

Abstract
Several aspects of mother-child relationships are associated with children’s internalizing problems. We examined longitudinal associations between mother-child conflict and children’s internalizing problems in middle childhood. Specifically, we examined whether conflict and children’s internalizing problems predict each other longitudinally in a sample of children from 3rd through 6th grade (N = 1,364) and their mothers using a cross-lagged panel model with random intercepts. In line with expectations, we found stable between-family differences in both mother-child conflict and children’s internalizing problems. Contrary to expectations, we did not find that mother-child conflict and children’s internalizing problems showed significant cross-lagged associations. However, mother-child conflict and children’s internalizing problems had correlated errors at each wave, indicating that these two constructs covary with each other concurrently at multiple times across development, independent of stable between-family associations (i.e., as one increases, so does the other, and vice versa). The results of this study point to the importance of using statistical approaches that can disentangle between-family differences from within-family processes. In future studies, shorter time scales (e.g., weeks or months) may better capture dynamic associations between parent-child conflict and internalizing problems.
Keywords: Parent-child conflict, internalizing problems, middle childhood
Internalizing problems, which include symptoms of depression and anxiety, are among the most prevalent mental health difficulties (Epkins & Heckler, 2011). Internalizing problems can emerge as young as early childhood, with the incidence increasing from childhood through adolescence (Brock & Kochanska, 2015; Cyranowski et al., 2000; Gilliom & Shaw, 2004; Hollenstein & Lougheed, 2013). Internalizing symptoms tend to present similarly in children and adolescents, and the same criteria are used to diagnose internalizing disorders in both developmental age ranges (McLellan & Hudson, 2017; Powell et al., 2017). Several family factors are associated with increased risk for youths’ internalizing problems, including family emotional climate, parental socialization of emotion, and relationship quality (Epkins & Heckler, 2011; Lougheed, 2020; Morris et al., 2018). Conflictual relationships between parents and children, specifically, may increase the risk for children’s internalizing problems because of their negative implications for children’s emotional development (Smith et al., 2019). It is important to understand how associations between these aspects of parental relationships and children’s internalizing problems unfold over time, for example, whether relationship characteristics and internalizing problems are mutually influential, or whether one tends to precede the other. The goal of this study is to disentangle the longitudinal associations between one aspect of parent-child relationships—parent-child conflict—and children’s internalizing problems during mid-childhood.
Multiple theoretical approaches such as developmental psychopathology (Cicchetti & Cohen, 2006), dynamic systems perspectives (Lougheed, 2020), and interpersonal theories (Epkins & Heckler, 2011; Joiner et al., 1999) point to the importance of parent-child relationships in the emergence and maintenance of internalizing problems. Common among these perspectives is the idea that interactions between parents and children shape children’s ability to manage emotions, which in turn (and in combination with other factors such as genetic propensity and event exposures) is associated with the likelihood that children develop internalizing problems. The developmental psychopathology perspective (Cicchetti & Cohen, 2006) is especially helpful when thinking about these complex developmental processes. This perspective emphasizes that gaining a complete understanding of psychopathology involves: research on both typical and atypical development; an emphasis on individual differences, given that similar developmental outcomes may be reached via different trajectories and that similar trajectories can lead to different outcomes; and disentangling complex associations between multiple levels of analysis (e.g., individual, social; Cicchetti & Cohen, 2006; Cicchetti & Rogosch, 1996). We draw on the developmental psychopathology approach to frame our examination of longitudinal, bidirectional associations between parent-child conflict and typically developing children’s internalizing problems, accounting for individual differences.
Associations between Parent-Child Conflict and Children’s Internalizing Problems
In middle childhood (approximately age 6 years until the onset of puberty, although specific definitions of this developmental period vary across research groups), the maturing capacity for self-regulation enables children to be less reliant on primary caregivers than they were in early childhood (Bosmans & Kerns, 2015). One implication of this maturation is that children may start to experience the early stages of autonomy development (Stuart Parrigon & Kerns, 2016). In day-to-day life, parent-child conflicts are an important context for children’s autonomy development, are a typical part of family life, and can be a feature of healthy relationships when family members assert their perspectives while working towards solutions (Laursen & Hafen, 2010). Parent-child conflict tends to peak in early adolescence (i.e., ages 10 to 13 years of age; Smetana, Campionne-Barr, & Metzger, 2006), and increases in conflict frequency and intensity may begin to manifest in middle childhood.
Conflicts in the context of supportive relationships that have a constructive outcome (e.g., greater mutual understanding; resolution of a problem) may be associated with beneficial outcomes for individuals such as improved relationship skills and ability to set boundaries (Laursen & Hafen, 2010). However, some patterns of parent-child conflicts are associated with relationship difficulties and children’s internalizing problems. For example, relationship quality may be relatively low in families where mother-child and father-child conflicts are frequent, intense, coercive, and unresolved (Laursen & Hafen, 2010; Sheeber et al., 2007). Such families with conflictual relationships may tend to have poor communication and problem-solving skills, which have been associated with youths’ internalizing problems (Sheeber et al., 2007). It is important to disentangle the direction of association between parent-child conflict and internalizing problems, and there are several hypotheses about the direction of effects. One hypothesis is that conflict contributes to children’s internalizing problems. Conflictual relationships may contribute to the risk for children’s internalizing problems, as a hostile family environment may trigger or exacerbate internalizing problems (Morris et al., 2007). A second hypothesis is that children’s internalizing problems contribute to greater conflict in the parent-child relationship. Internalizing problems can include irritability, which can lead to greater likelihood of conflictual interpersonal interactions (Joiner et al., 1999). A third hypothesis is a combination of the first two, and is that the effects between children’s internalizing problems and conflict are bidirectional (Lougheed, 2020)—increased child irritability associated with internalizing symptoms may increase the risk for parent-child conflict, and parent-child conflict in turn can reinforce children’s internalizing problems.
A number of studies have attempted to address the question of directional associations between parent-child conflict and children’s internalizing problems. Much of this research has focused on parent-adolescent relationships spanning youths’ ages from 11 to 17 years. Findings from research on parent-adolescent conflict are mixed and likely vary by the research method used. Some studies showed that mother-adolescent conflict (Allen et al., 2006) and parent-adolescent conflict (both mothers and fathers; Goodman et al., 2019; Samek et al., 2018) longitudinally predicts adolescents’ internalizing problems. Other studies have shown that adolescent internalizing problems and conflictual relationships with parents generally (Brière et al., 2013) and both mothers and fathers specifically (Lewis et al., 2014) predict each other longitudinally, although the link from internalizing problems to mother- and father-adolescent relationship difficulties may be stronger than the link from relationship difficulties to internalizing problems (Branje et al., 2010; Epkins & Heckler, 2011).
