

Abstract
Background
A fixed-dose combination of ledipasvir/sofosbuvir (LDV/SOF) is efficacious in treating chronic hepatitis C virus (HCV) infection; however, objective adherence to prescribed regimens in real-world clinical settings has not been well studied.
Objective
This study aimed to evaluate adherence and virologic outcomes in patients with chronic HCV infection treated with LDV/SOF using a novel digital medicine program that directly measures drug ingestion adherence.
Methods
This prospective, observational, open-label, single-arm pilot study was conducted at 2 clinical research sites and followed patients with HCV infection who were prescribed LDV/SOF along with an ingestible sensor. Patients were treated for 8 or 12 weeks. The main outcomes were ingestion adherence, medical interventions, virologic response, safety, and patient satisfaction.
Results
Of the 28 patients (mean 59 years, SD 7), 61% (17/28) were male, 61% (17/28) were non-Caucasian, and 93% (26/28) were treatment naïve. All 28 had genotype 1 HCV, and of these, 27 completed an 8- or 12-week treatment. Patients used the digital medicine program for 92% of the expected days; the overall mean ingestion adherence rate was 97%. Providers used the digital medicine program data for same-day medication therapy management in 39% (11/28) of patients. End-of-treatment response was achieved in all the available 21 of 28 patients. Sustained virologic response at 12 weeks or more was achieved in 26 of 28 patients; of the 2 patients who relapsed, one had less than 90% adherence and the other had greater than or equal to 95% adherence, lending insights into reasons for treatment failure. A total of 4 subjects reported nonserious adverse events, which were resolved.
Conclusions
The findings of this study suggest that digital medicines can be used for wirelessly observed therapy to support adherence to antiviral HCV therapy, reduce unnecessary medication wastage and retreatment costs, and potentially optimize sustained virologic response rates, especially in populations at high risk for nonadherence.
Keywords: chronic hepatitis C, HCV, compliance, sustained virologic response, antivirals, sofosbuvir
Introduction
Background
The World Health Organization estimated that in 2015, 71 million people worldwide were living with chronic hepatitis C virus (HCV) infection. Although recent studies report that the incidence of HCV has decreased during the past 50 years [1-3], estimates obtained from modeling suggest that in 2015, there were still 1.75 million new HCV infections worldwide—a global incidence rate of 23.7 per 100,000 [4]. It is estimated that up to 20% to 30% of individuals with chronic HCV infection will develop liver cirrhosis with associated complications, including hepatocellular carcinoma, liver decompensation, and increased mortality [4,5]. In addition, there has been a recent steep increase in HCV diagnoses in the United States, owing, in part, to the opioid epidemic [6]. Treatment for chronic HCV infection has evolved rapidly over the past 5 years, with new all-oral, single-tablet, direct-acting antiviral (DAA) agents. Among the currently available medications is a once-daily, fixed-dose combination of ledipasvir and sofosbuvir (LDV/SOF) for the treatment of chronic HCV genotype 1 (GT-1) infection [7].
A recent clinical trial investigating the efficacy of an LDV/SOF combined formulation, conducted in a real-world setting, showed high response rates in the per-protocol population following 8 weeks (98.2%) and 12 weeks (98.3%) but notably lower response rates in the intent-to-treat (ITT) population following 8 weeks (84.6%) and 12 weeks (85.1%) [8]. The differences between per-protocol and ITT outcomes highlight the importance of adherence and patient engagement to HCV therapy as an essential element in achieving sustained virologic response (SVR) or cure. In addition, in special populations, such as people who inject drugs, SVR rates are lower and are associated with better compliance [9].
A novel digital medicine program, Proteus Discover (Proteus Digital Health), evaluates medication adherence through wirelessly observed therapy and addresses these limitations [10]. The digital medicine program directly measures medication ingestion adherence, heart rate, physical activity, and other biometrics. It then provides real-time feedback to patients and health care providers via mobile devices and a dedicated Web portal to support patient self-management and facilitate therapy optimization by the provider.
Objective
This study aimed to evaluate medication ingestion adherence and virologic outcomes in patients with chronic HCV infection who were prescribed LDV/SOF along with the digital medicine program for wirelessly observed therapy. Safety and patient satisfaction related to digital medicine program were also assessed.
Methods
Study Design
This was a 24-week, single-arm, prospective, open-label, pilot study designed to assess real-world adherence to LDV/SOF treatment among patients with HCV infection using the digital medicine program. The study was conducted at 2 US clinical research sites from August 25, 2015, to November 9, 2017. Potential patients who met the inclusion criteria were identified through electronic medical records and contacted to assess their interest in study participation.
An independent investigational review board (E&I) approved the study protocol. All aspects of this study were conducted in accordance with the US Food and Drug Administration (FDA) regulations, the International Council for Harmonisation E6 (R1) guideline for Good Clinical Practice, and applicable local, state, and federal laws.
