

Abstract
This paper introduces a novel survey instrument to identify distinct components of nutrition knowledge and test for links between knowledge and dietary choices in Southern Malawi. Our first aim is to distinguish respondents' familiarity with recommended behaviours, such as when to start breastfeeding or introduce solid foods, from respondents' factual knowledge about mechanisms, such as whether biscuits or papaya and orange fruit or orange Fanta contribute more to future health. We find knowledge of nutrition behaviours to be strongly associated with more schooling, older age, and being female, whereas knowledge of mechanisms is associated only with training and employment as a health professional. We then test whether this expanded definition of nutrition knowledge is associated with dietary intake when controlling for other factors and find no significant links in these data. Results point to the need for knowledge surveys and public health behaviour‐change campaigns to address the kinds of information that might have the most influence on actual behaviour, potentially including the mechanisms involved in food composition, food safety, and disease transmission.
Keywords: Malawi, nutrition knowledge, women's dietary diversity
Key messages.
Existing surveys and programmes often target respondents' knowledge of recommended behaviours, with little attention to their factual knowledge of food composition, food safety, or disease transmission mechanisms that lead to those recommendations.
We pilot a novel survey instrument and find that knowledge of recommended behaviours is higher among wealthier respondents, but knowledge of nutrition mechanisms is higher only among those with formal training and employment as a health professional.
As in previous studies, we find little or no association between surveyed knowledge and nutrition behaviour, pointing to the need for both surveys and programmes to measure and improve the most influential kinds of nutrition knowledge.
1. INTRODUCTION
Despite substantial recent improvements, the prevalence of under‐five stunting in Malawi remains among the highest in the world. The most recent Demographic and Health Survey, conducted in 2015–2016, found a 37% prevalence rate for stunting among children under five, with some districts as high as 45% (National Statistical Office [Malawi] and ICF, 2017). Stunted growth begins in utero and is heavily influenced by mothers' actions, so conditions for women of reproductive age are of critical importance for both her own nutrition outcomes as well as for the health, well‐being, and potential economic and social contributions of future generations (Black et al., 2013; Hoddinott et al., 2013; Özaltin, Hill, & Subramanian, 2010).
Nutrition behaviours and outcomes are affected by numerous factors. In this paper, we focus on the role of nutrition knowledge and the mechanisms through which information and knowledge affect maternal diets. Maternal knowledge and maternal diets are important for the mother herself and also for infant and child health outcomes including birth weight, maternal and infant mortality, linear growth, and other long‐term child outcomes such as obesity and noncommunicable diseases in adulthood (Bhutta et al., 2008; Hoddinott et al., 2013; Prentice et al., 2013; Victora et al., 2008). Several studies have demonstrated socio‐economic factors and women's empowerment to be associated with women's dietary diversity and nutrition outcomes (Amugsi, Lartey, Kimani‐Murage, & Mberu, 2016; Kiboi, Kimiywe, & Chege, 2017; Malapit, Kadiyala, Quisumbing, Cunningham, & Tyagi, 2015; Snapp, Blackie, Gilbert, Bezner‐Kerr, & Kanyama‐Phiri, 2010). Across settings, significant predictors of women's dietary diversity consistently include wealth (assets and land); income (source and control over); household size; female headship; education; and age (Amugsi et al., 2016; Harris‐Fry et al., 2015; Kiboi et al., 2017; Rashid, Smith, & Rahman, 2011; Savy et al., 2008; Shamim et al., 2016; Torheim et al., 2004).
Our concern is with nutrition knowledge and mothers' own dietary diversity, building on studies in developed countries that find mixed evidence on adults' nutrition knowledge and their food consumption (Glewwe, 1999; Khalesi, Sharma, Irwin, & Sun, 2016; Tabbakh & Freeland‐Graves, 2016). Numerous studies link maternal nutrition knowledge and education to child feeding and children's nutrition outcomes (Abbi, Christian, Gujaral, & Gopaldas, 1988; Block, 2007; Boyle et al., 2006; Christiaensen & Alderman, 2004; Ruel, Habicht, Pinstrup‐Andersen, & Gröhn, 1992; Vollmer, Bommer, Krishna, Harttgen, & Subramanian, 2017; Webb & Block, 2004). To the best of our knowledge, there are no studies assessing the role of women's nutrition knowledge on her own dietary diversity or nutritional status in the developing world.
Our research aims to help explain maternal choices in terms of an expanded definition of nutrition knowledge, addressing the large literature on provision and measurement of nutrition information to change behaviour, often combined with support for production activities related to livestock and home gardening (Bhutta et al., 2008; HLPE, 2016). Previous studies relating nutrition knowledge to nutrition behaviours, outcomes, or intermediate indicators in developing country populations focus on respondents' familiarity with core nutrition messaging central to most maternal and child health and nutrition interventions (Karmacharya, Cunningham, Choufani, & Kadiyala, 2017). The conceptual framework for what constitutes nutrition knowledge typically includes nutrition and hygiene behaviours stemming from the Essential Nutrition Actions (Ahmed, 2013; Angeles, Skiles, Weaver, Mussa, & Sheahan, 2015; Daelmans, Dewey, & Arimond, 2008; World Health Organization (WHO), 2013). Such studies do not assess knowledge of the relationships between nutrients, toxins, and health outcomes relevant to undernutrition and food safety in developing countries (Debela, Demmler, Rischke, & Qaim, 2017). In developed countries, the conceptual framework of what constitutes nutrition knowledge follows seminal work by Wardle and Parmenter (Parmenter & Wardle, 1999; Wardle & Parmenter, 2000; Wardle, Parmenter, & Waller, 2000), which includes knowledge domains related to dietary recommendations, sources of nutrients, food choice, and diet–disease relationships (e.g., Williams, Campbell, Abbott, Crawford, & Ball, 2012). Though it includes nutrition literacy and knowledge of important relationships between food choices and health, this framework generally falls short of assessing knowledge of the underlying mechanisms that relate foods to health, which Dickson‐Spillmann and Siegrist (2011) call “declarative knowledge.” Additionally, this literature tends to focus on overnutrition whereas nutrition concerns in developing countries also include undernutrition of all forms, hygiene and care practices, and food safety (Barbosa, Vasconcelos, dos Santos Correia, & Ferreira, 2016).
Our proposed framework expands knowledge beyond familiarity with critical behaviours to include respondents' understanding of underlying mechanisms: how foods contribute to daily energy and health (such as eyesight and resistance to disease); the relationship between germs, clean hands, and disease; and the primary food safety issue of public health concern in the region—aflatoxin contamination (Matumba et al., 2014; Matumba, Monjerezi, Chirwa, Lakudzala, & Mumba, 2009; Monyo et al., 2012; Smith et al., 2015). Our approach is closest to that of Debela et al. (2017), who decompose types of maternal nutrition knowledge into food ingredients, dietary recommendations, and health consequences of not following recommended dietary practices, noting theirs is the first to examine different types of knowledge. To the best of our knowledge, no studies have examined such factual knowledge in the context of undernutrition, food choice in rapidly changing food environments, and issues of food safety in developing country populations. Particularly as processed foods become more readily available to and consumed by poor, rural households, nutrition outcomes will be influenced by the complex ways in which foods, nutrients, and toxins affect health (Black et al., 2013; Ng et al., 2014; Prentice, 2006). As food environments change, consumers may need more knowledge about functional relationships between food and health to guide their choices (Masters et al., 2015).
This study addresses the role of nutrition knowledge in the context of other factors affecting behaviour, notably household wealth and home food production. A broad literature examines the contribution of livestock and home gardening to food consumption and diet quality; findings highlight complex relationships mediated by factors including women's empowerment and access to markets (Hirvonen, Hoddinott, Minten, & Stifel, 2017; Jones, Shrinivas, & Bezner‐Kerr, 2014; Malapit et al., 2015). Regarding gardens, studies across multiple settings consistently find households with gardens more likely to consume fruits and vegetables, though these behaviours do not necessarily translate into nutrition outcomes (Herforth, 2010; Jones, 2016; Jones et al., 2014; Kumar, Harris, & Rawat, 2015; Malapit et al., 2015; Ruel & Alderman, 2013; Ruel, Quisumbing, & Balagamwala, 2018). Despite wide recognition of the potential for livestock keeping to contribute directly to nutrition through increased availability of animal‐source foods (ASFs), literature testing this hypothesis remains sparse (see Azzarri, Zezza, Haile, & Cross, 2015). The few existing studies find some positive associations between livestock keeping and ASFs consumption; however, the results appear to be very animal‐ and context‐specific (Fiorella, Chen, Milner, & Fernald, 2016; Hetherington, Wiethoelter, Negin, & Mor, 2017; Hirvonen et al., 2017; Hirvonen & Hoddinott, 2017; Romeo, Meerman, Demeke, Scognamillo, & Asfaw, 2016).
