

Abstract
Background and Aims
Changes in cannabis legalization and availability in Australia necessitate monitoring use and attitudes. We estimated age-period-cohort effects of past-year cannabis use and attitudes toward criminalization and legalization.
Design
Analysis of six waves of the Australian National Drug Strategy Household Survey (NDSHS) every 3 years (2001–2016).
Setting and participants
The study was nationally representative of Australian households using multistage random sampling, totaling 145168 respondents 18–79 years old. Data were collected using telephone, face-to-face, and drop-and-collect. Sample sizes per analysis varied based on data availability (~107000–127000 per model).
Measurements
Six waves of data for past-year cannabis use (by sex and education), attitudes toward criminalization and legalization.
Findings
Past-year cannabis use decreased in young adults ages 18–35 from 2001–2016 (25.1%–18.6%) and increased in middle adults ages 36–55 (8.6%–10.1%) and older adults ages 56–79 (0.6%–3.0%). We observed a positive period effect and negative cohort effect for recent cohorts for past-year use (e.g. 1955 cohort had 1.41 (95% CI: [1.11, 1.70]) increased log odds vs. 1998 cohort had −2.86 (95% CI: [−3.17, −2.55]) increased log odds) compared with the mean across years. Results were consistent by sex and varied by education. We observed a negative period effect for criminalization favorability (0.14 (95% CI: [0.003, 0.28]) increased log odds in 2001 vs. −0.31 (95% CI: [−0.45, −0.17]) increased log odds in 2016) and positive cohort effect for recent cohorts. Last, we observed a positive period effect for legalization support (−0.03 (95% CI: [−0.20, 0.14]) increased log odds in 2001 vs. 0.38 (95% CI: [0.22, 0.55]) increased log odds in 2016) and negative cohort effect for recent cohorts.
Conclusion
Cannabis use appears to be increasing in Australia among adults over 35, while decreasing among adolescents and young adults. Legalization support also appears to have been increasing since 2007, signaling discordance between use and attitudes among adolescents and young adults, and potentially predicting increases in use over time.
Keywords: Age-period-cohort, Australia, cannabis, cannabis policy, legalization, time trends, Australia
INTRODUCTION
In 2016, cannabis was the most commonly used illegal substance in Australia, with 10.4% of Australians 14 years or older reporting past-year use [1]. However, from 2001–2016 past-year cannabis use has generally declined among those aged 14–39 but either increased or remained stable for those ages 40 or older [1]. These differential age patterns within larger population trends suggest that cohort effects may influence recent cannabis use trends.
Laws regarding cannabis access have changed variably across countries. The United States (US) states are increasingly legalizing cannabis use [2], and in 2018, Canada passed the Cannabis Act, legalizing adult-only cannabis use nationwide [3]. However, Australian cannabis laws and policies have changed more slowly [4]. Several Australian states decriminalized cannabis use in the 1980s–1990s [5], and in 2019 the Australia Capital Territory became the first territory to legalize adult cannabis use [6]. However, cannabis use remains illegal under federal law [6]. Public knowledge of legislation adds further complexity. AUS study found that adolescents had lower knowledge of medical cannabis laws (MCL) than adults, adjusting for state-level cannabis use prevalence, MCL enactment, and open dispensaries [7]. Accumulating evidence indicates that cannabis use is changing at different rates than policy and attitude changes [8], suggesting that drivers of each should be considered as separate time-varying processes.
Examining age-period-cohort trends in cannabis use and attitudes toward use is critical to understanding how these outcomes portend changes in use over time. Existing research indicates that attitudes toward cannabis among young cohorts are becoming more favorable with no comparable changes in use [8], suggesting different underlying processes by age, period, and cohort. Age-period-cohort (APC) models identify particular cohorts at historical time periods that have high rates of use and allow us to examine how environmental changes affect health outcomes through period and/or cohort effects. Period effects refer to the variance over time in exposures that affect all age groups; for example, changes in cannabis legalization may manifest as period effects as they may influence access, availability, and use across age. Cohort effects refer to variance over time in exposures that affect age groups differently; for example, baby-boomers in the United States had higher rates of cannabis use in adolescence compared with previously born and later-born cohorts, coinciding with global political events and drug access, and these cohorts have maintained a unique rate of use through adulthood [9–11]. Existing APC analyses in several countries indicate that cannabis use trends have been driven by period and cohort effects to varying degrees. For example, US data indicate that past-month cannabis use increased in recent years, and 1950s cohorts had higher past-month use compared to 1940s cohorts [12]. However, age effects remained the strongest determinant of use, with peaks in young adulthood [12]. Another US study found that recent cannabis use increases were driven mostly by period effects, with both men and women exhibiting increases in recent years [13]. Frequent cannabis use also increased among US adolescents in recent decades with recent cohorts having a lower increase in use than older cohorts, consistent across sex, parental education, and race/ethnicity [14]. Other studies corroborate these observed cohort trends by sex. A meta-regression analysis of birth cohorts from 1941–1995 in 30 countries indicated sex convergence in cannabis use among recent cohorts [15]. Outside of the United States, an age-period-cohort analysis of past-year cannabis use in Germany revealed significant negative age effects comparable across sex, with no significant period or cohort effects, and that education had a negative influence on past-year cannabis use among men [16]. Additional studies have examined APC effects of legalization support. US adults have shown increases in legalization support beginning in the early 1990s coupled with steep declines in support as age increases and minimal cohort effects [17,18].
The evolving legal landscape of cannabis use in Australia warrants up-to-date APC analyses to monitor changes in use and legalization support. Furthermore, previous studies indicate that there may exist age-related trends in cannabis use [1,19]. The present study uses nationally representative data for 18–79 year-olds from the Australian National Drug Strategy Household Survey (NDSHS) (2001–2016) to examine past-year cannabis use trends and legalization attitudes. We use hierarchical age-period-cohort (HAPC) models to parse APC effects at the population level. We also conduct subgroup analyses by sex to test whether, similar to the United States [13], both men and women would exhibit increases in cannabis use observed through similar period effects. Last, we conduct subgroup analyses by educational attainment to test whether cannabis use trends among individuals with lower educational attainment would remain unchanged as observed in other studies [20], exhibited through flatter period effects.
METHODS
Data
We obtained data from NDSHS, a nationally representative household-level survey of Australians aged 14+. Australian Institute of Health and Welfare (AIHW) conducts this survey every 3 years since 1985 and uses multistage random sampling with stratification by state, territory, and part of state [1]. Methods of data collection changed over time, including telephone, face-to-face, and drop-and-collect. The 2004 survey used different data collection methods, and differences in prevalence of lifetime cannabis use were minimal (31.9%–35.2%), suggesting pooled analyses will produce consistent estimates [21]. Weights were assigned to produce a representative sample of English-speaking Australians residing in private dwellings and incorporated geographical stratification, household size, age, and sex [22]. Survey response rates were relatively consistent across the study period, ranging from 46.0% in 2004 to 51.6% in 2007 [1,21,23]. Non-response rates for variables used in our analysis were low, with the highest percentage of missingness pertaining to the question on education (4.0%). Participants with missing data were excluded.
We excluded respondents aged 80+ because of the lack of disaggregated age data in some survey waves and less than 18-year-olds as there were not enough cohort years to reliably estimate cohort effects. Therefore, the overall sample used six survey waves from 2001–2016, comprising 145168 respondents. Sample sizes for analyses varied based on availability of data and ranged from ~107000–127000 per model.
