

Abstract
Human-human social touch improves mood and alleviates pain. No studies have so far tested the effect of human-robot emotional touch on experimentally induced pain ratings, on mood and on oxytocin levels in healthy young adults. Here, we assessed the effect of touching the robot PARO on pain perception, on mood and on salivary oxytocin levels, in 83 young adults. We measured their perceived pain, happiness state, and salivary oxytocin. For the 63 participants in the PARO group, pain was assessed in three conditions: Baseline, Touch (touching PARO) and No-Touch (PARO present). The control group (20 participants) underwent the same measurements without ever encountering PARO. There was a decrease in pain ratings and in oxytocin levels and an increase in happiness ratings compared to baseline only in the PARO group. The Touch condition yielded a larger decrease in pain ratings compared to No-Touch. These effects correlated with the participants’ positive perceptions of the interaction with PARO. Participants with higher perceived ability to communicate with PARO experienced a greater hypoalgesic effect when touching PARO. We show that human-robot social touch is effective in reducing pain ratings, improving mood and - surprisingly - reducing salivary oxytocin levels in adults.
Subject terms: Emotion, Social behaviour, Empathy, Pain, Stress and resilience
Introduction
Social interaction is one of the most basic survival needs of humans1. Both in childhood2–5 and in older ages6–8, the impact of social connections on health seems to be crucial. For example, poor social relationships and social isolation were associated with high incidence of general morbidity9,10, stress disorders11,12 and chronic pain11,13,14. Close relationships, however, were found to be a protective factor against stress and pain disorders15–18. Close interpersonal relationships often involve emotional touch, which may act as a mediating factor in the effect of social relationships on pain relief. Emotional touch is defined as a pleasant touch between two humans19. Emotional touch may include active touching (i.e. stroking another person), passive touching (being touched by another person) or dyadic touching (i.e. hand holding)20,21. Indeed, several studies have found that handholding22 and hugging23 reduce the physiological and psychological response to stress among men and women. It was suggested that empathic abilities of both the person touching and the person touched play a fundamental role in this effect24. Emotional touch also stimulates the hypothalamic-pituitary system to secrete oxytocin20,25, a hormone that has been characterized as having a central role in mediating feelings of love, social attachment and communication in both animals and humans26–29. In an animal study, there was an increase in pain thresholds following petting, as well as following injection of oxytocin. In both situations (petting or injection of oxytocin), the effect on the pain threshold disappeared with the administration of an oxytocin antagonist30. Similarly, in humans, Kreuder et al.31, recently demonstrated that administration of nasal oxytocin enhances the pain-relieving effects of social support in romantic couples. In addition, it was found that being touched by another person32 and handholding with a spouse33,34 induce a reduction in pain ratings among women. The level of the analgesic effect when holding a partner’s hand was associated with the toucher’s empathic tendencies33. These studies suggest that emotional touch may lead to decreased sensitivity to pain that may be associated with the release of oxytocin. How, then, can the beneficial effect of emotional touch on the perception of pain be provided to individuals who do not have access to it? One way to fill this need may be through a social robot. A social robot may take on a human-like35,36 or a pet-like appearance, or move like one e.g37,38.. It is designed to create social relationships with people39 for either entertainment40, education41, or for therapeutic purposes42,43. Shibata44 developed a seal-like robot named PARO designed to elicit a feeling of social connection. Interaction with PARO was found to improve mood45,46, and to reduce stress and anxiety of older people, and of individuals with dementia45–47, as well as to improve the mood of pediatric patients48. In one study, participants interacted with PARO for the duration of one year, during which the effects on mood were maintained46. In addition, interaction with PARO49 and with a humanoid robot50 was found to reduce stress, anxiety and pain levels during medical procedures (chemotherapy among women and vaccination among children, respectively). However, a recent review concluded that better methodology and measures are needed to draw conclusions about the effect of human-robot social interactions on pain51. Indeed, no controlled studies specifically examined the effect of the robot’s touch as opposed to the robot’s presence, without any physical contact, on the perception of pain. In addition, no controlled studies have examined the effect of human-robot social interaction on either oxytocin secretion or on experimentally induced pain ratings.
The aim of the current experiment was, therefore, to examine the effect of interaction with the social robot PARO on pain perception, emotional state, and salivary oxytocin levels. Specifically, we examined, in a group of men and women: (1) What is the effect of human-robot interaction on the (a) happiness state, (b) salivary oxytocin levels and (c) pain perception? (2) What is the effect of social robot’s touch vs. the social robot’s presence on pain perception? (3) Are there correlations between pain perception and (a) the level of salivary oxytocin; and (b) the participant’s perception of the interaction with the robot?
Methods
Participants
Eighty-three healthy adults (42 female, 41 male; age: 25.1 ± 2.7 years old (mean ± STD)) were allocated using a computer-generated simple random sampling, into one of two groups: the PARO-Interaction (PARO) group (63 participants, 32 female, 31 male; 25.2 ± 2.4 years old), or the control group (20 participants, 10 female, 10 male; 24.4 ± 2.2 years old). The participants were recruited by advertisements posted throughout the university campus and on social media. Exclusion criteria were acute or chronic pain, present or previous pathology in the arms (testing site), bruises or any other skin lesions on the arms, diseases causing potential neural damage (e.g., diabetes), systemic and mental illnesses (e.g., anxiety disorders, major depression, bipolar disorder), and communication disabilities. Written informed consent was obtained from all the participants. Written informed consent for publication of identifying images in an online open-access publication was obtained from the persons photographed. The experiment was approved by the institutional review board of Ben-Gurion University. All experimental procedures were performed in accordance with this ethical approval.
Study design
The 63 participants enrolled in the PARO group comprised the main study group. These participants interacted with PARO and were tested before, during and after the interaction in a within-subjects design. In order to rule out any carry-over effects – that is, the effects of repeated pain measurements on participants’ pain perception – we included a control group of 20 participants, who did not interact with PARO. The control group’s size was informed by;52–54 the PARO group was larger, to account for the randomized allocation into different experimental sequences within it (see details below). Differences between participants in the PARO and the control groups were calculated as a between-subject analysis.
Equipment
PARO robot
PARO is a therapeutic robot baby harp seal, manufactured by the Intelligent System Research Institute of Japan’s National Institute of Advanced Industrial Science and Technology. PARO is intended to have a calming effect and to elicit emotional responses in patients55. It is outfitted with dual 32-bit processors, three microphones, twelve tactile sensors covering its fur, touch-sensitive whiskers, and a system of motors and actuators that move its limbs and body. The robot responds to petting by moving its tail and opening and closing its eyes. It seeks out eye contact and produces sounds similar to a real baby seal55. PARO was classified as a Class 2 medical device by U.S. regulators in 2009, and is completely safe for human interaction56.
Thermal stimulator
Heat stimuli were delivered using a Peltier-based computerized thermal stimulator (TSA II, Medoc Ltd., Ramat-Ishai, Israel), with a 3 × 3 cm contact probe that was attached to the ventral aspect of the non-dominant forearm by means of a Velcro band. The baseline temperature of the stimulator was set to 35 °C for all the tests. The stimulator is accurate to within ±0.3 °C.
Visual analog scale (VAS)
The visual analog scale (VAS) is a form of direct scaling technique, in which line length is the response continuum53. The VAS has been reported as a valid and reliable measure for the intensity of pain53. Pain ratings were recorded by a custom-made application to digitally record the participants’ VAS responses, installed on a mobile device. Sliding the finger on the screen of the mobile device from left to right covers the corresponding portion of the screen in red (see Fig. 1), which, in turn, corresponds to the extent to which the participants experiences the stimulus as painful. The left end of the screen was defined as corresponding to ‘no pain sensation’, and the right end of the screen corresponded to ‘the most intense pain sensation imaginable’. The custom-made application translated the final horizontal finger location to a number on a scale from zero to 10.
Figure 1.
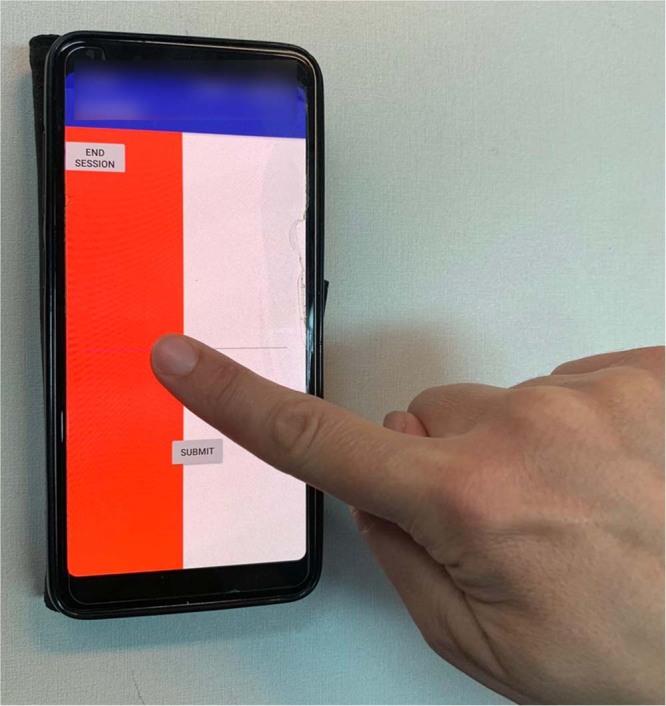
An illustration of the VAS application used to rate pain levels. In order to rate the intensity of pain, the participants were asked to slide their finger from left to right on the screen of the device. Sliding the finger revealed a red area that expanded as the participant slid his or her finger further to the right. The leftmost edge of the screen was defined to have a value of zero (no pain), and the rightmost edge was defined to have a value of 10 (the most intense pain).
