

Supplemental Digital Content is available in the text
Keywords: acupuncture and moxibustion, GRADE, overview, primary osteoporosis, PRISMA, ROBIS
Abstract
Primary osteoporosis (PO) is a common disease that was characterized by a systemic impairment of bone mass and microarchitecture that results in fragility fractures and constitutes a pressing public health problem. But the effect of acupuncture or moxibustion treatment for PO is controversial.
To provide a comprehensive systematic overview of current evidence from systematic reviews (SR)/Meta-analysis of acupuncture treatment for PO pertaining to risk of bias, quality of evidence and report quality.
A total of 9 international and Chinese databases were searched for SR/meta-analysis of randomized controlled trials (RCTs). The risk of bias of SR/meta-analysis was appraised using the risk of bias in systematic reviews (ROBIS) instrument, the quality of the evidence was evaluated via Grading of Recommendations Assessment, Development and Evaluation (GRADE), and the report quality of the included studies are estimated by Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA).
According to ROBIS, only 2 articles were with risk of low bias; according to PRISMA, and most articles were reported incomplete, mainly in Q2, Q7, Q24, and Q27; according to GRADE, a total of 28 outcome indicators were evaluated under 4 different interventions of experimental group and control group: the evidence quality of bone mineral density (BMD) from treatment of acupuncture and moxibustion/acupuncture and moxibustion plus was high or moderate; Visual Analogue Score (VAS) of acupuncture plus moxibustion or acupuncture plus moxibustion plus other was low or very low; clinical effectiveness of acupuncture plus moxibustion or acupuncture plus moxibustion plus other was uncertain.
Acupuncture and moxibustion can improve the BMD of PO patients according to high-quality evidence, and may benefit VAS, pain score, clinical efficacy based on moderate or low-quality evidence. Further research that provides higher quality evidence of SR/RCTs of acupuncture and moxibustion treatment for PO is required.
1. Introduction
Primary Osteoporosis (PO) is a common disease that was characterized by a systemic impairment of bone mass and microarchitecture that results in fragility fractures.[1] After the age of 50, Osteoporosis becomes much more common, particularly for postmenopausal women.[2,3] Osteoporosis is a major health problem because of the fractures that lead to impair the quality of life as well as increases economic burden worldwide. In Korea, the residual lifetime risk of osteoporosis-related fractures for individuals aged 50 is estimated to be 59.5% for women and 23.8% for men.[4] In Switzerland, the cost of osteoporosis was estimated to rise from Confederation Helvetica Franc (CHF) 2.1 billion in 2010 to CHF 2.6 billion in 2025, corresponding to an increase of 29%.[5] Therefore, treatment of osteoporosis has significance to prevent fractures for patients and ease the socio-economic burden.
Anti-osteoporosis medicine remains the main therapeutic method in the clinical practice guidelines.[6,7] There is evidence of an effect for several drugs such as Bisphosphonates, Estrogen, and Calcium.[8,9] However, due to the adverse effects of medication are frequently experienced, such as Bisphosphonates cause osteonecrosis of the jaw, esophageal cancer, and renal failure, and Raloxifene is associated with an increased risk of deep vein thrombosis and pulmonary embolism,[10–12] thus some patients are turning to complementary and alternative therapies to treat osteoporosis.[13,14]
Acupuncture and moxibustion therapy, a traditional Chinese medicine treatment, boosts a good clinical efficacy worldwide.[15] The potential benefits of using acupuncture and moxibustion in osteoporosis mainly involve improvements in Bone mineral density (BMD), and treatment of acute fracture-related pain.[16,17] Previous animal studies have shown that acupuncture and moxibustion improve BMD, bone strength as well as hormone levels.[18–21] While the evidence that acupuncture can have beneficial effects on osteoporosis is moderately convincing in animals experiments, there is still not enough or strong evidence that acupuncture and moxibustion work in human subjects.
The aim of this overview was, therefore, to comprehensive summary and critically evaluate the current evidence from systematic reviews (SR)/Meta-analysis pertaining to risk of bias and quality of evidence and methodological quality of systematic reviews of acupuncture treatment for primary osteoporosis.
2. Methods
2.1. Registration
The protocol of this overview has been registered with the international prospective register of systematic reviews (PROSPERO, http://www.crd.york.ac.uk/PROSPERO), and the registration number is CRD42019121417. The overview of SR/Meta-analysis will be reported according to the guidelines of the PRISMA.[22]
2.2. Inclusion criteria for this overview
2.2.1. Types of studies
SR/Meta-analysis of randomized controlled trials (RCTs)/cross-controlled trials (CCTs)/other types like semi-randomized controlled trials were included, in which acupuncture and moxibustion were utilized as the treatment for the PO. No language limitation was used.
