

Abstract
Objective:
In order to better understand factors motivating eating disorder (ED) behaviors and better identify persons at-risk for these behaviors, we sought to identify which personality domains and facets were associated with behaviors for weight control.
Methods:
ED behavior information was gathered from the University of North Carolina Alumni Heart Study using the question, “have you ever used any of the following to lose weight?” Respondents endorsed any combination of the following: “Vomiting,” “Fasting,” “Laxatives,” “Excessive physical exercise.” Personality was measured using the Revised NEO Personality Inventory (NEO-PI-R). One-way ANOVAs were performed comparing personality domains and facets to reported ED behaviors, computed both as separate behaviors and the number of cumulative behaviors.
Results:
Of 3496 respondents, 9.41% endorsed ever having used at least one ED behavior, with the majority endorsing only a single ED behavior. For both sexes, endorsing greater numbers of ED behaviors was associated with higher scores on Neuroticism and Openness. For women, the strongest associations for behaviors with personality were: excessive exercise with high Impulsiveness; fasting with high Impulsiveness and low Gregariousness; laxative use/purging with high scores on Activity and Feelings. For men, the strongest associations were: excessive exercise with high Impulsiveness; fasting with high Ideas; laxative use/purging with low Modesty.
Discussion:
Data collected from this sample showed a sex-modulated pattern of association between personality domains and facets with ED behaviors. Our findings support that obtaining personality profiles of individuals exhibiting subclinical eating behaviors will enhance our understanding of who is at risk of developing an ED diagnosis.
Keywords: Eating disorders, Eating behaviors, NEO-PI-R, Personality, Weight control
1. Introduction
Despite the relatively low incidence of formally diagnosed eating disorders (EDs), such as anorexia nervosa (AN; 0.8% incidence per year) and bulimia nervosa (BN; 2.2% incidence per year), an unhealthy preoccupation with body weight is rather common (MacLaren & Best, 2009; Stice, Marti, & Rohde, 2013). Over 17% of women and 13.1% of men engage in subclinical ED behaviors; including fasting, self-induced vomiting (purging), laxative or diuretic use, and binge eating (Touchette et al., 2011; Tylka & Subich, 2002). These subclinical behaviors contribute to the development of formal ED criteria as well as negative physical and mental health consequences (Herzog, Hopkins, & Burns, 1993; Thomas, Vartanian, & Brownell, 2009). Nutritional restriction can greatly impact physical health via altered hormonal regulation, which further affects bone health, thyroid function, and reproductive ability, to list a few (Donaldson & Gordon, 2015). Also, the risks of functional impairment, mental health disorders, and suicidality are increased for patients with EDs (Stice et al., 2013). These increased risks highlight the substantial need to both better understand factors motivating these subclinical ED behaviors, and to enhance our ability to identify persons at-risk for, or currently engaging in, these behaviors.
One means of improving our understanding of specific symptomology and ED behaviors is through better recognition of connections between eating behaviors and personality. More specifically, in the context of disordered eating behaviors, a patient's unique personality profile can provide a valuable means for evaluating and predicting ED development and treatment outcomes (Levallius, Clinton, Backstrom, & Norring, 2015). Personality has been implicated in affecting the expression of symptoms, recovery time, and relapse risk (Goodwin, Haycraft, Willis, & Meyer, 2011). Further, patients with EDs and comorbid personality pathologies have been shown to have greater psychological distress and mood disturbances, a more severe disease course, and an overall poorer treatment outcome (Claes et al., 2006; Tasca et al., 2009). Despite these connections with personality, few studies have evaluated personality relationships with specific subclinical weight loss behaviors and the frequencies in which they are reported.
One personality domain with strong ties to multiple psychiatric disorders, including the development and persistence of EDs, is Neuroticism (Terracciano et al., 2009; Widiger & Costa, 2012). Neuroticism represents the proneness of the individual to experience unpleasant and disturbing emotions, such as anxiety, anger, and depression, and corresponds to disturbances in thoughts and actions. High scores in the Neuroticism domain predict both overweight and underweight status, and patients with EDs score higher on Neuroticism compared to control participants (De Bolle et al., 2011; Terracciano et al., 2009). In patients hospitalized for AN, facets of Neuroticism, including Self-Consciousness and Vulnerability to Stress, are elevated during hospitalization and at follow-up, suggesting that these personality attributes could contribute to either the susceptibility of patients to develop AN or represent the lasting effects of the illness (McCormick et al., 2009).
The construct of impulsivity has long been of interest to clinicians as well as researchers seeking to understand the maladaptive thoughts, feelings and behaviors that characterize ED behaviors. Recently, Whiteside and Lynam used the Five-Factor Model of personality to understand the different impulsivity dispositions or expressions (Whiteside & Lynam, 2001). These dispositions include Sensation-Seeking/Excitement-Seeking (E5 facet of E in the NEO-PI-R) or the tendency to pursue novel or exciting stimuli; low Deliberation or lack of planning (C6 facet of Conscientiousness (C) in the NEO-PI-R); low Self-Discipline or low perseverance when distracted or tired (C5 facet of C in the NEO-PI-R); and negative Urgency or the tendency to engage in rash action in response to strong negative emotions (high N5 facet of Neuroticism (N) in the NEO-PI-R). Fischer, Peterson, and McCarthy (2013) demonstrated that the Impulsiveness facet of Neuroticism (N5) was positively correlated with bulimic symptoms but low Deliberation (C6 facet of Conscientiousness) was not (Fischer et al., 2013). They concluded that “negative urgency may be a predictor of bulimic behavior rather than lack of planning, although both are subtle variations on the theme of deficient impulse control.” While measures of negative urgency have been consistently associated with ED behaviors, findings for other impulsivity dispositions have been less consistent (Racine et al., 2013; Wenzel, Weinstock, Vander Wal, & Weaver, 2014).
