

Abstract
The role of accommodation in myopia development and progression has been debated for decades. More recently, the understanding of the mechanisms involved in accommodation and the consequent alterations in ocular parameters has expanded. This International Myopia Institute white paper reviews the variations in ocular parameters that occur with accommodation and the mechanisms involved in accommodation and myopia development and progression. Convergence is synergistically linked with accommodation and the impact of this on myopia has also been critiqued. Specific topics reviewed included accommodation and myopia, role of spatial frequency, and contrast of the task of objects in the near environment, color cues to accommodation, lag of accommodation, accommodative-convergence ratio, and near phoria status. Aspects of retinal blur from the lag of accommodation, the impact of spatial frequency at near and a short working distance may all be implicated in myopia development and progression. The response of the ciliary body and its links with changes in the choroid remain to be explored. Further research is critical to understanding the factors underlying accommodative and binocular mechanisms for myopia development and its progression and to guide recommendations for targeted interventions to slow myopia progression.
Keywords: accommodation, binocular vision, myopia development, myopia progression, emmetropization
The association between sustained near work demanding high levels of ocular accommodation and the development of myopia has been well documented.1 Epidemiologic studies have also shown a correlation between the amount of near work and the onset and progression of myopia.2–4 Consequently, increased accommodative effort required during near work has been proposed as a causative factor in the development of myopia. However, the relationship between accommodative demand and myopia is complex. Due to the synergistic response of the vergence system, the status of binocular vision at near work also varies with accommodation, yet the impact of heterophoria at near work on myopia onset and progression is not fully understood. This article provides a comprehensive review of the research evidence on the influence of accommodation and binocular vision in myopia development and progression; it also translates the current evidence and main findings to clinical practice.
Variations in Ocular Structure During Accommodation
Owing to the purported links between accommodative dysfunction and myopia, investigations of structural and functional differences in the accommodative apparatus and associated ocular elements are of particular interest. One of the broader academic and clinical motivations driving such endeavors is the opportunity to elucidate structural variations or trends that may be predictive of specific patterns of myopia progression, for example, in identifying those at particular risk of the onset of myopia, high myopia, or rapid progression of myopia.
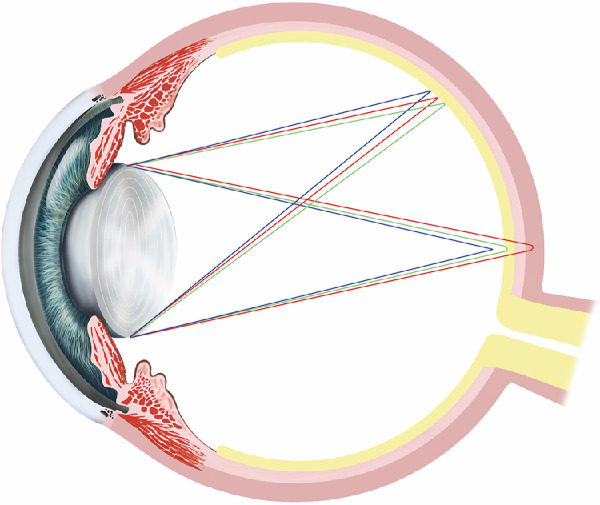
To facilitate the understanding of how and why the structure of a myopic eye may affect accommodative behavior, the following section presents a brief review of the mechanism of human accommodation. Although the literature stands equivocal concerning the exact mechanism, it does largely acquiesce to a Helmholtzian model of accommodation (1855). In this model, the ciliary muscle (a smooth muscle ring) is in a relaxed state while viewing an object at optical infinity. As the apex of the ciliary muscle has a relatively large diameter in this state of relaxation, the anterior zonular fibers from which the crystalline lens is suspended are maintained under tension due to strain from the posterior pars plana fibers. Consequently, the stretched anterior zonules exert strong radial forces on the capsule and flatten the crystalline lens. When the eye shifts focus to a near target, the ciliary muscle contracts, moving its mass anteriorly and centripetally and releasing tension on the zonules. Helmholtz proposed that this structural change occurs because the capsule and the lens matrix are inherently elastic; when freed from the zonular pull, the lens, with the aid of its capsule, can assume an axially thicker5–16 and rounder shape, with a reduced diameter.17–22 Refractive change during accommodation is primarily attributable to an increase in anterior surface curvature of the crystalline lens surface5,23,24 and a simultaneous smaller increase in posterior surface curvature.6,25,26 These dimensional changes result in a reduction in anterior chamber depth, yet overall an increase in anterior segment length (distance from the cornea to the posterior surface of the lens).10,12,27 Once accommodation ceases (Fig. 1), the ciliary muscle is thought to return to its relaxed position as a result of elastic recoil imparted by the choroid.28
Figure 1.

Differences in anterior eye structure in the relaxed (unaccommodated) and accommodated eye. Copyright © 2021 by IMI.
Despite the advent of high-resolution and dynamic ocular imaging systems allowing visualization of many previously unknown anatomic subtleties, the iris still prevents imaging of the key accommodative structures. These limitations also apply to studies attempting to determine whether accommodative mechanics differ as a function of ametropia. Consequently, at present, several models exist, with varying levels of evidence regarding accommodation induced structural changes that may be instrumental in myopia onset and progression.
It is well documented from biometric studies that increased vitreous chamber depth is the primary structural change in the majority of cases of myopia,29 and that myopic eyes are generally globally larger and longer than emmetropic eyes.30,31 The literature also reports other differences in ocular structure as a function of ametropia, including corneal curvature32–35 anterior chamber depth,36 crystalline lens thickness,37–39 choroidal thickness,40 and scleral rigidity.41,42 The anatomic complexities of each of these structures in relation to accommodation and refractive error give rise to potential corollaries for accommodative performance and myopia progression.
The first consideration is the nature of global eye size in terms of the optics of the eye and the implications for accommodative performance. Davies and colleagues43 explained using ray tracing that axially myopic and axially hyperopic eyes show different vergence contributions for light rays entering the anterior segment. They attributed this optical behavior to a consequence of “natural damping” associated with negative vergence and axial length changes. The spectacle corrected myope also has to accommodate and converge less for a near target than an emmetrope does due to the prismatic effect of the lenses.44 Therefore, accommodative response for a similar demand will be slightly greater in a longer (myopic) eye compared to a shorter (hyperopic) eye due to differences in eye size.
Changes in the Anterior Segment in Relation to Accommodation and Myopia
Pupil Size
Given the evidence that axial growth is influenced by visual experience inclusive of retinal image quality and optical defocus45–48 and data suggesting that myopes display unusually high levels of aberration and/or larger accommodative lags relative to those who remain emmetropic,49–59 the role of the pupil in myopigenesis is unclear. As the pupil acts as an aperture stop, theoretically, inter- and intra-individual pupil size variations present a potential innate and dynamic physiological mechanism whereby optical image properties, including retinal image blur, higher-order aberrations, depth of focus, and accommodative lag, could differ between myopes and nonmyopes or fluctuate in a myopigenic fashion over time contributing to progression in susceptible individuals.60 Generally, larger pupil diameters lead to greater wave-front aberrational blur,61 whereas during accommodation, the blurring effect of a given dioptric lag would be proportionally greater due to the larger retinal blur circle diameter.60
Nonetheless, most human studies have failed to find significant differences in unaccommodated pupil diameter between age-matched emmetropic and myopic groups.60,62–65 A few studies have reported a weakly associated increase in pupil diameter in myopes, but these studies have important design limitations, including differences in target distance66 or age67 between groups. Further, anecdotal evidence supporting a lack of correlation can be drawn from numerous studies that report isocoria in anisometropes, which is counter to expectation should more myopic eyes have systematically larger pupils.60,68 Differences in pupil size or response during steady-state accommodation or the notion of systematically higher levels of retinal image blur in myopes with larger pupils are also unsupported by in vivo data.60,65
It would therefore seem plausible that pupillary characteristics in accommodated and unaccommodated eyes are independent of ametropia and the notion that pupil-related factors play a role in myopia genesis is currently unsubstantiated. It should, however, be noted that the aforementioned studies show considerable variations among individuals, generally examine adult populations, and do not differentiate between progressive and stable myopia. It has been suggested that different trends may be evident in more homogenized refractive error or age groups, particularly pediatric populations.60
Ciliary Muscle
As ciliary muscle contraction is a prerequisite to accommodation,69 interest in morphological differences in ciliary muscle anatomy has increased70 in the context of how they may contribute to the association between nearwork and myopia. In the unaccommodated state, myopic children71–74 and adults75–79 have been shown to have thicker ciliary muscles in the posterior-most aspect, typically 2 to 3 mm behind the scleral spur,70,71,73–76,78 with thickness correlating positively with increasing axial length. Meanwhile, some studies have also reported a thinner anterior portion of the ciliary muscle in axially longer eyes.73,79,80 In hypermetropic children, the ciliary muscle shows its maximum thickness anteriorly, approximately 1 mm from the scleral spur.73 Interocular differences have been reported in anisometropia, with significantly thicker muscles observed in eyes that have unilateral high myopia compared with the fellow eye.76 Furthermore, region-specific differences in thickness have also been reported, with the longitudinal fiber portion being thicker and the apical fiber region being thinner in the more myopic eye.79 Nonetheless, Sheppard and Davies81 found a positive correlation between axial length and ciliary muscle length, but not between axial length and ciliary muscle thickness when considered as distances from the scleral spur as a percentage of the total length of the ciliary muscle.
Studies examining general ciliary muscle morphology under various accommodative demands,77,81–85 have suggested a linear relationship between ciliary muscle thickness and accommodative response,74,82,86 showing that the muscle thickens anteriorly and thins posteriorly with increasing accommodative effort.74,81,82 Sheppard and Davies81 and Lewis et al.74 examined accommodation-induced morphological changes between refractive groups and found no dependence of the ciliary muscle accommodative response on axial length or ciliary muscle baseline thickness. Interestingly, Jeon et al.77 reported reduced movement of the ciliary muscle during accommodation in individuals with increased axial length and ciliary muscle thickness. However, as accommodation responses were not assessed, it remains unclear whether there was a smaller relative change in crystalline lens thickness per unit of accommodative response for eyes with longer axial lengths,43 or whether there were functional consequences (e.g. increased lag).
Although it is clear that differences in ciliary muscle anatomy between myopes and nonmyopes exist, if or how this would translate into a myopigenic effect remains undetermined. Only minor differences in accommodative behavior (optical coherence tomography [OCT] assessed microfluctuations of accommodation, velocity of accommodation and disaccommodation, and lag of accommodation) occur between emmetropes and myopes despite the morphological differences between them,86 suggesting that ciliary muscle size may not be a contributing or critical factor in myopia development. Nonetheless, other models have been proposed.
One early suggestion is that the ciliary muscle tonus could in turn affect choroidal tension, resulting in axial length change (see later section regarding transient axial elongation).87 Alternatively, a thicker ciliary muscle might prevent the equatorial stretch, which can occur with myopia and thus maintain emmetropia, thereby being a factor in myopigenesis.88 However, a myopic shift in refraction has been found not to be associated with a change in ciliary muscle thickness over time in children.89 A hypertrophic ciliary muscle could theoretically lead to myopia development, perhaps due to poor contractibility resulting in accommodative inaccuracies and chronic retinal hyperopic defocus under nearwork conditions. Seemingly, the evidence that children and adults with myopia have higher accommodative lags than emmetropes, and that higher lags of accommodation are associated with faster myopia progression support this.50,55,57,90 However, most studies concede that high accommodative lag is more likely to represent a consequence, rather than a stimulus for myopia,91–93 and the relatively thinner anterior muscle in myopes has been suggested to be indicative that the increase in myopic ciliary muscle length may occur as a result of the muscle mass relocating to a more posterior position due to axial elongation, rather than the ciliary muscle undergoing related growth-related hypertrophy.81
Crystalline Lens
Structural changes in the crystalline lens are central to myopia development. Crystalline lens power reduces markedly during infancy,94 with substantial inhibition of lens thinning and flattening evident 1 year before or within a year of myopia onset in children.95 This phenomenon is concomitant with a reduction in both the refractive index and the dioptric power of the crystalline lens.95 These findings support the notion that early onset myopia results from a breakdown in the independent relationship between lens changes and axial elongation.95 Interestingly, it has been shown that there is a tendency for the crystalline lens to be thinner in myopic eyes than emmetropic eyes,37–39 despite the apparent breakdown in co-ordination between lens thinning and axial growth. However, due to difficulties obtaining in vivo data of the crystalline lens’ parameters as it accommodates, little is known about whether there are relevant functional implications of crystalline lens size or anatomic features, such as refractive index and rigidity, and whether these parameters differ between refractive groups.
Changes in the Posterior Segment in Relation to Accommodation and Myopia
Ostensibly, performance variation in the accommodative apparatus represents the most obvious anatomic candidate capable of precipitating myopia; yet, structural changes within the posterior segment during accommodation are emerging as being more likely to promote a myopic shift in susceptible eyes.
Various experimental paradigms using partial coherence interferometry96–98 and optical low coherence reflectometry99–102 have shown that the eye experiences a transient period of axial elongation after brief periods of sustained accommodation, both on axis96–100,102 and in the periphery,101 with the magnitude of change increasing with larger accommodative demand.99 The exact mechanics by which the accommodative process instigates this phenomenon remains unclear; however, it is a long-held belief that the accommodating ciliary muscle applies an internal mechanical force upon the globe.87,103 One such proposal is that posterior pole elongation occurs to maintain ocular volume despite the decreases in scleral and choroidal equatorial circumference, which arises owing to the increasing force exerted on the equatorial choroid by the contraction of the ciliary smooth muscle.96,97 Although data to explicitly evidence a mechanical force model are scarce, Croft and colleagues104 have reported centripetal movement of both the equatorial choroid and retina in rhesus monkeys during Edinger-Westphal stimulated accommodation, seemingly fitting this hypothesis.
