

Abstract
Although Indoleamine 2,3-dioxygenase (IDO), tryptophan-2,3-dioxygenase (TDO), and aryl hydrocarbon receptor (AHR) are involved in cancer immune escape, their prognostic impact on diffuse large B-cell lymphoma (DLBCL) is unknown.
To examine the prognostic impact of IDO, TDO, and AHR on patients with DLBCL.
This was a retrospective study on treatment-naïve patients with newly diagnosed DLBCL at the Henan Province People's Hospital between 01/2012 and 06/2015. Patients with inflammatory reactive lymph nodes were included as controls. All cases were reviewed by 2 pathologists. IDO, TDO, and AHR positivity was determined through immunochemistry. Survival was examined using the Kaplan-Meier method and multivariable Cox analyses.
The positive expression of TDO (50.0% vs 16.7%, P = .005) and AHR (60.0% vs 8.3%, P < .001) were higher in DLBCL than in inflammatory control. The overall survival of IDO, TDO, and AHR positive expression in DLBCL patients was 34.6, 26.7, and 32.2 months, respectively, which is significantly shorter than that of the corresponding negative patients (49.0 months, P = .04; 58.2 months, P < .001; 58.0 months, P < .001; respectively). The multivariable analysis showed that TDO expression and Ann-Arbor stage were independently associated with PFS (TDO: HR = 8.347, 95%CI: 2.992–23.289, P < .001; stage: HR = 2.729, 95%CI: 1.571–4.739, P < .001) and OS (TDO: HR = 9.953, 95%CI: 3.228–30.686, P < .001; stage: HR = 2.681, 95%CI: 1.524–4.719, P = .001) in DLBCL patients.
Overexpression of IDO, TDO, and AHR is associated with poor survival of patients with DLBCL and could be involved in the immune escape of cancer cells. Further studies are necessary to determine whether these proteins can be targeted by treatment regimens.
Keywords: aryl hydrocarbon receptor; diffuse; indoleamine 2,3-dioxygenase; large B-cell; lymphoma; prognosis; tryptophan-2,3-dioxygenase
1. Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoid malignancy in adults, representing 30% to 40% of all newly diagnosed non-Hodgkin lymphomas and 37% of B-cell lymphomas.[1–3] Clinically, it is a heterogeneous class of B-cell lymphoma that is typically aggressive or advanced but is often curable even in advanced stages.[1–3] Recently, the treatment of DLBCL has improved owing to the development of targeted drugs that can treat this disease effectively.[4]
The management of DLBCL usually includes induction therapy combined with R-CHOP (Rituximab (R); cyclophosphamide (C); Adriamycin (H); vincristine (O); prednisone (P)) chemoimmunotherapy regimen and/or radiation therapy of the involved sites.[1–3] Therapy for relapsed or refractory disease is determined based on whether the patient is a suitable candidate for high-dose therapy or not.[1] The 5-year survival of patients who received CHOP is low; however, rituximab, which is included in the R-CHOP regimen, has revolutionized the management of DLBCL since its approval more than 20 years ago and is now part of the routine induction and maintenance therapies for DLBCL.[5] Nevertheless, rituximab is ineffective in a few patients; hence, it is necessary to distinguish these patients. The 5-year survival of patients with DLBCL in the United States is 62.8%.[4] Although the management of this disease has improved over the years, with a 5-year survival of 42% from 1997 to 1999 to 55% from 2006 to 2008 in Europe,[6] many patients are still unresponsive or poorly responsive to treatment, and their prognosis is dismal.
Certain cancers display sustained proliferative signaling and/or insensitivity to growth suppressors, and accordingly, the poor response to treatment seen in some patients can be explained.[7–9] Another emerging hallmark of cancer is its ability to evade immune system destruction (10, 11). There is significant evidence showing that both innate and adaptive immunity play crucial roles in eliminating nascent transformed cells.[12–14] Indoleamine 2,3-dioxygenase (IDO) exerts immunomodulatory effects due to its enzymatic activities catalyzing the essential amino acid L-tryptophan. IDO activity might play an important role in regulating immune responses exerted by antigen-presenting cells as a potent tool to help escape from the immune system.[15] Some cancer types use the tryptophan-catabolizing enzyme, tryptophan-2,3-dioxygenase (TDO), to inhibit CD8+ T cells.[16] The aryl hydrocarbon receptor (AHR) is involved in the oncogenesis, progression, invasion, and metastasis of cancers. In addition, AHR has been shown to be an immunosuppressive effector in the cancer microenvironment.[17] Elevated IDO1 and TDO activity and kynurenine levels are associated with increased tumor grade and poor prognosis in many cancers.[18]
Therefore, the overexpression of these enzymes is associated with cancer immune escape and tumor growth, but data about their prognostic impact on hematological cancers such as DLBCL are lacking. Hence, the present study aimed to examine the prognostic impact of IDO, TDO, and AHR overexpression in patients with DLBCL. The results could suggest eventual novel targets that can be utilized for managing DLBCL.