To advance our understanding of the relationship between personality and ED behaviors, we examined the association between personality and self-reported ED behaviors in a sample of college-educated men and women. Specifically, we sought to identify which personality domains and facets were associated with behaviors for weight control, including purging, excessive exercise, fasting, and the use of laxatives. We also investigated whether personality domains and facets were related to specific combinations of these abnormal eating behaviors.
2. Methods
Using data from the University of North Carolina Alumni Heart Study (UNCAHS), associations between personality and reported ED behaviors were examined. The UNCAHS is an ongoing longitudinal study of men, women, and their spouses, who enrolled in the University of North Carolina, Chapel Hill between 1964 and 1966. The cohort study was originally designed to examine personality as a predictor of coronary heart disease (CHD); thus, the emphasis has been on measures of CHD risk factors, and not psychiatric or EDs. ED behavior data were obtained from the 12th wave of the study, which was conducted in 2008 when the cohort was approximately age 60. The 12th wave reported on their lifetime prevalence of ED behaviors based on the following question: “Have you ever used any of the following to lose weight?” Answer choices included: Vomiting, Fasting, Laxatives, and Excessive Physical Exercise. Data was available from 3496 study participants at wave 12.
If no behavior was endorsed, zero behaviors was assumed and used for analyses. We developed two ED outcomes representing the presence or absence of each ED behavior; one described each behavior separately, and one described the cumulative number of ED behaviors reported as none, one, or two or more. Because purging and laxative use as separate ED behaviors were not observed with enough frequency, these two behaviors were analyzed together, reflecting current literature that commonly combines these behaviors based on their similar characterization (Herle et al., 2019; Liebman et al., 2019).
Personality was measured using the Revised NEO Personality Inventory (NEO-PI-R) (Costa & McCrae, 2008) which was administered twice in the cohort (1988-91 for Timepoint 1 and 1997 for Timepoint 2) and the two scores were averaged to reduce missing data. The NEO-PI-R has been developed over 30 years to specifically operationalize the Five-Factor Model of Personality, which is a hierarchical structural model with 5 higher order factors or domains: Neuroticism (N), Extraversion (E), Openness to Experience (O), Agreeableness (A), and Conscientiousness (C). For each of the 5 domains, there are 6 lower-order, or narrower, facets specified (Costa & McCrae, 2008). The NEOPI-R is widely used and has extensively documented psychometric information including different forms of reliability and extensive validity evidence. Internal consistency coefficients for both Forms R and S range from 0.86-.95 for domain scales and from 0.56-.90 for facet scales. The NEO PI-R is validated against other personality inventories as well as projective techniques.
2.1. Statistical analyses
Descriptive statistics were performed for those reporting none and any ED behaviors, as well as those reporting none, one, two, three, and four behaviors. For each ED behavior, analyses of variance (ANOVA) was used to assess differences in mean NEO domain and facet scores for the three ED behaviors and for ED frequency. A type 1 error rate of 0.05 was used as the cut-off for statistical significance without additional correction for multiple testing. Differences between none, one, or two or more ED behaviors was evaluated using an ANOVA with Dunnet's post-hoc test, where endorsing no eating behaviors was the reference. Linear regression was used to evaluate the linear relationship between zero, one, and two or more behaviors for each domain/facet and to determine whether personality domains were related to EDs independent of one another. Based on a prior hypothesis regarding sex differences in ED behaviors and personality, analyses were performed separately for men and women.
2.2. Data availability
Data are not publicly available due to the issues needed to protect confidentiality of the respondents. Data can be shared on the basis of negotiated agreements with Dr. Siegler, PI of UNCAHS.
3. Results
3.1. Characteristics of, and associations for, individual ED behaviors
Total frequency of reported ED behavior engagement for the 3496 participants (35.2% women) is presented in Table 1. As shown in Table 1, the reported lifetime prevalence of any ED behavior, including purging, fasting, laxative use, and excessive exercise, was 9.4% (n = 329). The most commonly reported behaviors were fasting (5.3% of the total sample) and excessive exercise (4.8%), while laxative use/purging (2.3%) were much less frequent (Table 1).
Table 1.
Eating disorder behaviors: Individual and cumulative frequencies.
| Sum of Reported ED Behaviors |
Women Only (n = 1230) |
Men Only (n = 2266) |
Total Sample (n = 3496) |
|---|---|---|---|
| 0 | (n = 1083) | (n = 2084) | (n = 3167) |
| 88.0 | 91.97 | 90.59 | |
| 1 | (n = 110) | (n = 136) | (n = 246) |
| 8.94 | 6.00 | 7.04 | |
| 2 | (n = 21) | (n = 40) | (n = 61) |
| 1.70 | 1.77 | 1.74 | |
| 3 | (n = 11) | (n = 6) | (n = 17) |
| 0.89 | 0.26 | 0.49 | |
| 4 | (n = 5) | (n = 0) | (n = 5) |
| 0.41 | 0.0 | 0.14 | |
| Excessive Exercise | (n = 57) | (n = 110) | (n = 167) |
| 4.63 | 4.86 | 4.78 | |
| Fasting | (n = 79) | (n = 107) | (n = 186) |
| 6.42 | 4.72 | 5.32 | |
| Laxative Use or Purging | (n = 62) | (n = 17) | (n = 79) |
| 5.04 | 0.75 | 2.26 |
Data above represent the frequencies in which eating disorder behaviors were reported together, from no behaviors reported (0), to all four eating disorder behaviors reported (4) as well as frequencies in which certain eating disorder behaviors are reported in women, men, and in the total sample.