Measures
Cannabis use
The NDSHS contains questions on cannabis use and attitudes toward use. Past-year cannabis use was estimated from the question: “Have you used marijuana/cannabis in the past 12 months? Yes/No”. Support for cannabis use criminalization was assessed using the question: “Do you think the possession of small quantities of marijuana/cannabis for personal use should be a criminal offense, that is, should offenders get a criminal record? Yes/No/Don’t know”. Support for cannabis use legalization was assessed using the question: “To what extent would you support or oppose the personal use of marijuana/cannabis being made legal? Strongly support/Support/Neither support or oppose/Oppose/Strongly oppose/Don’t know enough to say”. Minor wording changes occurred after 2001 in cannabis use questions; in 2001 cannabis was described as “marijuana (or cannabis)” and thereafter “marijuana/cannabis”. In addition, “don’t know” became an option for the latter two questions after 2001. These responses were dropped for consistency across years. Last, the question on legalization support was not asked of all respondents in 2007 and was omitted for those completing the survey using the computer-assisted telephone interviewing (CATI) phone interview (15.2% of the sample).
Period and birth cohort
Period was defined as the year in which the survey was conducted: 2001, 2004, 2007, 2010, 2013, and 2016. Cohort was calculated as survey year (period) minus the respondent’s age that year. To mitigate the effects of recall bias among older cohorts, we combined cohort years 1922–1940. All other cohorts were analyzed as individual years. Both period and cohort were modeled as categorical variables.
Sociodemographics
Sex (male vs. female), age (examined categorically in descriptive analyses and continuously in HAPC modeling), and education (completed vs. did not complete 12th grade) were included as covariates.
Analysis
Descriptive analyses were conducted to summarize age-specific trends of past-year cannabis use from 2001–2016. We then conducted APC analysis, which historically has been challenging as a result of the “identification problem” that occurs because of linear dependency of these variables (period = cohort + age) [24–28]. HAPC models circumvent this issue by modeling cross-classified random effects in which age and other individual-level data are considered fixed effects and periods and birth cohorts are considered random effects [24–28]. Therefore, the three variables are not assumed to be additive or linear as they would in a conventional regression, with all three variable simultaneously in the model. Rather, age effects are assumed to be fixed effects describing the overall variation in the outcome attributable to age, whereas period and cohort effects are random variables that describe overall variation in the intercept of the model across periods and cohorts [28]. Numerous demonstrations suggest that APC models can be estimated that allow period and cohort effects to be appropriately identified [24–28]. In considering how to interpret effects, the period effect indicates the overall change across time, controlling for age, and cohort variation. The cohort effect indicates how much that magnitude of change varies by birth cohort (averaged across ages). Therefore, a negative cohort effect suggests that period effect magnitude was more negative for that birth cohort compared to the mean of all birth cohorts. We estimated HAPC models of past-year cannabis use, attitudes toward criminalizing use, and attitudes toward supporting legalization, adjusting for the aforementioned covariates. We also conducted stratified analyses for past-year use by sex (controlling for age and education) and by education (controlling for sex and age) to compare with trends in other studies [14–16]. HAPC analyses were conducted in SAS, version 9.4 [29]. Graphs were generated in ggplot2 [30] in R.
Furthermore, we estimated the median odds ratio (MOR) to provide an estimate of effect sizes of period and cohort variation. MOR provides an intuitive measure of group-level effect size [31] and is equal to or greater than one [31,32]. If MOR is one, there is no difference in cannabis use outcomes among individuals in different periods or cohorts. MOR larger than one indicates that the prevalence of cannabis use outcomes differs by period and cohort and that controlling for individual-level covariates, period, and cohort are associated with differences in cannabis use outcome prevalence. The covariance for the MOR indicates the degree of correlation within two individuals from the same birth cohort that is not attributable to individual-level shared risk factors. We used the period and cohort covariance parameters from the HAPC models with the formulae from Merlo et al. to estimate MOR [31].
HAPC models have been criticized as being sensitive to modeling assumptions [33,34], namely that period and cohort effects are governed by mechanisms that are roughly similar between groups and independently operate within groups, and these effects are distributed independently of individual-level regressors [27]. Failure to satisfy these assumptions will result in misleading estimates. Although all regression models are sensitive to modeling assumptions [35], to test our models’ robustness we conducted sensitivity analyses using the Clayton and Schifflers approach for estimating APC effects [36,37], which has been performed on many other data [14,38–42]. In this approach, we estimated a parameter for the linear effect of age and the sum of the linear effects across time of period and cohort effects (termed “drift”). We estimated first and second-derivatives of the drift and regressed them on period and cohort to estimate relative risks for each. We chose 1959 as the reference cohort and 2007 as the reference period because they are the mid-points of each distribution, respectively. Modeling was conducted using “apc.fit” in the “Epi” R package [43].
The analysis was not pre-registered and the results should be considered exploratory.
RESULTS
Approximately 11% of participants reported past-year cannabis use in 2016. Prevalence of past-year cannabis use was highest among 18–22 year-olds and lower in older groups (Fig. 1). Over time, cannabis use decreased in young adults ages 18–35 (25.1%–18.6%) and increased in middle-aged adults ages 36–55 (8.6%–10.1%) and older adults ages 56–79 (0.6%–3.0%). Overall prevalence of past-year use was 13.9% for males and 8.0% for females. By education, overall prevalence of past-year use was 11.7% for those who completed 12th grade and 9.8% for those who did not.
Figure 1.
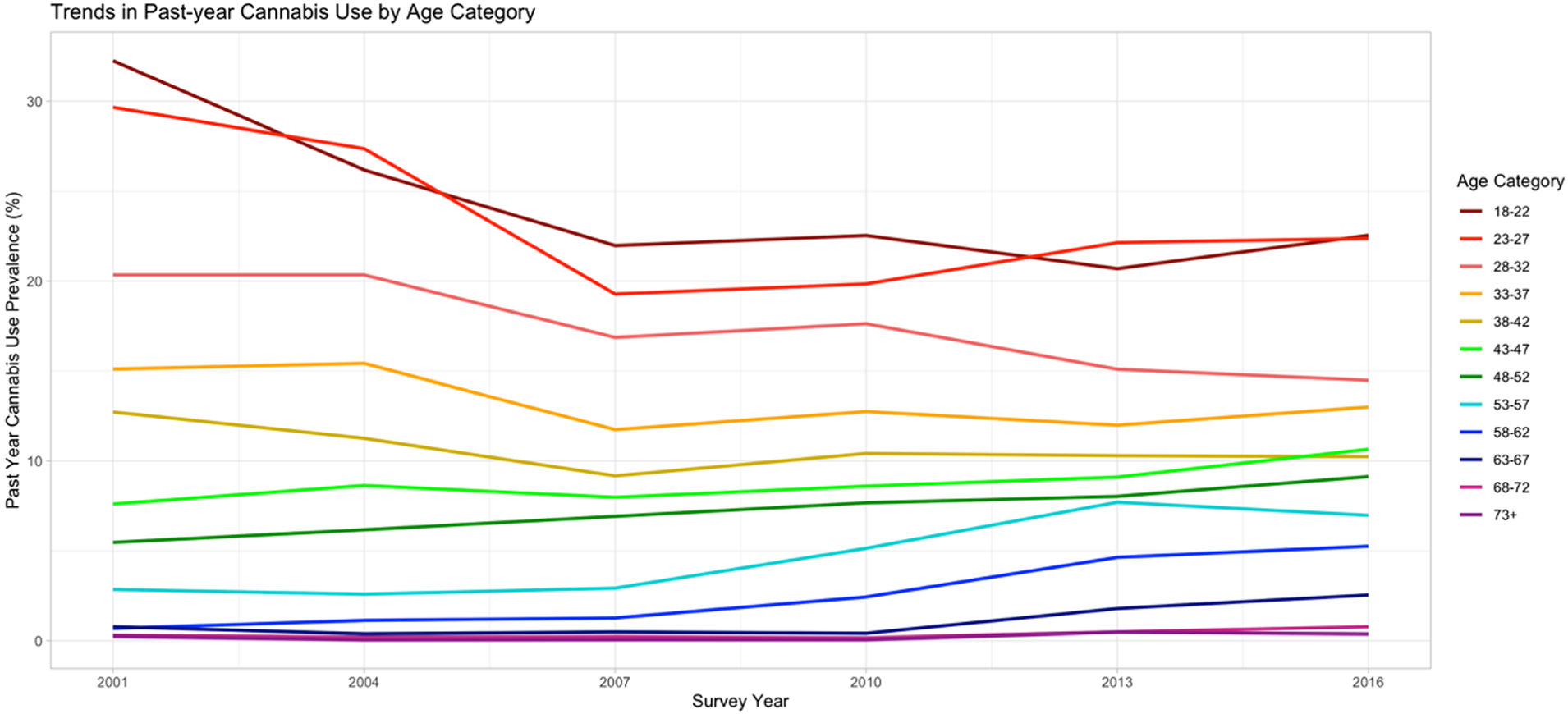
Trends in past-year cannabis use by age group in six waves of the Australian National Drug Strategy Household Survey from 2001–2016
Past-year cannabis use
Figure 2 describes period and cohort effects in cannabis use prevalence (Supporting Information Fig. S1 provides predicted probabilities by age). Overall, there is a positive period effect and a strong negative cohort effect for recent cohorts. Older cohorts had 1.18 (95% CI: [0.88, 1.48]) to 1.41 (95% CI: [1.12, 1.71]) increased log odds of recent cannabis use to the overall mean, but recent cohorts had −2.08 (95% CI: [−2.38, −1.78]) to −2.86 (95% CI: [−3.17, −2.55]) increased log odds to the overall mean.
