

Abstract
Background
Personality traits are related with risk of hazardous alcohol use and alcohol dependence. The Substance Use Risk Profile Scale (SURPS) measures personality traits associated with addictive substance abuse. We examined psychometric properties of the SURPS in Lithuanian population.
Materials and methods
Two hundred forty-seven participants (mean age 37.22 ± 0.78 years), were recruited from the local community and from an inpatient addiction treatment centre. Internal consistency, stability, factor structure, content validity, and external validity of the SURPS were examined. Hazardous alcohol use was evaluated by Alcohol Use Disorder Identification Test (AUDIT). Alcohol dependence diagnosis was established by International Classification of Diseases - 10 (ICD - 10). We also performed gender analyses for associations of personality traits with alcohol dependence and hazardous use of alcohol.
Results
The SURPS scale demonstrated appropriate internal validity, good temporal stability, and adequate criterion validity and construct validity. The SURPS scores of hopelessness, anxiety sensitivity and impulsivity were higher in the alcohol dependence group than in the control group for both males and females. Impulsivity and sensation seeking were associated with hazardous alcohol use and these associations were more prevalent in females.
Conclusions
Lithuanian translation of the SURPS scale was appropriate. The SURPS demonstrated good sensitivity for discriminating on alcohol dependence and was more sensitive for discriminating on hazardous alcohol use for females.
Keywords: Substance Use Risk Profile Scale, Alcohol dependence, Hazardous alcohol use, Scale adaptation, Personality
Introduction
Substance use disorders manifest as compulsive seeking and consumption of addictive substances despite harmful consequences [1]. The Diagnostic and Statistical Manual of Mental Disorders – 5 (DSM-5) describes substance use disorder as hazardous use of addictive substances causing social and interpersonal problems and neglect of major social roles [1]. Substance use induces tolerance, loss of consumption control, unpleasant withdrawal and reduced physical and mental health [1]. It is established that several personality traits are related with hazardous addictive substance use and subsequent dependence development [2, 3].
High rates of alcohol consumption is an important public health problem in Lithuania as the country has one of the highest alcohol consumption rates in Europe [4]. Better understanding of diverse pathogenesis of addiction disorders and predisposing factors would be beneficial in the development of more advanced prevention and treatment methods of addiction disorders [5]. Several questionnaires for evaluating personality traits and divergent psychological phenotypes associated with addiction risk were created, for example the Minnesota Multiphasic Personality Inventory [6], Tridimensional Personality Questionnaire [7] and Addiction Prone Personality Scale [8]. However, there is a shortage of specific substance abuse related psychometric instruments validated in Lithuanian population.
The Substance Use Risk Profile Scale (SURPS) was developed to reveal main reinforcement mechanisms of addictive substances use [9]. Addiction is multi-ethiological cluster of syndromes, therefore divergent phenotypes are expected. Different personality traits that predispose to vulnearability may also affect motivational cues of addictive substance use, choice of addictive substance, and risk for relapse [5, 10–12]. Better understanding in diverse pathogenesis of addiction disorders and predisposing factors would be beneficial in the development of more advanced prevention and treatment methods of addiction disorders [5].
Generally, two main theoretical motivation dimensions are distinguished: a positive reinforcement, that could be defined as higher reward dependence that manifests in approach behaviour; and a negative reinforcement, which reveals as seeking escape and avoidance of aversive stimulus [11, 13]. Addictive substances per se have rewarding properties [14], thus higher reward dependence may result in increased vulnerability to addictive disorders. Poor behavioural inhibition and self-regulation capacities are classical findings in studies of addiction prone personality [2, 3]. Moreover, the presence of attention deficit – hyperactivity disorder (ADHD) has been demonstrated to increase vulnearability to addiction development [15, 16]. These findings are anticipated, as addiction disorders manifest in loss of control upon use and compulsive consumption pattern. Impulsiveness is predisposed by neurobiological alterations and enhanced by the abuse of addictive substances [17]. In addition, sensation seeking can lead to experimentation with addictive substances that consequantially opens gates for addiction [18].
Another pathway to addiction might be related to negative affect, and hopelessness, depression and anxiety may also escalate the use of addictive substances [19, 20] especially when trying to cope with negative emotional states. Comorbidity of substance abuse and mental disorders with predominant negative affect is well known [21, 22] and chronic use of addictive substances can increase the susceptibility for negative affect by activating the hypothalamic-pituitary-adrenal axis [23].
The SURPS covers these two theoretical motivational dimensions of addiction by evaluating personality traits associated with the substance abuse and addiction risk, in particular: anxiety sensitivity, hopelessness, impulsivity and sensation seeking. Respondents scoring high on anxiety sensitivity and hopelessness subscales of the SURPS are more likely to use addictive substances in order to eliminate negative emotions, while respondents receiving high impulsivity and sensation seeking scores tend to use addictive substances in order to enhance positive emotions [9]. Thus, the SURPS questionnaire is useful for studying mechanisms of addictive substance consumption. Moreover, the scale includes 23 questions, is self-administered, brief and easy to apply which is beneficial in research studies.
The scale was validated in adolescents and young adults populations and has shown good reliability and also a predictive value in longitudinal studies [24]. The scale has demonstrated high intercultural validity and reliability, and is adapted for different languages, including French [24–26], English [9, 24, 26], Irish [24], German [24], Dutch [27], Bulgarian [28], Spainish [29, 30], Turkish [31], and others. However, only few studies included patients with clinical diagnosis of addiction [28, 32, 33].
The aim of our study was to validate the SURPS questionnaire in the Lithuanian population and to explore the psychometric properties of the scale. We investigated personality traits associated with hazardous alcohol use and dependence and evaluated the properties of the scale in middle-aged adults. Different patterns in hazardous alcohol use in males and females [34] encouraged us to examine divergent traits associated with addiction and hazardous use of alcohol between genders.
Methods
Participants
The study sample included 247 persons: 178 healthy volunteers, recruited from the local community by convenience and snowball sampling methods, and 69 patients diagnosed with alcohol dependence who were recruited from the Republican Centre for Addictive Disorders.
Study inclusion criteria were willingness to participate, age from 20 to 65 years, ability to provide written informed consent and comprehend Lithuanian. The study exclusion criteria were pregnancy and severe cognitive impairment that would interfere with ability to understand the study aims and procedures. The patients in treatment were included if they had alcohol use disorder according to the International Classification of Diseases - 10 (ICD-10) diagnostic criteria (F10.2, F10.3). Diagnosis of alcohol use disorder was established with respect to diagnostic criteria defined in ICD-10 by a psychiatrist who specialises in addiction disorders. Patients with polysubstance abuse (N = 8) were included in the study.
Procedure
The study protocol and consent procedures were approved by the Regional Bioethics Committee for Biomedical Research (Nr. BE-2-25). All participants signed written informed consent with ability to discontinue participation at any time. Participants were approached twice during the study. During the first visit respondents were asked to provide demographic data and to complete a battery of study questionnaires. Respondents were also asked to participate in a re-test survey of the SURPS scale and provide their contact details. Twenty-six participants were re-evaluated at 1 month after inclusion in the study. At both time points questionnaires were administered by paper-pencil method.