2.2.2. Types of participants
Participants who are adults diagnosed with PO using definitive diagnostic criteria or radiographically report the Chinese Medical Association criteria and guiding principles of clinical research on new drugs - PO was included. There is no restriction on gender or race.
2.2.3. Types of interventions
The studies of Acupuncture (electro-acupuncture, auricular acupuncture, warm-acupuncture and dry needling, etc.) and moxibustion used as an intervention to treat the PO were included. We also included trials that compared acupuncture and moxibustion plus another active treatment versus other active treatment alone.
2.2.4. Types of comparators
As to the control interventions, any form of therapy that did not involve acupuncture and moxibustion were included like medication, sham acupuncture, usual care, or no intervention.
2.2.5. Types of outcome measures
Trials results reported from each SR should include at least one of the following outcomes measures: BMD, clinical therapeutic effect, level of serum calcium, treatment effectiveness, pain score, level of serum alkaline phosphatase, osteocalcin. We compiled a table of any excluded studies, about which was plausible to expect that a reader would question why the study was not included.
2.2.6. Exclusion criteria for this overview
In this overview, SR/Meta-analysis which did not synthesize original data will be excluded.
2.3. Search methods for identification of studies
2.3.1. Database and search
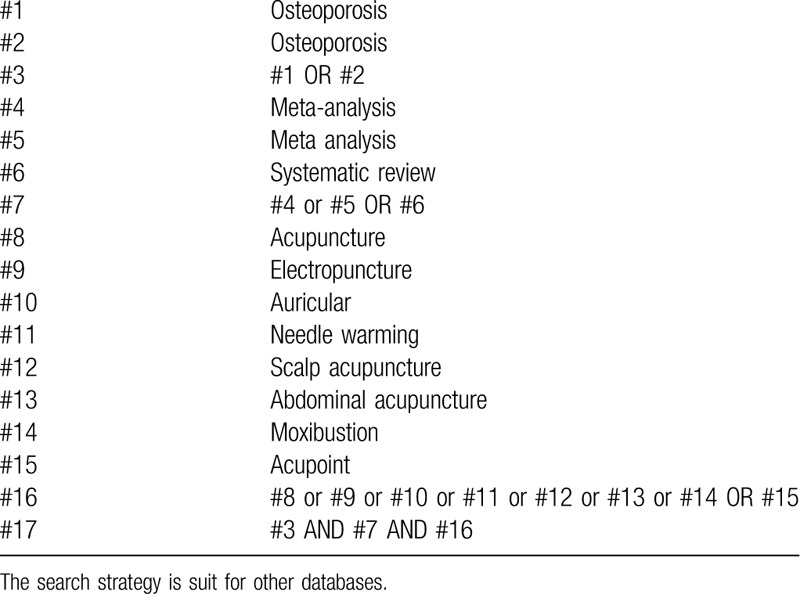
Five electronic international (Web of Science, The Cochrane Library, PubMed, MEDLINE, and EMBASE) and 4 Chinese electronic databases (China National Knowledge Infrastructure (CNKI), the Chinese Science and Technology Periodical Database (VIP), China Biology Medicine disc (CBM), and Wan Fang Digital Journals) from their inception until Dec 2018 were searched for potential SR. And we will also search systematic review or meta-analysis registration website (https://www.crd.york.ac.uk/PROSPERO/). We impose language restrictions on English and Chinese. The concrete search strategies are presented in Table 1.
Table 1.
Search strategy used in Cochrane library database.
2.3.2. Selection of SR
All the retrieved studies were imported into Endnote(X9) and filtered for the duplicated studies. Two reviewers (ZJ and WX) independently screened titles and abstracts for candidates according to the inclusion and exclusion criteria, then the full texts of potential articles were downloaded and determined eligibility independently by 2 reviewers (ZJ and WX). Discrepancies were resolved by a third reviewer (XQW), a list of all the excluded studies with reasons was present in Appendix I.
2.3.3. Data extraction
A standardized data extraction form was designed in advance. After all the included studies were identified, data were independently extracted from the reviews by 2 reviewers (ZJ and WX), and cross-checked on completion of extraction as follow: year of publication, number of patients enrolled, participant characteristics, features of interventions in treatment and control groups, types of outcome assessment, methodological quality of primary studies, data analysis approaches, sources of funding, any reported adverse events, and primary conclusion.