Measurements
Happiness state
Perceived happiness was evaluated using a VAS 10-cm line, printed on a sheet of paper, with 2 anchor points at its extremes, set as “not at all” (= 0) and “the most” (= 10), and participants were asked to mark on that scale, using a pen, how happy they felt. This method was found previously reliable and valid to measure the emotional state, including happiness57.
Empathic concern
Empathic concern was measured by the Empathic Concern subscale of the Interpersonal Reactivity Index (IRI). This is a 7-item questionnaire which assesses “other-oriented” feelings of sympathy and concern for others, found to have good reliability and sensitivity58.
Salivary oxytocin
Saliva samples of oxytocin were collected with salivates (Sarstedt, Rommels-dorft, Germany). Participants were asked to place a roll of cotton in their mouths, chew on it for a minute until it became saturated, and place it in a salivate tube. The samples were stored at −20 °C for approximately a week and then transported to the oxytocin laboratory where they were stored at −80 °C until they were assayed. Samples were thawed at room temperature for 10 minutes, followed by centrifugation (15 min., 3500 g, 4 C). Next, 1 ml of saliva was acidified with 1 ml of 0.1% trifluoroacetic acid (TFA) and centrifuged at 17000 ×g for 15 min at 4 °C. C18 Sep-Pak column (Waters, Ireland) were assembled onto vacuum manifold system (Waters, Ireland), and equilibrated with 1 ml of acetonitrile. Washing of columns was performed 5 times using TFA-H2O (in total: 15 ml), followed by applying of the supernatant onto the Sep-Pak vacuum manifold system, without vacuum, then an additional wash, as described. Elution of the samples was performed by applying 2 mL of an elution solution (95% acetonitrile 5% of 0.1% TFA-H2O) onto each column. Following extraction, collection and processing of saliva, measurements of human oxytocin concentrations were determined by an Enzyme-Linked Immunosorbent Essay (ELISA), using the Oxytocin ELISA kit (Abcam, Cambridge, UK). The ELISA plate was read at O.D. absorbance of 570 and 590 for Oxytocin (ELx808, Bio Tec Industries, VT). All samples were assayed and compared to a standard curve. Saliva concentration of the biomarkers was expressed as pg/ml.
Pain perception
Pain measurements were conducted at three time points during the experiments. The stimuli administered during these measurements were determined as follows:
Calibrating heat-pain intensity
To establish which temperatures elicit in each individual sensations of mild and strong pain, participants received a series of heat stimuli in a set of calibration trials. In each calibration trial, the starting temperature of the stimulator was 35 °C, and it increased at a rate of 2 °C/sec to a target temperature. The first target temperature was 40 °C. The target temperature was held for 6 sec, and participants were asked to rate the pain on the VAS. The temperature then returned to baseline (35 °C) by an active cooling mechanism. Following a 45-sec break, the subsequent trial was initiated. An interstimulus interval of 45 seconds was maintained and the contact probe was moved between stimulations to prevent sensitization. The target temperature was increased by 1 °C in each subsequent calibration trial until the participant reported a value of 6 (out of 10) on the VAS. The temperatures eliciting a value of 4 (mild pain) and a value of 6 (strong pain) on the VAS were documented and used for the rest of the experiment.
Pain measurements
In each of the three pain measurements, the temperatures eliciting a value of 4 and a value of 6 on the VAS were administered for 50 seconds with an inter-stimulus interval of 2 minutes. VAS pain ratings at the end of each stimulus was the outcome measure.
Structured interaction with PARO
During the 10 minutes of interaction with PARO, participants were asked to respond to questions, which encouraged them to examine PARO’s reactions (for example, indicate PARO’s reaction to petting it, to calling it by its name, etc.; See Supplementary Materials S1 for the full questionnaire). The goal of asking participants to fill out this questionnaire was to ensure that they spent the 10-minute session actively engaging with PARO.
Perceptions of the interaction with PARO
PARO’s perceived feelings, and participants’ feelings during the interaction with PARO, were evaluated using a 12-item custom-made questionnaire, to which participants responded using a 10-cm VAS line with 2 anchor points at its extremes, set to “not at all” (= 0) and “the most” (= 10) (see the full questionnaire in Supplementary Materials S2). The questionnaire was administered to the PARO group at the end of the experiment, at T4.
Procedure
Each participant was invited to a single testing session that lasted approximately 1 hour (see Fig. 2). The participants were instructed to avoid physical exercise and to refrain from smoking, eating or drinking (excluding water) for one hour before testing. Upon arrival, participants were divided semi-randomly to either the PARO or the control group. Testing took place in a quiet room. Temperature in the room was maintained at 25 °C. The participant sat in a comfortable armchair. Five minutes after arrival, the first happiness ratings and salivary oxytocin measurements were obtained (T1), followed by the pain-intensity calibration and the first pain measurement (Baseline; termed S1 in the control group, see Fig. 3A). Immediately after that, the second happiness ratings and salivary oxytocin measurements were obtained (T2). Participants in the PARO group then spent 10 min engaged in one of two activities they were semi-randomly assigned to: half of the participants in this group had a structured interaction with PARO (see below), and half were given an article to read on Maria Mitchel, an American astronomer. In the control group, all participants were given the article on Maria Mitchel to read during that 10-min period. Participants then underwent the third happiness ratings and salivary oxytocin measurements (T3). During T3, PARO was either present in the room (for the half of the PARO group which interacted with it for 10 minutes), or not present (for the half of the PARO group which read the article for 10 minutes). During the structured interaction with PARO, the experimenter introduced PARO to the participant and then left the participant alone in the room with PARO for 10 minutes. During the interaction, the participants completed a questionnaire that included questions about the interaction with PARO in order to ensure an active interaction experience (see section 3.5 above for details). The two subsequent pain measurements (Touch/No-Touch) in the PARO group were conducted while participants were either actively touching PARO (the ‘Touch’ condition, see Fig. 3C), or while PARO was co-present in the room with them, but with no physical touch between the participant and PARO (the ‘No-Touch’ condition, see Fig. 3B). The order at which the Touch and the No-Touch conditions were performed was semi-randomized across participants. The control group underwent the two subsequent measurements of pain intensity (S2 and S3) without ever encountering the PARO robot. Immediately after these, and while the participants were touching PARO, the forth happiness ratings and salivary oxytocin measurements were obtained (T4). Lastly, the participants completed the IRI questionnaire and rated their perceptions of the interaction with PARO.
Figure 2.

Flow chart of the experimental design.
Figure 3.

An illustration of the experimental setup. The participant (on the left) has the heat stimulator placed on her non-dominant arm, which is placed on the table. The experimenter (on the right) administers the accurate heat stimuli, and tracks them on the screen. (A) Baseline condition; PARO is not present. (B) No-Touch condition; PARO is present in the room, without physical contact with the participant. (C) Touch condition. PARO is placed on the table next to the participant, who touches it during the administration of the heat stimuli. In the control group, PARO was not present during the entire experimental session, as in (A).
The experimental protocol was approved by the Ethics Committee of the Ben-Gurion University of the Negev.
Data analysis
Data were analyzed using IBM SPSS statistic software version 25 (IBM, Armonk, NY, USA). Continuous variables are described as means ± SD. Sample size was calculated using G-Power59. For a sample size of 83 individuals, if α = 0.05 statistical power is 89%. All data underwent Kolmogorov-Smirnov analysis for normality of distribution. Parametric and nonparametric analyses of variance with corrected post hoc tests were used to evaluate the effect of experimental phase (T1/T2/T3/T4) and of group (PARO/Control group) on perceived happiness and on oxytocin levels and the effect of condition (Baseline/Touch/No-Touch in the PARO group and S1/S2/S3 in the control group) on pain ratings. Correlations between pairs of variables were calculated with Pearson’s r; p < 0.05 was considered significant. The Bonferroni correction was applied to multiple comparisons, where needed.
Results
Participants’ perceptions of the interaction with PARO
PARO’s perceived feelings during the interaction
The participants perceived PARO’s feelings during the interaction as happy (6.6 ± 2.2), satisfied (6.3 ± 2.2), wants to be petted (7.3 ± 2.2) and wants to communicate (6.8 ± 2.6). Low ratings were given to PARO feeling tired (3.1 ± 2.7), sad (2.0 ± 1.9) and angry (0.9 ± 1.1) (Fig. 4A). These perceptions of PARO’s feelings were recorded once, at T4.
Figure 4.

Participants’ perceptions of the interaction with PARO. (A) PARO’s perceived feelings, as evaluated by participants in the PARO group at the end of the experiment (at T4). (B) Participants’ impressions from their interaction with PARO (PARO group), which they reported at the end of the experiment (at T4). Values denote mean of visual analogue scale (VAS; 0–10) ± SEM.
