

Summary
Introduction
The magnitude and underlying determinants of socioeconomic inequality in dental flossing are poorly understood in Iran. This study aimed to measure and decompose socioeconomic inequalities in dental flossing in Ravansar, Iran.
Methods
Data of 10,002 individuals aged 35-65 years who participated in the Ravansar Non- communicable Diseases (RaNCD) cohort study in Kermanshah province, western Iran, were analyzed. Based on an asset-based method, socioeconomic status (SES) was measured using principal component analysis (PCA). The concentration index and curve were employed to measure socioeconomic inequality in dental flossing. Decomposition analysis was used to estimate the contribution of each determinant to the overall inequality.
Results
Of 10,002 participants, 11.74% were found to practice dental floss. The normalized CI for dental flossing was 0.327 in the entire population, 0.323 in females and 0.329 in males, indicating that the use of dental floss is more concentrated among high-SES individuals. The decomposition analysis indicated that SES (50.58%) and level of education (44.90%) respectively contributed the most to this inequality. Place of residence (10.55%) and age group (2.7%) were the next main contributors, respectively.
Conclusions
We found a low prevalence of dental flossing among participants in RaNCD study. We also observed a relatively high degree of pro-rich inequality in dental flossing. The observed inequality was mainly explained by socioeconomic status, level of education and place of residence. Policy interventions should consider these factors to reduce inequalities in dental flossing.
Keywords: Dental flossing, Health inequalities, Concentration index, Decomposition analysis
Introduction
Dental problems are major public health concerns [1] and impact negatively on the quality of life [2]. Almost all adult individuals in the world suffer from dental caries [3]. Oral and dental problems impose a substantial economic burden on individuals, households, and society as a whole [1]. Direct and indirect costs of oral diseases account for around 7% of global health expenditures, implying a high relevance for oral diseases prevention [4]. The disadvantaged bear the greatest fraction of the global burden of oral diseases [5].
It has been indicated that self-performed preventive strategies (e.g., tooth brushing and dental flossing) are cost-effective ways to improve oral health conditions [6]. Regular dental flossing can remove a large portion (i.e., up to 80%) of interdental plaque [7], which impacts both incidences of dental caries and the prevention of periodontal disease [8]. A systematic review indicated that dental flossing, in addition to tooth brushing, has a more effect on the reduction of gingivitis compared to toothbrushing alone [9]. For this reason, the American Dental Associations recommend flossing at least once a day to help remove plaque [10]. Although adherence to such oral hygiene behavior is necessary, a great proportion of individuals floss their teeth less than recommended [11].
Evidence shows that the practice of dental floss in many developing countries like Iran is still low [12]. Moreover, previous reports have indicated that the prevalence of oral and dental problems are unequally distributed across socioeconomic groups, so that individuals with lower socioeconomic status (SES) have a higher burden of dental diseases compared to those of higher SES [13-15]. Socioeconomic inequalities in oral health status have been observed in both developing and developed countries [16].
There is a limited number of studies that have assessed inequalities in oral health outcomes. Most of the existing studies in Iran have only assessed the relationship between SES and oral health status and behaviors, without measuring the extent of socioeconomic-related inequalities in this field [17]. Moreover, to the best of our knowledge, no study has been yet measured socioeconomic inequalities in the practice of dental floss as specific oral hygiene behavior. To fill this gap, this study aimed to quantify: 1) the degree of socioeconomic inequalities in dental flossing; (2) the contribution of each determinant to the measured inequality. The results may be helpful to plan public health policies in oral health fields.
Study population and methodology study setting and sample
This was a cross-sectional analysis of the Ravansar Non-communicable Disease (RaNCD) cohort study. The RaNCD is one of the Prospective Epidemiological Research Studies in IrAN (PERSIAN) [18]. The RaNCD covers adults, aged 35 to 65 years, living in rural and urban areas of Ravansar, which is geographically located in Kermanshah province, west of Iran. The initial sample consisted of 10,086 individuals, 84 of whom were excluded due to incomplete data.