1.1. Study design and patients
A retrospective study of patients diagnosed with DLBCL was conducted at the Department of Pathology of Henan Province People's Hospital between January 2012 and June 2015. The study was approved by the ethics committee of Henan Province People's Hospital, and the need for individual consent was waived by the committee.
All cases were histologically reviewed by 2 senior pathologists, according to the World Health Organization classification of tumors of hematopoietic and lymphoid tissues to confirm the diagnosis.[19] The inclusion criteria were as follows:
-
(1)
DLBCL diagnosis,
-
(2)
no prior cancer treatment, and
-
(3)
received R-CHOP chemoimmunotherapy.
The exclusion criteria were as follows:
-
(1)
primary DLBCL in the mediastinum, the skin, or the central nervous system;
-
(2)
HIV positive; or
-
(3)
incomplete follow-up data.
Patients with chronic inflammatory lymph nodes diagnosed during the same study period in the same hospital were included as inflammatory controls (including reactive hyperplastic lymph nodes).
All patients with DLBCL received R-CHOP as induction therapy as follows: rituximab, 375 mg/m2, day 0; adriamycin, 50 mg/m2, day 1; cyclophosphamide, 750 mg/m2, day 1; vincristine, 1.4 mg/m2, day 1; and prednisone, 100 mg/d, days 1 to 5. The patients received at least 6 cycles of the treatment. The response was evaluated with fluorine-18 2-fluoro-2-deoxyglucose PET and computed tomography ((18)F-FDG PET/CT). The definition of complete remission (CR) was determined by the reduction of the palpable mass to a normal size lymph node by CT with negative FDG-PET. FDG-PET was evaluated according to the criteria of the standardized uptake value.[20] Partial remission (PR) required a reduction of at least 50% in the sum of the products of the dimensions on CT with positive FDG-PET in the absence of newly developed lesions.
1.2. Immunohistochemistry (IHC)
Paraffin-embedded tissue sections of 3 to 5 μm in size were processed for hematoxylin & eosin staining and for IDO, TDO, and AHR IHC. After deparaffinization, heat-induced antigen retrieval was performed using citrate buffer, pH 6.0 (CC1 protocol, Ventana, Roche Diagnostics, Basel, Switzerland). IHC for IDO (clone 10.1, Chemicon, Temecula, CA), TDO, (Clone 1D1, Abcam, Cambridge, United Kingdom), and AHR (Clone RPT9, Abcam, Cambridge, United Kingdom) was performed according to the manufacturer's instruction of the SP (Biotin-Peroxidase Linking of Streptomyces) supersensitive kit (Fuzhou MaiXin Biotechnology Development Co, Fuzhou, China).
IHC-positive cells showed yellow particles in the cytoplasm or nucleus. According to the Fromwitz comprehensive scoring method, under high magnification (400×), 5 to 10 independent and mutually exclusive fields were selected to count 100 to 200 cancer cells, for a total of 1000 cancer cells. The percentage of positive cells was calculated as (positive cells / total cancer cell number) × 100%. The tissue was considered positive for IDO, TDO, or AHR if there was histological evidence of cell staining in at least 5% of the tumor cells.[21] The slides were reviewed by 2 pathologists using a double-headed microscope. When there was a discrepancy in scoring (most commonly 0% vs 5%), a third pathologist was invited.
1.3. Statistical analysis
Statistical analysis was performed using SPSS 21.0 (IBM, Armonk, NY,). The associations between the expression of IDO, TDO, or AHR and clinical and pathologic variables were assessed using the chi-square test or Fisher exact test. The progression-free survival (PFS) was calculated from the date of the final diagnosis to the date of death or relapse of DLBCL. The overall survival (OS) was calculated from the date of the final diagnosis to the date of death. Kaplan–Meier method was used to estimate the probability of survival, and the level of significance was assessed using the log-rank test. Multivariable analysis was carried out using the Cox regression model. A two-sided P value <.05 was considered statistically significant in all analyses.
2. Results
2.1. Patient characteristics
Sixty patients with DLBCL consisting of 42 males and 18 females were included in this study, and they were aged between 24 and 81 years (median of 56 years). The 24 patients in the control group included 15 males and 9 females, and they were aged between 6 and 73 years (median of 40 years). Based on the immunohistochemical Hans model,[22] there were 28 cases of germinal center B cells, and 32 cases of non-germinal center B cells. Thirty-three patients (55.0%) were Ann Arbor stage III or IV.
