

Abstract
Non-communicable disease (NCD) prevention efforts have traditionally targeted high-risk and high-burden populations. We propose an alteration in prevention efforts to also include emphasis and focus on low-risk populations, predominantly younger individuals and low-prevalence populations. We refer to this approach as “proactive prevention.” This emphasis is based on the priority to put in place policies, programs, and infrastructure that can disrupt the epidemiological transition to develop NCDs among these groups, thereby averting future NCD crises. Proactive prevention strategies can be classified, and their implementation prioritized, based on a 2-dimensional assessment: impact and feasibility. Thus, potential interventions can be categorized into a 2-by-2 matrix: high impact/high feasibility, high impact/low feasibility, low impact/high feasibility, and low impact/low feasibility. We propose that high impact/high feasibility interventions are ready to be implemented (act), while high impact/low feasibility interventions require efforts to foster buy-in first. Low impact/high feasibility interventions need to be changed to improve their impact while low impact/low feasibility might be best re-designed in the context of limited resources. Using this framework, policy makers, public health experts, and other stakeholders can more effectively prioritize and leverage limited resources in an effort to slow or prevent the evolving global NCD crisis.
Introduction
The majority of global non-communicable disease (NCD) burden is attributable to modifiable behavioral and environmental risk factors: tobacco use, unhealthy diet, physical inactivity, harmful alcohol use, and air pollution [1]. These risk factors have been highlighted as both high priority, and cost-effective targets for NCD prevention and control [2]. In many regions of the world, and in many populations, prevention efforts such as healthy eating, increasing physical activity, and smoking cessation focus on individuals who are already at high risk (e.g. due to the presence of metabolic risk factors) and populations with high prevalence of NCD, and are therefore largely “reactive” [2, 3]. These efforts reduce NCD prevalence, morbidity, and mortality, and as such need to continue.
However, there is an important gap. If the “reactive prevention” approach alone is implemented around the world, the global NCD community will likely soon be confronting a situation of “too little, too late.” To complement these efforts, there is therefore a concomitant need to target individuals at low risk and populations with relatively lower burden at the current critical time period. We call this approach “proactive prevention,” which refers to implementation of public health policy and other interventions that create environments and facilitate behaviors to disrupt the epidemiological transition and maintain the lower burden of low-risk individuals and low-NCD prevalence populations.
The most compelling reason to initiate proactive prevention is to slow or eliminate the development of a high disease burden at the population level. Even in countries with already high NCD burden, segments of the population, particularly children and adolescents, are at low risk or have not yet been afflicted [4]. Early health promotion efforts could delay or wholly prevent progression to overt NCDs over the course of their lifetime [4, 5], thus reducing premature death and disability. The critical window to pursue proactive prevention will soon no longer be present and the time to act is now!
In this paper, we first define and characterize low-burden and low-risk populations who have the highest potential benefit from proactive prevention strategies. We then propose a novel framework using concepts of impact and feasibility to stratify and prioritize potential proactive prevention interventions, highlighting evidence-based examples. Finally, we suggest a way forward for proactive prevention strategies to be realized. Our overall framework was initially developed by three of co-authors (RV, BN, SF), then modified in an iterative fashion in consultation and discussion with all co-authors. The final framework and approach was approved by consensus by all co-authors.
Target populations for proactive prevention
In the context of proactive prevention strategies, it is necessary to define what a “low-burden” or a “high-burden” population is. While we acknowledge that no absolute consensus will be achieved in terms of this distinction, we offer two illustrative examples of relatively “low-burden” populations. For instance, Fig 1 demonstrates that low- to mid-socio-demographic index populations currently have relatively lower mortality rates due to NCD risk factors, and therefore would benefit from proactive prevention efforts to maintain the lower NCD-related mortality rates [6]. Fig 2 portrays similar information, categorized by age rather than socio-demographic index, showing that younger individuals will largely benefit from proactive prevention as well [6]. We recognize and acknowledge that one of the limitations of a comparative risk assessment approach to estimating risk-attributable deaths or disability adjusted life years is that period effects are assumed for each age group when in reality present-day burden is a function of exposure in decades past. Proactive prevention therefore aims to decrease future length of exposure to NCD risk factors among these populations.
Fig 1. Deaths per 100,000 attributed to NCD risk factors, stratified by socio-demographic index (SDI) [6].
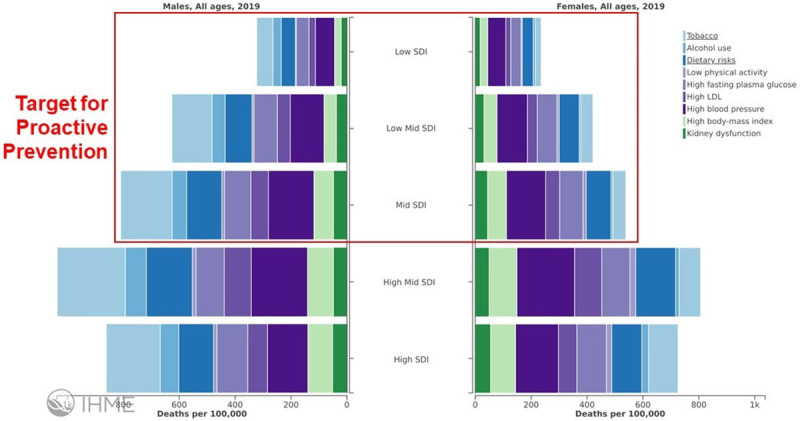
The potential for proactive prevention in relatively lower-burden populations is highlighted.