Instruments
Substance Use Risk Profile Scale
The SURPS scale contains 23 items measuring four personality traits related to substance abuse: hopelessness (7 items), anxiety sensitivity (5 items), impulsivity (5 items) and sensation seeking (6 items) [9]. It is a self-report questionnaire with possible answers to all questions ranging from 1 (strongly disagree) to 4 (strongly agree). All questions are scored by adding scores together with the exception of the hopelessness subscale which items are scored reversed. Higher score on each subscale indicates greater expression of the personality traits.
Barratt impulsiveness Scale – 11
The Barratt Impulsiveness Scale – 11 (BIS − 11) is a 30 – item self – report questionnaire designed to measure impulsivity with its three main factors: lack of attention, motor impulsivity and non-planning [35]. Participants respond on a 4 – point Likert-type scale with possible scores ranging from 1 (Rarely/Never) to 4 (Almost always/Always). Higher score indicates a greater level of impulsivity [35]. According to previous studies, internal consistency of this scale is acceptable (Cronbach alpha = 0.79) [36]. In our study the internal consistency of BIS-11 scale by Cronbach’s coefficient alpha was 0.82. The permission to use this scale in current research was obtained from scale copyright holder. The BIS-11 was adapted for use in Lithuania using a standard double-translation method by the study researchers [37]. The BIS-11 scale was used to evaluate validity of the SURPS subscale of impulsivity.
Ten item personality measure
The Ten Item Personality Measure (TIPI) consists of 10 items that measure the Big-Five personality domains: extroversion, agreeableness, conscientiousness, emotional stability and openness to experiences. Two items are used to evaluate each trait. Respondents are asked to specify how strongly he/she agrees with the given statement. Each item is rated on a 7 – point scale ranging from 1 (disagree strongly) to 7 (agree strongly). Lithuanian version of the TIPI has previously demonstrated good construct validity [38, 39].
The conscientiousness factor was chosen to evaluate validity of the SURPS subscale of impulsivity, emotional stability – the subscales of hopelessness and anxiety sensitivity, openness to experience factor - the subscale of sensation seeking, as these traits considerably overlap [40].
Patient Health questionnaire - 4
The Patient Health Questionnaire - 4 (PHQ-4) [41] is a 4 item inventory designed for brief assessment of depressive and anxiety symptoms. The first two items of the PHQ – 4 measures anxiety symptoms and the last two items measure the depressive symptoms. Responses are scored from 0 to 3 (0 = Not at all; 1 = Several days; 2 = More than half the days; 3 = Nearly every day).. Internal consistency by the Cronbach’s coefficient alpha was more than 0.8 in line to previous studies [41]. Internal reliability of the PHQ-4 in our study was 0.90. The PHQ-4 and its subscales are adapted and used in Lithuania [42]. In this study the PHQ-4 was used to evaluate convergent validity of the SURPS hopelessness and anxiety sensitivity subscales.
Alcohol Use disorder identification test
Hazardous alcohol consumption was evaluated using the Alcohol Use Disorder Identification Test (AUDIT) [43]. This 10-item scale measures three conceptual domains: frequency and amount of alcohol intake (items 1–3), dependence (items 4–6) and adverse consequences (items 7–10). Scale scores range from 0 to 40 points. Cut-off point of the scale is 8, which indicates a potential problem of alcohol use and risk of alcohol use disorder [43]. The AUDIT was developed by the World Health Organization (WHO) and is a freely accessible, valid, and reliable instrument which demonstrates high sensitivity and specificity for hazardous alcohol use [44]. The AUDIT was used to evaluate the external validity of the SURPS in our study.
Translation and adaptation procedure of the SURPS
Translation and adaptation procedure of the SURPS scale was implemented according to the second edition of the International Test Commission for translating and adapting tests [37] after obtaining a written permission from the copyright holder.
Translation of the SURPS to Lithuanian language was done by a native Lithuanian speaker medical doctor specializing in substance use disorders. A pilot study in 20 respondents was performed to assess the appropriateness and clarity of the translation. Minor corrections in question wording were made after the review of this pilot study results in research group discussions. Two independent translators made back-translations to the English language to determine any discrepancies. Translators were fluent in Lithuanian and English and were blinded to the original scale. After subsequent review of the translations and when consensus on translation accuracy was reached, Lithuanian translation of the SURPS was submitted to the author of the SURPS scale.
Statistical analysis
Statistical analysis was performed using the SPSS statistical package (IBM SPSS Statistics 20, Chicago, IL) and confirmatory factor analysis was performed using the AMOS statistical package. Nonparametric criteria were applied where appropriate because of not normal distribution of the SURPS subscale scores.
Internal consistency of the total SURPS scale and individual subscales was estimated by the Cronbach’s coefficient alpha, with value of 0.7 considered as acceptable [45]. Spearman’s correlation coefficients of the SURPS subscales with corresponding scales were examined to determine content validity.
Test-retest reliability of the SURPS was evaluated by the Spearman correlations for individual subscales and by mixed model intra-class correlation coefficient (ICC) for absolute agreement. ICC values below 0.5 were considered as poor, 0.5–0.75 as moderate, 0.75–0.9 as good, and > 0.9 as excellent [46].
Maximum likehood estimation confirmatory factor analysis (CFA) [47] with bootstrapping of 250 iterations was conducted to verify four factor structure of the SURPS. Model goodness-of-fit was estimated by relative χ2, Comparative Fit Index (CFI), Root Mean Square of Approximation (RMSEA), Normed Fit Index (NFI). Relative χ2 < 2, CFI > 0.9 and RMSEA < 0.08, NFI > 0.8 were considered as acceptable [48]. Covariances between factors were included in the model, because personality traits correlated in original scale and in scales validated in other populations. Significant covariances of items belonging to the same factor that resulted in better model fitting were included to model [9, 30]. Items with low weigh loading (< 0.4) were removed from the model. Configural invariance analysis stratified by gender was performed by testing the same model in males and females and by performing a combined group analysis [49]. Metric invariance was evaluated by constricting factor loadings for groups stratified on gender [49].
Clinical diagnosis of alcohol use disorder according to the ICD-10 criteria and the AUDIT results were used to establish discriminative validity of the SURPS. Participants were divided into three groups according to clinical diagnosis of alcohol use disorder and the AUDIT score: control group (AUDIT score < 8), hazardous use of alcohol (AUDIT score > 8 and no clinical diagnosis of alcohol use disorder) and alcohol dependence group (clinical diagnosis of alcohol use disorder). Differences between groups were evaluated by Kruskal – Wallis test. Post-hoc analysis for pairwise comparisons was performed with p-value adjustment for multiple comparisons.
Relative operating characteristic curves (ROC) were applied to evaluate sensitivity and specificity of the SURPS scale for alcohol dependence and hazardous alcohol use [50].
Results
Participants
The final sample consisted of 247 participants, as 4 of volunteers and 3 patients were excluded due to insufficient data (e.g. have not filled some of the scales) and included 108 males and 139 females. Mean age of participants was 37.22 (± 0.78) years. Proportion of females was higher in the control group and proportion of males was higher in the alcohol dependence group. Demographic and clinical data of participants are presented in Table 1.
Table 1.