The discovery of accommodation driven fluctuations in ocular length has given rise to the hypothesis that eyes which experience a greater magnitude of transient axial elongation may be more susceptible to permanent myopic shift.97 Indeed, this notion seemingly dovetails with the suspicion that ocular rigidity differences may make an axially myopic eye more pliant to transient elongation.97 There is now considerable evidence that myopic eyes demonstrate reduced posterior choroidal,105 scleral,106–109 and overall equatorial ocular wall41,110 thickness compared with emmetropic eyes. Nonetheless, it remains unclear whether an association exists between in vivo anterior ocular rigidity and myopia susceptibility or progression,41,42,111 particularly in light of the data derived from differential Schiotz tonometry, which suggests emmetropic and myopic adults112 and children41 have similar ocular rigidity and ocular wall stress.
To date, research comparing the magnitude of accommodation-induced transient axial elongation between emmetropic and myopic adults has produced contradictory findings, although it must be noted that studies have varied in design, type of accommodative stimulus, age range of participants, and refractive error. Mallen and colleagues97 reported the largest disparity with a mean elongation of 0.037 mm in emmetropes versus 0.058 mm in myopes for a 6.0 D accommodative stimulus. Although it has since been suggested that these values present an overestimation due to artefactual instrument optical path length errors,113 corrected values of 0.026 and 0.047 mm, respectively, are still in excess of those found by other studies.101 Other researchers have reported either no significant group difference,99,100,102 increased elongation in emmetropes,96 or only a very small, but significantly greater, transient axial elongation in myopes.99
Nonetheless, data suggesting no differences in the physical extent of relative elongation with ametropia do not necessarily rule out a potential role for transient axial elongation in accommodation-related myopia genesis,99 as this does not account for variations in duration or intensity of nearwork activities114 or other related features, which may even be responsible in isolation. All aforementioned studies are limited to providing a snapshot of biometric change during relatively short-duration accommodation tasks. The influence of longer periods of accommodation on transient axial elongation, and its ability and time period of recovery from these findings remain unknown.99
Although the mechanical model for transient axial elongation involves the choroid in an intermediary force transmission role, recent data indicate that its contribution may be substantially greater.40 Certainly, in spatial terms, choroidal thinning during accommodation accounts for a significant degree of total elongation.100,115,116 Woodman et al.100 examined the subfoveal choroidal thickness change during a sustained 4.0 D accommodation task and reported a −8 µm choroidal thinning and approximately 20 µm axial elongation in a cohort of myopic and emmetropic participants. Subsequent OCT studies with higher accommodative stimuli have produced consistent findings,115,116 and uncovered regional variations, with choroidal thinning being most prominent in temporal, inferior, and infero-temporal parafoveal zones (Fig. 2).115 Choroidal thinning under transient axial elongation is likely to represent an element of feedback response of the choroid resulting from the accommodation, rather than purely a mechanical consequence of ciliary muscle contraction. The potential role of the choroid in the regulation of eye growth is currently under much scrutiny as changes in choroidal thickness are known to accompany eye growth, be more marked in highly myopic eyes and be bidirectional, with myopigenic factors leading to choroidal thinning and myopia-protective factors leading to causing choroidal expansion.40 In the case of accommodation, choroidal thinning may be a compensatory mechanism to maintain a stable, optimally focused retinal image.40,117
Figure 2.
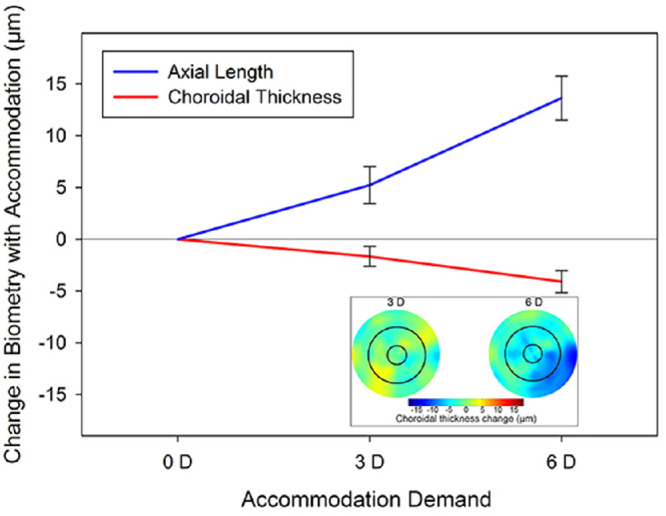
The changes in axial length (top, blue line) and choroidal thickness (bottom, red line) occurring during a short duration 3.0 D and 6.0 D accommodation task. Note the significant eye elongation and choroidal thinning that occurs at the higher accommodation demand. Inset illustrates the topographical choroidal thickness changes in the macular region occurring with 3.0 D and 6.0 D of accommodation (note that cool colors indicate a choroidal thinning with accommodation). From Woodman-Pieterse et al.115
How differences in choroidal thickness during accommodation may contribute to myopia development in the longer term is undetermined, and more work is needed to elucidate variations in response and recovery in myopes and emmetropes. Similarly, how changes in choroidal dynamics and position interact with other optical features of the myopic or pre-myopic eye, such as increased negative spherical aberration or accommodative lag, cannot be discounted as contributing factors to the development of myopia.40
Anterior Sclera
The semirigid scleral cup is the principal determinant of eye size and shape. During the development of myopia, the sclera undergoes a long-term, permanent remodeling process, whereby the structural and biomechanical properties of the sclera alter, making the globe more susceptible to expansion.106,118 Changes in eye shape occur globally in all three dimensions (horizontal, vertical, and axial), although the magnitude of changes may vary with dimensions. It has been shown in humans that, compared with the emmetropic eyes, the eyes with myopia are elongated in both equatorial and axial dimensions, although the globe is elongated more in the axial dimension, resulting in a more prolate shape of the eye.119 Significant negative correlations have also been reported between anterior scleral thickness near the scleral spur and increasing levels of myopia and axial length,120 consistent with the negative correlation between posterior sclera thickness and axial length.121 The scleral changes in myopia may thus occur well beyond the posterior pole and extend to the equatorial region or beyond.
The time courses of the accommodative system and scleral modeling vary substantially: accommodation has a much more rapid time course compared with scleral biomechanical changes in myopia.122 The close juxtaposition of the accommodation apparatus, including the ciliary body, with the anterior sclera makes it plausible that accommodation could affect the anterior scleral properties. Recent studies have provided some evidence that the scleral shape undergoes short-term changes with accommodation. Woodman-Pieterse et al. measured changes in the anterior temporal sclera (1, 2, and 3 mm posterior to the scleral spur) in adult myopes and emmetropes using high-resolution anterior OCT, whereas the subjects fixated monocularly at near accommodative stimuli of 0.0, 3.0, and 6.0 D through a custom-mounted Badal optometer.123 It was shown that the 6.0 D accommodative stimulus induced significant thinning of the anterior sclera, with more prominent changes in the myopic eyes at 3 mm posterior to the scleral spur for both accommodative stimuli. Niyazmand et al. reported changes in the shape of the anterior sclera in the horizontal meridian using eye surface profilometry in myopic and emmetropic young adults under conditions of 5.0 D accommodative demand, 9 degrees simulated convergence demand, and their combination.124 Although changes were primarily evident at the naso-scleral region, all three conditions produced a significant reduction in the sagittal height of the anterior sclera (i.e. a reduction in elevation of the anterior sclera), whereas accommodation also produced a significant flattening of the anterior eye surface, but only when coupled with simulated convergence. These findings suggest that the anterior sclera perhaps thins and moves forward in response to accommodation. However, the reported changes could be due to convergent eye movement associated with accommodation or medial rectus contraction rather than an optically driven scleral response.125
Mechanisms of How Accommodation Interrupts Emmetropization in Humans
Whereas emmetropization is the long-term response of the eye in reducing or eliminating the defocus perceived at the fovea, accommodation is the immediate response of the eye to eliminate or reduce the hyperopic defocus presented during near work. The accuracy of accommodation has long been linked to the accuracy of refractive error development. Larger lags associated with high accommodative demand produce hyperopic defocus at the fovea providing a stimulus for the eye to grow longer and become myopic.52,126 Previous studies have shown that myopic children accommodate less than emmetropic children.50,57,91,127–130 The higher lags are shown to persist in some studies even when a near addition is given to the myopic children, as they use the add power and underaccommodate.131 Several mechanisms have been proposed for how accommodation could cause myopia development in humans.
Accommodative Lag and Foveal Vision
Axial form deprivation due to the diffuse blur from high levels of accommodative lag and hyperopic defocus in the central retina could lead to the development or progression of myopia, as evidenced in animal experiments.52,132,133 To date, longitudinal studies comparing the magnitude of initial accommodative lag with subsequent myopia progression have come to conflicting conclusions.59,134 Accommodative lags of over 1.0 D are common during near vision in both emmetropes and myopes. These errors in accommodation are summarized for children in Table 1 and for young adults in Table 2. A lag of accommodation does not necessarily mean that the visual quality is poor during near vision. The need for accommodation will dependent on the range of clear focus which is influenced by monofocal and chromatic aberrations, pupil size,135 and neural factors.136 For a constant pupil diameter, differences in ocular aberrations between myopes and emmetropes are observed and are variable in both accommodative and nonaccommodative states.137,138 Attempts to slow myopia progression using interventions targeted at improving accommodative lag, such as progressive lens wear groups (PALs) have been largely unsuccessful, even when including children with high lags of accommodation and near esophoria.139–141 Cheng et al.141 additionally used base in prism along with progressive addition lenses to offset the positive-lens-induced exophoria and found no difference in myopia control efficacy in children with high lags of accommodation, however, the small gain in efficacy may be related to improved accommodation-convergence balance. The accommodative lag hypothesis in myopia thus remains contentious and warrants further investigation.
Table 1.
Effect of Refractive Error and Measurement Methods on Accommodation Errors at Near Vision in Children
| Paper | Measurement Method | Accommodation Stimuli | Mode of Myopic Correction | Age, y | Refractive Groups | AE, D | Summary of Results |
|---|---|---|---|---|---|---|---|
| Rouse et al. (1984)128 | MEM dynamic retinoscopy | Monocular FV usual near demand | Habitual spectacle correction | 5–11 | Not specified | −0.30 | Relationship between age and lag |
| Gwiazda et al. (1993)50 | Canon R–1 Autoref | Monocular FV/NL/PL 0–4 D demand | Soft contact lenses | 5–17 | EMMs MYPs EMMs MYPs | −0.30 FV −0.66 FV −0.56 NL −1.61 NL |
MYPs had greater lags than EMMs. Lags were greater for NL |
| Chen and O'Leary (2002)287 | Canon R–1 Autoref | Monocular FV/NL 0–4 D demand | N/A | 3–14 | EMMs | −0.29 FV −0.69 NL |
Lags greater for NL |
| McClelland et al. (2004)127 | Nott Dynamic Retinoscopy | Monocular FV 4–10 D demand | Habitual correction | 4–15 | Not specified | −0.30 at 4 D −2.50 at 10 D |
Lags increased as the demand increased |
| Mutti et al. (2006)91 | Grand Seiko WR5001K or Canon R–1 Autoref | BLV/FV 2 D and 4 D demand | Habitual spectacle correction | 6–15 | EMMs EMMs MYPs MYPs | −1.00 FV −0.91 BLV −1.12 FV −1.40 BLV |
Increased lags found in MYPs after they became myopic but not in EMMs who became MYPs |
| Langaas et al. (2008)143 | Plus Optix Power Refractor 11 | Binocular FV 0.25–4 D demand | Spectacle correction | Ave 13 14 | EMMs EOMs | −0.10 –0.10 | Lags were greater at the 2 D than the 4 D viewing condition |
| Weizhong et al. (2008)134 | Shin-Nippon Autoref | Monocular FV 3 D demand | Spectacle correction | Ave 11 | EOMs | −0.76 | No relationship between accommodation lag and myopia progression over 1 y |
| COMET 2 (2011)140 | Grand Seiko WR5001K | Monocular FV 3 D demand | Spectacle correction | 8–12 | MYPs SVL MYPs PAL | −1.40 −1.47 | Both myopic groups of children exhibited larger accommodative lags. The treatment effect of the PALs was greater in children with lags greater than −1.5 D. |
| Berntsen et al. (2011)139 | Grand Seiko WR5001K or Canon R–1 Autoref | BLV/FV 4 D demand | Spectacle correction | 6–14 | MYPs SVL | −1.59 | Myopic children had high lags of accommodation, but the magnitude of the lag was not related to the annual myopia progression |
| Yeo et al. (2013)218 | Shin-Nippon Autoref | Binocular FV 3 and 4 D demand | Spectacle correction | 7–12 | EMMs MYPs | −0.96 −1.01 | Chinese children had high lags of accommodation when reading either English or Chinese texts |
| Han et al. (2018)288 | Fused cross cyl | Binocular, Phoropter 4 D demand | Spectacle correction | 9–14 | MYPs SVL | −1.0 | Orthokeratology and concentric progressive lenses reduced the lag of accommodation |
| Ma et al. (2019)289 | Shin-Nippon Autoref | Monocular FV 3 D demand | Spectacle correction | 8–12 | MYPs SVL | −1.0 | Myopic children with high lags showed reduction in lag both with in office placebo therapy and accommodation vergence training |
| Chen et al. (2019)130 | Grand Seiko WR5001K | Monocular FV 4 D demand | Spectacle correction | 8–12 | EMMs MYPs SVL | −0.20 −0.65 | Myopic children had greater lags. Lags increased in mesopic lighting conditions |
AE, accommodative error at highest demand conditions; BLV, Badal lens viewing; EMMs, emmetropes; EOMs, early onset myopes; FV, free viewing; HS, Hartmann Shack; lag, accommodation lag; MYPs, myopes; N/A, not applicable; NL, negative lens series; PAL, progressive lens wear group; PL, positive lens series; SVL, single vision lens wear group; VA, visual acuity.
