

Abstract
Background
Case detection underestimates the burden of the COVID‐19 pandemic. Following the first COVID‐19 wave, we estimated the seroprevalence of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) among blood donors across Canada.
Study Design and Methods
This serial cross‐sectional study was conducted between May 9 and July 21, 2020 from blood donors donating at all Canadian Blood Services locations. We used the Abbott Architect assay to detect SARS‐CoV‐2 IgG antibodies from retention plasma. Seroprevalence was standardized to population‐level demographics and assay characteristics were adjusted using the Rogan‐Gladen equation. Results were stratified by region, age, ethnicity, ABO groups, and quantiles of material and social deprivation indices. Temporal trends were evaluated at 2‐week intervals. Univariate and multivariate logistic regression compared SARS‐CoV‐2 reactive to non‐reactive donors by sociodemographic variables.
Results
Overall 552/74642 donors, had detectable antibodies, adjusted seroprevalence was 7.0/1000 donors (95% CI; 6.3, 7.6). Prevalence was differential by geography, Ontario had the highest rate, 8.8/1000 donors (7.8, 9.8), compared to the Atlantic region 4.5/1000 donors (2.6, 6.4); adjusted odds ratio (aOR) 2.2 (1.5, 3.3). Donors that self‐identified as an ethnic minority were more likely than white donors to be sero‐reactive aOR 1.5 (1.2, 1.9). No temporal trends were observed.
Discussion
Worldwide, blood services have leveraged their operational capacity to inform public health. While >99% of Canadians did not show humoral evidence of past infection, we found regional variability and disparities by ethnicity. Seroprevalence studies will continue to play a pivotal role in evaluating public health policies by identifying trends and monitor disparities.
Keywords: blood donors, Canada, COVID‐19, SARS‐CoV‐2 seroprevalence
1. INTRODUCTION
Early in the pandemic, strict public health policies were implemented by provinces and territories across Canada to mitigate and contain the spread of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). 1 As a result, the first COVID‐19 wave peaked by late April and new infections and restrictions subsided by July. Consistent with many countries, after a period of relative inactivity, an upsurge of COVID‐19 cases began in late September, and as of November 2, 2020, Canada had a cumulative total of 236,841 cases recorded (6300 cases per million population). 2
Yet case detection by symptomatic testing or through contact tracing, reflects only a fraction of people exposed to SARS‐CoV‐2. Prevalence derived solely by case detection is underestimated by testing capacity/ restricted eligibility criteria, limitations in contact tracing, and missing cases among the asymptomatic, mildly symptomatic or people who never sought testing. 3 , 4 In contrast to diagnostic testing, seroprevalence studies aim to identify the proportion of a population ever exposed to SARS‐CoV‐2, independent of symptoms. This provides a more comprehensive representation of the burden of disease and population‐level immunity. As the pandemic continues, these studies will play a pivotal role in helping public health authorities assess policies, herd immunity, determine health capacity, procure adequate doses of vaccines, and coordinate their distribution. 5
In theory, calculating seroprevalence is straightforward, but the dynamic nature of a pandemic poses challenges. 6 Ideally serial sampling from the general population would provide the most generalizable results, but this approach is both time consuming and expensive. Worldwide blood services have leveraged their operational capacity to conduct seroprevalence studies among blood donors with the intent of informing public health policies. This departure from routine practice was necessary and endorsed by the World Health Organization (WHO) as many countries were not equipped to conduct nationally representative studies in their general population. For example, in Canada there are no prospective national biobanks and with health care managed by individual provinces, no mechanism in place to obtain and compare estimates using the same sampling protocol, analysis framework, and antibody assay across the country. The tradeoff of this readily available population is the selection bias known as the “healthy donor effect”. Characterized by donor eligibility criteria skewing blood donors to be healthier than the general population. 7
In April 2020, the Government of Canada launched the COVID‐19 Immunity Task Force (CITF) to track the spread of SARS‐CoV‐2 infections and to better understand the immune response to infection across diverse populations. In partnership with the CITF, the Canadian Blood Services, which spans all provinces (except Quebec) was in a unique position to conduct a national SARS‐CoV‐2 seroprevalence study in Canada. Following the first COVID‐19 wave, the objectives of this study were to assess temporal changes in seroprevalence over a 10‐week period and to determine how seroprevalence varied by geographical regions, age groups, ethnic minorities, and socioeconomic status.
2. METHODS
2.1. Study design and population sampling
This serial cross‐sectional study was conducted between May 9 and July 21, 2020 from all apheresis and whole blood donors donating at all Canadian Blood Services locations. 8 Canadian Blood Services collects blood from a combination of fixed and mobile sites in all larger cities and most urban areas from all provinces except Quebec. Donors must meet numerous selection criteria to ensure that they are in good health and at low risk of infectious disease. Extra EDTA plasma samples (Becton Dickson [BD], Mississauga, ON, Canada) are routinely collected and retained at the time of donation, in case additional laboratory tests are required. Beginning in March 2020, donors were deferred for 2 weeks if they were diagnosed with SARS‐CoV‐2 infection or if they were in contact with a known case. Donors were assessed at the door of the collection site and not permitted to enter if they had COVID‐19 risk factors and symptoms by questionnaire (n = 234) or elevated temperature (n = 967) or refusing to wear a mask (n = 71). Although there is no evidence that SARS‐CoV‐2 is transmissible by blood transfusion, these extra steps were put in place to enhance safety for donors and staff. 9 During the study period, all allogeneic donations with an extra EDTA sample available after all other operational testing had been completed were included. The Research Ethics Board of the Canadian Blood Services approved this study and exempted study‐specific consent since no confirmatory testing was performed. Donors were not informed of their antibody status.