VARIABLES
The SES of individuals was measured using an asset-based approach. The data on housing conditions (e.g. type of homeownership, the number of rooms,) infrastructure facilities (sanitation facility, source of drinking water) and ownership of a range of durable assets (e.g., car, dishwasher, television, etc.) was used to measure SES of individuals. The SES was constructed using principal component analysis (PCA) technique. The PCA generates the weight for each selected asset and then estimates a continuous index based on the sum of all weights of variables included in the PCA for each individual. The index was used to categorize individuals into five SES quintile (from poorest to richest) [19-22]. Other independent variables included age, sex, level of education, marital status and place of residence (i.e. urban and rural). Dental flossing was our dependent variable which was defined dichotomously.
MEASURING INEQUALITY
Inequality in the practice of dental floss was measured using the concentration index (CI). CI is defined based on a concentration curve (CC). These measures are widely used as standard tools for assessing inequalities in health [23, 24]. The concentration curve is a graphical representation of the degree of inequality that plots the cumulative percentage of the health outcome (vertical axis) against the cumulative percentage of the population, ranked based on their rank in SES group (horizontal axis). The 45º line represents perfect equality, meaning that everyone, regardless of their SES, has precisely the same value of the health outcome variable. If the health outcome variable is concentrated among low-SES individuals, the concentration curve lies above the equality line and vice versa. The further the curve is below (above) the 45º line, the more concentrated the health outcome variable is among the high-SES individuals (low-SES individuals). The CI, which ranges between -1 and +1, equals two times the space between the concentration curve and the equality line and shows whether the outcome variable is concentrated among low- or high-SES individuals. Negative and positive values of this index respectively show that the health outcome variable is more concentrated in low- and high-SES individuals, while zero values suggest that the health outcome variable is equally distributed among the SES groups. The following formula was used to calculate the CI [23]:
| (1) |
Where yi is the health outcome variable (i.e. dental flossing); μ denotes its mean; and ri represent the fractional rank of the ith individual in the socioeconomic distribution. As the dental flossing in this study was binary, we used Wagstaff’s normalization method to measure inequality in the use of dental floss as follow:
We decomposed the CI to determine the underlying causes of socioeconomic inequalities in dental flossing. According to Wagstaff for any linear additive regression model linking our health outcome variable (i.e. dental flossing), y to a set of k determinants, xk [25]:
| (2) |
The CI for dental flossing, y, can be decomposed as follows:
| (3) |
Where x̄k denotes the mean of determinant k; the CIk is the CI for  is the elasticity of dental flossing with respect to determinant k.
is the elasticity of dental flossing with respect to determinant k.
The elasticity of each determinant demonstrates the responsiveness of dental flossing to changes in the determinant. A positive elasticity means that individuals with this characteristic are more likely to practice dental floss. The GCε indicates the generalized CI for the error term. The first part in equation 3,  is the explained component and indicates the contribution of explanatory variables to the overall socioeconomic inequality in dental flossing. The second part of the equation, GCε / μ, is an unexplained (residual) component and shows the portion of the CI for dental flossing that cannot be explained by the systematic variations in the determinants across SES groups.
is the explained component and indicates the contribution of explanatory variables to the overall socioeconomic inequality in dental flossing. The second part of the equation, GCε / μ, is an unexplained (residual) component and shows the portion of the CI for dental flossing that cannot be explained by the systematic variations in the determinants across SES groups.
Wagstaff-type decomposition analysis was performed using the following formula [25]:
| (4) |
As our outcome variable was dichotomous, we used marginal effects obtained from the non- linear logit model in the decomposition analysis to estimate the contributions of the explanatory variables to the Cn. All analyses were conducted using STATA software version 14.
Results
A total of 10,002 adults with a mean age of 47.05 (SD ± 9.02) were included in the analysis, 5,259 (52.58%) of whom were women. Participants belonged to the age group of 35-44 years account for 44.07% of the sample and the majority of them was married (90.18%). Also, the illiterate participants accounted for 35.26% of the whole sample. About 11.74% of the study population practiced dental floss. The proportion of dental flossing was higher in the urban population, higher quintiles of SES, the age group of 34-45 and in participants with university degrees (Tab. I).
Tab. I.
