

Abstract
Background
There are spatial disparities in cardiovascular disease (CVD) mortality related to area‐level socioeconomic status (SES) disadvantage, but little is known about the spatial distribution of CVD mortality according to built environment factors. We examined joint associations of neighborhood walkability attributes and SES with CVD mortality rates through linkage of Japanese national data sets.
Methods and Results
National data were used from the 1824 municipalities (of the 1880 potentially eligible municipalities) across Japan. The outcome was mortality from CVD for a 5‐year period (2008–2012) for each municipality. A national index of neighborhood deprivation was used as an indicator of municipality‐level SES. A national walkability index (based on population density, road density, and access to commercial areas) was calculated. Compared with higher SES municipalities, relative rates for CVD mortality were significantly higher in medium SES municipalities (relative rate, 1.05; 95% CI, 1.02–1.07) and in lower SES municipalities (relative rate, 1.09; 95% CI, 1.07–1.12). There were walkability‐related gradients in CVD mortality within the high and medium SES areas, in which lower walkability was associated with higher rates of mortality; however, walkability‐related CVD mortality gradients were not apparent in lower SES municipalities.
Conclusions
CVD mortality rates varied not only by area‐level SES but also by walkability. Those living in areas of lower walkability were at higher risk of CVD mortality, even if the areas have a higher SES. Our findings provide a novel element of the evidence base needed to inform better allocation of services and resources for CVD prevention.
Keywords: built environment, deprivation, heart disease, urban design
Subject Categories: Epidemiology, Cardiovascular Disease
Nonstandard Abbreviations and Acronyms
- CVD
cardiovascular disease
- SES
socioeconomic status
Clinical Perspective
What Is New?
Cardiovascular disease mortality rates varied not only by area‐level socioeconomic status but also by walkability.
A novel finding of this study is that higher and medium socioeconomic status municipalities can also be at risk if their walkability is low.
What Are the Clinical Implications?
Our findings can contribute to better understanding of spatial distribution of disadvantage and health, identifying where additional resources and innovative prevention initiatives are needed to reduce cardiovascular disease risk.
Cardiovascular disease (CVD) is a leading cause of death worldwide,1 especially in the aging populations.2 There are wide geographic variations in CVD mortality.3, 4, 5, 6 For example, the age‐standardized rates of CVD mortality of 47 prefectures in Japan were found to range from 36 to 55 per 100 000, and disparities between prefectures have been increasing.2 Geographic disparities in CVD mortality can be related to socioeconomic status (SES) disadvantage.7
The unequal distribution of health‐enhancing resources and health‐damaging hazards between less disadvantaged and more disadvantaged locations can contribute to such inequalities, both within and between countries.8, 9, 10 Neighborhood‐level socioeconomic disadvantage has been shown to be detrimentally associated with CVD mortality among older British men, independent of individual‐level social class and CVD risk factors.11 Similar socioeconomic gradients in CVD mortality have been identified in both men and women in the United States.12
Built environment attributes can be associated with risk factors for CVD, including physical inactivity,13, 14 obesity,15 type 2 diabetes mellitus,16 and high blood pressure.17 For example, across 14 cities worldwide, residential density, street connectivity, and access to parks and public transit stops were found to be associated with adults’ physical activity.13 A recent systematic review of longitudinal studies also suggests that living in more walkable environments is protective against obesity, type 2 diabetes mellitus, and hypertension.17 As the built environment attributes conducive to lower levels of physical activity and greater chronic disease risk can be unequally geographically distributed,13, 18, 19 a better understanding of how built environmental attributes and area‐level SES are jointly related to CVD is needed. Such evidence will inform policymakers, urban design practitioners, and clinicians of future preventive strategies for CVD by identifying high‐risk areas.
Linking Japanese national databases on SES, the built environment, and CVD mortality, we examined joint associations of neighborhood walkability attributes and SES with CVD mortality rates.
Methods
Japan national data, obtained from several sources (as described in what follows), were linked at the municipality level. The data that support the findings of this study are available from the corresponding author upon reasonable request. There were a total of 1880 municipalities (186 wards, 760 cities, 750 towns, and 184 villages) in Japan in 2010.20 Institutional review board approval was not required for this study.