2. METHODS
2.1. Data and setting
Our data come from a survey of the beneficiaries and implementing partners of the United in Building and Advancing Life Expectations (UBALE) programme, led by Catholic Relief Services in three districts of Southern Malawi. UBALE consists of food transfers and biweekly visits by a community leader (henceforth “leader”) to each beneficiary household (henceforth “household”) to discuss a curriculum covering hygiene and sanitation, breastfeeding, complimentary feeding, and maternal nutrition. Eligible households had a pregnant woman and/or a child under 2 years old. A full questionnaire was collected from 54 leaders and 262 households in June–July 2017, employing a cross‐sectional quantitative survey with a three‐stage cluster sampling design, which randomly selected care groups (groups of community leaders coordinated by a health volunteer), two leaders per group and five households per leader. We sought primary caregivers, and most respondents were female. Dietary diversity was collected for all female respondents (303); 254 households and 49 leaders. The sample size was determined by budget and Catholic Relief Services goals, and the sample is representative of the household and leader population targeted by the Maternal and Child Health and Nutrition arm of the larger UBALE programme.
Basic demographic information and nutrition knowledge were also collected from 44 additional programme delivery actors including 26 health volunteers who coordinate community leaders locally and 18 health professionals who are field and office staff of the implementing organizations. These respondents were purposively selected as those responsible for the randomly selected leaders.
2.2. Measures of nutrition knowledge
Nutrition knowledge was measured by responses regarding knowledge of essential nutrition and hygiene actions (14 questions), food composition and contribution of foods to health (six questions), and knowledge of the nutritional qualities and consequences of mould on grains such as aflatoxins (three questions). Most included questions were based on the Essential Nutrition Actions, and correct responses were coded in adherence with WHO recommendations (Daelmans et al., 2008; WHO, 2013) and also drew from Angeles et al. (2015) and Ahmed (2013) due to their extensive nutrition and nutrition‐related health information and knowledge questions. Food composition questions were developed by the authors and validated by the interviewers; respondents were presented with a photo of two foods and asked which was more likely to contribute to either their energy for work or future health, with a choice between the two foods, that they are the same or “don't know.” Aflatoxin questions were repeated from earlier research among the same population in 2016 (see Data S1 for full instrument). The 23 questions were coded into 42 dichotomous variables (one variable for each correct response where respondents selected all that applied), 33 related to behaviours and 9 related to mechanisms, with a value of one for a correct answer and zero otherwise. Nutrition knowledge index scores are based on the per cent of correct responses given.
Trakman, Forsyth, Hoye, and Belski (2017) suggest that a well‐performing question for a nutrition knowledge questionnaire is one where 20–80% of all respondents answer correctly. We relaxed this recommendation for our analysis and include all questions answered correctly by 10–90% of respondents. Where used as an explanatory variable, we follow Debela et al. (2017), normalizing the per cent correct to the 95th percentile, such that each respondent is given a nutrition knowledge score ranging between 0 and 1, relative to the most knowledgeable respondents (the health professionals). To assess the sensitivity of results to the composition of nutrition knowledge questions, we separate indexes for behaviour and mechanism knowledge questions. We also tested additional measures using all 42 variables, following the most common approach found in the literature (e.g., Barbosa et al., 2016; Block, 2004; Debela et al., 2017; Karmacharya et al., 2017; Kigaru, Loechl, Moleah, & Ndungu, 2016; Mbuya, Menon, Habicht, Pelto, & Ruel, 2013), and also strict adherence to the Trakman et al. (2017) criterion that 20–80% of respondents answer correctly, with no significant differences from the results shown.
2.3. Measures of dietary diversity
In resource poor settings, dietary diversity has been established as a feasible and reliable metric by which to assess the micronutrient adequacy aspect of diet quality (Martin‐Prével et al., 2015). For children, established methods to measure dietary diversity and a validated dichotomous measure of minimum dietary diversity (MDD; associated with consumption of minimally acceptable levels of the key micronutrients of public health concern), have been in use for nearly a decade (Martin‐Prével et al., 2015; WHO, 2008, 2010). A similar measure has more recently been developed for women of reproductive age, MDD–women (MDD‐W), which is compatible with the MDD for children (FAO & FHI 360, 2016; Martin‐Prével et al., 2015).
We employed four measures of women's dietary diversity, stemming from the MDD‐W (FAO and FHI360, 2016; Martin‐Prével et al., 2015). The module elicits yes/no responses to the question “Yesterday during the day or night, did you eat or drink any ” followed by a list of 21 food item categories with common and culturally relevant example foods but does not collect quantities consumed. The indicator has been demonstrated to reflect micronutrient adequacy across 11 micronutrients (FAO and FHI360, 2016; Martin‐Prével et al., 2015). Following the prescribed methodology, the food items were combined into 10 food groups (starchy staples; pulses; nuts and seeds; dairy; meat, poultry and fish; eggs; dark green leafy vegetables; other vitamin‐A rich fruits and vegetables; other vegetables; and other fruits) and a dietary diversity score was given as the total number of food groups consumed.
First, the dietary diversity score is an interval measure of the number of food groups consumed, ranging from zero to 10. Second, meeting MDD adequacy is a dichotomous indicator defined as having consumed five or more food groups the previous day, the adequacy threshold validated as the minimum required to provide adequate micronutrient levels (Martin‐Prével et al., 2015). Because only 21% of respondents reached adequacy, we also relaxed the threshold to four or more (greater than the median) and three or more (the median or greater). There is a large difference in the percentage of respondents consuming more than the median (38%) and those consuming the median or above (74%). Third and fourth, we used any ASFs (flesh foods, eggs, dairy) and any micronutrient‐dense fruits and vegetables (MnD‐FFVs; dark leafy greens, vitamin‐A rich fruits and vegetables), both dichotomously defined as one if consumed, zero otherwise.
2.4. Statistical analysis
Our analysis involves two models; in the first, we include all respondents to estimate the determinants of nutrition knowledge and the second is limited to female household beneficiaries and community leaders to estimate associations between nutrition knowledge and the dietary diversity outcomes defined above. In both models, we control for respondent's education, age, and district. For the first model, we also control for programme role (beneficiary, leader, health volunteer, or health professional) and gender, relative to the baseline responses of a female respondent in a household enrolled in the programme. In the second model, we do not include role or gender but do control for household wealth quintile, based on an asset index (Vyas & Kumaranayake, 2006). Education is years of schooling; age is measured in years. Squared terms of education and age are used to capture non‐linearities in the functional form. As robustness checks, we also tested education quartiles and quintiles. The subpopulation of female households and leaders weights the regression in accordance with the survey design. Because the other implementing actors were purposively selected and therefore have no survey weight, the analysis of the full sample does not account for survey design.
The dietary diversity analysis regresses each of the outcomes on wealth quintile, livestock ownership, garden ownership, respondent education, and respondent age. The main specification uses all knowledge questions responded to correctly by 10–90% of respondents as the knowledge measure. Livestock is measured in tropical livestock units, based on type and number of animals (Chilonda & Otte, 2006). Garden ownership is a dichotomous indicator of having a garden. The additional covariates (wealth, education, age) reflect determinants of women's dietary diversity supported by the literature and are defined as above (Kiboi et al., 2017; Snapp & Fisher, 2014; Torheim et al., 2004).
We treated the dietary diversity score both as count data using a Poisson regression model and then also relaxed the assumption of equivalent distance between food groups and linear functional form using an ordered logit model. The dichotomous outcomes were estimated with logistic regression, and odds ratios are reported. As robustness checks, we also used the alternative measures of nutrition knowledge described above, education quartiles and quintiles, limited the sample to women of reproductive age (15–49), and trimmed livestock ownership to the 99th percentile to exclude extreme outliers. We found the results to be robust to the selection of knowledge measures, treatment of covariates, and sample. In all specifications, standard errors are heteroskedasticity‐robust and clustered at the care group level.
