

Abstract
Background
Dental caries is the most common multifactorial oral disease; it affects 60% to 90% of the global population. Dental caries is highly preventable through prevention behaviors aimed at improving oral hygiene, adequate fluoride usage, and dietary intake. Mobile apps have the potential to support patients with dental caries; however, little is known about the availability, target audience, quality, and features of these apps.
Objective
This review aims to systematically examine dental caries prevention apps; to describe their content, availability, target audience, and features; and to assess their quality.
Methods
We systematically identified and evaluated apps in a process paralleling a systematic review. This included a search strategy using search terms; an eligibility assessment using inclusion and exclusion criteria focused on accessibility and dental caries self-management behaviors, including oral hygiene, dietary intake, and fluoride usage; data extraction on app characteristics, including app store metrics; prevention behavior categorization; feature identification and description; a quality appraisal of all apps using the validated Mobile App Rating Scale (MARS) assessment tool; and data comparison and analysis.
Results
Using our search strategy, we retrieved 562 apps from the Google Play Store and iTunes available in Australia. Of these, 7.1% (40/562) of the apps fit our eligibility criteria, of which 55% (22/40) targeted adults, 93% (37/40) were free to download, and 65% (26/40) were recently updated. Oral hygiene was the most common dental caries prevention behavior domain, addressed in 93% (37/40) of the apps, while dietary intake was addressed in 45% (18/40) of the apps and fluoride usage was addressed in 42% (17/40) of the apps. Overall, 50% (20/40) of the apps addressed only 1 behavior, and 38% (15/40) of the apps addressed all 3 behaviors. The mean MARS score was 2.9 (SD 0.7; range 1.8-4.4), with 45% (18/40) of the apps categorized as high quality, with a rating above 3.0 out of 5.0. We identified 21 distinctive features across all dental caries prevention behaviors; however, the top 5 most common features focused on oral hygiene. The highest-ranking app was the Brush DJ app, with an overall MARS score of 4.4 and with the highest number of features (n=13). We did not find any apps that adequately addressed dental caries prevention behaviors in very young children.
Conclusions
Apps addressing dental caries prevention commonly focus on oral hygiene and target young adults; however, many are not of high quality. These apps use a range of features to support consumer engagement, and some of these features may be helpful for specific patient populations. However, it remains unclear how effective these apps are in improving dental caries outcomes, and further evaluation is required before they are widely recommended.
Keywords: dental caries, oral hygiene, self-management, mobile applications
Introduction
Background
Dental caries is a preventable, noncommunicable multifactorial disease that affects 60% to 90% of the population globally [1,2]. When left untreated, end-stage management of dental caries can result in pain, infection, and facial swelling, leading to emergency department presentations, especially for young children [3,4]. Although highly preventable, dental caries resulted in 70,200 preventable hospitalizations in Australia from 2016 to 2017 [5]. Dental caries prevention can be achieved at the individual level by addressing specific prevention behaviors, including adequate oral hygiene practices [3], age-appropriate topical fluoride usage [6], and diet modifications that reduce the amount of free sugar consumption [7]. At present, prevention behavior change interventions have included patient-focused dietary counseling and oral hygiene instruction, mostly delivered alongside operative clinical interventions in clinical settings [8,9]. However, these interventions are time intensive, workforce intensive, and expensive to deliver; also, without regular and repeated exposure, these interventions have shown inconsistent results on sustainably improved dental caries outcomes [9,10].
Growing mobile phone ownership globally and integration with the internet [11,12] have prompted the development of and research into mobile health (mHealth) interventions to address a broad range of behavior change practices for chronic disease management. These mHealth tools seek to modify a range of broad and specific behavioral factors related to diet [13], exercise [14], and medication adherence [15,16] to manage a range of chronic conditions, including diabetes [17,18], obesity [19,20], and cardiovascular diseases [15]. A variety of mHealth interventions have shown promising results in a variety of populations across the lifespan [21,22] and have particularly provided equitable support to remote, regional, and underserved populations [23-27]. Thus, it is necessary to both use and assess mHealth as a viable modality to support behavior change in the management of a range of noncommunicable diseases, including oral diseases, namely dental caries.
Apps for Dental Caries Prevention
Dental caries has many modifiable risk factors common to other noncommunicable diseases [4,28], driving a rationale for the adoption of innovative disease management approaches, including mHealth. Current research in mHealth for oral health has largely focused on addressing periodontal diseases through motivation for oral hygiene, with the delivery of simple text messages [29-31]. A recently published systematic review of the literature, focused on oral hygiene alone, highlighted the potential of mHealth interventions to improve oral health knowledge alongside modest clinical improvements in gum health in the adult and adolescent populations [29]. However, it remains unclear whether these results can be extended to address other dental caries risk factors, including a cariogenic diet and inadequate fluoride usage. Although important across the lifespan, preventive behaviors associated with appropriate fluoride usage and low sugar diets, including the timing of consumption are particularly influential in decreasing dental caries risk during the unique developmental stages of children aged younger than 6 years [3,8]. Uninformed parents could be at greater risk of their child experiencing a preventable hospitalization because of dental caries [5,10]. Although previous studies have focused on oral hygiene [29,32], it is important for this study to systematically scope the target audience and range of apps that addressed other dental caries prevention behaviors, including adequate fluoride usage and dietary modification.
Furthermore, 2 recent reviews on apps used in oral health focused on the information analysis of apps that targeted the adult population in the United States [33] and the United Kingdom [32]. These reviews found poor information quality and identified the need to comprehensively analyze the features available in the apps alongside the use of a validated quality rating scale. The Mobile App Rating Scale (MARS) is a validated scale that has been used in a wide range of health care contexts to comprehensively assess the quality of health apps. Further analysis of features also provides information on usability and the potential for longer-term engagement with an app. Therefore, this study aims to systematically examine oral health apps that address a range of modifiable dental caries prevention factors and to systematically describe their content, availability, target audience, features, and quality.
Methods
Systematic Search Strategy
This review was conducted using a stepwise approach according to a previously published methodology that parallels a systematic review (Figure 1) [15]. We searched the main app stores: Google Play Store and iTunes. Of the 5.6 million apps available internationally, Google Play offers 2.47 million apps, and iTunes offers 1.8 million apps [34]. The search was conducted on the Google Play Store and iTunes with the app store country and region set to Australia between January 8 and 19, 2019, using the top 8 key search terms. These search terms were chosen based on their performance in retrieving the highest number of relevant apps for dental caries prevention from preliminary searches. The final list was developed and agreed upon by all authors and focused on the self-management behaviors that support dental caries prevention across all age groups, including young children. These search terms included dental caries, early childhood caries, tooth decay, dental caries prevention, early childhood caries prevention, tooth decay prevention, saliva, and fluoride.
Figure 1.