2.2. SARS‐CoV‐2 antibody testing
Retention EDTA plasma samples were aliquoted and frozen at ‐20°C and processed at the Canadian Blood Services laboratory in Ottawa. The Abbott Architect SARS‐Cov‐2 IgG assay (chemiluminescent microparticle immunoassay [CMIA]) which measures IgG against the SARS‐CoV‐2 nucleocapsid antigen was used to detect qualitative reactivity. Based on the manufacturer's recommendation, we used the sample to cut off ratio of ≥1.4 to consider a sample positive. 10 , 11 , 12
2.3. Analysis
Deidentified data on demographic variables including donation date, location, year of birth, sex, ethnicity, ABO groups and postal code along with donor status (first‐time or repeat) and blood donor type (whole blood, apheresis plasma or platelets) were collected. Provinces were classified by geographical and economic regions across Canada. Donors self‐identified as either; White, Arabic, Asian, Aboriginal, Black, South Asian, Latin‐American, or Other. A priori, we regrouped ethnicities as “other” if they represented <5% of the analytical sample. Socioeconomic status was estimated by the Pampalon Material and Social Deprivation Indices (MSDI). 13 , 14 Material deprivation is associated with low education, insecure job situation, and insufficient income. Social deprivation refers to a fragile social network, characterized by individuals living alone, being a single parent, and separated, divorced or widowed. MSDI was derived from the 2016 Statistics Canada Census using the Postal CodeOM Conversion File (PCCF) to link postal codes to the dissemination area (DA) level (the smallest geographic unit available in the Canadian census, consisting of 400‐700 persons). 15 MSDI was categorized as quantiles; from the least deprived (1) to most deprived (5).
Unadjusted seroprevalence was calculated as the number of reactive samples divided by the total number of samples tested, the Exact method was used to estimate 95% confidence intervals (CI). We first standardized seroprevalence rates to population size, age and sex, using the residential Forward Sortation Area (FSA; first three characters in a Canadian postal code) publicly available through Statistic Canada (catalogue # 98‐400‐X2016008). We then used the Rogan‐Gladen equation to adjust standardized estimates for test performance characteristics (92.7% sensitivity and 99.9% specificity). 11 , 16 We evaluated temporal trends by linear regression at 2‐week intervals and stratified by geographical region, age groups, ethnicity and quantiles of MSDI. Univariate and multivariate logistic regression compared SARS‐CoV‐2 antibody reactive donors compared to non‐reactive donors. Missing data were assumed to be missing completely at random (MCAR).
2.4. Sensitivity analysis
To assess the generalizability of donors during the pandemic period, we compared their characteristics to donors from the previous year. Given the uncertainty of test characteristics, we evaluated seroprevalence at varying sensitivity cut‐offs (70%, 75%, 80%, 85%, 89% and 90%) as a function of varying specificity ranging from 100%, 99.9%, 99.8%, 99.7%, 99.6%, 99.5%. All analyses were conducted using SAS (version 9.4).
3. RESULTS
Between May 9 and July 21, 2020, 152,050 donations were collected (from 140,200 unique donors). Of these, 78,170 (51%) were screened for SARS‐CoV‐2 IgG antibodies, donations that were not tested were due to sample storage capacity or insufficient plasma after operational testing (this varied over time, see Table S1). There were 3528 donors that donated multiple times during the study period; 12 were positive at their first donation, no one seroconverted. After excluding repeated donations, 74,642 distinct donors were included in our analytic sample.
We summarized the donor characteristics and relevant population statistics stratified by geographical regions in Table S2. The proportion of donors from each jurisdiction reflected the population distribution of Canada. As expected, there were slightly more male donors compared to females, this was consistent across all geographical regions. Donors followed the population age structure for adults 17‐60 years old in Canada. The number of donors over the age of 60 years old was underrepresented relative to Canadians. Overall most donors self‐identified as white (70.8%). The proportion of ethnic minorities did vary across Canada, with the greatest proportion in British Columbia and smallest in Atlantic Canada. Overall the social deprivation index was equally represented. However, materially deprived areas were underrepresented. We evaluated the generalizability of blood donors during the pandemic period to the year before and found no appreciable differences.
We compared seroprevalence rates after weighting for population and test characteristics in Table 1. Overall during the 10‐week study period, the adjusted seroprevalence of SARS‐CoV‐2 was 7 per 1000 donors (95% CI 6.3, 7.6). Estimates did not change considerably after weighting for population or test characteristics. There were variations by geographic regions; seroprevalence ranged from 8.8 per 1000 donors (95% CI 7.8, 9.8) in Ontario to 4.5 per 1000 donors (95% CI 2.6, 6.4) in the Atlantic provinces. Overall, there were slight differences by age groups. Donors between 35 and 45 years old had the lowest seroprevalence rates (5.6 per 1000 donors) while donors 25‐35 years old had the highest rates (8.1 per 1000 donors) although none were statistically significant. Donors who self‐identified as white had significantly lower rates 6.6 per 1000 (95% CI 5.9, 7.4) compared to Indigenous populations 9.3 per 1000 (95% CI 2.1, 16.5), Asians 9.3 (95% CI 6.0, 12.7), and other minorities 10.9 (95% CI 8.4, 13.4). It should be noted ethnicity was missing for 11,095 (15%) of donors due to logistical reasons. There were no significant variations in seroprevalence by varying degrees of social or material deprivation or by ABO blood groups.
TABLE 1.