CVD Mortality
Mortality from CVD (the number of observed deaths from all types of CVD) for a 5‐year period (2008–2012) for each municipality was the outcome of the study. A cardiovascular death was adjudicated when the main cause of death on the death certificate was “Heart diseases excluding hypertensive diseases” (International Classification of Diseases, Tenth Revision (ICD‐10), codes: I01–I02.0, I05–I09, I20–I25, I27, and I30–I52). This was reported in the Vital Statistics provided by the Health Center Districts and Municipalities.21 Because the number of observed deaths depends on the size and age composition of each municipality, analyses were adjusted for the expected number of deaths, which was calculated using the following formula:
where p ik is the population size of a specific 5‐year age group k in municipality i, and r k is the annual national standard mortality for age group k.
The age‐specific populations for each municipality, p ik, were obtained from the 2010 Population Census of Japan.22 The national standard age‐specific mortality, r k, for the study period (2008–2012) was provided by the Ministry of Health, Labour and Welfare.21
Socioeconomic Status
A Japanese national index of neighborhood deprivation was used as an indicator of municipality‐level SES. This index was constructed based on the Breadline Britain poverty measure,23 and the European transnational ecological deprivation measure.24 The detailed methods of constructing this index have been described elsewhere.25 Briefly, this composite index included the weighted sums of several poverty‐related census variables (as of 2010), including unemployment rate, proportion of sales and service workers, proportion of agricultural workers, proportion of blue‐collar workers, proportion of rented houses, proportion of elderly single households, proportion of single‐mother households, and proportion of elderly couple households. The weights of these variables were taken from the estimated odds ratios in a logistic regression analysis used to predict “poverty households”, using microdata from Japanese social surveys measuring poverty.25 All municipality units were stratified into tertiles according to the score of deprivation: lower, medium, and higher SES municipalities.
Built Environmental Attributes
The study used 3 neighborhood built environmental attributes (and their composite) previously developed and calculated for the entire area of Japan.20 Briefly, population density, street density, and access to commercial areas were calculated at the municipality level using geographic information systems. These built environmental attributes were chosen based on previous studies showing their associations with physical activity.14, 26 It has been shown that high‐density neighborhoods with well‐connected streets tend to have more easily accessible commercial destinations, which can facilitate residents’ physical activity through convenience of, and purposes for, walking.27 Because most municipalities in Japan are not homogeneous (eg, consisting of more populated urban areas and less populated areas, such as agricultural land, forests, and mountains), simply calculating the mean environmental attributes within the municipality area can produce estimates that do not reflect the presence of less populated areas. To address this issue, we first measured the 3 environmental attributes at the neighborhood level (chocho‐aza, the smallest administrative unit in Japan, with an average population of about 500 people), then calculated population‐weighted average values (ie, summing each neighborhood's attributes multiplied by its population and dividing it by the entire population of the municipality).
The following data sources and methods were used to calculate each environmental attribute. Population density data at the chocho‐aza level were obtained from the 2010 Population Census of Japan.22 Street density data were available from the 2010 National Land Numerical Information 28 and was defined as the total length of streets within the area of the tertiary mesh. The tertiary mesh is an approximately 1×1‐km grid defined by latitude and longitude. The street density of each neighborhood was obtained from the mesh that included the centroid of the neighborhood. For access to commercial areas, retail area data for 2011 released by the Zenrin Co were used.29 For each neighborhood, straight distance from its centroid to the nearest boundary of a commercial area was used, as defined by a cluster of ≥10 retail destinations using a geographic information systems buffering technique. Retail destinations included grocery stores, supermarkets, clothing stores, household goods stores, hair salons, drug stores, restaurants, sporting goods stores, amusement facilities (eg, video game arcades, and movie theaters), professional offices (eg, medical clinics and real estate offices), banks, and accommodations. They did not include noncommercial destinations such as train stations, schools, and parks. A neighborhood walkability score was calculated by summing the Z scores of each of these 3 measures (the distance to commercial areas was reverse‐coded with higher scores indicating shorter distances). These attributes can be considered equivalent to 3 conventional components of walkability (population density, street connectivity, and land‐use diversity).30 Walkability and each component score were categorized into tertiles.
