

Abstract
Background:
Life events experienced during adolescence are associated with risk and resilience to heavy episodic drinking (HED; i.e., binge drinking). The current study builds on prior research using latent class analysis (LCA) to examine heterogeneity in patterns of adolescent life events at baseline to HED over the course of three years (4 timepoints) as part of the National Consortium on Alcohol and Neurodevelopment in Adolescence (NCANDA).
Methods:
Life event classes were modeled using LCA that characterized NCANDA participants based upon their responses to the Life Events Questionnaire (N = 467, age: M = 14.98, SD = 1.69, 49.7% female). These baseline latent life event classes were then compared to HED at baseline and years 1, 2 and 3 using multinomial logistic regression.
Results:
At baseline, the LCA characterized four classes of adolescents based on endorsement of life events: negative-relational conflict (n = 65, 13.9%), negative-financial problems (n = 49, 10.5%), low life events (n = 130, 27.8%), and positive life events (n = 223, 47.8%). Life event trajectories differed for the negative life event classes compared to the other two classes, with greater odds of HED in the negative-financial problems class at year 1.
Conclusion:
The four latent classes derived from the life events of NCANDA youth yielded a characterization of adolescents that could aid in understanding HED over the subsequent three years, suggesting that everyday life events may inform adolescent binge drinking.
Keywords: adolescence, life events, binge drinking, heavy episodic drinking, alcohol, latent class analysis
Introduction
A substantial body of literature has shown that serious negative life events (e.g., child abuse and neglect) can increase risk of heavy episodic drinking (HED; i.e., binge drinking) during adolescence (Anda et al., 2002; Dube et al., 2002, 2006; Keyes et al., 2012; Lee et al., 2012; Pilowsky et al., 2009; Schellekens et al., 2013; Strine, 2012; Timko et al., 2008). It has been estimated that 57.8% of adolescent alcohol is consumed as HED (Esser et al., 2017). HED is a high-risk form of alcohol use where the blood alcohol concentration exceeds the legal limit for driving (.08 grams percent or above in many states) in a short duration (often less than 2 hours; Esser et al., 2017). This rate of HED in adolescents far exceeds the 17.1% rate of HED in adults and has serious consequences (Kanny et al., 2018). Nearly 200,000 emergency room visits per year for people under the age of 21 years are due to alcohol related injuries associated with HED (Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality (SAMHSA), 2012). HED in adolescence has been reported to have unique risks that extend into adulthood including increased alcohol use disorders, suicide, violence, memory and learning problems, unintentional injuries, and other physical and mental health problems (Centers for Disease Control and Prevention (CDC), 2010; De Bellis et al., 2014; Kanny et al., 2018).
Adults retrospectively reporting more everyday negative life events during adolescence, such as family financial problems, conflict among parents or caregivers, and parental job loss, also reported more high-risk alcohol use, including HED (Chassin et al., 2002; Courtney and Polich, 2009; Hill et al., 2000; Naimi et al., 2003; Schulenberg et al., 1996; Wechsler, 1994). Other retrospective studies of adults also reported that greater exposure to negative life events during adolescence increased the odds of developing alcohol use disorder in adulthood (Anda et al., 2002; Anderson et al., 2010; Wu et al., 2010). Teens with negative life events have been found to be more than twice as likely to engage in high-risk substance use as compared to adolescents without negative life events (Chassin et al., 2002; Lee et al., 2012); however, positive life events were not examined. In addition, negative life events such as, family financial problems and relational conflict have been associated with higher rates of substance use and internalizing and externalizing problem behaviors in cross sectional research (Lewis et al., 2011; Thompson et al., 2012). Given the pervasiveness and seriousness of HED among adolescents and the impact of negative life events on adult alcohol use, prospective research aimed at identifying factors pertaining to prevention in adolescents is imperative.
Prior research on everyday life events and substance use in adolescence has tended to focus on the impact of negative life events (Lee et al., 2012; Myers et al., 2014), while fewer studies examine positive life events (Masten et al., 2004) and even fewer have examined both (for review see Masten, 2011). In studies examining the role positive life events to alcohol use, adolescents with more positive achievements in school and extracurricular activities as well as more favorable peer, community and familial relations reported lower rates of HED (Hemphill et al., 2011; Stone et al., 2012). Positive life events such as academic or athletic achievements as well as awards in and outside of school have been related to lower rates of HED and related problem behaviors among 11–14-year-olds (Traube et al., 2012). However, studies have yet to link positive and negative life events together to HED longitudinally during adolescence.
Models of resilience have emphasized the importance of identifying positive influences on adolescent development without ignoring risks. Resilience theory has posited that seemingly opposing components have to be considered to effectively identify adolescents who make healthy choices pertaining to HED despite adversity (Masten, 2011). Regardless of perceiving or experiencing risk or reward, the adolescent positively adapts (Luthar and Cicchetti, 2000). However, the mechanisms linking risk or threat to resilience (i.e., not engaging in HED) are largely unknown (Masten and Tellegen, 2012). Therefore, measuring positive life events along with the negative, while factoring in individual characteristics of the adolescent, such as socioeconomic status and family history, is needed to effectively characterize risk and resilience for engaging in HED during adolescence (Luthar and Cicchetti, 2000; Masten, 2011).
The present study begins to address these questions by prospectively and longitudinally examining classes of life events and their relation to HED in the National Consortium on Alcohol and Neurodevelopment in Adolescence (NCANDA) sample. This longitudinal multi-site study is currently following 831 adolescents starting at age 12–21 to identify neural mechanisms that contribute to alcohol use problems across development (Brown et al., 2015). A core dimension of NCANDA involves the ways in which life events contribute to psychobiological risk or resilience for engaging in HED during adolescence.
In this study we used a multivariate statistical approach, latent class analysis (LCA) to characterize patterns of life events among adolescents. This approach allows for identification of meaningful subgroups based on adolescent report of life events (Henry and Muthén, 2010; Nylund et al., 2007). Latent class approaches are advantageous because they generate empirically-determined groupings of individuals based on shared patterns of responses that, while potentially heterogeneous in the full sample, are more uniform within the latent classes. Latent class approaches have become a more common way to explore complex clustering of heterogeneous constructs (Berzenski and Yates, 2011; Nooner et al., 2010), particularly those with a range of valences (Mehta et al., 2013); however, it has not been applied to examine life events and HED longitudinally in adolescents.