Figure 2.
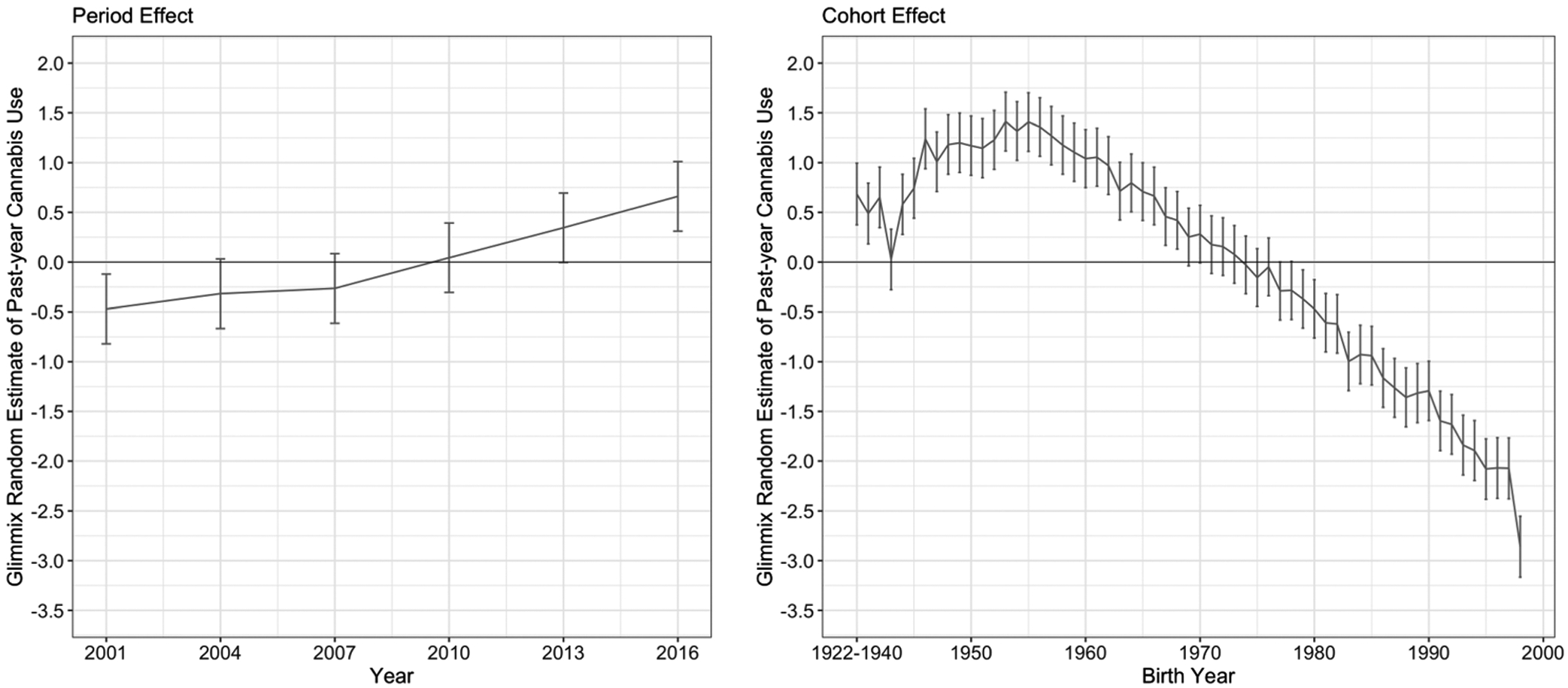
Hierarchical age-period-cohort estimates of period and cohort effects of past-year cannabis use among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016
Table 1 provides the period and cohort effects MOR, overall and by sex and education. The period effect MOR in past-year cannabis use was 1.37 (period covariance = 0.19, 95% CI: [0.07, 1.15]). Therefore, individuals from different periods with shared demographics had a median of 1.37 increased odds of heterogeneous cannabis use compared with individuals in the same period; in short, cannabis use clustered by period independently of individual-level odds of use. The cohort effect MOR in past-year cannabis use was 1.58 (cohort covariance = 1.29, 95% CI: [0.91, 1.95]). Therefore, the heterogeneity between cohorts was 1.58 higher than the individual odds of cannabis use among two individuals randomly chosen from different cohorts. In other words, cohorts shared odds of cannabis use that was not attributed only to individual-level factors. Results for past-year cannabis use were consistent by sex, with an increasing period effect, and declining cohort effect (Fig. 3) and relatively stable MOR (Table 1). However, we observed a larger cohort effect for those who completed 12th grade (Fig. 4), consistent with MOR (MOR = 2.93 vs. MOR = 1.34) and non-overlapping cohort covariance confidence intervals (95% CI: [5.13, 10.92] vs. 95% CI: [0.37, 0.78]).
Table 1.
Median odds ratio for the hierarchical age-period-cohort estimates of period and cohort effects among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
| Outcome | Cohort effect | Period effect | ||||
|---|---|---|---|---|---|---|
| Covariance Parameter Estimate (95% CI) | SE | Median Odds Ratio | Covariance Parameter Estimate (95°% CI) | SE | Median Odds Ratio | |
| Past year cannabis use | 1.29 [0.91, 1.95] | 0.25 | 1.58 | 0.19 [0.07, 1.15] | 0.12 | 1.37 |
| Male | 1.02 [0.72, 1.56] | 0.20 | 1.51 | 0.15 [0.06, 0.89] | 0.09 | 1.32 |
| Female | 1.78 [1.25, 2.75] | 0.35 | 1.72 | 0.25 [0.10, 1.55] | 0.16 | 1.44 |
| Completed 12th grade | 7.22 [5.13, 10.92] | 1.38 | 2.93 | 0.77 [0.30, 4.67] | 0.49 | 1.90 |
| Did not complete 12th grade | 0.52 [0.37, 0.78] | 0.10 | 1.34 | 0.06 [0.02, 0.37] | 0.04 | 1.20 |
| Cannabis use should be a criminal offense | 0.02 [0.02, 0.03] | 0.004 | 1.06 | 0.03 [0.01, 0.18] | 0.02 | 1.14 |
| Support legalization of cannabis | 0.06 [0.04, 0.09] | 0.01 | 1.10 | 0.04 [0.02, 0.26] | 0.03 | 1.17 |
CI = confidence interval; SE = standard error.