SARS‐COV‐2 seroprevalence per 1000 donors (95% confidence intervals)
| N | + | Crude (unweighted) | Population weighted | Sensitivity & specificity | Fully adjusted | ||
|---|---|---|---|---|---|---|---|
| Total | 74 642 | 552 | 7.4 (6.8, 8.0) | 7.5 (6.9, 8.1) | 6.9 (6.2,7.0) | 7.0 (6.3, 7.6) | |
|
Region |
British Columbia | 10 309 | 62 | 6.0 (4.6, 7.7) | 6.1 (4.9, 7.6) | 5.4 (3.8, 7.0) | 5.6 (4.2, 6.9) |
| Alberta | 12 107 | 60 | 5.0 (3.8, 6.4) | 5.4 (4.1, 7.0) | 4.3 (2.9, 5.6) | 4.8 (3.3, 6.2) | |
| Prairies | 6505 | 40 | 6.1 (4.4, 8.4) | 6.2 (4.4, 8.4) | 5.6 (3.5, 7.6) | 5.6 (3.6, 7.6) | |
| Ontario | 37 928 | 355 | 9.4 (8.4, 10.4) | 9.2 (8.2, 10.2) | 9.0 (8.0, 10.1) | 8.8 (7.8, 9.8) | |
| Atlantic | 7793 | 35 | 4.5 (3.1, 6.2) | 5.2 (3.6, 7.3) | 3.8 (2.2, 5.4) | 4.5 (2.6, 6.4) | |
| Sex | Female | 35 547 | 256 | 7.2 (6.3, 8.1) | 7.2 (6.3, 8.1) | 6.7 (5.7, 7.6) | 6.7 (5.8, 7.5) |
| Male | 39 095 | 296 | 7.6 (6.7, 8.5) | 7.8 (6.9, 8.8) | 7.1 (6.2, 8.0) | 7.3 (6.4, 8.3) | |
| Age | 17‐24 | 7165 | 61 | 8.5 (6.5, 10.9) | 8.1 (6.4, 10.1) | 8.1 (5.8, 10.4) | 7.6 (5.7, 9.5) |
| 25‐34 | 15 254 | 127 | 8.3 (6.9, 9.9) | 8.5 (7.0, 10.3) | 7.9 (6.4, 9.5) | 8.1 (6.5, 9.8) | |
| 35‐44 | 12 286 | 72 | 5.9 (4.6, 7.4) | 6.2 (4.8, 7.9) | 5.2 (3.8, 6.7) | 5.6 (4.1, 7.2) | |
| 45‐54 | 13 339 | 101 | 7.6 (6.2, 9.2) | 7.3 (5.9, 8.9) | 7.1 (5.5, 8.7) | 6.8 (5.2, 8.3) | |
| 55‐64 | 16 753 | 117 | 7.0 (5.8, 8.4) | 6.9 (5.7, 8.2) | 6.5 (5.1, 7.8) | 6.4 (5.1, 7.7) | |
| 65+ | 9845 | 74 | 7.5 (5.9, 9.4) | 8.1 (6.6, 9.9) | 7.0 (5.2, 8.9) | 7.7 (6.0, 9.4) | |
|
Ethnicity |
White | 52 852 | 370 | 7.0 (6.3, 7.7) | 7.1 (6.4, 7.9) | 6.5 (5.7, 7.2) | 6.6 (5.9, 7.4) |
| Aboriginal | 778 | 6 | 7.7 (2.8, 16.7) | 9.6 (3.8, 19.1) | 7.2 (0.6, 13.9) | 9.3 (2.1, 16.5) | |
| Asian | 3098 | 33 | 10.7 (7.3, 14.9) | 9.7 (6.8, 13.7) | 10.4 (6.5, 14.3) | 9.3 (6.0, 12.7) | |
| Others | 6819 | 80 | 11.7 (9.3, 14.6) | 11.1 (8.8, 13.8) | 11.6 (8.8, 14.3) | 10.9 (8.4, 13.4) | |
| Missing | 11 095 | 63 | 5.7 (4.4, 7.3) | 6.0 (4.7, 7.5) | 5.1 (3.5, 6.6) | 5.4 (4.0, 6.8) | |
| Social deprivation index | 1 | 14 004 | 118 | 8.4 (7.0, 10.1) | 8.3 (6.9, 9.9) | 8.0 (6.4, 9.7) | 7.9 (6.4, 9.4) |
| 2 | 13 865 | 90 | 6.5 (5.2, 8.0) | 7.0 (5.8, 8.6) | 5.9 (4.5, 7.4) | 6.5 (5.1, 7.9) | |
| 3 | 13 151 | 95 | 7.2 (5.8, 8.8) | 7.5 (6.1, 9.2) | 6.7 (5.2, 8.3) | 7.1 (5.5, 8.6) | |
| 4 | 12 341 | 88 | 7.1 (5.7, 8.8) | 7.2 (5.8, 8.9) | 6.6 (5.0, 8.2) | 6.7 (5.2, 8.3) | |
| 5 | 13 170 | 101 | 7.7 (6.3, 9.3) | 7.5 (6.0, 9.2) | 7.2 (5.6, 8.8) | 7.0 (5.4, 8.6) | |
| Missing | 8111 | 60 | 7.4 (5.6, 9.5) | 7.0 (5.3, 9.0) | 6.9 (4.9, 8.9) | 6.5 (4.6, 8.4) | |
|
Material deprivation index |
1 | 19 633 | 136 | 6.9 (5.8, 8.2) | 7.1 (6.0, 8.5) | 6.4 (5.1, 7.7) | 6.6 (5.4, 7.9) |
| 2 | 16 457 | 97 | 5.9 (4.8, 7.2) | 5.8 (4.7, 7.1) | 5.3 (4.0, 6.5) | 5.2 (4.0, 6.5) | |
| 3 | 13 872 | 126 | 9.1 (7.6, 10.8) | 9.0 (7.5, 10.7) | 8.7 (7.0, 10.4) | 8.6 (7.0, 10.2) | |
| 4 | 10 460 | 77 | 7.4 (5.8, 9.2) | 8.3 (6.7, 10.2) | 6.9 (5.1, 8.6) | 7.9 (6.1, 9.6) | |
| 5 | 6109 | 56 | 9.2 (6.9, 11.9) | 8.4 (6.4, 10.9) | 8.8 (6.2, 11.4) | 8.0 (5.8, 10.3) | |
| Missing | 8111 | 60 | 7.4 (5.6, 9.5) | 7.0 (5.3, 9.0) | 6.9 (4.9, 8.9) | 6.5 (4.6, 8.4) | |
| Week 1–2 | May 9‐23 | 12 921 | 106 | 8.2 (6.7, 9.9) | 8.2 (6.7, 10.0) | 7.8 (6.1, 9.5) | 7.8 (6.2, 9.5) |
| Week 3–4 | May 24‐Jun 7 | 16 167 | 120 | 7.4 (6.2, 8.9) | 7.5 (6.2, 8.9) | 6.9 (5.5, 8.4) | 7.0 (5.6, 8.4) |