3. RESULTS
3.1. Responses to nutrition knowledge questions by professional role
Table 1 presents the nutrition knowledge questions and per cent answering correctly, by role. Figure 1 shows the distribution of correct responses to behaviour and mechanism knowledge separately. Responses to just one mechanism question underscore the rationale for our expanded conceptual framework. When asked which contributes more to their future health: an orange fruit or an orange Fanta, only 51% of respondents answered correctly, no better than random guessing. Notably, 32% chose Fanta and another 17% selected that they are the same. At the same time, most respondents answered correctly to most of the common questions reflecting familiarity with key nutrition behaviours. At each level of the programme delivery chain (leaders, health volunteers, health professionals), we observed an increasing percentage of correct answers about the underlying mechanisms relating foods to health. This is to be expected given greater education; however, the Pearson's correlation coefficient between education and correct responses to these questions is only 0.35, suggesting formal schooling does not fully explain this factual understanding. No group answers all questions correctly, which is consistent with the need for continuing education particularly on topics such as breastfeeding and handwashing.
Table 1.
Knowledge of recommended behaviours and underlying mechanisms, by knowledge domain
| Topic | Correct response(s) | Per cent correct | ||||
|---|---|---|---|---|---|---|
| All (N = 360) | Households (N = 262) | Leaders (N = 54) | Volunteers (N = 26) | Profes‐sionals (N = 18) | ||
| Panel A: Nutrition behaviours | ||||||
| Infant and young child feeding | ||||||
| Initiate breastfeeding | Immediately or less than 1 hr after delivery | 91 | 89 | 94 | 100 | 100 |
| Give colostrum | Yes | 92 | 90 | 96 | 100 | 100 |
| Breastfeeding frequency | Whenever the baby wants | 9 | 10 | 7 | 8 | 6 |
| When you see the baby is hungry | 7 | 7 | 4 | 12 | 6 | |
| When the baby cries | 6 | 8 | 2 | 0 | 0 | |
| Frequently | 85 | 84 | 96 | 85 | 56 | |
| At least 8 times per day | 1 | 1 | 0 | 0 | 0 | |
| Exclusive breastfeeding to | 6 months | 91 | 88 | 96 | 100 | 100 |
| Introduction of liquids | 6 months | 82 | 82 | 85 | 88 | 67 |
| Introduction of solid foods | 6 months | 66 | 63 | 72 | 81 | 67 |
| Vitamin A supplementation | Twice per year | 30 | 27 | 31 | 31 | 72 |
| For child with diarrhoea: | 8 | 5 | 6 | 12 | 50 | |
| Give solid food | Yes | 1 | 1 | 0 | 4 | 11 |
| Amount | Same as usual | 77 | 74 | 81 | 85 | 89 |
| Give breastmilk | Yes | 77 | 74 | 81 | 85 | 89 |
| Amount | More than usual | 78 | 75 | 83 | 85 | 94 |
| Give other liquids | Yes | 58 | 52 | 72 | 73 | 83 |
| Amounts | More than usual | 99 | 99 | 100 | 100 | 100 |
| Give ORS | Yes | 72 | 66 | 80 | 100 | 94 |
| Give zinc | Yes | 97 | 97 | 100 | 96 | 100 |
| See health prof. | Yes | 91 | 89 | 94 | 100 | 100 |
| Hygiene & Sanitation | ||||||
| Occasions to wash hands | When they look dirtyb | 51 | 42 | 65 | 85 | 89 |
| Before preparing food | 31 | 31 | 31 | 27 | 39 | |
| Before breastfeeding | 45 | 40 | 46 | 77 | 72 | |
| Before eating | 96 | 94 | 100 | 100 | 100 | |
| After using the toilet | 67 | 63 | 70 | 81 | 94 | |
| After changing a diaper | 10 | 10 | 7 | 8 | 11 | |
| After working in the fields or caring for livestock | 13 | 11 | 20 | 4 | 17 | |
| Purpose of using soap in handwashingb | To help me by removing dirt and improving appearance | 76 | 73 | 74 | 96 | 100 |
| Actions to make drinking water safea | Boiling for at least 1 min | 78 | 78 | 81 | 77 | 56 |
| Adding purification tablets/drops | 96 | 95 | 96 | 96 | 100 | |
| During pregnancy | ||||||
| Visits to antenatal clinic | 4–9 | 88 | 89 | 83 | 92 | 67 |
| Food consumption | Eat more food | 78 | 74 | 85 | 92 | 78 |
| Harmful foods | None | 47 | 40 | 52 | 73 | 89 |
| Vitamin supplement | Yes | 82 | 80 | 83 | 81 | 100 |
| Panel B: Underlying mechanisms | ||||||
| Hygiene and sanitation (germ theory of disease) | ||||||
| Purpose of using soap in handwashingb | To help others by preventing transmission of disease | 76 | 73 | 74 | 96 | 100 |
| Food composition (function of nutrients) | ||||||
| More energy for work: | ||||||
| Onion or tomato? | Onion | 2 | 3 | 0 | 0 | 0 |
| Water or milk? | Milk | 45 | 43 | 46 | 38 | 83 |
| Contribution to future health:c | ||||||
| Orange fruit or a Fanta? | Orange | 51 | 45 | 52 | 69 | 100 |
| Nsima (maize meal) or Ndiwo (greens)? | Ndiwo | 36 | 33 | 39 | 23 | 94 |
| Biscuits or papaya? | Papaya | 86 | 85 | 87 | 81 | 100 |
| Food safety (control of contaminants) | ||||||
| Cooking eliminates mould | No | 54 | 53 | 56 | 46 | 72 |
| Animals affected by mould on feed grain | Yes | 48 | 42 | 59 | 65 | 67 |
| Animal source foods affected by mould on animal feed | Yes | 41 | 37 | 44 | 54 | 61 |
Note. Questions listed are in order asked within each domain.
A separate variable was coded for each correct response.
Postcoding generated a variable for at least one of the following: “When they look dirty” as an occasion to wash with soap, “To improve appearance” or “Both” as the reason for handwashing. A second variable was coded for a correct selection of “To prevent transmission of disease” or “Both” as the reason for handwashing.
“Other responses” were postcoded and any response between four and nine times were coded as correct.
Response options included each food, “they are the same,” and “don't know.”
Figure 1.
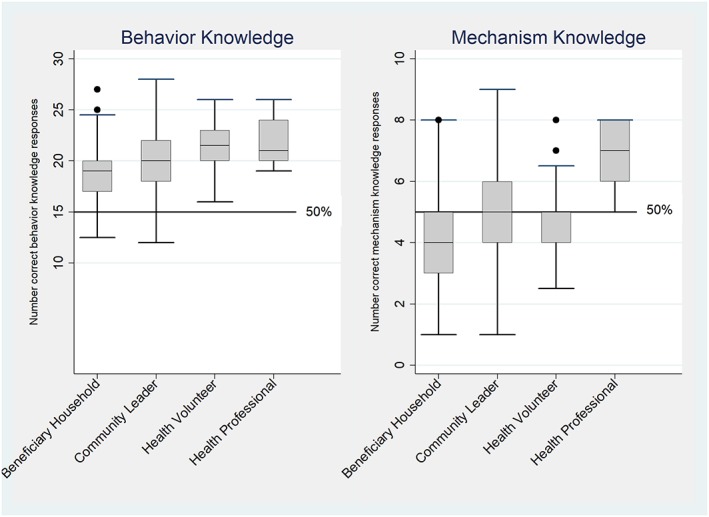
Distribution of behavioural knowledge and mechanism knowledge, by professional role
3.2. Sociodemographic determinants of each nutrition knowledge index
The regression results in Table 2 test for correlations between each index of nutrition knowledge and a variety of sociodemographic factors; Columns 1 and 2 provide results for the respondents with dietary diversity data (weighted by survey design), whereas Columns 3 and 4 include all respondents (unweighted). Most importantly, additional years of schooling is associated with a higher knowledge index for recommended behaviours, but not more knowledge of underlying nutritional mechanisms. A similar pattern is observed for age. Among female household respondents and leaders for whom wealth and dietary diversity data were collected, wealth is also associated with behaviour knowledge; however, the magnitude of this association is small in practical terms with each additional wealth quintile associated with less than 1 percentage point greater knowledge index score. For the full sample, female respondents and respondents who are health volunteers have greater knowledge of recommended nutrition behaviours. None of these are significantly associated with knowledge of nutrition mechanisms, however, as that index is significantly linked only with training and employment as a health professional in Column 4.
Table 2.