Prevalence of dental flossing in terms of determinant variables among cohort participants aged 35-65.
| Variables | N (%) | Prevalence rate (%) |
|---|---|---|
| Sex | ||
| Female | 5,259 (52.58) | 11.28 |
| Male | 4,743 (47.42) | 12.25 |
| Age group | ||
| 35-44 | 4,408 (44.07) | 17.38 |
| 45-54 | 3,327 (33.26) | 10.43 |
| 55-65 | 2,267 (22.67) | 2.69 |
| Marital status | ||
| Married | 9,020 (90.18) | 11.87 |
| Single/divorced/widowed | 982 (9.82) | 10.49 |
| Education | ||
| Illiterate | 4,591 (45.90) | 4.77 |
| Primary | 2,616 (26.15) | 10.86 |
| Intermediate | 1,064 (10.46) | 17.29 |
| Secondary | 968 (9.68) | 21.80 |
| Higher | 763 (7.63) | 36.17 |
| Economic status | ||
| Poorest | 2,001 (20.01) | 6.20 |
| Second poorest | 2,000 (20.00) | 7.10 |
| Middle | 2,003 (20.03) | 8.89 |
| Second richest | 1,998 (19.98) | 13.81 |
| Richest | 2,000 (20.00) | 22.70 |
| Place of residence | ||
| Urban | 5,916 (59.15) | 15.53 |
| Rural | 4,086 (40.85) | 6.24 |
The normalized CI was 0.327 for dental flossing in the entire population, 0.323 in the women and 0.329 in the men. The statistically significant positive value of the shows a higher concentration of practice of dental floss among high-SES individuals (Tab. II).
Tab. II.
Normalized concentration indices (95% Confidence Interval, standard error and p-value) for dental flossing.
| Sample | SE | Normalized CI | 95% CI | P-value | |
|---|---|---|---|---|---|
| Total | 10,002 | 0.017 | 0.327 | 0.292-0.361 | 0.000 |
| Male | 4,743 | 0.025 | 0.329 | 0.280-0.378 | 0.000 |
| Female | 5,259 | 0.024 | 0.323 | 0.275-0.372 | 0.000 |
The concentration curve of dental flossing lies below the line of perfect equality, meaning that the practice of dental floss is more concentrated among high-SES individuals. It indicates that there is inequality in the distribution of dental flossing favoring high-SES individuals (Fig. 1).
Fig. 1.
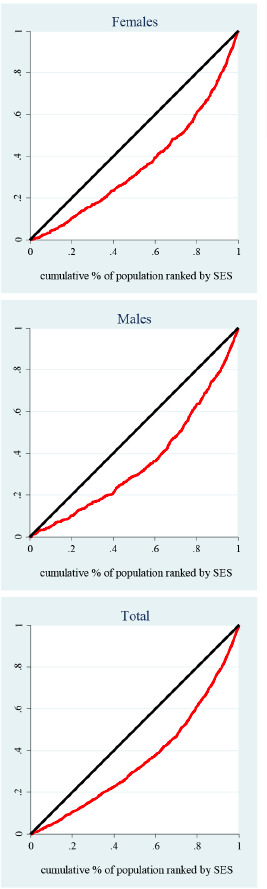
Concentration curves of dental flossing among participants of RaNCD cohort study.
The C for independent variables suggested that women and age group of 55-65 were more concentrated among the low-SES individuals. However, the married and urban participants were more concentrated among high-SES individuals. The decomposition analysis showed that SES (50.58%) and level of education (44.90%) respectively contribute the most to this inequality. The contribution of urban residence and age group in the observed inequalities was 10.55% and 2.70% respectively (Tab. III).
Tab. III.
Decomposition of concentration index for dental flossing.
