

Abstract
Objectives:
Fermentable carbohydrate is universally recognized as the major dietary risk factor for dental caries. We assessed the broader relationship between diet quality and dental caries in a diverse Latinx adult population.
Methods:
In a cross-sectional probability sample, 14,517 dentate men and women in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) received a dental examination and completed two 24-hours dietary recalls and a food propensity questionnaire. The 2010 Alternative Healthy Eating Index (AHEI) assessed diet quality and the National Cancer Institute method predicted usual intake of the 11 dietary components that comprise the AHEI. Dental caries experience was quantified using the decayed, missing and filled surfaces (DMFS) index. Covariates included sociodemographic and anthropometric characteristics. Survey multivariable-adjusted linear regression models quantified the relationship of 2010 AHEI score, and its 11 components, with DMFS.
Results:
In multivariable-adjusted models, each 10-unit increase in diet quality score was associated with 2.5 fewer (95% confidence interval: −3.4, −1.6) DMFS. The relationship was pronounced among foreign-born individuals, who com-prised three-quarters of the sample, irrespective of their length of US residence, but was not apparent among U.S.-born individuals. Greater intake of sugar-sweetened beverage and fruit juice was positively associated with dental caries, whereas vegetables (excluding potatoes); whole grains; and omega-3 fats were inversely associated with dental caries, independent of covariates and the other dietary components (all P < 0.05).
Conclusions:
An association between diet quality and dental caries was restricted to foreign-born Latinix and was not limited to the adverse impact of sugar-sweetened drinks.
Keywords: dietary patterns, adults, dental caries, epidemiology, sugars, oral health, Hispanic Americans, Migrant, nutrition surveys
Introduction
Dental caries is a highly prevalent disease, irreversible once cavitation occurs, and cumulative over the life span. Sugar consumption remains a causal risk factor for dental caries despite the widespread availability of fluorides.1 Free sugars in the form of sucrose, glucose, fructose, lactose, maltose and starch are a major modifiable etiological factor. Technically, free sugars are the monosaccharides and disaccharides added to foods and beverages during their processing, preparation or at the table, together with sugars naturally present in honey, syrups, fruit juices, and fruit juice concentrates. In their 2015 evidence-based guidelines, the World Health Organization recommends that children and adults restrict intake of free sugars to less than 5 percent of total energy intake to reduce the risk of dental caries over the life span.2
Remarkably, little human studies research has investigated dietary factors other than free sugars as risk or protective factors for dental caries. Several studies investigated intake of individual nutrients such as vitamin D.3 More commonly, studies investigated single components, such as starch,4 milk,5 cheese,6 or tea.7 Together these studies focused on the bioavailability, buffering capacity, consumption frequency, and retentive properties of these individual foods. An alternative approach is to conduct an assessment of the quality of the diet as a whole, considering the overall pattern of food groups consumed rather than the macronutrients alone.
The US conducts ongoing surveillance of dietary intake and dental caries of the noninstitutionalized civilian population through the National Health and Nutrition Examination Survey (NHANES). Although NHANES is a valuable resource at the population level, it lacks precision for the Latinx population, because Latinx of non-Mexican origin are aggregated, masking important variation between those groups.8 Hence, the rationale of this study was to determine the association between diet quality and dental caries experience in a diverse adult Latinx population and examine whether this relationship differed according to nativity status. The second objective was to test the hypothesis that individual dietary components did not differ in the strength of their association with dental caries experience.
Methods
The study was conducted with approval of institutional review boards at each participating institution and the National Heart, Lung and Blood Institute. Written informed consent was obtained from all study participants. This manuscript follows STROBE guidelines for the reporting of observational studies.
Study design, setting, and study population
This analysis reports cross-sectional baseline findings from the population-based, multi-center Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Methodological descriptions of the HCHS/SOL design and implementation9 as well as sample design and cohort selection10 are published. In brief, the study was designed to include adults from Cuban, Dominican, Mexican, Puerto Rican, Central American, and South American backgrounds from four US metropolitan areas, with high concentrations of targeted background groups. Using a stratified two-stage area probability sample design, census block groups were randomly selected in specified census tracts, and households were randomly selected from these census tracts. Households were screened for eligibility, and self-identified Hispanic/Latino adults 18–74 years of age were selected. A total of 16,415 adults enrolled from the Bronx, New York; San Diego, California; Chicago, Illinois; and Miami, Florida, between March 2008 and June 2011. Sampling weights were computed that reflect the probabilities of selection at each stage, non-response and were calibrated to the 2010 US Census population in the target area.
Dental caries experience
The term dental caries experience refers to both the diseased tissue and its treatment through tooth extraction and restoration. As such, it is a measure of lifetime disease and treatment. In epidemiologic surveys, the major measure of dental caries experience is the Decayed, Missing, Filled (DMF) index. When applied at the tooth surface level (five surfaces per posterior tooth and four per anterior tooth), it is called the DMFS index and is expressed as the total number of permanent tooth surfaces that are decayed (D), missing (M), or filled (F) in an individual.