Fig 2. Global death rate attributed to metabolic risk factors stratified by age [6].

The potential for proactive prevention relatively lower-burden individuals at younger ages is highlighted.
Prioritizing proactive prevention: Impact and feasibility
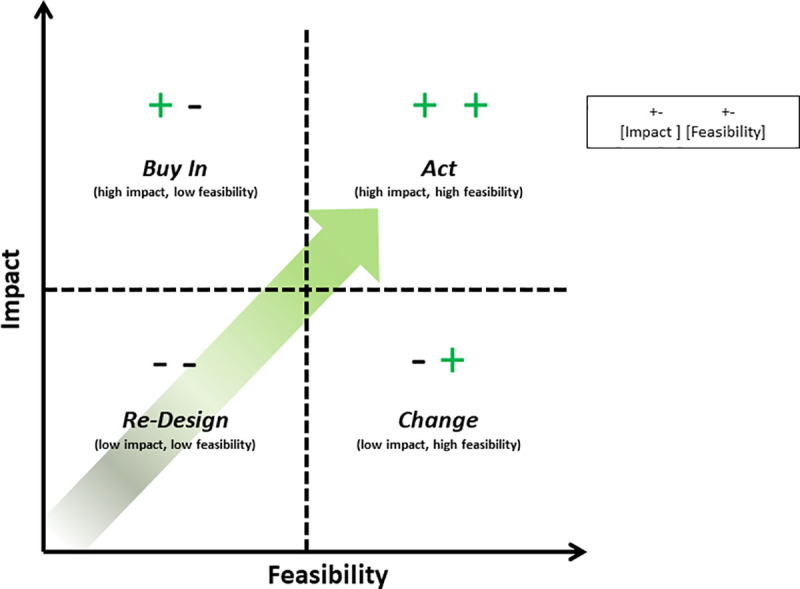
We propose a simple categorization scheme for potential proactive prevention interventions, “graded” along two dimensions: impact and feasibility. Each dimension—impact and feasibility—can be graded as “high” or “low” resulting in a simple 2x2 framework with four possible combinations: high-impact, high-feasibility (“Act”); high-impact, low-feasibility (“Buy In”); low-impact, high feasibility (“Change”); and low-impact, low-feasibility (“re-Design). It should be noted, however, that these categories fall along a continuum (Fig 3), and there are no specific cut-offs to determine what is “high” vs “low” impact or feasibility. In addition, these assessments will likely vary based upon the specific target population or geographic region of implementation. We have intentionally made this framework simplistic as our hope is to promote improved utility for policymakers and program implementers to help prioritize strategic proactive prevention interventions.
Fig 3. Impact and feasibility framework, illustrating the four graded categories of proactive prevention strategies: Act, buy in, change, re-design.
When referring to “impact,” we incorporate the following elements: (a) effectiveness of the intervention on reducing disability and deaths, (b) relevance to the intended recipients taking into account current burden and future risk based on exposure over time, (c) long-term positive and negative consequences of the intervention as well as consequences of inaction, (d) reach (the number of persons served by an intervention, their representativeness, and equity), (e) efficiency in the intervention’s use of resources, (f) sustainability in terms of long-term inputs to maintain the intervention, (g) scalability which refers to the potential for the intervention to be scaled up to larger communities and populations, and (h) expansion potential to new populations or settings [7, 8].
Feasibility encompasses the (a) acceptability of the intervention to recipients and stakeholders, demand for the intervention, (b) implementation insofar as an intervention can be enacted as designed in a real-world setting, (c) practicality in terms of resource constraints, (d) adaptability to various situations, and (e) integration with regard to the necessary system change needed to incorporate an intervention into existing infrastructure and communities [9]. Finally, ethical and human rights considerations should underlie the entire process of considering potential interventions and determining their impact or feasibility.
In summary, proactive prevention efforts can be prioritized in relation to an intervention’s impact and feasibility. As illustrated in Fig 3, interventions in quadrant A (“Act”) should be prioritized for implementation. Quadrant B (“Buy In”) requires mobilization efforts to gain buy in from various stakeholders. Quadrant C (“Change”) are those which should be modified for improved effectiveness before implementation is attempted. Finally, quadrant D (“re-Design”) interventions should be re-designed until both improved impact and feasibility can be demonstrated. In the following sections, we describe examples of proactive prevention interventions that illustrate our proposed impact-feasibility framework. These examples are not meant to be exhaustive, but rather illustrative, as we recognize that there are many more interventions that can fit into each of the categories.
High impact/high feasibility: Act
Interventions in the high impact/high feasibility category are the most vital and urgent to institute, they require us to ACT. These tend to be population-level interventions which are both effective and have a broad reach [3, 10]. This category usually involves government action in the form of fiscal policies or regulatory/legislative interventions and generally garner benefit by altering the choice architecture of citizens in favor of opting for the healthful intervention. They are often highly acceptable to the public with the public health benefit being understood and supported by the general population. These interventions sometimes have the additional beneficial consequence of being revenue-producing [11]. Exemplar interventions in this category are: excise taxes on tobacco, and trans-fatty acid elimination.