Table 2.
Effect of Refractive Error and Measurement Methods on Accommodation Errors at Near Work in Young Adults
| Paper | Measurement Method | Accommodation Stimuli | Mode of Myopic Correction | Age, y | Refractive Groups | AE (D) | AEI | ASRC | Summary of Results |
|---|---|---|---|---|---|---|---|---|---|
| McBrien and Millodot, (1986)49 | Canon R-1 Autoref | Binocular free viewing (FV) 0–5 D demand | Soft contact lenses | 18–23 | EMMs | −0.54 | EOMs and LOMs had greater lags than EMMs | ||
| EOMs | −0.69 | ||||||||
| LOMs | −0.83 | ||||||||
| Bullimore et al. (1992)290 | Canon R-1 Autoref | Monocular FV/NL/PL 1–5 D demand | Soft contact lenses | 19–23 | EMMs | −0.60 | LOMs had greater lags for passive tasks at high demands | ||
| LOMs | −0.73 | ||||||||
| Abbott et al. (1998)57 | Canon R–1 Autoref | Monocular FV/NL/PL 0–4 D demand | Soft contact lenses | 18–31 | EMMs | 0.01 NL | Progressing MYPs had greater lags for NL conditions only | ||
| SMs PMs | 0.01 NL −0.52 NL | ||||||||
| Jiang and Morse (1999)291 | Canon R-1 Autoref | Monocular Badal lens viewing BLV up to 5 D demand | Soft contact lenses or spectacles | 20–30 | EMMs | 0.74 | All 3 refractive groups had similar lags | ||
| SMs | 0.77 | ||||||||
| PMs | 0.67 | ||||||||
| Rosenfield et al. (2002)292 | Canon R–1 Autoref | Binocular FV 0–5 D demand | Soft contact lenses | 21–27 | EMMs | −0.34 FV | 0.99 | Greater lags found in stable MYPs than initial EMMs and MYPs that progressed over a 1 y period | |
| SMs | −0.34 FV | 0.96 | |||||||
| PMs | –0.20 FV | ||||||||
| Subbaram and Bullimore (2002)65 | Canon R–1 Autoref | Monocular BLV 0–4 D demand | Spectacles | 20–30 | EMMs | −0.29 | Small lags found in both refractive groups | ||
| PMs | −0.29 | ||||||||
| Seidel et al. (2003)293 | Canon R-1 Autoref | Monocular BLV 0–4.5 D demand | Soft contact lenses | 17–26 | EMMs | 0.81 | All 3 groups had similar lags but greater response variability in the myopic groups | ||
| LOMs | 0.81 | ||||||||
| EOMs | 0.80 | ||||||||
| Hazel et al. (2003)294 | Shin-Nippon Autoref SRW 5000 Wavefront Sensor (HS) | Monocular NL 0–4 D demand | Soft contact lenses | 18–27 | EMMs | −0.72 | Lags greater when measured with the autorefractor when adjusted for similar pupil size | ||
| MYPs | −1.01 | ||||||||
| EMMs | −0.50 HS | ||||||||
| MYPs | −0.43 HS | ||||||||
| Nakatsuka et al. (2003)54 | Open field autorefractor | Monocular FV 2-6.25 D demand | Habitual spectacle correction | 19–38 | EMMs | 1.02 | Good accommodative accuracy in both refractive groups | ||
| EOMs | 1.05 | ||||||||
| Schmid et al. (2005)295 | Shin-Nippon Autoref SRW 5000 | Monocular BLV 4 D demand | Soft contact lenses | 18–25 | EMMs | 0.29 | EMMs and MYPs had similar lags, response more accurate for smaller targets at the same distance | ||
| MYPs | 0.33 | ||||||||
| Day et al. (2006)296 | Shin-Nippon Autoref SRW 5000 | Monocular BLV 0–4 D demand | Soft contact lenses | Ave 22 | EMMs | 0.73 | EMMs and LOMs had greater lags than the EOMs | ||
| Ave 22 | EOMs | 0.86 | |||||||
| Ave 28 | LOMs | 0.70 | |||||||
| Allen and O'Leary (2006)59 | Power refractor | Monocular and Binocular FV 3 D demand | Habitual correction | 18–25 | EMMs | 0.35 | Increased binocular lags with increasing degree of myopia | ||
| EOMs | 0.41 | ||||||||
| LOMs | |||||||||
| Harb et al. (2006)162 | Power refractor | FV 3.5 D demand | Soft contact lenses | 22–28 | EMMs | −0.99 | Myopes had greater variability in their accommodation response and had larger lags at greater reading distances | ||
| MYPs | −0.99 | ||||||||
| Sreenivasan et al. (2013)297 | COAS Aberrometer | Monocular plus 3 Binocular tasks 1-5 D demand | Spectacle correction equivalent | 18–25 | EMMs | −0.70 | MYPs showed greater lags but had better near VA than EMMs | ||
| MYPs | −1.20 |
AE, accommodative error at highest demand conditions; AEI, accommodation error index; ASRC, slope of the accommodation stimulus response curve; BLV, Badal Lens Viewing; EMMs, emmetropes; EOMs, early onset myopes; FV, free viewing; HS, Hartmann Shack; lag, accommodation lag; LOMs, late onset myopes; MYPs, myopes; NL, negative lens series; PAL, progressive lens wear group; PL, positive lens series; PMs, progressing myopes; SMs, stable myopes; SVL, single vision lens wear group; VA, visual acuity.
Accommodative Instability
Besides inaccuracies in accommodation, it seems that accommodative instability (as assessed by objective dynamic accommodation recordings to different dioptric targets) may be important in myopia development as both children142,143 and adults144 with myopes showing less stable accommodation responses. Unstable accommodation responses would prevent the formation of a steady clear retinal image, with possible consequences for myopia development and progression.
Near Induced Transient Myopia
Another important characteristic of the accommodation response is that, after prolonged exposure to a near stimulus, there is normally a delay in accommodation relaxation when the person looks far away, termed “near work induced transient myopia.” Retinal defocus induced by near work induced transient myopia is larger and persists for longer in late-onset145 and progressing146,147 adult myopes and children in whom it lasts longer,148 indicating a possible contributing factor to permanent myopia.149 Interestingly, near work induced transient myopia is also increased in the more myopic eye compared with the fellow less myopic eye of anisomyopes.150
Near-Peripheral Vision and Accommodation
Relative peripheral refraction, measured as the difference between foveal and peripheral refractive error, is known to have a significant influence on myopia development and control.151,152 Myopes tend to have hyperopic relative peripheral refraction, whereas hyperopes have a myopic relative peripheral refraction.132,152 Changes in the shape of the eye with accommodation and accommodative lag could further influence the peripheral refractive error and also aberration changes with accommodation may effect off-axis refractive errors during accommodation. Myopes are likely to have larger ciliary muscle mass,78,153–155 therefore accommodation could lead to an expansion in the dimensions of the myopic eye due to the force created by the larger ciliary muscle. This would lead to changes in relative peripheral refraction in myopes. As previously discussed, evidence on clinically significant changes in axial length and central refractive error with near work is equivocal.156–158 Discrepancies in these studies can be attributed to the level of myopia in the participants and the techniques used, with significant differences in high myopes. Accommodation has been shown to induce the ocular shape to become more prolate.159 The changes in relative peripheral refraction with accommodation are modest and are relatively similar in myopes and emmetropes.157,160,161 Yet, the larger accommodative lags present during near work (which might be higher in myopic children due to the close working distances adopted) would increase the peripheral hyperopic defocus further in myopic eyes.162
Sensitivity to defocus in the peripheral retina is expected to be lower than the central retinal sensitivity. Cone and ganglion cell density and visual quality decreases with field angle, so peripheral visual resolution is low and has lower sensitivity to defocus. The depth of focus at a peripheral field of up to 45 degrees remains around ±1 D163; therefore, any changes in the peripheral focus of over ±1 D are likely to be perceived as defocussed in the peripheral retina and could disrupt the emmetropization process. Postural control is a requisite in maintaining a stable body and to ensure safety and prevent injuries and the visual system contributes significantly to postural stability.164,165 Myopes show a higher postural instability to peripheral stimuli and distortions presented in the stimuli than emmetropes, further indicating that the peripheral vision in myopes is likely to be more sensitive than in emmetropes.166 It has been shown that myopes display an asymmetry to defocus being less sensitive to negative defocus (hyperopic) than positive (myopic) defocus in both peripheral and central vision compared with a more symmetrical response in emmetropes.167–169 It has also been suggested that the eye derives the odd error cues for the direction of defocus using the oblique astigmatic foci (difference between radial and tangential foci) in the peripheral vision.135
Stimuli falling on the peripheral retina can elicit an accommodative response.170–172 However, the accuracy of accommodative response progressively reduces with retinal eccentricity. Hartwig et al.172 found that relative to accommodative stimulus-response slope to central targets, the rate of reduction in slope with peripheral accommodative stimuli was lower in myopes when compared with emmetropes. This finding supports previous studies that indicate that the peripheral retina in myopes is more sensitive to hyperopic defocus than emmetropes up to field angles of at least 15 degrees. Although these studies show that the peripheral retina can alter the accommodation response of the eye, the exact nature of the response and how this might summate with the stimuli falling on different regions of the retina is still unclear.
Sensitivity to Blur: Detection and Discrimination Thresholds
Blur sensitivity is decreased in adults with myopia,173,174 and the detrimental effect of central attention in peripheral vision is also larger in myopia.175 Schmidt et al.176 measured children's ability to detect blur and found no differences among refractive groups, but they did not evaluate blur discrimination. More recently, Labhishetty et al.177 showed that even though children with progressive myopia show increased depth of focus, they do not show increased blur detection thresholds. The effect of blur adaptation178,179 on blur sensitivity is also larger in early onset myopes compared to emmetropes,180 although this effect may only occur with isolated letters,181 perhaps due to lateral masking, and it is dependent on the lateral extent of the stimulus.182 These findings suggest that the reduced sensitivity to defocus in myopia may be compensated with higher level adaptation processes to preserve the subjective clarity even in the presence of decreased retinal image quality.177 One limitation is the lack of consideration of whether myopes regularly wore their full correction, thus potentially impacting on adaption.
Current models of refractive error development agree on the importance of image quality across the retina to guide emmetropization, not only at the fovea.183–187 It appears that a balance across the retina is critical for normal emmetropization; peripheral blur, with or without clear central vision, may induce myopia.184–188 Retinal defocus is known to decrease peripheral sensitivity, particularly to low light level stimuli.189 The human decoding system for blur is tuned for low and mid-spatial frequencies and appears to be located in the retinal near periphery (up to 15 degrees).182,190,191 Accommodation can also be elicited by near peripheral defocus,192,193 and myopes may demonstrate less effective peripheral accommodation.194
Greater losses of peripheral function have been noted in myopes than emmetropes,195–197 probably due to retinal expansion.198 Myopes also show a greater degree of adaptation to peripheral blur,199 and, unlike emmetropes, myopes do not show a constant pattern of peripheral defocus during accommodation.192 Differences in sensitivity to myopic and hyperopic defocus in the periphery are only seen in myopes, indicating different effects of radial and tangential blur during emmetropization.200
Spatial Frequency and Contrast Cues in Accommodation
Reading often requires viewing high-contrast text at close distances for prolonged periods. Spatial frequency and contrast of reading text are often limited in range when compared to natural scenes, which can lead to further spatial and contrast adaptation.122 Myopes show a reduced sensitivity to defocus blur when compared with non-myopes.168,169,201,202 The reduction in blur sensitivity diminishes the effect of accommodative lag on visual performance and increases blur and contrast adaptation in uncorrected myopes.203 Contrast adaptation leads to a decrease in contrast sensitivity at a specific spatial frequency after viewing high-contrast targets of a similar spatial frequency.204 The adaptation effect increases with time and a longer adaptation period requires a longer recovery period.205,206 A degraded retinal image as a consequence of contrast adaptation may lead to perceptual blur, which in turn could result in myopia development.207 During reading tasks, contrast adaptation is expected to reduce contrast sensitivity to spatial frequencies similar to the row or stroke frequency of the text.208 Studies on myopic children and adults have shown that myopes demonstrate a significantly higher level of contrast adaptation (nearly 2 times) in comparison to emmetropes.208,209 The contrast adaption was shown at different spatial frequencies in these two studies owing to differences in targets used (paper versus cathode ray tube display) and age of the participants (children versus adults). Nonetheless, the higher contrast adaptation levels, as seen in myopes, are expected to degrade retinal image significantly more in myopes during prolonged near tasks, therefore, possibly contributing to myopia development/progression. However, it is unclear whether these differences in contrast adaptation are a precursor or consequence of myopia.