Figure 3.
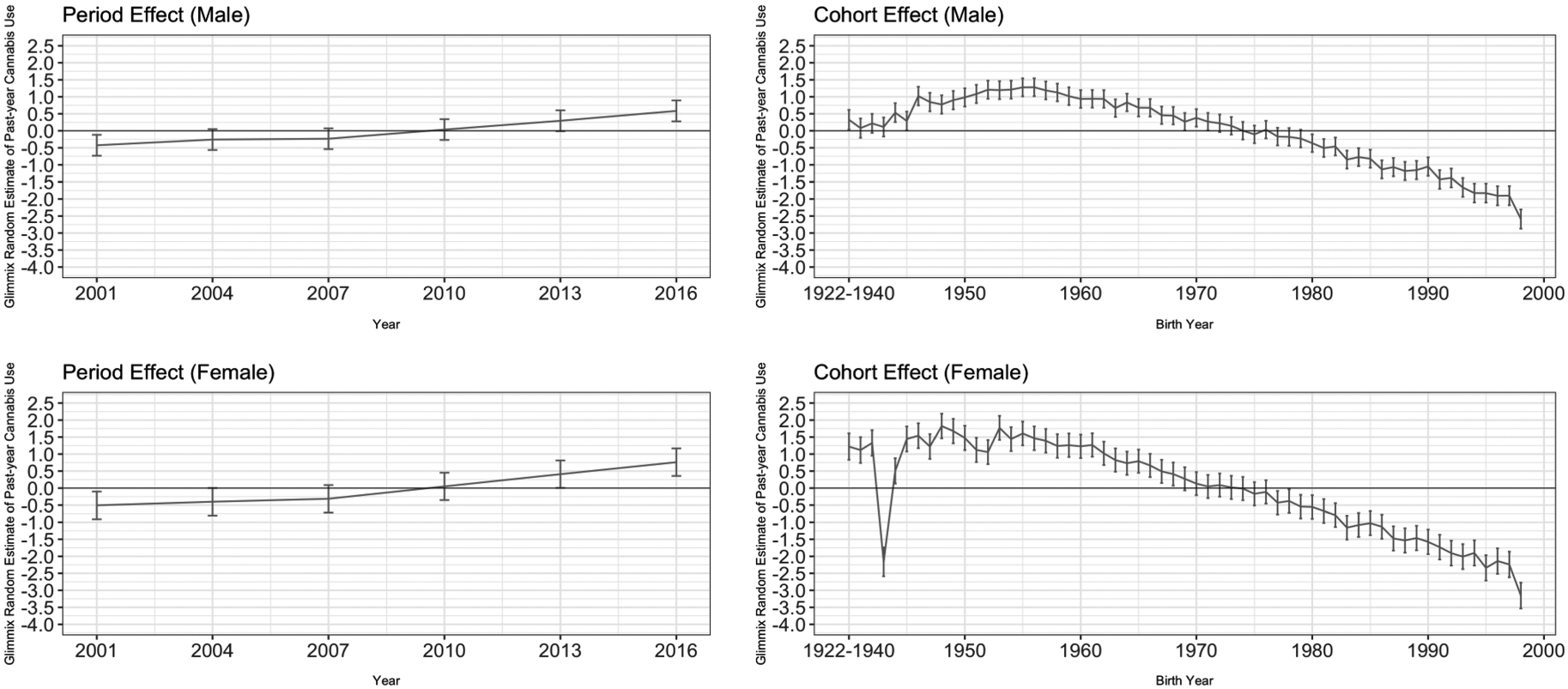
Hierarchical age-period-cohort estimates of period and cohort effects of past-year cannabis use among 18- to 79-year-olds by sex in six waves of the Australian National Drug Strategy Household Survey from 2001–2016
Figure 4.
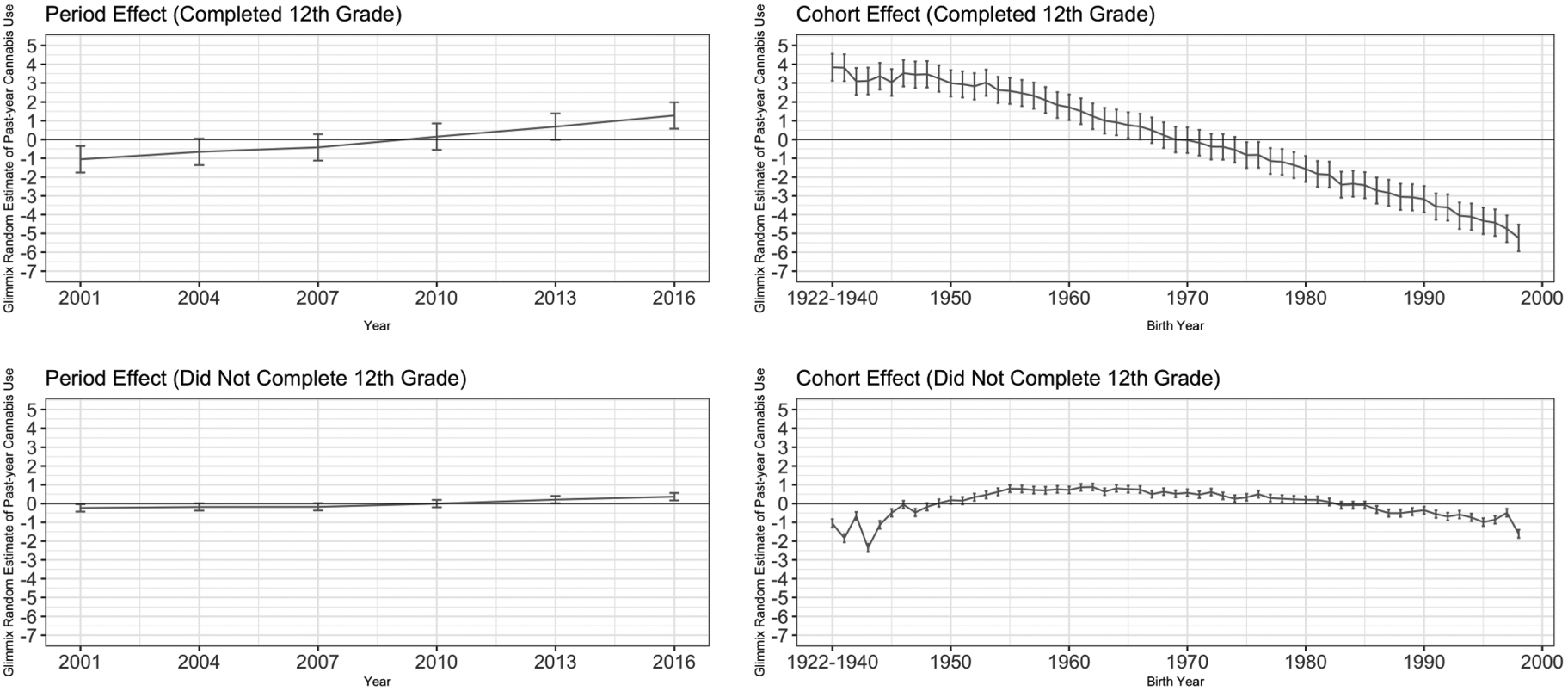
Hierarchical age–period–cohort estimates of period and cohort effects of past-year cannabis use among 18- to 79-year-olds by education in six waves of the Australian National Drug Strategy Household Survey from 2001–2016
Similar to the HAPC method, sensitivity analyses using the Clayton and Schifflers approach [36,37] revealed an increasing period effect in more recent periods and decreasing cohort effect in more recent cohorts, with consistency by sex but varying cohort effects by education (Supporting Information Figs. S2, S3, and S4).