Patients
The study enrolled adult patients diagnosed with chronic HCV infection to be initiated on fixed-dose LDV/SOF. Patients were included if they had HCV viremia greater than 50,000 IU/mL, capacity to use a smartphone or tablet (assessed by the investigators), and adequate data connectivity at home via cellular service or a secure wireless internet network. Patients were excluded from the study if any of the following criteria were met: history of skin sensitivity to adhesives, history of acute or chronic dermatitis, decompensated cirrhosis, liver transplant candidate, lack of insurance coverage for fixed-dose LDV/SOF, BMI greater than 40 kg/m2, and currently known to be pregnant or nursing an infant. For women of childbearing potential, the following exclusion criteria were considered: not using an acceptable form of contraception for at least 3 months before the start of the study and throughout the study, lactating, current participation in another clinical trial, terminal illness (≤1 year of life anticipated), inability to swallow pills, or any condition that in the investigator’s opinion could preclude safe participation in the study. All patients signed a written informed consent form before entering the study.
Digital Medicine Program
The digital medicine program consists of 3 components that function together: (1) LDV/SOF that was individually repackaged with FDA-approved ingestible sensors by a specialty pharmacy; (2) an FDA-approved wearable sensor patch, which is worn by the patient over the left upper quadrant and collects time-stamped medication ingestion events and physiologic metrics (eg, steps, activity, rest, and heart rate); (3) a mobile app and software that calculates and summarizes adherence patterns, physical activity, rest, and other self-entered clinical data that patients can view through a mobile device and providers can view through a secure Web portal. After being swallowed, the ingestible sensor activates after 2 to 3 min, sending a brief signal to the patch before passing through the body naturally. The digital medicine program directly measures medication ingestion adherence, providing objective data to patients and providers.
Procedures
At the screening visit, patients’ medical records were reassessed to confirm eligibility, baseline laboratory values were taken (per usual care), signed informed consent was obtained, and a urine sample for pregnancy testing was collected. Patients received hands-on training on using the digital medicine program and were instructed to change the sensor patch every 7 days or sooner, as determined by the sensor. Patients were taught to review the app daily to obtain feedback on their medication adherence. Patients used the digital medicine program for the duration of their 8- or 12-week treatment period. The determination of treatment duration was based on the patient’s baseline liver severity and HCV viral load as well as prior therapy.
Throughout the treatment period, a provider reviewed patients’ adherence data from a secure Web portal at their discretion. If a missed dose was detected, the patient was contacted by phone to account for the missing dose and was provided adherence counseling if needed. Nonadherent patients were asked to return to the clinic at weeks 4 or 6 for laboratory assessment and adherence counseling. Patients with high levels of adherence were not required to return to the clinic unless the provider wanted to assess other laboratory examinations, such as liver function tests. HCV viral load was assessed at the end of the treatment (8 or 12 weeks, depending on patient treatment plan) and at 12 weeks or more after the treatment ended. Patients also completed a satisfaction survey at the end of the treatment. All clinic procedures were performed per usual care except for the digital medicine program intervention, which prompted adherence interventions. Any technical issues were handled by Proteus Digital Health, and clinical issues were forwarded to the site for evaluation.
Outcomes
The primary end point of the study was the percentage of subjects with greater than or equal to 95% medication ingestion adherence. Ingestion nonadherence was defined as a failure to trigger iPad (Apple Inc) activation within the 4-hour window surrounding the scheduled dose, that is, the number of medication ingestions measured by the digital medicine program plus same-day patient confirmation of ingestions reported to the health care provider over the total expected number of ingestions during the treatment period. Other outcomes included virologic response, medical interventions made, safety of the digital medicine program, and patient satisfaction.
Statistical Analysis
Owing to the pilot nature of the study, a priori sample sizes were determined. All analyses were performed on the ITT population, defined as all patients who received at least one dose of the study medication. All end points were presented descriptively. Categorical variables were described as proportions, whereas continuous variables were described as mean (SD) or median (IQR) where appropriate. Multivariate linear regressions were conducted and used to assess demographic, clinical, and behavioral predictors of adherence using R version 3.5.1 (The R Foundation for Statistical Computing).
Results
Treatment Cohort
A total of 31 patients were screened, and of these patients, 28 met the inclusion criteria and were enrolled in the study (ITT population). All 28 patients (mean 59 years, SD 7; 61% [17/28] male; 61% [17/28] non-Caucasians; 93% [26/28] treatment naïve) had HCV GT-1. Moreover, 1 patient withdrew from the study 21 days after initiating digital medicine program use, and 27 patients completed digital medicine program use for 8 weeks (n=10) or 12 weeks (n=17) as prescribed. In addition, 13 (46%) patients had psychiatric comorbidities, and 9 (32%) of the patients had a history of drug abuse. Table 1 presents the baseline characteristics of enrolled patients.