2.3.4. Assessment of quality and risk of bias
Two authors (XQW and XGX) evaluated the quality and risk of bias of the included SR/Meta-analysis independently using ROBIS and PRISMA. The consensus was reached by a discussion between 2 reviewers and an independent decision was obtained from the expert (LFR) if necessary.
PRISMA statement: The PRISMA[23] Statement for reporting quality consists of a 27-item checklist and a four-phase flow diagram. The checklist included items deemed essential for transparent reporting of a systematic review. Each item of the PRISMA form was graded with a "complete report" score of 1, a "partial report" of 0.5, and an "unreported" score of 0, with a total score of 27. When the literature score is 21 to 27, the report is considered relatively complete; when the score is 15 to 21, the report is considered to have some defects; when the score is less than 15, it is considered that there are relatively serious information defects.
ROBIS tool: The aim of the ROBIS tool is to evaluate the level of bias present within a systematic review.[24] This tool assesses the level of bias across 4 domains: study eligibility criteria, identification and selection of studies, data collection, and domain of study appraisal, synthesis and findings. Each has signaling questions and judgment of concerns about the risk of bias.
2.3.5. Assessment of evidence quality
The evidence quality of the included SR/Meta-analysis was evaluated by the GRADE[25–28] approach. Two authors (LJ and SMS) independently assessed the evidence of the outcomes, and the downgraded or upgraded factors affecting the quality of evidence should be described in detail to guarantee the reliability and transparency of results. The factors were related to the risk of bias, inconsistency, indirectness, precision, and publication bias. The overall quality of evidence was judged as high, moderate, low, or very low.
3. Result
3.1.1. Basic characteristics of included SR/Meta-analysis
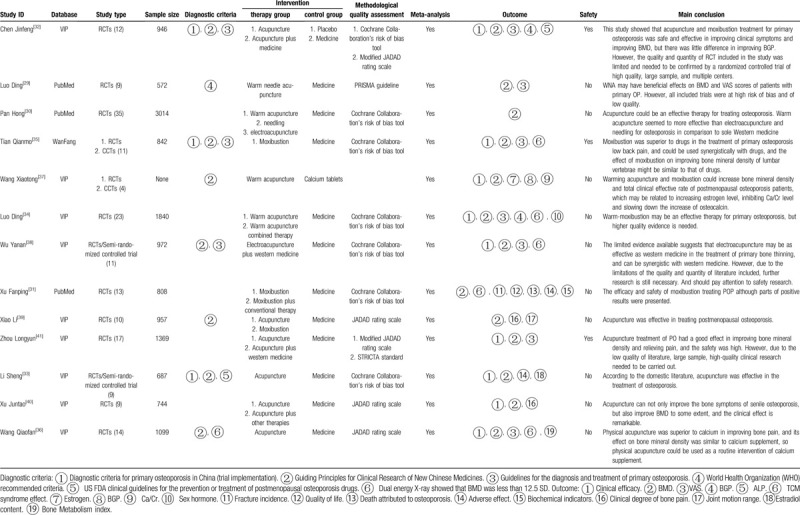
A total of 13 SR/Meta-analysis were included,[29–41] 3 in English,[29–31] 10 in Chinese,[32–41] and published in the years 2013 to 2018. The databases retrieved included the VIP, Wan Fang, and PubMed databases, the process of selection of study in Figure 1. All SR/Meta-analysis contained RCTs. Interventions in the therapy group were mainly acupuncture and moxibustion, or acupuncture and moxibustion combined with other therapies, and the control group was mainly conventional medicine and placebo. Different versions of Cochrane related handbooks or standards and the JADAD scale were used as the methodological quality assessment tools. Meta-analysis was performed in all SR/Meta-analysis. Outcome indicators were related to clinical efficacy, bone density, pain scores, and various blood biochemical indicators. Only 1 SR/Meta-analysis (Wang Qiaofan 2013) conducted a sensitivity analysis. Most studies supported the idea that acupuncture could improve osteoporosis. More details were summarized in Table 2.
Figure 1.