Statistical Analysis
To characterize municipality‐level variations in CVD mortality, we used standardized mortality ratios, calculated as follows:
Standardized mortality ratios indicate how each municipality's mortality is higher or lower than the national standard (set as 100). We conducted Poisson regression analyses with robust standard errors, using the number of observed deaths as the dependent variable, the expected number of deaths as the offset variable, and municipality‐level SES as the independent variable (reference: higher SES municipalities). Poisson regression rather than standard ordinary least squares was chosen because this is a standard way to model count data for deaths. These more robust estimators of standard errors of coefficients were used to deal with the overdispersion (poor fitting) of Poisson regression to the data. Our analysis examined the associations of CVD mortality with the joint category of area‐level SES and each walkability attribute. We produced the 3×3 categories of SES and walkability (or walkability attributes) and used them as the independent variable (reference: higher SES higher walkability). We also conducted SES‐specific analyses to examine whether mortality differed significantly according to walkability levels for each SES stratum. The interactions between SES (categorical) and walkability attributes (continuous) were examined to test effect modification by SES on the associations of walkability attributes with CVD mortality (Table S1). Analyses were conducted using Stata version 15.0 (StataCorp, College Station, Texas) and the level of significance was set at P<0.05.
Results
Of the 1880 potentially eligible municipalities, 56 were excluded because of lack of mortality data, leaving 1824 with full data. Table 1 shows the characteristics of participating municipalities, overall, and according to area‐level SES. Neighborhood walkability mean was significantly higher in higher SES municipalities than in medium and lower SES municipalities. Higher SES municipalities were also more densely populated, better connected, and had better access to commercial areas than medium and lower SES municipalities. Lower SES municipalities had a significantly higher CVD mortality than higher and medium SES municipalities (ANOVA test).
Table 1.
Characteristics of Municipalities in Japan, Overall, and According to Municipality‐Level SES
| Median (IQR) | ||||
|---|---|---|---|---|
| Total (N=1824) | Higher SES (n=608) | Medium SES (n=608) | Lower SES (n=608) | |
| Municipality size, km2 | 107.1 (38.9 to 254.2) | 56.8 (23.5 to 137.5) | 123.4 (48.6 to 264.7) | 175.3 (70.0 to 344.6) |
| Neighborhood walkability | −0.5 (−1.4 to 0.9) | 0.6 (−0.5 to 2.7) | −0.6 (−1.3 to 0.5) | −1.2 (−2.0 to 0.3) |
| Population density (1000 people/km2) | 1.6 (0.6 to 4.4) | 3.7 (1.5 to 8.1) | 1.3 (0.6 to 3.5) | 0.9 (0.3 to 2.0) |
| Access to commercial area, km | 1.9 (0.9 to 3.5) | 1.1 (0.5 to 2.0) | 2.0 (1.0 to 3.5) | 2.8 (1.6 to 4.8) |
| Percentages of older adults | 26.4 (21.9 to 31.5) | 21.9 (19.5 to 24.7) | 26.8 (22.7 to 30.9) | 31.7 (27.5 to 36.1) |
| SMR for CVD | 100.6 (90.0 to 113.1) | 97.6 (87.9 to 109.9) | 100.0 (90.2 to 112.4) | 104.7 (92.5 to 118.4) |
CVD indicates cardiovascular disease; IQR, interquartile range; SES, socioeconomic status; and SMR, standardized mortality ratio.
Table 2 shows the median standardized mortality ratios for municipalities categorized by tertiles of SES and each environmental attribute. As shown in Table 2, the CVD mortality in lower SES, higher walkability areas was 104.5, which was very similar to that of lower SES, medium/lower walkability areas (105.5 and 104.5, respectively), and there was a reasonable number of municipalities in the former category (n=82). Figure shows the distribution of CVD mortality (SMR), SES, and walkability across Japan. The distribution of specific environmental attributes is shown in Figure S1.
Table 2.
