

Abstract
Several important findings bearing on the prevention, detection and management of hypertension have been reported since publication of the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) Blood Pressure (BP) Guideline. This review summarizes and places in context the results of relevant observational studies, randomized clinical trials and meta-analyses published between January, 2018 and March, 2021. Topics covered include BP measurement, patient evaluation for secondary hypertension, cardiovascular disease (CVD) risk assessment and BP threshold for drug therapy, lifestyle and pharmacologic management, treatment target BP goal, management of hypertension in older adults, diabetes mellitus, chronic kidney disease, resistant hypertension, and optimization of care using patient, provider and health system approaches. Presenting new information in each of these areas has the potential to increase hypertension awareness, treatment and control which remain essential for the prevention of CVD and mortality in the future.
Keywords: blood pressure, hypertension, prevention, treatment, diagnosis, High Blood Pressure
Introduction
Globally, high blood pressure (BP) is the leading risk factor for cardiovascular disease (CVD) morbidity and mortality.1 In the United States, high BP ranks first among modifiable risk factors in population attributable CVD risk, accounting for the largest proportion of coronary heart disease (CHD), heart failure (HF) and stroke events.2 In adults with hypertension, control of BP with antihypertensive medication reduces the risk of CVD and all-cause mortality.3,4 Thus, hypertension is one of the most consequential and remediable threats to the health of individuals and society.
While BP lowering interventions can be used to prevent CVD events and mortality, this can only be achieved by preventing high BP and recognizing, treating and controlling hypertension.5 The first step in managing hypertension is accurate diagnosis. Once hypertension has been confirmed, lifestyle modification and pharmacological treatment can be initiated to reduce BP and CVD risk. Titration of nonpharmacological and medication interventions to maximum tolerable effectiveness and long-term persistence with the treatment regimen are essential for optimal BP control and CVD risk reduction.
In the United States, progress in the quest to reduce population BP over the past several decades has been quantified as trends in hypertension awareness, treatment and control to an SBP/DBP <140/90 mm Hg. In an analysis of National Health and Nutrition Examination Survey (NHANES) data, hypertension (SBP ≥140 mm Hg, DBP ≥90 mm Hg, or taking antihypertensive medication) awareness and treatment increased significantly in all age groups between 1999-2004 and 2011-2016 (approximately 85 and 79%, respectively, for adults ≥65 years in 2011-2016). However, the improvements primarily occurred between 1999-2004 and 2005-2010.6 Hypertension awareness and treatment rates in 2011-2016 were relatively high, providing limited opportunity for improvement. In contrast, NHANES analyses identify markedly suboptimal rates of BP control.6,7 Among all adults with hypertension, the proportion with BP controlled to a systolic BP (SBP)/diastolic BP (DBP) <140/90 mm Hg increased from 31.8% in 1999-2000 to 48.5% in 2007-08, peaked at 53.8% in 2013-14, and then declined to 43.7% in 2017-18.7 Among adults taking antihypertensive medication, the prevalence of SBP/DBP control to <140/90 mm Hg increased from 53.4% in 1999-2000 to 68.3 % in 2007-08, peaked at 72.2% in 2013-2014, and then declined to 64.8% in 2017-18, such that control rates in 2017-18 were similar to those in 2005-6.7 From a public health perspective, the substantial reduction in BP control from 2013-14 to 2017-18 is alarming.
In December 2013, the panel members appointed to the eighth Joint National Committee (JNC-8) published a report recommending a higher BP goal (SBP/DBP <150/90 mm Hg) for adults ≥ 60 years compared with the 2003 JNC-7 recommended target (SBP/DBP <140/90 mm Hg).8,9 A minority report from five of the 17 JNC-8 panel members warned that relaxation of the BP goal would reduce the intensity of antihypertensive drug therapy and level of BP control.10 In March 2017, a clinical practice guideline from the American College of Physicians (ACP) and the American Academy of Family Physicians (AAFP) also recommended initiation of antihypertensive treatment in adults ≥60 years with an SBP persistently ≥150 mm Hg to achieve an SBP <150 mm Hg, with the possibility of a lower initiation and target SBP of 140 mm Hg in those with a history of stroke, a transient ischemic attack, or other evidence of high CVD risk.11 It is conceivable that the JNC-8 panel members and ACP/AAFP guideline reports may be responsible for the diminution in hypertension control. In November 2017, the American College of Cardiology (ACC)/American Heart Association (AHA) in partnership with nine other professional societies published a BP guideline that redefined hypertension as a persistent average SBP ≥130 mm Hg or DBP ≥80 mm Hg (SBP ≥ 130 mm Hg for those ≥ 65 years of age), lowered the drug treatment threshold to an average SBP ≥ 130 mm Hg or DBP ≥80 mm Hg for adults with a 10-year atherosclerotic CVD (ASCVD) risk ≥10% and reduced the SBP/DBP goal of therapy to <130/80 mm Hg (SBP<130 mm Hg for those ≥ 65 years).12 These changes were prompted by data showing an approximately 2-fold increase in CVD events and mortality in adults with BP 130-139/80-89 mm Hg compared to those with normal BP (<120/80 mm Hg), attributable risk estimates that this category of BP accounts for more than 20% of the BP-related CVD events, the results of multiple randomized clinical trials [including the PREVER-Prevention Trial and the Systolic BP Intervention Trial (SPRINT)] and meta-analyses of trials showing reduced CVD events and death with goal BP <130/80 mm Hg.12 While the ACP and AAFP11 failed to endorse the 2017 ACC/AHA Guideline recommendations for a lower BP goal, the Guideline has been embraced by most professional societies with an interest in BP and by US governmental agencies, including the National Center for Health Statistics (NCHS) that oversees the NHANES. Adoption of the ACC/AHA recommendations has the potential to increase hypertension awareness, treatment and control, both by increasing the proportion of adults taking antihypertensive medication and by treatment intensification for those with BP levels above target.
A substantial worldwide decline in population BP has occurred since the initiation of hypertension prevention, detection, treatment and control programs in the 1960s and 70s.13 These BP reductions have been noted in high risk, socioeconomically disadvantaged populations, including in the Southeastern region of the United States, where population SBP levels declined by as much as 18 mm Hg over a 40 year period.14 This seems to have resulted from a downward shift in average BP across the entire distribution of BP, suggesting an effect of lifestyle changes in addition to pharmacologic antihypertensive treatment.
This review focuses on the prevention, detection and management of hypertension with emphasis on new information since the publication of the 2017 ACC/AHA BP Guideline12.
BP Measurement and the Diagnosis of Hypertension
The ability to measure BP accurately remains a major challenge for providers managing patients with hypertension. Office BP measurements for clinical care are meant to be similar to those utilized in the observational cohort studies that have documented risk at a given BP level and the antihypertensive clinical outcome trials that have documented the benefit of BP lowering.12,15 However, the time required for staff training and the need for efficiencies in provider workflow patterns continue to compromise the validity of office BP measurements used for diagnosing hypertension and assessing success in achieving hypertension treatment targets.15,16
The 2017 ACC/AHA BP Guideline supports use of oscillometric devices to obtain automated office BP (AOBP) measurements and recommends out-of-office BP readings to confirm high BPs in the office, and to recognize masked hypertension (MH) and white coat hypertension (WCH).12 The European Society of Hypertension recommended out-of-office BP in 2007 as a complement to office BP measurement.17 The National Institute for Health and Care Excellence (NICE) clinical guideline in 2010 was the first to recommend confirmation of the hypertension diagnosis using out-of-office measurements, although this was primarily to exclude overtreatment of patients with WCH.18 Since the publication of the 2017 ACC/AHA Guideline, other national guidelines have also recommended the use of out-of-office readings to exclude WCH and MH, though these readings were recommended to be complementary rather than preferred to office readings.19,20 Differences between office BP, AOBP, HBPM and ABPM are summarized in Supplemental Figure I.
AOBP monitors that can be programed to measure multiple BP readings automatically after the recommended rest period were also promoted by the 2017 ACC/AHA Guideline and 2019 AHA Scientific Statement.12,15 While earlier data suggested that BP varied with the presence or absence of staff during BP measurement with these devices,21 more recent studies have refuted this concern when the core recommendations for accurate measurement are respected.22–24 However, less active staff involvement can result in less staff time per reading compared to manual measurement (and potential cost savings).25 A challenge to the use of oscillometric devices in place of mercury and aneroid sphygmomanometers in clinical practice and research is the lack of independent validation of many such devices and the lack of requirement for validation of devices sold in most countries, including the US.15,26 Unfortunately, only 1 in 5 automated devices are validated for accuracy.27 Online listing of validated devices, including the newly released U.S. Blood Pressure Validated Device Listing are now readily available.28,29 Although well-designed comparisons of ABPM and HBPM are not available, some helpful reports have been published during the last two years. In a study of participants (N=333) with office BP < 140/90, ABPM was more sensitive in detecting MH than HBPM, with a MH prevalence of 25.8% overall and 11.1% at home, with 29-29.5% showing MH by both techniques. 30 In another study, HBPM was as effective as ABPM in predicting left ventricular mass index.31 A comparison of office and out-of-office BP measuring techniques is shown in Table 1.
Table 1.
Comparison of Office BP, Automated Office BP, ABPM and HBPM
| Characteristic | Standard Office BP | Automated Office BP (AOBP) | ABPM | HBPM |
|---|---|---|---|---|
| Measurement parameter(s) | Resting office BP | Resting office BP | Dynamic daytime BP (responses to exercise, meals, drugs); BP pattern (NH, nocturnal BP dipping, early AM BP surge) | Resting home BP |
| Detects WCH | No | No | Yes | Yes |
| Detects MH | No | No | +++ | ++ |
| Sensitivity for estimating CVD event risk | + | + | +++ | ++ |
| Sensitivity for estimating LVH risk | − | − | ++ | ++ |
| Use with BP telemonitoring | No | No | ++ | +++ |
ABPM, ambulatory blood pressure monitoring; BP, blood pressure; CVD, cardiovascular disease; HBPM, home blood pressure monitoring; LVH, left ventricular hypertrophy; MH, masked hypertension; NH, nocturnal hypertension; WCH, white coat hypertension.
Despite its lower sensitivity in detecting MH, HBPM remains the most practical option for recognition of MH and WCH as well as for BP monitoring, especially during medication titration and monitoring of treatment BP levels. However, careful attention to patient education is required in order for providers to have confidence accepting HBPM data over office readings to determine BP control (Table 2).12,32,33 In a study of community-dwelling adults (N=318), two readings taken in the morning and evening for a minimum of 3 days have proven sufficient for reliable estimation of out-of-office BP and for confirming the diagnosis of hypertension.34 HBPM has been particularly useful with the increasing need for virtual visits to manage hypertension during the COVID-19 pandemic.
Table 2.
Procedures for Use of HBPM*
| Instructions to staff |
| Patient training should occur under medical supervision and include: |
| • Information about hypertension |
| • Advice in selection of BP monitor |
| • Acknowledgment that individual BP readings may vary substantially |
| • Interpretation of results |
| Devices: |
| • Verify use of validated automated devices. Use of auscultatory devices (mercury, aneroid, or other) is not generally useful for HBPM because patients rarely master the technique required for measurement of BP with auscultatory devices. |
| • Monitors with provision for storage of readings in memory are preferred. |
| • Verify use of appropriate cuff size to fit the arm (Table 9). |
| • Verify that left/right inter-arm differences are insignificant. If differences are significant, instruct patient to measure BPs in the arm with higher readings. |
| Instructions Provided to Patients |
| Instructions on HBPM procedures: |
| • Avoid smoking, caffeinated beverages, or exercise within 30 min before BP measurements. |
| • Ensure ≥5 min of quiet rest before BP measurements. |
| • Sit correctly: |
| • Back straight and supported |
| • Sit with feet flat on the floor and legs uncrossed. |
| • Arm supported on a flat surface (such as a table), with the upper arm at heart level. |
| • Bottom of the cuff placed above the antecubital fossa (bend of the elbow). |
| • Remain still during BP measurement: |
| • Take multiple readings: |
| • At least 2 readings 1 min apart in morning before taking medications and in evening. |
| • Measure and record BP daily during week before a clinic visit and when instructed. |
| • Record all readings accurately: |
| • Monitors with built-in memory should be brought to all clinic appointments. |
| • BP should be based on an average of readings on ≥2 occasions for clinical decision making. |
Adapted from: Whelton PK, Carey RM, Aranow W, et al: Hypertension. 2018;71:e13-e115
Note: We encourage training and certification through PAHO or AHA/AMA Target BP virtual courses.
AHA, American Heart Association; AMA, American Medical Association; BP, blood pressure; HBPM, home blood pressure monitoring; PAHO, Pan American Health Organization.