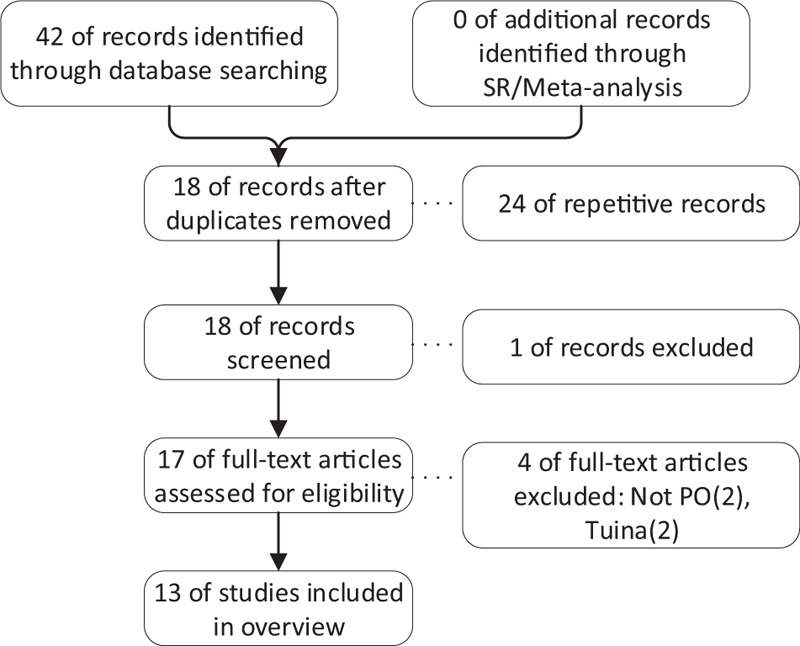
illustrate the process of study selection.
Table 2.
Basic characteristics of included SRs/Meta-analysis.
3.1.2. ROBIS evaluation results
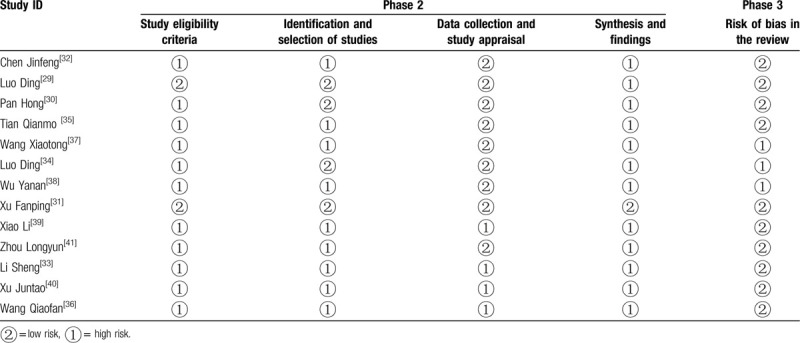
The ROBIS was used to evaluate the bias of the 13 included SR/Meta-analysis. In general, there were 26 (40%) low-risk results, and 39 (60%) results in high risk. Among all results, 10 SR/Meta-analysis was at low risk in Phase 3 (risk of bias in the review), 8 SR/Meta-analysis was at low risk in Domain 3 (data collection and study appraisal), 4 SR/Meta-analysis was at low risk in Domain 2 (identification and selection of studies), and 2 SR/Meta-analysis was at low risk in Domain1 (study eligibility criteria). More details were shown in Table 3.
Table 3.
ROBIS evaluation results of included SRs/Meta-analysis.
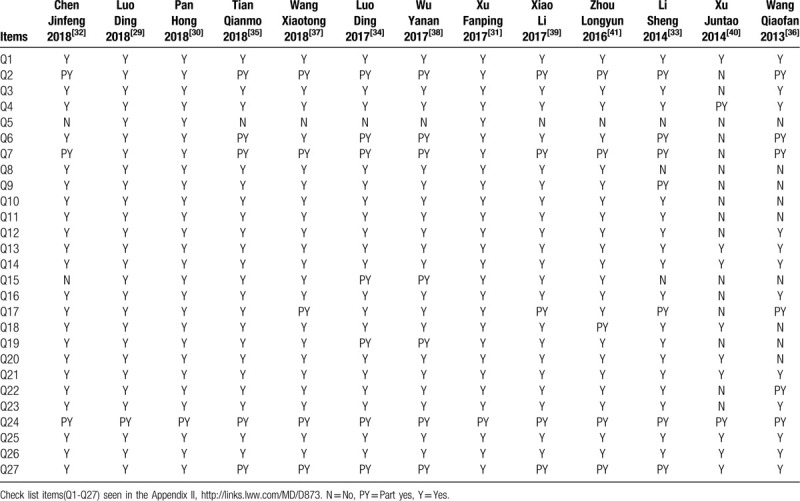
3.1.3. PRISMA evaluation results
The methodological quality of included SR/Meta-analysis was also assessed by PRISMA, and the Q1-Q27 as a replacement for items of PRISMA presented in Appendix II. The results showed that all reviews answered “Y” for Q1(Title), Q13(Summary measures) and Q14(Synthesis of results). For Q3(Rationale), Q4(Objectives), Q8(Search), Q9(Study selection), Q10(Data collection process), Q11(Data items), Q12(Risk of bias in individual studies), Q16(Additional analyses), Q18(Study characteristics), and Q20(Results of individual studies), most reviews (≥7) answered “Y”. All reviews answered “Y” to Q24(Summary of evidence). For Q2(Structured summary), Q7(Information sources), and Q27(Funding), the majority of reviews (at least 7 or more) answered “PY”. 10 reviews answered “N” to Q5. More details were summarized in Table 4.
