

Abstract
Background Maintaining a sufficient consultation length in primary health care (PHC) is a fundamental part of providing quality care that results in patient safety and satisfaction. Many facilities have limited capacity and increasing consultation time could result in a longer waiting time for patients and longer working hours for physicians. The use of simulation can be practical for quantifying the impact of workflow scenarios and guide the decision-making.
Objective To examine the impact of increasing consultation time on patient waiting time and physician working hours.
Methods Using discrete events simulation, we modeled the existing workflow and tested five different scenarios with a longer consultation time. In each scenario, we examined the impact of consultation time on patient waiting time, physician hours, and rate of staff utilization.
Results At baseline scenarios (5-minute consultation time), the average waiting time was 9.87 minutes and gradually increased to 89.93 minutes in scenario five (10 minutes consultation time). However, the impact of increasing consultation time on patients waiting time did not impact all patients evenly where patients who arrive later tend to wait longer. Scenarios with a longer consultation time were more sensitive to the patients' order of arrival than those with a shorter consultation time.
Conclusion By using simulation, we assessed the impact of increasing the consultation time in a risk-free environment. The increase in patients waiting time was somewhat gradual, and patients who arrive later in the day are more likely to wait longer than those who arrive earlier in the day. Increasing consultation time was more sensitive to the patients' order of arrival than those with a shorter consultation time.
Keywords: primary health care, waiting time, workflow, simulation and modeling, quality
Background and Significance
The length of consultation in primary health care (PHC) is a strong predictor of patient satisfaction, quality of care, and patient willingness to revisit. 1 2 3 4 5 Consultation time indicated by the time patients spend with their physicians. 6 7 When physicians do not spend enough time with patients, this lack of time is perceived as patients not receiving the care and attention they need to obtain a proper diagnosis and treatment. The patient–physician conversation is critical in establishing trust and understanding. Shorter consultation times negatively impact this trust and decrease patient confidence in physician judgments, the accuracy of diagnosis, and treatment plan provided. These factors can result in reduced patient compliance. 1 2 4 Longer consultation time allows physicians to communicate effectively for establishing trust, listening to patients, explaining the treatment recommended and the alternative treatments available, engage the patients in the treatment plan and decision-making, and provide education or advice.
Studies documented safety and quality concerns about shorter consultation times. 1 2 Although many factors contribute to the quality of care, some suggested that countries with longer consultation times tend to be associated with a higher quality of care and better health outcomes. 8 The length of consultation time varies greatly by countries ranging from 48 seconds in Bangladesh to 22.5 minutes in Sweden. 8 9 Prior research has shown that the consultation time at a PHC in Saudi Arabia was relatively short compared with most international standards. 8 9 10 11 A recent study shows that the average consultation time in a Saudi PHC ranges from a mean of M = 2.83 minutes, standard deviation (SD = 1.64) in rural areas to M = 7.43 minutes (SD = 6.79) in metropolitan areas. 9 An older study also reported somewhat similar results with an average consultation time of 5.09 minutes. 12
Although most physicians and health care managers agree about the importance of longer consultations, it is difficult in many cases due to limited facility capacity, heavy patient load, and a shortage of health care professionals. The impact of longer consultation times is felt by both health care professionals and patients, and is associated with lower patient satisfaction, including patients leaving the PHC without receiving treatment. 5
Health care workflow is a complex process with many intertwined users and activities and changing parts of the system will impact waiting time. 13 Balancing the tradeoff between consultation time and patient waiting time is an important decision that requires careful planning. Achieving the proper balance of increasing consultation time while avoiding critical long waiting times is the formula for quality improvement. 5 The ability to balance these two factors and quantify the relationship between them can have many practical implications. For example, preventing patients from leaving without being seen and reaching the optimum level of patient satisfaction.