Newer technologies for BP measurement that are less intrusive and provide a more complete profile of BP are on the horizon.35 These will require both validation for accuracy and their capacity to predict clinical outcomes. The ability to measure and compare central to brachial BP was proposed as a better way to predict CVD risk.36 However, a recent study in a large cohort (N = 13,461) suggested that measurement of central BP using the Sphygmocor device was no more predictive of CVD outcomes than AOBP readings obtained with the Omron 907 device.37
Patient Evaluation: Screening for Secondary Hypertension
The 2017 ACC/AHA Guideline provides detailed guidance on historical, physical and laboratory features that may suggest secondary hypertension and merit additional testing.12 It is particularly important to consider an evaluation for secondary causes when the patient is young or the hypertension is resistant to treatment. Identification of a secondary cause may cure hypertension, or improve BP control if a cure is not feasible. The approaches to management of renovascular hypertension and primary aldosteronism have recently been modified.
Renovascular hypertension
Several randomized controlled trials (RCTs) of renal artery interventions in ASCVD renovascular hypertension have failed to demonstrate an improvement in mortality or renal survival 38. A recent systematic review of 8 major RCTs reported reduction in DBP and the number of antihypertensive medications needed, but no differences in SBP or renal function after angioplasty.39
Even when significant ASCVD renal artery stenosis is confirmed, the optimal course of treatment is not clear, particularly with unilateral lesions.40 In most cases, unilateral lesions can be managed using medical therapy (renin-angiotensin system blockade) with periodic surveillance to ensure adequate perfusion of the contralateral non-stenotic kidney. However, for some patients, particularly those who are younger, have sudden onset of hypertension or have radiologic features that suggest fibromuscular dysplasia (FMD), direct intervention is often sensible (Table 3).41 For FMD this should consist of angioplasty without stents, whereas stents are needed for most atherosclerotic lesions to maintain long-term patency. For patients with bilateral hemodynamically significant stenosis, defined as a stenosis greater than 75%, intra-arterial intervention should be considered with careful assessment of patient risk for complications, especially renal athero-embolic events. In patients at high risk for complications from intra-arterial intervention, a trial of renin-angiotensin system blockade is an appropriate first step with careful monitoring of kidney function. If creatinine rises more than 30% or the patient develops sudden (flash) pulmonary edema, this will suggest the need for an invasive approach. Patients with severe bilateral stenosis were not included in the RCTs and require careful individualized decision-making with consideration of intervention to preserve kidney function.
Table 3.
Clinical Approaches to Renovascular Hypertension Evaluation and Treatment
| Cause | Patient characteristics | Risk factors | Screening, initial approaches | Confirmatory testing | Management options |
|---|---|---|---|---|---|
| Fibromuscular dysplasia | Female prevalence, age of onset 30s-50s, association with smoking, some with family history | Smoking | CT angiography MR angiography if CT not an option, Doppler US at specialized centers | Renal angiography | Angioplasty without stenting, rarely recurs vs medical therapy with renin-angiotensin blockade |
| Atherosclerotic disease | Male prevalence, older age of onset associated with atherosclerosis in multiple vascular beds, association with smoking, hyperlipidemia | CVD risk factors including smoking, hyperlipidemia | Doppler US CT or MR angiography | Renal angiography if intervention indicated | Unilateral disease: Medical therapy using renin-angiotensin blockade and management of CVD risk factors with interval monitoring of renal function and perfusion |
| Bilateral disease: Medical therapy using renin-angiotensin blockade and management of CVD risk factors with interval monitoring of renal function and perfusion, vs angioplasty with stenting with careful assessment of risks of intervention | |||||
| Aortic coarctation | Onset of hypertension prior to age 30 years, claudication symptoms | Bicuspid aortic valve | Measurement of brachial and popliteal BP CT angiography |
CT angiography | Referral to congenital heart disease or vascular medicine specialist |
CT, computerized tomography; CVD, cardiovascular disease; MR, magnetic resonance; US, ultrasound.
Primary aldosteronism
New evidence suggests that primary aldosteronism is part of a spectrum of aldosterone excess states. Recent publications suggest aldosterone excess plays a role in primary hypertension or intermediate conditions of relative aldosterone excess, a forme fruste of the full primary aldosteronism state. Data from Brown et.al.42 support consideration of primary aldosteronism even when the plasma aldosterone/renin ratio (ARR) screening test is negative. In an analysis of patient cohorts at 4 centers, including participants with normal BP, untreated stage 1 and stage 2 hypertension, and treated resistant hypertension (RH), ARR was compared to urinary aldosterone excretion measured after oral salt loading. Using a urinary aldosterone level > 12 ug/24h as the threshold for diagnosis, primary aldosteronism was present in 11.3% of normotensive patients, and up to 22% of those with hypertension, with increasing prevalence associated with greater severity of hypertension. The ARR had poor sensitivity and negative predictive value, particularly when renin was suppressed.42 Cohen et al.43 reported very low (1.6%) utilization of ARR screening for patients with RH in the Veterans Administration system suggesting that many cases of primary aldosteronism are missed. These findings suggest that aldosterone excess may play a role even in primary hypertension and may be unrecognized as a contributor to RH (Figure 1). For hypertensive patients with suppressed renin levels, especially those with uncontrolled or RH, it is important to go beyond the ARR to measure urinary aldosterone excretion under salt-loading conditions. Further, the concept of a spectrum of aldosterone excess mediated mechanisms may explain the effectiveness of mineralocorticoid receptor antagonists (MRAs) observed in the PATHWAY-2 trial of RH.44
Figure:
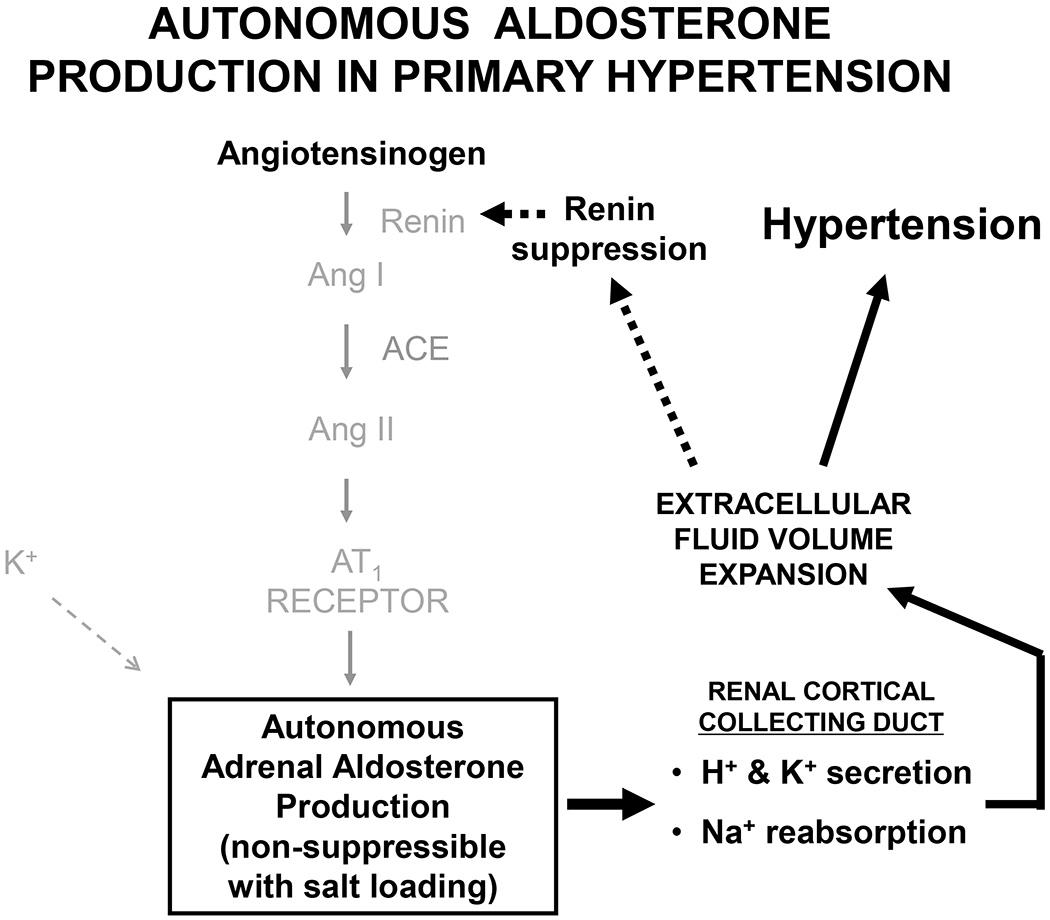
Schematic representation of the mechanisms of autonomous aldosterone production in primary hypertension. Aldosterone production from the adrenal zona glomerulosa is independent of the renin-angiotensin system and is not suppressible with dietary sodium loading. Excess aldosterone expands extracellular fluid volume by augmenting sodium reabsorption in the renal cortical collecting duct. Expanded fluid volume leads to hypertension and suppression of renin and the entire renin-angiotensin cascade. Increased aldosterone production is abnormal in the face of renin suppression but plasma aldosterone concentrations are lower than those of patients with classical overt primary aldosteronism. ACE, angiotensin converting enzyme; Ang, angiotensin; AT1, angiotensin type-1. Dashed line and grey tone indicates suppression.
CV Risk Assessment and BP Threshold for Drug Therapy
The 2017 ACC/AHA BP Guideline based decisions regarding initiation of medication on level of BP and estimation of ASCVD risk, supported by evidence from clinical trials and meta-analyses.12 The ACC/AHA risk calculator provides guidance for patients age 40-79 years, but does not apply to younger patients where data are lacking. Based on average risk in the landmark antihypertensive drug trials, a 10-year ASCVD ≥10% was identified as the cut point for definition of high risk.
Treatment of hypertension in young adults
With rising rates of overweight and obesity, in the US and globally, the prevalence of hypertension and diabetes mellitus (DM) resulting from insulin resistance has increased and may carry greater risk in the context of multiple CVD risk factors, even in the young.1 For young patients with isolated hypertension, lifetime risk of ASCVD is high. As the overall distribution of BP has shifted to a lower average value in the community, more CVD events are occurring at lower BP levels.14,45 This was recently shown to be true for young adults with hypertension who have earlier onset of CHD, HF, stroke, transient ischemic attacks and peripheral arterial disease requiring intervention. In the Coronary Artery Risk Development in Young Adults (CARDIA) longitudinal study of 3851 young adults followed over a median of 18.8 years, only 4% were taking medication for hypertension.46 Adjusted hazard ratios (HRs) for CVD events were 1.67 [95% confidence interval (CI), 1.01-2.77], 1.75 (95% CI, 1.22-2.53), and 3.49 (95% CI, 2.42-5.05), for elevated BP, and ACC/AHA stage 1 and stage 2 hypertension, respectively, compared to controls with normal BP.46 Supplemented by evidence for target organ damage (TOD) including LVH47 and brain volume and white matter changes48, high BP in the young may no longer be considered benign. Therefore, it may not be appropriate to delay antihypertensive pharmacologic treatment, even while lacking event-based RCT evidence for prevention of ASCVD. Young patients are reported to have lower awareness, slower time to diagnosis and poorer BP control than older patients. Concerns raised by providers relate to labeling of young adults with illness, medication safety concerns, especially in women of childbearing age, concerns related to potential misdiagnosis, and impact on life insurance rates. Both DBP and SBP are important for prediction of CVD risk in young adults. In a recently reported risk analysis conducted in almost 6.5 million Koreans, aged 20-39 years at baseline, who were followed for a median of 13.2 years, ACC/AHA stage 1 isolated systolic hypertension, isolated diastolic hypertension, and systolic/diastolic hypertension were associated with multivariate-adjusted hazard ratios of 1.36, 1.32, and 1.67, respectively, compared to normal BP.49
The evidence suggests treatment of hypertension in the young using lifestyle modification with the addition of BP lowering medications when lifestyle interventions are inadequate. Allowing a period of 6 to 12 months to institute lifestyle modification is reasonable but only in the absence of TOD. There is an urgent need for hypertension treatment event-based RCTs in the young which will likely require measuring TOD endpoints rather than only CV events and death.
Lifestyle Management: The Cornerstone of Prevention and Treatment
Numerous environmental factors are associated with BP, especially components of diet, physical activity, and alcohol consumption. In many instances, changes in exposure to these factors has led to a corresponding change in BP, with the best proven interventions being a healthy diet, reduced sodium intake, weight loss, augmentation of potassium intake, physical activity, and abstinence or moderation in alcohol consumption.12,50 These six interventions are effective for prevention of hypertension, treatment of hypertension, enhancing the effect of antihypertensive medication, and reducing the number of drugs needed to control BP (Table 4).
Table 4.