Table 4.
PRISMA evaluation results of included SRs/Meta-analysis.
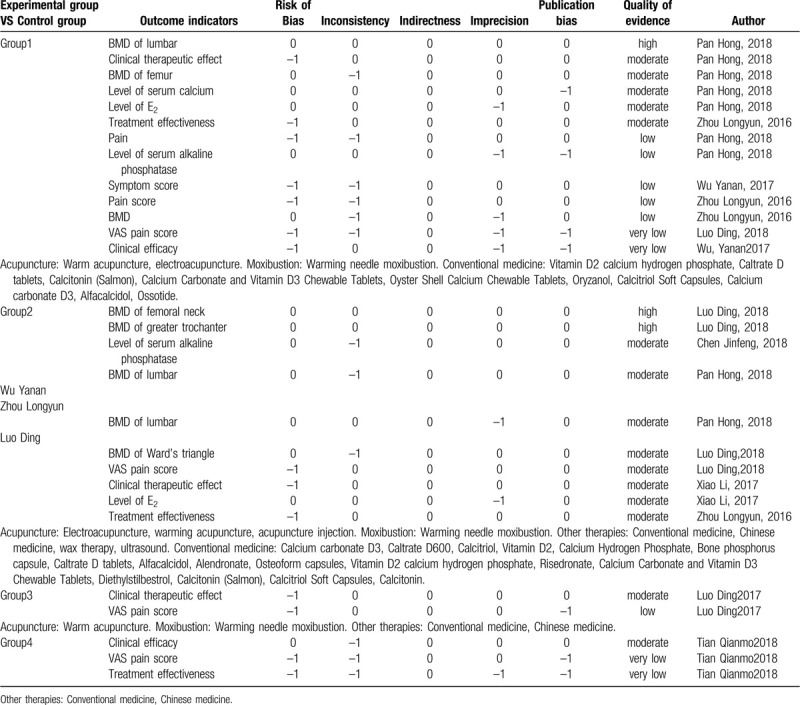
3.1.4. GRADE evaluation results
The quality of evidence of outcome indicators included in SR/Meta-analysis were assessed by GRADE. A total of 28 outcome indicators were evaluated under 4 different interventions of experimental group versus control group: Group1, Acupuncture plus moxibustion VS Conventional medicine; Group2, Acupuncture plus moxibustion plus Other therapies VS Conventional medicine; Group3, Acupuncture plus moxibustion plus Other therapies VS Chinese medicine; Group4, Moxibustion plus Other therapies VS Conventional drugs plus Chinese medicine. Among all outcome indicators, the quality of evidence was high in 3, moderate in 15, low in 6 and very low in 4. Among these 13 outcome indicators in group1, the quality of evidence was high in 1, moderate in 5, low in 5 and very low in 2. Among these 10 outcome indicators in group2, the quality of evidence was high in 2, moderate in 8. Among 2 indicators in group3, the quality of evidence was moderate in 1 and low in 1. Among these 3 outcome indicators in group4, the quality of evidence was moderate in 1 and very low in 2. More details were summarized in Table 5.
Table 5.
GRADE evaluation results of included SRs/meta-analysis.
4. Discussion
This overview summarizes 13 studies of acupuncture and moxibustion for the PO. High quality evidence suggests that acupuncture plus moxibustion whether plus or no other therapies can improve the BMD of PO patients. But the terminal outcome, such as rate of trip or fracture, still is lack, and the risk of bias and reporting quality of most included studies belongs to low or moderate. Hence, the high quality RCT and SR/meta-analysis still are needed to clarify the efficacy of acupuncture plus moxibustion for PO.