Demographic and clinical data of participants
| Control group | Particpants with hazardous use of alcohol | Patients with alcohol dependence | Statistics | P value | |
|---|---|---|---|---|---|
| χ2,df | |||||
| Total sample | 140 | 38 | 69 | ||
| Females, (%) | 101 (72.1%) | 18 (47.4%) | 20 (29.0%) | 36.43 (df = 2) | < 0.001 |
| Males, (%) | 39 (27.9%) | 20 (52.6%) | 49 (71.0%) | ||
| F, (df) | |||||
| Age, mean, (SD) | 35.64 (12.54) | 34.00 (12.07) | 42.22 (10.12) | 8.81 (df = 2) | < 0.001 |
| χ2,df | |||||
| Education | |||||
| Basic/secondary, (%) | 34 (24.3%) | 10 (26.3%) | 53 (76.8%) | 56.63 (df = 2) | < 0.001 |
| High school/ University, (%) | 106 (75.7%) | 28 (73.7%) | 16 (23.2%) | ||
| Marital status | |||||
| Single, (%) | 33 (23.6%) | 10 (26.3%) | 23 (33.3%) | 2.25(df = 2) | 0.32 |
| In relationship, (%) | 107 (76.4%) | 28 (73.7%) | 46 (66.7%) | ||
SD standard deviation; Hazardous use of alcohol – persons at risk of alcohol use disorder by cut-off value of 8 of Alcohol Use Disorder Identification test, but without established alcohol dependence diagnosis; df degrees of freedom
Psychometric properties of Substance Use Risk Profile Scale
Structural validity
CFA without included covariances of items resulted in a poor model fit: χ2 (df = 224) = 462.80, p < 0.001, relative χ2 = 2.06, CFI = 0.817, RMSEA = 0.066, NFI = 0.703). Items 22 and 6 had sub-threshold loading weights (< 0.4). Removal of items 6 and 22 and specifying covariances that were suggested by modification indices (between items 1 and 4, and 7 and 23), resulted in improved model fit: χ2 (df = 181) = 353.37, p < 0.001, relative χ2 = 1.95, CFI = 0.863, RMSEA = 0.062, NFI = 0.759). Even though the model fit indices CFI and NFI were slightly below desirable values, we relied on relative χ2 and RMSAE, which are less sensitive to sample size [51], which indicated an appropriate model fit. Four factor structure of the SURPS with included covariances of items is presented in Fig. 1.
Fig. 1.

Four factor structure of the Substance Use Risk Profile Scale with correlations of factors
Examination of factor covariances showed significant correlations between impulsivity and hopelessness, impulsivity and sensation seeking, impulsivity and anxiety sensitivity, hopelessness and anxiety sensitivity, sensation seeking and impulsivity (p < 0.05) and significant negative correlation between sensation seeking and anxiety sensitivity. Other tested covariances were insignificant.
Examination of model for groups stratified by gender demonstrated high configural gender non-invariance (Table 2). The model fit was worse in females than males. However, our study sample was limited, the design of study was explorative and RMSEA and relative χ2 were appropriate for both male and female groups. Therefore, we decided not to remove any more questions and performed analyses for males and females based on the same scale structure.
Table 2.
Configural and metric invariance of the model
| Model | χ2 | df | CFI | RMSEA | ΔCFI | ΔRMSEA | NFI | Relative χ2 |
|---|---|---|---|---|---|---|---|---|
| Baseline model | 353.37 | 181 | 0.86 | 0.06 | 0.76 | 1.95 | ||
| Males | 235.02 | 181 | 0.89 | 0.05 | 0.03 | −0.01 | 0.67 | 1.30 |
| Females | 350.08 | 181 | 0.79 | 0.08 | −0.07 | 0.02 | 0.65 | 1.93 |
| Combined baseline model for males and females | 581.06 | 362 | 0.83 | 0.05 | 0.03 | −0.01 | 0.66 | 1.62 |
| Combined baseline model for males and females, factor loadings constrained to be equal | 606.24 | 379 | 0.82 | 0.05 | 0.04 | −0.01 | 0.65 | 1.60 |
Baseline model – items 6, 22 removed, with covariances 1–4, 7–23 specified
CFI Comparative Fit Index, RMSEA Root Mean Square of Approximation, NFI Normed Fit Index
Internal consistency
Internal consistency of the SURPS subscales measured by the Cronbach coefficient alpha ranged from acceptable to good. The Cronbach’s coefficient alpha was 0.78 for hopelessness subscale, 0.71 for anxiety sensitivity subscale, 0.71 for impulsivity subscale and 0.70 for sensation seeking subscale. Cronbach’s coefficient alpha for the total SURPS scale was 0.74.
Temporal stability
Spearman correlations and ICCs indicated appropriate test-retest stability of the SURPS. There were strong correlations between the two assessment time points for score of the total SURPS scale (r = 0.64, p < 0.001), and scores on the SURPS subscales of hopelessness (r = 0.65, p < 0.001), anxiety sensitivity (r = 0.85, p < 0.001), impulsivity (r = 0.801, p < 0.001), and sensation seeking (r = 0.75, p < 0.001). The ICCs of two assessments documented moderate to good reliability: hopelessness 0.60 (95% CI 0.29–0.80), anxiety sensitivity: 0.80 (95% CI 0.61–0.90), impulsiveness: 0.81 (95% CI 046–0.91), sensation seeking: 0.75 (95% CI 0.52–0.88), total scale: 0. 72 (95% CI - 0.47 – 0.87).
Criterion validity
All subscales had medium to strong significant correlation with the corresponding constructs measured using different self-rating instruments. Spearman correlations of applied instruments are presented in Table 3. As expected, we found positive correlations between similar personality traits and negative correlations between opposite traits measured by the SURPS and corresponding instruments.
Table 3.
Correlations of the scales presenting the construct validity of the Substance Use Profile Scale
| SURPS Hopelessness | SURPS Anxiety Sensitivity | SURPS Impulsivity | SURPS Sensation Seeking | |
|---|---|---|---|---|
| BIS-11 Impulsivity | 0.40 ** | 0.25 ** | 0.62 ** | 0.10 |
| TIPI Extroversion | −0.22** | − 0.18 * | 0.05 | 0.13* |
| TIPI Agreeableness | 0.04 | 0.05 | −0.03 | − 0.10 |
| TIPI Conscientiousness | −0.25** | − 0.004 | − 0.30** | −0.08 |
| TIPI Emotional Stability | −0.29** | −0.31** | − 0.38** | 0.10 |
| TIPI Openness to Experiences | −0.32** | −0.14* | − 0.02 | 0.23** |
| PHQ-4 Depression | 0.42** | 0.34** | 0.42** | −0.05 |
| PHQ-4 Anxiety | 0.39** | 0.36** | 0.44** | −0.04 |
SURPS Substance Use Profile Scale, BIS – 11 Barratt Impulsiveness Scale 11, TIPI Ten Item Personality Measure
*- p < 0.05; **- p < 0.001
SURPS hopelessness subscale score correlated positively with the PHQ – 4 depression subscale score and negatively with the TIPI emotional stability subscale score; The SURPS subscale of anxiety sensitivity score correlated positively with the PHQ – 4 anxiety subscale score and negatively with the TIPI emotional stability score; the SURPS impulsivity subscale score correlated positively with the BIS-11 score and negatively correlated with the TIPI conscientiousness subscale score; the SURPS sensation seeking subscale score correlated positively with the TIPI openness to experience subscale score. In addition, there were medium positive correlations between internalising factors, as the SURPS hopelessness score correlated with the PHQ-4 anxiety score, and the SUPRS anxiety sensitivity correlated with the PHQ-4 depression subscale score. SURPS hopelessness and anxiety sensitivity scores demonstrated medium positive correlations with impulsivity measured by the BIS-11 and a modest negative correlation with conscientiousness subscale of the TIPI. The SURPS impulsivity subscale had medium positive correlations with the PHQ-4 depression and anxiety subscales and a medium negative correlation with the TIPI emotional stability subscale. Internalising traits of the SURPS negatively correlated with the TIPI experience seeking subscale. The SURPS sensation seeking subscale had a weak correlation with the TIPI extroversion subscale.