| Week 5–6 | Jun 8‐22 | 22 492 | 157 | 7.0 (5.9, 8.2) | 7.2 (6.2, 8.4) | 6.5 (5.3, 7.6) | 6.7 (5.6, 7.9) |
| Week 7‐8 | Jun 23‐Jul 7 | 18 068 | 126 | 7.0 (5.8, 8.3) | 7.0 (5.8, 8.3) | 6.5 (5.1, 7.8) | 6.4 (5.2, 7.7) |
| Week 9‐10 | Jul 8‐21 | 4994 | 43 | 8.6 (6.2, 11.6) | 8.6 (6.3, 11.4) | 8.2 (5.5, 11.0) | 8.2 (5.6, 10.8) |
| ABO groups | A | 25 715 | 181 | 7.0 (6.1, 8.1) | 6.8 (5.9, 7.9) | 6.5 (5.4, 7.6) | 6.3 (5.2, 7.4) |
| AB | 2964 | 26 | 8.8 (5.7 12.8) | 8.9 (5.8, 12.9) | 8.4 (4.8, 12.0) | 8.6 (4.9, 12.2) | |
| B | 8025 | 62 | 7.7 (5.9, 9.9) | 7.3 (5.6, 9.3) | 7.3 (5.2, 9.3) | 6.8 (4.8, 8.8) | |
| O | 37 936 | 283 | 7.5 (6.6, 8.4) | 7.8 (7.0, 8.8) | 7.0 (6.0, 7.9) | 7.4 (6.4, 8.3) |
Given recent reports questioning the sensitivity of the assay used in this study (Abbott Architect SARS‐Cov‐2 IgG assay CMIA), we conducted a sensitivity analysis to evaluate the effect of lower sensitivity and specificity on seroprevalence rates (Table S3). With a fixed specificity of 99.9%, only when the assay had a sensitivity as low as 70% did this lead to a statistically greater seroprevalence rate (9.1 per 1000 (95% CI 8.3, 10.0). In contrast, minor deviations from 100% specificity resulted in significantly lower seroprevalence rates.
Figure 1 illustrates the catchment area of the Canadian Blood Services and the seroprevalence within provinces divided by economic regions. Overall population dense areas had higher seroprevalence rates compared to more rural areas. Heterogenous seroprevalence was observed in each province (Figure S1). The highest seroprevalence rates within Ontario were the London area (10.9 per 1000 (95% CI 6.0, 15.8) and the metropolitan areas of Toronto (9.8 per 1000 (95% CI 8.2, 11.4).
FIGURE 1.
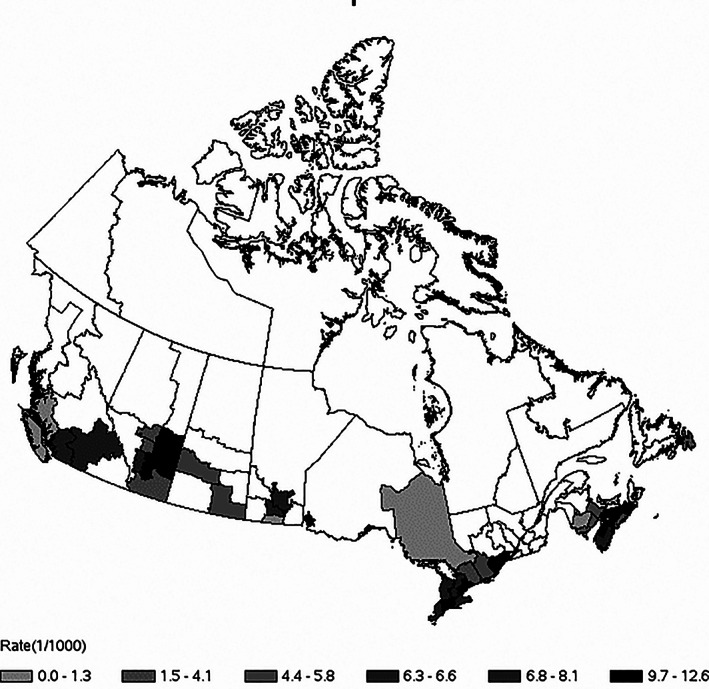
Seroprevalence by economic region across Canada. This map of Canada is divided by economic region (a grouping of census divisions derived by postal codes) a standard geographic unit for analysis. The seroprevalence rate is expressed per 1000 donors, darker shades represent greater seroprevalence. Seroprevalence was not calculated for regions with <200 donors (represented as white)
Overall, we found no temporal trends by 2‐week intervals (Figure 2(A)). While there were baseline differences by geographic regions, trends remained stable over the 10‐week period (Figure 2(B)). We compared weekly intervals to 2‐week intervals from Ontario (which had the largest sample size) and found no significant fluctuations (Figure S2). Temporal trends were not evident after stratifying by age groups, MSDI or ethnicity.
FIGURE 2.
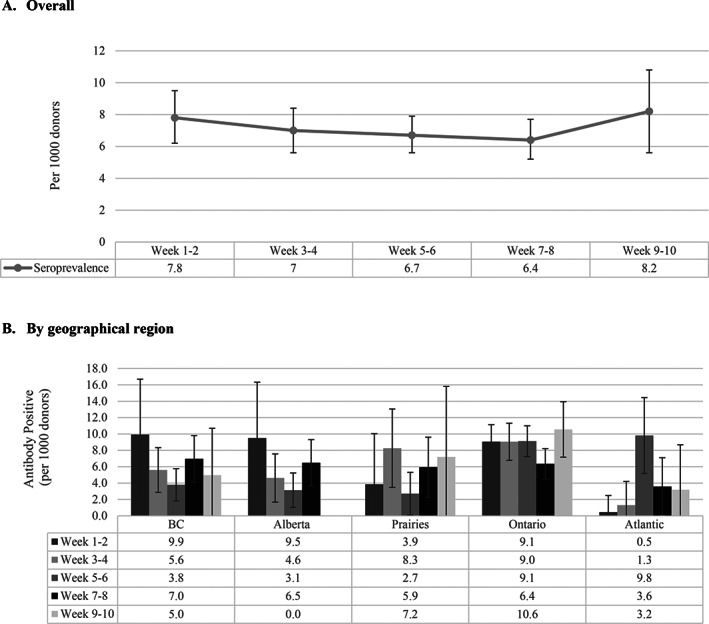
Temporal trends of SARS‐CoV‐2 Seroprevalence from May 9, 2020 to July 21, 2020. Temporal trends were assessed at approximately 2‐week intervals: Week 1‐2 (May 9–May 23); Week 3‐4 (May 24‐Jun 7); Week 5‐6 (Jun 8‐ Jun 22); Week 7‐8 (Jun 23‐ Jul 7); Week 9‐10 (Jul 8‐Jul 21). Panel (A) summarizes temporal trends of adjusted seroprevalence rates overall. Panel (B) stratifies adjusted seroprevalence by geographical region. All rates are expressed, per 1000 donors and 95% CI
Table 2 summarizes the associations between sociodemographic factors and reactive SARS‐CoV‐2 antibodies. By multivariable analysis, the odds of reactivity were significantly higher in Ontario (adjusted odds ratio (aOR) 2.2 (95% CI 1.5, 3.3) compared to Atlantic Canada; and by ethnic minorities, (aOR 1.5 (95% 1.2, 1.9) compared to donors self‐identified as White.
