

Abstract
Congenital cataract is one of the main causes of blindness in newborns and children. According to the World Health Organization (WHO), there are about 14 million children suffering from congenital cataract. Our study is based on 82 children, males – 46 (56.1%) and females – 36 (43.9%), with congenital cataract operated in the same ophthalmological centre in Bucharest, Romania. Of the 82 patients, 49 (59.76%) had bilateral cataract and 33 (40.24%) unilateral cataract. Clinically, the most frequent was the total cataract, followed by lamellar, nuclear and cerulean. We employed nine surgical approaches in our patients, depending on the type of intraocular lens (IOL). Morphologically, obvious changes were rendered evident at the level of anterior and posterior capsules, as well as subcapsular.
Keywords: congenital cataract, genetic disease, metabolic diseases, phenotypic heterogeneity, lens disorder
Introduction
Congenital cataract represents a transparency disorder of the lens present at birth or soon after. It is one of the main causes of treatable blindness or visual impairment in children [1,2]. In literature, its prevalence is 1–6 cases/10 000 births in economically developed countries and 5–15/10 000 births in the developing world [3,4,5]. The World Health Organization (WHO) estimates that there are over 14 million blind children worldwide, originating in bilateral cataract, i.e., over 50% of the causes of blindness [6].
The causes generating congenital cataract are varied, i.e., intrauterine infections, irradiation of the pregnant woman, medication during pregnancy, genetic or metabolic causes. In a large number of cases, the etiology of congenital cataract remains unknown. Research shows that 30% to 50% of congenital cataracts are caused by mutations in genes encoding proteins in the structure of the lens [7,8,9]. Identifying the etiological factors involved in the development of congenital cataracts is essential in order to prevent this pathology.
Congenital cataract is a continuous challenge for ophthalmologists because of the young age it occurs in, inducing amblyopia, nystagmus and strabismus. In the context of crystallin lens opacification, the opacification of the lens bag content as well as of the anterior and posterior capsules were identified. The modifications of the anterior capsule are represented by capsular fibrosis or anterior lenticonus and the changes in the posterior capsule by fibrosis or dysgenesis of the posterior capsule that affects the capsule, Berger’s space and the anterior hyaloid, generating an opaque block. Thus, congenital cataract was proved to be associated with considerable genetic and phenotypic heterogeneity [10,11]. The morphological types of congenital cataract can be classified in: nuclear, cortical, lamellar, anterior polar, posterior polar, pulverulent, total, etc. [9].
Aim
The authors’ aim was to clinically and pathologically analyze certain causes of congenital cataract and find correlations between the anatomic and histopathological (HP) form of the congenital cataract and the changes within the capsular bag.
Patients, Materials and Methods
This is a retrospective, interventional study carried out on 103 eyes, in 82 patients operated on between 2016 and 2020 at the Clinical Hospital of Ophthalmological Emergencies, Bucharest, Romania, by the same surgeon.
The patients under study were aged between six months and 18 years, males and females, and suffered from bilateral or unilateral cataract. The informed parents’ consent was taken for surgery and further use of the removed material in the present study. The authors also got the approval of the Board of Ethics of the Clinical Hospital of Ophthalmological Emergencies, Bucharest.
Pediatric investigation was very complex, including family histories of both child and parents in order to trace back potential genetic anomalies, particularly of bilateral cataract. Unilateral congenital cataracts were classified as idiopathic on account of family histories and laboratory test results.
All patients were subject to preoperative investigation, i.e., slit lamp examination of the compliant patients and examination under sedation of very young ones. Evaluation was done before and after inducing drug mydriasis.
Objective refraction was done in all patients, both manifest and cycloplegic. Toddlers under three years of age were examined under general anesthesia by using a portable refractometer. Children over three years of age were examined on a standard auto-refractometer. Cycloplegia was induced by topical administration of a drop of 1% Cyclopentolate hydrochloride (Cyclogyl® 1%) three times, at 10 minutes’ distance. Cycloplegic refractometry was carried out after 60 minutes from the instillation of the first drop. The fundus examination in all patients in which the opacity allowed it, was done, visualizing the optic nerve papilla, retina vessels and macula. This investigation was associated with a B-mode ultrasonography (US), when the cataract made impossible the former approach, with the aim at rendering evident potential vitreous or retinal anomalies. A- and B-mode US was performed on both eyes in order to compare the axial lengths of the two eyes. The lens power of the implant was settled by biometry, and by using a variety of formulae depending on the patient’s age. Surgical approach implied performing the anterior and posterior capsulorhexis (where it was possible). Surgical steps were: incision, staining of the anterior capsule for easier identification; injection of viscoelastic substance in the anterior chamber to maintain it deep and constant, as well as the protection of the corneal endothelium. Then, the anterior capsulorhexis followed by means of a capsulorhexis forceps; it was very attentively performed, following the contour of a plastic ring of a given diameter, adapted to the intended implant, placed on the anterior capsule and the aspiration of the lens substance (irrigation–aspiration method) or phacoemulsification in hard cataracts. The posterior capsulorhexis was performed after detaching the posterior capsule from the anterior hyaloid by injecting a bubble of viscoelastic substance within the space between the posterior capsule and the hyaloid. The next step was the implantation of the foldable artificial lens in the eye, with a different positioning technique depending on the type of implant chosen and the restoration of the anterior chamber, initially with air and hydrosuture of the paracentesis, followed by air-saline solution exchange.
Intraoperatively, 16 anterior crystallin capsules (Figure 1) and only nine posterior capsules were collected.
Figure 1.

