

Dear Editor,
Several skin lesions have been associated with COVID‐19, some of them classically related to other microbiological agents. 1 Recently, positivity for SARS‐CoV/SARS‐CoV‐2 virus spike protein has been reported by immunohistochemistry (IHC) in skin biopsies from patients with erythema multiforme‐like lesions or chilblains associated with COVID‐19. 2 , 3 Granuloma annulare (GA) can be triggered by different viruses such as the Epstein‐Barr virus (EBV), HIV, and hepatitis B and C. 4 Previously, we reported one patient with localized GA triggered after a SARS‐CoV‐2 infection. 5 Additionally, immunohistochemical staining and reverse transcription polymerase chain reaction (RT‐PCR) techniques for SARS‐CoV‐2 detection were carried out on skin biopsy, in order to expand the knowledge about the etiopathogenic role of the virus in this associated skin manifestation.
A 53‐year‐old female presented with an annular lesion on the second finger of her left hand and a papule on the knuckle of the same finger (Figure S1). She worked in a nursing home with COVID‐19 cases. Coinciding with the appearance of the lesions, the patient referred anosmia, dysgeusia, and cephalalgia. At that time, a nasopharyngeal RT‐PCR for SARS‐CoV‐2 was carried out, which was positive.
A month after the patient started with the cutaneous symptoms, she attended a dermatology appointment and skin biopsies of both lesions were performed. The histopathology revealed findings compatible with GA (Figure 1A). Serological tests were carried out, which were positive for SARS‐CoV‐2 IgG.
FIGURE 1.
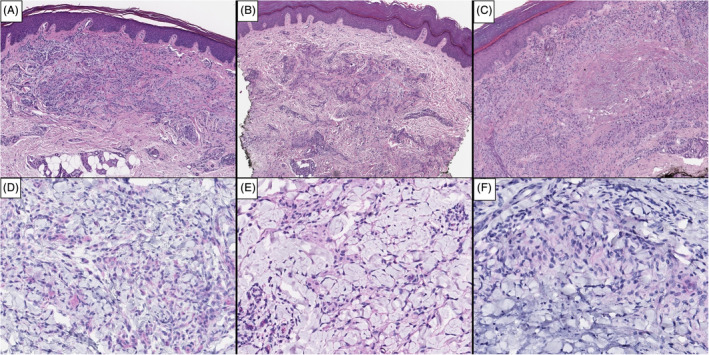
Immunohistochemical staining of granuloma annulare in biopsies from pre and post‐COVID‐19 patients. HE ×4 (A: Patient; B: Control‐1; C: Control‐2): at low power view, the three biopsies show the same type of lesion, with granulomatous pattern and necrobiotic changes. SARS‐CoV IHC ×20 (D: Patient; E: Control‐1; F: Control‐2): the three biopsies show red magenta granular deposits in the cytoplasm of histiocytes and giant cells within the infiltrate
For SARS‐CoV‐2 immunostains, we used a commercially available antibody against both SARS‐CoV spike and SARS‐CoV‐2 spike proteins (S2 subunit) (SARS‐CoV/SARS‐CoV‐2 spike 1A9; GeneTex, Inc., Irvine, California). The staining was optimized in our laboratory, using HRP Magenta as a chromogen system for IHC visualization on Dako Omnis. For SARS‐CoV‐2 RT‐PCR, a fresh skin biopsy (immersed in physiological saline medium) was sent for virological investigation to the Respiratory Virus and Influenza Unit of the National Microbiology Center (ISCIII, Madrid, Spain). The biopsy was processed within 24 hours after reception. RNA from skin tissue was extracted by using the QIAamp Mini Elute Virus spin kit in an automated extractor (QIAcube, Qiagen, Valencia, California). Detection of SARS‐CoV‐2 was performed by multiplex RT‐PCR real time assays based on published RT‐PCRs designed for E and N genes. 6
As negative controls, we selected two granuloma annulare biopsies performed during the months of January and February 2019, when the COVID‐19 pandemic was not yet a reality. The negative control‐1 corresponds to a granuloma annulare located on the back of the foot in an asymptomatic 55‐year‐old woman. The negative control‐2 corresponds to a granuloma annulare located on the back of the second finger of the hand in an asymptomatic 60‐year‐old woman.