Contrast adaptation has been shown to occur when the eye is exposed to positive (myopic) defocus but not to negative (hyperopic) defocus, however, the reason for this is currently unknown.210 In addition, McGonigle et al.208 found that myopes show higher levels of contrast adaptation after reading text on a cathode ray tube when compared to emmetropes, despite ensuring that there was no accommodative lag present in either group. The contrast adaptation differences between myopes and emmetropes are, therefore, unlikely to be caused due to larger lags seen in myopes when reading.91,211
In regions where the prevalence of myopia is high, children and adults read both Chinese and English. Chinese characters have a relatively greater content of high spatial frequency components compared to Latin characters.212 Accommodation to low spatial frequencies (1 c/deg or less) tends to produce higher lags; the optimal accommodative response is produced for spatial frequencies at the peak of photopic contrast sensitivity (3–5 c/deg).213–215 No systematic differences have been found in accommodative responses of emmetropes and myopes to sinusoidal grating targets of different spatial frequencies,216 nor to Chinese and Latin characters.217,218 Contrast adaptation too was similar for Chinese and Latin text, although it was found to be higher in myopes.209
Interactions of Monochromatic Aberrations and Accommodation
Higher-order aberrations affect the visual quality of the eye and provide odd-error signals, which can help the eye detect the direction of defocus thereby contributing to the regulation of accommodation and refractive error development. Spherical aberration can provide odd-error cues to identify the sign of defocus in the central visual field, whereas coma and astigmatism can provide the cues for direction of defocus in the peripheral visual field.135,219,220 Higher-order aberrations alter in a similar way to spherical and cylindrical refractive errors during emmetropization.221 The intersubject variability in higher-order aberrations is high and this may be why studies looking at differences in aberrations between myopes and emmetropes have reported inconclusive results, both in cross-sectional and longitudinal studies.137,138,222 The interaction between individual higher order aberrations, such as spherical aberration and defocus, is more likely to affect the visual quality and refractive development rather than the absolute magnitude of individual aberrations or the total root mean square error of higher-order aberrations. Higher order aberrations change with accommodation; spherical aberration has been consistently shown to have a negative shift with accommodation in young individuals with a greater change in myopes.138,223 Negative spherical aberration can improve image quality when it interacts with myopic defocus and can degrade image quality when combined with hyperopic defocus as produced by accommodative lag.220 It is therefore hypothesized that the higher accommodative lags during extended periods of near work in myopes, when combined with the negative spherical aberration produced during accommodation, would interact and degrade retinal image quality further in myopes more than that in emmetropes who experience lower lags during near work.
Color Based Cues
Longitudinal chromatic aberration can extend the best focus of the eye by approximately 2.0 D and, hence, can also provide the odd error cue for accommodation and emmetropization (Fig. 3). Accommodative response in humans also varies with wavelength, with the eye accommodating more for longer wavelength and showing an approximately 1.0 D difference in response across the visible spectrum.224 The difference in contrast produced due to longitudinal chromatic aberration between long and short-wavelength light can also help detect the direction of defocus.225 Although the eye can accommodate and emmetropize in the absence of chromatic cues, as shown by the monochromatic light studies in animals, the presence of chromatic signals seems to increase the response accuracy of both emmetropization and accommodation systems.226 It has been hypothesized that the myopic eye emmetropizes to reach optimal focus using either the red/green color sensitive mechanism or the luminance sensitive mechanism, relative to the optimal focus for the blue/yellow color, which is more myopically defocused.227 This hypothesis is supported by the fact that myopes show increased sensitivity to long wavelength cone contrast and reduced sensitivity to short wavelength cone contrast when compared to emmetropes.228 However, how this translates to a mechanism for myopia development is unclear.
Figure 3.
The visual stimulus from chromatic aberration in longitudinal (along the optic axis) and transverse (affecting the peripheral retinal image) planes. Copyright © 2021 by IMI.
Near Work Posture
Near working distances tend to be between 10 and 40 cms in 6 to 11-year-old children and children with habitually short reading distances are likely to have higher magnitudes of myopia.4,229–231 The relatively short near working distances in addition to the asymmetric head posture, as adopted by most children, can lead to differences in accommodative demands between the two eyes. As the reading distance is reduced, the intraocular difference in accommodative demand increases with all spatially extended tasks.232 As the working distance gets closer, the head tilt increases.129,233 With a head tilt, one eye would consistently encounter higher time-averaged accommodative demand than the other eye leading to aniso-accommodative demand. As accommodation is a binocular process, aniso-accommodation is likely to be rather small (0.25 D or less) between the two eyes.234,235 Therefore, substantial levels of blur can be perceived by the eye when the aniso-accommodative demand is coupled with high accommodative lags. Further, this nonuniform distribution of dioptric stimuli during near work could also exacerbate the effect of defocus in peripheral vision, particularly so when head tilts occur.
Working distance, head posture, and eye movements have been shown to be similar in adult myopes and emmetropes over relatively short periods of reading tasks.236–238 However, myopic Chinese children have been shown to have significantly closer working distances during near tasks, which tend to be closest with video game tasks on hand held devices.233 Working distance also reduces with increased attention and concentration.231 This could reduce the working distance with hand held devices when compared to previous studies conducted with paper based reading tasks. The closer working distances would lead to yet higher accommodative lags, further degrading vision particularly at higher spatial frequencies.
Differences in Indoor and Outdoor Environments as Related to Accommodation
It is well established that spending more time outdoors prevents myopia development and progression.239–257 One significant difference of outdoor versus indoor environments is the level and uniformity of dioptric blur across the retina190; objects are typically further away so there is less dioptric variation across the visual scenes in outdoor environments and pupil miosis is greater due to higher illumination levels leading to a greater depth of focus, therefore, less accommodative response is demanded.
Binocular Vision
Binocularity is important in the formation of the retinal image. Binocularity improves the accommodative response to defocus,258 and, in turn, blur due to defocus is a useful cue in binocularity.259,260 This effect may be different in myopes.261 Although emmetropization signals are found locally at the retinal level, binocular vision may play a significant role in retinal image focus and therefore in emmetropization and potentially for myopia development. Blur sensitivity, for example, is reduced in myopes under monocular but not binocular conditions.173 Myopes also show reduced stereopsis with flickering stimuli and greater binocular imbalance compared with emmetropes.262 Night myopia, or tonic accommodation, is reduced under binocular conditions263 and the accommodative gain is different with a translucent occluder over the nonviewing eye than binocularly in emmetropes but not in myopes.264
One method to clinically measure disturbances of binocular vision is the magnitude of the accommodative-convergence to accommodation (AC/A) ratio. Higher AC/A ratios have been documented in myopic children compared to emmetropic children.265 Studies have found the AC/A ratio to be elevated prior to myopia onset126 and as early as 4 years prior to myopia onset.266 The AC/A ratio has been found to reach its peak at myopia onset and remain both stable and raised through at least 5 years after myopia onset. The increased AC/A ratio in myopic children could result from a higher gain of the cross-link from accommodation to convergence, or it could represent an increased effort required per diopter of accommodative output, even if the accommodative convergence cross-link gain relationship may be relatively constant. Mutti and colleagues found a higher AC/A ratio correlated with a greater lag of accommodation, but was not associated with a faster rate of myopia progression.266 This effect may be related to the observed changes in the ciliary muscle between myopes and emmetropes.78,153 The effect of refractive error on phoria and AC/A is summarized in Table 3.
Table 3.
Effect of Refractive Error on Phoria and AC/A in Children and Young Adults
| Paper | Measurement Method | Mode of Myopic Correction | Age, y | Refractive Groups | Near Phoria (Δ) | Response AC/A (Δ/D) | Summary of Results |
|---|---|---|---|---|---|---|---|
| Rosenfield and Gilmartin (1987)298 | IR Autoref and Maddox rod | Trial frame and lenses | 18-27 | EMMs | 3.0 | Higher AC/A ratios in LOMs than EOMs than EMMs | |
| EOMs LOMs | 3.9 | ||||||
| 4.6 | |||||||
| Goss (1991)299 | Canon R-1 Autoref von Graefe phoria | Trial frame and lenses | 6-15 | EMMs | −2 exo | Onset of myopia preceded by vergence changes | |
| Became MYPs | +1 eso | ||||||
| Jiang (1995)300 | Canon R-1 Autoref Phoria method not mentioned | Trial frame and lenses | 18-27 | EMMs | 0.9 | Higher AC/A ratios in EMMs that became Myopes | |
| Became MYPs | 1.4 | ||||||
| Gwiazda et al. (1999)301 | Canon R-1 Autoref with attached motorized Risley prism and Maddox rod | Trial frame and lenses | 6-14 | EMMs | 3.9 | Higher AC/A ratios in myopic children | |
| MYPs | 6.4 | ||||||
| Mutti et al. (2000)265 | Simultaneous accommodation and vergence measures Canon R-1 Autoref Purkinje images I and IV | Habitual correction | 6-14 | EMMs | 3.9 | Higher AC/A ratios in myopic children | |
| MYPs | 6.4 | ||||||
| Chen et al. (2003)302 | Shin-Nippon Autoref with Howell Dwyer Card | Trial frame and lenses | 8-12 | EMMs | −0.7 exo | 2 | AC/A ratios and phoria were similar in EMMs and MYPs |
| MYPs | −1.0 exo | 3 | |||||
| Gwiazda et al. (2005)126 | Canon R-1 Autoref with attached motorized Risley prism and Maddox rod | Trial frame and lenses | 6-18 | EMMs | −2.9 exo | 7.5 | Elevated AC/A in EMMs who became myopic, 2 y prior to onset |
| Became MYPs | −0.4 exo | >9 | |||||
| Allen and O'Leary (2006)59 | PowerRefractor with a Bernell Muscle Imbalance Measure (MIM) test card and Maddox rod | Trial frame and lenses | 18-22 | EMMs | 3.5 | Elevated AC/A not related to myopia progression | |
| EOMs | 4.2 | ||||||
| LOMs | 3.6 | ||||||
| Price et al. (2013)274 | Shin-Nippon Autoref with Howell Dwyer Card | Trial frame and lenses | 14-21 | MYPs | 4 | Elevated AC/A was related to myopia progression | |
| Zadnik et al. (2015)303 | Simultaneous accommodation and vergence Canon R-1 Autoref Purkinje images I and IV | Habitual correction | 7-13 | EMMs | 4 | High AC/A myopia risk factor | |
| Became MYPs | 7 | ||||||
| Mutti et al. (2017)266 | Simultaneous accommodation and vergence Canon R-1 Autoref Purkinje images I and IV | Habitual correction | 6-14 | EMMs | 4 | AC/A increased up to 4 y prior to myopia onset | |
| Became MYPs | 7 |
AC/A, accommodation convergence to accommodation response ratio; EMMs, emmetropes; EOMs, early onset myopes; LOMs, late onset myopes; MYPs, myopes.
Theoretically, a greater AC/A is also likely to shift the eyes toward esophoria at near work in these myopic children. Near positive (base in) fusional vergences are also higher in progressing myopes.267 Interestingly, myopic children exhibit less convergent shifts in vergence adaptation compared to emmetropes, which could be attributed to higher accommodative adaptation (as assessed by changes in tonic accommodation).268 When myopia is controlled with orthokeratology, the child's zone of clear single binocular vision becomes more divergent and the accommodation responses increase relative to that measured under correction with single vision spectacles.269
Accommodation With Optical Myopia Control Interventions
All contemporary optical interventions for myopia are based on a common premise that reducing off-axis hyperopic blur or inducing off-axis myopic blur should slow the progression of myopia.152 Their optical designs incorporate one or more paracentral or peripheral zones of plus power around a central clear zone so as to induce areas of peripheral or simultaneous myopic blur in the retina while providing clear on-axis focus and vision through the center. Such dual power designs have the potential to interfere with the accommodative and binocular system, because myopic children may underaccommodate by looking through relative plus zones, further weakening the potentially diminished accommodative function due to myopia.
Several studies have investigated the effect of soft bifocal or multifocal contact lenses on accommodative response in adults, but the results are mixed. Some studies have shown either similar response to single vision contact lens wear270 or a lead of accommodation,271 others have shown increased accommodative lag,272 reduced monocular accommodative facility,273 and exophoric shifts at near.272 It has also been shown that spherical aberration modifying lenses do not affect accommodative facility and horizontal phoria,274 and adding negative aberration can improve the slope of the accommodation stimulus‐response curve, reducing lag of accommodation.275 Orthokeratology lens wear has also been shown to increase exophoria in young adult myopes.269 However, unlike soft multifocal lenses, orthokeratology lenses have been found to lower accommodative lags at near, prompting some to suggest that these lenses may be a better strategy to slow reduce myopia progression in adults with binocular vision disorders.276
Studies in children show reduced accommodation response and an increase in exophoria while wearing center-distance soft bifocal277 or multifocal contact lens278 compared with single vision contact lenses, suggesting that perhaps children resort to using the relative plus power in an attempt to relax accommodation. However, in other studies, no difference in binocular or accommodative function can be detected in children wearing dual-focus contact lenses or extended depth of focus lenses, compared with single vision contact lenses279–282 suggesting that they can accommodate normally using the distance portion of the lenses, but longer term monitoring is warranted.
Translation to Clinical Practice
Evidence from animal studies shows that exposure to hyperopic defocus results in a disruption to the normal emmetropization process and leads to the development of myopia.132 Although the evidence in humans is less clear, chronic retinal defocus at near work, due to a lag in accommodative response, is more frequent and often greater in myopes. This blur at near work has been suggested to trigger a series of biochemical events, which could result in scleral remodeling and axial elongation in an attempt to improve image clarity.132 Thus, addressing retinal blur arising from accommodation has been explored in human longitudinal studies, but results from these studies are mixed.152,283,284
A large-scale longitudinal cohort study has shown that an increased accommodative lag occurs in children after the onset of myopia.91 Therefore, an elevated accommodative lag is unlikely to be a useful predictive factor for the onset of myopia. Lag of accommodation has not been found to be associated with myopia progression.285 It is more probable that an increased hyperopic defocus from accommodative lag may be a consequence rather than a cause of myopia. Esophoria at near work has not been associated with myopia progression in studies using bifocal or progressive addition spectacle lenses (for review see Wildsoet et al.152) and may result as compensation for deficient accommodation rather than a causative factor for myopia progression.286
Concluding Remarks
It is evident that, to date, the role of accommodation and binocular vision in the development and progression of myopia is not fully understood. Aspects of blur from the lag of accommodation, the impact of spatial frequency at near work, and a short working distance may all be implicated in myopia development and progression. The response of the ciliary body and its links with changes in the choroid are still being explored with respect to myopia development and progression. Researchers have not ruled out the role of the accommodative system in this field, but current methods of intervention based on this theory have not yielded significant results. Based on the evidence to date, eye care practitioners should consider assessing the accommodation and convergence system in young myopes and those at risk of myopia development to ensure they manage their patients by providing a clear retinal image. Current evidence does not point toward a role for accommodation and binocular vision in myopia development and progression.