Intraoperative removal of anterior capsule
They were immediately put into 10% neutral buffered formalin (NBF) for fixation and further anatomic and HP analysis. Not all capsules could be taken, some being deteriorated or lost in the course of surgery; others, very small in size, particularly posterior ones, could not be histopathologically analyzed. After 24 hours fixation in 10% NBF, the biological samples were included in paraffin, in accordance with the HP protocol and processed for microscopy. Sections of 4 μm were performed and stained in Hematoxylin–Eosin (HE), in green light trichrome, following Goldner–Szekely (GS) and Periodic Acid–Schiff (PAS) and Periodic Acid–Schiff–Hematoxylin (PAS–H).
Results
The study was carried out on 82 patients, 46 (56.1%) males and 36 (43.9%) females. We could not elicit a statistically significant difference between the two genders (test ratio, p=0.12). Of the 82 patients, 49 (59.76%) presented bilateral cataract and 33 (40.24%) a unilateral form. We found a significant difference between the two types of cataract (test ratio, p=0.01).
Slit lamp examination was performed only on 103 eyes (a number of patients preferred to postpone surgery) and the following morphological cataract types were identified: total cataract – 29 (28.16%) cases; lamellar cataract – 17 (16.5%) cases; nuclear cataract – 12 (11.65%) cases; cerulean cataract – 11 (10.68%) cases; anterior polar cataract – 10 (9.71%) cases; posterior polar cataract – nine (8.74%) cases; sutural and pulverulent cataract – five (4.85%) cases; other lens transparency disorders – 10 (9.71%) cases (Figures 2,3,4,5,6,7,8).
Figure 2.

Distribution of congenital cataract in the study group
Figure 3.

Total cataract, opacifications are found in all crystallin layers
Figure 4.

Lamellar cataract
Figure 5.

Nuclear cataract
Figure 6.

Anterior polar cataract and anterior lenticonus
Figure 7.

Posterior polar cataract
Figure 8.

