

Key Points
Question
Is the risk of suicide among US nurses and physicians greater than that in the general population?
Findings
In this cohort study using data from 2007 to 2018 that included 2374 nurses, 857 physicians, and 156 141 individuals in the general population (age, ≥30 years), the suicide incidence rates per 100 000 in 2017-2018 among women were 17.1 for nurses, 10.1 for physicians, and 8.6 for the general population, and the suicide incidence rates per 100 000 in 2017-2018 among men were 31.1 for nurses, 31.5 for physicians, and 32.6 for the general population. The suicide risk compared with the general population was significantly increased for nurses but not for physicians.
Meaning
This study suggests that there was a significantly increased suicide risk for the usual occupation of nurse but not for physician.
Abstract
Importance
Nurses are the largest component of the US health care workforce. Recent research suggests that nurses may be at high risk for suicide; however, few studies on this topic exist.
Objectives
To estimate the national incidence of suicide among nurses and examine characteristics of nurse suicides compared with physicians and the general population.
Design, Setting, and Participants
This retrospective cohort study used US data from 159 372 suicides reported in the National Violent Death Reporting System from 2007 to 2018. With the use of workforce denominators, sex-specific suicide incidence estimates were generated among nurses, physicians, and the general population (age, ≥30 years). Associations between clinician type and method of suicide and results of toxicology examination at death were calculated, adjusted for sociodemographic characteristics. Statistical analysis was performed from October 16, 2020, to January 10, 2021.
Exposure
Occupation as a nurse or physician.
Main Outcome and Measures
Suicide incidence and characteristics associated with suicides.
Results
A total of 2374 suicides among nurses (1912 women [80.5%]; mean [SD] age, 52.8 [11.8] years), 857 suicides among physicians (723 men [84.4%]; mean [SD] age, 59.8 [15.3] years), and 156 141 suicides in the general population (121 483 men [77.8%]; mean [SD] age, 53.1 [14.7] years) were identified. Overall, suicide was more common among nurses compared with the general population (sex-adjusted incidence in 2017-2018, 23.8 per 100 000 vs 20.1 per 100 000; relative risk, 1.18 [95% CI, 1.03-1.36]). Among women in 2017-2018, the suicide incidence among nurses was 17.1 per 100 000 (506 among 2 966 048) vs 8.6 per 100 000 (8879 among 103 731 387) in the general female population (relative risk, 1.99 [95% CI, 1.82-2.18]). In absolute terms, being a female nurse was associated with an additional 8.5 suicides per 100 000 (95% CI, 7.0-10.0 per 100 000) compared with the general population of women. By sex, physician suicide rates were not statistically different from the general population other than among female physicians in 2011-2012 (11.7 per 100 000 [95% CI, 6.6-16.8 per 100 000] female physicians vs 7.5 per 100 000 [95% CI, 7.2-7.7 per 100 000] general population; P = .04). In terms of the characteristics of suicides, clinicians were more likely to use poisoning than the general population; for example, 24.9% (95% CI, 23.5%-26.4%) of nurses used poisoning compared with 16.8% (95% CI, 16.6%-17.0%) of the general suicide population. The presence of antidepressants, benzodiazepines, barbiturates, and opiates was more common among clinician suicides than suicides in the general population.
Conclusion and Relevance
This study suggests that, in the US, the risk of suicide compared with the general population was significantly greater for nurses but not for physicians. Further research is needed to assess whether interventions would be associated with benefit in reducing suicide risk among nurses.
This cohort study estimates the national incidence of suicide among nurses and examines characteristics of nurse suicides compared with physicians and the general population.
Introduction
In 2018, more than 48 000 individuals died by suicide, and in recent years, suicide has become one of the leading causes of death among US adults.1 International comparisons indicate that the US is among the countries with the highest rate of both suicide mortality and ideation and that the incidence of suicide is increasing.2 Suicide is a complex public health problem that entails an interplay among predisposing, environmental, and mediating factors.3 In particular, an individual’s occupation can impose specific stressors that place them at higher risk of suicide.4
Because of high job demands, avoidance of use of mental health services owing to fear of stigma, and greater access to means to complete suicide via medications, those who work in health care fields are considered to be at higher risk of suicide than the general public.5,6 Most of what is known about suicide among health care clinicians originated from studies of physicians.7 Depression, in particular, may interact with work stress, resulting in decreased work satisfaction and role conflicts and placing physicians at higher risk of suicidal ideation.8
To our knowledge, less is known about suicide among nurses. Although nursing is the largest health care profession (3.3 million nurses in the US),9 there are very few empirical studies of suicide among US nurses,10,11,12,13 too few to be included in a recent meta-analysis.7 However, recent studies found that the incidence of suicide among nurses is higher than that in the general population. A National Academy of Medicine publication raised awareness of the paucity of data on nurse suicide and called for national estimates.6
The objective of this study was to use US data on suicides over a 12-year period to estimate trends in the incidence and characteristics of suicide among US nurses and physicians and to compare the risk of suicide among US nurses and physicians with that of the general adult population.
