

Abstract
Background:
Currently, there are 2 mainstream treatments for displaced femoral neck fracture, including internal fixation and arthroplasty. However, there are still some controversial problems as to which treatment should be primarily chosen.
Methods:
The relevant studies comparing arthroplasty with internal fixation were searched in the databases of PubMed, Embase, and Cochrane Library. Finally, 31 relevant randomized controlled trials were included in this meta-analysis. The quality of studies was evaluated and meta-analyses were performed using RevMan 5.3 software. We also assessed the heterogeneity among studies and publication bias via the I-squared index and forest plots.
Results:
There was no significant difference between arthroplasty and internal fixation groups in patient mortality at both short-term and long-term points. However, patients treated with arthroplasty showed significantly lowered risks of reoperation both at short-term (5.6% vs 31.5%; relative risks (RR) = 0.19; 95% CI, 0.13–0.28; P < .00001) and long-term follow-up (9.5% vs 45.9%; RR = 0.23; 95% CI, 0.17–0.33; P < .00001). Similarly, arthroplasty-treated patients demonstrated a significant decrease in the risk of postoperation complications at short-term (10.3% vs 34.4%; RR = 0.37, 95% CI, 0.24–0.57; P < .00001) and long-term follow-up (11.7% vs 42.5%; RR = 0.30, 95% CI, 0.16–0.57; P < .0002). Besides, patients in the arthroplasty group were associated with better alleviation of pain postoperation (18.3% vs 31.1%; RR = 0.50, 95% CI, 0.33–0.78; P = .002).
In trial sequence analyses, all cumulative Z curves except that of mortality crossed the trial sequential monitoring boundaries and conventional boundaries, and required information size has been reached.
Conclusions:
Arthroplasty leads to a lower rate of reoperation, a reduced risk of complications, and a better alleviation of postoperation pain both at short-term and long-term follow-up. Most importantly, and according to trial sequence analyses, more than enough evidence has been achieved that arthroplasty does show better outcomes than internal fixation in terms of reoperation rate, complications, and postoperation pain.
Level of Evidence:
Therapeutic Level I. See Instructions for Authors for a complete description of levels of evidence.
Keywords: arthroplasty, femoral neck fracture, internal fixation
1. Introduction
With the growing number of the geriatric population and traffic accidents, patients with femoral neck fractures have been on the rise in the last 2 decades or 3.[1] Every year, about 1,600,000 individuals worldwide suffer from this kind of fracture and this number will continue to rise to 6.26 million by 2050.[2,3] Moreover, femoral neck fractures are usually characterized by the high incidence of nonunion and femoral head necrosis, which, therefore, result in a sharp increase in the morbidity and disability rate.[4]
Although there is a wide range of treatments that are currently available for those patients with displaced femoral neck fractures, arthroplasty (AR), including total hip arthroplasty (THA) and hemiarthroplasty (HA), and internal fixation (IF) are still the 2 primary alternatives. As for those young patients with good bone quality and good health, treatment of reduction with IF would be strongly recommended in most cases. However, for the elderly patients, the best option is still far from definite, so both AR and IF have been widely used in the treatment of displaced neck fractures.[5] On the one hand, AR is currently becoming increasingly popular amongst orthopaedists for its significantly lower incidence of reoperation rate and rapid functional recovery.[6,7] Nevertheless, AR, which involves extensive soft tissue dissection, also leads to prosthetic loosening,[8,9] dislocation,[10] and infection.[11] On the other hand, IF with screws and plates has been reported to be of significant advantage in terms of minor trauma, less blood loss, and shorter operative time, and is more likely to preserve the femoral head.[12,13] However, its disadvantages are apparent as well, such as the high incidence of nonunion and femoral head necrosis.[7] Therefore, despite an increasing number of studies on femoral neck fracture, it is still controversial regarding the optimal way of treating elderly patients.[14]
In order to provide more recent and convincing evidence for the treatment of displaced femoral neck fractures, we performed the meta-analysis including more recent randomized controlled trials (RCTs) to evaluate mortality, reoperation rate, complications, and pain between patients treated either by AR or by IF.[15–19] In addition, a trial sequential analysis (TSA) was used to determine whether there had been enough proof to convince us of the best option between AR and IF.
2. Materials and methods
2.1. Protocol and registration
This meta-analysis of RCTs was performed according to the preferred reporting items for systematic reviews and meta-analyses recommendations.[20] A protocol for this meta-analysis has been registered on PROSPERO, and the registration number is CRD42017074991.
2.2. Literature searches
We conducted the literature search to find the papers involved in comparing AR to IF in the treatment of femoral neck fractures. Two independent reviewers systematically searched the electronic database—PubMed (1966 to July 1, 2018), Embase (1974 to July 1, 2018), and the Cochrane Library (1996 to July 1, 2018) with no restriction of language and geography. Our searching strategy involves the different combinations of search terms, including femoral neck fractures, AR, IF, and their respective alternatives. Also, we performed a manual search to identify relevant studies.
