

Abstract
Background
Attention-deficit/hyperactivity disorder (ADHD) comorbid with sleep disturbances can produce profound disruption in daily life and negatively impact quality of life of both the child and the family. However, the temporal relationship between ADHD and sleep impairment is unclear, as are underlying common brain mechanisms.
Methods
This study used data from the Quebec Longitudinal Study of Child Development (n = 1601, 52% female) and the Adolescent Brain Cognitive Development Study (n = 3515, 48% female). Longitudinal relationships between symptoms were examined using cross-lagged panel models. Gray matter volume neural correlates were identified using linear regression. The transcriptomic signature of the identified brain-ADHD-sleep relationship was characterized by gene enrichment analysis. Confounding factors, such as stimulant drugs for ADHD and socioeconomic status, were controlled for.
Results
ADHD symptoms contributed to sleep disturbances at one or more subsequent time points in both cohorts. Lower gray matter volumes in the middle frontal gyrus and inferior frontal gyrus, amygdala, striatum, and insula were associated with both ADHD symptoms and sleep disturbances. ADHD symptoms significantly mediated the link between these structural brain abnormalities and sleep dysregulation, and genes were differentially expressed in the implicated brain regions, including those involved in neurotransmission and circadian entrainment.
Conclusions
This study indicates that ADHD symptoms and sleep disturbances have common neural correlates, including structural changes of the ventral attention system and frontostriatal circuitry. Leveraging data from large datasets, these results offer new mechanistic insights into this clinically important relationship between ADHD and sleep impairment, with potential implications for neurobiological models and future therapeutic directions.
Keywords: ADHD, Development, Dyssomnia, Longitudinal study, Neurodevelopmental, Parasomnia
Attention-deficit/hyperactivity disorder (ADHD) is the most prevalent neurodevelopmental disorder in children and persists into adulthood in 50% to 66% of cases (1, 2, 3). Sleep disturbances, composed of two main classifications (i.e., dyssomnia and parasomnia) (4), are extremely common, occurring in 25% to 55% of children with ADHD (5), and are associated with poor outcomes (6, 7, 8). Left untreated, such symptoms lead to untoward functional consequences in young people, including worse academic outcomes (9, 10, 11). Both ADHD symptoms and sleep problems can produce profound disruption in daily life and impact negatively quality of life of both the child and the family (12, 13, 14). ADHD symptoms such as hyperactivity can lead to longer sleep onset latency, more night awakening, and lower sleep quality (15), but disrupted sleep can also impair daytime attention, overlapping with the core symptoms of ADHD (16). Thus, these two conditions could mutually exacerbate each other (17). This complex relationship is of particular concern during childhood and adolescence when brain structures and associated functions are undergoing significant developmental changes (18, 19, 20). Both conditions have separately been linked to aberrant brain development (21, 22, 23, 24, 25). Therefore, greater knowledge of the temporal and neurobiological relationships between these two conditions is of considerable clinical and public health importance (26).
At the behavioral level, studies have reported associations between ADHD symptoms and sleep disturbance (27, 28, 29, 30), although most of this research has been cross-sectional. Furthermore, these studies often did not control for stimulant medication or examine brain substrates. At the neuroanatomical level, a wide range of brain abnormalities have been associated with ADHD (31), including structural abnormalities in both subcortical and cortical regions (32,33). In studies not considering ADHD symptoms, neuroanatomical correlates of sleep disturbances in patients with insomnia have also been identified in overlapping corticostriatal circuitry (34, 35, 36, 37). These findings often varied across studies, owing to both the heterogeneous nature of these conditions and methodological inconsistencies (e.g., age group recruited, symptom measurements used) (38,39). Nevertheless, one hypothesis is that delayed development of the cognitive control system (frontostriatal circuit) coupled with lower daytime arousal, implicating the salience/ventral attention pathway, contributes to these problems (40, 41, 42, 43, 44). While it has been hypothesized that common structural abnormalities of the frontostriatal and salience/ventral attention networks contribute to both conditions, this hypothesis has yet to be tested (45).
At the molecular level, ADHD has been associated with neurotransmitter systems, especially dopamine (46, 47, 48) and norepinephrine (49, 50, 51), which also play an important role in sleep regulation (52, 53, 54). For example, the locus coeruleus noradrenergic system, with widely projecting noradrenergic axons from brainstem to the central nervous system (e.g., hippocampus and neocortex), has been implicated in both attention and arousal (55). Dysregulation of this system has been hypothesized to be involved in not only sleep disturbances, but also the pathophysiology of ADHD (56). Therefore, investigating the interplay between sleep disturbances and ADHD symptoms may be particularly informative to shed new light on this hypothesis.
To our knowledge, no study to date using large-scale datasets has identified common brain abnormalities in both ADHD and sleep disturbance. Therefore, the objectives of the present study were 1) to uncover the temporal relationship between ADHD symptoms and sleep disturbances, 2) to identify the common neuroanatomical association shared between both symptom types, 3) to quantify the extent to which the identified neuroanatomical association was mediated through ADHD, and 4) to examine the gene expressions of which biological processes or functional pathways are associated with the mediation effect. To achieve these goals, we used 3 datasets: a longitudinal cohort of child development (n = 1601), a neuroimaging cohort with a longitudinal design (n = 3515), and an “all genes, all structures” gene expression survey in human brains (3702 samples with >62,000 gene probes per profile). We hypothesized that ADHD symptoms would contribute to subsequent sleep disturbances, that reduced gray matter volume (GMV) of frontostriatal and salience/ventral attention pathways would be common to both conditions, and that brain gene expression regulating the neurochemical systems above (dopamine, norepinephrine) would be related to mediating effects between brain structure and symptoms. Specifically, we postulated mechanistically that changes in brain structure and gene expression would contribute to ADHD, which in turn would contribute to sleep disturbance.
Methods and Materials
Participants and Behavioral Measures
We used data from the Quebec Longitudinal Study of Child Development (QLSCD) (57) as the discovery dataset for longitudinal analysis. Participants with at least one observation of ADHD symptoms or sleep disturbances at ages 7, 8, 10, 12, and 13 years were included in the present study (n = 1601). ADHD symptoms (total score, hyperactivity-impulsivity score, and inattention score) were measured using the teacher-rated Social Behavior Questionnaire (58). Sleep disturbances were assessed by 7 questions, which were answered by the mother (i.e., daytime sleepiness, sleep talking, sleep walking, night terror, nightmare, bruxism, and enuresis). The protocol of QLSCD was approved by the Quebec Institute of Statistics (Quebec City, Quebec, Canada) and the St-Justine Hospital Research Center (Montreal, Quebec, Canada) ethics committees. Written informed consent was obtained from all the participating families at each assessment. This cohort focused on behavioral measures and not brain imaging (Method S1 in Supplement 1).
The Adolescent Brain Cognitive Development (ABCD) Study is tracking the brain development and health of more than 10,000 children 9 to 11 years of age from 21 centers throughout the United States (https://abcdstudy.org). These centers obtained full written informed consent of parents and assent of all children, and research procedures and ethical guidelines were followed in accordance with the institutional review boards. We used data from 3515 subjects for whom both complete behavioral and magnetic resonance imaging (MRI) data were available at baseline; 3076 of these subjects had 1-year follow-up data available (Method S2 in Supplement 1). ADHD symptoms were measured using the parent-reported DSM-Oriented Attention Problem Scale of the Child Behavior Checklist (59). Sleep disturbances rated using the parent Sleep Disturbance Scale for Children (60) were further summarized into 2 dimensions: dyssomnias (disorders of initiating and maintaining sleep, sleep breathing disorders, and disorders of excessive somnolence) and parasomnias (disorders of arousal, sleep-wake transition disorders, and sleep hyperhidrosis) (61).
Structural MRI Data
In the ABCD Study, 3-dimensional T1-weighted images were collected using 3T scanners at 21 data collecting sites. The detailed MRI acquisition protocol is described elsewhere (62). We obtained minimally preprocessed MRI data using the ABCD Pipeline (https://abcdstudy.org/scientists-protocol.html), and voxel-based morphometry analysis was conducted using a Computational Anatomy Toolbox (CAT12) (http://dbm.neuro.uni-jena.de/cat) and SPM12 (http://www.fil.ion.ucl.ac.uk/spm). Briefly, images were segmented into gray matter (GM), white matter, and cerebrospinal fluid based on tissue probability maps for ages 9 to 11 produced by the TOM8 Toolbox (https://irc.cchmc.org/software/tom.php). Next, images were normalized to the Montreal Neurological Institute space using the DARTEL toolbox and Geodesic Shooting approach. The registered GM images were multiplied with the Jacobian determinants derived from the spatial normalization and then smoothed with an 8-mm full width at half maximum Gaussian kernel with the resulting voxel size 1.5 mm3. Finally, we calculated the mean image of all these smoothed GM images and focused our subsequent analyses within a mask of GM by retaining only those voxels with more than 10% GM tissue.
