

Abstract
Hypertension is a major risk factor for cardiovascular disease, but previous studies have mostly been limited to a single exam, a single cohort, a short follow-up period, or a limited number of outcomes. This study aimed to assess the association of 10-year cumulative systolic blood pressure in middle age with long-term risk of any cardiovascular disease, coronary heart disease, stroke, heart failure, all-cause mortality, and healthy longevity.
Individuals (11,502) from 5 racially/ethnically diverse US community-based cohorts were included in this study once they met all the inclusion criteria: ≥10yr of observation in the included cohort, aged 45-60yr, free of cardiovascular disease, and had ≥3 visits with blood pressure exams over the preceding 10yr. For each participant, systolic blood pressure level was predicted for each year of the 10yr prior inclusion, based on the available exams (Median of 4.0, spread over 9.1(range:7.2-10) years).
Lower 10-year cumulative systolic blood pressure was associated with 4.1yr longer survival and 5.4yr later onset of cardiovascular disease, resulting in living longer life with a shorter period with morbidity. Models adjusted for sociodemographic characteristics, cardiovascular risk factors, and index systolic blood pressure demonstrated associations of 10-year cumulative systolic blood pressure (per 130 mmHg×yr change, the threshold for stage-1 hypertension) with cardiovascular disease (HR:1.28, 95%CI:1.20-1.36), coronary heart disease (HR:1.29, 95%CI:1.19-1.40), stroke (HR:1.33, 95%CI:1.20-1.47), heart failure (HR:1.12, 95%CI: 1.02-1.23), and all-cause mortality (HR:1.21, 95%CI:1.14-1.29).
These findings emphasize the importance of 10-year cumulative systolic blood pressure as a risk factor to cardiovascular disease, above and beyond current systolic blood pressure.
Keywords: blood pressure, cardiovascular disease, hypertension, longevity, mortality
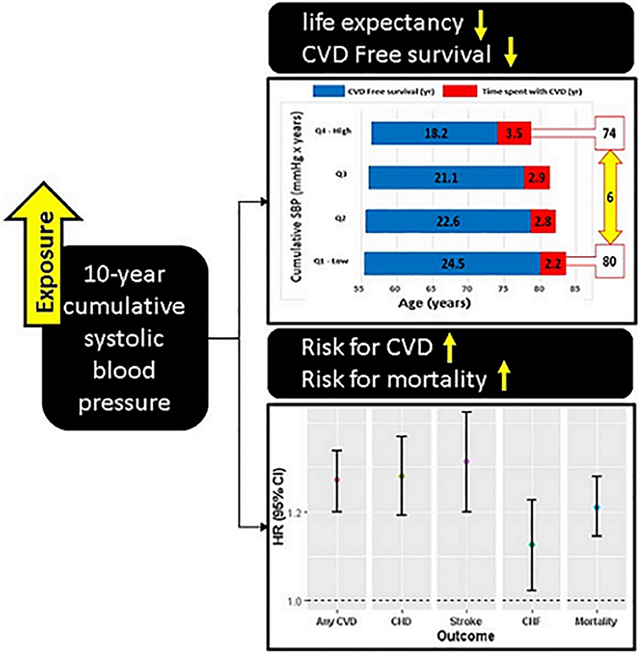
Graphical Abstract
Background
High blood pressure (BP) is a known risk factor for cardiovascular disease (CVD), with substantial population-attributable risk among White (21%)1 and Black (~35%)1, 2 adults. Many prior studies have predominantly focused on single measurements of BP measured at a single time point3 which may not adequately represent an individual’s long-term BP exposure. Some studies have assessed the association of BP level with CVD by using long-term BP features, such as average of subsequent measurements4-6 or change in BP status over time7. Those features, however, while not ignoring historical BP measurements, do not take into account the exposure time of each BP level and the risk that those features may convey. The previous studies that have examined longitudinal BP as a cumulative exposure, a measure which incorporates both BP level and exposure time, have been mostly limited to a single cohort or single electronic health record dataset4-6, 8 or had a only short follow-up period with insufficient time to develop CVD.9
Previous studies have demonstrated greater overall longevity among individuals with favorable BP.10, 11 However, the impact of BP on proportion of life lived free of disease, or healthspan, has been less well studied. An extended healthy life period represents an important goal as greater time spent with disease poses a tremendous burden on both individuals and the health system, with poor quality of life and greater expense. The association of cumulative exposure of systolic BP (SBP) with compression of CVD morbidity, that is, living longer and healthy life expectancy with a shorter period with morbidity, has not previously been examined.
This study aimed to assess the association of cumulative SBP in middle age with long-term risk of CVD and with healthy longevity, using individual-level pooled data from 5 racially and ethnically diverse US community-based CVD cohorts with an average of about 30 years of follow-up.
Methods
The data and materials that support the findings of this study can be requested from the corresponding authors and the National Heart, Lung, and Blood Institute BioLINCC.
Source and study population
The current study was based on the Lifetime Risk Pooling Project (LRPP), which has been previously described in detail 12. Briefly, data from 20 US community-based epidemiological cohort studies were pooled to form one individual-level dataset. All cohorts that had at least 1 baseline direct measurement of physiological or anthropometric variables at the baseline examination and ≥5 years of follow-up for any CVD outcome were included in the LRPP. LRPP cohorts that had standardized and repeated measurements of BP levels as well as all the individual CV diseases of interest were included in the present study. These cohorts include the Framingham Heart Study (FHS), Framingham Offspring Study (FOS), Coronary Artery Risk Development in Young Adults (CARDIA) study, Atherosclerosis Risk in Communities (ARIC) Study, and the Multi-Ethnic Study of Atherosclerosis (MESA) study. Individuals were included in the present study based on the following inclusion criteria and data requirements: aged 45-60 years, no history of CVD, ≥10 years of observation in the included cohort, and ≥3 visits with SBP exams over the preceding 10 years. Index-date was defined as the earliest exam that all these inclusion criteria are met.
Exposure variables
For all cohorts included, sitting SBP was defined for each visit as the mean of 2 or 3 manual mercury sphygmomanometer measurements taken by qualified personnel.