Latent class approaches have been applied to studies of trauma exposure and problem behaviors in national samples of adolescents (e.g., Ford et al., 2010; Nooner et al., 2010). Results provided evidence that adolescents who are in latent classes that are indicative of trauma are at increased risk of developing problem behaviors (i.e., internalizing and externalizing symptoms) and have distinct mental health outcomes and demographic characteristics compared to adolescents in other latent classes (Berzenski and Yates, 2011; Mehta et al., 2013) While HED was not examined in these studies, it is worthy of further study as HED has profound lifelong consequences, which first emerge during adolescence (e.g., Anderson et al., 2010; Bekman et al., 2011; Chassin et al., 2013; Clark et al., 1997; Hill et al., 2000).
The current study employed LCA in conjunction with the NCANDA cohort-sequential sample to characterize adolescent life events. This multivariate characterization of life events at baseline was then used to examine HED at four study timepoints: baseline, year one, year two and year three. Developmental traumatology theory posits that serious negative life events contribute to trajectories of psychopathology and that low rates of HED among youth who experience negative life events could be considered resilience (De Bellis, 2002). Taking this theoretical model into account, we hypothesized that adolescents with baseline life events involving more negative events would have more instances of binge drinking at baseline and across the next three years. We hypothesized sex differences such that males with more negative life events would have more binge drinking at each time point compared to females in the same class. We hypothesized that protective factors, such as adolescents in LCA classes with more academic achievements would have lower rates of binge drinking at baseline and over the next three years. Last, we hypothesized that resilient youth were those who had more negative life events and yet had low rates of HED over the next three years.
Methods
Participants & Procedures
The analyses focused on longitudinal phenotypic data collected at the five NCANDA sites (University of California San Diego, Duke University Medical Center, Oregon Health and Science University, SRI International, University of Pittsburgh). A summary of descriptive statistics for the sample can be found in Table 1. (Brown et al., 2015). Institutional review board approval was obtained at each study site. Minors provided written assent along with parent/legal guardian consent and adults consented before participating.
Table 1.
Descriptive statistics at baseline for NCNADA sample used in latent class analysis (N = 467).
| Variable | Mean | SD | |
|---|---|---|---|
| Age in Years | Baseline Range: 12–17.99 | 14.98 | 1.69 |
| HED (Binge Drinking) | Baseline Range: 0–52 | 0.32 | 2.66 |
| Year 1 Range: 0–43 | 0.85 | 3.69 | |
| Year 2 Range: 0–106 | 3.24 | 10.83 | |
| Year 3 Range: 0–90 | 4.80 | 13.22 | |
| Variables at Baseline | N | % | |
| Sex | Male | 235 | 50.3% |
| Female | 232 | 49.7% | |
| Total | 467 | 100.0% | |
| Ethnicity | Native American / American Indian | 1 | 0.2% |
| Asian | 29 | 6.2% | |
| Pacific Islander | 3 | 0.6% | |
| African-American / Black | 52 | 11.1% | |
| Caucasian / White | 333 | 71.3% | |
| Other | 49 | 10.5% | |
| Total | 467 | 100.0% | |
| SES - Parental Education |
6th grade | 1 | 0.2% |
| 8th grade | 3 | 0.6% | |
| 9th grade | 1 | 0.2% | |
| 10th grade | 2 | 0.4% | |
| 11th grade | 1 | 0.2% | |
| 12th grade | 22 | 4.7% | |
| 1 year of college | 12 | 2.6% | |
| 2 years of college | 27 | 5.8% | |
| 3 years of college | 12 | 2.6% | |
| 4 years of college | 143 | 30.6% | |
| 1 year of graduate or professional school | 23 | 4.9% | |
| 2 years of graduate or professional school | 102 | 21.8% | |
| 3 years of graduate or professional school | 19 | 4.1% | |
| 4+ years of graduate or professional school | 99 | 21.2% | |
| Total | 467 | 100.0% | |
A complete data approach was used, requiring participants to complete life events questions at baseline as well as the HED questions at baseline and years 1, 2, and 3. In these analyses, NCANDA participants who were 18-years-old or older at baseline were excluded due to the focus on adolescence. This meant that there were 467 adolescents available for the LCA using the three-step approach with multinomial logistic regression to look at HED over time. There were no statistically significant differences in terms of age, sex, ethnicity, site, or parental education, which was used as an indicator of socioeconomic status, between the adolescents who did and did not complete the life events questionnaire at baseline (all t-tests < 1.5, p-values >.05). Less than 5% of the data were missing and all were missing at random. There were not statistical differences in the aforementioned demographic characteristics for those with missing data versus those without (all t-tests < 1.0, p-values > .1). For missing data, we used the full information maximum likelihood (FIML) approach in Mplus (Graham et al., 2012). The sample of N = 467 included in the analyses thus reflected the larger NCANDA sample in socio-demographics (see Brown et al., 2015).
Measures
The NCANDA core phenotypic battery consisted of a comprehensive assessment of alcohol and substance use, mental health symptoms and diagnoses, and functioning across a range of domains including neuropsychiatric testing. For a full description of the NCANDA battery and details of the accelerated longitudinal design see Brown et al., 2015. The measures utilized for the present study are described in more detail below: The Life Events Questionnaire and Customary Drinking Drug Use Record.
The Life Events Questionnaire (LEQ: Masten et al., 1994) was collected at the baseline assessment. This is a 61-item binary (yes = 1/no = 0) scale that was designed to measure a spectrum of positive and negative life events in adolescents and young adults. For an item in the LEQ to be included in the LCA, responses to that item had to exhibit substantive variation in the sample (Henry and Muthén, 2010; Nylund et al., 2007). Forty-seven items had a mean and standard deviation at or close to zero (i.e., <0.1) and hence were not sufficiently endorsed to be useful for differentiation in the LCA. These items were thus excluded from analyses. The 14 items of the LEQ were used for the latent class analysis are displayed in Table 3. Of these 14 items, five items had a positive valence (i.e., outstanding achievement, leadership, academic award, award outside of school, athletic achievement) and nine had negative valence (i.e., death grandparent, parent work problem, parent lost job, family financial problem, argue with siblings, argue with parents, argue about friends, adults argue, broke up with romantic relationship).
Table 3.
