

ABSTRACT
This case report describes the treatment of a 48-year-old female patient, smoker, with a closed comminuted pilon fracture (AO/OTA 43-C2.1) and ipsilateral displaced intra-articular calcaneus fracture (AO/OTA 82-C3). Two independent circular frames were applied in a way to preserve tibiotalar range of motion (ROM). The posterior facet of the calcaneus fracture was reduced through a small incision anterior to the tip of the distal fibula. A frame consisting of a two-third ring was applied to the talus and a footplate to the calcaneus was used to hold the reduction of the posterior facet and to correct varus and length. Pilon fracture was similarly reduced with a percutaneous reduction technique and stabilized with the standard two Taylor spatial frame (TSF) rings. During the course of treatment, the tibiotalar joint ROM was maintained. The frame for the calcaneus fracture was removed 10 weeks after the surgery and the frame for the pilon fracture was removed 16 weeks after the surgery. The patient’s last follow-up was 34 months after the injury. She was ambulating independently without limp and she had resumed the preinjury activity level. She had symmetric tibiotalar ROM and 50% reduction in subtalar ROM. The American Orthopaedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot score was 76. Radiographs revealed healed pilon and calcaneus fractures, normal alignment of tibiotalar and subtalar joints, with some arthritic changes present to tibiotalar and subtalar joints. In conclusion, utilization of a “below the ankle” frame for the calcaneus fracture and a standard two-ring frame for the pilon fracture helps to avoid soft tissue complications and preserves tibiotalar ROM.
How to cite this article
Dimitroulias A, Harbacheuski R. Ipsilateral Pilon and Calcaneus Fractures: Treatment with Circular Frame without Spanning Ankle Joint. Strategies Trauma Limb Reconstr 2019;14(2):111–114.
Keywords: Calcaneus fracture, Circular external fixator, External fixator, Ilizarov, Pilon fracture, Taylor spatial frame
INTRODUCTION
Ipsilateral pilon and calcaneus fractures are of rare types. Only few reports exist in literature. Mittal et al.1 presented two cases treated with temporizing external fixation and open reduction internal fixation (ORIF) of both fractures after improvement in soft tissue edema. Another case of bilateral open pilon and calcaneus fractures was reported by Tiedeken et al.2 Pilon injury in this report was treated in staged fashion first with external fixation followed by ORIF, and calcaneus fracture was treated nonoperatively. Yu et al.3 similarly reported the treatment of four such injuries with delayed ORIF.
A case of ipsilateral pilon and calcaneus fracture is presented, who was treated initially with a temporary external fixator and subsequent application of two unlinked circular frames, thus allowing ankle range of motion (ROM) throughout the course of treatment.
CASE DESCRIPTION
A 48-year-old female victim of motor vehicle accident sustained a closed comminuted pilon (AO/OTA 43-C2.1) with comminuted distal fibula fracture and displaced intra-articular calcaneus fracture (AO/OTA 82-C3) (Figs 1 to 4). The patient also had right-side pneumothorax treated with a chest tube. On the day of admission, she had an ankle spanning external fixator applied for temporary stabilization, with the distal pins placed through talar body and medial cuneiform. Ankle computed tomography after application of spanning external fixator revealed improved articular alignment of the tibial plafond due to ligamentotaxis.
Fig. 1.

Injury lateral radiograph of the right ankle
Fig. 4.

Selected computed tomography sagittal plane reconstruction image after spanning external fixator application
After 16 days, the patient returned to the operating room for definitive fixation as due to chest trauma she was not cleared for earlier management. The patient was positioned supine. The pilon fracture was addressed first. Distraction of the fracture was maintained using the unilateral external fixator applied at the time of the initial surgery. A 155-mm full ring [Taylor spatial frame (TSF); Smith & Nephew, Memphis, TN] was mounted to mid-diaphysis of the tibia using two olive wires and two half pins. The articular reduction was then fine-tuned with a percutaneously placed pointed reduction clamp and then a 155 mm full ring was mounted to the distal tibia using one half pin and three olive wires. The circular frame was then locked in position with the six Fast-Fx struts and the unilateral fixator was removed.
Fig. 2.

Injury anterior-posterior radiograph of the right ankle
Fig. 3.