Transcriptomic Data
We used the transcriptomic data from 6 neurotypical adult brains in the Allen Human Brain Atlas (AHBA) (https://human.brain-map.org) (63). Because right hemisphere data were available for only 2 of the 6 donors in AHBA, we used samples in the left hemisphere only. We followed the preprocessing pipeline recommended by Arnatkevic Iūtė et al. (64), including probe-to-gene re-annotation, intensity-based data filtering, probe selection by mean, separating tissue samples into subcortical and cortical regions based on the Harvard-Oxford atlas (65), and within-donor normalization, finally resulting in 15,408 unique genes (Method S3 in Supplement 1).
Statistical Analysis
Cross-Lagged Panel Analysis
In QLSCD, the longitudinal associations between ADHD total score and sleep disturbance were examined using a random-intercepts cross-lagged panel model (RI-CLPM) (66). Compared with the traditional CLPM, RI-CLPM requires at least 3 data waves and more closely approximates causal inference by separating the within-person process from stable between-person differences through the inclusion of random intercepts (67). We followed the two analytical steps in Madigan et al. (68). First, the standard RI-CLPM was estimated; then we examined the contribution of covariates (i.e., sex, socioeconomic status, and ADHD medication at age 7) to the between-person factors. We also performed RI-CLPMs between sleep and ADHD symptom dimensions (i.e., hyperactivity-impulsivity and inattention). We conducted a false discovery rate (FDR) correction for the 16 between-wave associations examined (i.e., 8 autoregressive and 8 cross-lagged paths).
To provide more supporting evidence using an independent cohort, we conducted traditional CLPMs for ADHD symptoms and each of the 3 sleep disturbance scores (i.e., total score, dyssomnia, and parasomnia) in the ABCD Study. We controlled for several stable variables (i.e., sex, race, and site) and time-variant parameters (i.e., ADHD medication, household income, educational level of parents, body mass index, and puberty) in these models. Accounting for the family relatedness (i.e., the records of single, sibling, twin, and triplet provided in a questionnaire as well as the kinship reconstructed from the genetic data) (Method S4 in Supplement 1; the code is available at the following link: https://github.com/qluo2018/FamilyPermutationABCD), the statistical significance, denoted by pperm, was established by conducting 5000 times multilevel block permutations (69). We compared the strength between the sleep→ADHD path and the ADHD→sleep path by the Wald test. To test whether the findings were robust across data collection sites, we conducted a meta-analysis of the significant cross-lagged coefficient identified above (Method S5 in Supplement 1). The model parameters were estimated by the full information maximum likelihood method (70), and the model fit was interpreted using common thresholds of good fit (71).
Whole-Brain and Voxelwise Analysis (ABCD Cohort)
A linear regression model was conducted to investigate the relationship between GMVs and ADHD symptoms at baseline, using age, sex, handedness, race, puberty, body mass index, site, household income, parental education, head motion, and total intracranial volume as covariates of no interest. We conducted a multilevel block permutation-based cluster-level correction (5000 times) for multiple comparisons in the neuroimaging analysis (Method S4 in Supplement 1) (69,72,73). At voxel level, we used a 2-sided test with a significance level of α = .001, whereas at cluster level, we used a permutation-based familywise error correction with α = .05. Similarly, we examined the GMV correlates with the total sleep disturbance score (familywise error correction p < .05) and tested such correlations for 2 dimensions (i.e., dyssomnia and parasomnia, familywise error correction p < .025). Significant overlapping GMVs of ADHD and sleep were defined on the basis of a cluster having more than 217 voxels falling into the 90% confidence interval (CI) of the smoothing kernel voxels (74).
Mediation Analysis
As the directional association between ADHD symptoms and sleep disturbances was determined by the CLPM, we assessed the mediation effect of ADHD on the association between sleep and the overlapping clusters identified above. The analyses were performed using the mediation toolbox developed by Wager et al. (75) (https://github.com/canlab/MediationToolbox) with 10,000 bootstraps.
Furthermore, we conducted a whole-brain and voxelwise exploratory analysis of this mediation effect with 3000 bootstraps at each voxel and FDR correction among all voxels. We additionally required a significant GMV-sleep association (p < .005, 2-sided, uncorrected). The unthresholded bootstrap-based t map of the mediation effect was further used in the following analyses.
Transcriptomic Analysis
We used partial least square (PLS) regression to relate the mediation effect to the gene expression data in AHBA (76, 77, 78, 79). The response variable was an n × 1 matrix, which was calculated by the average t value of a spherical region of interest (ROI) (r = 4 mm) centered by the Montreal Neurological Institute coordinates of each gene expression sampling site (80). The predictor variable was an n (number of tissue samples) × 15,408 (number of genes) matrix. AHBA provided 182 tissue samples in left subcortical regions and 784 tissue samples in left cortical regions. Using a permutation test (5000 times), we selected the PLS components that explained more variance of the mediation effect than could be accounted for by chance (76,79). The first PLS component was the linear combination of the weighted gene expression scores, maximizing the covariance between the expression profile and the mediation profile in the brain. A z score was calculated for each weight in a PLS component as the ratio between each weight estimation and standard error given by 5000 bootstraps. Therefore, the genes could be ranked by their normalized contributions to the PLS component. We adapted the codes for PLS provided by others (76,79). Leave-one-out cross-validation (i.e., repeating the analysis by leaving 1 donor out at a time) was used to test the influence of individual donors on the results, and PLS analyses using 6-mm regions of interest or a refined brain atlas (78,81) were also performed and compared to ensure that the findings were not dependent on a particular definition of region of interest size.
We used GSEAPreranked (version 6.0.12) (82) with default settings to identify sets of genes associated with Gene Ontology terms of biological processes and Kyoto Encyclopedia of Genes and Genomes pathways. The 2 lists of genes (n = 15,408) for subcortical and cortical regions were ranked by z score and passed to GSEAPreranked. From the top positively and negatively correlated genes in each list, we obtained separate sets of enriched gene sets (S+ and S−, respectively). To demonstrate the robustness of the findings, we also applied a more stringent threshold (i.e., top 1% and bottom 1% genes based on z score) to identify significant enrichments using DAVID 6.8 (83). Gene sets were considered significantly enriched with FDR q values < .05.
Results
Demographics
From QLSCD, 1601 participants (829 [52%] female) with behavioral measurements that were longitudinally collected at 7, 8, 10, 12, and 13 years of age were entered into the current study (Table 1). From the ABCD Study, 3515 participants (1664 [48%] female, 10 ± 0.61 years old) who had both complete MRI data and behavioral measurements at baseline were used in the current study, of whom 3076 had complete behavioral assessments at a 1-year follow-up (11.03 ± 0.63 years old) (Table 2).
Table 1.
Characteristics of the Study Population in the Quebec Longitudinal Study of Child Development (QLSCD)
| Wave 1 |
Wave 2 |
Wave 3 |
Wave 4 |
Wave 5 |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (± SD) | n | Mean (± SD) | n | Mean (± SD) | n | Mean (± SD) | n | Mean (± SD) | n | |
| Sex, Male, n (%) | 772 (48.2%) | 1601 | ||||||||
| Age, Years | 7.15 (± 0.25) | 1468 | 8.15 (± 0.26) | 1421 | 10.15 (± 0.26) | 1295 | 12.14 (± 0.25) | 1353 | 13.14 (± 0.26) | 1252 |
| ADHD Medication, n (%) | 56 (3.8%) | 1468 | ||||||||
| SES | −0.01 (± 1.00) | 1467 | ||||||||
| ADHD Total Score | 2.64 (± 2.56) | 1303 | 2.55 (± 2.43) | 1267 | 2.31 (± 2.37) | 986 | 2.13 (± 2.21) | 1004 | 2.52 (± 2.56) | 992 |
| H-I Score | 2.05 (± 2.52) | 1302 | 1.90 (± 2.40) | 1266 | 1.62 (± 2.33) | 986 | 1.39 (± 2.09) | 999 | 1.48 (± 2.39) | 937 |
| IN Score | 3.79 (± 3.39) | 1303 | 3.77 (± 3.32) | 1281 | 3.63 (± 3.27) | 987 | 3.57 (± 3.32) | 1004 | 3.76 (± 3.25) | 1023 |
| Sleep Disturbance | 0.23 (± 0.25) | 1601 | 0.26 (± 0.25) | 1601 | 0.32 (± 0.24) | 1062 | 0.29 (± 0.22) | 1188 | 0.28 (0.22) | 832 |
Descriptive statistics are reported as mean (± SD) unless noted otherwise.