Family factors associated with increased risk for youths’ internalizing problems differ between childhood and adolescence (Collins & Laursen, 2004) and thus may show different associations with internalizing problems at different developmental stages. A few studies have examined the associations between parent-child conflict and internalizing problems in childhood. A longitudinal study of observed mother- and father-child relationship quality and children’s internalizing problems from age 4.5 to 10 years showed that negative aspects of the mother-child relationship (e.g., conflictual interactions) preceded increases in children’s internalizing problems (Brock & Kochanska, 2015). Yet another longitudinal study showed reciprocal associations between parent-reported warmth and harsh punishment (as reported by primarily biological mothers in the sample) and child-reported depressive symptoms from ages 7 years to 12 years, although the parent-child relationship was a stronger predictor of depressive symptoms than were depressive symptoms of the parent-child relationship (Hipwell et al., 2008). Evidence from another longitudinal study spanning 4th to 8th grade showed that child internalizing problems were associated with an increase in conflictual parent-child relationships, which in turn contributed to the stabilization of internalizing problems in adolescence (Yong et al., 2014). Taken together, the body of research spanning childhood and adolescence shows mixed evidence regarding the direction of associations between parent-child conflict and internalizing problems, although the evidence to date suggests that relationship issues predict internalizing problems more strongly than the other way around (see Epkins & Heckler, 2011 for review; Yong et al., 2014). In addition, the majority of work on this topic has been conducted on adolescent samples, which may not generalize to childhood samples given the confluence of biological, psychological, and social developments that are unique to adolescent development (Hollenstein & Lougheed, 2013).
Disentangling within- versus between-family associations.
Most of the studies on the longitudinal associations between parent-child relationship difficulties and children’s internalizing problems to date have used a cross-lagged panel model (CLPM). This analytic approach is an intuitive application of path modeling that involves simultaneously predicting two dependent variables (in this case conflict and internalizing problems) from the same variables at the previous time point. The analysis yields an auto-regressive effect for each variable (e.g., conflict at time t being predicted from conflict at time t-1) and a directional (cross-lagged) effect for each variable from the other variable at the previous time point (e.g., conflict at time t being predicted from internalizing problems at time t-1).
Recently, CLPMs have been criticized because cross-lagged effects are presumed and interpreted to index within-person (or in this case within-family) processes. However, these models can lead to grossly misspecified cross-lagged paths because the examination of within-family change processes requires accounting for the trait-like stability of a construct, and auto-regressive paths on their own do not adequately capture trait-like stability in a construct (Hamaker et al., 2015). Failure to adequately control for stable between-family differences can inflate cross-lagged and autoregressive paths and can even change the sign of the cross-lagged paths. Adding a random intercept to CLPMs corrects this bias by explicitly modeling stable between-family differences in each construct (conflict and youth internalizing) and the association of the two stable between-family factors in addition to the auto-regressive and cross-lagged paths. Thus, cross-lagged paths are interpreted as time-specific within-family associations in the random-intercept CLPM (RI-CLPM).
None of the research to date examining longitudinal associations between parent-child conflict and internalizing problems with CLPMs have used random intercepts. Therefore, existing literature on this topic (Branje et al., 2010; Brière et al., 2013; Goodman et al., 2019; Samek et al., 2018; Yong et al., 2014) may overestimate directional and/or transactional associations between conflict and internalizing problems. It is possible that these associations could be explained, at least in part, by between-family differences that persist over time rather than being within-family processes that unfold over time. It should be noted, however, that some studies to date have used other models to separate within- and between-family associations, such as multilevel models (e.g., Brock & Kochanska, 2015), generalized estimating equations (e.g., Hipwell et al., 2008), and some behavioral genetic designs (e.g., Lewis et al., 2014). Based on the findings from these studies, we may expect that cross-lagged associations from parent-child conflict to internalizing problems may be stronger than reciprocal associations, and that there will likely be a strong stable between-family correlation of the random intercepts (given that there is child-driven genetic covariation across these constructs; Lewis et al., 2014).
The role of gender.
Gender differences in internalizing problems are well established, with girls and women being more likely to experience them than boys and men (Cyranowski et al., 2000). This gender difference typically first emerges in adolescence and remains stable into adulthood (Holsen et al., 2000). Interpersonal perspectives suggest that gender differences in internalizing problems are related to gender differences in affiliative relationship patterns (e.g., girls’ greater need for close emotional communication, intimacy, and responsiveness; Cyranowski et al., 2000). Girls may be more likely to respond to relationship stressors in a way that exacerbates internalizing problems (Goodman et al., 2019; Rudolph et al., 2008). For example, if girls respond to conflicts with cognitive processes that up-regulate rather than resolve negative emotions (i.e., rumination), the emotion difficulties associated with internalizing problems may be reinforced (Nolen-Hoeksema, 2012). It may be these gendered affiliative tendencies together with the unique biopsychosocial transitions of female adolescents and the experience of negative life events trigger the onset of internalizing problems in adolescence (Cyranowski et al., 2000). Evidence on gender differences in the longitudinal associations between relationship difficulties and internalizing problems, however, is mixed. Some studies have found no significant differences between adolescent boys and girls on the longitudinal links between relationship difficulties (e.g., conflict) and internalizing problems (Goodman et al., 2019), whereas others suggest that girls may show a stronger association between maternal and paternal relationship difficulties and internalizing problems than boys (Finan et al., 2018; Lewis et al., 2014).
Less is known about the role of gender on internalizing symptoms in childhood. One longitudinal study found no gender differences in the mediating effects of parent-child conflict from late childhood to early adolescence (Yong et al., 2014). There is a dearth of research exploring gender differences in the longitudinal associations among children’s internalizing problems and difficulties in the parental relationship. Research in this area is needed because boys and girls show gender differences in affiliative tendencies in childhood (e.g., girls being more likely than boys to disclose emotions in relationships and to seek social support; Zeman & Shipman, 1997), and internalizing problems may begin to increase over childhood (Brock & Kochanska, 2015). Therefore, it is possible that gender plays an important role in the longitudinal associations between parent-child conflict and children’s internalizing problems, but whether or not this is the case is currently unknown.
