

Abstract
Homelessness affects tens of thousands of Canadians and has important health implications. Homeless people are at increased risk of dying prematurely and suffer from a wide range of health problems, including seizures, chronic obstructive pulmonary disease, musculoskeletal disorders, tuberculosis, and skin and foot problems. Homeless people also face significant barriers that impair their access to health care. More research is needed to identify better ways to deliver care to this population.
Homelessness, which is a focus of increasing concern in Canadian cities, has important health implications. Homeless people have high levels of morbidity and mortality and may experience significant barriers to accessing health care. This article addresses 3 key issues: first, who are the homeless? Second, what health problems are common among homeless people? Third, how does the health care system respond to the needs of the homeless?
Who are the homeless?
According to the United Nations, “absolute homelessness” describes the condition of people without physical shelter who sleep outdoors, in vehicles, abandoned buildings or other places not intended for human habitation. “Relative homelessness” describes the condition of those who have a physical shelter, but one that does not meet basic standards of health and safety; these include protection from the elements, access to safe water and sanitation, security of tenure, personal safety and affordability.1 In this review, “homeless people” refers to people who are sleeping in shelters for the homeless and those who are “absolutely homeless.”2 This is the definition that is most frequently used in health-related research. Although homelessness is commonplace in many developing countries, this review focuses on homelessness in Canada.1
The capacity of shelters for the homeless is a useful starting point for estimating the size of the homeless population (Table 1). These data suggest that each night about 8000 homeless people, that is, about 5 per 10 000 population, are sleeping in shelters in the 9 largest metropolitan areas of Canada. The number of individuals who use these shelters at least once over the course of a year is about 5 times this figure.4 In Toronto, for example, 28 800 people used such shelters in 1998.5
Table 1
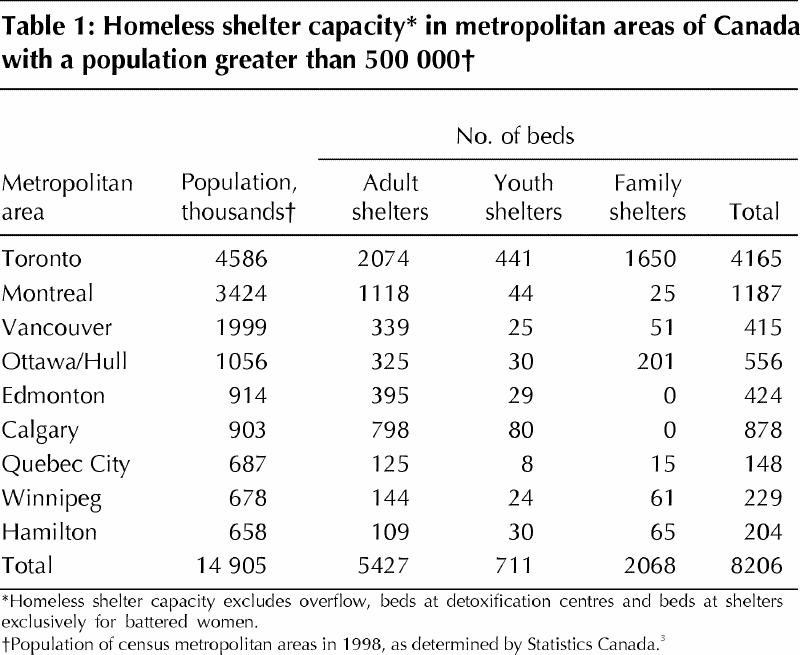
Shelter counts underestimate the number of homeless people because they do not include individuals who are sleeping on the street. Although these individuals are particularly difficult to count, they represent a sizable population in some cities. In Vancouver as many as 600 homeless people, or 3 per 10 000 population, sleep outside every night, thus exceeding the number of people staying in shelters.6
These figures indicate that the total number of homeless people in Canada on any given night is probably of the order of tens of thousands. In many cities, the number of people who are homeless has clearly increased in recent years. Toronto, which has the country's largest homeless population, has seen mean nightly shelter occupancy rise from 1902 individuals in 1990 to 3790 in 1998.5,7 Between 1992 and 1998, Calgary's homeless population more than doubled from 447 to 988.8 In Ottawa, the total number of overnight stays at men's shelters increased by about 8% between 1996 and 1998.9