2.3. Inclusion criteria and exclusion criteria
Studies were included if they met the following eligibility criteria: RCTs, subjects older than 60 with femoral neck fractures (Garden Stage III or IV), studies comparing AR with IF, clinical outcomes including at least one of the following: mortality, reoperation rate, and complications.
Exclusion criteria: non-RCTs; studies did not focus on the displaced hip fracture; review articles, letters, conference abstracts, and case reports.
2.4. Data extraction
Two authors independently screened all available and relevant data from the included studies. The following characteristics were extracted: name of the first author, publication year, interventions and the number of patients both in AR and IF groups, the follow-up years, as well as the clinical results including mortality rate, reoperation rate, and complications (such as fixation failure, dislocation, nonunion, peri-prosthetic fractures, femoral head necrosis, infection, etc.).
2.5. Data synthesis
The primary outcome was the short-term (within 5 years) and long-term (over 5 years) mortality, reoperation risk, complication rate, and pain after the treatment, IF or AR. The secondary outcomes included the TSA results as well as the sensitivity analysis results.
2.6. Risk of bias and methodological quality assessment
We assess the methodological quality of each study based on The Cochrane Collaboration's tool.[21] We primarily evaluated the following parts: randomization, allocation concealment, blinding, incomplete outcome data, and selective reporting. If there were any disagreement, we would discuss them again, and differences were resolved by a third reviewer. We also used GRADEpro to evaluate the quality of the eligible studies.[22]
2.7. Trial sequential analysis
It is widely accepted that a qualified meta-analysis should be at least as good as a high-quality RCT, so rigorous standards for a meta-analysis should not be neglected. We, therefore, used TSA, which is capable of controlling the risks of type I and type II errors and then calculated required information size (RIS) needed by systematic review and meta-analysis, to evaluate the reliability and conclusiveness of the acquired studies on the major results.[23,24] As previously described,[25] TSA would create a trial sequential monitoring boundary by adjusting the random errors before the implementation of TSA. Also, the horizontal line of Z = 1.96 acted as the traditional boundary of statistical significance in the process of TSA. See more details in supplementary file.
2.8. Statistical analysis
We conducted the meta-analysis by RevMan 5.3 software (The Nordic Cochrane Centre, Copenhagen, Denmark). We chose to compare the dichotomized results using RR and corresponding 95% CIs, and compare the continuous data using standard mean difference. Additionally, since both THA and HA were often seen being performed in the AR group, we made comparisons between the THA and IF, and between HA and IF, respectively. Chi-square and I2 tests were used to check the heterogeneity among studies. If the heterogeneity was lower than 50%, a fixed-effects model was used; otherwise, a random-effects model would be used. Publication bias was evaluated by a funnel plot based on the outcomes.
3. Results
3.1. Included studies and characteristics
A total of 1,352 records were identified through database searching, but 31 studies were included at last for full review and meta-analysis (Fig. 1). Characteristics of the included studies were shown in Table 1.[8–10,12,13,15–19,26–46]Figure 2 showed the risk of bias in the included trials. The quality assessment analysis indicated that the quality of the primary outcomes was moderate.
Figure 1.

A flow chart of the process of screening literature we applied for this study is shown.
Table 1.
Characteristics of included randomized controlled trials.
| Interventions | Number of patients | Follow-up | ||||
|---|---|---|---|---|---|---|
| Study | Year | Arthroplasty | Internal fixation | Arthroplasty | IF | months |
| Soreide[31] | 1979 | HA | Olmed screws | 53 | 51 | 14.5 |
| Sikorski[10] | 1981 | HA | Garden screws | 114 | 76 | 24 |
| Svenningsen[33] | 1985 | HA | Compression screw /McLaughlin nail/ plate | 59 | 110 | 36 |
| Skinner[32] | 1989 | HA/THA | Sliding compression screws | 180 | 91 | 12 |
| van Vugt[8] | 1993 | HA | Dynamic hip screw | 22 | 21 | 36 |
| Jónsson[37] | 1996 | THA | Hansson hook pins | 23 | 24 | 24 |
| Neander[38] | 1997 | THA | Two parallel Olmed screws | 43 | 57 | 18 |
| Johansson[27] | 2000 | THA | Two parallel Olmed screws | 50 | 50 | 24 |
| Ravikumar[9] | 2000 | HA | Two von Bahr screws | 47 | 53 | 60 |
| vanDortmont[39] | 2000 | HA | Dynamic hip screw | 29 | 28 | 24 |
| Davison[29] | 2001 | HA | Compression hip screw / two-hole plate | 187 | 93 | 60 |
| Puolakka[40] | 2001 | HA | Three Ullevaal screws | 15 | 16 | 24 |
| Parker[13] | 2002 | HA | Three AO screws | 229 | 226 | 12 |
| Rogmark[41] | 2002 | HA/THA | Hansson hook pins or Olmed screws | 192 | 217 | 24 |
| Roden[42] | 2003 | HA | Two von Bahr screws | 47 | 53 | 60 |
| Tidermark[35] | 2003 | THA | Two cannulated screws | 49 | 53 | 24 |
| Blomfeldt[36] | 2005 | THA | Two cannulated screws | 49 | 53 | 48 |
| Bj⊘rgul[43] | 2006 | HA | Olmed screws | 455 | 228 | 72 |
| Keating[28] | 2006 | HA/THA | Cancellous screws or sliding hip screw | 180 | 118 | 24 |
| Frihagen[12] | 2007 | HA | Two parallel cannulated screws | 110 | 112 | 24 |
| Heetveld[30] | 2007 | HA | Screws | 109 | 115 | 24 |
| Mouzopoulos[34] | 2008 | HA/THA | Richards plate-screw | 71 | 38 | 48 |
| Leonardsson[26] | 2010 | HA/THA | Hansson hook pins or Olmed screws | 192 | 217 | >60 |
| Parker[44] | 2010 | HA | screws | 229 | 226 | 180 |
| Chammout[45] | 2012 | THA | Two cannulated screws | 43 | 57 | >60 |
| Hedbeck[46] | 2013 | HA | Two cannulated screws | 29 | 30 | 24 |
| Cao[17] | 2014 | THA | Three hollow compression screws | 157 | 128 | 60 |
| Johansson[19] | 2014 | THA | Screw | 68 | 78 | >120 |
| Stoen[18] | 2014 | HA | Screws | 110 | 112 | >60 |
| Parker[15] | 2015 | HA | Screw/plate | 26 | 30 | 12 |
| Lu[16] | 2017 | HA | Cannulated screws | 37 | 41 | 36.8 |
Figure 2.

