

Abstract
This study examines the associations of multiple forms of perceived discrimination and negative neighborhood conditions with mental health and retirement age. Respondents aged 51+ from the Health and Retirement Study were selected in 2006 and surveyed through 2014. Ordinary least squares regressions evaluated associations. Bias-corrected bootstrap resampling method tested whether mental health mediated the relationships between disadvantages and retirement age. Major lifetime and work discrimination, as well as neighborhood conditions, were directly associated with earlier retirement. Individuals who did not experience disadvantages retired at age 65, whereas respondents with the highest levels of disadvantage retired earlier (62). Mental health partially mediated relationships between major lifetime discrimination, neighborhood conditions, and work discrimination with retirement age, whereas mental health fully mediated the relationship between everyday discrimination and retirement age. Efforts to promote civil rights, reduce discrimination, and enhance individual resilience may promote mental health and the capacity to work longer.
Keywords: Cumulative Dis/Advantage, Ecological Theory, Discrimination, Retirement
Population aging and the changing social contract on retirement have led to a cultural mantra: work longer (Morrow-Howell, Gonzales, Harootyan, Lee, & Lindberg, 2017; Munnell & Sass, 2008; White House Conference on Aging, 2015). Under the right conditions, engagement with the paid labor force longer in life can result in multiple benefits including improved health, reduced reliance on social insurance programs, increased contributions to the national economy, and stronger economic security for older adults and their families (Calvo, 2006; Calvo, Madero-Cabib, & Staudinger, 2017; Hao, 2008; Munnell & Sass, 2008). Yet, not everyone can work longer. Many employees with low education, poor health, and physically demanding jobs are pushed involuntarily into retirement (Calvo, Madero-Cabib, & Staudinger, 2017; Konig, Lindwall, & Johansson, 2018; Mosca & Barrett, 2016). Mermin, Johnson, & Murphy (2007a, 2007b) speculate that African Americans retire earlier due to discrimination. Krieger (2012) suggests social and economic disadvantages are structural and disproportionately affect minority populations and undermine health and opportunities for productivity in later life (Gonzales, Matz-Costa, Morrow-Howell, 2015).
Yet, a gap in the literature is whether and how cumulative (dis)advantages across ecological domains—including major lifetime discrimination, living in disadvantaged neighborhoods, chronic workplace discrimination, and everyday discrimination—relate to health and the age at which individuals retire. Despite strides in uncovering the relationship between various forms of cumulative (dis)advantage and socially critical outcomes such as well-being and retirement age, a host of gaps in the literature remain to be filled. First, a comparative analysis of numerous forms of cumulative (dis)advantage by race and ethnicity is missing, as racial/ethnic comparisons often take place within the confines of singular constructs. In the current study, we examine experiences of three types of discrimination and two indicators of neighborhood conditions by race and ethnicity. Second, we study the effects of multiple forms of cumulative (dis)advantage - as opposed to only one or two - on socially meaningful outcomes like mental well-being and retirement age. Doing so provides a more comprehensive test of the effects of cumulative disadvantages. Our models also include actual retirement behavior, as opposed to commonly-studied intentions to retire. Given that intentions and actual behavior can conflict, this distinction is important. Finally, an explanation of why cumulative disadvantage seemingly leads to earlier retirement is warranted; what explains this relationship? Drawing on a proposition in the ageism literature (Marchiondo, Gonzales, & Williams, 2018), we test mental health as a mediator in the relationship between various forms of cumulative (dis)advantage and retirement age.
Theory and Evidence
Cumulative (dis)advantage theory suggests that the quality of ecological domains (e.g., neighborhoods, workplaces), combined with psychosocial factors of interpersonal relationships, can improve or compromise health (Krieger, 2012; Dannefer, 2003). Discrimination occurs within and across ecological domains—housing, education, workplaces, neighborhoods, and in public spaces (Blank, Dadaby, & Citro, 2004). Although the research is siloed, there is growing evidence that health is associated with major lifetime discrimination (Ayalon & Gum, 2011); living in disadvantaged neighborhoods (Taylor, Repetti, & Seeman, 1997; Williams & Collins, 2001; Glymour, Mujahid, Wu, White, & Tchetgen Tchetgen, 2010); workplace discrimination (Deitch et al., 2003; Marchiondo, Gonzales, & Ran, 2015; McCluney, Schimtz, Hicken, & Sonnega, 2018); and everyday discrimination (Ayalon & Gum, 2011; Deitch et al., 2003; Lewis Aiello, Leurgans, Kelly, & Barnes 2010; Ong, Williams, Nwizu, & Gruenewald, 2017; Sutin, Stephan, Carretta, & Terracciano, 2015). Discrimination is socially, psychologically and physically stressful and is associated with depression, loneliness, life satisfaction, cognitive functioning, and reduced self-rated health (Han & Richardson, 2015; Luo, Xu, & Granberg, 2012; Sternthal, Slopen, & Williams, 2011; Flores et al., 2008). Studying the long-term relationships of these (dis)advantages with socially and financially meaningful constructs like mental well-being would advance knowledge of their comparative roles in shaping such outcomes – a goal of the current paper.
Only a few studies have combined experiences of discrimination and neighborhood contexts across ecological domains. Ong et al. (2017) utilized primary data from 223 African American adults aged 37-85 to explore health associations with acute and chronic discrimination. Their study revealed everyday mistreatment was associated with higher allostatic load, above and beyond the independent association of lifetime discrimination. Gerber and Sievert’s study in 2018 revealed that neighborhood disorder and social cohesion, as well as everyday discrimination, were associated with a number of adverse physical and mental health outcomes.
Health is a reliable predictor of employment in later life (Cortina, 2008; Munnell & Sass, 2008). One cross-sectional study found that age-based discrimination at work is associated with turnover and desire to retire (Marchiondo et al., 2015). Yet in a longitudinal study, perceived discrimination at work predicted job dissatisfaction, lower self-rated health, and elevated depressive symptoms, but was not associated with working past retirement age (Marchiondo, Gonzales, & Williams, 2018). Marchiondo, Gonzales, and Williams (2018) proposed that health might mediate the relationship between discrimination and retirement, thus explaining the absence of a direct effect in their study. For example, higher rates of disadvantages may lead to higher depressive symptoms and consequently may hasten retirement. Examining health as a potential mediator between disadvantages (perceived discrimination and neighborhood conditions) and retirement age is thus another contribution of the current study. Despite strong financial incentives to work longer among racial and ethnic minorities given a shortfall of retirement savings (Rhee, 2013), risk factors like discrimination may attenuate health—particularly, mental health—and reduce one’s capacity to work longer.