Item-Response Probabilities for the 4-Class Model (N = 467).
| Item | Negative RC | Negative FP | Low | Positive |
|---|---|---|---|---|
| 1. Death Grandparent | 0.187 | 0.047 | 0.145 | 0.078 |
| 2. Outstanding Achieve. | 0.843 | 0.867 | 0.606 | 0.921 |
| 3. Leadership | 0.447 | 0.330 | 0.106 | 0.563 |
| 4. Academic Award | 0.549 | 0.342 | 0.260 | 0.776 |
| 5. Award Outside School | 0.545 | 0.177 | 0.095 | 0.732 |
| 6. Athletic Achievement | 0.348 | 0.196 | 0.068 | 0.618 |
| 7. Parent Work Problem | 0.171 | 0.608 | 0.031 | 0.068 |
| 8. Parent Lost Job | 0.180 | 0.458 | 0.123 | 0.153 |
| 9. Family Finance Problem | 0.422 | 0.753 | 0.084 | 0.100 |
| 10. Argue with Siblings | 0.687 | 0.143 | 0.200 | 0.210 |
| 11. Argue with Parents | 0.899 | 0.259 | 0.122 | 0.053 |
| 12. Argue About Friends | 0.487 | 0.158 | 0.046 | 0.024 |
| 13 Adults Argue | 0.364 | 0.413 | 0.000 | 0.044 |
| 14. Broke-up Romantic | 0.448 | 0.256 | 0.117 | 0.216 |
| Class Prevalence |
13.9% n = 65 |
10.5% n = 49 |
27.8% n = 130 |
47.8% n = 223 |
RC = Relational Conflict; FP = Financial Problems.
Heavy episodic drinking (i.e., binge drinking) at baseline, year one, year two and year three was measured continuously with the Customary Drinking and Drug Use Record (CDDR; Brown et al., 1998), which asks, “During the past year, how many times have you consumed 4+ (females) / 5+ (males) drinks within an occasion?” To control for known potential factors that would led to risk/resilience, age, sex, parental highest level of education as an indicator of socioeconomic status, ethnicity, and family alcohol density were measured as described in Brown et al. (2015).
Statistical Analysis
The purpose of this study was to identify classes of adolescents in the NCANDA sample based upon self-report of life events at baseline and then to investigate these classes as a basis for examining longitudinal predictors of transition to HED at baseline and at years one through three. To assess class differences in life events, the three-step approach was used (Nylund-Gibson et al., 2014). Baseline life events were input into a LCA using Mplus version 8 (Muthén and Muthén, 2017). The goal of using LCA models was to identify underlying categorical latent variables capturing between-subject heterogeneity in response patterns about life events (Henry and Muthén, 2010). We then classified subjects into groups based on the posterior probability of class membership given their responses to the LEQ. At that point models with adequate fit were evaluated using model selection metrics. These metrics included: the Negative 2 Log-Likelihood, the Akaike Information Criteria, the Bayesian Information Criteria, the Adjusted Bayesian Information Criteria, the -Mendell-Rubin Adjusted Likelihood Ratio Test, the Lo-Mendell-Rubin Test, the Bootstrapped Log-Likelihood Ratio Test, and the Likelihood Ration Chi-Square (Henry and Muthén, 2010). After choosing the best model according to the above criteria, the classes comprising this model were named. These terms were not based on numeric cutoffs but were used as general descriptors for the overall pattern of life event responses for adolescents in a given class.
The three-step approach was used to prevent the classes from shifting as predictors and outcomes were added. In the first step as described above, the LCA model was estimated as a measurement model. In the second step, posterior probabilities from the first step were used to represent class assignments. In the third step, a multinomial logistic regression model was fit using the classes from the first step and the posterior probabilities from the second step (Kamata et al., 2018). To assess class differences on binge drinking longitudinally (i.e., baseline, year 1, year, 3, and year 3), we ran a multinomial logistic regression model while accounting for covariates. In this model, age, sex, ethnicity, socioeconomic status (parent’s highest education), and family alcohol density measured at baseline, were included as covariates. Models also controlled for baseline HED. Mplus version 8.0 with maximum likelihood estimator with robust standard errors for missing data was used to fit models (Muthén and Muthén, 2017).
Results
Descriptive statistics for the 467 adolescents included in the LCA models are found in Table 1.
LCA Models of LEQ:
The latent class models were fit for one through five classes using 14-tems from the Life Events Questionnaire (see Tables 2 and 3). The log likelihood was replicated for models one through four but was not replicated for model five indicating that the five class model may not be trustworthy because the results could not be replicated. The two class solution created positive and negative life events classes but was an overall poorer fit than the three or four class models (see Table 2). The three and four class models resulted in more nuanced class structure than the two class model and had overall better fit; they are therefore compared herein.
Table 2.
Fit and class separation statistics for LCA models of life events items at baseline for NCANDA sample (N = 467) with one through two through five latent classes.
| Class | −2LL | AIC | BIC | aBIC | Pearson χ2 | Entropy | LMRT | BLRT | LRχ2 | χ2 p-value |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | −4146.36 | 8320.71 | 8381.46 | 8337.01 | 3675.56 | -- | -- | -- | 1448.25 | -- |
| 2 | −4005.95 | 8069.90 | 8195.72 | 8103.66 | 4974.39 | 0.677 | 277.892 | −4146.36 | 1535.45 | .0062 |
| 3 | −3902.22 | 7892.44 | 8083.34 | 7943.66 | 4811.77 | 0.672 | 205.302 | −4005.95 | 1351.77 | .0063 |
| 4* | −3871.84 | 7861.68 | 8117.66 | 7930.36 | 4152.37 | 0.739 | 160.131 | −3902.22 | 1288.96 | <.001 |
| 5^ | −3851.38 | 7850.76 | 8171.82 | 7936.90 | 4052.56 | 0.763 | 140.491 | −3871.84 | 1287.00 | .0563 |
Note. −2LL = Negative 2 Log-Likelihood; AIC = Akaike Information Criteria; BIC = Bayesian Information Criteria; aBIC = Adjusted Bayesian Information Criteria; LMRT = Lo-Mendell-Rubin Adjusted Likelihood Ratio Test; LMRT = Lo-Mendell-Rubin Test; BLRT = Bootstrapped Log-Likelihood Ratio Test; LRχ2 = Likelihood Ration Chi-Square.
= best fitting model based on fit and interpretability.
= the model log likelihood value was not replicated.