Subluxation of the lens, associated with transparency disorders. Superior nasal zonular fibers are seen
Nine surgical approaches were used, depending on the type of intraocular lens (IOL) (Table 1). In single piece IOLs specially designed for the bag (44), only hydrophobic models were implanted. They were implanted in the bag after performing a posterior capsulorhexis (27 cases), or without performing a posterior capsulorhexis (six cases). In 11 cases, because of associated ocular complications (lens subluxation), the lens bag was anchored by suturing a capsular tension ring (Cionni) to the sclera. Because of the surgical difficulties and laxity of the zonula, posterior capsulorhexis could not be done.
Table 1.
Types of implant in our cases
|
Surgical approach |
In-the-bag IOL (33)* |
Sulcus-fixated IOL (24) |
BIL (27)# |
|
Posterior capsulorhexis |
27 (81.81%) |
22 (91.66%) |
27 (100%) |
|
No posterior capsulorhexis |
6 (18.18%) |
2 (8.33%) |
0 |
IOL: Intraocular lens; BIL: Bag-in-the-lens; *The approaches associating subluxation of the lens and zonular laxity were not considered; #Compulsory posterior capsulorhexis is assumed
In 24 cases, we used three piece IOLs specially designed for the sulcus: 17 IOLs were implanted in the sulcus, with the capture of the anterior and posterior capsule in front of the optic (this technique requires the formation of a posterior capsulorhexis), three were placed in the sulcus (posterior capsulorhexis was performed), without an optic capture, two were implanted in the sulcus, without forming a posterior capsulorhexis, and two were inserted in the bag, with the capture of the optic behind the posterior rhexis.
Bag-in-the-lens (BIL) IOLs are hydrophilic IOLs that require the capture of both posterior and anterior capsules within the groove that surrounds the optical part of the lens and are placed between the two perpendicular haptic pairs (anterior and posterior). They were inserted in 27 cases, all requiring the formation of a posterior capsulorhexis of equal size as the anterior one.
However, eight patients remained with aphakia and the lens will be implanted at a later stage, while the need to perform posterior capsulorhexis will be assessed at that time.
In the course of surgery, changes of anterior and posterior capsules were identified, a fact that required the performing of an anterior, and particularly of the posterior capsulorhexis. Thus, all patients with anterior polar cataract (10 cases) presented capsular fibrosis (six patients) or anterior lenticonus (four patients). Microphthalmia was identified in one case.
In the case of posterior polar cataract (nine cases), all patients had capsular modifications that required special care in the aspiration of the lens substance. In all instances, because of the changes in the posterior capsule, the optic axis was not completely transparent after the removal of the nucleus and required the formation of a posterior capsulorhexis.
The anomalies associated to posterior polar cataract found during the surgery were: posterior lenticonus (two cases), persistence of Cloquet’s canal (two cases), capsular fragility (three cases) and fibrosis (two cases).
Total cataract (29 cases), characterized by the complete opacification of the lens, required the staining of the anterior capsule in order to form the capsulorhexis. In three cases, the persistence of fetal vascularization was found, fibrosis (in anterior capsule) in eight cases, and posterior plaques in five cases.
As for nuclear cataracts (12 cases), no changes of the anterior capsule were identified intraoperative, but in three cases posterior plaques were seen. Lamellar cataract (17 cases) was associated with the dysgenesis of the posterior capsule and of Berger’s space, including anterior hyaloid in four cases.
In cerulean and sutural cataract, no changes were identified during the surgery; they were only visualized at the HP examination. The cases of ectopia lentis (11 cases) presented a reduced degree of opacification of the lens, with no impact on visual acuity, but displaying an important subluxation of the lens and a marked zonular laxity.
Best-corrected visual acuity (BCVA) was recorded before and immediately after surgery (Table 2). Evaluation of BCVA was performed by means of distance Snellen chart, and by using the cycloplegic refraction results of auto-refractometry. Only 57 eyes were included in our study because of the difficulty of evaluating visual acuity in toddlers (age under 4) and in the patients with severe mental retardation. After surgery, an important improvement of vision was seen, 21% of BCVA patients greater or equal to 0.5, as compared to 1.75% before surgery and BCVA between 0.1 and 0.5 in 43.85% as compared to 40.35% before surgery. In 11 (19.29%) cases, no improvement was seen because of deep amblyopia whose treatment should be extremely energetic and long, with uncertain results.
Table 2.
BCVA values in our study group
|
BCVA |
Preoperative |
Postoperative |
|
≤0.1 |
33 (57.89%) |
11 (19.29%) |
|
0.1–0.5 |
23 (40.35%) |
25 (43.85%) |
|
≥0.5 |
1 (1.75%) |
21 (36.84%) |
BCVA: Best-corrected visual acuity
Histopathology
Our HP study elicited both normal and abnormal areas at the level of the anterior capsule. As shown in Figures 9 and 10, the normal anterior capsule is a membrane of uniform thickness and structure, intensely stained in PAS-H, meaning high concentrations of glycosaminoglycans and proteoglycans. The posterior face is lined with a continual epithelium made up of cubic cells with round, equidistant nuclei and relatively homogenous cytoplasm. Epithelial cells are anchored to the structure of the dorsal face of the anterior capsule through their base pole (Figures 9 and 10).
Figure 9.