Dentate HCHS/SOL participants received a comprehensive dental examination at the baseline visit. At each field center, dentist examiners (n = 13 in total) completed training in the examination protocol; a modified version of the NHANES protocol. Examiners were centrally trained and calibrated against a standard examiner. Kappa statistics for inter-examiner reliability in recording decayed tooth surfaces, decayed/filled tooth surfaces, and missing teeth, respectively, were 0.77, 0.80, and 0.92.11 Examiners assessed all teeth except third molars with the aid of a surface reflecting mirror and an explorer. Recorders entered the examination calls in the HCHS/SOL Dental Data Entry System. Following a tooth count, examiners assessed each tooth surface. Dental decay on coronal tooth surfaces (D component of the DMFS index) included lesions with frank cavitation, as well as noncavitated lesions. Teeth extracted because of dental caries or periodontal disease were classified as missing (M component of the DMF index), but teeth not present due to trauma, orthodontic treatment or other nondisease-related causes were not counted as missing. A tooth surface that was filled with either a permanent or a temporary restoration as a result of dental caries was coded with the F component of the DMF index. Hence, the dependent variable was the DMFS index, a continuous variable, calculated as the sum of tooth surfaces that were decayed, missing or filled. DMFS scores per individual have a potential range from 0 to 128, with higher counts indicating more disease.
Diet quality and usual food intake
Bilingual interviewers, fluent in Spanish and English, obtained dietary intake information from two 24-hours dietary recalls using the Nutrition Data System for Research software (version 11) developed by the Nutrition Coordinating Center at the University of Minnesota. This version includes more than 18,000 foods in total, listing 8,000 brand-name products, and many Hispanic and Latino foods.8 The first dietary recall was conducted in person at the baseline interview, and the second was conducted by telephone within 30 days of the baseline visit.
Diet quality was assessed using the 2010 Alternative Healthy Eating Index-2010 (AHEI). This scale is composed of 11 dietary components proposed by Chiuve et al.12 based on foods and nutrients predictive of major chronic disease. Higher scores are assigned to higher intakes of six components: vegetables (excluding potatoes); fruits; whole grains; nuts and legumes; long-chain omega-3 fats (docosahexaenoic acid and eicosapentaenoic acid); and other polyunsaturated fatty acids. Lower scores are assigned for higher intakes of four components: red meat; trans-fats; sugar-sweetened beverages and fruit juice; and sodium. Finally, a moderate intake of alcohol is assigned the highest score, and a heavy intake was assigned the lowest score. Scores for whole grains, sodium and alcohol components are sex-specific. Dietary recalls with daily energy intake below the sequence-sex specific 1st percentile or above the 99th percentile were excluded, along with recalls deemed unreliable according to the interviewer. Each component was scored over a range from 0 (worst) to 10 (best), yielding an overall AHEI score with a potential range of 0–110, on which higher scores denote better reported adherence to this purportedly healthy diet.
In addition, a food propensity questionnaire administered at the 1-year follow-up call, asked participants to report frequencies of foods eaten in the previous year. Combined data from the two 24-hours recalls and the food propensity questionnaire were used to generate predicted usual intake of episodically consumed food groups, using the National Cancer Institute methodology.13 This methodology corrects for measurement error in assessing diet by combining two dietary intake instruments. We also included covariates that are known to be associated with differential measurement error (e.g., sex, age, Hispanic/Latino background) to account for some of the bias.
Covariates
Sociodemographic characteristics of age, sex, heritage background, socioeconomic status, nativity status, number of years lived in the United States and health insurance status were assessed in standardized interviews administered by bilingual interviewers. Socioeconomic status was assessed as annual household income (≤$15,000; >$15,000–< $30,000; and ≥ $30,000), and educational attainment (less than high school graduation; and high school graduate or greater). Health insurance was coded as insured or not insured. Nativity status took account of time in United States (US born; foreign born, ≥10 years in United States; and foreign born, <10 years in United States).
Anthropometry was conducted according to standardized protocols by trained personnel. Body mass index (BMI) was calculated as weight in kilograms, obtained with a digital scale (Tanita Body Composition Analyzer, TBF 300; Japan), divided by squared height in meters, measured with a wall stadiometer (SECA 222, Germany) (kg/m2). The continuous BMI term was categorized according to the World Health Organization classification: underweight or normal combined (BMI <25 kg/m2); overweight (BMI 25–29.9 kg/m2) or obese (BMI ≥30 kg/m2). Waist circumference was measured at the horizontal line just above the uppermost lateral border of the right ilium and hip circumference was measured at the level of maximal protrusion of the gluteal muscles. The waist-hip ratio (WHR) was calculated as the ratio of waist circumference to hip circumference. We applied the sex-specific cut-points for WHR risk recommended in a study of anthropometric measures in a Mexican sample.14 Low-risk WHR for women was ≤0.85 and for men was ≤0.90. High-risk WHR for women and men, respectively, were values higher than those cut-points.14
Statistical analyses
Of the 16,415 men and women in HCHS/SOL cohort, 15,577 were dentate, and 15,140 completed the dental examination. We excluded from analysis 151 participants who did not complete at least one reliable 24-hours dietary recall. We computed an “unreported” category for participants with unreported household income (n = 1,192) and excluded from analysis participants with incomplete observations for other covariates, yielding a final analytic sample of 14,517.
Data analyses were performed using Stata/SE 14.2 (StataCorp, College Station, TX), accounting for the complex survey sampling design and sampling weights. Differences were considered statistically significant at P < 0.05.
Univariate analysis modeled AHEI-2010 quintiles, to investigate a possible dose–response association with dental caries experience. Survey linear regression estimated beta coefficients and their 95% confidence intervals (CIs), modeling the change in DMFS per unit increase in AHEI score. In multivariable analysis of main effects, we rescaled the AHEI score by dividing it by 10, so that outcomes are interpretable per 10 units of AHEI. To account for the significant curvilinear relationship between age and DMFS, a quadratic term for age was added to multivariable models, in addition to age in years. As the relationship between BMI and DMFS was not linear, we included BMI categories in regression models. To determine whether current diet quality is more relevant to untreated dental caries, we also modeled the count of decayed tooth surfaces separately as a dependent variable. To determine whether the relationship between diet quality and DMFS differed according to nativity status and years lived in the United States, we fitted an interaction term to the multivariable model, computed as the product of AHEI score and nativity status. The testparm command tested the significance of the effect modification. Using the margins post-estimation commands, we computed linear predictions of DMFS for diet quality and graphed the result to help interpretation.