The risk of bias was assessed by ROBIS. Most studies belong to high risk with the same reason, including uncompleted literature search, identification and selection of studies, stressed statistically significant results, etc. The option of database and confirm of the search strategy are very important for SR/meta-analysis, and incorrect literature search will give rise to the risk of bias. So, a scientific and rigorous search strategy should be completed before start study. The screen of studies is also a key step for SR/meta-analysis, which may impact the results of the study. Hence, 2 researchers are needed to screen the studies and crosscheck the results to reduce bias. Another serious risk of bias reason form stressed the statistically significant results with more obvious in Chinese studies, which may exaggerate the efficacy. There is a problem with the integrated data method chosen for data synthesis, and the fixed effect model is still chosen for higher heterogeneity, which greatly increases the likelihood of positive results. A rigorous scientific attitude has been needed to produce high quality evidence.
The content quality of the included SR/Meta-analysis were assessed by PRISMA: 13 articles included did not provide the registration number of the systematic review; 7 articles did not report the source of funding in the study in detail, and the remaining 8 articles did not specifically describe and analyze the potential benefits and related conflicts of interest, which may have potential impact on the research results.
The evidence quality of the included SR/Meta-analysis was evaluated by GRADE. High quality of evidence show that warm acupuncture could increase the bone mineral density (BMD) of lumbar (SMD = 0.93, 95% CI = 0.65, 1.21),[30] BMD of the femoral neck (MD 0.14, 95% CI 0.08 to 0.21)[29] and greater trochanter (MD 0.09, 95% CI 0.04 to 0.15)[29] when compared with conventional medicine. Moderate quality of evidence shows that acupuncture plus moxibustion plus other therapies or not could improve the clinical therapeutic effect, BMD of femur, BMD of lumbar, BMD of Ward triangle, Level of serum alkaline phosphatase, Level of serum calcium, VAS pain score, and Level of E2 when compared with conventional medicine or Chinese medicine.[30,32,34,38,39,41]
According to the outcome indicators of the SR/meta-analysis in this study, the treatment of acupuncture or moxibustion may affect, but there are issues that we need to pay attention to in future research. With the development of evidence-based acupuncture and moxibustion, it is hoped that in the future, researchers will continue to promote standardization and precision through the techniques and operational procedures of acupuncture, so that more high-quality evidence can be provided in future clinical research, and acupuncture can be clinically wielded. The curative effect has obtained more scientific and objective evidence, promotes the modernization of acupuncture and moxibustion, and plays an important role in promoting the future integration of Chinese acupuncture and moxibustion. And the network meta-analysis for comparison based on the latest evidence is needed to identify the optimal intervention for the PO.
5. Conclusions
Acupuncture can improve BMD in patients with PO based on high-quality evidence, and can improve VAS, and pain score based on low- and medium-quality evidence. Further research is needed to provide higher quality SR/meta-analysis and randomized controlled trial evidence for acupuncture treatment of PO.
5.1. Strengths and Limitations of this study
-
1.
To the best of our knowledge, this is the first overview of SR or meta-analysis for PO with the ROBIS tool, GRADE, and PRISMA.
-
2.
The results of this overview will be beneficial to clinicians in making decisions in opting for method treating the disease, and help researcher to improve the quality of their study.
-
3.
The precise efficacy and safety of the intervention are still uncertain, and the optimal interventions cannot be compared, because the study does not involve quantitative or network meta-analysis methods.
Author contributions
Conceptualization: xu Guixing, Wang Xu.
Data curation: Xiao Qiwei.
Formal analysis: Xiao Qiwei, Zheng Qianhua, Cheng Ying.
Funding acquisition: Liang Fanrong.
Methodology: Xu Guixing, Xiao Qiwei, Zhou Jun, Wang Xu.
Supervision: Xu Guixing, Li Juan.
Writing – original draft: Xu Guixing, Xiao Qiwei, Zhou Jun, Wang Xu, Sun Mingsheng.
Writing – review & editing: Zheng Qianhua, Cheng Ying, Liang Fanrong.
Supplementary Material
Supplementary Material
Footnotes
Abbreviations: BMD = bone mineral density, CBM = China Biology Medicine disc, CCT = cross-controlled trials, CHF = Confederation Helvetica Franc, CNKI = China National Knowledge Infrastructure, GRADE = Grading of Recommendations Assessment, Development and Evaluation, MD = mean difference, PO = primary osteoporosis, PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-analyses, RCT = randomized controlled trial, ROBIS = Risk of bias in systematic reviews, SMD = standardized mean difference, SR = systematic review, VAS = Visual Analogue Score, VIP = the Chinese Science and Technology Periodical Database.