Methods
To examine suicide among US nurses, in this cohort study, we gathered national data from a variety of sources, including (1) suicide data from the Centers for Disease Control and Prevention National Violent Death Reporting System (NVDRS) and (2) workforce data from the US Bureau of Labor Statistics and the Association of American Medical Colleges State Physician Workforce Data. The combination of these data sets enabled us to estimate incidence trends and examine the characteristics associated with suicides among nurses, physicians, and the general adult (age, ≥30 years) population. Our study used data from decedents and publicly available data; therefore, it was deemed exempt from review by the University of Michigan’s Health and Behavioral Sciences institutional review board.
Study Population
The NVDRS is the largest collection of data on US suicides. We analyzed all suicide deaths reported in the NVDRS from 2007 to 2018 (eFigure 1 in the Supplement). The NVDRS collects data from death certificates, medical examiner reports, law enforcement reports, and toxicology examinations. Throughout the study time frame, the number of US states providing complete data on violent deaths to the NVDRS increased from 16 in 2007 to 38 in 2018. The NVDRS collects data using specific data abstraction protocols on the usual occupation of the decedent (obtained from the death certificate), suicide method (ie, how the death occurred), and results of toxicology examination at the time of death.14
The NVDRS collects the decedent’s usual occupation from a free-text field on the death certificate. The NVDRS adds occupational codes using the Standard Occupational Classification (SOC) System used by the US Bureau of Labor Statistics.15 We used both the free text and SOC System to identify nurse and physician suicides.
Two independent reviewers (M.A.D. and C.R.F.) read all free-text occupation descriptions. Our operational definition of a nurse suicide was a decedent whose usual occupation required holding a nursing diploma or associate degree in nursing, bachelor degree in nursing, or higher, indicated by terms such as registered nurse, R.N., nurse practitioner, or midwife. Nursing assistants and related phrases were excluded (eTable 1 in the Supplement). A broad list of terms was used to identify physician suicides, including terms related to physician specialties (eTable 2 in the Supplement). Occupations indicating a student status, such as “nursing student” and “medical student,” were excluded. The Cohen κ statistics for interrater reliability were 0.97 for the identification of nurse suicides and 0.91 for the identification of physician suicides. After independent review, discrepancies were discussed until consensus was achieved. In addition to the free text, SOC System codes were used to further identify nurse suicides and physician suicides. To mitigate the potential difference in age due to length of training necessary to obtain a professional degree between nurses, physicians, and individuals in the general population who died by suicide, we restricted our analyses to decedents who were 30 years or older at the time of death (eFigure 1 in the Supplement).
Method of Suicide
The NVDRS ascertains the suicide method by compiling data from death certificates, medical examiner reports, and law enforcement reports; the NVDRS reports the suicide method used. We categorized the method of suicide as firearm, hanging or suffocation, or poisoning (which includes suicide by use of either prescription or illicit drugs) vs all other causes.
Substances Identified in Toxicology Testing
Considering the higher use of poisoning as a suicide method among health care clinicians, we were particularly interested in the substances identified from toxicology examination results. A total of 97 946 of 159 372 decedents (61.5%) in the NVDRS underwent any toxicology testing. We report on key substances among decedents with valid test results that vary by substance. The substances that we examined included antidepressants, antipsychotics, benzodiazepines, barbiturates, opiates, amphetamines, and cocaine. Alcohol use at the time of death was identified as death of an individual with a blood alcohol level greater than 0.08%.
Workforce Estimates
To estimate trends in the incidence of suicide among nurses and physicians, we gathered workforce estimates by state from 2007 to 2018. State-level nursing workforce estimates were obtained from the US Bureau of Labor Statistics’ Occupation Employment Statistics program.16 After 2009, the SOC codes used by the Occupation Employment Statistics program were expanded from a single code to separate nurse practitioners, nurse midwives, and nurse anesthetists. We used SOC codes over time to generate consistent workforce estimates. Physician workforce estimates by state were obtained from the Association of American Medical Colleges State Physician Workforce Data.17 We selected this data source for physicians because it includes all specialties by state and is updated every other year.
The estimated yearly percentages of nurses and physicians who are female and male were obtained from the Current Population Survey throughout the study period.18 For each profession, we assumed the relative annual percentage female and male to be homogenous across US states. State estimates of the total female and male adult population (age, ≥30 years) were obtained from the US Census Bureau’s American Community Survey.19
Covariates
We used NVDRS data on basic sociodemographic characteristics, including age at the time of death, sex, and race/ethnicity as covariates. These measures were obtained from death certificates, medical examiner reports, and law enforcement reports. Race and ethnicity were combined into the following categories: non-Hispanic White, non-Hispanic Black, Hispanic, and other (ie, all other and multiple races/ethnicities). Marital status is associated with suicide risk20; therefore, we also identified decedents as married, never married, widowed or divorced, single, or having no other information provided.
