

Abstract
Obesity is established as a key correlate of severe SARS-CoV-2 outcomes. Multiple other epidemiological and immunological features are less well-defined including if obesity enhances susceptibility to SARS-CoV-2 infection, influences symptom phenotype, or impedes or alters the immune response to infection. Given the substantial global burden of obesity and given these uncertainties, we examined the epidemiology and immunology of obesity and SARS-CoV-2.
Methods:
Industry employees were invited to participate in a prospective SARS-CoV-2 serology-based cohort study. Blood and baseline survey measures that included demographics, comorbidities, and prior COVID-19 compatible symptoms were collected. Serological testing and interim symptom reporting were conducted monthly. SARS-CoV-2 immunoassays included an IgG ELISA targeting the spike RBD, multiarray Luminex targeting 20 viral antigens, pseudovirus neutralization, and T cell ELISPOT assays. Unadjusted and adjusted analyses were used to identify differences in seroprevalence, clinical features, and immune parameters by BMI.
Results:
Of 4469 individuals enrolled, 322 (7.21%) were seropositive. Adjusted seroprevalence was non-significantly lower with higher BMI. Obesity was associated with increased reporting of fever (OR 3.43 [95% CI 1.58-7.60]) and multiple other symptoms and aggregate measures. There were no identifiable differences in immune response between obese and non-obese individuals.
Discussion:
We present benchmark data from a prospective serology-based cohort on the immunoepidemiology of BMI and SARS-CoV-2. Our findings suggest obesity is not linked to an increased risk of SARS-CoV-2 infection; that symptom phenotype is strongly influenced by obesity; and that despite evidence of obesity-associated immune dysregulation in severe COVID-19, there is no evidence of a muted or suppressed immune response across multiple immune measures among non-severe infections.
Background
Obesity is a key risk factor for severe disease and death from novel coronavirus disease 2019 (COVID-19),1,2 the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). With over 1.9 billion people overweight or obese globally,3 implications for SARS-CoV-2 pandemic morbidity and mortality are substantial. Even after adjusting for age and obesity-related comorbidities such as diabetes, hypertension and coronary heart disease, obesity remains a strong independent predictor of excess morbidity and mortality.1,4,5 These findings although concerning are not entirely unexpected.6 Obesity and poor clinical outcomes have been described with other viral pathogens, most notably influenza A (H1N1) during the 2009 pandemic, when obesity was associated with increased hospitalizations, need for intensive care support, and deaths.4,7,8
In addition to the relationship between obesity and clinical outcomes, emerging evidence suggests a link between higher body mass index (BMI) and higher incidence rates of COVID-19 or SARS-CoV-2 infection 4,9,10 suggesting increased BMI may enhance susceptibility to infection. If correct, there would be important implications for individual-level risks and population-level transmission dynamics, particularly among populations with high rates of obesity.4 However, data supporting this association is limited, and given the absence of convincing precedent from other pathogens additional evidence is required to confirm these findings.
The influence of obesity specifically on the immune response to SARS-CoV-2 has also been the focus of intense recent attention.4,11 Obesity has been linked to less robust and/or effective immune response after natural influenza infection12 or vaccination,13 raising concerns about diminished protective immunity following natural SARS-CoV-2 infection or vaccination.4,14 This is particularly relevant given multiple phase II and III vaccine trials are underway, and the outcomes of these trials are likely to reframe the pandemic trajectory. However, again, the immunological features of SARS-CoV-2 infection and obesity are poorly characterized with limited directly relevant data.
Thus, given the essential connection between the epidemiology and immunology of infectious pathogens including SARS-CoV-2 and given substantial uncertainly about multiple features of obesity and SARS-CoV-2 we conducted an integrated immunoepidemiological investigation of obesity and SARS-CoV-2 through a prospective multi-site cohort study. This study aimed to identify if BMI is associated with (i) differential risks of testing positive for anti-SARS-CoV-2 IgG antibodies among a population unbiased to serostatus at study entry, (ii) variable reporting of COVID-19 compatible symptoms, and (iii) measurable differences in adaptive immune features.
Methods
Ethical Disclosures
The study protocol was approved by the Western Institutional Review Board. The use of de-identified data and biological samples was approved by the Mass General Brigham Healthcare Institutional Review Board. All participants provided written informed consent.
Study design, setting and study population
This is a prospective observational cohort study using serial serological assessment to characterize the immunoepidemiology of SARS-CoV-2 infection among a cohort of industry employees. Serostatus was unknown at the time of subject enrollment. The study population was comprised of Space Exploration Technologies Corporation employees, all of whom were invited to participate. A total of 4469 participants were enrolled out of a total of ~8400 employees from seven primary work locations in four U.S. states including California, Texas, Florida, and Washington. Study enrollment commenced 20 April and employees were invited to participate on a rolling basis through 28 July 2020. Serial blood sampling and interim symptom reporting were performed monthly.
Covariates
All participants completed a standardized baseline study survey that included demographic data (age, sex, race, ethnicity, primary work location, and number of individuals and children <18 years living in the subject household), medical history (weight, height, diabetes, asthma, chronic obstructive pulmonary disease, other lung disease, coronary heart disease, heart failure, high blood pressure, chronic kidney disease, stroke, any immunocompromised condition, any other significant medical condition, and smoking status), and COVID-19 compatible symptoms between March 1, 2020, and study enrollment including primary symptoms (fever, chills or feverish, cough, anosmia, ageusia) and other compatible symptoms (body or muscle aches, sore throat, nausea or vomiting, diarrhea, congestion, and increased fatigue/generalized weakness). Composite symptom measures included (i) any symptom, (ii) number of symptoms, (iii) ≥3 symptoms; (iv) ≥6 symptoms, (v) any primary symptom (vi) number of primary symptoms and (vii) ≥3 primary symptoms. Sequential blood sampling and interim symptom reporting using a standardized survey were performed monthly. The number of participants with missing data by covariate is listed in Table 1.