Determinants of behavioural knowledge and mechanism knowledge, by professional role
| Female households & leaders | All roles & genders | |||
|---|---|---|---|---|
| Behaviour knowledge | Mechanism knowledge | Behaviour knowledge | Mechanism knowledge | |
| (1) | (2) | (3) | (4) | |
| Wealth quintile | 0.00945 *** (0.00313) | 0.0163 (0.0101) | ||
| Female | 0.0548 *** (0.0187) | 0.00433 (0.0308) | ||
| Education (years) | 0.0171 *** (0.00592) | 0.0104 (0.00767) | 0.00855 * (0.00443) | 0.00696 (0.00861) |
| Education (years) squared | −0.000918 * (0.000535) | −0.000138 (0.000619) | −0.000120 (0.000398) | 0.000297 (0.000716) |
| Age | 0.0127 *** (0.00453) | 0.00195 (0.00791) | 0.00785 *** (0.00262) | 0.00651 (0.00572) |
| Age2 | −0.000160 ** (6.17e‐05) | −3.24e‐05 (0.000124) | −9.15e‐05 *** (3.40e‐05) | −9.16e‐05 (8.53e‐05) |
| Leader | −0.00448 (0.0181) | −0.0164 (0.0301) | 0.00769 (0.0195) | −0.0175 (0.0264) |
| Health volunteer | 0.0517 ** (0.0225) | −0.0128 (0.0429) | ||
| Health professional | 0.0561 (0.0373) | 0.167 *** (0.0624) | ||
| Chikwawa district | −0.00191 (0.0281) | −0.0340 (0.0359) | 0.0133 (0.0167) | −0.0232 (0.0280) |
| Nsanje district | −0.0112 (0.0319) | −0.0249 (0.0327) | −0.00172 (0.0178) | −0.0454 (0.0289) |
| Constant | 0.272*** (0.0882) | 0.362** (0.131) | 0.319*** (0.0575) | 0.334*** (0.107) |
| Observations | 248 | 248 | 359 | 359 |
| R 2 | 0.157 | 0.070 | 0.201 | 0.171 |
Note. Dependent variables are knowledge indexes, defined as per cent answered correctly out of 33 questions about recommended behaviours (such as when to start breastfeeding and when to start feeding solid foods) and 9 questions about functional mechanisms (such as which foods have more healthful nutrients, whether cooking makes food safer, and whether soap affects disease transmission). Wealth is quintiles of an asset index. Education is years of schooling. Age measured in years. The omitted category is respondents with 0–3 years of education residing in Blantyre Rural District. Columns 3 and 4 are unweighted. Heteroskedasticity robust standard errors (clustered at the care group level for Columns 1 and 2) are shown in parentheses, with significance levels denoted.
Bold used to emphasize results discussed in the paper.
P < 0.1.
P < 0.05.
P < 0.01.
The most important result of Table 2 is the difference between the determinants of behavioural knowledge (Columns 1 and 3) and the determinants of mechanistic knowledge (Columns 2 or 4). Answers to factual questions about food composition, food safety, and disease transmission are not significantly associated with wealth, years of schooling, age, or other factors but are associated only with being a health professional. Those individuals score 17 percentage points higher on the mechanism knowledge index than the next lower role category (health volunteers). In contrast, for health behaviours, being a health volunteer is associated with 5 percentage points higher behaviour knowledge score relative to the households or leaders. Our robustness checks found no evidence of heterogeneous effects by wealth or education, and the results were robust to the measures of nutrition knowledge and education used.
Results in Table 2 reveal that mechanism knowledge is higher among health professionals, whereas behaviour knowledge is higher among respondents with higher wealth, education and age, and also among health volunteers. Both types of knowledge could potentially lead respondents to consume healthier diets, which we test in Tables 3 and 4 below. Because all kinds of knowledge could potentially be linked to the quality of maternal decision‐making, we use the broadest possible combined index over all knowledge questions. Each analysis controls for home production of both livestock and garden products, as well as age and education. The analysis begins with 5 dichotomous dietary diversity outcomes in Table 3 and then considers the number of food groups in Table 4.
Table 3.
Determinants of binary dietary diversity outcomes (odds ratios)
| Number of food groups | |||||
|---|---|---|---|---|---|
| 5 or more | 4 or more | 3 or more | Any ASFs | Any MnD‐FFVs | |
| (1) | (2) | (3) | (4) | (5) | |
| Wealth quintile | 1.432 *** (0.169) | 1.341 ** (0.154) | 1.446 *** (0.186) | 1.285 ** (0.120) | 1.267 * (0.149) |
| Knowledge (all) | 1.395 (1.336) | 2.667 (3.372) | 2.338 (3.274) | 0.494 (0.635) | 0.562 (0.688) |
| Livestock | 0.929 (0.151) | 0.959 (0.109) | 1.000 (0.122) | 1.211 (0.177) | 0.943 (0.0708) |
| Garden | 0.414 *** (0.119) | 0.720 (0.251) | 1.362 (0.420) | 0.896 (0.325) | 4.019 *** (1.535) |
| Education (years) | 1.071 (0.0608) | 1.040 (0.0418) | 0.968 (0.0482) | 1.002 (0.0475) | 1.118 ** (0.0510) |
| Age | 1.014 (0.0280) | 0.997 (0.0236) | 0.945 *** (0.0135) | 0.983 (0.0220) | 0.987 (0.0230) |
| District fixed effects | Yes | Yes | Yes | Yes | Yes |
| Observations | 248 | 248 | 248 | 248 | 248 |
| F test | 3.553 | 2.232 | 3.433 | 3.334 | 4.780 |
| Prob > F | 0.0102 | 0.0695 | 0.0120 | 0.0137 | 0.00213 |
Note. Nutrition knowledge index defined as per cent answered correctly (out of all questions, behaviours and mechanisms combined) of the questions that were answered correctly by 10–90% of respondents, normalized to the 95th percentile. Wealth is quintiles of an asset‐based index. Livestock measured in TLUs. Education is years of schooling. Age measured in years. Constant terms not shown. Heteroskedasticity robust standard errors clustered at the care group level shown in parentheses, with significance levels denoted. ASFs: animal‐source foods; MnD‐FFVs: micronutrient‐dense fruits and vegetables; TLUs: tropical livestock units.
Bold used to emphasize results discussed in the paper.
P < 0.1.
P < 0.05.
P < 0.01.
Table 4.
Determinants of number of food groups consumed
| Poisson (beta coefficient) | Ordered logit (odds ratio) | |||||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| Wealth quintile | 0.0687*** (0.0213) | 0.0683*** (0.0203) | 0.0705*** (0.0216) | 1.409*** (0.158) | 1.412*** (0.151) | 1.423*** (0.163) |
| Knowledge (all) | 0.0630 (0.193) | 1.608 (1.639) | ||||
| Knowledge (behaviour) | 0.0848 (0.178) | 1.532 (1.488) | ||||
| Knowledge (mechanisms) | −0.0451 (0.140) | 1.007 (0.759) | ||||
| Livestock | −0.00915 (0.0224) | −0.00919 (0.0225) | −0.00917 (0.0225) | 0.951 (0.0935) | 0.950 (0.0932) | 0.950 (0.0951) |
| Garden | −0.0685 (0.0498) | −0.0666 (0.0508) | −0.0674 (0.0508) | 0.873 (0.218) | 0.882 (0.230) | 0.871 (0.233) |
| Education (years) | 0.00804 (0.00661) | 0.00788 (0.00659) | 0.00916 (0.00642) | 1.043 (0.0335) | 1.044 (0.0337) | 1.048 (0.0324) |
| District fixed effects | Yes | Yes | Yes | Yes | Yes | Yes |
| Observations | 248 | 248 | 248 | 248 | 248 | 248 |
| F test | 3.22 | 3.31 | 2.98 | 2.29 | 2.22 | 2.18 |
| Prob > F | 0.0175 | 0.0156 | 0.0247 | 0.0669 | 0.0747 | 0.0790 |
Note. Nutrition knowledge index defined as per cent answered correctly (out of all questions, behaviour questions or mechanisms questions only) of the questions that were answered correctly by 10–90% of respondents, normalized to the 95th percentile. Wealth is quintiles of an asset‐based index. Livestock measured in TLUs. Education is years of schooling. Age measured in years. Constant terms not shown. Heteroskedasticity robust standard errors clustered at the care group level shown in parentheses, with significance levels denoted. TLUs: tropical livestock units.
P < 0.1.
P < 0.05.
P < 0.01.
