

Abstract
Background
Nocturia is the most bothersome lower urinary tract symptoms (LUTS) and can significantly reduce men's quality of life. It is often poorly managed with conventional treatments.
Objective
The purpose of this study was to evaluate the self-assessed benefits of a prostate health dietary combination formulation on mild LUTS, especially nocturia in healthy males.
Methods
In an open label clinical study, thirty healthy male subjects with mild LUTS took one daily capsule of the product for 60 days. The primary outcome was self-assessed severity of LUTS using the International Prostate Symptoms Score (IPSS) questionnaire at Day 1 (baseline), Day 30 and Day 60. Safety and compliance were also evaluated.
Results
At Day 60, IPSS significantly decreased from baseline by 16.3% (3.6 ± 2.1 vs. 4.3 ± 1.5, p < 0.05). Although the reduction in IPSS did not reach statistical significance at Day 30, it was mostly driven by a 30.7% decrease (p < 0.05) in the nocturia sub-score compared with baseline. While 37% of subjects reported at baseline waking up 2‒3 times/night to void, none did so after taking the study product for 60 days. Compliance was very high throughout the study. No adverse events related to the study product were reported.
Conclusions
The study product might be a safe alternative for individuals willing to explore a non-conventional approach to manage their nocturia. A larger randomized placebo-controlled clinical trial is warranted to confirm these results. Clinical trial registry: Clinical Trials.gov. Registration number (September 1st, 2016): NCT02886832.
Keywords: Lower urinary tract symptoms, prostate, nocturia, dietary supplements
Introduction
Lower urinary tract symptoms (LUTS) in men encompass a large spectrum of clinical manifestations related to the bladder, urethra, and prostate. These symptoms are broadly categorized into voiding or obstructive (hesitancy, poor and/or intermittent stream, straining, prolonged micturition, feeling of incomplete bladder emptying, dribbling), and storage or irritative (frequency, urgency, urge incontinence, and nocturia) symptoms. LUTS are highly prevalent worldwide in males over 40.1 Not only are the symptoms troubling, but they also have a major impact on quality of life (QoL) as well as physical and mental health.2,3 The prevalence of LUTS markedly increases with age, rising to as high as 90% by age 90.4 With an aging population, LUTS is likely to become an increasingly substantial public health issue in the years to come.
One of the most common and bothersome LUTS is nocturia, defined as the need to wake up at night one or more times to void.5,6 This serious medical condition impacts over 40 million men in the United States, and its prevalence increases with age.7 A cross-sectional study conducted in a community setting showed that half of men aged > 50 years were affected by nocturia, which was the most detrimental symptom on QoL.8 Clinically relevant nocturia, defined as ≥ 2 voids/night, has been reported in up to 28‒62% in men aged 70‒80 years.9 Nocturia places a substantial burden on individuals as it not only severely disrupts sleep patterns, but also negatively affects daytime function.10 It is associated with reduced QoL, poor health, depression, increased mortality, and slipping and falling.6,11,12 Nocturia is a colossal economic burden, with an estimated direct cost of 1.5 billion dollars in related hip fractures in 2014.13 Yet, it is often trivialized, and its impact remains largely underestimated.14 Managing this symptom is challenging, as current conventional treatment options usually offer limited improvement and there is no therapy that would fully reverse and/or alleviate nocturia.15 Therefore, there is a need for more effective strategies to better manage this condition. According to a report published in 2011, roughly 50% of adults in the United States take dietary supplements for a variety of reasons.16 At a time when many are turning to complementary and alternative medicine because conventional treatments sometimes fail, dietary supplements are an increasingly attractive option, more so for those with mild LUTS who are reluctant to take standard medical treatments.17
The pathophysiology of LUTS is complex and multifactorial, and its underlying mechanisms are still poorly understood.18 The most common cause in men is benign prostatic hyperplasia (BPH) or enlarged prostate, a condition that typically affects the aging male population.19 Current conventional treatment modalities for LUTS include α-1 blockers, 5-α-reductase inhibitors, muscarinic receptor antagonists, β3-adrenergic agonists, and phosphodiesterase-5 inhibitors.20 These therapies, however, have shown limited efficacy at treating nocturia.21 Although some α-adrenergic receptor blockers and 5-α-reductase inhibitors are highly effective, they can have sexual adverse effects that cause many men to discontinue therapy.22 Many herbal supplements with numerous biological activities and beneficial effects on prostate health are used as complementary and alternative medications to manage symptoms of BPH, such as β-sitosterol, pygeum africanum, lycopene, boron, and melatonin.23–33
Therefore, the objective of this 60-day open label study was to assess the self-perceived benefits of a specifically formulated prostate health dietary supplement containing β-sitosterol, pygeum africanum bark extract, lycopene, boron, and melatonin on LUTS, especially on nighttime urination among generally healthy male participants.
Methods
Participants
We recruited subjects by means of posters and flyers, advertisement on social media, and e-mail blasts. Because prevalence of LUTS and nocturia increases with age, eligible participants were older healthy males aged 45‒75 years. Subjects also had to fully understood the procedures and requirements of the study, be willing to participate of their own free will and have mild LUTS [International Prostate Symptoms Score (IPSS) between 1 and 7] at the time of the screening evaluation. Subjects with a diagnosis of BPH, a history of bladder and/or prostate cancer, prior prostate or bladder surgery, Prostate-Specific Antigen (PSA) levels > 4 ng/mL, or actively seeking medical help for urological problems were excluded from the study.
Sample Size Calculation
In a study by Berges and colleagues, changes from baseline in the IPSS as the primary outcome ranged from 2 to 7 points, with a standard deviation of 3.8.34 On the basis of those results, sample size calculation for the current study determined that a minimum enrollment of 26 subjects would provide 80% power to detect a 3 point-change compared with baseline at a two-sided 0.05 level of significance with an estimated standard deviation of 3.8. Of 45 subjects screened for eligibility, and after considering a dropout rate of 10%, 30 participants were enrolled in the study.