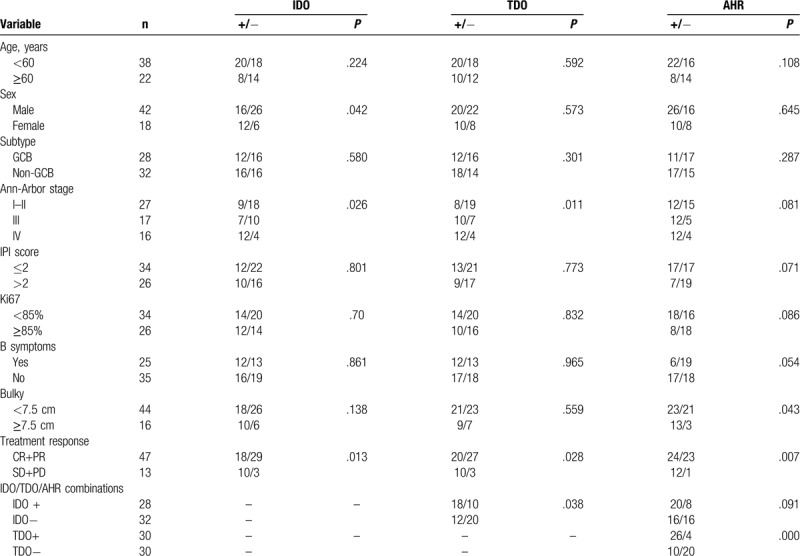
All patients received chemotherapy with 6 or 8 courses of R-CHOP, with or without adjuvant radiotherapy. Treatment response was evaluated after four courses of treatment, and follow-up was censored in December 2018. The median follow-up for all DLBCL patients was 35 months (range: 10–70 months). Overall clinicopathological characteristics and IHC results of the patients are summarized in Table 1.
Table 1.
Characteristics of the patients with DLBCL.
2.2. Protein expression of IDO, TDO, and AHR
The positive protein expression of IDO and TDO was identified based on the presence of light brown particles in the cytoplasm of cancer cells (Fig. 1). The staining pattern of AHR was largely cytoplasmic and nuclear (Fig. 1).
Figure 1.
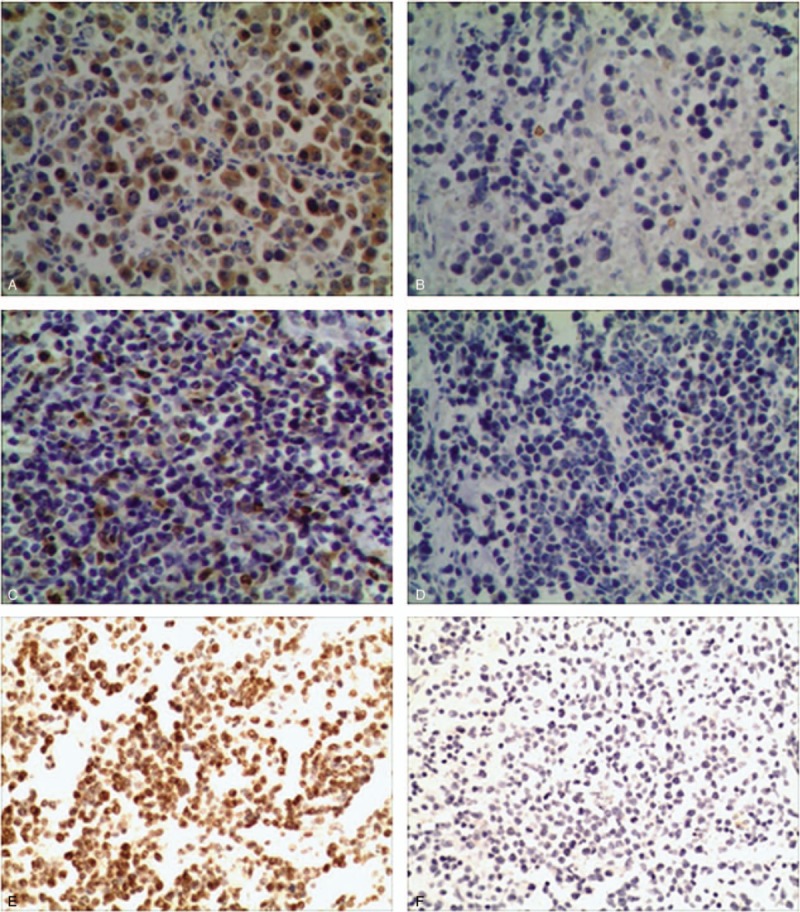
Staining patterns of IDO, TDO, and AHR in diffuse large B-cell lymphoma. (A) Positive for IDO. (B) Negative for IDO. (C) Positive for TDO. (D) Negative for TDO. (E) Positive for AHR. (F) Negative for AHR. AHR = aryl hydrocarbon receptor, IDO = Indoleamine 2,3-dioxygenase, TDO = tryptophan-2,3-dioxygenase.