Microscopic image of a normal area in the anterior capsule of the lens: thickness and evenness can be seen, and also the epithelial cells lining the posterior face. GS trichrome staining, ×400. GS: Goldner–Szekely
Figure 10.

Anterior capsule: intensive reaction to PAS. PAS–H staining, ×400. PAS–H: Periodic Acid–Schiff–Hematoxylin
In certain patients, suffering from cataract, the anterior capsule had an increased thickness, even (Figure 11) or uneven (Figures 12 and 13). The structure of the capsule appeared uneven and the epithelium was stratified and polyhedral.
Figure 11.

Anterior capsule zone and the significant thickening of the wall and the presence of stratified epithelium made up of polyhedral cells. PAS–H staining, ×400. PAS–H: Periodic Acid–Schiff–Hematoxylin
Figure 12.

Image of the anterior capsule, unevenly thickened, undulated, non-homogeneous structure, lined with bistratified polyhedral epithelium. PAS–H staining, ×400. PAS–H: Periodic Acid–Schiff–Hematoxylin
Figure 13.

Image of the anterior capsule, uneven thickened wall, lined with polyhedral multilayered epithelium. HE staining, ×400. HE: Hematoxylin–Eosin
The posterior capsule was undulated (Figure 14), deformed, with zig-zagging parts and non-homogeneous structure (Figure 15). The structure of the posterior capsule looked non-homogeneous sending a small content of proteoglycans of uneven distribution (Figure 16).
Figure 14.

Posterior capsule, undulated aspect. HE staining, ×200. HE: Hematoxylin–Eosin
Figure 15.

Posterior capsule, zig-zagging aspect. PAS–H staining, ×400. PAS–H: Periodic Acid–Schiff–Hematoxylin
Figure 16.

Posterior capsule, non-homogeneous thickness and structure. PAS–H staining, ×400. PAS–H: Periodic Acid–Schiff–Hematoxylin
On all HP samples, we identified an increased number of subcapsular oval nuclei, with irregular placement and orientation in the zone of the adult nucleus, and small necrotic zones, an aspect completely different from that of crystallin fibers (Figures 17 and 18). Moreover, the placement and aspect of nuclei signals disorder in the development and maturation of fibers in the crystallin structure. PAS–H staining has elicited a completely non-homogeneous disposal of glycosaminoglycans and proteoglycans in the lens structure (Figure 18).
Figure 17.
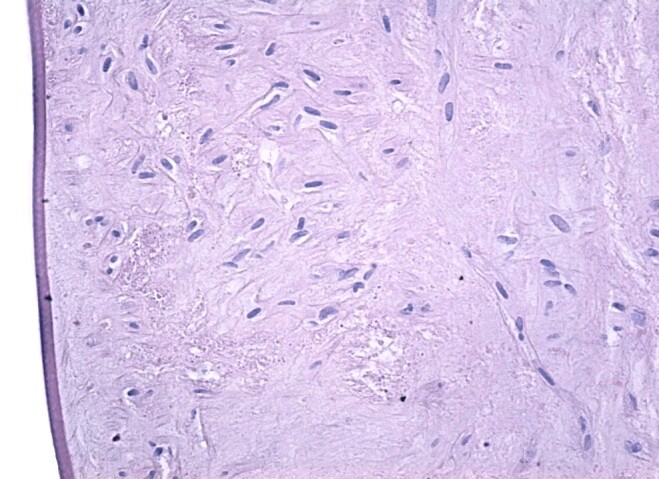
Epithelial cells from the adult lens nucleus, uneven displacement. HE staining, ×200. HE: Hematoxylin–Eosin
Figure 18.