The Current Study
The overarching goal of the current study was to disentangle the longitudinal associations between mother-child conflict and children’s internalizing problems in mid-childhood. Of available longitudinal studies, the evidence is mixed regarding whether mother-child conflict precedes children’s internalizing problems, children’s internalizing problems precede conflictual relationships, or whether there are bidirectional effects. In addition, few studies to date have examined the extent to which mother-child conflict and children’s internalizing problems reflect between-family differences versus within-family processes (for exceptions, see Brock & Kochanska, 2015; Lewis et al., 2014). It is also unknown whether longitudinal associations vary by child gender. We used data from a publicly available longitudinal study, the Study of Early Child Care and Youth Development (SECCYD), to test our three research questions focusing on relationships with mothers: (1) to what extent do mother-child conflict and children’s internalizing problems reflect stable between-family differences in middle childhood? In line with longitudinal studies examining both within- and between-family factors (Brock & Kochanska, 2015; Lewis et al., 2014), we expected between-family correlations such that families with higher conflictual mother-child relationships would tend to have children with higher internalizing problems. (2) Are the longitudinal associations between mother-child conflict and children’s internalizing problems directional, with one preceding the other, or are they bidirectional? Based on research to date (e.g., Epkins & Heckler, 2011; Yong et al., 2014), we expected that mother-child conflict would more strongly predict children’s internalizing problems over time than children’s internalizing problems would predict mother-child conflict. (3) Do the longitudinal associations between mother-child conflict and children’s internalizing problems vary by child gender? We hypothesized that the longitudinal associations would be stronger for girls than for boys. We tested our research questions using RI-CLPMs (Hamaker et al., 2015).
Method
Participants and Procedure
Data from the publicly available SECCYD were used in the present study. Detailed information on recruitment and the data achieve is available at https://www.icpsr.umich.edu.
SECCYD aimed to investigate various childcare factors related to health, academic, behavioral, emotional, and other developmental outcomes from infancy to middle adolescence. Participants were recruited in 1991 at 10 locations in the United States (Little Rock, AR; Irvine, CA; Lawrence, KS; Boston, MA; Hickory, NC; Philadelphia, PA; Pittsburgh, PA; Charlottesville, VA; Seattle, WA; Madison, WI) through hospitals visits. During selected 24-hr intervals among the selected hospitals, all women giving birth (N = 8,986) were screened for eligibility for the research. Some families (N = 3,142) were excluded due to the criteria such as not being proficient in English or planning to move within the next three years. An additional 1,353 families could not be reached or refused to participate in the study at a follow up phone interviews at two weeks. When children were one month old, home visits were completed among eligible families (N = 1,364) that were randomly chosen from the pool of remaining participants and data collection continued in four phases. At Phase I (birth to three years) of SECCYD, 1,364 children participated, and at Phase III (second through sixth grade) of the SECCYD retention rate was high (77.79 %) with 1,061 children. At recruitment, highest completed education was high school for 26% of mothers; 22% of mothers were from ethnic/racial minority backgrounds (i.e., non-White); and 21% of mothers had incomes lower than 200% of poverty line. For more details on sample characteristics, see the report by the NICHD Early Child Care Research Network (2005).
In the current study, approximately 51% of the children were male. Mothers’ mean number of years of education was 14.23 years at the time they were recruited into the study. Approximately 20% of the participants are from minority (Hispanic, African American and other) ethnic groups in the current sample. See Table 1 for the descriptive statistics of participant ethnicity and other demographic variables. The ethical approval for the current study was obtained from the Purdue University Institutional Review Board (#1908022540).
Table 1.
Descriptive Statistics
| N | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Internalizing (3rd grade) | 1026 | 48.43 | 9.90 | 33 | 82 |
| Internalizing (4th grade) | 1022 | 47.86 | 9.68 | 33 | 82 |
| Internalizing (5th grade) | 1017 | 48.74 | 9.78 | 33 | 86 |
| Internalizing (6th grade) | 1022 | 47.72 | 9.99 | 31 | 83 |
| Conflict (3rd grade) | 1027 | 16.13 | 6.05 | 7 | 32 |
| Conflict (4th grade) | 1021 | 15.94 | 5.91 | 7 | 35 |
| Conflict (5th grade) | 1015 | 16.37 | 5.99 | 7 | 35 |
| Conflict (6th grade) | 1023 | 16.77 | 6.20 | 7 | 33 |
| Male | 1364 | 0.52 | 0.50 | 0 | 1 |
| White | 1364 | 0.80 | 0.40 | 0 | 1 |
| Black | 1364 | 0.13 | 0.34 | 0 | 1 |
| Hispanic | 1364 | 0.05 | 0.21 | 0 | 1 |
| Other | 1364 | 0.02 | 0.14 | 0 | 1 |
| Mom Education | 1363 | 14.23 | 2.51 | 7 | 21 |
| Mom Vocabulary | 1167 | 99.01 | 18.35 | 40 | 159 |
| Mom Depression | 1026 | 9.08 | 8.85 | 0 | 55 |
| Family Income | 982 | 4.39 | 3.77 | 0.09 | 26.64 |
Note. For gender and race/ethnicity, the Ns are the number of responses on the categorical variables. The specific dummy coded variables reflect the proportion of the sample that falls into that category (i.e., if multiplied by 100 they would be the percentages)
Measures
Mother-child conflict.
The Conflict with Child subscale of Child-Parent Relationship Scale was used to assess mother-child conflict. Mothers reported mother-child conflict during home visits at third and fifth grades, and during the lab visit at fourth and sixth grades. The Child-Parent Relationship Scale was adapted from the Student-Teacher Relationship Scale (STRS; Pianta, 1994, 2001). This scale captures children’s attachment behaviors through parent report. Mothers responded to the items on 5-point Likert type scale from 1 (definitely does not apply) to 5 (definitely applies). Example items from Conflict with Child subscale include “My child and I always seem to be struggling with each other”, and “My child easily becomes angry at me”. Higher scores indicated higher conflict. Cronbach’s alpha of the Conflict with Child subscale ranged between .83 and .85 through third to sixth grades.
Internalizing problems.
Mothers reported their children’s internalizing problems during home visits at third and fifth grades, and during the lab visit at fourth and sixth grades. The Internalizing Problems subscale of Child Behavior Checklist (CBCL; (Achenbach, 1991) was used. The CBCL is a valid (Achenbach & Rescorla, 2000), and widely used instrument to measure social competence and problem behaviors among children aged between four and 18 years. Children’s behaviors (e.g., “Unhappy, sad, or depressed”) were scored on 3-point Likert-type scales from 0 (not true of the child) to 2 (very true of the child; Achenbach, 1991). Higher scores indicate greater internalizing problems.
Child, maternal, and family covariates.