Table 1.
Baseline demographics and characteristics (N=28).
| Characteristic | Value | |
| Male, n (%) | 17 (61) | |
| Age (years), mean (SD) | 59 (7) | |
| Genotype, n (%) | ||
|
|
1a | 25 (89) |
|
|
1b | 3 (11) |
| Race, n (%) | ||
|
|
Caucasian | 11 (39) |
|
|
African American | 10 (36) |
|
|
Hispanic/Latino | 4 (14) |
|
|
American Indian/Alaska Native and other | 3 (11) |
| Cirrhosis, n (%) | 1 (4) | |
| Prior treatment history, n (%) | ||
|
|
Treatment naïve | 26 (93) |
|
|
Previous treatment relapse | 2 (7) |
| Frequency of mobile phone use per week, n (%) | ||
|
|
<1 time | 3 (11) |
|
|
2-4 times | 4 (14) |
|
|
5-7 times | 21 (75) |
| Education level, n (%) | ||
|
|
Less than high school | 2 (7) |
|
|
Some high school or high school graduate | 12 (43) |
|
|
Some college or college graduate | 13 (46) |
|
|
Postgraduate education | 1 (4) |
| Income level (US $/year), n (%) | ||
|
|
<25,000 | 23 (82) |
|
|
≥25,000 | 5 (18) |
| Psychiatric comorbidity, n (%) | 13 (46) | |
| Prior or current drug abuse history, n (%) | 9 (32) | |
Adherence Outcomes
High rates of medication ingestion adherence were observed, with 89% of patients achieving greater than or equal to 95% adherence. Patients were connected to the digital medicine program for 92% of expected days, with an overall mean adherence rate of 97%. Using a stepwise approach to select variables to include in the model, multivariate linear regression showed that being African American, having high school education or less, and having a psychiatric comorbidity were found to be consistently significant predictors of nonadherence (Table 2). Mean adherence was lower in African Americans than others (88% vs 96%), those with high school education vs those with less (91% vs 96%), and individuals with a psychiatric comorbidity vs those without a psychiatric comorbidity (90% vs 96%). There was no difference in adherence between patients treated for 8 weeks vs 12 weeks.
Table 2.
Predictors of adherence using stepwise multivariate linear regression.
| Factors | Model coefficienta |
| Race⸺African American vs other | −8.8 |
| Education⸺high school graduate or less | −5.7 |
| Comorbidities⸺psychiatric comorbidity | −5.4 |
aOnly statistically significant factors (P<.05) are included.
Efficacy Outcomes
Virologic results at the end of the treatment were available for 21 patients, all of whom achieved an end-of-treatment response. All 28 subjects were assessed at 12 weeks or more posttreatment. Among those subjects, 26 (93%) achieved SVR, including 2 treatment-experienced patients who had previously failed treatment. Of the 2 subjects who did not achieve SVR, one had documented suboptimal adherence (<90%) and the other had greater than or equal to 95% adherence, suggesting viral resistance as the cause of relapse.
Provider Medication Interventions Made
Health care providers used the digital medicine program data for timely (same-day) assessment of medication ingestion adherence. A total of 130 documented initial missed doses occurred among 11 (39%) patients. Interventions made to mitigate nonadherence among these patients included 75 follow-up phone calls, 21 adherence counseling events, and 5 follow-up visits; some patients required multiple interventions per missed dose. No action was performed for the remaining 35 events (eg, patient unreachable).
Patient Satisfaction
Overall satisfaction with the use of the device was high among study subjects (Figure 1). Most (92%) patients completely or somewhat agreed that the DMP was easy to use in their daily routine and helped them feel more involved in managing their health care, 96% did not mind wearing the patch and sharing their data with their health care team, and 85% agreed that the DMP helped them understand the importance of taking their medications regularly.
Figure 1.
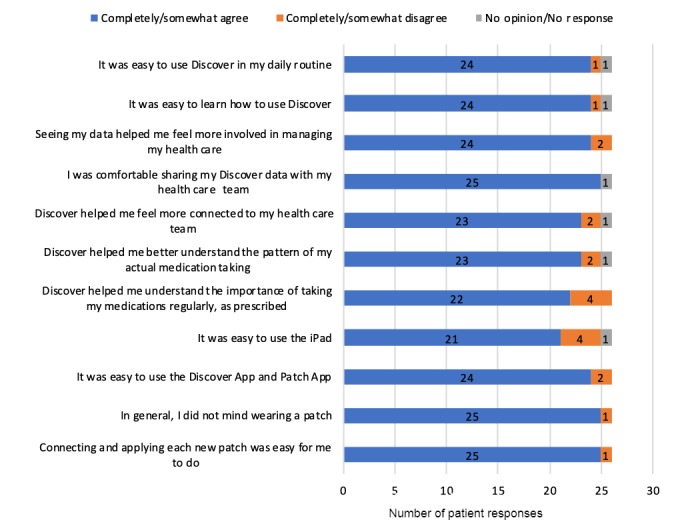
Patient satisfaction survey results (n=26).
