

Supplemental Digital Content is available in the text.
Keywords: comorbidities, coronavirus disease, demography, mortality, severe acute respiratory syndrome
Abstract
Background and Purpose:
No studies have reported the effect of the coronavirus disease 2019 (COVID-19) epidemic on patients with preexisting stroke. We aim to study the clinical course of COVID-19 patients with preexisting stroke and to investigate death-related risk factors.
Methods:
We consecutively included 651 adult inpatients with COVID-19 from the Central Hospital of Wuhan between January 2 and February 15, 2020. Data on the demography, comorbidities, clinical manifestations, laboratory findings, treatments, complications, and outcomes (ie, discharged or death) of the participants were extracted from electronic medical records and compared between patients with and without preexisting stroke. The association between risk factors and mortality was estimated using a Cox proportional hazards regression model for stroke patients infected with severe acute respiratory syndrome coronavirus 2.
Results:
Of the 651 patients with COVID-19, 49 with preexisting stroke tended to be elderly, male, had more underlying comorbidities and greater severity of illness, prolonged length of hospital stay, and greater hospitalization expenses than those without preexisting stroke. Cox regression analysis indicated that the patients with stroke had a higher risk of developing critical pneumonia (adjusted hazard ratio, 2.01 [95% CI, 1.27–3.16]) and subsequent mortality (adjusted hazard ratio, 1.73 [95% CI, 1.00–2.98]) than the patients without stroke. Among the 49 stroke patients, older age and higher score of Glasgow Coma Scale or Sequential Organ Failure Assessment were independent risk factors associated with in-hospital mortality.
Conclusions:
Preexisting stroke patients infected with severe acute respiratory syndrome coronavirus 2 were readily predisposed to death, providing an important message to individuals and health care workers that preventive measures must be implemented to protect and reduce transmission in stroke patients in this COVID-19 crisis.
Coronavirus disease 2019 (COVID-19) is an emerging infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and has become a worldwide pandemic. The COVID-19 pandemic is a global health emergency that has changed the world in an unprecedented way.
Recent studies have reported that COVID-19 patients with older age and underlying comorbidities have poor outcomes.1–3 In Wang’s study of 138 cases, 5.1% (n=7) patients had cerebrovascular diseases.1 In Guan’s study of 1590 cases, 1.9% (n=30) patients reported having cerebrovascular disease and severe cases were more likely to have it (50.0% versus 15.3%) compared with nonsevere cases.4 Stroke is the main clinical type of cerebrovascular disease. Stroke and ischemic heart disease have been the leading causes of death and disability-adjusted life-years at the national level in China in recent years.5 These data show that intensive attention should be paid to this special group with stroke in case of rapid deterioration. However, few studies have reported the clinical manifestations and disease progression of stroke patients infected with SARS-CoV-2.
In this study, we aim to analyze the data of all patients with COVID-19 admitted to the Central Hospital of Wuhan during the epidemic (1) to compare the clinical characteristics, laboratory findings, and outcomes between patients with and without stroke and (2) to investigate the clinical course and death-related risk factors for patients with stroke.
Methods
Data Disclosure Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Please contact the corresponding authors (Drs Yu and Chen).
Study Design and Participants
This single-center case series was conducted at the Central Hospital of Wuhan. All the 709 patients with SARS-CoV-2 infection admitted to the hospital were consecutively enrolled between January 2 and February 15, 2020. COVID-19 was diagnosed according to the interim guidance from the World Health Organization.6 The definite clinical outcomes (ie, discharged or death during hospitalization) were observed up to April 2, 2020, and 7 patients without clinical end point were excluded. We also excluded 2 pregnant women, 39 patients with COVID-19 who transferred to other hospitals, 1 patient with acute head trauma, and 9 patients with missing medical information. Finally, 651 patients with COVID-19 were included in this study (Figure I in the Data Supplement). The study was approved by the Ethics Committees of the Central Hospital of Wuhan. Written informed consent was waived by the institutional review board for the emerging infectious disease.
