

Key Points
Question
Do liberal vs restrictive transfusion strategies in extremely low-birth-weight infants improve survival and neurodevelopmental outcome at 24 months of corrected age?
Findings
In this randomized clinical trial that included 1013 infants with birth weights less than 1000 g, a strategy of liberal blood transfusions compared with restrictive blood transfusions resulted in a composite outcome of death or disability at 24 months of corrected age in 44.4% vs 42.9%, respectively, a difference that was not statistically significant.
Meaning
Among extremely low-birth-weight infants, a liberal blood transfusion strategy did not reduce the likelihood of death or disability at 24 months compared with a restrictive strategy.
Abstract
Importance
Red blood cell transfusions are commonly administered to infants weighing less than 1000 g at birth. Evidence-based transfusion thresholds have not been established. Previous studies have suggested higher rates of cognitive impairment with restrictive transfusion thresholds.
Objective
To compare the effect of liberal vs restrictive red blood cell transfusion strategies on death or disability.
Design, Setting, and Participants
Randomized clinical trial conducted in 36 level III/IV neonatal intensive care units in Europe among 1013 infants with birth weights of 400 g to 999 g at less than 72 hours after birth; enrollment took place between July 14, 2011, and November 14, 2014, and follow-up was completed by January 15, 2018.
Interventions
Infants were randomly assigned to liberal (n = 492) or restrictive (n = 521) red blood cell transfusion thresholds based on infants’ postnatal age and current health state.
Main Outcome and Measures
The primary outcome, measured at 24 months of corrected age, was death or disability, defined as any of cognitive deficit, cerebral palsy, or severe visual or hearing impairment. Secondary outcome measures included individual components of the primary outcome, complications of prematurity, and growth.
Results
Among 1013 patients randomized (median gestational age at birth, 26.3 [interquartile range {IQR}, 24.9-27.6] weeks; 509 [50.2%] females), 928 (91.6%) completed the trial. Among infants in the liberal vs restrictive transfusion thresholds groups, respectively, incidence of any transfusion was 400/492 (81.3%) vs 315/521 (60.5%); median volume transfused was 40 mL (IQR, 16-73 mL) vs 19 mL (IQR, 0-46 mL); and weekly mean hematocrit was 3 percentage points higher with liberal thresholds. Among infants in the liberal vs restrictive thresholds groups, the primary outcome occurred in 200/450 (44.4%) vs 205/478 (42.9%), respectively, for a difference of 1.6% (95% CI, −4.8% to 7.9%; P = .72). Death by 24 months occurred in 38/460 (8.3%) vs 44/491 (9.0%), for a difference of −0.7% (95% CI, −4.3% to 2.9%; P = .70), cognitive deficit was observed in 154/410 (37.6%) vs 148/430 (34.4%), for a difference of 3.2% (95% CI, −3.3% to 9.6%; P = .47), and cerebral palsy occurred in 18/419 (4.3%) vs 25/443 (5.6%), for a difference of −1.3% (95% CI, −4.2% to 1.5%; P = .37), in the liberal vs the restrictive thresholds groups, respectively. In the liberal vs restrictive thresholds groups, necrotizing enterocolitis requiring surgical intervention occurred in 20/492 (4.1%) vs 28/518 (5.4%); bronchopulmonary dysplasia occurred in 130/458 (28.4%) vs 126/485 (26.0%); and treatment for retinopathy of prematurity was required in 41/472 (8.7%) vs 38/492 (7.7%). Growth at follow-up was also not significantly different between groups.
Results
Among 1013 patients who were randomized (median gestational age at birth, 26.3 [interquartile range {IQR}, 24.9-27.6] weeks; 509 [50.2%] females), 928 (91.6%) completed the trial. Among infants in the liberal vs restrictive transfusion thresholds groups, respectively, incidence of any transfusion was 400/492 (81.3%) vs 315/521 (60.5%); median volume transfused was 40 mL (IQR, 16-73 mL ) vs 19 mL (IQR, 0-46 mL); and weekly mean hematocrit was 3 percentage points higher with liberal thresholds. The primary outcome was not significantly different between groups, nor were the secondary outcomes of death, cognitive deficit, or cerebral palsy. In the liberal vs restrictive thresholds groups, respectively, necrotizing enterocolitis requiring surgical intervention occurred in 20/492 (4.1%) vs 28/518 (5.4%); bronchopulmonary dysplasia occurred in 130/458 (28.4%) vs 126/485 (26.0%); and treatment for retinopathy of prematurity was required in 41/472 (8.7%) vs 38/492 (7.7%). Growth at follow-up was also not significantly different between groups.
| Outcomes | No./total (%) | Absolute difference, % (95% CI) | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|
| Liberal threshold | Restrictive threshold | ||||
| Death or neurodevelopmental impairment by 24 mo | 200/450 (44.4) | 205/478 (42.9) | 1.6 (−4.8 to 7.9) | 1.05 (0.80-1.39) | .72 |
| Death by 24 mo | 38/460 (8.3) | 44/491 (9.0) | −0.7 (−4.3 to 2.9) | 0.91 (0.58-1.45) | .70 |
| Cognitive deficit | 154/410 (37.6) | 148/430 (34.4) | 3.1 (−3.3 to 9.6) | 1.12 (0.83-1.51) | .47 |
| Cerebral palsy | 18/419 (4.3) | 25/443 (5.6) | −1.3 (−4.2 to 1.5) | 0.75 (0.40-1.40) | .37 |
Conclusions and Relevance
Among infants with birth weights of less than 1000 g, a strategy of liberal blood transfusions compared with restrictive transfusions did not reduce the likelihood of death or disability at 24 months of corrected age.
Trial Registration
ClinicalTrials.gov Identifier: NCT01393496
This randomized clinical trial assesses the effect of liberal vs restrictive red blood cell transfusion thresholds (based on postnatal age and current health state) on death or disability at 24 months of age among extremely low-birth-weight infants.
Introduction
It has been estimated that between 1990 and 2016, the overall burden from prematurity-related morbidity, including brain injury, measured as years lived with disability, had the largest increase among all common causes of disability.1
Extremely low-birth-weight (ELBW) infants, ie, those with birth weights of less than 1000 g, uniformly develop anemia of prematurity, caused by developmentally regulated physiological and nonphysiological, iatrogenic, and morbidity-related factors, as reviewed by Widness.2 This anemia may result in impaired oxygen supply to the brain and prematurity-related brain injury, especially in combination with apnea and intermittent hypoxemia or circulatory insufficiency during a period of rapid brain growth and development. Because of this concern, 50% to 80% of ELBW infants studied in 2006-2007 received 1 or more red blood cell transfusions (RBCTs) during their initial hospitalization.3,4 However, RBCTs can have complications,5 and in preterm infants, RBCTs have been associated with intraventricular hemorrhage,6,7 necrotizing enterocolitis,6,8,9 bronchopulmonary dysplasia,3,10 retinopathy of prematurity,11,12 and death.4
Restricting RBCTs to hemoglobin levels of less than 7 g/dL reduced rates of transfusion-related complications, appeared to be safe in short-term studies in pediatric intensive care,13 and was associated with improved survival in younger adults and those with lower severity of illness.14
However, post hoc analyses of the largest randomized trial on transfusion thresholds in ELBW infants to date, the Canadian Premature in Need of Transfusion (PINT) study, suggested that cognitive impairment may be more common with restrictive transfusion thresholds.15
Consequently, the Effects of Transfusion Thresholds on Neurocognitive Outcomes of Extremely Low-Birth-Weight Infants (ETTNO) trial was conducted in ELBW infants to investigate the effects of liberal vs restrictive RBCT strategies on survival and neurocognitive outcome at 24 months of corrected age.