Overall, extant literature has advanced knowledge of the associations between discrimination, facets of health, and some aspects of labor force participation. However, this body of research has important limitations, including cross-sectional designs, sole focus on one or two ecological domains of discrimination, and a paucity of studies examining associations with actual retirement behavior (as opposed to retirement intentions). Additionally, facets of health have been proposed as important mediators in the relationship between disadvantages across ecological domains and retirement age, yet this idea remains untested. We address these limitations in the current study. Guided by cumulative (dis)advantage theory and extant evidence, we hypothesize the following:
-
H1.
Racial and ethnic minorities will report greater levels of disadvantage when compared to Whites.
-
H2.
Racial and ethnic minorities will report lower levels of mental health when compared to Whites.
-
H3.
Cumulative disadvantages are negatively associated with retirement age (i.e., greater levels of disadvantages will result in younger retirement ages).
-
H4.
Cumulative disadvantages are positively associated with depressive symptomology.
-
H5.
Depressive symptomology is negatively associated with retirement age (i.e., higher levels of depressive symptomology will result in younger retirement ages).
-
H6.
Depressive symptomology will mediate the relationship between cumulative disadvantages and retirement age.
Methods
The Health and Retirement Study (HRS) is a longitudinal survey of a representative sample of older adults in the United States and is the premier data source for assessing changes in health, economic and social circumstances. The psychosocial constructs (e.g., major lifetime discrimination, neighborhood conditions, workplace discrimination, everyday discrimination) come from the Leave Behind Questionnaire which uses a rotational study design of a random subsample of the HRS. Baseline characteristics in 2006 were chosen because they have valid and reliable measures of multiple forms of discrimination and significantly more racial and ethnic minorities than in previous years. The remaining variables came from RAND HRS data files version P. Data were analyzed with Stata SE Version 15 and assessed with the survey prefix command (svy). The Leave Behind weight adjusted for population representativeness of older adults within the United States and was utilized for all analyses.
Sample
Individuals aged 51+ who responded to the Leave Behind Questionnaire and reported full-time, part-time, or unemployed in 2006 were selected (n=2,028). Among these adults, 958 retired between 2008 to 2014. The final analytic sample eligible for imputation consisted of 944 participants.
Measures
Retirement age (dependent variable).
Respondents were asked: “Are you working now, temporarily laid off, unemployed and looking for work, disabled and unable to work, retired, a homemaker, or what?” Many studies on retirement have used self-reported retirement status alone, which is an unreliable and imprecise measure. Here, the RAND HRS verified retirement status by cross-checking several survey items such as ‘not working any hours’ or ‘any weeks.’ If respondents answered “retired” and were not working any hours or any weeks, then we selected these individuals and coded them as retired. We then subtracted their birth year from the year of retirement (year of retirement – birth year = age of retirement) to construct the dependent variable. The average age of retirement was 65 (mode = 62; range: 53 - 92 years) and was normally distributed (skewness 0.95).
Major experiences of lifetime discrimination.
Respondents answered a six item scale on unfair treatment (Williams et al., 1997). The instructions read, “For each of the following events, please indicate whether the event occurred AT ANYPOINT IN YOUR LIFE…At any time in your life, have you ever been unfairly dismissed from a job? For unfair reasons, have you ever not been hired for a job? Have you ever been unfairly denied a promotion? Have you ever been unfairly prevented from moving into a neighborhood because the landlord or realtor refused to sell or rent you a house or apartment? Have you ever been unfairly denied a bank loan? Have you ever been unfairly stopped, searched, questioned, physically threatened or abused by the police?” A count of major discrimination is constructed by summing the number of affirmative responses (1=yes, 0=no). Due to skewness, we transformed the variable into the following groups: 1= no experiences (reference), 2 = one lifetime experience, 3 = two or more lifetime experiences. Previous studies have used this measure to understand the relationship between discrimination and health (Kessler, Mickelson & Williams, 1999; Williams et al., 2008; Williams, Yu, Jackson, & Anderson, 1997). However, none of these studies reported the Cronbach’s alpha which indicates the level of internal consistency. Cronbach’s alpha was 0.62.
Neighborhood disadvantage.
Two dimensions were used to measure subjective perceptions of neighborhood context: physical disorder and social cohesion (Glymour et al., 2010). The stem read: “These questions ask how you feel about your local area, that is, everywhere within a 20-minute walk or about a mile of your home” An index of physical disorder (α = 0.68) included average score of four items (vandalism and graffiti, fear to walk alone after dark, area is kept very clean, vacancy or deserted houses or storefronts). Response categories were measured using semantic differential scales ranging from 1 to 7 in which respondents marked the answer closer to a statement the more strongly they agree with it. Items were reverse coded, with higher values indicating greater physical disorder. Social cohesion (α = 0.821) used the average score of four items (I feel part of this area; trust people; people are friendly; people will help you). Similar to physical disorder, original response scales ranged from 1 to 7 in which respondents marked the answer closer to a statement the more strongly they agree with it. A higher score indicated higher levels of social incohesion.
Chronic workplace discrimination.
A six item measure designed to assess chronic discrimination experienced at work was used (Williams, Yu, Jackson, & Anderson, 1997). Respondents were told, “Here are some situations that can arise at work. Please tell me how often you have experienced them during the LAST 12 MONTHS… How often are you unfairly given a task at work that no one else wants to do? How often are you watched more closely than others? How often are you bothered by your supervisor or coworkers making slurs or jokes about women or racial or ethnic groups? How often do you feel that you have to work twice as hard as others at work? How often do you feel that you are ignored or not taken seriously by your boss? How often have you been unfairly humiliated in front of others at work? Response options ranged from 1 (never) to 6 (almost every day). Due to skewness, we transformed the variable to 1 = never (reference), 2 = less than once a year / a few times a year, 3 = a few times a month / at least once a week / almost every day. Cronbach’s alpha was 0.79.
Everyday discrimination.