3.3. Agricultural and knowledge determinants of maternal diet diversity
As shown in the main specifications (Columns 1, 4 and 5) of Table 3, household wealth is consistently associated with greater odds of consuming a more diverse diet. These results are robust to the presence of covariates, and the magnitude of the wealth effect is economically meaningful as each additional wealth quintile is associated with 1.4 times higher odds of meeting MDD adequacy. Having a garden is associated with four times higher odds of consuming any MnD‐FFV, while at the same time, it is associated with 0.4 times lower odds of meeting MDD adequacy. We also investigated the possibility of heterogeneous effects of nutrition knowledge by levels of the other covariates, available in Data S1. The results were similar across outcome measures, providing suggestive evidence that nutrition knowledge may be more strongly associated with dietary diversity for respondents who are wealthier, older, and have a garden; we did not observe evidence of any heterogeneous effects for the associations with MDD adequacy or MnD‐FFVs.
3.4. Agricultural and knowledge determinants for number of food groups consumed
Table 4 presents the results of the determinants of dietary diversity scores, using both the Poisson and ordered logistic regression models. We again find wealth consistently positively associated with greater dietary diversity. The Poisson regression results in Column 1 are interpreted as a per cent likelihood such that each additional wealth quintile is associated with a 6.7% greater likelihood of consuming the next higher number of food groups, statistically significant at the 1% level. The ordered logit model presents similar results, a one unit increase in wealth quintile is associated with 1.4 times greater the odds of consuming an additional food group, statistically significant at the 1% level. As above, the wealth coefficients were found to be robust to the inclusion of additional covariates, suggesting it is the primary driver among those investigated.
4. DISCUSSION
This paper introduces a new, expanded definition of nutrition knowledge, adding functional questions about nutritional mechanisms to standard questions about nutrition behaviours, and use the resulting data to test whether maternal knowledge of any type is associated with higher maternal diet quality given the respondent's socio‐economic characteristics. We make a novel contribution in two regards: by expanding the conceptual framework of nutrition knowledge to include both familiarity with behaviours and factual understanding of the underlying mechanisms relating foods, toxins, and behaviours to health and disease outcomes and by analysing the associations between nutrition knowledge, home production, and women's dietary diversity. Though different sociodemographic factors are found to be associated with behaviour versus mechanism knowledge, neither are found to be associated with any measures of dietary diversity. Consistent with prior literature, and to be expected, wealth is consistently found to be positively and significantly associated with dietary diversity and consumption of nutrient‐dense foods. We find no association between owning livestock and dietary diversity or the likelihood of consuming ASFs. We do find that owning a garden is positively associated with the likelihood of consuming any MnD‐FFVs but negatively associated with meeting MDD (MDD‐W), underscoring a potential trade‐off for interventions. Finally, we observe that nutrition knowledge may be a more important determinant of dietary diversity for older women and women in households owning fewer livestock.
Our expanded nutrition knowledge survey starts with a set of 23 questions coded into 33 measures of recommended behaviours for maternity care and diets in pregnancy, infant feeding and child diets, and hygiene and sanitation plus adds a set of nine new measures of food composition, food safety, and disease transmission. The new mechanistic questions concern functional relationships that underlie recommended behaviours. Our five new questions about food composition ask respondents to compare equal‐size portions of familiar foods and state which offers more energy for work each day or which contributes more to their future health. Our three new questions about food safety ask respondents, for instance, whether cooking eliminates the potentially harmful effects of mould on food, and our new question about disease transmission asks whether the purpose of using soap in handwashing is just to help oneself or also to help others.
To identify differences in how the two types of knowledge are formed, we compare their determinants and find that knowledge of nutrition behaviours is significantly associated with household wealth, education, age, and working as a health volunteer, but knowledge of nutrition mechanisms is significantly associated only with being trained and employed as a health professional. This suggests that knowledge of even the most basic nutrition mechanisms is not readily learned through primary and secondary education or public health campaigns but is consistently available to health professionals. The consequences of lack of such knowledge could be acute, particularly as rural populations increasingly confront more complex food environments and face food safety risks that are imperceptible to human senses. For instance, public health messaging in Malawi emphasizes eating from all six food groups. A respondent could be familiar with this guidance, have a desire to follow it and adequate resources to do so, but if she does not understand the difference between orange Fanta and a real orange, she may well choose the soda while believing she has consumed a fruit. Similarly, aflatoxin is toxic to human health at levels well below what can be detected by the senses and therefore requires factual understanding of its consequences in order to deliberately avoid exposure (FAO, 2004).
Specific questions from our pilot study clearly illustrate how respondents' factual knowledge about nutrition mechanisms might affect their choices, independently of whether they report knowing various recommended behaviours. Our questions were designed to avoid any need for scientific terminology, by focusing entirely on the functional attributes of foods, cooking, and soap. To measure respondents' understanding of what is in foods, we gave pairs of foods with markedly different composition in terms of dietary energy and essential micronutrients. For calorie content, for example, we asked “Comparing each of these two foods, which one do you think is likely to give you more energy for work each day: A glass of water, a glass of milk, are they the same, or you don't know?” Then, for micronutrient content, we asked “Comparing each of these two foods, which one do you think is likely to contribute more to your future health: An orange fruit, an orange Fanta, are they the same, or you don't know?” In both of those cases, households' and leaders responses were indistinguishable from random guessing: about half got the correct answer, implying that people looking to gain dietary energy or become healthier would not know which to choose. In contrast, 100% of health professionals recognized that future health would benefit more from an orange fruit than an orange Fanta, and 83% of them recognized there would be more energy for work in a glass of milk than a glass of water.
The comparison of fruit versus Fanta provides a benchmark case in which households' and leaders knowledge was as good as guessing, while all health professionals understood the difference. Two other pairs of food offer polar opposite examples, with the same question about contribution to future health asked about similar‐sized portions of biscuits versus papaya, and equal quantities of nsima (cooked maize meal) versus ndiwo (cooked green leafy vegetables). In the first comparison, most people understood that papaya contributes more to future health, with 86% of households and leaders giving the correct answer, whereas 100% of health professionals did so. For a starchy staple versus a green leafy vegetable, however, most households and leaders stated the opposite of the truth; only 36% chose the vegetables. Yet 94% of health professionals did so. Questions regarding food safety and disease transmission provide similar results. When asked “Can cooking a moldy food eliminate any health effects of the mold?” only 54% of villagers gave the correct answer (no), whereas 72% of health professionals did so. And when asked “What is the purpose of using soap when handwashing?” only 76% of households and leaders included “to help others by preventing transmission of disease,” whereas 100% of health professionals did so.
From these comparisons, it is clear that establishing a foundation of factual knowledge about food composition, food safety, and sanitation is a different thing than building familiarity with recommended behaviours. Adding our nine mechanism questions to the 33 behaviour questions provides a broader measure of nutrition knowledge than has previously been available in the literature. Future work will be needed to refine and validate questions for use in a standardized version of this instrument, but to illustrate its applicability, we use our expanded knowledge index to test whether more nutrition knowledge of any kind is associated with higher diet quality of female respondents. Previous studies that focus on maternal knowledge and child feeding practices, generally finding strong linkages between the two. When choosing foods for herself, however, mothers may face very different pressures than when feeding her child.
Like prior literature, we found wealth to be strongly positively associated with all dietary diversity outcomes measured, and conditional on that we found that nutrition knowledge had no additional explanatory power for women's dietary diversity measured in a variety of ways (Gewa & Leslie, 2015; Harris‐Fry et al., 2015; Jones, 2016; Jones et al., 2014). Consistent with prior studies, we observed that having a garden is associated with greater likelihood of consuming MnD‐FFVs, but we found that it is also negatively associated with meeting MDD levels presumably due to the absence of other foods. One explanation for this contrast could be that owning a garden is a symptom of omitted variables that lead households to rely more on their own production, which in turn is associated with lower dietary diversity than households that make more extensive use of markets. That finding presents a potential trade‐off for interventions between targeting the consumption of specific foods important for nutrition, in this case MnD‐FFVs, and promoting an overall diet diverse enough to provide adequate minimum macronutrient and micronutrient quantities.
There are several important implications of our findings. First, the omission of factual knowledge of underlying mechanisms linking foods to health in common measures of nutrition knowledge may fail to explain observed behaviours, particularly in complex food and food safety environments. We find evidence that respondents demonstrating familiarity with nutrition behaviours commonly promoted by maternal and child health interventions do not similarly demonstrate an understanding of the mechanisms through which foods and toxins affect health and that the latter is held more by health professionals than households and community leaders. As poor rural populations confront increasingly complex food environments, behavioural messages are likely to be insufficient to equip individuals with the ability to make nutritious and safe food choices as it is impossible to anticipate each of the possible choice sets likely to be faced and tailor behavioural messages accordingly.