The demographic characteristics of the homeless population vary significantly from city to city. Contrary to common stereotypes, homelessness affects a wide range of people, including families with children. Families occupy 42% of shelter beds in Toronto5 and about 35% of shelter beds in Ottawa.9 The average shelter stay for these families lasts 1.5–2 months.7,9 In contrast, other Canadian cities do not have significant numbers of homeless families. The phenomenon of homeless families in Toronto and Ottawa may reflect the convergence of multiple factors, including poverty, high housing costs and a shortage of subsidized public housing units.5,9,10
Single men constitute the largest segment of homeless people in most Canadian cities: about 70% of the homeless population in Vancouver,11 Edmonton12 and Calgary,8 and about 50% in Ottawa.9 In Toronto, single men occupy 35% of shelter beds.7 Although most single men stay in the shelter system for only a few nights, single men also account for 75% of chronically homeless individuals (those who stay in shelters for 1 year or more).7 Homeless men tend to be relatively young, with the majority between 25 and 44 years old.8,9,13
Single women account for about one-quarter of homeless people in Vancouver,11 Edmonton12 and Toronto,14 but as few as 10% of homeless people in cities such as Calgary8 and Ottawa.9 Studies in the United States suggest that a number of characteristics distinguish homeless single women from homeless women accompanied by children. Single women are more likely to be chronically homeless, older and to have a history of substance abuse or mental illness.15
The terms “homeless youth” and “street youth” are used interchangeably to refer to teenagers and young people below the age of 20–25 years. These young people first leave home at a mean age of 15 years, and many of them come from families where they experienced physical or sexual abuse.16,17 Toronto, Montreal and Vancouver have the largest numbers of street youth in Canada.17,18 Because most of these young people do not sleep in homeless shelters, shelter-based counts (Table 1) greatly underestimate the size of these populations. In Toronto, for example, about 75% of homeless youth do not use shelters.19
Aboriginal people are overrepresented in Canada's homeless population by a factor of about 10. Individuals of Aboriginal origin account for 35% of the homeless population in Edmonton,12 18% in Calgary,8 11% in Vancouver11 and 5% in Toronto,14 but only 3.8%, 1.9%, 1.7% and 0.4% of the general population of these cities respectively.20 A disproportionate number of homeless people who sleep on the street rather than in shelters are of Aboriginal origin.5,12
Health problems among homeless people
Homeless people have a greatly increased risk of death. Compared with the general youth population of Quebec, mortality rates among street youth in Montreal are 9 times higher for males and 31 times higher for females.21 Among men using shelters for the homeless in Toronto, mortality rates are 8.3 times higher than the mean for 18–24 year olds, 3.7 times higher than the mean for 25–44 year olds and 2.3 times higher than the mean for 45–64 year olds.13 However, death rates among homeless men in Toronto are about one-half that of homeless men in US cities.13 Mortality rates are lower in Canada because of a number of factors, including lower rates of homicide, HIV infection and, possibly, Canada's system of universal health insurance.