In comparing the three and four class solutions in Table 2, the four class model had lower values for all fit statistics except the Bayesian Information Criteria when compared to the three class model. The four class model also higher entropy than the three class model, which indicates higher quality of class separation (Muthén and Muthén, 2017). The chi-square difference test for the three versus the four-class solution was statistically significant (p < .05), favoring the four class model. The chi-square difference test was not significant when comparing the four class model to the five class model, indicating that the more parsimonious four-class model was the better fit. Taken together, we decided that the four class model had the best fit and present the results from that model.
Four Class LCA Model:
Visual inspection of probability loadings for the four-class model supported it as having the best overall fit and interpretability (see Tables 2 & 3, Figure 1). The first class in the four-class model, termed ‘Negative - Relational Conflict’ (Negative-RC, 13.9% of sample, n = 65), consisted of NCANDA adolescents who had the highest probabilities of endorsing items pertaining to arguing or having conflict with family members and friends and breaking up as compared to the three other classes. The second class, termed ‘Negative - Financial Problems’ (Negative-FP, 10.5%, n = 49), had the highest probabilities of endorsing items pertaining to parent work problems and financial difficulties. The third class, termed ‘Low Life Events’ (Low; 27.8%, n = 130) had a mix of positive and negative life events with lower probabilities across all life event items compared to the other classes. The fourth class, termed ‘Positive Life Events,’ (47.8%, n = 223) had the highest probability of endorsing items pertaining to leadership, achievement, and academic and non-academic awards.
Figure 1.
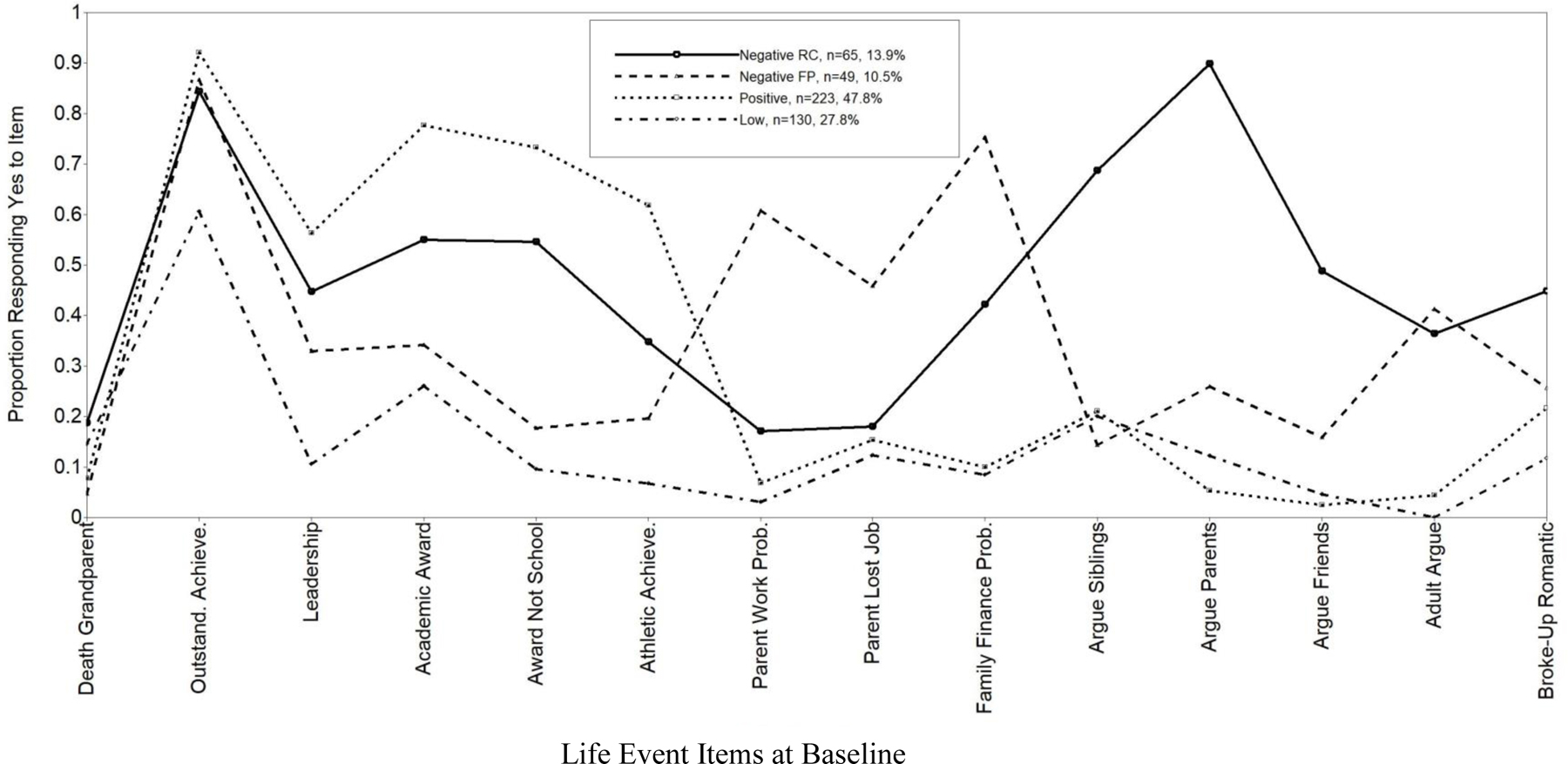
The 14-life event questionnaire items used in the present latent class analysis are on the x-axis and the probability of a particular class answering “yes” to an item on the life event questionnaire is represented on the y-axis (N = 467). Key located within table that indicates the percent of NCNADA youth each of the classes. RC = Relational Conflict; FP = Financial Problems.
Multinomial Logistic Regression:
The four-class LCA model was then used as a predictor of binge drinking in a follow up multinomial logistic regression model across four time points: baseline, year 1, year 2, and year 3. Covariates included in the models were age, sex, ethnicity and SES (parent’s highest education) and family alcohol density measured at baseline. The model also controlled for baseline HED. Table 4 depicts the odds ratios for each of the binge drinking years as well as the covariates. The largest class, the Positive life events class, was the comparison group throughout. Adolescents in the Negative – Relational Conflict were significantly less likely to engage in binge drinking at baseline than the Positive life events class (OR = .585, p<.001) . However, at year 1, youth in the Negative – Family Financial class were more likely to engage in binge drinking that the positive class (OR = 1.105, p <.05). There were not statistically significant differences on the baseline covariates (i.e., age, sex, ethnicity, SES, and family alcohol density). A model that used the covariates to predict the classes and then predict HED was also not statistically significant (OR = 0.00 – 0.14, p’s >.2).