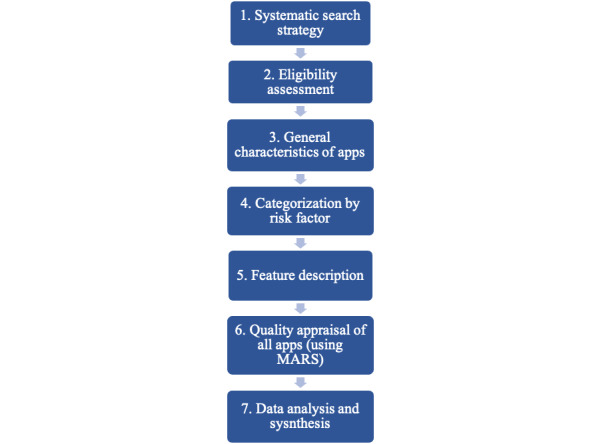
Schematic steps of the systematic review and quality evaluation. MARS: Mobile App Rating Scale.
Eligibility Assessment
All apps retrieved from the search were screened by 2 independent reviewers (RC and GW) for eligibility using prespecified inclusion and exclusion criteria (Textbox 1) that aimed to identify relevant apps that were accessible to most of the general public relevant to dental caries prevention.
Inclusion and exclusion criteria.
Inclusion criteria
The app focused on supporting the general public of any age to address prevention behaviors associated with dental caries prevention
-
The app addressed dental caries prevention factors:
Oral hygiene including toothbrushing
Fluoride usage
Diet modification
The app was accessible to the care context of Australia.
The app was in the English language.
Exclusion criteria
Apps targeted at clinicians or student clinicians
Apps that were not related to health and were considered arcade games only
Apps that addressed other health or oral health issues but were not specific to dental caries
Apps that were priced or had in-app purchases or electronic devices such as electric toothbrushes priced above Aus $3.00 (US $2.29), which is the average price that consumers are willing to pay for an app [35] to ensure affordability
Apps that were associated with a specific health clinic
General Characteristics of Apps
All apps that fit the inclusion criteria were downloaded on either the Android platform using a Samsung smartphone (Galaxy 9) or the iOS platform using an iPhone XR. The general characteristics of the apps were adapted from the classification section of the MARS tool (Multimedia Appendix 1) to describe the app name, app developer, date of the last update, platform (Google Play or iTunes), cost, star rating according to the app store, affiliations, target age groups, and focus of the app.
Categorization by Prevention Factors
Apps were categorized according to broad modifiable factors associated with dental caries prevention: oral hygiene, fluoride, and diet. For apps to be classified as addressing oral hygiene, at minimum, information about the importance of good oral hygiene for dental caries prevention had to be present in the app. Additional information and features could include a video demonstration of tooth brushing or interdental cleaning techniques, such as dental flossing, or gamification of toothbrushing, defined as the use of game elements in nongame contexts [36]. For fluoride, some information about the effects of fluoride from various modalities, including toothpaste or water consumption related to dental caries prevention, could be included. For diet, information on specific diet changes that could influence dental caries outcomes, for example, the use of a traffic light grading system to educate and encourage users to swap food choices to alternatives with less sugar [37], could be included.
Feature Description and Analysis
Features are elements of an app designed to increase interactivity and consumer engagement. For oral health apps, these features may include gamification and timers [33]. For the feature description, we identified and defined these through an iterative process combining terminology from previously published literature [15,38,39] with input from experts in the field and all authors. Further analysis was conducted to catalog the features of all apps stratified by the broad dental caries prevention factor each app addressed and to identify common features.
Quality Appraisal of Apps
All apps that fit the inclusion criteria were evaluated for quality using the MARS (Multimedia Appendix 1). This scale provides a standardized approach with 19 objective items and provides appraisal across 4 subscales: engagement, functionality, esthetics, and information quality [38,40]. The engagement subscale appraises whether the app was fun, interesting, customizable, and interactive (eg, push notifications, sends alerts) to the target audience. The functionality subscale assesses whether the app is correctly functioning and easy to learn, with easy navigations and logical flow. The esthetic subscale provides appraisal with regard to the general visual appeal and stylistic consistency of the app. Finally, the information subscale assesses the quality of the information, for example, whether the textual information and references are from credible sources. The overall MARS also sets a minimum quality threshold score of 3.0 out of 5.0, providing the ability to identify high-quality apps to patients and clinicians or further analysis [41]. It has been used in various contexts with excellent internal consistency and interrater reliability [15,42-46]. In total, 2 independent reviewers (RC and GW) were trained to use the MARS instruments through a web-based training program created by the MARS developers [38]. Each reviewer independently spent at least 30 min to thoroughly test each app on both devices. Data on the objective subscales of the MARS and additional features of the apps were extracted and entered into an Excel (Microsoft Corporation) spreadsheet. The items were rated on a 5-point scale (1: inadequate, 2: poor, 3: acceptable, 4: good, and 5: excellent). Any disagreements between the 2 reviewers were resolved by taking a consensus discussion. We calculated the means of the MARS and interrater reliability scores between reviewers using SPSS version 22.0 (IBM Corporation). High-quality apps were determined from the overall threshold score of 3 out of 5 in the overall mean score as defined by the developers of MARS, providing the ability to identify high-quality apps for further analysis [38,41].
Data Analysis and Synthesis
Further data analysis and synthesis were conducted based on the iteratively generated hypothesis from the initial MARS quality analysis. First, we wanted to compare the quality rating between apps that addressed a differing number and range of dental caries prevention factors. Second, the correlation between the MARS quality rating and the number of features across all apps was conducted.
Results
Systematic Search and Eligibility Assessment
Our systematic search retrieved a total of 562 apps, with 532 (94.7%) apps identified in the Google Play Store alone, 22 (5.3%) apps identified in iTunes alone, and 8 (1.4%) apps found in both stores. These apps were screened for eligibility, and 92.9% (522/562) were excluded based on the inclusion or exclusion criteria. The reasons for exclusion are presented in Textbox 1. A total of 40 (7.1%) unique apps were included for further analysis (Figure 2).
Figure 2.
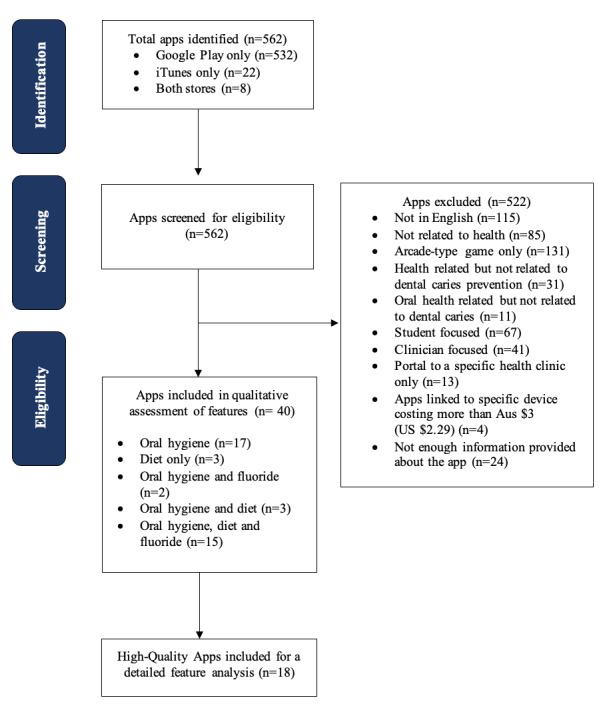
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of apps identified through the systematic search.