Participants’ feelings during the interaction with PARO
The participants gave high ratings to feeling good in the presence of PARO (7.6 ± 1.8), to pleasant sensation while touching PARO (7.7 ± 2.0) and to their willingness to meet PARO again (6.9 ± 2.7). Intermediate ratings were given to the question if PARO helped to reduce pain (5.2 ± 2.7) and to the question if they were able to communicate with PARO (4.7 ± 3.0) (Fig. 4B). There were significant correlations between the participants’ empathic concern and: (1) their good feelings in the presence of PARO (r = 0.27, p = 0.021) and (2) their pleasant sensation while touching PARO (r = 0.30, p = 0.012).
The effect of the interaction with PARO on the participants’ emotional state
A significant main effect of the experimental phase (T1/T2/T3/T4) was found for happiness ratings [F(3,83)=4.84, p < 0.05(. The effect of group (PARO/Control) was not significant [F(1,83)=1.71, p = 0.19]. However, the interaction phase*group was significant [F(3,83)=3.73, p < 0.05]. Post hoc comparisons revealed that there were similar ratings between groups at T1 (5.6 ± 1.9 in PARO and 5.6 ± 1.7 in controls, t(81)=0.62, p = 0.47) and T2 (5.3 ± 2.2 in PARO and 4.8 ± 2.3 in controls, t(81)=0.93, p = 0.18). However, at T3 there was an increase in happiness, compared to T1, in the PARO group (6.3 ± 1.9, t(62)= 3.52; t(19)=0.87, p < 0.001) but not in the control group (5.2 ± 2.3, t(19)=1.28, p = 0.20). As noted above, the PARO group included both those who spent the 10 minutes interacting with PARO, and those who read the article during the 10-min period. The difference between groups at T3 was significant (t(81)=2.08, p < 0.05). At T4 the happiness ratings remained higher than T1 in the PARO group (5.9 ± 2.2, (t(62)=1.44, p < 0.001) and did not change significantly in the control group (5.0 ± 2.4, t(19)=1.28, p = 0.11). The difference between groups at T4 did not reach significance (p = 0.05, Fig. 5). There were significant correlations between PARO’s perceived feelings and the change in happiness from T1 to T4 (see Table 1). The more participants perceived PARO to have more positive feelings, the happier they reported feeling themselves.
Figure 5.
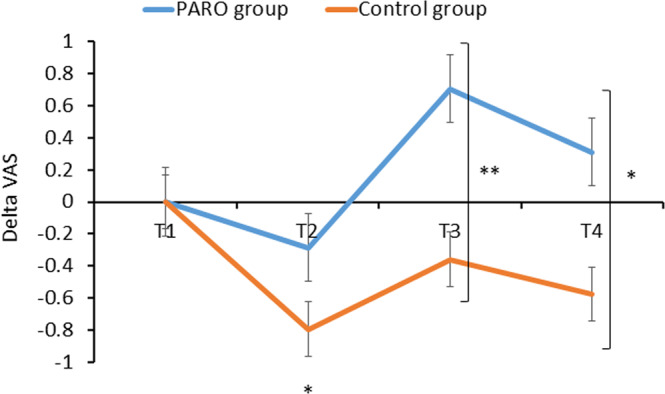
The change in perceived happiness at the four epochs of the study in the PARO and the control groups. A significant difference between groups was found at T3 (**p < 0.01) and T4 (*p < 0.05). At T2 happiness decreased significantly in the control group compared to T1 (p < 0.05). In the PARO group the change in happiness at T2 (compared to T1) was not significant, p = 0.06. At T3 Happiness increased significantly compared to T1 only in the PARO group (****p < 0.0001). Values denote mean of Δ visual analogue scale (VAS; 0–10) ± SEM. T1 – upon arrival; T2 – following the first pain-perception measurements; T3 – following 10 mins of either reading or interacting with PARO; T4 – completed while touching PARO (in the PARO group only), following the third, and last, pain-perception measurements.
Table 1.
Correlations between participants’ perceptions of PARO’s feelings, and the change in their happiness in the Touch condition compared to Baseline.
| PARO’s perceived feelings | |||
|---|---|---|---|
| Satisfied | Happy | Sad | |
| Δ Happiness (0–10) |
0.38** p < 0.005 |
0.37** p < 0.005 |
−0.57** p < 0.005 |
Shown here are the r values. **p < 0.005.
The effect of the interaction with PARO on salivary oxytocin levels
A significant main effect of the experimental phase (T1/T2/T3/T4) was found for oxytocin levels [F(3,82)=6.54, p < 0.01]. The effect of group (PARO/Control) was not significant [F(1, 82)= 0.49, p = 0.49]. However the interaction phase*group was significant [F(3,82)=5.16, p < 0.01]. Post hoc comparisons revealed that the levels of oxytocin were similar at time T1 in the PARO group (29.0 pg/ml±11.4) and in the control group (28.8 pg/ml ±8.0, t(81)=0.72, p = 0.47). In both groups oxytocin levels did not change at T2. However, in the PARO group, oxytocin levels decreased significantly at T3 to 26.6 pg/ml ±8.8 (t(61)=2.57, p < 0.01, a decrease of 2.8 pg/ml ±8.3) and decreased significantly further at T4 compared to T1 to 23.1 pg/ml ±10.2 (t(62)=5.73, p < 0.0001, a decrease of 5.9 pg/ml ±8.1). However, in the control group oxytocin levels did not change significantly at T3 (28.4 pg/ml ±10.5, t(19)=0.29, p = 0.39) or at T4 (28.5 pg/ml, t(19)=0.26; p = 0.40). The difference between groups in the reduction of oxytocin levels was significant at T3 (t(81)=0.75, p < 0.001) and T4 (t(81)=2.14, p < 0.05, see Fig. 6). As noted above, the PARO group included both those who spent the 10 minutes interacting with PARO, and those who read the article during the 10-min period.
Figure 6.
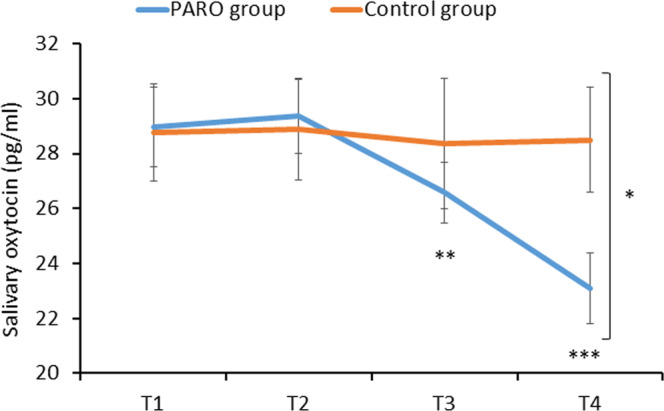
The change in oxytocin levels at the 4 epochs of the study in the PARO and the control groups. Oxytocin levels decreased significantly from T1 to T3 (**p < 0.01) and further from T1 to T4 (***p < 0.001) only in the PARO group. The difference in oxytocin levels between the groups was significant at T4 (*p < 0.05). Values denote mean salivary oxytocin levels (pg/ml) ± SEM. T1 – upon arrival; T2 – following the first pain-perception measurements; T3 – following 10 mins of either reading or interacting with PARO; T4 – completed while touching PARO (in the PARO group only), following the third, and last, pain-perception measurements.
There was a significant negative correlation between oxytocin levels at T4 and the participants’ willingness to meet PARO again (r = −0.46, p < 0.05).
The effect of the interaction with PARO on pain perception
Mild pain
A significant effect of condition (Baseline/Touch/No-Touch) was found in the PARO group (F2,62 = 4.33, p < 0.05) while no effect of condition (S1/S2/S3) was found in the control group (F2,20 = 1.16, p = 0.33). Post hoc tests revealed that in the PARO group there was a significant decrease in pain ratings from Baseline (1.4 ± 1.6) to the Touch condition (0.8 ± 1.4, t(62)=2.59, p < 0.05). No significant difference from Baseline was found at the No-Touch condition (1.1 ± 1.6, t(61)=1.74, p = 0.87, Fig. 7A). In other words, participants rated their pain sensation as significantly lower when touching the PARO robot, compared to Baseline pain ratings. When the robot was only co-present in the room with them, and there was no physical contact with it, their pain ratings were not significantly different from Baseline.
Figure 7.

The change in pain ratings across the three pain measurements in the PARO and the control groups. (A) Mild pain: In the PARO group, pain ratings decreased in the Touch condition compared to Baseline (*p < 0.05). (B) Strong pain: In both the PARO and the control groups, pain ratings decreased in the No-Touch/S2 and Touch/S3 conditions compared to Baseline/S1. In the PARO group there was a greater decrease in the Touch compared to the No-Touch condition (**p < 0.01). Values denote mean visual-analogue scale (VAS) ratings (0–10) ± SEM.
The decrease in mild-pain ratings from Baseline to Touch condition in the PARO group was significantly correlated with the perceived pain-alleviating effect of PARO (r = −0.34, p < 0.005; see Table 2) and with the level of salivary oxytocin at T4 (r = 0.24, p < 0.05).
Table 2.
Correlations between participants’ perceptions of the interaction with PARO, and the change in pain ratings in the Touch condition compared to Baseline.
| Participant’s perceptions of the interaction with PARO | |||||
|---|---|---|---|---|---|
| Good feelings | Pleasant touch | Able to communicate | Alleviating pain | Wish to meet again | |
| Δ Mild pain | NS | NS | NS | −0.34** p < 0.005 | NS |
| Δ Strong pain |
−0.31* p < 0.01 |
NS | NS |
−0.33** p < 0.005 |
−0.37** p < 0.005 |
Shown here are the r values. *p < 0.01, **p < 0.005, NS = not significant.