ADHD, attention-deficit/hyperactivity disorder; H-I, hyperactivity-impulsivity; IN, inattention; SES, socioeconomic status.
Table 2.
Characteristics of the Study Population in the Adolescent Brain Cognitive Development (ABCD) Study
| Baseline (n = 3515) | Follow-up (n = 3076) | |
|---|---|---|
| Age, Years | 10.00 (± 0.61) | 11.03 (± 0.63) |
| Sex, Male, n (%) | 1851 (52.7%) | 1610 (52.3%) |
| Puberty | 1.56 (± 0.46) | 1.79 (± 0.59) |
| BMI | 18.59 (± 4.00) | 19.45 (± 4.52) |
| Parental Education | 17.01 (± 2.47) | 17.16 (± 2.33) |
| Household Income | 7.52 (± 2.19) | 7.76 (± 2.06) |
| Race, n (%) | ||
| White | 2554 (72.7%) | 2307 (75%) |
| Black/African American | 327 (9.3%) | 244 (7.9%) |
| Asian | 182 (5.2%) | 155 (5%) |
| Other | 452 (12.9%) | 370 (12%) |
| Family Relationship, n (%)a | ||
| Single | 2680 (76.2%) | 2346 (76.3%) |
| Sibling | 196 (5.6%) | 166 (5.4%) |
| Twin | 630 (17.9%) | 558 (18.1%) |
| Triplet | 9 (0.3%) | 6 (0.2%) |
| ADHD Symptoms | 2.54 (± 2.91) | 2.36 (± 2.86) |
| ADHD Medication, n (%) | ||
| No medication | 3204 (91.2%) | 2820 (91.7%) |
| Stimulant only | 233 (6.6%) | 193 (6.3%) |
| Nonstimulant only | 31 (0.9%) | 27 (0.9%) |
| Stimulant + nonstimulant | 46 (1.3%) | 36 (1.2%) |
| Sleep Disturbance | ||
| Total score | 36.24 (± 7.87) | 36.41 (± 7.75) |
| Dyssomnia | 22.19 (± 5.49) | 22.66 (± 5.67) |
| Parasomnia | 14.05 (± 3.58) | 13.75 (± 3.32) |
Descriptive statistics are reported as mean (± SD) unless noted otherwise.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index.
Provided by a questionnaire (“acspsw02”) from ABCD dataset.
ADHD Symptoms Contributed to Sleep Disturbance in School-Aged Children
To test the directionality, if any, between ADHD symptoms and sleep disturbances, we conducted a longitudinal analysis using the QLSCD cohort. We found a between-person and time-invariant association between ADHD total score and sleep disturbance (β = .10, 95% CI [0.004, 0.20]). In the within-person and dynamic component of the model, we found that higher ADHD total score at age 8 years was associated with worse sleep disturbance at age 10 (noted as ADHD 8y→sleep 10y) (β = .10, 95% CI [0.02, 0.18], FDR q < .05) (Table S1 in Supplement 1; Figure 1). Considering the covariates (i.e., sex, socioeconomic status, and ADHD medication), ADHD 8y→sleep 10y remained significant (β = .11, 95% CI [0.03, 0.19], FDR q = .02) (Figure S1 in Supplement 1). Both additional analyses using the participants without ADHD medication only (n = 1095; β = .09, 95% CI [0.004, 0.18]) and using the participants who only had data at both ages 8 and 10 years (n = 1263; β = .09, 95% CI [0.01, 0.18]) (Result S1 in Supplement 1) confirmed the significance of ADHD 8y→sleep 10y. Similar results held for ADHD subscales (i.e., hyperactivity-impulsivity symptom and inattention symptom) (Figures S2 and S3 in Supplement 1).
Figure 1.

Cross-lagged analysis between attention-deficit/hyperactivity disorder (ADHD) and sleep disturbance in the Quebec Longitudinal Study of Child Development. Random-intercepts cross-lagged panel model of ADHD total score and sleep disturbance from ages 7 to 13 years in the Quebec Longitudinal Study of Child Development (n = 1601). Standardized estimates (95% confidence intervals) are presented. Solid lines represent statistical significance (p < .05), whereas dashed lines represent nonsignificance (p > .05). Model fit: root mean square error of approximation = 0.04; comparative fit index = 0.98; Tucker-Lewis index = 0.96; standardized root mean square residual = 0.04. aPathways constrained to 1.00 to isolate between-person factor.
Using the ABCD cohort, we found more supporting evidence that ADHD symptoms at age 10 were also associated with sleep disturbances at a 1-year follow-up (sleep total score: β = .09, 95% CI [0.06, 0.13], pperm < .001) (Figure S4A in Supplement 1), and the meta-analysis across all data collection sites showed that this association was also robust (meta-β = .09, 95% CI [0.04, 0.13]). In contrast, although the path coefficient of the opposite direction was significant in this large cohort, its effect size was weaker (p < .005 by Wald test) and not robust (Figure S5A, B in Supplement 1). Again, both additional analyses using the participants without ADHD medication only (n = 2902; β = .04, 95% CI [0.01, 0.08]) and using the participants who were diagnosed with ADHD at baseline (n = 281; β = .10, 95% CI [0.01, 0.20]) (Result S2 in Supplement 1) confirmed the significance of ADHD→sleep. Similar results held for sleep subscales (i.e., dyssomnia and parasomnia) (Figures S4 and S5 in Supplement 1).
Shared Neural Correlates Between ADHD Symptoms and Sleep Disturbances
To test the hypothesis that ADHD symptoms and sleep disturbances share common neural correlates, we conducted a neuroimaging analysis using the ABCD cohort at baseline. We found that ADHD symptoms were associated with lower GMV in 2 brain clusters (Figure 2A; Tables S2 and S3 in Supplement 1; Figures S6 and S7A in Supplement 1), while only the dyssomnia subscale was associated with lower GMV in 3 brain clusters (Figure 2B; Tables S3 and S4 in Supplement 1; Figure S7B in Supplement 1). Among these clusters, we found 3 overlapping areas, including in the bilateral insula, left caudate, and putamen (2762 voxels); in the right middle frontal gyrus and inferior frontal gyrus (2296 voxels); and in the right parahippocampus, hippocampus, and amygdala (419 voxels) (Figure 2C; Figure S7C in Supplement 1).
Figure 2.

Significant brain clusters associated with attention-deficit/hyperactivity disorder (ADHD) symptoms and dyssomnia in the Adolescent Brain Cognitive Development Study at baseline. Multiple comparison correction includes voxel-level p < .001 and cluster-level familywise error correction p < .05 for ADHD and p < .025 for dyssomnia estimated by a multilevel block permutation accounting for family relatedness. The color bar represents t value. Age, sex, handedness, race, puberty, body mass index, site, household income, parental education, head motion, and total intracranial volume were controlled for in all analyses. (A) Brain regions significantly associated with ADHD symptoms. (B) Brain regions significantly associated with dyssomnia. (C) Brain regions significantly associated with ADHD or dyssomnia. Red areas are associated with ADHD, blue areas are associated with dyssomnia, and purple areas are the overlapping regions. L, left; R, right.
Mediation Analysis: Identified Neural Correlates Contributed to Both ADHD Symptoms and Dyssomnia
Having identified that ADHD contributed to subsequent sleep problems in the longitudinal datasets, we were then interested in examining whether ADHD statistically contributed to anatomical brain changes linked with sleep problems cross-sectionally. Thus, we conducted a mediation analysis to quantify the brain→ADHD→sleep relationship. We found that 48.6% (95% CI [31.7%, 75.9%]) of the association between lower average GMV of the 3 overlapping areas identified above and higher dyssomnia was mediated by ADHD symptoms (the mediation effect of each area was between 45.2% and 49.7%) (Figure 3; Figure S8 in Supplement 1). Controlling for ADHD medication, this mediation effect remained significant (44.2%, 95% CI [27.3%, 77.2%]; path a ∗ b: −3.92, 95% CI [−5.64, −2.35]). The whole-brain exploratory analysis of the mediation effect identified a significant cluster that covered the overlapping areas identified above (Figure S9 in Supplement 1). We also confirmed that ADHD symptoms at baseline significantly mediated the association between the baseline GMV and the follow-up dyssomnia (Figure S10 in Supplement 1).