We used a five item scale that assesses experiences of hassles and incivility associated with perceived everyday discrimination. The instructions read, “In your day-to-day life how often have any of the following things happened to you? You are treated with less courtesy or respect than other people. You receive poorer service than other people at restaurants or stores. People act as if they think you are not smart. People act as if they are afraid of you. You are threatened or harassed.” Original response options ranged from 1 = almost every day to 6 = never. Due to skewness, we transformed the variable to 1 = never (reference), 2 = less than once a year / a few times a year, 3 = a few times a month / at least once a week / almost every day. Cronbach’s α was 0.74. Furthermore, respondents reflected on why they were discriminated against: “What do you think is the main reason for these experiences?” with response options being 1 (your ancestry or national origin), 2 (gender), 3 (race), 4 (age), 5 (religion), 6 (weight), 7 (physical disability), 8 (other aspect of physical appearance), 9 (sexual orientation), and 10 (financial status).
Summative disadvantage scale (SDS).
This measure was constructed by summing major experiences of lifetime discrimination, perceived physical disorder and social incohesion of neighborhoods, and chronic workplace discrimination. Everyday discrimination was excluded from the SDS because it was not associated with retirement age. The theoretical range of the SDS is five to 23, in which higher scores indicate higher disadvantage. Cronbach’s alpha was 0.77.
Mental health.
The Center for Epidemiologic Studies Depression (CES-D) scale was used to assess mental health (eight items that were dichotomized, yes=1, no=0). Sample items include “everything is an effort,” “felt sad,” and “could not get going.” Response options ranged from zero to eight, which is the summed score of the items. Positive items were reverse coded, such that higher values indicated greater depressive symptoms (Cronbach alpha = 0.78).
Race and ethnicity.
Three racial/ethnic groups were constructed: 1 = non-Hispanic Black or African American; 2 = Hispanic, Latinx or Mexican American/Chicanx; and 3 = non-Hispanic White/Caucasian. Non-Hispanic White/Caucasian was the reference group in regressions.
Covariates.
Age cohort (individuals born before 1924; Children of the Depression born 1924 to 1930; Health and Retirement Study Original Cohort born 1931 to 1941; War Baby cohort born 1942 to 1947; Early Baby Boomer cohort born 1948 to 1953; and Mid Baby Boomer cohort born 1954 to 1959), race and ethnicity, gender, education, marital status, total household income, total household assets, and health insurance are associated with retirement age (Munnell & Sass, 2008) and thus included in multivariate models as controls. Household income was log-transformed due to skewness, and total household assets was transformed using the inverse hyperbolic sine function and given positive values. Time was also controlled, given that the Great Recession occurred during this observation period.
Analytic Strategy
Ordinary least squares (OLS) regression models were used to test linear associations between socio-demographic, health, and disadvantage variables (the IVs) with retirement age (the DV). Diagnostics of the OLS models revealed no multicollinearity. Mediation models were performed to investigate whether mental health functioned as a mediator between discrimination and retirement age. Preacher and Hayes’s bias-corrected bootstrapping approach using 5,000 samples was performed to analyze the mediating effect. Bootstrapping reduces the effect of skewness and estimates the indirect effect. Multiple imputation methods were used with Stata Version 15. Non-imputed dated are reported in Table 1, following the suggestions from Curley, Krause, Feiock, and Hawkins (2019).
Table 1.
Univariate Results
| Overall (% or mean (SD)) | White | Black | Hispanic/Latinx | |
|---|---|---|---|---|
| Cohort (n=958) | ||||
| HRS/AHEAD/CODA | 25% | 25% | 24% | 25% |
| War Babies | 40% | 42% a | 31% | 36% |
| Early Baby Boomers | 35% | 33% | 45% | 39% |
| Retirement age (n=958) | 64.90 (0.21) | 65.00 (0.22) | 64.43 (0.37) | 64.66 (0.28) |
| Female (1) (n=958) | 50% | 49% | 55% | 51% |
| Average education (years) (n=956) | 13.33 (0.10) | 13.64 (0.09) ab | 12.67 (0.19) c | 11.10 (0.38) |
| Total household income (n=958) | $96,446 ($6,691) | $106,310 ab ($5,370) | $58,985 ($2,735) | $49,543 ($3,428) |
| Total household assets (n=958) | $466,643 ($39,046) | $ 525,299 ab ($45,882) | $227,801 ($16,651) | $207,955 ($15,349) |
| Marital status (n=958) | ||||
| Married/partnered | 71% | 74% a | 48% c | 67% |
| Not married/partnered | 29% | 26% | 52% | 33% |
| Number of health insurance plans (n=958) | 0.91 (0.02) | 0.95 (0.02) ab | 0.80 (0.04) | 0.73 (0.06) |
| Depressive symptoms (n=946) | 1.29 (0.07) | 1.21 (0.08) | 1.56 (0.13) | 1.58 (0.24) |
| Major lifetime discrimination (n=933) | ||||
| Never experienced | 62% | 64% a | 48% | 63% |
| One lifetime experience | 22% | 22% | 22% | 23% |
| Two or more experiences | 15% | 14% a | 31% c | 14% |
| Neighborhood physical disorder (n=936) | 2.38 (0.05) | 2.22 (0.05) ab | 2.95 (0.10) | 3.17 (0.06) |
| Neighborhood social incohesion (n=928) | 2.56 (0.05) | 2.46 (0.05) a | 2.95 (0.11) | 2.79 (0.08) |
| Chronic work discrimination (n=865) | ||||
| Never experienced | 27% | 26% | 32% | 36% |
| Less than once a year / a few times a year | 39% | 41% b | 33% | 24% |
| A few times a month / once a week / almost everyday | 34% | 33% | 36% | 39% |
| Everyday discrimination (n=951) | ||||
| Never experienced | 20% | 19% b | 22% | 33% |
| Less than once a year / a few times a year | 54% | 57% b | 47% | 38% |
| A few times a month / at least once a week / almost everyday | 26% | 24% | 32% | 29% |
| Summative Disadvantage Scale (n=818) | 8.41 (0.12) | 8.19 ab (0.11) | 9.53 (0.20) | 9.40 (0.19) |
Notes: Race (n=933), Whites=82%, Black= 10%, Hispanics/Latinx=8%
= Statistically significant at p<.05 between Whites and Blacks
= Statistically significant at p<.05 between Whites and Hispanics
= Statistically significant at p<.05 between Blacks and Hispanics
Results
The average age of retirement was 65. There were no statistically significant differences in the retirement age by race and ethnicity. The retirement age range was greater for Whites, reaching age 92, compared to maximum labor force participation ages of 79 for Blacks and 82 for Hispanics.