Data Collection
The demographic characteristics, comorbidities, clinical manifestations, laboratory findings, treatments, complications, and outcomes were extracted from electronic medical records by 3 first-line clinical physicians (Drs Sun, Liu, and Zhang). Then, a fourth researcher (Dr Chen) independently reviewed and checked the data. Considering that some stroke patients presented with various forms of disorder of consciousness on admission, we obtained data on their medical histories and preadmission information by accessing medical records from previous hospital visits and contacting with their close relatives.
Sequential Organ Failure Assessment (SOFA) scores were determined within 24 hours after admission. Glasgow Coma Scale (GCS), modified Rankin Scale, and Activity of Daily Living Scale scores were determined on admission for patients who had a preexisting stroke. Onset date was defined as the date on which symptoms appear. The time from first symptom to hospital admission, hospital stays, and clinical outcomes were recorded. SARS-CoV-2 in respiratory specimens was repeatedly detected by real-time RT-PCR as previously described.1
Disease Definition and Outcomes
An updated definition of stroke is an acute episode of focal dysfunction of the brain, retina, or spinal cord lasting longer than 24 hours, or of any duration if imaging (computed tomography or magnetic resonance imaging) or autopsy show focal infarction or hemorrhage relevant to the symptoms.7 The definition includes subarachnoid hemorrhage, which can be broadly classified into ischemic stroke and hemorrhagic stroke. Sepsis and septic shock were defined according to the 2016 Third International Consensus Definition for Sepsis and Septic Shock.8 Acute respiratory distress syndrome (ARDS) was defined according to the Berlin definition.9 Acute kidney injury was diagnosed in accordance with Kidney Disease Improving Global Guidelines.10 The illness severity and discharge criteria of COVID-19 were defined in accordance with the Chinese management guideline for COVID-19 (version 7.0).11 The primary outcome was all-cause mortality of stroke patients infected with SARS-CoV-2 during hospitalization, and the secondary outcome was the incidence of critical pneumonia.
Statistical Analysis
All continuous variables were presented as median (interquartile range) and compared by using the Mann-Whitney U test, while categorical variables were presented as n (%) and compared using the χ2 test or Fisher exact test. Kaplan-Meier methods were used for survival curve plotting and examined by log-rank or Mantel-Haenszel test. We performed Cox proportional hazards regression to estimate associations of stroke with the risk of developing critical pneumonia and subsequent mortality. The time to events is denoted as the time from admission to critical pneumonia/death or discharge. We further investigated several potential death-related risk factors among 49 stroke patients by using univariate and multivariate Cox regression. Previous studies reported older age and high SOFA score as risk factors for mortality in patients with COVID-19.12 Considering that the limited number of stroke patients (n=49) in our study might result in overfitting in the model and that most laboratory findings might be unavailable in emergency circumstances, we chose age, sex, and severity of illness scores (SOFA or GCS, modified Rankin Scale, and Activity of Daily Living Scale) in our multivariate Cox regression model. All analyses were performed using R software (The R Foundation, http://www.r-project.org, version 3.6.1). A 2-sided significance level of 0.05 was used to evaluate statistical significance.