Strong pain
A significant effect of condition (Baseline/Touch/No-Touch) was found in the PARO group (F2,62 = 17.87, p < 0.0001). The effect of condition (S1/S2/S3) was also significant in the control group (F2,20 = 7.78, p < 0.01). Post hoc tests revealed that in the PARO group there was a decrease in pain ratings from Baseline (5.1 ± 2.4) both to the No-Touch condition (4.1 ± 2.7, t(62)=3.44, p < 0.01) and to the Touch condition (3.1 ± 2.5, t(61)=6.23, p < 0.0001). The decrease in pain ratings was significantly greater in the Touch condition compared to No-Touch condition (t(61)=2.56, p < 0.01). In the control group, there was also a decrease in pain ratings from S1 (5.7 ± 2.7) to S2 (4.3 ± 3.2, t(19)=3.59, p < 0.05) and to S3 (4.8 ± 3.0, t(19)=2.64, p < 0.05). However, no significant difference was found between S2 and S3 (t(19)=1.51, p = 0.49, Fig. 7B).
The extent of the decrease in strong-pain ratings from Baseline to the Touch condition in the PARO group was significantly correlated with the participants’ perceived pain-alleviating effect of PARO (r = −0.33, p < 0.005), their positive feelings with respect to PARO (r = −0.31, p < 0.01) and the wish to meet PARO again (r = −0.37, p < 0.005; see Table 2).
High and low communication with PARO
In order to further investigate the effect of the interaction with PARO on emotions and pain perception, we divided the participants in the PARO group into high communicators (HC) and low communicators (LC). The division into the two groups was made using the median value of the perceived ability to communicate with PARO (4.7).
The mean communication ratings of HC (n = 31) and LC (n = 32) was 7.2 ± 1.9 vs. 2.1 ± 1.9 respectively (p < 0.0001; Fig. 8A). There was no significant difference between the subgroups in happiness ratings. However, oxytocin levels were lower in HC compared to LC. The difference between subgroups was significant at T1 (31.6 ± 13.4 pg/ml in LC and 26.4 ± 8.6 pg/ml in HC;t(61)=1.83, p < 0.05) and at T3 (28.6 ± 10.2 pg/ml in LC and 24.7 ± 7.0 pg/ml in HC;t(61)=1.75, p < 0.05; Fig. 8B). There was no difference between the HC and the LC in mild-pain ratings. However, the decrease in strong-pain ratings from Baseline to Touch condition was significantly greater in HC (2.5 ± 2.7) compared to LC (1.3 ± 1.8, t(61)=0.85, p < 0.05; Fig. 6C).
Figure 8.
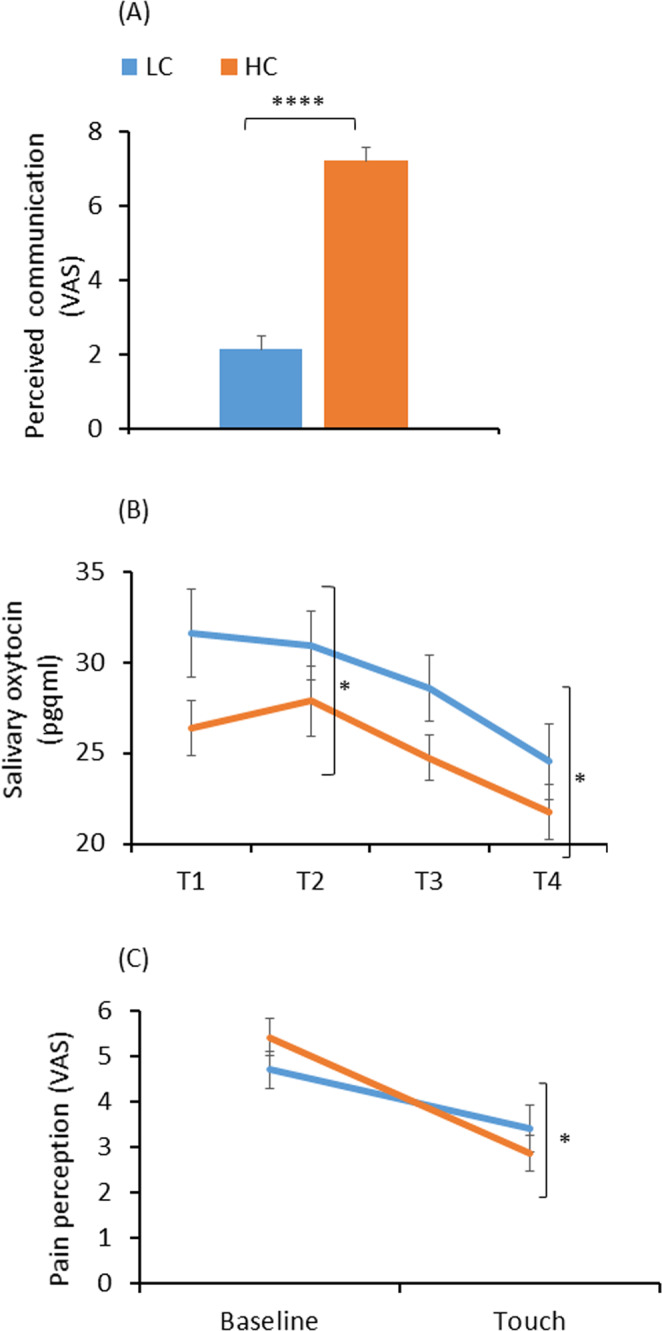
Differences between low communicators (LC) and high communicators (HC). (A) perceived ability to communicate with PARO (****p < 0.0001); (B) oxytocin levels. Significant difference at T1 and T3 (*p < 0.05); (C) Strong-pain ratings. The decrease in pain ratings from Baseline to Touch condition was greater in HC compared to LC (*p < 0.05). Values denote mean visual analogue scale (VAS; 0–10) (A,C) and mean salivary oxytocin (pg/ml) (B) ±SEM. T1 – upon arrival; T2 – following the first pain-perception measurements; T3 – following 10 mins of either reading or interacting with PARO; T4 – completed while touching PARO (in the PARO group only), following the third, and last, pain-perception measurements.
Discussion
The results revealed that interacting with the baby-seal PARO robot induced an increase in perceived happiness, a decrease in oxytocin levels and a reduction in pain ratings to both mild and strong heat stimuli. Moreover, the reduction in pain ratings was greater when touching the robot in contrast to being in the mere presence of it. The reduction in pain ratings was correlated with the participants’ positive perceptions of the interaction with PARO, and with oxytocin levels. This is the first study, to the best of our knowledge, to demonstrate a decrease in salivary oxytocin during social interaction.
The effect of the interaction with PARO on emotions
Happiness ratings increased significantly after the interaction with PARO. Happiness is considered to be a central human goal across cultures60 and is an important determinant of well-being61. As humans are inherently social, happiness is often related to social interaction. An extensive body of research emphasizes the key role of positive social connections in humans’ perceived happiness, satisfaction and stress buffering e.g62–65.. It appears that the effect of social connections on happiness is not exclusive to human-human interactions. Positive emotions, including happiness, were also found to be associated with interaction with companion animals66–68 and, in the recent two decades, with interactions with social robots69,70. Although there is broad evidence on the link between human-animal and human-robot social interactions and perceived happiness, stress and well-being, the majority of the studies examined either children, the elderly or hospitalized populations while only few focused on healthy adult population71; for review see67,72. Moreover, we could find only two controlled studies examining, as we did, the effect of controlled social interaction on the emotional state. Both of these investigated the effect of interaction with a social entity on the emotional state of children, using a pet dog73 or the PARO robot74. Both studies showed that the interaction with the social entity (pet dog or PARO robot) increased positive emotions, including happiness. Our current study, adds to the existing body of knowledge, in demonstrating that interaction with the PARO robot is effective in increasing perceived happiness also in healthy adults. The correlation we found between participants’ positive perceptions of PARO’s feelings and the increase in happiness further support this finding.
The effect of the interaction with PARO on oxytocin levels
In this study, oxytocin levels decreased only in the PARO group while no change in oxytocin levels was found in the control group throughout the experiment. In the PARO group, there was an inverse correlation between oxytocin levels and the sense of connection with PARO: the lower oxytocin levels were at T4, the higher was the participant’s willingness to meet it again. This is the first study to examine endogenous oxytocin levels during human-robot interaction (HRI). Over the last decade, several studies have examined the role of oxytocin in human relations. The strongest relationship was found with stress, with several studies showing that an increase in physiological and psychological stress is associated with an increase in endogenous oxytocin, whether in saliva or plasma75–79. Similarly, removal of a stressor induces a rapid decrease in oxytocin75–77. Moreover, a recent meta-analysis concluded that even a novel laboratory context may induce a significant oxytocin increase80. The results of these studies suggest that participants arriving to the novel laboratory setting in the current study may have experienced an increase in oxytocin levels during the first measurement of oxytocin (T1). The reduction in oxytocin levels at T3 and T4 in the PARO group may have resulted from participants feeling more at ease due to the interaction with PARO. That is, it appears that the interaction with PARO led to a decrease in stress and an accompanying rapid decrease in oxytocin levels. In contrast, control participants appear to have remained at higher levels of alertness throughout the experimental session, as evidenced by their unchanged salivary oxytocin levels. These findings support previous findings on the role of oxytocin as an important hormone in the stress system, which shows a positive association with cortisol80, known to respond to social stimuli.