TABLE 2.
Donor characteristics associated with SARS‐COV‐2 antibody reactivity
| Unadjusted OR (95% CI) | Adjusted a OR (95% CI) | ||
|---|---|---|---|
| Region | British Columbia | 1.5 (0.9, 2.4) | 1.4 (0.9, 2.3) |
| Alberta | 1.2 (0.8, 2.0) | 1.2 (0.7, 1.9) | |
| Prairie | 1.5 (0.9, 2.6) | 1.5 (0.9, 2.6) | |
| Ontario | 2.4 (1.6, 3.5) | 2.2 (1.5, 3.3) | |
| Atlantic Canad | REF | REF | |
| Sex | Female | REF | REF |
| Male | 1.0 (0.9, 1.2) | 1.0 (0.9, 1.3) | |
| Age | 17‐24 | 1.3 (0.9, 1.8) | 1.1 (0.8, 1.7) |
| 25‐35 | 1.2 (0.9, 1.6) | 1.2 (0.9, 1.6) | |
| 35‐45 | 0.8 (0.5, 1.0) | 0.8 (0.6, 1.2) | |
| 46‐55 | REF | REF | |
| 55‐65 | 1.0 (0.7, 1.3) | 1.1 (0.8, 1.5) | |
| 65+ | 1.1 (0.8, 1.5) | 1.3 (1.0, 1.9) | |
| Ethnicity b , c | White | REF | REF |
| Indigenous | 1.2 (0.5, 2.8) | 1.4 (0.6, 3.1) | |
| Asian | 1.6 (1.1, 2.3) | 1.6 (1.1, 2.3) | |
| Others | 1.6 (1.2, 2.0) | 1.5 (1.0, 1.9) | |
| Social deprivation index c | 1 | REF | REF |
| 2 | 0.7 (0.5, 1.0) | 0.8 (0.6, 1.0) | |
| 3 | 0.8 (0.6, 1.1) | 0.9 (0.7, 1.2) | |
| 4 | 0.8 (0.6, 1.1) | 0.9 (0.7, 1.2) | |
| 5 | 0.9 (0.7, 1.1) | 0.9 (0.7, 1.2) | |
| Material deprivation index c | 1 | REF | REF |
| 2 | 0.8 (0.6, 1.1) | 0.8 (0.6, 1.1) | |
| 3 | 1.4 (1.1, 1.8) | 1.3 (1.0, 1.7) | |
| 4 | 1.1 (0.8, 1.4) | 1.0 (0.7, 1.4) | |
| 5 | 1.4 (1.0, 1.9) | 1.2 (0.9, 1.7) | |
| ABO groups | A | REF | REF |
| AB | 1.2 (0.7, 1.9) | 1.1 (0.7, 1.8) | |
| B | 1.0 (0.7, 1.3) | 0.9 (0.6, 1.2) | |
| O | 1.1 (0.9, 1.3) | 1.0 (0.9, 1.3) |
Note: Statistically significantly results are bolded.
Adjusted model includes all variables listed in this table.
When ethnicity was dichotomized, ethnic minorities had aOR of 1.5 (95% CI 1.1, 1.9) compared to white donors.
Missing values are treated as Missing Completely at Random (MCAR) were excluded from the analysis.
4. DISCUSSION
SARS‐CoV‐2 seroprevalence studies are fundamental to effectively monitor the extent of the COVID‐19 epidemic and support authorities in making informed decisions. Following Canada's first wave, we found overall less than 1% of 74,642 blood donors between May 9 to July 21, 2020, had humoral evidence of infection with SARS‐CoV‐2. This low prevalence may reflect swift population‐level compliance to strict public health measures implemented early in the pandemic. Prevalence was differential by geographical regions but remained stable over the 10‐weeks. There was evidence of disparities by self‐reported ethnicity. If we extrapolated our findings, approximately 145,640 adults were unknowingly exposed to SARS‐CoV‐2; that is three times greater than reported by case detection until July 1, 2020. Modelling studies estimate that 60% to 80% of a population would need immunity to SARS‐CoV‐2 to achieve herd immunity. 17 Our study demonstrates that the vast majority of Canadians remained susceptible to SARS‐CoV‐2, and in the absence of an effective vaccine are far from reaching thresholds necessary to achieve herd immunity.
Blood services worldwide have responded to the COVID‐19 pandemic by leveraging their operational capacity and access to a healthy population to conduct seroprevalence studies. Within the first six months of the pandemic, 32/48 (73%) of blood services surveyed globally had already, or planned to, conduct seroprevalence studies to inform public health. 18 Sixteen countries, from North America (n = 3), South America (n = 1), Europe (n = 7), Africa (n = 2), and Asia (n = 3) have reported preliminary seroprevalence findings among blood donors, ranging from as high as 66% in parts of Brazil to as low as 0% in Jordan. 19 , 20
Among the G8 countries, the United States (US) was hardest hit by the COVID‐19 pandemic. Community transmission of SARS‐CoV‐2 was estimated to have begun in mid‐to‐late February. The first COVID‐19 wave peaked and plateaued by April 7, 2020 until the second wave, which peaked July 19. The American Red Cross conducted a sero‐survey of 953 926 donations (representing 40% of the blood collected in the US) between June 15 and August 23, 2020 and reported an overall seroprevalence of 1.8%, excluding high prevalence settings such as New York City and southern Florida. 21 All US census regions except the Northeast increased over the 10‐week period, most prominently in the South from 1.1% to 3.0%. Given the timing of their study, their seroprevalence estimates reflect a combination of the first and second wave in the US. Although geographically close, it is difficult to compare seroprevalence estimates between Canada and the US as access to healthcare and the public health response to the COVID‐19 pandemic was dramatically different.