Study Design
We conducted this 60-day single-group, single-center, open-label clinical trial at Life Extension Clinical Research (LECR), Inc. (Fort Lauderdale, FL) from the beginning of October 2017 to the end of November 2017. We scheduled three visits throughout the study to evaluate participants: Day 1 (baseline assessments), Day 30 (mid-study), and Day 60 (end of study). We conducted follow-up telephone interviews at Days 15 and 45 to discuss any change in medical history or concomitant medications, monitor adverse events, reinforce compliance, and remind subjects of the date and time of the next visit. During visits, body weight was measured after overnight fasting using a calibrated scale with no shoes on, and body mass index (BMI) was calculated using the standard formula. Blood pressure and heart rate were obtained with a Digital Blood Pressure Monitor Model UA-767 Plus device from LifeSource (ON, Canada). A fasting venous blood sample was also collected. Immediately following collection, tubes containing K2 EDTA were gently inverted to ensure proper mixing before centrifugation (10 minutes at 2,500 rpm). Serum was promptly collected, and specimens were refrigerated until shipped to LabCorp (Tampa, FL) for processing. Enzymatic methods (Roche Diagnostics Corporation, Indianapolis, IN) were used to assess glucose (assay No. 05168791), total cholesterol (assay No. 05168538), low-density lipoprotein (LDL) (assay No. 07005768), high-density lipoprotein (HDL) (assay No. 07528582), triglycerides (assay No. 05171407), aspartate aminotransferase (AST) (assay No. 05850819), and alanine aminotransferase (ALT) (assay No. 05850797) levels on a Roche/Hitachi Cobas c701/702 automated analyzer (Roche Diagnostics Corporation, Indianapolis, IN). PSA levels were measured using an electrochemiluminescent immunoassay on the Elecsys 1010/2010 and Modular Analytics E170 automated platform (Roche Diagnostics Corporation, Indianapolis, IN).
Intervention
We instructed subjects to take one (1) daily capsule of a dietary supplement containing β-sitosterol, pygeum africanum bark extract, lycopene, boron, and melatonin (Life Extension, Fort Lauderdale, FL), 1 hour before bedtime with water for 60 days.
Outcomes
The primary outcome was change from baseline in the IPSS total score at Days 30 and 60. The IPSS is a validated tool commonly used to assess severity of LUTS. This questionnaire consists of 7 questions on filling/storage and voiding/obstructive symptoms (incomplete emptying, frequency, intermittency, urgency, weak stream, straining and nocturia), each with a severity scale ranging from 0 to 5 [an additional question addresses QoL]. Higher scores indicate greater severity. Total IPSS scores are stratified into mild (1‒7), moderate (8‒19), and severe (20‒35) symptoms. Secondary outcomes included change from baseline at Days 30 and 60 in anthropometric measurements (body weight and BMI), PSA levels, and IPSS QoL question (score 1‒25). International Index of Erectile Function (IIEF)-5 questionnaire (also known as Sexual Health Inventory for Men (SHIM)) and SF-36 Health Survey were also secondary outcomes. The IIEF-5 is a short sexual activity questionnaire used as a diagnostic tool for erectile dysfunction (ED). Each of the 5 questions are scored from 0 to 5 where lower values indicate poor sexual function. Based on scores ranging from 1 to 25, ED is classified into four categories: severe (1–7), moderate (8–11), mild to moderate (12–16), mild (17–21), and no ED (22–25).35 The SF-36 Health Survey consists of 11 questions with mental and physical health components designed to capture individuals’ perceptions of their own health and well-being.
Compliance
At Days 30 and 60, subjects were asked to return containers to measure remaining study product, discuss adherence, and calculate compliance. Subjects were counseled when compliance was less than 85%. Participants were asked to not transfer the study product from the original container to another container.
Safety
We assessed safety and tolerability of the study product through evaluation of change from baseline in vital signs (blood pressure and heart rate) and blood chemistry (glucose levels, lipid profile, and hepatic function) at Days 30 and 60. We monitored signs of adverse events continuously and thoroughly documented them throughout the study. Participants had to contact LECR immediately if experiencing any unwanted reaction. We evaluated and classified adverse events according to severity (mild, moderate, severe, or life-threatening) and relationship to the study product (not related, unlikely related, possibly related, probably related, or definitely related) following a set of guidelines recommended by the National Center for Complementary and Integrative Health.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical standards set forth in the Helsinki Declaration. A signed informed consent was obtained from each participant. Subjects were permitted to discontinue participation at any time without providing reasons. The study protocol was approved by IntegReview Investigational Review Board. Clinical trial registry: Clinical Trials.gov. Registration number (September 1st, 2016): NCT02886832.
Statistical Analysis
We used GraphPad Prism software, version 5.01 (Abacus Concepts GraphPad Software, San Diego, USA) to perform statistical analyses. Results in tables are presented as mean and standard deviation (SD). We used the Shapiro-Wilk Test to assess normal distribution of the data sets. Based on results of the normality test, we analyzed changes from baseline at Day 30 and/or Day 60 with either one-way ANOVA repeated measures with Dunnett’s post-test or Friedman non-parametric one-way ANOVA repeated measures with Dunn’s post-test. The level of significance was set at p < 0.05.
Results
Clinical Characteristics at Baseline
All participants (N = 30) completed the study. Mean age was 58.5 ± 7.7 years. Subjects were overweight (84.6 ± 15.9 kg mean body weight, 26.4 ± 3.9 kg/m2 body mass index), but otherwise healthy. Blood pressure and heart rate were within normal range (Table 1).
Table 1.
Clinical Characteristics of Participants (N = 30) at Baseline.
| Characteristic | Mean ± SD |
|---|---|
| Age (years) | 58.5 ± 7.7 |
| Weight (kg) | 84.6 ± 15.9 |
| Body Mass Index (kg/m2) | 26.4 ± 3.9 |
| Systolic Blood Pressure (mmHg) | 122.6 ± 10.0 |
| Diastolic Blood Pressure (mmHg) | 77.8 ± 7.8 |
| Heart Rate (beats/min) | 60.3 ± 7.2 |
Abbreviation: SD, standard deviation.
Primary Outcome
Self-reported IPSS total score was 4.3 ± 1.5 at baseline, indicative of very mild LUTS. After 30 days on the investigational product, IPSS total score decreased by 13.9% compared with baseline, although this was not statistically significant. Importantly, after 60 days of supplementation, the IPSS total score significantly decreased by 16.3% (0.7 points, p < 0.05) relative to baseline (Table 2). The reduction in IPSS total score at Day 30 was mostly driven by a significant 30.7% decrease (0.4 episodes/night, p < 0.05) in nocturia sub-score compared with baseline. The number of subjects experiencing nocturia after supplementation with the investigational product decreased dramatically. The proportion of participants reporting to wake up at least one time per night to void decreased from 87% (26/30) at baseline to 23% (7/30) after 60 days. In addition, while 37% (11/30) of subjects reported severe nocturia waking up 2‒3 times per night to void at baseline, none did so after taking the study product for 60 days. By the end of the study there was an almost 6-fold increase [13% at baseline (4/30) to 77% (23/30) at Day 60] in percentage of participants who had an uninterrupted night without the need to wake up to urinate (Figure 1).