Table 1.
Characteristics and serostatus of study participants (n=4469)
| Characteristic1 | All participants (n=4469) | Seropositive participants (n=322) |
OR (95% CI) | P-Value5 | |
|---|---|---|---|---|---|
| N | N | % | |||
|
Age group | |||||
| 18-29 y | 1668 | 133 | 8.0% | ref | |
| 30-39 y | 1761 | 104 | 5.9% | 0.72 (0.56 to 0.94) | 0.0174* |
| 40-49 y | 584 | 50 | 8.6% | 1.08 (0.77 to 1.52) | 0.6545 |
| 50-59 y | 315 | 26 | 8.3% | 1.04 (0.67 to 1.61) | 0.8666 |
| 60+ y | 85 | 2 | 2.4% | 0.28 (0.07 to 1.14) | 0.076 |
|
BMI | |||||
| <18.5 | 34 | 3 | 8.8% | 1.44 (0.43 to 4.80) | 0.5500 |
| 18.5-<25 | 1686 | 106 | 6.3% | ref | |
| 25-<30 | 1523 | 101 | 6.6% | 1.06 (0.80 to 1.40) | 0.6916 |
| 30-<35 | 676 | 61 | 9.0% | 1.48 (1.06 to 2.05) | 0.0196* |
| 35-<40 | 246 | 23 | 9.3% | 1.54 (0.96 to 2.47) | 0.0742 |
| ≥40 | 105 | 5 | 4.8% | 0.75 (0.30 to 1.87) | 0.5308 |
|
Ethnicity | |||||
| Not Hispanic/Not Latinx | 2492 | 113 | 4.5% | ref | |
| Hispanic/Latinx | 1274 | 155 | 12.2% | 2.91 (2.26 to 3.75) | <0.0001**** |
|
Race | |||||
| White | 2862 | 185 | 6.5% | ref | |
| American Indian/Alaska Native | 32 | 3 | 9.4% | 1.50 (0.45 to 4.96) | 0.5092 |
| Asian | 442 | 18 | 4.1% | 0.61 (0.37 to 1.01) | 0.0535 |
| Black | 72 | 2 | 2.8% | 0.41 (0.10 to 1.70) | 0.2207 |
| Native Hawaiian/Pacific Islander | 29 | 2 | 6.9% | 1.07 (0.25 to 4.54) | 0.9249 |
| More than one race | 292 | 13 | 4.5% | 0.67 (0.38 to 1.20) | 0.1796 |
|
Sex2 | |||||
| Female | 600 | 40 | 6.7% | ref | |
| Male | 3730 | 267 | 7.2% | 1.08 (0.77 to 1.52) | 0.6634 |
|
Children ≤ 18 y in household | |||||
| No | 3014 | 204 | 6.8% | ref | |
| Yes | 1342 | 106 | 7.9% | 1.18 (0.93 to 1.51) | 0.1808 |
|
No. in household | |||||
| 1 | 640 | 41 | 6.4% | ref | |
| 2-4 | 3027 | 214 | 7.1% | 1.11 (0.79 to 1.57) | 0.5490 |
| >4 | 659 | 51 | 7.7% | 1.23 (0.80 to 1.88) | 0.3499 |
|
Primary work location | |||||
| Cape Canaveral, Florida | 268 | 17 | 6.3% | ref | |
| Hawthorne, California | 2859 | 111 | 3.9% | 0.60 (0.35 to 1.01) | 0.0544 |
| McGregor, Texas | 257 | 21 | 8.2% | 1.31 (0.68 to 2.55) | 0.4202 |
| Seattle, Washington | 253 | 5 | 2.0% | 0.30 (0.11 to 0.82) | 0.0190* |
| South Texas, Texas | 712 | 160 | 22.5% | 4.28 (2.54 to 7.21) | <0.0001**** |
| Other | 69 | 1 | 1.4% | 0.23 (0.03 to 1.79) | 0.1623 |
|
Comorbidities3,4 | |||||
| Asthma | 368 | 20 | 5.4% | 0.72 (0.45 to 1.15) | 0.1721 |
| Hypertension | 356 | 26 | 7.3% | 1.02 (0.67 to 1.54) | 0.9405 |
| Diabetes mellitus | 101 | 11 | 10.9% | 1.59 (0.84 to 3.01) | 0.1509 |
| Coronary heart disease | 17 | 1 | 5.9% | 0.80 (0.11 to 6.08) | 0.8329 |
| Stroke | 9 | 2 | 22.2% | 3.70 (0.76 to 17.87) | 0.1039 |
| Emphysema/COPD | 9 | 1 | 11.1% | 1.61 (0.20 to 12.93) | 0.6532 |
| Cancer - not receiving treatment | 39 | 2 | 5.1% | 0.69 (0.17 to 2.89) | 0.6163 |
| Other lung disease | 26 | 2 | 7.7% | 1.07 (0.25 to 4.56) | 0.9233 |
| Other immunocompromised | 61 | 4 | 6.6% | 0.92 (0.33 to 2.55) | 0.8710 |
| Other chronic medical condition | 176 | 9 | 5.1% | 0.72 (0.36 to 1.43) | 0.3471 |
|
Smoking history | |||||
| Never | 3769 | 263 | 7.0% | ref | |
| Prior | 367 | 24 | 6.5% | 0.93 (0.61 to 1.44) | 0.7514 |
| Current | 229 | 23 | 10.0% | 1.49 (0.95 to 2.33) | 0.0826 |
Not reported data: age group (n=56), BMI (199), ethnicity (703), race (740), sex (139), children in HH (113), No. in HH (143), primary location (51), comorbidities (105)
Four (4) reported “other sex”, none were seropositive
For comorbidities reference value for OR is no. COPD chronic obstuctive pulmonary disease
Other comorbidities with no seropositive participants: chronic kidney disease (10), Heart failure (4), Cancer receiving treatment (3), Other heart disease (22).