High excise taxes on tobacco
The reduction of tobacco usage by a variety of policies has been extensively studied [12] and endorsed by the World Health Organization (WHO) [13]. Implementation of tobacco taxes are one of the most effective means of tobacco reduction when compared to other methods, and this intervention has been studied in many different countries using a variety of tax structures [14, 15]. In the short-term, it is second only to comprehensive smoke-free air laws, while in the long-term it has the largest overall effect [12]. Tobacco taxes also have the lowest estimated annual cost of tobacco control measures as estimated by the WHO, and have the added benefit of generating revenue that can be invested in health promotion efforts [12, 16].
Trans-fatty acid elimination
Various methods to reduce the consumption of trans-fatty acids (TFAs) have been studied, including dietary counseling, food labeling, voluntary food reformulation, and legislation of TFA maximums [17]. The single intervention with the highest level of effectiveness in reducing daily dietary TFA intake has been legislation [17, 18]. As an upstream intervention, well implemented legislation has a population-level reach and impact that is substantial [19]. It is relevant population-wide as cardiovascular disease is a long-term consequence of TFA intake for all people. It is sustainable as high TFA foods are essentially eliminated as a dietary option. Despite the feasibility concerns such as acceptability and demand that accompany most public health legislative efforts, TFA bans have been in effect for many years in several places worldwide, with Denmark being an early adopter, as well as New York City [17, 18]. Other countries, such as South Africa and Columbia have mandatory limits, and the WHO is calling for a worldwide ban by the year 2023 [20].
High impact/low feasibility: Buy In
High Impact/low feasibility opportunities should also be prioritized to slow the impending NCD crisis. These generally share some of the characteristics of the “Act” interventions above. These are usually far-reaching population-level interventions; however, they are often characterized by lower acceptability to governments due to high costs of implementation, long-term investment, practical constraints such as infrastructure changes, and market distortion. The potential impact of interventions in this category can be significant, but only if we can obtain BUY IN to overcome the initial barriers to these upstream interventions. The two examples illustrative of this category are: restructuring built environments to encourage physical activity and implementing subsidies for healthier fruits and vegetables.
Restructuring built environments to encourage physical activity
Many studies have shown associations between built environment attributes and the amount of physical activity of people, with evidence accumulating on the health benefits of living in neighborhoods with well-connected street networks, pedestrian access, and recreational facilities [21–24]. Neighborhood features such as street connectivity, residential density, leisure space and availability of traffic devices improve neighborhood walkability and promote walking, leisure and transport related to physical activity such as biking. This has been demonstrated for young adults, the elderly and children [25–28]. For example, there is extensive evidence that the availability of parks, playgrounds, and green spaces as well as other neighborhood features such as walkability and safety, profoundly shape children’s daily physical activity patterns [29–33]. Moreover, a broader, more ambitious built environment agenda would integrate physical activity with road safety measures in urban settings and thus have large co-benefits with injury prevention. This is particularly relevant in low-income countries where rapid urbanization continues.
Implementing subsidies for healthier fruits and vegetables
The WHO recommends that individuals consume at least 400 grams (equal to five servings) of fruits and vegetables (F&V) per day [34]. There are multiple barriers to achieving this recommendation. F&V and healthier diets generally cost more than foods of lower nutritional value [35]. There is a 22% supply gap in meeting current need for F&V, with low-income countries experiencing the largest gap [36]. There is substantial evidence of the benefit of subsidies for F&V on increased consumption. A review of studies employing subsidies to promote healthy food purchase and consumption (including F&V) showed that in 19 of the 20 reviewed studies, subsidies on healthier foods resulted in significant increase in the purchase and consumption of promoted products [37]. One large-scale example of F&V subsidization is the European School Fruit Scheme which since 2017 has been combined with a dairy scheme; the scheme provides free F&V to approximately 159,000 schools and is financed by a combination of EU, national, private, and parental contributions [37, 38]. In an evaluation of the scheme in Germany, an increase of F&V intake from 1.26 to 2.02 times per day was observed after one year’s delivery of the program [39]. In the United States, subsidization of F&V in the Supplemental Nutrition Assistance Program (SNAP) is associated with increased consumption of F&V [40, 41]. However, increasing the supply of F&V requires changing incentives within food production systems [42] and a shift away from the current emphasis on staple grain production [43]. Money budgeted toward ineffective subsidies, such as grain production or fossil fuels, have the potential to be reallocated toward F &V to overcome cost barriers [44]. Trade policies and the need to change dietary behavior also remain among the potential roadblocks, as there continue to be substantial challenges, both within countries and trans-nationally, to enact and implement the necessary policies to achieve this goal.