Standardized Mortality Ratios for CVD by Joint Category of Municipality‐Level SES and Built Environmental Attributes
| Environmental Attributes | Median (IQR) SMR | ||
|---|---|---|---|
| Higher SES | Medium SES | Lower SES | |
| Neighborhood walkability | |||
| Higher (0.3 to 8.6) | 94.7 (86.3–105.9) | 98.5 (89.0–109.3) | 104.5 (95.9–114.7) |
| Medium (−1.0 to 0.3) | 101.7 (91.4–112.9) | 99.6 (89.3–112.9) | 105.5 (94.2–117.3) |
| Lower (−27.8 to −1.0) | 101.3 (92.4–115.6) | 101.7 (93.3–114.5) | 104.5 (90.9–120.1) |
| Population density (people/km2) | |||
| Higher (3068 to 26 578) | 94.7 (86.7–106.2) | 98.3 (88.5–109.7) | 104.4 (95.1–114.9) |
| Medium (895 to 3068) | 99.6 (89.9–111.7) | 99.5 (89.9–111.7) | 105.4 (93.1–118.8) |
| Lower (5 to 895) | 104.6 (92.6–117.8) | 101.8 (92.0–115.7) | 104.4 (91.8–119.6) |
| Road density, m/km2 | |||
| Higher (9387 to 36 979) | 94.5 (86.3–105.3) | 98.0 (89.3–109.2) | 104.1 (95.1–114.0) |
| Medium (5009 to 9387) | 101.9 (91.6–112.6) | 100.7 (90.0–113.7) | 103.0 (90.7–115.8) |
| Lower (0 to 5009) | 104.3 (93.1–118.7) | 101.0 (90.8–112.8) | 105.5 (92.8–121.4) |
| Access to commercial areas, m | |||
| Closer (21 to 1221) | 94.8 (86.8–105.9) | 98.6 (88.4–110.3) | 106.9 (96.2–119.9) |
| Medium (1221 to 2774) | 100.3 (90.0–111.2) | 100.0 (90.4–112.8) | 105.0 (95.1–115.7) |
| Farther (2774 to 75 083) | 103.9 (92.6–120.5) | 101.2 (91.4–113.7) | 103.9 (90.2–119.8) |
CVD indicates cardiovascular disease; IQR, interquartile range; and SMR, standardized mortality ratio.
Figure 1. Distribution of the standardized mortality ratios for CVD, socioeconomic status, and neighborhood walkability across Japan.
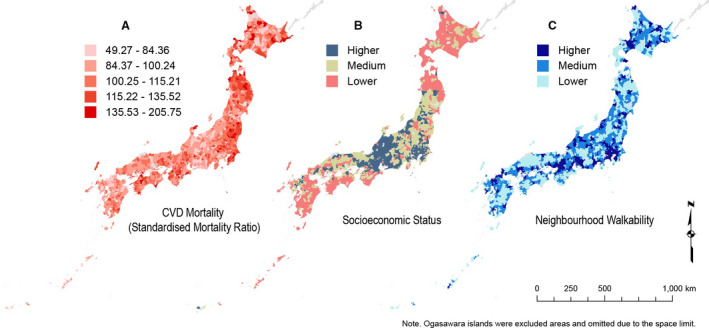
CVD indicates cardiovascular disease.
Regression analyses for the whole sample found that lower and medium SES municipalities had 9% higher (95% CI, 1.07–1.12) and 5% higher (95% CI, 1.02–1.07) CVD mortality relative to higher SES municipalities. Table 3 shows the relative rates for CVD mortality for the joint categories of SES and walkability attributes. In the higher SES areas, the relative rate for lower walkability areas was 1.08 (95% CI, 1.03–1.13) relative to higher walkability area (reference). There was a similar CVD walkability gradient in the medium SES areas. The relative rate for lower, medium, and higher walkability areas were 1.08 (95% CI, 1.05–1.11), 1.07 (95% CI, 1.04–1.10), and 1.04 (95% CI, 1.00–1.07) (reference: high SES and high walkability). However, there were no significant differences in CVD mortality, according to walkability in the lower SES areas. The relative rate for lower, middle, and higher walkability areas (reference: high SES and high walkability) were 1.09 (95% CI, 1.06–1.12), 1.09 (95% CI, 1.05–1.13), and 1.11 (95% CI, 1.06–1.16). Similar patterns were observed for each specific walkability component (population density, road density, and access to commercial areas). The interaction of SES and walkability was marginally significant between lower and higher SES municipalities (P<0.1) but not significant between medium and higher SES municipalities (Table S1).
Table 3.