P-values unadjusted for multiple hypothesis testing:
<0.05.
<0.01,
<0.001,
<0.0001
Laboratory analyses
Serological analyses were performed on sera using the Ragon/MGH enzyme-linked immunosorbent assay, which detects IgG against the receptor binding domain (RBD) of the SARS-CoV-2 spike glycoprotein using a previously described method15 (Supplemental 1). Assay performance has been externally validated in a blinded fashion at 99·6% specific and benchmarked against commercial EUA approved assays.16 Immune profiling methods are detailed in Supplement 1. Briefly, specific antibody subclasses, isotypes and FcγR binding against SARS-CoV-2 RBD, nucleocapsid and full spike proteins were assessed using a custom Luminex multiplexed assay (Luminex Corp, TX, USA). Viral neutralization was assessed on a 2019-nCoV pseudovirus neutralization assay, as described previously17 with neutralization titer defined as the sample dilution associated with a 50% reduction in luminescent units. The presence of neutralizing activity was defined as a titer >20. T cell activity was assessed on an enzyme-linked interferon-gamma immunospot assay (ELISPOT) with ≥ 25 spot forming cells (SPC) per 106 peripheral blood mononuclear cells (PBMCs) considered positive.
Data classification and analyses
Serostatus was determined by the presence or absence of IgG against SARS-CoV-2 RBD. BMI was calculated by dividing weight in kilograms by height in meters squared and categorized by underweight (<18·5 kg/m2), normal weight (18·5 to 24 kg/m2; reference), overweight (25 to 29 kg/m2), obesity class 1 (30 to 34 kg/m2), obesity class 2 (35 to 39 kg/m2), and obesity class 3 or severe obesity (≥40 kg/m2) according to the World Health Organization.
We performed discrete analyses to address the three aims of the study. For assessment of risk of seropositivity by BMI, the primary exposure of interest was BMI and the outcome variable of interest was seropositivity at any time point. We assessed the unadjusted and adjusted association between a range of demographic (n=7) and medical history (n=17) covariates using χ2 to compare proportions and ANOVA or Kruskal-Wallis tests to compare means. For adjusted analyses, we constructed a multivariable logistic regression model that included, in addition to BMI and serostatus, age, sex, ethnicity, race, comorbidities, primary work location, number of individuals in the household, and children in the household.
To understand if obesity status is associated with differential reporting of symptoms, we computed the proportion of seropositive individuals reporting each of 11 COVID-19 compatible symptoms stratified by obesity status. Symptoms were analyzed from the period preceding the first seropositive result. For example, if an individual was seronegative at baseline and seropositive at the subsequent time point, the symptoms reported between those timepoints were analyzed. The primary exposure of interest was obesity, and the outcome variables of interest were symptoms and composite symptom measures. Given recent data suggesting the adverse impact of obesity on COVID-19 mortality may decline with age,9 we assessed if similar age-dependent obesity risk may be observed for symptom reporting by conducting subgroup analysis stratified by < or ≥ 40 years, with categorization selected due to sparsity of older participants.
Lastly, given an accumulation of evidence that obesity impairs the immune response to a range of pathogens6,13,18–20 we stratified 20 discrete immune features by obesity status to identify univariate differences. We also performed uniform manifold approximation and projection (UMAP)21 a mathematical approach for exploratory analyses that constructs a visualizable summary of multiple subjects’ characteristics, with each point representing an individual and clusters representing underlying uniformities in subject characteristics.
Binomial exact 95% confidence intervals were calculated and p-values < 0·05 were considered statistically significant· For adjusted analyses, variables with a p-value <0·10 were assessed by backward elimination and excluded if the p-value was >0·10 and did not meaningfully alter the point estimates of the remaining variables. Luminex UMAP and Mann-Whitney U Tests were conducted using scikit-learn, a machine learning toolkit for the Python programming language. Analyses were performed using the R software package (Version 4·0, www.R-project.org/) or the Python programming language (Version 3·7, python.org).
Results
A total of 4469 Space Exploration Technologies Corporation employees out of a total of ~8400 employees (53%) were enrolled. Baseline characteristics are included in Table 1. Mean BMI was 27·1 kg/m2 (SD 5·4) with a median of 25·8 kg/m2 (range 15·6—60·9). Most subjects were normal weight (18·5—24 kg/m2) (1686, 39·5%) or overweight (25—29 kg/m2) (1523, 35·7%), and 24·1% and 0·80% met criteria for obese (≥30 kg/m2) and underweight (≤18·5 kg/m2) respectively.