Low impact/high feasibility: Change
Low impact/high feasibility interventions tend to be less “whole population”-based than the above two categories. They may only target certain segments of the population, reducing reach and overall impact, but are often easier to enact because aspects such as demand, practicality, and the ability to implement the intervention are far greater. This type of intervention less often needs governmental changes in policy or legislation, so there are fewer bureaucratic challenges. Public health interventions falling in this category would benefit from CHANGE to improve impact, as it is imperative to allocate available resources to those interventions with optimal public health benefit to curb the increases in NCDs. Examples of interventions that would benefit from change include: child obesity prevention strategies, and mass media campaigns to address NCD risk factors.
Child obesity prevention strategies
Obesity in children and adolescents continues to increase worldwide and is recognized as a major contributing risk factor to premature mortality due to NCDs [45]. However, most school-based educational strategies have had little to no impact on prevention of obesity and have been characterized by sustainability challenges [4, 46, 47]. A recent modeling study assessed a package of interventions for NCD risk reduction among adolescents, targeting tobacco smoking, alcohol use, tax on sugar-sweetened beverages, and a school-based program for physical activity and healthy diet [4]. Although the study predicted a mortality benefit from the school-based program, its benefit-cost ratio was very low because costs were so high [4]. In summary, child obesity programs appear to need to be multi-faceted and include home- and community-based aspects. In addition, these programs must be supported by policy to address social, economic, and environmental determinants of health [46, 48, 49].
Mass media campaigns to address NCD risk factors
Implementing mass media campaigns as public health initiatives has been common practice for decades [50]. Generally, mass media campaigns are a simple way to increase knowledge and awareness of an issue. However, while abundant, such campaigns are ultimately inconsistent in their impact. While some campaigns have shown moderate to strong evidence for benefit in combatting certain risk factors, such as tobacco use, physical activity, and nutrition, other research on alcohol use, certain cancer screenings, mental health, obesity and more have not shown evidence for benefit [51, 52]. Furthermore, impact is inconsistent and mixed across the literature for the same behaviors or conditions [53]. Certain changes that may improve impact could include: a) adopting strategies that have been successful by increasing the length of time and intensity, targeting specific audiences and cultural contexts, or restructuring the delivery (e.g. positive vs. negative messaging); or b) by expanding to a more comprehensive strategy, incorporating proven behavioral change theory, innovative information technology, as well as targeting policy and environmental factors, beyond solely providing public education and communication [51, 53, 54].
Low impact/low feasibility: Re-Design
Public health interventions which fall in the low impact/low feasibility category should be RE-DESIGNED
While these interventions have the potential to have widespread impact, in practice they have generally had only modest impact on individual risk factor profiles and therefore are characterized by less overall impact. The effectiveness of the intervention itself may be questionable, or its cost high. Unlike the “act” and “buy in” options, these interventions are generally downstream and favor individual behavioral change, leaving individuals with unhealthy alternatives that may appear more desirable in the short-term. This limits acceptability and expansion potential. Two representative examples for this category are: altering food environments, and cookstove interventions to reduce household air pollution.
Altering food environments
Redesigning grocery store aisles or lunch-rooms has been proposed as an intervention that leverages changing consumers’ choice architecture when they shop for food. It combines built environment strategies with socio-behavioral approaches to change and includes receding unhealthy foods to the background with healthier foods made more prominent. These interventions aim to consciously or sub-consciously increase preference for healthier options [55]. While theoretically attractive, there is limited evidence of low quality that redesigning food acquisition environments has substantial impact on food choices [55, 56]. The feasibility of grocery store re-design is limited by the fact that ‘junk’ food in general tends to be a leading source of income for grocery stores, therefore making a strategy likely to reduce revenue and profits less acceptable to store owners [57]. Second, in some settings, healthier food options tend to be less affordable than junk food (e.g. a bag of chips costing less than a fruit salad) [57]. Finally, the effect of redesigning food acquisition environments on actual food consumption and on overall health outcomes remains unknown.
Cookstove interventions
Improved cookstove initiatives (ICIs) target reducing household air pollution (HAP) for individuals who utilize solid fuel sources such as firewood and charcoal for cooking in households or restaurant settings. Solid fuel is commonly used in LMICs [58], results in high levels of indoor air pollutants [59], and can lead to chronic respiratory diseases, CVD, and lung cancer [1]. ICIs aim to increase efficiency of energy use and reduce exposure to household air pollution [60]. The feasibility of ICIs is limited by partial adoption and intermittent use, reflecting persistence of cooking over open stoves [61]. In addition, the impact of ICIs on health outcomes is unclear. ICIs reduce HAP levels by 50–90%, although there is a lot of variability based on the type of stove used, with chimney stoves performing best [61, 62]. Despite this, the average post-intervention levels of HAP remain higher than those recommended by WHO, posing residual health risks to individuals [63, 64]. Recent systematic reviews reported inconclusive findings of ICIs on health outcomes [65]. Potential strategies to reduce household air pollution sufficient to exert health benefit include enabling complete adoption of ICIs [66], as well as encouraging the shift to cleaner fuel sources in addition to improved cookstoves [67].
Discussion/way forward
The rationale to pursue an approach of proactive prevention is to expand the target for preventive interventions to include currently low-burden populations, in order to prevent future premature death and disability from NCDs and most efficiently use limited budget and healthcare resources. We have introduced a simple framework to evaluate potential proactive prevention interventions, assessing both impact and feasibility. As a result, it is possible to prioritize actions that are high-impact and high-feasibility, while working to address and change other interventions that are either less impactful or less feasible.