The predicted components of the AHEI were measured on different scales (i.e., servings/d, mg/d, % calories). To permit comparison of the relative importance of their associations with dental caries experience, we standardized these 11 variables ((AHEI – AHEI mean)/standard deviation to convert scores to a mean of zero and a standard deviation of one).
Results
Dentate individuals had a mean DMFS of 29.2 (range 0–128), meaning that 29 tooth surfaces, on average, showed evidence of past or present coronal dental caries (Table 1). Since dental caries is a unidirectional and progressive disease, DMFS was higher across successive age groups. DMFS was inversely associated with socioeconomic status and positively associated with BMI and waist-hip ratio. In unadjusted analysis, DMFS increased across successive AHEI quintiles. This counterintuitive relationship is explained by the confounding effect of age on the association between diet quality and DMFS (Table S1). Among adults aged 55 and older, 36.0 percent had AHEI scores in the highest quintile, compared with 5.0 percent in the lowest quintile. Effects were similar when the count of decayed tooth surfaces was modeled as the dependent variable (Table S2) as expected, since the mean number of decayed surfaces was 1.12 (standard error = 0.04).
Table 1.
Dental Caries Experience and Diet Quality by Sociodemographic and Health Characteristics, Hispanic Community Health Study/Study of Latinos (N = 14,517), 2008–2011
| Unadjusted N | Weighted col % | DMFS, mean* | 95% Conf. Interval | P-value | AHEI mean† | 95% Conf. Interval | P-value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | 14,517 | 100.0 | 29.2 | 28.2 | 30.1 | 47.5 | 47.2 | 47.8 | ||
| Age (years) | ||||||||||
| 18–34 | 3,472 | 40.2 | 12.2 | 11.7 | 12.8 | <0.001 | 44.7 | 44.3 | 45.1 | <0.001 |
| 35–44 | 2,710 | 21.8 | 26.4 | 25.3 | 27.5 | 47.7 | 47.2 | 48.3 | ||
| 45–54 | 4,407 | 19.0 | 39.9 | 38.5 | 41.2 | 49.1 | 48.6 | 49.6 | ||
| ≥55 | 3,928 | 19.0 | 57.6 | 55.9 | 59.3 | 51.5 | 51.1 | 52.0 | ||
| Sex | ||||||||||
| Women | 8,665 | 51.8 | 32.8 | 31.6 | 34.0 | <0.001 | 46.4 | 46.1 | 46.8 | <0.001 |
| Men | 5,852 | 48.2 | 25.2 | 24.2 | 26.2 | 48.7 | 48.3 | 49.1 | ||
| Heritage group | ||||||||||
| Cuban | 1,967 | 19.1 | 40.3 | 38.5 | 42.0 | 43.7 | 43.3 | 44.0 | <0.001 | |
| Dominican Republic | 1,269 | 9.6 | 30.5 | 27.8 | 33.2 | <0.001 | 48.3 | 47.7 | 48.8 | |
| Mexican | 6,032 | 39.2 | 22.4 | 21.4 | 23.3 | 51.9 | 51.6 | 52.3 | ||
| Puerto Rican | 2,296 | 15.4 | 32.5 | 30.9 | 34.1 | 41.6 | 41.3 | 42.0 | ||
| Central American | 1,558 | 7.5 | 27.2 | 25.5 | 29.0 | 47.0 | 46.6 | 47.5 | ||
| South American | 950 | 4.9 | 36.7 | 34.1 | 39.4 | 45.8 | 45.2 | 46.5 | ||
| More than one, Other | 445 | 4.2 | 21.4 | 17.0 | 25.8 | 46.3 | 45.3 | 47.2 | ||
| Annual household income | ||||||||||
| ≤$15,000 | 4,409 | 28.6 | 34.0 | 32.5 | 35.5 | <0.001 | 47.1 | 46.7 | 47.5 | <0.001 |
| >$15,000 – <$30,000 | 4,564 | 29.9 | 27.7 | 26.4 | 28.9 | 47.8 | 47.4 | 48.2 | ||
| ≥$30,000 | 4,352 | 32.8 | 25.8 | 24.5 | 27.1 | 48.2 | 47.7 | 48.8 | ||
| Unreported | 1,192 | 8.8 | 30.9 | 28.6 | 33.3 | 45.1 | 44.4 | 45.7 | ||
| Educational attainment | ||||||||||
| Less than high school | 5,379 | 31.3 | 32.9 | 31.5 | 34.3 | <0.001 | 48.8 | 48.3 | 49.2 | <0.001 |
| ≥High school graduate | 9,138 | 68.7 | 27.4 | 26.5 | 28.4 | 46.9 | 46.6 | 47.3 | ||
| Health insurance status | ||||||||||
| Not insured | 7,290 | 50.7 | 25.9 | 24.8 | 27.0 | <0.001 | 47.8 | 47.4 | 48.2 | 0.006 |
| Insured | 7,227 | 49.3 | 32.5 | 31.2 | 33.8 | 47.2 | 46.8 | 47.6 | ||
| Nativity status | ||||||||||
| US born | 2,566 | 23.4 | 17.5 | 16.5 | 18.4 | <0.001 | 44.3 | 43.9 | 44.7 | <0.001 |
| Foreign born, ≥10 y in United States | 8,541 | 48.7 | 35.7 | 34.5 | 36.9 | 49.5 | 49.2 | 49.9 | ||
| Foreign born, <10 y in United States | 3,410 | 27.9 | 27.5 | 26.0 | 29.0 | 46.7 | 46.1 | 47.3 | ||
| Body mass index (kg/m2) | ||||||||||
| Underweight/normal, <25 | 2,936 | 23.1 | 24.1 | 22.8 | 25.4 | <0.001 | 46.3 | 45.8 | 46.8 | <0.001 |