Acknowledgments
Supported by the International Myopia Institute. The publication costs of the International Myopia Institute reports were supported by donations from the Brien Holden Vision Institute, Carl Zeiss Vision, CooperVision, Essilor, and Alcon.
Medical illustrations by Joanna Culley BA (Hons) MMAA, RIP joanna@medical-artist.com, www.medical-artist.com.
Disclosure: N.S. Logan, CooperVision (F, R), Essilor (C, R), Hoya (F), Zeiss (F); H. Radhakrishnan, None; F.E. Cruickshank, CooperVision (R); P.M. Allen, None; P.K. Bandela, None; L.N. Davies, None; S. Hasebe, None; S. Khanal, None; K.L. Schmid, Carl Zeiss Vision Australia (F); F.A. Vera-Diaz, None; J.S. Wolffsohn, Alcon (R), Allergan (R), Atia Vision (C), Contamac (C), CooperVision (C), Essilor (C), Johnson & Johnson (R), Novartis (C), Rayner (C), Thea pharmaceuticals (C)
References
- 1. Rosenfield M, Gilmartin B.. Myopia and Nearwork. Woburn, MA: Butterworth-Heinemann; 1998. [Google Scholar]
- 2. Mutti DO, Mitchell GL, Moeschberger ML, Jones LA, Zadnik K.. Parental myopia, near work, school achievement, and children's refractive error. Invest Ophthalmol Vis Sci. 2002; 43(12): 3633–3640. [PubMed] [Google Scholar]
- 3. Saw SM, Tong L, Chua WH, et al.. Incidence and progression of myopia in Singaporean school children. Invest Ophthalmol Vis Sci. 2005; 46(1): 51–57. [DOI] [PubMed] [Google Scholar]
- 4. Ip JM, Saw SM, Rose KA, et al.. Role of near work in myopia: findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008; 49(7): 2903–2910. [DOI] [PubMed] [Google Scholar]
- 5. Koretz JF, Cook CA, Kaufman PL.. Accommodation and presbyopia in the human eye: changes in the anterior segment and crystalline lens with focus. Invest Ophthalmol Vis Sci. 1997; 38(3): 569–578. [PubMed] [Google Scholar]
- 6. Kirschkamp T, Dunne M, Barry JC.. Phakometric measurement of ocular surface radii of curvature, axial separations and alignment in relaxed and accommodated human eyes. Ophthalmic Physiol Opt. 2004; 24(2): 65–73. [DOI] [PubMed] [Google Scholar]
- 7. Richdale K, Bullimore MA, Zadnik K.. Lens thickness with age and accommodation by optical coherence tomography. Ophthalmic Physiol Opt. 2008; 28(5): 441–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Doyle L, Little JA, Saunders KJ.. Repeatability of OCT lens thickness measures with age and accommodation. Optom Vis Sci. 2013; 90(12): 1396–1405. [DOI] [PubMed] [Google Scholar]
- 9. Shum PJT, Ko LS, Ng CL, Lin SL.. A biometric study of ocular changes during accommodation. Am J Ophthalmol. 1993; 115(1): 76–81. [DOI] [PubMed] [Google Scholar]
- 10. Drexler W, Baumgartner A, Findl O, Hitzenberger CK, Fercher AF.. Biometric investigation of changes in the anterior eye segment during accommodation. Vision Res. 1997; 37(19): 2789–2800. [DOI] [PubMed] [Google Scholar]
- 11. Dubbelman M, Van Der Heijde GL, Weeber HA.. Change in shape of the aging human crystalline lens with accommodation. Vision Res. 2005; 45(1): 117–132. [DOI] [PubMed] [Google Scholar]
- 12. Ostrin L, Kasthurirangan S, Win-Hall D, Glasser A.. Simultaneous measurements of refraction and A-scan biometry during accommodation in humans. Optom Vis Sci. 2006; 83(9): 657–665. [DOI] [PubMed] [Google Scholar]
- 13. Tsorbatzoglou A, Németh G, Széll N, Biró Z, Berta A.. Anterior segment changes with age and during accommodation measured with partial coherence interferometry. J Cataract Refract Surg. 2007; 33(9): 1597–1601. [DOI] [PubMed] [Google Scholar]
- 14. Strenk SA, Strenk LM, Semmlow JL, DeMarco JK.. Magnetic resonance imaging study of the effects of age and accommodation on the human lens cross-sectional area. Investig Ophthalmol Vis Sci. 2004; 45(2): 539–545. [DOI] [PubMed] [Google Scholar]
- 15. Strenk SA, Strenk LM, Koretz JF.. The mechanism of presbyopia. Prog Retin Eye Res. 2005; 24(3): 379–393. [DOI] [PubMed] [Google Scholar]
- 16. Hermans E, Dubbelman M, van der Heijde R, Heethaar R.. The shape of the human lens nucleus with accommodation. J Vis. 2007; 7(10): 16. [DOI] [PubMed] [Google Scholar]
- 17. Glasser A, Kaufman PL.. The mechanism of accommodation in primates. Ophthalmology. 1999; 106(5): 863–872. [DOI] [PubMed] [Google Scholar]
- 18. Strenk SA, Semmlow JL, Strenk LM, Munoz P, Gronlund-Jacob J, DeMarco JK.. Age-related changes in human ciliary muscle and lens: a magnetic resonance imaging study. Invest Ophthalmol Vis Sci. 1999; 40(6): 1162–1169. [PubMed] [Google Scholar]
- 19. Richdale K, Bullimore MA, Sinnott LT, Zadnik K.. The effect of age, accommodation, and refractive error on the adult human eye. Optom Vis Sci. 2016; 93(1): 3–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Tse PU, Whitney D, Anstis S, Cavanagh P.. Voluntary attention modulates motion-induced mislocalization. J Vis. 2011; 11(3): 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Jones CE, Atchison DA, Pope JM.. Changes in lens dimensions and refractive index with age and accommodation. Optom Vis Sci. 2007; 84(10): 990–995. [DOI] [PubMed] [Google Scholar]
- 22. Khan A, Pope JM, Verkicharla PK, Suheimat M, Atchison DA.. Change in human lens dimensions, lens refractive index distribution and ciliary body ring diameter with accommodation. Biomed Opt Express. 2018; 9(3): 1272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Koretz JF, Cook CA, Kaufman PL.. Aging of the human lens: changes in lens shape upon accommodation and with accommodative loss. J Opt Soc Am A. 2002; 19(1): 144. [DOI] [PubMed] [Google Scholar]
- 24. Rosales P, Dubbelman M, Marcos S, van der Heijde R. Crystalline lens radii of curvature from Purkinje and Scheimpflug imaging. J Vis. 2006; 6(10): 1057–1067. [DOI] [PubMed] [Google Scholar]
- 25. Garner LF, Yap MKH.. Changes in ocular dimensions and refraction with accommodation. Ophthalmic Physiol Opt. 1997; 17(1): 12–17. [PubMed] [Google Scholar]
- 26. Ciuffreda KJ. The Glenn A. Fry invited lecture. Accommodation to gratings and more naturalistic stimuli. Optom Vis Sci. 1991; 68(4): 243–260. [DOI] [PubMed] [Google Scholar]
- 27. Bolz M, Prinz A, Drexler W, Findl O.. Linear relationship of refractive and biometric lenticular changes during accommodation in emmetropic and myopic eyes. Br J Ophthalmol. 2007; 91(3): 360–365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gullstrand A. In: Appendices II and IV. In Helmholtz's Handbuch Der Physiologischen Optik.; 1909:Vol 1, pp. 301–358, 382-414. [Google Scholar]
- 29. Tian Y, Tarrant J, Wildsoet CF. Optical and biometric characteristics of anisomyopia in human adults. Ophthalmic Physiol Opt. 2011; 31(5): 540–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Atchison DA, Jones CE, Schmid KL, et al.. Eye shape in emmetropia and myopia. Invest Ophthalmol Vis Sci. 2004; 45(10): 3380–3386. [DOI] [PubMed] [Google Scholar]
- 31. Logan NS, Gilmartin B, Wildsoet CF, Dunne MCM. Posterior retinal contour in adult human anisomyopia. Invest Ophthalmol Vis Sci. 2004; 45(7): 2152–2162. [DOI] [PubMed] [Google Scholar]
- 32. Chang SW, Tsai IL, Hu FR, Lin LLK, Shih YF.. The cornea in young myopic adults. Br J Ophthalmol. 2001; 85(8): 916–920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Grosvenor T, Goss DA. Role of the cornea in emmetropia and myopia. Optom Vis Sci. 1998; 75(2): 132–145. [DOI] [PubMed] [Google Scholar]
- 34. Garner LF, Stewart AW, Owens H, Kinnear RF, Frith MJ. The Nepal longitudinal study: biometric characteristics of developing eyes. Optom Vis Sci. 2006; 83(5): 274–280. [DOI] [PubMed] [Google Scholar]
- 35. Goss DA, Van Veen HG, Rainey BB, Feng B.. Ocular components measured by keratometry, phakometry, and ultrasonography in emmetropic and myopic optometry students. Optom Vis Sci. 1997; 74(7): 489–495. [DOI] [PubMed] [Google Scholar]
- 36. Scott R, Grosvenor T. Structural model for emmetropic and myopic eyes. Ophthalmic Physiol Opt. 1993; 13(1): 41–47. [DOI] [PubMed] [Google Scholar]
- 37. McBrien NA, Adams DW.. A longitudinal investigation of adult-onset and adult-progression of myopia in an occupational group: refractive and biometric findings. Invest Ophthalmol Vis Sci. 1997; 38(2): 321–333. [PubMed] [Google Scholar]
- 38. McBrien NA, Millodot M.. A biometric investigation of late onset myopic eyes. Acta Ophthalmol. 1987; 65(4): 461–468. [DOI] [PubMed] [Google Scholar]
- 39. Zadnik K, Mutti DO, Fusaro RE, Adams AJ.. Longitudinal evidence of crystalline lens thinning in children. Invest Ophthalmol Vis Sci. 1995; 36(8): 1581–1587. [PubMed] [Google Scholar]
- 40. Read SA, Fuss JA, Vincent SJ, Collins MJ, Alonso-Caneiro D. Choroidal changes in human myopia: insights from optical coherence tomography imaging. Clin Exp Optom. 2019; 102(3): 270–285. [DOI] [PubMed] [Google Scholar]
- 41. Schmid KL, Li RWH, Edwards MH, Lew JKF.. The expandability of the eye in childhood myopia. Curr Eye Res. 2003; 26(2): 65–71. [DOI] [PubMed] [Google Scholar]
- 42. Patel H, Gilmartin B, Cubbidge RP, Logan NS.. In vivo measurement of regional variation in anterior scleral resistance to Schiotz indentation. Ophthalmic Physiol Opt. 2011; 31(5): 437–443. [DOI] [PubMed] [Google Scholar]
- 43. Davies LN, Dunne MCM, Gibson GA, Wolffsohn JS.. Vergence analysis reveals the influence of axial distances on accommodation with age and axial ametropia. Ophthalmic Physiol Opt. 2010; 30(4): 371–378. [DOI] [PubMed] [Google Scholar]
- 44. Hunt OA, Wolffsohn JS, García-Resúa C.. Ocular motor triad with single vision contact lenses compared to spectacle lenses. Contact Lens Anterior Eye. 2006; 29(5): 239–245. [DOI] [PubMed] [Google Scholar]
- 45. Diether S, Schaeffel F.. Local changes in eye growth after imposed local defocus. Invest Ophthalmol Vis Sci. 1996; 37(3): 659–668. [Google Scholar]
- 46. Wildsoet CF. Active emmetropization — evidence for its existence and ramifications for clinical practice. Ophthalmic Physiol Opt. 1997; 17(4): 279–290. [PubMed] [Google Scholar]
- 47. Smith EL, Hung LF, Arumugam B.. Visual regulation of refractive development: Insights from animal studies. Eye. 2014; 28(2): 180–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Troilo D, Smith EL, Nickla DL, et al.. IMI – report on experimental models of emmetropization and myopia. Invest Ophthalmol Vis Sci. 2019; 60(3): M31–M88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. McBrien NA, Millodot M.. Amplitude of accommodation and refractive error. Invest Ophthalmol Vis Sci. 1986; 27(7): 1187–1190. [PubMed] [Google Scholar]
- 50. Gwiazda J, Thorn F, Bauer J, Held R.. Myopic children show insufficient accommodative response to blur. Invest Ophthalmol Vis Sci. 1993; 34(3): 690–694. [PubMed] [Google Scholar]
- 51. Gwiazda JE, Hyman L, Norton TT, et al.. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2004; 45(7): 2143–2151. [DOI] [PubMed] [Google Scholar]
- 52. Charman WN. Near vision, lags of accommodation and myopia. Ophthalmic Physiol Opt. 1999; 19(2): 126–133. [DOI] [PubMed] [Google Scholar]
- 53. Seidemann A, Schaeffel F.. An evaluation of the lag of accommodation using photorefraction. Vision Res. 2003; 43(4): 419–430. [DOI] [PubMed] [Google Scholar]
- 54. Nakatsuka C, Hasebe S, Nonaka F, Ohtsuki H.. Accommodative lag under habitual seeing conditions: comparison between adult myopes and emmetropes. Jpn J Ophthalmol. 2003; 47(3): 291–298. [DOI] [PubMed] [Google Scholar]
- 55. Gwiazda J, Bauer J, Thorn F, Held R.. A dynamic relationship between myopia and blur-driven accommodation in school-aged children. Vision Res. 1995; 35(9): 1299–1304. [DOI] [PubMed] [Google Scholar]
- 56. Drobe B, de Saint-André R. The pre-myopic syndrome. Ophthalmic Physiol Opt. 1995; 15(5): 375–378. [PubMed] [Google Scholar]
- 57. Abbott ML, Schmid KL, Strang NC.. Differences in the accommodation stimulus response curves of adult myopes and emmetropes. Ophthalmic Physiol Opt. 1998; 18(1): 13–20. [PubMed] [Google Scholar]