While there are already examples of proactive prevention that have been implemented, much more needs to be done to protect and support low-burden populations that are at potential future increased risk. We encourage policymakers, program planners, community leaders, and individuals to actively promote a proactive prevention agenda in their respective spheres of influence. Coupling policy interventions can maximize population health impact. Municipalities can be effective implementers of global and national goals and priorities, particularly if they subscribe to a “Health in All Policies” approach to decision making [68]. It will be important to maximize impact and feasibility of potential interventions and strategies. This will require transdisciplinary and multi-sectoral collaboration, as well as community engagement, to improve, re-design, change, and increase buy-in, in order to be able to act. We recognize that the pathway forward might not be straightforward, easy, or linear. However, it is important to act now, before it is too late.
Data Availability
All relevant data are available from the Institute for Health Metrics and Evaluation (www.healthdata.org/data-visualization/gbd-compare).
Funding Statement
The authors have no funding to disclose.
References
- 1.Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018;392(10159):1923–94. Epub 2018/11/30. 10.1016/S0140-6736(18)32225-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Beaglehole R, Bonita R, Horton R, Adams C, Alleyne G, Asaria P, et al. Priority actions for the non-communicable disease crisis. Lancet (London, England). 2011;377(9775):1438–47. Epub 2011/04/09. 10.1016/S0140-6736(11)60393-0 . [DOI] [PubMed] [Google Scholar]
- 3.Benzinger CP RG, Moran AE. The global burden of disease study and the preventable burden of NCD. Global Heart. 2016;11(4):393–7. 10.1016/j.gheart.2016.10.024 [DOI] [PubMed] [Google Scholar]
- 4.Watkins D, Hale J, Hutchinson B, Kataria I, Kontis V, Nugent R. Investing in non-communicable disease risk factor control among adolescents worldwide: a modelling study. 2019;4(2):e001335 10.1136/bmjgh-2018-001335%JBMJGlobalHealth [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mikkelsen B, Williams J, Rakovac I, Wickramasinghe K, Hennis A, Shin H-R, et al. Life course approach to prevention and control of non-communicable diseases. BMJ. 2019;364:l257 10.1136/bmj.l257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Institute for Health Metrics and Evaluation (IHME). GBD Compare. Available from: http://www.healthdata.org/data-visualization/gbd-compare. [Accessed 6 October 2020]
- 7.Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–7. 10.2105/ajph.89.9.1322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rogers P. Overview of Impact Evaluation. Methodological Briefs: Impact Evaluation 1 [Internet]. 2014. [Google Scholar]
- 9.Bowen DJ, Kreuter M, Spring B, Cofta-Woerpel L, Linnan L, Weiner D, et al. How we design feasibility studies. American journal of preventive medicine. 2009;36(5):452–7. Epub 2009/04/14. 10.1016/j.amepre.2009.02.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McIntyre L, Kirkpatrick S, McLaren L. Rose's population strategy of prevention need not increase social inequalities in health. International Journal of Epidemiology. 2009;39(2):372–7. 10.1093/ije/dyp315 [DOI] [PubMed] [Google Scholar]
- 11.Gaziano TA. Economic burden and the cost-effectiveness of treatment of cardiovascular diseases in Africa. Heart. 2008;94(2):140–4. 10.1136/hrt.2007.128785 . [DOI] [PubMed] [Google Scholar]
- 12.Levy DT, Tam J, Kuo C, Fong GT, Chaloupka F. The Impact of Implementing Tobacco Control Policies: The 2017 Tobacco Control Policy Scorecard. Journal of public health management and practice: JPHMP. 2018;24(5):448–57. Epub 2018/01/19. 10.1097/PHH.0000000000000780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Preventing Chronic Diseases: A Vital Investment: WHO Global Report. Organization WH, editor. Geneva: World Health Organization; 2005. [Google Scholar]
- 14.Guindon GE, Paraje GR, Chaloupka FJ. The impact of prices and taxes on the use of tobacco products in Latin America and the Caribbean. Am J Public Health. 2015;105(3):e9–19. Epub 2015/01/21. 10.2105/AJPH.2014.302396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shang C, Lee HM, Chaloupka FJ, Fong GT, Thompson M, O'Connor RJ. Association between tax structure and cigarette consumption: findings from the International Tobacco Control Policy Evaluation (ITC) Project. Tobacco control. 2019;28(Suppl 1):s31–s6. Epub 2018/05/26. 10.1136/tobaccocontrol-2017-054160 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fuster V, Vedanthan R. Cardiovascular disease and the UN Millennium Development Goals: time to move forward. Nat Clin Pract Cardiovasc Med. 2008;5(10):593 10.1038/ncpcardio1353 . [DOI] [PubMed] [Google Scholar]