In emergency departments, for example, one study quantified the exact duration of time in which patients are willing to wait before leaving without being seen. 14 Although the exact duration of patients' willingness to wait at PHC may differ from emergency departments, the concept will apply to other health care setting. 5 Optimizing waiting time and consultation time will require quantifying the tradeoff between the two factors to obtain the optimum satisfaction for patients. In primary health care, the consultation time was found to be a strong predictor of patients' satisfaction, even stronger than patient waiting time. 5 When comparing satisfaction levels for patients who spent approximately 5, 10, or 15 minutes with their physicians, the reported level of satisfaction was 18, 78.7, and 92.7%, respectively. 5 Incorporating this information into the scheduling systems could improve the optimization process. Huang and Verduzco incorporated clinic constraints such as average patient wait time, average physician idle time, overtime, finish time, and lunch hours to reduce waiting time. 15
The existing status of primary health care centers shows a clear need for rebalancing these two components. Prior studies have found that the consultation length is relatively short (∼5 minutes) compared with the recommended national standard. 9 In addition, a wide range of variation was reported by different PHC centers ranging from 2.07 minutes in rural areas to 9.73 minutes in metropolitan areas. 9
To investigate the tradeoff between consultation length and waiting time, we propose the use of a simulation. Discrete event simulation (DES) modeling is especially useful for complex relationships where multiple variables can produce an enormous number of possible outcomes. 16 Workflow simulation has successfully been used to solve workflow and time problems in health care, industry, engineering, and business. 17 18 19 20 It enables the testing of different hypotheses in a risk-free environment and has been used to quantify variables and illustrate different workflow processes. The majority of earlier simulation studies which included patients waiting time were for the design or comparison of scheduling systems. 21 22 They often focus on optimizing the existing systems and improving the capacity of health care facilities. 15 21 22 23 24 Studies in the field of Health Informatics, however, used simulation modeling to examine the impact of information technologies on patients waiting time. 17 18 On the other hand, studies from the operations research and operations management fields examine the impact access and scheduling policies and government intervention on patients waiting time. 25 26 Little is known about the impact of longer consultation time on patients' waiting time. In this study, we will examine the impact of increasing consultation time on patients waiting time, physicians' utilization, and working hours.
Methods
The study was approved by the Biomedical Research Ethical Committee at Jazan University decision number REC39/4-S005. An iterative data collection and analysis process was conducted using direct observation, opportunistic interviews, and simulation development. We followed the (Borycki 2006) methodological framework for workflow mapping and simulation developments. 27 The framework covers the fundamental phases of simulation developments typically needed for simulation studies, and it was also designed to be used for simulation studies in clinical workflow. 18 27 28 29 The selection of the (Borycki 2006) framework was also because of its relevance to the field of biomedical informatics. The framework was also consistent with the criteria recommended by Fone et al for reporting simulation and modeling studies. The minimum criteria include clear aims and objectives, information on model specification, parameter data, assumptions, validation, and results. 30 The detailed description of each step is described below.
Context and Data Collection
Due to the variation found in the waiting and consultation time across different PHC centers, we focused on a single site. 9 This was especially important for validating the simulation model. The PHC center observed operates under the Saudi Ministry of Health. The services provided by the PHC were mostly general physician- and family doctor-related services. The PHC diagnose and treat both new and follow-up patients. The majority of visits related to chronic conditions, vaccinations, or other symptoms such as cough, fever, and respiratory infection. The PHC also receive patients during their initial point of contact before being referred to a specialist at hospitals.
Data were collected via both direct observation, opportunistic interview, and filled-out forms. Before data collection, research assistants were instructed and trained on workflow concepts, mapping, and other observation techniques. Three research assistants conducted the observations. Two of the three assistants were health informatics students in the last year of an undergrad bachelor degree program, and one was a teaching assistant. Before the observation, research assistants visited the PHC center for 3 days to familiarize themselves with the workflow.
A total of 36 hours of direct observation was conducted until a saturation of data was achieved. 31 The observation was conducted to collect the following information: tasks completed by patients, duration of tasks, sequence of tasks, and the probability of going through each task. Using a stopwatch, pen, and paper, research assistants recorded the duration of each task and the number of patients going from one task to the next. These measurements were later used to calculate the probability of going through a particular event. The opportunistic interview was used to investigate unusual events and to determine why some patients took longer than others on a task or decided to be directed to a different route.
We asked health care professionals at the PHC clinic to complete a simple form ( Supplementary Table S1 [available in the online version]) to estimate the duration of each task observed. Although data from direct observations are often more accurate than data estimates, the direct observation was limited as it only reflected the time in which the observation took place. Studies have shown that patient flow and waiting time may be influenced by many factors such as the day of the week, holidays, and season. 32 33 Therefore, an accurate time estimation from direct observation only is impractical. Multiple sources of information were important to account for potential fluctuations. When a difference was observed between the estimated and direct observation data, it was discussed with the health care professional for clarification.
Simulation Developments and Analysis
The simulation and mapping developments were created by using the information collected from both the observed and estimated tasks. The DES was developed using AnyLogic simulation software ( Fig. 1 ). The specific parameters included fly-in fly-out queuing technique for the waiting areas, service delay for services, and seize and release for resources. The queuing capacity was set to 50, but the maximum number reached while running the system was 29.
Fig. 1.