| Marginal effects | Elasticity | Ck 1 | Cont. 2 | % Cont. 2 | Summed % | |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Female | 0.049 | 0.222 | -0.075 | -0.016 | -5.1 | -5.1 |
| Age group | ||||||
| 35-44 | ||||||
| 45-54 | -0.032 | -0.092 | 0.041 | -0.003 | -1.17 | 2.70 |
| 55-65 | -0.093 | -0.209 | -0.070 | 0.012 | 3.87 | |
| Marital status | ||||||
| Married | -0.0007 | -0.005 | 0.026 | -0.0001 | -0.04 | -0.04 |
| Education | ||||||
| Illiterate | ||||||
| Primary | 0.058 | 0.131 | 0.004 | 0.0005 | 0.16 | 44.90 |
| Intermediate | 0.124 | 0.112 | 0.114 | 0.013 | 3.94 | |
| Secondary | 0.163 | 0.134 | 0.237 | 0.032 | 9.79 | |
| Higher | 0.251 | 0.163 | 0.620 | 0.101 | 31.00 | |
| Socioeconomic status | ||||||
| Poorest | ||||||
| Second poorest | -0.002 | -0.004 | -0.453 | 0.002 | 0.68 | 50.58 |
| Middle | 0.010 | 0.018 | 0.0003 | 0.000 | 0.001 | |
| Second richest | 0.046 | 0.078 | 0.453 | 0.035 | 10.89 | |
| Richest | 0.082 | 0.140 | 0.906 | 0.127 | 39.00 | |
| Place of residence | ||||||
| Urban | 0.050 | 0.252 | 0.136 | 0.034 | 10.55 | 10.55 |
| Total explained | 0.339 | 103.6 | ||||
| Residual | -0.011 | -3.6 | ||||
| Total | 0.327 | 100 | ||||
1: concentration index of each determinants
2: contribution of each determinant to the observed inequality.
Discussion
In the present study, we measured and decomposed socioeconomic inequalities in dental flossing among adults who participated in RaNCD cohort study, Ravansar, Iran. To the best of the authors’ knowledge, no studies have so far been conducted on measuring socioeconomic inequality in the practice of dental floss as a recommended self-care dental practice. We found a prevalence of 11.74% for dental flossing, indicating not satisfactory flossing behavior in the sample. Previous studies [3, 26] also highlighted a poor dental hygiene behavior in Iran. A study on the general population in 2011 with 12,105 individuals reported a prevalence of 16.8% for dental flossing in Iran [3]. In addition to a low prevalence of dental flossing, we found an unequal distribution of the practice of dental floss favoring individuals with higher SES in Ravansar. Previous studies conducted on socioeconomic inequality in oral health in different countries generally suggest inequality in oral health status and behaviors [27-30]. For example, in line with our findings, a study conducted in Brazil indicated that preventive dental care was more concentrated among high-SES groups [16]. A study in the UK also found an unequal distribution in oral health behaviors favoring high-SES groups [30]. In addition, previous works have shown socioeconomic inequality in the practice of hygiene products such as mouthwashes and toothbrushes as well as receiving dental care [28, 29, 31 32].
The decomposition analysis showed that SES and level of education respectively made the most positive contributions to the socioeconomic inequality in flossing behavior. These results imply that the socioeconomic inequality in dental flossing would have been reduced if these determinants had no impact on oral health behaviors or were equally distributed across the SES groups. In accordance with our results, Asgari et al. found that daily tooth brushing and the practice of dental floss are significantly associated with socioeconomic status [33].
Previous studies also have indicated that SES and level of education are the main contributors to socioeconomic inequalities in oral health and the practice of dental care services [16, 30]. Other main contributors to the observed inequality were the place of residence and older age groups. Some studies have also indicated an association between the area of residence and oral health status [17, 34, 35]. In our sample, rural individuals flossed their teeth less frequently than urban individuals. This rural-urban gap may be due to the fact that rural areas tend to have a large proportion of individuals with lower education levels and those with low SES. In general, having a higher level of education and living in a socioeconomically advantaged area result in further opportunities to adopt healthier habits and benefit from health-promoting behaviors [36, 37]. SES and level of education have remained important issues to consider in formulating policies to reduce inequalities in flossing behavior in developing countries including Iran. Our findings suggest that to address inequalities in dental flossing these factors should be considered in policy interventions. For example, providing special services to individuals of low-SES groups and those with lower educational levels may reduce socioeconomic inequality in flossing behavior. In addition, improving oral health literacy by providing educational programs especially in these groups may be effective in mitigating socioeconomic inequality in the practice of dental floss. The study had some limitations. First, although we used a relatively large sample, the participants were not necessarily representative of Iranian adults. Therefore, further studies on the inequality of flossing behavior at national and subnational levels in Iran are recommended. The cross- sectional nature of the study was another limitation, as it did not show causality. Longitudinal studies are recommended to be designed and conducted in the future to judge the causal relationship.
Conclusions
This study indicated a low prevalence and relatively a high degree of pro-rich inequality in the practice of dental floss among Iranian adults. Socioeconomic status, level of education and place of residence contributed the most to the measured inequality. These factors should be considered in formulating intervention programs.