Relative Rates of CVD Mortality for Joint Categories of Municipality‐Level SES and Built Environmental Attributes
| Environmental Attributes | Relative Rate (95% CI) | ||
|---|---|---|---|
| Higher SES | Medium SES | Lower SES | |
| Population density | |||
| Higher (3068 to 26 578) | 1 | 1.04 (1.00–1.07)a | 1.10 (1.06–1.15)a |
| Medium (895 to 3067) | 1.01 (0.98–1.05) | 1.06 (1.03–1.10)a | 1.09 (1.06–1.13)a |
| Lower (5 to 895) | 1.11 (1.06–1.16)a | 1.09 (1.05, 1.12)a | 1.10 (1.06–1.13)a |
| Road density | |||
| Higher (9387 to 36 979) | 1 | 1.04 (1.01–1.07)a | 1.11 (1.07–1.16)a |
| Medium (5009 to 9379) | 1.04 (1.00–1.07)a | 1.07 (1.04–1.11)a | 1.08 (1.05–1.12)a |
| Lower (0 to 4988) | 1.08 (1.03–1.13)a | 1.07 (1.04–1.10)a | 1.11 (1.08–1.14)a |
| Access to commercial area | |||
| Closer (9387 to 36 979) | 1 | 1.03 (1.00–1.07)a | 1.11 (1.06–1.16)a |
| Medium (1221 to 2772) | 1.01 (0.98–1.04) | 1.08 (1.04–1.11)a | 1.10 (1.06–1.14)a |
| Farther (2774 to 75 083) | 1.09 (1.04–1.14)a | 1.06 (1.03–1.10)a | 1.08 (1.05–1.12)a |
| Neighborhood walkability | |||
| Higher (0.3 to 8.5) | 1 | 1.04 (1.00–1.07)a | 1.11 (1.06–1.16)a |
| Medium (−1.0 to 0.3) | 1.02 (0.99–1.06) | 1.07 (1.04–1.10)a | 1.09 (1.05–1.13)a |
| Lower (−27.8 to −1.0) | 1.08 (1.03–1.13)a | 1.08 (1.05–1.11)a | 1.09 (1.06–1.12)a |
CVD indicates cardiovascular disease; and SES, socioeconomic status.
P<0.05.
Discussion
We found SES‐related disparities in CVD mortality in Japan: Those living in lower SES areas were higher in CVD mortality than those in higher SES areas, which is consistent with evidence from Western countries.11, 12 Our findings add to such findings and extend them to the context of Japan, where the geographic disparities in mortality are increasing.2 We also identified another level of variability in CVD mortality within higher and medium SES municipalities, where CVD mortality was significantly greater in lower walkable municipalities. For lower SES areas, CVD mortality rates were higher, with no gradient according to walkability. The results observed for lower SES areas may be attributable to residents’ perception of walkability attributes. An Australian study reported that those with lower SES tend to consider their environments not so walkable even if they live in high walkable areas.31 A lack of concordance between objective and perceived walkable attributes may have implications for residents’ predispositions to walk or not to do so. Alternatively, lower SES areas may have relevant barriers to walking, not measured in the study. These may include environmental or sociocultural factors that act to discourage residents from walking or otherwise being physically active in their neighborhoods. There is also a possibility that food environments may differ between lower SES and higher SES municipalities32: Residents of lower SES higher walkability areas may have better access to nutritionally deficient foods (eg, fast food) than those of high SES higher walkability areas. Further research is needed to understand why higher walkability may not the beneficial for residents’ CVD mortality in lower SES municipalities.
Our findings suggest that the geographic distribution of CVD mortality may depend not only on social deprivation but also on built environmental attributes. We found that the difference in CVD mortality between lower and higher SES municipalities was 7%. The results shown in Table S1 indicate that the effect sizes for walkability attributes were modest and of similar magnitude for those of SES, within the higher SES municipalities. Although the effect sizes were smaller for medium SES municipalities and nonsignificant in lower SES municipalities, our findings suggest that the impact of walkability on CVD mortality may be comparable to that of SES in some localities. These findings will help identify areas where residents are at higher risk for developing CVD. Previous studies showed that residents of neighborhoods with lower SES are more likely to die from CVD, but our findings add that those living in areas higher in SES but lower in walkability are also at risk.