Table 4:
Life evens class differences in adolescent HED from baseline to year 3 with covariates. Positive class (the largest class; n = 223, 47.8%) is the reference.
| 1. Negative – Relational Conflict (n = 65, 13.9%) | 2. Negative – Family Financial (n = 49, 10.5%) | 3. Low Life Events (n = 130, 27.8%) | Pairwise comparisons | ||||
|---|---|---|---|---|---|---|---|
| Est. (SE) | OR | Est. (SE) | OR | Est. (SE) | OR | p < 0.05 | |
| Covariates | |||||||
| Age | 0.095 (0.088) | 1.100 | −0.159 (0.100) | 0.853 | −0.081 (0.070) | 0.922 | |
| Sex | −0.345 (0.301) | 0.708 | 0.041 (0.330) | 1.042 | 0.243 (0.229) | 1.275 | |
| Ethnicity | 0.031 (0.105) | 1.032 | −0.101 (0.125) | 0.904 | −0.146 (0.087) | 0.864 | |
| SES | −0.053 (0.056) | 0.948 | 0.010 (0.069) | 1.010 | 0.027 (0.050) | 1.027 | |
| Baseline HED | −0.483 (0.853) | 0.617 | −0.812 (0.934) | 0.444 | −0.536 (0.557) | 0.585 | |
| Fam. Hist. Alcoholism | −0.512 (0.617) | 0.600 | −1.201 (0.688) | 0.301 | −0.033 (0.272) | 0.967 | |
| HED | |||||||
| Baseline | −0.537** (0.187) | 0.585 | 0.003 (0.114) | 1.003 | 0.064 (0.038) | 1.066 | 1 < 2, 3, 4 |
| Year 1 | 0.090 (0.061) | 1.094 | 0.100* (0.049) | 1.105 | −0.003 (0.046) | 0.997 | 1, 2 > 3, 4 |
| Year 2 | −0.014 (0.027) | 0.986 | −0.002 (0.022) | 0.998 | 0.022 (0.015) | 1.022 | |
| Year 3 | −0.015 (0.020) | 0.986 | −0.037 (0.035) | 0.964 | −0.005 (0.012) | 0.995 |
Note: Models account for age, sex, ethnicity, SES, baseline HED, and family history of alcoholism. Sample sizes for each class are based on modal assignment using posterior probability of class membership.
p < 0.05
p < 0.01
p < 0.001.
Discussion
This longitudinal study with the NCANDA sample characterizes a range of positive and negative life events to aid in understanding adolescent HED over the course of three years. We used a multivariate statistical approach, which yielded four latent classes of life events at baseline. The four-class structured derived from the LCA included: (1) a Negative-Relational Conflict class that had the highest proportion of adolescents responding affirmatively to life event items pertaining to family conflict, (2) a Negative-Financial Problems class that had the highest proportion of adolescents responding affirmatively to items pertaining to financial difficulties in the family, (2) a Low life event class that had a range of positive and negative life events with overall lower endorsement across all types of life events, and (4) a Positive life event class that had the highest proportion of adolescents responding affirmatively to items related to achievements and awards.
Our hypothesis pertaining to negative life events being related to more occurrences of HED was partially supported. Adolescents in the Negative-Financial Problems class reported more binge drinking than the Positive life events class at year 1. However, these results were not seen at years 2 and 3. Risk factors can change over time. It is still useful to see where these risks emerge and for whom to develop the best targeted intervention and prevention strategies. Given that the NCANDA study is ongoing, it could prove useful to follow these trajectories into young adulthood when youth may have more independence and financial means to purchase alcohol.
We also hypothesized that males who experienced more negative life events would have more HED than females but we did not find any effects for sex at any of our time points. This does not mean that sex differences do not exist in relation to HED. It may mean that the everyday life events explored in this study may not be a key indicator of sex differences in relation to HED.
Our hypothesis that adolescents with more positive life events, such as those represented in the Positive life events class, would have lower rates of binge drinking at baseline and over the next three years was partially supported longitudinally. At year 1, adolescents in the Positive class had lower odds of engaging in HED than Negative – Relational Conflict class. However, adolescents in the Positive class similar odds of binge drinking at years 2 and 3. This finding has been reflected in the literature in that adolescents engaging in sports events commonly engage in alcohol use, athletic achievement was one of the positive life events in the latent class analysis (Kwan et al., 2014; Sønderlund et al., 2014). Since NCANDA is a normative sample, it is important to note that these differences in HED are relative differences and that overall the rates of HED in the NCANDA sample are low. These features of the HED in the sample could have influenced the multinomial logistic regression analysis. Longitudinal results pertaining to the higher rates for the Negative – Family Financial class at year 1 correspond to prior retrospective reports of adults (Anderson et al., 2010; Dube et al., 2002) as well as cross sectional findings of HED in adolescence (Chassin et al., 2002; Clark et al., 1997; Courtney and Polich, 2009). Differences may not have been as pronounced as in those studies because the NCANDA sample is a community sample whereas those studies were primarily in clinical samples, which tend to have higher rates of HED (Bekman et al., 2013; Hill et al., 2000). The observed relationship of life event classes to HED at year 1 could have implications for prevention and intervention research. Specifically, it could point to a differential approach for HED prevention and intervention for adolescents who may initiate HED for reasons related to family financial difficulties, which is common in adolescence (Chung et al., 2016). Also, it speaks to the need to follow this cohort through young adulthood to see if trajectories mirror clinical samples or follow a different pattern, which the NCANDA study has the capacity to do.
Last, our hypothesis that resilient youth defined as adolescents who had more negative life events and yet had lower rates of HED over the next three years was not supported overall. Youth in the Negative – Relational Conflict class had lower HED at baseline but had comparable HED to the other classes as years 1, 2, and 3. It would be overstating the present results to say that negative life events somehow confer resilience to HED. The present study focuses on the ways in which everyday life events in the latent classes may relate to HED but life events is only one of many factors that may contribute to HED. While everyday life events may not have related to HED in exactly the manner expected, such as is the case with trauma and adverse childhood experiences (De Bellis, 2002; Dube et al., 2002; Timko et al., 2008), it is still worth exploring due to the fact that everyday life events are pervasive in adolescents’ lives (Clark et al., 1997; Lee et al., 2012). The adolescents in the Negative classes may have other factors, such as financial limitations in the family, preventing them from attending social situations where adolescents typically have access to alcohol and that may contribute to the observed lower rates of binge drinking and were beyond the scope of the present investigation. In addition, the Negative classes were the smallest classes and results require replication with other large-scale samples and/or further analysis over longer intervals to determine implications of positive and negative life events on adolescent HED.