Ethical statement
The ethics committee of Kermanshah University of Medical Sciences approved the study (Ethics Code: IR.KUMS.REC.1398.327).
Figures and tables
Acknowledgements
The present study used the data obtained from Ravansar non-communicable (RaNCD) cohort study as one regional part of the PERSIAN cohort study.
Funding sources: this work was funded by Kermanshah University of Medical Sciences (KUMS). The Iranian Ministry of Health and Medical Education also has contributed to the funding used in the PERSIAN Cohort through Grant no 700/534.
Footnotes
Conflict of interest statement
The authors declare no conflict of interest.
Authors’ contributions
MS and FN, contributed to conception and design of the study, analysis and interpretation of the data. MS and FN drafted and critically revised the manuscript. YP, BH and MMN contributed to data collection and critical revision of the manuscript. BKM and HA performed a search of the literature and contributed to critical revision of the manuscript. All authors read and approved the final manuscript.
References
- [1].Jin L, Lamster I, Greenspan J, Pitts N, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis 2016;22:609-19. https://doi.org/10.1111/odi.12428 - Epub 2016 Jan 20. 10.1111/odi.12428 [DOI] [PubMed] [Google Scholar]
- [2].Cohen-Carneiro F, Souza-Santos R, Rebelo MAB. Rebelo, Quality of life related to oral health: contribution from social factors. Cien Saude Colet 2011;16:1007-15. https://doi.org/10.1590/s1413-81232011000700033 10.1590/s1413-81232011000700033 [DOI] [PubMed] [Google Scholar]
- [3].Asgari F, Majidi A, Koohpayehzadeh J, Etemad K, Rafei A. Oral hygiene status in a general population of Iran, 2011: a key lifestyle marker in relation to common risk factors of non-communicable diseases, Int J Health Policy Manag 2015;4:343-52. https://doi.org/10.15171/ijhpm.2015.18 10.15171/ijhpm.2015.18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Hyde S, Dupuis V, Mariri BP, Dartevelle S. Prevention of tooth loss and dental pain for reducing the global burden of oral diseases. Int Dent J 2017;67:19-25. https://doi.org/10.1111/idj.12328 10.1111/idj.12328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Marcenes W, Kassebaum NJ, Bernabé E, Flaxman A, Naghavi M, Lopez A, Murray CJ. Global burden of oral conditions in 1990-2010: a systematic analysis. J Dent Res 2013;92:592-7. https://doi.org/10.1177/0022034513490168 - Epub 2013 May 29. 10.1177/0022034513490168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Araujo MWB, Charles CA, Weinstein RB, McGuire JA, Parikh-Das AM, Du Q, Zhang J, Berlin JA, Gunsolley JC. Meta-analysis of the effect of an essential oil containing mouthrinse on gingivitis and plaque. J Am Dent Assoc 2015;146:610-22. https://doi.org/10.1016/j.adaj.2015.02.011 10.1016/j.adaj.2015.02.011 [DOI] [PubMed] [Google Scholar]
- [7].Fleming E.B, Nguyen D, Afful J, Carroll MD, Woods PD. Prevalence of daily flossing among adults by selected risk factors for periodontal disease - United States, 2011-2014. J Periodontol 2018;89:933-9. https://doi.org/10.1002/JPER.17-0572 10.1002/JPER.17-0572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Hamilton K, Bonham M, Bishara J, Kroon J, Schwarzer R. Translating dental flossing intentions into behavior: a longitudinal investigation of the mediating effect of planning and self-efficacy on young adults. Int J Behav Med 2017;24:420-7. https://doi.org/10.1007/s12529-016-9605-4 10.1007/s12529-016-9605-4 [DOI] [PubMed] [Google Scholar]
- [9].Worthington HV, MacDonald L, Pericic TP, Sambunjak D, Johnson TM, Imai P, Clarkson JE. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev 2019;4:CD012018 https://doi.org/10.1002/14651858.CD012018.pub2 10.1002/14651858.CD012018.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].American Dental Association (ADA). Statement on regular brushing and flossing to help prevent oral infections. 2019. Available from: https://www.ada.org/en/press-room/news-releases/2013-archive/august/american-dental-association-statement-on-regular-brushing-and-flossing-to-help-prevent-oral