In addition to the primary measures of interest above, several aspects of child, mother, and family status were measured to include in analyses. Gender (1 = male, 0 = female) and ethnicity (dummy codes for Black, Hispanic, and Other with White as the reference group) were included as child covariates. Maternal education, maternal vocabulary and maternal depression were included as maternal covariates. Maternal education was assessed by the years of completed schooling when the child was one month old. Maternal vocabulary was measured by the Peabody Picture Vocabulary Test-Revised when the child was three years old (Dunn & Dunn, 1981). Maternal depression was assessed by Center for Epidemiological Studies Depression Scale (Radloff, 1977) by mother report during the home visits at 3rd grade. Although the items were rated on 4-point Likert type scale from 1 (less than once a week) to 4 (5–7 days a week), they were transformed to be on a scale of 0–3 to match the original scale. An example item is “I thought my life had been a failure.”. The Cronbach’s alpha of the scale was .90. Family income was reported during the home visits at 3rd grade and included as family-level covariate. It was measured by the income-to-needs ratio (i.e., where one represents the federal poverty level, values less than one represent families living below the poverty level, and values greater than one represent families living above the poverty level).
Analytic Plan
We conducted data management and descriptive statistics in Stata 15 (StataCorp, 2017), and all structural equation models in Mplus 8 (Muthén & Muthén, 2017). Next, we conducted a series of model-building steps to ensure an appropriate base-model for hypothesis testing. First, we ran measurement models with random intercepts and autoregressive paths independently for mother-child conflict and child internalizing problems to determine whether autoregressive paths should be constrained to be equal across time or freely estimated. Next, we combined the selected models for mother-child conflict and child internalizing problems into a single RI-CLPM without any covariates to examine model fit. Finally, our primary model used to test our research questions included the single RI-CLPM specification with covariates predicting the random intercepts. Covariates included mother’s vocabulary, education, and depression (from the 3rd grade wave), race/ethnicity, family income-to-needs ratio (from the 3rd grade wave), and gender. Hypothesis 1 (that there would be stable between-family correlations of higher conflictual mother-child relationships with higher child internalizing problems) was tested by the included correlation between the two random intercepts. Hypothesis 2 (that mother-child conflict would more strongly predict children’s internalizing problems over time than children’s internalizing problems would predict mother-child conflict) was tested first by observing whether the cross-lagged paths in each direction were significant. If paths were significant in one or both directions, differences in magnitude were tested by constraining them to equality in a nested model and observing whether there was a decrement in model fit in doing so.
Next, we conducted a multiple group analysis consisting of two models in order to explore gender differences in order to test hypothesis 3 (that the longitudinal associations would be stronger for girls than for boys). Model 1 was an unconstrained model: our primary model—excluding gender as a covariate—with random intercepts, factor loadings, and paths freely estimated for males and females. The only estimates constrained equal between males and females were the time-specific intercepts for mother-child conflict and child internalizing problems (this was required for the model to converge in Mplus). Model 2 was a nested model that constrained factor loadings and path estimates for males and females to be equal. A decrement in model fit (a significant chi-square test), comparing Model 2 to Model 1 would indicate the presence of gender differences; a non-significant chi-square would indicate no decrement in model fit.
Finally, as sensitivity analyses to provide a direct comparison to most of the literature, we ran two additional CLPMs without random intercepts. One model included one lag (the autoregressive path from the prior time point only, t-1), and the other model included two lags (the autoregressive path from the prior time point, t-1, and the autoregressive path from two time points before, t-2). Differences in model conclusions are presented in the Results and interpreted in the Discussion.
Missing data and attrition.
Missing data was handled by using Full Information Maximum Likelihood (FIML) in all analyses. FIML uses all available information in the model and does not restrict the analyses to cases with no missing data, leading to less biased estimates than list-wise deletion and performing similarly to multiple imputation methods (Acock, 2012). Relatively little data on our primary constructs were lost due to attrition given the scope of the study as birth cohort design. Of the original 1364 participants, 1090 (80%) provided at least one observation on mother-child conflict or internalizing problems (911 provided complete data on both constructs from third through sixth grade). Our primary model was run on the subsample of 1090 that provided at least one observation on mother-child conflict or internalizing and the results were nearly identical and came to the same conclusions (results available by request). Gender and race/ethnicity experienced no missing data. The number of observations for all variables included in analyses are reported in Table 1.
Results
Descriptive Statistics and Correlations
In general, children’s levels of internalizing problems and mother-child conflict were stable from third to sixth grade (see Table 1). They were also moderately correlated across time points (rs ranged from .34 to .47, ps < .001, see Table 2). Of the covariates, maternal depression at third grade was most consistently correlated with children’s internalizing and mother-child conflict, followed by family income-to-needs ratios and maternal education.
Table 2.
Correlation Matrix
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | |
|---|---|---|---|---|---|---|---|---|
| 1. Internalizing (3rd grade) | — | |||||||
| 2. Internalizing (4th grade) | .73*** | — | ||||||
| 3. Internalizing (5th grade) | .67*** | .73*** | — | |||||
| 4. Internalizing (6th grade) | .63*** | .67*** | .73*** | — | ||||
| 5. Conflict (3rd grade) | .44*** | .39*** | .36*** | .35*** | — | |||
| 6. Conflict (4th grade) | .42*** | .47*** | .42*** | .37*** | .77*** | — | ||
| 7. Conflict (5th grade) | .37*** | .37*** | .40*** | .34*** | .68*** | .75*** | — | |
| 8. Conflict (6th grade) | .35*** | .38*** | .40*** | .41*** | .65*** | .69*** | .71*** | — |
| Male | .01 | −.01 | .01 | .01 | −.04 | −.01 | −.04 | −.07* |
| White | −.00 | .03 | .02 | .03 | .05 | .05 | −.00 | −.02 |
| Black | .00 | −.01 | −.01 | −.03 | −.06 | −.04 | −.01 | .00 |
| Hispanic | −.00 | −.02 | −.03 | −.02 | .03 | .05 | .05 | .06* |
| Other | .00 | −.02 | .02 | .02 | −.06 | −.11*** | −.07* | −.07* |
| Mom Education | −.07* | −.10** | −.07* | −.04 | −.07* | −.07* | −.09** | −.12*** |
| Mom Vocabulary | −.03 | −.06 | −.01 | .00 | −.03 | −.07* | −.07* | −.09** |
| Mom Depression | .32*** | .30*** | .30*** | .26*** | .26*** | .27*** | .27*** | .29*** |
| Family Income | −.11*** | −.14*** | −.11*** | −.11** | −.09** | −.10** | −.11*** | −.12*** |
Note.
p < .05;
p < .01;
p < .001.
Model Building
All model-fit statistics are presented in Table S1. For the measurement models, chi-squared difference tests suggested that the model with constrained autoregressive paths fit significantly worse for mother-child conflict, but the model with constrained estimated autoregressive paths did not provide a worse fit to the data for child internalizing problems (see Table S1). Thus, the two measurement models (including freely estimated autoregressive paths for mother-child conflict, but constrained auto-regressive paths for child internalizing problems) were combined into a RI-CLPM that fit the data well. The primary model additionally including covariates also fit the data very well (Table S1). In the multiple group analysis exploring gender differences, constraining estimates for males and females did not result in a decrement in model fit (Table S1), contrary to the third hypothesis, and thus results from the primary model—the most parsimonious model—are presented.