General Characteristics of Apps
Most of the apps (37/40, 93%) were free to download, with only 3 of the 40 apps (8%) incurring a cost between Aus $0.99 (US $0.75) and Aus $2.99 (US $2.29) on iTunes alone. More than half (26/40, 65%) of the apps included were recent and current, as they were last updated either in 2018 or 2019. A total of 29 out of 40 apps (73%) were available on the Google Play Store only, and 3 out of 40 apps (8%) were available on the iTunes store only; 20% (8/40) of the apps were available in both stores (Multimedia Appendix 2).
Most (27/40, 68%) of the apps’ affiliations were unknown, and 9 of 40 apps (23%) had clear commercial affiliations. Only 10% (4/40) of apps had affiliations with a university, and 50% (2/4) of these apps, namely, Brush DJ and My Dental-Care - Your Guide to Oral Health, had affiliations with the UK National Health Service, a government affiliation. More than half (22/40, 55%) of the apps were targeted toward adults or young adults, with 63% (14/22) of these apps also targeted adolescents. Apps classified as targeting a general audience were 18% (7/40), whereas 28% (11/40) of apps were targeted at children aged older than 7 years. When analyzing the focus of the app, half (20/40, 50%) of the apps focused on information provision, such as health-seeking behaviors. The other half of the apps provided additional behavior change prompts, with 70% (14/20) of the apps providing specific goal setting functions within the app.
Categorization by Prevention Factor
Of the 40 included apps addressing a range of dental caries prevention factors, 37 (93%) addressed oral hygiene, 17 (43%) addressed fluoride, and 21 (53%) addressed diet (Figure 3). Furthermore, 50% (20/40) of apps addressed only one of these factors for oral health, 12% (5/40) of apps addressed 2 factors, and 38% (15/40) of apps addressed all 3 factors. Of the 20 apps that addressed only 1 factor, 17 (85%) addressed oral hygiene alone and 3 (15%) addressed diet alone. Of the 5 apps that addressed 2 factors, these combinations included oral hygiene and fluoride with 2 (40%) apps and oral hygiene and diet with 3 (60%) apps (Figure 4).
Figure 3.
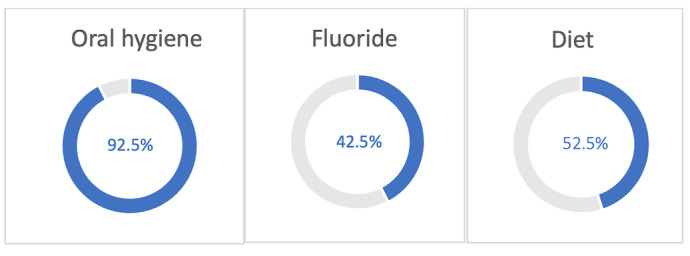
Percentage of all apps that addressed each prevention factor.
Figure 4.
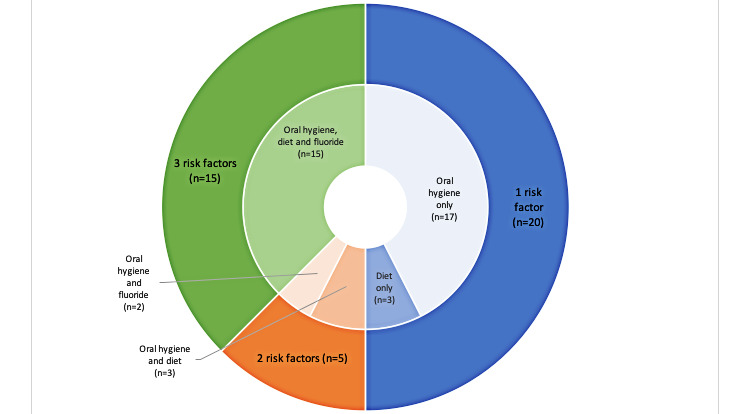
Categorization of apps according to the number and types of prevention factors addressed. (The outer rim indicates the number of prevention factors each app addressed. The inner rim shows the combination of the types of prevention factors that each app addressed).
Of the 40 apps that fit our inclusion criteria, 37 (93%) addressed oral hygiene, 17 (43%) addressed fluoride, and 21 (53%) addressed diet.
Feature Description and Analysis
A total of 21 features were identified; these features were grouped into general and specific features related to each dental caries prevention factor, including oral hygiene, fluoride usage, and diet. The list of features and descriptions are outlined in Textbox 2; each feature was given a label to allow for a corresponding reference to Multimedia Appendix 3. Most of the unique features identified were associated with oral hygiene (9/21, 43% features), compared with fluoride (2/21, 10% of features) and diet (5/21, 24% of features; Multimedia Appendix 3). Other than web-based social media support, considered to be a general feature, the top 5 most common features found in all apps addressed oral hygiene (Figure 5). The Brush DJ app had the highest number of features at 13 (Multimedia Appendix 3). Of 37 of 40 apps that addressed oral hygiene, 17 (46%) had the tooth brush timer as the most common feature, followed by goal setting (9/37, 24% of apps), gamification (8/37, 22% of apps), and 5 apps (14%) with a video demonstration of oral hygiene techniques. The Brush DJ app and the Disney Magic Timer app had the highest number of oral hygiene–related features, with each of these apps having 78% (7/9) of these features. Only 12% (2/17) of apps that addressed the fluoride prevention factor adequately provided additional information and used visual aids to support the information provided, for example, the appropriate amount of fluoride toothpaste that should be dispensed for children. These 2 apps, namely, My Dental-Care - Your Guide to Oral Health and Brush DJ, were also the only apps that were affiliated with both a university and government health service. Of the 21 apps that addressed diet, the Food For Teeth - Food Database and Diet Diary app was the only app that included additional features such as an ability to record a diet diary, with a database of food items, including their pictures and serving size embedded in a traffic light system [47].
Features of high-quality apps based on the Mobile App Rating Scale.