Risk of bias summary: judgements about each risk of bias item for each included study.
3.2. Clinical outcomes
3.2.1. Mortality
Twenty studies, on a total of 2,354 patients in AR group and 1,914 patients in IF group, provided the short-term mortality rate, whereas 14 studies, on a total of 1,391 patients in AR group and of 1,380 patients in IF group, provided the long-term mortality rate. We found no differences either in short-term mortality (RR = 1.07; 95% CI, 0.94–1.20; P = .24) (Fig. 3), or in long-term mortality (RR = 1.02; 95% CI, 0.92–1.12; P = .86) (Fig. 4). We chose to use a fixed-effect model as there was no significant heterogeneity between studies in all groups (P = .24, I2 = 17%, and P = .86, I2 = 0%, respectively).
Figure 3.

Forest plot of comparison of mortality at short term including the subgroups of Mortality-HA, Mortality-THA, and Mortality-HA/THA. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
Figure 4.
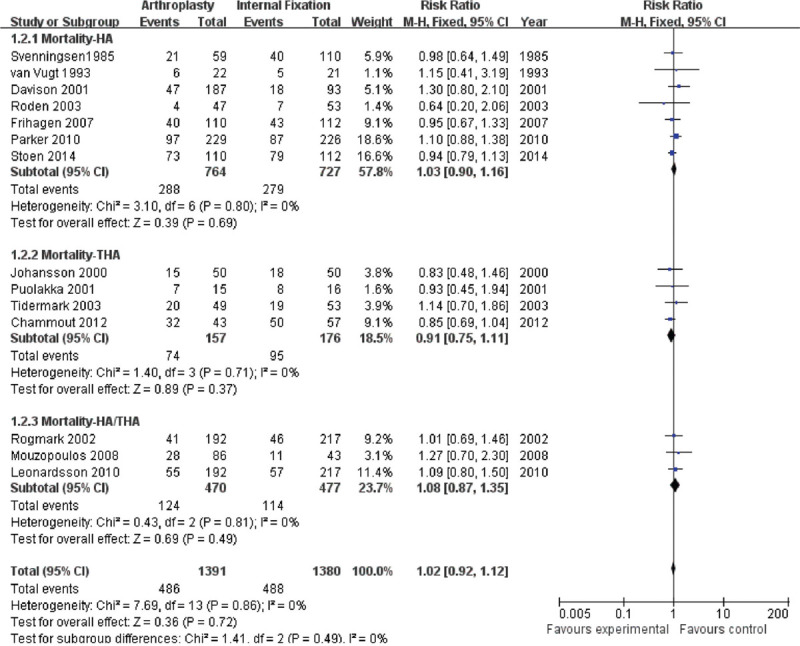
Forest plot of comparison of mortality at long term including the subgroups of Mortality-HA, Mortality-THA, and Mortality-HA/THA. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
The TSA was conducted in light of short-term and long-term mortality in control group of 19% and 37%, a relative risk increase in the experimental group of 15% and 1%, and diversity of 23% and 0%, respectively. The RIS was 8,204 and 5,449 participants. The cumulative Z curve (blue line) crossed neither the trial sequential monitoring boundaries (red inward slash) nor the conventional boundaries (black dotted line), but it entered the futility area (Fig. S1). The TSA-adjusted 95% CI of RR was 0.90 to 1.27 and 0.85 to 1.19.