Longitudinal Associations between Internalizing and Mother-Child Conflict
The results of the RI-CLPM are presented in Figure 1. As expected in the first hypothesis, the random intercepts between children’s internalizing problems and mother-child conflict were moderately correlated (r = 0.49, p < .001), suggesting that relatively stable between-family differences account for part of the association between the two constructs. The constructs also had significantly correlated errors at each time point, although these were weaker in magnitude than the correlation between random intercepts. These correlated errors suggest that time-specific variations in mother-child conflict and child internalizing problems are related to each other (rs ranged from 0.12 to 0.28, ps < .01), such that positive deviations in children’s internalizing problems are associated with positive deviations in mother-child conflict (and vice versa) at each specific wave (i.e., beyond relative stability in both constructs). Although autoregressive paths for both mother-child conflict and for child internalizing problems were significant, these paths were relatively small in magnitude.
Figure 1. Random Intercept Cross-Lagged Panel Model for Internalizing and Conflict.
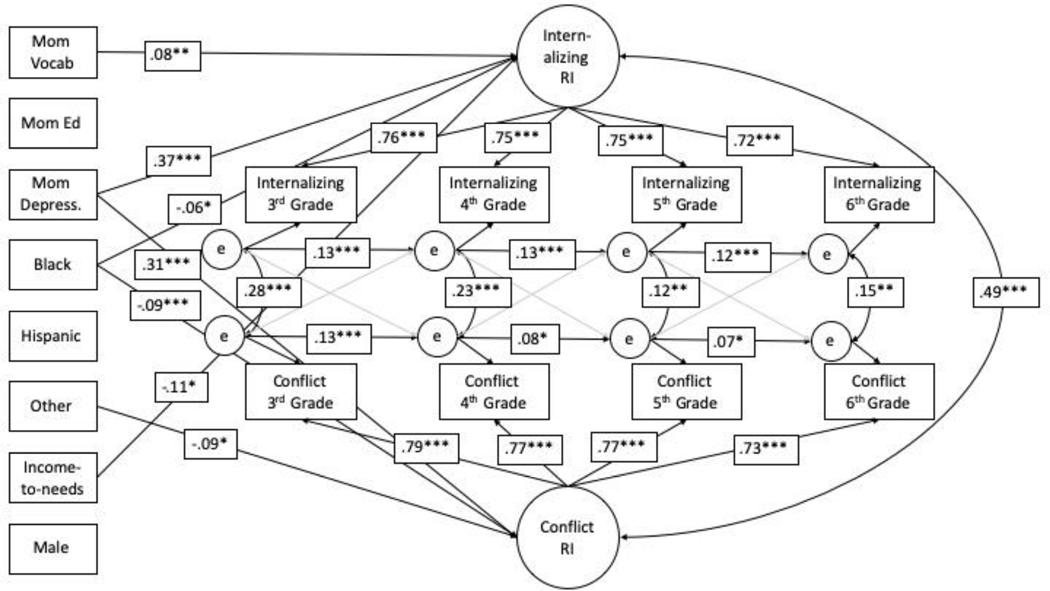
Only significant paths from covariates to random intercepts shown. Cross-lagged paths included, but are not significant (shown as grey). * p < .05. ** p < .01. *** p < .001.
Our second hypothesis was that mother-child conflict would more strongly predict children’s internalizing problems over time than children’s internalizing problems would predict mother-child conflict. Contrary to expectations, no significant cross-lagged paths emerged. Specifically, prior time-point specific variation in child internalizing problems did not predict subsequent time-point specific variation in mother-child conflict, or vice versa.
Gender differences.
Model 1 with paths freely estimated for males and females are presented in Figure S1 as a test of our third hypothesis that longitudinal associations would be stronger for females than males. Although some differences emerged in which associations were statistically significant, the majority of associations were similar in magnitude between males and females, which was contrary to our expectations. In addition, as noted above, in the group analyses, the model with constrained estimates between males and females estimated the data very well and did not result in a decrement in model fit relative to the unconstrained model and was thus preferred to the model that freely estimated associations (see Table S1). Notably, in the model with freely estimated cross-lagged paths for each gender, none reached statistical significance, which is consistent with conclusions drawn from the primary model.1
Covariates.
A few covariates emerged as significant predictors of the random intercepts (see Table S2 for all unstandardized coefficients, standard errors, and p-values from the model). Maternal depressive symptoms significantly predicted children’s internalizing problems (β = 0.37, p < .001) and mother-child conflict (β = 0.31, p < .001). Black children, compared to White children, had significantly fewer internalizing problems (β = −0.06, p = 0.04) and significantly less mother-child conflict (β = −0.09, p < .001). Families with higher income-to-needs ratios had children with significantly fewer internalizing problems (β = −0.11, p = 0.02), although higher maternal education was associated with significantly more internalizing problems (β = 0.08, p = 0.01).
Sensitivity analyses with cross-lagged panel models.
Finally, we also estimated two CLPMs with no random intercepts: one using autoregressive paths (see Figure S2) with a single lag of one time point (t-1), and the other using autoregressive paths with two lags (t-1 and t-2; see Figure S3). The model with a single lagged path fit significantly worse than the model with two lagged paths (see Table S1). In the model including two lags, all autoregressive paths from t-1 and from t-2 were statistically significant. Statistically significant bidirectional paths emerged as well. Third grade internalizing problems significantly predicted fourth grade mother-child conflict (β = 0.07, p < .001); fourth grade mother-child conflict significantly predicted fifth grade internalizing (β = 0.06, p = .033); and, fifth grade internalizing significantly predicted sixth grade mother-child conflict (β = 0.09, p = .001).
Discussion
Our primary aim in the current study was to disentangle the longitudinal associations between mother-child conflict and children’s internalizing problems in middle childhood. We examined the extent of between-family differences and within-family processes in these longitudinal associations by incorporating random intercepts into our CLPM analytic approach. We found that mother-child conflict and children’s internalizing problems were relatively stable between 3rd and 6th grade, that the relatively stable factors of each construct were positively correlated, and that their error terms were positively correlated at each time point, which were in line with expectations. However, contrary to expectations, we found no cross-lagged associations between mother-child conflict and children’s internalizing problems (i.e., no significant bidirectional paths). In addition, we did not observe gender differences in the longitudinal associations between mother-child conflict and children’s internalizing symptoms, which was also contrary to our expectations.