Selected computed tomography coronal plane reconstruction image after spanning external fixator application
The calcaneus fracture was then addressed. Using a previously described technique,4 a “below the ankle frame” was constructed. Two crossed olive wires were placed through the tuber of calcaneus and tensioned on a footplate. Two olive wires then were placed through the talus and mounted on a two-third ring. Distraction between the talus and the calcaneus rings was achieved using threaded rods. Following that, a sinus tarsi approach was done utilizing a 4 cm incision starting 1 cm distal to the fibula toward the fourth metatarsal. The tarsal sinus was entered and the displaced posterior facet of calcaneus was identified. Using a small periosteal elevator, it was elevated against the talus to its anatomic position. An olive wire was placed through the elevated posterior facet toward the sustentaculum tali, it was tensioned and mounted to the two-third ring. The calcaneal and talar rings were held into position with the two threaded rods.
The ankle joint was free to move, allowing approximately 15° of total ROM before the distal tibia and talar rings contact each other (Fig. 5).
Fig. 5.
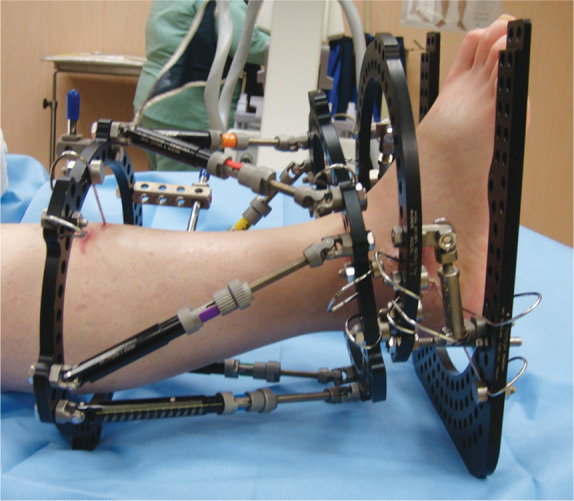
Clinical photograph of the patient's right ankle after application of the two independent circular frames
Postoperatively the patient was encouraged to perform ankle ROM exercises. Appropriate strut adjustments were done to the tibial frame to correct alignment (7 mm of lateral translation). Adjustment schedule was generated using web-based TSF software. Articular alignment of the pilon fracture remained satisfactory during the frame alignment period. The patient remained nonweight-bearing for 10 weeks. Following that the frame used for the calcaneus fracture was removed along with one of the wires from the proximal tibial ring (due to infected pin site) and 2 weeks later the patient started weight-bearing as tolerated. Five months after the initial application of the TSF for the tibial fracture, this was removed and the patient continued weight-bearing as tolerated.
During the last follow-up examination 34 months after the initial injury, she was ambulating independently without assistive device and without any limp and she had completely resumed the preinjury activity level. She had symmetric tibiotalar ROM and 50% reduction in subtalar ROM on the injured side. The AOFAS Ankle–Hindfoot score was 76. Radiographs revealed healed pilon and calcaneus fractures, normal alignment of tibiotalar and subtalar joints, with some arthritic changes present to tibiotalar and subtalar joints (Figs 6 and 7). The hindfoot had symmetric alignment (Fig. 8).
Fig. 6.

Anterior-posterior radiograph of the right ankle during last follow-up
Fig. 7.