-
General features:
Updates conducted in 2018 or 2019: recent updates to ensure that glitches are resolved
Data security: developer ensures data security, in accordance with mobile app regulatory statement, for example, Health Insurance Portability and Accountability Act compliance
Data exporting and sharing to clinicians: ability to link information readily to the clinician or the electronic health record
Tracking of dental appointments: ability to record dental appointments
Online social media support: ability to connect to social media networks such as Facebook
-
Features related to oral hygiene:
Tooth brushing timer: timer to encourage patients to brush for a certain amount of time
Tips for better oral hygiene: evidence-based information to improve oral hygiene
Video demonstration: demonstration of brushing techniques via videos
Goal setting: ability for user to input specific oral hygiene focused goal
Tracking of oral health behavior: availability of statistics and charts on trends and adherence rates
Push notifications (reminders): alert on the phone to remind patients to behavior change, for example, brushing their teeth
Gamification: apps that use game elements to encourage users to brush their teeth. This can include virtual reality battles to encourage brushing length
Incentivization: earn prizes for virtual characters or cryptocurrency—may be reduce the cost of your next appointment
Sync to other apps on the phone: for example, the app may sync to a playlist to encourage brushing
-
Features related to fluoride:
Provision of fluoride information: information about fluoride usage is in accordance with country guidelines
Pictures of the amount of toothpaste: visual aids to demonstrate the amount of fluoride toothpaste that is to be placed on the toothbrush
-
Features related to diet:
Provision of dietary information: information about the connection between dietary habits and dental caries information on alternatives
Diet diary: ability for the user to input food intake and time of consumption
Text search for food items: search bar to allow ease of entry of the food item consumed
Pictures of food: picture of food to correspond to diet diary with a traffic light grading system to encourage users to consider low sugar alternatives
Serving size of food: ability to record the amount and not just the type of food consumed
Figure 5.
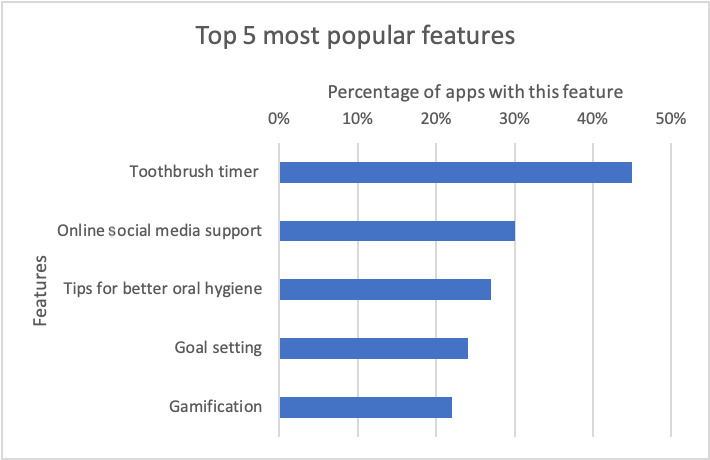
Top 5 most common features found in apps.
Quality Appraisal of Apps
Of the 40 apps, 18 (45%) were considered high quality, determined by reaching the minimum overall MARS threshold score of 3.0 out of 5.0. However, the MARS quality rating for each of the 40 apps found only 10 (25%) of these apps scored above 3.0 in all 4 subscales (Multimedia Appendix 4). The results also did not indicate that any single item in either of the 4 MARS subscales stood out. The interrater reliability between the reviewers, calculated from the overall and subscale scores of MARS for all apps, was excellent through the use of a two-way mixed intraclass correlation coefficient of 0.907 (95% CI 0.873-0.932). The Brush DJ app was the highest rated app with an overall MARS score of 4.4. This app also scored above the threshold for all subscales. The Brush DJ was also the only app that had scientific literature published, where a cross-sectional user acceptability questionnaire demonstrated 70.0% (133/189) of participants self-reported that the app motivated them to brush their teeth for longer [48]. However, the clinical effectiveness of this app is yet to be trialed using a study design that measures clinical health outcomes. Given the availability of only 1 app with supporting scientific literature published in this emerging field of inquiry, we followed the methodology adopted by other researchers in this situation [41] and excluded item 19 from our final calculation of the overall information subscale.
Data Analysis and Synthesis
Further data analysis and synthesis was developed based on an iteratively generated hypothesis from the initial MARS quality analysis. First, we wanted to compare MARS scores between apps that addressed a differing number and range of prevention factors. Second, because the app that had the highest MARS rating also had the highest number of features, we hypothesized a correlation between MARS scores and the number of features identified in each app. Table 1 shows that apps addressing the oral hygiene factor had the highest mean overall MARS scores (3.3) compared with apps addressing a combination of other factors: diet (2.2), oral hygiene and fluoride (1.9), and oral hygiene and diet (2.2). Apps addressing oral hygiene alone also had the highest subscale scores in engagement (3.3), functionality (3.8), and aesthetics (3.3). Although oral hygiene apps ranked equal to apps that addressed all 3 factors in the mean information subscale, with a MARS score (2.9), the percentage of apps that were considered high quality was more consistent for apps addressing all 3 factors (8/15, 54%; Table 1). Apps that addressed the oral hygiene factor alone had the highest percentage of apps that were considered high quality in the engagement (10/17, 59%) and esthetic (13/17, 76%) subscales. Apps that addressed all 3 factors were more likely to score above the threshold in the MARS information subscale (8/15, 54%) compared with apps that addressed 1 (7/20, 35%) factor. Of the apps, 20% (3/15) that addressed all 3 factors also ranked comparatively poorly on engagement scores compared with 59% of apps (10/17) that addressed only the oral hygiene factor.
Table 1.
Mobile App Rating Scale quality rating summary in dental caries prevention factor categories.
| MARSa subscale | 1 factor | 2 factors | 3 factors | |||||||
|
|
Oral hygiene only (n=17) | Diet only (n=3) | Oral hygiene and fluoride (n=2) | Oral hygiene and diet (n=3) | Oral hygiene, diet, and fluoride (n=15) | |||||
|
|
MARS score, mean (SD) | Quality appsb, n (%) | MARS score, mean (SD) | Quality apps, n (%) | MARS score, mean (SD) | Quality apps, n (%) | MARS score, mean (SD) | Quality apps, n (%) | MARS score, mean (SD) | Quality apps, n (%) |
| Overall | 3.3 (0.5) | 10 (59) | 2.7 (0.6) | 0 (0) | 1.9 (0.2) | 0 (0) | 2.6 (1.2) | 1 (33) | 2.9 (0.8) | 6 (40) |
| Engagement | 3.0 (0.6) | 10 (59) | 2.3 (0.5) | 0 (0) | 1.3 (0.1) | 0 (0) | 2.8 (1.3) | 1 (33) | 2.5 (0.9) | 3 (20) |
| Functionality | 3.9 (0.7) | 15 (88) | 3.8 (0.0) | 3 (100) | 2.6 (0.2) | 0 (0) | 2.6 (1.3) | 1 (33) | 3.6 (0.7) | 12 (80) |
| Aesthetics | 3.3 (0.7) | 13 (76) | 2.4 (0.2) | 0 (0) | 1.8 (0.2) | 0 (0) | 2.4 (1.4) | 1 (33) | 2.6 (0.7) | 5 (33) |
| Informationc | 2.9 (0.7) | 7 (41) | 2.2 (1.3) | 1 (33) | 1.9 (0.4) | 0 (0) | 2.2 (1.3) | 1 (33) | 2.9 (0.8) | 8 (54) |
aMARS: Mobile App Rating Scale.
bPercentage of apps determined to be of high quality, determined by an overall score that reached above the minimum threshold score of above 3.0 out of 5.0.
cItem 19 of the information subscale was excluded from the final calculation, as only 1 app supported the scientific literature published in this emerging field of inquiry, a similar methodology adopted by other researchers in this context [41].