Table 2.
Change in International Prostate Symptom Score (IPSS) Total and Individual Symptom Sub-Scores at Day 30 and Day 60.
| Parameters Mean ± SD | Baseline | Day 30 | Day 60 |
|---|---|---|---|
| IPSS total | 4.3 ± 1.5 | 3.7 ± 2.0 | 3.6 ± 2.1* |
| IPSS individual symptom sub-scores | |||
| Incomplete emptying | 0.40 ± 0.56 | 0.40 ± 0.50 | 0.47 ± 0.50 |
| Frequency | 0.53 ± 0.62 | 0.53 ± 0.57 | 0.47 ± 0.57 |
| Intermittency | 0.57 ± 0.62 | 0.53 ± 0.73 | 0.40 ± 0.62 |
| Urgency | 0.57 ± 0.68 | 0.43 ± 0.63 | 0.43 ± 0.57 |
| Weak stream | 0.80 ± 0.76 | 0.73 ± 0.58 | 0.53 ± 0.63 |
| Straining | 0.17 ± 0.38 | 0.20 ± 0.41 | 0.23 ± 0.43 |
| Nocturia | 1.30 ± 0.79 | 0.90 ± 0.61* | 1.03 ± 0.72 |
Abbreviations: IPSS, International Prostate Symptom Score; SD, standard deviation.
*p < 0.05 compared with baseline with non-parametric Friedman one-way ANOVA repeated measures and Dunn’s multiple comparison post-test.
Figure 1.
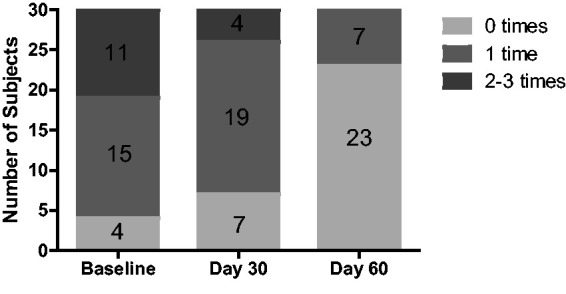
Number of Subjects Waking Up 0, 1, and 2‒3 Times per Night to Void at Baseline, Day 30, and Day 60.
Secondary Outcomes
Body weight, BMI, and PSA
There was no statistically significant change in body weight, BMI, and PSA either after 30 or 60 days of supplementation with the investigational product (Table 3).
Table 3.
Anthropometric Measurements, Vital Signs, and Blood Chemistry at Baseline, Day 30, and Day 60.
| Parameter Mean ± SD | Baseline | Day 30 | Day 60 |
|---|---|---|---|
| Anthropometric measurements | |||
| Body Weight (kg) | 84.6 ± 15.9 | 84.9 ± 15.4 | 84.6 ± 14.9 |
| Body Mass Index (kg/m2) | 26.4 ± 3.9 | 26.5 ± 3.8 | 26.4 ± 3.6 |
| Vital signs | |||
| Systolic Blood Pressure (mmHg) | 122.6 ± 10.0 | 116 .4 ± 10.3*** | 118.6 ± 10.3* |
| Diastolic Blood Pressure (mmHg) | 77.8 ± 7.8 | 74.7 ± 7.9* | 75.1 ± 7.4* |
| Heart Rate (beats/min) | 60.3 ± 7.2 | 62.5 ± 9.9 | 60 .3 ± 9.2 |
| Blood chemistry | |||
| PSA (ng/mL) | 1.6 ± 0. 9 | 1.5 ± 0.8 | 1.5 ± 0.9 |
| Glucose (mg/dL) | 93.1 ± 9.0 | 95.0 ± 7.4 | 96.6 ± 7.2* |
| AST (IU/L) | 22.5 ± 5.8 | 22.1 ± 6.2 | 21.7 ± 5.0 |
| ALT (IU/L) | 24.0 ± 9.0 | 23.4 ± 7.7 | 23.6 ± 7.6 |
| Total cholesterol (mg/dL) | 198.5 ± 35.4 | 193.2 ± 37.6 | 190.1 ± 37.0 |
| HDL cholesterol (mg/dL) | 55.1 ± 13.7 | 54.3 ± 13.5 | 55.3 ± 13.8 |
| LDL cholesterol (mg/dL) | 124.5 ± 33.9 | 119.7 ± 32.5 | 115.6 ± 31.1* |
| Total cholesterol/HDL ratio | 3.8 ± 1.1 | 3.7 ± 1.0 | 3.5 ± 1.1* |
| LDL/HDL ratio | 2.4 ± 1.0 | 7.7 ± 29.7 | 2.2 ± 0.8* |
| Triglycerides (mg/dL) | 95.0 ± 43.0 | 96.2 ± 50.8 | 96.7 ± 54.1 |
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PSA, prostate-specific antigen; SD, standard deviation.
*p < 0.05 compared with baseline with one-way ANOVA repeated measures and Dunnett’s multiple comparison post-test.
IPSS Quality of Life score
There was no statistically significant change from baseline (1.7 ± 1.2) in IPSS QoL score after 30 (1.4 ± 1.2) and 60 days (1.3 ± 1.0). The number of subjects who reported being delighted, pleased and mostly satisfied (score 0‒2) with their quality of life increased from 22 at baseline to 25 (+13.6%) at Day 30 and 28 (+27.3%) at Day 60. Concomitantly, the number of subjects who reported having mixed feelings (score 3) and being mostly dissatisfied (score 4) decreased from 8 at baseline to 5 (–37.5%) after 30 days and 2 (–75%) after 60 days (Figure 2).
Figure 2.
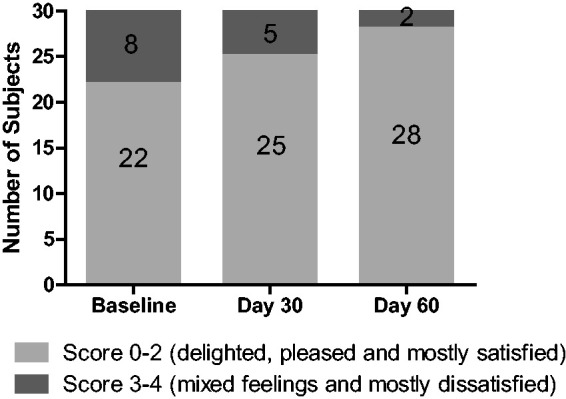
Number of Subjects Who Scored 0‒2 and 3‒4 in the International Prostate Symptoms Score Quality of Life Questionnaire at Baseline, Day 30, and Day 60.