Safety Findings
A total of 4 nonserious, device-related adverse events were reported in 4 subjects during the study. These adverse events were reflective of commonly reported symptoms of irritant contact dermatitis (rash). Of these, 1 reported adverse event (itching) was assessed by the investigator as severe and resolved without any action taken with the DMP device. The remaining 3 reported adverse events of rash were assessed by the investigator as mild in severity and resolved.
Discussion
Principal Findings
This real-world pilot study in a cohort of patients with chronic HCV infection demonstrated that the use of the DMP with same-day interventions (when needed) prompted high rates of medication adherence (97%), despite the presence of multiple risk factors for nonadherence, such as race, psychiatric comorbidities, and substance use or abuse. More importantly, SVR at 12 weeks or more was achieved in 92.8% (26/28) of the patients. Patients were connected to the DMP 92% of the time, indicating high patient engagement, and the system was easy to use even in those patients with historically low mobile phone use. In addition, the DMP had a favorable safety profile and provided data to facilitate timely adherence interventions. Thus, the unique ability of the DMP to provide objective adherence data enabled timely medication interventions aimed at improving adherence and optimizing outcomes, even in high-risk patients who have previously failed therapy.
Large clinical trials have demonstrated that treatment with once-daily, combined, fixed-dose LDV/SOF therapy is effective in achieving SVR in a vast majority of patients with chronic HCV infection [8,11-13]. However, adherence to prescribed treatment regimens is critical to achieving treatment success [14]. Nonadherence to HCV DAA regimens has been shown to be associated with a lower rate of SVR [12], particularly in patients with psychiatric illness [15]. Current indirect assessment methods (eg, medication possession ratios, patient self-report, pill counts, and electronic pill bottles) may overestimate actual medication adherence [16]. In contrast, DMP addresses the inherent limitations of these methods through direct objective measurement of medication ingestion. In addition, and perhaps more importantly, it allows real-time digital intervention by patients and/or clinicians when doses are not recorded as ingested.
High levels of adherence have been reported in large clinical trials using various measurement assessments, including electronic medication event monitoring (MEM) caps, pill counts, and patient reports [12,13]. However, the accuracy of the current measurement methods may be questionable because of the limitations of each. For example, patients may purposefully mislead the MEM system by accidentally actuating the container without taking the medication [17]. Intentional manipulation of pill counts (pill dumping) and falsified patient reports to appear adherent must also be considered when measuring medication adherence [17]. None of these methods allow the patient or provider an opportunity to respond quickly or proactively to perceived missed doses [18,19]. Although measurement of the proportion of days covered is commonly used to assess long-term adherence in patients with chronic illnesses [20], the use of prescription refill data does not allow for timely detection of nonadherence, and it does not necessarily indicate that all the medications have been taken [21].
Medication adherence is of particular concern among patients with HCV treated with fixed-dose LDV/SOF therapy, many of whom are at high risk for nonadherence because of transient living situations, depression, neurocognitive impairment, psychiatric comorbidities, and concurrent alcohol and other substance abuse [22,23]. As successful treatment is dependent on strict adherence to the prescribed medication regimen, nonadherence may result in the same poor clinical outcomes (eg, liver cirrhosis, hepatocellular carcinoma, liver decompensation, and increased mortality) associated with nontreatment [4,5].
The DMP has been studied in multiple therapeutic areas, including cardiovascular and infectious diseases. In a randomized controlled trial of the DMP compared with usual care in patients with hypertension and diabetes, those using the DMP with their prescribed medications experienced greater reductions in systolic blood pressure (BP; mean change −24.6 vs −15.2; mean difference −9.4; SE 2.7; 95% CI −14.6 to −4.2 mm Hg) and glycohemoglobin (mean change −0.08% vs 0.28%; mean difference −0.57%; 95% CI −1.53 to 0.39) at 12 weeks [24]. In addition, a significantly higher number of subjects reached their BP goal in the DMP group compared with those in usual care after 12 weeks (98% vs 52%; mean difference 46%; 95% CI 7.1% to 84.5%). The DMP was also studied as wirelessly observed therapy in the setting of tuberculosis treatment, demonstrating a positive detection accuracy for wirelessly observed therapy of 98.4% (95% CI 97.5% to 99%) and confirming 54% more doses than even the previous gold standard of directly observed therapy [25]. The accuracy and objectivity of this DMP at quantifying and recording medication adherence have been firmly established in the literature [26].