Methods
Trial Design and Oversight
This multicenter, outcome assessor–blinded, parallel-group randomized superiority trial of liberal vs restrictive RBCT strategies was conducted at 36 centers in Europe in compliance with international harmonized guidelines on good clinical practice and the German Pharmaceutical Act. The trial was approved by the German Federal Authority (Paul Ehrlich Institute), the leading Ethics Committee Tübingen, and all ethics committees responsible for participating institutions. After provision of oral and written information, written informed consent was obtained from parents before enrollment. The study protocol is available in Supplement 1.
An independent data and safety monitoring committee supervised the trial after 100, 300, 500, and 700 randomized patients were discharged from the hospitals.
Patients
The only inclusion criterion was a birth weight of 400 g to 999 g. Exclusion criteria were gestational age at birth greater than 29 weeks, 6 days; major anomalies (eg, chromosomal anomalies, cyanotic heart defects, syndromes affecting long-term outcome) or malformations requiring surgical correction during the neonatal period; participation in studies precluding participation in this trial; lack of viability; or comfort care. For multiple pregnancies, only the eligible neonate who was delivered first was enrolled.
Randomization and Masking
Within 72 hours after birth, infants were randomly assigned to 1 of 2 parallel treatment groups. Randomization was stratified by center and birth weight (400-749 g and 750-999 g). The random sequence was computer generated with variable block size (2-10) using the software RandList version 2.1 (DatInf) by personnel not otherwise involved in the study. Allocation concealment was ensured using sequentially numbered, sealed, opaque envelopes. Caregivers were not blinded to treatment, but outcome assessors (pediatric neurologists, psychologists, ophthalmologists, etc) were not aware of treatment group.
Trial Procedures
In both treatment groups, the RBCT hematocrit trigger thresholds prescribed by the study protocol from randomization to discharge home (or transfer) depended on the infants’ postnatal age and current state of health (critical vs noncritical), and exceptions to these guidelines were permitted (but not obligatory) only in case of major surgery and a few other emergencies (Table 1; eTable 1 in Supplement 2).
Table 1. Red Blood Cell Transfusion Hematocrit Trigger Thresholds.
| Postnatal age | Red blood cell transfusion threshold, %a | |||
|---|---|---|---|---|
| Liberal | Restrictive | |||
| Critical health state | Noncritical health state | Critical health state | Noncritical health state | |
| From randomization to 7 d after birthb | <41 | <35 | <34 | <28 |
| 8-21 d | <37 | <31 | <30 | <24 |
| >21 d | <34 | <28 | <27 | <21 |
In both treatment groups, the red blood cell transfusion trigger thresholds were applied from randomization to discharge home (or transfer). Trigger thresholds also depended on current state of health; critical was defined as an infant having at least 1 of the following criteria: invasive mechanical ventilation, continuous positive airway pressure with fraction of inspired oxygen >0.25 for >12 hours per 24 hours, treatment for patent ductus arteriosus, acute sepsis or necrotizing enterocolitis with circulatory failure requiring inotropic/vasopressor support, >6 nurse-documented apneas requiring intervention per 24 hours, or >4 intermittent hypoxemic episodes with pulse oximetry oxygen saturation <60%. Exceptions from these guidelines were permitted (but not obligatory) in case of major surgery, major hemorrhage (estimated blood loss >10% of an infant’s blood volume), unexplained lactic acidosis (arterial lactate >4 mmol/L), and unforeseen emergencies. Trigger thresholds in 34 centers were strictly based on venous or arterial hematocrit values only (obtained predominantly from complete blood cell counts and rarely from centrifuged hematocrit capillaries). Four centers (36 patients) used hemoglobin trigger thresholds, with hemoglobin concentrations also determined by co-oximetry/photometry from capillary blood samples; see eTable 1 in the Supplement for the corresponding hemoglobin trigger thresholds applied in these centers.
From randomization to 7 days after birth does not include the full 7 days depending on the time point of randomization.
If an indication was met, a dose of 20 mL/kg of standard whole blood–derived, leukocyte-depleted erythrocyte concentrate was administered per RBCT in both treatment groups. Selection, labeling, and handling of erythrocyte concentrate was according to centers’ practices and had to meet national guidelines and regulations. In 1394 (64%) of 2162 RBCTs, blood cells had been irradiated.
Administration of erythropoietin was prohibited. Standardization of delayed cord clamping/umbilical cord milking, prerandomization RBCT thresholds, and iron, protein, vitamin B12, and folic acid supplementation were recommended as described in the study protocol (Supplement 1).
Outcomes
The primary outcome measure was the incidence of death or neurodevelopmental impairment by 24 (±1) months of corrected age. Neurodevelopmental impairment was defined as any of the following: (1) cognitive deficit, defined as a Mental Developmental Index (MDI) score on the Bayley Scales of Infant Development Second Edition (Bayley 2) of less than 85, a Bayley 2 cognitive raw score below the lower margin of the MDI, inability to be tested because of severe impairment, another cognitive test (eg, Bayley Third Edition) score of more than 1 SD below the mean, or assessment by the child’s pediatrician indicating cognitive deficit; (2) cerebral palsy, defined according to the Surveillance of Cerebral Palsy in Europe network16,17; or (3) severe visual or hearing impairment, defined as best corrected visual acuity of less than 6/60 and/or need for hearing aid or cochlear implant. Presence of a single component indicating neurodevelopmental impairment was sufficient for the diagnosis. If information on 1 or more component was missing, while none of the other components indicated neurodevelopmental impairment, the latter was considered incomplete/nonassessable. Application of the Bayley Scales was required to be done by trained examiners. Scores on both the MDI and the Psychomotor Development Index (PDI) of the Bayley Scales are standardized to a mean of 100 and a standard deviation of 15, with a range from 50 to 150.
Secondary outcome measures were the individual components of the composite primary outcome, the incidence of cognitive deficit (defined as an MDI score less than 70), the MDI score, and the PDI score. Further secondary end points were measures of growth at discharge and follow-up, length of hospital stay, and the time intervals from birth to final discontinuation of positive pressure respiratory support, respiratory stimulant (methylxanthine) therapy, and gavage feeding.
Further end points were Gross Motor Function Classification System score and incidence of all major complications of prematurity (ie, bronchopulmonary dysplasia, retinopathy of prematurity, necrotizing enterocolitis, intestinal perforation, brain injury on cranial ultrasound, patent ductus arteriosus requiring therapy, and nosocomial infections) as defined in the study protocol (Supplement 1).
Adverse events were reported spontaneously according to guidelines on good clinical practice or recorded systematically (complications of prematurity).
Sample size calculations were based on χ2 tests with 80% power, a 2-sided α = .05 significance level, and rates for the primary outcome estimated from the PINT trial15 of 109/213 (51%; liberal threshold group) vs 126/208 (61%; restrictive threshold group), as described in more detail in the eAppendix in Supplement 2. Three hundred ninety patients in each group were required to demonstrate a difference based on the assumption of an absolute risk reduction of 10 percentage points. The assumed rate for loss to follow-up through 24 months was secondarily adjusted from 15% to 20% (amendment to the protocol in 2014 based on information from the German Neonatal Network). Consequently, the trial needed to enroll 980 infants to ascertain data on the primary outcome in 780 infants.
Statistical Analysis
The analysis of the primary outcome in the population of all randomized patients was performed according to randomized treatment group assignment by logistic regression with the factors of treatment, center, and birth weight stratum to test the null hypothesis of equal proportions in the 2 treatment groups. The assumption of no outliers in standardized residuals was assessed graphically (eFigure 1 in Supplement 2). In a prespecified sensitivity analysis, the primary outcome was analyzed in the population of all randomized patients using a worst-case scenario in which all missing 2-year outcomes were counted as death or neurodevelopmental impairment.