The positive expression rates of IDO were 46.7% (28/60) in DLBCL and 25% (6/24) in inflammatory controls (P = .068). The positive expression rates of TDO were higher in DLBCL (50.0%) than in inflammatory control (16.7%, P = .005). In addition, the positive expression rates of AHR were higher in DLBCL (60.0%) than in inflammatory control (8.3%, P < .001).
2.3. Associations between the expression of IDO, TDO, or AHR and clinicopathological characteristics of DLBCL
We compared the associations between the expression of IDO, TDO, or AHR and the clinicopathological characteristics of DLBCL (Table 1). The expression rate of IDO was significantly higher in female patients (66.7%) than in male patients (38.1%, P = .042). With advancing Ann Arbor stages (III or IV), the positive rates of IDO and TDO were higher than Ann Arbor stages I and II (P < .05). High AHR expression in patients with bulkiness (P = .043). Patients with low IDO, TDO, and AHR expression rates had better treatment response (CR + PR, complete remission + PR) than those with high IDO, TDO, and AHR expression rates (P < .05).
2.4. Overall survival according to IDO, TDO, and AHR
The OS of IDO-positive, TDO-positive, and AHR-positive DLBCL patients was 34.6, 26.7, and 32.2 months, respectively, which was significantly shorter than that of the corresponding negative patients (49.0 months, P = .04; 58.2 months, P < .001; 58.0 months, P < .001; respectively) (Fig. 2A–C). Patients with positive AHR, IDO, and/or TDO had poor OS compared to those with AHR expression alone (27.6 vs 56.7 months, P < .001) (Fig. 2D). The patients with positive expression of all 3 biomarkers had the worst OS. However, patients with negative expression of all 3 biomarkers had the best OS, while patients with inconsistent results had an intermediary OS (22.1 vs 61.7 vs 42.8 months, P < .001) (Fig. 2E).
Figure 2.
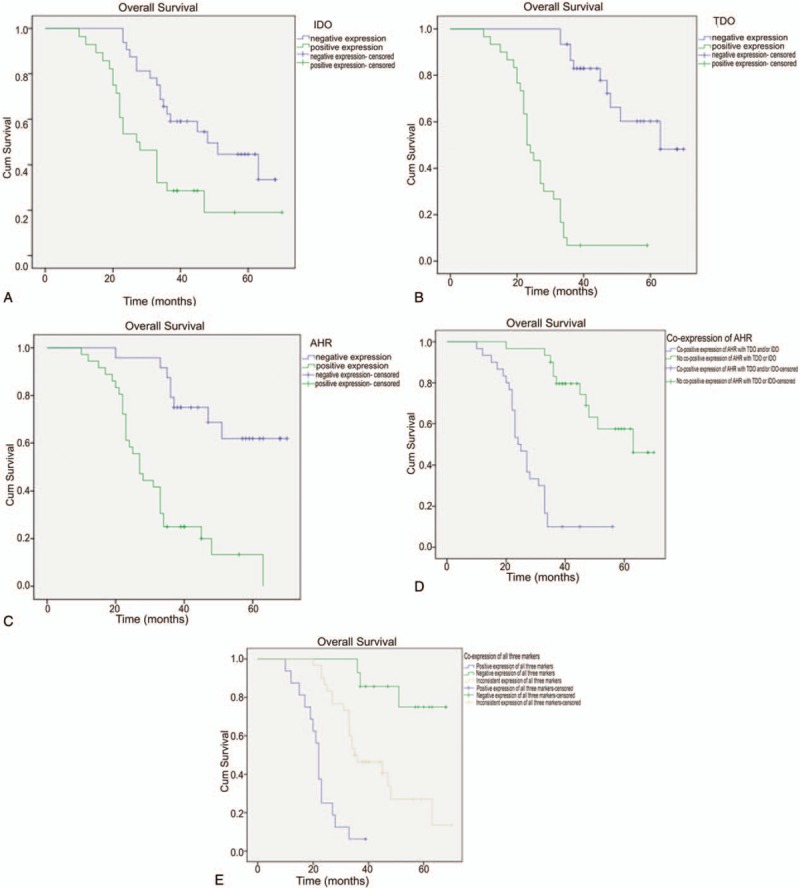
Overall survival analysis of patients positive for IDO. (A; P = .004), TDO (B; P < .001), and AHR (C; P < .001). (D) OS of patients with AHR expression combined with positive IDO and/or TDO (blue line) vs AHR expression alone (green line) (P < .001). (E) OS of patients with positive expression of all 3 markers (IDO, TDO, and AHR; blue line) vs negative expression of all 3 markers (green line) vs inconsistent expression among the 3 markers (yellow line) (P < .001).