Homeless people suffer from a wide range of medical problems.11,22,23 Disease severity can be remarkably high because of factors such as extreme poverty, delays in seeking care, nonadherence to therapy, cognitive impairment and the adverse health effects of homelessness itself.22 Homeless people in their forties and fifties often develop health disabilities that are more commonly seen only in people who are decades older.24 Individuals living on the street tend to have a worse health status than shelter residents.25
Medical problems that are particularly prevalent among homeless adults include seizures, chronic obstructive pulmonary disease, arthritis and other musculoskeletal disorders.23 Conditions such as hypertension, diabetes and anemia are often inadequately controlled and may go undetected for long periods.25,26 Respiratory tract infections are common. Oral and dental health is often poor.27,28
Skin and foot problems are frequently seen among the homeless. People living on the street are particularly prone to develop skin diseases such as cellulitis, impetigo, venous stasis disease, scabies and body lice.29 Foot disorders such as onychomycosis, tinea pedis, corns and callouses, and immersion foot are usually the result of inadequate footwear, prolonged exposure to moisture, long periods of walking and standing, and repetitive minor trauma.30,31 Proper foot care requires early detection of problems, education regarding foot hygiene and the provision of adequate shoes and socks.30
Homeless people are at increased risk of contracting tuberculosis (TB), and this diagnosis should be considered in any homeless individual with a fever and a persistent productive cough.32 Conditions favouring TB outbreaks in shelters include crowding, large transient populations and inadequate ventilation.33 More than half of all TB cases among homeless people represent clusters of primary tuberculosis rather than reactivation of old disease.34,35 Published data on TB in Canada's homeless population are limited. The incidence of active TB among homeless people in Toronto is 71 per 100 000 (about 10 times the average Ontario rate).35
Treatment of active TB in homeless people can be complicated by nonadherence to therapy, prolonged infectivity and the development of drug resistance.36 Directly observed therapy results in higher cure rates and fewer relapses.37,38 Homeless people with positive tuberculin skin tests without active TB may be considered for directly observed prophylaxis.39
Common risk factors for HIV infection in homeless youth in Canada include prostitution, multiple sexual partners, inconsistent use of condoms and injection drug use.17,18,40 Infection rates were 2.2% and 11.3% among homeless youth seeking HIV testing at 2 clinics in Vancouver in 1988.41 The higher rate was seen at a clinic that served street youth involved in prostitution. In contrast, the prevalence of HIV infection was only 0.6% in a convenience sample of homeless youth surveyed in Toronto in 1990.42
The pattern of HIV risk factors in homeless adults is distinct from that of youth. In a 1997 study of a representative sample of adults using shelters for the homeless in Toronto, 25% had a history of using injection drugs and 41% had a history of using crack cocaine.14 These drug use behaviours, rather than sexual behaviours, were associated with an increased likelihood of HIV infection. The overall HIV infection rate in this study was 1.8%.14
Sexual and reproductive health is a major issue for street youth. In Montreal, 25% of homeless youth have engaged in prostitution.18 Sexually transmitted diseases are widespread, even among street youth who do not work as prostitutes; gonorrhea and Chlamydia are the most prevalent infections.17 Anecdotal reports suggest that pregnancy is common among street youth in Canada; in a recent study in the United States, 10% of homeless females aged 14–17 years were found to be pregnant.43
Violence is a constant threat to the health of homeless people. A survey in Toronto found that 40% of homeless individuals had been assaulted and 21% of homeless women had been raped in the previous year.23 Homeless men are about 9 times more likely to be murdered than their counterparts in the general population.13
Unintentional injuries are a leading cause of morbidity and mortality, especially among homeless men.13 Injuries are often the result of falls or being struck by a motor vehicle.13 Deaths due to an unintentional overdose of drugs or alcohol, or both, are also common.13 Exposure to the elements is a major hazard. In cold weather, the risk of frostbite and hypothermia is substantial,23 and deaths due to freezing are not uncommon.44 In hot weather, severe sunburn and heatstroke can occur.