Secondary outcome variables were compared between treatment groups by logistic regression (binary) and by analysis of variance (quantitative) because these were approximately normally distributed using the factors of treatment, center, and birth weight stratum (if iterations converged; otherwise, reduced models were fitted). Post hoc, risk differences with 95% confidence intervals were calculated for binary primary and secondary outcome variables without adjustment for center and birth weight because perinatal characteristics were similar in both groups and sample sizes per center were small.
Analyses of secondary outcomes as well as prespecified sensitivity and subgroup analyses were performed in all randomized patients according to their randomly allocated treatment group. Predefined subgroup analyses of the primary outcome variable, cerebral palsy, and the MDI score were performed for males vs females, lower vs higher birth weight strata, and lower vs higher pulse oximetry oxygen saturation target range (by center standard). Post hoc analyses for differences in treatment effects between subgroups were performed by the Breslow-Day test. A predefined per-protocol analysis was performed for all randomized infants who did not violate inclusion/exclusion criteria and underwent transfusion according to protocol from randomization until discharge home (in whom all RBCTs were according to trigger thresholds or exceptional indications, and all hematocrit measurements below trigger thresholds were followed by RBCT within 2 days).
All tests were 2-sided at a significance level of P = .05. Because of the potential for type I error due to multiple comparisons, findings of the analyses of secondary end points should be interpreted as exploratory.
It was decided post hoc, but before data analysis, to analyze and report on RBCT only until 36 weeks of postmenstrual age because of very small/nonrepresentative numbers beyond that date (eTable 2 in Supplement 2). Rates of cognitive deficit according to mode of classification were descriptively compared post hoc between treatment groups. Also post hoc, the German Neonatal Network database was searched for ELBW infants born during the recruitment period of this trial for comparison of gestational age at birth to exclude a selection bias (eTable 3 in Supplement 2).
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc).
Results
Between July 14, 2011, and November 14, 2014, a total of 1013 infants (median gestational age at birth, 26.3 [interquartile range, 24.9-27.6] weeks; 509 [50.2%] females) were enrolled into the study; 492 were randomized to liberal thresholds and 521 to restrictive thresholds (Figure 1). Of these infants, 977 (96.4%) were enrolled in 32 level III/IV neonatal intensive care units (NICUs) in Germany, 30 (3.0%) in 2 NICUs in Denmark, 5 (0.5%) in 1 NICU in the Czech Republic, and 1 (0.1%) in Estonia. The median number of infants with birth weights of less than 1500 g admitted to these NICUs was 90 (interquartile range, 66-112) per year during the preceding 5 years. The number of infants each site contributed to the study is provided in eTable 4 in Supplement 2.
Figure 1. Flow of Participants in the Effects of Transfusion Thresholds on Neurocognitive Outcomes of Extremely Low-Birth-Weight Infants (ETTNO) Trial.

RBCT indicates red blood cell transfusion.
aMore than 1 reason was possible.
bMore than 1 reason was possible. Because investigators’ decisions not to approach parents could have introduced selection bias (eg, by preventing the sickest infants to enter this study), the study population was compared with the cohort of the German Neonatal Network database and no indication of selection bias was found (eTable 3 in Supplement 2).
c“Missed” indicates not approached despite being eligible; reason not known.
dGestational age at birth <23 weeks was not a predefined exclusion criterion, but some centers opted not to include these infants. Ten infants with gestational age at birth <23 weeks are listed under various other exclusion criteria.
eAccording to the investigator at the site, the parents provided consent, but during on-site monitoring (after discharge), no signed consent form was found, and investigators were unable to locate the family to renew the consent.
fRandomization was stratified by center and birth weight stratum (400-749 g and 750-999 g). Stratification by 36 centers and variable block size (2-10) accounted for the difference in the number of enrolled infants between treatment groups.
The last follow-up examination was scheduled in April 2017; however, the last child’s pediatrician follow-up examination occurred on January 15, 2018.
Infants were similar between treatment groups regarding perinatal risk factors and baseline characteristics (Table 2; eTable 5 in Supplement 2).
Table 2. Patient and Maternal Characteristics, Details of Delivery, and Prerandomization Transfusions.
| Characteristics | Liberal transfusion threshold (n = 492)a | Restrictive transfusion threshold (n = 521)a |
|---|---|---|
| Gestational age at birth, median (IQR), wk | 26.1 (24.9-27.6) | 26.4 (25.0-27.6) |
| Birth weight, median (IQR), g | 745 (636-900) | 750 (630-890) |
| Birth weight stratum, g, No. (%) | ||
| <750 | 250 (51) | 255 (49) |
| ≥750 | 242 (49) | 266 (51) |
| Head circumference at birth, median (IQR), cm | 23.0 (22.0-24.5) [n = 486] | 23.0 (22.0-24.5) [n = 514] |
| Sex, No. (%) | ||
| Female | 246 (50) | 263 (50) |
| Male | 246 (50) | 258 (50) |
| Singleton, No. (%) | 405 (82) | 407 (78) |
| Age at randomization, mean (SD), d | 2.5 (0.7) | 2.5 (0.7) |
| Maternal age at delivery, mean (SD), y | 30.9 (5.8) [n = 491] | 31.2 (5.9) [n = 520] |
| Any antenatal corticosteroids, No./total (%) | 432/484 (89) | 451/515 (88) |
| No. of completed courses of antenatal corticosteroids, median (IQR) | 1 (0-2) [n = 484] | 1 (0-2) [n = 515] |
| Cesarean delivery, No./total (%) | 441/492 (90) | 456/520 (88) |
| Delayed cord clamping, No./total (%) | 308/492 (63) | 319/519 (61) |
| Intubated at birth, No. (%) | 254 (52) | 264 (51) |
| RBCTs prior to randomization | ||
| Any RBCT before randomization, No. (%) | 121 (25) | 123 (24) |
| No. of RBCTs before randomization, No. (%) | ||
| 0 | 371 (75) | 398 (76) |
| 1 | 95 (19) | 94 (18) |
| 2 | 16 (3) | 26 (5) |
| 3 | 8 (2) | 2 (0.4) |
| 4 | 2 (0.4) | 1 (0.2) |
Abbreviations: IQR, interquartile range; RBCT, red blood cell transfusion.
Denominators are as specified in column heads unless otherwise indicated.
In 10 infants (4 in the liberal threshold group; 6 in the restrictive threshold group), consent was withdrawn before 36 weeks of postmenstrual age. Nineteen infants (6 in the liberal threshold group; 13 in the restrictive threshold group) were withdrawn from their assigned treatment group before discharge home: 12 (3 in the liberal threshold group; 9 in the restrictive threshold group) by the treating physician because of severe illness (of these, 8 infants died), 6 (3 in each group) after transfer to hospitals not following the assigned guidelines, and 1 (restrictive threshold group) after reaching 40 weeks of postmenstrual age (Figure 1).
Seventy-nine percent of infants (391/492) in the liberal threshold group and 60% (311/521) in the restrictive threshold group received at least 1 RBCT between randomization and 36 weeks of postmenstrual age (eTable 2 in Supplement 2). There was a large difference in the number of RBCTs administered (Figure 2) between treatment groups, and the cumulative volumes transfused through 36 weeks of postmenstrual age were higher in the liberal threshold group than in the restrictive threshold group (median, 40 mL [interquartile range, 16-73 mL] vs 19 mL [interquartile range, 0-46 mL]). Weekly mean hematocrit values were 3 percentage points higher in the liberal threshold group (Figure 2; eTable 6 in Supplement 2).
Figure 2. Treatment Effect on Hematocrit and Number of Red Blood Cell Transfusions (RBCTs).