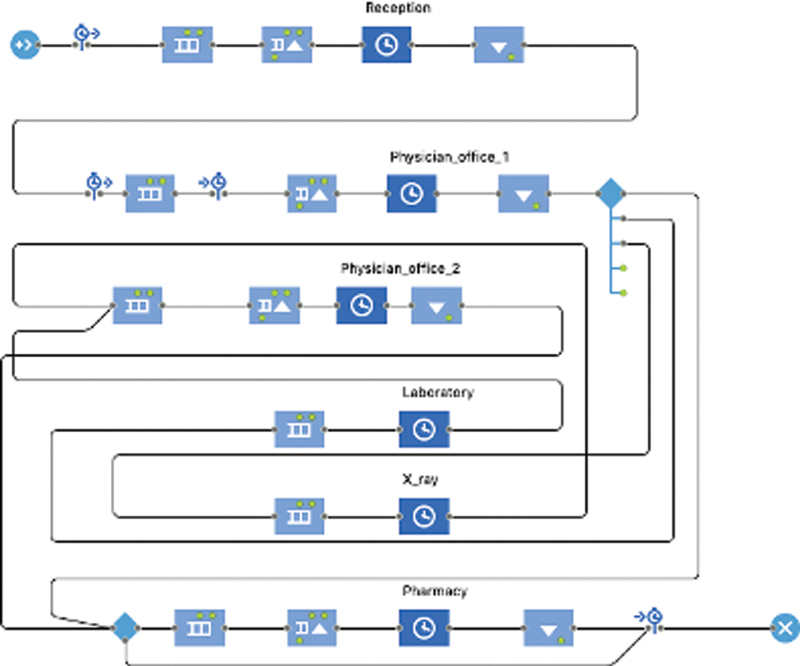
Primary health care simulation model.
Our goal was to predict the system's behavior in different scenarios. We created five different scenarios by manipulating consultation times. The model developed using the different methods was referred to as the baseline scenario ( Table 1 ). The baseline scenario model was tested and validated using face validation and event validation techniques. 34 We ran the simulation for a typical workday (8 hours) and with an estimated patient load (88 patients per day). The 8 hours was the duration of patient flow.
Table 1. Simulation input parameters.
| Duration of patient flow | 8 h |
|---|---|
| Patient flow rate | 11 patients per hour (88 patients per day) |
| Reception time (clerk) | (0.6, 1.9, 5) min |
| Consulting time (physicians) | (3.3, 5, 20) min |
| Additional time spent with patients returning from laboratory or X-ray (physicians) | (2, 4, 10) min |
| Laboratory time | (7, 15, 20) min |
| X-ray | (5, 10, 15) min |
| Pharmacy | (1, 2, 5) min |
| Probability distribution | Physicians to pharmacy 0.74 Physicians to laboratory 0.12 Physicians to X-ray 0.03 Physicians to discharge 0.11 |
| Probability distribution | Physician to pharmacy 0.87 Physician to exit 0.13 |
| Number of health care professionals | One clerk Two physicians One laboratory technician One X-ray technician One pharmacist |
After modeling the existing baseline, the simulation model was employed to test the what-if scenarios. The targeted duration for consultation time selected in this study was an average of 10 minutes. 5 We developed five different scenarios by increasing consultation time by 1 minute in each scenario ( Table 2 ). To maintain the distribution of consultation time, the 1-minute increments were added to the minimum, average, and maximum ( Table 2 ). We performed a random seed approach in which we collected the output of 100 runs for each scenario and calculated the average, standard deviation, and standard error of the mean for each scenario ( Supplementary Figs. S1 and S2 [available in the online version]).
Table 2. The length of consultation in each scenario.
| Scenario | Consultation time (minimum, average, maximum) minutes |
|---|---|
| Baseline | (3.3, 5, 20) |
| Scenario one | (4.3, 6, 21) |
| Scenario two | (5.3, 7, 22) |
| Scenario three | (6.3, 8, 23) |
| Scenario four | (7.3, 9, 24) |
| Scenario five | (8.3, 10, 25) |
Our main purpose was to estimate the impact of longer consultation time on patient waiting time. By running the simulation model for each scenario, we collected the following parameters:
Consultation time refers to the time patients and physicians spend together at the physician office. 6 7
Patient waiting time refers to the time that the patient spends in the waiting area before seeing the physician.
Total duration of visit refers to the total time the patient spends in the PHC center.
Total PHC working time refers to the total time needed for the clinic to complete all patient visits in a given day, assuming that there are 88 patients seen per day.
Level of resource utilization refers to various resources that are needed for daily operation including reception staff (clerks), physicians, and pharmacists.
The simulation output was exported and analyzed. The analysis included bar charts, line graphs, and paired sample t -test. The analysis was performed using Excel and the Statistical Package for the Social Sciences SPSS v23.
Results
In this study, we simulated the existing workflow and tested five different scenarios. Each scenario represented a 1-minute increase in consultation length. In each scenario, the duration of time each patient spent in the waiting room and the total duration of time spent at the PHC (total duration of visit) was calculated ( Fig. 2 ). At baseline, the average waiting time was 9.87 minutes and gradually increased to 89.93 minutes in scenario five. By increasing the consultation time from 5 to 10 minutes, the average waiting time increased from 9.87 to 89.93 minutes. We found that for every minute increase in the consultation length, there was a somewhat steady proportional increase in both waiting time and total visit duration.