Statistical Analysis
Statistical analysis was performed from October 16, 2020, to January 10, 2021. We aggregated our numerators and denominators into 2-year increments to estimate suicide incidence over time. The number of states participating in the NVDRS varied during the 12-year period; thus, we included the relevant states with census data for each given year to estimate respective workforces (eTable 3 in the Supplement). To test whether variable state involvement affected our results, we conducted a sensitivity analysis in which we restricted our analyses to the 16 states that participated in the NVDRS throughout the entire 12-year period. Previous research has uncovered significant differences in suicide ideation and mortality by sex.21,22 Considering this finding along with the fact that nurses are predominantly female and a higher proportion of physicians is male, we stratified incidence estimates by sex. We standardized the sex distribution of nurses and physicians to the 2018 US population (age, ≥30 years) when comparing relative risks (RRs) for suicide between groups.
For descriptive analyses of sociodemographic characteristics, we used t tests, χ2 tests, and 1-way analysis of variance to compare groups. Logit models were used to calculate the adjusted association between being a health care professional (either nurse or physician) and the method of suicide and substances identified at death. Models were adjusted for age at death, sex, race/ethnicity, and marital status. All analyses were based on complete case analysis. Marital status was the only covariate with missing values (unknown for 1.4% of decedents [2199 of 159 372]). The statistical significance level was set at a critical α level of .05 and was 2-sided. Analyses were performed using Stata, version 16.0 (StataCorp LLC) and SAS, version 9.4 (SAS Institute Inc).
Results
A total of 159 372 suicides from 2007 to 2018 among decedents aged 30 years or older were assessed. Reviewing all 24 028 free-text occupation descriptions reported in the NVDRS resulted in the identification of 2374 suicides among nurses, 857 suicides among physicians, and 156 141 suicides in the general population (eFigure 1 in the Supplement). The mean (SD) age of nurse decedents was 52.8 (11.8) years, 1912 (80.5%) were female, 462 (19.5%) were male, and 2166 (91.2%) were non-Hispanic White (Table 1). Among physician decedents, the mean (SD) age was 59.8 (15.3) years, 723 (84.4%) were male, 134 (15.6%) were female, and 724 (84.5%) were non-Hispanic White. Nurse decedents were less likely to be married than physician decedents (944 [39.8%] vs 480 [56.0%]; P < .001). Compared with the general population, nurse decedents were more likely to be female (1912 [80.5%] vs 34 658 [22.2%]), less racially diverse (non-Hispanic White, 2166 [91.2%] vs 135 615 [86.9%]), and less likely to be never married (338 [14.2%] vs 33 662 [21.6%]).
Table 1. Characteristics of Suicides Among Nurses Compared With Physicians and the General Adult Population.
| Characteristic | Nurse | Physician | P value for difference between nurses and physiciansa | General populationb | P value for difference across all groupsa |
|---|---|---|---|---|---|
| Total sample, No. | 2374 | 857 | NA | 156 141 | NA |
| By year, No. (%) | |||||
| 2007-2008 | 207 (8.7) | 75 (8.8) | .86 | 15 267 (9.8) | .38 |
| 2009-2010 | 220 (9.3) | 87 (10.2) | 16 207 (10.4) | ||
| 2011-2012 | 303 (12.8) | 105 (12.3) | 19 405 (12.4) | ||
| 2013-2014 | 358 (15.1) | 116 (13.5) | 21 511 (13.8) | ||
| 2015-2016 | 557 (23.5) | 201 (23.5) | 35 398 (22.7) | ||
| 2017-2018 | 729 (30.7) | 273 (31.9) | 48 353 (31.0) | ||
| Sociodemographic | |||||
| Age, mean (SD), y | 52.8 (11.8) | 59.8 (15.3) | <.001 | 53.1 (14.7) | <.001 |
| Sex, No. (%) | |||||
| Male | 462 (19.5) | 723 (84.4) | <.001 | 121 483 (77.8) | <.001 |
| Female | 1912 (80.5) | 134 (15.6) | 34 658 (22.2) | ||
| Race/ethnicity, No. (%) | |||||
| Non-Hispanic White | 2166 (91.2) | 724 (84.5) | <.001 | 135 615 (86.9) | <.001 |
| Non-Hispanic Black | 72 (3.0) | 33 (3.9) | 7630 (4.9) | ||
| Hispanic | 58 (2.4) | 24 (2.8) | 6790 (4.4) | ||
| Otherc | 78 (3.3) | 76 (8.9) | 6106 (3.9) | ||
| Marital status, No. (%)d | |||||
| Married | 944 (39.8) | 480 (56.0) | <.001 | 61 318 (39.4) | <.001 |
| Never married | 338 (14.2) | 115 (13.4) | 33 662 (21.6) | ||
| Single, widowed, or divorced | 1074 (45.2) | 261 (30.5) | 58 981 (37.8) | ||
| Unknown | NA | NA | 2180 (1.4) |
Abbreviations: ANOVA, analysis of variance, NA, not applicable.
The t test or 1-way ANOVA was used to compare mean values, and the χ2 test was used to compare proportions.
General population refers to adults (age, ≥30 years) who are not nurses or physicians.
Refers to all other races and ethnicities and individuals of multiple racial/ethnic backgrounds.
Column total does not sum to 100% owing to missing data (not displayed for data suppression purposes).