Second, our study highlights a potential trade‐off between increasing consumption of MnD‐FFVs versus improving overall dietary diversity when those with a garden are more likely to consume MnD‐FFVs and less likely to meet MDD adequacy. Gardens require an investment by the household in land, financial resources, and time and could potentially divert resources from other uses that might be more effective in achieving greater diet quality. A better understanding of the potential trade‐offs and opportunity costs for households in constructing and tending gardens would be important to take into consideration in cost–benefit analyses of alternative approaches to improving household nutrition. These forces are also likely mediated by market access, which the present study did not measure.
Third, there may be a disconnect between familiarity with pronutrition behaviours and women's own food consumption. As noted above, there is strong evidence that maternal nutrition knowledge and education impact children's dietary diversity. That we do not observe a similar pattern between nutrition knowledge and women's own dietary diversity is concerning given the importance of maternal health for child outcomes. With no other studies of nutrition knowledge and women's dietary diversity, we cannot compare our results with those found by others, yet if true, there are several plausible explanations for our findings. Our nutrition knowledge measure includes more behaviours specific to children relative to those specific to women, and this imbalance could drive our results. Relatedly, most nutrition interventions contain more child‐specific messages, which could mediate the relationship between a woman's knowledge and her own dietary diversity in multiple ways. Women could fail to draw connections between the information presented for children and her own health, or the emphasis towards children's nutrition could influence prioritizing children's diets over women's diets. The interventions themselves could cause such prioritization or could reinforce existing social norms that bias resources towards children and away from women in the household, or some combination thereof. Finally, the relationship is likely mediated by women's empowerment, which our study did not capture. Even where women have little bargaining power, they may be able to exercise more influence over children's health and diets than their own.
This study provides a first effort to quantify individuals' factual knowledge about nutrition mechanisms, in addition to their knowledge of recommended nutrition behaviours, and test for links between this expanded definition of nutrition knowledge and the respondent's own dietary intake. We find great disparities among respondents in both kinds of knowledge, and wide variation across questions in what people know. Future work will be needed to identify the most effective questions for a survey that would compare respondents to the most knowledgeable individuals in any given setting, test for linkages between knowledge and behaviour, and be used to design and monitor interventions aimed at communicating knowledge for behaviour change.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
KS analysed the data and prepared the manuscript. WM conceptualized the study and oversaw the questionnaire development and analysis and contributed to the manuscript. All authors reviewed and provided input on the final article.
Supporting information
Data S1 Supporting information item
ACKNOWLEDGMENTS
The protocol was reviewed and approved by the Tufts University Institutional Review Board for Social, Behavioral and Educational Research (Protocol number 1703011) and by the National Commission for Science and Technology in Malawi (Protocol number P06/17/182). The contents are the responsibility of the authors and do not necessarily reflect the views of Catholic Relief Services, USAID, or the United States Government.
We are especially grateful to our skilled enumerators, Joseph Antonio, Chimwemwe Amini, Agatha Kaira, Deborah Kamanga, Robert Msukwa, and Gertrude Mwale and to partners at CRS Malawi Angela Tavares, Mary Mpinda, Mcleonard Kalonga, and other partners Aaron Banda (CADECOM), Anacklet Lupiya (CARE), Doris Mphande (Save the Children), all of the field officers and the other CRS Malawi and UBALE staff members who supported this work. Particular thanks are due to the respondents, whose willingness to share their experiences in this survey could help guide future interventions in Malawi and elsewhere. Survey instrument, data, and model code for replication are available at http://sites.tufts.edu/willmasters/research/ubale.
Schneider K, Masters WA. Orange Fanta versus orange fruit: A novel measure of nutrition knowledge in Malawi. Matern Child Nutr. 2019;15:e12656 10.1111/mcn.12656
Footnotes
The micronutrients are thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, vitamin A, vitamin C, calcium, iron and zinc. Criteria for the selection of micronutrients included known public health concern and data availability. Data considerations included availability of food composition tables and an estimated average requirement; for these reasons, vitamin D and iodine were not included. Although a set of agreed upon nutrients of concern exist for infants and young children (WHO & UNICEF, 1998), no such list exists for women and the available information is scarce (Kennedy & Meyers, 2005; Martin‐Prével et al., 2015).
REFERENCES
- Abbi, R. , Christian, P. , Gujaral, S. , & Gopaldas, T. (1988). Mother's nutrition knowledge and child nutrition status in India. Food and Nutrition Bulletin, 10(3), 51–54. [Google Scholar]
- Ahmed, A . (2013). Bangladesh Integrated Household Survey Questionnaire—2011–12. Retrieved September 29, 2017, from https://dataverse.harvard.edu/file.xhtml?fileId=2435038&version=RELEASED&version=.2
- Amugsi, D. A. , Lartey, A. , Kimani‐Murage, E. , & Mberu, B. U. (2016). Women's participation in household decision‐making and higher dietary diversity: Findings from nationally representative data from Ghana. Journal of Health, Population and Nutrition, 35(1), 16 10.1186/s41043-016-0053-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angeles, G. , Skiles, M. , Weaver, E. , Mussa, R. , & Sheahan, K. (2015). Impact evaluation: Integrating nutrition in value chains (INVC) in feed the future Malawi baseline report.
- Azzarri, C. , Zezza, A. , Haile, B. , & Cross, E. (2015). Does livestock ownership affect animal source foods consumption and child nutritional status? Evidence from rural Uganda. Journal of Development Studies, 51(8), 1034–1059. 10.1080/00220388.2015.1018905 [DOI] [Google Scholar]
- Barbosa, L. B. , Vasconcelos, S. M. L. , dos Santos Correia, L. O. , & Ferreira, R. C. (2016). Nutrition knowledge assessment studies in adults: A systematic review. Ciência & Saúde Coletiva, 21(2), 449–462. 10.1590/1413-81232015212.20182014 [DOI] [PubMed] [Google Scholar]
- Bhutta, Z. A. , Ahmed, T. , Black, R. E. , Cousens, S. , Dewey, K. , Giugliani, E. , … Shekar, M. (2008). What works? Interventions for maternal and child undernutrition and survival. Lancet, 371(9610), 417–440. 10.1016/S0140-6736(07)61693-6 [DOI] [PubMed] [Google Scholar]
- Black, R. E. , Victora, C. G. , Walker, S. P. , Bhutta, Z. A. , Christian, P. , De Onis, M. , … Uauy, R. (2013). Maternal and child undernutrition and overweight in low‐income and middle‐income countries. Lancet, 382(9890), 427–451. 10.1016/S0140-6736(13)60937-X [DOI] [PubMed] [Google Scholar]
- Block, S. A. (2004). Maternal nutrition knowledge and the demand for micronutrient‐rich foods: Evidence from Indonesia. The Journal of Development Studies, 40(6), 82–105. 10.1080/0022038042000233812 [DOI] [Google Scholar]
- Block, S. A. (2007). Maternal nutrition knowledge versus schooling as determinants of child micronutrient status. Oxford Economic Papers, 59(2), 330–353. 10.1093/oep/gpm001 [DOI] [Google Scholar]