- 17.Hyseni L, Bromley H, Kypridemos C, O'Flaherty M, Lloyd-Williams F, Guzman-Castillo M, et al. Systematic review of dietary trans-fat reduction interventions. Bulletin of the World Health Organization. 2017;95(12):821–30g. Epub 2017/12/05. 10.2471/BLT.16.189795 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Downs SM, Bloem MZ, Catterall E, Wu JH, Zheng M, Thomas B, et al. The Impact of Policies to Reduce trans Fat Consumption: A Systematic Review of the Evidence. Current Developments in Nutrition. 2017;1(12). 10.3945/cdn.117.000778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kontis V, Cobb LK, Mathers CD, Frieden TR, Ezzati M, Danaei G. Three Public Health Interventions Could Save 94 Million Lives in 25 Years. Circulation. 2019;140(9):715–25. Epub 2019/06/11. 10.1161/CIRCULATIONAHA.118.038160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ghebreyesus TA, Frieden TR. REPLACE: a roadmap to make the world trans fat free by 2023. Lancet (London, England). 2018;391(10134):1978–80. Epub 2018/05/19. 10.1016/S0140-6736(18)31083-3 . [DOI] [PubMed] [Google Scholar]
- 21.Arango CM, Paez DC, Reis RS, Brownson RC, Parra DC. Association between the perceived environment and physical activity among adults in Latin America: a systematic review. Int J Behav Nutr Phys Act. 2013;10:122 Epub 2013/11/01. 10.1186/1479-5868-10-122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Malambo P, Kengne AP, De Villiers A, Lambert EV, Puoane T. Built Environment, Selected Risk Factors and Major Cardiovascular Disease Outcomes: A Systematic Review. PLoS One. 2016;11(11):e0166846 Epub 2016/11/24. 10.1371/journal.pone.0166846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Orstad SL, McDonough MH, Stapleton S, Altincekic C, Troped PJ. A systematic review of agreement between perceived and objective neighborhood environment measures and associations with physical activity outcomes. Environ Behav. 2016;(49):904–32. [Google Scholar]
- 24.Vancampfort D, Stubbs B, Sallis JF, Nabanoba J, Basangwa D, Oyeyemi AL, et al. Associations of the Built Environment With Physical Activity and Sedentary Time in Ugandan Outpatients With Mental Health Problems. J Phys Act Health. 2019;16(4):243–50. Epub 2019/03/14. 10.1123/jpah.2018-0355 [DOI] [PubMed] [Google Scholar]
- 25.Wilson LA, Giles-Corti B, Burton NW, Giskes K, Haynes M, Turrell G. The association between objectively measured neighborhood features and walking in middle-aged adults. Am J Health Promot. 2011;25(4):e12–21. Epub 2011/04/12. . [PubMed] [Google Scholar]
- 26.Ding D, Sallis JF, Kerr J, Lee S, Rosenberg DE. Neighborhood environment and physical activity among youth a review. American journal of preventive medicine. 2011;41(4):442–55. Epub 2011/10/04. 10.1016/j.amepre.2011.06.036 . [DOI] [PubMed] [Google Scholar]
- 27.Barnett DW, Barnett A, Nathan A, Van Cauwenberg J, Cerin E, Council on E, et al. Built environmental correlates of older adults' total physical activity and walking: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2017;14(1):103 Epub 2017/08/09. 10.1186/s12966-017-0558-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Davison KK, Lawson CT. Do attributes in the physical environment influence children's physical activity? A review of the literature. Int J Behav Nutr Phys Act. 2006;3:19 Epub 2006/07/29. 10.1186/1479-5868-3-19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Macdonald L, McCrorie P, Nicholls N, Olsen JR. Active commute to school: does distance from school or walkability of the home neighbourhood matter? A national cross-sectional study of children aged 10–11 years, Scotland, UK. BMJ open. 2019;9(12):e033628 Epub 2019/12/26. 10.1136/bmjopen-2019-033628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Buck C, Tkaczick T, Pitsiladis Y, De Bourdehaudhuij I, Reisch L, Ahrens W, et al. Objective measures of the built environment and physical activity in children: from walkability to moveability. Journal of urban health: bulletin of the New York Academy of Medicine. 2015;92(1):24–38. Epub 2014/11/09. 10.1007/s11524-014-9915-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Colabianchi N, Clennin MN, Dowda M, McIver KL, Dishman RK, Porter DE, et al. Moderating effect of the neighbourhood physical activity environment on the relation between psychosocial factors and physical activity in children: a longitudinal study. Journal of epidemiology and community health. 2019;73(7):598–604. Epub 2019/04/11. 10.1136/jech-2018-211456 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Schule SA, Fromme H, Bolte G. Built and socioeconomic neighbourhood environments and overweight in preschool aged children. A multilevel study to disentangle individual and contextual relationships. Environmental research. 2016;150:328–36. Epub 2016/06/25. 10.1016/j.envres.2016.06.024 . [DOI] [PubMed] [Google Scholar]