Fig. 2.
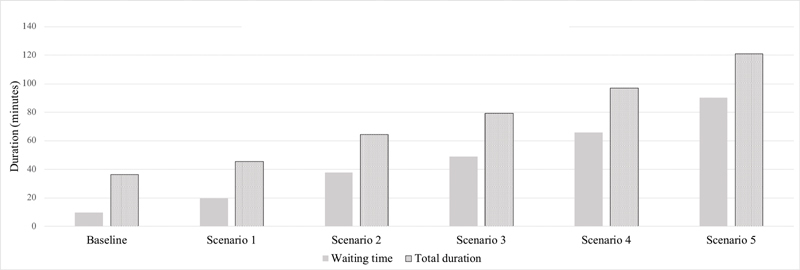
Average waiting time and duration of visits in each scenario.
To examine system behavior over the time, we plotted patient waiting time based on the order in which they arrived ( Fig. 3 ). The baseline status shows that the order of patient arrival does not seem to impact the time spent in the waiting area. By increasing the length of consultation by 1 minute (scenario one), we found a slight increase in the waiting time as more patients are added to the system. Fig. 3 also shows that patients waiting time gradually increase as more patients are added, and the system tendency is to have longer waiting times as more patients arrive increase by increasing the consultation length increases.
Fig. 3.
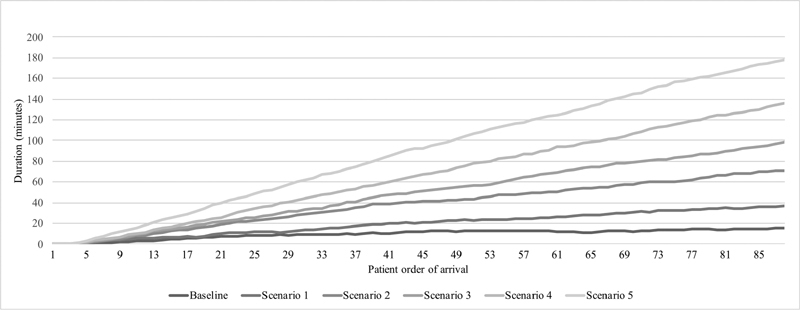
The duration of patients waiting time by patients' order or arrival.
Generally, patients who arrived first are expected to spend less time in the waiting area. As more patients arrive, the queue will increase and patients will wait longer. This represents the effect of patient accumulation in the waiting area. A smooth and sustainable system would have a steady flow in which system processing is proportionate to the rate of incoming patients. This would require maintaining a constant number of patients in the waiting area. The paired sample t -test comparison of patients waiting time showed a statistically significant difference between the baseline waiting time and all scenarios ( Table 3 ).
Table 3. The waiting time paired sample t -test comparison between the baseline (M = 9.87, standard deviation = 4.37) and each scenario .
| Scenario compared with the baseline | M (minutes) | SD | p -Value (two-tailed) | Standard error Mean | 95% CI a | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Scenario one | 19.54 | 10.96 | 0.000 | 1.16 | 17.22 | 21.87 |
| Scenario two | 37.72 | 21.19 | 0.000 | 2.25 | 33.23 | 42.21 |
| Scenario three | 49.01 | 29.60 | 0.000 | 3.15 | 42.74 | 55.28 |
| Scenario four | 65.75 | 41.38 | 0.000 | 4.41 | 56.98 | 74.51 |
| Scenario five | 89.93 | 54.49 | 0.000 | 5.80 | 78.39 | 101.48 |
95% confidence interval of the difference.
Similarly, the total duration of visits was less than 50 minutes in the baseline scenario. In scenario one, the first 50 patients spent less than 50 minutes and gradually increase to near 60 minutes by the end of the day ( Fig. 4 ) and scenarios with a longer consultation time showed a steeper slope.
Fig. 4.
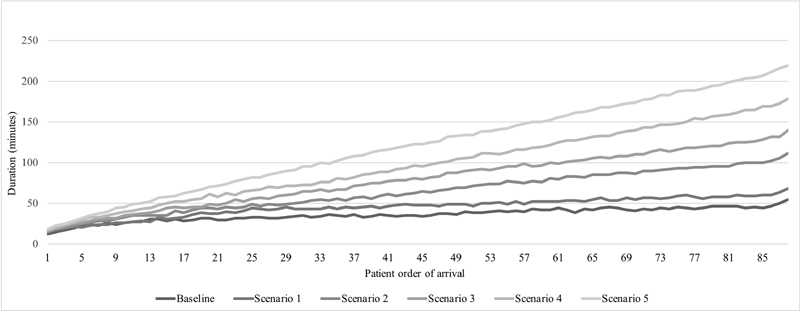
The total duration of patients visit by patients' order or arrival.