In an effort to provide more details on the effect of different types of AR on mortality, we also compared the short-term and long-term mortality between HA and IF group [(14 studies of short-term mortality (labeled as A) and 5 studies of long-term mortality (labeled as B)], and between THA and IF group [(7 studies of short-term mortality (labeled as C) and 3 studies of long-term mortality (labeled as D)]. Similarly, the pooled analysis showed that there was no difference in comparison of the mortality of either THA or hip AR with IF at short-term and long-term follow-ups. Their statistical results were shown in sequence (Figs. 3 and 4): A (RR = 1.08; 95% CI, 0.95–1.23; P = .25); B (RR = 1.03; 95% CI, 0.90–1.16; P = 0.69); C (RR = 1.01; 95% CI, 0.71–1.43; P = 0.97); D (RR = 0.91; 95% CI, 0.75–1.11; P = .37). We used a fixed-effect model, as there was no significant heterogeneity (A: P = .06, I2 = 41%; B: P = .68, I2 = 0%; C: P = .07, I2 = 38%; D: P = 0.71, I2 = 0%).
The TSA was conducted based on the incidence of short-term mortality in HA group in control group of 20%, a relative risk increase in the experimental group of 10%, and diversity of 49%. The RIS was 25,260 participants, 12.5% of which were accrued in our meta-analysis. The cumulative Z curve (blue line) crossed neither the trial sequential monitoring boundaries (red inward slash) nor the conventional boundaries (black dotted line), and the RIS was far from being reached (Fig. S2). The TSA-adjusted 95% CI of RR was from 0.63 to 1.82.
3.2.2. Reoperation rate
Twenty-three studies, on a total of 2,383 patients in the AR group and of 1,914 patients in the IF group, provided the short-term reoperation rate, whereas 7 studies, on a total of 933 patients in the AR group and of 849 patients in the IF group, provided the long-term reoperation rate. There were statistical heterogeneities between studies in 2 groups (P < .00001, I2 = 74%; P = .03, I2 = 62%), so we used a random-effect model instead. The pooled results showed that AR group was associated with a lower short-term reoperation rate (RR = 0.19; 95% CI, 0.13–0.28; P < .00001), and a lower long-term reoperation rate (RR = 0.23; 95% CI, 0.17–0.33; P < .00001) (Figs. 5 and 6).
Figure 5.

Forest plot of comparison of reoperation at short term including the subgroups of Reoperation-HA, Reoperation-THA, and Reoperation-HA/THA. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
Figure 6.

Forest plot of comparison of reoperation at long term including the subgroups of Reoperation-HA, Reoperation-THA, and Reoperation-HA/THA. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
The TSA was conducted based on the rate of short-term reoperation in the control group of 30%, a relative risk reduction in the experimental group of 20%, and diversity of 56%. The cumulative Z curve (blue line) crossed the trial sequential monitoring boundaries, and conventional boundaries and the RIS was reached (Fig. S3). The TSA-adjusted 95% CI of RR was adjusted from 0.14 to 0.19.
Again, we conducted the subgroup analysis of reoperation rate between THA and IF and HA and IF. The heterogeneity tests between THA and IF showed that it was present in both short-term and long-term reoperation rate (P = .96, I2 = 0%; P = .30, I2 = 16%), whereas the heterogeneity tests between HA and IF showed that there was no significant heterogeneity in long-term reoperation rate (P = .44, I2 = 0%), but it was obviously heterogeneous in short-term reoperation rate (P < .0001, I2 = 74%). Therefore, the random-effect model was used for comparing short-term reoperation rate between HA and IF, whereas the fixed-effect model was used for all other comparisons. The pooled RRs for short-term and long-term reoperation rate after HA was compared to IF were 0.21 (95% CI, 0.13–0.35; P < .00001) and 0.17 (95% CI, 0.12–0.24; P < .00001), respectively, (Figs. 5 and 6). And the pooled RRs for short-term and long-term reoperation rate after THA was compared to IF were 0.11 (95% CI, 0.06–0.21; P < .00001) and 0.35 (95% CI, 0.23–0.53; P < .00001), respectively, (Figs. 5 and 6). It was clear that patients treated by AR (either THA or HA) were more likely to have fewer reoperations at short-term and long-term than patients treated by IF (P < .00001).
The TSA was conducted based on the rate of short-term reoperation in HA group in the control group of 30%, a relative risk reduction in the experimental group of 50%, and diversity of 74%. The cumulative Z curve (blue line) crossed the trial sequential monitoring boundaries and the conventional boundaries, and the RIS was reached (Fig. S4). The TSA-adjusted 95% CI of RR was from 0.16 to 0.25.
3.2.3. Complications
Twenty studies, on a total of 1,740 patients in the AR group and of 1,693 patients in the IF group, provided the data of surgical complications as a whole, including the short-term and long-term complications. Due to the high heterogeneity (P < .00001, I2 = 83%; P < .00001, I2 = 89), we used the random-effect model to perform the analysis. The pooled analysis revealed a lower risk both at short-term (RR = 0.37, 95% CI, 0.24–0.57; P < .00001) (Fig. 7) and long-term (RR = 0.30, 95% CI, 0.16–0.57; P < .0002) (Fig. 8) of postoperative complications in the AR group when compared to that in the IF group, so we speculated that AR might be superior to IF regarding the postoperative complications.