It was not possible to directly test whether the relationships observed could be attributable to differences in physical activity levels because municipality‐level data on physical activity were unavailable at the national scale. Physical activity is protective against CVD,33 and those living in higher SES areas tend to be more active during leisure time.34, 35 Although research has consistently shown associations of walkability and physical activity in Japan and several other countries,13, 20 it has been shown that the relationships between walkability and physical activity can differ between higher and lower SES areas. For instance, a recent study in Japan found that walking for exercise was associated with multiple walkability attributes in high SES areas but not in low SES areas.36 Similarly, an Australian study showed that frequent walking during leisure time was associated with a perceived environmental attribute (walking infrastructure) only in higher SES areas.37 Thus, it is possible that different levels of recreational physical activity between lower and higher walkability in higher SES areas may contribute to the heterogeneous distribution of CVD mortality in higher SES municipalities in this study. However, physical activity is one of many potential pathways that can link area characteristics (SES, walkability) and CVD. Further research is needed to examine behavioral and other mechanisms to better understand the geographic distributions of CVD.
Our study has limitations. Our design was cross‐sectional and ecological in nature, based on the most relevant available national‐level data aggregated at the level of municipalities. Thus, causal relationships between variables could not be determined. Because our study covered almost all municipalities in Japan, we were constrained to the use of a limited number of environmental attributes that were available at the national scale. Therefore, there may be other environmental attributes, such as availability of green spaces, access to public transport, motor traffic, and food environment, that may influence the relationships between SES and CVD mortality. We used municipalities as our spatial units, some of which are large and not homogeneous within their areas. Research using a smaller area unit is needed to replicate these findings. In addition, although the use of expected mortality rate has limitations, it has realistic utility in the context of our study. CVD mortality data from 2008 to 2012 were available for this study. Future studies using more recent CVD mortality data could investigate temporal relationships between SES/walkability variables and CVD mortality. Also, given the limited relevant data available at the national level, we could not control for other major potential confounders such as smoking rates or air pollution exposures. Furthermore, areas where people's daily activity takes place may not be aligned with the spatial boundaries of municipalities, which limits how accurately the actual environment to which residents were exposed could be characterized. Capturing accurate activity spaces is an ongoing challenge in the broader field of health and place.38 Although built environmental attributes such as population density and street layout are unlikely to substantially change in a short period of time, there was a temporal difference between our environmental attributes (2010–2011) and CVD mortality (2008–2012) data.
Building on and expanding the known disparities of CVD mortality by area‐level SES, we identified that urban design attributes further contribute to its geographic distribution. Confirming previous research, we found that lower SES areas have a higher risk of developing CVD. A novel finding of this study is that higher and medium SES municipalities can also be at risk if their walkability is low. Our findings may contribute to a better understanding of spatial distribution of disadvantage and health, identifying where additional resources and innovative prevention initiatives are needed to reduce CVD risk. Future research at a finer spatial scale can further improve the prediction of priority areas for CVD prevention.
Sources of Funding
Dr Nakaya was supported by a Japan Society for the Promotion of Sciences (KAKENHI Grant 20H00040). Dr Hanibuchi was supported by a Japan Society for the Promotion of Sciences (KAKENHI Grant 18KK0371 and 17H00947). Dr Owen is supported by a National Health and Medical Research Council of Australia (NHMRC) Centre of Research Excellence Grant (#1057608), NHMRC Senior Principal Research Fellowship (#1118225), and the Victorian Government’s Operational Infrastructure Support Program. Dr Oka was supported by the Ministry of Education, Culture, Sports, Science and Technology‐Supported Program for the Strategic Research Foundation at Private Universities 2015–2019 the Japan Ministry of Education, Culture, Sports, Science and Technology (S1511017).
Disclosures
None.
Supporting information
Table S1 Figure S1
(J Am Heart Assoc. 2020;9:e016152 DOI: 10.1161/JAHA.119.016152.)
For Sources of Funding and Disclosures, see page 7.