These results illustrate the value of multidimensional characterizations to find novel and nuanced relationships between the contribution of everyday events and complex developmental constructs such as adolescent engagement in HED over time. Adolescents who were in the Negative – Relational Conflict class at baseline were found to have lower odds of engaging in HED than the other classes at baseline, followed by comparable odds at the later years. This suggests that there may be different pathways for alcohol use behavior versus other problematic behaviors during adolescence and that adolescent HED may not necessarily be linearly linked to negative everyday life events. HED may be a more heavily influenced by socially constructed pathway in adolescences (Chung et al., 2016) as well as by trauma (Anda et al., 2002; De Bellis, 2002; Timko et al., 2008). We expected to see sex differences with boys having more HED than girls but we did not see that. Still, in examining patterns of risk and resilience to HED, sex should be examined in the NCANDA sample as additional factors, including those related to trauma, will become available as the data is collected in future years. It will be important to see how a latent class structure of life events that also includes trauma-related factors may be related to HED patterns at years four and five when this sample enters the peak developmental period for this high-risk behavior.
While the present study has strengths including a large, prospective, sample of adolescents and a multivariate statistical approach, it had some limitations that should be noted. First, because we sought to classify a latent independent variable with a dependent count variable at 4 timepoints while accounting for key covariates, we were not able to do the analysis in one step. While the present results are accurate, trajectory-based approaches could be explored in the future. Also, the latent class analysis was based on one measure of life events. This means that the results are limited to the items used. In addition, cognitive factors related to life events, such as perceived intensity or controllability, were not measured in the present study but could be included in future research. Future analyses with different variability assumptions could also be designed to evaluate all responses of the LEQ. Additionally, in the second wave of the NCANDA consortium (NCANDA-2), the World Health Organization’s Adverse Childhood Experiences Questionnaire and the Childhood Trauma Questionnaire were added at all sites to increase the depth and breadth of life event and trauma related information within the sample (Bellis et al., 2014; Fink et al., 1995). While data from these measures were not available for the present study, they will be included in future models.
As dictated by our latent class analysis approach, life events were characterized at baseline, but we recognize that additional positive and negative life events continue to occur during adolescence. Future analyses could examine the interplay of HED and life events more dynamically over time. This will be possible in upcoming work when the sample ages into the early twenties and base rates of HED peak (Chassin et al., 2002). In addition, while the present study controlled for family history of alcohol use and baseline HED in the years 1–3, it did not explicitly evaluate the role of other substances such as marijuana, which can be associated with alcohol use (De Bellis et al., 2013; Primack et al., 2009). While this was beyond the scope of the present paper focused on life events and HED, other substances could be evaluated in future research.
These results inform public policy in that everyday life negative life events that may confer risk for HED should be targeted in prevention programs. Prevention programs tend to focus on social risk factors (e.g., peer pressure) while putting less evidence on family factors that are not directly tied to alcohol or substance use (e.g., arguing with adults). However, this study has provided preliminary support for these everyday negative life events playing a role in HED. Given the prevalence of HED during adolescence, targeting everyday negative life events that pertain to family stability (e.g., parental work problems) but are not directly tied to alcohol use per se, may be important for helping vulnerable youth make healthy choices when it comes to alcohol. Similarly, from a clinical practice perspective, these findings suggest that clinicians working with adolescents should include HED assessments in treatment plans regardless of the presenting problem as it is a common problem behavior that is tied to everyday life events experienced by many adolescents regardless of the issue that may have brought them into treatment.
This work takes a step forward in prospectively examining the ways in which life events may confer risk and resilience for engaging in HED in adolescence over the course of three years. The present findings illustrate that adolescents who report more negative life events are less likely to engage in HED at baseline but more likely to engage in HED later on (Nusslock and Miller, 2016). This illustrates the importance of taking longitudinal approaches to studying the development and maintenance of high-risk behaviors like HED, as it is common for them to change over time. While everyday negative life events confer greater risk at some timepoints, risk for those with more everyday negative life events is comparable to those without at other time points. This does not mean that risk has disappeared, rather it illustrates that there are a host of factors that change throughout development to confer risk and resilience to HED. Everyday life events are just one predictor and future models should include dimensions of life events that target more serious trauma and abuse, which will be available in upcoming years of NCADNA. Unraveling complex longitudinal relationships such as those between life events and HED is a needed step forward in developing evidence-based strategies to foster healthy adolescent development.
Acknowledgments
Funding sources: Reported data was obtained from the multisite National Consortium on Alcohol & Neurodevelopment in Adolescence (NCANDA) study, which is supported by the U.S. National Institute on Alcohol Abuse and Alcoholism with co-funding from the National Institute on Drug Abuse, the National Institute of Mental Health, and the National Institute of Child Health and Human Development grant numbers: AA021697 (Pfefferbaum and Pohl), AA021695 (Brown and Tapert), AA021692 (Tapert), AA021696 (Colrain and Baker), AA021681 (De Bellis), AA021690 (Clark), and AA021691 (Nagel).
Footnotes
Disclosure: There are no conflicts of interest.