Viral spike protein is considered to be detected by conventional IHC as fine‐to‐coarse, bright red granular deposits in the cytoplasm of cutaneous dermal vessels and eccrine cells (both secretory and excretory). 7 In our patient, the same pattern of positivity was found in the cytoplasm of granuloma annulare hystiocites (Figure 1D). Similar results were observed in both negative controls (Figure 1E,F). The parallelism between the SARS‐CoV‐2 immunostaining in our patient and the two control specimens could be due to a lack of specificity against SARS‐CoV spike and SARS‐CoV‐2 spike proteins with the stains used, requiring a careful interpretation to avoid false positive results. 8
SARS‐CoV‐2 specific RT‐PCR performed in skin biopsy specimen was negative. This result defends that the pathogenesis and appearance of granuloma annulare in our patient could be explained by an indirect effect after the activation and response of the immune system induced by the SARS‐CoV‐2 virus rather than by the direct role of the virus on the skin lesion.
Since there are many cutaneous manifestations related to the SARS‐CoV‐2 virus, 1 but their etiopathogenic mechanisms remain unexplained, further investigations with new, more specific immunohistochemical stains and specific RT‐PCR techniques on skin biopsies will be necessary to better understand the relationship between the SARS‐CoV‐2 virus and all its associated skin manifestations.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
AUTHORS CONTRIBUTION
The authors contributed to the conception, design, data collection, analysis and interpretation of data, writing, review, and approval of the manuscript.
Supporting information
Figure S1 Clinical image of granuloma annulare. Annular plaque on the second finger of the left hand and a papule on the knuckle of the same finger
{kind=link}
ACKNOWLEDGMENT
The patients in this manuscript have given written informed consent to publication of their case details. This research received no specific grant from any funding agency in the public, commercial or not‐for‐profit sectors.
DATA AVAILABILITY STATEMENT
The authors confirm that the data supporting the findings of this study are available within the article.
REFERENCES
- 1. Galván Casas C, Català A, Carretero Hernández G, et al. Classification of the cutaneous manifestations of COVID‐19: a rapid prospective nationwide consensus study in Spain with 375 cases. Br J Dermatol. 2020;183(1):71‐77. 10.1111/bjd.19163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Colmenero I, Santonja C, Alonso‐Riaño M, et al. SARS‐CoV‐2 endothelial infection causes COVID‐19 chilblains: histopathological, immunohistochemical and ultrastructural study of seven paediatric cases. Br J Dermatol. 2020;183:729‐737. 10.1111/bjd.19327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Torrelo A, Andina D, Santonja C, et al. Erythema multiforme‐like lesions in children and COVID‐19. Pediatr Dermatol. 2020;37(3):442‐446. 10.1111/pde.14246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Piette EW, Rosenbach M. Granuloma annulare: pathogenesis, disease associations and triggers, and therapeutic options. J Am Acad Dermatol. 2016;75(3):467‐479. 10.1016/j.jaad.2015.03.055. [DOI] [PubMed] [Google Scholar]
- 5. García‐Gil MF, Monte Serrano J, García García M, Matovelle Ochoa C, Ara‐Martín M. Granuloma annulare triggered by SARS‐CoV‐2 infection. The first reported case. J Dermatol. 2020;48:e1‐e2. 10.1111/1346-8138.15594. [DOI] [PubMed] [Google Scholar]
- 6. Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019‐nCoV) by real‐time RT‐PCR. Euro Surveill. 2020;25(3):2000045. 10.2807/1560-7917.ES.2020.25.3.2000045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Santonja C, Heras F, Núñez L, Requena L. COVID‐19 chilblain‐like lesion: immunohistochemical demonstration of SARS‐CoV‐2 spike protein in blood vessel endothelium and sweat gland epithelium in a polymerase chain reaction‐negative patient. Br J Dermatol. 2020;183(4):778‐780. 10.1111/bjd.19338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Baeck M, Hoton D, Marot L, Herman A. Chilblains and COVID‐19: why SARS‐CoV‐2 endothelial infection is questioned. Br J Dermatol. 2020;183:1152‐1153. 10.1111/bjd.19489. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Clinical image of granuloma annulare. Annular plaque on the second finger of the left hand and a papule on the knuckle of the same finger
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.