An important factor to consider when testing a scenario is to examine the rate of resource utilization. We examined resource utilization rate for those who serve the majority of patients (reception staff, physicians, pharmacists, etc.). Staff that serve less than 10% of patients such as X-ray and laboratory technicians were not included. We also presented the total duration needed by the PHC center to complete the total number of patients (88) in a day. The reception staff utilization ranged from 31.78 to 40.59% ( Table 4 ). Staff utilization rate increases as the total PHC working time decreases. This relationship is also seen in the inverse. The baseline scenario has the highest utilization rate of 40.59% and the lowest PHC working time of 542.24 minutes. On the other hand, the lowest rate of utilization, 31.78%, was observed in scenario four which has the longest PHC working time of 709.78 minutes. Physicians had a utilization rate that ranged from 82.64% in the baseline scenario to 93.38% in scenario five. Increasing the average length of consultation from 5 to 10 minutes resulted in increasing the rate of utilization by 10.74%. This was combined with an increase in total PHC working time of 167.54 minutes.
Table 4. Level of utilization and total time needed to complete cases.
| Scenario number | Baseline | One | Two | Three | Four | Five | |
|---|---|---|---|---|---|---|---|
| Level of utilization % | Reception | 40.59 | 37.37 | 36.78 | 34.32 | 32.31 | 31.78 |
| Physicians | 82.64 | 85.55 | 89.64 | 92.05 | 91.95 | 93.38 | |
| Pharmacists | 20.91 | 19.41 | 18.48 | 17.26 | 15.82 | 15.14 | |
| Total PHC working time (min) |
542.24 | 579.61 | 593.97 | 630.82 | 680.51 | 709.78 | |
Discussion
A sufficient consultation time is a fundamental part of providing quality care, ensuring patient safety, and helping to obtain patient satisfaction. This study examined the impact of increasing consultation time on patient waiting time, working hours, and the rate of staff utilization. We tested five different scenarios by incrementally adding one minute to the average length of consultation in each scenario.
Achieving a sufficient consultation length has been a major concern in primary health care. 1 2 3 4 35 36 Although no international consensus is available for the optimum consultation length in primary health care, internationally, the consultation length ranges from 48 seconds in Bangladesh to 22.5 minutes in Sweden. 8 Most studies found that a 5-minute consultation time is below the acceptable range and that a 10-minute consultation time would be more desirable. 37 38 In this study, our aim was to increase the average consultation time from 5 to 10 minutes. Studies showed that the impact of consultation time on patient satisfaction is almost three times the impact of waiting time. 5 Studies also showed that about half the patients at emergency departments (51%) are willing to wait for up to 2 hours before leaving without being seen. 14 However, these critical thresholds may vary by patient location and demographics. By understanding the relationship between consultation time and waiting time in a given context, we can utilize the approach demonstrated in our study to identify the optimum length of consultation.
Our results showed that waiting time is not evenly distributed over the patients and waiting time aggravates toward the end of the session. In the baseline scenario, the waiting time was somewhat consistent for all patients. However, increasing the average length of consultation to 10 minutes in scenario five resulted in about a 70-minute increase in the average waiting time. The average increase in waiting time does not apply to all patients evenly. The impact of consultation length on waiting time increase toward the end of the day. This seems to be a result in the increasing queue of patients in the waiting area that suggests that if a block of free time during the middle of the day was added during which no patients were added, the number of queued patients in the waiting area would decrease. This block of time can be achieved through scheduling modifications that are designed to maintain a constant flow of patients. 23 Studies have also utilized patients' characteristics and demographics information to optimize scheduling systems and reduce waiting time. 23 24
Due to the complex and interconnected nature of health care systems, the impact of longer consultation time did not only impact waiting times. There is also an impact on the total time needed by the PHC to complete all patients in a day. By controlling for patient arrival rate, increasing the length of consultation time from 5 to 10 minutes would increase the PHC's daily working time by 167.54 minutes. The system would generally be expected to react to the increased consultation time by increasing resource utilization rate, but physician utilization rate at the baseline was high at 82.64%. As a result, the system offsets the increased utilization by increasing total working hours since physicians cannot significantly increase their already high utilization rate. This process demonstrates how the system can cascade effects from one part of the system to the other.
Future studies should be cautious when interpreting the results of waiting time if the date is collected in a cross-sectional manner. The majority of workflow studies would either report the distribution or the average of multiple observations in a given timeframe. Workflow is a dynamic process, and the temporal and sequential components are fundamental parts that explain workflow and system behavior. Our results demonstrate that the average waiting time may not be an accurate representation of system behavior, and how the waiting time is experienced by patients. The order of patient arrival is a strong influence that impacts those who arrive later in the day more than those who arrive earlier. Workflow studies should also report any blocked-out time or breaks in the scheduling system. Many studies showed the benefit of redesigning scheduling techniques for achieving a steady flow of patients. 15 23 24 39 Some of them also accounted for the waiting time distribution across the different patients. 15 23 24 39 We also recommend examining the effect of workflow redesign on the waiting time.