Sensitivity
Median scores and interquartile ranges of the scores on the SURPS subscales and the total scale and differences between groups of control, hazardous alcohol use and alcohol dependence are presented in Table 4.
Table 4.
Differences of SURPS scores in participants with alcohol dependence, hazardous use of alcohol and controls
| Control group | Hazardous use of alcohol | Alcohol dependence | |||||
|---|---|---|---|---|---|---|---|
| Mean | Median, [Q1-Q3] | Mean | Median, [Q1-Q3] | Mean | Median, [Q1-Q3] | H, (df = 2) | |
| Hopelessness | |||||||
| Total sample | 12.33 | 12 [10–14] | 13.18 | 12.5 [10–14] | 14.83 | 15** [13–18] | 25.32 |
| Males | 12.26 | 12 [10–14] | 12.45 | 12 [10–14] | 15.18 | 15** [13–18] | 17.19 |
| Females | 12.37 | 12 [10–14] | 13.94 | 13 [11.75–14.25] | 13.95 | 14 [12.25–16.75] | 5.63 |
| Anxiety sensitivity | |||||||
| Total sample | 11.86 | 12 [10–14] | 12.76 | 13 [11–15] | 13.32 | 14** [11–16] | 18.03 |
| Males | 10.67 | 10 [9–12] | 11.75 | 12 [9–14] | 13.33 | 14** [11–16] | 15.24 |
| Females | 12.37 | 13 [10–15] | 13.88 | 14 [11–15.25] | 15.25 | 15** [13.25–17.75] | 14.92 |
| Impulsivity | |||||||
| Total sample | 8.33 | 8 [7–10] | 9.00 | 9 [7–10.25] | 10.74 | 13** [11–14] | 41.15 |
| Males | 7.85 | 8 [7–9] | 8.35 | 8 [6.25–10] | 10.59 | 11** [9–12] | 25.11 |
| Females | 8.51 | 8 [7–10] | 9.72 | 9.5 [7.75–12] | 11.10 | 10.5** [10–13] | 19.65 |
| Sensation seeking | |||||||
| Total sample | 12.18 | 12 [9–16] | 13.76 | 14** [12–16.25] | 13.45 | 13* [11–16] | 9.50 |
| Males | 13.54 | 13 [11–16] | 13.60 | 14 [12–16.75] | 13.96 | 14 [12–16] | 0.13 |
| Females | 11.65 | 12 [9–14] | 13.94 | 14** [12–16.25] | 12.20 | 11 [8.5–14.75] | 6.45 |
| Total scale | |||||||
| Total sample | 44.71 | 44 [41–49] | 48.68 | 48** [43.75–53] | 52.90 | 53** [47.5–58] | 55.71 |
| Males | 44.31 | 44 [40–49] | 46.15 | 44.5 [41.25–50.5] | 53.06 | 53** [47–58.5] | 31.40 |
| Females | 44.86 | 45 [41–49] | 51.50 | 51** [47.75–54.25] | 52.50 | 52.5** [48–57.5] | 26.30 |
Q1 quartile 1, Q3 quartile 3, df degrees of freedom
* - p < 0.05, compared to control group; **- adjusted p < 0.05, compared to control group
Patients with alcohol dependence scored significantly higher than the control group on all SURPS subscales. However, the significance of sensation seeking was not maintained after p-value adjustment, and also in gender separate analysis. Stratification by gender revealed that scores of hopelessness were higher in alcohol dependent males but not females.
Hazardous alcohol use as indicated by the AUDIT test cut-off value of 8 was significantly associated with sensation seeking. Stratification by gender revealed that sensation seeking was driven by female group and an association of impulsivity to hazardous use of alcohol was present in females but not males.
Accuracy of the SURPS subscales for discriminating groups of alcohol dependence versus control and of hazardous alcohol use versus control measured by areas under the curves (AUC) are presented in Table 5. Investigation of the ROC curves suggested that the SURPS scale had good sensitivity for alcohol dependence (AUC = 0.81; Fig. 2). There were no meaningful differences in the AUCs for alcohol dependant males and females. However, for hazardous alcohol use, the AUC indicated poor sensitivity of the SURPS scale (AUC = 0.65; Fig. 3). Gender analysis suggested that the SURPS scale was more sensitive for females (AUC = 0.78) than for males for predicting hazardous alcohol use (AUC = 0.56).
Table 5.
Sensitivity of SURPS scale for alcohol dependence and hazardous alcohol use
| Area under the curve (AUC), [95% Cl.] | ||
|---|---|---|
| Hazardous alcohol use versus control | Alcohol dependence versus control | |
| Total sample | 0.65* [0.55–0.77] | 0.81** [0.75–0.88] |
| Males | 0.56 [0.40–0.72] | 0.83** [0.75–0.92] |
| Females | 0.78** [0.66–0.89] | 0.79** [0.67–0.91] |
Hazardous alcohol use – participants who scored 8 or more in the AUDIT test but had no established diagnosis of alcohol dependence. Control – participants without alcohol dependence diagnosis and scored less than 8 in the AUDIT
*- p < 0.05, for the null hypothesis AUC =0.5; **- p < 0.001, for the null hypothesis AUC =0.5
Fig. 2.

Receiver operating characteristic curve (ROC) for alcohol dependence. Sensitivity of Substance Use Risk Profile Scale measured by Area Under the Curve (AUC) on predicting alcohol dependence. AUC = 0.81, p < 0.001
Fig. 3.