IgG against the SARS-CoV-2 spike RBD protein was detected in 322/4469 (7·21%) of study participants. Of the 322 seropositive individuals, five (1·6%) were hospitalized and none required critical care support or died. Unadjusted seropositivity rates are detailed in Table 1; they were higher in South Texas (Odd Ratio 4·28 [95% CI, 2·54 to 7·21), p<0·0001]) and among Hispanics (2·91 [95% CI 2·226—3·75], p<0·0001); and they were lower in Seattle, Washington (0·30 [95% CI, 0·11 to 0·82], p=0·02]), and in the 30—39 year compared to the 18—29 year age group (0·72 [ 95% CI, 0·56 to 0·94, p=0·02). Adjusted associations for all covariates are listed in Table 1; only primary work location was retained as significantly associated with serostatus with increased OR in South Texas (OR 4·28 [2·54 -7·21], pcO-OOOl) and lower in Seattle (OR 0·30 [0·11—0·82], p=0·02) largely reflecting local transmission rates. The strong univariate association between Hispanic ethnicity and serostatus was not retained after adjusting for work location (OR 1·27 [0·94—1·73], p=0·12).
BMI and serostatus
Of the 4469 participants, 4270 (95·5%) provided weight and height data and are included in BMI analyses. The unadjusted risks of seropositivity stratified by BMI are listed in the Table 1; only BMI 30 to 34 kg/m2 (versus normal/healthy weight, 18·5—24 kg/m2) was associated with differential serostatus (OR 1·48 [1·06 to 2·05], p<0·02). However, after adjusting for all candidate variables (Table 1), no association was detected. In fact, higher BMI and in particular severe obesity (BMI >40 kg/m2) trended non-significantly to lower seroprevalence (Figure 1A). Subgroup analysis from a single high prevalence location where, given the high force of infection as evidenced by high seroprevalence (22·5% versus 4·2% for all other sites combined), we predict risks for infection — including any effect of BMI — would be more clearly delineated (Supplementary 2). Findings were similar to the primary analysis with no evidence of increased seroprevalence with increasing BMI. Rather, point prevalence measures consistently trended lower than normal/healthy weight (Figure 1B).
Figure 1. Forest plots of adjusted odds ratio for seropositivity by BMI as a categorical variable with normal BMI (18·5-<25) as reference.
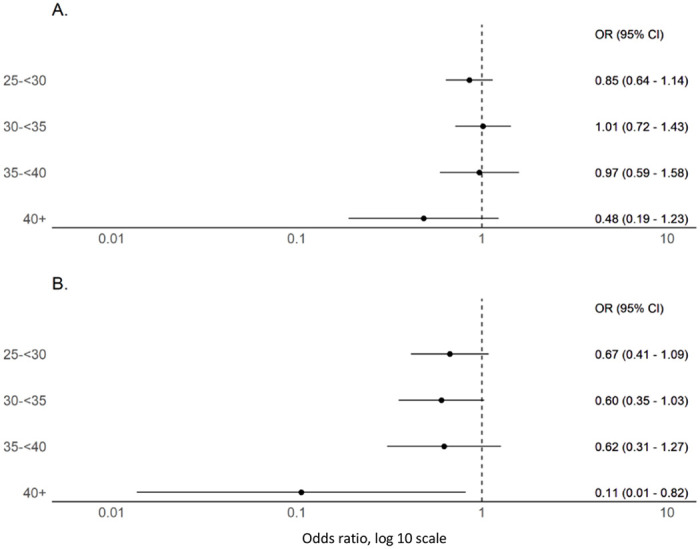
(A) Includes participants with BMI measures and demonstrates a non-significant trend to declining seroprevalence with BMI ≥40 kg/m2 when compared to normal/healthy weight (BMI 18·5-24 kg/m2) (n=4270). (B) Includes only participants from a single high seroprevalence (22·5%) location in South Texas where the high force of infection may more clearly delineate infection risks (n=629).
BMI and COVID-19 compatible symptoms
Of 262 seropositive participants with complete symptom data, three (1·1%) were underweight (BMI<18·5 kg/m2), 89 (34·0%) normal weight (BMI 18·5—24 kg/m2), 89 (34·0%) overweight (BMI 25—29 kg/m2), and 81 (30·9%) obese (BMI ≥30 kg/m2). A total of 106/262 (40·5%) reported one or more of 11 COVID-19- compatible symptoms and 68/262 (26·0%) reported one or more of five primary COVID-19 symptom. When comparing symptoms between normal weight and overweight (but not obese) individuals, there were no meaningful differences or trends (Supplementary 3) and therefore subsequent analyses were stratified by obese versus non-obese.
Obesity was associated with increased reporting of multiple symptoms including fever (OR 3·43 [95% CI 1·58—7·60]), chills or feverish but no measured fever (OR 2·64 [1·33—5·27]), myalgias (OR 2·29 [1·18—4·42]), and ≥6 symptoms (OR 2·26 [1·10—4·64]). With the exception of congestion (0·87 [0·43—1·70]), a similar and consistent but non-significant trend was observed for all symptoms (Figure 2). Overall, obese individuals registered more symptoms (2·26 versus 1·40, OR 1·10 [1·02—1·22]) and more primary symptoms (1·05 versus 0·58, OR 1·24 [1·04—1·48]) than non-obese. Differential symptom reporting was more pronounced in those under 40 years of age. Fever was more commonly reported among obese vs non-obese individuals under 40 years of age (OR 4·99 [1·97—13·35]) but not over 40 years (OR 1·32 [0·30—5·57]). Similarly, reporting ≥6 symptoms was more common among obese vs non—obese under 40 years (OR 3·0 [1·32—6·85]) but not for those greater than 40 years (OR 0·94 [0·18—4·26]). A strikingly similar trend was observed for the majority of other symptoms and aggregate symptom measures (Figure 3). No similar age-dependent effect on obesity and symptomatology was observed among age groups < 40 years of age (Supplementary 4).