Results
Clinical Features, Laboratory Findings, and Mortality
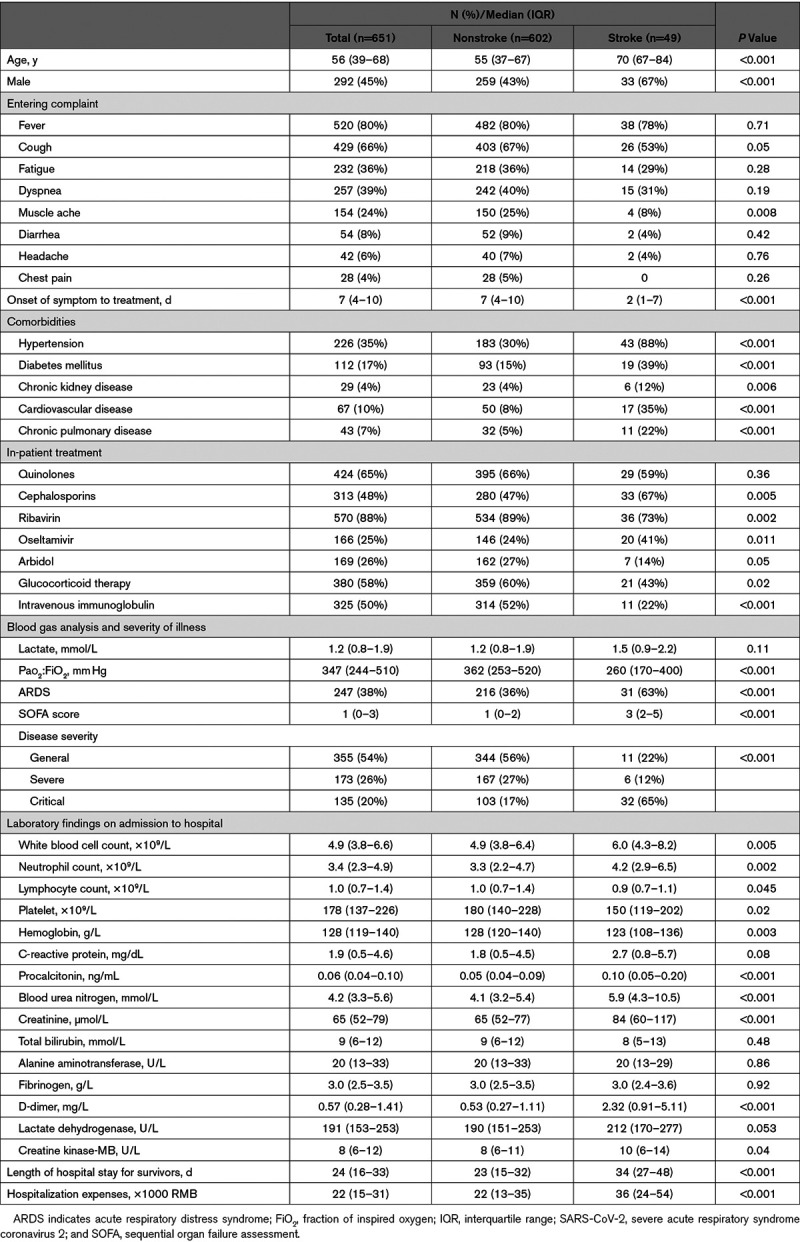
Among 651 hospitalized patients with COVID-19 (Table 1), 602 (92%) reported having nonstroke while 49 (8%) having stroke. The median age was 56 years, and 292 (45%) patients were male. Compared with patients without stroke, the patients with stroke were elderly (70 versus 55 years, P<0.001) and more likely to be male. The appearance of first symptoms included fever (n=520 [80%]), cough (n=429 [66%]), fatigue (n=232 [36%]), and dyspnea (n=257 [39%]) and did not differ significantly between the patients with and without stroke. Compared with the patients without stroke, the patients with stroke were more likely to have underlying comorbidities, including hypertension, diabetes mellitus, cardiovascular, chronic pulmonary disease, and chronic kidney disease. Most patients were empirically treated with antibiotics and antiviral therapy. Glucocorticoid (58%) and intravenous immunoglobulin (50%) were empirically used for anti-inflammatory treatment. The patients with stroke had higher SOFA scores and more easily developed ARDS and critical pneumonia than the patients without stroke. In terms of laboratory findings at admission, the patients with stroke showed significantly higher counts of white blood cells and neutrophils and levels of procalcitonin, blood urea nitrogen, creatinine, D-dimer, and creatine kinase-MB but significantly lower counts of lymphocytes, platelets, and hemoglobin than the patients without stroke. The length of hospital stay and the hospitalization expenses in the stroke patients were much higher than those in the patients without stroke.
Table 1.
Clinical Features and Laboratory Findings of Patients Infected With SARS-CoV-2 With or Without Stroke
The mortality was higher among the patients with stroke than among the patients without stroke (22 [45%] versus 57 [9%]; P<0.001), as shown in the Kaplan-Meier survival curves in Figure 1A and 1B. In multivariable Cox regression models, the patients with stroke had a higher risk of critical pneumonia (adjusted hazard ratio, 2.01 [95% CI, 1.27–3.16]) and subsequent mortality (adjusted hazard ratio, 1.73 [95% CI, 1.00–2.98]) compared with the patients without stroke after adjusted for age, sex, and comorbidities (Figure 1C).