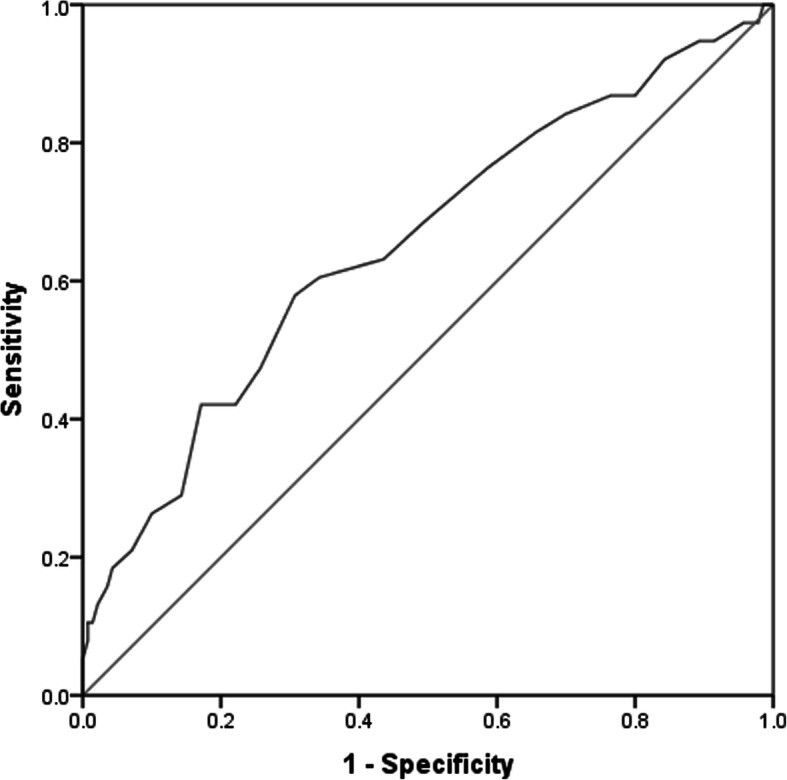
Receiver operating characteristic curve (ROC) for hazardous alcohol use. Sensitivity of Substance Use Risk Profile Scale measured by Area Under the Curve (AUC) on predicting hazardous alcohol use (AUDIT score ≥ 8, but no established diagnosis of alcohol dependence). AUC = 0.65, p < 0.05
Discussion
In this study we aimed to evaluate psychometric properties of the SURPS scale in Lithuanian population. The scale demonstrated appropriate internal validity, good temporal stability, adequate criterion validity, and sensitivity. The construct validity of the scale was appropriate after removal of two items. We examined differences of scores of the SURPS subscales in groups stratified by alcohol dependence, hazardous alcohol use and control to evaluate the sensitivity of the scale. Alcohol dependence group scored higher than the control group in hopelessness, anxiety and impulsivity. Association of the SURPS scores with hazardous use of alcohol was marginal and driven by females.
CFA without added correlations between items 1 and 4, 7 and 23, indicated poor model fitting, thus these correlations were added into the model similarly to other studies of the SURPS scale because of similar wording of questions [9, 30]. Item 6 (“I enjoy new and exciting experiences even if they are unconventional.”) and item 22 (“I feel I have to be manipulative to get what I want.”) had sub-threshold standardized loading coefficients in the CFA and were excluded resulting in appropriate model fit of SURPS scale according to the RMSEA and relative χ2.
Obstacles with the originally proposes four factor structure of SURPS were encountered in prior studies. Specifically, cross-loading of item 16 was also reported in other adaptations of the SURPS scale [26, 31, 33, 45, 52]. Because of cross-loadings, item 16 was removed in a few studies on the SURPS [26, 33, 45, 52], but retained in the Turkish adaptation in order to preserve the original structure of the scale [31]. Moreover, there were suggestions to shorten the scale by removing problematic items: 20 item scale was used in Canada [52] and a 15 item SURPS variant in the USA [53].
The SURPS had appropriate internal consistency and criterion validity. These findings were similar to the original [9] and other SURPS scale validation studies [26, 28–31, 33]. There were small to medium correlations of SURPS internalizing trait subscales (hopelessness and anxiety sensitivity) with impulsivity measured by the BIS-11 and the SURPS impulsiveness subscale. Scores of the SURPS impulsivity subscale had medium correlations with the PHQ-4 depression and anxiety scores. Similar correlation of internalizing traits with impulsivity was also found in other SURPS studies [9, 24, 25, 28, 45]. The tendency for higher hopelessness and anxiety could be associated with higher impulsivity level as impulsive behaviour might reveal itself in negative affects [54]. Diagnosis of alcohol dependence was associated with higher scores on all SURPS subscales except sensation seeking suggesting good sensitivity of the SURPS scale in alcohol dependent individuals. Only a few studies examined properties of the SURPS scale in clinical samples. In Bulgaria, patients were diagnosed with alcohol abuse and dependence according to the DSM-IV criteria [28]. Authors demonstrated associations of impulsivity and sensation seeking with alcohol abuse and an association between impulsivity and alcohol dependence. There was no association of hopelessness and anxiety sensitivity neither with alcohol abuse, nor with dependence in Bulgaria [28]. Nevertheless, in a clinical sample in the USA, hopelessness and anxiety sensitivity were associated with the number of drinks per occasion and alcohol related problems [33]. Moreover, in the USA the internalizing traits were related with both negative reinforcement (coping with emotions) and positive reinforcement (enhancement) motives for consuming alcohol [33]. Whilst the original scale validation study by Woicik et al. [9] have not included clinical samples, authors measured alcohol abuse and dependence symptoms by the Comprehensive Drinker Profile. Alcohol abuse and dependence symptoms were associated with hopelessness, impulsivity and sensation seeking [9]. These divergent findings of personality trait relation to alcohol abuse and dependence suggests inter-cultural differences, and subsequent possibility of the need for different approaches in treatment methods in different populations.
Only a few studies have demonstrated associations of anxiety sensitivity with alcohol use and abuse [9, 51]. The authors of the scale hypothesised that the associations of anxiety sensitivity with abuse of psychotropic substances is more explicit in later stages of addiction development [9]. Our findings agree with this hypothesis, as the scores of anxiety sensitivity subscale were significantly higher in the alcohol dependence group and showed only marginal associations with risky use of alcohol. Chronic alcohol use is known to attenuate hypothalamic-pituitary-adrenal axis, which increases vulnerability to stress and is associated with withdrawal-induced anxiety and dysphoria [55].
We also examined the association of the SURPS scores with hazardous alcohol use as defined using the AUDIT cut-off value of 8. Most prior studies examined the SURPS properties in adolescents and young adults (e.g. university students). In our study participants were older (mean age 37.22 ± 0.78 years), thus we attempted to extend the knowledge of the SURPS properties in adult population. We found that female hazardous users of alcohol scored higher on the SURPS impulsivity and sensation seeking subscales. These findings are congruent with a study from Spain, which also measured hazardous alcohol use by the AUDIT [30]. Other studies using the SURPS scale demonstrated that personality relation with increased risk for alcohol use and abuse were reliant on population and alcohol use measurements [51]. Higher impulsivity and sensation seeking was a common finding in adolescent and young adults with alcohol use and abuse [9, 25, 27, 45, 51, 52]. Impulsive traits and sensation seeking as measured by the SURPS were also linked to higher AUDIT scores [24] and for alcohol use and abuse [27, 51, 52]. Absence of internalising trait association with alcohol abuse was consistent with some studies on adolescents and young adults [24, 27, 30, 51].
Most of prior studies using the SURPS have adjusted their analyses by gender [9, 24, 27, 51, 52], but there is a lack of SURPS studies that provided the gender separate analysis on sensitivity. The divergent findings of personality trait relation to gender alcohol use was demonstrated in France [25]. Few studies demonstrated that males scored more on sensation seeking and females more on anxiety sensitivity or hopelessness [9, 24, 25, 30]. However, in some studies there were no differences in SURPS scores between genders [51].