- [11].Gholami M, Knoll N, Schwarzer R. A brief self-regulatory intervention increases dental flossing in adolescent girls. Int J Behav Med 2015;22:645-51. https://doi.org/10.1007/s12529-014-9459-6 10.1007/s12529-014-9459-6 [DOI] [PubMed] [Google Scholar]
- [12].Kauer B, Schütz J, Colussi PR, Oppermann RV, Haas AN, Rösing CK. Self-reported use of dental floss over 13 years: relationship with family income, mother’s age and educational level. Oral Health Prev Dent 2016;14:33-9. https://doi.org/10.3290/j.ohpd.a34375 10.3290/j.ohpd.a34375 [DOI] [PubMed] [Google Scholar]
- [13].Capurro DA, Davidsen M. Socioeconomic inequalities in dental health among middle-aged adults and the role of behavioral and psychosocial factors: evidence from the Spanish National Health Survey. Int J Equity Health 2017;16:34 https://doi.org/10.1186/s12939-017-0529-7 10.1186/s12939-017-0529-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Guarnizo-Herreño CC, Watt RG, Fuller E, Steele JG, Shen J, Morris S, Wildman J, Tsakos G. Socioeconomic position and subjective oral health: findings for the adult population in England, Wales and Northern Ireland. BMC Public Health 2014;14:827 https://doi.org/10.1186/1471-2458-14-827 10.1186/1471-2458-14-827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Tsakos G, Demakakos P, Breeze E, Watt RG. Social gradients in oral health in older adults: findings from the English longitudinal survey of aging. Am J Public Health 2011;101:1892-9. https://doi.org/10.2105/AJPH.2011.300215 - Epub 2011 Aug 18. 10.2105/AJPH.2011.300215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Bof de Andrade F, Drumond Andrade FC, Noronha K. Measuring socioeconomic inequalities in the use of dental care services among older adults in Brazil. Community Dent Oral Epidemiol 2017;45:559-66. https://doi.org/10.1111/cdoe.12323 - Epub 2017 Jul 26. 10.1111/cdoe.12323 [DOI] [PubMed] [Google Scholar]
- [17].Safiri S, Kelishadi R, Heshmat R, Rahimi A, Djalalinia S, Ghasemian A, et al. Socioeconomic inequality in oral health behavior in Iranian children and adolescents by the Oaxaca-Blinder decomposition method: the CASPIAN-IV study. Int J Equity Health 2016;15:143 https://doi.org/10.1186/s12939-016-0423-8 10.1186/s12939-016-0423-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Lindmark U, Hakeberg M, Hugoson A. Sense of coherence and its relationship with oral health-related behaviour and knowledge of and attitudes towards oral health. Community Dent Oral Epidemiol 2011;39:542-53. https://doi.org/10.1111/j.1600-0528.2011.00627.x - Epub 2011 Jul 11. 10.1111/j.1600-0528.2011.00627.x [DOI] [PubMed] [Google Scholar]
- [19].Sahn DE, Stifel D. Exploring alternative measures of welfare in the absence of expenditure data. Rev. Income Wealth 2003;49:463-89. https://doi.org/10.1111/j.0034-6586.2003.00100.x 10.1111/j.0034-6586.2003.00100.x [DOI] [Google Scholar]
- [20].Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan 2006;21:459-68. https://doi.org/10.1093/heapol/czl029 10.1093/heapol/czl029 [DOI] [PubMed] [Google Scholar]
- [21].Howe LD, Hargreaves JR, Huttly SR. Issues in the construction of wealth indices for the measurement of socio-economic position in low-income countries. Emerg Themes Epidemiol 2008;5:3 https://doi.org/10.1186/1742-7622-5-3 10.1186/1742-7622-5-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].McKenzie DJ. Measuring inequality with asset indicators. J Popul Econ 2005;18:229-60. https://doi.org/10.1007/s00148-005-0224-7 10.1007/s00148-005-0224-7 [DOI] [Google Scholar]