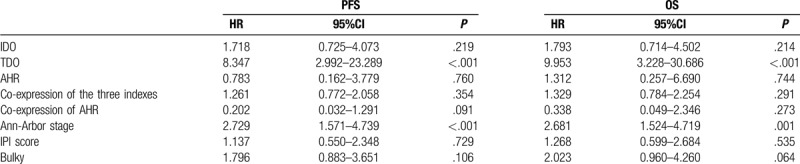
2.5. Multivariable analysis
The multivariable analysis (Table 2) showed that TDO expression (HR = 8.347, 95%CI: 2.992–23.289, P < .001) and Ann-Arbor stage (HR = 2.729, 95%CI: 1.571–4.739, P < .001) were independently associated with PFS in DLBCL patients. In addition, TDO expression (HR = 9.953, 95%CI: 3.228–30.686, P < .001) and Ann-Arbor stage (HR = 2.681, 95%CI: 1.524–4.719, P = .001) were independently associated with OS in DLBCL patients.
Table 2.
Multivariable analyses of PFS and OS in patients with DLBCL variables.
3. Discussion
Immune escape is the hallmark of malignant tumors, and the understanding of natural immune responses to cancer has improved in recent years. Tumor cells might escape or attenuate this immune response in the following ways:
-
(1)
lack of T cell recognition of tumor through impaired antigen presentation on the tumor surface;
-
(2)
lack of T cell recognition of tumor due to mutations in MHC genes or genes needed for antigen processing;
-
(3)
inhibition of T cell activation through the production of immunosuppressive proteins.[10–14]
In addition, some signaling networks are dysregulated and thus contribute to malignant transformation and tumor maintenance. Indeed, in DLBCL, B-cell antigen receptor signals are rewired in certain lymphoma types and promote cell growth and survival of the malignant cell clones.[23] In chronic neutrophilic leukemia (CNL) and acute myeloid leukemia (AML), by analyzing phosphoproteomics of mutated granulocyte colony-stimulating factor receptor (G-CSFR), it was discovered that the existing effective drugs could kill the cells with the mutated receptor.[24,25] Tumor cells may activate some response pathways to environmental stress, such as oxidative stress,[26] so that they can survive in harsh environments and spread to distant places. Therefore, many kinds of proteins and pathways are involved in the development of tumors, especially the immune escape of tumors, but the present study focused on IDO, TDO, and AHR, which are known to possess immunomodulatory effects.[15–17]
IDO, TDO, and AHR are involved in cancer immune escape,[17,19,21] but their impact on the prognosis of DLBCL is unknown. Therefore, this study aimed to examine the prognostic impact of IDO, TDO, and AHR overexpression on patients with DLBCL. The results strongly suggest that the overexpression of IDO, TDO, and AHR is associated with low survival of patients with DLBCL and could be involved in the immune escape of cancer cells. Further studies are required to determine whether these proteins can be targeted by treatment regimens.
Hosts possess T cells that are specific to tumor antigens and can participate in tumor rejection, but the tumors can evolve to escape those T cells.[27] Tryptophan metabolism has been suggested to participate in this process of immune escape from T cells.[28] IDO degrades tryptophan into kynurenine, and this metabolite inhibits T cell proliferation and induces T cell apoptosis.[29,30] IDO can not only be expressed by tumor cells,[31] but also by dendritic cells found in tumor-draining lymph nodes.[32] Previous studies showed that the serum levels of kynurenine were elevated in patients with T cell lymphoma and had prognostic significance in patients treated with R-CHOP.[33,34] A similar relationship was also observed in DLBCL,[15] and in solid tumors.[35,36] In the present study, patients with IDO-positive DLBCL had a shorter PFS than those with IDO-negative DLBCL (35 vs 49 months), as supported by previous studies.[15] Kryachok et al[37] showed that IDO expression correlated with disease progression and prognosis of patients with DLBCL, particularly in those affected with the ABC subtype. Moreover, Nam et al[38] showed that IDO-positive cells were associated with better prognosis in patients with central nervous system DLBCL. While previous studies suggest that IDO positivity can be associated with either worse or better prognosis. This can be due to a number of factors, such as the subtype of DLBCL and the site being involved. Hence, additional studies are necessary to examine the exact role of IDO in cancer. The answer may come from many clinical trials on IDO inhibition that are currently in progress.[35]
TDO is a functional ortholog to IDO and catalyzes the same reaction, but its expression is normally restricted to the liver, where it plays a role in regulating the serum tryptophan levels.[39] Greene et al[16] revealed the possible involvement of TDO in breast cancer prognosis, particularly estrogen receptor-negative stage III-IV breast cancer. The present study is the first to show an independent association of TDO expression with PFS in patients with DLBCL. Previous studies showed that low serum tryptophan levels were associated with poor prognosis in a number of cancer types,[40–42] but it is unknown whether this is due to enhanced tryptophan catabolism by the liver or by the cancer cells. Additional studies will be needed to examine this issue.