Different patterns of alcohol use/abuse between genders are well known. Males tend to use alcohol more frequently and more hazardously [34]. One of the systems of alcohol abuse profiling, the Cloninger typology, has shown that personality types of risk of alcohol abuse interact with gender, with harm avoidance being more explicit for females and motives of sensation seeking for males [56]. Therefore, the differences of explication of personality traits as measured by the SURPS and knowledge of divergent pathways in addiction disorders for genders encouraged us to perform gender separate analyses of SURPS external validity. Here, gender separate analysis for alcohol dependence suggested that hopelessness was associated with alcohol dependence in males but not females. Motives of consumption of alcohol as a coping tool have previously been demonstrated to be more frequent for males [34].
In comparison of groups of hazardous alcohol uses and control, gender separate analysis demonstrated that associations of sensation seeking and impulsivity with hazardous alcohol use were driven by females. These findings suggest that the SURPS was more sensitive for females on hazardous alcohol use in our study. However, it is important to notice that Lithuania has overall high alcohol consumption that is driven by males [57]. Therefore, hazardous alcohol use for Lithuanian males could be predisposed more by cultural rather than inherited or personality factors.
Strengths and limitations
Most of the research on the SURPS scale included adolescents or student samples and only few studies included patients with clinical diagnosis of addiction. We demonstrated an appropriate validity of SURPS scale in clinical sample. Knowledge of the SURPS validity and especially of personality traits expression in alcohol dependence would be beneficial for research studies and subsequent choices for personalized treatment methods [56]. Efficacy of current substance disorders treatment methods is poor, only 30% rate is reached when treatment success is evaluated as staying in abstinence [58], although personalised treatment approaches were demonstrated to be more efficient [5, 59].
Moreover, we provided a gender separate analysis for evaluation of SURPS sensitivity. Our results suggested that SURPS scale was more sensitive for females on discriminating hazardous alcohol use. However, the sample size in our study was limited, thus results for gender differences should be interpreted with caution.
Conclusions
We demonstrated an appropriate validity of the Lithuanian translation of the SURPS scale. The SURPS demonstrated good discriminating value for alcohol dependence in our sample. Persons with a diagnosis of alcohol dependence scored higher on the SURPS subscales of hopelessness, anxiety sensitivity and impulsivity. Hazardous alcohol use was associated with impulsivity and sensation seeking, but these associations were driven by females.
However, two questions (items 6 and 22) were removed from the scale to achieve appropriate construct validity and there was a configural gender non-invariance of the scale. Therefore, our results should be interpreted with caution and studies re-evaluating factor structure of the SURPS in Lithuanian populations are encouraged. Nevertheless, the SURPS demonstrated appropriate sensitivity for discriminating alcohol dependence, suggesting that it could be useful for selecting personality targeted alcohol misuse prevention and treatment approaches.
Acknowledgements
Not applicable.
Abbreviations
- SURPS
Substance Use Risk Profile Scale
- AUDIT
Alcohol Use Disorder Identification Test
- ICD – 10
International Classification of Diseases – 10
- DSM-5
Diagnostic and Statistical Manual of Mental Disorders – 5
- MMPI
Minnesota Multiphasic Personality Inventory
- TPQ
Tridimensional Personality Questionnaire
- APP
Addiction Prone Personality Scale
- BIS − 11
Barratt Impulsiveness Scale – 11
- TIPI
Ten Item Personality Measure
- PHQ-4
Patient Health Questionnaire - 4
- WHO
World Health Organization
- EFA
Exploratory factor analysis
- CFA
Confirmatory factor analysis
- CFI
Comparative Fit Index
- RMSEA
Root Mean Square of Approximation
- NFI
Normed Fit Index
- ROC
Relative operating characteristic curve
- AUC
Area under the curve
- SD
Standard deviation
- df
Degrees of freedom
- Q1
Quartile 1
- Q3
Quartile 3
Authors’ contributions
M.K.: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – Original Draft Preparation, Writing – Review & Editing; A.Pr.: Conceptualization, Methodology, Writing – Review & Editing; A.B.: Methodology, Supervision, Writing – Review & Editing; J.J.: Investigation, Methodology, Writing – Original Draft Preparation, Writing – Review & Editing; D.J.: Investigation, Writing – Review & Editing; A.Pl.: Investigation, Writing – Review & Editing; I.L.: Writing – Original Draft Preparation; L.S.: Funding Acquisition, Project Administration, Supervision, Writing – Original Draft Preparation, Writing – Review & Editing; R.J.: Conceptualization,. Funding Acquisition, Project Administration, Supervision, Writing – Review & Editing. The author(s) read and approved the final manuscript.
Funding
This work was supported by joint KTU-LSMU-VDU-LEI Research Projects Fund.
Availability of data and materials
All necessary data is included in the manuscript. Additional data is available from corresponding author upon request.
Ethics approval and consent to participate
The study protocol and consent procedures were approved by the Regional Bioethics Committee for Biomedical Research (Nr. BE-2-25). All participants signed written informed consent with ability to discontinue participation at any time.
Consent for publication
Not applicable.
Competing interests
The authors declare having no conflict of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Hasin DS, O’Brien CP, Auriacombe M, Borges G, Bucholz K, Budney A, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013;170(8):834–851. doi: 10.1176/appi.ajp.2013.12060782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hakulinen C, Hintsanen M, Munafò MR, Virtanen M, Kivimäki M, Batty GD, et al. Personality and smoking: individual-participant meta-analysis of nine cohort studies. Addiction. 2015;110(11):1844–1852. doi: 10.1111/add.13079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hakulinen C, Elovainio M, Batty GD, Virtanen M, Kivimäki M, Jokela M. Personality and alcohol consumption: pooled analysis of 72,949 adults from eight cohort studies. Drug Alcohol Depend. 2015;151:110–114. doi: 10.1016/j.drugalcdep.2015.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lyszczarz B. Production losses associated with alcohol-attributable mortality in the European Union. Int J Environ Res Public Health. 2019;16(19):3536. doi: 10.3390/ijerph16193536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Foulds J, Newton-Howes G, Guy NH, Boden JM, Mulder RT. Dimensional personality traits and alcohol treatment outcome: a systematic review and meta-analysis. Addiction. 2017;112(8):1345–1357. doi: 10.1111/add.13810. [DOI] [PubMed] [Google Scholar]
