorithms containing brief prioritized information. This approach is rapidly spreading in trauma and operating room settings and other acute care environments should follow soon.
Contributor Information
Jean-Louis Vincent, Email: jlvincen@ulb.ac.be
O. Gajic, Email: gajic.ognjen@mayo.edu
References
- 1.Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet. 2010;376:1339–1346. doi: 10.1016/S0140-6736(10)60446-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Barie PS, Ho VP. The value of critical care. Surg Clin North Am. 2012;92:1445–1462. doi: 10.1016/j.suc.2012.09.001. [DOI] [PubMed] [Google Scholar]
- 3.Linko R, Suojaranta-Ylinen R, Karlsson S, Ruokonen E, Varpula T, Pettila V. One-year mortality, quality of life and predicted life-time cost-utility in critically ill patients with acute respiratory failure. Crit Care. 2010;14:R60. doi: 10.1186/cc8957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. [DOI] [PubMed] [Google Scholar]
- 5.Kohn LT, Corrigan JM, Donaldson MS. To Err is Human : Building a Safer Health System. Washington: National Academy Press; 2000. [PubMed] [Google Scholar]
- 6.Pronovost PJ, Berenholtz SM, Ngo K, et al. Developing and pilot testing quality indicators in the intensive care unit. J Crit Care. 2003;18:145–155. doi: 10.1016/j.jcrc.2003.08.003. [DOI] [PubMed] [Google Scholar]
- 7.Ilan R, Fowler RA, Geerts R, Pinto R, Sibbald WJ, Martin CM. Knowledge translation in critical care: factors associated with prescription of commonly recommended best practices for critically ill patients. Crit Care Med. 2007;35:1696–1702. doi: 10.1097/01.CCM.0000269041.05527.80. [DOI] [PubMed] [Google Scholar]
- 8.Moreno RP, Rhodes A, Donchin Y. Patient safety in intensive care medicine: the Declaration of Vienna. Intensive Care Med. 2009;35:1667–1672. doi: 10.1007/s00134-009-1621-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pickering BW, Litell JM, Herasevich V, Gajic O. Clinical review: the hospital of the future – building intelligent environments to facilitate safe and effective acute care delivery. Crit Care. 2012;16:220. doi: 10.1186/cc11142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gawande A. The Checklist Manifesto : How To Get Things Right. 1. New York: Metropolitan Books; 2010. [Google Scholar]
- 11.Wyer PC, Rowe BH. Evidence-based reviews and databases: are they worth the effort? Developing evidence summaries for emergency medicine. Acad Emerg Med. 2007;14:960–964. doi: 10.1111/j.1553-2712.2007.tb02373.x. [DOI] [PubMed] [Google Scholar]
- 12.Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355:2725–2732. doi: 10.1056/NEJMoa061115. [DOI] [PubMed] [Google Scholar]
- 13.Gawande AA, Arriaga AF. A simulation-based trial of surgical-crisis checklists. N Engl J Med. 2013;368:1460. doi: 10.1056/NEJMc1213744. [DOI] [PubMed] [Google Scholar]
- 14.Treadwell JR, Lucas S, Tsou AY (2013) Surgical checklists: a systematic review of impacts and implementation. BMJ Qual Saf (in press) [DOI] [PMC free article] [PubMed]
- 15.Pronovost P, Berenholtz S, Dorman T, Lipsett PA, Simmonds T, Haraden C. Improving communication in the ICU using daily goals. J Crit Care. 2003;18:71–75. doi: 10.1053/jcrc.2003.50008. [DOI] [PubMed] [Google Scholar]