AHR is involved in cancer development and is an immunosuppressive effector in cancer microenvironment.[17] More specifically, it is an immunosuppressive effector of T cells and dendritic cells.[43] AHR overexpression can enhance the proliferation, invasion, metastasis, and angiogenesis of cancer cells,[44] but the exact mechanisms of tumor immune escape by AHR remains poorly understood.[17] Nevertheless, kynurenine produced by IDO and TDO is known to activate AHR, which in turn controls the expression of IDO and TDO.[45] This vicious circle can rapidly lead to tryptophan depletion in the tumor microenvironment, suppressing T cell responses, and promoting the differentiation of regulatory T cells, thereby participating in tumor immune escape.[44,45] As demonstrated in the present study, DLBCL patients positive for IDO, TDO, and AHR had a worse prognosis than those with negative IDO, TDO, and/or AHR. A previous study showed that AHR is activated in 14% to 24% of lymphomas, but without a specific pattern, according to subtypes.[46] In the present study, the frequencies of IDO, TDO, and AHR positivity were higher in patients with DLBCL than in patients with inflammatory lymph nodes, supporting the involvement of the IDO/TDO/AHR axis in DLBCL development. Nevertheless, the discrepancies among studies could be due to the subtype of DLBCL, the site where DLBCL occurs, or the intrinsic genetics associated with the studied population. This will need to be explored in future studies.
The present study has a few limitations. This was a retrospective study of archived tissue specimens, and no serum was available to examine serum tryptophan and kynurenine levels. In addition, the sample size was relatively small and limited to a single type of lymphoma. All patients were treated with R-CHOP, and untreated patients were not included. Additional studies on cell lines should provide additional mechanistic insights for the involvement of the IDO/TDO/AHR axis in cancer immune escape.
In conclusion, the overexpression of IDO, TDO, and AHR is associated with low survival of patients with DLBCL and could be involved in the immune escape of cancer cells. Further studies are necessary to determine whether these proteins could be targeted by treatment regimens.
Author contributions
Xiangli Chen and Yuzhu Zang conceived and designed research; Jianmin Guo, Yin Zhang and Yacai Wang collected data and conducted research; Dujuan Li, Yacai Wang and Yuqi Lin were responsible for immunohistochemistry and pathological section reading; Xiangli Chen, Yuqi Lin and Zhenghong Wei wrote the initial paper; Xiangli Chen revised the paper; Xiangli Chen had primary responsibility for final content. All authors read and approved the final manuscript.
Footnotes
Abbreviations: AHR = aryl hydrocarbon receptor, CR = complete remission, DLBCL = diffuse large B-cell lymphoma, IDO = Indoleamine 2,3-dioxygenase, IHC = immunohistochemistry, OS = overall survival, PFS = progression-free survival, PR = partial remission, TDO = tryptophan-2,3-dioxygenase.
How to cite this article: Chen X, Zang Y, Li D, Guo J, Wang Y, Lin Y, Wei Z. IDO, TDO, and AHR overexpression is associated with poor outcome in diffuse large B-cell lymphoma patients in the rituximab era. Medicine. 2020;99:21(e19883).
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
This work was supported by the [funding agency #1 National Nature Sciences Found of China] under grant [number 81300417]; [funding agency #2 the Medical Science and Technology Research Key Project of Henan Province] under grant [number 201202019].
The study was approved by the ethics committee of Henan Province People's Hospital. The need for individual consent was waived by the committee.
The authors have no conflicts of interests to disclose.