Figure 7.

Forest plot of comparison of complication at short term including the subgroups of Complication-HA, Complication-THA, and Complication-HA/THA. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
Figure 8.

Forest plot of comparison of complication at long term including the subgroups of Complication-HA, Complication-THA, and Complication-HA/THA. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
Subgroup analysis showed that HA was also associated with a lower risk of complications both at short-term (RR = 0.48, 95% CI, 0.27–0.85; P = 0.01) and at long-term (RR = 0.17, 95% CI, 0.12–0.25; P < 0.00001) (Figs. 7 and 8) when compared to IF. As for THA, although it demonstrated a lower risk of complications at short-term (RR = 0.20, 95% CI, 0.12–0.34; P < .00001) (Fig. 7), it did not show a statistically significant difference at long-term (RR = 0.68, 95% CI, 0.23–1.97; P = .48) (Fig. 8). We used the random-effect model as well by virtue of their high heterogeneity (P < .00001, I2 = 83% at short-term; P < .00001, I2 = 89% at long-term).
We particularly removed the feeling of pain from various complications for the comparison between AR and IF because the degree of pain is one of the most critical factors that determine a patient's quality of life. Similarly, we used the random-effect model on account of its high heterogeneity (P < .00001, I2 = 85%). Moreover, the pooled RRs for postoperative pain after AR compared to IF were 0.50 (95% CI, 0.33–0.78; P = .002) (Fig. 9), so it seemed that patients treated by AR felt less pain than those treated by IF.
Figure 9.

Forest plot of comparison of postoperative pain. Experimental = Arthroplasty, Control = Internal Fixation, M-H = Mantzel-Haenzel method.
The TSA was conducted in light of short-term complications, total complications, and pain in the control group of 30%, a relative risk reduction in the experimental group of 30%, and diversity of 85%, 81%, and 89%, respectively. The RIS was 4,808, 5,848, and 7,003 participants, respectively. The cumulative Z curve (blue line) crossed the trial sequential monitoring boundaries (red inward slash) before the RIS has been reached (Fig. S5). The TSA-adjusted 95% CI of RR was adjusted from 0.25 to 0.37, 0.21 to 0.30, and 0.48 to 0.80.
3.3. Sensitivity analysis
For those tests with high heterogeneity, we also performed the sensitivity analysis. We removed 1 study at a time and analyzed the rest to evaluate whether the overall result could have been significantly affected by 1 single study. The results of sensitivity analysis found that no single study had a significant influence on pooled RRs (Figs. S6–10).
3.4. Publication bias
In order to check for the underlying publication bias, we used the Begg funnel plot (standard error (SE) of the log RR). Also, the results showed no publication bias (Figs. S11–17).
4. Discussion
Currently, the best treatment for patients with femoral neck fractures, particularly in elderly patients, is still undetermined. Previous evidence[7] had shown that patients treated with AR were superior to those treated with IF on the whole. However, most of the studies they collected were observational studies and lacked related quality control. Therefore, the reliability of their conclusions was limited. With the continuous advent of some new evidence of the comparison of AR and IF, we performed this meta-analysis of 31 RCTs in order to provide a latest and more reliable conclusion of the best treatment for patients with femoral neck fractures. The composite results revealed that compared to IF, AR was associated with fewer secondary operations and lower risk of postoperative complications, as well as no increased mortality. Additionally, AR was superior to IF with respect to the postoperative pain that patients suffered.
Mortality is one of the most essential clinical assessment criteria and possible crucial factors to determine whether patients should be treated with AR or IF. Patients treated by AR were allegedly characterized by higher mortality when compared to those treated by IF. Some studies[6,26] showed that there was an increasing trend in the RR of mortality within the early 4 months after AR compared to the same period after IF. However, Hudson et al[47] reported higher mortality in patients treated by IF when they took into consideration the age, gender, and comorbidities in their study. Nonetheless, in our meta-analysis, it suggests similar mortality for AR and IF in the treatment of patients with femoral neck fractures either within 5 years or more than five years. Also, similar to the comparison of AR and IF in the mortality, the results of the comparison between THA and IF or between HA and IF show no difference in mortality. In other words, the application of AR, regardless of THA or HA, for treating femoral neck fractures will not increase the possibility of death at short-term and long-term follow-ups.
The reoperation rate is also a key factor for assessing AR and IF. It has been reported that the reoperation rate after IF was changed from 30% to 50%[48] and was far higher than that after AR.[49] In our meta-analysis, similar results for IF were observed. We reported that AR could effectively reduce the risk of reoperation at short-term and long-term periods. Furthermore, THA or HA did not change the overall pooled effect of AR compared to IF in the reoperation rate. This can be partly attributed to the high risk of complications after IF, which will be discussed in detail later.