Disadvantages and Mental Health by Race and Ethnicity
Table 1 provides univariate results. More than half of Blacks (52%) had experienced major lifetime discrimination, compared with 37% of Hispanics (p<.10) and 36% of Whites (p<.05). Three out of ten (31%) Blacks had experienced two or more episodes of major lifetime discrimination, whereas 14% of Whites and Hispanics had experienced this intensity of major lifetime discrimination. Specifically, when compared to Whites, Blacks reported greater rates of unfairly not being hired for a job (p<.05), being denied job promotions (p<.05), prevented from moving into certain neighborhoods (p<.001), denied bank loans (p<.001), and unfairly stopped, searched, questioned, physically threatened or abused by the police (p<.05). When compared to Hispanics, Blacks reported higher rates of being prevented from moving into certain neighborhoods (p<.05) and being denied bank loans (p<.05).
On average, Blacks and Hispanics lived in more physically disadvantageous neighborhoods when compared with Whites (p<.05). On average, Blacks reported higher levels of perceived social incohesion than Whites (p<.05).
Whites, Blacks, and Hispanics reported high rates of chronic discrimination at work. Nearly three-quarters (74%) of Whites reported annual work discrimination, compared 68% of Blacks (68%) and 64% of Hispanics.
Eight out of ten Whites (81%) experienced everyday discrimination in the past year, compared with Blacks (78%, p<.05) and Hispanics (67%, p<.05). The everyday discrimination scale queried about attribution (i.e., main reason for these experiences). Among the entire sample, respondents attributed discrimination to age (28%), gender (16%), weight (12%), race (8%), physical appearance (7%), ancestry (5%), physical disability (4%), and sexual orientation (1%). When stratified by race and ethnicity, the ranking of attribution shifts among minorities. Blacks overwhelmingly reported discrimination due to race (46%), age (14%), gender (11%), and ancestry (11%). Hispanics reported discrimination due to their age (22%), race (18%), ancestry (15%), physical appearance (14%), and gender (12%).
Depressive symptoms were not statistically significant across Whites, Blacks, and Hispanics.
Multivariate Regression Analyses
Major lifetime discrimination was also associated with earlier retirement (Model II). Compared to individuals who had never experienced major lifetime discrimination, those who experienced one or two or more events retired earlier (b= −0.650, p<.05; b= −0.883, p<.01, respectively). Greater neighborhood physical disorder resulted in earlier retirement age (b= −0.267, p<.01, Model III). Similarly, higher levels of social incohesion were associated with earlier retirement (b= −0.315, p<.05, Model IV). Chronic work discrimination related to earlier retirement. Compared to those who never experienced chronic work discrimination, respondents who experienced work discrimination on a yearly basis reported earlier retirement ages (b= −0.913, p<.01; Model V).
Compared to participants who never experienced everyday discrimination, those who experienced this discrimination on a monthly, weekly, or daily basis were trending towards statistical significance of retirement age and in the expected direction (b= −0.818, p<.07; Table 2b, Model VI).
Table 2b.
Associations of Disadvantages and Health with Retirement Age
| Model IV b (SE) |
t | Model V b (SE) |
t | Model VI b (SE) |
t | |
|---|---|---|---|---|---|---|
| Time | 1.540 (0.14) | 10.96 *** | 1.550 (0.14) | 11.43 *** | 1.533 (0.14) | 10.75 *** |
| Cohort (ref=HRS/AHEAD/CODA) | ||||||
| War babies | −5.769 (0.40) | −14.44 *** | −5.758 (0.40) | −14.53 *** | −5.760 (0.40) | −14.46 *** |
| Early Baby Boomers | −10.177 (0.46) | −21.91 *** | −10.208 (0.45) | −22.63 *** | −10.160 (0.45) | −22.53 *** |
| Race (ref=White) | ||||||
| Black/African American | −0.017 (0.40) | −0.04 | −0.158 (0.40) | −0.40 | −0.116 (0.39) | −0.30 |
| Hispanic/Latinx | 0.096 (0.40) | 0.24 | −0.057 (0.41) | −0.14 | −0.022 (0.41) | −0.05 |
| Female (ref) | −1.360 (0.19) | −7.03 *** | −1.291 (0.20) | −6.30 *** | −1.327 (0.20) | −6.49 *** |
| Education (years) | 0.017 (0.05) | 0.34 | 0.035 (0.05) | 0.71 | 0.024 (0.05) | 0.50 |
| Marital status (ref=married) | −0.977 (0.32) | −3.09 ** | −0.929 (0.31) | −2.99 ** | −0.942 (0.31) | −3.06 ** |
| Household income | 0.004 (0.16) | 0.02 | 0.011 (0.16) | 0.07 | 0.021 (0.16) | 0.13 |
| Household assets | 0.003 (0.01) | 0.28 | 0.002 (0.01) | 0.18 | 0.003 (0.01) | 0.28 |
| Health insurance plans | −0.395 (0.23) | −1.70 | −0.312 (0.23) | −1.38 | −0.305 (0.22) | −1.40 |
| Depressive symptoms | −0.229 (0.06) | −3.75 *** | −0.256 (0.07) | −3.93 *** | −0.251 (0.06) | −4.19 *** |
| Social incohesion | −0.315 (0.12) | −2.63 * | ||||
| Work discrimination1 | ||||||
| Less than once a year /a few times a year | −0.913 (0.31) | −2.92 ** | ||||
| A few times a month / once a week /almost everyday | −0.575 (0.36) | −1.61 | ||||
| Everyday discrimination1 | ||||||
| Less than once a year / a few times a year | −0.571 (0.36) | −1.60 | ||||
| A few times a month / at least once a week / almost everyday | −0.818 (0.44) | −1.87 |
Notes:
=p<.001
=p<.01
=p<.05;
=reference group is ‘Never experienced’
Next, we examined the extent to which the SDS predicted retirement age, controlling for mental health and the covariates (Table 3). SDS related to earlier retirement (b= −0.202, p< .001), indicating that every unit increase on the SDS resulted in a 0.20-year reduction in retirement age. This suggests that individuals with no reported disadvantages on the SDS retired at age 65, whereas respondents with the highest levels of disadvantages retired at age 62, controlling for other variables.