When analyzing the number of features, high-quality apps, categorized as those with an overall MARS score above 3, had almost double the mean number of features compared with low-quality apps, which was consistent across all categories (Multimedia Appendix 5). However, when comparing the individual apps with the MARS quality rating, the correlation between quality and the number of features showed variance and showed only a moderate general trend that high-quality apps had more features compared with low-quality apps (Figure 6).
Figure 6.
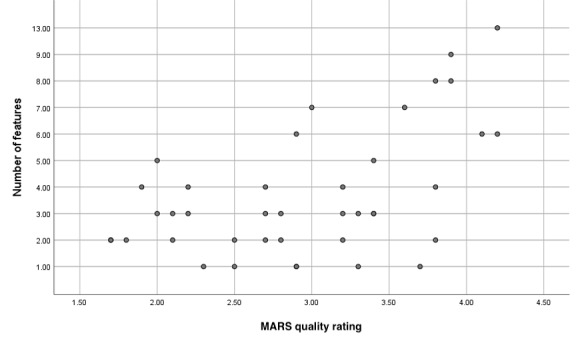
Number of features compared with the MARS quality rating scale for each app. MARS: Mobile App Rating Scale.
Discussion
Principal Findings
Our study identified and assessed the characteristics, features, and quality of 40 apps targeted at the general public addressing a range of dental caries prevention factors. Less than half (18/40, 45%) of the apps were considered good quality (based on the overall MARS); however, only 25% (10/40) of apps were considered high quality across all 4 subscales of MARS. Most apps (37/40, 93%) focused on oral hygiene, and these apps were also more likely to contain a higher number of features and target the young adults or adolescent population. Only 13% (5/40) of apps addressed all 3 factors and were considered high quality, indicating only a small number of apps that could be further tested for clinical effectiveness specific to the adolescent or young adult populations. This could be recommended for the highest rated app, Brush DJ, which scored highly across all 4 subscales, demonstrating that it is possible to create an app that is able to provide good information and be aesthetically appealing. We did not find any high-quality apps targeted to parents of very young children that would address the specific dental caries prevention behaviors associated with caring for children aged between 0 and 6 years. Therefore, our study indicates an opportunity for future high-quality app development that addresses a range of dental caries prevention behaviors alongside a consideration for esthetics and engaging features to support this target parent population.
Comparison With Prior Work
This study goes further than 2 previous reviews of mHealth apps focused on oral hygiene only [32] and oral health promotion in adult populations only [33] by scoping a broad range of dental caries prevention factors. Our study also responds to the need for feature analysis and quality appraisal outlined by the 2 most recent reviews on apps used for oral health [32,33]. First, our study provides the feature analysis of apps addressing a range of dental caries prevention behaviors, including diet modification and adequate fluoride usage. Second, the study provides an in-depth quality appraisal using the MARS tool. Consistent with the information quality concerns raised by these previous reviews, our analysis found 24 of 40 (60%) apps to be of low quality according to the MARS tool, yet still available to the general public. To address the issue of app quality [32], the National Health Service in the United Kingdom has created a digital app library that could be a trusted source of information for both clinicians and patients [49].
Our quality appraisal using the MARS assessment identified Brush DJ to be the highest-ranking app in quality and features, a similar finding from previously published reviews focused on oral hygiene in the United Kingdom [32]. At present, the Brush DJ app is the only app endorsed by the National Health Service’s digital app library [50]. Further well-designed clinical trials to determine the clinical efficacy of this app within the adolescent or young adult target populations should be undertaken. These clinical trials should have a clear clinical question with a good study design and be a randomized controlled trial where possible, with defined measurable health outcomes and a complementary economic evaluation [51]. Clinical effectiveness shown through improvements in measurable health outcomes will facilitate a more widespread adoption of this app and other effective apps in clinical practice.
Implications
Dental caries is a multifactorial disease with varied risk factors that may impact individual patients differently during their life course [2,3]. Our study identified a lack of apps targeted to parents of children that adequately addressed prevention behaviors associated with fluoride usage and low-cariogenic diets for children aged younger than 6 years [3,52]. Given the paucity surrounding the clinical efficacy of mHealth apps in the field of dentistry [29], before a well-designed clinical trial can be conducted in this target population [48,53], a high-quality app needs to be designed. This app must target specific behaviors relevant to a broad range of dental caries prevention behaviors and contain evidence-based information, with appropriate features and esthetics to ensure the engagement of parents. To date, no high-quality app has achieved this. Thus, more user-focused, iterative co-designed research [54] relevant to the target population is needed to determine engaging features that will address all relevant dental caries prevention behaviors. Our assessment of features will provide a blueprint to assist future researchers engaged in qualitative user engagement research with parents, patients, clinicians, professional dental associations, health services, and research organizations [51,55] to develop a high-quality app that could then be trialed for clinical effectiveness.
Limitations
Our review was conducted in Australia in 2019, and the included apps were limited to those available in Australian app stores at the specific time of the systematic search. Most apps included in this review have been developed in predominately English-speaking countries outside Australia, the United Kingdom, Canada, Asia, and the United States. We recognize that there may be apps developed in other languages or only available in country-specific app stores that were not included in our review. However, we did find a similar number of apps for the final analysis when using search terms similar to previous studies undertaken in other countries, including the United Kingdom [32] and the United States [33]. Second, in our study, MARS was used by researchers with clinical backgrounds in the field of oral health and primarily reflected this perspective. Our scoping study did not involve patients as participants and highlights the importance of conducting further complementary research that involves end users and giving voice to the patient’s perspective during the development of future apps and mHealth interventions [56].
Conclusions
The increasing use of mHealth apps driven by increasing public use of mobile devices presents a call for dental researchers, health system managers, policy makers, and health professionals to engage with and provide more rigorous scientific recommendations around oral health apps. Our study provides a systematic and detailed analysis of the current availability, target audience, quality, and features of apps targeted toward dental caries. Quality was variable across the apps and mainly targeted the adolescent and adult populations. The most common features found in high-quality apps, such as gamification and goal setting, still focus on oral hygiene factors. It is unclear if these features can be used to address other dental caries prevention factors such as fluoride and diet modification. There was also an identified gap in apps available to support the target audience of parents of young children. There is a real need to co-design and create apps that address a broad range of modifiable risk factors associated with dental caries targeted at parents of children aged younger than 6 years. To ensure the highest quality in apps, the co-design process should include the clinician, researcher, and patient perspectives on evidence-based information and engaging features. Further studies are needed to determine the clinical efficacy of these apps before they can be widely recommended.