The main exposure variable, i.e. cumulative 10-year SBP (Cum10ySBP), was defined for the 10 years before the index date (Exposure period, years 1-10) based on the predicted SBP level in each year (Figure 1). Specifically, by using a nonparametric quadratic spline-based mixed-effects model, we estimated the subject-specific SBP trajectories throughout the exposure period (years 1-10) for all participants. The area under the curve over 10 years was calculated as an overall cumulative exposure Cum10ySBP and expressed in mmHg x years. This unit integrates the SBP level with the exposure duration into one cumulative value, so for example, the Cum10ySBP of individual who maintained 120 mmHg over the 10 years prior index date was calculated as 1200 mmHg x years. This method was selected due to its ability to tailor a nonlinear SBP curve over the exposure period13. Cumulative SBP was also defined for the early exposure period, that is, years 1 to 5 (CumSBP1-5y) and for the proximal exposure period, i.e. years 6 to 10 (CumSBP6-10y) and as a categorical variable based on quartiles (Figure 1).
Figure 1: Study Design and Definition of the Exposure Variables.

This figure depicts the study periods and the definition of the variables across the study timeline
Outcomes assessment
Incidence of any CVD (yes/no), coronary heart disease (CHD), stroke, congestive heart failure (CHF), all-cause mortality, and years of healthy longevity during the follow-up period were defined as the study outcomes. CVD diagnosis was defined as CHD death or non-fatal myocardial infarction, fatal or non-fatal stroke, CHF, or cardiovascular death. Diagnoses ascertainment were made by trained physician-adjudicators and have been used extensively in each of the cohorts7, 12. All outcomes were ascertained from index date until the end of observation in the included cohorts, with nearly-complete ascertainment of vital status in each of the cohorts12, 14-17.
Statistical analysis
Participants were categorized into four groups by their cohort-specific Cum10ySBP quartile ranking. Baseline characteristic were compared by Cum10ySBP quartiles status using generalized linear models for continuous variables and chi-square tests for categorical variables, as appropriate. The mean survival time or years lived free from CVD, with CVD, and overall were estimated using Irwin’s restricted mean by Cum10ySBP quartiles category18. Healthy longevity was evaluated based on overall survival; absolute CVD free survival, that is, the number of years between index age and the occurrence of first CVD event; absolute time spent with CVD, that is, the number of years and the proportion between occurrence of first CVD event and death or end of study; and the proportions of life lived free of CVD and spent with CVD.
To assess the association of cumulative SBP and any CVD, CHD, stroke, and CHF, Fine and Gray subdistribution hazard competing risk models were applied which account for the effect of competing risks of death19. Cox proportional hazards method was used for the association of cumulative SBP with all-cause mortality. Continuous Cum10ySBP scaled per 130mmHg x years units (the threshold for stage 1 hypertension)20 and categorical cum10ySBP quartile were fitted in the model respectively, and the models were set as unadjusted and adjusted with age, sex, race, education, body mass index (BMI), smoking status, diabetes, total cholesterol level, and use of hypertensive medications. To evaluate the effect associated with cumulative BP above and beyond index SBP level (i.e. the level at index date), multivariate models, with and without index SBP, were used. To assess whether there are critical periods of exposure, that is, the effect associated with cumulative BP varies between early exposure and exposure levels more proximal to the end of follow-up, as well as whether early cumulative SBP associated with CVD and mortality even after several years, a model that includes two main exposure variables, one for the early exposure period (CumSBP1-5y) and the other for the proximal exposure period (CumSBP6-10y), was applied. Models for the association of Cum10ySBP with any CVD were also implemented separately for race-sex subgroups and for age subgroups (45-55, >55), as well as after excluding individuals who reported taking antihypertensive medications any time prior index date.
Variance Inflation Factors (VIFs) were calculated to test for multicollinearity between the independent variables. All analyses were performed using SAS version 9.4 and R version 3.6.1. A two-sided P value <0.05 denoted statistical significance.
Results
Of 38,054 individuals in FHS, FOS, CARDIA, ARIC, and MESA studies, 12,925 (34%) individuals were excluded from the study due to inappropriate age or history of CVD (Figure 2). An additional 13,627, who did not meet the data requirement of ≥10yr of observation in the included cohort with ≥3 visits with SBP exam over the 10 years before index date, were also excluded from the analysis. Non-fulfillment of the data requirement was mainly due to an inappropriate data structure (11,073 81.3%), that is, lack of ≥3 study visits due to study design, rather than the failure to reach the SBP measurements due to individual participant loss to follow-up. These 13,627 individuals were more likely to be Blacks and smokers and had lower level of education than those included in the study (table S1). The total study population included 11,502 individuals, aged 45 to 60 years, with no history of CVD, and with ≥3 visits with SBP exam over the 10 years prior to the index date (Figure 2). Main characteristics of the study cohort are summarized in Table 1. A median of 4.0 visits with BP measurements (ranged from 3 to 6 visits) were available for each individual during the 10 years pre-index date. Theses available exams were spread over a median of 9.1 years (range: 7.2-10 years). The mean (SD) of the Cum10ySBP, calculated as the area under the 10-years SBP curve, was 1212 (154) mmHg x years, reflecting an average annual exposure of 121.2 mmHg per year. During a median of 12.9 years of follow-up, 1958 (17.0%), 1058 (9.2%), 697 (6.1%), 759 (6.6%), and 2624 (22.8%) participants had incident CVD, CHD, stroke, CHF, or all-cause mortality, respectively. Absolute rate per 1000 person-years was higher for all outcomes with higher Cum10ySBP level.
Figure 2: Selection of Study Population.

This flow chart shows the establishment of the study cohort according to the study inclusion and exclusion criterion
* 11,073 (81.3%) failed to fulfill the data requirement due to an inappropriate data structure.