References
- Anda RF, Whitefield CL, Felitti VJ, Chapman D, Edwards VJ, Dube SR, and Williamson D (2002). Adverse childhood experiences, alcoholic parents, and later risk of alcoholism and depression. Psychiatr. Serv [DOI] [PubMed]
- Anderson KG, Ramo DE, Cummins KM, and Brown SA (2010). Alcohol and drug involvement after adolescent treatment and functioning during emerging adulthood. Drug Alcohol Depend 107, 171–181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bekman NM, Anderson KG, Trim RS, Metrik J, Diulio AR, Myers MG, and Brown SA (2011). Thinking and drinking: Alcohol-related cognitions across stages of adolescent alcohol involvement. Psychol. Addict. Behav 25, 415–425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bekman NM, Winward JL, Lau LL, Wagner CC, and Brown SA (2013). The impact of adolescent binge drinking and sustained abstinence on affective state. Alcohol Clin Exp Res 37, 1432–1439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bellis MA, Hughes K, Leckenby N, Jones L, Baban A, Kachaeva M, Povilaitis R, Pudule I, Qirjako G, Ulukol B, et al. (2014). Adverse childhood experiences and associations with health-harming behaviours in young adults: surveys in eight eastern European countries. Bull. World Health Organ 92, 641–655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berzenski SR, and Yates TM (2011). Classes and Consequences of Multiple Maltreatment: A Person-Centered Analysis. Child Maltreat 16, 250–261. [DOI] [PubMed] [Google Scholar]
- Brown SA, Myers MG, Lippke L, Tapert SF, Stewart DG, and Vik PW (1998). Psychometric evaluation of the Customary Drinking and Drug Use Record (CDDR): a measure of adolescent alcohol and drug involvement. J. Stud. Alcohol 59, 427–438. [DOI] [PubMed] [Google Scholar]
- Brown SA, Brumback T, Tomlinson K, Cummins K, Thompson WK, Nagel BJ, De Bellis MD, Hooper SR, Clark DB, Chung T, et al. (2015). The National Consortium on Alcohol and NeuroDevelopment in Adolescence (NCANDA): A Multisite Study of Adolescent Development and Substance Use. J. Stud. Alcohol Drugs 76, 895–908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) (2010). Alcohol-Related Disease Impact (ARDI) (Atlanta, GA: CDC; ). [Google Scholar]
- Chassin L, Pitts SC, and Prost J (2002). Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: predictors and substance abuse outcomes. J. Consult. Clin. Psychol 70, 67–78. [PubMed] [Google Scholar]
- Chassin L, Sher KJ, Hussong A, and Curran P (2013). The developmental psychopathology of alcohol use and alcohol disorders: Research achievements and future directions. Dev. Psychopathol 25, 1567–1584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chung T, Creswell KG, Bachrach R, Clark DB, and Martin CM (2016). Adolescent binge drinking: Developmental context and opportunities for prevention. Alcohol Res. Curr. Rev [PMC free article] [PubMed]
- Clark DB, Lesnick L, and Hegedus AM (1997). Traumas and Other Adverse Life Events in Adolescents With Alcohol Abuse and Dependence. J. Am. Acad. Child Adolesc. Psychiatry 36, 1744–1751. [DOI] [PubMed] [Google Scholar]
- Courtney KE, and Polich J (2009). Binge drinking in young adults: Data, definitions, and determinants. Psychol. Bull 135, 142–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Bellis MD (2002). Developmental traumatology: a contributory mechanism for alcohol and substance use disorders. Psychoneuroendocrinology 27, 155–170. [DOI] [PubMed] [Google Scholar]
- De Bellis MD, Wang L, Bergman SR, Yaxley RH, Hooper SR, and Huettel SA (2013). Neural mechanisms of risky decision-making and reward response in adolescent onset cannabis use disorder. Drug Alcohol Depend 133, 134–145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dube SR, Anda RF, Felitti VJ, Edwards VJ, and Croft JB (2002). Adverse childhood experiences and personal alcohol abuse as an adult. Addict. Behav 27, 713–725. [DOI] [PubMed] [Google Scholar]
- Dube SR, Miller JW, Brown DW, Giles WH, Felitti VJ, Dong M, and Anda RF (2006). Adverse childhood experiences and the association with ever using alcohol and initiating alcohol use during adolescence. J. Adolesc. Health 38, 444.e1–444.e10. [DOI] [PubMed] [Google Scholar]
- Esser MB, Clayton H, Demissie Z, Kanny D, and Brewer RD (2017). Current and Binge Drinking Among High School Students — United States, 1991–2015. MMWR Morb. Mortal. Wkly. Rep 66, 474–478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fink LA, Bernstein D, Handelsman L, Foote J, and Lovejoy M (1995). Initial reliability and validity of the childhood trauma interview: a new multidimensional measure of childhood interpersonal trauma. Am. J. Psychiatry 152, 1329–1335. [DOI] [PubMed] [Google Scholar]
- Ford JD, Elhai JD, Connor DF, and Frueh BC (2010). Poly-Victimization and Risk of Posttraumatic, Depressive, and Substance Use Disorders and Involvement in Delinquency in a National Sample of Adolescents. J. Adolesc. Health 46, 545–552. [DOI] [PubMed] [Google Scholar]
- Graham JW, Cumsille PE, and Shevock AE (2012). Methods for Handling Missing Data In Handbook of Psychology, Second Edition, Weiner I, ed. (Hoboken, NJ, USA: John Wiley & Sons, Inc.), p. hop202004. [Google Scholar]
- Hemphill SA, Heerde JA, Herrenkohl TI, Patton GC, Toumbourou JW, and Catalano RF (2011). Risk and Protective Factors for Adolescent Substance Use in Washington State, the United States and Victoria, Australia: A Longitudinal Study. J. Adolesc. Health 49, 312–320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry KL, and Muthén B (2010). Multilevel Latent Class Analysis: An Application of Adolescent Smoking Typologies With Individual and Contextual Predictors. Struct. Equ. Model. Multidiscip. J 17, 193–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill KG, White HR, Chung IJ, Hawkins JD, and Catalano RF (2000). Early adult outcomes of adolescent binge drinking: person- and variable-centered analyses of binge drinking trajectories. Alcohol. Clin. Exp. Res 24, 892–901. [PMC free article] [PubMed] [Google Scholar]
- Kamata A, Kara Y, Patarapichayatham C, and Lan P (2018). Evaluation of Analysis Approaches for Latent Class Analysis with Auxiliary Linear Growth Model. Front. Psychol 9, 130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kanny D, Naimi TS, Liu Y, Lu H, and Brewer RD (2018). Annual Total Binge Drinks Consumed by U.S. Adults, 2015. Am. J. Prev. Med 54, 486–496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keyes KM, McLaughlin KA, Koenen KC, Goldmann E, Uddin M, and Galea S (2012). Child maltreatment increases sensitivity to adverse social contexts: neighborhood physical disorder and incident binge drinking in Detroit. Drug Alcohol Depend 122, 77–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwan M, Bobko S, Faulkner G, Donnelly P, and Cairney J (2014). Sport participation and alcohol and illicit drug use in adolescents and young adults: A systematic review of longitudinal studies. Addict. Behav 39, 497–506. [DOI] [PubMed] [Google Scholar]