- Boyle, M. H. , Racine, Y. , Georgiades, K. , Snelling, D. , Hong, S. , Omariba, W. , … Rao‐Melacini, P. (2006). The influence of economic development level, household wealth and maternal education on child health in the developing world. Social Science and Medicine, 63(8), 2242–2254. 10.1016/j.socscimed.2006.04.034 [DOI] [PubMed] [Google Scholar]
- Chilonda, P. , & Otte, J. (2006). Indicators to monitor trends in livestock production at national, regional and international levels. Livestock Research for Rural Development, 18(8), 2–10. [Google Scholar]
- Christiaensen, L. , & Alderman, H. (2004). Child malnutrition in Ethiopia: Can maternal knowledge augment the role of income? Economic Development and Cultural Change, 52(2), 287–312. 10.1086/380822 [DOI] [Google Scholar]
- Daelmans, B. , Dewey, K. , & Arimond, M. (2008). New and updated indicators for assessing infant and young child feeding. Food and Nutrition Bulletin, 30(2), 256–262. [DOI] [PubMed] [Google Scholar]
- Debela, B. L. , Demmler, K. M. , Rischke, R. , & Qaim, M. (2017). Maternal nutrition knowledge and child nutritional outcomes in urban Kenya. Appetite, 116, 518–526. 10.1016/j.appet.2017.05.042 [DOI] [PubMed] [Google Scholar]
- Dickson‐Spillmann, M. , & Siegrist, M. (2011). Consumers' knowledge of healthy diets and its correlation with dietary behaviour. Journal of Human Nutrition and Dietetics, 24(1), 54–60. 10.1111/j.1365-277X.2010.01124.x [DOI] [PubMed] [Google Scholar]
- FAO (2004). Worldwide regulations for mycotoxins in food and feed in 2003 In Worldwide regulations for mycotoxins in food and feed in 2003. Rome: Food and Agriculture Organization of the United Nations. [Google Scholar]
- FAO , & FHI 360. (2016). Minimum dietary diversity for women—A guide to measurement. Food and nutrition technical assistance III. Rome: FAO and FANTA. [Google Scholar]
- Fiorella, K. J. , Chen, R. L. , Milner, E. M. , & Fernald, L. C. H. H. (2016). Agricultural interventions for improved nutrition: A review of livelihood and environmental dimensions. Global Food Security, 8, 39–47. 10.1016/j.gfs.2016.03.003 [DOI] [Google Scholar]
- Gewa, C. , & Leslie, T. (2015). Distribution and determinants of young child feeding practices in the East African region: Demographic health survey data analysis from 2008–2011. Journal of Health, Population and Nutrition, 34(6), 14 10.1186/s41043-015-0008-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glewwe, P. (1999). Why does mother's schooling raise child health in developing countries? Evidence from why does mother's schooling raise child health in developing countries? Evidence from Morocco. The Journal of Human Resources, 34(1), 124–159. 10.2307/146305 [DOI] [Google Scholar]
- Harris‐Fry, H. , Azad, K. , Kuddus, A. , Shaha, S. , Nahar, B. , Hossen, M. , … Fottrell, E. (2015). Socio‐economic determinants of household food security and women's dietary diversity in rural Bangladesh: A cross‐sectional study. Journal of Health, Population and Nutrition, 33(2), 1–12. 10.1186/s41043-015-0022-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herforth, A. (2010). Nutrition and the environment: Fundamental to food security in Africa In Pinstrup‐Andersen P. (Ed.), The African food system and its interaction with human health and nutrition (pp. 128–160). Ithaca, NY: Cornell University Press; 10.7591/j.ctt7zd0x.14 [DOI] [Google Scholar]
- Hetherington, J. B. , Wiethoelter, A. K. , Negin, J. , & Mor, S. M. (2017). Livestock ownership, animal source foods and child nutritional outcomes in seven rural village clusters in Sub‐Saharan Africa. Agriculture & Food Security, 6(1), 9 10.1186/s40066-016-0079-z [DOI] [Google Scholar]
- Hirvonen, K. , & Hoddinott, J. (2017). Agricultural production and children's diets: Evidence from rural Ethiopia. Agricultural Economics, 48(4), 469–480. 10.1111/agec.12348 [DOI] [Google Scholar]
- Hirvonen, K. , Hoddinott, J. , Minten, B. , & Stifel, D. (2017). Children's diets, nutrition knowledge, and access to markets. World Development, 95, 303–315. 10.1016/j.worlddev.2017.02.031 [DOI] [Google Scholar]
- HLPE (2016). Sustainable agricultural development for food security and nutrition: HLPE high level panel of experts what roles for livestock? . Rome: Committee on World Food Security. [Google Scholar]
- Hoddinott, J. , Behrman, J. R. , Maluccio, J. A. , Melgar, P. , Quisumbing, A. R. , Ramirez‐Zea, M. , … Martorell, R. (2013). Adult consequences of growth failure in early childhood. American Journal of Clinical Nutrition, 98(5), 1170–1178. 10.3945/ajcn.113.064584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones, A. D. (2016). On‐farm crop species richness is associated with household diet diversity and quality in subsistence‐ and market‐oriented farming households in Malawi. The Journal of Nutrition, 147(1), 86–96. 10.3945/jn.116.235879 [DOI] [PubMed] [Google Scholar]
- Jones, A. D. , Shrinivas, A. , & Bezner‐Kerr, R. (2014). Farm production diversity is associated with greater household dietary diversity in Malawi: Findings from nationally representative data. Food Policy, 46, 1–12. 10.1016/j.foodpol.2014.02.001 [DOI] [Google Scholar]
- Karmacharya, C. , Cunningham, K. , Choufani, J. , & Kadiyala, S. (2017). Grandmothers' knowledge positively influences maternal knowledge and infant and young child feeding practices. Public Health Nutrition, 20, 1–10. 10.1017/S1368980017000969 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy, E. , & Meyers, L. (2005). Dietary Reference Intakes: development and uses for assessment of micronutrient status of women—a global perspective. American Journal of Clinical Nutrition, 81(suppl), 1194S–1197S. [DOI] [PubMed] [Google Scholar]
- Khalesi, S. , Sharma, S. , Irwin, C. , & Sun, J. (2016). Dietary patterns, nutrition knowledge and lifestyle: Associations with blood pressure in a sample of Australian adults (the Food BP study). Journal of Human Hypertension, 30(10), 581–590. 10.1038/jhh.2016.22 [DOI] [PubMed] [Google Scholar]
- Kiboi, W. , Kimiywe, J. , & Chege, P. (2017). Determinants of dietary diversity among pregnant women in Laikipia County, Kenya: A cross‐sectional study. BMC Nutrition, 3 10.1186/s40795-017-0126-6 [DOI] [Google Scholar]
- Kigaru, D. M. D. , Loechl, C. , Moleah, T. , & Ndungu, Z. W. (2016). Nutrition knowledge, attitude and practices among urban primary school children in Nairobi City, Kenya: A KAP study. BMC Nutrition, 1(2015), 1–8. 10.1186/s40795-015-0040-8 [DOI] [Google Scholar]
- Kumar, N. , Harris, J. , & Rawat, R. (2015). If they grow it, will they eat and grow? Evidence from Zambia on agricultural diversity and child undernutrition. Journal of Development Studies, 51(8), 1060–1077. 10.1080/00220388.2015.1018901 [DOI] [Google Scholar]
- Malapit, H. J. L. , Kadiyala, S. , Quisumbing, A. , Cunningham, K. , & Tyagi, P. (2015). Women's empowerment mitigates the negative effects of low production diversity on maternal and child nutrition in Nepal. The Journal of Development Studies, 51(8), 1097–1123. 10.1080/00220388.2015.1018904 [DOI] [Google Scholar]
- Martin‐Prével, Y. , Allemand, P. , Wiesmann, D. , Arimond, M. , Ballard, T. , Deitchler, M. , … Moursi, M. (2015). Moving forward: On choosing a standard operational indicator of women's dietary diversity. Rome: FAO. [Google Scholar]
- Masters, W. A. , Colaiezzi, B. , Dennison, K. , Hill, J. , Jordan‐Bell, E. , Kablan, A. , … Oehmke, J. (2015). Agricultural policy for improved nutrition in Africa and Asia: Evidence to guide the US Government's investments in food security. Food Security, 7(3), 747–750. 10.1007/s12571-015-0444-y [DOI] [Google Scholar]
- Matumba, L. , Monjerezi, M. , Biswick, T. , Mwatseteza, J. , Makumba, W. , Kamangira, D. , & Mtukuso, A. (2014). A survey of the incidence and level of aflatoxin contamination in a range of locally and imported processed foods on Malawian retail market. Food Control, 39(1), 87–91. 10.1016/j.foodcont.2013.09.068 [DOI] [Google Scholar]
- Matumba, L. , Monjerezi, M. , Chirwa, E. , Lakudzala, D. , & Mumba, P. (2009). Natural occurrence of AFB 1 in maize and effect of traditional maize flour production on AFB 1 reduction in Malawi. African Journal of Food Science, 3(12), 413–425. [Google Scholar]