The prevalence of mental illness and substance abuse among homeless people is difficult to determine precisely, but consistent patterns have emerged from methodologically rigorous studies conducted in the United States and Canada.14,45 Contrary to popular misconceptions, only a small proportion of the homeless population has schizophrenia. The lifetime prevalence of schizophrenia is only 6% among Toronto's homeless population,14 and US studies have found prevalence rates of 10%–13%.45 Affective disorders are much more common, with lifetime prevalence rates in the range of 20%–40%.14,45
Alcohol use disorders are widespread, with lifetime prevalence rates of about 60% among homeless men.45 Problems with alcohol are 6–7 times more prevalent among homeless people than in the general population.45 Fewer data are available on the abuse of substances other than alcohol; in US studies, the median prevalence of drug use disorders is 30%.46 Cocaine (especially crack) and marijuana are the illicit drugs that are most often used by homeless people in Canada.11,14,47 Dual diagnosis with both mental illness and substance abuse is not uncommon in this population.14,45,46
Patterns of substance abuse and mental illness vary across demographic subgroups. Homeless single women are more likely to have mental illness alone, without any substance use disorder.45 The prevalence of substance use disorders in men is about twice that in single women.45 Compared with all other subgroups of homeless people, female heads of homeless families have far lower rates of both substance abuse and mental illness.10
Homelessness and the health care system
Homeless adults have high levels of health care use48 and often obtain their care in emergency departments.23,49 Homeless people are admitted to hospital up to 5 times more often than the general population50 and stay in hospital longer than other low-income patients.51 These prolonged stays in hospital result in significant excess health care costs.51 Unfortunately, homeless patients are sometimes discharged to shelters, even when their ability to cope in such a setting is marginal at best. One solution to this problem is the development of respite facilities to provide homeless people with a protected environment for recuperation after a stay in hospital.52
Homeless people face many barriers that impair their access to health care.53 Lack of health insurance is a problem for most homeless people in the United States.53 Although Canada has a system of universal health insurance, many homeless people do not possess proof of coverage because their identification has been lost or stolen.54 In Toronto, 7% of homeless individuals report having been refused health care at least once because they lacked a health insurance card.23 In addition, many homeless people do not fill prescriptions they have received because they do not have insurance benefits and cannot afford the cost of the medication.55
Homeless people face other barriers to health care that are unrelated to insurance status. Homelessness entails a daily struggle for the essentials of life. These competing priorities may impede homeless adults from using health care services, particularly those perceived as discretionary.56 In addition, many health recommendations regarding rest or dietary changes may be unattainable. In Toronto, 72% of homeless people with diabetes report difficulties managing their condition that are usually related to their diet and the logistic challenges of coordinating meals with medications.26
The health care system often fails to provide adequate treatment for homeless people with mental illness or substance abuse.22,57,58 The assertive community treatment (ACT) model is an effort to address this problem. An ACT team of psychiatrists, nurses and social workers follows a small caseload of homeless mentally ill clients, seeking them out in the community to provide high-intensity mental health treatment and case management.59 Compared with usual care, patients receiving ACT have fewer psychiatric inpatient days, more days in community housing and greater improvements in their symptoms.59,60
Conclusion
Homelessness affects a significant number of Canadians of all ages and is associated with a high burden of illness, yet the health care system may not adequately meet the needs of homeless people. More research is needed to identify better ways to deliver care to this population. Health interventions alone, however, are unlikely to overcome the adverse effects of homelessness and related social ills. The search for long-term solutions to the problem of homelessness itself must remain a key priority.
Footnotes
This article has been peer reviewed.
Acknowledgements: Dr. Hwang is the recipient of a Career Scientist Award from the Ontario Ministry of Health. The results and conclusions are those of the author, and no official endorsement by the ministry is intended or should be inferred.
Competing interests: None declared.
Reprint requests to: Dr. Stephen W. Hwang, Shuter Wing 2-026, St. Michael's Hospital, 30 Bond St., Toronto ON M5B 1W8; fax 416 864-5485; hwangs@smh.toronto.on.ca
References
- 1.Begin P, Casavant L, Chenier NM. Homelessness. Ottawa: Library of Parliament, Parliamentary Research Branch, Document PRB 99-1E. Available: www.parl.gc.ca/36/refmat/library/PRBpubs/prb991-e.htm (accessed 2000 Nov 15).
- 2.Jencks C. The Homeless. Cambridge (MA): Harvard University Press; 1994.
- 3.Population of census metropolitan areas. Ottawa: Statistics Canada; 2000. Available: www.statcan.ca/english/Pgdb/People/Population/demo05.htm (accessed 2000 Nov 20).