Figure 3.
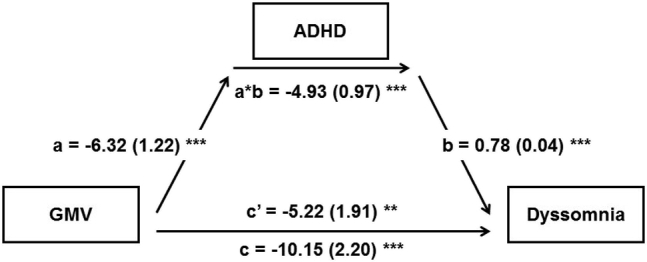
Associations of average overlapping gray matter volume (GMV), attention-deficit/hyperactivity disorder (ADHD) symptoms, and dyssomnia. Mediation model using the average overlapping GMV as the predictor, ADHD as the mediator, and dyssomnia as the dependent variable. Age, sex, handedness, race, puberty, body mass index, site, household income, parental education, head motion, and total intracranial volume were used as covariates of no interest. Path a measures the association between the predictor and the mediator; path b represents the effect of the mediator on the dependent variable while controlling for the predictor; path c measures the total relationship between the predictor and the dependent variable; path c′ measures the direct effect; the mediation effect is the product of path a and path b (a ∗ b). ∗∗p < .01, ∗∗∗p < .001.
Relationship Between the Mediation Effect and Brain Gene-Expression Profiles
Given that the strength of the brain→ADHD→sleep relationship had a heterogeneous spatial distribution among different brain areas, we further conducted a transcriptomic analysis to identify its association with the gene expressions in brain tissues. In the model for the subcortical regions, only the first PLS component was significant (i.e., explained 30% of the variance of the mediation effect, p < .001 by permutation) (additional details and validations in Results S3–S6 in Supplement 1). After the FDR correction, the S− gene sets in subcortical regions were enriched in 104 relevant biological processes (Table S7 in Supplement 2) and 26 relevant Kyoto Encyclopedia of Genes and Genomes pathways (Table S8 in Supplement 2). Enriched biological processes included chemical synaptic transmission, while enriched Kyoto Encyclopedia of Genes and Genomes pathways included circadian entrainment and dopaminergic synapse. These findings were also enriched in the top 1% gene set (Table S6 in Supplement 1). More enrichment findings of the S+ gene sets and the cortical regions are listed in Tables S9–S14 in Supplement 2.
Discussion
This study demonstrated that the cross-lagged association of ADHD at baseline with sleep disturbance at follow-up was stronger than the cross-lagged association in the opposite direction. Neuroimaging analysis revealed that smaller volumes, mainly in the cognitive control system and the salience/ventral attention system, constituted a common neurobiological substrate linking both ADHD and sleep disturbance. Among the subcortical structures, we identified a number of genes with higher expression levels in those brain areas where a greater proportion of the brain-sleep association was mediated by ADHD. These genes included those playing key roles in dopamine signaling and in the circadian cycle. The findings are in keeping with our hypothesis that changes in brain structure and gene expression contribute to ADHD, which in turn leads to sleep disturbance.
To our knowledge, this is the first study using RI-CLPM to address the longitudinal associations between ADHD with sleep disturbances. RI-CLPM offers potential advantages over other statistical approaches, such as providing closer approximation of causal inference (67). Although cross-sectional associations between ADHD and sleep disturbances have been reported, little is known about the longitudinal relationships. Most longitudinal studies examined unidirectional associations only, such as early sleep patterns predicting later ADHD symptoms (84,85) or childhood ADHD symptoms being associated with adulthood sleep quality (86). In the QLSCD cohort, we found that the strength of the ADHD→sleep relationship peaked between 8 and 10 years of age. However, this finding did not necessarily suggest an age-restricted relationship. For example, the ADHD symptoms at age 10 might indirectly influence the sleep disturbances at age 12 via elevating the sleep disturbances at age 10 (Figure 1).
We found that ADHD symptoms and dyssomnia were associated with common reductions of GM in the right frontal gyrus, bilateral insula, left striatum, right amygdala, and hippocampus. Structural abnormalities of these regions have previously been reported separately in ADHD (87, 88, 89) and dyssomnia (35,36,90, 91, 92). Our findings are in keeping with prior data, but crucially extend beyond it to identify common underpinnings of these 2 related pathologies by leveraging a large dataset (93). These neural regions play a cardinal role in high-level cognitive functions (frontostriatal circuitry) (94) and in the salience/ventral attention system (95).
Cognitive domains contingent on the frontostriatal circuitry are often impaired in ADHD (96) and in people with sleep disturbances (97). The striatum is connected to prefrontal cortex (98,99) and is particularly implicated in ADHD (100) as well as being important for sleep-wake regulation (101) and arousal (35). Disturbances in the maturation of such frontostriatal circuitry may contribute to cognitive problems often found in ADHD, such as difficulties in self-regulation (102), cognitive control (103), and reward processing (104). Notably, attention and arousal closely interact with each other (105), and their interaction has been hypothesized to be mainly located at the salience/ventral attention pathway. Our findings are in keeping with disruption of these pathways being associated with ADHD and sleep disturbances, particularly with regard to the right inferior frontal cortex, right temporoparietal junction, right middle frontal gyrus, and anterior insular cortex (105, 106, 107). Such ADHD-related brain abnormalities have been posited to reflect delayed development of frontostriatal circuitry underlying cognitive control (21,108).
Notably, our findings provide novel insights into neurobiological mechanisms contributing to the relationship between ADHD symptoms and sleep disturbances. Specifically, we demonstrated that lower GMV in key brain regions was associated with ADHD and dyssomnia and that 40% of this neuroanatomical association was mediated by the impact of ADHD on sleep. Furthermore, our enrichment analysis of this mediation effect highlighted several overlapping pathways (Figure S15 in Supplement 1), including the circadian entrainment pathway and neural signaling pathways (e.g., chemical synaptic transmission, dopaminergic synapse, glutamatergic synapse). Particularly, the neuroanatomical associations of sleep disturbances were mediated to a greater extent by ADHD symptoms in subcortical regions with higher gene expression levels of these pathways (Figure S16 in Supplement 1). Therefore, if a given ADHD treatment targets one of these pathways, it might reduce the ADHD component in sleep disturbances (109). However, approximately half of the brain-sleep association was not mediated by ADHD symptoms, suggesting that not all GMV reductions common to ADHD and dyssomnia stem from ADHD itself. This suggests that additional sleep management strategies are needed from a treatment perspective, even though treating ADHD itself may lead to sleep improvements, provided that such treatments do not have their own deleterious effects (110).
Our study has several limitations. Using 2 large longitudinal cohorts, we observed a significant temporal relationship between ADHD symptoms and subsequent sleep disturbances in school-aged children. This relationship was greatest between ages 8 and 10 years in QLSCD and between ages 10 and 11 years in the ABCD Study. There are several possible reasons for this cohort difference, including the following: 1) As these 2 cohorts were collected 10 years apart (i.e., the QLSCD children were born in 1997–1998, while the ABCD Study children were born in 2007–2008), the same chronological age may not reflect the same pubertal stage in these 2 cohorts. 2) Given the significant development during adolescence, it is also possible that a 1-year follow-up after 10 years of age can be different from a 2-year follow-up after the same age. It is possible that future longitudinal studies could directly investigate these points.
Conclusions
Analysis of 2 large longitudinal cohorts combined with the largest neuroimaging cohort of school-aged children to date revealed a strong ADHD-driven effect on subsequent sleep disturbance and identified common neuroanatomical correlates of both ADHD symptoms and sleep disturbances. We found that ADHD substantially mediated common neuroanatomical changes linked with both problems, highlighting the need to develop precision treatment approaches that integrate multimodal approaches to mitigate both ADHD symptoms and sleep disturbances.