- 16.Weiss CH, Moazed F, McEvoy CA, et al. Prompting physicians to address a daily checklist and process of care and clinical outcomes: a single-site study. Am J Respir Crit Care Med. 2011;184:680–686. doi: 10.1164/rccm.201101-0037OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gawande A. The checklist: if something so simple can transform intensive care, what else can it do? New Yorker. 2007;10:86–101. [PubMed] [Google Scholar]
- 18.Arriaga AF, Bader AM, Wong JM, et al. Simulation-based trial of surgical-crisis checklists. N Engl J Med. 2013;368:246–253. doi: 10.1056/NEJMsa1204720. [DOI] [PubMed] [Google Scholar]
- 19.Lee MJ, Gershengorn HB, Dinkels M, et al. Checklist For Lung Injury Prevention (CLIP): A pilot study on implementation across multiple hospitals and multiple clinical areas. San Francisco: American Thoracic Society; 2012. p. A6567. [Google Scholar]
- 20.Byrnes MC, Schuerer DJ, Schallom ME, et al. Implementation of a mandatory checklist of protocols and objectives improves compliance with a wide range of evidence-based intensive care unit practices. Crit Care Med. 2009;37:2775–2781. doi: 10.1097/CCM.0b013e3181a96379. [DOI] [PubMed] [Google Scholar]
- 21.DuBose JJ, Inaba K, Shiflett A, et al. Measurable outcomes of quality improvement in the trauma intensive care unit: the impact of a daily quality rounding checklist. J Trauma. 2008;64:22–29. doi: 10.1097/TA.0b013e318161b0c8. [DOI] [PubMed] [Google Scholar]
- 22.Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt Comm J Qual Patient Saf. 2005;31:243–248. doi: 10.1016/s1553-7250(05)31031-2. [DOI] [PubMed] [Google Scholar]
- 23.Safar P. Critical care medicine – quo vadis? Crit Care Med. 1974;2:1–5. doi: 10.1097/00003246-197401000-00001. [DOI] [PubMed] [Google Scholar]
- 24.Cowley RA. A total emergency medical system for the State of Maryland. Md State Med J. 1975;24:37–45. [PubMed] [Google Scholar]
- 25.Cowley RA. Trauma center. A new concept for the delivery of critical care. J Med Soc N J. 1977;74:979–987. [PubMed] [Google Scholar]
- 26.Dong Y, Chbat NW, Gupta A, Hadzikadic M, Gajic O. Systems modeling and simulation applications for critical care medicine. Ann Intensive Care. 2012;2:18. doi: 10.1186/2110-5820-2-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–1377. doi: 10.1056/NEJMoa010307. [DOI] [PubMed] [Google Scholar]
- 28.Sebat F, Musthafa AA, Johnson D, et al. Effect of a rapid response system for patients in shock on time to treatment and mortality during 5 years. Crit Care Med. 2007;35:2568–2575. doi: 10.1097/01.CCM.0000287593.54658.89. [DOI] [PubMed] [Google Scholar]
- 29.Miller RR, 3rd, Dong LNNC, et al. Multicenter implementation of a severe sepsis and septic shock treatment bundle. Am J Respir Crit Care Med. 2013;188:77–82. doi: 10.1164/rccm.201212-2199OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: a model for large scale knowledge translation. BMJ. 2008;337:a1714. doi: 10.1136/bmj.a1714. [DOI] [PubMed] [Google Scholar]
- 31.Nolan JP, Soar J, Zideman DA, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation. 2010;81:1219–1276. doi: 10.1016/j.resuscitation.2010.08.021. [DOI] [PubMed] [Google Scholar]
- 32.McAuley D, Hillman KM, Bion J (2005) Clinical examination. Ramsay G, Hinds C (eds) European Society of Intensive Care Medicine (ESICM) Patient-centered Acute Care Training (PACT) Module.