Of the study members (n = 3496) in this report, average age at the times the key variables were measured were as follows: For women (n = 1230), personality assessments were at 45.40 ± 3.82 years, and ED behavior assessments were at 60.02 ± 3.85 years. For men (n = 2266), personality assessments were at 45.35 ± 3.01 years, and ED behaviors assessments were at 61.29 ± 2.60 years. In women, high Neuroticism domain scores were associated with all three ED behaviors; in contrast, higher Neuroticism domain scores for men were associated with only excessive exercise (Tables 1 and 2, Fig. 1, p < .05 for all). As expected from the literature (reviewed in Introduction) only the Impulsiveness facet (N5) of the Neuroticism domain was significantly related to all 3 ED behaviors in both women and men. Few of the other facets of Neuroticism showed any significant associations. For both men and women, higher scores in the Extraversion domain, and specifically the Activity facet, were related to excessive exercise. For men, higher scores in Extraversion were also related to laxative use/purging. Interestingly, lower Gregariousness (E2) scores in both women and men were significantly related to laxative use or purging behaviors. Surprisingly, the Excitement-Seeking (E5) facet of E, akin to Sensation–Seeking, was unrelated to the 3 ED behaviors in women, while in men, E5 was related to excessive exercise.
Table 2.
Mean scores on NEO-PI-R by eating disorder behavior.
| Women (n = 1230) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Excessive Exercise | Fasting | Laxative Use/Purging | ||||||||||
| No | Yes | No | Yes | No | Yes | |||||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| Neuroticism | 52.86 | 0.27 | 55.93* | 1.24 | 52.84 | 0.28 | 55.52* | 1.20 | 52.86 | 0.27 | 55.78* | 1.50 |
| N1: Anxiety | 52.77 | 0.26 | 54.01 | 1.29 | 52.77 | 0.26 | 53.65 | 1.13 | 52.74 | 0.26 | 54.72 | 1.41 |
| N2: Angry Hostility | 49.98 | 0.26 | 52.47 | 1.37 | 49.97 | 0.26 | 52.04 | 1.12 | 49.97 | 0.26 | 52.66* | 1.46 |
| N3: Depression | 51.52 | 0.27 | 53.65 | 1.40 | 51.43 | 0.27 | 54.61** | 1.25 | 51.48 | 0.27 | 54.55* | 1.46 |
| N4: Self-Consciousness | 51.36 | 0.26 | 53.20 | 1.41 | 51.32 | 0.26 | 53.40 | 1.33 | 51.39 | 0.26 | 52.36 | 1.41 |
| N5: Impulsiveness | 51.46 | 0.26 | 58.00**** | 1.37 | 51.44 | 0.26 | 56.57**** | 1.19 | 51.58 | 0.26 | 54.54* | 1.47 |
| N6: Vulnerability | 51.18 | 0.27 | 52.20 | 1.34 | 51.23 | 0.27 | 50.91 | 1.16 | 51.16 | 0.26 | 52.50 | 1.52 |
| Extraversion | 49.94 | 0.26 | 52.62* | 1.49 | 50.09 | 0.26 | 49.24 | 1.23 | 50.00 | 0.26 | 51.03 | 1.36 |
| E1: Warmth | 51.18 | 0.26 | 50.98 | 1.42 | 51.28 | 0.26 | 49.22 | 1.24 | 51.19 | 0.26 | 50.69 | 1.40 |
| E2: Gregariousness | 49.53 | 0.29 | 48.22 | 1.54 | 49.74 | 0.29 | 44.81**** | 1.28 | 49.54 | 0.29 | 48.25 | 1.40 |
| E3: Assertiveness | 52.02 | 0.27 | 51.22 | 1.47 | 52.05 | 0.27 | 50.94 | 1.26 | 51.96 | 0.27 | 52.73 | 1.42 |
| E4: Activity | 53.17 | 0.26 | 56.51* | 1.18 | 53.30 | 0.26 | 53.28 | 1.13 | 53.16 | 0.26 | 56.53** | 1.19 |
| E5: Excitement-Seeking | 45.20 | 0.23 | 46.85 | 1.10 | 45.20 | 0.23 | 46.29 | 1.05 | 45.21 | 0.23 | 46.48 | 1.15 |
| E6: Positive Emotions | 51.59 | 0.28 | 53.90 | 1.25 | 51.61 | 0.28 | 52.93 | 1.18 | 51.64 | 0.28 | 52.54 | 1.24 |
| Openness | 55.15 | 0.28 | 56.45 | 1.56 | 54.98 | 0.29 | 59.26*** | 1.09 | 55.09 | 0.28 | 57.92* | 1.50 |