- 33.Sanders T, Feng X, Fahey PP, Lonsdale C, Astell-Burt T. The influence of neighbourhood green space on children's physical activity and screen time: findings from the longitudinal study of Australian children. Int J Behav Nutr Phys Act. 2015;12:126 Epub 2015/10/01. 10.1186/s12966-015-0288-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ford ES, Zhao G, Li C. Pre-diabetes and the risk for cardiovascular disease: a systematic review of the evidence. Journal of the American College of Cardiology. 2010;55(13):1310–7. Epub 2010/03/27. 10.1016/j.jacc.2009.10.060 . [DOI] [PubMed] [Google Scholar]
- 35.James WP, Nelson M, Ralph A, Leather S. Socioeconomic determinants of health. The contribution of nutrition to inequalities in health. BMJ. 1997;314(7093):1545–9. Epub 1997/05/24. 10.1136/bmj.314.7093.1545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Siegel KR, Ali MK, Srinivasiah A, Nugent RA, Narayan KM. Do we produce enough fruits and vegetables to meet global health need? PLoS One. 2014;9(8):e104059 Epub 2014/08/08. 10.1371/journal.pone.0104059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.An R. Effectiveness of subsidies in promoting healthy food purchases and consumption: a review of field experiments. Public Health Nutr. 2013;16(7):1215–28. Epub 2012/11/06. 10.1017/S1368980012004715 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.World Health Organization. Using price policies to promote healthier diets. 2015. [Google Scholar]
- 39.Methner S, Maschkowski G, Hartmann M. The European School Fruit Scheme: impact on children's fruit and vegetable consumption in North Rhine-Westphalia, Germany. Public Health Nutr. 2017;20(3):542–8. Epub 2016/10/04. 10.1017/S1368980016002652 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Durward CM, Savoie-Roskos M, Atoloye A, Isabella P, Jewkes MD, Ralls B, et al. Double Up Food Bucks Participation is Associated with Increased Fruit and Vegetable Consumption and Food Security Among Low-Income Adults. J Nutr Educ Behav. 2019;51(3):342–7. Epub 2018/10/21. 10.1016/j.jneb.2018.08.011 . [DOI] [PubMed] [Google Scholar]
- 41.Steele-Adjognon M, Weatherspoon D. Double Up Food Bucks program effects on SNAP recipients' fruit and vegetable purchases. BMC Public Health. 2017;17(1):946 Epub 2017/12/14. 10.1186/s12889-017-4942-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.HLPE. Nutrition and food systems: a report by the high level panel of experts on food security and nutrition on the committee on world food security. 2017. [Google Scholar]
- 43.Pingali P. Agricultural policy and nutrition outcomes–getting beyond the preoccupation with staple grains. Food Secur. (7):583–91. [Google Scholar]
- 44.Watkins DA, Yamey G, Schäferhoff M, Adeyi O, Alleyne G, Alwan A, et al. Alma-Ata at 40 years: reflections from the Lancet Commission on Investing in Health. The Lancet. 2018;392(10156):1434–60. 10.1016/S0140-6736(18)32389-4 [DOI] [PubMed] [Google Scholar]
- 45.Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. International Journal of Obesity. 2011;35(7):891–8. 10.1038/ijo.2010.222 [DOI] [PubMed] [Google Scholar]
- 46.Fernandez-Jimenez R, Al-Kazaz M, Jaslow R, Carvajal I, Fuster V. Children Present a Window of Opportunity for Promoting Health: JACC Review Topic of the Week. Journal of the American College of Cardiology. 2018;72(25):3310–9. Epub 2018/12/12. 10.1016/j.jacc.2018.10.031 . [DOI] [PubMed] [Google Scholar]
- 47.Fernandez-Jimenez R, Jaslow R, Bansilal S, Santana M, Diaz-Munoz R, Latina J, et al. Child Health Promotion in Underserved Communities: The FAMILIA Trial. Journal of the American College of Cardiology. 2019;73(16):2011–21. Epub 2019/04/27. 10.1016/j.jacc.2019.01.057 . [DOI] [PubMed] [Google Scholar]
- 48.Busch V, van Opdorp PAJ, Broek J, Harmsen IA. Bright spots, physical activity investments that work: JUMP-in: promoting physical activity and healthy nutrition at primary schools in Amsterdam. British journal of sports medicine. 2018;52(20):1299–301. Epub 2017/10/07. 10.1136/bjsports-2017-097713 . [DOI] [PubMed] [Google Scholar]
- 49.Takens FE, Busch V, Ujčič-Voortman JK, van Eijsden M, Chinapaw MJM. The Unique Extended Selection Cohorts Design for the Evaluation of the School-Based Jump-In Intervention on Dietary Habits: A Study Protocol. International journal of environmental research and public health. 2020;17(4). Epub 2020/02/15. 10.3390/ijerph17041145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Noar SM. A 10-year retrospective of research in health mass media campaigns: where do we go from here? J Health Commun. 2006;11(1):21–42. Epub 2006/03/21. 10.1080/10810730500461059 . [DOI] [PubMed] [Google Scholar]
- 51.Gill T, Boylan S. Public Health Messages: Why Are They Ineffective and What Can Be Done? Current Obesity Reports. 2012;1(1):50–8. [Google Scholar]
- 52.Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet (London, England). 2010;376(9748):1261–71. Epub 2010/10/12. 10.1016/S0140-6736(10)60809-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Stead M, Angus K, Langley T, Katikireddi SV, Hinds K, Hilton S, et al. Mass media to communicate public health messages in six health topic areas: a systematic review and other reviews of the evidence. Public Health Research. Southampton (UK) 2019. [PubMed] [Google Scholar]