Table 1:
Characteristics of the study cohort
| Baseline characteristics | Total (N=11,502) |
Quartile 1 (n=2,874) |
Quartile 2 (n=2,876) |
Quartile 3 (n=2,878) |
Quartile 4 (n=2,874) |
|---|---|---|---|---|---|
| Age, Mean (SD), y* | 55.9 (3.8) | 55.5 (3.8) | 55.8 (3.9) | 56.1 (3.6) | 56.4 (3.6) |
| Sex, n (%)* | |||||
| Women | 6422 (55.8) | 1970 (68.5) | 1547 (53.8) | 1397 (48.5) | 1508 (52.5) |
| Men | 5080 (44.2) | 904 (31.5) | 1329 (46.2) | 1481 (51.5) | 1366 (47.5) |
| Race, n (%)* | |||||
| White | 9285 (80.7) | 2569 (89.4) | 2422 (84.2) | 2248 (78.1) | 2046 (71.2) |
| Black | 2217 (19.3) | 305 (10.6) | 454 (15.8) | 630 (21.9) | 828 (28.8) |
| SBP, mean (SD), mm Hg* | 124.8 (18.6) | 108.4 (10.6) | 119.6 (10.8) | 128.4 (12.9) | 142.8 (17.8) |
| DBP, mean (SD), mm Hg* | 75.6 (11.0) | 67.5 (8.2) | 73.7 (8.3) | 77.9 (9.2) | 83.3 (11.4) |
| BMI, mean (SD)*† | 28.5 (5.8) | 26.3 (5.1) | 28.2 (5.4) | 29.2 (5.7) | 30.3 (6.4) |
| Total cholesterol, mean (SD), mg/dL‡ | 207.4 (42.5) | 205.9 (40.3) | 207.9 (43.2) | 206.6 (42.4) | 209.3 (43.8) |
| HDL cholesterol, mean (SD), mg/dL*§ | 53.7 (17.5) | 57.7 (18.0) | 53.4 (16.7) | 52.0 (17.6) | 51.6 (17.2) |
| Diabetes, n (%)* | 1156 (10.1) | 122 (4.2) | 213 (7.4) | 336 (11.7) | 485 (16.9) |
| Education, n (%)* | |||||
| Less than grade 12 | 1483 (12.9) | 300 (10.4) | 369 (12.9) | 380 (13.2) | 434 (15.1) |
| High School | 3236 (28.1) | 739 (25.7) | 793 (27.6) | 818 (28.4) | 886 (30.8) |
| College | 6783 (59.0) | 1835 (63.9) | 1714 (59.6) | 1680 (58.4) | 1554 (54.1) |
| Current smoker, n (%) | 2480 (21.6) | 668 (23.3) | 593 (20.6) | 595 (20.7) | 624 (21.7) |
| Antihypertensive medication, n (%)*∥ | 3005 (26.5) | 194 (6.8) | 460 (16.2) | 826 (29.0) | 1525 (53.8) |
| Cum10ySBP, mean (SD), mmHg x years*¶ | 1212 (154) | 1049 (69) | 1156 (59) | 1244 (67) | 1399 (126) |
| CumSBP1-5y, mean (SD), mmHg x years*# | 598 (78) | 518 (36) | 570 (32) | 614 (37) | 691 (67) |
| CumSBP6-10y, mean (SD), mmHg x years*,** | 614 (79) | 531 (36) | 586 (32) | 630 (37) | 708 (67) |
| Outcomes | |||||
| Any CVD | |||||
| Total, n (%)* | 1958 (17.0) | 312 (10.9) | 424 (14.7) | 514 (17.9) | 708 (24.6) |
| Events/1000 person-years | 15.5 | 9.4 | 13.1 | 16.5 | 24.0 |
| CHD | |||||
| Total, n (%)* | 1058 (9.2) | 159 (5.5) | 225 (7.8) | 298 (10.4) | 376 (13.1) |
| Events/1000 person-years | 8.0 | 4.7 | 6.7 | 9.2 | 12.0 |
| Stroke | |||||
| Total, n (%)* | 697 (6.1) | 110 (3.8) | 151 (5.3) | 177 (6.2) | 259 (9.0) |
| Events/1000 person-years | 5.2 | 3.2 | 4.6 | 5.3 | 8.1 |
| CHF | |||||
| Total, n (%)* | 759 (6.6) | 103 (3.6) | 163 (5.7) | 187 (6.5) | 306 (10.7) |
| Events/1000 person-years | 5.6 | 3.0 | 4.8 | 5.6 | 9.5 |
| All-cause mortality* | |||||
| Total, n (%) | 2624 (22.8) | 570 (19.8) | 619 (21.5) | 656 (22.8) | 779 (27.1) |
| Events/1000 person-years | 19.1 | 16.2 | 17.8 | 19.1 | 23.3 |
Abbreviations: BMI, body mass index; CHD, coronary heart disease; CHF, congestive heart failure; Cum10ySBP, cumulative systolic blood pressure for the exposure period, years 1-10; CumSBP1-5y, cumulative systolic blood pressure for the early exposure period, years 1-5; CumSBP6-10y, cumulative systolic blood pressure for the proximal exposure period, years 6-10; CVD, cardiovascular disease; DBP, Diastolic blood pressure; HDL, High-density lipoprotein; and SBP, Systolic blood pressure.
Significant value of <.01
BMI was calculated as weight in kilograms divided by height in meters squared
Significant value of <.05
Data on HDL cholesterol were missing for 808 individuals
Data on antihypertensive medication use were missing for 143 individuals
Cum10ySBP was calculated as the area under the SBP curve over the exposure period (mmHg x years)
CumSBP1-5y was calculated as the area under the SBP curve over the early exposure period (mmHg x years)
CumSBP6-10y was calculated as the area under the SBP curve over the proximal exposure period (mmHg x years)
As illustrated in Figure 3, higher Cum10ySBP was associated with shorter overall survival in which participants died an average of 4.1 years earlier and also had an earlier onset of CVD by 5.4 years (yr). This means that in addition to a longer overall lifespan, the proportion of life lived free of disease was higher among those with lower Cum10ySBP resulting in compression of CVD morbidity and extension of CVD-free survival. Specifically, life expectancy was 82.2yr, 81.2yr, 80.1yr, and 78.1yr for quartiles 1, 2, 3, and 4 of Cum10ySBP, respectively. Individuals with the lowest Cum10ySBP (quartile 1) at index date lived, on average, an additional 24.5 years after the index age free of CVD and spent 2.2 yr (2.7%) on average with CVD. With higher Cum10ySBP, the CVD-free survival after index date was lower (22.6 yr, 21.1 yr, and 18.2 yr, P value for trend <0.001), and the absolute time (2.8, 2.9, and 3.5 years for quartile 2, 3, and 4, respectively) and relative proportion of time (3.4%, 3.6%, and 4.5% for quartile 2, 3, and 4, respectively) spent with CVD after the index date was higher. When stratified by sex and race, the shorter average healthspan and longer average time spent with CVD remained consistent (figure S1).