Six Best Proven Nonpharmacological Recommendations for Prevention and Management of Hypertension.
| Recommendation | Intervention | Regimen and Dosage | Approximate SBP Lowering (mm Hg) | |
|---|---|---|---|---|
| Hypertension | No hypertension | |||
| Healthy diet | DASH diet is the best studied/proven healthy diet for BP lowering | Fruits, vegetables, whole grains, low-fat dairy products, with reduced saturated and total fat content. Limited dose-response information. | −5 | −3 |
| Weight loss | Calorie reduction and physical activity | Optimal goal is to achieve ideal body wight but any weight loss is desirable. Linear dose-response relationship. Expect about 1 mm Hg reduction in SBP for every 1 Kg weight loss. | −5 | −3 |
| Reduced dietary sodium intake | Dietary change | Optimal dietary intake goal is <1500 mg sodium/day, but any reduction is desirable. Linear dose-response relationship. Expect about 1-3 mm Hg reduction in SBP for a 1,000 mg reduction in sodium intake in adults with/without hypertension | −5 | −3 |
| Increased dietary potassium intake | Dietary change (preferred over pill supplementation) | Optimal goal of 3500 – 5000 mg potassium/day. Greater BP lowering identified in those consuming more dietary sodium. Nonlinear U-shaped dose-response relationship. Quality of evidence lower than for sodium reduction. | −5 | −3 |
| Physical activity | Aerobic exercise (best evidence) | Exercise such as brisk walking, 5-7 times /week (30-60 minutes/session), aiming for at least 150 minutes/week. Gradual start up. Warm up at start and cool down at end of each session. | −5 | −3 |
| Dynamic resistance exercise (evidence less robust) | Exercise such as weight-lifting or circuit training, at least 2-3 times/week. Generally requires guidance/supervision by exercise professional. Often used as a supplement to aerobic exercise. | −4 | −2 | |
| Isometric resistance exercise (evidence least robust) | Exercise such as hand-grip training regimens, at least 3-4 times/week. | −4 | −2 | |
| Moderation in alcohol intake | Reduction in alcohol consumption | In adults who drink alcohol, intake goal: Men: ≤2 standard drinks/day Women: ≤1 standard drink/day |
−4 | −3 |
DASH, dietary approaches to stop hypertension; SBP, systolic blood pressure.
A recent meta-analysis confirmed the efficacy of nonpharmacological interventions for prevention of hypertension in trials that were conducted in low- and middle-income countries.51 Fu et al.52 conducted a series of clinical trials network meta-analyses to estimate the comparative effectiveness of 22 different interventions for lowering BP in two groups of adults (those with an SBP ≥140 mm Hg, DBP ≥90 mm Hg, or taking antihypertensive medication, and those with an SBP 120-139 mm Hg or DBP 80-89 mm Hg). Based on the BP lowering effects in pooled analyses and the GRADE estimated quality of the underlying data53, they concluded that an intervention based on the Dietary Approaches to Stop Hypertension (DASH) was superior to usual care and all other nonpharmacological interventions in lowering SBP. Unfortunately, differences in study design, intervention methods, the samples studied, and other aspects of the clinical trials that were compared make it difficult to conduct a fair comparison. The greatest impediment to accepting the conclusion that the DASH diet provides superior BP lowering compared to the other interventions recommended in the 2017 ACC/AHA Guideline is that the DASH diet trials included in the Fu et al.52 meta-analyses were feeding studies, whereas most of the other interventions were evaluated in trials that employed behavior change interventions. Feeding studies provide a very efficient means to change diet but they are expensive and the efficacy in such studies is not generalizable. In clinical practice, behavior change and pill supplementation are the only practical approaches to implementing nonpharmacological recommendations, with behavior change being the preferred approach.12 In a three-arm behavioral change trial (N = 810; baseline mean SBP/DBP = 134.9/84.8 mm Hg), that compared usual care, an “established” BP lowering intervention (weight loss, sodium reduction, increased physical activity, and limited alcohol intake), and addition of the DASH diet to the “established” intervention, both active interventions were effective compared to usual care (approximately 4 mm Hg SBP net difference), but addition of the DASH diet to the “established” diet provided no additional statistically significant lowering of SBP (P = 0.43).54 It may be better to accept that each of the nonpharmacological interventions recommended in the 2017 ACC/AHA Guideline is effective and use of two or more interventions is likely to result in a more substantial effect.55 Likewise, each of the interventions has greater efficacy at higher starting levels of BP. A pragmatic approach in clinical and public health practice is to decide which of the proven interventions are likely to be of greatest benefit based on an individual’s or population’s lifestyle and their perceived willingness to embrace the interventions. Specifically, is overweight, excessive sodium or alcohol consumption, or unhealthy diet the biggest problem and which of the possible interventions is likely to be embraced with the most enthusiasm?
The greatest potential for a population-wide nonpharmacological intervention is gradual reduction in the addition of sodium during food processing and preparation.56 Resolve to Save Lives, the World Health Organization, the World Hypertension League and others are collaborating to achieve the goal of sodium reduction globally.57–60 A new biostatistical method, which facilitates aggregation of data from two-armed RCTs, the most common type of experimental contrast, has made estimation of the dose-response relationship between sodium and BP more feasible.61 Filippini et al.62 used this method to conduct a sodium-BP dose-response meta-analysis based on 81 clinical trials with a minimal duration of four weeks. They identified a substantially linear dose-response relationship between sodium intake and BP across the entire range of exposure, with a 100 mmol/d reduction in sodium being associated with a 5.43 mm Hg reduction in SBP. The results were similar for those with or without hypertension, except that the former group exhibited a steeper decrease in BP following sodium reduction. These findings support the lower sodium intake target (<1,500 mg/d) recommended by the AHA63, compared to the <2,300 mg/d target endorsed by the 2019 National Academies of Sciences, Engineering, and Medicine Dietary Reference Intakes Review Committee64, or the <2,000 mg/d target advocated in 2012 by the World Health Organization.65 However, the findings also suggest benefit from any reduction in sodium intake that can be achieved.
In a separate analysis of 32 RCTs, Filippini et al.66 reported a U-shaped pattern for the dose-response relationship between potassium intake and BP, with the optimal BP lowering effect occurring for potassium intakes in the range of 90-150 mmol/d. The BP lowering effect was greater in participants with compared to those without hypertension and for those at higher levels of sodium intake.
Several reports have confirmed the errors associated with use of spot urines to estimate 24-hour urinary sodium intake.67–70 Spot urines provide systematically biased estimates of 24-hour urinary excretion, with over-estimation at lower intakes of sodium and under-estimation at higher intakes.67 Likewise, use of spot urines to estimate 24-hour urinary sodium intake yields a J-shaped relationship with mortality whereas the relationship is linear when 24-hour urine collections are used to assess the relationship.67 The World Hypertension League published a position paper on use of spot urines, short duration timed collections, and 24-hour collections to assess dietary sodium intake.71 The position paper endorsed use of a single 24-hour urine measurement over a series of days from a representative population sample for estimation of a population’s current 24-hour dietary sodium ingestion and an average of at least three non-consecutive 24-hour urinary collections was recommended for estimation of current usual dietary sodium intake in individuals. Despite the well-documented errors resulting from use of spot urines to estimate average intake of dietary sodium, leading peer-reviewed journals continue to publish manuscripts in which dietary sodium intake has been estimated using spot urines. 72–74
Pharmacological Management
The 2017 ACC/AHA Guideline and other recent guidelines continue to recommend thiazide or thiazide-type diuretics, calcium channel blockers (CCBs), angiotensin converting enzyme inhibitors (ACEIs), and angiotensin receptor blockers (ARBs) as initial drug choices, and for subsequent add-on therapy, based on their efficacy in reducing BP and documented benefit in reducing clinical outcomes.12,19,75 Beta-blockers are generally not recommended as first line agents in patients without CHD or heart failure due to lesser benefit on stroke reduction compared with agents from the other recommended classes.12,20,75,76 Spironolactone or eplerenone are recommended for BP control in patients with RH.12,77
Chlorthalidone and indapamide, thiazide-like diuretics, have a longer duration of action compared to thiazide diuretics and are the preferred diuretics for management of hypertension. HCTZNetwork meta-analyses have shown benefit of chlorthalidone over HCTZ on clinical outcomes, although a large (N=730,225) retrospective, non-randomized observational study of new users of chlorthalidone (N=36,918) compared to HCTZ from administrative databases failed to document a significant difference in effectiveness.78 The VA Diuretic Comparison Project, a randomized comparison of chlorthalidone and HCTZ effects on clinical outcomes in 13,500 patients, is scheduled for completion by the end of 2022.79
Some glucose lowering agents, particularly glucagon-like peptide-1 (GLP-1) receptor agonists and sodium glucose cotransporter-2 (SGLT-2) inhibitors significantly improve CVD and kidney outcomes, especially in diabetic patients with and without hypertension. They also reduce BP significantly, with SGLT-2 inhibitors seeming to have the largest effect.80,81 The magnitude of BP lowering (2-4 mm Hg on 24 hour ABPM) with these agents is less than with most first-line antihypertensive agents. Given this and their greater cost, SGLT-2 inhibitors should be prescribed primarily for glucose lowering rather than for treatment of high BP.
Despite the lower BP targets recommended in the 2017 ACC/AHA Guideline, hypertension control rates in the US remain suboptimal even by the higher JNC-7 BP treatment targets, largely due to under-treatment, especially in Black patients.82 Quality improvement interventions have increased BP control overall and in race-ethnic subgroups, but a 5-10% difference in control rates persists between Black and non-Black adults. Clinician inertia and patient nonadherence to the prescribed treatment continue as major contributors to inadequate BP control. A recent report from a quality improvement project aimed at more accurate BP measurement, reducing therapeutic inertia, and increasing treatment adherence over 6 months demonstrated sustained SBP lowering of 12.7 mm Hg for an additional 6 months compared to a 5 mm Hg SBP decline during the baseline period in patients with uncontrolled BP, P<0.0001.83 However, clinician inertia was only reduced from 52% to 49.5%. No race/ethnic difference in BP control was noted with the BP regimen utilized in the SPRINT even in the < 120 mmHg arm where chlorthalidone, the primary diuretic, and amlodipine, the primary CCB, were provided at no cost to the study participants.84 The effectiveness, safety, and cost-effectiveness of 90 compared to 30 day prescription refills in improving adherence has also been demonstrated.85 The major elements of an effective antihypertensive drug treatment program are provided in Table 5.
Table 5.
Keys to Effective Blood Pressure Control in Adults with Hypertension
| 1. Agree (patient and provider) on blood pressure target |
| 2. Use fixed dose combinations |
| 3. Substitute long-acting chlorthalidone for hydrochlorothiazide (alternatively indapamide) |
| 4. Use long acting amlodipine as first line calcium channel blocker |
| 5. Monthly visits until blood pressure target achieved |
| 6. Replace prescription of 30 day with 90 day refills, if allowed |
| 7. Use telehealth strategies to augment office-based management |
| 8. Enhance connectivity between patient, provider and electronic health record for better feedback and communication |
| 9. Screen for social determinants of health and consideration of obstacles to care |
| 10. Use multidisciplinary team-based care to enhance lifestyle and medication adherence and to solve social issues |
BP Goal
RCTs have demonstrated that the risk of CVD can be greatly reduced with effective antihypertensive therapy.3,4 Choice of an optimal goal for BP treatment should be based on a balance between the best level for CVD prevention and the risk of untoward side effects resulting from the treatment.
On the basis of new evidence, the 2017 ACC/AHA Guideline reduced the SBP/DBP goal from that recommended in the 2003 JNC-7 [<140/90 mm Hg for most adults but <130/80 mm Hg for those with DM or chronic kidney disease (CKD)] to <130/80 mm Hg for most adults but an SBP <130 mm Hg for noninstitutionalized ambulatory community-dwelling adults ≥65 years of age.12 Evidence supporting this guideline change included results of the SPRINT as well as multiple systematic reviews and meta-analyses, as summarized in several post-guideline reports.86–88 In addition, a recent direct meta-analysis by Sakima et al.89, restricted to 19 trials in which adults with hypertension were randomly assigned to a different BP target, reported a significant reduction in major CVD events, MI and stroke in those assigned to more versus less intensive treatment and in subgroup analysis identified a BP target of < 130/80 mmHg as optimal for CVD protection. Likewise, a meta-analysis of four RCTs conducted in patients with prior stroke documented a significant reduction in recurrent stroke among those randomized to more intensive BP reduction.90
Concerns have been raised that the CVD and all-cause mortality benefit of intensive BP control in the SPRINT might have been offset by an increased rate of treatment adverse effects. This concern was largely assuaged by the recent demonstration that intensive BP control is not associated with other causes of hospitalization.91 Another widespread concern, especially in older adults, had been that more intensive antihypertensive treatment might increase the frequency and/or severity of orthostatic hypotension, leading to falls, syncope and/or CVD events. This concern was put to rest by two reports by Juraschek et al.92,93 examining the SPRINT data and the aggregated individual patient data from multiple clinical trials for association of intensive treatment with orthostatic hypotension. In the SPRINT, orthostatic hypotension was more common in the standard treatment group and was not associated with a higher rate of CVD events or with syncope, electrolyte abnormalities, injurious falls or acute renal failure.92,94 In the Juraschek et al.93 meta-analysis of 18,466 participants, including those in the SPRINT, intensive BP lowering treatment also reduced the risk of orthostatic hypotension, possibly due to improvement in baroreflex function and diastolic filling while reducing left ventricular hypertrophy and/or arterial stiffness. Thus, asymptomatic orthostatic hypotension during hypertension treatment should not trigger automatic down-titration of therapy, even in the setting of a lower BP goal.