References
- 1. Lüscher TF. Prevention: some important steps forward, but many unmet needs in a world with cardiovascular disease as the leading cause of death. Eur Heart J. 2016;37:3179–3181. [DOI] [PubMed] [Google Scholar]
- 2. Nomura S, Sakamoto H, Glenn S, Tsugawa Y, Abe SK, Rahman MM, Brown JC, Ezoe S, Fitzmaurice C, Inokuchi T. Population health and regional variations of disease burden in Japan, 1990–2015: a systematic subnational analysis for the Global Burden of Disease Study 2015. Lancet. 2017;390:1521–1538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mensah GA, Goff DC, Gibbons GH. Cardiovascular mortality differences—place matters. JAMA. 2017;317:1955–1957. [DOI] [PubMed] [Google Scholar]
- 4. Okwuosa IS, Lewsey SC, Adesiyun T, Blumenthal RS, Yancy CW. Worldwide disparities in cardiovascular disease: challenges and solutions. Int J Cardiol. 2016;202:433–440. [DOI] [PubMed] [Google Scholar]
- 5. Casper M, Kramer MR, Quick H, Schieb LJ, Vaughan AS, Greer S. Changes in the geographic patterns of heart disease mortality in the United States: 1973 to 2010. Circulation. 2016;133:1171–1180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Barr DA. Geography as disparity: the shifting burden of heart disease. Circulation. 2016;133:1151–1154. [DOI] [PubMed] [Google Scholar]
- 7. Schultz WM, Kelli HM, Lisko JC, Varghese T, Shen J, Sandesara P, Quyyumi AA, Taylor HA, Gulati M, Harold JG. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. 2018;137:2166–2178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Marmot M, Friel S, Bell R, Houweling TAJ, Taylor S. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372:1661–1669. [DOI] [PubMed] [Google Scholar]
- 9. Petrovic D, de Mestral C, Bochud M, Bartley M, Kivimäki M, Vineis P, Mackenbach J, Stringhini S. The contribution of health behaviors to socioeconomic inequalities in health: a systematic review. Prev Med. 2018;113:15–31. [DOI] [PubMed] [Google Scholar]
- 10. Nakaya T, Yuri I. The Atlas of Health Inequalities in Japan. Springer:Cham, Switzerland; 2020. [Google Scholar]
- 11. Ramsay S, Morris R, Whincup P, Subramanian S, Papacosta A, Lennon LT, Wannamethee S. The influence of neighbourhood‐level socioeconomic deprivation on cardiovascular disease mortality in older age: longitudinal multilevel analyses from a cohort of older British men. J Epidemiol Community Health. 2015;69:1224–1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Major JM, Doubeni CA, Freedman ND, Park Y, Lian M, Hollenbeck AR, Schatzkin A, Graubard BI, Sinha R. Neighborhood socioeconomic deprivation and mortality: NIH‐AARP diet and health study. PLoS One. 2010;5:e15538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Sallis JF, Cerin E, Conway TL, Adams MA, Frank LD, Pratt M, Salvo D, Schipperijn J, Smith G, Cain KL. Physical activity in relation to urban environments in 14 cities worldwide: a cross‐sectional study. Lancet. 2016;387:2207–2217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sugiyama T, Neuhaus M, Cole R, Giles‐Corti B, Owen N. Destination and route attributes associated with adults’ walking: a review. Med Sci Sports Exerc. 2012;44:1275–1286. [DOI] [PubMed] [Google Scholar]
- 15. Mackenbach JD, Rutter H, Compernolle S, Glonti K, Oppert J‐M, Charreire H, De Bourdeaudhuij I, Brug J, Nijpels G, Lakerveld J. Obesogenic environments: a systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health. 2014;14:233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Den Braver N, Lakerveld J, Rutters F, Schoonmade L, Brug J, Beulens J. Built environmental characteristics and diabetes: a systematic review and meta‐analysis. BMC Med. 2018;16:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Chandrabose M, Rachele J, Gunn L, Kavanagh A, Owen N, Turrell G, Giles‐Corti B, Sugiyama T. Built environment and cardio‐metabolic health: systematic review and meta‐analysis of longitudinal studies. Obes Rev. 2019;20:41–54. [DOI] [PubMed] [Google Scholar]
- 18. King KE, Clarke PJ. A disadvantaged advantage in walkability: findings from socioeconomic and geographical analysis of national built environment data in the United States. Am J Epidemiol. 2014;181:17–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Owen N, Sugiyama T, Koohsari MJ, De Bourdeaudhuij I, Hadgraft N, Oyeyemi A, Aguinaga‐Ontoso I, Mitáš J, Troelsen J, Davey R. Associations of neighborhood environmental attributes with adults’ objectively‐assessed sedentary time: IPEN adult multi‐country study. Prev Med. 2018;115:126–133. [DOI] [PubMed] [Google Scholar]
- 20. Hanibuchi T, Nakaya T, Yonejima M, Honjo K. Perceived and objective measures of neighborhood walkability and physical activity among adults in Japan: a multilevel analysis of a nationally representative sample. Int J Environ Res Public Health. 2015;12:13350–13364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ministry of Health LaW . The specified report of vital statistics, health centre district and municipality vital statistics from 2008 to 2012. 2012.