International Index of Erectile Function (IIEF)-5
At baseline, the IIEF-5 score was 21.8 ± 2.6, indicating participants did not experience ED upon enrollment in the study. There was no statistically significant change in IIEF-5 score compared with baseline (21.8 ± 2.6) either after 30 (22.1 ± 2.5) or 60 (22.5 ± 2.7) days of supplementation with the investigational product.
SF-36 Health Survey
There was no statistically significant change in either the physical or emotional health component of the SF-36 Health Survey either at Day 30 or Day 60 compared with baseline (Table 4).
Table 4.
Scores From the SF-36 Health Survey at Baseline, Day 30, and Day 60.
| Parameters Mean ± SD | Baseline | Day 30 | Day 60 |
|---|---|---|---|
| Physical health component | |||
| Physical functioning | 92.7 ± 19.7 | 87.3 ± 26.8 | 96.5 ± 9.5 |
| Role limitations–Physical health | 93.3 ± 25.4 | 94.2 ± 22.4 | 97.5 ± 10.1 |
| Energy/fatigue | 77.5 ± 13.3 | 79.8 ± 10.8 | 75.5 ± 14.8 |
| General health | 85.7 ± 14.7 | 86.8 ± 12.8 | 86.7 ± 11.7 |
| Pain | 89.3 ± 16.7 | 89.9 ± 16.5 | 87.4 ± 18.8 |
| Emotional health component | |||
| Emotional well-being | 86.0 ± 9.6 | 88.3 ± 8.9 | 88.8 ± 11.1 |
| Role limitations–Emotional problems | 98.9 ± 6.1 | 100.0 ± 0.0 | 98.9 ± 6.9 |
| Social functioning | 95.8 ± 12.0 | 98.8 ± 6.9 | 97.1 ± 10.2 |
Abbreviation: SD, standard deviation.
Compliance
Average compliance with the study product was very high throughout the study (98.5 ± 4.9%) with similar rates of adherence at Day 30 (98.3 ± 6.7%) and Day 60 (98.7 ± 6.4%).
Safety
Adverse events
Seven (7) out of 30 enrolled study participants reported adverse events (23%). However, the reported unwanted effects were either not related or unlikely to be related to the study product. No subjects withdrew because of adverse events. On the basis of these results, the product evaluated in this study appears safe and well tolerated.
Vital signs
Within normal range at baseline, a significant 5.1% drop in the systolic blood pressure (122.6 ± 10.0 mmHg vs. 116.4 ± 10.3 mmHg, p < 0.0001) was recorded after 30 days of supplementation. Furthermore, at the same time point, a significant 4% decrease in the diastolic blood pressure (77.8 ± 7.8 mmHg vs. 74.7 ± 7.9 mmHg, p < 0.05) was also observed. After 60 days of supplementation, both systolic and diastolic blood pressure significantly decreased by 3.3% (122.6 ± 10.0 mmHg vs. 118.6 ± 10.3, p < 0.05) and 3.5% (77.8 ± 7.8 vs. 75.1 ± 7.4 mmHg, p < 0.05), respectively compared with baseline. Heart rate was also within normal range at baseline and did not significantly change either at Day 30 or Day 60 (Table 3).
Blood chemistry
At Day 60, blood glucose significantly increased by 3.8% relative to baseline (p < 0.05) but remained within normal limits. Liver enzymes AST and ALT were within normal range at baseline and did not change significantly either at Day 30 or Day 60. Blood lipids were also within normal limits at baseline, except LDL levels (124.5 ± 33.9 mg/dL), which were above the LabCorp upper reference limit. After 60 days of supplementation with the investigational product, although LDL cholesterol levels significantly decreased by 7.2% at Day 60 (p < 0.01) compared with baseline, they were still above normal range. At Day 60, total cholesterol/HDL and LDL/HDL ratios significantly decreased by 7.9% (p < 0.01) and 8.3% (p < 0.01), respectively, compared with baseline. Triglyceride and HDL cholesterol levels did not significantly change either at Day 30 or Day 60 (Table 3).
Discussion
In this open-label study, we found that males with mild LUTS who took one capsule of the prostate health formulation before bedtime for 60 days reported a significant reduction in the frequency of nighttime urination. Compliance was very high, and the product was safe and well tolerated throughout the study. Participants who received the dietary supplementation were overall healthy, although moderately overweight. This observation is in line with epidemiological data indicating that overweight men are more likely to develop LUTS compared with men of normal weight.36 In addition, subjects were in their late 50’s on average, had not received a diagnosis of BPH, and were not actively seeking medical treatment or advice for their urological problems. However, they complained of mild LUTS and nocturia which could be due to early stage age-related enlargement of the prostate, and therefore were likely to benefit from supplementation with the formulation tested in this study.