Attitudes toward criminalization
Figure 5 describes period and cohort effects for the prevalence of favoring criminalization. We observed a negative period effect and positive cohort effect for recent cohorts. Whereas older cohorts had −0.08 (95% CI: [−0.12, −0.04]) to −0.22 (95% CI: [−0.26, −0.18]) decreased log odds of favorable attitudes to the overall mean. The most recent cohort had 0.53 (95% CI: [0.50, 0.57]) increased log odds to the overall mean. The period effect MOR was 1.14 (period covariance = 0.03, 95% CI: [0.01, 0.18]), and the cohort effect MOR was 1.06 (cohort covariance = 0.02, 95% CI: [0.02, 0.03]) (Table 1).
Figure 5.
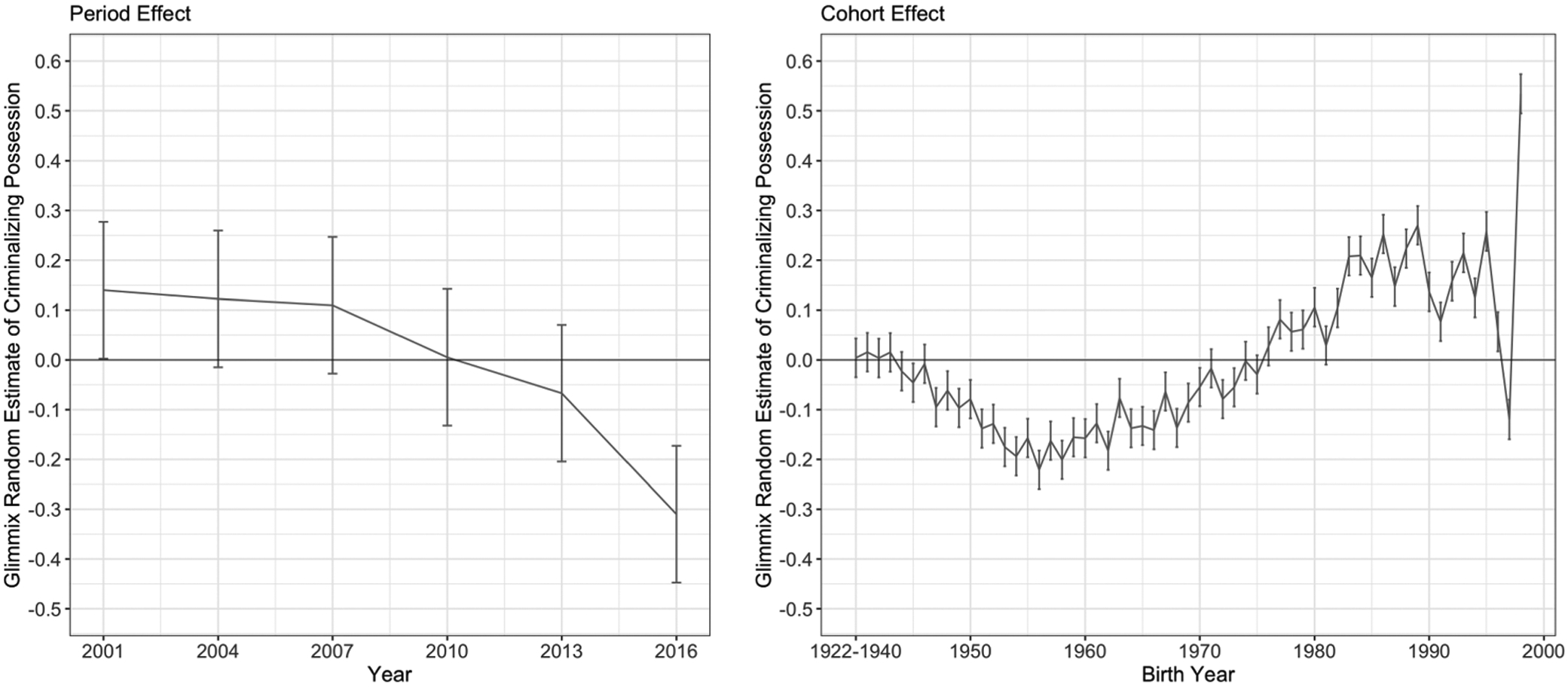
Hierarchical age-period-cohort estimates of period and cohort effects of favorable attitudes toward criminalizing cannabis possession and personal use among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016
Sensitivity analyses also revealed decreasing period effect in more recent periods and increasing cohort effect in more recent cohorts (Supporting information Fig. S5).
Attitudes toward supporting cannabis legalization
Figure 6 describes period and cohort effects for the prevalence of cannabis legalization support. We observed a positive period effect beginning in 2007 and a negative cohort effect for recent cohorts compared to older cohorts, especially those born in the 1950s. Older cohorts had 0.08 (95% CI: [0.01, 0.14]) to 0.35 (95% CI: [0.29, 0.41]) increased log odds of supporting legalization to the overall mean, but the most recent cohort had −0.82 (95% CI: [−0.88, −0.75]) increased log odds to the overall mean. The period effect MOR was 1.17 (period covariance = 0.04, 95% CI: [0.02, 0.26]), and the cohort effect MOR was 1.10 (cohort covariance = 0.06, 95% CI: [0.04, 0.09]) (Table 1).
Figure 6.