As for the occurrence of major postoperative complications, such as fixation failure, dislocation, nonunion, peri-prosthetic fractures, femoral head necrosis, and infection, our meta-analysis revealed that compared to IF, AR was associated with a lower risk of complications either at short-term or at long-term follow-ups, or overall, which was likely to be attributed to lower risk of nonunion or femoral head necrosis.[6,27]
Additionally, we compared AR and IF in the pain rate, which was significantly higher in the IF group. We believed that reasons behind this were that patients treated with IF, as reported by previous studies,[7,9,13,28,29] were more likely to suffer from nonunion and femoral head necrosis, which would definitely increase the risk of pain.
Based on results from the sequential analysis, all the calculated RIS required to produce a reliable conclusion in mortality between AR (including THA and HA) and IF was far more than the number of patients we included. What's more, neither did the results of the current trial on mortality cross the traditional threshold (Z = 1.96) nor the threshold of sequential analysis, meaning that, until now, we are still not sure which treatment, AR or IF, has higher mortality and further research is needed. However, unlike results from sequential analysis of mortality, results on reoperation rate, complications, and pain showed positive findings. Not only did they cross the traditional threshold (Z = 1.96), but they also crossed the threshold of sequential analysis. In other words, the cumulative evidence from the comparison of the risk of reoperation and complications between AR (including THA and HA) and IF were reliable and conclusive. Therefore, there should be no need for further research on the comparison between AR and IF in terms of reoperation rate and postoperative complication.
However, there are 3 limitations to our study. First, some of the trials included in this meta-analysis may have deficiencies in the methodologic quality. For instance, there are 4 studies[30–33] that adopted quasi-random or nonrandom methods to conduct their research. One study[34] failed to conceal random allocation, and only several studies[12,28–30,34–36] made it clear that they had used blinding for the type of treatment. For another, although we conducted the subgroup analysis on THA or HA, the effects of different types of AR (THA or HA, cemented or un-cemented) and IF (screws, plates, etc.) on the treatment outcomes were unavoidable. Besides, we included a relatively massive number of studies from 1979 to 2018, in which there may be some unknown biases and high heterogeneity. In addition, although there were some similar meta-analyses[50–52] published before, our study here had its own advantages. First of all, far more recent research and a considerable number of patients were included in our meta-analysis, which was more likely to offer reliable and convincing conclusions. Also, we applied many methods to evaluate the quality and heterogeneity of each RCT. Most importantly, when compared to other meta-analyses, this meta-analysis was highlighted by the application of TSA, that showed its outstanding advantages of evaluating the reliability and conclusiveness of the acquired studies on the major results. Under TSA, we could safely draw the conclusion that AR was indeed superior to IF concerning reoperation rate, complications, and postoperation pain in the treatment of the femoral neck fracture.
5. Conclusion
In summary, we recommend that the AR should be considered first in the treatment of elderly patients with displaced femoral neck fractures. And, as we have obtained sufficient evidence so far, more studies on the comparison of reoperation rate, complications, and postoperation pain between AR and IF might only outlive their usefulness in the future. Still, more well-designed and high-quality research with long-term follow-ups are needed to determine the optimal treatment with lower mortality.
Acknowledgments
This research is supported by the projects of the international cooperation and exchanges of the National Natural Science Foundation of China (81520108017).
Supplementary Material
References
- 1.Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;11:897–902. [DOI] [PubMed] [Google Scholar]
- 2.Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;12:1726–1733. [DOI] [PubMed] [Google Scholar]
- 3.Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359:1761–1767. [DOI] [PubMed] [Google Scholar]
- 4.van Balen R, Steyerberg EW, Polder JJ, et al. Hip fracture in elderly patients: outcomes for function, quality of life, and type of residence. Clin Orthop Relat Res. 2001;390:232–243. [PubMed] [Google Scholar]
- 5.Murphy DK, Randell T, Brennan KL, et al. Treatment and displacement affect the reoperation rate for femoral neck fracture. Clin Orthop Relat Res. 2013;471:2691–2702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bhandari M, Devereaux PJ, Swiontkowski MF, et al. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. J Bone Joint Surg Am. 2003;85:1673–1681. [DOI] [PubMed] [Google Scholar]