Table 3.
Associations between Summative Disadvantages Scale and Retirement Age
| Model VII b (SE) |
t | |
|---|---|---|
| Controls | ||
| Time | 1.543 (0.14) | 10.95 *** |
| Cohort (ref=HRS/AHEAD/CODA) | ||
| War babies | −5.743 (0.40) | −14.32 *** |
| Early Baby Boomers | −10.106 (0.47) | −21.52 *** |
| Race (ref=White/Caucasian) | ||
| Black/African American | 0.102 (0.41) | 0.25 |
| Hispanic/Latinx | 0.166 (0.41) | 0.40 |
| Female (ref) | −1.379 (0.20) | −6.79 *** |
| Education (years) | 0.013 (0.05) | 0.27 |
| Marital status (ref=married) | −0.953 (0.30) | −3.13 ** |
| Household income | −0.062 (0.16) | −0.39 |
| Household assets | 0.005 (0.01) | 0.42 |
| Health insurance plans | −0.414 (0.23) | −1.81 |
| Depressive symptoms | −0.199 (0.06) | −3.27 ** |
| Summative Disadvantage Scale | −0.202 (0.05) | −3.85 *** |
Notes:
=p<.001
=p<.01
=p<.05
Mediation Analyses
Disadvantages and Mental Health.
When compared to individuals who had not experienced major lifetime discrimination, respondents who experienced two or more major episodes of lifetime discrimination reported higher levels of depressive symptoms (b= 0.511, p<.05). Physical disorder of the neighborhood was positively associated with depressive symptoms (b= 0.213, p<.01). Similarly, social incohesion was associated with higher levels of depressive symptoms (b= 0.268, p<.001). Respondents who reported work discrimination on a monthly/daily basis had higher depressive symptoms when compared to individuals who had not experienced work discrimination (b= 0.827, p<.001). Individuals who experienced everyday discrimination on a monthly/daily basis reported higher depressive symptoms when compared to individuals who did not perceive everyday discrimination (b= 0.658, p<.01). The SDS was positively associated with mental health, meaning every unit increase in the SDS resulted in a 0.16 unit increase in depressive symptomology (b= 0.167, p<.001).
Mental Health and Retirement Age.
Mental health was negatively associated with retirement age (i.e., higher levels of depressive symptomology were associated with a 0.27 year reduction in retirement ages, b=−.265, p<.001, Model I). The relationship between depressive symptomology and retirement age was stable across all Models (I-VI), such that worse mental health was associated with earlier retirement ages.
Bias-Corrected Bootstrap Resampling Results.
Mental health partially mediated the relationships between major lifetime discrimination (b= −0.060, 95% CI: −0.098 to −0.022), physical disorder (b= −0.089, 95% CI: −0.120 to −0.057); social incohesion (b= −0.125, 95% CI: −0.168 to −0.081); work discrimination (b= −0.128, 95% CI: −0.174 to −0.083); and SDS (b= −0.057, 95% CI: −0.077, −0.036). Mental health fully mediated the relationship between everyday discrimination and retirement age (b= −0.121, 95% CI: −0.174 to −0.069).
Discussion
An important contribution of the current study is that it reveals disadvantages across ecological domains and associations with mental health and retirement age. While cumulative (dis)advantage research often takes a life-course approach (e.g., the association of financial hardship in childhood and financial strain in adulthood with health outcomes in later life, see Szanton, Thorpe & Whitfield, 2010), in this study, we view (dis)advantages over one’s lifetime as well as disadvantages that accumulate (or pile up) at a particular life stage. Each aspect of discrimination and neighborhood disadvantage (Models I-VI), as well as the combined aspects (Model VII), related to worse mental health and earlier retirement. Although more research on psychometric properties are warranted on key constructs, this study offers a way to explore how these disadvantages reinforce each other and leads to compromised mental health and earlier retirement.
Evidence from this population-based study supports key concepts of cumulative disadvantage theory, specifically accumulated risks across multiple domains, that undermine mental health and employment in later life, supporting hypotheses three through six. Mental health is an important area for interventions, given that it is a mechanism that compromises retirement age. These results help to reconcile inconsistent relationships between discrimination, particularly at work, and retirement age in several previous studies (Marchiondo et al., 2015; Marchiondo et al., 2018). These findings point to strategies for interventions that we discuss below with implications.
Hostility, incivility, bias, unfair treatment, and exclusion because of age were common experiences across this older racially and ethnically diverse sample. Some differences in disadvantage did emerge but several were not in the expected direction. For example, Whites reported higher work and everyday discrimination when we expected people of color to report higher levels of discrimination. This may explain why there was not a statistically significant difference in depressive symptoms or retirement age by race and ethnicity (Mermin, Johnson & Murphy, 2007b). These findings do not support the first or second hypothesis but suggests there might be latent groups that perceive disadvantages because of their age along with their race, ethnicity, gender, weight, or physical appearance (Mouzon, Taylor, Nguyen, Ifatunji & Chatters, 2019). This warrants future research.
Several conceptual and empirical limitations of this study are worth noting. Unfortunately, only the Everyday Discrimination Scale asked about attribution. Querying about attribution for major lifetime discrimination and work discrimination can enhance our understanding of why individuals believe they were targeted for discrimination. Latent class analysis, along with intersectionality theory, could be used to identify unique profiles of older individuals.
Second, measures of discrimination were not routinely administered in the Health and Retirement Study and sometimes demonstrated poor reliability (e.g., Major Lifetime Discrimination), which limited our understanding of the timing of events as they relate to health and economic outcomes. The Health and Retirement Study might consider including these measures on a more regular basis and with discrimination measures with higher reliability and validity (such as the Workplace Age Discrimination Scale by Marchiondo, Gonzales, & Ran, 2015). Furthermore, exploratory and confirmatory factor analyses are needed to examine the psychometric properties of the Summative Disadvantage Scale, a novel construct in this study.