Figure 3: Overall Survival, CVD Free Survival and Time Spent With CVD After Index Date*,†.
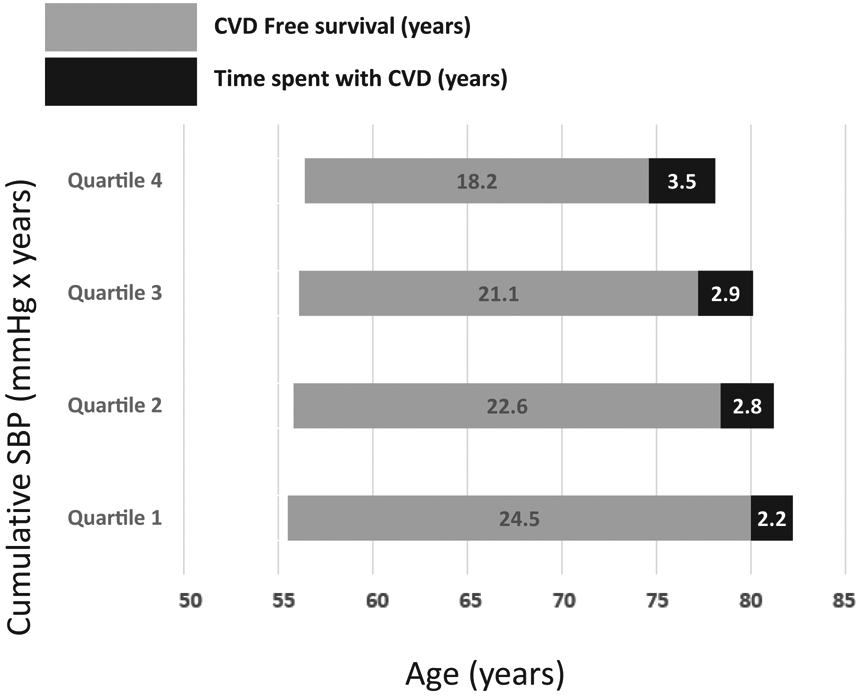
This flow chart shows the overall survival, CVD Free survival and time spent with CVD after the index date according to 10 years cumulative systolic blood pressure quartiles.
* Average age (years) at index date was 55.5yr, 55.8yr, 56.1yr, and 56.4yr for quartile 1, quartile 2, quartile 3, and quartile 4, respectively.
† Mean life expectancy was 82.2yr, 81.2yr, 80.1yr, and 78.1yr for quartile 1, quartile 2, quartile 3, and quartile 4, respectively.
Table 2 shows the association of cumulative SBP measured on a continuous scale with long-term risk of CVD. Unadjusted hazards models demonstrated significant associations between Cum10ySBP and incidence of CVD, CHD, stroke, CHF, and all-cause mortality, with higher risk as the cumulative SBP increased. These associations remained even after adjustment for age, sex, race, education, BMI, smoking status, diabetes, total cholesterol level, and use of hypertensive medications as well as when index SBP was included into the models.
Table 2:
Association of cumulative systolic blood pressure level (continuous scale) with hazards of cardiovascular disease (per 130 mm Hg x year)*
| Hazards of cardiovascular disease | Model A | Model B† | Model C‡ |
|---|---|---|---|
| Unadjusted | Adjusted, not including index SBP |
Adjusted, Including index SBP | |
| Hazard ratio (95% CI) for Any CVD§,∥,¶ | |||
| Cum10ySBP | 1.43 (1.38-1.48) | 1.35 (1.30-1.40) | 1.28 (1.20-1.36) |
| CumSBP1-5y | 1.37 (1.15-1.63) | 1.29 (1.08-1.55) | 1.37 (1.14-1.66) |
| CumSBP6-10y | 1.50 (1.26-1.78) | 1.41 (1.18-1.68) | 1.16 (0.91-1.48) |
| Hazard ratio (95% CI) for CHD§,∥,# | |||
| Cum10ySBP | 1.41 (1.36-1.47) | 1.35 (1.28-1.42) | 1.29 (1.19-1.40) |
| CumSBP1-5y | 1.42 (1.13-1.77) | 1.45 (1.15-1.82) | 1.54 (1.20-1.96) |
| CumSBP6-10y | 1.41 (1.13-1.77) | 1.26 (1.00-1.59) | 1.02 (0.74-1.42) |
| Hazard ratio (95% CI) for Stroke§,∥,** | |||
| Cum10ySBP | 1.42 (1.34-1.49) | 1.39 (1.31-1.47) | 1.33 (1.20-1.47) |
| CumSBP1-5y | 1.24 (0.99-1.65) | 1.24 (0.93-1.67) | 1.28 (0.95-1.73) |
| CumSBP6-10y | 1.62 (1.22-2.2) | 1.54 (1.16-2.05) | 1.41 (0.97-2.04) |
| Hazard ratio (95% CI) for CHF§,∥,‡‡ | |||
| Cum10ySBP | 1.38 (1.31-1.44) | 1.23 (1.16-1.30) | 1.12 (1.02-1.23) |
| CumSBP1-5y | 1.06 (0.82-1.38) | 0.92 (0.70-1.20) | 0.98 (0.74-1.29) |
| CumSBP6-10y | 1.79 (1.37-2.33) | 1.63 (1.25-2.11) | 1.34 (0.94-1.92) |
| Hazard ratio (95% CI) for all-cause mortality‡‡,∥,§§ | |||
| Cum10ySBP | 1.29 (1.25-1.34) | 1.25 (1.20-1.30) | 1.21 (1.14-1.29) |
| CumSBP1-5y | 1.24 (1.07-1.45) | 1.22 (1.04-1.44) | 1.25 (1.06-1.48) |
| CumSBP6-10y | 1.34 (1.15-1.56) | 1.27 (1.09-1.48) | 1.16 (0.95-1.42) |
Abbreviations: SBP, Systolic blood pressure; CVD, cardiovascular disease; CHD, coronary heart disease; CHF, congestive heart failure; Cum10ySBP, cumulative systolic blood pressure for the exposure period, years 1-10; CumSBP1-5y, cumulative systolic blood pressure for the early exposure period, years 1-5; CumSBP6-10y, cumulative systolic blood pressure for the proximal exposure period, years 6-10
All HR presented are per 130 mmHg x yr change
Model adjusted for age, sex, race, education, BMI, smoking status, diabetes, total cholesterol level, and use of hypertensive medications
Model adjusted for age, sex, race, education, BMI, smoking status, diabetes, total cholesterol level, use of hypertensive medications, and index SBP
Fine & Gray’s subdistribution method was used to account for competing risk
CumSBP1-5y and CumSBP6-10y were included simultaneously in same model. No multicollinearity between these two variables was observed (VIFs: <6.8)
n (%) of any CVD events: 1958 (17.0)
n (%) of CHD events = 1058 (9.2%)
n (%) of stroke events = 697 (6.1%)
n (%) of CHF events = 759 (6.6%)
Cox proportional hazards method was used for the association of cumulative BP with all-cause mortality
n (%) of all-cause mortality events = 2624 (22.8%)
Figure 4 shows significant association of Cum10ySBP quartiles with CVD incidence, with higher risk as the cumulative SBP increased [Cum10ySBP: HRquartile2: 1.32 (1.14-1.53), HRquartile3: 1.63 (1.41-1.88), and HRquartile4: 2.32 (1.93-2.58)] (Figure 2a Model B). This association remained even when index SBP was also incorporated into the model [Cum10ySBP: HRquartile2: 1.14 (0.97-1.32), HRquartile3: 1.21 (1.03-1.42), and HRquartile4: 1.33 (1.10-1.61)] (Figure 4 Model C). The greater risk associated with higher cumulative SBP quartiles was also observed when evaluating separately for CHD and CHF (Figures 4b and 4d, respectively).