| O1: Fantasy | 53.29 | 0.27 | 56.42* | 1.30 | 53.19 | 0.27 | 57.27*** | 1.16 | 53.30 | 0.27 | 56.04* | 1.26 |
| O2: Aesthetics | 54.32 | 0.25 | 55.58 | 1.46 | 54.27 | 0.25 | 56.14 | 1.06 | 54.34 | 0.25 | 55.03 | 1.39 |
| O3: Feelings | 55.61 | 0.24 | 57.93 | 1.08 | 55.56 | 0.24 | 58.13* | 1.04 | 55.57 | 0.24 | 58.69** | 1.26 |
| O4: Actions | 52.69 | 0.26 | 53.46 | 1.41 | 52.62 | 0.26 | 54.69 | 1.18 | 52.65 | 0.26 | 54.51 | 1.31 |
| O5: Ideas | 50.41 | 0.28 | 49.41 | 1.58 | 50.19 | 0.28 | 53.65** | 1.17 | 50.33 | 0.28 | 51.55 | 1.56 |
| O6: Values | 52.89 | 0.26 | 55.10 | 1.21 | 52.82 | 0.26 | 55.65* | 1.03 | 52.86 | 0.26 | 55.66* | 1.21 |
| Agreeableness | 52.61 | 0.24 | 51.07 | 1.09 | 52.64 | 0.24 | 51.03* | 1.14 | 52.64 | 0.24 | 50.47 | 1.31 |
| A1: Trust | 52.59 | 0.23 | 52.69 | 1.17 | 52.70 | 0.23 | 50.63 | 1.23 | 52.60 | 0.23 | 52.38 | 1.26 |
| A2: Straightforwardness | 51.76 | 0.23 | 50.91 | 1.27 | 51.78 | 0.23 | 50.81 | 1.12 | 51.73 | 0.23 | 51.74 | 1.20 |
| A3: Altruism | 51.78 | 0.22 | 52.10 | 1.15 | 51.81 | 0.22 | 51.51 | 0.98 | 51.84 | 0.22 | 50.82 | 1.26 |
| A4: Compliance | 51.28 | 0.25 | 49.53 | 1.29 | 51.26 | 0.25 | 50.41 | 1.05 | 51.33 | 0.25 | 48.57* | 1.28 |
| A5: Modesty | 50.13 | 0.24 | 48.23 | 1.15 | 50.08 | 0.24 | 49.67 | 1.14 | 50.11 | 0.24 | 48.87 | 1.28 |
| A6: Tender-mindedness | 51.01 | 0.24 | 51.29 | 1.16 | 51.08 | 0.24 | 49.88 | 1.05 | 51.07 | 0.24 | 49.79 | 1.08 |
| Conscientiousness | 51.64 | 0.29 | 50.38 | 1.24 | 51.66 | 0.29 | 50.40 | 1.14 | 51.58 | 0.29 | 51.93 | 1.28 |
| C1: Competence | 53.49 | 0.25 | 50.93* | 1.23 | 53.48 | 0.25 | 51.83 | 1.03 | 53.41 | 0.25 | 53.05 | 1.19 |
| C2: Order | 49.09 | 0.30 | 47.40 | 1.53 | 49.13 | 0.31 | 47.16 | 1.26 | 49.10 | 0.31 | 47.42 | 1.33 |
| C3: Dutifulness | 51.79 | 0.23 | 49.95 | 1.26 | 51.78 | 0.23 | 50.51 | 1.10 | 51.71 | 0.23 | 52.01 | 1.19 |
| C4: Achievement Striving | 49.36 | 0.27 | 50.16 | 1.41 | 49.40 | 0.27 | 49.17 | 1.21 | 49.31 | 0.27 | 51.28 | 1.48 |
| C5: Self-Discipline | 48.16 | 0.29 | 47.59 | 1.17 | 48.21 | 0.29 | 46.89 | 1.26 | 48.16 | 0.29 | 47.51 | 1.38 |
| C6: Deliberation | 51.85 | 0.26 | 48.79* | 1.31 | 51.92 | 0.26 | 48.40** | 1.07 | 51.86 | 0.26 | 48.66* | 1.24 |
p < .05;
p < .01;
p < .001;
p < .0001 based on one-way ANOVA comparing personality domains and facets to eating disorder behaviors. SE = standard error.
Fig. 1. Mean Domain Scores by Endorsement of Eating Disorder Behavior:
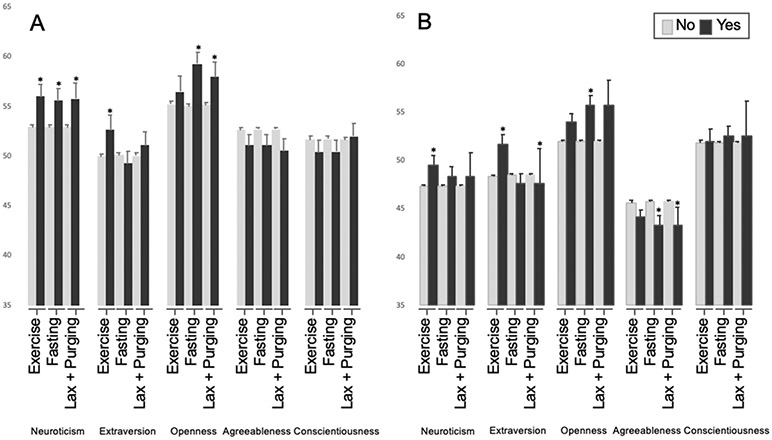
Bars represent mean scores on each domain as determined by the NEO-PI-R grouped by endorsement or denial of each eating disorder behavior. Error bars represent standard error. A = women, B = men. *p < .05 for yes compared to no.
For both sexes, higher Openness domain scores were related to fasting (p < .001). Although the individual Openness facet scores related to fasting differed slightly between sexes, in both men and women, four of the six facets of Openness were significantly related to fasting (Tables 2 and 3). Notably unique to men and not women, lower Agreeableness domain scores were associated with both fasting (p < .05) and laxative use/purging (p < .001, Table 3). Both sexes showed little relationship between Conscientiousness domain scores and ED behaviors. However, lower Deliberation facet scores were related to each of the ED behaviors in women only.
Table 3.
Mean scores on NEO-PI-R by eating disorder behavior.