- Lee GP, Storr CL, Ialongo NS, and Martins SS (2012). Association between Adverse Life Events and Addictive Behaviors among Male and Female Adolescents: Sex Differences in Addictive Behaviors and Adverse Events. Am. J. Addict 21, 516–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis TL, Kotch J, Wiley TRA, Litrownik AJ, English DJ, Thompson R, Zolotor AJ, Block SD, and Dubowitz H (2011). Internalizing Problems: A Potential Pathway From Childhood Maltreatment to Adolescent Smoking. J. Adolesc. Health 48, 247–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luthar SS, and Cicchetti D (2000). The construct of resilience: Implications for interventions and social policies. Dev. Psychopathol 12, 857–885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS (2011). Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Dev. Psychopathol 23, 493–506. [DOI] [PubMed] [Google Scholar]
- Masten AS, and Tellegen A (2012). Resilience in developmental psychopathology: contributions of the Project Competence Longitudinal Study. Dev Psychopathol 24, 345–361. [DOI] [PubMed] [Google Scholar]
- Masten AS, Neemann J, and Andenas S (1994). Life Events and Adjustment in Adolescents: The Significance of Event Independence, Desirability, and Chronicity. J. Res. Adolesc 4, 71–97. [Google Scholar]
- Masten AS, Burt KB, Roisman GI, Obradovic J, Long JD, and Tellegen A (2004). Resources and resilience in the transition to adulthood: Continuity and change. Dev. Psychopathol 16. [DOI] [PubMed] [Google Scholar]
- Mehta D, Klengel T, Conneely KN, Smith AK, Altmann A, Pace TW, Rex-Haffner M, Loeschner A, Gonik M, Mercer KB, et al. (2013). Childhood maltreatment is associated with distinct genomic and epigenetic profiles in posttraumatic stress disorder. Proc. Natl. Acad. Sci. U. S. A 110, 8302–8307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén BO, and Muthén LK (2017). Mplus Version 8 (Los Angeles, CA: Muthén & Muthén; ). [Google Scholar]
- Myers B, McLaughlin KA, Wang S, Blanco C, and Stein DJ (2014). Associations between childhood adversity, adult stressful life events, and past-year drug use disorders in the National Epidemiological Study of Alcohol and Related Conditions (NESARC). Psychol. Addict. Behav 28, 1117–1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, and Marks JS (2003). Binge drinking among US adults. JAMA J. Am. Med. Assoc 289, 70–75. [DOI] [PubMed] [Google Scholar]
- Nooner KB, Litrownik AJ, Thompson R, Margolis B, Margolis B, English DJ, Knight ED, Everson MD, and Roesch S (2010). Youth self-report of physical and sexual abuse: a latent class analysis. Child Abuse Negl 34, 146–154. [DOI] [PubMed] [Google Scholar]
- Nusslock R, and Miller GE (2016). Early-Life Adversity and Physical and Emotional Health Across the Lifespan: A Neuroimmune Network Hypothesis. Biol. Psychiatry 80, 23–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nylund KL, Asparouhov T, and Muthén BO (2007). Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. Multidiscip. J 14, 535–569. [Google Scholar]
- Nylund-Gibson K, Grimm R, Quirk M, and Furlong M (2014). A Latent Transition Mixture Model Using the Three-Step Specification. Struct. Equ. Model. Multidiscip. J 21, 439–454. [Google Scholar]
- Pilowsky DJ, Keyes KM, and Hasin DS (2009). Adverse Childhood Events and Lifetime Alcohol Dependence. Am. J. Public Health 99, 258–263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Primack BA, Kraemer KL, Fine MJ, and Dalton MA (2009). Media Exposure and Marijuana and Alcohol Use Among Adolescents. Subst. Use Misuse 44, 722–739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schellekens AFA, Franke B, Ellenbroek B, Cools A, de Jong CAJ, Buitelaar JK, and Verkes R-J (2013). COMT Val158Met modulates the effect of childhood adverse experiences on the risk of alcohol dependence: Gene environment interaction. Addict. Biol 18, 344–356. [DOI] [PubMed] [Google Scholar]
- Schulenberg J, O’Malley PM, Bachman JG, Wadsworth KN, and Johnston LD (1996). Getting drunk and growing up: trajectories of frequent binge drinking during the transition to young adulthood. J. Stud. Alcohol 57, 289–304. [DOI] [PubMed] [Google Scholar]
- Sønderlund AL, O’Brien K, Kremer P, Rowland B, De Groot F, Staiger P, Zinkiewicz L, and Miller PG (2014). The association between sports participation, alcohol use and aggression and violence: A systematic review. J. Sci. Med. Sport 17, 2–7. [DOI] [PubMed] [Google Scholar]
- Stone AL, Becker LG, Huber AM, and Catalano RF (2012). Review of risk and protective factors of substance use and problem use in emerging adulthood. Addict. Behav 37, 747–775. [DOI] [PubMed] [Google Scholar]
- Strine T (2012). Associations Between Adverse Childhood Experiences, Psychological Distress, and Adult Alcohol Problems. Am. J. Health Behav 36. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality (SAMHSA) (2012). The DAWN Project: Highlights of the 2010 Drug Abuse Warning Network (DAWN) Findings on Drug-Related Emergency Department Visits (Rockville, MD: SAMHSA; ). [PubMed] [Google Scholar]
- Thompson R, Litrownik AJ, Isbell P, Everson MD, English DJ, Dubowitz H, Proctor LJ, and Flaherty EG (2012). Adverse experiences and suicidal ideation in adolescence: Exploring the link using the LONGSCAN samples. Psychol. Violence 2, 211–225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Timko C, Sutkowi A, Pavao J, and Kimerling R (2008). Women’s childhood and adult adverse experiences, mental health, and binge drinking: The California Women’s Health Survey. Subst. Abuse Treat. Prev. Policy 3, 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Traube DE, James S, Zhang J, and Landsverk J (2012). A national study of risk and protective factors for substance use among youth in the child welfare system. Addict. Behav 37, 641–650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler H (1994). Health and Behavioral Consequences of Binge Drinking in College: A National Survey of Students at 140 Campuses. JAMA 272, 1672. [PubMed] [Google Scholar]
- Wu NS, Schairer LC, Dellor E, and Grella C (2010). Childhood trauma and health outcomes in adults with comorbid substance abuse and mental health disorders. Addict. Behav 35, 68–71. [DOI] [PMC free article] [PubMed] [Google Scholar]