- 7.Ye CY, Liu A, Xu MY, et al. Arthroplasty versus internal fixation for displaced intracapsular femoral neck fracture in the elderly: systematic review and meta-analysis of short- and long-term effectiveness. Chin Med J (Engl). 2016;129:2630–2638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.van Vugt AB, Oosterwijk WM, Goris RJ. Osteosynthesis versus endoprosthesis in the treatment of unstable intracapsular hip fractures in the elderly. A randomised clinical trial. Arch Orthop Trauma Surg. 1993;113:39–45. [DOI] [PubMed] [Google Scholar]
- 9.Ravikumar KJ, Marsh G. Internal fixation versus hemiarthroplasty versus total hip arthroplasty for displaced subcapital fractures of femur—13 year results of a prospective randomised study. Injury. 2000;31:793–797. [DOI] [PubMed] [Google Scholar]
- 10.Sikorski JM, Barrington R. Internal fixation versus hemiarthroplasty for the displaced subcapital fracture of the femur. A prospective randomised study. J Bone Joint Surg Br. 1981;63-B:357–361. [DOI] [PubMed] [Google Scholar]
- 11.Parker MJ, Pryor GA. Internal fixation or arthroplasty for displaced cervical hip fractures in the elderly: a randomised controlled trial of 208 patients. Acta Orthop Scand. 2000;71:440–446. [DOI] [PubMed] [Google Scholar]
- 12.Frihagen F, Nordsletten L, Madsen JE. Hemiarthroplasty or internal fixation for intracapsular displaced femoral neck fractures: randomised controlled trial. BMJ. 2007;335:1251–1254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Parker MJ, Khan RJ, Crawford J, et al. Hemiarthroplasty versus internal fixation for displaced intracapsular hip fractures in the elderly. A randomised trial of 455 patients. J Bone Joint Surg Br. 2002;84:1150–1155. [DOI] [PubMed] [Google Scholar]
- 14.Parker M, Johansen A. Hip fracture. BMJ. 2006;333:27–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Parker MJ. Hemiarthroplasty versus internal fixation for displaced intracapsular fractures of the hip in elderly men: a pilot randomised trial. Bone Joint J. 2015;97-B:992–996. [DOI] [PubMed] [Google Scholar]
- 16.Lu Q, Tang G, Zhao X, et al. Hemiarthroplasty versus internal fixation in super-aged patients with undisplaced femoral neck fractures: a 5-year follow-up of randomized controlled trial. Arch Orthop Trauma Surg. 2017;137:27–35. [DOI] [PubMed] [Google Scholar]
- 17.Cao L, Wang B, Li M, et al. Closed reduction and internal fixation versus total hip arthroplasty for displaced femoral neck fracture. Chin J Traumatol. 2014;17:63–68. [PubMed] [Google Scholar]
- 18.Stoen RO, Lofthus CM, Nordsletten L, et al. Randomized trial of hemiarthroplasty versus internal fixation for femoral neck fractures: no differences at 6 years. Clin Orthop Relat Res. 2014;472:360–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Johansson T. Internal fixation compared with total hip replacement for displaced femoral neck fractures: a minimum fifteen-year follow-up study of a previously reported randomized trial. J Bone Joint Surg Am. 2014;96:e46. [DOI] [PubMed] [Google Scholar]
- 20.McInnes MDF, Moher D, Thombs BD, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. JAMA. 2018;319:388–396. [DOI] [PubMed] [Google Scholar]
- 21.Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Brok J, Thorlund K, Gluud C, et al. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta-analyses. J Clin Epidemiol. 2008;61:763–769. [DOI] [PubMed] [Google Scholar]
- 24.Wetterslev J, Thorlund K, Brok J, et al. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J Clin Epidemiol. 2008;61:64–75. [DOI] [PubMed] [Google Scholar]
- 25.Wang G, Liu H, Wang C, et al. Cinacalcet versus Placebo for secondary hyperparathyroidism in chronic kidney disease patients: a meta-analysis of randomized controlled trials and trial sequential analysis. Sci Rep. 2018;8:3111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Leonardsson O, Sernbo I, Carlsson A, et al. Long-term follow-up of replacement compared with internal fixation for displaced femoral neck fractures: results at ten years in a randomised study of 450 patients. J Bone Joint Surg Br. 2010;92:406–412. [DOI] [PubMed] [Google Scholar]
- 27.Johansson T, Jacobsson SA, Ivarsson I, et al. Internal fixation versus total hip arthroplasty in the treatment of displaced femoral neck fractures: a prospective randomized study of 100 hips. Acta Orthop Scand. 2000;71:597–602. [DOI] [PubMed] [Google Scholar]
- 28.Keating JF, Grant A, Masson M, et al. Randomized comparison of reduction and fixation, bipolar hemiarthroplasty, and total hip arthroplasty. Treatment of displaced intracapsular hip fractures in healthy older patients. J Bone Joint Surg Am. 2006;88:249–260. [DOI] [PubMed] [Google Scholar]
- 29.Davison JN, Calder SJ, Anderson GH, et al. Treatment for displaced intracapsular fracture of the proximal femur. A prospective, randomised trial in patients aged 65 to 79 years. J Bone Joint Surg Br. 2001;83:206–212. [DOI] [PubMed] [Google Scholar]
- 30.Heetveld MJ, Raaymakers EL, Luitse JS, et al. Femoral neck fractures: can physiologic status determine treatment choice? Clin Orthop Relat Res. 2007;461:203–212. [DOI] [PubMed] [Google Scholar]