Figure 4: The Association of 10 Years Cumulative Systolic Blood Pressure Quartiles with Cardiovascular Disease and All-Cause Mortality*,†,‡.
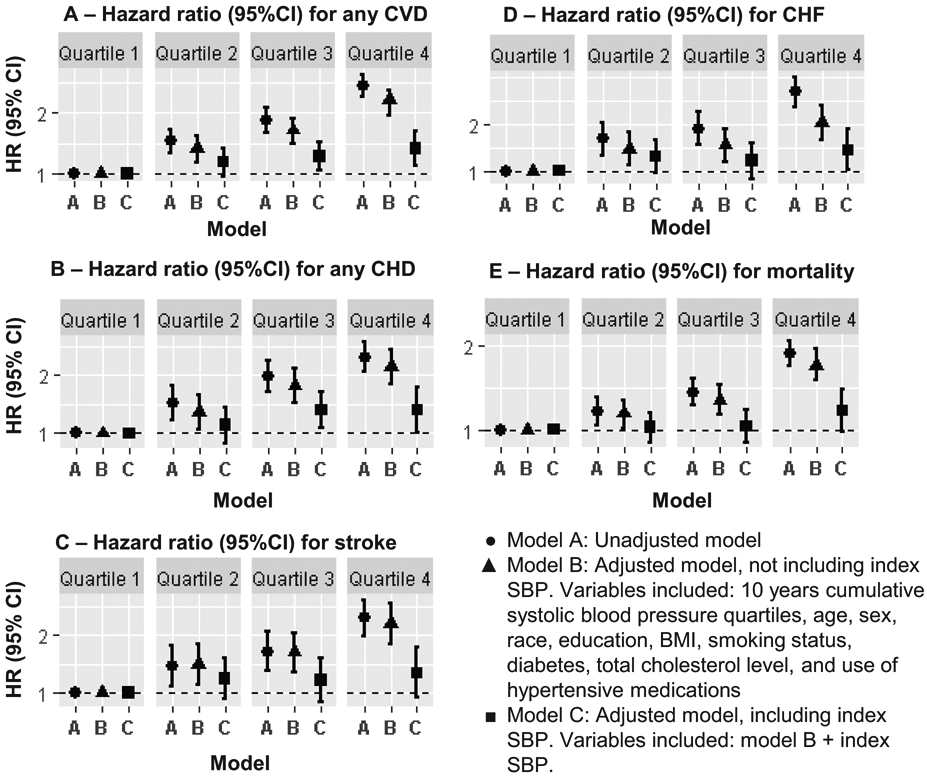
Five forest plots show adjusted HRs for any cardiovascular disease, coronary heart disease, stroke, congestive heart failure, and all-cause mortality
* Participants were categorized into four groups by their cohort-specific Cum10ySBP quartile ranking. The median Cum10ySBP level of quartile 1, quartile2, quartile 3, and quartile 4 was 990, 1103, 1197, and 1308 for MESA study; 1026, 1118, 1204, and 1328 for ARIC study; 1036, 1119, 1293, and 1305 for CARDIA study; 1081, 1182, 1269, and 1392 for FOS; and 1152, 1261, 1361, and 1525 for FHS, respectively.
† For all models, quartile 1 (i.e. the quartile with the median Cum10ySBP in the normal range) was defined as the reference group.
‡ For CVD outcomes (Figures A to D), Fine & Gray's subdistribution method was used to account for the effects of competing risks of death. Cox proportional hazards method was used for the association of Cum10ySBP with all-cause mortality (Figure E).
The association of cumulative SBP measured on a continuous scale with long-term risk of CVD remained after excluding 3005 (26.5%) individuals who reported taking antihypertensive medications any time prior index date, as well as when models were applied separately for age and race-sex subgroups (table S2). Introduction the interaction term of age group by Cum10ySBP was statistically significant for the adjusted models, with and without the index SBP, with greater association of Cum10ySBP with any CVD among younger (45-55) than older (>55) participants. Multiplicative interaction term of race-sex group by Cum10ySBP was not statistically significant.
To assess whether there are critical periods of exposure, cumulative SBP exposure was split into early (CumSBP1-5y) and proximal (CumSBP6-10y) exposure windows (Table 2). Adjusted models, not including SBP measured at index date, demonstrated significant associations of CumSBP6-10y (i.e. proximal exposure) with any CVD (HR, 1.41 [95%CI, 1.18-1.68]), CHD (HR, 1.26 [95%CI, 1.00-1.59]), stroke H(R, 1.54 [95%CI, 1.16-2.05]), CHF (HR, 1.63 [95%CI, 1.25-2.11], and mortality HR, 1.27 [95%CI, 1.09-1.48]. However, when index SBP was also included in the model, those associations were disappeared. As for CumSBP1-5y, early cumulative SBP was associated with any CVD, CHD, and mortality with adjustment for baseline characteristics except SBP (any CVD HR, 1.29 [95%CI, 1.08-1.55]; CHD HR, 1.45 [95%CI, 1.15-1.82]; and mortality HR, 1.22 [95%CI, 1.04-1.44]). These associations were all preserved when index SBP was also included in the model (any CVD HR, 1.37 [95%CI, 1.14-1.66]; CHD HR, 1.54 [95%CI, 1.20-1.96]; and mortality HR, 1.25 [95%CI, 1.06-1.48]).