Trends and Incidence of Suicide
From 2007-2008 to 2017-2018, nurses had a higher suicide incidence than that of the general population, with modest increases over time (Figure 1). However, suicide incidence among male nurses decreased to below that of the general population in 2017-2018. During the 12-year period, suicide incidence among physicians was not statistically different from that of the general population except among female physicians in 2011-2012 (11.7 per 100 000 [95% CI, 6.6-16.8 per 100 000] female physicians vs 7.5 per 100 000 [95% CI, 7.2-7.7 per 100 000] general population; P = .04) (eTable 4 in the Supplement). In the sensitivity analysis restricted to states that participated in the NVDRS throughout the entire period, incidence estimates did not differ appreciably (eFigure 2 in the Supplement).
Figure 1. Unadjusted Trends in Suicide Incidence Among Nurses, Physicians, and the General Adult Population for Women and Men.
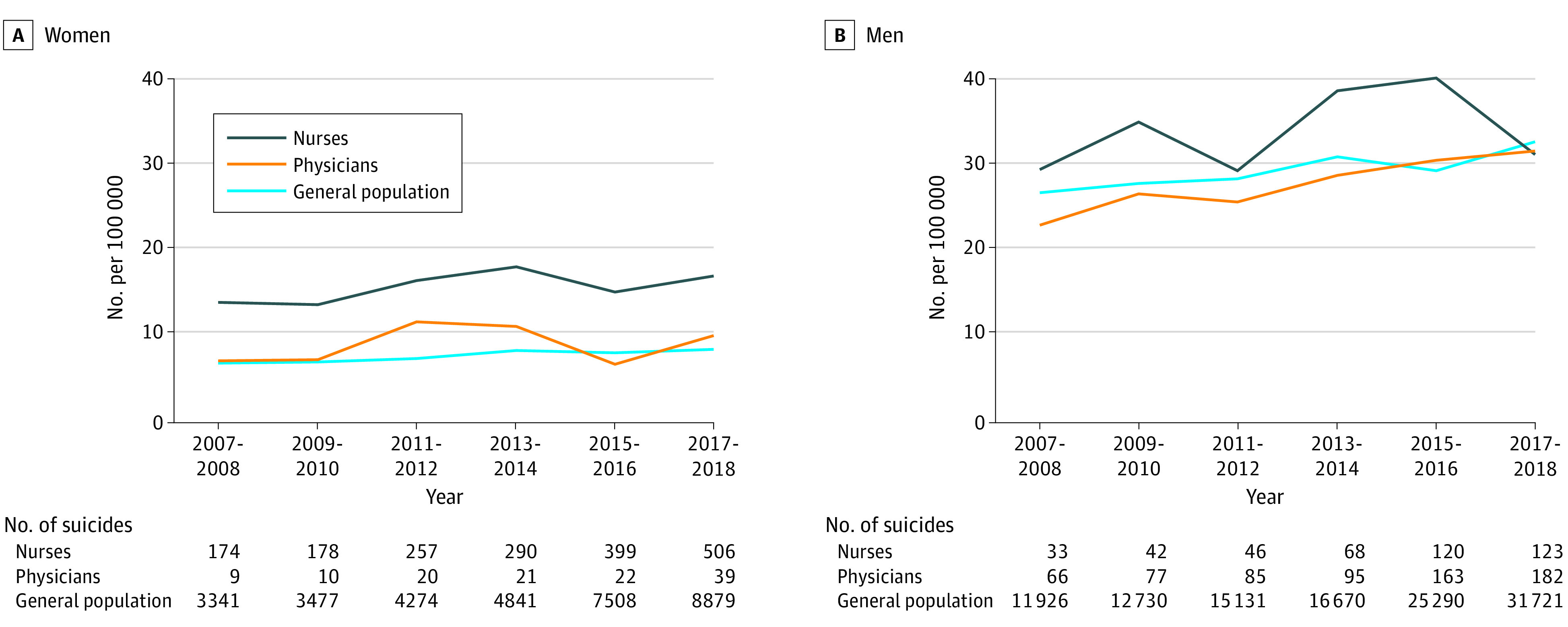
The numbers of suicides do not sum to total for each group in Table 1 because analyses are restricted to states with 2 years of data for each time point. Suicide incidence estimates can be found in eTable 4 in the Supplement. General population refers to adults (age, ≥30 years) who are not nurses or physicians.
Adjusted for sex differences in 2017-2018, nurses exhibited a higher incidence of suicide compared with the general population (23.8 per 100 000 vs 20.1 per 100 000; RR, 1.18 [95% CI, 1.03-1.36]) (Table 2). Among women in 2017-2018, the suicide incidence among nurses was 17.1 per 100 000 (506 of 2 966 048) vs 8.6 per 100 000 (8879 of 103 731 387) in the general female population (RR, 1.99 [95% CI, 1.82-2.18]) (Table 2 and eTable 4 in the Supplement). In absolute terms, being a female nurse was associated with an additional 8.5 suicides per 100 000 (95% CI, 7.0-10.0 per 100 000) compared with the general population of women. Among men in 2017-2018, suicide incidence among nurses (31.1 per 100 000 [123 of 395 462]) did not statistically differ compared with the general population of men (32.6 per 100 000 [31 721 of 97 384 882]).