| Overweight, 25–29.9 | 5,449 | 37.3 | 30.0 | 28.8 | 31.2 | 48.3 | 47.9 | 48.7 | ||
| Obese, ≥30 | 6,132 | 39.6 | 31.3 | 30.0 | 32.5 | 47.5 | 47.1 | 47.8 | ||
| Waist-hip ratio (sex specific)‡) | ||||||||||
| Low risk | 2,060 | 14.7 | 26.9 | 25.3 | 28.4 | <0.001 | 45.0 | 44.4 | 45.5 | <0.001 |
| High risk | 12,457 | 85.3 | 29.6 | 28.6 | 30.5 | 47.9 | 47.6 | 48.3 | ||
| AHEI score quintiles | ||||||||||
| Q1 (range: 28.17, 41.46) | 2,266 | 20.0 | 23.7 | 22.4 | 25.0 | <0.001 | 37.9 | 37.7 | 38.0 | <0.001 |
| Q2 (range: 41.47, 45.25) | 2,400 | 20.0 | 27.9 | 26.2 | 29.6 | 43.2 | 43.1 | 43.2 | ||
| Q3 (range: 45.26, 49.21) | 2,772 | 20.0 | 30.7 | 28.9 | 32.5 | 46.9 | 46.9 | 47.0 | ||
| Q4 (range: 49.22, 53.90) | 3,078 | 20.0 | 31.3 | 29.5 | 33.0 | 51.1 | 51.1 | 51.2 | ||
| Q5 (range: 53.91, 77.74) | 4,001 | 20.0 | 32.2 | 30.9 | 33.6 | 58.4 | 58.3 | 58.6 | ||
AHEI, Alternative Healthy Eating Index; DMFS, decayed, missing and filled tooth surfaces.
Examiner-determined dental caries experience is quantified as the sum of the number of decayed (D), missing (M) and filled (F) tooth surfaces (S) from 28 teeth (third molars were not examined).
Alternative Health Eating Index-2010 score, in which higher scores denote a better quality diet [range from 0 to 110].
Low risk for waist to hip ratio is ≤0.85 for women and ≤ 0.90 for men.
The overall mean AHEI score was 47.5, ranging from 28 to 78. Men had higher diet quality scores than women (Table 1). Univariate analysis showed that, on average, individuals with better diet quality were older, had higher household income, but lower educational attainment. Among the heritage groups, individuals of Mexican origin had highest diet quality scores, followed by Dominican Republicans, while individuals of Puerto Rican origin had the lowest scores. The diet quality of US-born individuals was markedly poorer than that of the foreign-born.
An unadjusted comparison of predicted usual intake of the 11 dietary components comprising the 2010 AHEI score (Supporting Information Table S3), showed that US-born individuals had statistically significantly worse diet quality scores for each component than foreign-born individuals.
In the regression model adjusted only for field center, sex and age (Table 2, model 1), each 10-unit increase in AHEI was associated with 3.23 (95% CI: −3.94, −2.51) fewer DMF surfaces. This attenuated to 2.53 fewer DMF surfaces (95% CI: −3.43, −1.62) per 10-unit increase in AHEI in the fully adjusted model. Substantial differences in dental caries experience were observed between Heritage groups, even after adjustment for age. Individuals of Cuban origin had approximately 12 more affected tooth surfaces on average than those of Mexican origin.
Table 2.
Multivariable-Adjusted Regression Coefficients (95% CI) for Dental Caries Experience, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
| Model 1 adjusted for field center, age and sex |
Model 2 adjusted for all covariates |
|||||||
|---|---|---|---|---|---|---|---|---|
| β-coefficient | 95% CI | P-value | β-coefficient | 95% CI | P-value | |||
| AHEI, per 10 units* | −3.23 | −3.94 | −2.51 | <0.001 | −2.53 | −3.43 | −1.62 | <0.001 |
| Age (years) | 0.64 | 0.44 | 0.83 | <0.001 | 0.66 | 0.46 | 0.86 | <0.001 |
| Age squared | 0.01 | 0.00 | 0.01 | <0.001 | 0.01 | 0.00 | 0.01 | <0.001 |
| Sex | ||||||||
| Women | 4.95 | 4.01 | 5.88 | <0.001 | 5.69 | 4.64 | 6.73 | <0.001 |
| Men | Referent | Referent | ||||||
| Field center | ||||||||
| Bronx | Referent | Referent | ||||||
| Chicago | −2.30 | −3.77 | −0.83 | 0.002 | −0.06 | −1.62 | 1.50 | 0.942 |
| Miami | 1.34 | −0.18 | 2.86 | 0.083 | −3.53 | −5.63 | −1.43 | 0.001 |
| San Diego | −3.22 | −4.82 | −1.62 | <0.001 | 0.68 | −1.35 | 2.70 | 0.511 |
| Heritage group | ||||||||
| Dominican Republic | 5.98 | 4.04 | 7.92 | <0.001 | ||||
| Central American | 4.98 | 3.14 | 6.82 | <0.001 | ||||
| Cuban | 11.65 | 9.36 | 13.94 | <0.001 | ||||
| Mexican | Referent | |||||||