Acknowledgments and Disclosures
This work was supported by the National Natural Science Foundation of China (Grant Nos. 81873909 and 81930095 [to QL], Grant Nos. 61932008 and 61772368 [to XZ], and Grant No. 91630314 [to JF]), Natural Science Foundation of Shanghai (Grant No. 17ZR1444400 [to QL]), Clare Hall, University of Cambridge (Visiting Fellowship [to QL]), Wellcome Trust Clinical Fellowship (Reference No. 110049/Z/15/Z [to SRC]), National Key Research and Development Program of China (Grant No. 2018YFC0910500 [to XZ] and Grant No. 2018YFC1312900 [to JF]), Lucy Cavendish College, University of Cambridge (Henslow Fellowship funded by the Cambridge Philosophical Society [to SM]), 111 Project (Grant No. B18015 [to JF]), Key Project of Shanghai Science &Technology (Grant No. 16JC1420402 [to JF]), Shanghai Municipal Science and Technology Major Project (Grant No. 2018SHZDZX01 [to JF]), Zhangjiang Lab (to JF), Canada Research Chair (Tier 1) Program (Grant No. 950-231862 [to MB]) and National Institute of Health Research Cambridge Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the National Institute of Health Research or the Department of Health and Social Care.
The QLSCD was supported by the Fondation Lucie et André Chagnon, Institut de la Statistique du Québec, Ministère de l’Éducation et de l’Enseignement supérieur, Ministère de la Famille, Institut de recherche Robert-Sauvé en santé et en sécurité du travail, Centre hospitalier universitaire Sainte-Justine, and Ministère de la Santé et des Services sociaux du Québec (source: data compiled from the final master file E1-E20 from the QLSCD [1998–2017], ©Gouvernement du Québec, Institut de la statistique du Québec).
Parts of data used in the preparation of this article were obtained from the ABCD Study (https://abcdstudy.org), held in the National Institute of Mental Health Data Archive. This is a multisite, longitudinal study designed to recruit more than 10,000 children 9–10 years of age and follow them over 10 years into early adulthood. The ABCD Study is supported by the National Institutes of Health and additional federal partners (Grant Nos. U01DA041022, U01DA041028, U01DA041048, U01DA041089, U01DA041106, U01DA041117, U01DA041120, U01DA041134, U01DA041148, U01DA041156, U01DA041174, U24DA041123, and U24DA041147). A full list of supporters is available at https://abcdstudy.org/nih-collaborators.
A listing of participating sites and a complete listing of ABCD Study investigators can be found at https://abcdstudy.org/principal-investigators.html. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in analysis or writing of this article. This article reflects the views of the authors and may not reflect the opinions or views of the National Institutes of Health or ABCD consortium investigators. The ABCD data repository grows and changes over time. The ABCD data used in this report came from National Institute of Mental Health data (https://doi.org/10.15154/1460410).
We thank Dr. Simon R. White for statistical advice and support, the children and families whose ongoing participation made this study possible, the coordinators of the QLSCD and the Quebec Institute of Statistics, and all the interviewers who assessed the mothers and children during this study.
SRC consults for Promentis Pharmaceuticals and Ieso Digital Health and receives a stipend from Elsevier for editorial journal work (Neuroscience & Biobehavioral Reviews and Comprehensive Psychiatry). BJS consults for Cambridge Cognition, Greenfield BioVentures, and Cassava Sciences. All other authors report no biomedical financial interests or potential conflicts of interest.
Footnotes
CS, QL, and SRC contributed equally to this work.
Supplementary material cited in this article is available online at https://doi.org/10.1016/j.biopsych.2020.03.010.
Contributor Information
Qiang Luo, Email: qluo@fudan.edu.cn.
Jianfeng Feng, Email: jianfeng64@gmail.com.
Supplementary Material
References
- 1.Polanczyk G., De Lima M.S., Horta B.L., Biederman J., Rohde L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am J Psychiatry. 2007;164:942–948. doi: 10.1176/ajp.2007.164.6.942. [DOI] [PubMed] [Google Scholar]
- 2.Barkley R.A., Fischer M., Smallish L., Fletcher K. The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. J Abnorm Psychol. 2002;111:279–289. [PubMed] [Google Scholar]
- 3.Lara C., Fayyad J., De Graaf R., Kessler R.C., Aguilar-Gaxiola S., Angermeyer M. Childhood predictors of adult attention-deficit/hyperactivity disorder: Results from the World Health Organization World Mental Health Survey Initiative. Biol Psychiatry. 2009;65:46–54. doi: 10.1016/j.biopsych.2008.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Petit D., Touchette E., Tremblay R.E., Boivin M., Montplaisir J. Dyssomnias and parasomnias in early childhood. Pediatrics. 2007;119:1016–1025. doi: 10.1542/peds.2006-2132. [DOI] [PubMed] [Google Scholar]
- 5.Lunsford-Avery J.R., Krystal A.D., Kollins S.H. Sleep disturbances in adolescents with ADHD: A systematic review and framework for future research. Clin Psychol Rev. 2016;50:159–174. doi: 10.1016/j.cpr.2016.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chang Z., Lichtenstein P., D’Onofrio B.M., Sjolander A., Larsson H. Serious transport accidents in adults with attention-deficit/hyperactivity disorder and the effect of medication: A population-based study. JAMA Psychiatry. 2014;71:319–325. doi: 10.1001/jamapsychiatry.2013.4174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mick E., Biederman J., Jetton J., Faraone S.V. Sleep disturbances associated with attention deficit hyperactivity disorder: The impact of psychiatric comorbidity and pharmacotherapy. J Child Adolesc Psychopharmacol. 2000;10:223–231. doi: 10.1089/10445460050167331. [DOI] [PubMed] [Google Scholar]
- 8.Gottlieb D.J., Ellenbogen J.M., Bianchi M.T., Czeisler C.A. Sleep deficiency and motor vehicle crash risk in the general population: A prospective cohort study. BMC Med. 2018;16:44. doi: 10.1186/s12916-018-1025-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Loe I.M., Feldman H.M. Academic and educational outcomes of children with ADHD. J Pediatr Psychol. 2007;32:643–654. doi: 10.1093/jpepsy/jsl054. [DOI] [PubMed] [Google Scholar]
- 10.Efron D., Sciberras E., Anderson V., Hazell P., Ukoumunne O.C., Jongeling B. Functional status in children with ADHD at age 6–8: A controlled community study. Pediatrics. 2014;134:992–1000. doi: 10.1542/peds.2014-1027. [DOI] [PubMed] [Google Scholar]
- 11.American Psychiatric Association . 5th ed. American Psychiatric Association; Arlington, VA: 2013. Diagnostic and Statistical Manual of Mental Disorders. [Google Scholar]
- 12.Danckaerts M., Sonuga-Barke E.J., Banaschewski T., Buitelaar J., Dopfner M., Hollis C. The quality of life of children with attention deficit/hyperactivity disorder: A systematic review. Eur Child Adolesc Psychiatry. 2010;19:83–105. doi: 10.1007/s00787-009-0046-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Martin J., Hiscock H., Hardy P., Davey B., Wake M. Adverse associations of infant and child sleep problems and parent health: An Australian population study. Pediatrics. 2007;119:947–955. doi: 10.1542/peds.2006-2569. [DOI] [PubMed] [Google Scholar]