| Men (n = 2264–2266) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Excessive Exercise | Fasting | Laxative Use/Purging | ||||||||||
| No | Yes | No | Yes | No | Yes | |||||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| Neuroticism | 47.24 | 0.19 | 49.49* | 0.96 | 47.29 | 0.19 | 48.30 | 0.98 | 47.31 | 0.19 | 50.70 | 2.49 |
| N1: Anxiety | 48.34 | 0.19 | 50.14 | 0.87 | 48.37 | 0.19 | 49.32 | 0.97 | 48.38 | 0.18 | 52.32 | 2.46 |
| N2: Angry Hostility | 49.66 | 0.20 | 50.84 | 0.95 | 49.66 | 0.20 | 50.83 | 0.99 | 49.68 | 0.20 | 54.97* | 2.22 |
| N3: Depression | 48.32 | 0.18 | 50.15* | 0.97 | 48.33 | 0.19 | 49.78 | 0.91 | 48.38 | 0.18 | 50.31 | 2.45 |
| N4: Self-Consciousness | 47.79 | 0.18 | 48.63 | 0.89 | 47.78 | 0.18 | 48.93 | 0.90 | 47.82 | 0.18 | 49.67 | 2.36 |
| N5: Impulsiveness | 49.69 | 0.18 | 53.53**** | 0.91 | 49.74 | 0.18 | 52.40** | 0.87 | 49.81 | 0.18 | 56.02** | 2.57 |
| N6: Vulnerability | 46.51 | 0.17 | 47.56 | 0.94 | 46.57 | 0.17 | 46.06 | 0.88 | 46.57 | 0.17 | 43.83 | 2.77 |
| Extraversion | 48.31 | 0.19 | 51.61*** | 0.99 | 48.47 | 0.19 | 47.64 | 0.96 | 48.41 | 0.19 | 53.37* | 3.50 |
| E1: Warmth | 46.95 | 0.21 | 48.75 | 1.04 | 47.07 | 0.21 | 45.85 | 1.03 | 46.99 | 0.20 | 51.46 | 3.65 |
| E2: Gregariousness | 48.81 | 0.20 | 50.59 | 0.91 | 48.91 | 0.20 | 48.08 | 1.06 | 48.84 | 0.20 | 54.30* | 3.81 |
| E3: Assertiveness | 54.88 | 0.19 | 55.86 | 0.96 | 54.89 | 0.19 | 55.52 | 0.99 | 54.89 | 0.19 | 58.80 | 2.87 |
| E4: Activity | 52.98 | 0.18 | 55.75** | 0.91 | 53.06 | 0.18 | 53.78 | 0.90 | 53.06 | 0.18 | 57.73* | 2.46 |
| E5: Excitement-Seeking | 50.16 | 0.16 | 52.66** | 0.72 | 50.20 | 0.16 | 51.65 | 0.85 | 50.23 | 0.16 | 54.22 | 2.90 |
| E6: Positive Emotions | 48.30 | 0.20 | 50.92** | 1.03 | 48.41 | 0.20 | 48.31 | 1.05 | 48.40 | 0.19 | 49.90 | 3.06 |
| Openness | 51.93 | 0.21 | 53.96 | 0.93 | 51.86 | 0.21 | 55.75*** | 0.89 | 52.00 | 0.20 | 54.25 | 2.55 |
| O1: Fantasy | 53.21 | 0.19 | 55.12* | 0.87 | 53.24 | 0.19 | 54.45 | 0.90 | 53.27 | 0.18 | 56.11 | 2.35 |
| O2: Aesthetics | 48.85 | 0.20 | 50.93* | 0.89 | 48.84 | 0.20 | 51.31* | 0.93 | 48.94 | 0.20 | 49.22 | 2.78 |
| O3: Feelings | 50.17 | 0.18 | 52.44* | 0.94 | 50.22 | 0.18 | 51.27 | 1.03 | 50.23 | 0.18 | 55.07* | 1.91 |
| O4: Actions | 47.57 | 0.20 | 49.05 | 0.93 | 47.55 | 0.20 | 49.64* | 0.95 | 47.62 | 0.19 | 50.10 | 2.97 |
| O5: Ideas | 51.88 | 0.20 | 53.35 | 0.90 | 51.78 | 0.20 | 56.00**** | 0.85 | 51.92 | 0.19 | 54.88 | 2.65 |
| O6: Values | 52.04 | 0.20 | 54.00* | 0.83 | 52.00 | 0.20 | 54.92** | 0.79 | 52.11 | 0.19 | 53.40 | 2.37 |
| Agreeableness | 45.62 | 0.18 | 44.12 | 0.73 | 45.66 | 0.18 | 43.43* | 0.95 | 45.61 | 0.18 | 37.88*** | 1.75 |
| A1: Trust | 50.80 | 0.17 | 51.32 | 0.74 | 50.83 | 0.17 | 50.62 | 0.86 | 50.83 | 0.17 | 47.95 | 2.76 |
| A2: Straightforwardness | 48.09 | 0.18 | 45.82* | 0.81 | 48.07 | 0.18 | 46.35 | 0.87 | 48.03 | 0.17 | 43.01* | 2.14 |
| A3: Altruism | 47.23 | 0.17 | 47.73 | 0.90 | 47.31 | 0.17 | 45.58* | 0.92 | 47.25 | 0.17 | 46.41 | 2.55 |
| A4: Compliance | 47.31 | 0.18 | 45.66 | 0.78 | 47.29 | 0.18 | 45.95 | 0.92 | 47.28 | 0.18 | 41.34* | 1.71 |
| A5: Modesty | 46.89 | 0.19 | 45.18 | 0.98 | 46.90 | 0.19 | 44.84* | 1.10 | 46.87 | 0.18 | 38.26*** | 2.25 |
| A6: Tender-mindedness | 46.24 | 0.19 | 46.32 | 0.93 | 46.31 | 0.19 | 44.56 | 1.03 | 46.28 | 0.19 | 40.28* | 3.40 |
| Conscientiousness | 51.81 | 0.20 | 51.93 | 1.26 | 51.78 | 0.20 | 52.47 | 1.11 | 51.78 | 0.20 | 56.37 | 3.71 |
| C1: Competence | 54.09 | 0.18 | 53.74 | 1.02 | 54.07 | 0.18 | 54.20 | 0.96 | 54.06 | 0.18 | 57.38 | 3.40 |
| C2: Order | 48.78 | 0.20 | 49.56 | 1.07 | 48.80 | 0.20 | 48.85 | 1.03 | 48.79 | 0.20 | 52.31 | 3.08 |
| C3: Dutifulness | 52.66 | 0.17 | 51.14 | 1.01 | 52.63 | 0.17 | 51.87 | 0.97 | 52.61 | 0.17 | 51.48 | 3.15 |
| C4: Achievement Striving | 51.27 | 0.20 | 53.17 | 1.13 | 51.29 | 0.21 | 52.69 | 1.01 | 51.30 | 0.20 | 58.13** | 3.10 |
| C5: Self-Discipline | 49.38 | 0.20 | 49.31 | 1.10 | 49.36 | 0.20 | 49.81 | 1.03 | 49.38 | 0.19 | 50.46 | 3.61 |
| C6: Deliberation | 52.53 | 0.18 | 50.80 | 0.97 | 52.47 | 0.18 | 52.12 | 0.88 | 52.45 | 0.18 | 54.11 | 2.78 |
Data shown are mean scores on the NEO-PI-R by endorsement or denial of specific eating disorder behaviors in men.
p < .05;
p < .01;
p < .001;
p < .0001 based on one-way ANOVA comparing personality domains and facets to eating disorder behaviors.