Proteoglycans of non-homogeneous, disorderly distribution within the structure of the congenitally cataracted eye. PAS–H staining, ×400. PAS–H: Periodic Acid–Schiff–Hematoxylin
Discussion
Congenital cataract is a major cause of visual impairment in children [1]. It may occur as a single condition or in association with other ocular, somatic or neuropsychiatric disorders [6, 12]. Congenital cataract identified at birth or in the first decade rises many unknown issues, henceforth their multiple clinical aspects [13].
Congenital cataract is hereditary, up to 25% of the cases, of which 75% are autosomal dominant [14,15]. Today, 115 genes associated to syndromic and non-syndromic cataract were found, while 38 genes were identified as causes of a cataract-associated disease [6].
Genetic mutation affects various components in the lens structure. According to Shiels & Hejtmancik (2017), about 45% of the genetic mutations have an impact on crystallin proteins, about 16% of genetic mutations affect connexins, 12% act on growth and transcription factors, while 8% on metabolism, including the lipid metabolism [11]. The great clinical variety of congenital cataract is accounted for by the fact that the same genetic mutation generates radically different cataract phenotypes in different families; while differing genetic mutations can trigger similar morphological cataracts, which suggests that, apart from genetic mutations, there are additional factors, i.e., potential environmental factors that are involved in morphological variety [11].
“Crystallins” represent over 90% of the soluble proteins existing in the human lens structure. They have a great importance in maintaining the refraction index in the lens [16]. In the human lens three main classes of “crystallins” have been identified, i.e., α-crystallin – representing 40%, β-crystallin – about 35% and γ-crystallin – 25% [5, 17,18].
Mutations of genes codifying “crystallins” and “connexins” are found in congenital cataract, not associated with genetic syndromes, while mutations of α-crystallin lead to lamellar, nuclear and posterior polar cataract.
In literature, lamellar congenital cataract is thought to be the most frequently encountered form of cataract in pediatric patients [19].
Wilson et al. (2011) reported a ratio of 54% of nuclear cataract in the 83 eyes under study and an increased rate of modifications in the posterior capsule. In this study, total cataract has been identified only in 4% of the cases [20].
In a recent study, Long et al. (2017) reported a prevalence of 32.9% of total cataracts, 30.4% – nuclear cataracts, anterior polar – 8%, posterior polar – 13.5% and lamellar 9.6% [21]. Our results are similar, especially regarding the prevalence of total cataract – 28%, lamellar – 16% (the most frequent type reported in literature) and nuclear 11%. An increased prevalence of total cataracts in our study might be accounted for by opacification at birth and negligence (especially unilateral cataract that led to amblyopia) of milder forms of cataracts that progressed or suffered trauma. This fact can be demonstrated by the intraoperative discovery of posterior capsular plaques.
In the case of anterior polar cataract, in our study, all patients (10 cases) presented changes in the anterior capsule. This could be anticipated, but it can lead to intra-operative complications, such as capsulorhexis skidding, with failure to achieve a centered, curvilinear capsulorhexis, and implantation of a lens that requires a properly performed capsulorhexis.
In posterior polar cataracts, modifications were found in all patients, a fact that confirms the difficult surgery in this type of cataract. The fragility of the posterior capsule might lead to intraoperative ruptures, preventing the removal of the nucleus and aspiration of the remaining cortex. Studies have been done that compared surgical complications in posterior polar cataract removed by phacoemulsification and extracapsular cataract extraction (ECCE).
Osher et al. (1990) found no discrepancies in the ratio of posterior capsule breakage by phacoemulsification and ECCE; problems appeared while cleansing the posterior capsule after the removal of the nucleus [22].
Das et al. (2008) concluded that phacoemulsification is to be used in soft cataracts – given the low rate of complications – while ECCE is recommended in hard cataracts and plaques over 4 mm [23]. In our study, all cataract cases were soft; therefore, we never used ECCE.