| Puerto Rican | 2.89 | 0.80 | 4.98 | 0.007 | ||||
| South American | 10.71 | 8.40 | 13.03 | <0.001 | ||||
| More than one, Other | 4.06 | 1.12 | 7.00 | 0.007 | ||||
| Annual household income | ||||||||
| ≤$15,000 | Referent | |||||||
| >$15,000–<$30,000 | −1.97 | −3.02 | −0.92 | <0.001 | ||||
| ≥$30,000 | −1.90 | −3.17 | −0.64 | 0.003 | ||||
| Unreported | −0.86 | −2.49 | 0.77 | 0.302 | ||||
| Educational attainment | ||||||||
| Less than high school | 0.65 | −0.40 | 1.69 | 0.225 | ||||
| ≥High school graduate | Referent | |||||||
| Health insurance | ||||||||
| Not insured | −1.17 | −2.02 | −0.31 | 0.007 | ||||
| Insured | Referent | |||||||
| Nativity | ||||||||
| US born | −0.80 | −2.19 | 0.58 | 0.253 | ||||
| Foreign born, ≥10 y in United States | 0.15 | −1.04 | 1.33 | 0.808 | ||||
| Foreign born, <10 y in United States | Referent | |||||||
| Body mass index (kg/m2) | ||||||||
| Underweight/normal, <25 | Referent | |||||||
| Overweight, 25–29.9 | −1.57 | −2.68 | −0.46 | 0.006 | ||||
| Obese, ≥30 | −0.79 | −1.91 | 0.34 | 0.170 | ||||
| Waist-hip ratio (sex specific) | ||||||||
| Low risk | Referent | |||||||
| High risk | 2.56 | 1.28 | 3.83 | <0.001 | ||||
| Constant | 4.13 | −0.16 | 8.41 | 0.059 | −2.72 | −8.48 | 3.05 | 0.355 |
Dental caries experience is quantified as the sum of the number of DMFS from 28 teeth assessed (third molars not examined). Model 2 additionally adjusts for heritage group, income, education, health insurance, nativity, body mass index and waist-hip ratio.
AHEI, Alternative Healthy Eating Index; DMFS, decayed, missing and filled tooth surfaces.
The continuous AHEI scale was rescaled in units of 10.
A significant effect modification of nativity status was observed (Pinteraction < 0.001; Figure 1) implying a protective effect of healthful diet on oral health among foreign-born individuals. Foreign-born individuals with poor diet quality had substantially more disease than US-born adults with poor diet quality. Yet foreign-born individuals with high diet quality had substantially less disease than their US-born counterparts. The difference in DMFS between AHEI scores of 30 and 70 for foreign-born individuals was approximately 12 tooth surfaces. This effect was not limited to recent migrants, as it persisted among those who had lived in the United States for at least 10 years. Among US-born individuals, a better quality diet was nonsignifi-cantly associated with lower DMFS.
Figure 1.
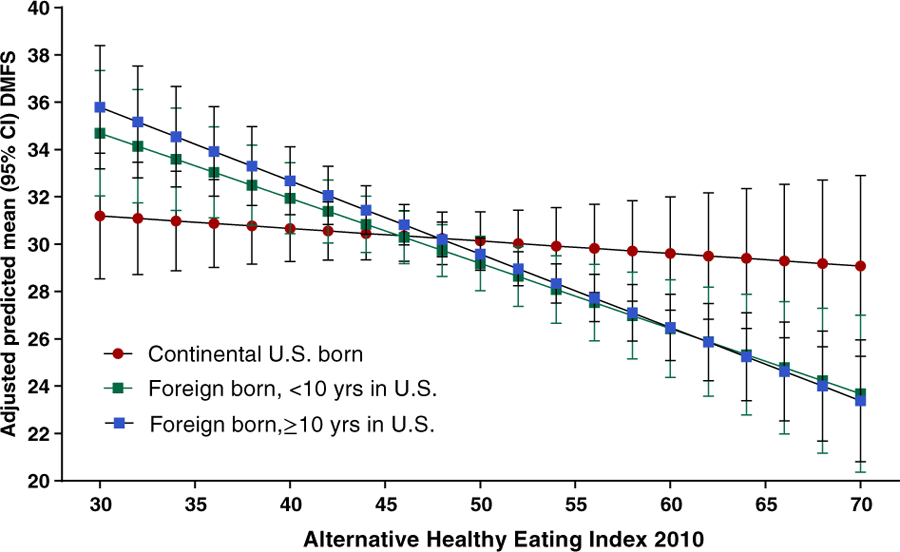
Predicted number of tooth surfaces affected by dental caries experience (DMFS) according to diet quality assessed by the 2010 Alternative Healthy Eating Index (higher scores denote better quality). Values are adjusted marginal means and standard errors predicted from a multivariable-adjusted linear regression model. A statistically significant effect modification of nativity status is evident (P < 0.001), whereby the inverse association between a better quality diet and dental caries experience is pronounced among foreign-born individuals. Model adjusts for field center, sex, age in years, age squared, heritage group, household income, education, health insurance status, body mass index, and waist to hip ratio (N = 14,517).
Comparison of the standardized predicted usual intake of the AHEI components (Table 3), confirmed the expected relationship between dietary sugars and dental caries. For each standard deviation increase in sugar-sweetened drinks and fruit juice, dental caries experience increased by 0.88 tooth surfaces (95% CI: 0.34, 1.42) after adjusting for covariates. Of the three dietary components that showed protective associations, whole grains showed the strongest relative effect. Each standard deviation increase in whole grains was associated with 1.22 fewer DMFS (95% CI: −1.95, −0.49). The other two protective components with similar relative importance were vegetables (without potatoes) and long-chain omega-3 fatty acids [eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)].