Table 2. Relative Risk Comparing Suicide Incidence Among Nurses and Physicians With the General Adult Populationa.
| Characteristic | Relative risk (95% CI) | ||
|---|---|---|---|
| Nurse vs general populationa | Physician vs general populationa | Nurse vs physician | |
| Overallb | 1.18 (1.03-1.36) | 1.01 (0.79-1.30) | 1.17 (0.88-1.55) |
| By sex | |||
| Women | 1.99 (1.82-2.18) | 1.18 (0.86-1.60) | 1.70 (1.22-2.35) |
| Men | 0.95 (0.80-1.14) | 0.97 (0.84-1.12) | 0.99 (0.79-1.24) |
General population refers to adults (age, ≥30 years) who are not nurses or physicians. Incidence rates are based on 2017-2018 data (most recent data available). Absolute values for comparative measures by sex can be found in Figure 1 (eTable 4 in the Supplement).
Overall relative risk standardized for difference in sex distribution among nurses and physicians (2018 US age, ≥30 years population used as reference).
In 2017-2018, the suicide incidence was 31.5 per 100 000 among male physicians (182 of 577 862) vs 32.6 per 100 000 in the general population of men (31 721 of 97 384 882) (RR, 0.97 [95% CI, 0.84-1.12]) (Table 2). Suicide incidence was not statistically different among female physicians vs the general population of women (RR, 1.18 [95% CI, 0.86-1.60]).
When comparing suicide incidence among nurses with that of physicians, the only statistically significant difference was among women. In 2017-2018, the suicide incidence among female nurses was 17.1 per 100 000 (506 of 2 966 048) vs 10.1 per 100 000 female physicians (39 of 387 689) (RR, 1.70 [95% CI, 1.22-2.35]) (Table 2). In absolute terms, being a female nurse compared with a female physician was associated with an additional 7.0 suicides per 100 000 (95% CI, 3.5-10.5 per 100 000).
Characteristics of Suicide
Method of Suicide
Adjusted for sociodemographic differences, both nurses and physicians were statistically more likely to use poisoning and less likely to use a firearm than individuals in the general population who died by suicide (Figure 2); 24.9% (95% CI, 23.5%-26.4%) of nurse suicides involved poisoning vs 16.8% (95% CI, 16.6%-17.0%) of suicides in the general population. Nurses who died by suicide exhibited similar methods as physicians yet were less likely to use hanging or suffocation than physicians (ie, 19.4% [95% CI, 17.7%-21.0%] of nurses vs physicians, 24.1% [95% CI, 21.2%-27.1%] of physicians).
Figure 2. Adjusted Method of Suicide Among Nurses, Physicians, and the General Adult Population (n = 155 919).

Percentages are adjusted for age, sex, race/ethnicity, and marital status. Error bars indicate 95% CIs. General population refers to adults (age, ≥30 years) who are not nurses or physicians.
Substances Identified in Toxicology Examination
After adjustment for sociodemographic differences, both nurses and physicians who died by suicide were statistically more likely to have certain medications identified in the toxicology examination than were individuals among the general population who died by suicide (Figure 3). For instance, 46.0% (95% CI, 40.1%-51.3%) of physician suicides had evidence of antidepressants identified vs 36.4% (95% CI, 36.0%-36.8%) of suicides in the general population. Compared with the general population, nurse decedents had statistically significantly higher levels of antidepressants (44% vs 36%), benzodiazepines (42.0% vs 32.7%), and opiates (33.7% vs 27.4%) identified in the toxicology examination at the time of death.
Figure 3. Adjusted Substances Identified in Toxicology Examination at Time of Suicide Death Among Nurses, Physicians, and the General Adult Population.