Siatiri & Moghimi (2006) [24] never reported rupture of the posterior capsule, but in 18.4% they left the capsular opacity in place, and the visual axis not completely transparent and required further capsulotomy using neodymium-doped yttrium aluminum garnet (Nd:YAG) laser. We do not concur to this approach, particularly in pediatric cataract, in young patients who do not cooperate in the Nd:YAG laser session. In order to clear the visual axis and avoid its re-opacification, we recommend posterior capsulorhexis per primam, as we did in the nine cases of posterior polar cataract.
Lamellar cataracts were associated with dysgenesis of the posterior capsule, which prevented the creation of the posterior capsulorhexis and required anterior vitrectomy (four cases). Nuclear cataracts did not pose any problems; posterior plaques were associated in four cases. In cerulean and sutural cataracts, no difficulties were associated to the morphological type.
Intraoperatively, capsular fibrosis, posterior capsular plaques and presence of fetal vascularization were found in total cataracts. Capsular fibrosis is somewhat unexpected as child’s lens capsule is more elastic than in the adult [25].
In the present study, as we mentioned before, the preoperative clinical examination of patients was complex, with the aim to identify any genetic or chromosomal abnormalities transmitted from parents. The clinical examination was associated with imaging, general and ocular US and, when needed, we also used computed tomography (CT) or magnetic resonance imaging (MRI) examination in order to identify other lesions than the ocular ones. US can render evident eye anomalies, including congenital cataract, in prenatal [26] or post partum examinations, as well as essential information regarding the anatomy of the eye and other organs and systems [27].
The authors report on the most important data regarding modifications of the lens and eye morphology, which were obtained by slit lamp examination. However, certain lens modifications were identified during surgery.
The HP examinations performed showed several structural changes of the lens affected by the congenital cataract, which, in our opinion, are the expression of cellular and even molecular changes. Like other authors, we have found that, morphologically, congenital cataracts can affect any structure of the lens, which gives great clinical variability of the disease [28,29]. Thus, microscopic changes were highlighted both at the level of the capsule (anterior and posterior), but also subcapsular, variable from one area to another, the expression of genetic and molecular changes. We believe that these cellular and molecular changes underlie the change in the overall refractive index of the lens and produce more or less intense visual disturbances.
The most significant changes were at the level of the posterior capsule. According to literature, thinning and bending of the posterior capsule can promote progressive destruction of the lens fibers and further formation of cataract [30,31]. We must say that the lens is a unique, complex structure made up of special cells and proteins whose alteration, genetically or environmentally induced, leads to visual disturbances, including cataract [32,33,34,35,36].
Conclusions
The authors present an analysis and a classification of congenital cataract, i.e., an interventional study in the course of which capsules were collected and histopathologically analyzed, proving that only in the course of surgery, capsular modifications accompanying lens opacities can be evaluated. In all forms of congenital cataract analyzed, varying HP changes were seen in the anterior and posterior capsules. This finding completely justifies modern surgical approach in the treatment of congenital cataract, posterior capsulotomy per primam. A posterior capsule with anatomopathological alterations that is not surgically removed at the proper time will undergo additional opacifications because of the migration of anterior epithelial cells (Elschnig’s pearls) and/or fibrosis, which will decisively contribute to the re-opacification of the visual axis and compromise of postoperative result.
Conflict of interests
The authors declare that they have no conflict of interests.
Authors’ contribution