Figure 1.
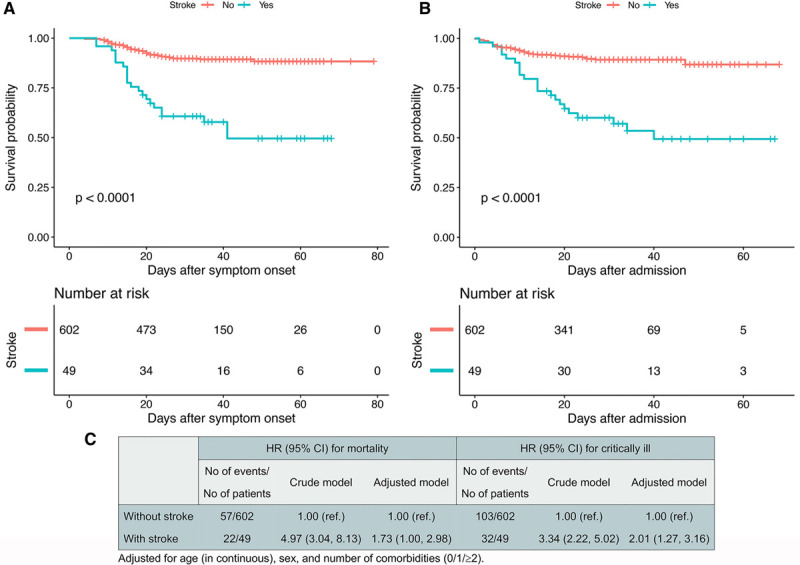
Mortality during hospitalization between patients with vs without preexisting stroke. A and B, Kaplan-Meier survival curves for mortality during the time from symptom onset (A) and admission (B). C, Patients with preexisting stroke had a higher risk of critical pneumonia and subsequent mortality.
Clinical Course and Death-Related Risk Factors in Stroke Patients
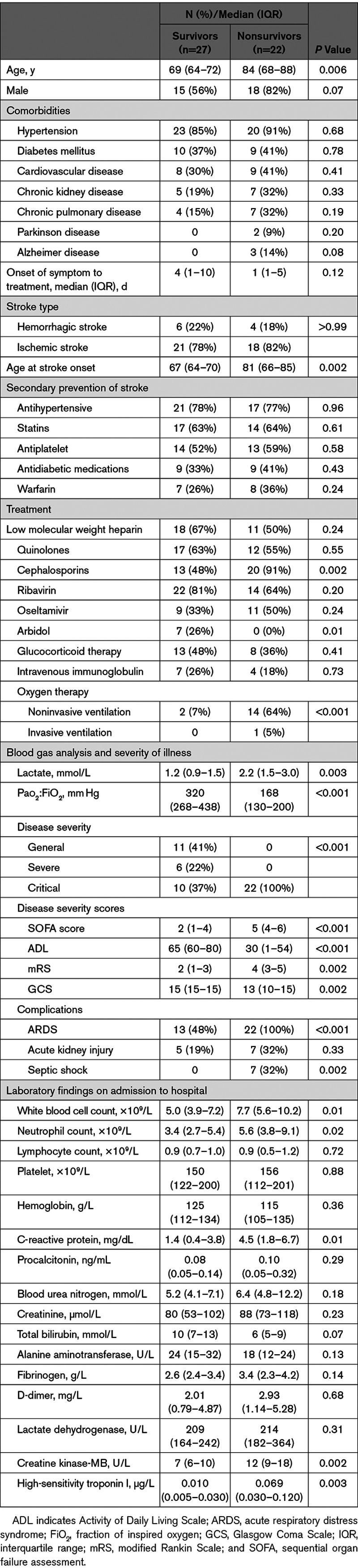
As presented in Table 2, compared with the survivors, the nonsurvivors were older (median age 84 versus 69 years, P<0.05). Ischemic stroke was the main stroke type. No significantly differences were found in the use of secondary prevention medications and low molecular weight heparin between the survival and nonsurvival groups. Meanwhile, increased proportion of noninvasive and invasive ventilation was observed in the nonsurviving group compared with the surviving group. The disease severity evaluation and laboratory examination were analyzed. Compared with the survival group, the nonsurvival group had 22 (100%) critical cases and significantly worse disease severity scores on the day of hospital admission (all P <0.05 for SOFA, Activity of Daily Living Scale, modified Rankin Scale, and GCS). The nonsurvivors had significantly higher white blood cell, neutrophil count, and levels of C-reactive protein, creatine kinase-MB, lactate, and high-sensitivity troponin I compared with the survivors (Table 2). Acute kidney injury, septic shock, and ARDS were the most frequently observed complications. The frequencies of sepsis shock and ARDS complications were significantly higher in the nonsurvivors than the survivors.