The simulation allowed our study to capture the temporal component of the system with fine incremental changes. This can be extended by examining the past system behavior under different conditions. One way is to utilize the electronic health records (EHR) timestamps for data collection instead of traditional observation. The use of EHR timestamps can be a practical alternative to examine the temporal dimension in the clinical workflow. 40 41 42 43 44
Studies documented the effect of longer working hours on physician mental load, stress level, and burnout. 45 46 Physicians' mental load could possibly increase the time taken to process information and increase the consultation time. Quantifying the impact of these factors on consultation time and understanding the magnitude of its effect with respect to the time elapsed after working will improve the process of staffing and scheduling. With the increasing number of patients and shortage of physicians, many studies are focusing on scheduling optimization for increasing the number of patients per day. We recommend taking a holistic approach and accounting for the mental and psychological impact of physicians as well as clinic resources. Quantifying the stress level and reliance of health care workers and incorporating them into the process optimization plan is essential for avoiding burnout as well as the safety and quality of care.
Conclusion
The impact of increasing the consultation time on patient waiting time was not direct and immediate, but gradually developed after patients accumulated in the system. The relationship is not evenly distributed as those who arrive later will wait much longer than those who arrive earlier. The relationship between consultation time and patient waiting time cannot be examined in an isolated system because there are other ramifications to consider including patient order of arrival and time that the clinic has been open.
Clinical Relevance Statement
Increasing the consultation time is essential for improving the quality and safety of care as well as the level enhancing patient satisfaction. Allocating sufficient time enables physicians to safely conduct the necessary steps for ensuring the safety of care such as reviewing patient's history, communicate more effectively with their patients, documenting patient's information more accurately, discuss the treatment options, and provide patients education. However, with the shortage of physicians and increasing demand for health care services, providing a high standard of care for all patients will be difficult. Estimating the impact of longer consultation is essential for physicians and decision-makers to manage their time and plan their delivery of care.
Multiple Choice Questions
-
Which of the following factors can be impacted by increasing the duration of consultation time?
Staff utilization rate
Patients waiting time
The total facility working hours
All of the above
Correct Answer: The correct answer is option d. All the factors mentioned can be impacted by increasing the length of consultation. When the rate of physician utilization becomes high, patients waiting time start to increase. Consequently, the facility working ours will also increase.
-
Which of the following is rarely reported in the literature but important to consider when measuring and comparing patients waiting time in health care facilities?
The reason for patient visits
The minimum and maximum waiting time
The mean and mode of waiting time
The patient's order of arrival
Correct Answer: The correct answer is option d. Workflow is a dynamic process, and the waiting time was not distributed equally across all patients. When the patients' consultation is lower than the rate of patients' arrival, the number of patients in the waiting area starts to increase and those who arrive later will have a longer waiting time.
Acknowledgment
We would like to thank the PHC centers for their collaboration and facilitation during the data collection and observation. A special thanks to Mr. Ayman S. Alamoudi and the students for their help with the data collection.
Conflict of Interest None declared.
Protection of Human and Animal Subjects
No human subjects were involved in the project.