Our results are similar to those reported in recent adherence and efficacy studies [8,11-13]. However, deriving correlations between adherence and treatment effect is problematic. For example, Petersen et al [13] reported 97.6% adherence as measured by an MEM system but provided no data regarding treatment effect. Conversely, neither of the 2 efficacy studies reported medication adherence data [8,11]. In addition, a recent study highlighted the ineffectiveness of low-cost reminder devices in improving adherence among nonadherent patients with chronic conditions, suggesting the need for objectivity, effectual interventions, and personalized feedback [27].
Strengths and Limitations
A key strength of our study was the ability to directly measure medication ingestion, providing objective adherence data to better inform medical decision making. Although the small study population does not allow for definitive assessment of correlations between adherence and treatment effect, positive associations can be inferred from the timely interventions on missed doses, thereby improving adherence, which is expected to result in SVR. By extension, another positive point is the ability to improve patient care by contacting patients in real time and proactively assisting with missed doses.
Our study is limited by the single-arm design that precludes direct comparison with a usual care group. Furthermore, because of the small sample size, our results may not accurately reflect the broader population of patients with chronic HCV infection [28]. A larger multicenter clinical trial is currently underway to confirm and further elucidate these findings.
As reported by Moreno et al [29], improving patient access to HCV treatment will likely yield significant cost reductions for payers, accrued from the long-term reduction in prevalent and incident cases, mortality, and medical costs. Technology such as DMP could ensure that more patients with risk factors for nonadherence can complete therapy to ensure maximal real-world SVR rates. As reported in this study, although 6 patients failed to attend the end-of-treatment assessment for unknown reasons, all 28 patients were assessed at the 12-week or more evaluation period, where 26 (93%) achieved SVR. Patients were connected to the digital medicine program 92% of the expected days, indicating high patient engagement, and the system was easy to use even in those patients with historically low mobile phone use. In addition, the digital medicine program had a favorable safety profile and provided data to facilitate timely adherence interventions.
Conclusions
These data suggest that the digital medicine program can support adherence to therapy, enhance patient engagement, reduce unnecessary medication wastage, and optimize SVR rates in patients with chronic HCV infection, including those with multiple risk factors for nonadherence and in those who have previously failed therapy.
Acknowledgments
This study was funded by Proteus Digital Health.
Abbreviations
- BP
blood pressure
- DAA
direct-acting antiviral
- FDA
Food and Drug Administration
- GT-1
genotype 1
- HCV
hepatitis C virus
- ITT
intent-to-treat
- LDV/SOF
ledipasvir/sofosbuvir
- MEM
medication event monitoring
- SVR
sustained virologic response
Footnotes
Authors' Contributions: MB, YK, and CL contributed to the conception and design of the study. All authors contributed to data acquisition and analysis, critical review, scientific input, and final approval, and approved the final version of the paper.
Conflicts of Interest: YK and MT are employees of Proteus Digital Health. MB has received research support from AbbVie, Allergan, Assembly Biosciences, Boehringer-Ingelheim, Intercept, Genfit, Gilead, Novartis, and Pfizer and has received speaker fees from AbbVie, Gilead, and Intercept. CL received research funding from Gilead, AbbVie, and Proteus. CP and LM report no disclosures.
References