Although we controlled for time in the multivariate models given a number of unobserved factors during the Great Recession as well as changes in retiree’s lives, future longitudinal research on discrimination and labor force status could employ fixed and mixed models to control for unobserved factors. While discrimination and neighborhood conditions were self-assessed, future research could reveal how subjective and objective indices are related to health and retirement age. Propensity score analyses could enable an understanding of causal inference. Finally, mortality may affect these estimates, and we are unable to address them given the current survey approach. It is likely that individuals who experience high levels of cumulative disadvantages may have died at young ages (possibly before the age of 50 or during the observation period); thus, they would not be in these analyses. For these reasons, results may be underestimated.
Implications
Delaying retirement from age 62 to 65 could bolster retirement security for individuals and families, as well as benefit society (Johnson, 2018). The timing of retirement (early retirement, retire at the full retirement age, or delayed retirement) affects the monthly amount of retirement income and security, as well as the nation’s gross domestic product and economy (Munnell & Sass, 2008). Federal, state and employer policies and practices that protect individuals from work discrimination will likely result in expanding the productive engagement for all workers. The Protecting Older Workers Against Discrimination Act (S. 443) is a bipartisan bill currently under review in Congress. Passing this piece of legislation would reinstate the original intent of age being a factor, as opposed to the primary factor when pursuing discrimination claims via the Age Discrimination in Employment Act (learn more here: https://www.congress.gov/bill/115th-congress/senate-bill/443/text). Similarly, the Fair Employment Protection Act (S. 2019) aims to protect individuals from modern and covert forms of discrimination based on age and other characteristics within the workplace (learn more here: https://www.congress.gov/bill/115th-congress/senate-bill/2019). The Department of Labor can collaboratively work with the president to develop guidelines for workplace or antidiscrimination statues through executive order.
While social policy is an important intervention at the macro and meso levels, interventions at the individual level that target the nature of prejudice are also important. Organizational psychology research offers several ideas on how to challenge stereotyping, incivility, hostility, and unfair treatment, including swift, just, and consistent sanctioning of instigators within organizations; developing a “common in-group identity model” within the workplace; increasing personal awareness about biases and attitudinal dispositions, as well as fostering the ability to see an individual as unique rather than as a stereotype (Pettigrew & Tropp, 2006). Clinicians and mental health counselors could validate older adults’ experiences (Li, Gee & Dong, 2019) and provide psycho-education to help older adults recognize discrimination, identify protective factors (e.g., mediation, spirituality, religiosity, physical exercise) and other copies strategies to enhance individual resilience (Gonzales, Lee & Harrotyan, 2019). The clinical expertise of mental health professionals within work and community settings could bolster help older adults cope with discrimination and depression, which could improve mental health and extend work lives. Multipronged interventions aimed at individuals, organizations, and federal levels will promote a society that is cohesive, just, free from discrimination, healthy and productive.
Social disadvantages are structural and complex. Older adults in our study reported a number of inequitable incidences on the basis of multiple characteristics and across a variety of ecological contexts. Cumulative (dis)advantage theory was a useful framework to discern how mental health mediates the relationship between disadvantages and the age at which individuals retire. Social policies and practices that reduce incivility, bias, discrimination, social incohesion and prejudice in the ecological environment can be viewed as prevention strategies to mental health issues and will likely increase the capacity to work longer.
Figure 1.
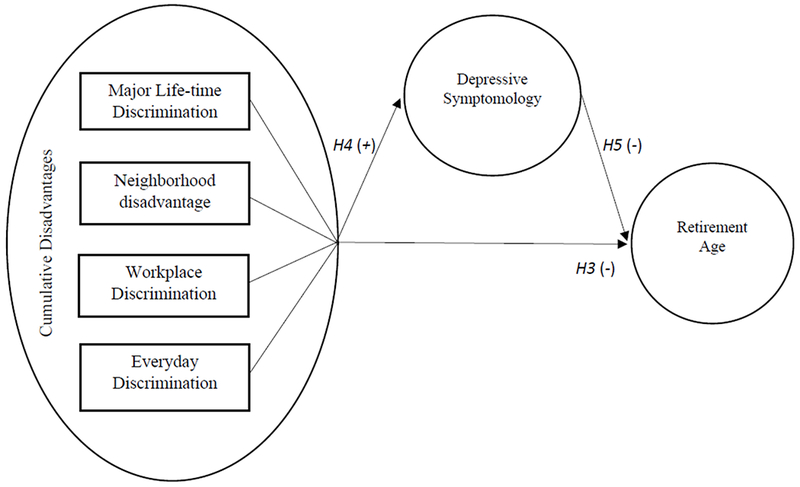
Conceptual framework of cumulative disadvantages and associations with mental health and retirement age.
Table 2a.
Associations of Disadvantages and Health with Retirement Age
| Model I b (SE) |
t | Model II b (SE) |
t | Model III b (SE) |
t | |
|---|---|---|---|---|---|---|
| Time | 1.538 (0.14) | 10.81 *** | 1.530 (0.14) | 10.69 *** | 1.539 (0.14) | 10.81 *** |
| Cohort (ref=HRS/AHEAD/CODA) | ||||||
| War babies | −5.778 (0.40) | −14.31 *** | −5.744 (0.41) | −14.02 *** | −5.778 (0.40) | −14.42 *** |
| Early Baby Boomers | −10.230 (0.45) | −22.69 *** | −10.157 (0.45) | −22.58 *** | −10.192 (0.46) | −22.40 *** |
| Race (ref=White) | ||||||
| Black/African American | −0.103 (0.39) | −0.26 | 0.007 (0.39) | 0.02 | 0.038 (0.40) | 0.10 |
| Hispanic/Latinx | 0.062 (0.40) | 0.15 | 0.061 (0.40) | 0.15 | 0.220 (0.42) | 0.52 |
| Female (ref) | −1.302 (0.20) | −6.62 *** | −1.371 (0.20) | −6.72 *** | −1.317 (0.20) | −6.61 *** |
| Education (years) | 0.026 (0.05) | 0.55 | 0.036 (0.05) | 0.77 | 0.014 (0.05) | 0.28 |
| Marital status (ref=married) | −0.956 (0.31) | −3.06 ** | −0.980 (0.30) | −3.22 ** | −0.933 (0.31) | −3.04 ** |
| Household income | 0.038 (0.16) | 0.23 | 0.008 (0.16) | 0.05 | −0.026 (0.16) | −0.16 |
| Household assets | 0.002 (0.01) | 0.15 | 0.003 (0.01) | 0.25 | 0.003 (0.01) | 0.29 |
| Health insurance plans | −0.317 (0.22) | −1.43 | −0.331 (0.22) | −1.51 | −0.370 (0.22) | −1.66 |
| Depressive symptoms | −0.265 (0.06) | −4.16 *** | −0.247 (0.06) | −3.84 *** | −0.241 (0.06) | −3.90 *** |
| Lifetime discrimination 1 | ||||||
| One experience | −0.650 (0.309) | −2.10 * | ||||
| Two or more experiences | −0.883 (0.30) | −2.93 ** | ||||
| Physical disorder | −0.267 (0.09) | −3.04 ** |
Notes:
=p<.001
=p<.01
=p<.05;
=reference group is “Never experienced”
Acknowledgements and Funders.