- 4.Wright JD, Devine JA. Housing dynamics of the homeless: implications for a count. Am J Orthopsychiatry 1995:65:320-9. [DOI] [PubMed]
- 5.Golden A, Currie WH, Greaves E, Latimer EJ. Taking responsibility for homelessness: an action plan for Toronto. Report of the Mayor's Homelessness Action Task Force. Toronto: City of Toronto; 1999. Available: www.city.toronto.on.ca/mayor/homelessnesstf.htm (accessed 2000 Nov 15).
- 6.Prevention of homelessness. Vancouver: City of Vancouver; 1998. Available: www.city.vancouver.bc.ca/commsvcs/housing/sochouse/1council/1998/98-12-17.htm (accessed 2000 Nov 20).
- 7.The Toronto report card on homelessness 2000. Toronto: City of Toronto; 2000. Available: www.city.toronto.on.ca/homelessness/index.htm (accessed 2000 Nov 15).
- 8.Count of homeless persons in downtown Calgary, May 21, 1998. Calgary: City of Calgary, Community and Social Development Department, Social Research Unit. Available: www.gov.calgary.ab.ca/81/research/hless98.pdf (accessed 2000 Nov 15).
- 9.Homelessness in Ottawa-Carleton, April 1999. Ottawa: Region of Ottawa-Carleton. Policy, Planning and Performance Management Services Branch. Available: www.rmoc.on.ca/rmoc/Agendas_and_Minutes/Community_Services/15Apr99 (accessed 2000 Nov 20). (Note: after reaching this site, one must select “Item 6,” which will open HOMELESS2.PDF)
- 10.Shinn M, Weitzman BC, Stojanovic D, Knickman JR, Jimenez L, Duchon L, et al. Predictors of homelessness among families in New York City: from shelter request to housing stability. Am J Public Health 1998;88:1651-7. [DOI] [PMC free article] [PubMed]
- 11.Acorn S. Mental and physical health of homeless persons who use emergency shelters in Vancouver. Hosp Community Psychiatry 1993;44:854-7. [DOI] [PubMed]
- 12.A count of homeless persons in Edmonton. Edmonton: Edmonton Homelessness Count Committee. Available: www.gov.edmonton.ab.ca/comm_services/city_wide_services/housing/homeless_nov99.pdf (accessed 2000 Nov 20).
- 13.Hwang SW. Mortality among men using homeless shelters in Toronto, Ontario. JAMA 2000:283:2152-7. [DOI] [PubMed]
- 14.Mental Health Policy Research Group. Mental illness and pathways into homelessness: proceedings and recommendations. Toronto: Canadian Mental Health Association; 1998.
- 15.Burt MR, Cohen BE. Differences among homeless single women, women with children, and single men. Soc Probl 1989;36:508-24.
- 16.Janus MD, Archambault FX, Brown SW, Welsh LA. Physical abuse in Canadian runaway adolescents. Child Abuse Negl 1995;19:433-47. [DOI] [PubMed]
- 17.Radford JL, King AJC, Warren WK. Street youth and AIDS. Ottawa: Health and Welfare Canada; 1989.
- 18.Roy E, Haley N, Lemire N, Boivin JF, Leclerc P, Vincelette J. Hepatitis B virus infection among street youths in Montreal. CMAJ 1999;161(6):689-93. Available: www.cma.ca/cmaj/vol-161/issue-6/0689.htm [PMC free article] [PubMed]
- 19.Community Social Planning Council of Toronto. Surviving the street: street youth & squeegeeing in Toronto. Toronto: The Council; 1998.
- 20.Population by Aboriginal group, 1996 census, census metropolitan areas. Ottawa: Statistics Canada; 1996. Available: www.statcan.ca/english/Pgdb/People/Population/demo39b.htm (accessed 2000 Nov 15).
- 21.Roy E, Boivin JF, Haley N, Lemire N. Mortality among street youth. Lancet 1998;352:32. [DOI] [PubMed]
- 22.Wood D, editor. Delivering health care to homeless persons. The diagnosis and management of medical and mental healthconditions. New York: Springer Publishing; 1992.