How to cite this article: Guixing X, Qiwei X, Jun Z, Xu W, Qianhua Z, Ying C, Mingsheng S, Juan L, Fanrong L. Acupuncture and moxibustion for primary osteoporosis: An overview of systematic review. Medicine. 2020;99:9(e19334).
XG, XQ, and ZJ contributed equally to this article.
This work was financially funded by the National Natural Science Foundation of China (grant numbers 81590950 and 81704137).
This overview not involve private information from personal or imperil their rights, so, ethical approval is not required.
We declare that we have no conflict of interest.
PROSPERO registration number: CRD42019121417.
References
- [1].Rachner TD, Khosla S, Hofbauer LC. Osteoporosis: now and the future. Lancet 2011;377:1276–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Cosman F, de Beur SJ, LeBoff MS, et al. Erratum to: Clinician's guide to prevention and treatment of osteoporosis. Osteoporos Int 2015;26:2045–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Cosman F, de Beur SJ, LeBoff MS, et al. Clinician's guide to prevention and treatment of osteoporosis. Osteoporos Int 2014;25:2359–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Park C, Ha YC, Jang S, et al. The incidence and residual lifetime risk of osteoporosis-related fractures in Korea. J Bone Miner Metab 2011;29:744–51. [DOI] [PubMed] [Google Scholar]
- [5].Svedbom A, Ivergard M, Hernlund E, et al. Epidemiology and economic burden of osteoporosis in Switzerland. Arch Osteoporos 2014;9:187. [DOI] [PubMed] [Google Scholar]
- [6].Khan SN, Craig L, Wild R. Osteoporosis: therapeutic guidelines. Guidelines for practice management of osteoporosis. Clin Obstet Gynecol 2013;56:694–702. [DOI] [PubMed] [Google Scholar]
- [7].Compston J, Bowring C, Cooper A, et al. Diagnosis and management of osteoporosis in postmenopausal women and older men in the UK: National Osteoporosis Guideline Group (NOGG) update 2013. Maturitas 2013;75:392–6. [DOI] [PubMed] [Google Scholar]
- [8].Yeap SS, Hew FL, Lee JK, et al. The Malaysian Clinical Guidance on the management of postmenopausal osteoporosis, 2012: a summary. Int J Rheum Dis 2013;16:30–40. [DOI] [PubMed] [Google Scholar]
- [9].Crandall CJ, Newberry SJ, Diamant A, et al. Comparative effectiveness of pharmacologic treatments to prevent fractures: an updated systematic review. Ann Intern Med 2014;161:711–23. [DOI] [PubMed] [Google Scholar]
- [10].Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321–33. [DOI] [PubMed] [Google Scholar]
- [11].Kotian P, Boloor A, Sreenivasan S. Study of adverse effect profile of parenteral zoledronic acid in female patients with osteoporosis. J Clin Diagn Res 2016;10:OC04–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].McClung M, Harris ST, Miller PD, et al. Bisphosphonate therapy for osteoporosis: benefits, risks, and drug holiday. Am J Med 2013;126:13–20. [DOI] [PubMed] [Google Scholar]
- [13].Lin X, Xiong D, Peng YQ, et al. Epidemiology and management of osteoporosis in the People's Republic of China: current perspectives. Clin Interv Aging 2015;10:1017–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Yen L, Jowsey T, McRae IS. Consultations with complementary and alternative medicine practitioners by older Australians: results from a national survey. BMC Complement Altern Med 2013;13:73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Chon TY, Lee MC. Acupuncture Mayo Clin Proc 2013;88:1141–6. [DOI] [PubMed] [Google Scholar]
- [16].Mak JC. Acupuncture in osteoporosis: more evidence is needed. Acupunct Med 2015;33:440–1. [DOI] [PubMed] [Google Scholar]
- [17].Lee JH, Choi TY, Lee MS, et al. Acupuncture for acute low back pain: a systematic review. Clin J Pain 2013;29:172–85. [DOI] [PubMed] [Google Scholar]
- [18].Wang HD, Chen Z, Inoue I, et al. Effects of electroacupuncture at GB points on markers of osteoporosis and bodyweight in ovariectomised rats. Acupunct Med 2015;33:465–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Zhou J, Li X, Liao Y, et al. Effects of electroacupuncture on bone mass and cathepsin K expression in ovariectomised rats. Acupunct Med 2014;32:478–85. [DOI] [PubMed] [Google Scholar]