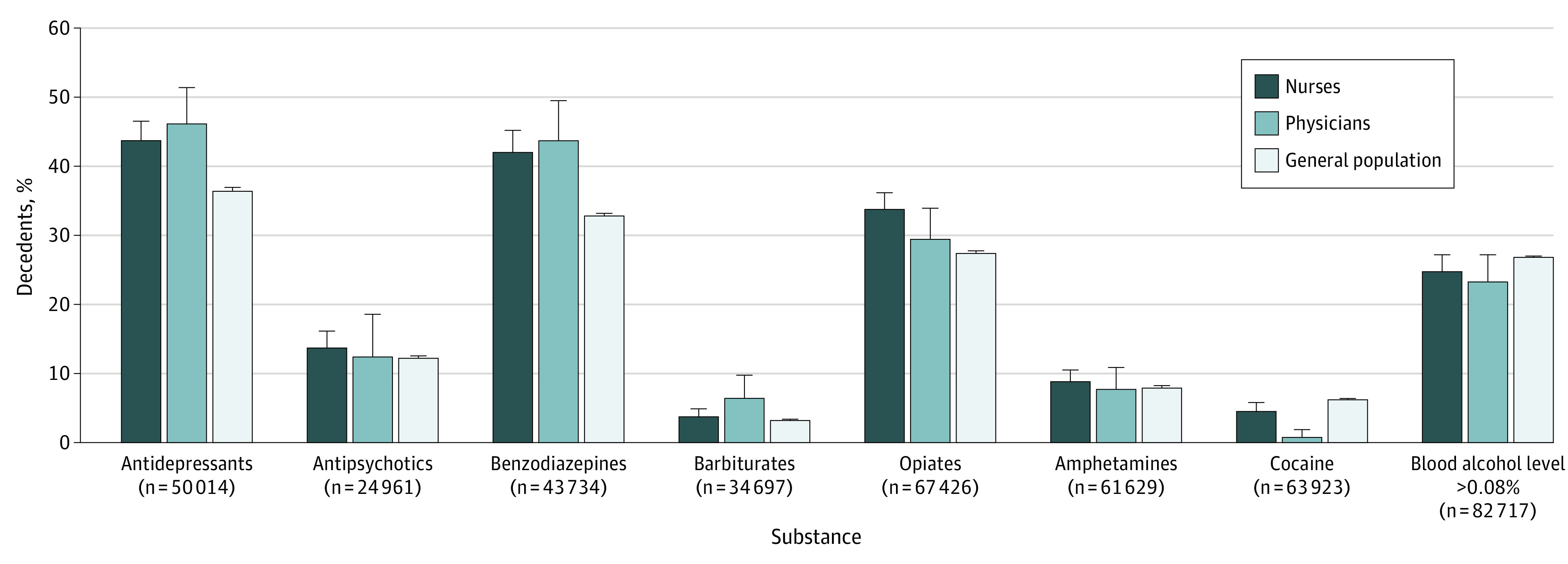
A decedent can use more than 1 substance; therefore, totals do not sum to 100%. Percentages are adjusted for age, sex, race/ethnicity, and marital status. Error bars indicate 95% CIs. General population refers to adults (age, ≥30 years) who are not nurses or physicians.
Discussion
In the US between 2007 and 2018, the incidence of suicide among nurses was significantly greater than among the general population; in contrast, the incidence among physicians was not statistically different from that in the general population. The methods of suicide and substances identified during the toxicology examinations among nurses and physicians are similar to each other, with some evidence of higher substance use compared with individuals in the general population who die by suicide. Nurses who died by suicide had the highest rate of antipsychotics, opiates, and amphetamines in the toxicology examination.
Early studies of nurse suicides that analyzed data from the 1980s to the 1990s produced conflicting results. One report with a large sample of nurses from 1982 to 1996 found no difference in suicide incidence vs the general population23; however, another study that used 1990 data found an increased risk.24 More recent studies report a relative difference when comparing nurses with the general population.10,11,12,13 For instance, using 2014 NVDRS data, Davidson and colleagues11 reported the RR of suicide among female nurses vs the general population to be 1.58 (95% CI, 1.34-1.85). This present analysis highlights that incidence rates of suicide among nurses are higher than that of both the general population and physicians.
Suicide rates of physicians were not statistically different from the general US population. Across the world, suicide rates are reportedly higher among physicians than the general population.7,25 A recent meta-analysis found that considerable heterogeneity exists across studies (I2 = 93.9%; P < .001) and that the association differed by sex.7 The risk of suicide among female physicians was considerably higher than that of the general female population (standardized mortality ratio, 1.94 [95% CI, 1.49-2.58]), but the risk among male physicians was less pronounced compared with that of the general male population (standardized mortality ratio, 1.24 [95% CI, 1.05-1.43]). The present study did not identify a statistically significant difference in men or women. Several possibilities may explain the observed lack of increased suicide risk among physicians compared with the general population. Prior studies had limited generalizability (ie, small sample size and limited geographic scope) or used data from an earlier time period (only 1 study12 used data after 2000), and many were conducted outside the US.
Among prior studies of suicide among US physicians, only 6 estimated the actual incidence of suicide as opposed to reporting solely standardized mortality ratios, and only 3 used data that spanned multiple states.12,26,27,28,29,30 The sex-specific incidence estimates in this present study most closely align with the suicide incidence reported by Petersen and Burnett,26 who used data from 26 states during the period from 1984 to 1992 among decedents of similar age. Those authors estimated the suicide incidence to be 21.3 per 100 000 among male physicians and 11.8 per 100 000 among female physicians, similar to our findings of 22.9 per 100 000 among male physicians and 7.2 per 100 000 among female physicians in 2007-2008. Early US studies27,29 used different data sources that included obituaries and American Medical Association workforce estimates. Another speculative cause of the observed lack of increased suicide risk among physicians compared with the general population could be undercoding of death as suicide by medical examiners who completed the report for physician colleagues.
The overall profile of suicide method and results of toxicology examination at death appeared similar among nurses and physicians. Similar to other studies,11,31 this study finds that—likely owing to access and knowledge about prescription medications—poisoning is the most common method of suicide among nurses and physicians. Both nurses and physicians were more likely to have antidepressants, benzodiazepines, and barbiturates identified in the results of the toxicology examination. The higher presence of barbiturates at death is notable because of their infrequent clinical use.