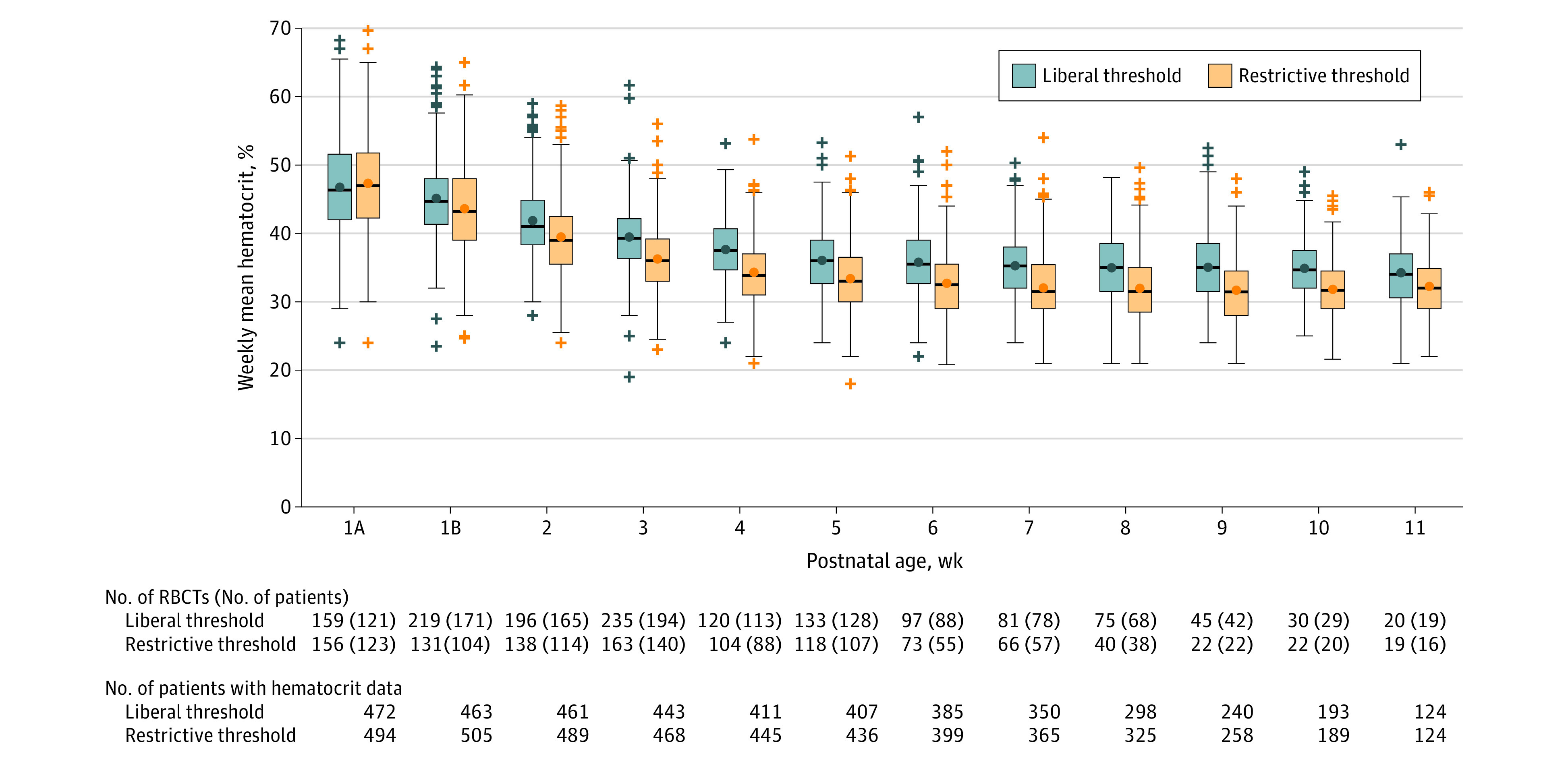
Weekly mean hematocrit values (limited to hematocrit values documented until 36 weeks of postmenstrual age and truncated when less than 20% of the population remained, ie, at 11 weeks of postnatal age). Week 1A refers to the days of the first week of postnatal age up to randomization and week 1B refers to the days of the first week of postnatal age after randomization. Hematocrit values were derived from clinically indicated complete blood cell counts (or, rarely, from centrifuged hematocrit capillaries), documented as observed. Hematocrit values of 36 patients at 4 centers were at least in part estimated from hemoglobin concentrations. For each week, a mean value of all documented hematocrit values was calculated, resulting in a weekly mean hematocrit for each infant who had ≥1 hematocrit measurement in that week. Boxes indicate interquartile ranges; bars inside the boxes, medians; circles inside boxes, means; whiskers, highest and lowest values within 1.5 times the interquartile range; and markers outside the boxes, outlying data. Weekly mean hematocrit values are significantly different between the treatment groups from week 1b through week 11. See eTable 6 in Supplement 2 for differences in means; see eFigure 3 in Supplement 2 for weekly mean hematocrit values in the per-protocol population.
Primary Outcome
The primary outcome of death or neurodevelopmental impairment at 24 months of corrected age was ascertained in 450 patients (91.5%) and 478 patients (91.7%) in the liberal and restrictive threshold groups, respectively. In the liberal and restrictive threshold groups, respectively, primary outcome data were missing in 5 and 8 infants due to withdrawn consent; 27 and 22 infants were lost to follow-up, and in 10 and 13, neurodevelopmental impairment was not assessable due to missing component data (Figure 1). The rates of death or neurodevelopmental impairment were 44.4% vs 42.9%, for a risk difference of 1.6% (95% CI, −4.8% to +7.9%) and an odds ratio of 1.05 (95% CI, 0.80-1.39; P = .72) adjusted for center and birth weight stratum (Table 3). Standardized residual plots are provided in eFigure 1 and results of the Hosmer-Lemeshow goodness-of-fit test and contingency coefficient c are provided in eTable 7 in Supplement 2.
Table 3. Primary and Secondary End Points.
| End points | Liberal transfusion threshold | Restrictive transfusion threshold | Absolute difference, % (95% CI)a | Odds ratio or adjusted difference in least-square means (95% CI)b | P valuec |
|---|---|---|---|---|---|
| Primary end point | |||||
| Death or neurodevelopmental impairment by 24 mo, No./total (%)d | 200/450 (44.4) | 205/478 (42.9) | 1.6 (−4.8 to 7.9) | 1.05 (0.80 to 1.39) | .72 |
| Secondary end points | |||||
| Death by 24 mo, No./total (%) | 38/460 (8.3) | 44/491 (9.0) | −0.7 (−4.3 to 2.9) | 0.91 (0.58 to 1.45)e | .70 |
| Cognitive deficit, No./total (%)f | 154/410 (37.6) | 148/430 (34.4) | 3.1 (−3.3 to 9.6) | 1.12 (0.83 to 1.51) | .47 |
| Cognitive deficit defined by Bayley 2 MDI score, No./total (%)f | |||||
| <85 | 143/378 (37.8) | 139/387 (35.9) | 1.9 (−4.9 to 8.8) | 1.09 (0.81 to 1.46)e | .58 |
| <70 | 71/378 (18.8) | 62/387 (16.0) | 2.8 (−2.6 to 8.1) | 1.21 (0.83 to 1.76)e | .31 |
| Bayley 2 MDI score, mean (SD)f | 92.6 (16.5) [n = 336] | 92.4 (17.5) [n = 360] | 0.2 (−2.4 to 2.7) | 0.4 (−2.1 to 2.9)g | .75 |
| Cerebral palsy, No./total (%) | 18/419 (4.3) | 25/443 (5.6) | −1.3 (−4.2 to 1.5) | 0.75 (0.40 to 1.40)e | .37 |
| Bayley 2 PDI score, mean (SD)f | 89.3 (15.1) [n = 315] | 89.2 (15.4) [n = 312] | 0.0 (−2.4 to 2.4) | 0.1 (−2.0 to 2.2)g | .92 |
| GMFCS score I-V, No./total (%)h | 34/416 (8.2) | 42/440 (9.5) | −1.4 (−5.2 to 2.4) | 0.84 (0.53 to 1.36)e | .48 |
| Severe visual impairment, No./total (%)i | 10/417 (2.4) | 12/443 (2.7) | −0.3 (−2.4 to 1.8) | 0.88 (0.61 to 2.07)e | .77 |
| Severe hearing impairment, No./total (%)j | 4/418 (1.0) | 6/443 (1.4) | −0.4 (−1.8 to 1.0) | 0.70 (0.20 to 2.51)e | .59 |
| Length of hospital stay, mean (SD), d | 93 (41) [n = 489] | 92 (38) [n = 510] | 0.7 (−4.2 to 5.6) | −0.0 (−4.7 to 4.7)g | 1.00 |
| Duration of support, postnatal age, mean (SD), dk | |||||
| At end of invasive ventilatory supportl | 23 (28) [n = 298] | 23 (26) [n = 321] | 0.1 (−4.2 to 4.3) | 0.0 (−4.1 to 4.1)g | 1.00 |
| At last positive pressure respiratory supportl | 53 (31) [n = 451] | 53 (29) [n = 475] | 0.5 (−3.3 to 4.6) | −0.1 (−3.4 to 3.1)g | .94 |
| At last supplemental oxygen | 52 (33) [n = 371] | 50 (33) [n = 378] | 2.7 (−2.1 to 7.4) | 1.6 (−2.5 to 5.8)g | .44 |
| At last caffeine administration | 69 (26) [n = 417] | 70 (26) [n = 425] | −1.0 (−4.6 to 2.5) | −2.0 (−5.1 to 1.1)g | .20 |
| At end of gavage feeding | 75 (25) [n = 422] | 77 (27) [n = 441] | −1.6 (−5.1 to 1.8) | −2.6 (−5.5 to 0.4)g | .09 |
Abbreviations: Bayley 2, Bayley Scales of Infant Development second edition; GMFCS, Gross Motor Function Classification System; MDI, Mental Developmental Index; PDI, Psychomotor Developmental Index.