Supplementation for 60 days with the investigational product resulted in a significant 16% reduction from baseline in self-reported IPSS total score. This reduction was driven by a significant 30% decrease in nocturia IPSS sub-score after 30 days. Data also showed a sharp 64% decrease from baseline in the number of subjects who reported waking up at least one time per night to void after 60 days of supplementation. Upon completion of the study, no participants complained of waking up 2‒3 times per night compared with 37% at baseline, and the proportion of subjects who reported not having to wake up to void increased almost 6-fold compared with baseline. Among the many herbal supplements prescribed to manage symptoms of LUTS and BPH, saw palmetto (Serenoa repens) extract in monotherapy is one of the most popular in the United States and Europe. However, evidence shows mixed results and variability in measured outcomes, including nocturia which might be due to a lack of standardization of tested forms as the amount of active ingredients (sterols, fatty acids) varies widely across products.24,37–42 In combination with lycopene and selenium, saw palmetto has demonstrated some potential in the management of symptoms of BPH.43 Other phytotherapeutic compounds have shown beneficial effects on BPH symptoms.44–47 The product tested in our study is a dietary supplement formulation combining β-sitosterol, pygeum africanum bark extract, lycopene, boron, and melatonin to support prostate health. β-sitosterol is a phytosterol derived from pine tree and found in saw palmetto berry. In 2 randomized, placebo-controlled, double-blind clinical studies conducted in patients with BPH, β-sitosterol led to a significant decrease in IPSS total score and improvement of urinary flow parameters after 4 weeks and 6 months of treatment.48,49 A Cochrane systematic review found that β-sitosterol treatments helped relieving urinary symptoms and flow measures in males with mild to moderate BPH.50 These observations suggest that β-sitosterol might be an effective strategy to manage urinary symptoms of BPH.23 β-sitosterol is possibly exerting these beneficial effects through inhibition of 5-α-reductase, which converts testosterone into dihydrotestosterone, known to be involved in prostate cell proliferation.51,52 β-sitosterol has also been shown to inhibit growth and induce apoptosis of human prostate cancer LNCaP cells in vitro.53 Inflammation plays a key role in the pathogenesis of LUTS secondary to BPH.54 Experimental evidence also points to anti-inflammatory activities of β-sitosterol among other beneficial effects.28 Pygeum africanum bark extract is another ingredient of the investigational product tested in this study. Pygeum africanum is the scientific name for the African cherry tree and the bark of this tree has been used in Africa to improve urinary symptoms and bladder discomfort for centuries. A Cochrane meta-analysis of 18 clinical trials involving 1,500 patients with BPH concluded that pygeum africanum bark can modestly, yet significantly improve urologic symptoms especially nocturia.26 In preclinical research, pygeum africanum bark has been shown to display anti-proliferative and anti-apoptotic effects on human prostate cells from patients with BPH, as well as other pharmacologic and anti-inflammatory properties relevant to BPH.27,55 Lycopene, a powerful antioxidant found in tomatoes and several other red or pink fruits and vegetables is another ingredient featured in the investigational product that helps promoting prostate health.29 High intake of lycopene has been associated with reduced risk of prostate cancer and prostate cancer-specific mortality.30,31 Experimental studies suggest lycopene might do so by inhibiting growth factor signaling pathways, including insulin-like growth factor-1 (IGF-1), elevated levels of which have been associated with increased risk of prostate cancer.56–58 Lycopene also inhibits expression of pro-inflammatory cytokines interleukin-6 and interleukin-8, as well as androgen activation and signaling involved in the pathophysiology of BPH.57–60 Lycopene can inhibit growth of normal human prostate epithelial cells as well.32 The formulation tested in our study also contains the trace mineral boron (or boric acid), which has numerous health benefits.61 In an animal model of prostate cancer, boron was found to decrease PSA levels, reduce growth rate and size of tumors, and decrease IGF-1 expression in tumors.33 Interestingly, boron has the ability to block ryanodine receptors and reduce the release of calcium from the endoplasmic reticulum in prostate cancer cells, thereby reducing intracellular calcium signaling which is a key regulator of cell proliferation.62 Melatonin, a hormone produced in the brain which is involved in the regulation of sleep-wake cycles was also part of the study formulation. Beyond sleep support, evidence suggests a correlation between melatonin levels and nocturia. Sugaya and colleagues have reported a reduction in nighttime plasma levels of melatonin in subjects with nocturia compared with those who do not suffer from this condition.63 Furthermore, lower melatonin levels have been found in individuals complaining of bothersome nocturia compared with those who do not perceive nocturia as bothersome.64,65 In 2 randomized placebo-controlled trials, melatonin taken daily for 4 weeks was effective at significantly reducing nocturia in subjects suffering from LUTS.25,64 This beneficial effect might be mediated through high-affinity melatonin receptors expressed in human BPH and PC3 tumor epithelial cells.66,67 Evidence shows that anti-proliferative effects of melatonin in androgen-sensitive LNCaP human prostate tumor cells are melatonin receptor MT1-dependent.68
Systolic and diastolic blood pressure also decreased significantly on average by 5.1 and 2.9 mm Hg, respectively after supplementation with the investigational product. However, the clinical relevance of those beneficial effects remains to be established in subjects whose blood pressure was within normal range upon enrollment in the study. While the underlying mechanisms are currently unknown, some evidence suggests that this positive impact might be attributed to lycopene. Although results from epidemiological studies have reported conflicting results, a meta-analysis of intervention trials suggests that supplementation with lycopene might decrease blood pressure, which is consistent with our observations.69–71 Subjects who took the prostate health formulation also experienced a significant reduction in LDL cholesterol levels which were within normal range when the study began. Total cholesterol/HDL and LDL/HDL cholesterol ratios also significantly decreased but to a lesser extent. The mechanisms behind this favorable effect of the investigational product on lipid profile have yet to be defined. However, evidence suggests that β-sitosterol may be at least partially responsible for this outcome. The reason is that β-sitosterol is a phytosterol naturally occurring in plants with a structure similar to cholesterol with the ability to reduce intestinal cholesterol absorption and serum LDL-cholesterol levels.72,73 In addition, a systematic review and meta-analysis of randomized controlled trials found a significant association between melatonin supplementation and reduction in triglycerides and total cholesterol levels.74 However, our study did not report any significant changes in those lipid fractions following 60 days of supplementation with the prostate health formulation. Moreover, the dietary supplement that participants took appears to have an effect on glucose homeostasis as shown by a slight increase in serum glucose levels following 60 days of supplementation. However, they remain in the healthy range for the entire duration of the study. Again, the clinical significance of such a small change is ambiguous in individuals with glucose levels within normal limits throughout the study. The mechanisms involved are currently undetermined. Nevertheless, there is experimental evidence indicating that β-sitosterol and lycopene have the ability to decrease blood glucose levels in the context of diabetes.75–77 The question whether this effect might be due to one ingredient in particular in the formulation or a combination of ingredients with differential effects on glucose metabolism remains open to discussion.
Strengths and limitations
One strength of the study is it was conducted in a real-world setting with only 2 required follow-up visits to LECR. This design has the advantage of allowing subjects to be involved in a clinical study in the context of their normal day-to-day life with minimal disruption. Another strength is the very high compliance rate, which indicates that participants did not have any difficulties adhering to the assigned dosing schedule. The study also had limitations. One is this single-center study used a convenience sample, and not a population-based sample. Therefore, study results lack external validity and may not be applicable to the general population. In addition, strong causal conclusions are not merited. Next, the open label design increased risk of potential bias, as participants had knowledge of the product they were taking. Also, it was an uncontrolled single-arm prospective study with no placebo group. Thus, no definite conclusion about the clinical efficacy of the tested formulation can be drawn from this preliminary study. Lastly, the biological activity and clinical efficacy of β-sitosterol and pygeum africanum extracts contained in the formulation evaluated in this study are likely to differ from extracts manufactured and distributed by other suppliers. Therefore, the effects reported in our study might not be extrapolated to others that might be observed with different formulations featuring β-sitosterol and pygeum africanum. Slight unpredictable batch-to-batch variations in the concentration of active ingredients are also to be expected and might account for occasional differences in biological effects of our prostate health formulation.