Supplementary Material
References
- 1.Stewart M A. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152(09):1423–1433. [PMC free article] [PubMed] [Google Scholar]
- 2.Kaplan S H, Greenfield S, Ware J E., JrAssessing the effects of physician-patient interactions on the outcomes of chronic disease Med Care 198927(3, Suppl):S110–S127. [DOI] [PubMed] [Google Scholar]
- 3.Bawakid K, Rashid O A, Mandoura N, Usman Shah H B, Ahmed W A, Ibrahim A. Patients' satisfaction regarding family physician's consultation in primary healthcare centers of Ministry of Health, Jeddah. J Family Med Prim Care. 2017;6(04):819–823. doi: 10.4103/jfmpc.jfmpc_170_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kleij K-S, Tangermann U, Amelung V E, Krauth C. Patients' preferences for primary health care: a systematic literature review of discrete choice experiments. BMC Health Serv Res. 2017;17(01):476. doi: 10.1186/s12913-017-2433-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Anderson R T, Camacho F T, Balkrishnan R. Willing to wait?: the influence of patient wait time on satisfaction with primary care. BMC Health Serv Res. 2007;7(01):31. doi: 10.1186/1472-6963-7-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rossiter C, Reynolds J. Automatic monitoring of the time waited in out-patient departments. Med Care. 1963:218–225. [Google Scholar]
- 7.Vissers J. Selecting a suitable appointment system in an outpatient setting. Med Care. 1979;17(12):1207–1220. doi: 10.1097/00005650-197912000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Irving G, Neves A L, Dambha-Miller H. International variations in primary care physician consultation time: a systematic review of 67 countries. BMJ Open. 2017;7(10):e017902. doi: 10.1136/bmjopen-2017-017902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jabour A M. The impact of electronic health records on the duration of patients' visits: time and motion study. JMIR Med Inform. 2020;8(02):e16502. doi: 10.2196/16502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Al-Ahmadi H, Roland M. Quality of primary health care in Saudi Arabia: a comprehensive review. Int J Qual Health Care. 2005;17(04):331–346. doi: 10.1093/intqhc/mzi046. [DOI] [PubMed] [Google Scholar]
- 11.El Mahalli A A, Akl O A, Al-Dawood S F. WHO/INRUD patient care and facility-specific drug use indicators at primary health care centres in Eastern province, Saudi Arabia. East Mediterr Health J. 2012;18(11):1086–1090. doi: 10.26719/2012.18.11.1086. [DOI] [PubMed] [Google Scholar]
- 12.AL FARIS . al-Faris E A, al-Dayel M A, Ashton C. The effect of patients' attendance rate on the consultation in a health centre in Saudi Arabia. Fam Pract. 1994;11(04):446–452. doi: 10.1093/fampra/11.4.446. [DOI] [PubMed] [Google Scholar]
- 13.Bruijns S R, Wallis L A, Burch V C. Effect of introduction of nurse triage on waiting times in a South African emergency department. Emerg Med J. 2008;25(07):395–397. doi: 10.1136/emj.2007.049411. [DOI] [PubMed] [Google Scholar]
- 14.Shaikh S B, Jerrard D A, Witting M D, Winters M E, Brodeur M N. How long are patients willing to wait in the emergency department before leaving without being seen? West J Emerg Med. 2012;13(06):463–467. doi: 10.5811/westjem.2012.3.6895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Huang Y, Verduzco S. Appointment template redesign in a women's health clinic using clinical constraints to improve service quality and efficiency. Appl Clin Inform. 2015;6(02):271–287. doi: 10.4338/ACI-2014-10-RA-0094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Borycki E M, Kushniruk A, Keay E, Nicoll J, Anderson J, Anderson M. Toward an integrated simulation approach for predicting and preventing technology-induced errors in healthcare: implications for healthcare decision-makers. Healthc Q. 2009:90–96. doi: 10.12927/hcq.2009.20974. [DOI] [PubMed] [Google Scholar]
- 17.Vahdat V, Griffin J A, Stahl J E, Yang F C. Analysis of the effects of EHR implementation on timeliness of care in a dermatology clinic: a simulation study. J Am Med Inform Assoc. 2018;25(07):827–832. doi: 10.1093/jamia/ocy024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Thorwarth M, Arisha A.Application of discrete-event simulation in health care: a reviewAccessed 2009 at:https://arrow.tudublin.ie/buschmanrep/3/
- 19.Chen B L, Li E D, Yamawuchi K, Kato K, Naganawa S, Miao W J. Impact of adjustment measures on reducing outpatient waiting time in a community hospital: application of a computer simulation. Chin Med J (Engl) 2010;123(05):574–580. [PubMed] [Google Scholar]
- 20.Aeenparast A, Tabibi S J, Shahanaghi K, Aryanejhad M B. Reducing outpatient waiting time: a simulation modeling approach. Iran Red Crescent Med J. 2013;15(09):865–869. doi: 10.5812/ircmj.7908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Welch J D, Bailey N T.Appointment systems in hospital outpatient departments Lancet 19521(6718):1105–1108. [DOI] [PubMed] [Google Scholar]
- 22.Ho C-J, Lau H-S. Minimizing total cost in scheduling outpatient appointments. Manage Sci. 1992;38(12):1750–1764. [Google Scholar]