- 33.Kortbeek JB, Turki ASA, Ali J, et al. Advanced trauma life support, 8th edition, the evidence for change. J Trauma. 2008;64:1638–1650. doi: 10.1097/TA.0b013e3181744b03. [DOI] [PubMed] [Google Scholar]
- 34.Mackenzie R, Sutcliffe RC. Immediate assessment and management of acute medical emergencies. J R Army Med Corps. 2002;148:276–287. doi: 10.1136/jramc-148-03-13. [DOI] [PubMed] [Google Scholar]
- 35.Balas MC, Vasilevskis EE, Burke WJ, et al. Critical care nurses’ role in implementing the “ABCDE bundle” into practice. Crit Care Nurse. 2012;32:35–38. doi: 10.4037/ccn2012229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Runciman WB, Kluger MT, Morris RW, Paix AD, Watterson LM, Webb RK. Crisis management during anaesthesia: the development of an anaesthetic crisis management manual. Qual Saf Health Care. 2005;14:e1. doi: 10.1136/qshc.2002.004101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Safar P, Brown TC, Holtey WJ, Wilder RJ. Ventilation and circulation with closed-chest cardiac massage in man. JAMA. 1961;176:574–576. doi: 10.1001/jama.1961.03040200010003. [DOI] [PubMed] [Google Scholar]
- 38.Styner JK. The birth of advanced trauma life support. J Trauma Nurs. 2006;13:41–44. doi: 10.1097/00043860-200604000-00003. [DOI] [PubMed] [Google Scholar]
- 39.Pickering BW, Gajic O, Ahmed A, Herasevich V, Keegan MT. Data utilization for medical decision making at the time of patient admission to ICU. Crit Care Med. 2013;41:1502–1510. doi: 10.1097/CCM.0b013e318287f0c0. [DOI] [PubMed] [Google Scholar]
- 40.Pickering BW, Herasevich V, Ahmed A, Gajic O. Novel Representation of Clinical Information in the ICU: Developing User Interfaces which Reduce Information Overload. Appl Clin Inform. 2010;1:116–131. doi: 10.4338/ACI-2009-12-CR-0027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ahmed A, Chandra S, Herasevich V, Gajic O, Pickering BW. The effect of two different electronic health record user interfaces on intensive care provider task load, errors of cognition, and performance. Crit Care Med. 2011;39:1626–1634. doi: 10.1097/CCM.0b013e31821858a0. [DOI] [PubMed] [Google Scholar]
- 42.Zurovac D, Sudoi RK, Akhwale WS, et al. The effect of mobile phone text-message reminders on Kenyan health workers’ adherence to malaria treatment guidelines: a cluster randomised trial. Lancet. 2011;378:795–803. doi: 10.1016/S0140-6736(11)60783-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Checklist for early recognition and treatment of acute illness (CERTAIN) official website (2013) Available at http://www.icertain.org. Accessed November 2013
- 44.The iCertain Project (2013) European Society of Critical Care Medicine (ESICM), Minutes of the Global Intensive Care working group meeting, Brussels. Available at http://www.esicm.org/upload/5191ebaf1b026-protokollmeetingbrusselsmarch2013.pdf. Accessed November 2013
- 45.Hales BM, Pronovost PJ. The checklist – a tool for error management and performance improvement. J Crit Care. 2006;21:231–235. doi: 10.1016/j.jcrc.2006.06.002. [DOI] [PubMed] [Google Scholar]
- 46.Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ. 2000;320:745–749. doi: 10.1136/bmj.320.7237.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP. The improvement guide : a practical approach to enhancing organizational performance, 2nd edn. San Francisco, California: Jossey-Bass Publishers; 2009. [Google Scholar]
- 48.Winters BD, Gurses AP, Lehmann H, Sexton JB, Rampersad CJ, Pronovost PJ. Clinical review: checklists – translating evidence into practice. Crit Care. 2009;13:210. doi: 10.1186/cc7792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Botwinick L, Bisognano M, Haraden C. Leadership Guide to Patient Safety. Institute for Healthcare Improvement (IHI) Innovation Series white paper. 2006. [Google Scholar]