- [23].O’Donnell O, Van Doorslaer E, Wagstaff A, Lindelow M. Analyzing health equity using household survey data. World Bank Publications retrieved from:. https://openknowledge.worldbank.org/bitstream/handle/10986/6896/424800ISBN978011OFFICIAL0USE0ONLY10.pdf?sequence=1&isAllowed=y
- [24].Wagstaff A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ 2005;14:429-32. https://doi.org/10.1002/hec.953 10.1002/hec.953 [DOI] [PubMed] [Google Scholar]
- [25].Wagstaff A, Van Doorslaer E, Watanabe N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J Econom 2003;112:207-23. https://doi.org/10.1016/S0304-4076(02)00161-6 10.1016/S0304-4076(02)00161-6 [DOI] [Google Scholar]
- [26].Kasmaei P, Shokravi FA, Hidarnia A, Hajizadeh E, Atrkar-Roushan Z, Shirazi KK, Montazeri A. Brushing behavior among young adolescents: does perceived severity matter. BMC Public Health 2014;14:8 https://doi.org/10.1186/1471-2458-14-8 10.1186/1471-2458-14-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Levin K, Currie C. Inequalities in toothbrushing among adolescents in Scotland 1998-2006. Health Educ Res 2008;24:87-97. https://doi.org/10.1093/her/cym096 - Epub 2008 Jan 31. 10.1093/her/cym096 [DOI] [PubMed] [Google Scholar]
- [28].Perera I, Ekanayake L. Influence of oral health-related behaviours on income inequalities in oral health among adolescents. Community Dent Oral Epidemiol 2011;39:345-51. https://doi.org/10.1111/j.1600-0528.2010.00606.x - Epub 2011 Jan 17. 10.1111/j.1600-0528.2010.00606.x [DOI] [PubMed] [Google Scholar]
- [29].Polk DE, Weyant RJ, Manz MC. Socioeconomic factors in adolescents’ oral health: are they mediated by oral hygiene behaviors or preventive interventions? Community Dent Oral Epidemiol 2010; 38:1-9. https://doi.org/10.1111/j.1600-0528.2009.00499.x - Epub 2009 Oct 21. 10.1111/j.1600-0528.2009.00499.x [DOI] [PubMed] [Google Scholar]
- [30].Shen J, Wildman J, Steele J. Measuring and decomposing oral health inequalities in an UK population. Community Dent Oral Epidemiol 2013;41:481-9. https://doi.org/10.1111/cdoe.12071 - Epub 2013 Aug 31. 10.1111/cdoe.12071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Allin S. Does equity in healthcare use vary across Canadian provinces? Healthc Policy 2008;3:83-99. [PMC free article] [PubMed] [Google Scholar]
- [32].Wamala S, Merlo J, Boström G. Inequity in access to dental care services explains current socioeconomic disparities in oral health: the Swedish National Surveys of Public Health 2004-2005. J Epidemiol Community Health 2006;60:1027-33. https://doi.org/10.1136/jech.2006.046896 10.1136/jech.2006.046896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Asgari I, Ahmady AE. Social factors and dental health in the urban adolescents of Isfahan, Iran. Oral Health Dent Manag 2014;13:798-804. [PubMed] [Google Scholar]
- [34].Ha DH, Do LG, Luzzi L, Mejia GC, Jamieson L. Changes in area-level socioeconomic status and oral health of indigenous Australian children. Journal of Health Care for the Poor and Underserved 2016;27:110-4. https://doi.org/10.1353/hpu.2016.0034 10.1353/hpu.2016.0034 [DOI] [PubMed] [Google Scholar]
- [35].Jamieson LM, Thomson WM. Adult oral health inequalities described using area-based and household-based socioeconomic status measures. J Public Health Dent 2006;66:104-9. https://doi.org/10.1111/j.1752-7325.2006.tb02564.x 10.1111/j.1752-7325.2006.tb02564.x [DOI] [PubMed] [Google Scholar]
- [36].Hakeem FF, Sabbah W. Is there socioeconomic inequality in periodontal disease among adults with optimal behaviours. Acta Odontol Scand 2019;77:400-7. https://doi.org/10.1080/00016357.2019.1582795 - Epub 2019 Mar 28. 10.1080/00016357.2019.1582795 [DOI] [PubMed] [Google Scholar]
- [37].Sabbah W, Sheiham A. The relationships between cognitive ability and dental status in a nationasample of USA adults. Intelligence 2010;38:605-10. https://doi.org/10.1016/j.intell.2010.08.003 10.1016/j.intell.2010.08.003 [DOI] [Google Scholar]