Abbreviations
- MARS
Mobile App Rating Scale
- mHealth
mobile health
Appendix
Mobile App Rating Scale tool developed by Queensland University of Technology (QUT).
General characteristics of all apps.
Comparative analysis of quality features present in all apps.
Quality evaluation of all apps according to the objective subscales of the Mobile App Rating Scale (MARS) quality appraisal tool.
Mean number of features present in high-quality versus low-quality apps within dental caries prevention factors.
Footnotes
Authors' Contributions: RC, the lead author, provided substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work and drafting the work. KS provided substantial contributions to the conception or design of the work or interpretation of data for the work. GW provided substantial contributions to the acquisition and analysis of the work and drafted this work. WS provided substantial contributions to the conception or design of the work. HS provided substantial contributions to the conception or design of the work. CC, an equal last author, provided substantial contributions to the conception or design of the work and the analysis and interpretation of data for the work. MI, an equal last author, provided substantial contributions to the conception or design of the work and the acquisition, analysis, or interpretation of data for the work and had drafted the work.
All authors revised this work critically for important intellectual content and had final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of Interest: None declared.
References
- 1.Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. 2015 May;94(5):650–8. doi: 10.1177/0022034515573272. [DOI] [PubMed] [Google Scholar]
- 2.Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, Tagami J, Twetman S, Tsakos G, Ismail A. Dental caries. Nat Rev Dis Primers. 2017 May 25;3:17030. doi: 10.1038/nrdp.2017.30. [DOI] [PubMed] [Google Scholar]
- 3.Phantumvanit P, Makino Y, Ogawa H, Rugg-Gunn A, Moynihan P, Petersen PE, Evans W, Feldens CA, Lo E, Khoshnevisan MH, Baez R, Varenne B, Vichayanrat T, Songpaisan Y, Woodward M, Nakornchai S, Ungchusak C. WHO global consultation on public health intervention against early childhood caries. Community Dent Oral Epidemiol. 2018 Jun;46(3):280–7. doi: 10.1111/cdoe.12362. [DOI] [PubMed] [Google Scholar]
- 4.Peres MA, Macpherson LM, Weyant RJ, Daly B, Venturelli R, Mathur MR, Listl S, Celeste RK, Guarnizo-Herreño CC, Kearns C, Benzian H, Allison P, Watt RG. Oral diseases: a global public health challenge. Lancet. 2019 Jul 20;394(10194):249–260. doi: 10.1016/S0140-6736(19)31146-8. [DOI] [PubMed] [Google Scholar]
- 5.Al Rawahi SH, Asimakopoulou K, Newton JT. Theory based interventions for caries related sugar intake in adults: systematic review. BMC Psychol. 2017 Jul 25;5(1):25. doi: 10.1186/s40359-017-0194-z. https://bmcpsychology.biomedcentral.com/articles/10.1186/s40359-017-0194-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Walsh T, Worthington HV, Glenny AM, Marinho VC, Jeroncic A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019 Mar 04;3:CD007868. doi: 10.1002/14651858.CD007868.pub3. http://europepmc.org/abstract/MED/30829399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Moynihan P, Makino Y, Petersen PE, Ogawa H. Implications of WHO guideline on sugars for dental health professionals. Community Dent Oral Epidemiol. 2018 Feb;46(1):1–7. doi: 10.1111/cdoe.12353. [DOI] [PubMed] [Google Scholar]
- 8.Arrow P, Raheb J, Miller M. Brief oral health promotion intervention among parents of young children to reduce early childhood dental decay. BMC Public Health. 2013 Mar 20;13:245. doi: 10.1186/1471-2458-13-245. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-13-245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Harris R, Gamboa A, Dailey Y, Ashcroft A. One-to-one dietary interventions undertaken in a dental setting to change dietary behaviour. Cochrane Database Syst Rev. 2012 Mar 14;(3):CD006540. doi: 10.1002/14651858.CD006540.pub2. http://europepmc.org/abstract/MED/22419315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Henshaw M, Borrelli B, Gregorich S, Heaton B, Tooley E, Santo W, Cheng N, Rasmussen M, Helman S, Shain S, Garcia R. Randomized trial of motivational interviewing to prevent early childhood caries in public housing. JDR Clin Trans Res. 2018 Oct;3(4):353–365. doi: 10.1177/2380084418794377. http://europepmc.org/abstract/MED/30238060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Share of mobile phone users that use a smartphone in Australia from 2014 to 2019. Statista. 2019. Aug 27, [2019-08-27]. https://www.statista.com/statistics/257041/smartphone-user-penetration-in-australia/
- 12.Silver L, Huang C. Social activities, information seeking on subjects like health and education top the list of mobile activities. Pew Research Center. 2019. Aug 22, [2019-08-27]. https://www.pewresearch.org/internet/2019/08/22/social-activities-information-seeking-on-subjects-like-health-and-education-top-the-list-of-mobile-activities/
- 13.Kebede MM, Liedtke TP, Möllers T, Pischke CR. Characterizing active ingredients of eHealth interventions targeting persons with poorly controlled type 2 diabetes mellitus using the behavior change techniques taxonomy: scoping review. J Med Internet Res. 2017 Oct 12;19(10):e348. doi: 10.2196/jmir.7135. https://www.jmir.org/2017/10/e348/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nelligan RK, Hinman RS, Atkins L, Bennell KL. A short message service intervention to support adherence to home-based strengthening exercise for people with knee osteoarthritis: intervention design applying the behavior change wheel. JMIR Mhealth Uhealth. 2019 Oct 18;7(10):e14619. doi: 10.2196/14619. https://mhealth.jmir.org/2019/10/e14619/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Santo K, Richtering SS, Chalmers J, Thiagalingam A, Chow CK, Redfern J. Mobile phone apps to improve medication adherence: a systematic stepwise process to identify high-quality apps. JMIR Mhealth Uhealth. 