- 58. He JC, Gwiazda J, Thorn F, Held R, Vera-Diaz FA.. The association of wavefront aberration and accommodative lag in myopes. Vision Res. 2005; 45(3): 285–290. [DOI] [PubMed] [Google Scholar]
- 59. Allen PM, O'Leary DJ. Accommodation functions: co-dependency and relationship to refractive error. Vis Res. 2006; 46(4): 491–505. [DOI] [PubMed] [Google Scholar]
- 60. Charman WN, Radhakrishnan H.. Accommodation, pupil diameter and myopia. Ophthalmic Physiol Opt. 2009; 29(1): 72–79. [DOI] [PubMed] [Google Scholar]
- 61. Applegate RA, Donnelly WJ III, Marsack Koenig JDDE. Three-dimensional relationship high-order root-mean-square between wavefront error, pupil diameter, and aging. J Opt Soc Am A. 2007; 24(3): 578–587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Winn B, Whitaker D, Elliott DB, Phillips NJ.. Factors affecting light-adapted pupil size in normal human subjects. Invest Ophthalmol Vis Sci. 1994; 35(3): 1132–1137. [PubMed] [Google Scholar]
- 63. Jones R. Do women and myopes have larger pupils? Invest Ophthalmol Vis Sci. 1990; 31(7): 1413–1415. [PubMed] [Google Scholar]
- 64. Brown SM, Bradley JC.. Pupil size in refractive surgery candidates [1]. J Refract Surg. 2005; 21(3): 303. [DOI] [PubMed] [Google Scholar]
- 65. Subbaram M V., Bullimore MA.. Visual acuity and the accuracy of the accommodative response. Ophthalmic Physiol Opt. 2002; 22(4): 312–318. [DOI] [PubMed] [Google Scholar]
- 66. Hirsch MJ, Weymouth FW.. Pupil size in ametropia. J Appl Physiol. 1949; 1(9): 646–648. [DOI] [PubMed] [Google Scholar]
- 67. Chaidaroon W, Juwattanasomran W.. Colvard pupillometer measurement of scotopic pupil diameter in emmetropes and myopes. Jpn J Ophthalmol. 2002; 46(6): 640–644. [DOI] [PubMed] [Google Scholar]
- 68. Bremner FD. The Pupil: Anatomy, Physiology, and Clinical Applications: By Loewenfeld Irene E.. 1999. Oxford, UK: Butterworth-Heinemann. 2278. ISBN 0-750-67143-2. [Google Scholar]
- 69. Ciuffreda KJ. Accommodation, the Pupil, and Presbyopia. In: Benjamin William J. Borish's Clinical Refraction Second Edition. New York, NY: Elsevier; 2006: 93–144. [Google Scholar]
- 70. Wagner S, Zrenner E, Strasser T.. Ciliary muscle thickness profiles derived from optical coherence tomography images. Biomed Opt Express. 2018; 9(10): 5100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Bailey MD, Sinnott LT, Mutti DO.. Ciliary body thickness and refractive error in children. Invest Ophthalmol Vis Sci. 2008; 49(10): 4353–4360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Schultz KE, Sinnott LT, Mutti DO, Bailey MD.. Accommodative fluctuations, lens tension, and ciliary body thickness in children. Optom Vis Sci. 2009; 86(6): 677–684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Pucker AD, Sinnott LT, Kao CY, Bailey MD.. Region-specific relationships between refractive error and ciliary muscle thickness in children. Invest Ophthalmol Vis Sci. 2013; 54(7): 4710–4716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Lewis HA, Kao CY, Sinnott LT, Bailey MD.. Changes in ciliary muscle thickness during accommodation in children. Optom Vis Sci. 2012; 89(5): 727–737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Oliveira C, Tello C, Liebmann JM, Ritch R. Ciliary body thickness increases with increasing axial myopia. Am J Ophthalmol. 2005; 140(2): 324–325. [DOI] [PubMed] [Google Scholar]
- 76. Muftuoglu O, Hosal BM, Zilelioglu G.. Ciliary body thickness in unilateral high axial myopia. Eye. 2009; 23(5): 1176–1181. [DOI] [PubMed] [Google Scholar]
- 77. Jeon S, Lee WK, Lee K, Moon NJ.. Diminished ciliary muscle movement on accommodation in myopia. Exp Eye Res. 2012; 105: 9–14. [DOI] [PubMed] [Google Scholar]
- 78. Buckhurst H, Gilmartin B, Cubbidge RP, Nagra M, Logan NS.. Ocular biometric correlates of ciliary muscle thickness in human myopia. Ophthalmic Physiol Opt. 2013; 33(3): 294–304. [DOI] [PubMed] [Google Scholar]
- 79. Kuchem MK, Sinnott LT, Kao CY, Bailey MD.. Ciliary muscle thickness in anisometropia. Optom Vis Sci. 2013; 90(11): 1312–1320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Wagner S, Schaeffel F, Zrenner E, Straßer T.. Prolonged nearwork affects the ciliary muscle morphology. Exp Eye Res. 2019; 186: 107741. [DOI] [PubMed] [Google Scholar]
- 81. Sheppard AL, Davies LN.. In vivo analysis of ciliary muscle morphologic changes with accommodation and axial ametropia. Invest Ophthalmol Vis Sci. 2010; 51(12): 6882–6889. [DOI] [PubMed] [Google Scholar]
- 82. Richdale K, Sinnott LT, Bullimore MA, et al.. Quantification of age-related and per diopter accommodative changes of the lens and ciliary muscle in the emmetropic human eye. Invest Ophthalmol Vis Sci. 2013; 54(2): 1095–1105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Lossing LA, Sinnott LT, Kao CY, Richdale K, Bailey MD.. Measuring changes in ciliary muscle thickness with accommodation in young adults. Optom Vis Sci. 2012; 89(5): 719–726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Ruggeri M, de Freitas C, Williams S, et al.. Quantification of the ciliary muscle and crystalline lens interaction during accommodation with synchronous OCT imaging. Biomed Opt Express. 2016; 7(4): 1351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Zhou SB, Li H, Tan J, Hong HF.. Anterior segment changes during accommodation in myopia with OCT. Int Eye Sci. 2013; 13(6): 1209–1211. [Google Scholar]
- 86. Wagner S, Zrenner E, Strasser T.. Emmetropes and myopes differ little in their accommodation dynamics but strongly in their ciliary muscle morphology. Vision Res. 2019; 163: 42–51. [DOI] [PubMed] [Google Scholar]
- 87. Van Alphen GWHM. Choroidal stress and emmetropization. Vision Res. 1986; 26(5): 723–734. [DOI] [PubMed] [Google Scholar]
- 88. Mutti DO. Hereditary and environmental contributions to emmetropization and myopia. Optom Vis Sci. 2010; 87(4): 255–259. [DOI] [PubMed] [Google Scholar]
- 89. Bailey MD. How should we measure the ciliary muscle? Invest Ophthalmol Vis Sci. 2011; 52(3): 1817–1818. [DOI] [PubMed] [Google Scholar]
- 90. Gwiazda J, Thorn F, Held R.. Accommodation, accommodative convergence, and response AC/A ratios before and at the onset of myopia in children. Optom Vis Sci. 2005; 82(4): 273–278. [DOI] [PubMed] [Google Scholar]
- 91. Mutti DO, Mitchell GL, Hayes JR, et al.. Accommodative lag before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2006; 47(3): 837–846. [DOI] [PubMed] [Google Scholar]
- 92. Rosenfield M, Desai R, Portello JK.. Do progressing myopes show reduced accommodative responses? Optom Vis Sci. 2002; 79(4): 268–273. [DOI] [PubMed] [Google Scholar]
- 93. Weizhong L, Zhikuan Y, Wen L, Xiang C, Jian G.. A longitudinal study on the relationship between myopia development and near accommodation lag in myopic children. Ophthalmic Physiol Opt. 2008; 28(1): 57–61. [DOI] [PubMed] [Google Scholar]
- 94. Wood ICJ, Mutti DO, Zadnik K.. Crystalline lens parameters in infancy. Ophthalmic Physiol Opt. 1996; 16(4): 310–317. [PubMed] [Google Scholar]
- 95. Mutti DO, Mitchell GL, Sinnott LT, et al.. Corneal and crystalline lens dimensions before and after myopia onset. Optom Vis Sci. 2012; 89(3): 251–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Drexler W, Findl O, Schmetterer L, Hitzenberger CK, Fercher AF.. Eye elongation during accommodation in humans: differences between emmetropes and myopes. Invest Ophthalmol Vis Sci. 1998; 39(11): 2140–2147. [PubMed] [Google Scholar]
- 97. Mallen EAH, Kashyap P, Hampson KM.. Transient axial length change during the accommodation response in young adults. Invest Ophthalmol Vis Sci. 2006; 47(3): 1251–1254. [DOI] [PubMed] [Google Scholar]
- 98. Woodman EC, Read SA, Collins MJ, et al.. Axial elongation following prolonged near work in myopes and emmetropes. Br J Ophthalmol. 2011; 95(5): 652–656. [DOI] [PubMed] [Google Scholar]
- 99. Read SA, Collins MJ, Woodman EC, Cheong SH.. Axial length changes during accommodation in myopes and emmetropes. Optom Vis Sci. 2010; 87(9): 656–662. [DOI] [PubMed] [Google Scholar]
- 100. Woodman EC, Read SA, Collins MJ.. Axial length and choroidal thickness changes accompanying prolonged accommodation in myopes and emmetropes. Vision Res. 2012; 72: 34–41. [DOI] [PubMed] [Google Scholar]
- 101. Aldossari H, Suheimat M, Atchison DA, Schmid KL.. Effect of accommodation on peripheral eye lengths of emmetropes and myopes. Optom Vis Sci. 2017; 94(3): 361–369. [DOI] [PubMed] [Google Scholar]
- 102. Laughton DS, Sheppard AL, Mallen EAH, Read SA, Davies LN.. Does transient increase in axial length during accommodation attenuate with age? Clin Exp Optom. 2017; 100(6): 676–682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. van Alphen GWHM, Graebel WP.. Elasticity of tissues involved in accommodation. Vision Res. 1991; 31(7-8): 1417–1438. [DOI] [PubMed] [Google Scholar]
- 104. Croft MA, Nork MT, Mcdonald JP, Katz A, Lütjen-Drecoll E, Kaufman PL.. Accommodative movements of the vitreous membrane, choroid, and sclera in young and presbyopic human and nonhuman primate eyes. Invest Ophthalmol Vis Sci. 2013; 54(7): 5049–5058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Ikuno Y, Tano Y.. Retinal and choroidal biometry in highly myopic eyes with spectral-domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2009; 50(8): 3876–3880. [DOI] [PubMed] [Google Scholar]
- 106. Summers Rada JA, Shelton S, Norton TT.. The sclera and myopia. Exp Eye Res. 2006; 82(2): 185–200. [DOI] [PubMed] [Google Scholar]
- 107. Pekel G, Yaʇci R, Acer S, Ongun GT, Çetin EN, Simavli H.. Comparison of corneal layers and anterior sclera in emmetropic and myopic eyes. Cornea. 2015; 34(7): 786–790. [DOI] [PubMed] [Google Scholar]
- 108. Ohno-Matsui K, Akiba M, Modegi T, et al.. Association between shape of sclera and myopic retinochoroidal lesions in patients with pathologic myopia. Invest Ophthalmol Vis Sci. 2012; 53(10): 6046–6061. [DOI] [PubMed] [Google Scholar]
- 109. Friedman E. Scleral Rigidity, Venous Obstruction, and Age-Related Macular Degeneration: A Working Hypothesis. In: BenEzra D, Ryan SJ, Glaser BM, Murphy RP, eds. Ocular Circulation and Neovascularization. Netherlands, US: Springer; 1987: 197–204. [Google Scholar]
- 110. Guthoff R, Berger RW, Draeger J.. Ultrasonographic measurement of the posterior coats of the eye and their relation to axial length. Graefe's Arch Clin Exp Ophthalmol. 1987; 225(5): 374–376. [DOI] [PubMed] [Google Scholar]
- 111. Dastiridou AI, Ginis HS, de Brouwere D, Tsilimbaris MK, Pallikaris IG.. Ocular rigidity, ocular pulse amplitude, and pulsatile ocular blood flow: the effect of intraocular pressure. Invest Ophthalmol Vis Sci. 2009; 54(3): 287–2092. [DOI] [PubMed] [Google Scholar]
- 112. Wong E, Yap MKH.. Factors affecting ocular rigidity in the Chinese. Clin Exp Optom. 1991; 74(5): 156–159. [Google Scholar]
- 113. Atchison DA, Smith G.. Possible errors in determining axial length changes during accommodation with the IOLMaster. Optom Vis Sci. 2004; 81(4): 283–286. [DOI] [PubMed] [Google Scholar]
- 114. Read SA, Collins MJ, Becker H, et al.. Changes in intraocular pressure and ocular pulse amplitude with accommodation. Br J Ophthalmol. 2010; 94(3): 332–335. [DOI] [PubMed] [Google Scholar]
- 115. Woodman-Pieterse EC, Read SA, Collins MJ, Alonso-Caneiro D. Regional changes in choroidal thickness associated with accommodation. Invest Ophthalmol Vis Sci. 2015; 56(11): 6414–6422. [DOI] [PubMed] [Google Scholar]