Conclusions
Healthy males with mild LUTS reported a striking reduction in the episodes of nocturia while taking the prostate health dietary supplement. The formulation of the investigational product could be considered as a safe and attractive alternative option for individuals with mild LUTS symptoms willing to explore a non-conventional approach to manage their nocturia. Supplementation with the study product may also help support healthy blood pressure and lipid profile. The underlying mechanisms are not fully understood and need to be further investigated. A larger scale randomized placebo-controlled study is needed to confirm these preliminary promising results.
Acknowledgments
We are grateful to the volunteers who participated in the study. We also would like to thank Shayna Sandhaus, PhD, Lori Feldman, RD, CCRC and Jana Barlic-Dicen, PhD for reviewing this manuscript.
Footnotes
Author Contributions: SPH conducted and managed the study. SVJ and AGS participated in the conception and design of the study. MP analyzed and interpreted data and wrote the manuscript. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time of preparing this manuscript, all the authors were employed at Life Extension.
Research ethics and patient consent: The study was conducted in accordance with the ethical standards set forth in World Medical Association Declaration of Helsinki. A signed informed consent was obtained from each participant. Subjects were permitted to discontinue participation at any time without providing reasons. The study protocol was approved by IntegReview Investigational Review Board.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Supplement Formulators, Inc. (Fort Lauderdale, FL).
ORCID iD: Marianne Pons https://orcid.org/0000-0001-7650-8503
References
- 1.Irwin DE, Kopp ZS, Agatep B, Milson I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011; 108(7):1132–1138. [DOI] [PubMed] [Google Scholar]
- 2.Coyne KS, Wein AJ, Tubaro A, et al. The burden of lower urinary tract symptoms: evaluating the effect of LUTS on health-related quality of life, anxiety and depression: EpiLUTS. BJU Int. 2009; 103 Suppl 3:4–11. [DOI] [PubMed] [Google Scholar]
- 3.Dunphy C, Laor L, Te A, Kaplan S, Chughtai B. et al. Relationship between depression and lower urinary tract symptoms secondary to benign prostatic hyperplasia. Rev Urol. 2015; 17(2):51–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Smith DP, Weber MF, Soga K, et al. Relationship between lifestyle and health factors and severe lower urinary tract symptoms (LUTS) in 106,435 middle-aged and older Australian men: population-based study. PLoS One. 2014; 9(10):e109278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Van Kerrebroeck P, Abrams P, Chaikin D, et al. The standardization of terminology in nocturia: report from the standardization subcommittee of the International Continence Society. BJU Int. 2002; 90 Suppl 3:11–15. [DOI] [PubMed] [Google Scholar]
- 6.Everaert K, Anderson P, Wood R, Andersson FL, Holm-Larsen T. et al. Nocturia is more bothersome than daytime LUTS: results from an observational, real-life practice database including 8659 European and American LUTS patients. Int J Clin Pract. 2018; 72(6):e13091. [DOI] [PubMed] [Google Scholar]
- 7.Zumrutbas AE, Bozkurt AI, Alkis O, Toktas C, Cetinel B, Aybek Z. et al. The prevalence of nocturia and nocturnal polyuria: can new cutoff values be suggested according to age and sex? Int Neurourol J. 2016; 20(4):304–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miranda Ede P, Gomes CM, Torricelli FC, et al. Nocturia is the lower urinary tract symptom with greatest impact on quality of life of men from a community setting. Int Neurourol J. 2014; 18(2):86–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Oelke M, De Wachter S, Drake MJ, et al. A practical approach to the management of nocturia. Int J Clin Pract. 2017; 71(11):▪. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shao IH, Wu CC, Hsu HS, et al. The effect of nocturia on sleep quality and daytime function in patients with lower urinary tract symptoms: a cross-sectional study. Clin Interv Aging. 2016; 11:879–885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kupelian V, Wei JT, O’Leary MP, Norgaard JP, Rosen RC, McKinlay JB. et al. Nocturia and quality of life: results from the Boston area community health survey. Eur Urol. 2012; 61(1):78–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kim SY, Bang W, Kim MS, Park B, Kim JH, Choi HG. et al. Nocturia is associated with slipping and falling. PLoS One. 2017; 12(1):e0169690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Holm-Larsen T. The economic impact of nocturia. Neurourol Urodyn. 2014; 33 Suppl 1:S10–S14. [DOI] [PubMed] [Google Scholar]
- 14.Stanley N. The underestimated impact of nocturia on quality of life. Eur Urol Suppl. 2005; 4(7):17–9. [Google Scholar]
- 15.Welliver C, Sulaver R, Whittington A, et al. Analyzing why men seek treatment for lower urinary tract symptoms and factors associated with nonimprovement. Urology. 2015; 86(5):862–867. [DOI] [PubMed] [Google Scholar]
- 16.Bailey RL, Gahche JJ, Lentino CV, et al. Dietary supplement use in the United States, 2003–2006. J Nutr. 2011; 141(2):261–266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eliaz I, Weil E, Wilk B. Improvements in self-reported lower urinary tract symptoms with prostate health supplement. Altern Ther Health Med. 2018; 24(5): 26–32. [PubMed] [Google Scholar]
- 18.Lee CL, Kuo HC. Pathophysiology of benign prostate enlargement and lower urinary tract symptoms: Current concepts. Ci Ji Yi Xue Za Zhi. 2017; 29(2):79–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Medina JJ, Parra RO, Moore RG. Benign prostatic hyperplasia (the aging prostate). Med Clin North Am. 1999; 83(5):1213–1229. [DOI] [PubMed] [Google Scholar]
- 20.Dimitropoulos K, Gravas S. New therapeutic strategies for the treatment of male lower urinary tract symptoms. Res Rep Urol. 2016; 8:51–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fine ND, Weiss JP, Wein AJ. Nocturia: consequences, classification, and management. F1000Res. 2017; 6:1627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Roehrborn CG. Lower urinary tract symptoms, benign prostatic hyperplasia, erectile dysfunction, and phosphodiesterase-5 inhibitors. Rev Urol. 2004; 6(3):121–127. [PMC free article] [PubMed] [Google Scholar]