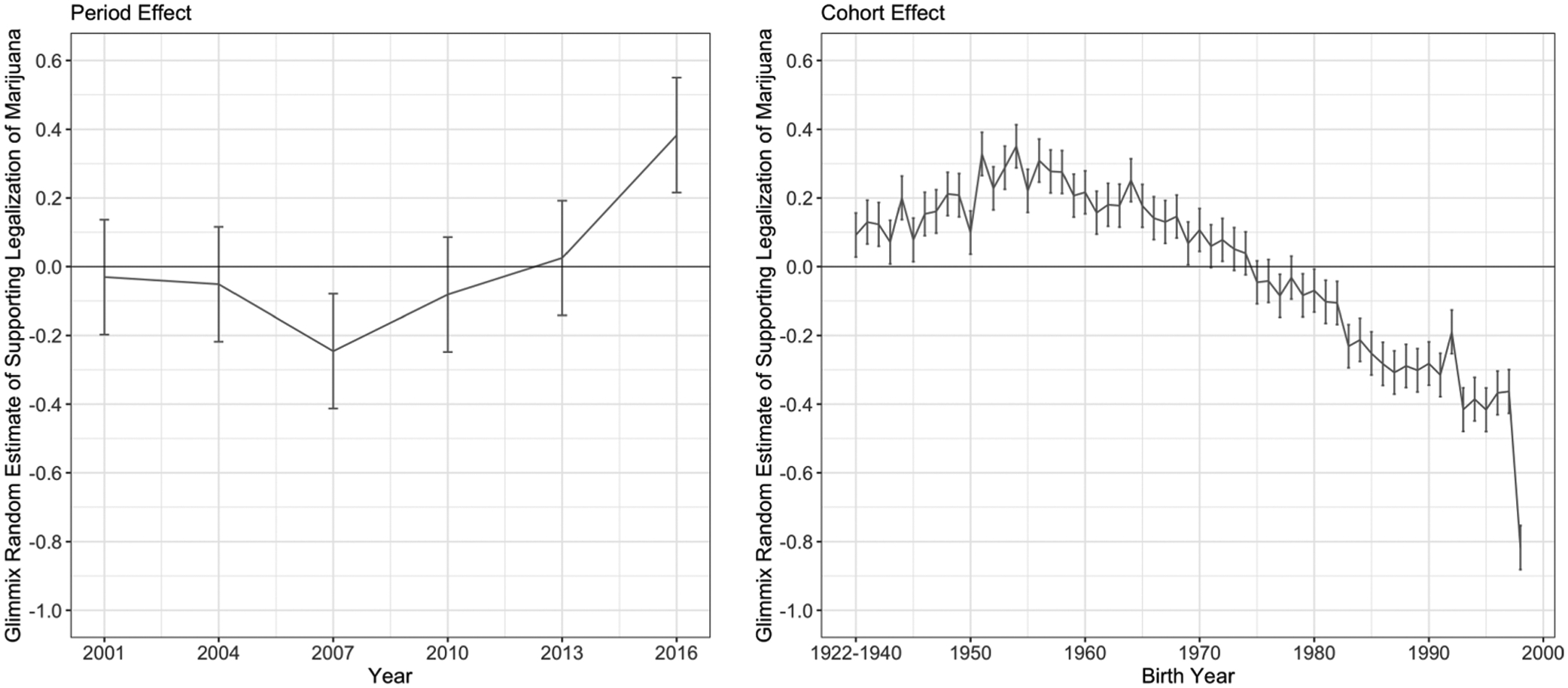
Hierarchical age-period-cohort estimates of period and cohort effects of favorable attitudes toward cannabis legalization among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016
Sensitivity analyses also revealed decreasing period effect in more recent periods and increasing cohort effect in more recent cohorts (Supporting Information Fig. S6).
DISCUSSION
This study is the first to use nationally representative Australian data to examine APC effects of past-year cannabis use and legalization attitudes. We document increasing period effects in past-year use and decreasing cohort effects. These results are consistent with descriptive data indicating mid-life increases in use in Australia. Past-year use increased alongside favorable attitudes toward cannabis, with notable exceptions. We observe declining trends in criminalization support, particularly among 1950s and 1960s birth cohorts, with more restrictive attitudes among recent cohorts, although the cohort effect levels off after 1990. We also see increases in legalization support since 2007. However, recent cohorts’ legalization support was lower than mid-20th century cohorts.
These results are similar to APC effects observed in other countries. US studies found an increasing period effect for past use in later survey years, especially among mid-20th century birth cohorts [12,13], with the strongest cohort effect for past-month use observed among the 1950 cohort [12]. Similarly, cannabis use increased dramatically in cohorts born post-1945 compared to pre-1945 [13]. These results are consistent with a historical liberalization of cannabis use in the 1960s–1970s across countries, including the United States [44], the United Kingdom [45], Canada [46], and Australia [47], coinciding with these cohorts’ transition into young adulthood. Our results also indicate that these cohorts decreasingly favored criminalization and increasingly supported legalization, consistent with increasing use among Australian youth in the 1970s [47]. In sum, our results along with the aforementioned studies indicate that as people born in the mid-20th century entered adulthood, their rates of cannabis use and legalization support increased, in an overall political environment that favored decriminalization.
Other results from our study also support existing findings. Our subgroup analysis of past-year cannabis use indicates little variation in period and cohort effects by sex; given that gender differences in cannabis use has been declining in recent cohorts [9,15], these data indicate that period and cohort effects are similar within gender groups, suggesting that convergence in gender differences are potentially because of slope acceleration in the cohort effect rather than qualitative differences in period and cohort effects. Analyses focused on testing potential gender by cohort interactions are an important next step. We observed stronger positive period effects and stronger negative cohort effects among those who completed 12th grade, suggesting that past-year cannabis use is increasing faster in this group, but the magnitude of increase is not as strong among the youngest cohorts. The minimal period and cohort effect among those who did not complete 12th grade is consistent with an Australian study that found that frequent cannabis use rates have remained unchanged in this group [20]. Therefore, our results along with other studies [20,48] suggest that educational attainment may differentially predict trends in cannabis use. In addition, we found a positive period effect for cannabis legalization support, consistent with two US studies [17,18]. However, we found a negative cohort effect for recent cohorts, whereas the aforementioned studies found minimal cohort effect [17,18]. The reasons why cannabis use is declining in younger cohorts remain unknown but is a pattern observed for other substances such as alcohol [49], and externalizing behaviors such as deviance and crime [50], suggesting that cannabis use patterns can be generalized to other behaviors. As trends in cannabis use continue being uncovered, assessing commonality in risk factors for other substance use is critical.
These results suggest a dismantling of the expected parallel relationship between cannabis use and legalization attitudes. We observe decreasing past-year use among young adults and increasing legalization support, albeit a slower increase than among older adults. This is consistent with US data that show increases in adolescent cannabis use have not accompanied rapid decreases in risk perception, signaling discordance portending increases in adolescent use over time [8]. Less restrictive attitudes may foreshadow future increases in use, especially within the context of other substance use trends. Historically, alcohol [51,52] and tobacco use [52] have been associated with an increased risk for subsequent cannabis use. However, alcohol and tobacco use are declining in Australia [1] and, therefore, adolescents have lower risk for cannabis use initiation. This may reflect the dampening of potential cannabis use increases that would have occurred if alcohol and tobacco use increased [53]. Nevertheless, as attitudes toward cannabis become favorable and availability increases [4,6], decreases in tobacco and alcohol use may be insufficient in decreasing youth cannabis use. Although cannabis decriminalization may have social benefits such as decreased drug-related arrests [54,55], assessment of potential relationships between increased availability and increased harms associated with use is critical. For example, data from the United States indicate that MCL and dispensaries were associated with traffic fatality reduction [56]. However, MCL have also been associated with increased risk of cannabis use disorder [57,58] and their associations with reducing prescription opioid mortality have been inconsistent and inconclusive [59].
Our study has several limitations. We used cross-sectional surveys and did not have longitudinal information on the life course of individuals from varying birth cohorts, which is ideal for HAPC modeling. The data are also self-reported and, therefore, may be susceptible to recall and reporting bias. The survey instrument experienced slight wording changes over time, leading to possible inconsistencies in question interpretations. Although alternative explanations for the large cohort covariance for 12th grade completion are possible, we did not have sufficient information for different educational cut-points to test alternative hypotheses. It is also possible that other concurrent trends not addressed in this study may affect cannabis use trends. Standard errors for cross-classified random effects models did not incorporate the complex survey design weights, which may affect confidence interval ranges. Last, high-risk populations, such as incarcerated or homeless individuals, were not reached in the household survey and were excluded.
The ever-changing landscape of cannabis legalization and availability necessitate the monitoring of changes in use and attitudes toward legalization. This study provides evidence that although variance in past-year cannabis use prevalence is increasing over time, prevalence is decreasing among recent cohorts. Variance in legalization support prevalence is also increasing, signaling discordance between use and attitudes among young adults portending a rise in use in this group as cannabis becomes increasingly legalized.
Supplementary Material
Figure S1 Prevalence and predicted probability of past-year cannabis use by age in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S2 Sensitivity analysis of age-period-cohort estimates of past-year cannabis use among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S3 Sensitivity analysis of age-period-cohort estimates of past-year cannabis use among 18- to 79-year-olds by sex in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S4 Sensitivity analysis of age-period-cohort estimates of past-year cannabis use among 18- to 79-year-olds by education in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S5 Sensitivity analysis of age-period-cohort estimates of attitudes toward criminalizing cannabis possession and personal use among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S6 Sensitivity analysis of age-period-cohort t estimates of favorable attitudes toward cannabis legalization among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Footnotes
Declaration of interests
None.