The AHA’s Life’s Simple 7 focuses on cardiovascular health factors for primordial or primary prevention of CVD (smoking, body mass index, physical activity, total cholesterol, diet, BP and fasting glucose).95,96 The AHA Life’s Simple 7 online survey tool increases patient awareness of their BP and other related comorbidities such as DM, obesity and high sodium intake.97. Treating hypertension to goal aims to achieve ideal cardiovascular health.
Older Adults
Professional societies provide conflicting advice on best practices for management of hypertension in older adults. The 2017 ACC/AHA Guideline recommends a treatment goal of <130 mm Hg for noninstitutionalized ambulatory community-dwelling older adults (≥65 years of age) and an individualized team-based approach, based on clinical judgement and patient preference, for those with a high burden of comorbidity and limited life expectancy.12 In adults at high risk for CVD, including older adults, Hypertension Canada 2020 recommends initiation of antihypertensive medication in those with an SBP ≥130 mm Hg and treatment to an SBP goal <120 mm Hg.98 The National Heart Foundation of Australia hypertension guideline recommends initiating antihypertensive drug therapy in “patients at moderate absolute CVD risk (10-15% 5-year risk) with persistent BP ≥140 mm Hg and/or ≥90 mm Hg diastolic” and an initial SBP/DBP target of <140/90 mm Hg or lower, if tolerated, with an SBP goal of <120 mm Hg in older adults (>75 years), if tolerated.99 At the other extreme, the American College of Physicians (ACP) and American Academy of Family Physicians (AAFP) recommend that adults ≥60 years with a persistent SBP ≥150 mm Hg should be treated with antihypertensive medication to achieve a target SBP of <150 mm Hg, with consideration of a <140 mm Hg target in those with a history of stroke, transient ischemic attack, or other unspecified evidence of high risk for CVD.11
Population modeling studies100,101 have suggested substantial health benefits from implementation of the 2017 ACC/AHA Guideline recommendations compared with those in the 2003 JNC 7 Report9 or the 2014 JNC-8 Panel Members Report8. In US adults ≥40 years, Bundy et al.100 estimated that in comparison to the 2014 JNC-8 Panel Members Report recommendations, implementation of the 2017 ACC/AHA Guideline recommendations would result in an annual reduction of 340,000 CVD events and 157,000 deaths (Table 6). In an analysis confined to adults ≥60 years, Jaeger et al.102 identified a high 10-year risk of ASCVD (18.0%) in adults for whom the ACC/AHA but not the ACP/AAFP Guideline recommends antihypertensive drug therapy. Among adults already taking antihypertensive medication, the 10-year risk of ASCVD in those recommended intensification of therapy by the ACC/AHA, but not the ACP/AAFP, was also high (18.2%). Thus, the ACC/AHA Guideline is more effective than the ACP/AAFP Guideline in identifying adults ≥60 years of age at high CVD risk for the initiation and intensification of antihypertensive drug therapy.
Table 6.
Simulation study by Bundy et al.100 comparing estimated annual prevention of CVD events and deaths by adhering to 2014 JNC-8 panel recommendations or the 2017 ACC/AHA BP Guideline.
| Basis for Estimation | |
| (1) | Estimation of proportion of US adults in BP categories using NHANES |
| (2) | Incidence of major CVD events & all-cause mortality by modeling 4 large community-based cohort studies (ARCS, CV Health, Framingham, MESA) |
| (3) | Network meta-analysis (42 RCTs) to estimate HRs for outcomes and determine population-attributable risks and events reduced. |
| Characteristic | 2014 Evidence-Based Guideline | 2017 ACC/AHA Guideline |
|---|---|---|
| BP threshold (mm Hg) for initiation of antihypertensive drugs | ≥140/90 (<age 60) ≥150/90 (≥age 60) |
≥140/90 (gen. population) ≥130/80 (high CVD risk) |
| BP goal (mm Hg) of treatment | <140/90 (<age 60) <150/90 (≥age 60) |
<130/80 |
| Annual CVD event reduction (≥age 40) | 270,000 | 610,000 (NNT=70) |
| Annual reduction in death (≥age 40) | 177,000 | 334,000 (NNT=129) |
Note: Sensitivity analysis determined that, even if 100% implementation of the 2017 guideline were not achieved, the CVD event and death reductions would still be significantly larger compared to the 2014 guideline. ACC, American College of Cardiology; AHA, American Heart Association; ARCS, Atherosclerosis Risk in Communities Study, BP, blood pressure; CV, cardiovascular; CVD, cardiovascular disease; JNC, Joint National Committee; MESA, Multi-Ethnic Study of Atherosclerosis Study; NHANES, National Health and Nutrition Examination Survey; NNT, number needed to treat; RCT, randomized controlled trial.
During the past two years, several additional original research papers and meta-analyses have contributed to our understanding of the management of hypertension in older adults.103–106 In an analysis of the overall SPRINT cohort [N=9361; mean age=67.9 years; median follow-up (FU) = 3.34 years], mild cognitive impairment (MCI) was detected in 239 of the 4678 participants (16.2 per 1000 person-years) randomized to intensive antihypertensive treatment (SBP target <120 mm Hg) compared with 284 of the 4683 participants (19.4 per 1000 person-years) randomized to standard antihypertensive treatment (SBP target <140 mm Hg), resulting in a HR (95% CI) of 0.83, 0.70 – 0.99.103 In a randomized comparison of participants with a median FU of 5.11 years (trial and extended post-trial FU), there was a significant difference in both MCI (HR, 95% CI = 0.81, 0.69 – 0.95; P = 0.007) and the composite of dementia and MCI (HR, 95% CI = 0.85, 0.74 – 0.97; P = 0.01), and a nonsignificant trend for benefit in dementia per se (HR, 95% CI = 0.83, 0.67 – 1.04).103 During FU, CVD events occurred much earlier than dementia indicating the need for trials with a longer period of treatment and FU than occurred in the SPRINT where the trial was stopped prematurely due to CVD and all-cause mortality benefit after a median FU of only 3.26 years.
In a subset of 670 SPRINT participants (mean age = 67.3 years) who were evaluated with brain magnetic resonance imaging (MRI) at baseline and after four years of FU (N = 449), randomization to intensive treatment was associated with a smaller increase in cerebral white matter lesion volume, an independent risk factor for cognitive decline and dementia, compared to standard treatment during trial FU.104 Similar apparent MRI benefits were noted in the INFINITY trial and during extended FU in the ACCORD trial.105,106
In a secondary analysis, confined to SPRINT participants who were ≥80 years at baseline (N = 1167; mean age = 83.5 years), those randomized to intensive and standard treatment achieved a mean SBP of 123.9 mm Hg and 135.3 mm Hg, respectively, resulting a somewhat smaller mean difference between the two groups (11.5 mm Hg)107 than the average difference (14.8 mm Hg) noted in the overall trial cohort (N = 9361).94,103 Despite this and the smaller sample size, randomization to intensive treatment lowered the risk of major CVD events (HR, 95% CI = 0.67, 0.50 – 0.90), all-cause mortality (HR 0.67, 95% CI 0.48 – 0.93), and MCI (HR 0.72, 95% CI 0.53 – 0.98) compared with standard treatment.107 The CVD and mortality benefits resulting from intensive therapy were similar to those reported in an earlier subgroup analysis confined to participants ≥75 years (N = 2636).108 In the SPRINT participants ≥80 years, there was no evidence that gait speed modified the treatment effect on major CVD events or all-cause mortality, but the participants with higher baseline Montreal Cognitive Assessment (MoCA) scores experienced significantly better CVD and all-cause mortality outcomes compared to their counterparts with lower MoCA scores (0.01 and 0.003, respectively).107
In a meta-analysis that included 14 RCTs (N = 96158; mean age = 69 years), BP lowering (12 trials; N = 92,135; mean FU = 4.1 years) resulted in a small but significant reduction in the risk of dementia or cognitive impairment [odds ratio (OR), 95% CI: 0.93, 0.88 – 0.98).109 There was no convincing evidence for the superiority of any class of antihypertensive medication in the prevention of dementia or cognitive decline in a meta-analysis of 21 cohort studies (N = 43,049) and eight clinical trials (N = 13,817), two of which were treated as cohort studies in the analysis, where the mean age of most participants was between 70 and 79 years.110
Several ongoing SPRINT-like RCTs are being conducted in Brazil and China in patients with hypertension and diabetes and with hypertension and stroke.111 These trials are utilizing study designs that allow for continued treatment and trial assessment of dementia should a convincing difference in CVD events occur prior to the planned end of the trial. Collectively, they will contribute to our understanding of the optimal SBP treatment target for prevention of CVD, all-cause mortality, MCI, and dementia, overall and in subgroups, including in older adults.
Diabetes Mellitus (DM)
High BP and type 2 DM frequently coexist, with hypertension being reported in approximately 80% of patients with DM. In cohort studies, the combination of hypertension and DM has been repeatedly shown to dramatically increase the risk of CVD compared to either risk factor on its own.112 Lifestyle modification is central to prevention and management of both DM and hypertension, with an emphasis on weight loss and physical activity for prevention and control of DM.113,114 Addition of antihypertensive drug therapy is recommended because most patients with the combination of hypertension and DM are at high risk for ASCVD.12 In addition, most surveys suggest that clinicians do not formally estimate CVD/ASCVD risk even when recommended by guidelines.115 The benefits of antihypertensive drug therapy for management of hypertension in patients with DM have been extensively demonstrated in individual RCTs and meta-analyses of clinical trials.3,116 All recommended classes of antihypertensive drug therapy, including diuretics, are similarly effective for prevention of CVD, except in those with heavy proteinuria and/or advanced kidney disease where renin-angiotensin system inhibitors are indicated.12 Typically, a combination of two or three agents is required to achieve BP targets.
There is substantial guideline concordance for an SBP goal of <130 mm Hg in most adults with hypertension and DM.12,19,117 For example, in 95.7% of adults on antihypertensive medication who remain above their recommended BP goal both the ACC/AHA BP Guideline and American Diabetes Association (ADA) Position Statement recommend intensification of therapy.118 The Action to Control Cardiovascular Risk in Diabetes BP Trial (ACCORD BP) was based on a factorial design, in which the planned analysis assumed no interaction between the different treatments being studied (BP lowering and glycemic control).119 The ACCORD BP results indicate this assumption was not realized, with the consequence that the planned analysis yielded results that are unreliable.119 In a secondary post hoc analysis, the participants randomized to intensive BP lowering (SBP target <120 mm Hg) and standard glycemic control derived CVD prevention benefits that were comparable those seen with intensive BP lowering in the SPRINT.120 There was no evidence of CVD benefit in the participants randomized to intensive BP lowering and intensive glycemic control. However, after the intensive glycemic intervention was discontinued, due to harm, CVD prevention in those randomized to intensive BP lowering changed to a pattern like that seen in SPRINT.120 In a secondary analysis of 10,948 Action in Diabetes and Vascular Disease (ADVANCE) RCT participants, all of whom had DM at baseline, treatment with a perindopril-indapamide combination significantly reduced mortality and major CVD (macrovascular and microvascular) events compared to placebo, irrespective of baseline SBP or a 10-year ASCVD risk <20% or ≥20%.121 In those with a baseline SBP <140 mm Hg, most of the active therapy benefit resulted from treatment in the group with a baseline SBP 130-139 mm Hg – a finding that supports the 2017 ACC/AHA Guideline recommendation to treat such individuals with a combination of nonpharmacological therapy and antihypertensive medication, especially those with a 10-year ASCVD risk ≥10%.12
Chronic Kidney Disease (CKD)
The inclusion and careful renal disease monitoring of patients with stage 3-4 CKD in the SPRINT has expanded our understanding of the kidney function changes that occur with intensive BP control. Subgroup analysis yielded similar benefits for prevention of CVD and all-cause mortality compared to what was identified in the full cohort, with very low rates of the main renal endpoint in those with CKD at baseline (halving of eGFR or development of ESRD). When lesser degrees of kidney function decline were considered, there was a higher risk of ≥ 30% decline in eGFR and lower albumin excretion rates with intensive therapy compared to standard therapy reported for both patients with and without CKD at baseline. Intensive treatment was associated with higher rates of reported acute kidney injury serious adverse events.122,123 However, additional analyses suggest these changes were hemodynamic and were not associated with urinary biomarkers of kidney damage which were lower in the intensive treatment group.124 Similar findings were reported for a sub-study of ACCORD participants.125 These results which support a benign hemodynamic process rather than permanent injury as the mechanism for a rise in serum creatinine remain preliminary, covering only the first 1-2 years of treatment; thus, additional longer term data will be needed to confirm the findings.