References
- [1].NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). B-Cell Lymphomas. Version 1.2019. Fort Washington: National Comprehensive Cancer Network; 2018. [Google Scholar]
- [2].Sehn LH, Gascoyne RD. Diffuse large B-cell lymphoma: optimizing outcome in the context of clinical and biologic heterogeneity. Blood 2015;125:22–32. [DOI] [PubMed] [Google Scholar]
- [3].Martelli M, Ferreri AJ, Agostinelli C, et al. Diffuse large B-cell lymphoma. Crit Rev Oncol Hematol 2013;87:146–71. [DOI] [PubMed] [Google Scholar]
- [4].Vermaat JS, Pals ST, Younes A, et al. Precision medicine in diffuse large B-cell lymphoma: hitting the target. Haematologica 2015;100:989–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Salles G, Barrett M, Foa R, et al. Rituximab in B-cell hematologic malignancies: a review of 20 years of clinical experience. Adv Ther 2017;34:2232–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Sant M, Minicozzi P, Mounier M, et al. Survival for haematological malignancies in Europe between 1997 and 2008 by region and age: results of EUROCARE-5, a population-based study. Lancet Oncol 2014;15:931–42. [DOI] [PubMed] [Google Scholar]
- [7].Fouad YA, Aanei C. Revisiting the hallmarks of cancer. Am J Cancer Res 2017;7:1016–36. [PMC free article] [PubMed] [Google Scholar]
- [8].Giancotti FG. Deregulation of cell signaling in cancer. FEBS Lett 2014;588:2558–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Feitelson MA, Arzumanyan A, Kulathinal RJ, et al. Sustained proliferation in cancer: mechanisms and novel therapeutic targets. Semin Cancer Biol 2015;35 Suppl:S25–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Messerschmidt JL, Prendergast GC, Messerschmidt GL. How cancers escape immune destruction and mechanisms of action for the new significantly active immune therapies: helping nonimmunologists decipher recent advances. Oncologist 2016;21:233–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Vinay DS, Ryan EP, Pawelec G, et al. Immune evasion in cancer: mechanistic basis and therapeutic strategies. Semin Cancer Biol 2015;35:S185–98. [DOI] [PubMed] [Google Scholar]
- [12].Gajewski TF, Schreiber H, Fu YX. Innate and adaptive immune cells in the tumor microenvironment. Nat Immunol 2013;14:1014–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Disis ML. Immune regulation of cancer. J Clin Oncol 2010;28:4531–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Grizzi F, Bianchi P, Malesci A, et al. Prognostic value of innate and adaptive immunity in colorectal cancer. World J Gastroenterol 2013;19:174–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Ninomiya S, Hara T, Tsurumi H, et al. Indoleamine 2,3-dioxygenase in tumor tissue indicates prognosis in patients with diffuse large B-cell lymphoma treated with R-CHOP. Ann Hematol 2011;90:409–16. [DOI] [PubMed] [Google Scholar]
- [16].Greene LI, Bruno TC, Christenson JL, et al. A role for tryptophan-2,3-dioxygenase in CD8 T-cell suppression and evidence of tryptophan catabolism in breast cancer patient plasma. Mol Cancer Res 2019;17:131–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Xue P, Fu J, Zhou Y. The aryl hydrocarbon receptor and tumor immunity. Front Immunol 2018;9:286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Reznik E, Luna A, Aksoy BA, et al. A landscape of metabolic variation across tumor types. Cell Syst 2018;6:301–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed.Lyon: International Agency for Research on Cancer; 2008. [Google Scholar]
- [20].Taghipour M, Marcus C, Jones S, et al. The value of fourth and subsequent post-treatment 18F-FDG PET/CT scans in the management of patients with non-Hodgkin's lymphoma. Nucl Med Commun 2016;37:699–704. [DOI] [PubMed] [Google Scholar]
- [21].Choe JY, Yun JY, Jeon YK, et al. Indoleamine 2,3-dioxygenase (IDO) is frequently expressed in stromal cells of Hodgkin lymphoma and is associated with adverse clinical features: a retrospective cohort study. BMC Cancer 2014;14:335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004;103:275–82. [DOI] [PubMed] [Google Scholar]
- [23].Häupl B, Urlaub H, Oellerich T. Phosphoproteomic analysis of signaling pathways in lymphomas. Methods Mol Biol 2019;1956:371–81. [DOI] [PubMed] [Google Scholar]
- [24].Dwivedi P, Muench DE, Wagner M, et al. Time resolved quantitative phospho-tyrosine analysis reveals Bruton's Tyrosine kinase mediated signaling downstream of the mutated granulocyte-colony stimulating factor receptors. Leukemia 2019;33:75–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Dwivedi P, Muench DE, Wagner M, et al. Phospho serine and threonine analysis of normal and mutated granulocyte colony stimulating factor receptors. Sci Data 2019;6:1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Gaman MA, Epingeac ME, Gaman AM. The evaluation of oxidative stress and high-density lipoprotein cholesterol levels in diffuse large B-cell lymphoma. Revista de Chimie 2019;70:977–80. [Google Scholar]