- 14.Dey M., Castro R.P., Haug S., Schaub M.P. Quality of life of parents of mentally-ill children: A systematic review and meta-analysis. Epidemiol Psychiatr Sci. 2019;28:563–577. doi: 10.1017/S2045796018000409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Becker S.P., Langberg J.M., Eadeh H.M., Isaacson P.A., Bourchtein E. Sleep and daytime sleepiness in adolescents with and without ADHD: Differences across ratings, daily diary, and actigraphy. J Child Psychol Psychiatry. 2019;60:1021–1031. doi: 10.1111/jcpp.13061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sawyer A.C., Clark C.R., Keage H.A., Moores K.A., Clarke S., Kohn M.R. Cognitive and electroencephalographic disturbances in children with attention-deficit/hyperactivity disorder and sleep problems: New insights. Psychiatry Res. 2009;170:183–191. doi: 10.1016/j.psychres.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 17.Hvolby A. Associations of sleep disturbance with ADHD: Implications for treatment. Atten Defic Hyperact Disord. 2015;7:1–18. doi: 10.1007/s12402-014-0151-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Crowley S.J., Wolfson A.R., Tarokh L., Carskadon M.A. An update on adolescent sleep: New evidence informing the perfect storm model. J Adolesc. 2018;67:55–65. doi: 10.1016/j.adolescence.2018.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Colrain I.M., Baker F.C. Changes in sleep as a function of adolescent development. Neuropsychol Rev. 2011;21:5–21. doi: 10.1007/s11065-010-9155-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dahl R.E. Adolescent brain development: A period of vulnerabilities and opportunities. Keynote address. Ann N Y Acad Sci. 2004;1021:1–22. doi: 10.1196/annals.1308.001. [DOI] [PubMed] [Google Scholar]
- 21.Shaw P., Malek M., Watson B., Sharp W., Evans A., Greenstein D. Development of cortical surface area and gyrification in attention-deficit/hyperactivity disorder. Biol Psychiatry. 2012;72:191–197. doi: 10.1016/j.biopsych.2012.01.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jan J.E., Reiter R.J., Bax M.C., Ribary U., Freeman R.D., Wasdell M.B. Long-term sleep disturbances in children: A cause of neuronal loss. Eur J Paediatr Neurol. 2010;14:380–390. doi: 10.1016/j.ejpn.2010.05.001. [DOI] [PubMed] [Google Scholar]
- 23.Feinberg I., Campbell I.G. Longitudinal sleep EEG trajectories indicate complex patterns of adolescent brain maturation. Am J Physiol Regul Integr Comp Physiol. 2013;304:R296–303. doi: 10.1152/ajpregu.00422.2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Telzer E.H., Goldenberg D., Fuligni A.J., Lieberman M.D., Galvan A. Sleep variability in adolescence is associated with altered brain development. Dev Cogn Neurosci. 2015;14:16–22. doi: 10.1016/j.dcn.2015.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Shaw P., Eckstrand K., Sharp W., Blumenthal J., Lerch J.P., Greenstein D. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proc Natl Acad Sci U S A. 2007;104:19649–19654. doi: 10.1073/pnas.0707741104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yoon S.Y.R., Jain U., Shapiro C. Sleep in attention-deficit/hyperactivity disorder in children and adults: Past, present, and future. Sleep Med Rev. 2012;16:371–388. doi: 10.1016/j.smrv.2011.07.001. [DOI] [PubMed] [Google Scholar]
- 27.Owens J.A., Maxim R., Nobile C., McGuinn M., Msall M. Parental and self-report of sleep in children with attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 2000;154:549–555. doi: 10.1001/archpedi.154.6.549. [DOI] [PubMed] [Google Scholar]
- 28.Cortese S., Faraone S.V., Konofal E., Lecendreux M. Sleep in children with attention-deficit/hyperactivity disorder: Meta-analysis of subjective and objective studies. J Am Acad Child Adolesc Psychiatry. 2009;48:894–908. doi: 10.1097/CHI.0b013e3181ac09c9. [DOI] [PubMed] [Google Scholar]
- 29.Paavonen E.J., Raikkonen K., Lahti J., Komsi N., Heinonen K., Pesonen A.K. Short sleep duration and behavioral symptoms of attention-deficit/hyperactivity disorder in healthy 7- to 8-year-old children. Pediatrics. 2009;123:857–864. doi: 10.1542/peds.2008-2164. [DOI] [PubMed] [Google Scholar]
- 30.Didriksen M., Thorner L.W., Erikstrup C., Pedersen O.B., Paarup H.M., Petersen M. Self-reported restless legs syndrome and involuntary leg movements during sleep are associated with symptoms of attention deficit hyperactivity disorder. Sleep Med. 2019;57:115–121. doi: 10.1016/j.sleep.2019.01.039. [DOI] [PubMed] [Google Scholar]
- 31.Faraone S.V., Asherson P., Banaschewski T., Biederman J., Buitelaar J.K., Ramos-Quiroga J.A. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers. 2015;1:15020. doi: 10.1038/nrdp.2015.20. [DOI] [PubMed] [Google Scholar]
- 32.Hoogman M., Bralten J., Hibar D.P., Mennes M., Zwiers M.P., Schweren L. Subcortical brain volume differences of participants with ADHD across the lifespan: An ENIGMA collaboration. Lancet Psychiatry. 2017;4:310–319. doi: 10.1016/S2215-0366(17)30049-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hoogman M., Muetzel R., Guimaraes J.P., Shumskaya E., Mennes M., Zwiers M.P. Brain imaging of the cortex in ADHD: A coordinated analysis of large-scale clinical and population-based samples. Am J Psychiatry. 2019;176:531–542. doi: 10.1176/appi.ajp.2019.18091033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Altena E., Vrenken H., Van Der Werf Y.D., van den Heuvel O.A., Van Someren E.J. Reduced orbitofrontal and parietal gray matter in chronic insomnia: A voxel-based morphometric study. Biol Psychiatry. 2010;67:182–185. doi: 10.1016/j.biopsych.2009.08.003. [DOI] [PubMed] [Google Scholar]
- 35.Stoffers D., Altena E., van der Werf Y.D., Sanz-Arigita E.J., Voorn T.A., Astill R.G. The caudate: A key node in the neuronal network imbalance of insomnia? Brain. 2013;137:610–620. doi: 10.1093/brain/awt329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Riemann D., Voderholzer U., Spiegelhalder K., Hornyak M., Buysse D.J., Nissen C. Chronic insomnia and MRI-measured hippocampal volumes: A pilot study. Sleep. 2007;30:955–958. doi: 10.1093/sleep/30.8.955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Chen M.C., Chang C., Glover G.H., Gotlib I.H. Increased insula coactivation with salience networks in insomnia. Biol Psychol. 2014;97:1–8. doi: 10.1016/j.biopsycho.2013.12.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Samea F., Soluki S., Nejati V., Zarei M., Cortese S., Eickhoff S.B. Brain alterations in children/adolescents with ADHD revisited: A neuroimaging meta-analysis of 96 structural and functional studies. Neurosci Biobehav Rev. 2019;100:1–8. doi: 10.1016/j.neubiorev.2019.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Spiegelhalder K., Regen W., Baglioni C., Nissen C., Riemann D., Kyle S.D. Neuroimaging insights into insomnia. Curr Neurol Neurosci Rep. 2015;15:9. doi: 10.1007/s11910-015-0527-3. [DOI] [PubMed] [Google Scholar]
- 40.Hiscock H., Sciberras E. Academic Press; London: 2019. Sleep and ADHD: An Evidence-Based Guide to Assessment and Treatment. [Google Scholar]
- 41.Owens J., Gruber R., Brown T., Corkum P., Cortese S., O’Brien L. Future research directions in sleep and ADHD: Report of a consensus working group. J Atten Disord. 2013;17:550–564. doi: 10.1177/1087054712457992. [DOI] [PubMed] [Google Scholar]
- 42.Baird A.L., Coogan A.N., Siddiqui A., Donev R.M., Thome J. Adult attention-deficit hyperactivity disorder is associated with alterations in circadian rhythms at the behavioural, endocrine and molecular levels. Mol Psychiatry. 2012;17:988–995. doi: 10.1038/mp.2011.149. [DOI] [PubMed] [Google Scholar]
- 43.Hegerl U., Hensch T. The vigilance regulation model of affective disorders and ADHD. Neurosci Biobehav Rev. 2014;44:45–57. doi: 10.1016/j.neubiorev.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 44.Bioulac S., Micoulaud-Franchi J.-A., Philip P. Excessive daytime sleepiness in patients with ADHD—diagnostic and management strategies. Curr Psychiatry Rep. 2015;17:69. doi: 10.1007/s11920-015-0608-7. [DOI] [PubMed] [Google Scholar]
- 45.Owens J.A. The ADHD and sleep conundrum: A review. J Dev Behav Pediatr. 2005;26:312–322. doi: 10.1097/00004703-200508000-00011. [DOI] [PubMed] [Google Scholar]
- 46.Volkow N.D., Wang G.-J., Kollins S.H., Wigal T.L., Newcorn J.H., Telang F. Evaluating dopamine reward pathway in ADHD: Clinical implications. JAMA. 2009;302:1084–1091. doi: 10.1001/jama.2009.1308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Volkow N.D., Wang G.-J., Newcorn J., Fowler J.S., Telang F., Solanto M.V. Brain dopamine transporter levels in treatment and drug naive adults with ADHD. Neuroimage. 2007;34:1182–1190. doi: 10.1016/j.neuroimage.2006.10.014. [DOI] [PubMed] [Google Scholar]