Figure 2.
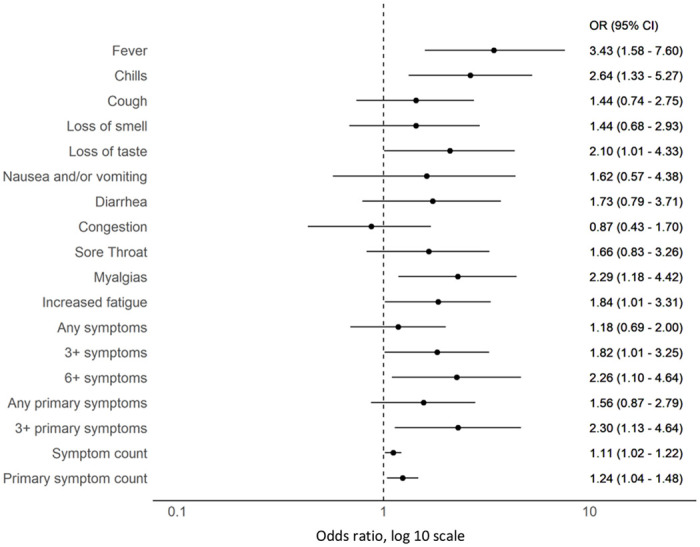
Forest plot of odds ratios of reported COVID-19 compatible symptoms among obese (n=85) versus non-obese (n=179) SARS-CoV-2 seropositive individuals
Figure 3.
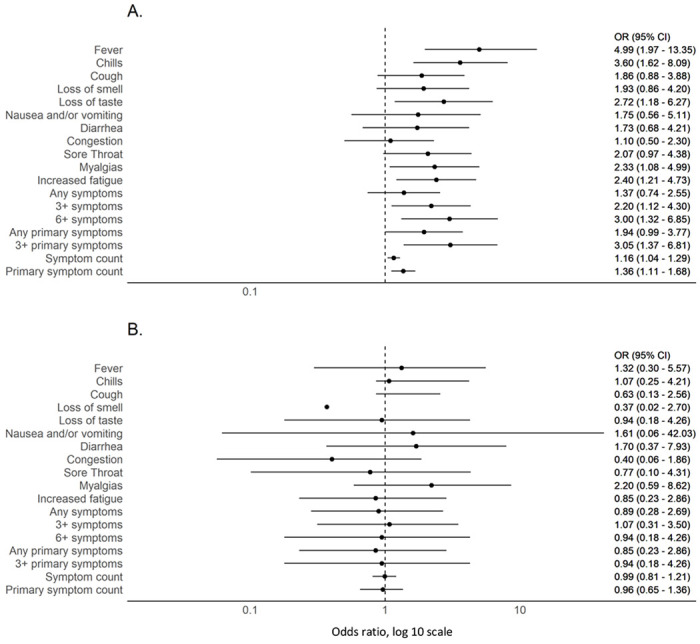
Forest plot of odds ratios of COVID-19 compatible symptoms among obese versus non-obese SARS-CoV-2 seropositive individuals stratified by (A) <40 years (n=195) and (B) ≥ 40 years (n=67)
Obesity and functional immune response
Among the same 262 seropositive individuals, peak SARS-CoV-2 RBD IgG titers were 0·92 ug/ml (SD 2·47) among obese (n=81) and 1·12 ug/ml (SD 3·21) among non-obese (n=181) participants (p=0·601). Deep immune profiling was performed among a subset of 77 participants including 25 obese and 52 non-obese individuals. Mean ELISA nucleocapsid titers were 0·35 (SD 0·48) among obese individuals and 0·30 (0·34) for non-obese individuals (p=0·57). Viral neutralization activity (titer >20) was detected in 3/25 (12·0%) and 6/52 (11·5%) of obese and non-obese individuals respectively (p=0·95). When assessing 20 immune features measured by Luminex, no univariate differences were observed between obesity categories, with sparse levels across both obese and non-obese individuals tightly linked to antibody titers (Figure 4A, Supplementary 5). Similarly, no clustering or trends between BMI and immunological features were identifiable either by UMAP (Figure 4B) or Spearman’s correlation (Figure 4C).
Figure 4. Limited influence of BMI on SARS-CoV-2 antibody profiles (n=77).
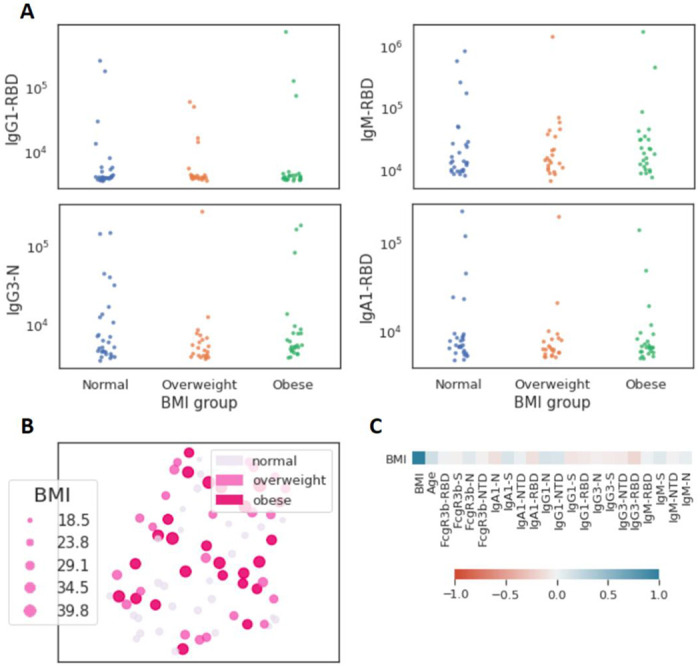
(A) The dot plots show similar mean fluorescent intensity levels of IgG1, IgM, IgG3, and IgA levels across individuals classified as normal weight (n=29), overweight (n=23), and obese (n=25). (B) The uniform manifold approximation and projection (UMAP) shows the relationship between antibody profiles and BMI (dot size, color intensity), highlighting the limited influence of BMI on shaping SARS-CoV-2 antibody responses. (C) Correlation plot of shows limited correlation between BMI and 20 immunological features.