Table 2.
Comparison of Clinical Characteristics Between Survivors and Nonsurvivors With Stroke
Looking at the whole clinical course of 49 patients with stroke, the median duration of symptoms was 21 days for the survivors, whereas the flu-like symptoms persisted until death for the nonsurvivors (Figure 2). For the survivors, the median duration of viral shedding was 27 days, and the longest observed duration among the survivors was 46 days while the virus was continuously detectable until death in the nonsurvivors. ARDS developed at a median of 10 days after illness onset among the survivors, whereas a median of 3 days in the nonsurvivors followed by acute kidney injury (7 days) and shock (14 days).
Figure 2.
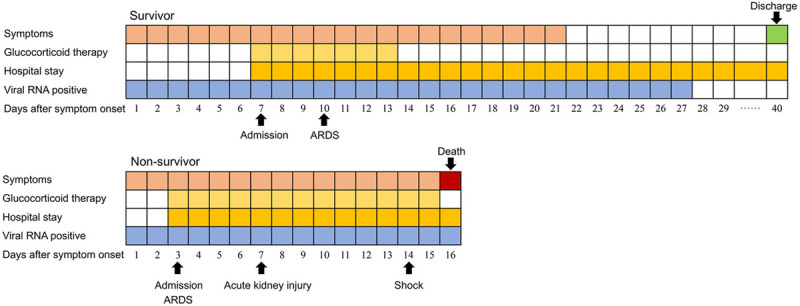
Clinical courses of symptoms and outcomes and viral shedding from symptom onset and in stroke patients hospitalized with coronavirus disease 2019 (COVID-19). The Figure shows median duration of symptoms, hospital stay, viral shedding from symptom onset, glucocorticoid therapy, onset of complications and outcomes.
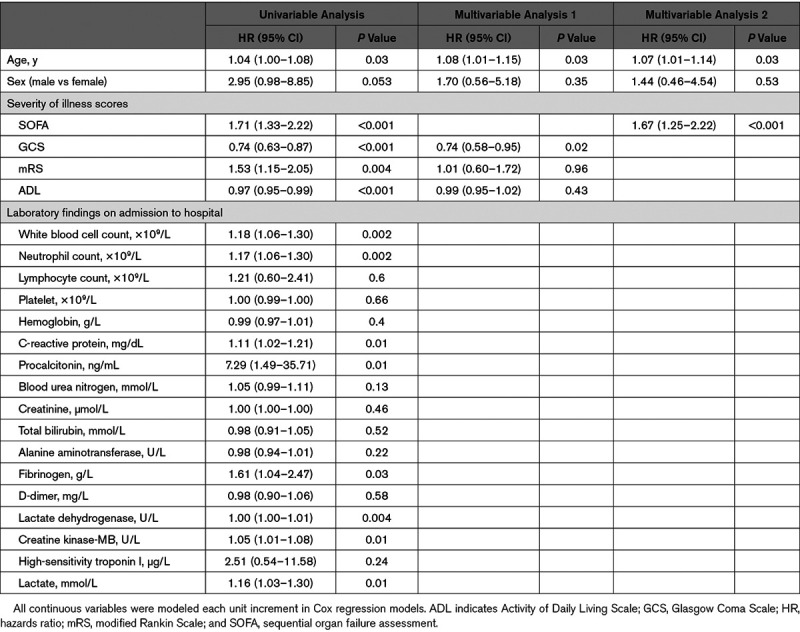
Univariate Cox regression analyses identified several death-related risk factors, including age, severity of illness scores, white blood cell count, neutrophil count, and levels of C-reactive protein, procalcitonin, fibrinogen, lactate dehydrogenase, creatine kinase-MB, and lactate. Considering that most laboratory findings might be unavailable in emergency circumstances, we chose age, sex, and severity of illness scores (SOFA or GCS, modified Rankin Scale, Activity of Daily Living Scale) for multivariate Cox regression analysis. We found older age and lower score of GCS or SOFA as independent risk factors for fatal outcomes (Table 3).