- 48.Volkow N.D., Wang G.-J., Newcorn J.H., Kollins S.H., Wigal T.L., Telang F. Motivation deficit in ADHD is associated with dysfunction of the dopamine reward pathway. Mol Psychiatry. 2011;16:1147–1154. doi: 10.1038/mp.2010.97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Arnsten A.F., Lombroso P.J. Genetics of childhood disorders: XVIII. ADHD, Part 2: Norepinephrine has a critical modulatory influence on prefrontal cortical function. J Am Acad Child Adolesc Psychiatry. 2000;39:1201–1203. doi: 10.1097/00004583-200009000-00022. [DOI] [PubMed] [Google Scholar]
- 50.Yang L., Wang Y.-F., Li J., Faraone S.V. Association of norepinephrine transporter gene with methylphenidate response. J Am Acad Child Adolesc Psychiatry. 2004;43:1154–1158. doi: 10.1097/01.chi.0000131134.63368.46. [DOI] [PubMed] [Google Scholar]
- 51.Del Campo N., Chamberlain S.R., Sahakian B.J., Robbins T.W. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biol Psychiatry. 2011;69:e145–157. doi: 10.1016/j.biopsych.2011.02.036. [DOI] [PubMed] [Google Scholar]
- 52.Reyes B., Carvalho A., Vakharia K., Van Bockstaele E. Amygdalar peptidergic circuits regulating noradrenergic locus coeruleus neurons: Linking limbic and arousal centers. Exp Neurol. 2011;230:96–105. doi: 10.1016/j.expneurol.2011.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Berridge C.W., Arnsten A.F. Psychostimulants and motivated behavior: Arousal and cognition. Neurosci Biobehav Rev. 2013;37:1976–1984. doi: 10.1016/j.neubiorev.2012.11.005. [DOI] [PubMed] [Google Scholar]
- 54.Monti J.M., Monti D. The involvement of dopamine in the modulation of sleep and waking. Sleep Med Rev. 2007;11:113–133. doi: 10.1016/j.smrv.2006.08.003. [DOI] [PubMed] [Google Scholar]
- 55.Berridge C.W., Waterhouse B.D. The locus coeruleus-noradrenergic system: Modulation of behavioral state and state-dependent cognitive processes. Brain Res Brain Res Rev. 2003;42:33–84. doi: 10.1016/s0165-0173(03)00143-7. [DOI] [PubMed] [Google Scholar]
- 56.Biederman J., Spencer T. Attention-deficit/hyperactivity disorder (ADHD) as a noradrenergic disorder. Biol Psychiatry. 1999;46:1234–1242. doi: 10.1016/s0006-3223(99)00192-4. [DOI] [PubMed] [Google Scholar]
- 57.Jetté M., Des Groseilliers L. Survey Description and Methodology in Longitudinal Study of Child Development in Québec (ÉLDEQ 1998-2002) Institut de la statistique du Québec; Québec: 2000. Description of the statistical methodology of ÉLDEQ 1998-2002 (5-month-old infants) pp. 33–36. [Google Scholar]
- 58.Tremblay R.E., Loeber R., Gagnon C., Charlebois P., Larivée S., LeBlanc M. Disruptive boys with stable and unstable high fighting behavior patterns during junior elementary school. J Abnorm Child Psychol. 1991;19:285–300. doi: 10.1007/BF00911232. [DOI] [PubMed] [Google Scholar]
- 59.Aebi M., Winkler Metzke C., Steinhausen H.-C. Accuracy of the DSM-oriented attention problem scale of the child behavior checklist in diagnosing attention-deficit hyperactivity disorder. J Atten Disord. 2010;13:454–463. doi: 10.1177/1087054708325739. [DOI] [PubMed] [Google Scholar]
- 60.Bruni O., Ottaviano S., Guidetti V., Romoli M., Innocenzi M., Cortesi F. The Sleep Disturbance Scale for Children (SDSC) Construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J Sleep Res. 1996;5:251–261. doi: 10.1111/j.1365-2869.1996.00251.x. [DOI] [PubMed] [Google Scholar]
- 61.Spruyt K., Cluydts R., Verleye G.B. Pediatric sleep disorders: Exploratory modulation of their relationships. Sleep. 2004;27:495–501. doi: 10.1093/sleep/27.3.495. [DOI] [PubMed] [Google Scholar]
- 62.Casey B., Cannonier T., Conley M.I., Cohen A.O., Barch D.M., Heitzeg M.M. The Adolescent Brain Cognitive Development (ABCD) study: Imaging acquisition across 21 sites. Dev Cogn Neurosci. 2018;32:43–54. doi: 10.1016/j.dcn.2018.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Hawrylycz M.J., Lein E.S., Guillozet-Bongaarts A.L., Shen E.H., Ng L., Miller J.A. An anatomically comprehensive atlas of the adult human brain transcriptome. Nature. 2012;489:391–399. doi: 10.1038/nature11405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Arnatkevic Iūtė A., Fulcher B.D., Fornito A. A practical guide to linking brain-wide gene expression and neuroimaging data. Neuroimage. 2019;189:353–367. doi: 10.1016/j.neuroimage.2019.01.011. [DOI] [PubMed] [Google Scholar]
- 65.Desikan R.S., Ségonne F., Fischl B., Quinn B.T., Dickerson B.C., Blacker D. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 2006;31:968–980. doi: 10.1016/j.neuroimage.2006.01.021. [DOI] [PubMed] [Google Scholar]
- 66.Hamaker E.L., Kuiper R.M., Grasman R.P. A critique of the cross-lagged panel model. Psychol Methods. 2015;20:102–116. doi: 10.1037/a0038889. [DOI] [PubMed] [Google Scholar]
- 67.Berry D., Willoughby M.T. On the practical interpretability of cross-lagged panel models: Rethinking a developmental workhorse. Child Dev. 2017;88:1186–1206. doi: 10.1111/cdev.12660. [DOI] [PubMed] [Google Scholar]
- 68.Madigan S., Browne D., Racine N., Mori C., Tough S. Association between screen time and children’s performance on a developmental screening test. JAMA Pediatr. 2019;173:244–250. doi: 10.1001/jamapediatrics.2018.5056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Winkler A.M., Webster M.A., Vidaurre D., Nichols T.E., Smith S.M. Multi-level block permutation. Neuroimage. 2015;123:253–268. doi: 10.1016/j.neuroimage.2015.05.092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Muthén B., Kaplan D., Hollis M. On structural equation modeling with data that are not missing completely at random. Psychometrika. 1987;52:431–462. [Google Scholar]
- 71.Hu L., Bentler P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6:1–55. [Google Scholar]
- 72.Smith S.M., Nichols T.E., Vidaurre D., Winkler A.M., Behrens T.E., Glasser M.F. A positive-negative mode of population covariation links brain connectivity, demographics and behavior. Nat Neurosci. 2015;18:1565–1567. doi: 10.1038/nn.4125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Marquand A.F., Haak K.V., Beckmann C.F. Functional corticostriatal connection topographies predict goal directed behaviour in humans. Nat Hum Behav. 2017;1:0146. doi: 10.1038/s41562-017-0146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Luo Q., Chen Q., Wang W., Desrivieres S., Quinlan E.B., Jia T. Association of a schizophrenia-risk nonsynonymous variant with putamen volume in adolescents: A voxelwise and genome-wide association study. JAMA Psychiatry. 2019;76:435–445. doi: 10.1001/jamapsychiatry.2018.4126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Wager T.D., Davidson M.L., Hughes B.L., Lindquist M.A., Ochsner K.N. Prefrontal-subcortical pathways mediating successful emotion regulation. Neuron. 2008;59:1037–1050. doi: 10.1016/j.neuron.2008.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Whitaker K.J., Vertes P.E., Romero-Garcia R., Vasa F., Moutoussis M., Prabhu G. Adolescence is associated with genomically patterned consolidation of the hubs of the human brain connectome. Proc Natl Acad Sci U S A. 2016;113:9105–9110. doi: 10.1073/pnas.1601745113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Romero-Garcia R., Warrier V., Bullmore E.T., Baron-Cohen S., Bethlehem R.A.I. Synaptic and transcriptionally downregulated genes are associated with cortical thickness differences in autism. Mol Psychiatry. 2019;24:1053–1064. doi: 10.1038/s41380-018-0023-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Morgan S.E., Seidlitz J., Whitaker K.J., Romero-Garcia R., Clifton N.E., Scarpazza C. Cortical patterning of abnormal morphometric similarity in psychosis is associated with brain expression of schizophrenia-related genes. Proc Natl Acad Sci U S A. 2019;116:9604–9609. doi: 10.1073/pnas.1820754116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Vertes P.E., Rittman T., Whitaker K.J., Romero-Garcia R., Vasa F., Kitzbichler M.G. Gene transcription profiles associated with inter-modular hubs and connection distance in human functional magnetic resonance imaging networks. Philos Trans R Soc Lond B Biol Sci. 2016;371 doi: 10.1098/rstb.2015.0362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Albaugh M.D., Orr C., Chaarani B., Althoff R.R., Allgaier N., D’Alberto N. Inattention and reaction time variability are linked to ventromedial prefrontal volume in adolescents. Biol Psychiatry. 2017;82:660–668. doi: 10.1016/j.biopsych.2017.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Romero-Garcia R., Atienza M., Clemmensen L.H., Cantero J.L. Effects of network resolution on topological properties of human neocortex. Neuroimage. 2012;59:3522–3532. doi: 10.1016/j.neuroimage.2011.10.086. [DOI] [PubMed] [Google Scholar]