Lateral radiograph of the right ankle during last follow-up
Fig. 8.
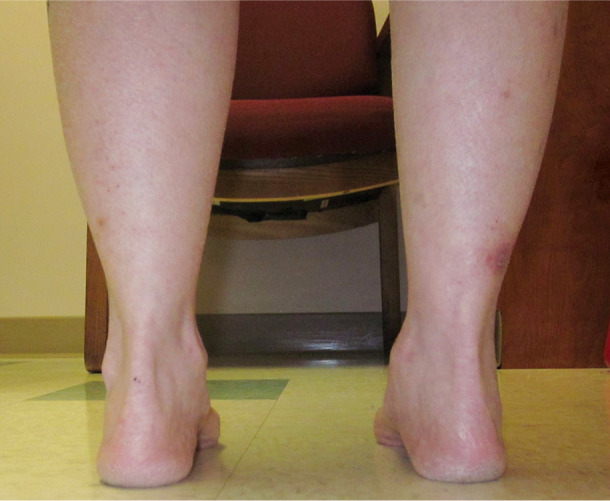
Clinical photograph of the patient's hindfoot alignment during last follow-up
DISCUSSION
Pilon fractures and fractures of the calcaneus are associated with significant soft tissue injury and complications after ORIF. The concomitant presence of both these injuries is additive and compromises even further with the soft tissue envelope. Therefore, soft tissue-friendly surgical techniques are preferred for the treatment of these complex injuries. The advantage of thin wire frame fixation of pilon fractures leaving ankle joint free has been described in the past with successful results.5 Minimally invasive reduction techniques of calcaneus fractures and external fixation that allows ankle ROM have the advantage of minimizing the insult to the soft tissues.4,6 Here we propose that two techniques combined together provide a safe and effective way to treat both injuries. Ankle joint ROM is maintained throughout the course of treatment, decreasing the risk of stiffness. Alternatively, both external fixators can be rigidly linked together, which would allow for tibiotalar joint distraction (arthrodiastasis). This can improve cartilage proteoglycan metabolism after the injury.7 In this case report, however, we preferred to leave both frame unlinked to allow for early ankle ROM after the injury.
Mittal et al. reported two cases of ipsilateral pilon and calcaneus fractures treated with ORIF. First the calcaneus fracture was treated, with the patient in the lateral position followed by addressing the pilon fracture with the patient in the supine position. The method we describe allows for the entire procedure done in supine position with no need for the patient repositioning. This can be advantageous for multitrauma patients. Additionally, on our case report we were able to avoid open reduction in the pilon fracture. This is particularly important as some authors showed that circular frames are associated with less bony or soft tissue complications compared to ORIF for type C pilon fractures.8–11
Disadvantages of the technique are associated with the inherent problems of external fixator device, most commonly pin tract infections. Some fractures may not be amenable for this technique—mainly calcaneus fractures AO/OTA 82-C4 and severely comminuted pilon fractures (C3) not reduced by ligamentotaxis. In conclusion, in this case report, we combined a standard two-ring frame for the pilon fracture and a “below the ankle” frame for the calcaneus fracture. This technique can help avoid soft tissue complications and preserve ankle ROM throughout the course of treatment of ipsilateral pilon and calcaneus fractures.
Footnotes
Source of support: Nil
Conflict of interest: None
REFERENCES
- 1.Mittal R, Matthews SJ, Zavras DT, et al. Management of ipsilateral pilon and calcaneal fractures: a report of 2 cases. J Foot Ankle Surg. 2004;;43((2):):123––130.. doi: 10.1053/j.jfas.2004.01.006. DOI: [DOI] [PubMed] [Google Scholar]
- 2.Tiedeken NC, Hampton D, Shaffer G. Landing on your own two feet: a case report of bilateral calcaneus and open pilon fractures. J Foot Ankle Surg. 2014;;53((5):):647––651.. doi: 10.1053/j.jfas.2014.04.015. DOI: [DOI] [PubMed] [Google Scholar]
- 3.Yu GR, Fan J, Zhou JQ, et al. Characteristics and surgical treatment of combined calcaneal fractures. Zhonghua Wai Ke Za Zhi. 2010;;48((11):):842––846.. [PubMed] [Google Scholar]
- 4.Malizos KN, Bargiotas K, Papatheodorou L, et al. The below-the-ankle circular frame: a new technique for the treatment of displaced calcaneal fractures. J Foot Ankle Surg. 2006;;45((5):):295––299.. doi: 10.1053/j.jfas.2006.06.005. DOI: [DOI] [PubMed] [Google Scholar]
- 5.Bozkurt M, Ocguder DA, Ugurlu M, et al. Tibial pilon fracture repair using Ilizarov external fixation, capsuloligamentotaxis, and early rehabilitation of the ankle. J Foot Ankle Surg. 2008;;47((4):):302––306.. doi: 10.1053/j.jfas.2008.02.013. DOI: [DOI] [PubMed] [Google Scholar]
- 6.Dayton P, Feilmeier M, Hensley NL. Technique for minimally invasive reduction of calcaneal fractures using small bilateral external fixation. J Foot Ankle Surg. 2014;;53((3):):376––382.. doi: 10.1053/j.jfas.2014.01.017. DOI: [DOI] [PubMed] [Google Scholar]
- 7.van Valburg AA, Van Roermund PM, Marijnissen AC. Joint distraction in treatment of osteoarthritis (II): effects on cartilage in a canine model. Osteoarthritis Cartilage. 2000;;8((1):):1––8.. doi: 10.1053/joca.1999.0263. DOI: [DOI] [PubMed] [Google Scholar]
- 8.Watson JT, Moed BR, Karges DE, et al. Pilon fractures. Treatment protocol based on severity of soft tissue injury. Clin Orthop Relat Res. 2000;((375):):78––90.. doi: 10.1097/00003086-200006000-00010. DOI: [DOI] [PubMed] [Google Scholar]
- 9.Endres T, Grass R, Biewener A, et al. Advantages of minimally-invasive reposition, retention, and Ilizarov-(hybrid)fixation for pilon-tibial-fractures fractures with particular emphasis on C2/C3 fractures. Unfallchirurg. 2004;;107((4):):273––284.. doi: 10.1007/s00113-004-0742-x. DOI: [DOI] [PubMed] [Google Scholar]
- 10.Jacob N, Amin A, Giotakis N, et al. Management of high-energy tibial pilon fractures. Strategies Trauma Limb Reconstr. 2015;;10((3):):137––147.. doi: 10.1007/s11751-015-0231-5. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lovisetti G, Agus MA, Pace F, et al. Management of distal tibial intra-articular fractures with circular external fixation. Strategies Trauma Limb Reconstr. 2009;;4((1):):1––6.. doi: 10.1007/s11751-009-0050-7. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]