Disentangling Within- and Between-Family Associations: Considering Time Scale
The idea that developmental processes at multiple levels of analysis (e.g., individual and social levels) are transactional is central to the developmental psychopathology approach (Cicchetti & Cohen, 2006). Some studies on parent-child relationships and children’s internalizing problems provide evidence for such bidirectional associations (e.g., Hipwell et al., 2008; Yong et al., 2014); however, the majority of studies on this topic to date do not account for between-family differences in their tests of within-family processes. As a consequence, estimates of directional associations between mother-child conflict and children’s internalizing symptoms may be inaccurate (Hamaker et al., 2015). The results of our study highlight the differences in conclusions drawn when random intercepts are incorporated into CLPMs versus not. Had we not accounted for stable between-family differences with random intercepts, we would have concluded from these data that in middle childhood, children’s internalizing problems predict subsequent mother-child conflict, which in turn predicts greater children’s internalizing problems. However, these directional associations were not found in the model incorporating random intercepts, which suggests that the bidirectional effects found in past literature using CLPMs may be influenced by relatively stable between-family differences that were not accounted for.
It is important to note that both the RI-CLPM and the CLPM with two lags fit the data well, but the CLPM with one lag did not. Well-fitting models are not proof of their accuracy (Tomarken & Waller, 2003), but the key conceptual distinctions should be considered between the RI-CLPM and CLPM with two lags in comparing them. In the RI-CLPM, the assumption is that unobserved factors contribute to relative stability in both constructs across time (potentially due to stable environments or individual characteristics). In the CLPM with two lags, stability in the constructs is generated by both t-1 and t-2 autoregressive paths. The causal inferences for this model would imply that both mother-child conflict and internalizing is not only temporally related to subsequent mother-child conflict and internalizing (t-1), but also have delayed sleeper effects that operate independent of the intermediary behaviors (t-2) and covariates. Thus, the RI-CLPM aligns better with current theory on developmental influences (i.e., both proximal construct-specific and broader stable influences), and the CLPM with two lags is largely inconsistent with most theoretical explanations.
There are several possible explanations of the null directional effects in the results of our RI-CLPM. One is that there is a true lack of bidirectional associations between mother-child conflict and children’s internalizing problems in middle childhood. Another explanation is that the lack of significant associations are Type II errors. Given these possible explanations and in the context of our overall results, the lack of directional associations observed in the current study may also have to do with the time scale at which data were collected. Our results showed that the error terms between mother-child conflict and children’s internalizing problems covary over time—as one increases in a given year, so does the other (independent of relative stability), and vice versa. The extent of conflict in mother-child relationships can vary on the time scales of months, weeks, days, and hours (Lougheed, 2019, 2020). We speculate that, while the current study does not provide evidence that mother-child conflict and children’s internalizing problems are bidirectionally associated over yearly development, the potential causal bidirectional effects may manifest on shorter timescales (e.g., weeks, months). It will be important for future research to incorporate multiple time scales into studies such as with multiple burst designs (Ram & Diehl, 2015). Multiple burst designs involve “bursts” of intensive longitudinal assessments at short time scales (e.g., behavioral observations of mother-child conflicts, daily experience sampling of conflict) that are repeated over longer time scales such as months or years (Lougheed, 2020). This type of design would enable researchers to more thoroughly disentangle the direction of associations between conflict and internalizing problems that we observed in their correlated error terms. This approach would be more closely aligned to the theoretical tenets of developmental psychopathology that individual development is embedded in social processes at multiple levels (Cicchetti & Cohen, 2006; Granic, 2005).
The Role of Gender
Gender differences in socioemotional development can manifest in middle childhood (Chaplin & Aldao, 2013), and thus it was contrary to our expectations that we did not observe significant gender differences in the associations between mother-child conflict and children’s internalizing problems. Previous research has shown that pubertal development is linked to both parent relationships (Marceau et al., 2015; Paikoff & Brooks-Gunn, 1991) and adolescent internalizing problems (Cyranowski et al., 2000). We speculate that any gender differences in the longitudinal associations between mother-child conflict and children’s internalizing problems, if they exist, may manifest around the same time that gender differences in internalizing problems become apparent in adolescence (Cyranowski et al., 2000).
Limitations and Future Directions
Our results should be interpreted in the context of a few limitations of the current study. First, mother-child conflict and children’s internalizing symptoms were measured once per year, and future studies should use designs with a shorter time scale, as discussed above. Second, it will be important for future research to be conducted longitudinally from middle childhood through adolescence to gain a clearer understanding of if, and when, conflictual relationships and internalizing problems become linked. Longitudinal designs spanning the years before, during, and after puberty will have the greatest potential to determine if and when gender is associated with longitudinal links between mother-child conflicts and children’s internalizing problems.
Third, all measures used in the current study were mother-report questionnaires, and thus shared method variance could explain some of the findings of the current study. In this study, the sole use of mother-report questionnaires may have inflated the correlations between the random intercepts. Our results are somewhat inconsistent with other studies on bidirectional associations between negative aspects of parent-child relationships and children’s internalizing problems that have either obtained data from multiple reporters or examined observed relationship characteristics with multiple family members. For example, one study found bidirectional associations between mother-reported negative parenting and subsequent daughter-reported depressed mood (Hipwell et al., 2008). Another study showed that observed negativity (e.g., conflictual interactions) in mother-child but not father-child relationships were associated with subsequent increases in children’s internalizing symptoms (Brock & Kochanska, 2015). Future research on parent-child conflict and children’s internalizing problems should incorporate measures from multiple reporters to reduce the potential influence of shared method variance.
There are several other important directions for future research. One is to examine children’s externalizing symptoms in relation to parent-child conflict and children’s internalizing symptoms. Internalizing and externalizing symptoms can be comorbid in middle childhood, and children’s externalizing problems have been associated with parent-child conflicts (Granic & Lougheed, 2016). Another future direction is to simultaneously examine change over time in parental symptoms (e.g., internalizing, externalizing). In our study, we found that maternal depression was positively associated with stable between-family differences in both child internalizing symptoms and parent-child conflict. However, parental symptoms may vary over time in ways that predict both children’s symptoms and parent-child conflict (Lougheed, 2020). It is also important for future research to examine how conflict and internalizing problems are associated in other family relationships (e.g., children’s relationships with fathers, non-biological parents and other caregivers) and in more diverse samples.
Conclusion
The results of this study show that mother-child conflict and children’s internalizing problems covary longitudinally in middle childhood—as one increases or decreases on a year-to-year basis, so does the other. These results suggest that both of these aspects of children’s lives are related to each other, although not through cross-lagged associations at a yearly time scale when between-family differences have been accounted for. Future studies that incorporate methods that are more directly aligned with the developmental psychopathology approach (Cicchetti & Cohen, 2006; Granic, 2005) by incorporating multiple time scales (e.g., multiple burst designs) and that account for both within-family processes and between-family differences (i.e., random intercepts) will be powerful for disentangling the associations between family relationship processes and children’s internalizing problems.