- 23.Crowe C, Hardill K. Nursing research and political change: the street health report. Can Nurse 1993;89:21-4. [PubMed]
- 24.Gelberg L, Linn LS, Mayer-Oakes SA. Differences in health status between older and younger homeless adults. J Am Geriatr Soc 1990;38:1220-9. [DOI] [PubMed]
- 25.Gelberg L, Linn LS. Assessing the physical health of homeless adults. JAMA 1989;262:1973-9. [PubMed]
- 26.Hwang SW, Bugeja AL. Barriers to appropriate diabetes management among homeless people in Toronto. CMAJ 2000;163(2):161-5. Available: www .cma.ca/cmaj/vol-163/issue-2/0161.htm [PMC free article] [PubMed]
- 27.Lee J, Gaetz S, Goettler F. The oral health of Toronto's street youth. J Can Dent Assoc 1994;60:545-8. [PubMed]
- 28.Pizem P, Massicotte P, Vincent JR, Barolet RY. The state of oral and dental health of the homeless and vagrant population of Montreal. J Can Dent Assoc 1994;60:1061-5. [PubMed]
- 29.Moy JA, Sanchez MR. The cutaneous manifestations of violence and poverty. Arch Dermatol 1992;128:829-39. [PubMed]
- 30.Wrenn K. Foot problems in homeless persons. Ann Intern Med 1990;113:567-9. [DOI] [PubMed]
- 31.Wrenn K. Immersion foot. A problem of the homeless in the 1990s. Arch Intern Med 1991;151:785-8. [DOI] [PubMed]
- 32.Prevention and control of tuberculosis among homeless persons. Recommendations of the Advisory Council for the Elimination of Tuberculosis. MMWR 1992;41:13-23. [PubMed]
- 33.Nolan CM, Elarth AM, Barr H, Saeed AM, Risser DR. An outbreak of tuberculosis in a shelter for homeless men. A description of its evolution and control. Am Rev Respir Dis 1991;143:257-61. [DOI] [PubMed]
- 34.Barnes PF, el-Hajj H, Preston-Martin S, Cave MD, Jones BE, Otaya M, et al. Transmission of tuberculosis among the urban homeless. JAMA 1996;275:305-7. [PubMed]
- 35.Yuan L, Simor AE, Louie L, Pollock S, Gould R, Jamieson F. Tuberculosis clusters among the homeless in Toronto, Canada. 37th Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC); 1997 Sept 28-Oct 1; Toronto.
- 36.Pablos-Mendez A, Knirsch CA, Barr RG, Lerner BH, Frieden TR. Nonadherence in tuberculosis treatment: predictors and consequences in New York City. Am J Med 1997;102:164-70. [DOI] [PubMed]
- 37.Weis SE, Slocum PC, Blais FX, King B, Nunn M, Matney GB, et al. The effect of directly observed therapy on the rates of drug resistance and relapse in tuberculosis. N Engl J Med 1994;330:1179-84. [DOI] [PubMed]
- 38.Schluger N, Ciotoli C, Cohen D, Johnson H, Rom WN. Comprehensive tuberculosis control for patients at high risk for noncompliance. Am J Respir Crit Care Med 1995;151:1486-90. [DOI] [PubMed]
- 39.Nazar-Stewart V, Nolan CM. Results of a directly observed intermittent isoniazid preventive therapy program in a shelter for homeless men. Am Rev Respir Dis 1992;146:57-60. [DOI] [PubMed]
- 40.MacDonald NE, Fisher WA, Wells GA, Doherty JA, Bowie WR. Canadian street youth: correlates of sexual risk-taking activity. Pediatr Infect Dis J 1994; 13:690-7. [PubMed]
- 41.Manzon L, Rosario M, Rekart ML. HIV seroprevalence among street involved Canadians in Vancouver. AIDS Educ Prev 1992;Fall(Suppl):86-9. [PubMed]
- 42.Wang EE, King S, Goldberg E, Bock B, Milner R, Read S. Hepatitis B and human immunodeficiency virus infection in street youths in Toronto, Canada. Pediatr Infect Dis J 1991;10:130-3. [DOI] [PubMed]
- 43.Greene JM, Ringwalt CL. Pregnancy among three national samples of runaway and homeless youth. J Adolesc Health 1998;23:370-7. [DOI] [PubMed]
- 44.Tanaka M, Tokudome S. Accidental hypothermia and death from cold in urban areas. Int J Biometeorol 1991;34:242-6. [DOI] [PubMed]
- 45.Fischer PJ, Breakey WR. The epidemiology of alcohol, drug, and mental disorders among homeless persons. Am Psychol 1991;46:1115-28. [DOI] [PubMed]
- 46.Lehman AF, Cordray DS. Prevalence of alcohol, drug, and mental disorders among the homeless. Contemp Drug Probl 1993;20:355-83.