Supporting Information
Additional supporting information may be found online in the Supporting Information section at the end of the article.
References
- 1.Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2016: Detailed Findings Canberra; 2017. https://www.aihw.gov.au/getmedia/15db8c15-7062-4cde-bfa4-3c2079f30af3/21028a.pdf.aspx?inline=true
- 2.DISA Global Solutions. Map of Marijuana Legality by State. 2019. Available at: https://disa.com/map-of-marijuana-legality-by-state (accessed 11 October 2019).
- 3.Minister of Justice. Cannabis Act. Canada; 2019. https://laws-lois.justice.gc.ca/PDF/C-24.5.pdf [Google Scholar]
- 4.Hughes C The Australian (illicit) drug policy timeline: 1985–2016. 2016. Available at: http://dpmp.unsw.edu.au/resource/drug-policy-timeline
- 5.Ritter A, Sotade O Explaining the declining rates of past year cannabis use in Australia: a first pass. Drug Alcohol Rev 2017; 36: 602–8. 10.1111/dar.12553 [DOI] [PubMed] [Google Scholar]
- 6.Kwai I In a First for Australia, the Capital Legalizes Recreational Marijuana. New York Times. https://www.nytimes.com/2019/09/25/world/australia/marijuana-cannabis-recreational-legal.html. Published September 25, 2019. [Google Scholar]
- 7.Mauro PM, Santaella-Tenorio J, Perlmutter AS, Hasin DS, Mauro CM, Martins SS Correct knowledge of medical cannabis legal status in one’s own state: differences between adolescents and adults in the United States, 2004–2013. Addict Behav 2019; 88: 23–8. 10.1016/j.addbeh.2018.07.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sarvet AL, Wall MM, Keyes KM, Cerdá M, Schulenberg JE, O’Malley PM, et al. Recent rapid decrease in adolescents’ perception that marijuana is harmful, but no concurrent increase in use. Drug Alcohol Depend 2018; 186: 68–74. 10.1016/j.drugalcdep.2017.12.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kerr WC, Greenfield TK, Bond J, Ye Y, Rehm J Age-period-cohort influences on trends in past year marijuana use in the US from the 1984, 1990, 1995 and 2000 National Alcohol Surveys. Drug Alcohol Depend 2007; 86: 132–8. 10.1016/j.drugalcdep.2006.05.022 [DOI] [PubMed] [Google Scholar]
- 10.Miech R, Koester S Trends in U.S., past-year marijuana use from 1985 to 2009: an age-period-cohort analysis. Drug Alcohol Depend 2012; 124: 259–67. 10.1016/j.drugalcdep.2012.01.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Han BH, Palamar JJ Marijuana use by middle-aged and older adults in the United States, 2015–2016. Drug Alcohol Depend 2018; 191: 374–81. 10.1016/j.drugalcdep.2018.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chawla D, Yang YC, Desrosiers TA, Westreich DJ, Olshan AF, Daniels JL Past-month cannabis use among U.S. individuals from 2002–2015: an age-period-cohort analysis. Physiol Behav 2018; 193: 177–82. 10.1016/j.drugalcdep.2018.05.03 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kerr WC, Lui C, Ye Y Trends and age, period and cohort effects for marijuana use prevalence in the 1984–2015 US National Alcohol Surveys. Addiction 2018; 113: 473–81. 10.1111/add.14031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hamilton AD, Jang JB, Patrick ME, Schulenberg JE, Keyes KM Age, period and cohort effects in frequent cannabis use among US students: 1991–2018. Addiction 2019; 114: 1763–72. 10.1111/add.14665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chapman C, Slade T, Swift W, Keyes K, Tonks Z, Teesson M Evidence for sex convergence in prevalence of cannabis use: a systematic review and meta-regression. J Stud Alcohol Drugs 2017; 78: 344–52. 10.15288/jsad.2017.78.344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Piontek D, Kraus L, Pabst A, Legleye S An age-period-cohort analysis of cannabis use prevalence and frequency in Germany, 1990–2009. J Epidemiol Community Health 2012; 66: 908–13. 10.1136/jech-2011-200180 [DOI] [PubMed] [Google Scholar]
- 17.Campbell W, Twenge J, Carter N Support for marijuana (cannabis) legalization: untangling age, period, and cohort effects. Coll Psychol 2017; 3: 1–9. 10.1525/collabra.45 [DOI] [Google Scholar]
- 18.Schwadel P, Ellison CG Period and cohort changes in Americans’ support for marijuana legalization: convergence and divergence across social groups. Sociol Q 2017; 58: 405–28. 10.1080/00380253.2017.1331715 [DOI] [Google Scholar]
- 19.Roxburgh A, Hall WD, Degenhardt L, McLaren J, Black E, Copeland J, et al. The epidemiology of cannabis use and cannabis-related harm in Australia 1993–2007. Addiction 2010; 105: 1071–9. 10.1111/j.1360-0443.2010.02903.x [DOI] [PubMed] [Google Scholar]
- 20.Chan GCK, Leung J, Quinn C, Weier M, Hall W Socio-economic differentials in cannabis use trends in Australia. Addiction 2017; 113: 454–61. 10.1111/add.14010 [DOI] [PubMed] [Google Scholar]
- 21.Roy Morgan Research. National Drug Strategy Household Survey 2004-Technical Report. Melbourne; 2005. [Google Scholar]
- 22.Australian Institute of Health and Welfare. National Drug Strategy Household Survey. 2019. Available at: https://www.aihw.gov.au/about-our-data/our-data-collections/national-drug-strategyhousehold-survey (accessed 10 October 2019).
- 23.Australian Institute of Health and Welfare. National Drug Strategy Household Survey Report 2010. Canberra; 2011. [Google Scholar]
- 24.Yang Y, Fu WJ, Land KC A methodological comparison of age-period-cohort models: the intrinsic estimator and conventional generalized linear models. Soc Methodol 2004; 34: 75–110. 10.1111/j.0081-1750.2004.00148.x [DOI] [Google Scholar]
- 25.Yang Y Bayesian inference for hierarchical age-period-cohort models of repeated cross-section survey data. Soc Meth 2006; 36: 39–74. [Google Scholar]
- 26.Yang Y, Land KC A mixed models approach to the age-period-cohort analysis of repeated cross-section surveys, with an application to data on trends in verbal test scores. Soc Meth 2006; 36: 75–97. 10.1111/j.1467-9531.2006.00175.x [DOI] [Google Scholar]
- 27.Yang Y, Land KC Age-period-cohort analysis of repeated cross-section surveys fixed or random effects? Soc Met Res 2008; 36: 297–326. [Google Scholar]
- 28.Yang Y, Land KC Mixed Effects Models: Hierarchical APC-Cross- Classified Random Effects Models (HAPC-CCREM), Part I: The Basics. In: Keiding N, Morgan BJT, Wikle CK, van der Heijden P, editors. Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications. Boca Raton, FL: CRC Press; 2013, pp. 191–230. [Google Scholar]
- 29.SAS Institute Inc. SAS [computer program]. Version 9.4 2014.