- 1.Bruggmann P, Berg T, Øvrehus AL, Moreno C, Mello CE, Roudot-Thoraval F, Marinho RT, Sherman M, Ryder SD, Sperl J, Akarca U, Balık I, Bihl F, Bilodeau M, Blasco AJ, Buti M, Calinas F, Calleja JL, Cheinquer H, Christensen PB, Clausen M, Coelho HS, Cornberg M, Cramp ME, Dore GJ, Doss W, Duberg AS, El-Sayed MH, Ergör G, Esmat G, Estes C, Falconer K, Félix J, Ferraz ML, Ferreira PR, Frankova S, García-Samaniego J, Gerstoft J, Giria JA, Gonçales FL, Gower E, Gschwantler M, Pessôa MG, Hézode C, Hofer H, Husa P, Idilman R, Kåberg M, Kaita KD, Kautz A, Kaymakoglu S, Krajden M, Krarup H, Laleman W, Lavanchy D, Lázaro P, Marotta P, Mauss S, Correa MC, Müllhaupt B, Myers RP, Negro F, Nemecek V, Örmeci N, Parkes J, Peltekian KM, Ramji A, Razavi H, Reis N, Roberts SK, Rosenberg WM, Sarmento-Castro R, Sarrazin C, Semela D, Shiha GE, Sievert W, Stärkel P, Stauber RE, Thompson AJ, Urbanek P, van Thiel I, van Vlierberghe H, Vandijck D, Vogel W, Waked I, Wedemeyer H, Weis N, Wiegand J, Yosry A, Zekry A, van Damme P, Aleman S, Hindman SJ. Historical epidemiology of hepatitis C virus (HCV) in selected countries. J Viral Hepat. 2014 May;21(Suppl 1):5–33. doi: 10.1111/jvh.12247. [DOI] [PubMed] [Google Scholar]
- 2.Saraswat V, Norris S, de Knegt RJ, Sanchez Avila JF, Sonderup M, Zuckerman E, Arkkila P, Stedman C, Acharya S, Aho I, Anand AC, Andersson MI, Arendt V, Baatarkhuu O, Barclay K, Ben-Ari Z, Bergin C, Bessone F, Blach S, Blokhina N, Brunton CR, Choudhuri G, Chulanov V, Cisneros L, Croes EA, Dahgwahdorj YA, Dalgard O, Daruich JR, Dashdorj NR, Davaadorj D, de Vree M, Estes C, Flisiak R, Gadano AC, Gane E, Halota W, Hatzakis A, Henderson C, Hoffmann P, Hornell J, Houlihan D, Hrusovsky S, Jarčuška P, Kershenobich D, Kostrzewska K, Kristian P, Leshno M, Lurie Y, Mahomed A, Mamonova N, Mendez-Sanchez N, Mossong J, Nurmukhametova E, Nymadawa P, Oltman M, Oyunbileg J, Oyunsuren T, Papatheodoridis G, Pimenov N, Prabdial-Sing N, Prins M, Puri P, Radke S, Rakhmanova A, Razavi H, Razavi-Shearer K, Reesink HW, Ridruejo E, Safadi R, Sagalova O, Sanduijav R, Schréter I, Seguin-Devaux C, Shah SR, Shestakova I, Shevaldin A, Shibolet O, Sokolov S, Souliotis K, Spearman CW, Staub T, Strebkova EA, Struck D, Tomasiewicz K, Undram L, van der Meer AJ, van Santen D, Veldhuijzen I, Villamil FG, Willemse S, Zuure FR, Silva MO, Sypsa V, Gower E. Historical epidemiology of hepatitis C virus (HCV) in select countries - volume 2. J Viral Hepat. 2015 Jan;22(Suppl 1):6–25. doi: 10.1111/jvh.12350. [DOI] [PubMed] [Google Scholar]
- 3.Liakina V, Hamid S, Tanaka J, Olafsson S, Sharara AI, Alavian SM, Gheorghe L, El Hassan ES, Abaalkhail F, Abbas Z, Abdou A, Abourached A, Al Braiki F, Al Hosani F, Al Jaberi K, Al Khatry M, Al Mulla MA, Al Quraishi H, Al Rifai A, Al Serkal Y, Alam A, Alashgar HI, Alawadhi S, Al-Dabal L, Aldins P, Alfaleh FZ, Alghamdi AS, Al-Hakeem R, Aljumah AA, Almessabi A, Alqutub AN, Alswat KA, Altraif I, Alzaabi M, Andrea N, Assiri AM, Babatin MA, Baqir A, Barakat MT, Bergmann OM, Bizri AR, Blach S, Chaudhry A, Choi MS, Diab T, Djauzi S, El Khoury S, Estes C, Fakhry S, Farooqi JI, Fridjonsdottir H, Gani RA, Ghafoor Khan A, Goldis A, Gottfredsson M, Gregorcic S, Hajarizadeh B, Han KH, Hasan I, Hashim A, Horvath G, Hunyady B, Husni R, Jafri W, Jeruma A, Jonasson JG, Karlsdottir B, Kim DY, Kim YS, Koutoubi Z, Lesmana LA, Lim YS, Löve A, Maimets M, Makara M, Malekzadeh R, Matičič M, Memon MS, Merat S, Mokhbat JE, Mourad FH, Muljono DH, Nawaz A, Nugrahini N, Priohutomo S, Qureshi H, Rassam P, Razavi H, Razavi-Shearer D, Razavi-Shearer K, Rozentale B, Sadik M, Saeed K, Salamat A, Salupere R, Sanai FM, Sulaiman AS, Sayegh RA, Schmelzer JD, Sibley A, Siddiq M, Siddiqui AM, Sigmundsdottir G, Sigurdardottir B, Speiciene D, Sulaiman A, Sultan MA, Taha M, Tarifi H, Tayyab G, Tolmane I, Ud Din M, Umar M, Valantinas J, Videčnik-Zorman J, Yaghi C, Yunihastuti E, Yusuf MA, Zuberi BF, Gunter J. Historical epidemiology of hepatitis C virus (HCV) in select countries - volume 3. J Viral Hepat. 2015 Dec;22(Suppl 4):4–20. doi: 10.1111/jvh.12475. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization . Global Hepatitis Report, 2017. Geneva: World Health Organization; 2017. [Google Scholar]
- 5.Sangiovanni A, Prati GM, Fasani P, Ronchi G, Romeo R, Manini M, Del Ninno E, Morabito A, Colombo M. The natural history of compensated cirrhosis due to hepatitis C virus: A 17-year cohort study of 214 patients. Hepatology. 2006 Jun;43(6):1303–10. doi: 10.1002/hep.21176. [DOI] [PubMed] [Google Scholar]
- 6.Zibbell JE, Asher AK, Patel RC, Kupronis B, Iqbal K, Ward JW, Holtzman D. Increases in acute hepatitis C virus infection related to a growing opioid epidemic and associated injection drug use, United States, 2004 to 2014. Am J Public Health. 2018 Feb;108(2):175–81. doi: 10.2105/AJPH.2017.304132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Harvoni (R) (ledipasvir and sofosbuvir) package insert. Accessed June 11, 2019 https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212477s000lbl.pdf.