An updated Kidney Disease Improving Global Outcomes (KDIGO) BP guideline has been released.126 The report recommends standardized office BP measurements, preferably using an automated device, and intensive antihypertensive therapy with a target SBP of <120 mm Hg for all patients with CKD not on dialysis, including those with and without DM.
Resistant hypertension
Resetting the general BP goal for antihypertensive therapy to <130/80 mm Hg by the 2017 ACC/AHA guideline de facto changed the definition of treatment RH.12 This change was reconfirmed by the 2018 AHA Scientific Statement on RH77 which formally defined the disorder as BP that remains uncontrolled above goal in spite of the concurrent use of 3 antihypertensive drugs of different classes. These pharmacologic classes commonly include a long-acting CCB, a blocker of the renin-angiotensin system (ie. ACEI or ARB) and a diuretic, and all 3 agents should be administered at maximum or maximally tolerated doses and at the appropriate dosing interval. RH also includes patients whose BP is controlled at or below goal but requiring ≥4 antihypertensive agents of different classes to achieve target.77
A critical change in the definition of RH in the 2018 AHA Scientific Statement was that pseudo-resistance (ie. error in BP measurement, the white coat effect and/or suboptimal adherence to the antihypertensive drug regimen) now must be excluded before a patient can be labeled as having RH.77 Exclusion of pseudo-resistance before making the diagnosis of RH was also recommended by the 2018 European Society of Cardiology (ESC)/European Society of Hypertension (ESH) BP guideline.19 While the new goal for BP control in the office is now <130/80 mm Hg, it is important to remember that office BP should be confirmed using out-of-office measurements and that the 24-h ABPM goal is now <125/75 mm Hg as recently validated.12,15, 77,127
Under the new definition of RH using the 130/80 mm Hg cutoff, its prevalence was expected to escalate dramatically, placing an exponential burden on the healthcare system. However, population modeling studies have estimated that this change would result in only about a 2% increase in the prevalence of RH (from 17.7 to 19.7%) in the United States.128
The importance of RH is its association with higher CVD and kidney disease risk compared to hypertension without resistance, but the prognosis of RH using the current definition had not been studied.77 The first evidence was provided by a large RH cohort study from Korea (2000 participants) with the white coat effect excluded demonstrating that the risk for major adverse cardiovascular events (MACE; myocardial infarction, stroke, heart failure or CV death) and adverse kidney outcomes was similar under the 2018 AHA as compared with earlier definitions of RH with no significant difference for predicting MACE.129
In addition to cardiac, central nervous system and kidney target organ damage, aortic stiffness had been demonstrated both as a pathogenetic factor and a consequence of the hypertensive process, but the prognostic importance of aortic stiffness in RH per se had not previously been evaluated. A large cohort study (891 participants) of patients with RH demonstrated that patients with increased aortic stiffness, as measured by carotid-femoral pulse wave velocity (cfPWV), had a significant 2.2- to 2.6-fold increased risk of CVD events and mortality.130 Increased aortic stiffness predicted adverse cardiovascular outcomes and mortality and improved CVD risk stratification in RH.130 Thus, cfPWV measurement might be considered in the work up and management of RH.
In the management of RH, it has heretofore been unclear which BP measurements optimally predict TOD and prognosis. A large cohort study (1726 participants) of RH has shown that ABPM seems to be more strongly associated with adverse CVD and mortality outcomes than clinic BP and that BP measured during follow up with patients on treatment was more strongly associated with adverse outcomes than baseline BPs.131 Measurement of ambulatory rather than clinic BP, and on-treatment BP as opposed to baseline measurements, improved risk discrimination for prediction of adverse outcomes. Uncontrolled ABPM levels were associated with adverse outcomes, whereas office BP levels after adjustment for ambulatory BP were not. Furthermore, the previous and new lower BP cutoffs for RH were approximately equivalent in their strengths of association with adverse outcomes. These results encourage the use of serial ABPM in the management of patients with RH.131
Both the 2017 ACC/AHA guideline and the 2018 AHA Scientific Statement on RH recommend comprehensive screening for secondary causes of hypertension in all patients with RH12,77. Primary aldosteronism has a particularly high (≈20%) prevalence in RH and is relatively easy to screen with an ARR.77,132 At least 2 studies have confirmed the abysmal rates (1.6 - 2.1%) of screening for primary aldosteronism in RH.43,133 Given the recent discovery of a higher prevalence of autonomous aldosterone production than previously recognized in primary hypertension42, the devastating CVD and renal consequences of primary aldosteronism beyond those for primary hypertension and the availability of specific treatment in the form of adrenalectomy for unilateral and MRAs for bilateral disease132, these studies uncovering poor detection effort provide a clarion call to increase screening for primary aldosteronism in RH, and indeed in all patients with hypertension.
The 2018 AHA Scientific Statement on RH presented a new evidence-based template for the therapeutic sequence, first recommending optimization of the 3 drug regimen (agent, dose and timing), followed by substitution of a thiazide-like diuretic (chlorthalidone or indapamide) for hydrochlorothiazide.77 If BP remains uncontrolled, the Statement recommends addition of a MRA (spironolactone or eplerenone) on the basis of demonstrated superiority over other 4th drug options in PATHWAY-2.44,77,134 Beyond this recommendation, all others are expert opinion only.
The available MRAs each have potential problems in the treatment of RH. Spironolactone displays cross-inhibition of the androgen receptor resulting in reproductive hormone-related adverse effects, and eplerenone is less potent and has a shorter half-life requiring twice daily dosing to control BP. Esaxerenone is a non-steroidal, potent, selective MRA with the potential for fewer side effects. In a double-blind, large-scale RCT in patients with primary hypertension and normal GFR, esaxerenone was noninferior to eplerenone in lowering BP for 12 weeks.135 Non-steroidal MRAs such as esaxerenone and finerenone have great potential in lowering BP in RH without inducing hyperkalemia, a potential adverse effect of steroidal MRAs, especially in adults with reduced GFR. Meanwhile, the AMBER trial has demonstrated that K+-binding agent patiromer can enable the use of spironolactone with less hyperkalemia in patients with RH and CKD.136 As demonstrated by a secondary analysis of SPRINT, irrespective of the pharmacologic agents employed, intensive BP lowering is superior to standard treatment in terms of CVD outcomes in RH.137
Optimization of Care Using Patient, Provider and Health System Approaches
Hypertension is a chronic disease process requiring accurate detection and lifelong management to maximize clinical outcomes. Optimization of hypertension care demands, first and foremost, affordable and sustainable access to care. This includes patient identification; patient and clinician agreement on the appropriate BP goal; shared decision-making that facilitates the patient’s benefit, goals and values; BP monitoring at both patient and practice levels; implementation of team-based care with defined team member roles; appropriate lifestyle recommendations and counseling; systematic follow up; minimization of clinician inertia in the initiation and intensification of treatment; promotion of a high level of adherence to the therapeutic regimen, and the use of electronic medical records, mobile health technologies, BP self-monitoring and telemonitoring, and other novel technologies.5 Overall, governmental, health system, payor and community resources must be united and deployed to provide patient self-management support, health care delivery design, decision support and clinical information systems that, when integrated, result in informed, activated patients and prepared, anticipatory practice teams working together to improve care and outcomes.5,138,139
Clinician therapeutic inertia, defined as suboptimal prescription of antihypertensive therapy, has been identified as a major barrier preventing patients with hypertension from achieving their guideline-recommended BP goals. The US National Ambulatory Medical Care Survey indicates that in 41.7 million primary care visits (2005-2012) in patients with SBP ≥140 mm Hg or DBP ≥ 90 mm Hg, new antihypertensive medication was only initiated in 7 million (16.8%).140,141 Reasons for failing to initiate or intensify antihypertensive therapy include lack of time, workflow constraints, concern about side effects, lack of knowledge to make pharmacologic agent and/or dosing decisions and uncertainty about the patient’s out-of-office BP. Overcoming clinician inertia can be accomplished through an integrated health system model of care. For example, BP control rates exceed the national average in the Kaiser Permanente and Veterans Affairs health systems, where the approach to BP control is systematic. Identifying patients with hypertension, standardizing BP measurements, and using a stepwise treatment algorithm have led to an increase in BP control rates from 54% in 2004 to 84% in 2010 in the Kaiser Permanente Southern California health system.142
Another major cause of uncontrolled BP is suboptimal adherence to the antihypertensive regimen, including failure to (1) initiate pharmacotherapy, (2) take medications as frequently as prescribed, and (3) persevere on therapy long-term.143 Barriers to the achievement of a high level of adherence include limited access to care, cost, social determinants of health, complex medication regimens, inconvenient medication dosing and frequency, behavioral factors and adverse effects of medications in asymptomatic patients. While still a work in progress, detection of poor adherence ranges from simple, low cost screening tests in patients with uncontrolled BP to electronic and biochemical monitoring in those with RH. Consistently effective intervention strategies include increased patient-clinician communication, use of electronic communication methods, patient education and lifestyle and behavioral counseling.143
One of the most important strategies to improve outcomes in the care of hypertension is team-based care, a multidisciplinary team surrounding the patient, to optimize the quality of care. The team includes the patient at the center, the primary clinician and other health professionals (eg. nurses, pharmacists, physician assistants, dieticians, lifestyle counselors, social and community health care workers) each with specifically designated responsibilities in care. These health care professionals complement the primary clinician by providing process support and sharing the responsibilities of care.
Several clinical trials on the effectiveness of team-based care are available, but their individual participant size has generally been too small to provide the statistical power necessary to demonstrate effectiveness in lowering BP. Comparative effectiveness of various implementation strategies in BP reduction in patients with hypertension was recently assessed in a systematic review and meta-analysis of over 100 trials in 55,920 patients.144 Team-based care with medication titration by a non-physician resulted in lowering of SBP by 7.1 mm Hg (95% CI 8.9-5.2) and by a physician by 6.2 mm Hg (95% CI 8.1-4.2). Multilevel strategies without team-based care also significantly lowered SBP (by 5 mm Hg). At the patient level, health coaching reduced office SBP by 3.9 mm Hg and HBPM by 3.7 mm Hg. Multilevel, multicomponent implementation strategies with and without team-based care are the most effective methods of BP control among hypertensive patients.144 Thus, implementation strategies targeting multilevel or patient level barriers to care are appropriate methods to control BP in hypertensive patients. With the evidence currently available, these methods should now be scaled up for clinical practice and public health programs to improve BP control in communities.
Pharmacists have been widely employed in team-based care for hypertension.145 A recent meta-analysis of 6 randomized trials involving 2,573 participants demonstrated that pharmacist interventions resulted in better BP control than usual care [OR 1.53 (CI 1.15-2.04), P<0.01].146 Pharmacist interventions using home-based BP telemonitoring were superior to usual care, whereas pharmacist intervention without BP telemonitoring did not improve BP control. In addition, a pharmacist-led intervention in a community setting for non-Hispanic Black male patrons of barbershops with uncontrolled BP resulted in a mean SBP reduction of 21.6 mm Hg greater than usual care at 6 months.147 An advantage of pharmacist-provided hypertension care is that the effects often persist beyond the initial intervention period.
Advances in health information technology, including electronic health records and high-speed communications, provide ideal opportunities for improving BP control in patients with hypertension. Telemedicine is a revolutionary patient management tool facilitating interactive communication between the patient and the health care team from remote sites.148 Telemedicine combines various forms of information technology to deliver care, consultation, medical education, and specific health and clinical services, including monitoring. Telemonitoring, a specific application of telemedicine, refers to remote monitoring of various vital and nonvital parameters, including BP, that are automatically communicated directly to the health care team.
Until recently, evidence for the use of BP self-monitoring and telemonitoring to titrate antihypertensive medication by physicians was equivocal. However, telemonitoring and/or self-monitoring of BP in the TASMINH4 trial provided new evidence that physician drug titration using patient self-monitoring led to lower BP and that including telemonitoring led to lower BP more rapidly than self-monitoring alone.149 These approaches were also cost-effective.150
Several meta-analyses based on numerous RCTs reported to date provide moderate to high level evidence that home BP telemonitoring enhances hypertension management and improves BP control in hypertensive patients.148 The most successful BP telemonitoring approach seems to be BP data exchange with a case manager (eg. nurse or pharmacist) combined with education on lifestyle, risk factors and appropriate dosing of antihypertensive medications. Proactive intervention driven by the health care professional, rather than passive intervention, seems to provide the best and most long-lasting effects. A recent position paper on the use of telemedicine in the management of hypertension concludes that current evidence supports the use of telemedicine and BP telemonitoring, particularly in patients with difficult to control hypertension or those with poor adherence to their antihypertensive regimen.148
Conclusions
Hypertension is the world’s leading risk factor for CVD and mortality. Since publication of the 2017 ACC/AHA BP Guideline, several new findings have emerged which, taken together, can better inform the approach to the prevention, detection and management of hypertension. The major findings (January, 2018-March, 2021) and their relevance to the management of hypertension are summarized in Table 7. This new information has the potential to increase hypertension awareness, treatment and control which are bedrock for the prevention of CVD morbidity and mortality in the future.