- 23.Wilt TJ, MacDonald R, Ishani A. beta-sitosterol for the treatment of benign prostatic hyperplasia: a systematic review. BJU Int. 1999; 83(9):976–983. [DOI] [PubMed] [Google Scholar]
- 24.Keehn A, Lowe FC. Complementary and alternative medications for benign prostatic hyperplasia. Can J Urol. 2015; 22 Suppl 1:18–23. [PubMed] [Google Scholar]
- 25.Drake MJ, Mills IW, Noble JG. Melatonin pharmacotherapy for nocturia in men with benign prostatic enlargement. J Urol. 2004; 171(3):1199–1202. [DOI] [PubMed] [Google Scholar]
- 26.Ishani A, MacDonald R, Nelson D, Rutks I, Wilt T J. et al. Pygeum africanum for the treatment of patients with benign prostatic hyperplasia: a systematic review and quantitative meta-analysis. Am J Med. 2000; 109(8):654–664. [DOI] [PubMed] [Google Scholar]
- 27.Andro MC, Riffaud JP. Pygeum africanum extract for the treatment of patients with benign prostatic hyperplasia: a review of 25 years of published experience. Cur Ther Res. 1995; 56(8):796–817. [Google Scholar]
- 28.Saeidnia S, Manayi A, Gohari AR, Abdollahi M. et al. The story of beta-sitosterol—a review. Eur J Med Plants. 2014; 4(5):590–609. [Google Scholar]
- 29.Chen P, Zhang W, Wang X, et al. Lycopene and risk of prostate cancer: a systematic review and meta-analysis. Medicine (Baltimore). 2015; 94(33):e1260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Giovannucci E, Rimm EB, Liu Y, Stampfer MJ, Willet WC. et al. A prospective study of tomato products, lycopene, and prostate cancer risk. J Natl Cancer Inst. 2002; 94(5):391–398. [DOI] [PubMed] [Google Scholar]
- 31.Wang Y, Jacobs EJ, Newton CC, McCullough ML. et al. Lycopene, tomato products and prostate cancer-specific mortality among men diagnosed with nonmetastatic prostate cancer in the Cancer Prevention Study II Nutrition Cohort. Int J Cancer. 2016; 138(12):2846–2855. [DOI] [PubMed] [Google Scholar]
- 32.Obermuller-Jevic UC, Olano-Martin E, Corbacho AM, et al. Lycopene inhibits the growth of normal human prostate epithelial cells in vitro. J Nutr. 2003; 133(11): 3356–3360. [DOI] [PubMed] [Google Scholar]
- 33.Gallardo-Williams MT, Chapin RE, King PE, et al. Boron supplementation inhibits the growth and local expression of IGF-1 in human prostate adenocarcinoma (LNCaP) tumors in nude mice. Toxicol Pathol. 2004; 32(1):73–78. [DOI] [PubMed] [Google Scholar]
- 34.Berges RR, Windeler J, Trampisch HJ, Senge T. et al. Randomised, placebo-controlled, double-blind clinical trial of beta-sitosterol in patients with benign prostatic hyperplasia. Beta-sitosterol Study Group. Lancet. 1995; 345(8964): 1529–1532. [DOI] [PubMed] [Google Scholar]
- 35.Rosen RC, Cappelleri JC, Smith MD, Lipsky MD, Pena BM. et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999; 11(6):319–326. [DOI] [PubMed] [Google Scholar]
- 36.Parsons JK, Messer K, White M, et al. Obesity increases and physical activity decreases lower urinary tract symptom risk in older men: the osteoporotic fractures in men study. Eur Urol. 2011; 60(6):1173–1180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Penugonda K, Lindshield BL. Fatty acid and phytosterol content of commercial saw palmetto supplements. Nutrients. 2013; 5(9):3617–3633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wilt TJ, Ishani A, Stark G, MacDonald R, Lau J, Mulrow C. et al. Saw palmetto extracts for treatment of benign prostatic hyperplasia: a systematic review. JAMA. 1998; 280(18):1604–1609. [DOI] [PubMed] [Google Scholar]
- 39.Mantovani F. Serenoa repens in benign prostatic hypertrophy: analysis of 2 Italian studies. Minerva Urol Nefrol. 2010; 62(4):335–40. [PubMed] [Google Scholar]
- 40.MacDonald R, Tacklind JW, Rutks I, et al. Serenoa repens monotherapy for benign prostatic hyperplasia (BPH): an updated Cochrane systematic review. BJU Int. 2012; 109(12):1756–1761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tacklind J, Macdonald R, Rutks I, Wilt TJ. et al. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2012. ;12:CD001423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Vela-Navarrete R, Alcaraz A, Rodriguez-Antolin A, et al. Efficacy and safety of a hexanic extract of Serenoa repens (Permixon((R))) for the treatment of lower urinary tract symptoms associated with benign prostatic hyperplasia (LUTS/BPH): systematic review and meta-analysis of randomised controlled trials and observational studies. BJU Int. 2018; 122(6):1049–1065. [DOI] [PubMed] [Google Scholar]
- 43.Minutoli L, Bitto A, Squadrito F, et al. et al. Serenoa Repens, lycopene and selenium: a triple therapeutic approach to manage benign prostatic hyperplasia. Curr Med Chem. 2013; 20(10):1306–1312. [DOI] [PubMed] [Google Scholar]
- 44.MacDonald R, Ishani A, Rutks I, Wilt TJ. et al. A systematic review of Cernilton for the treatment of benign prostatic hyperplasia. BJU Int. 2000; 85(7):836–841. [DOI] [PubMed] [Google Scholar]
- 45.Shrivastava A, Gupta VB. Various treatment options for benign prostatic hyperplasia: a current update. J Midlife Health. 2012; 3(1):10–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Vahlensieck W, Theurer C, Pfitzer E, Patz B, Banik N, Engelmann U. et al. Effects of pumpkin seed in men with lower urinary tract symptoms due to benign prostatic hyperplasia in the one-year, randomized, placebo-controlled GRANU study. Urol Int. 2015; 94(3):286–295. [DOI] [PubMed] [Google Scholar]
- 47.Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled, crossover study. J Herb Pharmacother. 2005; 5(4):1–11. [PubMed] [Google Scholar]
- 48.Berges RR, Kassen A, Senge T. Treatment of symptomatic benign prostatic hyperplasia with beta-sitosterol: an 18-month follow-up. BJU Int. 2000; 85(7):842–846. [DOI] [PubMed] [Google Scholar]
- 49.Klippel KF, Hiltl DM, Schipp B. A multicentric, placebo-controlled, double-blind clinical trial of beta-sitosterol (phytosterol) for the treatment of benign prostatic hyperplasia. German BPH-Phyto Study group. Br J Urol. 1997; 80(3):427–432. [PubMed] [Google Scholar]