Another vein of research points to a positive association between oxytocin and social interaction, which at first seems to be at odds with the current findings. These studies focus on positive interactions with romantic partners or with family members, such as during parent-infant bonding25,81 and romantic relationships20,31,82 However, interactions with non-close others seem to be less effective in activating oxytocin release. For example, a study conducted with chimpanzees found that oxytocin elevation was specific to grooming kin or potential mating partners while no increase in oxytocin was found for grooming chimpanzees that did not have a strong social bond83. Among humans, Feldman et al.25 demonstrated increase in both salivary and plasma oxytocin only among mothers displaying high levels of affectionate contact during mother-infant interaction. Thus, it appears that there is a U-shaped relationship between oxytocin secretion, stress, and social bonding. The interaction with PARO appears to have reduced the stress level of participants, leading to a reduction in salivary oxytocin levels, compared to controls, who did not meet PARO, and their salivary oxytocin levels remained constant. Indeed, several studies show that the effect of oxytocin on behavior is context-dependent and may induce, at the same time, bonding and trust toward in-group members, while increasing aggression and mistrust toward out-group members;84–92 for a review see93. For example, administration of nasal oxytocin enhanced cautious behavior and feeling of mistrust during a social dilemma88 as well as promoted aggressive behavior during a social game89.
These results suggest that a decrease in oxytocin levels may facilitate trust and sociability with members of an out-group. Since individuals may identify robots as out-group members94, the observed decrease in oxytocin levels might be related to the participants’ inclination to lower their aggression toward it and to establish their trust in it. The negative correlation found between oxytocin levels and participants’ willingness to meet PARO again, further support this explanation.
In the current study, we had nearly equal numbers of males and females in both the PARO and the control groups, and we did not test the effects of gender on oxytocin levels. The observed effect of the interaction with PARO on oxytocin levels thus appears to be in addition to any gender effects, if those exist. As endogenous oxytocin levels appear to depend on a variety of factors95, it would be instructive to test, in a future study, whether gender plays a role in endogenous oxytocin levels when interacting with a social robot.
The effect of the interaction with PARO on pain perception
The results reveal diminished levels of pain during the interaction with PARO compared to baseline and compared to the control group. The decrease in pain ratings was more pronounced in the Touch condition compared to the No-Touch condition. Thus, this study highlights remarkable benefits of human-robot social interactions on pain perception. In accordance with our findings, previous data indicate that interaction with PARO or humanoid robot reduces clinical pain among pediatric patients96, cancer patients49 and children undergoing medical procedures50,97. It is important to note that this is the first study to examine the effect of HRI on pain perception among healthy adults. Moreover, it is the first to examine the effect of HRI on pain in a controlled laboratory setting. There are several possible explanations to our findings. First, our finding that touching PARO had the strongest effect in alleviating pain compared to its presence in the room without any physical contact and compared to the control condition, where participants did not meet PARO at all, highlights the effect of social touch on pain alleviation. This is the first study to examine the effect of touching a robot on experimentally induced pain perception. However, among humans, previous studies have found that holding a partner’s hand decreased pain ratings compared to the mere presence of the partner in the room, a stranger’s touch or no interaction, and compared to squeezing a ball33,34. In the current study, the participants gave high ratings to their positive feelings towards PARO. Research indeed suggests that social HRI, and particularly touching a robot, induce positive feelings towards it98,99. Thus, we speculate that touching PARO enabled participants to form an emotional connection with it, which led to similar beneficial outcomes on pain perception as was found during a partner’s touch33,34. It can be also speculated that the interaction with PARO attenuated pain by promoting relaxation. Indeed, recent evidence suggest that touching a robot can reduce stress99. Moreover, Robinson et al.100 showed that stroking PARO reduced blood pressure and heart rate and was accompanied by feelings of happiness and relaxation. Furthermore, there is evidence that high psychosocial stress enhances pain101,102. Indeed, some relaxation techniques were found effective in attenuating pain103–105. Taken together, it is possible that the interaction with PARO led to a more relaxed state of mind and thus reduced pain perception.
Another possible explanation of our finding is that the interaction with PARO distracted the participants away from pain. Changing the focus of attention away from painful stimuli was shown to be efficacious in altering pain perception106–108. Thus, it is possible that having a novel stimulus like PARO in the room distracted the participants away from pain, leading to reduced pain ratings. However, the presence of PARO in the room without any physical contact did not affect mild-pain ratings and affected strong-pain ratings to a lesser extent than did the condition when participants touched PARO. Notably, PARO was active in the No-Touch condition: participants looked at it and were aware of the sounds and movements it made. Thus, if distraction is at play here, then touching PARO provides a more effective distraction than its mere presence in the room. Furthermore, it is likely that there is more at play here than mere distraction, as evidenced by the significantly more pronounced effect that the interaction with PARO had on pain perception in the high-communicators group, suggesting the social aspect of the interaction played a role in modulating pain perception.
One may also speculate that the effect of touching PARO’s fur on pain perception stems from the tactile stimulation of touching a soft object. It was previously demonstrated that tactile stimulation could decrease nociceptive input109,110. This effect is attributed to the capability of sensory fibers to suppress the transmission of nociceptive input111,112. However, this analgesic effect strongly depends on the relative spatial location of the tactile and nociceptive stimuli within the same dermatome. In general, the closer the nociceptive and tactile stimuli, the more powerful the analgesia109,110. In this current study, participants touched PARO in a remote area to the nociceptive stimuli (the arm they used for petting PARO was the opposite arm from the one on which the heat stimuli were applied), thus, this explanation is less probable.
Willemse & Erp99 found that touching a robot is effective in increasing the perceived intimacy with the robot and reducing physiological stress response, and is not dependent on whether there is a prior session of interaction with the robot. Thus, it is likely that, in our experiment, the social touch with PARO induced an effect on both emotions and pain perception regardless of the presence of a preliminary bonding session. This is clinically important since using a robot in the clinical field to improve positive emotions and reduce pain does not seem to require prior acquaintance and hence is easier to implement. Moreover, the effect of touching PARO on pain reduction was demonstrated both in mild and strong pain intensity. This finding further illustrates the clinical potential of human-robot social touch on pain management.
The control group also experienced a reduction in pain ratings compared to baseline levels after reading the Wikipedia article. However, this reduction was significantly smaller compared to the reduction in pain perception in the PARO group. This reduction can be explained by a regression to the mean113, or that reading the article induced a certain level of relaxation and hence reduced pain ratings somewhat.
We further found positive correlations between the empathic concern scores and the participants’ positive perceptions of the interaction with PARO. It has been shown that activation of brain networks involved in the perception of empathy are associated with both pain and social touch24,114. This suggests an interesting basis for future exploration of the connection between empathic concern level, and the pain-alleviating effect of touch in human-robot social interactions. It is possible that high empathic ability enables participants to embrace positive social relationship with PARO, which would amplify the pain-alleviating effect of touching it. This research direction would dovetail with a recent study showing that the empathic abilities of the partner predict the magnitude of pain reduction during touch between partners33.
Further exploring interpersonal traits, the division of the PARO group according to their perceived ability to communicate with PARO revealed that participants classified as “high communicators” exhibited greater pain reduction as well as lower oxytocin levels compared to “low communicators”. These results, along with the significant correlations between participants’ perceptions of the interaction with PARO and the change in pain ratings, demonstrate that the effect of touching PARO on pain perception largely depends on the participant’s ability to form a social connection with PARO. It was found that the ability to communicate contributes to the extraversion personality trait115. It was further shown that a short human-robot social interaction can predict extraversion in a way comparable to the predictive power of human-human interactions116. Other studies demonstrated that high extraverted people exhibit higher affective trust117 and obtain greater benefits from social connection64,117, particularly from social touch117. Our findings thus add to the current literature in demonstrating that high communicators reap greater benefits from the interaction with PARO.
In summary, this study indicates that social touch with PARO robot alleviates pain, increases happiness state and decreases oxytocin levels. Participants with higher perceived ability to communicate with PARO display greater pain alleviation as well as lower oxytocin levels. These findings reveal a profound effect of human-robot social interaction on pain and emotions and hence extend the current knowledge on the impact of social touch on pain and emotions, and offer new strategies for pain management and for improving well-being.
Supplementary information
Acknowledgements
The authors would like to thank Alona Kuzmina for analyzing the salivary oxytocin samples, and Ariel Bistritsky for developing the mobile VAS application. The research was partially supported by the Helmsley Charitable Trust through the Agricultural, Biological and Cognitive Robotics Initiative and by the Marcus Endowment Fund, both at the Ben-Gurion University of the Negev. Financial support was provided by the Rosetrees Trust, the Borten Family Foundation, and the Consolidated Anti-Aging Foundation grants. This research was also supported by the Israel Science Foundation (grants No. 535/16 and 2166/16), the Israel Pain Association, and received funding from the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement No 754340.
Author contributions
N.G. and S.L. designed the experiment. N.G. carried out the experiment and analyzed the data. F.U. performed the lab analysis of the oxytocin samples and commented on the manuscript. N.G. and S.L. interpreted the results and wrote the manuscript. S.L. supervised the project.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors have no competing interests as defined by Nature Research, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
is available for this paper at 10.1038/s41598-020-66982-y.