- [27].Boon T, van der Bruggen P. Human tumor antigens recognized by T lymphocytes. J Exp Med 1996;183:725–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Mellor AL, Munn DH. Tryptophan catabolism and T-cell tolerance: immunosuppression by starvation? Immunol Today 1999;20:469–73. [DOI] [PubMed] [Google Scholar]
- [29].Frumento G, Rotondo R, Tonetti M, et al. Tryptophan-derived catabolites are responsible for inhibition of T and natural killer cell proliferation induced by indoleamine 2,3-dioxygenase. J Exp Med 2002;196:459–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Uyttenhove C, Pilotte L, Theate I, et al. Evidence for a tumoral immune resistance mechanism based on tryptophan degradation by indoleamine 2,3-dioxygenase. Nat Med 2003;9:1269–74. [DOI] [PubMed] [Google Scholar]
- [31].Zahm CD, Johnson LE, McNeel DG. Increased indoleamine 2,3-dioxygenase activity and expression in prostate cancer following targeted immunotherapy. Cancer Immunol Immunother 2019;68:1661–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Ye Z, Yue L, Shi J, et al. Role of IDO and TDO in cancers and related diseases and the therapeutic implications. J Cancer 2019;10:2771–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Hoshi M, Ito H, Fujigaki H, et al. Indoleamine 2,3-dioxygenase is highly expressed in human adult T-cell leukemia/lymphoma and chemotherapy changes tryptophan catabolism in serum and reduced activity. Leuk Res 2009;33:39–45. [DOI] [PubMed] [Google Scholar]
- [34].Yoshikawa T, Hara T, Tsurumi H, et al. Serum concentration of L-kynurenine predicts the clinical outcome of patients with diffuse large B-cell lymphoma treated with R-CHOP. Eur J Haematol 2010;84:304–9. [DOI] [PubMed] [Google Scholar]
- [35].Hornyak L, Dobos N, Koncz G, et al. The role of indoleamine-2,3-dioxygenase in cancer development, diagnostics, and therapy. Front Immunol 2018;9:151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Brochez L, Chevolet I, Kruse V. The rationale of indoleamine 2,3-dioxygenase inhibition for cancer therapy. Eur J Cancer 2017;76:167–82. [DOI] [PubMed] [Google Scholar]
- [37].Kryachok I, Skrypets T, Novosad O, et al. The role of indoleamine 2,3-dioxygenase expression in diffuse large B-cell lymphoma prognosis. Ann Oncol 2016;27:313–7. [Google Scholar]
- [38].Nam SJ, Kim S, Kwon D, et al. Prognostic implications of tumor-infiltrating macrophages, M2 macrophages, regulatory T-cells, and indoleamine 2,3-dioxygenase-positive cells in primary diffuse large B-cell lymphoma of the central nervous system. Oncoimmunology 2018;7:e1442164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Zhai L, Spranger S, Binder DC, et al. Molecular pathways: targeting IDO1 and other tryptophan dioxygenases for cancer immunotherapy. Clin Cancer Res 2015;21:5427–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Lyon DE, Walter JM, Starkweather AR, et al. Tryptophan degradation in women with breast cancer: a pilot study. BMC Res Notes 2011;4:156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Tang X, Lin CC, Spasojevic I, et al. A joint analysis of metabolomics and genetics of breast cancer. Breast Cancer Res 2014;16:415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Weinlich G, Murr C, Richardsen L, et al. Decreased serum tryptophan concentration predicts poor prognosis in malignant melanoma patients. Dermatology 2007;214:8–14. [DOI] [PubMed] [Google Scholar]
- [43].Vorderstrasse BA, Kerkvliet NI. 2,3,7,8-Tetrachlorodibenzo-p-dioxin affects the number and function of murine splenic dendritic cells and their expression of accessory molecules. Toxicol Appl Pharmacol 2001;171:117–25. [DOI] [PubMed] [Google Scholar]
- [44].Opitz CA, Litzenburger UM, Sahm F, et al. An endogenous tumour-promoting ligand of the human aryl hydrocarbon receptor. Nature 2011;478:197–203. [DOI] [PubMed] [Google Scholar]
- [45].Platten M, von Knebel Doeberitz N, Oezen I, et al. Cancer immunotherapy by targeting IDO1/TDO and their downstream effectors. Front Immunol 2015;5:673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Sanna S, Satta G, Padoan M, et al. Activation of the aryl hydrocarbon receptor and risk of lymphoma subtypes. Int J Mol Epidemiol Genet 2017;8:40–4. [PMC free article] [PubMed] [Google Scholar]