The current literature suggests that SARS‐CoV‐2 was circulating in Europe before North America. 22 , 23 Among the European countries, Canada's epidemic reflects most closely that of Germany with a cumulative incidence of 6505 cases per million compared to 6300 per million in Canada, as of November 2, 2020. Like Canada, Germany also implemented strict social distancing policies early and their first wave peaked by the end of March. Based on a study of 3186 blood donors from three German states, between March and June 2020, seroprevalence was estimated at <1% overall, ranging from 0.7% in Hesse to 1.2% in Lower‐Saxony. 24 In comparison, national blood donor seroprevalence studies from other European countries were higher after their first wave. For example, in Denmark, based on 20,640 blood donors, adjusted seroprevalence was 1.9% (95% CI, 0.8, 2.3) between April 6 and May 3, 2020 (first wave peaked April 8). 25 In the Netherlands, between April 1‐15, seroprevalence increased from 3.1% to 5.0% between May 10 and 20, among 7361 donations. 26
While our study includes blood donors across nine provinces in Canada, Canadian Blood Services does not collect blood donations from the province of Quebec. Researchers at Héma‐Québec conducted a similar blood donor study in Quebec (n = 7691) and found a SARS‐CoV‐2 seroprevalence of 2.2%, between May 25 and July 9, 2020, consistent with greater case detection. Quebec was considered Canada's COVID‐19 epicenter, making up half of Canada's cumulative incidence. 27
The catchment area of the Canadian Blood Services locations limits donors from rural regions of Canada, which may limit the generalizability of the results. Also blood donors are known to be generally healthy, non‐pregnant adults who may not represent the general population. 7 One could suspect seroprevalence may be underestimated, since unhealthy donors are deferred and through the “healthy donor effect” and donors maybe more compliant than the general population to adhere non‐pharmaceutical interventions. However, our results were similar with seroprevalence estimates from public health reports in British Columbia, Alberta and Ontario, which used residual sera from clinical tests, albeit much smaller sample sizes. A study from British Columbia, including children and adults from the Greater Vancouver Area between May 15 and May 27, found 4/885 specimens were reactive, resulting in an age‐standardized seroprevalence of 0.6% (95% CI 0.2, 1.4%). 28 During the first week of June, Alberta analyzed 9400 samples and reported <1% of specimens were positive for SARS‐CoV‐2 antibodies. 29 In the most populated province of Ontario, three cross‐sectional surveys were conducted in April (n = 827), May (n = 1061) and June (n = 7014). 30 After adjusting for population weights and test characteristics, seroprevalence was 0.5% (95% CI 0.1, 1.5) in March and increased to 1.5% (95% CI 0.7, 2.2) in May and 1.1% (95% CI 0.8, 1.3) in June. Given the comparable results, we believe our sample to be relatively representative of the adult population in Canada.
To inform public policy, it will be important to identify local epidemics so that targeted interventions are implemented. Averaging prevalence rates into a single summary may miss significant differences, as social determinants of health likely differentially affect a person's exposure to the SARS‐CoV‐2 virus, vulnerability to infections, and healthcare access. 31 , 32 , 33 Consistent with reports from the US and UK, we found minority populations in Canada had greater exposure to SARS‐CoV‐2, at rates that were disproportionate to white donors. 34 , 35 , 36 , 37 Donors residing in the most material‐deprived areas did not have significantly greater rates of SARS‐CoV‐2 than those in more affluent neighborhoods. This contrasted a study by Ontario's Public Health Agency which found neighborhoods at the highest level of material deprivation experienced two‐times the rates of COVID‐19 cases compared to neighborhoods with the least material deprivation. 38 The difference between our study and Ontario's report may reflect the limited number of donors from materially deprived neighborhoods. 7
Our study has other limitations. There are complex interactions between the accuracy of the assays, antibody kinetics, and population‐level epidemic changes that may bias seroprevalence studies. After exposure to SARS‐CoV‐2, depending on the severity of the disease most people develop an IgG antibody response between 10 and 28 days post infection. 39 , 40 A recent study compared multiple serological assays and found the Abbott assay (used in this study) had lower sensitivity (92.7% [95% CI 90.2, 94.8%]) at ≥20 days post‐symptom onset compared to other commercial assays. 11 Specificity was excellent 99.9% (95% CI 99.4, 100%). However, when restricted to a period of ≥30 days post‐symptoms, sensitivity was comparable to the other assays (>98%). 11 Given that blood donors must be healthy at the time of donation and are deferred for 2‐weeks after a known diagnosis, lower sensitivity early in the infection are unlikely to affect our results. More recently, a study evaluated test characteristics up to 64 days post infection and found specificity remained excellent, but between 21 and 64 days the Abbott assay had an average sensitivity of 83% (95% CI 65%, 94%). 12 We conducted a sensitivity analysis to evaluate multiple sensitivity thresholds and revealed in our low prevalence setting the sensitivity would have to be as low as 70% to have any substantive impact on our seroprevalence estimate. However, even small decrements in specificity have a major impact on the positive predictive value. Lowering the specificity from 99.9% to 99.7% reduced prevalence rates significantly. Therefore, it is possible the seroprevalence observed could be even lower if a sizable proportion was false positive. We also note that similar to other coronaviruses the longevity of detectable antibodies is limited. 41 Among convalescent plasma donors, antibodies began to wane by 100 days thus a limited window of time to detect antibodies. 42 Due to the nature of the study design, the date of infection was not known in our study. However, we did not observe decreases in seropositivity temporally. Therefore, the impact of waning antibody is likely minimal since our study was conducted within about 100 days of the peak of the first wave; this may be more of an issue in the future. Furthermore, a recent longitudinal study revealed waning antibody response was not correlated with T‐cell response which is necessary for long‐term immunity. 43 Serial cross‐sectional studies to evaluate the dynamic nature of the COVID‐19 epidemic in conjunction with cohort studies to evaluate the rate of waning antibodies among asymptomatic and mildly symptomatic cases will be necessary in the future.