References
- 1.Berscheid, E. The human’s greatest strength: Other humans., 37–47 (American Psychological Association, 2003).
- 2.Frank DA, Klass PE, Earls F, Eisenberg L. Infants and young children in orphanages: One view from pediatrics and child psychiatry. Pediatrics. 1996;97:569–578. [PubMed] [Google Scholar]
- 3.Rutter, M. Maternal deprivation. Handbook of Parenting Volume 4 Social Conditions and Applied Parenting, 181 (2002).
- 4.Rutter M, O’connor TG. Are there biological programming effects for psychological development? Findings from a study of Romanian adoptees. Developmental psychology. 2004;40:81. doi: 10.1037/0012-1649.40.1.81. [DOI] [PubMed] [Google Scholar]
- 5.Thompson RA. Social support and child protection: Lessons learned and learning. Child Abuse & Neglect. 2015;41:19–29. doi: 10.1016/j.chiabu.2014.06.011. [DOI] [PubMed] [Google Scholar]
- 6.Holt-Lunstad J. Why social relationships are important for physical health: A systems approach to understanding and modifying risk and protection. Annual review of psychology. 2018;69:437–458. doi: 10.1146/annurev-psych-122216-011902. [DOI] [PubMed] [Google Scholar]
- 7.Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social connection as a public health priority in the United States. American Psychologist. 2017;72:517. doi: 10.1037/amp0000103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.DeWall CN, Bushman BJ. Social acceptance and rejection: The sweet and the bitter. Current Directions in Psychological Science. 2011;20:256–260. [Google Scholar]
- 9.Cohen S. Social relationships and health. American psychologist. 2004;59:676. doi: 10.1037/0003-066X.59.8.676. [DOI] [PubMed] [Google Scholar]
- 10.Umberson D, Karas Montez J. Social relationships and health: A flashpoint for health policy. Journal of health and social behavior. 2010;51:S54–S66. doi: 10.1177/0022146510383501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ciechanowski P, Sullivan M, Jensen M, Romano J, Summers H. The relationship of attachment style to depression, catastrophizing and health care utilization in patients with chronic pain. Pain. 2003;104:627–637. doi: 10.1016/S0304-3959(03)00120-9. [DOI] [PubMed] [Google Scholar]
- 12.Galovski T, Lyons JA. Psychological sequelae of combat violence: A review of the impact of PTSD on the veteran’s family and possible interventions. Aggression and violent behavior. 2004;9:477–501. [Google Scholar]
- 13.Forgeron PA, et al. Social functioning and peer relationships in children and adolescents with chronic pain: A systematic review. Pain Research and Management. 2010;15:27–41. doi: 10.1155/2010/820407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rintala, D. H., Hart, K. A. & Priebe, M. M. Predicting consistency of pain over a 10-year period in persons with spinal cord injury. Journal of Rehabilitation Research & Development41 (2004). [DOI] [PubMed]
- 15.Åslund C, Larm P, Starrin B, Nilsson KW. The buffering effect of tangible social support on financial stress: influence on psychological well-being and psychosomatic symptoms in a large sample of the adult general population. International journal for equity in health. 2014;13:85. doi: 10.1186/s12939-014-0085-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Divney AA, et al. Depression during pregnancy among young couples: the effect of personal and partner experiences of stressors and the buffering effects of social relationships. Journal of pediatric and adolescent gynecology. 2012;25:201–207. doi: 10.1016/j.jpag.2012.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Koopman C, Hermanson K, Diamond S, Angell K, Spiegel D. Social support, life stress, pain and emotional adjustment to advanced breast cancer. Psycho‐Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer. 1998;7:101–111. doi: 10.1002/(SICI)1099-1611(199803/04)7:2<101::AID-PON299>3.0.CO;2-3. [DOI] [PubMed] [Google Scholar]
- 18.Turner, J. B. & Turner, R. J. In Handbook of the sociology of mental health 341–356 (Springer, 2013).
- 19.Gliga T, Farroni T, Cascio CJ. Social touch: A new vista for developmental cognitive neuroscience? Developmental cognitive neuroscience. 2019;35:1. doi: 10.1016/j.dcn.2018.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schneiderman I, Zagoory-Sharon O, Leckman JF, Feldman R. Oxytocin during the initial stages of romantic attachment: relations to couples’ interactive reciprocity. Psychoneuroendocrinology. 2012;37:1277–1285. doi: 10.1016/j.psyneuen.2011.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Prescott TJ, Diamond ME, Wing AM. Active touch sensing. Philosophical Transactions of the Royal Society B. 2011;366:2989–2995. doi: 10.1098/rstb.2011.0167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Coan JA, Schaefer HS, Davidson RJ. Lending a hand: Social regulation of the neural response to threat. Psychological science. 2006;17:1032–1039. doi: 10.1111/j.1467-9280.2006.01832.x. [DOI] [PubMed] [Google Scholar]
- 23.Cohen S, Janicki-Deverts D, Turner RB, Doyle WJ. Does hugging provide stress-buffering social support? A study of susceptibility to upper respiratory infection and illness. Psychological science. 2015;26:135–147. doi: 10.1177/0956797614559284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bufalari I, Ionta S. The social and personality neuroscience of empathy for pain and touch. Frontiers in human neuroscience. 2013;7:393. doi: 10.3389/fnhum.2013.00393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Feldman R, Gordon I, Schneiderman I, Weisman O, Zagoory-Sharon O. Natural variations in maternal and paternal care are associated with systematic changes in oxytocin following parent–infant contact. Psychoneuroendocrinology. 2010;35:1133–1141. doi: 10.1016/j.psyneuen.2010.01.013. [DOI] [PubMed] [Google Scholar]
- 26.Barrett C, Arambula S, Young L. The oxytocin system promotes resilience to the effects of neonatal isolation on adult social attachment in female prairie voles. Translational psychiatry. 2015;5:e606. doi: 10.1038/tp.2015.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Carter CS. Neuroendocrine perspectives on social attachment and love. Psychoneuroendocrinology. 1998;23:779–818. doi: 10.1016/s0306-4530(98)00055-9. [DOI] [PubMed] [Google Scholar]
- 28.Moberg, K. U. & Moberg, K. The oxytocin factor: Tapping the hormone of calm, love, and healing. (Da Capo Press, 2003).
- 29.Uvnäs-Moberg K, Arn I, Magnusson D. The psychobiology of emotion: the role of the oxytocinergic system. International journal of behavioral medicine. 2005;12:59–65. doi: 10.1207/s15327558ijbm1202_3. [DOI] [PubMed] [Google Scholar]
- 30.Agren G, Lundeberg T, Uvnäs-Moberg K, Sato A. The oxytocin antagonist 1-deamino-2-D-Tyr-(Oet)-4-Thr-8-Orn-oxytocin reverses the increase in the withdrawal response latency to thermal, but not mechanical nociceptive stimuli following oxytocin administration or massage-like stroking in rats. Neuroscience letters. 1995;187:49–52. doi: 10.1016/0304-3940(95)11335-t. [DOI] [PubMed] [Google Scholar]
- 31.Kreuder AK, et al. Oxytocin enhances the pain‐relieving effects of social support in romantic couples. Human brain mapping. 2019;40:242–251. doi: 10.1002/hbm.24368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Krahé C, Drabek MM, Paloyelis Y, Fotopoulou A. Affective touch and attachment style modulate pain: a laser-evoked potentials study. Philosophical Transactions of the Royal Society B: Biological Sciences. 2016;371:20160009. doi: 10.1098/rstb.2016.0009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Goldstein P, Weissman-Fogel I, Shamay-Tsoory SG. The role of touch in regulating inter-partner physiological coupling during empathy for pain. Scientific reports. 2017;7:3252. doi: 10.1038/s41598-017-03627-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Master SL, et al. A picture’s worth: Partner photographs reduce experimentally induced pain. Psychological Science. 2009;20:1316–1318. doi: 10.1111/j.1467-9280.2009.02444.x. [DOI] [PubMed] [Google Scholar]
- 35.Feingold Polak R, et al. Differences between young and old users when interacting with a humanoid robot: a qualitative usability study. Paladyn, Journal of Behavioral Robotics. 2018;9:183–192. [Google Scholar]
- 36.Feingold Polak, R. & Levy-Tzedek, S. A Social Robot for Rehabilitation: Expert Clinicians and Post-Stroke Patients’ Evaluation Following a Long-Term Intervention. In Proceedings of the 2020 ACM/IEEE International Conference on Human-Robot Interaction (pp. 151–160).
- 37.Eizicovits D, Edan Y, Tabak I, Levy-Tzedek S. Robotic gaming prototype for upper limb exercise: Effects of age and embodiment on user preferences and movement. Restorative neurology and neuroscience. 2018;36:261–274. doi: 10.3233/RNN-170802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kashi S, Levy-Tzedek S. Smooth leader or sharp follower? Playing the mirror game with a robot. Restorative neurology and neuroscience. 2018;36:147–159. doi: 10.3233/RNN-170756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Li J, Chignell M. Communication of emotion in social robots through simple head and arm movements. International Journal of Social Robotics. 2011;3:125–142. [Google Scholar]
- 40.Hoffman G, Weinberg G. Interactive improvisation with a robotic marimba player. Autonomous Robots. 2011;31:133–153. [Google Scholar]
- 41.Clabaugh, C., Tsiakas, K. & Mataric, M. In Proceedings of the Synergies between Learning and Interaction Workshop, IROS, Vancouver, BC, Canada. 24–28.