Cătălina-Ioana Tătaru and Adrian Costache equally contributed to the manuscript.
References
- 1.Tartarella MB, Britez-Colombi GF, Milhomem S, Lopes MCE, Fortes Filho JB. Pediatric cataracts: clinical aspects, frequency of strabismus and chronological, etiological, and morphological features. Arq Bras Oftalmol. 2014;77(3):143–147. doi: 10.5935/0004-2749.20140037. [DOI] [PubMed] [Google Scholar]
- 2.Yu Y, Wu M, Chen X, Zhu Y, Gong X, Yao K. Identification and functional analysis of two novel connexin 50 mutations associated with autosome dominant congenital cataracts. Sci Rep. 2016;6:26551–26551. doi: 10.1038/srep26551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Holmes JM, Leske DA, Burke JP, Hodge DO. Birth prevalence of visually significant infantile cataract in a defined U.S. population. Ophthalmic Epidemiol. 2003;10(2):67–74. doi: 10.1076/opep.10.2.67.13894. [DOI] [PubMed] [Google Scholar]
- 4.Song Z, Si N, Xiao W. A novel mutation in the CRYAA gene associated with congenital cataract and microphthalmia in a Chinese family. BMC Med Genet. 2018;19(1):190–190. doi: 10.1186/s12881-018-0695-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kumar M, Agarwal T, Kaur P, Kumar M, Khokhar S, Dada R. Molecular and structural analysis of genetic variations in congenital cataract. Mol Vis. 2013;19:2436–2450. [PMC free article] [PubMed] [Google Scholar]
- 6.Berry V, Georgiou M, Fujinami K, Quinlan R, Moore A, Michaelides M. Inherited cataracts: molecular genetics, clinical features, disease mechanisms and novel therapeutic approaches. Br J Ophthalmol. 2020 doi: 10.1136/bjophthalmol-2019-315282. [DOI] [PubMed] [Google Scholar]
- 7.Lampi KJ, Ma Z, Shih M, Shearer TR, Smith JB, Smith DL, David LL. Sequence analysis of betaA3, betaB3, and betaA4 crystallins completes the identification of the major proteins in young human lens. J Biol Chem. 1997;272(4):2268–2275. doi: 10.1074/jbc.272.4.2268. [DOI] [PubMed] [Google Scholar]
- 8.Mohammadpour M, Shaabani A, Sahraian A, Momenaei B, Tayebi F, Bayat R, Mirshahi R. Updates on managements of pediatric cataract. J Curr Ophthalmol. 2018;31(2):118–126. doi: 10.1016/j.joco.2018.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Liu Q, Zhu S. Clinical characteristics of congenital lamellar cataract and myopia in a Chinese family. Biosci Rep. 2020;40(2):BSR20191349–BSR20191349. doi: 10.1042/BSR20191349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Graw J. The genetic and molecular basis of congenital eye defects. Nat Rev Genet. 2003;4(11):876–888. doi: 10.1038/nrg1202. [DOI] [PubMed] [Google Scholar]
- 11.Shiels A, Hejtmancik JF. Mutations and mechanisms in congenital and age-related cataracts. Exp Eye Res. 2017;156:95–102. doi: 10.1016/j.exer.2016.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhang L, Fu S, Ou Y, Zhao T, Su Y, Liu P. A novel nonsense mutation in CRYGC is associated with autosomal dominant congenital nuclear cataracts and microcornea. Mol Vis. 2009;15:276–282. [PMC free article] [PubMed] [Google Scholar]
- 13.Van Looveren J, Van Gerwen V, Schildermans K, Laukens K, Baggerman G, Tassignon MJ. Proteomic analysis of posterior capsular plaques in congenital unilateral cataract. Acta Ophthalmol. 2018;96(8):e963–e969. doi: 10.1111/aos.13782. [DOI] [PubMed] [Google Scholar]
- 14.Haargaard B, Wohlfahrt J, Fledelius HC, Rosenberg T, Melbye M. A nationwide Danish study of 1027 cases of congenital/infantile cataracts: etiological and clinical classifications. Ophthalmology. 2004;111(12):2292–2298. doi: 10.1016/j.ophtha.2004.06.024. [DOI] [PubMed] [Google Scholar]
- 15.Yi J, Yun J, Li ZK, Xu CT, Pan BR. Epidemiology and molecular genetics of congenital cataracts. Int J Ophthalmol. 2011;4(4):422–432. doi: 10.3980/j.issn.2222-3959.2011.04.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Beby F, Morle L, Michon L, Bozon M, Edery P, Burillon C, Denis Ph. The genetics of hereditary cataract. J Fr Ophtalmol. 2003;26(4):400–408. [PubMed] [Google Scholar]
- 17.Raju I, Abraham EC. Congenital cataract causing mutants of αA-crystallin/sHSP form aggregates and aggresomes degraded through ubiquitin-proteasome pathway. PLoS One. 2011;6(11):e28085–e28085. doi: 10.1371/journal.pone.0028085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Raju I, Oonthonpan L, Abraham EC. Mutations in human αA-crystallin/sHSP affect subunit exchange interaction with αB-crystallin. PLoS One. 2012;7(2):e31421–e31421. doi: 10.1371/journal.pone.0031421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cantor LB, Rapuano CJ, Cioffi GA. 2017–2018 Basic and Clinical Science Course (BCSC) 2. San Francisco, CA, USA: American Academy of Ophthalmology; 2017. Section 11: Lens and cataract . Available at: https://www.aao.org/assets/9c6f2834-24c7-428a-a004-6f09048254a0/636312524130900000/bcsc1718-s11-pdf. [Google Scholar]