Supplementary Material
Acknowledgments
A cooperative agreement (5 U10 HD027040) between the study investigators and the Eunice Kennedy Shriver National Institute of Child Health and Human Development supported the design and data collection of the Study of Early Childcare and Youth Development (SECCYD) from birth through age 15 years. The content is solely the responsibility of the authors and does not necessarily reflect the views of the NICHD or NICHD Early Child Care Research Network. We gratefully acknowledge the support of the Center for Families (Purdue University). Dr. Marceau was supported by the National Institute on Drug Abuse (K01 DA039288).
Footnotes
We also ran models that only examined males and females separately (available by request). For males, the cross-lagged effect between 5th grade internalizing and 6th grade conflict became statistically significant, β = .07, p = .045. Given the strength of association was similar to the original model, β = .04, and the p-value was just below the threshold for significance without any correction for multiple testing, we interpret the null cross-lagged findings from the multiple group analysis.
Conflicts of interest: None.
References
- Achenbach TM (1991). Manual for the Child Behavior Checklist/4–18 and Profile. University of Vermont, Department of Psychiatry. [Google Scholar]
- Achenbach TM, & Rescorla LA (2000). Manual for the ASEBA preschool forms and profiles (Vol. 30). University of Vermont, Research Center for Children, Youth, and Families. [Google Scholar]
- Acock AC (2012). What to do about missing values. In Cooper H, Camic PM, Long DL, Panter AT, Rindskopf D. & Sher KJ (Eds.), Data analysis and research publication. APA Handbook of research methods in psychology, Vol. 3. (pp. 27–50). Washington, DC: American Psychological Association. [Google Scholar]
- Allen JP, Insabella G, Porter MR, Smith FD, Land D, & Phillips N. (2006). A social–interactional model of the development of depressive symptoms in adolescence. Journal of Consulting and Clinical Psychology, 74(1), 55–65. doi: 10.1037/0022-006X.74.1.55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bosmans G, & Kerns KA (2015). Attachment in middle childhood: Progress and prospects. In Bosmans G. & Kerns KA (Eds.), New Directions for Child and Adolescent Development (Vol. 148, pp. 1–14). doi: 10.1002/cad.20100 [DOI] [PubMed] [Google Scholar]
- Branje SJT, Hale WW, Frijns T, & Meeus WHJ (2010). Longitudinal associations between perceived parent-child relationship quality and depressive symptoms in adolescence. Journal of Abnormal Child Psychology, 38(6), 751. doi: 10.1007/s10802-010-9401-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brière FN, Archambault K, & Janosz M. (2013). Reciprocal prospective associations between depressive symptoms and perceived relationship with parents in early adolescence. The Canadian Journal of Psychiatry, 58(3), 169–176. [DOI] [PubMed] [Google Scholar]
- Brock R, & Kochanska G. (2015). Decline in the quality of family relationships predicts escalation in children’s internalizing symptoms from middle to late childhood. Journal of Abnormal Child Psychology, 43(7), 1295–1308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaplin TM, & Aldao A. (2013). Gender differences in emotion expression in children: A meta-analytic review. Psychological Bulletin, 139(4), 735–765. doi: 10.1037/a0030737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D, & Cohen DJ (Eds.). (2006). Developmental psychopathology (2nd ed.). John Wiley & Sons. [Google Scholar]
- Cicchetti D, & Rogosch FA (1996). Equifinality and multifinality in developmental psychopathology. Development and Psychopathology, 8(4), 597–600. [Google Scholar]
- Collins WA, & Laursen B. (2004). Changing relationships, changing youth. The Journal of Early Adolescence, 24(1), 55–62. doi: 10.1177/0272431603260882 [DOI] [Google Scholar]
- Cyranowski JM, Frank E, Young E, & Shear K. (2000). Adolescent onset of the gender difference in lifetime rates of major depression. Archives of General Psychiatry, 57(1), 21–27. [DOI] [PubMed] [Google Scholar]
- Dunn LM, & Dunn LM (1981). Peabody Picture Vocabulary Test—Revised manual for Forms L and M. American Guidance Service. [Google Scholar]
- Epkins CC, & Heckler DR (2011). Integrating etiological models of social anxiety and depression in youth: Evidence for a cumulative interpersonal risk model. Clinical Child and Family Psychology Review, 14(4), 329–376. [DOI] [PubMed] [Google Scholar]
- Finan LJ, Ohannessian CM, & Gordon MS (2018). Trajectories of depressive symptoms from adolescence to emerging adulthood: The influence of parents, peers, and siblings. Developmental Psychology, 54(8), 1555–1567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilliom M, & Shaw DS (2004). Codevelopment of externalizing and internalizing problems in early childhood. Development and Psychopathology, 16(2), 313–333. [DOI] [PubMed] [Google Scholar]
- Goodman RJ, Samek DR, Wilson S, Iacono WG, & Mcgue M. (2019). Close relationships and depression: A developmental cascade approach. Development and Psychopathology, 31(4), 1451. doi: 10.1017/S0954579418001037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granic I. (2005). Timing is everything: Developmental psychopathology from a dynamic systems perspective. Developmental Review, 25(3), 386–407. doi: 10.1016/j.dr.2005.10.005 [DOI] [Google Scholar]
- Granic I, & Lougheed JP (2016). The role of anxiety in coercive family processes with aggressive children. In Dishion TJ & Snyder J. (Eds.), The Oxford Handbook of Coercive Relationship Dynamics (pp. 231–248). Oxford University Press. [Google Scholar]
- Hamaker EL, Kuiper RM, & Grasman RPPP (2015). A critique of the cross-lagged panel model. Psychological Methods, 20(1), 102–116. doi: 10.1037/a0038889 [DOI] [PubMed] [Google Scholar]
- Hipwell A, Keenan K, Kasza K, Loeber R, Stouthamer-Loeber M, & Bean T. (2008). Reciprocal influences between girls’ conduct problems and depression, and parental punishment and warmth: A six year prospective analysis. Journal of Abnormal Child Psychology, 36(5), 663–677. doi: 10.1007/s10802-007-9206-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollenstein T, & Lougheed JP (2013). Beyond storm and stress: Typicality, transactions, timing, and temperament to account for adolescent change. American Psychologist, 68(6), 444. doi: 10.1037/a0033586 [DOI] [PubMed] [Google Scholar]