Lastly, given evidence that T cells may be key mediators of adaptive immunity in SARS-CoV-2, we examined responses to nucleocapsids protein or spike protein overlapping peptide pools quantified by IFN-g ELISpot among 12 obese and 28 non-obese individuals. There was no difference in the proportion with SARS-CoV-2 T cell activity (≥25 SFC/106 PBMCs) against nucleocapsid peptides (3/12 [25%] versus 7/28 [25·0%]) or spike peptides (3/12 [25%] versus 7/28 [25·0%]). In fact, the only difference observed was higher SFC against nucleocapsid (mean 124 SFC/106 PBMCs [SD 77] versus 47 SFC/106 PBMCs [SD 14], p=0·02) but not spike (44 SFC/106 PBMCs [SD 4·0] versus 44 SFC/106 PBMCs [SD 20·0], ρ=1·00) among obese versus non-obese individuals with T cell activity.
Discussion
We present data from a large multi-site prospective cohort of non-hospitalized individuals unbiased to serostatus at study entry to investigate the association between BMI, SARS-CoV-2 serostatus, COVID-19 compatible symptoms, and functional and non-functional immune measures. Given the prevalence of overweight/obese among adults is close to 70% in most high income countries and ≥50%, in many lower and middle income countries, the scientific and public health implications for the current pandemic are substantial 4. Unlike prior studies, we did not observe an increase in infection or COVID-19 prevalence with increasing BMI but rather identified a trend to decreasing risk among the highest BMI classes. We also provide benchmark data on the association between reported COVID-19 symptoms and BMI, identifying evidence for more frequent reporting of multiple symptoms including fever, myalgia, chills, and total COVID-19 compatible symptoms among obese individuals. Finally, we examined immune features of infection to probe for differential immune signatures associated with obesity status. By combining traditional epidemiological approaches with deep immune profiling, we provide new insights into the epidemiology and immune characteristics of obesity in SARS-CoV-2 infections.
Prior studies that report an association between increased risk of COVID-19 or SARS-CoV-2 infection with higher BMI are intriguing and raise important questions about factors driving transmission. Given the enormous global burden of overweight and obese adults, delineating risks for infection is a public health priority. Interestingly, our findings appear to diverge from recent data that examines the risk for COVID-19 by BMI including a nationwide case-control study from South Korea9 and a cross-sectional study from a primary care surveillance network in the United Kingdom22 that identify an increased risk of COVID-19 with increasing BMI; and a recent meta-analysis of 20 studies that reported a pooled increased risk of 46·0% (OR = 1·46; 95% CI, 1·30-1·65; p < 0·0001) with 18 of 20 studies demonstrating higher COVID-19 risk among obese individuals.4 Our study did not identify an increase in adjusted seroprevalence with increasing BMI and conversely identified a trend to lower infection risk with higher obesity classes. This trend was consistent when both considering all data and when performing subgroup analysis on a high transmission site where the increased force of infection would be expected to more precisely delineate heterogeneity in infection risks. Reasons for the difference between our and prior study outcomes may be multifactorial with differences in study design and population behaviors likely influencing findings. However, we believe the primary difference is we examined SARS-CoV-2 infection risk using serological methods unbiased to exposure risks or presence or absence of symptoms at study entry versus other studies examining risks for clinically apparent infection (i.e. COVID-19). Given obese individuals exhibit more pronounced symptomatology including fever, as our data indicates, this population is more likely to meet testing criteria, more likely to be tested and therefore more likely to be over-represented in studies that identify cases through routine surveillance approaches.23,24 As such, although our study findings appear inconsistent with most prior studies of obesity risk, in fact the question being asked was different. Our study examined SARS-CoV-2 infection risk, as measured by the presence of SARS-CoV-2 antibodies, while prior studies examined the risk of clinical disease. Unfortunately, conflation of COVID-19 with SARS-CoV-2 infection is commonplace, as evidenced by confusion over case-versus infection-fatality rate.24
Our finding that obesity is associated with increased COVID-19 compatible symptoms among SARS-CoV-2 seropositive individuals provides benchmark data for understanding symptom heterogeneity in mild infections by BMI. We demonstrate that not only are well established measures of severe disease such as hospitalization, intensive care requirements and death more common among obese individuals 5,25,26 but that obesity is also an important driver of increased symptomatology in non-severe infections. While our data does not provide insights into the mechanism driving these findings, it informs our understanding of symptomatology and obesity, guides our interpretation of epidemiological data, and highlights the potential implication of using passively collected symptom-driven surveillance data to characterize the epidemiology of infectious pathogens. We also identify an interesting influence of age on obesity symptom reporting, with a compelling association below 40 years of age but near complete absence of effect in older adults. These findings are notable given they imply the established interaction between obesity and age on COVID-19 morbidity and mortality, with obesity disproportionately driving increased disease severity among younger age groups,5,25 extend throughout the spectrum of disease and are not restricted to severe disease. The reasons for this phenomenon are unclear and deserve study but do fit within the broader understanding of obesity and age in which the all-cause relative risk of death associated with increasing BMI decreases with age.27