- 82.Subramanian A., Tamayo P., Mootha V.K., Mukherjee S., Ebert B.L., Gillette M.A. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci U S A. 2005;102:15545–15550. doi: 10.1073/pnas.0506580102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Huang D.W., Sherman B.T., Lempicki R.A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat Protoc. 2009;4:44–57. doi: 10.1038/nprot.2008.211. [DOI] [PubMed] [Google Scholar]
- 84.Touchette É., Petit D., Séguin J.R., Boivin M., Tremblay R.E., Montplaisir J.Y. Associations between sleep duration patterns and behavioral/cognitive functioning at school entry. Sleep. 2007;30:1213–1219. doi: 10.1093/sleep/30.9.1213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Gregory A.M., Eley T.C., O’Connor T.G., Plomin R. Etiologies of associations between childhood sleep and behavioral problems in a large twin sample. J Am Acad Child Adolesc Psychiatry. 2004;43:744–751. doi: 10.1097/01.chi/0000122798.47863.a5. [DOI] [PubMed] [Google Scholar]
- 86.Gregory A.M., Agnew-Blais J.C., Matthews T., Moffitt T.E., Arseneault L. ADHD and sleep quality: Longitudinal analyses from childhood to early adulthood in a twin cohort. J Clin Child Adolesc Psychol. 2017;46:284–294. doi: 10.1080/15374416.2016.1183499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Norman L.J., Carlisi C., Lukito S., Hart H., Mataix-Cols D., Radua J. Structural and functional brain abnormalities in attention-deficit/hyperactivity disorder and obsessive-compulsive disorder: A comparative meta-analysis. JAMA Psychiatry. 2016;73:815–825. doi: 10.1001/jamapsychiatry.2016.0700. [DOI] [PubMed] [Google Scholar]
- 88.Castellanos F.X., Proal E. Large-scale brain systems in ADHD: Beyond the prefrontal–striatal model. Trends Cogn Sci. 2012;16:17–26. doi: 10.1016/j.tics.2011.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Proal E., Reiss P.T., Klein R.G., Mannuzza S., Gotimer K., Ramos-Olazagasti M.A. Brain gray matter deficits at 33-year follow-up in adults with attention-deficit/hyperactivity disorder established in childhood. Arch Gen Psychiatry. 2011;68:1122–1134. doi: 10.1001/archgenpsychiatry.2011.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Joo E.Y., Noh H.J., Kim J.-S., Koo D.L., Kim D., Hwang K.J. Brain gray matter deficits in patients with chronic primary insomnia. Sleep. 2013;36:999–1007. doi: 10.5665/sleep.2796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Altena E., Van Der Werf Y.D., Sanz-Arigita E.J., Voorn T.A., Rombouts S.A., Kuijer J.P. Prefrontal hypoactivation and recovery in insomnia. Sleep. 2008;31:1271–1276. [PMC free article] [PubMed] [Google Scholar]
- 92.Guadagni V., Burles F., Ferrara M., Iaria G. Sleep quality and its association with the insular cortex in emotional empathy. Eur J Neurosci. 2018;48:2288–2300. doi: 10.1111/ejn.14124. [DOI] [PubMed] [Google Scholar]
- 93.Cortese S. Sleep and ADHD: What we know and what we do not know. Sleep Med. 2015;16:5–6. doi: 10.1016/j.sleep.2014.10.003. [DOI] [PubMed] [Google Scholar]
- 94.Chudasama Y., Robbins T.W. Functions of frontostriatal systems in cognition: Comparative neuropsychopharmacological studies in rats, monkeys and humans. Biol Psychol. 2006;73:19–38. doi: 10.1016/j.biopsycho.2006.01.005. [DOI] [PubMed] [Google Scholar]
- 95.Vossel S., Geng J.J., Fink G.R. Dorsal and ventral attention systems: Distinct neural circuits but collaborative roles. Neuroscientist. 2014;20:150–159. doi: 10.1177/1073858413494269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Rubia K. Cognitive neuroscience of attention deficit hyperactivity disorder (ADHD) and its clinical translation. Front Hum Neurosci. 2018;12:100. doi: 10.3389/fnhum.2018.00100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Maquet P. The role of sleep in learning and memory. Science. 2001;294:1048–1052. doi: 10.1126/science.1062856. [DOI] [PubMed] [Google Scholar]
- 98.Cohen M.X., Schoene-Bake J.-C., Elger C.E., Weber B. Connectivity-based segregation of the human striatum predicts personality characteristics. Nat Neurosci. 2009;12:32–34. doi: 10.1038/nn.2228. [DOI] [PubMed] [Google Scholar]
- 99.Draganski B., Kherif F., Klöppel S., Cook P.A., Alexander D.C., Parker G.J. Evidence for segregated and integrative connectivity patterns in the human basal ganglia. J Neurosci. 2008;28:7143–7152. doi: 10.1523/JNEUROSCI.1486-08.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Nakao T., Radua J., Rubia K., Mataix-Cols D. Gray matter volume abnormalities in ADHD: Voxel-based meta-analysis exploring the effects of age and stimulant medication. Am J Psychiatry. 2011;168:1154–1163. doi: 10.1176/appi.ajp.2011.11020281. [DOI] [PubMed] [Google Scholar]
- 101.Lazarus M., Huang Z.-L., Lu J., Urade Y., Chen J.-F. How do the basal ganglia regulate sleep–wake behavior? Trends Neurosci. 2012;35:723–732. doi: 10.1016/j.tins.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 102.Marsh R., Maia T.V., Peterson B.S. Functional disturbances within frontostriatal circuits across multiple childhood psychopathologies. Am J Psychiatry. 2009;166:664–674. doi: 10.1176/appi.ajp.2009.08091354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Durston S., van Belle J., de Zeeuw P. Differentiating frontostriatal and fronto-cerebellar circuits in attention-deficit/hyperactivity disorder. Biol Psychiatry. 2011;69:1178–1184. doi: 10.1016/j.biopsych.2010.07.037. [DOI] [PubMed] [Google Scholar]
- 104.Hu Y., Salmeron B.J., Gu H., Stein E.A., Yang Y. Impaired functional connectivity within and between frontostriatal circuits and its association with compulsive drug use and trait impulsivity in cocaine addiction. JAMA Psychiatry. 2015;72:584–592. doi: 10.1001/jamapsychiatry.2015.1. [DOI] [PubMed] [Google Scholar]
- 105.Coull J.T. Neural correlates of attention and arousal: Insights from electrophysiology, functional neuroimaging and psychopharmacology. Prog Neurobiol. 1998;55:343–361. doi: 10.1016/s0301-0082(98)00011-2. [DOI] [PubMed] [Google Scholar]
- 106.Corbetta M., Shulman G.L. Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci. 2002;3:201–215. doi: 10.1038/nrn755. [DOI] [PubMed] [Google Scholar]
- 107.Uddin L.Q. Salience processing and insular cortical function and dysfunction. Nat Rev Neurosci. 2015;16:55–61. doi: 10.1038/nrn3857. [DOI] [PubMed] [Google Scholar]
- 108.Arnsten A.F., Rubia K. Neurobiological circuits regulating attention, cognitive control, motivation, and emotion: Disruptions in neurodevelopmental psychiatric disorders. J Am Acad Child Adolesc Psychiatry. 2012;51:356–367. doi: 10.1016/j.jaac.2012.01.008. [DOI] [PubMed] [Google Scholar]
- 109.Furrer M., Jaramillo V., Volk C., Ringli M., Aellen R., Wehrle F.M. Sleep EEG slow-wave activity in medicated and unmedicated children and adolescents with attention-deficit/hyperactivity disorder. Transl Psychiatry. 2019;9:324. doi: 10.1038/s41398-019-0659-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Sciberras E., Mulraney M., Mensah F., Oberklaid F., Efron D., Hiscock H. Sustained impact of a sleep intervention and moderators of treatment outcome for children with ADHD: A randomised controlled trial. Psychol Med. 2020;50:210–219. doi: 10.1017/S0033291718004063. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.