- Holsen I, Kraft P, & Vittersø J. (2000). Stability in depressed mood in adolescence: Results from a 6-year longitudinal panel study. Journal of Youth and Adolescence, 29(1), 61–78. [Google Scholar]
- Joiner T, Coyne JC, & Blalock J. (1999). On the interpersonal nature of depression: Overview and synthesis. In Joiner T. & Coyne JC (Eds.), The interactional nature of depression: Advances in interpersonal approaches.: Vol. xiv (pp. 3–19). American Psychological Association. [Google Scholar]
- Laursen B, & Hafen C. (2010). Future directions in the study of close relationships: Conflict is bad (except when it’s not). Social Development, 19(4), 858–872. doi: 10.1111/j.1467-9507.2009.00546.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis G, Collishaw S, Thapar A, & Harold GT (2014). Parent-child hostility and child and adolescent depression symptoms: The direction of effects, role of genetic factors and gender. European Child & Adolescent Psychiatry, 23(5). [DOI] [PubMed] [Google Scholar]
- Lougheed JP (2019). Conflict dynamics and the transformation of the parent-adolescent relationship. In Kunnen S, van der Gaag M, de Ruiter-Wilcox N, & Jeronimus B. (Eds.), Psychosocial Development in Adolescence: Insights from the Dynamic Systems Approach. Routledge. [Google Scholar]
- Lougheed JP (2020). Parent-adolescent dyads as temporal interpersonal emotion systems. Journal of Research on Adolescence, 30(2), 26–40. doi: 10.1111/jora.12526 [DOI] [PubMed] [Google Scholar]
- Marceau K, Ram N, & Susman EJ (2015). Development and lability in the parent–child relationship during adolescence: Associations with pubertal timing and tempo. Journal of Research on Adolescence, 25(3), 474–489. doi: 10.1111/jora.12139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLellan LF, & Hudson JL (2017). Generalised Anxiety Disorder. In Goldstein S. & DeVries M. (Eds.), Handbook of DSM-5 Disorders in Children and Adolescents (pp. 193–212). Springer International Publishing. doi: 10.1007/978-3-319-57196-6_9 [DOI] [Google Scholar]
- Morris AS, Cui L, Criss MM, & Simmons WK (2018). Emotion regulation dynamics during parent-child interactions: Implications for research and practice. In Cole PM & Hollenstein T. (Eds.), Emotion Regulation: A Matter of Time. Routledge. [Google Scholar]
- Morris AS, Silk JS, Steinberg L, Myers SS, & Robinson LR (2007). The role of the family context in the development of emotion regulation. Social Development, 16(2), 361–388. doi: 10.1111/j.1467-9507.2007.00389.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Mplus user’s guide (Version 8) [Computer software]. Muthén & Muthén. [Google Scholar]
- NICHD Early Child Care Research Network. (2005). Child care and child development: Results from the NICHD study of early child care and youth development. Guilford Press. [Google Scholar]
- Nolen-Hoeksema S. (2012). Emotion regulation and psychopathology: The role of gender. Annual Review of Clinical Psychology, 8, 161–187. doi: 10.1146/annurev-clinpsy-032511-143109 [DOI] [PubMed] [Google Scholar]
- Paikoff RL, & Brooks-Gunn J. (1991). Do parent-child relationships change during puberty? Psychological Bulletin, 110(1), 47–66. [DOI] [PubMed] [Google Scholar]
- Pianta RC (1994). Patterns of relationships between children and kindergarten teachers. Journal of School Psychology, 32(1), 15–31. doi: 10.1016/0022-4405(94)90026-4 [DOI] [Google Scholar]
- Pianta RC (2001). Student-Teacher Relationship Scale. PAR, Inc. [Google Scholar]
- Powell AK, Ocean SE, & Stanick CF (2017). Depressive disorders. In Goldstein S. & De Vries M. (Eds.), Handbook of DSM-5 Disorders in Children and Adolescents (pp. 151–172). Springer International Publishing. [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self report depression scale for research in general population. Applied Psychological Measurement, 1(3), 385–401. doi: 10.1177/014662167700100306 [DOI] [Google Scholar]
- Ram N, & Diehl M. (2015). Multiple time-scale design and analysis: Pushing towards real-time modeling of complex developmental processes. In Diehl M, Hooker K, & Sliwinski MJ (Eds.), Handbook of intraindividual variability across the lifespan (pp. 308–323). Routledge. [Google Scholar]
- Rudolph KD, Flynn M, & Abaied JL (2008). A developmental perspective on interpersonal theories of youth depression. In Abela JR & Hankin BL (Eds.), Handbook of depression in children and adolescents (pp. 79–102). Guilford Press. [Google Scholar]
- Samek DR, Wilson S, Mcgue M, & Iacono WG (2018). Genetic and environmental influences on parent-child conflict and child depression through late adolescence. Journal of Clinical Child & Adolescent Psychology, 47(sup1), S5–S20. doi: 10.1080/15374416.2016.1141357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheeber LB, Davis B, Leve C, Hops H, & Tildesley E. (2007). Adolescents’ relationships with their mothers and fathers: Associations with depressive disorder and subdiagnostic symptomatology. Journal of Abnormal Psychology, 116(1), 144–154. doi: doi: 10.1037/0021-843X.116.1.144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smetana JG, Campionne-Barr N, & Metzger A. (2006). Adolescent development in interpersonal and societal contexts. Annual Review of Psychology, 57, 255–284. doi: 10.1146/annurev.psych.57.102904.190124 [DOI] [PubMed] [Google Scholar]
- Smith O, Nelson J, & Adelson M. (2019). Interparental and parent–child conflict predicting adolescent depressive symptoms. Journal of Child and Family Studies, 28(7), 1965–1976. doi: 10.1007/s10826-019-01424-6 [DOI] [Google Scholar]
- StataCorp. (2017). Stata Statistical Software: Release 15. StataCorp LP. [Google Scholar]
- Stuart Parrigon K, & Kerns K. (2016). Family processes in child anxiety: The long-term impact of fathers and mothers. Journal of Abnormal Child Psychology, 44(7), 1253–1266. [DOI] [PubMed] [Google Scholar]
- Tomarken AJ, & Waller NG (2003). Potential problems with “well fitting” models. Journal of Abnormal Psychology, 112(4), 578–598. doi: 10.1037/0021-843X.112.4.578 [DOI] [PubMed] [Google Scholar]
- Yong M, Fleming CB, Mccarty CA, & Catalano RF (2014). Mediators of the associations between externalizing behaviors and internalizing symptoms in late childhood and early adolescence. The Journal of Early Adolescence, 34(7), 967–1000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeman J, & Shipman K. (1997). Social-contextual influences on expectancies for managing anger and sadness: The transition from middle childhood to adolescence. Developmental Psychology, 33(6), 917–924. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.