Table 3.
Cox Regression Analysis of Death-Related Risk Factors in Stroke Patients
Discussion
To our knowledge, no previous studies have investigated the relationship between preexisting stroke and disease progression among patients hospitalized with SARS-CoV-2. In the present study, we identified the differences in the clinical characteristics and laboratory findings between COVID-19 patients with and without preexisting stroke. Second, the clinical courses, outcomes, and death-related risk factors were investigated in the stroke patients. Our findings highlight that strong personal protection provisions are important for patients with stroke and that intensive surveillance or treatment should be considered when they are infected with SARS-CoV-2.
The present work found that the stroke patients with SARS-CoV-2 infection was associated with higher risk of critical pneumonia and mortality compared with patients without stroke. Several potential explanations for poor outcomes are considered. Stroke patients were always older and had more comorbidities, which might be related to weak immune functions and poor organ function and lead to increased mortality. However, we found that the association between stroke and adverse outcome was independent of age, sex, and comorbidities in the Cox regression model which suggested that there were other factors increasing the mortality except for the currently widely recognized age and comorbidities. Previous studies have reported infection is a frequent poststroke complication and contributes to a poor functional stroke outcome.13 The immunosuppression after stroke has been linked to increased risk of infection.14 Systemic inflammatory reaction and systemic disturbances were more severe in stroke patients after infection. The present study found that the stroke patients had abnormal laboratory markers on admission, including elevated levels of white blood cell, neutrophil, C-reactive protein, procalcitonin, D-dimer, blood urea nitrogen, creatinine, and creatine kinase-MB and decreased levels of lymphocyte and platelet count compared with the patients without stroke. This result suggests that cytokine cascade, excessive inflammatory reaction, coagulation dysfunction, and organ injury might aggravate the stroke patient’s prognosis owing to SARS-CoV-2 infection. Additionally, in a recent study of 214 patients with COVID-19, 78 (36.4%) had various neurological manifestations that involved central nervous system, peripheral nervous system, and skeletal muscles,15 suggesting possible neurological injury from SARS-CoV-2. It appears to be an interplay of systemic disturbances and local neurological injury that cause a double hit for patients with preexisting stroke and lead to a poor outcome. In our study of 49 stroke cases infected with SARS-CoV-2, the overall mortality rate was 45%, which was much higher than the nationwide stroke mortality rate (114.8 per 100 000 person-years) and COVID-19 mortality rate (2.3%) in China.16,17 In addition, the patients with stroke had a 65% proportion of critical, which is higher than the average 5% critical rate of COVID-19 cases in mainland China,17 which can explain the longer length of hospital stay and higher hospitalization expenses in the patients with stroke than the patients without stroke.
The SARS-CoV-2 epidemic spreads rapidly by human-to-human transmission during the early phase of SARS-CoV-2 outbreaks,18 which exacerbated the shortage of medical resources, including staff and intensive care unit beds. Thus far, no approved preventative vaccines or approved therapies are available for COVID-19, although several are being actively studied.19 Importantly, we observed the median duration of viral shedding was 27 days among the survivors while the virus was continuously detectable until death in the nonsurvivors. In a prior report on the clinical course of 191 patients hospitalized for SARS-CoV-2, the median duration of viral shedding was 20 days (range: 8–37 days) for survivors.12 Notably, we found the duration of viral shedding in patients with stroke was apparently longer, and the longest duration was 46 days. This observation indicated that stroke patient with SARS-CoV-2 infection may harbor the virus for an extended period and require longer time for clinical care and treatment. Our findings highlight the importance of strict sterilization, isolation, and medical care to reduce infection risk for patients with stroke. Similarly, we can detect and treat COVID-19 early by SARS-CoV-2 nucleic acid detection and chest computed tomography, especially for those who had speech disorders.