Absolute differences were calculated post hoc for binary and continuous end points, without adjustment for center or birth weight stratum.
Odds ratios were calculated by logistic regression with the factors of treatment, center, and birth weight stratum (400-749 g or 750-999 g). Standardized residuals as well as the results of the Hosmer-Lemeshow goodness-of-fit test and contingency coefficient c are provided in eTable 7 in the Supplement. Reduced models (with a factor of treatment only) were fitted if iterations did not converge. Differences in least-square means were calculated for continuous variables by analysis of variance with the factors of treatment, center, and birth weight stratum (400-749 g or 750-999 g). Normal probability plots are provided in eTable 7.
P values were calculated by logistic regression for binary end points and by analysis of variance for continuous end points.
Neurodevelopmental impairment was defined as any of the following: cognitive deficit defined as a Bayley 2 MDI score <85 or similar indications of cognitive deficit, cerebral palsy, or severe visual or hearing impairment.
Logistic regression with a factor of treatment only.
Both the MDI and PDI scores are standardized to a mean of 100 (SD, 15) with a range from 50 to 150. For cognitive deficit as a component of the primary outcome, other cognitive assessments were taken into account if no Bayley test was available, as described in the Methods section of the text. Data for the rows with MDI scores <85 and <70 and PDI scores <85 are based on infants with attempted Bayley 2 testing only (including infants whose raw scores were so low that MDI/PDI was <50). Analyses of the MDI and PDI as continuous variables are based on complete Bayley 2 data only.
Adjusted difference in least-square means.
GMFCS scores of I, II, III, IV, and V indicate increasing degrees of gross motor function impairment, whereas 0 indicates that there is no deficit. GMFCS score was defined as a “further end point,” not as a secondary end point, in the study protocol. The presentation of the GMFCS data herein deviates from the statistical analysis plan, which foresaw presentation as median (interquartile range), due to the low rate of GMFCS scores >0.
Defined as best corrected visual acuity <6/60.
Defined as need for hearing aid or cochlear implant.
Analyses of the duration of various forms of support are limited to infants who received that therapeutic intervention (eg, 158 infants in the liberal threshold group and 155 infants in the restrictive threshold group never received invasive ventilatory support through an endotracheal tube, so duration of invasive ventilation is reported in only 298 and 321 infants) and discontinued the intervention before the day of discharge home.
Because nonparametric analyses would not have enabled adjustment for center and birth weight stratum, mean (SD) and results of analysis of variance are reported.
Secondary Outcomes
There were no statistically significant differences between treatment groups in rates of components of the primary outcome or incidence of cognitive deficit (defined as MDI score <70), the MDI score, the PDI score, length of hospital stay, or time intervals from birth to final discontinuation of invasive respiratory support, positive pressure respiratory support, respiratory stimulant therapy, and gavage feeding (Table 3).
A total of 38 (8.3%) of 460 infants followed up through 24 months died in the liberal threshold group vs 44 (9.0%) of 491 in the restrictive threshold group (risk difference, −0.7% [95% CI, −4.3% to 2.9%]; odds ratio, 0.91 [95% CI, 0.58-1.45]; P = .70). Postnatal age at death (eFigure 2 in Supplement 2) and causes of death (eTable 8 in Supplement 2) were similar in both groups.
Weight, head circumference, and length at 36 weeks of postmenstrual age and at follow-up were also not significantly different between groups, except for weight at 36 weeks of postmenstrual age, which was higher in the liberal threshold group (mean, 2113 g [SD, 356 g] vs 2068 g [SD, 361 g]; difference in least-square means, 44 g [95% CI, 3-85 g]; P = .04) (eTable 9 in Supplement 2).
The rates of common complications of prematurity such as necrotizing enterocolitis, bronchopulmonary dysplasia, and retinopathy of prematurity and other serious adverse events were not significantly different between treatment groups (Table 4).
Table 4. Complications of Prematurity and Other Serious Adverse Events Documented After Randomization.
| Events | No./total (%) | Absolute difference, % (95% CI) | |
|---|---|---|---|
| Liberal transfusion threshold (n = 492) | Restrictive transfusion threshold (n = 521) | ||
| Any intraventricular/periventricular hemorrhagea | 117/492 (23.8) | 113/521 (21.7) | 2.1 (−3.1 to 7.3) |
| Intraventricular/periventricular hemorrhage grade 3 or 4a | 40/492 (8.1) | 35/521 (6.7) | 1.4 (−1.8 to 4.6) |
| Cystic periventricular leukomalaciab | 23/492 (4.7) | 30/521 (5.8) | −1.1 (−3.8 to 1.7) |
| Bronchopulmonary dysplasiac | 130/458 (28.4) | 126/485 (26.0) | 2.4 (−3.3 to 8.1) |
| Necrotizing enterocolitisd | 26/492 (5.3) | 32/518 (6.2) | −0.9 (−3.8 to 2.0) |
| Surgical necrotizing enterocolitis | 20/492 (4.1) | 28/518 (5.4) | −1.3 (−4.0 to 1.3) |
| Focal intestinal perforation | 31/492 (6.3) | 33/518 (6.4) | −0.1 (−3.1 to 2.9) |
| Retinopathy of prematurity | |||
| Any | 257/472 (54.5) | 261/492 (53.1) | 1.4 (−4.9 to 7.7) |
| Maximum stage ≥3 | 75/472 (15.9) | 64/492 (13.0) | 2.9 (−1.6 to 7.3) |
| Receiving therapy | 41/472 (8.7) | 38/492 (7.7) | 1.0 (−2.5 to 4.4) |
| Patent ductus arteriosus | |||
| Any therapy | 204/492 (41.5) | 196/518 (37.8) | 3.6 (−2.4 to 9.7) |
| Ligation/any therapy | 51/204 (25.0) | 52/196 (26.5) | −1.5 (−10.1 to 7.0) |
| Culture-proven sepsis excluding coagulase-negative staphylococcie | |||
| Any | 59/492 (12.0) | 61/518 (11.8) | 0.2 (−3.8 to 4.2) |
| No. of episodes | |||
| 0 | 433 (88.0) | 457 (88.2) | |
| 1 | 50 (10.1) | 51 (9.8) | |
| 2 | 6 (1.2) | 8 (1.5) | |
| 3 | 3 (0.6) | 2 (0.4) | |
| Culture-proven sepsis with coagulase-negative staphylococcie | |||
| Any | 54/492 (11.0) | 62/518 (12.0) | −1.0 (−4.9 to 2.9) |
| No. of episodes | |||
| 0 | 438 (89.0) | 456 (88.0) | |
| 1 | 48 (9.8) | 57 (11.0) | |
| 2 | 5 (1.0) | 5 (1.0) | |
| >2 | 1 (0.2) | 0 | |
| Clinical sepsise | |||
| Any | 142/492 (28.9) | 153/518 (29.5) | −0.7 (−6.3 to 4.9) |
| No. of clinical sepsis episodes | |||
| 0 | 350 (71.1) | 365 (70.5) | |
| 1 | 98 (19.9) | 112 (21.6) | |
| 2 | 32 (6.5) | 27 (5.2) | |
| 3 | 9 (1.8) | 9 (1.7) | |
| >3 | 3 (0.6) | 5 (1.0) | |
| Pneumoniae | |||
| Any | 30/492 (6.1) | 32/518 (6.2) | −0.1 (−3.0 to 2.9) |
| No. of pneumonia episodes | |||
| 0 | 462 (93.9) | 486 (93.8) | |
| 1 | 26 (5.3) | 23 (4.4) | |
| 2 | 3 (0.6) | 4 (0.8) | |
| 3 | 1 (0.2) | 2 (0.4) | |
| >3 | 0 | 3 (0.6) | |
| No. of additional serious adverse eventsf | 15 | 29 | |
| No. of potentially related serious adverse eventsg | 3 | 1 | |
Data on intraventricular/periventricular hemorrhage include findings already evolving before randomization. Findings of prerandomization head ultrasound are shown in eTable 5 in the Supplement.