This work was supported by a grant from the U.S. Social Security Administration (SSA) funded as part of the Retirement Research Consortium at Boston College’s Steven H. Sandell Grant Program, Retirement Research Center (Gonzales, PI); the National Institute on Minority Health and Health Disparities’ Loan Repayment Program (Gonzales, PI), and Boston University’s Peter T. Paul Career Award (Gonzales, PI). We thank Dr. William V. Padula at John Hopkins Bloomberg School of Public Health and Lindsey Jung, Masters Student at Boston University’s School of Public Health for suggestions to earlier versions of this manuscript.
Footnotes
IRB. The study received exempt status from Boston University’s IRB No. 4532X.
Conflicts of Interests. The authors do not have any conflicts of interests.
HIPPA. There are no HIPAA Identifiers.
References
- Ayalon L, & Gum AM (2011). The relationships between major lifetime discrimination, everyday discrimination, and mental health in three racial and ethnic groups of older adults. Aging & Mental Health, (15), 587–594, DOI: 10.1080/13607863.2010.543664. [DOI] [PubMed] [Google Scholar]
- Barnes LL, Lewis TT, Begeny CT, Yu L, Bennett DA, & Wilson RS (2012). Perceived discrimination and cognition in older African Americans. Journal of the International Neuropsychological Society, 18(5), 856–865. DOI: 10.1017/S1355617712000628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blank RM, Dadaby M, & Citro CF (2004). Measuring racial discrimination. Washington, DC: The National Academies Press; DOI: 10.17226/10887. [DOI] [Google Scholar]
- Calvo E (2006). Does working longer make people healthier and happier? Center for Retirement Research at Boston College. Retrieved July 15, 2019, from https://crr.bc.edu/wp-content/uploads/2007/10/wp_2007-181-508.pdf
- Calvo E, Madero-Cabib I, & Staudinger UM (2017). Retirement sequences of older Americans: Moderately destandardized and highly stratified across gender, class, and race. The Gerontologist. DOI: 10.1093/geront/gnx052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carolan K, Gonzales E, Lee K, & Harootyan B (2018). Institutional and Individual Factors Affecting Health and Employment among Low-Income Women with Chronic Health Conditions. Journals of Gerontology: Social Sciences. DOI: 10.1093/geronb/gby149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cortina LM (2008). Unseen injustice: Incivility as modern discrimination in organizations. Academy of Management Review, 33(1), 55–75. DOI: 10.5465/amr.2008.27745097. [DOI] [Google Scholar]
- Curley C, Krause R, Feiock R, & Hawkins C (2019). Dealing with Missing Data: A Comparative Exploration of Approaches Using the Integrated City Sustainability Database. Urban Affairs Review, 55(2), 591–615. [Google Scholar]
- Dannefer D (2003). Cumulative advantage/disadvantage and the life course: Cross-fertilizing age and social science theory. Journal of Gerontology: Social Sciences, 58B, S327–S337. DOI: 10.1093/geronb/58.6.S327. [DOI] [PubMed] [Google Scholar]
- Deitch EA, Barsky A, Butz RM, Chan S, Brief AP, & Bradley JC (2003). Subtle yet significant: The existence and impact of everyday racial discrimination in the workplace. Human Relations; 56(11), 1299–1324. DOI: 10.1177/00187267035611002. [DOI] [Google Scholar]
- Flores E, Tschann JM, Dimas JM, Bachen EA, Pasch LA, & de Groat CL (2008). Perceived discrimination, perceived stress, and mental and physical health among Mexican-origin adults. Hispanic Journal of Behavioral Sciences, 30(4), 401–424. DOI: 10.1177/0739986308323056. [DOI] [Google Scholar]
- Gerber LM, & Sievert LL, (2018). Neighborhood disorder, exposure to violence, and perceived discrimination in relation to symptoms in midlife women. Women’s Midlife Health, 4(14). DOI: 10.1186/s40695-018-0043-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glymour MM, Mujahid M, Wu Q, White K, & Tchetgen Tchetgen EJ (2010). Neighborhood disadvantage and self-assessed health, disability, and depressive symptoms: Longitudinal results from the Health and Retirement Study. Annals of Epidemiology, 20(11), 856–861. DOI: 10.1016/j.annepidem.2010.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzales E, Matz-Costa C & Morrow-Howell N (2015). White House Conference on Aging 2015. Increasing Opportunities for the Productive Engagement of Older Adults: A Response to Population Aging. The Gerontologist, Special Issue for the Policy Forum DOI: 10.1093/geront/gnu176. [DOI] [PubMed] [Google Scholar]
- Gonzales E, Lee K, & Harootyan B (2019). Voices from the Field: Ecological Factors that Promote Employment and Health among Low-Income Older Adults with Implications for Direct Social Work Practice. Clinical Social Work Journal. DOI: 10.1007/s10615-019-00719-x. [DOI] [Google Scholar]
- Han J, & Richardson VE (2015). The relationships among perceived discrimination, self-perceptions of aging, and depressive symptoms: A longitudinal examination of age discrimination. Aging & Mental Health, 19(8), 747–755. DOI: 10.1080/13607863.2014.962007. [DOI] [PubMed] [Google Scholar]
- Hao Y (2008). Productive activities and psychological well-being among older adults. Journals of Gerontology: Social Sciences, 63B(2), S64–S72. DOI: 10.1093/geronb/63.2.S64. [DOI] [PubMed] [Google Scholar]
- Konig S, Lindwall M, & Johansson (2018). Involuntary and delayed retirement as a possible health risk for lower educated retirees. Journal of Population Ageing, 1–15. DOI: 10.1007/s12062-018-9234-6. [DOI] [Google Scholar]