For women, the individual ED behaviors most strongly associated with personality facets were: excessive exercise with Impulsiveness (p < .001); fasting with Impulsiveness and Gregariousness (p < .001, for both); and laxative use/purging with Activity and Feelings (p < .01, for both). Similarly, for men, excessive exercise was associated with high scores on Impulsiveness (p < .0001); fasting was most strongly associated with high scores on Ideas (p < .0001); and laxative use/purging with lower scores on Modesty (p < .001).
3.2. Characteristics of, and associations for, multiple ED behaviors
Of the 9.4% reporting any abnormal eating behavior, 74.8% of those endorsed only a single ED behavior, while 25.2% endorsed two or more behaviors; only five people (0.14%), all women, reported engaging in all four ED behaviors (Table 1). The most common behaviors reported in combination were fasting and excessive exercise. Though men and women similarly reported both fasting and excessive exercise, a greater proportion of women than men reported laxative use/purging.
At the domain level in both men and women, reporting more ED behaviors was associated with higher scores on Neuroticism (p < .01, for both) and Openness (p < .001 and p < .01, respectively) and lower scores on Agreeableness (p < .001 and p < .01, respectively) (Supplement Table 1). Higher scores on Extraversion were associated with more ED behaviors in men only (p < .05). Linear regression modeling showed the relationships between increasing numbers of ED behaviors and these personality domains (high Neuroticism and Openness, as well as low Agreeableness in women and high Extraversion in men) were independent of one another (Supplement Table 2). At the facet level, reporting more ED behaviors was associated with high scores on Impulsiveness in both sexes (p < .0001). Only in women, reporting more ED behaviors was associated with a low Deliberation score (p < .001) (Supplement Table 1).
4. Discussion
Using the UNCAHS, a cohort of college-educated, middle-aged persons, self-reported ED behaviors were associated with a number of personality domains and facets. For this large, non-treatment seeking sample, notable domain associations for ED behaviors included higher Neuroticism and Openness and lower Agreeableness. Interestingly, sex modulated the patterns of association between personality and ED behaviors. For example, in addition to the domains above, higher Extraversion was associated with more ED behaviors in men only. These associations provide insights into better understanding the underlying motivations for ED behaviors and may provide an opportunity for identification of individuals in a pre-clinical state.
Our work supports prior evidence of associations between ED behaviors and high Neuroticism. A high score on Neuroticism typically indicates individuals more likely to suffer from feelings of anxiety, depression, and anger, in addition to engaging in behaviors that act on those feelings. High scores on Neuroticism have been consistently related to not only EDs, but other psychiatric disorders, as well (De Bolle et al., 2011; McCormick et al., 2009; Terracciano et al., 2009). Subtypes of anorexia, including restricting and binging/purging types, have demonstrated higher scores on Neuroticism when compared to a sample of non-eating disordered women (Bollen & Wojciechowski, 2004). In our sample, high Neuroticism scores were significantly correlated with all three of the ED behaviors in women (and excessive exercise in men), demonstrating consistency with the current literature.
In a similar non-clinical sample that studied undergraduate students, the combination of high Neuroticism and low Extraversion was implicated as a risk factor for EDs (MacLaren & Best, 2009). Comparably, a clinical sample of women patients diagnosed with EDs demonstrated a high Neuroticism and low Extraversion and Openness score compared to controls (De Bolle et al., 2011). In our sample, there were similar strong relationships between higher Neuroticism scores and women reporting ED behaviors. However, rather than low Extraversion and Openness scores, women with higher Extraversion and Openness scores reported more excessive exercise and fasting, respectively. This finding is potentially due to the nature of our cohort as a whole: our data only reflect self-reported behaviors, and no follow-up was completed to determine if those who reported ED behaviors in this sample developed a formal diagnosis of an ED.
In men, higher scores on Extraversion were associated with engaging in more ED behaviors, specifically excessive exercise and laxative use/purging. In women, higher Extraversion scores were related only to excessive exercise. Thus, for men, there appears a connection between Extraversion and both of these ED behaviors; one possibility is that men are more likely to participate in sports where weight loss is strongly encouraged, such as wrestling. However, these speculations merit much more investigation. In addition to higher scores on Extraversion, ED behaviors in men were most strongly associated with low scores on Agreeableness. These findings in men are consistent with the literature, in that groups defined as addicted to exercise had significantly higher scores on Extraversion and lower scores on Agreeableness than controls (Lichtenstein, Christiansen, Elklit, Bilenberg, & Stoving, 2014). Individuals who score low on Agreeableness tend to be egocentric and competitive, while those who score high on Extraversion prefer large groups and are assertive and active; these definitions are consistent with the findings in this cohort as men tended to report excessive exercise more frequently than the other ED behaviors.
In our sample, the most notable personality facet associated with ED behaviors was Impulsiveness, which reflects an inability to control cravings and urges and the potential to engage in a variety of harmful acts. Individuals with high Impulsiveness scores perceive their desires to be so strong that they cannot resist them; low scorers on Impulsiveness find it easier to resist such urges and temptations and have a higher tolerance for frustration. Higher scores on Impulsiveness were significantly correlated with the frequency of reported ED behaviors in both sexes. This finding could explain why those who decide to engage in subclinical ED behaviors seem to be unaware of potential future adverse consequences (i.e., a clinical diagnosis of an ED). Previous data have revealed that the level of Impulsiveness could predict the subtype of ED; compared to patients with AN, patients with BN generally score higher on N5 (MacLaren & Best, 2009; Podar, Hannus, & Allik, 1999). This may reflect faulty behavioral control in the presence of feelings or attempts to cope with excessive levels of negative affect. In this cohort, high Impulsiveness scores were also significantly associated with both fasting and the use of excessive exercise for weight control in both men and women. Along with the current literature, our results highlight the importance of understanding these impulsive traits in the etiology and progression of EDs, as this Impulsiveness facet has been linked to an increased risk of poor treatment outcomes and worsened long-term prognoses (Claes, Vandereycken, & Vertommen, 2004).