Data on cystic periventricular leukomalacia include findings already evolving before randomization. Rates of cystic periventricular leukomalacia at baseline were 1 (0.2%) and 5 (1%) in the liberal and restrictive threshold groups, respectively.
Bronchopulmonary dysplasia was determined based on need for positive pressure respiratory support or supplemental oxygen at 36 weeks of postmenstrual age, including a room air test if indicated. The rates of death before 36 weeks of postmenstrual age precluding the diagnosis by definition were 29 (6%) and 30 (6%) in the liberal and restrictive threshold groups, respectively.
Necrotizing enterocolitis was diagnosed if criteria for modified Bell stage ≥IIa were present.
Blood culture–proven sepsis, clinical sepsis, and pneumonia were recorded according to the German Nosocomial Infection Surveillance System for Preterm Infants in Neonatology Departments and ICU Infection Surveillance (Neo-KISS) criteria (https://www.nrz-hygiene.de/en/surveillance/hospital-infection-surveillance-system/neo-kiss/), with data given for the number of separate episodes of illness meeting the diagnostic criteria.
Additional serious adverse events limited to those reported in >2 infants included, in the liberal vs restrictive threshold groups, respectively: volvulus (n = 3 vs n = 4), cytomegalovirus infection (n = 1 vs n = 4), meningitis (n = 2 vs n = 4), and renal failure (n = 1 vs n = 2).
Four serious adverse events (1 necrotizing enterocolitis, 1 cytomegalovirus infection, and 2 sepsis) were considered by local investigators to be possibly or probably related to the assigned threshold or a preceding red blood cell transfusion (neither the cytomegalovirus infection nor the sepsis were microbiologically proven to be related to the red blood cell transfusion).
Rates of cognitive deficit according to mode of classification, analyzed post hoc, were not significantly different between groups (eTable 10 in Supplement 2).
Sensitivity, Per-Protocol, and Subgroup Analyses
Sensitivity analysis for the primary outcome in the population of all randomized patients showed rates of 242/492 (49.2%) vs 248/521 (47.6%) in the liberal vs restrictive threshold groups, with a risk difference of 1.6% (95% CI, −4.6% to 7.7%), consistent with the primary analysis (eTable 11 in Supplement 2).
Twenty-two infants were erroneously included (4 of whom met exclusion criteria). Red blood cell transfusion was missed (ie, no RBCT was done within 48 hours of a hematocrit below the assigned threshold) in 65 infants in the liberal threshold group and 5 infants in the restrictive threshold group. One hundred ninety-seven non–protocol-justified RBCTs occurred in 47 infants in the liberal threshold group (34 in the lower and 13 in the higher birth weight strata) and in 97 infants in the restrictive threshold group (70 in the lower and 27 in the higher birth weight strata). In 95 of 197 non–protocol-justified RBCTs, pre-RBCT hematocrit was no more than 2 percentage points higher than the assigned threshold. After exclusion of these 232 infants (211 infants with complete primary outcome data), results of the per-protocol analysis with respect to the primary outcome and all secondary outcomes remained unchanged (eTable 12 in Supplement 2). eFigure 3 in Supplement 2 shows the hematocrit values in the per-protocol population.
An additional 265 RBCTs not meeting trigger thresholds were administered in the context of surgery (37 and 89), lactic acidosis (18 and 40), bleeding (6 and 18), and other unforeseen emergencies (32 and 88) in 34 and 66 infants in the liberal and restrictive threshold groups, respectively (eTable 2 in Supplement 2).
In predefined subgroup analyses, there were no statistically significant differences in treatment effects between birth weight strata (400-749 g vs 750-999 g), sex, and high or low institutional pulse oximetry oxygen saturation target range subgroups with regard to the primary end point, the incidence of cerebral palsy, or the MDI score (eTables 13, 14, and 15 in Supplement 2).
Post hoc comparison of gestational age at birth between infants recruited in this trial and ELBW infants in the German Neonatal Network database born during the same period did not indicate any selection bias (eTable 3 in Supplement 2).
Discussion
This study compared the effects of liberal vs restrictive transfusion strategies on death or disability at 24 months of corrected age in ELBW infants and found that liberal transfusion strategies did not reduce the likelihood of death or disability or any component thereof.
Extremely low-birth-weight infants are particularly prone to intermittent hypoxemia from week 2 to weeks 6 through 8 after birth,18 and such hypoxemic episodes, particularly if prolonged, are associated with adverse long-term outcomes.19 If this association reflects a causal relationship, the degree of anemia and the thresholds indicating RBCT may be an important link. It was therefore of particular concern that Whyte et al15 reported the 18- to 21-month follow-up data of the PINT trial indicating rates of cognitive deficit (defined as a Bayley-2 MDI score <70) of 24% vs 18% in the restrictive threshold group vs the liberal threshold group, a difference that was not statistically significant but would be of clinical importance if real. Post hoc analyses indicated that the mean MDI score was 3.5 points lower, and the proportion of infants with MDI scores lower than 85 was 11 percentage points higher, in the restrictive threshold group.15
Conversely, RBCTs have also been associated with adverse outcomes such as death,4 retinopathy of prematurity,11,12 bronchopulmonary dysplasia,3,10,20 intraventricular hemorrhage,6,7 and necrotizing enterocolitis,6,8,9,21 but such associations may not reflect causality.22,23
To resolve this uncertainty, this trial was designed to compare the effects of liberal vs restrictive transfusion strategies. The trigger thresholds applied in this study reflected contemporary neonatal care24 and were in agreement with available evidence.25 The restrictive thresholds mimicked those used in the restrictive threshold group of the PINT study,26 and it was consensus at that time that transfusion thresholds for ELBW infants should not be more restrictive.27 With increasing postnatal age enabling postnatal circulatory adaptation, lower levels of hematocrit seemed tolerable, and higher levels were maintained in critically ill infants, taking into account the need for respiratory or circulatory support as well as the frequency and severity of intermittent hypoxemic episodes. To reflect clinical reality, RBCTs were allowed independent of the assigned transfusion thresholds during surgery or other emergencies.