- 116. Huang F, Huang S, Xie R, et al.. The effect of topical administration of cyclopentolate on ocular biometry: an analysis for mouse and human models. Sci Rep. 2017; 7(1): 9952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. May CA. Non-vascular smooth muscle cells in the human choroid: distribution, development and further characterization. J Anat. 2005; 207(4): 381–390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Backhouse S, Gentle A.. Scleral remodelling in myopia and its manipulation: a review of recent advances in scleral strengthening and myopia control. Ann Eye Sci. 2018; 3(1): 5. [Google Scholar]
- 119. Atchison DA, Pritchard N, Schmid KL, Scott DH, Jones CE, Pope JM.. Shape of the retinal surface in emmetropia and myopia. Invest Ophthalmol Vis Sci. 2005; 46(8): 2698–2707. [DOI] [PubMed] [Google Scholar]
- 120. Oliveira C, Tello C, Liebmann J, Ritch R. Central corneal thickness is not related to anterior scleral thickness or axial length. J Glaucoma. 2006; 15(3): 190–194. [DOI] [PubMed] [Google Scholar]
- 121. Norman RE, Flanagan JG, Rausch SM, et al.. Dimensions of the human sclera: thickness measurement and regional changes with axial length. Exp Eye Res. 2010; 90(2): 277–284. [DOI] [PubMed] [Google Scholar]
- 122. Wallman J, Winawer J.. Homeostasis of eye growth and the question of myopia. Neuron. 2004; 43(4): 447–468. [DOI] [PubMed] [Google Scholar]
- 123. Woodman-Pieterse EC, Read SA, Collins MJ, Alonso-Caneiro D. Anterior scleral thickness changes with accommodation in myopes and emmetropes. Exp Eye Res. 2018; 177: 96–103. [DOI] [PubMed] [Google Scholar]
- 124. Niyazmand H, Read SA, Atchison DA, Collins MJ.. Effects of accommodation and simulated convergence on anterior scleral shape. Ophthalmic Physiol Opt. 2020; 40(4): 482–490. [DOI] [PubMed] [Google Scholar]
- 125. Schachar RA, Kamangar F.. Sclera does not change its shape during accommodation. Ophthalmic Physiol Opt. 2017; 37(5): 624–625. [DOI] [PubMed] [Google Scholar]
- 126. Gwiazda J, Thorn F, Held R.. Accommodation, accommodative convergence, and response AC/A ratios before and at the onset of myopia in children. Optom Vis Sci. 2005; 82(4): 273–278. [DOI] [PubMed] [Google Scholar]
- 127. McClelland JF, Saunders KJ.. Accommodative lag using dynamic retinoscopy: age norms for school-age children. Optom Vis Sci. 2004; 81(12): 929–933. [PubMed] [Google Scholar]
- 128. Rouse MW, Hutter RF, Shiftlett R.. A normative study of the accommodative lag in elementary school children. Am J Optom Physiol Opt. 1984; 61(11): 693–697. [DOI] [PubMed] [Google Scholar]
- 129. Li SM, Li SY, Kang MT, et al.. Near work related parameters and myopia in Chinese children: the Anyang Childhood Eye Study. PLoS One. 2015; 10(8): e0134514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Chen AH, Ahmad A, Kearney S, Strang N.. The influence of age, refractive error, visual demand and lighting conditions on accommodative ability in Malay children and adults. Graefes Arch Clin Exp Ophthalmol. 2019; 257(9): 1997–2004. [DOI] [PubMed] [Google Scholar]
- 131. Altoaimi BH, Kollbaum P, Meyer D, Bradley A.. Experimental investigation of accommodation in eyes fit with multifocal contact lenses using a clinical auto-refractor. Ophthalmic Physiol Opt. 2018; 38(2): 152–163. [DOI] [PubMed] [Google Scholar]
- 132. Troilo D, Smith 3rd EL, Nickla DL, et al.. IMI - report on experimental models of emmetropization and myopia. Invest Ophthalmol Vis Sci. 2019; 60(3): M31–M88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Flitcroft DI. A model of the contribution of oculomotor and optical factors to emmetropization and myopia. Vis Res. 1998; 38(19): 2869–2879. [DOI] [PubMed] [Google Scholar]
- 134. Weizhong L, Zhikuan Y, Wen L, Xiang C, Jian G.. A longitudinal study on the relationship between myopia development and near accommodation lag in myopic children. Ophthalmic Physiol Opt. 2008; 28(1): 57–61. [DOI] [PubMed] [Google Scholar]
- 135. Charman WN. Keeping the world in focus: how might this be achieved? Optom Vis Sci. 2011; 88(3): 373–376. [DOI] [PubMed] [Google Scholar]
- 136. Dhallu SK, Sheppard AL, Drew T, et al.. Factors influencing pseudo-accommodation—the difference between subjectively reported range of clear focus and objectively measured accommodation range. Vision. 2019; 3(3): 34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137. Charman WN. Aberrations and myopia. Ophthalmic Physiol Opt. 2005; 25(4): 285–301. [DOI] [PubMed] [Google Scholar]
- 138. Hughes RP, Vincent SJ, Read SA, Collins MJ.. Higher order aberrations, refractive error development and myopia control: a review. Clin Exp Optom. 2020; 103(1): 68–85. [DOI] [PubMed] [Google Scholar]
- 139. Berntsen DA, Sinnott LT, Mutti DO, Zadnik K, CLEERE Study Group. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vision Res. 2011; 51(9): 1039–1046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140. Correction of Myopia Evaluation Trial 2 Study Group for the Pediatric Eye Disease Investigator Group. Progressive-addition lenses versus single-vision lenses for slowing progression of myopia in children with high accommodative lag and near esophoria. Invest Ophthalmol Vis Sci. 2011; 52(5): 2749–2757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Cheng D, Woo GC, Drobe B, Schmid KL.. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014; 132(3): 258–264. [DOI] [PubMed] [Google Scholar]
- 142. Langaas T, Riddell PM.. Accommodative instability: relationship to progression of early onset myopia. Clin Exp Optom. 2012; 95(2): 153–159. [DOI] [PubMed] [Google Scholar]
- 143. Langaas T, Riddell PM, Svarverud E, Ystenaes AE, Langeggen I, Bruenech JR.. Variability of the accommodation response in early onset myopia. Optom Vis Sci. 2008; 85(1): 37–48. [DOI] [PubMed] [Google Scholar]
- 144. Maiello G, Kerber KL, Thorn F, Bex PJ, Vera-Diaz FA.. Vergence driven accommodation with simulated disparity in myopia and emmetropia. Exp Eye Res. 2018; 166: 96–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Ciuffreda KJ, Wallis DM.. Myopes show increased susceptibility to nearwork aftereffects. Invest Ophthalmol Vis Sci. 1998; 39(10): 1797–1803. [PubMed] [Google Scholar]
- 146. Vera-Díaz FA, Strang NC, Winn B.. Nearwork induced transient myopia during myopia progression. Curr Eye Res. 2002; 24(4): 289–295. [DOI] [PubMed] [Google Scholar]
- 147. Ciuffreda KJ, Vasudevan B.. Nearwork-induced transient myopia (NITM) and permanent myopia - is there a link? Ophthalmic Physiol Opt. 2008; 28(2): 103–114. [DOI] [PubMed] [Google Scholar]
- 148. Wolffsohn JS, Gilmartin B, Li RW, et al.. Nearwork-induced transient myopia in preadolescent Hong Kong Chinese. Invest Ophthalmol Vis Sci. 2003; 44(5): 2284–2289. [DOI] [PubMed] [Google Scholar]
- 149. Ciuffreda KJ, Vasudevan B.. Effect of nearwork-induced transient myopia on distance retinal defocus patterns. Optometry. 2010; 81(3): 153–156. [DOI] [PubMed] [Google Scholar]
- 150. Lin Z, Vasudevan B, Liang YB, et al.. Nearwork-induced transient myopia (NITM) in anisometropia. Ophthalmic Physiol Opt. 2013; 33(3): 311–317. [DOI] [PubMed] [Google Scholar]
- 151. Charman WN, Radhakrishnan H.. Peripheral refraction and the development of refractive error: a review. Ophthalmic Physiol Opt. 2010; 30(4): 321–338. [DOI] [PubMed] [Google Scholar]
- 152. Wildsoet CF, Chia A, Cho P, et al.. IMI – Interventions Myopia Institute: Interventions for controlling myopia onset and progression report. Invest Ophthalmol Vis Sci. 2019; 60(3): M106–M131. [DOI] [PubMed] [Google Scholar]
- 153. Bailey MD, Sinnott LT, Mutti DO.. Ciliary body thickness and refractive error in children. Invest Ophthalmol Vis Sci. 2008; 49(10): 4353–4360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154. Oliveira C, Tello C, Liebmann JM, Ritch R. Ciliary body thickness increases with increasing axial myopia. Am J Ophthalmol. 2005; 140(2): 324–325. [DOI] [PubMed] [Google Scholar]
- 155. Sheppard AL, Davies LN.. In vivo analysis of ciliary muscle morphologic changes with accommodation and axial ametropia. Invest Ophthalmol Vis Sci. 2010; 51(12): 6882-6889. 7. [DOI] [PubMed] [Google Scholar]
- 156. Radhakrishnan H, Charman WN.. Refractive changes associated with oblique viewing and reading in myopes and emmetropes. J Vis. 2007; 7(8): 1–15. [DOI] [PubMed] [Google Scholar]
- 157. Whatham A, Zimmermann F, Martinez A, et al.. Influence of accommodation on off-axis refractive errors in myopic eyes. J Vis. 2009; 9(3): 14.1–13. [DOI] [PubMed] [Google Scholar]
- 158. Davies LN, Mallen EA.. Influence of accommodation and refractive status on the peripheral refractive profile. Br J Ophthalmol. 2009; 93(9): 1186–1190. [DOI] [PubMed] [Google Scholar]
- 159. Walker TW, Mutti DO.. The effect of accommodation on ocular shape. Optom Vis Sci. 2002; 79(7): 424–430. [DOI] [PubMed] [Google Scholar]
- 160. Calver R, Radhakrishnan H, Osuobeni E, O'Leary D. Peripheral refraction for distance and near vision in emmetropes and myopes. Ophthalmic Physiol Opt. 2007; 27(6): 584–593. [DOI] [PubMed] [Google Scholar]
- 161. Mathur A, Atchison DA, Charman WN.. Effect of accommodation on peripheral ocular aberrations. J Vis. 2009; 9(12): 20 1-11. [DOI] [PubMed] [Google Scholar]
- 162. Harb E, Thorn F, Troilo D.. Characteristics of accommodative behavior during sustained reading in emmetropes and myopes. Vis Res. 2006; 46(16): 2581–2592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163. Wang YZ, Thibos LN, Bradley A.. Effects of refractive error on detection acuity and resolution acuity in peripheral vision. Invest Ophthalmol Vis Sci. 1997; 38(10): 2134–2143. [PubMed] [Google Scholar]
- 164. Verbecque E, Vereeck L, Hallemans A.. Postural sway in children: a literature review. Gait Posture. 2016; 49: 402–410. [DOI] [PubMed] [Google Scholar]
- 165. Najafpour Z, Godarzi Z, Arab M, Yaseri M.. Risk factors for falls in hospital in-patients: a prospective nested case control study. Int J Heal Policy Manag. 2019; 8(5): 300–306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166. Sayah DN, Asaad K, Hanssens JM, Giraudet G, Faubert J.. Myopes show greater visually induced postural responses than emmetropes. Invest Ophthalmol Vis Sci. 2016; 57(2): 551–556. [DOI] [PubMed] [Google Scholar]
- 167. Rosen R, Lundstrom L, Unsbo P.. Sign-dependent sensitivity to peripheral defocus for myopes due to aberrations. Invest Ophthalmol Vis Sci. 2012; 53(11): 7176–7182. [DOI] [PubMed] [Google Scholar]
- 168. Radhakrishnan H, Pardhan S, Calver RI, O'Leary DJ. Effect of positive and negative defocus on contrast sensitivity in myopes and non-myopes. Vis Res. 2004; 44(16): 1869–1878. [DOI] [PubMed] [Google Scholar]
- 169. Radhakrishnan H, Pardhan S, Calver RI, O'Leary DJ. Unequal reduction in visual acuity with positive and negative defocusing lenses in myopes. Optom Vis Sci. 2004; 81(1): 14–17. [DOI] [PubMed] [Google Scholar]
- 170. Bullimore MA, Gilmartin B.. Retinal eccentricity and the accommodative response. Am J Optom Physiol Opt. 1987; 64(8): 644–645. [PubMed] [Google Scholar]
- 171. Gu YC, Legge GE.. Accommodation to stimuli in peripheral vision. J Opt Soc Am A. 1987; 4(8): 1681–1687. [DOI] [PubMed] [Google Scholar]
- 172. Hartwig A, Charman WN, Radhakrishnan H.. Accommodative response to peripheral stimuli in myopes and emmetropes. Ophthalmic Physiol Opt. 2011; 31(1): 91–99. [DOI] [PubMed] [Google Scholar]
- 173. Maiello G, Walker L, Bex PJ, Vera-Diaz FA.. Blur perception throughout the visual field in myopia and emmetropia. J Vis. 2017; 17(5): 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174. Rosenfield M, Abraham-Cohen JA.. Blur sensitivity in myopes. Optom Vis Sci. 1999; 76(5): 303–307. [DOI] [PubMed] [Google Scholar]
- 175. Kerber K, Thorn F, Bex PJ, Vera-Diaz FA.. Peripheral awareness and the effect of central attentional load in myopia. Optom Vis Sci 2014; 91: E-abstract 145175. [Google Scholar]
- 176. Schmid KL, Robert Iskander D, Li RWH, Edwards MH, Lew JKF. Blur detection thresholds in childhood myopia: single and dual target presentation. Vision Res. 2002; 42(2): 239–247. [DOI] [PubMed] [Google Scholar]