- 42.Kellmeyer P, Mueller O, Feingold-Polak R, Levy-Tzedek S. Social robots in rehabilitation: A question of trust. Sci. Robot. 2018;3:eaat1587. doi: 10.1126/scirobotics.aat1587. [DOI] [PubMed] [Google Scholar]
- 43.Langer A, Feingold-Polak R, Mueller O, Kellmeyer P, Levy-Tzedek S. Trust in Socially Assistive Robots: Considerations for use in Rehabilitation. Neuroscience & Biobehavioral Reviews. 2019;104:231–239. doi: 10.1016/j.neubiorev.2019.07.014. [DOI] [PubMed] [Google Scholar]
- 44.Shibata, T. Integration of therapeutic robot, paro, into welfare systems. Proceedings of the 28th Annual European Conference on Cognitive Ergonomics 3 (2010).
- 45.Moyle, W. et al. Social robots helping people with dementia: Assessing efficacy of social robots in the nursing home environment. 6th International Conference on Human System Interactions (HSI). 608–613 (2013).
- 46.Wada, K., Shibata, T., Saito, T., Sakamoto, K. & Tanie, K. Psychological and social effects of one year robot assisted activity on elderly people at a health service facility for the aged. Proceedings of the 2005 IEEE international conference on robotics and automation. 2785-2790 (2005).
- 47.Wada K, Shibata T. Living with seal robots—its sociopsychological and physiological influences on the elderly at a care house. IEEE transactions on robotics. 2007;23:972–980. [Google Scholar]
- 48.Shibata, T. et al. Mental commit robot and its application to therapy of children. IEEE/ASME International Conference on Advanced Intelligent Mechatronics. 1053–1058 (2001).
- 49.Eskander R, Tewari K, Osann K, Shibata T. Pilot study of the PARO therapeutic robot demonstrates decreased pain, fatigue, and anxiety among patients with recurrent ovarian carcinoma. Gynecologic Oncology. 2013;130:e144–e145. [Google Scholar]
- 50.Beran TN, Ramirez-Serrano A, Vanderkooi OG, Kuhn S. Humanoid robotics in health care: An exploration of children’s and parents’ emotional reactions. Journal of health psychology. 2015;20:984–989. doi: 10.1177/1359105313504794. [DOI] [PubMed] [Google Scholar]
- 51.Trost MJ, Ford AR, Kysh L, Gold JI, Matarić M. Socially Assistive Robots for Helping Pediatric Distress and Pain. The Clinical Journal of Pain. 2019;35:451–458. doi: 10.1097/AJP.0000000000000688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Koyama Y, Koyama T, Kroncke AP, Coghill RC. Effects of stimulus duration on heat induced pain: the relationship between real-time and post-stimulus pain ratings. Pain. 2004;107:256–266. doi: 10.1016/j.pain.2003.11.007. [DOI] [PubMed] [Google Scholar]
- 53.Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17:45–56. doi: 10.1016/0304-3959(83)90126-4. [DOI] [PubMed] [Google Scholar]
- 54.Sue Carter C, et al. Oxytocin: Behavioral Associations and Potential as a Salivary Biomarker. Annals of the New York Academy of Sciences. 2007;1098:312–322. doi: 10.1196/annals.1384.006. [DOI] [PubMed] [Google Scholar]
- 55.Wada, K., Shibata, T., Saito, T. & Tanie, K. Effects of robot assisted activity for elderly people at day service center and analysis of its factors. Proceedings of the 4th World Congress on Intelligent Control and Automation 1301–1305 (2002).
- 56.Calo, C. J., Hunt-Bull, N., Lewis, L. & Metzler, T. Ethical implications of using the paro robot, with a focus on dementia patient care. Workshops at the Twenty-Fifth AAAI Conference on Artificial Intelligence (2011).
- 57.Monk TH. A visual analogue scale technique to measure global vigor and affect. Psychiatry research. 1989;27:89–99. doi: 10.1016/0165-1781(89)90013-9. [DOI] [PubMed] [Google Scholar]
- 58.Davis MH. Measuring individual differences in empathy: Evidence for a multidimensional approach. Journal of personality and social psychology. 1983;44:113. [Google Scholar]
- 59.Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods. 2007;39:175–191. doi: 10.3758/bf03193146. [DOI] [PubMed] [Google Scholar]
- 60.Veenhoven R. Informed pursuit of happiness: What we should know, do know and can get to know. Journal of Happiness Studies. 2015;16:1035–1071. [Google Scholar]
- 61.Steptoe A. Happiness and health. Annual review of public health. 2019;40:339–359. doi: 10.1146/annurev-publhealth-040218-044150. [DOI] [PubMed] [Google Scholar]
- 62.Hooghe M, Vanhoutte B. Subjective well-being and social capital in Belgian communities. The impact of community characteristics on subjective well-being indicators in Belgium. Social Indicators Research. 2011;100:17–36. [Google Scholar]
- 63.Hsu H-C, Chang W-C. Social connections and happiness among the elder population of Taiwan. Aging & mental health. 2015;19:1131–1137. doi: 10.1080/13607863.2015.1004160. [DOI] [PubMed] [Google Scholar]
- 64.Oerlemans WG, Bakker AB, Veenhoven R. Finding the key to happy aging: A day reconstruction study of happiness. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2011;66:665–674. doi: 10.1093/geronb/gbr040. [DOI] [PubMed] [Google Scholar]
- 65.Requena F. Welfare systems, support networks and subjective well-being among retired persons. Social Indicators Research. 2010;99:511–529. [Google Scholar]
- 66.Bao KJ, Schreer G. Pets and happiness: Examining the association between pet ownership and wellbeing. Anthrozoös. 2016;29:283–296. [Google Scholar]
- 67.Beetz A, Uvnäs-Moberg K, Julius H, Kotrschal K. Psychosocial and psychophysiological effects of human-animal interactions: the possible role of oxytocin. Frontiers in psychology. 2012;3:234. doi: 10.3389/fpsyg.2012.00234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Walsh F. Human‐animal bonds I: The relational significance of companion animals. Family process. 2009;48:462–480. doi: 10.1111/j.1545-5300.2009.01296.x. [DOI] [PubMed] [Google Scholar]
- 69.Góngora Alonso S, et al. Social Robots for People with Aging and Dementia: A Systematic Review of Literature. Telemedicine and e-Health. 2018;25:533–540. doi: 10.1089/tmj.2018.0051. [DOI] [PubMed] [Google Scholar]
- 70.Moerman CJ, van der Heide L, Heerink M. Social robots to support children’s well-being under medical treatment: A systematic state-of-the-art review. Journal of Child Health Care. 2019;23:596–612. doi: 10.1177/1367493518803031. [DOI] [PubMed] [Google Scholar]
- 71.Fiocco A, Hunse A. The buffer effect of therapy dog exposure on stress reactivity in undergraduate students. International journal of environmental research and public health. 2017;14:707. doi: 10.3390/ijerph14070707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Broadbent E. Interactions with robots: The truths we reveal about ourselves. Annual review of psychology. 2017;68:627–652. doi: 10.1146/annurev-psych-010416-043958. [DOI] [PubMed] [Google Scholar]
- 73.Kerns KA, Stuart‐Parrigon KL, Coifman KG, van Dulmen MH, Koehn A. Pet dogs: Does their presence influence preadolescents’ emotional responses to a social stressor? Social Development. 2018;27:34–44. doi: 10.1111/sode.12246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Crossman MK, Kazdin AE, Kitt ER. The influence of a socially assistive robot on mood, anxiety, and arousal in children. Professional Psychology: Research and Practice. 2018;49:48. [Google Scholar]
- 75.Bernhard A, et al. Adolescent oxytocin response to stress and its behavioral and endocrine correlates. Hormones and behavior. 2018;105:157–165. doi: 10.1016/j.yhbeh.2018.08.010. [DOI] [PubMed] [Google Scholar]
- 76.de Jong TR, et al. Salivary oxytocin concentrations in response to running, sexual self-stimulation, breastfeeding and the TSST: The Regensburg Oxytocin Challenge (ROC) study. Psychoneuroendocrinology. 2015;62:381–388. doi: 10.1016/j.psyneuen.2015.08.027. [DOI] [PubMed] [Google Scholar]
- 77.Jurek B, Neumann ID. The oxytocin receptor: from intracellular signaling to behavior. Physiological reviews. 2018;98:1805–1908. doi: 10.1152/physrev.00031.2017. [DOI] [PubMed] [Google Scholar]
- 78.Pierrehumbert B, et al. Oxytocin response to an experimental psychosocial challenge in adults exposed to traumatic experiences during childhood or adolescence. Neuroscience. 2010;166:168–177. doi: 10.1016/j.neuroscience.2009.12.016. [DOI] [PubMed] [Google Scholar]
- 79.Taylor SE, et al. Relation of oxytocin to psychological stress responses and hypothalamic-pituitary-adrenocortical axis activity in older women. Psychosomatic medicine. 2006;68:238–245. doi: 10.1097/01.psy.0000203242.95990.74. [DOI] [PubMed] [Google Scholar]