2016 Dec 02;4(4):e132. doi: 10.2196/mhealth.6742. https://mhealth.jmir.org/2016/4/e132/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Badawy SM, Shah R, Beg U, Heneghan MB. Habit strength, medication adherence, and habit-based mobile health interventions across chronic medical conditions: systematic review. J Med Internet Res. 2020 Apr 28;22(4):e17883. doi: 10.2196/17883. https://www.jmir.org/2020/4/e17883/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pfammatter A, Spring B, Saligram N, Davé R, Gowda A, Blais L, Arora M, Ranjani H, Ganda O, Hedeker D, Reddy S, Ramalingam S. mHealth intervention to improve diabetes risk behaviors in India: a prospective, parallel group cohort study. J Med Internet Res. 2016 Aug 05;18(8):e207. doi: 10.2196/jmir.5712. https://www.jmir.org/2016/8/e207/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lunde P, Nilsson BB, Bergland A, Kværner KJ, Bye A. The effectiveness of smartphone apps for lifestyle improvement in noncommunicable diseases: systematic review and meta-analyses. J Med Internet Res. 2018 May 04;20(5):e162. doi: 10.2196/jmir.9751. https://www.jmir.org/2018/5/e162/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kay MC, Burroughs J, Askew S, Bennett GG, Armstrong S, Steinberg DM. Digital weight loss intervention for parents of children being treated for obesity: a prospective cohort feasibility trial. J Med Internet Res. 2018 Dec 20;20(12):e11093. doi: 10.2196/11093. https://www.jmir.org/2018/12/e11093/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Haas K, Hayoz S, Maurer-Wiesner S. Effectiveness and feasibility of a remote lifestyle intervention by dietitians for overweight and obese adults: pilot study. JMIR Mhealth Uhealth. 2019 Apr 11;7(4):e12289. doi: 10.2196/12289. https://mhealth.jmir.org/2019/4/e12289/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Albanese-O'Neill A, Schatz DA, Thomas N, Bernhardt JM, Cook CL, Haller MJ, Bernier AV, Silverstein JH, Westen SC, Elder JH. Designing online and mobile diabetes education for fathers of children with type 1 diabetes: mixed methods study. JMIR Diabetes. 2019 Aug 06;4(3):e13724. doi: 10.2196/13724. https://diabetes.jmir.org/2019/3/e13724/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yerrakalva D, Yerrakalva D, Hajna S, Griffin S. Effects of mobile health app interventions on sedentary time, physical activity, and fitness in older adults: systematic review and meta-analysis. J Med Internet Res. 2019 Nov 28;21(11):e14343. doi: 10.2196/14343. https://www.jmir.org/2019/11/e14343/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Anderson-Lewis C, Darville G, Mercado RE, Howell S, Di Maggio S. mHealth technology use and implications in historically underserved and minority populations in the united states: systematic literature review. JMIR Mhealth Uhealth. 2018 Jun 18;6(6):e128. doi: 10.2196/mhealth.8383. https://mhealth.jmir.org/2018/6/e128/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Somers C, Grieve E, Lennon M, Bouamrane M, Mair FS, McIntosh E. Valuing mobile health: an open-ended contingent valuation survey of a national digital health program. JMIR Mhealth Uhealth. 2019 Jan 17;7(1):e3. doi: 10.2196/mhealth.9990. https://mhealth.jmir.org/2019/1/e3/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Saleh S, Farah A, Dimassi H, El Arnaout N, Constantin J, Osman M, El Morr C, Alameddine M. Using mobile health to enhance outcomes of noncommunicable diseases care in rural settings and refugee camps: randomized controlled trial. JMIR Mhealth Uhealth. 2018 Jul 13;6(7):e137. doi: 10.2196/mhealth.8146. https://mhealth.jmir.org/2018/7/e137/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hughson J, Daly J, Woodward-Kron R, Hajek J, Story D. The rise of pregnancy apps and the implications for culturally and linguistically diverse women: narrative review. JMIR Mhealth Uhealth. 2018 Nov 16;6(11):e189. doi: 10.2196/mhealth.9119. https://mhealth.jmir.org/2018/11/e189/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Willcox JC, Dobson R, Whittaker R. Old-fashioned technology in the era of 'Bling': is there a future for text messaging in health care? J Med Internet Res. 2019 Dec 20;21(12):e16630. doi: 10.2196/16630. https://www.jmir.org/2019/12/e16630/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Watt RG, Daly B, Allison P, Macpherson LM, Venturelli R, Listl S, Weyant RJ, Mathur MR, Guarnizo-Herreño CC, Celeste RK, Peres MA, Kearns C, Benzian H. Ending the neglect of global oral health: time for radical action. Lancet. 2019 Jul 20;394(10194):261–272. doi: 10.1016/S0140-6736(19)31133-X. [DOI] [PubMed] [Google Scholar]
- 29.Toniazzo MP, Nodari D, Muniz FW, Weidlich P. Effect of mHealth in improving oral hygiene: a systematic review with meta-analysis. J Clin Periodontol. 2019 Mar;46(3):297–309. doi: 10.1111/jcpe.13083. [DOI] [PubMed] [Google Scholar]
- 30.Borrelli B, Henshaw M, Endrighi R, Adams WG, Heeren T, Rosen RK, Bock B, Werntz S. An interactive parent-targeted text messaging intervention to improve oral health in children attending urban pediatric clinics: feasibility randomized controlled trial. JMIR Mhealth Uhealth. 2019 Nov 11;7(11):e14247. doi: 10.2196/14247. https://mhealth.jmir.org/2019/11/e14247/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Marshman Z, Ainsworth H, Chestnutt IG, Day P, Dey D, El Yousfi S, Fairhurst C, Gilchrist F, Hewitt C, Jones C, Kellar I, Pavitt S, Robertson M, Shah S, Stevens K, Torgerson D, Innes N. Brushing RemInder 4 Good oral HealTh (BRIGHT) trial: does an SMS behaviour change programme with a classroom-based session improve the oral health of young people living in deprived areas? A study protocol of a randomised controlled trial. Trials. 2019 Jul 23;20(1):452. doi: 10.1186/s13063-019-3538-6. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-019-3538-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Parker K, Bharmal RV, Sharif MO. The availability and characteristics of patient-focused oral hygiene apps. Br Dent J. 2019 Apr;226(8):600–604. doi: 10.1038/s41415-019-0197-7. [DOI] [PubMed] [Google Scholar]
- 33.Tiffany B, Blasi P, Catz SL, McClure JB. Mobile apps for oral health promotion: content review and heuristic usability analysis. JMIR Mhealth Uhealth. 2018 Sep 04;6(9):e11432. doi: 10.2196/11432. https://mhealth.jmir.org/2018/9/e11432/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Clements J. Number of apps available in leading app stores as of 3rd quarter 200. Statista. 2020. [2020-03-01]. https://www.statista.com/statistics/276623/number-of-apps-available-in-leading-app-stores/