Table 7.
Summary of Major Findings (January, 2018-March, 2021) and Relevance to the Management of Hypertension
| • BP control rates increased steadily until 2013-14 after which they have declined. Adherence to 2017 ACC/AHA BP Guideline recommendations has the potential to reverse this alarming trend. |
| • Out-of-office BP readings (ABPM or HBPM) continue to be recommended to detect WCH and MH, with ABPM more sensitive to detect MH. |
| • HBPM is the most practical method to document BP for medication titration towards the achievement and maintenance of BP goal. |
| • Autonomous aldosterone production may play a role in the pathogenesis of Stages 1 and 2 hypertension and resistant hypertension. All adults with difficult to control or resistant hypertension should be screened for primary aldosteronism. If aldosterone to renin ratio is low but plasma renin is low, consider 24 hour urine aldosterone measurement during salt loading (high sodium diet) conditions. |
| • Young adults with hypertension have earlier onset of CVD events compared with those with normal BP. Thus, it may be inappropriate to delay treatment, even though RCT evidence is lacking. The evidence supports initial management in young adults with evidence of TOD with lifestyle modification for 6-12 months followed by antihypertensive drug therapy if BP remains above goal. |
| • Lifestyle modification continues to be the cornerstone of antihypertensive therapy. Each nonpharmacological intervention is effective in lowering BP, and concurrent use of 2 or more interventions results in additive effects. Lifestyle modification improves the effectiveness of pharmacologic therapy. |
| • Intensive BP control is not associated with increased hospitalization and does not increase the risk of orthostatic hypotension. Asymptomatic orthostatic hypotension in hypertensive adults is not associated with higher rates of CVD events, syncope, injurious falls or acute renal failure and should not be a reason to withdraw or down-titrate treatment. |
| • For older adults with hypertension, intensive BP lowering may prevent or at least partially arrest cognitive decline. |
| • The definition of resistant hypertension is BP ≥130/80 mm Hg in adults on ≥3 antihypertensive medications of different classes, prescribed at maximum or maximally tolerated doses, or BP <130/80 mm Hg but requiring ≥4 antihypertensive drugs after exclusion of pseudo-resistance (inaccurate BP measurement, the white coat effect and/or suboptimal drug adherence). |
| • Multilevel, multicomponent implementation strategies, including team-based care, are the most effective methods of BP control in hypertensive patients. |
| • Home BP self-monitoring and telemonitoring are effective in facilitating antihypertensive drug titration leading to achievement and maintenance of BP goal. |
ABPM, ambulatory blood pressure monitoring; ACC, American College of Cardiology; AHA, American Heart Association; BP, blood pressure; HBPM, home blood pressure monitoring; MH, masked hypertension; TOD, target organ damage; WCH, white coat hypertension.
Supplementary Material
Acknowledgments
Sources of Funding
Dr. Carey is Principal Investigator and Project Director of an NIH Research Grant (R01-HL-128189) and Program Project Grant (P01-HL-074940), respectively. Dr. Wright is supported by a grants from the Ohio Department of Medicaid and Agency for Health Care Research & Quality (1U18HS027944-01). Dr. Taler is a staff physician at Mayo Clinic, Rochester, MN with no outside funding to disclose. Dr. Whelton was supported by a National Institute of General Medical Sciences, Centers of Biomedical Research Excellence award NIGMS P30-GM-109036.
Non-standard Abbreviations and Acronyms
- AAFP
American Academy of Family Physicians
- ABPM
Ambulatory blood pressure monitoring
- ACC
American College of Cardiology
- ACCORD
Action to Control Cardiovascular Risk in Diabetes
- ACCORD-BP
Action to Control Cardiovascular Risk in Diabetes Blood Pressure
- ACEI
angiotensin converting enzyme inhibitor
- ACP
American College of Physicians
- ADA
American Diabetes Association
- ADVANCE
Action in Diabetes and Vascular Disease
- AHA
American Heart Association
- ARR
aldosterone/renin ratio
- ARB
angiotensin receptor blocker
- ASCVD
atherosclerotic cardiovascular disease
- AOBP
automated office blood pressure
- BP
blood pressure
- CARDIA
Coronary Artery Risk Development in Young Adults
- CCB
calcium channel blocker
- cfPWV
carotid-femoral pulse wave velocity
- CHD
coronary heart disease
- CI
confidence interval
- CVD
cardiovascular disease
- DASH
Dietary Approaches to Stop Hypertension
- DBP
diastolic blood pressure
- DM
diabetes mellitus
- eGFR
estimated glomerular filtration rate
- ESRD
end-stage renal disease
- FMD
fibromuscular dysplasia
- FU
follow up
- HBPM
home blood pressure monitoring
- HF
heart failure
- HR
hazard ratio
- JNC
Joint National Committee
- KDIGO
Kidney Disease Improving Global Outcomes
- MACE
major adverse cardiovascular events
- MH
masked hypertension
- MoCA
Montreal Cognitive Assessment
- MRA
mineralocorticoid receptor antagonist
- MRI
magnetic resonance imaging
- NHANES
National Health and Nutrition Examination Survey
- NICE
National Institute for Health and Care Excellence
- OR
odds ratio
- RCT
randomized controlled trial
- RH
resistant hypertension
- SBP
systolic blood pressure
- TOD
target organ damage
- WCH
white coat hypertension
Footnotes
Disclosures
Dr. Carey was Vice-Chair of the 2017
ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults Writing Committee, Chair of the AHA Scientific Statement on Resistant Hypertension Writing Committee and a Member of the 2019 AHA Scientific Statement on Measurement of Blood Pressure in Humans Writing Committee. . Dr. Wright was a member of the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults Writing Committee and the 2019 AHA Scientific Statement on Measurement of Blood Pressure in Humans. Dr. Taler was a member of the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults Writing Committee and a Member of the 2018 AHA Scientific Statement on Resistant Hypertension Writing Committee. Dr. Whelton was Chair of the SPRINT Steering Committee and Chair of the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults.
References
- 1.Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular disease and risk factors; 1990-2019: Update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76:2982–3021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pencina MJ, Navar AM, Wojdyla D, Sanchez RJ, Khan I, Elassal J, D’Agostino RB Sr, Peterson ED, Sniderman AD. Quantifying importance of major risk factors for coronary heart disease. Circulation. 2019;139:1603–1611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, Chalmers J, Rodgers A, Rahimi K. Blood pressure lowering for the prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–967. [DOI] [PubMed] [Google Scholar]
- 4.Bundy JD, Li C, Stuchlik P, Bu X, Kelly TN, Mills KT, He H, Chen J, Whelton PK, He J. Systolic blood pressure reduction and risk of cardiovascular disease and mortality: a systematic review and network meta-analysis. JAMA Cardiol. 2017;2:775–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Carey RM, Muntner P, Bosworth HB, Whelton PK. Prevention and control of hypertension. JACC Health Promotion Series. J Am Coll Cardiol. 2018;72:1278–1293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Foti K, Wang D, Appel LJ, Selvia E. Hypertension awareness, treatment and control in US adults: trends in the hypertension control cascade by population subgroup (National Health and Nutrition Examination Survey, 1999-2016). Am J Epidemiol. 2019;188:2165–2174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Muntner P, Hardy ST, Fine LJ, Jaeger BC, Wozniak G, Levitan EB, Colantonio LD. Trends in blood pressure control among US adults with hypertension, 1999-2000 to 2017-2018. JAMA. 2020;324:1190–1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.James PA, Oparil S, Carter BL et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC-8). JAMA. 2014;31:507–520. [DOI] [PubMed] [Google Scholar]
- 9.Chobanian AV, Bakris GL, Black HR, et al. ; Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Hypertension. 2003; 42:1206–52. [DOI] [PubMed] [Google Scholar]
- 10.Wright JT Jr, Fine LJ, Lackland DT, Ogedegbe G, Dennison-Himmelfarb C. Evidence supporting a systolic blood pressure goal of less than 150 mm Hg in patients age 60 years or older: the minority view. Ann Int Med. 2014;160:499–503. [DOI] [PubMed] [Google Scholar]
- 11.Qaseem A, Wilt TJ, Rich R, et al. Pharmacologic treatment of hypertension in adults aged 60 years or older to higher versus lower blood pressure targets: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2017;166:430–437. [DOI] [PubMed] [Google Scholar]
- 12.Whelton PK, Carey RM, Aronow WS, et al. A guideline for the prevention, detection, evaluation and management of high blood pressure. A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e13–e115. [DOI] [PubMed] [Google Scholar]
- 13.Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, Chen J, He J. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lackland DT, Howard VJ, Cushman M, Oparil S, Kissela B, Safford MM, Kleindorfer DO, McClure LA, Howard G. Forty-year shifting distribution of systolic blood pressure with population hypertension treatment and control. Circulation. 2020;142:1524–1531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Muntner P, Shimbo D, Carey RM, et al. Measurement of blood pressure in humans: a Scientific Statement of the American Heart Association. Hypertension. 2019;73:e35–e66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Drawz PE, Agarwal A, Dwyer JP, et al. Concordance between blood pressure in the Systolic Blood Pressure Intervention Trial and in routine clinical practice. JAMA Intern Med. 2020;180:1655–1663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mancia G, De Backer G, Dominiczak AF, et al. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens, 2007;25:1105–1187. [DOI] [PubMed] [Google Scholar]
- 18.Excellence NIfHaC. Hypertension:the clinical management of primary hypertension in adults: clinical guidelines: methods, evidence and recommendations. National Institute for Health and Clinical Excellence. 2011. http://publications.nice.org.uk/hypertension-cg127. Published 2011.
- 19.Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. [DOI] [PubMed] [Google Scholar]
- 20.Nerenberg KA, Zarnke KB, Leung AA, et al. Hypertension Canada’s 2018 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children. Can J Cardiol. 2018;34:506–525. [DOI] [PubMed] [Google Scholar]
- 21.Myers MG. A short history of automated office blood pressure - 15 years to SPRINT. J Clin Hypertens (Greenwich). 2016;18:721–724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Johnson KC, Whelton PK, Cushman WC, et al. Blood Pressure Measurement in SPRINT (Systolic Blood Pressure Intervention Trial). Hypertension. 2018;71:848–857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bauer F, Seibert FS, Rohn B, Bauer KAR, Rolshoven E, Babel N, Westhoff TH. Attended versus unattended blood pressure measurement in a real life setting. Hypertension. 2018;71:243–249. [DOI] [PubMed] [Google Scholar]
- 24.Kollias A, Stambolliu E, Kyriakoulis KG, Gravvani A, Stergiou GS. Unattended versus attended automated office blood pressure: Systematic review and meta-analysis of studies using the same methodology for both methods. J Clin Hypertens (Greenwich). 2019;21:148–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yarows SA. How to measure blood pressure in primary care offices to assure accuracy while maintaining efficiency. J Clin Hypertens (Greenwich). 2017;19:1386–1387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cohen JB, Padwal RS, Gutkin M, et al. History and justification of a National Blood Pressure Measurement Validated Device Listing. Hypertension. 2019;73:258–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stergiou GS, Alpert BS, Mieke S, Wang J, O’Brien E. Validation protocols for blood pressure measuring devices in the 21st century. J Clin Hypertens (Greenwich). 2018;20:1096–1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.STRIDE BP. https://www.stridebp.org/. Accessed 7 February 2021.
- 29.US blood pressure validated device listing. https://www.validatebp.org/. Accessed 7 February 2021.
- 30.Anstey DE, Muntner P, Bello NA, Pugliese DN, Yano Y, Kronish IM, Reynolds K, Schwartz JE, Shimbo D. Diagnosing masked hypertension using ambulatory blood pressure monitoring, home blood pressure monitoring, or both? Hypertension. 2018;72:1200–1207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Schwartz JE, Muntner P, Kronish IM, Burg MM, Pickering TG, Bigger JT, Shimbo D. Reliability of office, home, and ambulatory blood pressure measurements and correlation with left ventricular mass. J Am Coll Cardiol. 2020;76:2911–2922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.PAHO/RESOLVE/WHL certification course. https://www.campusvirtualsp.org/en/node/29166.