Limitations
This study has several limitations. First, our study was an observational design that used previously collected data. Although this study accounted for basic sociodemographic differences, the potential association of residual confounding with outcomes cannot be excluded. Second, many of the measures used in the NVDRS rely on interpretation by coders—identification of the decedent’s usual occupation from death certificates may be subject to occasional misclassification. Furthermore, health professions may be underreported given the fact that level of training (ie, holding a professional degree) is not used by the NVDRS. Third, although this study used the most consistent state-level workforce estimates available to estimate suicide incidence, an error may exist in workforce estimates, and the estimates by age in each year were not available. In a sensitivity analysis, we did not find that the distribution of age among nurses would have biased results in a meaningful way (eFigure 3 in the Supplement). Specifically, among women. there are more nurses in the age range from 55 to 64 years, which does not correspond to the highest suicide incidence observed at 50 to 54 years of age in the general population. National data on the distribution of age among physicians was not available. Fourth, while this study was restricted based on an age of 30 years or older, it did not apply a maximum age. Therefore, our estimates include a small number of nurse and physician decedents who may have been retired. They also exclude suicides among nurses aged 21 to 30 years; however, they are counted in the workforce estimate (ie, denominator of incidence estimates), which biases the incidence toward the null. Fifth, given that not all states participate in the NVDRS, our results may not be generalizable to the entire US population.
Conclusions
In the US, the suicide rate among nurses exceeds that in the general population. Initiatives to promote clinician well-being should include a particular focus on nurses. Our findings contribute to a growing body of literature suggesting that health care institutions should routinely assess clinician well-being and intervene if necessary, the benefits of which may extend well beyond the clinicians themselves.32
eFigure 1. Flow Diagram for the Identification of Nurse and Physician Suicides in the National Violent Death Reporting System Database
eTable 1. De-identified Terms From Free Text Used to Identify Nurse Suicides in the National Violent Death Reporting System Database
eTable 2. De-identified Terms From Free Text Used to Identify Physician Suicides in the National Violent Death Reporting System Database
eTable 3. States With Complete Data on Suicides Included in the National Violent Death Reporting System Database From 2007 to 2018
eTable 4. Unadjusted Trends in Suicide Incidence, Attributable Risk, and Relative Risk Among Nurses, Physicians, and the General Adult Population from 2007-08 to 2017-18
eFigure 2. Unadjusted Trends in Suicide Incidence Among Nurses, Physicians, and the General Adult Population for Women (A) and Men (B) Restricted to States That Participated in the National Violent Death Reporting System Database throughout 2007 to 2018
eFigure 3. Age Distribution of US Nurses, Age Distribution of General Population, and Suicide Incidence in the General Population
References
- 1.Centers for Disease Control and Prevention . WISQARS: leading causes of death reports, 1981-2019. Updated February 20, 2020. Accessed October 15, 2020. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html
- 2.World Health Organization . Preventing Suicide: A Global Perspective. World Health Organization Press; 2014. [Google Scholar]
- 3.Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227-1239. doi: 10.1016/S0140-6736(15)00234-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Milner A, Spittal MJ, Pirkis J, LaMontagne AD. Suicide by occupation: systematic review and meta-analysis. Br J Psychiatry. 2013;203(6):409-416. doi: 10.1192/bjp.bp.113.128405 [DOI] [PubMed] [Google Scholar]
- 5.Center C, Davis M, Detre T, et al. Confronting depression and suicide in physicians: a consensus statement. JAMA. 2003;289(23):3161-3166. doi: 10.1001/jama.289.23.3161 [DOI] [PubMed] [Google Scholar]
- 6.Davidson J, Mendis J, Stuck AR, DeMichele G, Zisook S. Nurse suicide: breaking the silence. National Academy of Medicine. Published January 8, 2018. Accessed October 15, 2020. https://nam.edu/nurse-suicide-breaking-the-silence/
- 7.Dutheil F, Aubert C, Pereira B, et al. Suicide among physicians and health-care workers: a systematic review and meta-analysis. PLoS One. 2019;14(12):e0226361. doi: 10.1371/journal.pone.0226361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Schwenk TL, Gorenflo DW, Leja LM. A survey on the impact of being depressed on the professional status and mental health care of physicians. J Clin Psychiatry. 2008;69(4):617-620. doi: 10.4088/JCP.v69n0414 [DOI] [PubMed] [Google Scholar]
- 9.Health Resources and Services Administration, National Center for Health Workforce Analysis. 2018 National Sample Survey of Registered Nurses: brief summary of results. United States Dept of Health and Human Services. Accessed November 15, 2020. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/data-research/nssrn-summary-report.pdf