As expected, a larger proportion of women reported ED behaviors compared to men (11.9% versus 8.0%, respectively), and only women reported engaging in all four ED behaviors. Unique to men, more reported ED behaviors were correlated with higher scores on Extraversion. Taken together, our findings indicate that abnormal ED behaviors have important, and likely sex-specific, ties to personality characteristics.
4.1. Strengths/limitations of study
The strengths and limitations of this paper reflect those of the UNCAHS. The study population mirrored the sex ratio of the students at UNC in the 1960s when the cohort was recruited as there were more men than women in the study. Measures were collected at different points in time, thus the personality measurement was, on average, 15 years before the report of the ED behavior engagement. We are limited as we do not know when the reported ED behaviors occurred, or how long they lasted, or even if they were all practiced at the same points in time.
This work was part of a longitudinal observational study of CHD and CHD risk, and ED behaviors were assessed using a single item framed in the context of weight control. This item was added to gauge interest for a potential study devoted to weight loss behaviors and CHD risk. Our past work on weight and personality patterns during midlife also found personality associations by sex for domains of Neuroticism, Extraversion and Conscientiousness (Brummett et al., 2006). Thus, new data on the architecture of ED behaviors would be important to understand the lasting impact later in life of persons with a history of EDs, specifically designed to understand the natural history of EDs and personality as they both change over time.
The UNCAHS is a mail survey and has inherent limitations. Survey data allows for subjective reporting by participants, and self-reports of ED behaviors could not be confirmed within the UNCAHS cohort. Additionally, as the question was asked retrospectively, recall of ED behaviors could be biased by faulty memory or a social desirability bias. The question asked on the UNCAHS survey allowed participants to check “yes” if they have ever engaged in ED behaviors, but did not have participants answer “no”; for the purposes of this study, absence of an answer on the ED behavior question was interpreted as a participant not engaging in those behaviors. The recording of only positive answers represents a limitation to the study since there is no way to distinguish a “no” answer from other negative reasons. Nevertheless, these limitations notwithstanding, by utilizing a large sample within the UNCAHS cohort, the present study was able to investigate the associations of personality and ED behaviors in a homogenous, non-clinical, non-treatment seeking sample.
4.2. Conclusion
Our study found unique, sex-specific patterns of associations between personality domains and facets and reported ED behaviors. Our findings indicated that when measuring personality and considering sub-clinical ED behaviors, a facet-level assessment yields critical information and gives insight into unique personality factors contributing to these behaviors. Thus, by obtaining personality profiles of individuals who exhibit subclinical ED behaviors, it will be possible to gain a better understanding, and potentially help develop a formula for pre-screening, of persons at risk of developing a diagnosis of an ED.
Supplementary Material
Footnotes
Ethics statement
This study utilized data from the UNC Alumni Heart Study, which was approved by the Institutional Review Board at Duke University (Pro00013233). All participants in the longitudinal study were made aware of the risks and benefits associated with the investigation and have signed a written consent to participate.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.appet.2020.104669.
References
- Bollen E, & Wojciechowski FL (2004). Anorexia nervosa subtypes and the big five personality factors. European Eating Disorders Review, 12(2), 117–121. Retrieved from https://onlinelibrary.wiley.com/doi/abs/10.1002/erv.551. [Google Scholar]
- Brummett BH, Babyak MA, Williams RB, Barefoot JC, Costa PT, & Siegler IC (2006). NEO personality domains and gender predict levels and trends in body mass index over 14 years during midlife. Journal of Research in Personality, 40(3), 222–236. 10.1016/j.jrp.2004.12.002. [DOI] [Google Scholar]
- Claes L, Vandereycken W, Luyten P, Soenens B, Pieters G, & Vertommen H (2006). Personality prototypes in eating disorders based on the Big Five model. Journal of Personality Disorders, 20(4), 401–416. 10.1521/pedi.2006.20.4.401. [DOI] [PubMed] [Google Scholar]
- Claes L, Vandereycken W, & Vertommen H (2004). Personality traits in eating-disordered patients with and without self-injurious behaviors. Journal of Personality Disorders, 18(4), 399–404. 10.1521/pedi.18.4.399.40346. [DOI] [PubMed] [Google Scholar]
- Costa PT Jr., & McCrae RR (2008). The revised NEO personality inventory (NEO-PI-R). The SAGE Handbook of personality theory and assessment. Retrieved from http://sk.sagepub.com/reference/hdbk_personalitytheory2 doi: 10.4135/9781849200479. [DOI] [Google Scholar]
- De Bolle M, De Clercq B, Pham-Scottez A, Mels S, Rolland JP, Guelfi JD, & De Fruyt F (2011). Personality pathology comorbidity in adult females with eating disorders. Journal of Health Psychology, 16(2), 303–313. 10.1177/1359105310374780. [DOI] [PubMed] [Google Scholar]
- Donaldson AA, & Gordon CM (2015). Skeletal complications of eating disorders. Metabolism Clinical and Experimental, 64(9), 943–951. 10.1016/j.metabol.2015.06.007. Retrieved from https://ac.els-cdn.com/S0026049515001687/1-s2.0-S0026049515001687-main.pdf?_tid=c3cc80b8-1426-4643-97b8-7ed17283043c&acdnat=1555440530_bd5c22908f0298f42a0cb9c516b388bd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fischer S, Peterson CM, & McCarthy D (2013). A prospective test of the influence of negative urgency and expectancies on binge eating and purging. Psychology of Addictive Behaviors, 27(1), 294–300. 10.1037/a0029323. [DOI] [PubMed] [Google Scholar]