- 6.MacAndrew C. The differentiation of male alcoholic outpatients from nonalcoholic psychiatric outpatients by means of the MMPI. Q J Stud Alcohol. 1965;26(2):238–246. [PubMed] [Google Scholar]
- 7.Cloninger CR. A systematic method for clinical description and classification of personality variants. Arch Gen Psychiatry. 1987;44(6):573. doi: 10.1001/archpsyc.1987.01800180093014. [DOI] [PubMed] [Google Scholar]
- 8.Barnes GE, Murray RP, Patton D, Bentler PM, Anderson R. The addiction-prone personality. New York: Kluwer Academic/ Plenum Publishers; 2000. [Google Scholar]
- 9.Woicik PA, Stewart SH, Pihl RO, Conrod PJ. The substance use risk profile scale: A scale measuring traits linked to reinforcement-specific substance use profiles. Addict Behav. 2009;34(12):1042–1055. doi: 10.1016/j.addbeh.2009.07.001. [DOI] [PubMed] [Google Scholar]
- 10.Malmberg M, Overbeek G, Monshouwer K, Lammers J, Vollebergh WAM, Engels RCME. Substance use risk profiles and associations with early substance use in adolescence. J Behav Med. 2010;33(6):474–485. doi: 10.1007/s10865-010-9278-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cho SB, Su J, Kuo SI-C, Bucholz KK, Chan G, Edenberg HJ, et al. Positive and negative reinforcement are differentially associated with alcohol consumption as a function of alcohol dependence. Psychol Addict Behav. 2019;33(1):58–68. doi: 10.1037/adb0000436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Raketic D, Barisic JV, Svetozarevic SM, Gazibara T, Tepavcevic DK, Milovanovic SD, et al. Five-factor model personality profiles: the differences between alcohol and opiate addiction among females. Psychiatr Danub. 2017;29(1):74–80. doi: 10.24869/psyd.2017.74. [DOI] [PubMed] [Google Scholar]
- 13.Gentry RN, Schuweiler DR, Roesch MR. Dopamine signals related to appetitive and aversive events in paradigms that manipulate reward and avoidability. Brain Res. 2019;1713:80–90. doi: 10.1016/j.brainres.2018.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nutt DJ, Lingford-Hughes A, Erritzoe D, Stokes PRA. The dopamine theory of addiction: 40 years of highs and lows. Nat Rev Neurosci. 2015;16(5):305–312. doi: 10.1038/nrn3939. [DOI] [PubMed] [Google Scholar]
- 15.Levy S, Katusic SK, Colligan RC, Weaver AL, Killian JM, Voigt RG, et al. Childhood ADHD and Risk for Substance Dependence in Adulthood: A Longitudinal, Population-Based Study. Skoulakis EMC, editor. PLoS ONE. 2014;9(8):e105640. doi: 10.1371/journal.pone.0105640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wilens TE, Martelon M, Joshi G, Bateman C, Fried R, Petty C, et al. Does ADHD predict substance-use disorders? A 10-year follow-up study of young adults with ADHD. J Am Acad Child Adolesc Psychiatry. 2011;50(6):543–553. doi: 10.1016/j.jaac.2011.01.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Grant JE, Chamberlain SR. Impulsive action and impulsive choice across substance and behavioral addictions: cause or consequence? Addict Behav. 2014;39(11):1632–1639. doi: 10.1016/j.addbeh.2014.04.022. [DOI] [PubMed] [Google Scholar]
- 18.Bidwell LC, Knopik VS, Audrain-Mcgovern J, Glynn TR, Spillane NS, Ray LA, et al. Novelty seeking as a phenotypic marker of adolescent substance use. Subst Abus Res Treat. 2015;9s1:SART.S22440. doi: 10.4137/sart.s22440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Young-Wolff KC, Kendler KS, Sintov ND, Prescott CA. Mood-related drinking motives mediate the familial association between major depression and alcohol dependence. Alcohol Clin Exp Res. 2009;33(8):1476–1486. doi: 10.1111/j.1530-0277.2009.00978.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Grant VV, Stewart SH, Mohr CD. Coping-anxiety and coping-depression motives predict different daily mood-drinking relationships. Psychol Addict Behav. 2009;23(2):226–237. doi: 10.1037/a0015006. [DOI] [PubMed] [Google Scholar]
- 21.Davis L, Uezato A, Newell JM, Frazier E. Major depression and comorbid substance use disorders. Curr Opin Psychiatry. 2008;21(1):14–18. doi: 10.1097/YCO.0b013e3282f32408. [DOI] [PubMed] [Google Scholar]
- 22.Torvik FA, Rosenström TH, Gustavson K, Ystrom E, Kendler KS, Bramness JG, et al. Explaining the association between anxiety disorders and alcohol use disorder: A twin study. Depress Anxiety. 2019;36(6):522–532. doi: 10.1002/da.22886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Becker HC. Influence of stress associated with chronic alcohol exposure on drinking. Neuropharmacology. 2017;122:115–126. doi: 10.1016/j.neuropharm.2017.04.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jurk S, Kuitunen-Paul S, Kroemer NB, Artiges E, Banaschewski T, Bokde ALW, et al. Personality and Substance Use: psychometric evaluation and validation of the Substance Use Risk Profile Scale (SURPS) in English, Irish, French, and German adolescents. Alcohol Clin Exp Res. 2015;39(11):2234–2248. doi: 10.1111/acer.12886. [DOI] [PubMed] [Google Scholar]
- 25.Ali A, Carré A, Hassler C, Spilka S, Vanier A, Barry C, et al. Risk factors for substances use and misuse among young people in France: What can we learn from the Substance Use Risk Profile Scale? Drug Alcohol Depend. 2016;163:84–91. doi: 10.1016/j.drugalcdep.2016.03.027. [DOI] [PubMed] [Google Scholar]
- 26.Castonguay-Jolin L, Perrier-Ménard E, Castellanos-Ryan N, Parent S, Vitaro F, Tremblay RE, et al. Validation de la traduction française de la SURPS pour une population d adolescents québécois. Can J Psychiatr. 2013;58(9):538–545. doi: 10.1177/070674371305800909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Malmberg M, Kleinjan M, Overbeek G, Vermulst AA, Lammers J, Engels RCME. Are there reciprocal relationships between substance use risk personality profiles and alcohol or tobacco use in early adolescence? Addict Behav. 2013;38(12):2851–2859. doi: 10.1016/j.addbeh.2013.08.003. [DOI] [PubMed] [Google Scholar]
- 28.Long EC, Milcheva S, Psederska E, Vasilev G, Bozgunov K, Nedelchev D, Gillespie NA, Vassileva J. Validation of the Substance Use Risk Profile Scale (SURPS) With Bulgarian Substance Dependent Individuals. Frontiers in psychology. 2018;9:2296. 10.3389/fpsyg.2018.02296. [DOI] [PMC free article] [PubMed]
- 29.Robles-García R, Fresán A, Castellanos-Ryan N, Conrod P, Gómez D, et al. Spanish version of the Substance Use Risk Profile Scale: factor structure, reliability, and validity in Mexican adolescents. Psychiatry Res. 2014;220(3):1113–1117. doi: 10.1016/j.psychres.2014.08.057. [DOI] [PubMed] [Google Scholar]
- 30.Fernández-Calderón F, Díaz-Batanero C, Rojas-Tejada AJ, Castellanos-Ryan N, Lozano-Rojas ÓM. Adaptación a la población española de la Escala de Perfil de Riesgo de Consumo de Drogas (EPRCD) y estudio de sus propiedades psicométricas. Adicciones. 2017;30(3):208. doi: 10.20882/adicciones.909. [DOI] [PubMed] [Google Scholar]