Table 3.
Associations Between Transformed (z-score)¶ Predicted Usual Intake of AHEI Dietary Components and Dental Caries Experience (DMFS), Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
| Minimally adjusted* |
Covariate-adjusted† |
Fully adjusted‡) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β-coefficient | 95% CI | P value | β-coefficient | 95% CI | P-value | β-coefficient | 95% CI | P value | ||||
| Transformed predicted usual intake¶ | ||||||||||||
| Vegetables without potatoes | −1.16 | −1.74 | −0.59 | <0.001 | −0.85 | −1.39 | −0.31 | 0.002 | −0.74 | −1.33 | −0.16 | 0.013 |
| Whole grains | −3.07 | −3.71 | −2.44 | <0.001 | −1.42 | −2.15 | −0.68 | <0.001 | −1.22 | −1.95 | −0.49 | 0.001 |
| Long-chain (n-3) fats (EPA + DHA) | −0.72 | −1.24 | −0.20 | 0.007 | −0.93 | −1.46 | −0.41 | 0.001 | −0.73 | −1.33 | −0.13 | 0.017 |
| Nuts and legumes | −0.65 | −1.22 | −0.08 | 0.025 | −0.36 | −0.91 | 0.19 | 0.195 | −0.24 | −0.79 | 0.32 | 0.400 |
| Whole fruit | −0.66 | −1.19 | −0.13 | 0.015 | −0.38 | −0.92 | 0.15 | 0.160 | −0.09 | −0.66 | 0.49 | 0.768 |
| Polyunsaturated fatty acids | −0.10 | −0.56 | 0.37 | 0.687 | −0.50 | −0.99 | −0.01 | 0.047 | −0.34 | −0.86 | 0.18 | 0.198 |
| Transfat | 0.11 | −0.38 | 0.61 | 0.649 | 0.25 | −0.31 | 0.81 | 0.380 | −0.02 | −0.60 | 0.55 | 0.941 |
| Red/processed meat | 1.71 | 0.98 | 2.43 | <0.001 | 0.92 | 0.10 | 1.74 | 0.028 | 0.58 | −0.34 | 1.51 | 0.218 |
| Sugar-sweetened drinks/fruit juice | 0.97 | 0.46 | 1.48 | <0.001 | 1.06 | 0.55 | 1.56 | <0.001 | 0.88 | 0.34 | 1.42 | 0.001 |
| Sodium | 0.83 | 0.17 | 1.49 | 0.014 | 0.13 | −0.55 | 0.81 | 0.714 | 0.50 | −0.38 | 1.38 | 0.265 |
| Alcohol | 0.04 | −0.35 | 0.43 | 0.829 | 0.06 | −0.34 | 0.45 | 0.784 | 0.02 | −0.38 | 0.41 | 0.936 |
Dental caries experience is quantified as the sum of the number of decayed, missing and filled tooth surfaces from 28 teeth assessed (third molars not examined).
AHEI, Alternative Healthy Eating Index; DMFS, decayed, missing and filled tooth surfaces.
Estimates adjusted for field center, age, age squared, and sex.
Estimates additionally adjusted for Heritage group, income, education, health insurance, body mass index and waist-hip ratio.
Estimates additionally adjusted for all the other dietary components.
Predicted usual intake is standardized to have a mean of zero and a standard deviation of 1.
Discussion
In this study of Latinx adults, better diet quality was inversely associated with dental caries experience. Each 10-unit increase in diet quality score was associated with 2.5 (95% CI: −3.4, −1.6) fewer affected tooth surfaces, after adjusting for potential confounding of age and other sociodemographic characteristics, body mass index and waist-hip ratio. A novel finding was that sugar-sweetened drinks/fruit juices was not the only 2010 AHEI dietary component associated with dental caries experience. Greater intakes of long-chain omega-3 fats, whole grains, and vegetables (excluding potatoes) were each inversely associated with dental caries, independently of the other dietary components and the covariates.
Of interest, the inverse association between diet quality and dental caries experience was restricted to foreign-born individuals, who represented three-quarters of participants in this study, and the association remained strong after 10 years residence in the United States. For all 11 dietary components, foreign-born Hispanic/Latinos had healthier scores than the US-born individuals, suggestive of a healthy immigrant effect. What our cross-sectional study is unable to evaluate, is whether acculturation to the United States is responsible for poorer quality diet scores observed among US-born immigrants.