- 8.Buggisch P, Vermehren J, Mauss S, Günther R, Schott E, Pathil A, Boeker K, Zimmermann T, Teuber G, Vornkahl H, Simon K, Niederau C, Wedemeyer H, Zeuzem S. Real-world effectiveness of 8-week treatment with ledipasvir/sofosbuvir in chronic hepatitis C. J Hepatol. 2018 Apr;68(4):663–71. doi: 10.1016/j.jhep.2017.11.009. [DOI] [PubMed] [Google Scholar]
- 9.Rosenthal E, Hill K, Nussdorf L, Mathur P, Gross C, Silk R, Akoth E, Sternberg D, Sidique N, Chaudhury C, Emmanuel B, Masur H, Kottilil S, Kattakuzhy S. Collocation of Buprenorphine with HCV treatment to improve adherence and reduce harm in PWID with HCV: Preliminary data from the ANCHOR study. J Hepatology. 2018;68:S51–13. doi: 10.1016/s0168-8278(18)30322-2. http://www.natap.org/2018/AASLD/AASLD_15.htm. [DOI] [Google Scholar]
- 10.Browne SH, Peloquin C, Santillo F, Haubrich R, Muttera L, Moser K, Savage GM, Benson CA, Blaschke TF. Digitizing medicines for remote capture of oral medication adherence using co-encapsulation. Clin Pharmacol Ther. 2018 Mar;103(3):502–10. doi: 10.1002/cpt.760. http://europepmc.org/abstract/MED/28597911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Curry MP, Tapper EB, Bacon B, Dieterich D, Flamm SL, Guest L, Kowdley KV, Lee Y, Milligan S, Tsai N, Younossi Z, Afdhal NH. Effectiveness of 8- or 12-weeks of ledipasvir and sofosbuvir in real-world treatment-naïve, genotype 1 hepatitis C infected patients. Aliment Pharmacol Ther. 2017 Sep;46(5):540–8. doi: 10.1111/apt.14204. doi: 10.1111/apt.14204. [DOI] [PubMed] [Google Scholar]
- 12.Younossi ZM, Stepanova M, Henry L, Nader F, Younossi Y, Hunt S. Adherence to treatment of chronic hepatitis C: from interferon containing regimens to interferon and ribavirin free regimens. Medicine (Baltimore) 2016 Jul;95(28):e4151. doi: 10.1097/MD.0000000000004151. doi: 10.1097/MD.0000000000004151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Petersen T, Townsend K, Gordon LA, Sidharthan S, Silk R, Nelson A, Gross C, Calderón M, Proschan M, Osinusi A, Polis MA, Masur H, Kottilil S, Kohli A. High adherence to all-oral directly acting antiviral HCV therapy among an inner-city patient population in a phase 2a study. Hepatol Int. 2016 Mar;10(2):310–9. doi: 10.1007/s12072-015-9680-7. http://europepmc.org/abstract/MED/26612014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McHutchison JG, Poynard T, Esteban-Mur R, Davis GL, Goodman ZD, Harvey J, Ling M, Garaud JJ, Albrecht JK, Patel K, Dienstag JL, Morgan T, International Hepatitis Interventional Therapy Group Hepatic HCV RNA before and after treatment with interferon alone or combined with ribavirin. Hepatology. 2002 Mar;35(3):688–93. doi: 10.1053/jhep.2002.31870. [DOI] [PubMed] [Google Scholar]
- 15.Altstadt AR, Holznecht C, Rahman SI, Rein L, Szabo A, Saeian K. Non-adherence diminishes real-world SVR12 in an inter-disciplinary care clinic. Gastroenterology. 2016;150(4):S1039. doi: 10.1016/S0016-5085(16)33512-0. doi: 10.1016/S0016-5085(16)33512-0. [DOI] [Google Scholar]
- 16.Blaschke TF, Osterberg L, Vrijens B, Urquhart J. Adherence to medications: insights arising from studies on the unreliable link between prescribed and actual drug dosing histories. Annu Rev Pharmacol Toxicol. 2012;52:275–301. doi: 10.1146/annurev-pharmtox-011711-113247. [DOI] [PubMed] [Google Scholar]
- 17.Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi: 10.1155/2015/217047. doi: 10.1155/2015/217047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006 May 16;144(10):705–14. doi: 10.7326/0003-4819-144-10-200605160-00004. [DOI] [PubMed] [Google Scholar]
- 19.Veterans Administration Office of Public Health/Population Health and VA Pharmacy Benefits Management Services. 2018. Aug, Report: Treating Hepatitis C in Veterans Affairs (VA)arly Experience with Sofosbuvir-based Regimes https://www.hepatitis.va.gov/pdf/treatment-considerations-2018-08-27.pdf.