- 35.Peng W, Kanthawala S, Yuan S, Hussain SA. A qualitative study of user perceptions of mobile health apps. BMC Public Health. 2016 Nov 14;16(1):1158. doi: 10.1186/s12889-016-3808-0. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-016-3808-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Floryan M, Chow PI, Schueller SM, Ritterband LM. The model of gamification principles for digital health interventions: evaluation of validity and potential utility. J Med Internet Res. 2020 Jun 10;22(6):e16506. doi: 10.2196/16506. https://www.jmir.org/2020/6/e16506/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dunford E, Trevena H, Goodsell C, Ng KH, Webster J, Millis A, Goldstein S, Hugueniot O, Neal B. FoodSwitch: a mobile phone app to enable consumers to make healthier food choices and crowdsourcing of national food composition data. JMIR Mhealth Uhealth. 2014 Aug 21;2(3):e37. doi: 10.2196/mhealth.3230. https://mhealth.jmir.org/2014/3/e37/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M. Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth. 2015 Mar 11;3(1):e27. doi: 10.2196/mhealth.3422. https://mhealth.jmir.org/2015/1/e27/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chen J, Cade JE, Allman-Farinelli M. The most popular smartphone apps for weight loss: a quality assessment. JMIR Mhealth Uhealth. 2015 Dec 16;3(4):e104. doi: 10.2196/mhealth.4334. https://mhealth.jmir.org/2015/4/e104/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Stoyanov SR, Hides L, Kavanagh DJ, Wilson H. Development and validation of the user version of the Mobile Application Rating Scale (uMARS) JMIR Mhealth Uhealth. 2016 Jun 10;4(2):e72. doi: 10.2196/mhealth.5849. https://mhealth.jmir.org/2016/2/e72/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mani M, Kavanagh DJ, Hides L, Stoyanov SR. Review and evaluation of mindfulness-based iPhone apps. JMIR Mhealth Uhealth. 2015 Aug 19;3(3):e82. doi: 10.2196/mhealth.4328. https://mhealth.jmir.org/2015/3/e82/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cheng H, Tutt A, Llewellyn C, Size D, Jones J, Taki S, Rossiter C, Denney-Wilson E. Content and quality of infant feeding smartphone apps: five-year update on a systematic search and evaluation. JMIR Mhealth Uhealth. 2020 May 27;8(5):e17300. doi: 10.2196/17300. https://mhealth.jmir.org/2020/5/e17300/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Siddique AB, Krebs M, Alvarez S, Greenspan I, Patel A, Kinsolving J, Koizumi N. Mobile apps for the care management of chronic kidney and end-stage renal diseases: systematic search in app stores and evaluation. JMIR Mhealth Uhealth. 2019 Sep 04;7(9):e12604. doi: 10.2196/12604. https://mhealth.jmir.org/2019/9/e12604/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.LeBeau K, Huey LG, Hart M. Assessing the quality of mobile apps used by occupational therapists: evaluation using the user version of the mobile application rating scale. JMIR Mhealth Uhealth. 2019 May 01;7(5):e13019. doi: 10.2196/13019. https://mhealth.jmir.org/2019/5/e13019/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Woods LS, Duff J, Roehrer E, Walker K, Cummings E. Patients' experiences of using a consumer mHealth app for self-management of heart failure: mixed-methods study. JMIR Hum Factors. 2019 May 02;6(2):e13009. doi: 10.2196/13009. https://humanfactors.jmir.org/2019/2/e13009/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Messner E, Terhorst Y, Barke A, Baumeister H, Stoyanov S, Hides L, Kavanagh D, Pryss R, Sander L, Probst T. The German version of the Mobile App Rating Scale (MARS-G): development and validation study. JMIR Mhealth Uhealth. 2020 Mar 27;8(3):e14479. doi: 10.2196/14479. https://mhealth.jmir.org/2020/3/e14479/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Volkova E, Li N, Dunford E, Eyles H, Crino M, Michie J, Ni Mhurchu C. 'Smart' RCTs: development of a smartphone app for fully automated nutrition-labeling intervention trials. JMIR Mhealth Uhealth. 2016 Mar 17;4(1):e23. doi: 10.2196/mhealth.5219. https://mhealth.jmir.org/2016/1/e23/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Underwood B, Birdsall J, Kay E. The use of a mobile app to motivate evidence-based oral hygiene behaviour. Br Dent J. 2015 Aug 28;219(4):E2. doi: 10.1038/sj.bdj.2015.660. [DOI] [PubMed] [Google Scholar]
- 49.Guidance for health app developers, commissioners and assessors. United Kingdom National Health Service. 2019. Aug 13, [2019-10-14]. https://digital.nhs.uk/services/nhs-apps-library/guidance-for-health-app-developers-commissioners-and-assessors.
- 50.British Dental Journal Brush DJ app dentist wins funding boost. Br Dent J. 2019 Mar 22;226(6):387–387. doi: 10.1038/s41415-019-0186-x. https://www.nature.com/articles/s41415-019-0186-x#citeas. [DOI] [Google Scholar]
- 51.Becker S, Miron-Shatz T, Schumacher N, Krocza J, Diamantidis C, Albrecht U. mHealth 2.0: experiences, possibilities, and perspectives. JMIR Mhealth Uhealth. 2014 May 16;2(2):e24. doi: 10.2196/mhealth.3328. https://mhealth.jmir.org/2014/2/e24/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Tinanoff N, Baez RJ, Diaz Guillory C, Donly KJ, Feldens CA, McGrath C, Phantumvanit P, Pitts NB, Seow WK, Sharkov N, Songpaisan Y, Twetman S. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int J Paediatr Dent. 2019 May;29(3):238–248. doi: 10.1111/ipd.12484. [DOI] [PubMed] [Google Scholar]
- 53.Scheerman JF, van Empelen P, van Loveren C, van Meijel B. A mobile app (WhiteTeeth) to promote good oral health behavior among Dutch adolescents with fixed orthodontic appliances: intervention mapping approach. JMIR Mhealth Uhealth. 2018 Aug 17;6(8):e163. doi: 10.2196/mhealth.9626. https://mhealth.jmir.org/2018/8/e163/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Mummah SA, Robinson TN, King AC, Gardner CD, Sutton S. IDEAS (Integrate, Design, Assess, and Share): a framework and toolkit of strategies for the development of more effective digital interventions to change health behavior. J Med Internet Res. 2016 Dec 16;18(12):e317. doi: 10.2196/jmir.5927. https://www.jmir.org/2016/12/e317/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Health and wellbeing apps. Australian Government Health Department. 2019. [2019-10-17]. https://www.healthdirect.gov.au/health-and-wellbeing-apps.
- 56.Greenhalgh T, Hinton L, Finlay T, Macfarlane A, Fahy N, Clyde B, Chant A. Frameworks for supporting patient and public involvement in research: systematic review and co-design pilot. Health Expect. 2019 Aug;22(4):785–801. doi: 10.1111/hex.12888. http://europepmc.org/abstract/MED/31012259. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Mobile App Rating Scale tool developed by Queensland University of Technology (QUT).
General characteristics of all apps.
Comparative analysis of quality features present in all apps.
Quality evaluation of all apps according to the objective subscales of the Mobile App Rating Scale (MARS) quality appraisal tool.
Mean number of features present in high-quality versus low-quality apps within dental caries prevention factors.