- 50.Myburgh JA, Chapman MJ, Szekely SM, Osborne GA. Crisis management during anaesthesia: sepsis. Qual Saf Health Car. 2005;14:e22. doi: 10.1136/qshc.2002.004234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hart EM, Owen H (2005) Errors and omissions in anesthesia: a pilot study using a pilot’s checklist. Anesth Analg 246–250 [DOI] [PubMed]
- 52.Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360:491–499. doi: 10.1056/NEJMsa0810119. [DOI] [PubMed] [Google Scholar]
- 53.de Vries EN, Hollmann MW, Smorenburg SM, Gouma DJ, Boermeester MA. Development and validation of the SURgical PAtient Safety System (SURPASS) checklist. Qual Saf Health Care. 2009;18:121–126. doi: 10.1136/qshc.2008.027524. [DOI] [PubMed] [Google Scholar]
- 54.Rao K, Lucas DN, Robinson PN. Surgical safety checklists in obstetrics. Int J Obstet Anesth. 2010;19:235–236. doi: 10.1016/j.ijoa.2009.09.008. [DOI] [PubMed] [Google Scholar]
- 55.Ziewacz JE, Arriaga AF, Bader AM, et al. Crisis checklists for the operating room: development and pilot testing. J Am Coll Surg. 2011;213:212–217. doi: 10.1016/j.jamcollsurg.2011.04.031. [DOI] [PubMed] [Google Scholar]
- 56.Bliss LA, Ross-Richardson CB, Sanzari LJ, et al. Thirty-day outcomes support implementation of a surgical safety checklist. J Am Coll Surg. 2012;215:766–776. doi: 10.1016/j.jamcollsurg.2012.07.015. [DOI] [PubMed] [Google Scholar]
- 57.Young GB, Frewen T, Barr HW, et al. Checklist for diagnosis of brain death. Can J Neurol Sci. 1991;18:104. doi: 10.1017/s0317167100031395. [DOI] [PubMed] [Google Scholar]
- 58.Bergeron N, Dubois MJ, Dumont M, Dial S, Skrobik Y. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27:859–864. doi: 10.1007/s001340100909. [DOI] [PubMed] [Google Scholar]
- 59.Quinio P, Baczynski S, Dy L, Ferrec G, Catineau J, de Tinténiac A. Evaluation of a medical equipment checklist before intensive care room opening. Ann Fr Anesth Reanim. 2003;22:284–290. doi: 10.1016/S0750-7658(03)00093-5. [DOI] [PubMed] [Google Scholar]
- 60.Walsh TS, Dodds S, McArdle F. Evaluation of simple criteria to predict successful weaning from mechanical ventilation in intensive care patients. Br J Anaesth. 2004;92:793–799. doi: 10.1093/bja/aeh139. [DOI] [PubMed] [Google Scholar]
- 61.Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014–2020. doi: 10.1097/01.CCM.0000142399.70913.2F. [DOI] [PubMed] [Google Scholar]
- 62.Berenholtz SM, Milanovich S, Faircloth A, et al. Improving care for the ventilated patient. Jt Comm J Qual Saf. 2004;30:195–204. doi: 10.1016/s1549-3741(04)30021-3. [DOI] [PubMed] [Google Scholar]
- 63.Hall RI, Rocker GM, Murray D. Simple changes can improve conduct of end-of-life care in the intensive care unit. Can J Anaesth. 2004;51:631–636. doi: 10.1007/BF03018408. [DOI] [PubMed] [Google Scholar]
- 64.Lee MJ, Gershengorn HB, Dinkels M, et al. Checklist for lung injury prevention (CLIP): A pilot study on implementation across multiple hospitals and multiple clinical areas. Am J Respir Crit Care Med. 2012;185:A6567. doi: 10.1164/rccm.201202-0203ED. [DOI] [Google Scholar]
- 65.Harrahill M, Bartkus E. Preparing the trauma patient for transfer. J Emerg Nurs. 1990;16:25–28. [PubMed] [Google Scholar]
- 66.Djogovic D, Green R, Keyes R, et al. Canadian Association of Emergency Physicians sepsis treatment checklist: optimizing sepsis care in Canadian emergency departments. CJEM. 2012;14:36–39. doi: 10.2310/8000.2011.110610. [DOI] [PubMed] [Google Scholar]
- 67.Wolff AM, Taylor SA, McCabe JF. Using checklists and reminders in clinical pathways to improve hospital inpatient care. Med J Aust. 2004;181:428–431. doi: 10.5694/j.1326-5377.2004.tb06366.x. [DOI] [PubMed] [Google Scholar]
- 68.World Health Organization (2009) Patient care checklist. Available at: http://www.who.int/csr/resources/publications/swineflu/ah1n1_checklist.pdf Accessed Nov 2013