This study showed that a liberal transfusion strategy did not reduce the likelihood of death or disability compared with a restrictive strategy. The apparent discrepancy with the post hoc analyses of the PINT trial15 may be explained by the fact that the PINT investigators were more adherent to the assigned transfusion thresholds and that the resulting mean hematocrit and/or hemoglobin values were about 3 percentage points higher per 10 g/L in both groups in the present study compared with the PINT trial. Differences in neonatal care (due to different health care systems and/or advances in treatments during the 10 years between the 2 trials) may also have contributed. The upcoming results of the ongoing Transfusion of Prematures (TOP) trial (NCT01702805) of the National Institute of Child Health and Human Development Neonatal Research Network may shed further light on this discussion and enable an individual patient data meta-analysis.
In keeping with the PINT trial,26 hospital outcomes were not significantly different in both groups, suggesting that associations of RBCT with complications of prematurity do not reflect causal relationships (at least within the RBCT strategies applied herein).
Limitations
This study has several limitations. First, 8% of randomized patients were not able to be included in analysis of the primary outcome, mainly due to loss to follow-up. Second, a substantial proportion of infants received at least 1 RBCT that was not justified by the study protocol (144/1013 [14%]) or did not receive an RBCT within 48 hours of a (potentially single) hematocrit value below the assigned threshold (70/1013 [7%]) during the (on average) 10-week treatment period, potentially blunting any treatment effect. However, analysis of the per-protocol population who were treated according to protocol at all times confirmed the primary analysis. Because non–protocol-justified RBCTs were predominantly administered to infants with birth weights below 750 g in the restrictive threshold group, the proportions of low and high birth weight strata were skewed in the per-protocol population: 190/370 (51%) in the low birth weight stratum and 180/370 (49%) in the high birth weight stratum in the liberal threshold group vs 177/411 (43%) and 234/411 (57%) in the restrictive threshold group. Third, the lower rates of death and bronchopulmonary dysplasia in this trial compared with those of a recent European multicenter study on inhaled budesonide in extremely low-gestational-age infants (NEUROSIS),28 despite a similar mean gestational age at birth, might indicate that the sickest extremely preterm infants may not have been enrolled because of a more delayed recruitment (mean 2.5 days in this trial vs median 6 hours in NEUROSIS), patient selection by the local investigators, or higher anxiety among parents with sick infants related to RBCT compared with inhaled budesonide. Fourth, the separation in hematocrit values (and hence in oxygen-carrying capacity) achieved may be considered too small (and the level of resulting mean hematocrit values too high) to cause a difference in outcome; however, more liberal or more restrictive guidelines would not have been acceptable to the (German) neonatal community. Fifth, recruitment for the trial extended over a period of 40 months, and changes in neonatal practice over time may have occurred during that period and introduced bias. Sixth, mean age at randomization was 2.5 days; hence, no conclusion can be drawn on what level of hematocrit is required during the first 2 days after birth. Seventh, generalizability to other populations might be limited by the predominantly white German study population. Eighth, the nonmasking of parents and neonatal caregivers by nature of the intervention may have introduced bias in the nonobjective short-term outcomes.
Conclusions
Among infants with birth weights of less than 1000 g, a strategy of liberal blood transfusions compared with restrictive transfusions did not reduce the likelihood of death or disability at 24 months of corrected age.
Trial Protocol
eTable 1. Red Blood Cell Transfusion Hemoglobin Trigger Thresholds (4 Centers, 36 Patients)
eTable 2. Number of Red Blood Cell Transfusions and Volumes Transfused
eTable 3. Study Population Versus Patients Enrolled in German Neonatal Network 2011-2014
eTable 4. Patient Recruitment by Study Site
eTable 5. Additional Patient Characteristics before Randomization
eTable 6. Weekly Mean Hematocrit Values [in %] by Treatment Group
eTable 7. Model Diagnostics for Primary and Secondary Outcome Analyses in the Main Publication
eTable 8. Timing and Causes of Death
eTable 9. Growth Data
eTable 10. Post Hoc Analysis of Cognitive Deficit by Mode of Classification in Survivors
eTable 11. Sensitivity Analysis of the Primary Outcome
eTable 12. Primary and Secondary Endpoints in the Per Protocol Population
eTable 13. Pre-Defined Subgroup Analysis 1: Rate of Primary Outcome and Key Secondary Outcomes by Birthweight Stratum and Transfusion Trigger Thresholds
eTable 14. Pre-Defined Subgroup Analysis 2: Rate of Primary Outcome and Key Secondary Outcomes by Gender and Transfusion Trigger Thresholds
eTable 15. Pre-Defined Subgroup Analysis 3: Rate of Primary Outcome and Key Secondary Outcomes by Institutional Spo2-Target Range and Transfusion Trigger Thresholds
eFigure 1. Standardized Residual Plots (Analysis of the Primary Outcome)
eFigure 2. Overall Survival
eFigure 3. Treatment Effect on Weekly Mean Hematocrit in the Per-Protocol Population
eAppendix. Additional Information on Sample Size Calculation
eReferences
Data Sharing Statement
References
- 1.Vos T, Abajobir AA, Abate KH, et al. ; GBD 2016 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-1259. doi: 10.1016/S0140-6736(17)32154-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Widness JA. Pathophysiology of anemia during the neonatal period, including anemia of prematurity. Neoreviews. 2008;9(11):e520. doi: 10.1542/neo.9-11-e520 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Valieva OA, Strandjord TP, Mayock DE, Juul SE. Effects of transfusions in extremely low birth weight infants: a retrospective study. J Pediatr. 2009;155(3):331-337. doi: 10.1016/j.jpeds.2009.02.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.dos Santos AM, Guinsburg R, de Almeida MF, et al. ; Brazilian Network on Neonatal Research . Red blood cell transfusions are independently associated with intra-hospital mortality in very low birth weight preterm infants. J Pediatr. 2011;159(3):371-376. doi: 10.1016/j.jpeds.2011.02.040 [DOI] [PubMed] [Google Scholar]
- 5.Stainsby D, Jones H, Wells AW, Gibson B, Cohen H; SHOT Steering Group . Adverse outcomes of blood transfusion in children: analysis of UK reports to the serious hazards of transfusion scheme 1996-2005. Br J Haematol. 2008;141(1):73-79. doi: 10.1111/j.1365-2141.2008.07022.x [DOI] [PubMed] [Google Scholar]
- 6.Christensen RD, Baer VL, Del Vecchio A, Henry E. Unique risks of red blood cell transfusions in very-low-birth-weight neonates: associations between early transfusion and intraventricular hemorrhage and between late transfusion and necrotizing enterocolitis. J Matern Fetal Neonatal Med. 2013;26(suppl 2):60-63. doi: 10.3109/14767058.2013.830495 [DOI] [PubMed] [Google Scholar]