One explanation for the lack of association between diet quality and caries experience among US-born individuals is that their lifetime exposure to other protective factors may overwhelm any additional benefit of a healthy diet. For example, lifetime exposure to community water fluoridation, fluoridated toothpaste, oral hygiene instruction and preventive dental services may obscure the impact of diet. Although Argentina, Chile, Peru, Guyana, Panama, and Guatemala have water fluoridation schemes, population coverage of fluoridated water is comparatively low, ranging from 2 percent in Peru to 65 percent in Chile,15 compared to 74% of US population served by community water systems. Fluoride is critical to remineralization of the hard tooth tissue. In fact, water fluoridation was included among 10 great public health achievements of the last century for its effects in reducing prevalence and severity of dental caries by the Centers for Disease Control and Prevention.16 The estimated prevented fraction of caries averted by water fluoridation is 35 percent (95% CI: 13%–51%) according to a systematic review that compared adults with lifelong water fluoridation exposure, versus no exposure.17
Our finding that adults of Mexican origin had best diet quality conforms with temporal trends assessed over successive NHANES cycles, from 1999 to 2010. In that analysis, where diet quality of assessed using the AHEI, Mexican Americans had the best quality diet among racial/ethnic groups, including the aggregated “Other Hispanics” category at each NHANES cycle, while non-Hispanic blacks had the poorest diet quality.18 Since Hispanic/Latinos and non-Hispanic blacks have similar socioeconomic profiles,19 this supports the argument that diet choices are influenced by factors other than income and education. Our finding that men had a better quality diet than women differs from the US general population,20,21 but conforms with the Multiethnic Cohort study, in which a higher proportion of women than men had 2010 AHEI scores in lowest quartile22 and conforms with a study of South Asian immigrants to the United States, in which men’s diets were of better diet quality than women’s.23
There is biologic plausibility for a protective effect of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) against dental caries. While these long-chain omega-3 polyunsaturated fatty acids, derived from fatty fish, are best known for their anti-inflammatory benefits, new evidence is emerging of their antibacterial properties. Two laboratory studies observed antibacterial effects of EPA and DHA against bacteria involved in periodontal pathology,24,25 and another found antibacterial effects of EPA and DHA against Streptococcus mutans, the predominant cariogenic bacte-rium.26 It is also possible that whole grains and vegetables exert a protective effect by inhibiting oral microflora growth on the tooth surface and thereby limiting acid production, although the evidence remains inconclusive.
Our study builds on a sparse literature of the relationship between dietary patterns and dental caries. Among African American adults with household incomes below 250 percent of the federal poverty level (n = 821), dietary patterns were determined by factor analysis of diet interview data. Investigators found a positive monotonic association between energy from simple sugars and dental caries experience.27 Energy from carbohydrates was also positively associated with caries, but the association was weaker and nonmonotonic. No association was found between dental caries and intakes of vegetables, fruit, grain, meat, dairy products, and a variety of beverages. These null associations might be due to type 2 error due to the overall poor diet quality among these individuals; fewer than 10 percent reported consuming two or more servings of vegetables per day, or two or more servings of fruit.27
The literature for children is slightly larger. Zaki et al. used the 2005 Healthy Eating Index (2005 HEI) – a precursor to the 2010 AHEI with 12 dietary components – to determine the association between diet quality and dental caries in 60 preschool children. Compared to children with dental caries, caries-free children had higher total scores – indicating a better quality diet – and higher component scores for “whole fruit” and “milk.”28 In another study using nationally representative NHANES III data, Nunn et al. computed Healthy Eating Index (HEI) scores for 3,912 dentally examined children aged 2–5 years in. High scores for the fruit, dairy, and cholesterol components of the HEI were associated with a lower prevalence of dental caries.29 Unlike these indices, the 2010 AHEI did not include whole fruit and milk as specific dietary components.
Consistent with earlier diet quality indices, development of the 2010 AHEI was based on food and nutrients predictive of major chronic disease, such as cardiovascular disease, type 2 diabetes and cancer, whose proinflammatory pathways differ from the etiology of dental caries. A diet quality index developed specifically for dental caries would better inform us about dietary risk and protective factors for this disease. However as the public is encouraged to adhere to established dietary indices, such as the 2010 AHEI, that are informed by contemporary nutrition science, it is informative to learn of any benefit, or harm, they may confer to oral health. The finding that a diet conforming to dietary guidelines is associated with lower lifetime experience of dental caries in permanent teeth has generalizability to the broader American adult population.
Supplementary Material
Table S1 Cross tabulation of age group and AHEI quintiles, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
Table S2. Multivariable-adjusted regression coefficients (95% CI) for the association between diet quality and count of decayed tooth surfaces, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
Table S3. Unadjusted mean and standard error (SE) NCI(a) predicted usual intake of dietary components(b), stratified by nativity status, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
References
- 1.Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. J Dent Educ. 2001. October;65(10):1017–23. [PubMed] [Google Scholar]
- 2.World Health Organization. Guideline: sugars intake for adults and children. Geneva: World Health Organization; 2015. [PubMed] [Google Scholar]
- 3.Hujoel PP. Vitamin D and dental caries in controlled clinical trials: systematic review and meta-analysis. Nutr Rev. 2013;71(2):88–97. [DOI] [PubMed] [Google Scholar]