- 31.Uygun SD, Cop E, Uneri OS, Ozdel K, Atar E, Munir KM. Psychometric evaluation of the Turkish version of the Substance Use Risk Profile Scale in adolescents. J Ethn Subst Abuse. 2019;2:1–16. doi: 10.1080/15332640.2019.1657542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Chen F, Yang H, Bulut O, Cui Y, Xin T. Examining the relation of personality factors to substance use disorder by explanatory item response modeling of {DSM}-5 symptoms. Tye M, editor. PLOS ONE. 2019;14(6):e0217630. doi: 10.1371/journal.pone.0217630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Schlauch RC, Crane CA, Houston RJ, Molnar DS, Schlienz NJ, Lang AR. Psychometric evaluation of the Substance Use Risk Profile Scale (SURPS) in an inpatient sample of substance users using cue-reactivity methodology. J Psychopathol Behav Assess. 2015;37(2):231–246. doi: 10.1007/s10862-014-9462-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nolen-Hoeksema S, Hilt L. Possible contributors to the gender differences in alcohol use and problems. J Gen Psychol. 2006;133(4):357–374. doi: 10.3200/GENP.133.4.357-374. [DOI] [PubMed] [Google Scholar]
- 35.Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51(6):768–774. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- 36.Fossati A, Di Ceglie A, Acquarini E, Barratt ES. Psychometric properties of an Italian version of the Barratt impulsiveness Scale-11 (BIS-11) in nonclinical subjects. J Clin Psychol. 2001;57(6):815–828. doi: 10.1002/jclp.1051. [DOI] [PubMed] [Google Scholar]
- 37.International Test Commission ITC guidelines for translating and adapting tests (second edition) Int J Test. 2018;18(2):101–134. [Google Scholar]
- 38.Bunevicius A, Katkute A, Bunevicius R. Symptoms of anxiety and depression in medical students and in humanities students: relationship with big-five personality dimensions and vulnerability to stress. Int J Soc Psychiatry. 2008;54(6):494–501. doi: 10.1177/0020764008090843. [DOI] [PubMed] [Google Scholar]
- 39.Bunevicius A, Staniute M, Brozaitiene J, Stropute D, Bunevicius R, Denollet J. Type D (distressed) personality and its assessment with the DS14 in Lithuanian patients with coronary artery disease. J Health Psychol. 2013;18(9):1242–1251. doi: 10.1177/1359105312459098. [DOI] [PubMed] [Google Scholar]
- 40.Aluja A, Garcıa O, Garcia LF. Relationships among extraversion, openness to experience, and sensation seeking. Pers Individ Dif. 2003;35(3):671–680. [Google Scholar]
- 41.Kroenke K, Spitzer RL, Williams JBW, Lowe B. An ultra-brief screening Scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613–621. doi: 10.1176/appi.psy.50.6.613. [DOI] [PubMed] [Google Scholar]
- 42.Bunevicius A, Deltuva V, Tamasauskas S, Tamasauskas A, Bunevicius R. Screening for psychological distress in neurosurgical brain tumor patients using the patient Health Questionnaire-2. Psychooncology. 2013;22(8):1895–1900. doi: 10.1002/pon.3237. [DOI] [PubMed] [Google Scholar]
- 43.Bohn MJ, Babor TF, Kranzler HR. The Alcohol Use Disorders Identification Test (AUDIT): validation of a screening instrument for use in medical settings. J Stud Alcohol. 1995;56(4):423–432. doi: 10.15288/jsa.1995.56.423. [DOI] [PubMed] [Google Scholar]
- 44.Reinert DF, Allen JP. The Alcohol Use Disorders Identification Test (AUDIT): a review of recent research. Alcohol Clin Exp Res. 2002;26(2):272–279. [PubMed] [Google Scholar]
- 45.Castellanos-Ryan N, O’Leary-Barrett M, Sully L, Conrod P. Sensitivity and specificity of a brief personality screening instrument in predicting future substance use, emotional, and behavioral problems: 18-month predictive validity of the Substance Use Risk Profile Scale. Alcohol Clin Exp Res. 2012;37:E281–E290. doi: 10.1111/j.1530-0277.2012.01931.x. [DOI] [PubMed] [Google Scholar]
- 46.Koo TK, Li MY. A guideline of selecting and reporting Intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Yuan K-H, Chan W, Bentler PM. Robust transformation with applications to structural equation modelling. Br J Math Stat Psychol. 2000;53(1):31–50. doi: 10.1348/000711000159169. [DOI] [PubMed] [Google Scholar]
- 48.Matsunaga M. Item parceling in structural equation modeling: A primer. Commun Methods Meas. 2008;2(4):260–293. [Google Scholar]
- 49.Putnick DL, Bornstein MH. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. 2016;41:71–90. doi: 10.1016/j.dr.2016.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Swets J. Measuring the accuracy of diagnostic systems. Science (80- ) 1988;240(4857):1285–1293. doi: 10.1126/science.3287615. [DOI] [PubMed] [Google Scholar]
- 51.Newton NC, Barrett EL, Castellanos-Ryan N, Kelly E, Champion KE, Stapinski L, et al. The validity of the Substance Use Risk Profile Scale (SURPS) among Australian adolescents. Addict Behav. 2016;53:23–30. doi: 10.1016/j.addbeh.2015.09.015. [DOI] [PubMed] [Google Scholar]
- 52.Krank M, Stewart SH, O’Connor R, Woicik PB, Wall A-M, Conrod PJ. Structural, concurrent, and predictive validity of the Substance Use Risk Profile Scale in early adolescence. Addict Behav. 2011;36(1–2):37–46. doi: 10.1016/j.addbeh.2010.08.010. [DOI] [PubMed] [Google Scholar]
- 53.Blanchard BE, Stevens AK, Sher KJ, Littlefield AK. Reexamining the psychometric properties of the Substance Use Risk Profile Scale. Assessment. 2020;27(3):454–471. doi: 10.1177/1073191118820135. [DOI] [PubMed] [Google Scholar]
- 54.Herman AM, Critchley HD, Duka T. Risk-Taking and Impulsivity: The Role of Mood States and Interoception. Frontiers in psychology. 2018;9:1625. 10.3389/fpsyg.2018.01625. [DOI] [PMC free article] [PubMed]
- 55.Koob G. Drug addiction, dysregulation of reward, and allostasis. Neuropsychopharmacology. 2001;24(2):97–129. doi: 10.1016/S0893-133X(00)00195-0. [DOI] [PubMed] [Google Scholar]
- 56.Gierski F, Benzerouk F, De Wever E, Duka T, Kaladjian A, Quaglino V, et al. Cloninger’s temperament and character dimensions of personality and binge drinking among college students. Alcohol Clin Exp Res. 2017;41(11):1970–1979. doi: 10.1111/acer.13497. [DOI] [PubMed] [Google Scholar]
- 57.Buccelli C, Della Casa E, Paternoster M, Niola M, Pieri M. Gender differences in drug abuse in the forensic toxicological approach. Forensic Sci Int. 2016;265:89–95. doi: 10.1016/j.forsciint.2016.01.014. [DOI] [PubMed] [Google Scholar]
- 58.Dawson DA, Goldstein RB, Grant BF. Rates and correlates of relapse among individuals in remission from DSM-IV alcohol dependence: A 3-year follow-up. Alcohol Clin Exp Res. 2007;31(12):2036–2045. doi: 10.1111/j.1530-0277.2007.00536.x. [DOI] [PubMed] [Google Scholar]
- 59.Dimaggio G, D’Urzo M, Pasinetti M, Salvatore G, Lysaker PH, Catania D, et al. Metacognitive interpersonal therapy for co-occurrent avoidant personality disorder and Substance abuse. J Clin Psychol. 2015;71(2):157–166. doi: 10.1002/jclp.22151. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All necessary data is included in the manuscript. Additional data is available from corresponding author upon request.