- 80.Brown CA, Cardoso C, Ellenbogen MA. A meta-analytic review of the correlation between peripheral oxytocin and cortisol concentrations. Frontiers in neuroendocrinology. 2016;43:19–27. doi: 10.1016/j.yfrne.2016.11.001. [DOI] [PubMed] [Google Scholar]
- 81.Feldman R, Gordon I, Zagoory‐Sharon O. Maternal and paternal plasma, salivary, and urinary oxytocin and parent–infant synchrony: considering stress and affiliation components of human bonding. Developmental science. 2011;14:752–761. doi: 10.1111/j.1467-7687.2010.01021.x. [DOI] [PubMed] [Google Scholar]
- 82.Schneiderman I, Kanat-Maymon Y, Zagoory-Sharon O, Feldman R. Mutual influences between partners’ hormones shape conflict dialog and relationship duration at the initiation of romantic love. Social Neuroscience. 2014;9:337–351. doi: 10.1080/17470919.2014.893925. [DOI] [PubMed] [Google Scholar]
- 83.Crockford C, et al. Urinary oxytocin and social bonding in related and unrelated wild chimpanzees. Proceedings of the Royal Society B: Biological Sciences. 2013;280:20122765. doi: 10.1098/rspb.2012.2765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Campbell A. Attachment, aggression and affiliation: the role of oxytocin in female social behavior. Biological psychology. 2008;77:1–10. doi: 10.1016/j.biopsycho.2007.09.001. [DOI] [PubMed] [Google Scholar]
- 85.Campbell P, Ophir AG, Phelps SM. Central vasopressin and oxytocin receptor distributions in two species of singing mice. Journal of Comparative Neurology. 2009;516:321–333. doi: 10.1002/cne.22116. [DOI] [PubMed] [Google Scholar]
- 86.De Dreu CK, et al. The neuropeptide oxytocin regulates parochial altruism in intergroup conflict among humans. Science. 2010;328:1408–1411. doi: 10.1126/science.1189047. [DOI] [PubMed] [Google Scholar]
- 87.Dębiec J. Peptides of love and fear: vasopressin and oxytocin modulate the integration of information in the amygdala. Bioessays. 2005;27:869–873. doi: 10.1002/bies.20301. [DOI] [PubMed] [Google Scholar]
- 88.Declerck CH, Boone C, Kiyonari T. The effect of oxytocin on cooperation in a prisoner’s dilemma depends on the social context and a person’s social value orientation. Social cognitive and affective neuroscience. 2013;9:802–809. doi: 10.1093/scan/nst040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Ne’eman R, Perach-Barzilay N, Fischer-Shofty M, Atias A, Shamay-Tsoory S. Intranasal administration of oxytocin increases human aggressive behavior. Hormones and behavior. 2016;80:125–131. doi: 10.1016/j.yhbeh.2016.01.015. [DOI] [PubMed] [Google Scholar]
- 90.Pedersen CA. Biological aspects of social bonding and the roots of human violence. Annals of the New York Academy of Sciences. 2004;1036:106–127. doi: 10.1196/annals.1330.006. [DOI] [PubMed] [Google Scholar]
- 91.Pfundmair M, Reinelt A, DeWall CN, Feldmann L. Oxytocin strengthens the link between provocation and aggression among low anxiety people. Psychoneuroendocrinology. 2018;93:124–132. doi: 10.1016/j.psyneuen.2018.04.025. [DOI] [PubMed] [Google Scholar]
- 92.Romney C, Hahn-Holbrook J, Norman GJ, Moore A, Holt-Lunstad J. Where is the love? A double-blind, randomized study of the effects of intranasal oxytocin on stress regulation and aggression. International journal of psychophysiology. 2019;136:15–21. doi: 10.1016/j.ijpsycho.2018.08.010. [DOI] [PubMed] [Google Scholar]
- 93.Shamay-Tsoory SG, Abu-Akel A. The social salience hypothesis of oxytocin. Biological psychiatry. 2016;79:194–202. doi: 10.1016/j.biopsych.2015.07.020. [DOI] [PubMed] [Google Scholar]
- 94.Edwards C, Edwards A, Stoll B, Lin X, Massey N. Evaluations of an artificial intelligence instructor’s voice: Social Identity Theory in human-robot interactions. Computers in Human Behavior. 2019;90:357–362. [Google Scholar]
- 95.Quintana, D. S. & Guastella, A. An Allostatic Theory of Oxytocin Signaling. (2019). [DOI] [PubMed]
- 96.Okita SY. Self–Other’s Perspective Taking: The Use of Therapeutic Robot Companions as Social Agents for Reducing Pain and Anxiety in Pediatric Patients. Cyberpsychology, Behavior, and Social Networking. 2013;16:436–441. doi: 10.1089/cyber.2012.0513. [DOI] [PubMed] [Google Scholar]
- 97.Stinson, J., Jibb, L., Nathan, P., Beran, T. & Hum, V. Using a humanoid robot to reduce procedural pain in children with cancer: a pilot randomized controlled trial. Pediatric Blood & Cancer. S54–S55 (Wiley-Blackwell, NJ USA). [DOI] [PubMed]
- 98.Nie, J., Park, M., Marin, A. L. & Sundar, S. S. Can you hold my hand? Physical warmth in human-robot interaction. 7th ACM/IEEE International Conference on Human-RobotInteraction (HRI). 201–202 (2012).
- 99.Willemse, C. J. & van Erp, J. B. Social Touch in Human–Robot Interaction: Robot-Initiated Touches can Induce Positive Responses without Extensive Prior Bonding. International journal of social robotics, 1–20 (2018).
- 100.Robinson H, MacDonald B, Broadbent E. Physiological effects of a companion robot on blood pressure of older people in residential care facility: A pilot study. Australasian journal on ageing. 2015;34:27–32. doi: 10.1111/ajag.12099. [DOI] [PubMed] [Google Scholar]
- 101.Geva N, Pruessner J, Defrin R. Acute psychosocial stress reduces pain modulation capabilities in healthy men. PAIN. 2014;155:2418–2425. doi: 10.1016/j.pain.2014.09.023. [DOI] [PubMed] [Google Scholar]
- 102.Geva N, Pruessner J, Defrin R. Triathletes lose their advantageous pain modulation under acute psychosocial stress. Medicine & Science in Sports & Exercise. 2017;49:333–341. doi: 10.1249/MSS.0000000000001110. [DOI] [PubMed] [Google Scholar]
- 103.Dunford E, Thompson M. Relaxation and mindfulness in pain: A review. Reviews in pain. 2010;4:18–22. doi: 10.1177/204946371000400105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Kwekkeboom KL, Gretarsdottir E. Systematic review of relaxation interventions for pain. Journal of nursing scholarship. 2006;38:269–277. doi: 10.1111/j.1547-5069.2006.00113.x. [DOI] [PubMed] [Google Scholar]
- 105.Smith, C. A. et al. Relaxation techniques for pain management in labour. Cochrane Database of Systematic Reviews3 (2018). [DOI] [PMC free article] [PubMed]
- 106.Chayadi E, McConnell BL. Gaining insights on the influence of attention, anxiety, and anticipation on pain perception. Journal of Pain Research. 2019;12:851. doi: 10.2147/JPR.S176889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.DeMore M, Cohen LL. Distraction for pediatric immunization pain: A critical review. Journal of Clinical Psychology in Medical Settings. 2005;12:281–291. [Google Scholar]
- 108.Johnson MH, Breakwell G, Douglas W, Humphries S. The effects of imagery and sensory detection distractors on different measures of pain: how does distraction work? British Journal of Clinical Psychology. 1998;37:141–154. doi: 10.1111/j.2044-8260.1998.tb01290.x. [DOI] [PubMed] [Google Scholar]
- 109.Mancini F, Beaumont A-L, Hu L, Haggard P, Iannetti GDD. Touch inhibits subcortical and cortical nociceptive responses. Pain. 2015;156:1936. doi: 10.1097/j.pain.0000000000000253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Mancini F, Nash T, Iannetti GD, Haggard P. Pain relief by touch: a quantitative approach. PAIN®. 2014;155:635–642. doi: 10.1016/j.pain.2013.12.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Bourne S, Machado AG, Nagel SJ. Basic anatomy and physiology of pain pathways. Neurosurgery Clinics. 2014;25:629–638. doi: 10.1016/j.nec.2014.06.001. [DOI] [PubMed] [Google Scholar]
- 112.Melzack R. From the gate to the neuromatrix. Pain. 1999;82:S121–S126. doi: 10.1016/S0304-3959(99)00145-1. [DOI] [PubMed] [Google Scholar]
- 113.Barnett AG, Van Der Pols JC, Dobson AJ. Regression to the mean: what it is and how to deal with it. International journal of epidemiology. 2004;34:215–220. doi: 10.1093/ije/dyh299. [DOI] [PubMed] [Google Scholar]
- 114.De Vignemont F, Singer T. The empathic brain: how, when and why? Trends in cognitive sciences. 2006;10:435–441. doi: 10.1016/j.tics.2006.08.008. [DOI] [PubMed] [Google Scholar]
- 115.Akert RM, Panter AT. Extraversion and the ability to decode nonverbal communication. Personality and Individual Differences. 1988;9:965–972. [Google Scholar]
- 116.Rahbar, F. et al. In International Conference on Social Robotics. 543–553 (Springer).
- 117.Erk SM, Toet A, Van Erp JB. Effects of mediated social touch on affective experiences and trust. PeerJ. 2015;3:e1297. doi: 10.7717/peerj.1297. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.