Another important finding of our study was that older age and higher SOFA score were independent risk factors for the in-hospital mortality of patients with stroke infected with SARS-CoV-2, similar to a previous report that the odds of death due to COVID-19 increases with age, SOFA, and high D-dimer levels on admission.12 Older patients usually have higher incidence and longer duration of comorbidities and poor compensatory organ function, which might explain the higher mortality among elderly than among younger patients. SOFA score is a good diagnostic marker used to quantify the degree of organ dysfunction on admission in sepsis and septic shock patients.20 In the current study, we found that sepsis shock was common and occurred in 32% of nonsurviving patients with stroke. The GCS was a part of SOFA score and has remained the gold standard for assessment of impaired consciousness in all patient populations, especially for patients with stroke. Our study also indicated that age and GCS score were the risk factors for predicting inhospital mortality and enabled rapid risk stratification for patients with stroke infected with SARS-CoV-2 in the setting of a tertiary care hospital in low-middle income countries where the most of laboratory findings might not be available during the emergency. Patients who had high GCS score can be followed by further assessment of SOFA score after admitting to a relevant specialty or intensive care unit for treatment.
Although we did not find that D-dimer was a risk factor for in-hospital mortality, stroke patients always had high D-dimer levels than patients without stroke at admission. Elevated plasma D-dimer levels indicated enhanced fibrinolytic activity, which signifies that the body’s system is in a hypercoagulable state. Previous studies have confirmed that elevated plasma D-dimer levels can predict early neurological deterioration21 and that D-dimer levels are associated with reocclusion.22 Therefore, the high D-dimer levels in the patients with stroke may be related to the risk of reocclusion or secondary acute stroke. These findings suggest the importance of dynamic detection of D-dimer levels and implementation of corresponding preventive measures. A recent study showed that anticoagulant therapy mainly with low molecular weight heparin appears to be associated with better prognosis in severe COVID-19 patients meeting sepsis-induced coagulopathy criteria or with markedly elevated D-dimer.23 Moreover, anticoagulant therapy is especially important for preexisting stroke patients to prevent recurrent stroke.
The study has several limitations. First, some critically ill patients who need to receive invasive mechanical ventilation or extracorporeal membrane oxygenation were transferred to other hospitals due to the requirement for effective integration of medical resources during the early phase of outbreak. This situation might affect our research result. However, the proportion of these patients was not high. Second, we cannot exclude the residual confounding and potential bias due to the observational nature of the present study. Third, despite the significant results observed, the sample size of patients with stroke in the present study was limited. Further studies are warranted to provide more evidence on clinical course, risk factors, and therapeutic efficacy of stroke patients infected with SARS-CoV-2.
Conclusions
In summary, patients with stroke infected with SARS-CoV-2 had a higher risk for critically ill and mortality, harbored the virus for an extended period, and required longer time for clinical care and treatment. Vigorous efforts should be exerted to protect and reduce transmission in patients with stroke.
Sources of Funding
This study was supported by the Health and Family Planning Commission of Wuhan Municipality, grant number WX18A02.
Disclosures
None.
Supplemental Materials
Figure I
Supplementary Material
{kind=link}
Footnotes
Nonstandard Abbreviations and Acronyms
- ARDS
- acute respiratory distress syndrome
- COVID-19
- coronavirus disease 2019
- FiO2
- fraction of inspired oxygen
- GCS
- Glasgow Coma Scale
- SARS-CoV-2
- severe acute respiratory syndrome coronavirus 2
- SOFA
- Sequential Organ Failure Assessment
Drs Zhang, Sun, Yujun Wang, and Xiaopin Wang contributed equally.
For Sources of Funding and Disclosures, see page 2682.
The Data Supplement is available with this article at https://www.ahajournals.org/doi/suppl/10.1161/STROKEAHA.120.030642.