The world continues to grapple with the greatest health emergency of the century. Globally countries are faced with making real‐time decisions requiring them to balance the social/economic costs of public health policies and the risk of an uncontrolled epidemic. High‐quality data is required to inform these decisions. Blood services have risen to the occasion, leveraging their capacity and access to a representative healthy adult population, to lead SARS‐CoV‐2 seroprevalence studies worldwide. This study serves as an example of how blood services can partner with public health to conduct surveillance studies, supporting future collaborations. The results of our study suggest Canadians were compliant with social distancing policies reflective of low seroprevalence. However, since the first wave, restrictions have relaxed, pandemic fatigue has set in and cold Canadian winters will push more people inside; all factors likely to increase infection rates. Continuous seroprevalence surveys will be necessary to identify dynamic trends and monitoring disparities particularly in densely populated communities that would be otherwise missed by case detection alone.
CONFLICT OF INTEREST
SJD has acted as a content expert for respiratory viruses for Johnson & Johnson (Janssen). The remaining authors have no conflicts of interest to disclose.
Supporting information
Appendix S1: Supporting information
ACKNOWLEDGMENTS
We kindly acknowledge the dedicated work of laboratory and operations staff at Canadian Blood Services. This project was supported by funding from the Government of Canada, through the COVID‐19 Immunity Task Force.
Saeed S, Drews SJ, Pambrun C, Yi Q‐L, Osmond L, O'Brien SF. SARS‐CoV‐2 seroprevalence among blood donors after the first COVID‐19 wave in Canada. Transfusion. 2021;61:862–872. 10.1111/trf.16296
Funding information Government of Canada
REFERENCES
- 1. Detsky AS, Bogoch II. COVID‐19 in Canada: Experience and response. JAMA. 2020;324(8):743–4. [DOI] [PubMed] [Google Scholar]
- 2. Coronavirus Disease (COVID‐19) : Outbreak update. Available from: https://www.canada.ca/en/public‐health/services/diseases/2019‐novel‐coronavirus‐infection.html#a1
- 3. Burgess S, Ponsford MJ, Gill D. Are we underestimating seroprevalence of SARS‐CoV‐2? BMJ. 2020;370:m3364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ng DL, Goldgof GM, Shy BR, Levine AG, Balcerek J, Bapat SP, et al. SARS‐CoV‐2 seroprevalence and neutralizing activity in donor and patient blood. Nat Commun. 2020;11(1):4698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Metcalf CJE, Farrar J, Cutts FT, Basta NE, Graham AL, Lessler J, et al. Use of serological surveys to generate key insights into the changing global landscape of infectious disease. Lancet. 2016;388(10045):728–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Clapham H, Hay J, Routledge I, Takahashi S, Choisy M, Cummings D, et al. Seroepidemiologic study designs for determining SARS‐COV‐2 transmission and immunity. Emerg Infect Dis. 2020;26(9):1978–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Atsma F, de Vegt F. The healthy donor effect: A matter of selection bias and confounding. Transfusion. 2011;51:1883–5. [DOI] [PubMed] [Google Scholar]
- 8. Canadian Blood Services . Available from: https://www.blood.ca/en.
- 9. Leblanc J‐F, Germain M, Delage G, OʼBrien S, Drews SJ, Lewin A. Risk of transmission of severe acute respiratory syndrome Coronavirus‐2 by transfusion: A literature review. Transfusion. 2020;60:3046–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. SARS‐COV‐2 Immunoassays . Available from: https://www.corelaboratory.abbott/us/en/offerings/segments/infectious‐disease/sars‐cov‐2.
- 11. National SARS‐CoV‐2 Serology Assay Evaluation Group . Performance characteristics of five immunoassays for SARS‐CoV‐2: A head‐to‐head benchmark comparison. Lancet Infect Dis. 2020;20(12):1390–400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tan SS, Saw S, Chew KL, Huak CY, Khoo C, Pajarillaga A, et al. Head‐to‐head evaluation on diagnostic accuracies of six SARS‐CoV‐2 serological assays. Pathology. 2020;52:770–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pampalon R, Hamel D, Gamache P, Raymond G. A deprivation index for health planning in Canada. Chronic Dis Can. 2009;29(4):178–91. [PubMed] [Google Scholar]
- 14. Pampalon R, Hamel D, Gamache P, Philibert MD, Raymond G, Simpson A. An area‐based material and social deprivation index for public health in Québec and Canada(link is external). Can J Public Health. 2012;103(8):17–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Postal CodeOM Conversion File (PCCF) , Reference Guide, 2017. (statcan.gc.ca) [Last accessed Feb 16, 2021].