- 10.Davidson JE, Proudfoot J, Lee K, Terterian G, Zisook S. A longitudinal analysis of nurse suicide in the United States (2005-2016) with recommendations for action. Worldviews Evid Based Nurs. 2020;17(1):6-15. doi: 10.1111/wvn.12419 [DOI] [PubMed] [Google Scholar]
- 11.Davidson JE, Proudfoot J, Lee K, Zisook S. Nurse suicide in the United States: analysis of the Center for Disease Control 2014 National Violent Death Reporting System dataset. Arch Psychiatr Nurs. 2019;33(5):16-21. doi: 10.1016/j.apnu.2019.04.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Davidson JE, Stuck AR, Zisook S, Proudfoot J. Testing a strategy to identify incidence of nurse suicide in the United States. J Nurs Adm. 2018;48(5):259-265. doi: 10.1097/NNA.0000000000000610 [DOI] [PubMed] [Google Scholar]
- 13.Patrician PA, Peterson C, McGuinness TM. Suicide among RNs: an analysis of 2015 data from the National Violent Death Reporting System. Am J Nurs. 2020;120(10):24-28. doi: 10.1097/01.NAJ.0000718624.25806.3f [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ertl A, Sheats KJ, Petrosky E, Betz CJ, Yuan K, Fowler KA. Surveillance for violent deaths — National Violent Death Reporting System, 32 states, 2016. MMWR Surveill Summ. 2019;68(9):1-36. doi: 10.15585/mmwr.ss.6809a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.U.S. Bureau of Labor Statistics . Standard occupational classification. 2019. Accessed October 15, 2020. https://www.bls.gov/soc/
- 16.U.S. Bureau of Labor Statistics . Occupational employment statistics. 2019. Accessed October 15, 2020. https://www.bls.gov/oes/
- 17.Association of American Medical Colleges . State physician workforce data report. Accessed October 15, 2020. https://www.aamc.org/data-reports/workforce/report/state-physician-workforce-data-report
- 18.U.S. Bureau of Labor Statistics . Women: labor force, employment, and unemployment statistics for women. Updated February 26, 2021. Accessed October 15, 2020. https://www.bls.gov/cps/demographics.htm#women
- 19.United States Census Bureau . American Community Survey data. Accessed August 15, 2019. https://www.census.gov/programs-surveys/acs/data.html
- 20.Kposowa AJ. Marital status and suicide in the National Longitudinal Mortality Study. J Epidemiol Community Health. 2000;54(4):254-261. doi: 10.1136/jech.54.4.254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Borges G, Nock MK, Haro Abad JM, et al. Twelve-month prevalence of and risk factors for suicide attempts in the World Health Organization World Mental Health Surveys. J Clin Psychiatry. 2010;71(12):1617-1628. doi: 10.4088/JCP.08m04967blu [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192(2):98-105. doi: 10.1192/bjp.bp.107.040113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Feskanich D, Hastrup JL, Marshall JR, et al. Stress and suicide in the Nurses’ Health Study. J Epidemiol Community Health. 2002;56(2):95-98. doi: 10.1136/jech.56.2.95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Stack S. Occupation and suicide. Soc Sci Q. 2001;82(2):384-396. doi: 10.1111/0038-4941.00030 [DOI] [Google Scholar]
- 25.Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302. doi: 10.1176/appi.ajp.161.12.2295 [DOI] [PubMed] [Google Scholar]
- 26.Petersen MR, Burnett CA. The suicide mortality of working physicians and dentists. Occup Med (Lond). 2008;58(1):25-29. doi: 10.1093/occmed/kqm117 [DOI] [PubMed] [Google Scholar]
- 27.Pitts FN Jr, Schuller AB, Rich CL, Pitts AF. Suicide among U.S. women physicians, 1967-1972. Am J Psychiatry. 1979;136(5):694-696. doi: 10.1176/ajp.136.5.694 [DOI] [PubMed] [Google Scholar]
- 28.Revicki DA, May HJ. Physician suicide in North Carolina. South Med J. 1985;78(10):1205-1207. doi: 10.1097/00007611-198510000-00016 [DOI] [PubMed] [Google Scholar]
- 29.Rich CL, Pitts FN Jr. Suicide by male physicians during a five-year period. Am J Psychiatry. 1979;136(8):1089-1090. doi: 10.1176/ajp.136.8.1089 [DOI] [PubMed] [Google Scholar]
- 30.Rose KD, Rosow I. Physicians who kill themselves. Arch Gen Psychiatry. 1973;29(6):800-805. doi: 10.1001/archpsyc.1973.04200060072011 [DOI] [PubMed] [Google Scholar]
- 31.Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. Gen Hosp Psychiatry. 2013;35(1):45-49. doi: 10.1016/j.genhosppsych.2012.08.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB. Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016;11(7):e0159015. doi: 10.1371/journal.pone.0159015 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Flow Diagram for the Identification of Nurse and Physician Suicides in the National Violent Death Reporting System Database
eTable 1. De-identified Terms From Free Text Used to Identify Nurse Suicides in the National Violent Death Reporting System Database
eTable 2. De-identified Terms From Free Text Used to Identify Physician Suicides in the National Violent Death Reporting System Database
eTable 3. States With Complete Data on Suicides Included in the National Violent Death Reporting System Database From 2007 to 2018
eTable 4. Unadjusted Trends in Suicide Incidence, Attributable Risk, and Relative Risk Among Nurses, Physicians, and the General Adult Population from 2007-08 to 2017-18
eFigure 2. Unadjusted Trends in Suicide Incidence Among Nurses, Physicians, and the General Adult Population for Women (A) and Men (B) Restricted to States That Participated in the National Violent Death Reporting System Database throughout 2007 to 2018
eFigure 3. Age Distribution of US Nurses, Age Distribution of General Population, and Suicide Incidence in the General Population