- 54.Tabassum R, Froeschl G, Cruz JP, Colet PC, Dey S, Islam SMS. Untapped aspects of mass media campaigns for changing health behaviour towards non-communicable diseases in Bangladesh. Global Health. 2018;14(1):7 Epub 2018/01/20. 10.1186/s12992-018-0325-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Broers VJV, De Breucker C, Van den Broucke S, Luminet O. A systematic review and meta-analysis of the effectiveness of nudging to increase fruit and vegetable choice. European journal of public health. 2017;27(5):912–20. Epub 2017/06/29. 10.1093/eurpub/ckx085 . [DOI] [PubMed] [Google Scholar]
- 56.Hartmann-Boyce J, Bianchi F, Piernas C, Payne Riches S, Frie K, Nourse R, et al. Grocery store interventions to change food purchasing behaviors: a systematic review of randomized controlled trials. The American journal of clinical nutrition. 2018;107(6):1004–16. Epub 2018/06/06. 10.1093/ajcn/nqy045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lent MR, Vander Veur SS, McCoy TA, Wojtanowski AC, Sandoval B, Sherman S, et al. A randomized controlled study of a healthy corner store initiative on the purchases of urban, low-income youth. Obesity. 2014;22(12):2494–500. 10.1002/oby.20878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Chafe ZA, Brauer M, Klimont Z, Van Dingenen R, Mehta S, Rao S, et al. Household cooking with solid fuels contributes to ambient PM2.5 air pollution and the burden of disease. Environmental health perspectives. 2014;122(12):1314–20. Epub 2014/09/06. 10.1289/ehp.1206340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Naeher LP, Brauer M, Lipsett M, Zelikoff JT, Simpson CD, Koenig JQ, et al. Woodsmoke Health Effects: A Review. Inhalation Toxicology. 2007;19(1):67–106. 10.1080/08958370600985875 [DOI] [PubMed] [Google Scholar]
- 60.Hooper LG, Dieye Y, Ndiaye A, Diallo A, Sack CS, Fan VS, et al. Traditional cooking practices and preferences for stove features among women in rural Senegal: Informing improved cookstove design and interventions. PloS one. 2018;13(11):e0206822–e. 10.1371/journal.pone.0206822 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Puzzolo E, Pope D, Stanistreet D, Rehfuess EA, Bruce NG. Clean fuels for resource-poor settings: A systematic review of barriers and enablers to adoption and sustained use. Environmental research. 2016;146:218–34. Epub 01/13. 10.1016/j.envres.2016.01.002 . [DOI] [PubMed] [Google Scholar]
- 62.Pope D, Bruce N, Dherani M, Jagoe K, Rehfuess E. Real-life effectiveness of 'improved' stoves and clean fuels in reducing PM(2.5) and CO: Systematic review and meta-analysis. Environ Int. 2017;101:7–18. Epub 01/28. 10.1016/j.envint.2017.01.012 . [DOI] [PubMed] [Google Scholar]
- 63.Jetter J, Zhao Y, Smith KR, Khan B, Yelverton T, DeCarlo P, et al. Pollutant Emissions and Energy Efficiency under Controlled Conditions for Household Biomass Cookstoves and Implications for Metrics Useful in Setting International Test Standards. Environmental Science & Technology. 2012;46(19):10827–34. 10.1021/es301693f [DOI] [PubMed] [Google Scholar]
- 64.Sambandam S, Balakrishnan K, Ghosh S, Sadasivam A, Madhav S, Ramasamy R, et al. Can Currently Available Advanced Combustion Biomass Cook-Stoves Provide Health Relevant Exposure Reductions? Results from Initial Assessment of Select Commercial Models in India. EcoHealth. 2015;12(1):25–41. 10.1007/s10393-014-0976-1 [DOI] [PubMed] [Google Scholar]
- 65.Quansah R, Semple S, Ochieng CA, Juvekar S, Armah FA, Luginaah I, et al. Effectiveness of interventions to reduce household air pollution and/or improve health in homes using solid fuel in low-and-middle income countries: A systematic review and meta-analysis. Environ Int. 2017;103:73–90. Epub 03/22. 10.1016/j.envint.2017.03.010 . [DOI] [PubMed] [Google Scholar]
- 66.Klasen E, Miranda JJ, Khatry S, Menya D, Gilman RH, Tielsch JM, et al. Feasibility intervention trial of two types of improved cookstoves in three resource-limited settings: study protocol for a randomized controlled trial. Trials. 2013;14:327–. 10.1186/1745-6215-14-327 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Quinn A, Bruce N, Puzzolo E, Dickinson K, Sturke R, Jack DW, et al. An analysis of efforts to scale up clean household energy for cooking around the world. Energy Sustain Dev. 2018;46:1–10. Epub 2019/03/20. 10.1016/j.esd.2018.06.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Schillinger D, Handley M, Wang F, Hammer H. Effects of self-management support on structure, process, and outcomes among vulnerable patients with diabetes: a three-arm practical clinical trial. Diabetes care. 2009;32(4):559–66. 10.2337/dc08-0787 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All relevant data are available from the Institute for Health Metrics and Evaluation (www.healthdata.org/data-visualization/gbd-compare).