All the models described above met the proportional hazards assumption.
Discussion
In this study, individuals in middle age from 5 US community-based CVD cohorts, who were exposed to lower levels of cumulative SBP over 10 years, had a lower risk for CVD and death throughout follow-up. Ten years cumulative SBP remained associated with CVD incidence even after adjustment for index SBP, as well as when stratified the population by age and race-sex categories. In addition, lower levels of cumulative SBP over 10 years was associated with extended overall survival and later onset of CVD, resulting in a longer and healthier lifespan. A special report from the American Heart Association and American College of Cardiology recognized that the majority of the heart attacks and strokes among adults occur due to cumulative exposure to preventable causal risk factors 21, 22. Our findings confirm that cumulative exposure to high SBP is a major risk factor for CVD.
Previous studies have demonstrated the importance of long-term exposure to SBP on incident CVD and mortality. These studies support the life course approach to CVD, suggesting that CVD disease onset is associated with life course risk factors in addition to risk factors measured at a single point of time23. Since SBP level raises with age for most individuals24, the association of long-term exposure of SBP throughout lifetime with CVD outcomes is particularly of interest. As early as 2002, Vasan et al.4 demonstrated the independent association of time-averaged recent and remote antecedent BP measures with CVD, above and beyond current BP. In 2012, Allen et al 7 showed impact of BP change in middle age on the remaining lifetime risk for CVD. Compared with those studies, the present study benefitted from assessing the cumulative SBP as the area under the SBP curve, and was able to capture the impact of the exposure time of each BP level in addition to the impact of the exposure level. A study by Wang at al. 9 demonstrated higher CVD and mortality risk associated with cumulative BP among the Chinese population. The main limitation of that study was the short follow-up period of only three years for cardiovascular and cerebrovascular events and four years for all-cause mortality. This study assessed longer long-term risk, which is more clinically meaningful than short-term estimates, especially for those with low short-term risk 25, 26.
The additional information regarding longevity and compression of morbidity provided a more complete overview on the contribution of low level of cumulative SBP to prevention of CVD. In a major study on younger employees in the Chicago area 27, favorable cardiovascular health extended the survival of the participants by almost 4 years and postponed the onset of cardiovascular morbidity by 7 years. Favorable cardiovascular health was defined as having favorable levels of BP, cholesterol, diabetes, smoking, and BMI. In the present study, we demonstrated that lower cumulative level of SBP alone was associated with later onset of any CVD by >5 years and longer survival by 4 years. These findings highlight hypertension as a core health factor associated with CVD.
The association of cumulative SBP with CVD outcomes and mortality above and beyond a single BP level at index date demonstrates that Individuals with similar contemporary SBP may be at different long-term risks for CVD due to differences in their cumulative exposure to SBP, and therefore cumulative SBP may be used to stratify individuals based on their risk for CVD.
The observed associations of early cumulative SBP during mid-life with later any CVD, CHD, and mortality also demonstrate the importance of the life course approach by suggesting that early adulthood may be a critical period in the accumulation of cardiovascular risk and that early cumulative SBP remembered by the body even after several years. These findings are consistent with a study by Zhang et al 28, which demonstrated association between cumulative exposure to high SBP during young adulthood and later life CVD risk, independent of later adult exposures. Our study was similar to that study with respect to the study population. Both studies pooled together US cohorts with information spanning the life course. While the primary outcomes of interest on Zhang et al study included incident CHD, heart failure, and stroke, our study incorporated any CVD, CHD, CHF, stroke, all-cause mortality, as well as healthy longevity. In addition, in Zhang et al’s study, many BP measures were imputed, especially for the early exposure (age 18 to 39 years) where in-person exams were lacking in most cohorts included. In this study, the inclusion of individuals with at least 3 visits with BP exam during the 10 years before the index date allowed us to rely on a median of 4.0 visits with actual BP for each individual to define the exposure variable. Our analysis also accounted for the effects of competing risks of death; a substantial analysis when a long-term risk is evaluated29, 30. The greater risk for CVD observed among younger (45-55) than older (>55) participants is also suggests that early middle age is a critical period for future CVD event. This finding is consistent with previous studies which demonstrated greater risk for CVD and mortality with young-onset Hypertension31, 32.
Strengths of the present study include a comprehensive sample which was comprised from 5 large diverse US cohorts with information spanning adulthood; long-term follow-up; assessment of any CVD, CHD, stroke, CHF, all-cause mortality, and healthy longevity in the same sample; and availability of longitudinal BP measurements which enabled us to define a longitudinal exposure to BP level over 10 years in the middle age and taking into account both the exposure level and the cumulative time under each level.
This study also has some limitations. The first limitation is the observational nature of the study and the limited ability to make causal inference. Second, while the study sample consisted of 11,502 individuals, 13,627 were excluded due to data requirements. Those individuals were more likely to be Blacks and smokers and had lower level of education than those included in the study, which may result in bias toward null. The relatively low representation of Blacks limited our ability to evaluate the compression of CVD morbidity among sex and race strata, as presented in figure S1, although a similar trend was found for the different subgroups. Third, although pooling five different cohort studies provided large-scale data as necessary to evaluate long-term risk, there was a potential for birth cohort effects. To consider cohort impact, we defined Cum10ySBP quartiles separately for each cohort.
Conclusions
Ten-year cumulative exposure to SBP is a risk factor to CVD and all-cause mortality, above and beyond current SBP. High level of 10-year cumulative exposure to SBP is associated with greater CVD risk. Individuals with similar contemporary SBP may be at different long-term risks for CVD due to differences in their cumulative exposure to SBP. Therefore, cumulative SBP may be used to stratify individuals based in their risk for CVD. In addition, lower level of 10-year cumulative exposure to SBP postpones the onset of CVD by 5.4 years, and extends the overall survival by 4.1 years (compared with almost 4 years extended survival associated with favorable cardiovascular health measured at one point of time).