- 7.Baer VL, Lambert DK, Henry E, Snow GL, Butler A, Christensen RD. Among very-low-birth-weight neonates is red blood cell transfusion an independent risk factor for subsequently developing a severe intraventricular hemorrhage? Transfusion. 2011;51(6):1170-1178. doi: 10.1111/j.1537-2995.2010.02980.x [DOI] [PubMed] [Google Scholar]
- 8.Paul DA, Mackley A, Novitsky A, Zhao Y, Brooks A, Locke RG. Increased odds of necrotizing enterocolitis after transfusion of red blood cells in premature infants. Pediatrics. 2011;127(4):635-641. doi: 10.1542/peds.2010-3178 [DOI] [PubMed] [Google Scholar]
- 9.Mohamed A, Shah PS. Transfusion associated necrotizing enterocolitis: a meta-analysis of observational data. Pediatrics. 2012;129(3):529-540. doi: 10.1542/peds.2011-2872 [DOI] [PubMed] [Google Scholar]
- 10.Ghirardello S, Dusi E, Cortinovis I, et al. Effects of red blood cell transfusions on the risk of developing complications or death: an observational study of a cohort of very low birth weight infants. Am J Perinatol. 2017;34(1):88-95. [DOI] [PubMed] [Google Scholar]
- 11.Slidsborg C, Jensen A, Forman JL, et al. Neonatal risk factors for treatment-demanding retinopathy of prematurity: a Danish national study. Ophthalmology. 2016;123(4):796-803. doi: 10.1016/j.ophtha.2015.12.019 [DOI] [PubMed] [Google Scholar]
- 12.Inder TE, Clemett RS, Austin NC, Graham P, Darlow BA. High iron status in very low birth weight infants is associated with an increased risk of retinopathy of prematurity. J Pediatr. 1997;131(4):541-544. doi: 10.1016/S0022-3476(97)70058-1 [DOI] [PubMed] [Google Scholar]
- 13.Lacroix J, Hébert PC, Hutchison JS, et al. ; TRIPICU Investigators; Canadian Critical Care Trials Group; Pediatric Acute Lung Injury and Sepsis Investigators Network . Transfusion strategies for patients in pediatric intensive care units. N Engl J Med. 2007;356(16):1609-1619. doi: 10.1056/NEJMoa066240 [DOI] [PubMed] [Google Scholar]
- 14.Hébert PC, Wells G, Blajchman MA, et al. ; Transfusion Requirements in Critical Care Investigators; Canadian Critical Care Trials Group . A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care.. N Engl J Med. 1999;340(6):409-417. doi: 10.1056/NEJM199902113400601 [DOI] [PubMed] [Google Scholar]
- 15.Whyte RK, Kirpalani H, Asztalos EV, et al. ; PINTOS Study Group . Neurodevelopmental outcome of extremely low birth weight infants randomly assigned to restrictive or liberal hemoglobin thresholds for blood transfusion. Pediatrics. 2009;123(1):207-213. doi: 10.1542/peds.2008-0338 [DOI] [PubMed] [Google Scholar]
- 16.Cans C; Surveillance of Cerebral Palsy in Europe . Surveillance of Cerebral Palsy in Europe: a collaboration of cerebral palsy surveys and registers. Dev Med Child Neurol. 2000;42(12):816-824. doi: 10.1111/j.1469-8749.2000.tb00695.x [DOI] [PubMed] [Google Scholar]
- 17.Christine C, Dolk H, Platt MJ, Colver A, Prasauskiene A, Krägeloh-Mann I; SCPE Collaborative Group . Recommendations from the SCPE collaborative group for defining and classifying cerebral palsy. Dev Med Child Neurol Suppl. 2007;109:35-38. [DOI] [PubMed] [Google Scholar]
- 18.Di Fiore JM, Bloom JN, Orge F, et al. A higher incidence of intermittent hypoxemic episodes is associated with severe retinopathy of prematurity. J Pediatr. 2010;157(1):69-73. doi: 10.1016/j.jpeds.2010.01.046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Poets CF, Roberts RS, Schmidt B, et al. ; Canadian Oxygen Trial Investigators . Association between intermittent hypoxemia or bradycardia and late death or disability in extremely preterm infants. JAMA. 2015;314(6):595-603. doi: 10.1001/jama.2015.8841 [DOI] [PubMed] [Google Scholar]
- 20.Silvers KM, Gibson AT, Russell JM, Powers HJ. Antioxidant activity, packed cell transfusions, and outcome in premature infants. Arch Dis Child Fetal Neonatal Ed. 1998;78(3):F214-F219. doi: 10.1136/fn.78.3.F214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Blau J, Calo JM, Dozor D, Sutton M, Alpan G, La Gamma EF. Transfusion-related acute gut injury: necrotizing enterocolitis in very low birth weight neonates after packed red blood cell transfusion. J Pediatr. 2011;158(3):403-409. doi: 10.1016/j.jpeds.2010.09.015 [DOI] [PubMed] [Google Scholar]
- 22.Kirpalani H, Whyte R. Truths, associations, and hypotheses. J Pediatr. 2011;159(3):359-361. doi: 10.1016/j.jpeds.2011.05.002 [DOI] [PubMed] [Google Scholar]
- 23.Hay S, Zupancic JA, Flannery DD, Kirpalani H, Dukhovny D. Should we believe in transfusion-associated enterocolitis? applying a GRADE to the literature. Semin Perinatol. 2017;41(1):80-91. doi: 10.1053/j.semperi.2016.09.021 [DOI] [PubMed] [Google Scholar]
- 24.Guillén U, Cummings JJ, Bell EF, et al. International survey of transfusion practices for extremely premature infants. Semin Perinatol. 2012;36(4):244-247. doi: 10.1053/j.semperi.2012.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Whyte R, Kirpalani H. Low versus high haemoglobin concentration threshold for blood transfusion for preventing morbidity and mortality in very low birth weight infants. Cochrane Database Syst Rev. 2011;(11):CD000512. doi: 10.1002/14651858.CD000512.pub2 [DOI] [PubMed] [Google Scholar]
- 26.Kirpalani H, Whyte RK, Andersen C, et al. The Premature Infants in Need of Transfusion (PINT) study: a randomized, controlled trial of a restrictive (low) versus liberal (high) transfusion threshold for extremely low birth weight infants. J Pediatr. 2006;149(3):301-307. doi: 10.1016/j.jpeds.2006.05.011 [DOI] [PubMed] [Google Scholar]
- 27.Bell EF. When to transfuse preterm babies. Arch Dis Child Fetal Neonatal Ed. 2008;93(6):F469-F473. doi: 10.1136/adc.2007.128819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bassler D, Plavka R, Shinwell ES, et al. ; NEUROSIS Trial Group . Early inhaled budesonide for the prevention of bronchopulmonary dysplasia. N Engl J Med. 2015;373(16):1497-1506. doi: 10.1056/NEJMoa1501917 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eTable 1. Red Blood Cell Transfusion Hemoglobin Trigger Thresholds (4 Centers, 36 Patients)
eTable 2. Number of Red Blood Cell Transfusions and Volumes Transfused
eTable 3. Study Population Versus Patients Enrolled in German Neonatal Network 2011-2014
eTable 4. Patient Recruitment by Study Site
eTable 5. Additional Patient Characteristics before Randomization
eTable 6. Weekly Mean Hematocrit Values [in %] by Treatment Group
eTable 7. Model Diagnostics for Primary and Secondary Outcome Analyses in the Main Publication
eTable 8. Timing and Causes of Death
eTable 9. Growth Data
eTable 10. Post Hoc Analysis of Cognitive Deficit by Mode of Classification in Survivors
eTable 11. Sensitivity Analysis of the Primary Outcome
eTable 12. Primary and Secondary Endpoints in the Per Protocol Population
eTable 13. Pre-Defined Subgroup Analysis 1: Rate of Primary Outcome and Key Secondary Outcomes by Birthweight Stratum and Transfusion Trigger Thresholds
eTable 14. Pre-Defined Subgroup Analysis 2: Rate of Primary Outcome and Key Secondary Outcomes by Gender and Transfusion Trigger Thresholds
eTable 15. Pre-Defined Subgroup Analysis 3: Rate of Primary Outcome and Key Secondary Outcomes by Institutional Spo2-Target Range and Transfusion Trigger Thresholds
eFigure 1. Standardized Residual Plots (Analysis of the Primary Outcome)
eFigure 2. Overall Survival
eFigure 3. Treatment Effect on Weekly Mean Hematocrit in the Per-Protocol Population
eAppendix. Additional Information on Sample Size Calculation
eReferences
Data Sharing Statement