- 4.Halvorsrud K, Lewney J, Craig D, Moynihan PJ. Effects of starch on Oral health: systematic review to inform WHO guideline. J Dent Res. 2019;98(1):46–53. [DOI] [PubMed] [Google Scholar]
- 5.Rodriguez G, Ruiz B, Faleiros S, Vistoso A, Marro ML, Sanchez J et al. Probiotic compared with standard Milk for high-caries children: a cluster randomized trial. J Dent Res. 2016;95(4):402–7. [DOI] [PubMed] [Google Scholar]
- 6.Herod EL. The effect of cheese on dental caries: a review of the literature. Austral Dent J. 1991;36(2):120–5. [DOI] [PubMed] [Google Scholar]
- 7.Gul P, Akgul N, Seven N. Anticariogenic potential of white cheese, xylitol chewing gum, and black tea. Eur J Dent. 2018;12(2):199–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Siega-Riz AM, Sotres-Alvarez D, Ayala GX, Ginsberg M, Himes JH, Liu K, Loria CM, Mossavar-Rahmani Y, Rock CL, Rodriguez B, Gellman MD, Van Horn L. Food-group and nutrient-density intakes by Hispanic and Latino backgrounds in the Hispanic community health study/study of Latinos. Am J Clin Nutr. 2014;99(6):1487–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sorlie PD, Aviles-Santa LM, Wassertheil-Smoller S, Kaplan RC, Daviglus ML, Giachello AL, Schneiderman N, Raij L, Talavera G, Allison M, Lavange L, Chambless LE, Heiss G. Design and implementation of the Hispanic community health study/study of Latinos. Ann Epidemiol. 2010;20(8): 629–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lavange LM, Kalsbeek WD, Sorlie PD, Aviles-Santa LM, Kaplan RC, Barnhart J, Liu K, Giachello A, Lee DJ, Ryan J, Criqui MH, Elder JP. Sample design and cohort selection in the Hispanic community health study/study of Latinos. Ann Epidemiol. 2010;20(8): 642–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Beck JD, Youngblood M Jr, Atkinson JC, Mauriello S, Kaste LM, Badner VM, Beaver S, Becerra K, Singer R. The prevalence of caries and tooth loss among participants in the Hispanic community health study/study of Latinos. J Am Dent Assoc. 2014;145(6):531–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chiuve SE, Rimm EB, Hu FB, Stampfer MJ, Willett WC, Fung TT, Wang M, McCullough ML. Alternative dietary indices both strongly predict risk of chronic disease. J Nutr. 2012;142(6):1009–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tooze JA, Midthune D, Dodd KW, Freedman LS, Krebs-Smith SM, Subar AF, Guenther PM, Carroll RJ, Kipnis V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J Am Diet Assoc. 2006;106(10):1575–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Berber A, Gomez-Santos R, Fanghanel G, Sanchez-Reyes L. Anthropometric indexes in the prediction of type 2 diabetes mellitus, hypertension and dyslipidaemia in a Mexican population. Int J Obes Relat Metab Disord. 2001;25(12):1794–9. [DOI] [PubMed] [Google Scholar]
- 15.British Fluoridation Society. One in a million: the facts about water fluoridation, 3rd edition. Journal [serial on the Internet]. 2012. Date: Available from: https://www.bfsweb.org/one-in-a-million.
- 16.Centers for Disease C, Prevention. Ten great public health achievements—United States, 1900–1999. MMWR Morb Mortal Wkly Rep. 1999;48(12):241–3. [PubMed] [Google Scholar]
- 17.Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007; 86(5):410–5. [DOI] [PubMed] [Google Scholar]
- 18.Wang DD, Leung CW, Li Y, Ding EL, Chiuve SE, Hu FB, Willett WC. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern Med. 2014; 174(10):1587–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fontenot K, Semega J, Kollar M. In: USC B, editors Current Population Reports: Income and Poverty in the United States:2017. Washington, DC: U.S. Government Printing Office; 2018. p. P60–263. [Google Scholar]
- 20.Guenther PM, Kirkpatrick SI, Reedy J, Krebs-Smith SM, Buckman DW, Dodd KW, Casavale KO, Carroll RJ. The healthy eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 dietary guidelines for Americans. J Nutr. 2014;144(3):399–407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hiza HA, Casavale KO, Guenther PM, Davis CA. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J Acad Nutr Diet. 2013;113(2):297–306. [DOI] [PubMed] [Google Scholar]
- 22.Jacobs S, Harmon BE, Ollberding NJ, Wilkens LR, Monroe KR, Kolonel LN, Le Marchand L, Boushey CJ, Maskarinec G. Among 4 diet quality indexes, only the alternate Mediterranean diet score is associated with better colorectal cancer survival and only in African American women in the multiethnic cohort. J Nutr. 2016;146(9):1746–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khan SA, Jackson RT, Momen B. The relationship between diet quality and acculturation of immigrated south Asian American adults and their association with metabolic syndrome. PLoS one. 2016;11(6):e0156851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Choi JS, Park NH, Hwang SY, Sohn JH, Kwak I, Cho KK, Choi IS. The antibacterial activity of various saturated and unsaturated fatty acids against several oral pathogens. J Environ Biol. 2013;34(4):673–6. [PubMed] [Google Scholar]
- 25.Sun M, Zhou Z, Dong J, Zhang J, Xia Y, Shu R. Antibacterial and antibiofilm activities of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) against periodontopathic bacteria. Microb Pathog. 2016;99:196–203. [DOI] [PubMed] [Google Scholar]
- 26.Sun M, Dong J, Xia Y, Shu R. Antibacterial activities of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) against planktonic and biofilm growing Streptococcus mutans. Microb Pathog. 2017;107:212–8. [DOI] [PubMed] [Google Scholar]
- 27.Burt BA, Kolker JL, Sandretto AM, Yuan Y, Sohn W, Ismail AI. Dietary patterns related to caries in a low-income adult population. Caries Res. 2006;40(6):473–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zaki NA, Dowidar KM, Abdelaziz WE. Assessment of the healthy eating Index-2005 as a predictor of early childhood caries. Int J Paediatr Dent. 2015;25(6): 436–43. [DOI] [PubMed] [Google Scholar]
- 29.Nunn ME, Braunstein NS, Krall Kaye EA, Dietrich T, Garcia RI, Henshaw MM. Healthy eating index is a predictor of early childhood caries. J Dent Res. 2009;88(4): 361–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Cross tabulation of age group and AHEI quintiles, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
Table S2. Multivariable-adjusted regression coefficients (95% CI) for the association between diet quality and count of decayed tooth surfaces, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)
Table S3. Unadjusted mean and standard error (SE) NCI(a) predicted usual intake of dietary components(b), stratified by nativity status, Hispanic Community Health Study/Study of Latinos, 2008–2011 (N = 14,517)