- 50.Wilt T, Ishani A, MacDonald R, Stark G, Mulrow C, Lau J. et al. Beta-sitosterols for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2000; 2:CD001043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Cabeza M, Bratoeff E, Heuze I, Ramírez E, Sanchez M, Flores E. et al. Effect of beta-sitosterol as inhibitor of 5 alpha-reductase in hamster prostate. Proc West Pharmacol Soc. 2003; 46:153–155. [PubMed] [Google Scholar]
- 52.Carson C, III, Rittmaster R. The role of dihydrotestosterone in benign prostatic hyperplasia. Urology. 2003; 61(4):2–7. [DOI] [PubMed] [Google Scholar]
- 53.von Holtz RL, Fink CS, Awad AB. Beta-Sitosterol activates the sphingomyelin cycle and induces apoptosis in LNCaP human prostate cancer cells. Nutr Cancer. 1998; 32(1):8–12. [DOI] [PubMed] [Google Scholar]
- 54.Ficarra V, Rossanese M, Zazzara M, et al. The role of inflammation in lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) and its potential impact on medical therapy. Curr Urol Rep. 2014; 15(12):463. [DOI] [PubMed] [Google Scholar]
- 55.Quiles MT, Arbos MA, Fraga A, de Torres IM, Reventos J, Morote J. et al. Antiproliferative and apoptotic effects of the herbal agent Pygeum africanum on cultured prostate stromal cells from patients with benign prostatic hyperplasia (BPH). Prostate. 2010; 70(10):1044–1053. [DOI] [PubMed] [Google Scholar]
- 56.Shi R, Berkel HJ, Yu H. Insulin-like growth factor-I and prostate cancer: a meta-analysis. Br J Cancer. 2001; 85(7): 991–996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Wertz K, Siler U, Goralczyk R. Lycopene: modes of action to promote prostate health. Arch Biochem Biophys. 2004; 430(1):127–134. [DOI] [PubMed] [Google Scholar]
- 58.Trejo-Solis C, Pedraza-Chaverri J, Torres-Ramos M, et al. Multiple molecular and cellular mechanisms of action of lycopene in cancer inhibition. Evid Based Complement Alternat Med. 2013; 2013:705121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Penna G, Fibbi B, Amuchastegui S, et al. Human benign prostatic hyperplasia stromal cells as inducers and targets of chronic immuno-mediated inflammation. J Immunol. 2009; 182(7):4056–4064. [DOI] [PubMed] [Google Scholar]
- 60.Izumi K, Mizokami A, Lin WJ, Lai KP, Chang C. et al. Androgen receptor roles in the development of benign prostate hyperplasia. Am J Pathol. 2013; 182(6):1942–1949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Pizzorno L. Nothing boring about boron. Integr Med: Clin J. 2015; 14(4):35–48. [PMC free article] [PubMed] [Google Scholar]
- 62.Henderson K, Stella SL, Kobylewski S, Eckhert CD. et al. Receptor activated Ca(2+) release is inhibited by boric acid in prostate cancer cells. PLoS One. 2009; 4(6):e6009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Sugaya K, Nishijima S, Oda M, Owan T, Miyazato M, Ogawa Y. et al. Biochemical and body composition analysis of nocturia in the elderly. Neurourol Urodyn. 2008; 27(3):205–211. [DOI] [PubMed] [Google Scholar]
- 64.Sugaya K, Nishijima S, Miyazato M, et al. Effects of melatonin and rilmazafone on nocturia in the elderly. J Int Med Res. 2007; 35(5):685–691. [DOI] [PubMed] [Google Scholar]
- 65.Sugaya K, Nishijima S, Miyazato M, et al. Investigation of biochemical factors related to non-bothersome noctural urination. Biochem Res. 2007; 28(4):213–217. [DOI] [PubMed] [Google Scholar]
- 66.Gilad E, Laudon M, Matzkin H, et al. et al. Functional melatonin receptors in human prostate epithelial cells. Endocrinology. 1996; 137(4):1412–1417. [DOI] [PubMed] [Google Scholar]
- 67.Gilad E, Laufer M, Matzkin H, Zisapel N. et al. Melatonin receptors in PC3 human prostate tumor cells. J Pineal Res. 1999; 26(4):211–220. [DOI] [PubMed] [Google Scholar]
- 68.Xi SC, Siu SW, Fong SW, Shiu SY. et al. Inhibition of androgen-sensitive LNCaP prostate cancer growth in vivo by melatonin: association of antiproliferative action of the pineal hormone with mt1 receptor protein expression. Prostate. 2001; 46(1):52–61. [DOI] [PubMed] [Google Scholar]
- 69.Engelhard YN, Gazer B, Paran E. Natural antioxidants from tomato extract reduce blood pressure in patients with grade-1 hypertension: a double-blind, placebo-controlled pilot study. Am Heart J. 2006; 151(1):100. [DOI] [PubMed] [Google Scholar]
- 70.Kim JY, Paik JK, Kim OY, et al. Effects of lycopene supplementation on oxidative stress and markers of endothelial function in healthy men. Atherosclerosis. 2011; 215(1):189–195. [DOI] [PubMed] [Google Scholar]
- 71.Li X, Xu J. Lycopene supplement and blood pressure: an updated meta-analysis of intervention trials. Nutrients. 2013; 5(9):3696–3712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.De Smet E, Mensink RP, Plat J. Effects of plant sterols and stanols on intestinal cholesterol metabolism: suggested mechanisms from past to present. Mol Nutr Food Res. 2012; 56(7):1058–1072. [DOI] [PubMed] [Google Scholar]
- 73.Racette SB, Lin X, Lefevre M, et al. Dose effects of dietary phytosterols on cholesterol metabolism: a controlled feeding study. Am J Clin Nutr. 2010; 91(1):32–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Mohammadi-Sartang M, Ghorbani M, Mazloom Z. Effects of melatonin supplementation on blood lipid concentrations: a systematic review and meta-analysis of randomized controlled trials. Clin Nutr. 2018; 37(6 Pt A):1943–1954. [DOI] [PubMed] [Google Scholar]
- 75.Gupta R, Sharma AK, Dobhal MP, Sharma MC, Gupta RS. et al. Antidiabetic and antioxidant potential of β-sitosterol in streptozotocin-induced experimental hyperglycemia. J Diabetes. 2011; 3(1):29–37. [DOI] [PubMed] [Google Scholar]
- 76.Ramalingam S, Packirisamy M, Karuppiah M, et al. Effect of β-sitosterol on glucose homeostasis by sensitization of insulin resistance via enhanced protein expression of PPRγ and glucose transporter 4 in high fat diet and streptozotocin-induced diabetic rats. Cytotechnology. 2020; 72(3):357–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Yin Y, Zheng Z, Jiang Z. Effects of lycopene on metabolism of glycolipid in type 2 diabetic rats. Biomed Pharmacother. 2019; 109:2070–2077. [DOI] [PubMed] [Google Scholar]