Given the fundamental role of the adaptive immune response in both the resolution of infection and the severity of disease,11 we also probed multiple binding and functional immune markers to assess differential immune responses between obese and non-obese individuals. While, previous studies noted poor seroconversion and inadequate seroprotection across vaccine trials,28 we did not detect meaningful differences in binding or neutralizing antibodies, T cell activity, or other functional humoral measures by BMI. These findings, while notable, should be considered in the context of this largely asymptomatic and pauci-symptomatic cohort, that may not capture the full range of disease burden associated with SARS-CoV-2 infection. Yet, the overlapping and indistinguishable antibody and T-cell helper profiles point to unaltered adaptive immunity with BMI, raising the possibility that BMI-driven immunological changes during SARS-CoV-2 infection may manifest largely within the innate immune response. Significant alterations in chronic inflammation, particularly driven by persistent innate cytokine responses from adipocytes, have been noted in the setting of obesity.29 Dissecting the influence of adipocyte inflammatory responses, associated cytokine storm, and enhanced symptomatology, particularly among individuals with a high BMI, may point to mechanistic differences in viral sensing across populations. These data point to remaining knowledge gaps on the relative importance and interplay of the humoral, cellular and innate immunity in SARS-CoV-2 infection and disease.30
Limitations
Although this study is unique in combining a large prospective, multisite serology-based SARS-CoV-2 cohort with deep immune profiling, there are limitations. The study population are industry employees with over-representation – compared to the US population -- of persons of Hispanic ethnicity, white race, male sex, and younger individuals with lower rates of comorbidities including obesity and as such findings may not be generalizable. Given 53% of the invited employees participated in the study, an unmeasured selection bias may have been introduced. Several additional potential study limitations should be noted but any impact of these limitations would be expected to be evenly distributed across cohort participants and therefore not introduce a systematic bias and impact study findings. These include (i) limited recall of COVID-19 compatible symptoms, (ii) delayed seroconversion relative to reported symptoms, so depending on timing of infection and blood sampling, some registered symptoms may not be due to SARS-CoV-2 infection, and (ii) false positive serological results. Lastly, behavioral factors, which can be critical drivers of transmission, and may be influenced by BMI, were not assessed in this study.
Conclusion
We demonstrate that obesity is associated with increased symptomatology in mild COVID-19 infections, suggesting obesity impacts the pathophysiology of COVID-19 throughout the spectrum of disease severity. Our findings do not, however, suggest that obesity increases susceptibility to SARS-CoV-2 infection, nor did we identify immunological features differentiating obese from non-obese individuals in mild and asymptomatic infection.
Supplementary Material
Acknowledgements
We acknowledge support from Space Exploration Technologies Corporation, the Brigham and Women’s Department of Emergency Medicine, the Ragon Institute of MGH, MIT and Harvard, the Massachusetts Consortium on Pathogen Readiness (MassCPR), the NIH (3R37AI080289-11S1), FDA HHSF223201810172C, and the Gates foundation Global Health Vaccine Accelerator Platform funding. We thank Nancy Zimmerman, Mark and Lisa Schwartz, an anonymous donor (financial support), Terry and Susan Ragon, and the SAMANA Kay MGH Research Scholars award for their support. EJN is supported by the CDC (U01 GH002238). SMS was partially supported by the US Food and Drug Administration (HHSF223201810172C). DAL was partially supported by the National Institute for Allergy and Infectious Disease (U19 AI135995). We would also like to thank Eric Fischer for S protein production efforts and Jared Feldman, Blake Marie Hauser, Tim Caradonna and Aaron Schmidt for generating receptor binding domain antigen.
Footnotes
Conflict of interest
GA is a founder of Seromyx Systems Inc., a company developing platform technology that describes the antibody immune response. GA’s interests were reviewed and are managed by Massachusetts General Hospital and Partners Healthcare in accordance with their conflict of interest policies. PS is a co-founder of, shareholder in, and advisor to Sherlock Biosciences, Inc, as well as a Board member of and shareholder in Danaher Corporation. MJG, SB, YH, JR, EP, BM, ASM and ERM are employees of Space Exploration Technologies Corp. All other authors have declared that no conflict of interest exists.