Perspectives
BP is a known risk factor for CVD, but many prior studies have predominantly focused on BP measured at a single point of time and the cumulative exposure time for hypertension was not taken into account. By utilizing pooled data from 5 racially and ethnically diverse US community-based CVD cohorts (n=11502), we demonstrated greater risk for any CVD, CHD, stroke, CHF, and all-cause mortality, with greater 10-years cumulative exposure to SBP, above and beyond current BP. In addition, lower 10-years cumulative exposure to SBP extended the overall survival by 4.1 years and postponed the onset of CVD by 5.4 years.
The observed association of cumulative SBP with CVD outcomes and mortality above and beyond a single BP level at index date demonstrates that Individuals with similar contemporary SBP may be at different long-term risk for CVD due to differences in their cumulative exposure to SBP, and therefore cumulative SBP may be used to stratify individuals based in their risk for CVD.
Supplementary Material
Figure S1: Overall survival, CVD Free survival and time spent with CVD after index date stratified by sex and race
This flow chart shows the overall survival, CVD Free survival and time spent with CVD after the index date according to 10 years cumulative systolic blood pressure quartiles, stratified by sex and race
Novelty and Significance.
- What Is New?
- Lower levels of cumulative systolic blood pressure over 10 years is associated with lower ~13 years risk for cardiovascular disease and death and with extended overall survival and later onset of cardiovascular disease.
- What Is Relevant?
- Primordial prevention of blood pressure elevation is particularly important to reduce the cumulative burden of systolic blood pressure and ultimately prevent cardiovascular disease outcomes.
- Summary
- Lower 10 years cumulative systolic blood pressure level is associated with lower risk for cardiovascular disease and with significantly greater healthy longevity. The risk for any cardiovascular disease, coronary heart disease, stroke, congestive heart failure, and all-cause mortality increased with increases in cumulative systolic blood pressure, above and beyond current blood pressure level.
Acknowledgments
The authors thank the investigators, participants, and staff of the Framingham Heart Study (FHS), Framingham Offspring Study (FOS), Coronary Artery Risk Development in Young Adults (CARDIA) study, Atherosclerosis Risk in Communities (ARIC) Study, the Multi-Ethnic Study of Atherosclerosis (MESA) study, and the Lifetime Risk Pooling Project (LRPP). Dr. Orna Reges thanks the American Heart Association for the Children’s Strategically Focused Research Networks (SFRN) postdoctoral fellowship, and the Israel Scholarship Education Foundation for their support.
Sources of Funding
The Cardiovascular Lifetime Risk Pooling Project has been supported by the National Heart, Lung, and Blood Institute (grant R21HL085375).
Dr. Orna Reges as a postdoctoral fellow is bening supported by the American Heart Association for the Children’s Strategically Focused Research Networks (SFRN) (grant 17SFRN33700101).
Footnotes
Disclosure
All authors declare that they have no conflict of interest.
References
- 1.Cheng S, Claggett B, Correia AW, Shah AM, Gupta DK, Skali H, Ni H, Rosamond WD, Heiss G, Folsom AR, Coresh J, Solomon SD. Temporal trends in the population attributable risk for cardiovascular disease: The atherosclerosis risk in communities study. Circulation. 2014;130:820–828 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Clark D 3rd, Colantonio LD, Min YI, Hall ME, Zhao H, Mentz RJ, Shimbo D, Ogedegbe G, Howard G, Levitan EB, Jones DW, Correa A, Muntner P. Population-attributable risk for cardiovascular disease associated with hypertension in black adults. JAMA Cardiol. 2019:1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Au R, Kannel WB, Wolf PA. The lifetime risk of stroke: Estimates from the framingham study. Stroke. 2006;37:345–350 [DOI] [PubMed] [Google Scholar]
- 4.Vasan RS, Massaro JM, Wilson PW, Seshadri S, Wolf PA, Levy D, D'Agostino RB, Framingham Heart S. Antecedent blood pressure and risk of cardiovascular disease: The framingham heart study. Circulation. 2002;105:48–53 [DOI] [PubMed] [Google Scholar]
- 5.Lee DS, Massaro JM, Wang TJ, Kannel WB, Benjamin EJ, Kenchaiah S, Levy D, D'Agostino RB Sr., Vasan RS. Antecedent blood pressure, body mass index, and the risk of incident heart failure in later life. Hypertension. 2007;50:869–876 [DOI] [PubMed] [Google Scholar]
- 6.Bonifonte A, Ayer T, Veledar E, Clark A, Wilson PW. Antecedent blood pressure as a predictor of cardiovascular disease. J Am Soc Hypertens. 2015;9:690–696 e691 [DOI] [PubMed] [Google Scholar]
- 7.Allen N, Berry JD, Ning H, Van Horn L, Dyer A, Lloyd-Jones DM. Impact of blood pressure and blood pressure change during middle age on the remaining lifetime risk for cardiovascular disease: The cardiovascular lifetime risk pooling project. Circulation. 2012;125:37–44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ayala Solares JR, Canoy D, Raimondi FED, Zhu Y, Hassaine A, Salimi-Khorshidi G, Tran J, Copland E, Zottoli M, Pinho-Gomes AC, Nazarzadeh M, Rahimi K. Long-term exposure to elevated systolic blood pressure in predicting incident cardiovascular disease: Evidence from large-scale routine electronic health records. J Am Heart Assoc. 2019;8:e012129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang YX, Song L, Xing AJ, Gao M, Zhao HY, Li CH, Zhao HL, Chen SH, Lu CZ, Wu SL. Predictive value of cumulative blood pressure for all-cause mortality and cardiovascular events. Sci Rep. 2017;7:41969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vaduganathan M, Claggett BL, Juraschek SP, Solomon SD. Assessment of long-term benefit of intensive blood pressure control on residual life span: Secondary analysis of the systolic blood pressure intervention trial (sprint). JAMA Cardiol. 2020;5:576–581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stamler J, Stamler R, Neaton JD, Wentworth D, Daviglus ML, Garside D, Dyer AR, Liu K, Greenland P. Low risk-factor profile and long-term cardiovascular and noncardiovascular mortality and life expectancy: Findings for 5 large cohorts of young adult and middle-aged men and women. JAMA. 1999;282:2012–2018 [DOI] [PubMed] [Google Scholar]