- 20.Zhu VJ, Tu W, Rosenman MB, Overhage JM. A comparison of data driven-based measures of adherence to oral hypoglycemic agents in Medicaid patients. AMIA Annu Symp Proc. 2014;2014:1294–301. http://europepmc.org/abstract/MED/25954441. [PMC free article] [PubMed] [Google Scholar]
- 21.Weiss JJ, Bräu N, Stivala A, Swan T, Fishbein D. Review article: adherence to medication for chronic hepatitis C - building on the model of human immunodeficiency virus antiretroviral adherence research. Aliment Pharmacol Ther. 2009 Jul;30(1):14–27. doi: 10.1111/j.1365-2036.2009.04004.x. doi: 10.1111/j.1365-2036.2009.04004.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wagner GJ, Ryan GW. Hepatitis C virus treatment decision-making in the context of HIV co-infection: the role of medical, behavioral and mental health factors in assessing treatment readiness. AIDS. 2005 Oct;19(Suppl 3):S190–8. doi: 10.1097/01.aids.0000192089.54130.b6. [DOI] [PubMed] [Google Scholar]
- 23.Martín-Santos R, Díez-Quevedo C, Castellví P, Navinés R, Miquel M, Masnou H, Soler A, Ardevol M, García F, Galeras JA, Planas R, Solà R. De novo depression and anxiety disorders and influence on adherence during peginterferon-alpha-2a and ribavirin treatment in patients with hepatitis C. Aliment Pharmacol Ther. 2008 Feb 1;27(3):257–65. doi: 10.1111/j.1365-2036.2007.03568.x. doi: 10.1111/j.1365-2036.2007.03568.x. [DOI] [PubMed] [Google Scholar]
- 24.Frias J, Virdi N, Raja P, Kim Y, Savage G, Osterberg L. Effectiveness of digital medicines to improve clinical outcomes in patients with uncontrolled hypertension and type 2 diabetes: prospective, open-label, cluster-randomized pilot clinical trial. J Med Internet Res. 2017 Jul 11;19(7):e246. doi: 10.2196/jmir.7833. https://www.jmir.org/2017/7/e246/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Browne S, Moser K, Low J, Vaida F, Tucker-Maytom A, Gonzalez-Garcia J. Wirelessly observed therapy is accurate and confirms more TB medication doses than directly observed therapy. Int J Tuberc Lung Dis. 2017;21(11, Suppl2):S65. http://www.abstractserver.com/TheUnion2017/TheUnion2017_Abstracts_Web.pdf. [Google Scholar]
- 26.Hafezi H, Robertson TL, Moon GD, Au-Yeung K, Zdeblick MJ, Savage GM. An ingestible sensor for measuring medication adherence. IEEE Trans Biomed Eng. 2015 Jan;62(1):99–109. doi: 10.1109/TBME.2014.2341272. [DOI] [PubMed] [Google Scholar]
- 27.Choudhry NK, Krumme AA, Ercole PM, Girdish C, Tong AY, Khan NF, Brennan TA, Matlin OS, Shrank WH, Franklin JM. Effect of reminder devices on medication adherence: The REMIND randomized clinical trial. JAMA Intern Med. 2017 May 1;177(5):624–31. doi: 10.1001/jamainternmed.2016.9627. http://europepmc.org/abstract/MED/28241271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.McHutchison JG, Manns M, Patel K, Poynard T, Lindsay KL, Trepo C, Dienstag J, Lee WM, Mak C, Garaud J, Albrecht JK, International Hepatitis Interventional Therapy Group Adherence to combination therapy enhances sustained response in genotype-1-infected patients with chronic hepatitis C. Gastroenterology. 2002 Oct;123(4):1061–9. doi: 10.1053/gast.2002.35950. [DOI] [PubMed] [Google Scholar]
- 29.Moreno GA, Wang A, González YS, Espinosa OD, Vania DK, Edlin BR, Brookmeyer R. Value of comprehensive HCV treatment among vulnerable, high-risk populations. Value Health. 2017 Jun;20(6):736–44. doi: 10.1016/j.jval.2017.01.015. https://linkinghub.elsevier.com/retrieve/pii/S1098-3015(17)30085-2. [DOI] [PubMed] [Google Scholar]