References
- 1.Hamer M, Gale CR, Kivimäki M, Batty GD. Overweight, obesity, and risk of hospitalization for COVID-19: A community-based cohort study of adults in the United Kingdom. Proc Natl Acad Sci. 2020; 117(35):21011–21013. doi: 10.1073/pnas.2011086117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Seidu S, Gillies C, Zaccardi F, et al. The impact of obesity on severe disease and mortality in people with SARS-CoV-2: A systematic review and meta-analysis. Endocrinol Diabetes Metab. 2020. doi: 10.1002/edm2.176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.WHO. Obesity and overweight: Fact sheet. WHO Media Cent. 2020. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- 4.Popkin BM, Du S, Green WD, et al. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes Rev. doi: 10.1111/obr.13128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tartof SY, Qian L, Hong V, et al. Obesity and Mortality Among Patients Diagnosed With COVID-19: Results From an Integrated Health Care Organization. Ann Intern Med. doi: 10.7326/m20-3742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Falagas ME, Kompoti M. Obesity and infection. Lancet Infect Dis. 2006. doi: 10.1016/S1473-3099(06)70523-0 [DOI] [PubMed] [Google Scholar]
- 7.Kwong JC, Campitelli MA, Rosella LC. Obesity and respiratory hospitalizations during influenza seasons in Ontario, Canada: A cohort study. Clin Infect Dis. 2011;53(5):413–421. doi: 10.1093/cid/cir442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Centers for Disease Control and Prevention (CDC). Intensive-care patients with severe novel influenza A (H1N1) virus infection - Michigan, June 2009. MMWR Morb Mortal Wkly Rep. 2009;58:749–752. [PubMed] [Google Scholar]
- 9.Jung C-Y, Park H, Kim DW, et al. Association between Body Mass Index and Risk of COVID-19: A Nationwide Case-Control Study in South Korea. Clin Infect Dis. 2020. doi: 10.1093/cid/ciaa1257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ghoneim S, Umer Butt M, Hamid O, Shah A, Asaad I. The incidence of COVID-19 in patients with metabolic syndrome and non-alcoholic steatohepatitis: A population-based study. Metab Open. doi: 10.1016/j.metop.2020.100057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.García LF. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front Immunol. 2020. doi: 10.3389/fimmu.2020.01441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Karlsson EA, Sheridan PA, Beck MA. Diet-Induced Obesity Impairs the T Cell Memory Response to Influenza Virus Infection. J Immunol. 2010;184(6):3127–3133. doi: 10.4049/jimmunol.0903220 [DOI] [PubMed] [Google Scholar]
- 13.Neidich SD, Green WD, Rebeles J, et al. Increased risk of influenza among vaccinated adults who are obese. IntJ Obes. 2017;41(9):1324–1330. doi: 10.1038/ijo.2017.131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wadman M. Why COVID-19 is more deadly in people with obesity—even if they’re young. Science, https://www.sciencemag.org/news/2020/09/why-covid-19-more-deadly-people-obesity-even-if-theyre-young. [Google Scholar]
- 15.Roy V, Fischinger S, Atyeo C, et al. SARS-CoV-2-specific ELISA development. J Immunol Methods. 2020. doi: 10.1016/j.jim.2020.112832 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nilles EJ, Karlson EW, Norman M, et al. Evaluation of two commercial and two non-commercial immunoassays for the detection of prior infection to SARS-CoV-2. medRxiv. 2020. doi: 10.1101/2020.06.24.20139006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Atyeo C, Fischinger S, Zohar T, et al. Distinct Early Serological Signatures Track with SARS-CoV-2 Survival. Immunity. 2020. doi: 10.1016/j.immuni.2020.07.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Milner JJ, Sheridan PA, Karlsson EA, Schultz-Cherry S, Shi Q, Beck MA. Diet-Induced Obese Mice Exhibit Altered Heterologous Immunity during a Secondary 2009 Pandemic H1N1 Infection. J Immunol. 2013;191(5):2474–2485. doi: 10.4049/jimmunol.1202429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sheridan PA, Paich HA, Handy J, et al. Obesity is associated with impaired immune response to influenza vaccination in humans. Int J Obes. 2012;36(8):1072–1077. doi: 10.1038/ijo.2011.208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zimmermann P, Curtis N. Factors that influence the immune response to vaccination. Clin Microbiol Rev. 2019;32(2):e00084–18. doi: 10.1128/CMR.00084-18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Becht E, McInnes L, Healy J, et al. Dimensionality reduction for visualizing single-cell data using UMAP. Nat Biotechnol. 2019. doi: 10.1038/nbt.4314 [DOI] [PubMed] [Google Scholar]
- 22.de Lusignan S, Dorward J, Correa A, et al. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study. Lancet Infect Dis. 2020. doi: 10.1016/S1473-3099(20)30371-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gibbons CL, Mangen MJJ, Plass D, et al. Measuring underreporting and under-ascertainment in infectious disease datasets: A comparison of methods. BMC Public Health. 2014;14(147). doi: 10.1186/1471-2458-14-147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lipsitch M, Donnelly CA, Fraser C, et al. Potential biases in estimating absolute and relative case-fatality risks during outbreaks. PLoS Negl Trop Dis. 2015. doi: 10.1371/journal.pntd.0003846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kass DA, Duggal P, Cingolani O. Obesity could shift severe COVID-19 disease to younger ages. Lancet. 2020;395(10236):1544–1545. doi: 10.1016/S0140-6736(20)31024-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Deng M, Qi Y, Deng L, et al. Obesity as a Potential Predictor of Disease Severity in Young COVID-19 Patients: A Retrospective Study. Obesity. doi: 10.1002/oby.22943 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Villareal DT, Apovian CM, Kushner RF, Klein S. Obesity in older adults: Technical review and position statement of the American Society for Nutrition and NAASO, The Obesity Society. Am J Clin Nutr. 2005;82(5):923–934. doi: 10.1093/ajcn/82.5.923 [DOI] [PubMed] [Google Scholar]
- 28.Painter SD, Ovsyannikova IG, Poland GA. The weight of obesity on the human immune response to vaccination. Vaccine. 2015. doi: 10.1016/j.vaccine.2015.06.101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Méry G, Epaulard O, Borel AL, Toussaint B, Le Gouellec A. COVID-19: Underlying Adipokine Storm and Angiotensin 1–7 Umbrella. Front Immunol. 2020. doi: 10.3389/fimmu.2020.01714 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Moderbacher CR, Ramirez SI, Dan JM, et al. Antigen-specific adaptive immunity to SARS-CoV-2 in acute COVID-19 and associations with age and disease severity. Cell. doi: 10.1016/j.cell.2020.09.038 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.