- Goodwin H, Haycraft E, Willis AM, & Meyer C (2011). Compulsive exercise: The role of personality, psychological morbidity, and disordered eating. International Journal of Eating Disorders, 44(7), 655–660. 10.1002/eat.20902. Retrieved from https://onlinelibrary.wiley.com/doi/pdf/10.1002/eat.20902. [DOI] [PubMed] [Google Scholar]
- Herle M, Stavola B, Hubel C, Abdulkadir M, Ferreira DS, Loos RJF, … Micali N (2019). A longitudinal study of eating behaviours in childhood and later eating disorder behaviours and diagnoses. British Journal of Psychiatry, 1–7. 10.1192/bjp.2019.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herzog DB, Hopkins JD, & Burns CD (1993). A follow-up study of 33 subdiagnostic eating disordered women. International Journal of Eating Disorders, 14(3), 261–267. . [DOI] [PubMed] [Google Scholar]
- Levallius J, Clinton D, Backstrom M, & Norring C (2015). Who do you think you are? - personality in eating disordered patients. 3, 3 Journal of Eating Disorders. 10.1186/s40337-015-0042-6. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4359531/pdf/40337_2015_Article_42.pdf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lichtenstein MB, Christiansen E, Elklit A, Bilenberg N, & Stoving RK (2014). Exercise addiction: A study of eating disorder symptoms, quality of life, personality traits and attachment styles. Psychiatry Research, 215(2), 410–416. 10.1016/j.psychres.2013.11.010. Retrieved from https://ac.els-cdn.com/S0165178113007427/1-s2.0-S0165178113007427-main.pdf?_tid=f791293c-92f8-47a4-bec9-de22f0cd271e&acdnat=1549991677_5d008462c6c1a1e915830b082c57daee. [DOI] [PubMed] [Google Scholar]
- Liebman RE, Coniglio KA, Becker KR, Tabri N, Keshishian AC, Wons O, & Thomas JJ (2019). Behavioral inhibition moderates the association between overvaluation of shape and weight and noncompensatory purging in eating disorders. International Journal of Eating Disorders. 10.1002/eat.23195. [DOI] [PubMed] [Google Scholar]
- MacLaren VV, & Best LA (2009). Female students' disordered eating and the big five personality facets. Eating Behaviors, 10(3), 192–195. 10.1016/j.eatbeh.2009.04.001. Retrieved from https://www.sciencedirect.com/science/article/pii/S147101530900035X?via%3Dihub. [DOI] [PubMed] [Google Scholar]
- McCormick LM, Keel PK, Brumm MC, Watson DB, Forman-Hoffman VL, & Bowers WA (2009). A pilot study of personality pathology in patients with anorexia nervosa: Modifiable factors related to outcome after hospitalization. Eating and Weight Disorders, 14(2–3), e113–120. [DOI] [PubMed] [Google Scholar]
- Podar I, Hannus A, & Allik J (1999). Personality and affectivity characteristics associated with eating disorders: A comparison of eating disordered, weight-preoccupied, and normal samples. Journal of Personality Assessment, 73(1), 133–147. 10.1207/s15327752jpa730109. Retrieved from https://www.tandfonline.com/doi/pdf/10.1207/S15327752JPA730109?needAccess=true. [DOI] [PubMed] [Google Scholar]
- Racine SE, Keel PK, Burt SA, Sisk CL, Neale M, Boker S, et al. (2013). Exploring the relationship between negative urgency and dysregulated eating: Etiologic associations and the role of negative affect. Journal of Abnormal Psychology, 122(2), 433–444. 10.1037/a0031250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Marti CN, & Rohde P (2013). Prevalence, incidence, impairment, and course of the proposed DSM-5 eating disorder diagnoses in an 8-year prospective community study of young women. Journal of Abnormal Psychology, 122(2), 445–457. 10.1037/a0030679. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/23148784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tasca GA, Demidenko N, Krysanski V, Bissada H, Illing V, Gick M, et al. (2009). Personality dimensions among women with an eating disorder: Towards reconceptualizing DSM. European Eating Disorders Review, 17(4), 281–289. 10.1002/erv.938. Retrieved from https://onlinelibrary.wiley.com/doi/pdf/10.1002/erv.938. [DOI] [PubMed] [Google Scholar]
- Terracciano A, Sutin AR, McCrae RR, Deiana B, Ferrucci L, Schlessinger D, et al. (2009). Facets of personality linked to underweight and overweight. Psychosomatic Medicine, 71(6), 682–689. 10.1097/PSY.0b013e3181a2925b. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2711222/pdf/nihms-99149.pdf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas JJ, Vartanian LR, & Brownell KD (2009). The relationship between eating disorder not otherwise specified (EDNOS) and officially recognized eating disorders: meta-analysis and implications for DSM. Psychological Bulletin, 135(3), 407–433. 10.1037/a0015326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Touchette E, Henegar A, Godart NT, Pryor L, Falissard B, Tremblay RE, et al. (2011). Subclinical eating disorders and their comorbidity with mood and anxiety disorders in adolescent girls. Psychiatry Research, 185(1–2), 185–192. 10.1016/j.psychres.2010.04.005. [DOI] [PubMed] [Google Scholar]
- Tylka TL, & Subich LM (2002). A preliminary investigation of the eating disorder continuum with men. Journal of Counseling Psychology, 49(2), 273–279. 10.1037/0022-0167.49.2.273. [DOI] [Google Scholar]
- Wenzel KR, Weinstock J, Vander Wal JS, & Weaver TL (2014). Examining the role of negative urgency in a predictive model of bulimic symptoms. Eating Behaviors, 15(3), 343–349. 10.1016/j.eatbeh.2014.04.014. [DOI] [PubMed] [Google Scholar]
- Whiteside SP, & Lynam DR (2001). The five factor model and impulsivity: Using a structural model of personality to understand impulsivity. Personality and Individual Differences, 30(4), 669–689. 10.1016/s0191-8869(00)00064-7. [DOI] [Google Scholar]
- Widiger TA, & Costa PT Jr. (2012). Integrating normal and abnormal personality structure: The five-factor model. Journal of Personality, 80(6), 1471–1506. 10.1111/j.1467-6494.2012.00776.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are not publicly available due to the issues needed to protect confidentiality of the respondents. Data can be shared on the basis of negotiated agreements with Dr. Siegler, PI of UNCAHS.