- 22. Statistics Bureau of Japan . Population census. 2015.
- 23. Dorling D, Rigby J, Wheeler B, Ballas D, Thomas B, Fahmy E, Gordon D, Lupton R. Poverty, Wealth and Place in Britain, 1968 to 2005. The Policy Press: Bristol, UK; 2007. [Google Scholar]
- 24. Pornet C, Delpierre C, Dejardin O, Grosclaude P, Launay L, Guittet L, Lang T, Launoy G. Construction of an adaptable European transnational ecological deprivation index: the French version. J Epidemiol Community Health. 2012;66:982–989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Nakaya T, Honjo K, Hanibuchi T, Ikeda A, Iso H, Inoue M, Sawada N, Tsugane S; JPHC Study Group . Associations of all‐cause mortality with census‐based neighbourhood deprivation and population density in Japan: a multilevel survival analysis. PLoS One. 2014;9:e97802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Kärmeniemi M, Lankila T, Ikäheimo T, Koivumaa‐Honkanen H, Korpelainen R. The built environment as a determinant of physical activity: a systematic review of longitudinal studies and natural experiments. Ann Behav Med. 2018;52:239–251. [DOI] [PubMed] [Google Scholar]
- 27. Koohsari MJ, Owen N, Cole R, Mavoa S, Oka K, Hanibuchi T, Sugiyama T. Built environmental factors and adults’ travel behaviors: role of street layout and local destinations. Prev Med. 2017;96:124–128. [DOI] [PubMed] [Google Scholar]
- 28. National Spatial Planning and Regional Policy Bureau . The National Land Numerical Information. 2010.
- 29. Akiyama Y, Sengoku H, Shibasaki R. Development of commercial accumulation statistics throughout Japan and utilization environment of them. Theor Appl GIS. 2013;21:97–106. (In Japanese). [Google Scholar]
- 30. Mavoa S, Boulangé C, Eagleson S, Stewart J, Badland HM, Giles‐Corti B, Gunn L. Identifying appropriate land‐use mix measures for use in a national walkability index. J Transp Land Use. 2018;11:681–700. [Google Scholar]
- 31. Gebel K, Bauman A, Owen N. Correlates of non‐concordance between perceived and objective measures of walkability. Ann Behav Med. 2009;37:228–238. [DOI] [PubMed] [Google Scholar]
- 32. Fleischhacker SE, Evenson KR, Rodriguez DA, Ammerman AS. A systematic review of fast food access studies. Obes Rev. 2011;12:e460–e471. [DOI] [PubMed] [Google Scholar]
- 33. Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, Casanova A, Swaminathan S, Anjana RM, Kumar R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high‐income, middle‐income, and low‐income countries: the PURE study. Lancet. 2017;390:2643–2654. [DOI] [PubMed] [Google Scholar]
- 34. Cleland V, Ball K, Crawford D. Socioeconomic position and physical activity among women in Melbourne, Australia: does the use of different socioeconomic indicators matter? Soc Sci Med. 2012;74:1578–1583. [DOI] [PubMed] [Google Scholar]
- 35. Turrell G, Haynes M, Burton NW, Giles‐Corti B, Oldenburg B, Wilson L‐A, Giskes K, Brown WJ. Neighborhood disadvantage and physical activity: baseline results from the HABITAT multilevel longitudinal study. Ann Epidemiol. 2010;20:171–181. [DOI] [PubMed] [Google Scholar]
- 36. Koohsari MJ, Hanibuchi T, Nakaya T, Shibata A, Ishii K, Liao Y, Oka K, Sugiyama T. Associations of neighborhood environmental attributes with walking in Japan: moderating effects of area‐level socioeconomic status. J Urban Health. 2017;94:847–854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Sugiyama T, Howard NJ, Paquet C, Coffee NT, Taylor AW, Daniel M. Do relationships between environmental attributes and recreational walking vary according to area‐level socioeconomic status? J Urban Health. 2015;92:253–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Smith L, Foley L, Panter J. Activity spaces in studies of the environment and physical activity: a review and synthesis of implications for causality. Health Place. 2019;58:102113. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Figure S1