- 47.Smart RG, Adlaf EM. Substance use and problems among Toronto street youth. Br J Addict 1991;86:999-1010. [DOI] [PubMed]
- 48.Padgett D, Struening EL, Andrews H. Factors affecting the use of medical, mental health, alcohol, and drug treatment services by homeless adults. Med Care 1990;28:805-21. [DOI] [PubMed]
- 49.Padgett DK, Struening EL, Andrews H, Pittman J. Predictors of emergency room use by homeless adults in New York City: the influence of predisposing, enabling and need factors. Soc Sci Med 1995;41:547-56. [DOI] [PubMed]
- 50.Martell JV, Seitz RS, Harada JK, Kobayashi J, Sasaki VK, Wong C. Hospitalization in an urban homeless population: the Honolulu Urban Homeless Project. Ann Intern Med 1992;116:299-303. [DOI] [PubMed]
- 51.Salit SA, Kuhn EM, Hartz AJ, Vu JM, Mosso AL. Hospitalization costs associated with homelessness in New York City. N Engl J Med 1998;338:1734-40. [DOI] [PubMed]
- 52.Goetcheus J, Gleason MA, Sarson D, Bennett T, Wolfe PB. Convalescence: for those without a home — developing respite services in protected environments. In: Brickner PW, Scharer LK, Conanan BA, Savarese M, Scanlan BC, editors. Under the safety net. The health and social welfare of the homeless in the United States. New York: WW Norton & Co.; 1990. p. 169-83.
- 53.Stark LR. Barriers to health care for homeless people. In: Jahiel RI, editor. Homelessness: a prevention-oriented approach. Baltimore: Johns Hopkins University Press; 1992. p. 151-64.
- 54.Hwang SW, Windrim PM, Svoboda TJ, Sullivan WF. Physician payment for the care of homeless perople. CMAJ 2000;163(2):170-1. Available: www .cma.ca/cmaj/vol-163/issue-2/0170.htm [PMC free article] [PubMed]
- 55.Hwang SW, Gottlieb JL. Drug access among homeless men in Toronto. CMAJ 1999;160(7):1021. Available: www.cma.ca/cmaj/vol-160/issue-7/1021.htm [PMC free article] [PubMed]
- 56.Gelberg L, Gallagher TC, Andersen RM, Koegel P. Competing priorities as a barrier to medical care among homeless adults in Los Angeles. Am J Public Health 1997;87:217-20. [DOI] [PMC free article] [PubMed]
- 57.Lamb HR, Bachrach LL, Kass FI. Treating the homeless mentally ill. A report of the Task Force on the Homeless Mentally Ill. Washington: American Psychiatric Association; 1992.
- 58.Bhugra D. Homelessness and mental health. New York: Cambridge University Press; 1996.
- 59.Lehman AF, Dixon LB, Kernan E, DeForge BR, Postrado LT. A randomized trial of assertive community treatment for homeless persons with severe mental illness. Arch Gen Psychiatry 1997;54:1038-43. [DOI] [PubMed]
- 60.Wasylenki DA, Goering PN, Lemire D, Lindsey S, Lancee W. The hostel outreach program: assertive case management for homeless mentally ill persons. Hosp Community Psychiatry 1993;44:848-53. [DOI] [PubMed]