- 20.Wilson ME, Trivedi RH, Morrison DG, Lambert SR, Buckley EG, Plager DA, Lynn MJ, Infant Aphakia Treatment Study Group The Infant Aphakia Treatment Study: evaluation of cataract morphology in eyes with monocular cataracts. J AAPOS. 2011;15(5):421–426. doi: 10.1016/j.jaapos.2011.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Long E, Lin Z, Chen J, Liu Z, Cao Q, Lin H, Chen W, Liu Y. Monitoring and morphologic classification of pediatric cataract using slit-lamp-adapted photography. Transl Vis Sci Technol. 2017;6(6):2–2. doi: 10.1167/tvst.6.6.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Osher RH, Yu BC, Koch DD. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg. 1990;16(2):157–162. doi: 10.1016/s0886-3350(13)80724-9. [DOI] [PubMed] [Google Scholar]
- 23.Das S, Khanna R, Mohiuddin SM, Ramamurthy B. Surgical and visual outcomes for posterior polar cataract. Br J Ophthalmol. 2008;92(11):1476–1478. doi: 10.1136/bjo.2007.129403. [DOI] [PubMed] [Google Scholar]
- 24.Siatiri H, Moghimi S. Posterior polar cataract: minimizing risk of posterior capsule rupture. Eye (Lond) 2006;20(7):814–816. doi: 10.1038/sj.eye.6702023. [DOI] [PubMed] [Google Scholar]
- 25.Medsinge A, Nischal KK. Pediatric cataract: challenges and future directions. Clin Ophthalmol. 2015;9:77–90. doi: 10.2147/OPTH.S59009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chen PF, Tsai PY, Cheng YC, Lee CT, Chang CH. Congenital cataracts diagnosed by prenatal ultrasound. Taiwan J Obstet Gynecol. 2015;54(4):461–462. doi: 10.1016/j.tjog.2015.06.004. [DOI] [PubMed] [Google Scholar]
- 27.Costache A, Dumitru M, Anghel I, Cergan R, Anghel AG, Sarafoleanu C. Ultrasonographic anatomy of head and neck – a pictorial for the ENT specialist. Med Ultrason. 2015;17(1):104–108. doi: 10.11152/mu.2013.2066.171.aco. [DOI] [PubMed] [Google Scholar]
- 28.Reddy MA, Francis PJ, Berry V, Bhattacharya SS, Moore AT. Molecular genetic basis of inherited cataract and associated phenotypes. Surv Ophthalmol. 2004;49(3):300–315. doi: 10.1016/j.survophthal.2004.02.013. [DOI] [PubMed] [Google Scholar]
- 29.Churchill A, Graw J. Clinical and experimental advances in congenital and paediatric cataracts. Philos Trans R Soc Lond B Biol Sci. 2011;366(1568):1234–1249. doi: 10.1098/rstb.2010.0227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Amaya L, Taylor D, Russell-Eggitt I, Nischal KK, Lengyel D. The morphology and natural history of childhood cataracts. Surv Ophthalmol. 2003;48(2):125–144. doi: 10.1016/s0039-6257(02)00462-9. [DOI] [PubMed] [Google Scholar]
- 31.Ding X, Xiang L, Wang Q, Wang D, Chang P, Li Z, Zhao Y, Chu F, Ma C, Zhao YE. Clinical characteristics and surgical safety in congenital cataract eyes with three pathological types of posterior capsule abnormalities. J Ophthalmol. 2020;2020:6958051–6958051. doi: 10.1155/2020/6958051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rossi M, Morita H, Sormunen R, Airenne S, Kreivi M, Wang L, Fukai N, Olsen BR, Tryggvason K, Soininen R. Heparan sulfate chains of perlecan are indispensable in the lens capsule but not in the kidney. EMBO J. 2003;22(2):236–245. doi: 10.1093/emboj/cdg019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Barraquer RI, Michael R, Abreu R, Lamarca J, Tresserra F. Human lens capsule thickness as a function of age and location along the sagittal lens perimeter. Invest Ophthalmol Vis Sci. 2006;47(5):2053–2060. doi: 10.1167/iovs.05-1002. [DOI] [PubMed] [Google Scholar]
- 34.Song S, Landsbury A, Dahm R, Liu Y, Zhang Q, Quinlan RA. Functions of the intermediate filament cytoskeleton in the eye lens. J Clin Invest. 2009;119(7):1837–1848. doi: 10.1172/JCI38277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Danysh BP, Duncan MK. The lens capsule. Exp Eye Res. 2009;88(2):151–164. doi: 10.1016/j.exer.2008.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Augusteyn RC. On the growth and internal structure of the human lens. Exp Eye Res. 2010;90(6):643–654. doi: 10.1016/j.exer.2010.01.013. [DOI] [PMC free article] [PubMed] [Google Scholar]