- 33.AHA/AMA Target BP training course (https://targetbp.org/tools_downloads/cme-course-measuring-blood-pressure-accurately-step-1-in-hypertension-control/)
- 34.Bello NA, Schwartz JE, Kronish IM, Oparil S, Anstey DE, Wei Y, Cheung YKK, Muntner P, Shimbo D. Number of measurements needed to obtain a reliable estimate of home blood pressure: results from the Improving the Detection of Hypertension Study. J Am Heart Assoc. 2018;7:e008658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kario K Management of hypertension in the digital era: small wearable monitoring devices for remote blood pressure monitoring. Hypertension. 2020;76:640–650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Roman MJ, Devereux RB, Kizer JR, Lee ET, Galloway JM, Ali T, Umans JG, Howard BV. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the Strong Heart Study. Hypertension. 2007;50:197–203. [DOI] [PubMed] [Google Scholar]
- 37.Lamarche F, Agharazii M, Madore F, Goupil R. Prediction of cardiovascular events by type I central systolic blood pressure: A prospective study. Hypertension. 2020:HYPERTENSIONAHA12016163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cooper CJ, Murphy TP, Cutlip DE, et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. 2014;370:13–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Piaggio D, Bracale U, Pecchia L, Di Taranto MD, Sodo M, Bracale UM. Endovascular treatment versus medical therapy for hypertensive patients with renal artery stenosis: an updated systematic review. Ann Vasc Surg. 2019;61:445–54. [DOI] [PubMed] [Google Scholar]
- 40.Courand PY, Dinic M, Lorthioir A, et al. Resistant hypertension and atherosclerotic renal artery stenosis: effects of angioplasty on ambulatory blood pressure. a retrospective uncontrolled single-center study. Hypertension. 2019;74:1516–23. [DOI] [PubMed] [Google Scholar]
- 41.Gornik HL, Persu A, Adlam D, et al. First International Consensus on the diagnosis and management of fibromuscular dysplasia. Vasc Med. 2019;24: 164–189. [DOI] [PubMed] [Google Scholar]
- 42.Brown JM, Siddiqui M, Calhoun DA, Carey RM, Hopkins PN, Williams GH, Vaidya A. The unrecognized prevalence of primary aldosteronism: a cross-sectional study. Ann Intern Med. 2020;173:10–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cohen JB, Cohen DL, Herman DS, Leppert JT, Byrd JB, Bhalla V. Testing for primary aldosteronism and mineralocorticoid receptor antagonist use among U.S. Veterans : A retrospective cohort study. Ann Intern Med. 2020.doi: 10.7326/M20-4873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Williams B, MacDonald TM, Morant S, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386:2059–2068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Tajeu GS, Booth JN III, Colantonio LD, et al. Incident cardiovascular disease among adults with blood pressure <140/90 mm Hg, Circulation. 2017;136:798–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Yano Y, Reis JP, Colangelo LA, et al. Association of blood pressure classification in young adults using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline with cardiovascular events later in life. JAMA. 2018;320:1774–1782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Drukteinis JS, Roman MJ, Fabsitz RR, Lee ET, Best LG, Russell M, Devereux RB. Cardiac and systemic hemodynamic characteristics of hypertension and prehypertension in adolescents and young adults: the Strong Heart Study. Circulation. 2007;115:221–227. [DOI] [PubMed] [Google Scholar]
- 48.Williamson W, Lewandowski AJ, Forkert ND, et al. Association of cardiovascular risk factors with MRI indices of cerebrovascular structure and function and white matter hyperintensities in young adults. JAMA. 2018;320:665–673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lee H, Yano Y, Cho SMJ, Park JH, Park S, Lloyd-Jones DM, Kim HC. Cardiovascular risk of isolated systolic or diastolic hypertension. Circulation. 2020;141:1778–1786. [DOI] [PubMed] [Google Scholar]
- 50.Whelton PK, He J, Appel LJ, et al. Primary prevention of hypertension: clinical and public health advisory from The National High Blood Pressure Education Program. JAMA. 2002;288:1882–1888. [DOI] [PubMed] [Google Scholar]
- 51.Saif-Ur-Rahman KM, Shariful Islam S, Hasan M, Hossain S, Mamun R, Shafique S, Mamun A, Khalequzzaman M, Haseen F, Rahman A, Anwar I. Nonpharmacological interventions for the prevention of hypertension in low- and middle-income countries: a systematic review and meta-analysis. J Hum Hypertens. 2019;33:786–794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Fu J, Liu Y, Zhang L, et al. Nonpharmacologic interventions for reducing blood pressure in adults with prehypertension to established hypertension. J Am Heart Assoc. 2020;9:e016804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Puhan MA, Schunemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, Kessels AG, Guyatt GH, Group GW. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. [DOI] [PubMed] [Google Scholar]
- 54.Appel LJ, Champagne CM, Harsha DW, et al. Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA. 2003;289:2083–2093. [DOI] [PubMed] [Google Scholar]
- 55.Whelton PK, Appel LJ, Espeland MA, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE). TONE Collaborative Research Group. JAMA. 1998;279:839–846. [DOI] [PubMed] [Google Scholar]
- 56.Whelton PK, He J. Health effects of sodium and potassium in humans. Curr Opin Lipidol. 2014;25:75–79. [DOI] [PubMed] [Google Scholar]
- 57.Ide N, Ajenikoko A, Steele L, Cohn J, C JC, Frieden TR and Cobb LK. Priority Actions to Advance Population Sodium Reduction. Nutrients. 2020;12:2543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Campbell NRC, Ordunez P, Giraldo G, Rodriguez Morales YA, Lombardi C, and Khan T PR, Tsuyuki RT, Varghese C. WHO HEARTS, a global program to reduce cardiovasculardisease burden: Experience implementing in the America’s and opportunities in Canada. Can J Cardiol. 2020.doi: 10.1016/j.cjca.2020.12.004. [DOI] [PubMed] [Google Scholar]
- 59.Campbell NRC, Schutte AE, Varghese CV, et al. Sao Paulo call to action for the prevention and control of high blood pressure: 2020. J Clin Hypertens (Greenwich). 2019;21:1744–1752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Campbell NRC, Webster J, Blanco-Metzler A, et al. Packages of sodium (salt) sold for consumption and salt dispensers should be required to have a front of package health warning label: a position statement of the World Hypertension League, national and international health and scientific organizations. J Clin Hypertens (Greenwich). 2019;21:1623–1625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Crippa A, Discacciati A, Bottai M, Spiegelman D, Orsini N. One-stage dose-response meta-analysis for aggregated data. Stat Methods Med Res. 2019;28:1579–1596. [DOI] [PubMed] [Google Scholar]
- 62.Filippini T MM, Whelton PK, Naska A, Orsini N, Vinceti M. Dose-response modeling of blood pressure effects of sodium reduction: a meta-analysis of randomized controlled trials. Circulation. 2021;(ePub ahead of print). doi: 10.1161/CIRCULATIONAHA.120.050371.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Whelton PK, Appel LJ, Sacco RL, et al. Sodium, blood pressure, and cardiovascular disease: further evidence supporting the American Heart Association sodium reduction recommendations. Circulation. 2012;126:2880–2889. [DOI] [PubMed] [Google Scholar]
- 64.National Academies of Sciences, Engineering, and Medicine: Food and Nutrition Board; Committee to Review the dD Reference Intakes for Sodium and Potassium. Oria M, Harrison M, Stallings VA, eds. Dietary reference intakes for sodium and potassium. Washington (DC); National Academies Press (US). 2019. March 5. [PubMed] [Google Scholar]
- 65.Organization WH. WHO Guideline: Sodium intake for adults and children 2012. Geneva: World Health Organization. 2012. [PubMed] [Google Scholar]
- 66.Filippini T, Naska A, Kasdagli MI, et al. Potassium intake and blood pressure: A dose-response meta-analysis of randomized controlled trials. J Am Heart Assoc. 2020;9:e015719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.He FJ, Campbell NRC, Ma Y, MacGregor GA, Cogswell ME, Cook NR. Errors in estimating usual sodium intake by the Kawasaki formula alter its relationship with mortality: implications for public health. Int J Epidemiol. 2018;47:1784–1795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Naser AM, Rahman M, Unicomb L, Doza S, Anand S, Chang HH, Luby SP, Clasen TF, Narayan KMV. Comparison of Urinary Sodium and Blood Pressure Relationship From the Spot Versus 24-Hour Urine Samples. J Am Heart Assoc. 2019;8:e013287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Charlton K, Ware LJ, Chidumwa G, Cockeran M, Schutte AE, Naidoo N, Kowal P. Prediction of 24-hour sodium excretion from spot urine samples in South African adults: a comparison of four equations. J Hum Hypertens. 2020;34:24–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Xu J, Zhang J, Liu M, Bai Y, Guo X, Dong J, Xu A, Wu J. Estimating 24-hour sodium excretion from spot urine samples in Chinese adults: can spot urine substitute 24-hour urine samples? Nutrients. 2020;12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Campbell NRC, He FJ, Tan M, et al. The International Consortium for Quality Research on Dietary Sodium/Salt (TRUE) position statement on the use of 24-hour, spot, and short duration (<24 hours) timed urine collections to assess dietary sodium intake. J Clin Hypertens (Greenwich). 2019;21:700–709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Mente A, O’Donnell M, Rangarajan S, et al. Urinary sodium excretion, blood pressure, cardiovascular disease, and mortality: a community-level prospective epidemiological cohort study. Lancet. 2018;392:496–506. [DOI] [PubMed] [Google Scholar]
- 73.Welsh CE, Welsh P, Jhund P, et al. Urinary sodium excretion, blood pressure, and risk of future cardiovascular disease and mortality in subjects without prior cardiovascular disease. Hypertension. 2019;73:1202–1209. [DOI] [PubMed] [Google Scholar]
- 74.O’Donnell M, Mente A, Alderman MH, et al. Salt and cardiovascular disease: insufficient evidence to recommend low sodium intake. Eur Heart J. 2020;41:3363–3373. [DOI] [PubMed] [Google Scholar]
- 75.Excellence NIfHaC. Hypertension in adults: diagnosis and management. 2019. https://www.nice.org.uk/guidance/ng136. Published August 28, 2019.
- 76.Thomopoulos C, Bazoukis G, Tsioufis C, Mancia G. Beta-blockers in hypertension: overview and meta-analysis of randomized outcome trials. J Hypertens. 2020;38:1669–1681. [DOI] [PubMed] [Google Scholar]
- 77.Carey RM, Calhoun DA, Bakris GL, et al. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association. Hypertension. 2018;72:e53–e90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Hripcsak G, Suchard MA, Shea S, et al. Comparison of cardiovascular and safety outcomes of chlorthalidone vs hydrochlorothiazide to treat hypertension. JAMA Intern Med. 2020;180:542–551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Lederle FA, Cushman WC, Ferguson RE, Brophy MT, Fiore Md LD. Chlorthalidone versus hydrochlorothiazide: a new kind of Veterans Affairs Cooperative Study. Ann Intern Med. 2016;165:663–664. [DOI] [PubMed] [Google Scholar]
- 80.Goud A, Zhong J, Peters M, Brook RD, Rajagopalan S. GLP-1 agonists and blood pressure: a review of the evidence. Curr Hypertens Rep. 2016;18:16. [DOI] [PubMed] [Google Scholar]
- 81.Georgianos PI, Agarwal R. Ambulatory blood pressure reduction with SGLT-2 inhibitors: dose-response meta-analysis and comparative evaluation with low-dose hydrochlorothiazide. Diabetes Care. 2019;42:693–700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Langford AT, Akinyelure OP, Moore TL Jr., et al. Underutilization of treatment for Black adults with apparent treatment-resistant hypertension: JHS and the REGARDS Study. Hypertension. 2020;76:1600–1607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Egan BM, Sutherland SE, Rakotz M, Yang J, Hanlin RB, Davis RA, Wozniak G. Improving hypertension control in primary care with the Measure Accurately, Act Rapidly, and Partner With Patients Protocol. Hypertension. 2018;72:1320–1327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Still CH, Rodriguez CJ, Wright JT, et al. Clinical outcomes by race and ethnicity in the Systolic Blood Pressure Intervention Trial (SPRINT): A randomized clinical trial. Am J Hypertens. 2018;31:97–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Taitel M, Fensterheim L, Kirkham H, Sekula R, Duncan I. Medication days’ supply, adherence, wastage, and cost among chronic patients in Medicaid. Medicare Medicaid Res Rev. 2012;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Reboussin DM, Carey RM, Whelton PK. Evidence supporting the blood pressure treatment goal of less than 130/80 mmHg. Hypertension. 2019;73:972–974. doi: 10.1161/HYPERTENSIONAHA.119.12804. [DOI] [PubMed] [Google Scholar]
- 87.Gidding SS, Whelton PK, Carey RM, Levine GN. Writing a trustworthy hypertension guideline.. J Am Coll Cardiol.. 2019.74:2424–2427. [DOI] [PubMed] [Google Scholar]
- 88.Carey RM, Whelton PK. The evidence for the universal BP goal of < 130/80 mm Hg Is strong: Controversies in Hypertension – Pro. Hypertension. 2020;76:1384–1390. doi:1161/HYPERTENSIONAHA.12014647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Sakima A, Satonaka H, Nishida N, Yatsu K, Arima H. Optimal blood pressure target for patients with hypertension: a systematic review and meta-analysis. Hypertension Research. 2019;42:483–495. [DOI] [PubMed] [Google Scholar]
- 90.Kitagawa K, Yamamoto Y, Arima H. Effect of standard versus intensive blood pressure control on risk of recurrent stroke: a randomized clinical trial and meta-analysis. JAMA Neurol. 2019;76:1309–1318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Rocco MV, Comeau ME, Marion MC, Freedman BI, Hawfield AT, Langefeld CD, for the SPRINT Research Group. Effects of intensive systolic blood pressure control on all-cause hospitalizations. Hypertension. 2020;76:1717–1724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Juraschek SP, Taylor AA, Wright JT Jr, et al. Sprint Research Group. Orthostatic hypotension, cardiovascular outcomes, and adverse events: results from SPRINT. Hypertension. 2020;75:660–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Juraschek SP, Hu J-R, Cluett JL, et al. Effects of intensive blood pressure treatment on orthostatic hypotension. Ann Int Med. 2020;174:58–68. doi: 10.7326/M20-4298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2003–2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the AHA strategic impact goal through 2020 and beyond. Circulation. 2010;121:586–613. [DOI] [PubMed] [Google Scholar]
- 96.Angell SY, McConnell MV, Anderson CAM, et al. The AHA 2030 Impact Goal: a presidential advisory from the AHA. Circulation. 2020;e120–e138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.My Life Check/Life’s Simple.