- 30.Wickham H, Chang W ggplot2 2.1.0. Documentation 2014. Available at: http://ggplot.yhathq.com/
- 31.Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health 2006; 60: 290–7. 10.1136/jech.2004.029454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Larsen K, Merlo J Appropriate assessment of neighborhood effects on individual health: integrating random and fixed effects in multilevel logistic regression. Am J Epidemiol 2005; 161: 81–8. 10.1093/aje/kwi017 [DOI] [PubMed] [Google Scholar]
- 33.Bell A, Jones K Don’t birth cohorts matter? A commentary and simulation exercise onReither, Hauser, and Yang’s (2009) age-period-cohort study ofobesity. Soc Sci Med 2014; 101: 176–80. 10.1016/j.socscimed.2013.09.004 [DOI] [PubMed] [Google Scholar]
- 34.Bell A, Jones K The hierarchical age-period-cohort model: why does it find the results that it finds? Qual Quant 2018; 52: 783–99. 10.1007/s11135-017-0488-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Reither EN, Land KC, Jeon SY, Powers DA, Masters RK, Zheng H, et al. Clarifying hierarchical age-period-cohort models: a rejoinder to Bell and Jones. Soc Sci Med 2015; 145: 125–8. 10.1016/j.socscimed.2015.07.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Clayton D, Schifflers E Models for temporal variation in cancer rates. I: Age–period–cohort models Stat Med 1987; 6: 449–67. 10.1002/sim.4780060405 [DOI] [PubMed] [Google Scholar]
- 37.Clayton D, Schifflers E Models for temporal variation in cancer rates. II: Age–period–cohort models Stat Med 1987; 6: 469–81. 10.1002/sim.4780060406 [DOI] [PubMed] [Google Scholar]
- 38.Ananth CV, Friedman AM, Keyes KM, Lavery JA, Hamilton A, Wright JD Primary and repeat cesarean deliveries: a population-based study in the United States, 1979–2010. Epidemiology 2017; 28: 567–74. 10.1097/EDE.0000000000000658 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Jang JB, Patrick ME, Keyes KM, Hamilton AD, Schulenberg JE Frequent binge drinking among US adolescents, 1991 to 2015. Pediatrics 2017; 139. 10.1542/peds.2016-4023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Keyes KM, Ananth CV Age, period, and cohort effects in perinatal epidemiology: implications and considerations. Paediatr Perinat Epidemiol 2014; 28: 277–9. 10.1111/ppe.12129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Keyes KM, Maslowsky J, Hamilton A, Schulenberg J The great sleep recession: changes in sleep duration among US adolescents, 1991–2012. Pediatrics 2015; 135: 460–8. 10.1542/peds.2014-2707 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Keyes KM, Rutherford C, Hamilton A, Palamar JJ Age, period, and cohort effects in synthetic cannabinoid use among US adolescents, 2011–2015. Drug Alcohol Depend 2016; 166: 159–67. 10.1016/j.drugalcdep.2016.07.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.R Core Team. The R Project for Statistical Computing. https://www.r-project.org. Published 2019. Accessed December 13, 2019.
- 44.US Commission on Marihuana and Drug Abuse [Shaffer Commission]. Marihuana: A Signal of Misunderstanding. the Technical Papers of the First Report of the National Commission on Marihuana and Drug Abuse. Washington, DC; 1972. [Google Scholar]
- 45.Advisory Committee on Drug Dependence. Cannabis [The Wootton Report]. London; 1968. [Google Scholar]
- 46.Commission of Inquiry into the Non-Medical Use of Drugs [Le Dain Commission]. Report of the Canadian Government Commission of Inquiry into the Non-Medical Use of Drugs. Ottawa, Canada; 1972. 10.1037/h0082207 [DOI] [Google Scholar]
- 47.Hall WD The contribution of research to the development of a national cannabis policy in Australia. Addiction 2008; 103: 712–20. 10.1111/j.1360-0443.2008.02169.x [DOI] [PubMed] [Google Scholar]
- 48.Silins E, Fergusson DM, Patton GC, Horwood LJ, Olsson CA, Hutchinson DM, et al. Adolescent substance use and educational attainment: an integrative data analysis comparing cannabis and alcohol from three Australasian cohorts. Drug Alcohol Depend 2015; 156: 90–6. 10.1016/j.drugalcdep.2015.08.034 [DOI] [PubMed] [Google Scholar]
- 49.Livingston M, Raninen J, Slade T, Swift W, Lloyd B, Dietze P Understanding trends in australian alcohol consumption—an age-period-cohort model. Addiction 2016; 111: 1590–8. 10.1111/add.13396 [DOI] [PubMed] [Google Scholar]
- 50.Keyes KM, Gary DS, Beardslee J, Prins SJ, O’Malley PM, Rutherford C, et al. Joint effects of age, period, and cohort on conduct problems among American adolescents from 1991 through 2015. Am J Epidemiol 2018; 187: 548–57. 10.1093/aje/kwx268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Wagner FA, Anthony JC Into the world of illegal drug use: exposure opportunity and other mechanisms linking the use of alcohol, tobacco, marijuana, and cocaine. Am J Epidemiol 2002; 155: 918–25. 10.1093/aje/155.10.918 [DOI] [PubMed] [Google Scholar]
- 52.Nelson SE, van Ryzin MJ, Dishion TJ Alcohol, marijuana, and tobacco use trajectories from age 12 to 24 years: demographic correlates and young adult substance use problems. Dev Psychopathol 2014; 27: 253–77. 10.1017/S0954579414000650 [DOI] [PubMed] [Google Scholar]
- 53.Miech R, Johnston L, O’Malley PM Prevalence and attitudes regarding marijuana use among adolescents over the past decade. Pediatrics 2017; 140. 10.1542/peds.2017-0982 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Firth CL, Maher JE, Dilley JA, Darnell A, Lovrich NP Did marijuana legalization in Washington state reduce racial disparities in adult marijuana arrests? Subst Use Misuse 2019; 54: 1582–7. 10.1080/10826084.2019.1593007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Plunk AD, Peglow SL, Harrell PT, Grucza RA Youth and adult arrests for cannabis possession after decriminalization and legalization of cannabis. JAMA Pediatr 2019; 173: 763–9. 10.1001/jamapediatrics.2019.1539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Santaella-Tenorio J, Mauro CM, Wall MM, Kim JH, Cerdá M, Keyes KM, et al. US traffic fatalities, 1985–2014, and their relationship to medical marijuana laws. Am J Public Health 2017; 107: 336–42. 10.2105/AJPH.2016.303577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hasin DS, Sarvet AL, Cerdá M, Keyes KM, Stohl M, Galea S, et al. US adult illicit cannabis use, cannabis use disorder, and medical marijuana laws: 1991–1992 to 2012–2013. JAMA Psychiat 2017; 74: 579–88. 10.1001/jamapsychiatry.2017.0724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Cerdá M, Mauro C, Hamilton A, Levy NS, Santaella- Tenorio J, Hasin D, et al. Association between recreational marijuana legalization in the United States and changes in marijuana use and cannabis use disorder from 2008 to 2016. JAMA Psychiat 2019; 77: 165–71. 10.1001/jamapsychiatry.2019.3254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Chihuri S, Li G State marijuana laws and opioid overdose mortality. Inj Epidemiol 2019; 6. 10.1186/s40621-019-0213-z [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Prevalence and predicted probability of past-year cannabis use by age in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S2 Sensitivity analysis of age-period-cohort estimates of past-year cannabis use among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S3 Sensitivity analysis of age-period-cohort estimates of past-year cannabis use among 18- to 79-year-olds by sex in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S4 Sensitivity analysis of age-period-cohort estimates of past-year cannabis use among 18- to 79-year-olds by education in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S5 Sensitivity analysis of age-period-cohort estimates of attitudes toward criminalizing cannabis possession and personal use among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.
Figure S6 Sensitivity analysis of age-period-cohort t estimates of favorable attitudes toward cannabis legalization among 18- to 79-year-olds in six waves of the Australian National Drug Strategy Household Survey from 2001–2016.