- Krieger N (2012). Methods for the scientific study of discrimination and health: An eco-social approach. American Journal of Public Health, 102(5), 936–945. DOI: 10.2105/AJPH.2011.300544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis TT, Aiello AE, Leurgans S, Kelly J, & Barnes LL (2010). Self-reported experiences of everyday discrimination are associated with elevated C-reactive protein levels in older African-American adults. Brain, Behavior, and Immunity, 24, 438–443. DOI: 10.1016/j.bbi.2009.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li LW, Gee GC & Dong XQ (2019). Associations of self-reported discrimination and suicide ideation in older Chinese Americans. American Journal of Geriatric Psychiatry, 26(1), 42–51. DOI: 10.1016/j.jagp.2017.08.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo Y, Xu J, & Granberg E (2012). A longitudinal study of social status, perceived discrimination, and physical and emotional health among older adults. Research on Aging, 34, 275–301, DOI: 10.1177/0164027511426151. [DOI] [Google Scholar]
- Marchiondo L, Gonzales E, & Ran S (2015). Development and Validation of the Workplace Age Discrimination Scale (WADS). Journal of Business and Psychology; DOI: 10.1007/s10869-015-9425-6. [DOI] [Google Scholar]
- Marchiondo L, Gonzales E, & Williams L (2017). Workplace Age Discrimination: Long-Term Relationships with Health and Retirement Intentions. Journal of Gerontology: Social Sciences. DOI: 10.1093/geronb/gbx095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCluney CL, Schmitz LL, Hicken MT, & Sonnega A (2018). Structural racism in the workplace: Does perception matter for health inequalities? Social Science & Medicine, 199, 106–114. DOI: 10.1016/j.socscimed.2017.05.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mermin GBT, Johnson RW, & Murphy DP (2007a). Why do boomers plan to work longer? Journals of Gerontology: Social Sciences, 62(5), S286–S294. DOI: 10.1093/geronb/62.5.S286. [DOI] [PubMed] [Google Scholar]
- Mermin GBT, Johnson RW, & Murphy DP (2007b). Racial differences in baby boomers’ retirement expectations. Retrieved on July 15, 2019 from https://www.urban.org/sites/default/files/publication/46166/311414-Racial-Differences-in-Baby-Boomers-Retirement-Expectations.PDF.
- Kessler RC, Mickelson KD, & Williams DR (1999). The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior, 40, 208–230. [PubMed] [Google Scholar]
- Morrow-Howell N, Gonzales E, Harootyan B, Lee YJ & Lindberg B (2017). Approaches, Policies, and Practices to Support the Productive Engagement of Older Adults. Journal of Gerontological Social Work, 60, 193–200, DOI: 10.1080.01634372.2016.1275912. [DOI] [PubMed] [Google Scholar]
- Mosca I & Barrett A, (2016). The impact of voluntary and involuntary retirement on mental health: Evidence from Older Irish Adults. Journal of Mental Health Policy & Economics, 19(1), 33–44. [PubMed] [Google Scholar]
- Mouzon DM, Taylor RJ, Nguyen AW, Ifatunji MA, & Chatters LM (2019). Everyday discrimination typologies among older African Americans: The roles of gender and socioeconomic status. Journals of Gerontology: Social Sciences. DOI: 10.1093/geronb/gbz088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Munnell A, & Sass SA (2008). Working longer: The solution to the retirement income challenge. Washington, DC: Brookings Institute Press. [Google Scholar]
- Ong DA, Williams DR, Nwizu U, & Gruenewald TL, (2017). Everyday unfair treatment and multisystem biological dysregulation in African American adults. Cultural Diversity and Ethnic Minority Psychology, 23(1), 27–35. DOI: 10.1037/cdp0000087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pettigrew TF, & Tropp LR (2006). A meta-analytic test of intergroup contact theory. Journal of Personality and Social Psychology. 2006; 90: 751–783. DOI: 10.1037/0022-3514.90.5.751. [DOI] [PubMed] [Google Scholar]
- Rhee N (2013). Race and retirement insecurity in the United States. Washington, DC: National Institute on Retirement Security; Retrieved on July 19, 2019 from https://www.giaging.org/documents/NIRS_Report_12-10-13.pdf Published December 10, 2013. [Google Scholar]
- Sternthal MJ, Slopen N, & Williams DR (2011). Racial disparities in health: how much does stress really matter? Du Bois Review: Social Science Research on Race, 5(1), 95–113. DOI: 10.1017/S1742058X11000087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutin AR, Stephan Y, Carretta H, & Terracciano A (2015). Perceived discrimination and physical, cognitive, and emotional health in older adulthood. The American Journal of Geriatric Psychiatry, 23(2), 171–179. DOI: 10.1016/j.jagp.2014.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szanton SL, Thorpe RJ, & Whitfield KE (2010). Life-course financial strain and health in African Americans. Social Science & Medicine, 71(2), 259–265. DOI: 10.1016/j.socscimed.2010.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor SE, Repetti RL, & Seeman T (1997). Health psychology: What is an unhealthy environment and how does it get under the skin? Annual Review of Psychology, 48(1): 411–447. [DOI] [PubMed] [Google Scholar]
- White House Conference on Aging, (2015). White House Conference on Aging Final Report. Retrieved on July 15, 2019 from https://whitehouseconferenceonaging.gov/2015-whcoa-final-report.pdf. [Google Scholar]
- Williams DR, Yu Y, Jackson JS, & Anderson NB (1997). Racial differences in physical and mental health: socio-economic status, stress and discrimination. Journal of Health Psychology, 2, 335–351. [DOI] [PubMed] [Google Scholar]
- Williams DR, & Collins C (2001). Racial residential segregation: A fundamental cause of racial disparities in health. Public Health Reports, 116, 404–416. DOI: 10.1093/phr/116.5.404. [DOI] [PMC free article] [PubMed] [Google Scholar]