- 23.Huang Y L. The development of patient scheduling groups for an effective appointment system. Appl Clin Inform. 2016;7(01):43–58. doi: 10.4338/ACI-2015-08-RA-0097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Huang Y, Hanauer D A. Patient no-show predictive model development using multiple data sources for an effective overbooking approach. Appl Clin Inform. 2014;5(03):836–860. doi: 10.4338/ACI-2014-04-RA-0026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pazoki M, Samarghandi H. Regulating patient care in walk-in clinics. Omega. 2020:102200. [Google Scholar]
- 26.Ahmadi-Javid A, Jalali Z, Klassen K J. Outpatient appointment systems in healthcare: A review of optimization studies. Eur J Oper Res. 2017;258(01):3–34. [Google Scholar]
- 27.Use of simulation approaches in the study of clinician workflow AMIA Annual Symposium Proceedings Borycki E M.American Medical Informatics AssociationAccessed 2006 at:https://www.researchgate.net/publication/6565340_Use_of_simulation_in_the_study_of_clinician_workflow [PMC free article] [PubMed]
- 28.Anderson J G. Evaluation in health informatics: computer simulation. Comput Biol Med. 2002;32(03):151–164. doi: 10.1016/s0010-4825(02)00012-4. [DOI] [PubMed] [Google Scholar]
- 29.Günal M M, Pidd M. Discrete event simulation for performance modelling in health care: a review of the literature. J Simul. 2010;4(01):42–51. [Google Scholar]
- 30.Fone D, Hollinghurst S, Temple M. Systematic review of the use and value of computer simulation modelling in population health and health care delivery. J Public Health Med. 2003;25(04):325–335. doi: 10.1093/pubmed/fdg075. [DOI] [PubMed] [Google Scholar]
- 31.Fusch P I, Ness L R. Are we there yet? Data saturation in qualitative research. Qual Rep. 2015;20(09):1408. [Google Scholar]
- 32.Castner J, Yin Y, Loomis D, Hewner S. Medical Mondays: ED utilization for Medicaid recipients depends on the day of the week, season, and holidays. J Emerg Nurs. 2016;42(04):317–324. doi: 10.1016/j.jen.2015.12.010. [DOI] [PubMed] [Google Scholar]
- 33.Shaw K N, Lavelle J M. VESAS: a solution to seasonal fluctuations in emergency department census. Ann Emerg Med. 1998;32(06):698–702. doi: 10.1016/s0196-0644(98)70070-8. [DOI] [PubMed] [Google Scholar]
- 34.Sargent R G.Validation and verification of simulation models. in WSC'991999 Winter Simulation Conference Proceedings. Simulation-A Bridge to the Future (Cat. No. 99CH37038). Accessed 1999 at:https://ieeexplore.ieee.org/document/823050/similar#similar
- 35.Patients' Satisfaction with Primary Health Care Centers' Services, Majmaah, Kingdom of Saudi of Saudi Arabia . Mohamed E Y, Sami W, Alotaibi A, Alfarag A, Almutairi A, Alanzi F. Patients' satisfaction with primary health care centers' services, Majmaah, Kingdom of Saudi of Saudi Arabia. Int J Health Sci (Qassim) 2015;9(02):163–170. [PMC free article] [PubMed] [Google Scholar]
- 36.Bielen F, Demoulin N. Waiting time influence on the satisfaction-loyalty relationship in services. Manag Serv Qual. 2007;17(02):174–193. [Google Scholar]
- 37.Rimmer A.GPs want longer consultations, BMA survey finds. British Medical Journal Publishing GroupAccessed April 10, 2015 at:https://www.bmj.com/content/350/bmj.h1910 [DOI] [PubMed]
- 38.Wilson A. Consultation length in general practice: a review. Br J Gen Pract. 1991;41(344):119–122. [PMC free article] [PubMed] [Google Scholar]
- 39.Mondschein S V, Weintraub G Y. Appointment policies in service operations: a critical analysis of the economic framework. Prod Oper Manag. 2003;12(02):266–286. [Google Scholar]
- 40.Jabour A M, Dixon B E, Jones J F, Haggstrom D A. Data quality at the Indiana State Cancer Registry: an evaluation of timeliness by cancer type and year. J Registry Manag. 2016;43(04):168–173. [PubMed] [Google Scholar]
- 41.Jabour A M, Dixon B E. Monitoring public health reporting: data tracking in cancer registries. Online J Public Health Inform. 2018;10(03):e220. doi: 10.5210/ojphi.v10i3.9432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Jabour A, Dixon B E, Jones J F, Haggstrom D A. Examining Cancer Case Reporting Processes and Timeliness: Preliminary Results. AMIA Annual Symposium. 2015.
- 43.Hribar M R, Read-Brown S, Reznick L. Secondary use of EHR timestamp data: validation and application for workflow optimization. AMIA Annu Symp Proc. 2015;2015:1909–1917. [PMC free article] [PubMed] [Google Scholar]
- 44.Aboumater H J, Winner L E, Davis R O. No time to waste: decreasing patient wait times for chemotherapy administration using automated prioritization in an oncology pharmacy system. Am J Manag Care. 2008;14(05):309–316. [PubMed] [Google Scholar]
- 45.Suzuki S. Exhausting physicians employed in hospitals in japan assessed by a health questionnaire. Sangyo Eiseigaku Zasshi. 2017;59(04):107–118. doi: 10.1539/sangyoeisei.16-022-E. [DOI] [PubMed] [Google Scholar]
- 46.Lee B-J, Park S G, Min K B. The relationship between working condition factors and well-being. Ann Occup Environ Med. 2014;26(01):34. doi: 10.1186/s40557-014-0034-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.