- 12.Wilkins JT, Karmali KN, Huffman MD, Allen NB, Ning H, Berry JD, Garside DB, Dyer A, Lloyd-Jones DM. Data resource profile: The cardiovascular disease lifetime risk pooling project. Int J Epidemiol. 2015;44:1557–1564 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rice JA, Wu CO. Nonparametric mixed effects models for unequally sampled noisy curves. Biometrics. 2001;57:253–259 [DOI] [PubMed] [Google Scholar]
- 14.Zamani P, Jacobs DR Jr., Segers P, Duprez DA, Brumback L, Kronmal RA, Lilly SM, Townsend RR, Budoff M, Lima JA, Hannan P, Chirinos JA. Reflection magnitude as a predictor of mortality: The multi-ethnic study of atherosclerosis. Hypertension. 2014;64:958–964 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Windham BG, Griswold ME, Lirette S, Kucharska-Newton A, Foraker RE, Rosamond W, Coresh J, Kritchevsky S, Mosley TH Jr. Effects of age and functional status on the relationship of systolic blood pressure with mortality in mid and late life: The aric study. J Gerontol A Biol Sci Med Sci. 2017;72:89–94 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tsao CW, Lyass A, Enserro D, Larson MG, Ho JE, Kizer JR, Gottdiener JS, Psaty BM, Vasan RS. Temporal trends in the incidence of and mortality associated with heart failure with preserved and reduced ejection fraction. JACC Heart Fail. 2018;6:678–685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Elfassy T, Swift SL, Glymour MM, Calonico S, Jacobs DR Jr., Mayeda ER, Kershaw KN, Kiefe C, Zeki Al Hazzouri A. Associations of income volatility with incident cardiovascular disease and all-cause mortality in a us cohort. Circulation. 2019;139:850–859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Karrison TG. Use of irwin's restricted mean as an index for comparing survival in different treatment groups--interpretation and power considerations. Control Clin Trials. 1997;18:151–167 [DOI] [PubMed] [Google Scholar]
- 19.Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. Journal of the American Statistical Association. 1999;94:496–509 [Google Scholar]
- 20.Whelton PK, Carey RM. The 2017 american college of cardiology/american heart association clinical practice guideline for high blood pressure in adults. JAMA Cardiol. 2018;3:352–353 [DOI] [PubMed] [Google Scholar]
- 21.Lloyd-Jones DM, Huffman MD, Karmali KN, Sanghavi DM, Wright JS, Pelser C, Gulati M, Masoudi FA, Goff DC Jr. Estimating longitudinal risks and benefits from cardiovascular preventive therapies among medicare patients: The million hearts longitudinal ascvd risk assessment tool: A special report from the american heart association and american college of cardiology. Circulation. 2017;135:e793–e813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lloyd-Jones DM, Huffman MD, Karmali KN, Sanghavi DM, Wright JS, Pelser C, Gulati M, Masoudi FA, Goff DC Jr. Estimating longitudinal risks and benefits from cardiovascular preventive therapies among medicare patients: The million hearts longitudinal ascvd risk assessment tool: A special report from the american heart association and american college of cardiology. J Am Coll Cardiol. 2017;69:1617–1636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hardy R, Lawlor DA, Kuh D. A life course approach to cardiovascular aging. Future Cardiol. 2015;11:101–113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hardy ST, Holliday KM, Chakladar S, Engeda JC, Allen NB, Heiss G, Lloyd-Jones DM, Schreiner PJ, Shay CM, Lin D, Zeng D, Avery CL. Heterogeneity in blood pressure transitions over the life course: Age-specific emergence of racial/ethnic and sex disparities in the united states. JAMA Cardiol. 2017;2:653–661 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Elward KS, Simpson RJ Jr., Mendys P. Improving cardiovascular risk reduction for primary prevention--utility of lifetime risk assessment. Postgrad Med. 2010;122:192–199 [DOI] [PubMed] [Google Scholar]
- 26.Berger JS, Jordan CO, Lloyd-Jones D, Blumenthal RS. Screening for cardiovascular risk in asymptomatic patients. J Am Coll Cardiol. 2010;55:1169–1177 [DOI] [PubMed] [Google Scholar]
- 27.Allen NB, Zhao L, Liu L, Daviglus M, Liu K, Fries J, Shih YT, Garside D, Vu TH, Stamler J, Lloyd-Jones DM. Favorable cardiovascular health, compression of morbidity, and healthcare costs: Forty-year follow-up of the cha study (chicago heart association detection project in industry). Circulation. 2017;135:1693–1701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zhang Y, Vittinghoff E, Pletcher MJ, Allen NB, Zeki Al Hazzouri A, Yaffe K, Balte PP, Alonso A, Newman AB, Ives DG, Rana JS, Lloyd-Jones D, Vasan RS, Bibbins-Domingo K, Gooding HC, de Ferranti SD, Oelsner EC, Moran AE. Associations of blood pressure and cholesterol levels during young adulthood with later cardiovascular events. J Am Coll Cardiol. 2019;74:330–341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Feinstein M, Ning H, Kang J, Bertoni A, Carnethon M, Lloyd-Jones DM. Racial differences in risks for first cardiovascular events and noncardiovascular death: The atherosclerosis risk in communities study, the cardiovascular health study, and the multi-ethnic study of atherosclerosis. Circulation. 2012;126:50–59 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Huffman MD, Berry JD, Ning H, Dyer AR, Garside DB, Cai X, Daviglus ML, Lloyd-Jones DM. Lifetime risk for heart failure among white and black americans: Cardiovascular lifetime risk pooling project. J Am Coll Cardiol. 2013;61:1510–1517 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lloyd-Jones DM, Evans JC, Levy D. Hypertension in adults across the age spectrum: Current outcomes and control in the community. JAMA. 2005;294:466–472 [DOI] [PubMed] [Google Scholar]
- 32.Wang C, Yuan Y, Zheng M, Pan A, Wang M, Zhao M, Li Y, Yao S, Chen S, Wu S, Xue H. Association of age of onset of hypertension with cardiovascular diseases and mortality. J Am Coll Cardiol. 2020;75:2921–2930 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1: Overall survival, CVD Free survival and time spent with CVD after index date stratified by sex and race
This flow chart shows the overall survival, CVD Free survival and time spent with CVD after the index date according to 10 years cumulative systolic blood pressure quartiles, stratified by sex and race