- 16. Lang Z, Reiczigel J. Confidence limits for prevalence of disease adjusted for estimated sensitivity and specificity. Prev Vet Med. 2014;113:13–22. [DOI] [PubMed] [Google Scholar]
- 17. Fontanet A, Cauchemez S. COVID‐19 herd immunity: Where are we? Nat Rev Immunol. 2020;20(10):583–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. O'Brien SF, Lieshout‐Krikke RW, Lewin A, Erikstrup C, Steele WR, Uzicanin S, Custer B. Research initiatives of blood services worldwide in response to the covid‐19 pandemic. Vox Sanguinis 2020. 10.1111/vox.12995. [DOI] [PubMed] [Google Scholar]
- 19. Buss LF, Prete CA, Abrahim CMM, Mendrone A, Salomon T, de Almeida‐Neto C, et al. Three‐quarter attack rate of SARS‐CoV‐2 in the Brazilian Amazon during a largely unmitigated epidemic. Science. 2020;371(6526):288–292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Sughayer MA, Mansour A, Al Nuirat A, Souan L, Ghanem M, Siag M. The effect of strict lock down measures on COVID‐19 seroprevalence rate and herd immunity. medRxiv. 2020. 10.1101/2020.06.06.20123919. [DOI] [Google Scholar]
- 21. Dodd RY, Xu M, Stramer SL. Change in donor characteristics and antibodies to SARS‐CoV‐2 in donated blood in the US, June‐august 2020. JAMA. 2020;324:1677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. CDC COVID‐19 Response Team , Jorden MA, Rudman SL, Villarino E, Hoferka S, et al. Evidence for limited early spread of COVID‐19 within the United States, January–February 2020. MMWR Morb Mortal Wkly Rep. 2020;69:680–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Deslandes A, Berti V, Tandjaoui‐Lambotte Y, Alloui C, Carbonnelle E, Zahar JR, et al. SARS‐CoV‐2 was already spreading in France in late December 2019. Int J Anti Agents. 2020;55(6):106006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Fischer B, Knabbe C, Vollmer T. SARS‐CoV‐2 IgG seroprevalence in blood donors located in three different federal states, Germany, march to June 2020. Euro Surveill. 2020;25(28);2001285. 10.2807/1560-7917.ES.2020.25.28.2001285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Erikstrup C, Hother CE, Pedersen OBV, Mølbak K, Skov RL, Holm DK, Sækmose SG, Nilsson AC, Brooks P T, Boldsen JK, Mikkelsen C, Gybel‐Brask M, Sørensen E, Dinh KM, Mikkelsen S, Møller B Kuno, Haunstrup T, Harritshøj L, Jensen BA, Hjalgrim H, Lillevang ST. Ullum H Estimation of SARS‐CoV‐2 Infection Fatality Rate by Real‐time Antibody Screening of Blood Donors. Clinical Infectious Diseases 2021;72(2):249–253. 10.1093/cid/ciaa849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Slot E, Hogema BM, Reusken CBEM, Reimerink JH, Molier M, Karregat JHM, et al. Low SARS‐CoV‐2 seroprevaluence in blood donors in the early COVID‐19 epidemic in The Netherlands. Nat Commun. 2020;11(1):5744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Blood donor seroprevalence study: 2.23% of Quebec adults contracted COVID‐19. [cited 2021 Jan 6]. Available from: https://www.hema‐quebec.qc.ca/publications/communiques/archives/2020/communiques‐2020/etude‐seroprevalence‐resultats.en.html.
- 28. Skowronski DM, Sekirov I, Sabaiduc S, Zou M, Morshed M, Lawrence D, et al. Low SARS‐CoV‐2 sero‐prevalence based on anonymized residual sero‐survey before and after first wave measures in British Columbia, Canada, march‐may 2020. medRxiv. 2020. 10.1101/2020.07.13.20153148. [DOI] [Google Scholar]
- 29. Alberta news report\Alberta receives serology test results for COVID‐19 antibodies, records 113 new cases. 2020. Available from: www.globalnews.ca/new/7235508/alberta-covid-19-update-july-30/.
- 30. Public health of Ontario report. Available from: https://www.publichealthontario.ca/-/media/documents/ncov/epi/2020/07/covid-19-epi-seroprevalence-in-ontario.pdf?la=en.
- 31. Cockerham WC, Hamby BW, Oates GR. The social determinants of chronic disease. Am J Prev Med. 2017;52(1 Suppl 1):S5–S12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Adler NE, Newman K. Socioeconomic disparities in health: Pathways and policies. Health Aff. 2002;21(2):60–76. [DOI] [PubMed] [Google Scholar]
- 33. Burstrom B, Tao W. Social determinants of health and inequalities in COVID‐19. Eur J Public Health. 2020;30(4):617–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Thakur N, Lovinsky‐Desir S, Bime C, Wisnivesky JP, Celedón JC. The structural and social determinants of the racial/ethnic disparities in the U.S. COVID‐19 pandemic. What's our role? Am J Respir Crit Care Med. 2020;202(7):943–949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Tai DBG, Shah A, Doubeni CA, Sia IG, Wieland ML. The disproportionate impact of COVID‐19 on racial and ethnic minorities in the United States. Clin Infect Dis. 2020;72(4):703–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Yancy CW. COVID‐19 and African Americans. JAMA. 2020;323:1891–2. [DOI] [PubMed] [Google Scholar]
- 37. Public Health England . Disparities in the risk and outcomes of COVID‐19. 2020. [cited 2020 Jun 2]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/889861/disparities_review.pdf.
- 38. Ontario Report . Enhanced epidemiological summary COVID‐19 in Ontario – A Focus on Material Deprivation. Available from: https://www.publichealthontario.ca/‐/media/documents/ncov/epi/2020/06/covid‐19‐epi‐material‐deprivation.pdf?la=en.
- 39. Xiao AT, Gao C, Zhang S. Profile of specific antibodies to SARS‐CoV‐2: The first report. J Infect. 2020;81(1):147–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Huang M, Lu Q‐B, Zhao H, Zhang Y, Sui Z, Fang L, et al. Temporal antibody responses to SARS‐CoV‐2 in patients of coronavirus disease. Cell Discov. 2020;6(64):64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Wu L‐P, Wang N‐C, Chang Y‐H, Tian XY, Na DY, Zhang LY, et al. Duration of antibody responses after severe acute respiratory syndrome. Emerg Infect Dis. 2007;13(10):1562–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Perreault J, Tremblay T, Fournier MJ, Drouin M, Beaudoin‐Bussières G, Prévost J, et al. Waning of SARS‐CoV‐2 RBD antibodies in longitudinal convalescent plasma samples within four months after symptom onset. Blood. 2020;136:2588–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Bilich T, Nelde A, Heitmann JS, Maringer Y, Roerden M, Bauer J, et al. Differential kinetics of T cell and antibody responses delineate dominant T cell epitopes in long‐term immunity after COVID‐19. 2020; (Under Review). https://www.researchsquare.com/article/rs-114499/v1.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1: Supporting information