References
- 1.Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 20203231061–1069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, Wu Y, Zhang L, Yu Z, Fang M, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 20208475–481doi: 10.1016/S2213-2600(20)30079-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 20203231775–1776 [DOI] [PubMed] [Google Scholar]
- 4.Guan WJ, Liang WH, Zhao Y, Liang HR, Chen ZS, Li YM, Liu XQ, Chen RC, Tang CL, Wang T, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. 2020;55:2000547. doi: 10.1183/13993003.00547-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, Li X, Wang L, Wang L, Liu Y, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 20193941145–1158doi: 10.1016/S0140-6736(19)30427-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World; Health Organization. Clinical Management of COVID-19. Https://www.Who.Int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. Accessed May 27, 2020. [PubMed]
- 7.Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJ, Culebras A, Elkind MS, George MG, Hamdan AD, Higashida RT, et al. ; American Heart Association Stroke Council, Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Peripheral Vascular Disease; Council on Nutrition, Physical Activity and Metabolism An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013442064–2089doi: 10.1161/STR.0b013e318296aeca [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, Deutschman CS, Angus DC, Rubenfeld GD, Singer M; Sepsis Definitions Task Force Developing a new definition and assessing new clinical criteria for septic shock: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016315775–787doi: 10.1001/jama.2016.0289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS; ARDS Definition Task Force Acute respiratory distress syndrome: the Berlin definition. JAMA 20123072526–2533doi: 10.1001/jama.2012.5669 [DOI] [PubMed] [Google Scholar]
- 10.Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012120c179–c184doi: 10.1159/000339789 [DOI] [PubMed] [Google Scholar]
- 11.National Health Commission & National Administration of Traditional Chinese Medicine Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin Med J (Engl) 20201331087–1095doi: 10.1097/CM9.0000000000000819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 20203951054–1062doi: 10.1016/S0140-6736(20)30566-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Heikinheimo T, Broman J, Haapaniemi E, Kaste M, Tatlisumak T, Putaala J. Preceding and poststroke infections in young adults with first-ever ischemic stroke: effect on short-term and long-term outcomes. Stroke 2013443331–3337doi: 10.1161/STROKEAHA.113.002108 [DOI] [PubMed] [Google Scholar]
- 14.Dirnagl U, Klehmet J, Braun JS, Harms H, Meisel C, Ziemssen T, Prass K, Meisel A. Stroke-induced immunodepression: experimental evidence and clinical relevance. Stroke 2007382 suppl770–773doi: 10.1161/01.STR.0000251441.89665.bc [DOI] [PubMed] [Google Scholar]
- 15.Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, Chang J, Hong C, Zhou Y, Wang D, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol 202077683–690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, Wang L, Jiang Y, Li Y, Wang Y, et al. ; NESS-China Investigators Prevalence, incidence, and mortality of stroke in China: results from a Nationwide Population-Based Survey of 480 687 adults. Circulation 2017135759–771doi: 10.1161/CIRCULATIONAHA.116.025250 [DOI] [PubMed] [Google Scholar]
- 17.Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 20203231239–1242 [DOI] [PubMed] [Google Scholar]
- 18.Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, Ren R, Leung KSM, Lau EHY, Wong JY, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med 20203821199–1207doi: 10.1056/NEJMoa2001316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chen WH, Strych U, Hotez PJ, Bottazzi ME. The SARS-CoV-2 vaccine pipeline: an overview. Curr Trop Med Rep 2020761–64 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016315801–810doi: 10.1001/jama.2016.0287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Barber M, Langhorne P, Rumley A, Lowe GD, Stott DJ. D-dimer predicts early clinical progression in ischemic stroke: confirmation using routine clinical assays. Stroke 2006371113–1115doi: 10.1161/01.STR.0000209240.63821.1a [DOI] [PubMed] [Google Scholar]
- 22.Li W, Ding J, Sui X, Qi Z, Wu L, Sun C, Ji K, Ma Q, Ji X, Liu KJ. Prognosis and risk factors for reocclusion after mechanical thrombectomy. Ann Clin Transl Neurol 20207420–428doi: 10.1002/acn3.50999 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost 2020181094–1099doi: 10.1111/jth.14817 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.