- Mbuya, M. N. N. , Menon, P. , Habicht, J.‐P. , Pelto, G. H. , & Ruel, M. T. (2013). Maternal knowledge after nutrition behavior change communication is conditional on both health workers' knowledge and knowledge‐sharing efficacy in rural Haiti. The Journal of Nutrition, 143, 2022–2028. 10.3945/jn.113.178442 [DOI] [PubMed] [Google Scholar]
- Monyo, E. S. , Njoroge, S. M. C. , Coe, R. , Osiru, M. , Madinda, F. , Waliyar, F. , … Anitha, S. (2012). Occurrence and distribution of aflatoxin contamination in groundnuts (Arachis hypogaea L) and population density of Aflatoxigenic Aspergilli in Malawi. Crop Protection, 42, 149–155. 10.1016/j.cropro.2012.07.004 [DOI] [Google Scholar]
- National Statistical Office [Malawi] and ICF (2017). Malawi Demographic and Health Survey 2015–2016. Malawi and Rockville, MD: Zomba. [Google Scholar]
- Ng, M. , Fleming, T. , Robinson, M. , Thomson, B. , Graetz, N. , Margono, C. , … Gakidou, E. (2014). Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet, 384(9945), 766–781. 10.1016/S0140-6736(14)60460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Özaltin, E. , Hill, K. , & Subramanian, S. V. (2010). Association of maternal stature with offspring mortality, underweight, and stunting in low‐to middle‐income countries. JAMA, 303(15), 1507–1516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parmenter, K. , & Wardle, J. (1999). Development of a general nutrition knowledge questionnaire for adults. European Journal of Clinical Nutrition, 53(4), 298–308. 10.1038/sj.ejcn.1600726 [DOI] [PubMed] [Google Scholar]
- Prentice, A. M. (2006). The emerging epidemic of obesity in developing countries. International Journal of Epidemiology, 35(1), 93–99. 10.1093/ije/dyi272 [DOI] [PubMed] [Google Scholar]
- Prentice, A. M. , Ward, K. A. , Goldberg, G. R. , Jarjou, L. M. , Moore, S. E. , Fulford, A. J. , & Prentice, A. (2013). Critical windows for nutritional interventions against stunting. American Journal of Clinical Nutrition, 97(5), 911–918. 10.3945/ajcn.112.052332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rashid, D. A. , Smith, L. C. , & Rahman, T. (2011). Determinants of dietary quality: Evidence from Bangladesh. World Development, 39(12), 2221–2231. 10.1016/j.worlddev.2011.05.022 [DOI] [Google Scholar]
- Romeo, A. , Meerman, J. , Demeke, M. , Scognamillo, A. , & Asfaw, S. (2016). Linking farm diversification to household diet diversification: evidence from a sample of Kenyan ultra‐poor farmers. Food Security, 8(6), 1069–1085. 10.1007/s12571-016-0617-3 [DOI] [Google Scholar]
- Ruel, M. T. , & Alderman, H. (2013). Nutrition‐sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? Lancet, 382(9891), 536–551. 10.1016/S0140-6736(13)60843-0 [DOI] [PubMed] [Google Scholar]
- Ruel, M. T. , Habicht, J. P. , Pinstrup‐Andersen, P. , & Gröhn, Y. (1992). The mediating effect of maternal nutrition knowledge on the association between maternal schooling and child nutritional status in Lesotho. American Journal of Epidemiology, 135(8), 904–914. [DOI] [PubMed] [Google Scholar]
- Ruel, M. T. , Quisumbing, A. R. , & Balagamwala, M. (2018). Nutrition‐sensitive agriculture: What have we learned so far? Global Food Security, 17, 128–153. 10.1016/j.gfs.2018.01.002 [DOI] [Google Scholar]
- Savy, M. , Martin‐Prével, Y. , Danel, P. , Traissac, P. , Dabiré, H. , & Delpeuch, F. (2008). Are dietary diversity scores related to the socio‐economic and anthropometric status of women living in an urban area in Burkina Faso? Public Health Nutrition, 11(02), 132–141. 10.1017/S1368980007000043 [DOI] [PubMed] [Google Scholar]
- Shamim, A. A. , Mashreky, S. R. , Ferdous, T. , Tegenfeldt, K. , Roy, S. , Rahman, A. K. M. F. , … Shaheen, N. (2016). Pregnant women diet quality and its sociodemographic determinants in Southwestern Bangladesh. Food and Nutrition Bulletin, 37(1), 14–26. 10.1177/0379572116632137 [DOI] [PubMed] [Google Scholar]
- Smith, L. E. , Prendergast, A. J. , Turner, P. C. , Mbuya, M. N. N. , Mutasa, K. , Kembo, G. , & Stoltzfus, R. J. (2015). The potential role of mycotoxins as a contributor to stunting in the SHINE Trial. Clinical Infectious Diseases, 61, S733–S737. 10.1093/cid/civ849 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snapp, S. S. , Blackie, M. J. , Gilbert, R. A. , Bezner‐Kerr, R. , & Kanyama‐Phiri, G. Y. (2010). Biodiversity can support a greener revolution in Africa. Proceedings of the National Academy of Sciences of the United States of America, 107(48), 20840–20845. 10.1073/pnas.1007199107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snapp, S. S. , & Fisher, M. (2014). “Filling the maize basket” supports crop diversity and quality of household diet in Malawi. Food Security, 7(1), 83–96. 10.1007/s12571-014-0410-0 [DOI] [Google Scholar]
- Tabbakh, T. , & Freeland‐Graves, J. H. (2016). The home environment: A mediator of nutrition knowledge and diet quality in adolescents. Appetite, 105, 46–52. 10.1016/j.appet.2016.05.002 [DOI] [PubMed] [Google Scholar]
- Torheim, L. E. , Ouattara, F. , Diarra, M. M. , Thiam, F. D. , Barikmo, I. , Hatløy, A. , & Oshaug, A. (2004). Nutrient adequacy and dietary diversity in rural Mali: Association and determinants. European Journal of Clinical Nutrition, 58(4), 594–604. 10.1038/sj.ejcn.1601853 [DOI] [PubMed] [Google Scholar]
- Trakman, G. L. , Forsyth, A. , Hoye, R. , & Belski, R. (2017). Developing and validating a nutrition knowledge questionnaire: Key methods and considerations. Public Health Nutrition, 20, 1–10. 10.1017/S1368980017001471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Victora, C. G. , Adair, L. , Fall, C. , Hallal, P. C. , Martorell, R. , Richter, L. , & Sachdev, H. S. (2008). Maternal and child undernutrition: Consequences for adult health and human capital. Lancet, 371(9609), 340–357. 10.1016/S0140-6736(07)61692-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vollmer, S. , Bommer, C. , Krishna, A. , Harttgen, K. , & Subramanian, S. V. (2017). The association of parental education with childhood undernutrition in low‐ and middle‐income countries: Comparing the role of paternal and maternal education. International Journal of Epidemiology, 46(1), 312–323. 10.1093/ije/dyw133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vyas, S. , & Kumaranayake, L. (2006). Constructing socio‐economic status indices: How to use principal components analysis. Health Policy and Planning, 21(6), 459–468. 10.1093/heapol/czl029 [DOI] [PubMed] [Google Scholar]
- Wardle, J. , & Parmenter, K. (2000). Evaluation and design of nutrition knowledge measures. Journal of Nutrition Education, 32(5), 269–277. 10.1016/S0022-3182(00)70575-9 [DOI] [Google Scholar]
- Wardle, J. , Parmenter, K. , & Waller, J. (2000). Nutrition knowledge and food intake. Department of Epidemiology and Public Health, 34(3), 235–243. [DOI] [PubMed] [Google Scholar]
- Webb, P. , & Block, S. (2004). Nutrition information and formal schooling as inputs to child nutrition. Economic Development and Cultural Change, 52(4), 801–820. 10.1086/420901 [DOI] [Google Scholar]
- World Health Organization (WHO) (2008). Indicators for assessing infant and young child feeding practices (part 1). Geneva: World Health Organization. [Google Scholar]
- World Health Organization (WHO) (2010). Indicators for assessing infant and young child feeding practices (part 3). Geneva: World Health Organization. [Google Scholar]
- World Health Organization (WHO) (2013). Essential nutrition actions: Improving maternal, newborn, infant and young child health and nutrition. Geneva: World Health Organization. [PubMed] [Google Scholar]
- World Health Organization (WHO) & United Nations Children's Fund (UNICEF) (1998). Complementary feeding of young children in developing countries: A review of current scientific knowledge. Geneva: World Health Organization. [Google Scholar]
- Williams, L. , Campbell, K. , Abbott, G. , Crawford, D. , & Ball, K. (2012). Is maternal nutrition knowledge more strongly associated with the diets of mothers or their school‐aged children? Public Health Nutrition, 15(08), 1396–1401. 10.1017/S1368980011003430 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1 Supporting information item