- [20].Inoue M, Nakajima M, Hojo T, et al. The effect of electroacupuncture on osteotomy gap healing in a rat fibula model. Acupunct Med 2013;31:222–7. [DOI] [PubMed] [Google Scholar]
- [21].He J, Yang L, Qing Y, et al. Effects of electroacupuncture on bone mineral density, oestradiol level and osteoprotegerin ligand expression in ovariectomised rabbits. Acupunct Med 2014;32:37–42. [DOI] [PubMed] [Google Scholar]
- [22].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Moher D, Liberati A, Tetzlaff J, et al. Reprint--preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther 2009;89:873–80. [PubMed] [Google Scholar]
- [24].Whiting P, Savovic J, Higgins JP, et al. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 2016;69:225–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Guyatt GH, Oxman AD, Kunz R, et al. Incorporating considerations of resources use into grading recommendations. BMJ 2008;336:1170–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336:924–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Guyatt GH, Oxman AD, Kunz R, et al. Going from evidence to recommendations. BMJ 2008;336:1049–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Jaeschke R, Guyatt GH, Dellinger P, et al. Use of GRADE grid to reach decisions on clinical practice guidelines when consensus is elusive. BMJ 2008;337:a744. [DOI] [PubMed] [Google Scholar]
- [29].Luo D, Jr, Liu Y, Jr, Wu Y, Jr, et al. Warm needle acupuncture in primary osteoporosis management: a systematic review and meta-analysis. Acupunct Med 2018;36:215–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Pan H, Jin R, Li M, et al. The effectiveness of acupuncture for osteoporosis: a systematic review and meta-analysis. Am J Chin Med 2018;46:489–513. [DOI] [PubMed] [Google Scholar]
- [31].Xu F, Huang M, Jin Y, et al. Moxibustion treatment for primary osteoporosis: A systematic review of randomized controlled trials. PLoS One 2017;12:e0178688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Chen Jinfeng, Zhang Renwen, Mo Zhuo mao, et al. Meta analysis of acupuncture treatment of primary osteoporosis. J Liao Ning Univ TCM 2018;20(4.): [Google Scholar]
- [33].Li Sheng, Zhang Fengzheng, Wang Hongdu, et al. Systematic review of literatures of acupuncture and moxibustion for treatment of postmenopausal osteoporosis (PMO). J Luzhou Med Coll 2014;37: [Google Scholar]
- [34].Luo D, Wu Yanan, Liu Yue, et al. Warm needle acupuncture treatment for primary osteoporosis: a systematic review. Chin J Gerontol 2017;37:4. [Google Scholar]
- [35].Tian Qianmo, Xu Daoming, Wu Wenzhong, et al. Systematic review for clinical effect of moxibustion in treatment of primary osteoporosis. Tianjin J TCM 2018;35:684–90. [Google Scholar]
- [36].Wang Qiaofna, Li Jiqing, Zhang Lianhua. Acupuncture treatment for primary osteoporosis: a systematic review. Chin J Gerontol 2013;33(13.): [Google Scholar]
- [37].Wang Xiaotong, Lin Haixiong, Chen Zhixuan, et al. Systematic review for clinical effect and bone metabolic of warm needle moxibustion in treatment of postmenopausal osteoporosis. J Liao Ning of TCM 2018;45(3.): [Google Scholar]
- [38].Wu Yanan, Ding L, Fu Wenbin. The efficacy of electro-acupuncture on primary osteoporosis: Meta-analysis and systematic evaluation. Chin J Osteoporos 2017;23(2.): [Google Scholar]
- [39].Xiao Li, Chen Guo, Long Kangsheng, et al. Meta-analysis of the therapeutic effect of acupuncture on postmenopausal osteoporosis and acupoint selection method. J Xiangnan Univ (Med Sci) 2016;18(4.): [Google Scholar]
- [40].Xu Juntao, Shen Xinyun, Cao Qixin, et al. The effect of acupuncture on sneile osteoporosis: a systematic review. Zhejiang J Inte Traditional Chin West Med 2014;24(4.): [Google Scholar]
- [41].Zhou Longyun, Huang Guicheng, Guo Yang, et al. Effect and safety of acupuncture treatment of primary osteoporosis: a systematic review and meta-analysis. J Liao Ning of TCM 2016;(12.):43. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.