- 31.Soreide O, Molster A, Raugstad TS. Internal fixation versus primary prosthetic replacement in acute femoral neck fractures: a prospective, randomized clinical study. Br J Surg. 1979;66:56–60. [DOI] [PubMed] [Google Scholar]
- 32.Skinner P, Riley D, Ellery J, et al. Displaced subcapital fractures of the femur: a prospective randomized comparison of internal fixation, hemiarthroplasty and total hip replacement. Injury. 1989;20:291–293. [DOI] [PubMed] [Google Scholar]
- 33.Svenningsen S, Benum P, Nesse O, et al. [Femoral neck fractures in the elderly—a comparison of 3 treatment methods]. Nord Med. 1985;100:256–259. [PubMed] [Google Scholar]
- 34.Mouzopoulos G, Stamatakos M, Arabatzi H, et al. The four-year functional result after a displaced subcapital hip fracture treated with three different surgical options. Int Orthop. 2008;32:367–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tidermark J, Ponzer S, Svensson O, et al. Internal fixation compared with total hip replacement for displaced femoral neck fractures in the elderly. A randomised, controlled trial. J Bone Joint Surg Br. 2003;85:380–388. [DOI] [PubMed] [Google Scholar]
- 36.Blomfeldt R, Tornkvist H, Ponzer S, et al. Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled trial performed at four years. J Bone Joint Surg Am. 2005;87:1680–1688. [DOI] [PubMed] [Google Scholar]
- 37.Jonsson B, Sernbo I, Carlsson A, et al. Social function after cervical hip fracture. A comparison of hook-pins and total hip replacement in 47 patients. Acta Orthop Scand. 1996;67:431–434. [DOI] [PubMed] [Google Scholar]
- 38.Neander G, Adolphson P, von Sivers K, et al. Bone and muscle mass after femoral neck fracture. A controlled quantitative computed tomography study of osteosynthesis versus primary total hip arthroplasty. Arch Orthop Trauma Surg. 1997;116:470–474. [DOI] [PubMed] [Google Scholar]
- 39.van Dortmont LM, Douw CM, van Breukelen AM, et al. Cannulated screws versus hemiarthroplasty for displaced intracapsular femoral neck fractures in demented patients. Ann Chir Gynaecol. 2000;89:132–137. [PubMed] [Google Scholar]
- 40.Puolakka TJ, Laine HJ, Tarvainen T, et al. Thompson hemiarthroplasty is superior to Ullevaal screws in treating displaced femoral neck fractures in patients over 75 years. A prospective randomized study with two-year follow-up. Ann Chir Gynaecol. 2001;90:225–228. [PubMed] [Google Scholar]
- 41.Rogmark C, Carlsson A, Johnell O, et al. A prospective randomised trial of internal fixation versus arthroplasty for displaced fractures of the neck of the femur. Functional outcome for 450 patients at two years. J Bone Joint Surg Br. 2002;84:183–188. [DOI] [PubMed] [Google Scholar]
- 42.Roden M, Schon M, Fredin H. Treatment of displaced femoral neck fractures: a randomized minimum 5-year follow-up study of screws and bipolar hemiprostheses in 100 patients. Acta Orthop Scand. 2003;74:42–44. [DOI] [PubMed] [Google Scholar]
- 43.Bjorgul K, Reikeras O. Hemiarthroplasty in worst cases is better than internal fixation in best cases of displaced femoral neck fractures: a prospective study of 683 patients treated with hemiarthroplasty or internal fixation. Acta Orthop. 2006;77:368–374. [DOI] [PubMed] [Google Scholar]
- 44.Parker MJ, Pryor G, Gurusamy K. Hemiarthroplasty versus internal fixation for displaced intracapsular hip fractures: a long-term follow-up of a randomised trial. Injury. 2010;41:370–373. [DOI] [PubMed] [Google Scholar]
- 45.Chammout GK, Mukka SS, Carlsson T, et al. Total hip replacement versus open reduction and internal fixation of displaced femoral neck fractures: a randomized long-term follow-up study. J Bone Joint Surg Am. 2012;94:1921–1928. [DOI] [PubMed] [Google Scholar]
- 46.Hedbeck CJ, Inngul C, Blomfeldt R, et al. Internal fixation versus cemented hemiarthroplasty for displaced femoral neck fractures in patients with severe cognitive dysfunction: a randomized controlled trial. J Orthop Trauma. 2013;27:690–695. [DOI] [PubMed] [Google Scholar]
- 47.Hudson JI, Kenzora JE, Hebel JR, et al. Eight-year outcome associated with clinical options in the management of femoral neck fractures. Clin Orthop Relat Res. 1998;348:59–66. [PubMed] [Google Scholar]
- 48.Parker MJ, Raghavan R, Gurusamy K. Incidence of fracture-healing complications after femoral neck fractures. Clin Orthop Relat Res. 2007;458:175–179. [DOI] [PubMed] [Google Scholar]
- 49.Parker MJ, Gurusamy K. Internal fixation versus arthroplasty for intracapsular proximal femoral fractures in adults. Cochrane Database Syst Rev. 2006;4:CD001708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Gao H, Liu Z, Xing D, et al. Which is the best alternative for displaced femoral neck fractures in the elderly?: A meta-analysis. Clin Orthop Relat Res. 2012;470:1782–1791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Jiang J, Yang CH, Lin Q, et al. Does arthroplasty provide better outcomes than internal fixation at mid- and long-term followup? A meta-analysis. Clin Orthop Relat Res. 2015;473:2672–2679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Dai Z, Li Y, Jiang D. Meta-analysis comparing arthroplasty with internal fixation for displaced femoral neck fracture in the elderly. J Surg Res. 2011;165:68–74. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.