- 98.Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada’s 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children. Can J Cardiol. 2020;36:596–624. [DOI] [PubMed] [Google Scholar]
- 99.Gabb GM, Mangoni AA, Anderson CS, et al. Guideline for the diagnosis and management of hypertension in adults. 2016. Med J Aust. 2016:205:85–89. [DOI] [PubMed] [Google Scholar]
- 100.Bundy JD, Mills KT, Chen J, Li C, Greenland P, He J. Estimating the Association of the 2017 and 2014 Hypertension Guidelines With Cardiovascular Events and Deaths in US Adults: An Analysis of National Data. JAMA Cardiol. 2018;3:572–581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Bress AP, Colantonio LD, Cooper RS, et al. Potential Cardiovascular Disease Events Prevented with Adoption of the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline. Circulation. 2019;139:24–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Jaeger BC, Anstey DE, Bress AP, et al. Cardiovascular disease and mortality in adults aged ≥60 years according to recommendations by the American College of Cardiology/American Heart Association and American College of Physicians/American Academy of Family Physicians. Hypertension. 2019;73:327–334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Williamson JD, Pajewski NM, Auchus AP, et al. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical Ttial. JAMA. 2019;321:553–561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Nasrallah IM, Pajewski NM, Auchus AP, et al. Association of intensive vs standard blood pressure control with cerebral white matter lesions. JAMA. 2019;322:524–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.White WB, Wakefield DB, Moscufo N, Guttmann CRG, Kaplan RF, Bohannon RW, Fellows D, Hall CB, Wolfson L. Effects of intensive versus standard ambulatory blood pressure control on cerebrovascular outcomes in older people (INFINITY). Circulation. 2019;140:1626–1635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Murray AM, Hsu FC, Williamson JD, et al. ACCORDION MIND: results of the observational extension of the ACCORD MIND randomised trial. Diabetologia. 2017;60:69–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Pajewski NM, Berlowitz DR, Bress AP, Intensive vs standard blood pressure control in adults 80 years or older: a secondary analysis of the Systolic Blood Pressure Intervention Trial. J Am Geriatr Soc. 2020;68:496–504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Williamson JD, Supiano MA, Applegate WB, et al. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >/=75 years: a randomized clinical trial. JAMA. 2016;315:2673–2682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Hughes D, Judge C, Murphy R, Loughlin E, Costello M, Whiteley W, Bosch J, O’Donnell MJ, Canavan M. Association of blood pressure lowering with incident dementia or cognitive impairment: a systematic review and meta-analysis. JAMA. 2020;323:1934–1944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Peters R, Yasar S, Anderson CS, et al. Investigation of antihypertensive class, dementia, and cognitive decline: a meta-analysis. Neurology. 2020;94:e267–e281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Gorelick PB, Whelton PK, Sorond F, Carey RM. Blood pressure management in stroke. Hypertension. 2020;76:1688–1695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, Deanfield J, Smeeth L, Timmis A, Hemingway H. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet Diabetes Endocrinol. 2015;3:105–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.The Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369:145–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan DM, Diabetes Prevention Program Research G. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Whelton PK, Campbell NRC, Lackland DT, Parati G, Ram CVS, Weber MA , Zhang XH. Strategies for prevention of cardiovascular disease in adults with hypertension. J Clin Hypertens (Greenwich). 2020;22:132–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Thomopoulos C, Parati G, Zanchetti A. Effects of blood-pressure-lowering treatment on outcome incidence in hypertension: 10 - Should blood pressure management differ in hypertensive patients with and without diabetes mellitus? Overview and meta-analyses of randomized trials. J Hypertens. 2017;35:922–944. [DOI] [PubMed] [Google Scholar]
- 117.de Boer IH, Bangalore S, Benetos A, Davis AM, Michos ED, Muntner P, Rossing P, Zoungas S and Bakris G. Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care. 2017;40:1273–1284. [DOI] [PubMed] [Google Scholar]
- 118.Muntner P, Whelton PK, Woodward M, Carey RM. A comparison of the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline and the 2017 American Diabetes Association Diabetes and Hypertension Position Statement for U.S. Adults With Diabetes. Diabetes Care. 2018;41:2322–2329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Group AS, Cushman WC, Evans GW, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Beddhu S, Chertow GM, Greene T, et al. Effects of intensive systolic blood pressure lowering on cardiovascular events and mortality in patients with type 2 diabetes mellitus on standard glycemic control and in those without diabetes mellitus: reconciling results rrom ACCORD BP and SPRINT. J Am Heart Assoc. 2018;7:e009326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Rahman F, McEvoy JW, Ohkuma T, et al. Effects of blood pressure lowering on clinical outcomes according to baseline blood pressure and cardiovascular risk in patients with type 2 diabetes mellitus. Hypertension. 2019;73:1291–1299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Cheung AK, Rahman M, Reboussin DM, et al. Effects of intensive BP control in CKD. J Am Soc Nephrol. 2017;28:2812–2823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Beddhu S, Rocco MV, Toto R, et al. Effects of intensive systolic blood pressure control on kidney and cardiovascular outcomes in persons without kidney disease: A secondary analysis of a randomized trial. Ann Intern Med. 2017;167:375–383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Malhotra R, Katz R, Jotwani V, et al. Urine markers of kidney tubule cell injury and kidney function decline in SPRINT trial participants with CKD. Clin J Am Soc Nephrol. 2020;15:349–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Nadkarni GN, Chauhan K, Rao V, Ix JH, Shlipak MG, Parikh CR, Coca SG. Effect of intensive blood pressure lowering on kidney tubule injury: findings from the ACCORD trial study participants. Am J Kidney Dis. 2019;73:31–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.KDIGO BP guideline (reference to be added in proof).
- 127.Cheng Y-B, Thijs L, Zhang ZY, et al. Outcome-driven thresholds for ambulatory blood pressure based on the new American College of Cardiology/American Heart Association classification of hypertension. Hypertension. 2019;74:776–783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Carey RM, Sakhuja S, Calhoun D, Whelton PK, Muntner P. Prevalence of apparent treatment resistant hypertension in the United States: comparison of the 2008 and 2018 American Heart Association Scientific Statements on resistant hypertension. Hypertension. 2019;73:424–431.doi: 10.1161HYPERTENSIONAHA.118.12191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Chun K-H, Lee CJ, Oh J, Lee S-H, Kang S-M, Kario K, Park S. Prevalence and prognosis of the 2018 vs 2008 AHA definition of apparent treatment resistant hypertension in high risk hypertension patients. J Clin Hypertens. 2020;22:2093–2102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Cardoso CRL, Salles GC, Salles GF. Prognostic impact of aortic stiffness in patients with resistant hypertension: a prospective cohort study. Hypertension. 2019;73:728–735. [DOI] [PubMed] [Google Scholar]
- 131.Cardoso CRL, Salles GC, Salles GF. Prognostic importance of on-treatment clinic and ambulatory blood pressures on resistant hypertension. Hypertension. 2020;75:1184–1194. [DOI] [PubMed] [Google Scholar]
- 132.Funder JW, Carey RM, Mantero F, Reincke M, Hirotaka S, Stowasser M, Young WF Jr. The management of primary aldosteronism: case detection, diagnosis and treatment. An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016; 101:1889–1916. [DOI] [PubMed] [Google Scholar]
- 133.Jaffe G, Gray Z, Krishnam G, Stedman M, Zhang Y, Han J, Chertow GM. Leppert JT, Balla V. Screening rates for primary aldosteronism in resistant hypertension: a cohort study. Hypertension. 2020;75:650–659. [DOI] [PubMed] [Google Scholar]
- 134.Williams B, MacDonald TM, Morant SV, et al. Endocrine and haemodynamic changes in resistant hypertension, and blood pressure responses to spironolactone and amiloride: the PATHWAY-2 mechanisms sub-studies. Lancet Diabetes Endocrinol. 2018;6:464–475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Ito S, Itoh H, Rakugi H, Okuda Y, Yoshimura M, Yamakawa S. Double blind randomized phase 3 study comparing esaxerenone (CS-3150) with eplerenone in patients with essential hypertension (ESAX-HTN Study). Hypertension. 2020;75:51–58. [DOI] [PubMed] [Google Scholar]
- 136.Agarwal R, Rossignol P, Romero A, Garza D, Mayo MR, Warren S, Mo J, White WB, Williams B. Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): a phase 2, randomized, double-blind, placebo-controlled trial. Lancet. 2019;394:1540–1550. [DOI] [PubMed] [Google Scholar]
- 137.Tsujimoto T, Kajio H. Intensive blood pressure treatment for resistant hypertension: secondary analysis of a randomized controlled trial. Hypertension. 2019;73:415–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Casey DE, Daniel D, Bhatt J, Carey RM, Commodore-Mensah Y, Holmes A, Smith AP, Wozniak G, Wright JT Jr. Controlling high blood pressure: an evidence-based blueprint for change. Am J Med Quality. 2021;(in press) [DOI] [PubMed] [Google Scholar]
- 139.Sigmund CD, Appel L, Arnett D, et al. Report of the NHLBI Working Group on Hypertension: Barriers to translation. Hypertension. 2020; doi: 10.1161/HYPERTENSIONAHA.119.13887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Mu L, Kukamai KJ. Treatment intensification for hypertension in US ambulatory medical care. J Am Heart Assoc. 2016;5:e004188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Milman T, Joundi RA, Alotaibi NM, Saposnik G. Clinical inertia in pharmacological management of hypertension: a systematic review and meta-analysis. Medicine (Baltimore). 2018;97:e11121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Sim JJ, Handler J, Jacobsen SJ, Kanter MH. Systemic implementation strategies to improve hypertension: the Kaiser Permanente Southern California experience. Can J Cardiol. 2014;30:544–552. doi: 10.1016/j.cjca.2014.01.003 [DOI] [PubMed] [Google Scholar]
- 143.Burnier M, Egan BM. Adherence in hypertension: a review of prevalence, risk factors, impact and management. Circ Res. 2019;124:1124–1140. [DOI] [PubMed] [Google Scholar]
- 144.Mills KT, Obst KM, Shen W, et al. Comparative effectiveness of implementation strategies for blood pressure control in hypertensive patients: a systematic review and meta-analysis. Ann Intern Med. 2018; 168:110–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Santschi V, Chiolara A, Colosimo AL, Platt RW, Taffe P, Burnier M, Burnand B, Paradis G. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. JAHA. 2014;3:e000718. doi: 10.1161/JAHA.113000718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Nakanishi M, Mizuno T, Mizokami F, Koscki T, Takahashi K, Tsuboi N, Katz M, Lee J, Yamada S. Impact of pharmacist intervention for blood pressure control in patients with chronic kidney disease: a meta-analysis of randomized clinical trials. J Clin Pharm Ther. 2021;46:114–120. [DOI] [PubMed] [Google Scholar]
- 147.Victor RG, Lynch K, Li N, Blyler C, Muhammad E, Handler J, et al. Cluster randomized trial of pharmacist-driven blood pressure reduction in black barbershops. N Engl J Med. 2018;378:1291–1301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Omboni S, McManus RJ, Bosworth HB, et al. Evidence and recommendations on the use of telemedicine for the management of arterial hypertension: an international expert position paper. Hypertension, 2020;76:1368–1383. [DOI] [PubMed] [Google Scholar]
- 149.McManus RJ, Mant J, Franssen M, et al. Efficacy of self-monitored blood pressure, with or without telemonitoring, for titration of antihypertensive medication: an unmasked randomized controlled trial. Lancet,. 2018;391:949–959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Monahan M, Jowett S, Franssen M, Grant S, Greenfield S, Hobbs FDR, Hodgkinson J, Mant J, McManus RJ. Cost-effectiveness of telemonitoring and self-monitoring of blood pressure for antihypertensive titration in the primary care (TASMINH4). Hypertension. 2019;73:1231–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.