- 177. Labhishetty V, Chakraborty A, Bobier WR.. Is blur sensitivity altered in children with progressive myopia? Vision Res. 2019; 154: 142–153. [DOI] [PubMed] [Google Scholar]
- 178. Rosenfield M, Hong SE, George S.. Blur adaptation in myopes. Optom Vis Sci. 2004; 81(9): 657–662. [DOI] [PubMed] [Google Scholar]
- 179. McGonigle C, van der Linde I, Pardhan S, Engel SA, Mallen EAH, Allen PM.. Myopes experience greater contrast adaptation during reading. Vision Res. 2016; 121: 1–9. [DOI] [PubMed] [Google Scholar]
- 180. Cufflin MP, Mankowska A, Mallen EAH.. Effect of blur adaptation on blur sensitivity and discrimination in emmetropes and myopes. Invest Ophthalmlogy Vis Sci. 2007; 48(6): 2932–2939. [DOI] [PubMed] [Google Scholar]
- 181. Wang B, Ciuffreda KJ, Vasudevan B.. Effect of blur adaptation on blur sensitivity in myopes. Vision Res. 2006; 46(21): 3634–3641. [DOI] [PubMed] [Google Scholar]
- 182. Venkataraman AP, Winter S, Unsbo P, Lundstrom L.. Blur adaptation: contrast sensitivity changes and stimulus extent. Vision Res. 2015; 110: 100–106. [DOI] [PubMed] [Google Scholar]
- 183. Schaeffel F. Myopia: what is old and what is new ? Optom Vis Sci. 2016; 93(9):1022–1030. [DOI] [PubMed] [Google Scholar]
- 184. Wallman J, Gottlieb MD, Rajaram V, Fugate-Wentzek LA.. Local retinal regions control local eye growth and myopia. Science. 1987; 237(4810): 73–77. [DOI] [PubMed] [Google Scholar]
- 185. Smith EL, Ramamirtham R, Qiao-Grider Y, et al.. Effects of foveal ablation on emmetropization and form-deprivation myopia. Invest Ophthalmol Vis Sci. 2007; 48(9): 3914–3922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 186. Huang J, Hung LF, Smith EL.. Effects of foveal ablation on the pattern of peripheral refractive errors in normal and form-deprived infant rhesus monkeys (Macaca mulatta). Invest Ophthalmol Vis Sci. 2011; 52(9): 6428–6434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187. Smith EL, Hung LF, Huang J, Arumugam B.. Effects of local myopic defocus on refractive development in monkeys. Optom Vis Sci. 2013; 90(11): 1176–1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188. Smith EL, Hung LF.. The role of optical defocus in regulating refractive development in infant monkeys. Vision Res. 1999; 39(8): 1415–1435. [DOI] [PubMed] [Google Scholar]
- 189. Hirasawa K, Shoji N.. Effect of optical defocus on the kinetic perimetry in young myopic participants. Curr Eye Res. 2015; 40(8): 847–852. [DOI] [PubMed] [Google Scholar]
- 190. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012; 31(6): 622–660. [DOI] [PubMed] [Google Scholar]
- 191. Chin MP, Chu PHW, Cheong AMY, Chan HHL.. Human electroretinal responses to grating patterns and defocus changes by global flash multifocal electroretinogram. PLoS One. 2015; 10(4): 1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192. Lundström L, Mira-Agudelo A, Artal P.. Peripheral optical errors and their change with accommodation differ between emmetropic and myopic eyes. J Vis. 2009; 9(6): 17.1–11. [DOI] [PubMed] [Google Scholar]
- 193. Mathur A, Atchison DA, Charman WN.. Effect of accommodation on peripheral ocular aberrations. J Vis. 2009; 9(2009): 1–11. [DOI] [PubMed] [Google Scholar]
- 194. Hartwig A, Charman WN, Radhakrishnan H.. Accommodative response to peripheral stimuli in myopes and emmetropes. Ophthalmic Physiol Opt. 2011; 31(1): 91–99. [DOI] [PubMed] [Google Scholar]
- 195. Vera-Diaz FA, McGraw P V, Strang NC, Whitaker D.. A psychophysical investigation of ocular expansion in human eyes. Invest Ophthalmol Vis Sci. 2005; 46(2): 758–763. [DOI] [PubMed] [Google Scholar]
- 196. Ehsaei A, Chisholm CM, Pacey IE, Mallen EAH.. Visual performance fall-off with eccentricity in myopes versus emmetropes. J Optom. 2013; 6(1): 36–44. [Google Scholar]
- 197. Chui TYP, Yap MKH, Chan HHL, Thibos LN.. Retinal stretching limits peripheral visual acuity in myopia. Vision Res. 2005; 45(5): 593–605. [DOI] [PubMed] [Google Scholar]
- 198. Atchison DA, Schmid KL, Pritchard N.. Neural and optical limits to visual performance in myopia. Vision Res. 2006; 46(21): 3707–3722. [DOI] [PubMed] [Google Scholar]
- 199. Ghosh A, Zheleznyak L, Barbot A, Jung HW, Yoon G.. Neural adaptation to peripheral blur in myopes and emmetropes. Vision Res. 2017; 132: 69–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200. Rosén R, Lundström L, Unsbo P.. Sign-dependent sensitivity to peripheral defocus for myopes due to aberrations. Invest Ophthalmol Vis Sci. 2012; 53(11): 7176–7182. [DOI] [PubMed] [Google Scholar]
- 201. Abraham-Cohen JA. Blur sensitivity in myopes. Optom Vis Sci. 1999; 76(5): 303–307. [DOI] [PubMed] [Google Scholar]
- 202. Vasudevan B, Ciuffreda KJ, Wang B.. Objective blur thresholds in free space for different refractive groups. Curr Eye Res. 2006; 31(2): 111–118. [DOI] [PubMed] [Google Scholar]
- 203. Rosenfield M, Hong SE, George S.. Blur adaptation in myopes. Optom Vis Sci. 2004; 81(9): 657–662. [DOI] [PubMed] [Google Scholar]
- 204. Blakemore C, Campbell FW.. On the existence of neurones in the human visual system selectively sensitive to the orientation and size of retinal images. J Physiol. 1969; 203(1): 237–260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 205. Georgeson MA, Georgeson JM.. Facilitation and masking of briefly presented gratings: time-course and contrast dependence. Vision Res. 1987; 27(3): 369–379. [DOI] [PubMed] [Google Scholar]
- 206. Magnussen S, Greenlee MW.. Marathon adaptation to spatial contrast: saturation in sight. Vision Res. 1985; 25(10): 1409–1411. [DOI] [PubMed] [Google Scholar]
- 207. Schaeffel F. Myopia: the importance of seeing fine detail. Curr Biol. 2006; 16(7): R257–R259. [DOI] [PubMed] [Google Scholar]
- 208. McGonigle C, van der Linde I, Pardhan S, Engel SA, Mallen EAH, Allen PM.. Myopes experience greater contrast adaptation during reading. Vision Res. 2016; 121: 1–9. [DOI] [PubMed] [Google Scholar]
- 209. Yeo ACH, Atchison DA, Schmid KL.. Effect of text type on near work-induced contrast adaptation in myopic and emmetropic young adults. Invest Ophthalmol Vis Sci. 2013; 54(2): 1478–1483. [DOI] [PubMed] [Google Scholar]
- 210. Ohlendorf A, Schaeffel F.. Contrast adaptation induced by defocus - a possible error signal for emmetropization? Vision Res. 2009; 49(2): 249–256. [DOI] [PubMed] [Google Scholar]
- 211. Collins MJ, Buehren T, Iskander DR.. Retinal image quality, reading and myopia. Vision Res. 2006; 46(1-2): 196–215. [DOI] [PubMed] [Google Scholar]
- 212. Majaj NJ, Pelli DG, Kurshan P, Palomares M.. The role of spatial frequency channels in letter identification. Vision Res. 2002; 42(9): 1165–1184. [DOI] [PubMed] [Google Scholar]
- 213. Bour LJ. The influence of the spatial distribution of a target on the dynamic response and fluctuations of the accommodation of the human eye. Vision Res. 1981; 21(8): 1287–1296. [DOI] [PubMed] [Google Scholar]
- 214. Charman WN, Tucker J.. Dependence of accommodation response on the spatial frequency spectrum of the observed object. Vision Res. 1977; 17(1): 129–139. [DOI] [PubMed] [Google Scholar]
- 215. Owens DA. A comparison of accommodative responsiveness and contrast sensitivity for sinusoidal gratings. Vision Res. 1980; 20(2): 159–167. [DOI] [PubMed] [Google Scholar]
- 216. Taylor J, Charman WN, O'Donnell C, Radhakrishnan H. Effect of target spatial frequency on accommodative response in myopes and emmetropes. J Vision. 2009; 9(1): 16 1-14. [DOI] [PubMed] [Google Scholar]
- 217. Radhakrishnan H, Hartwig A, Charman WN, Llorente L.. Accommodation response to Chinese and Latin characters in Chinese-illiterate young adults. Clin Exp Optom. 2015; 98(6): 527–534. [DOI] [PubMed] [Google Scholar]
- 218. Yeo ACH, Atchison DA, Schmid KL.. Children's accommodation during reading of Chinese and English texts. Optom Vis Sci. 2013; 90(2): 156–163. [DOI] [PubMed] [Google Scholar]
- 219. Wilson BJ, Decker KE, Roorda A.. Monochromatic aberrations provide an odd-error cue to focus direction. J Opt Soc Am A Opt Image Sci Vis. 2002; 19(5): 833–839. [DOI] [PubMed] [Google Scholar]
- 220. Thibos LN, Bradley A, Liu T, Lopez-Gil N.. Spherical aberration and the sign of defocus. Optom Vis Sci. 2013; 90(11): 1284–1291. [DOI] [PubMed] [Google Scholar]
- 221. Brunette I, Bueno JM, Parent M, Hamam H, Simonet P.. Monochromatic aberrations as a function of age, from childhood to advanced age. Invest Ophthalmol Vis Sci. 2003; 44(12): 5438–5446. [DOI] [PubMed] [Google Scholar]
- 222. Mathur A, Atchison DA, Charman WN.. Myopia and peripheral ocular aberrations. J Vision. 2009; 9(10): 15. [DOI] [PubMed] [Google Scholar]
- 223. Radhakrishnan H, Charman WN.. Age-related changes in ocular aberrations with accommodation. J Vision. 2007; 7(7): 11 1-21. [DOI] [PubMed] [Google Scholar]
- 224. Seidemann A, Schaeffel F.. Effects of longitudinal chromatic aberration on accommodation and emmetropization. Vision Res. 2002; 42(21): 2409–2417. [DOI] [PubMed] [Google Scholar]
- 225. Autrusseau F, Thibos L, Shevell SK.. Chromatic and wavefront aberrations: L-, M- and S-cone stimulation with typical and extreme retinal image quality. Vision Res. 2011; 51(21-22): 2282–2294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226. Rucker F. Monochromatic and white light and the regulation of eye growth. Exp Eye Res. 2019; 184: 172–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 227. Rucker FJ. The role of luminance and chromatic cues in emmetropisation. Ophthalmic Physiol Opt. 2013; 33(3): 196–214. [DOI] [PubMed] [Google Scholar]
- 228. Rucker FJ, Kruger PB.. Cone contributions to signals for accommodation and the relationship to refractive error. Vision Res. 2006; 46(19): 3079–3089. [DOI] [PubMed] [Google Scholar]
- 229. Rosenfield M, Wong NN, Solan HA.. Nearwork distances in children. Ophthalmic Physiol Opt. 2001; 21(1): 75–76. [DOI] [PubMed] [Google Scholar]
- 230. Quek TPL, Chua CG, Chong CS, et al.. Prevalence of refractive errors in teenage high school students in Singapore. Ophthalmic Physiol Opt. 2004; 24(1): 47–55. [DOI] [PubMed] [Google Scholar]
- 231. Wang Y, Bao J, Ou L, Thorn F, Lu F.. Reading behavior of emmetropic schoolchildren in China. Vision Res. 2013; 86: 43–51. [DOI] [PubMed] [Google Scholar]
- 232. Charman WN. Aniso-accommodation as a possible factor in myopia development. Ophthalmic Physiol Opt. 2004; 24(5): 471–479. [DOI] [PubMed] [Google Scholar]
- 233. Bao J, Drobe B, Wang Y, Chen K, Seow EJ, Lu F.. Influence of near tasks on posture in myopic Chinese schoolchildren. Optom Vis Sci. 2015; 92(8): 908–915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234. Flitcroft DI, Judge SJ, Morley JW.. Binocular interactions in accommodation control: effects of anisometropic stimuli. J Neurosci. 1992; 12(1): 188–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 235. Koh LH, Charman WN.. Accommodative responses to anisoaccommodative targets. Ophthalmic Physiol Opt. 1998; 18(3): 254–262. [PubMed] [Google Scholar]
- 236. Hartwig A, Gowen E, Charman WN, Radhakrishnan H.. Binocular saccades in myopes and emmetropes. Optom Vis Sci. 2013; 90(9): 980–987. [DOI] [PubMed] [Google Scholar]
- 237. Hartwig A, Gowen E, Charman WN, Radhakrishnan H.. Analysis of head position used by myopes and emmetropes when performing a near-vision reading task. Vision Res. 2011; 51(14): 1712–1717. [DOI] [PubMed] [Google Scholar]
- 238. Hartwig A, Gowen E, Charman WN, Radhakrishnan H.. Working distance and eye and head movements during near work in myopes and non-myopes. Clin Exp Optom. 2011; 94(6): 536–544. [DOI] [PubMed] [Google Scholar]
- 239. Rose KA, French AN, Morgan IG.. Environmental factors and myopia: Paradoxes and prospects for prevention. Asia-Pacific J Ophthalmol. 2016; 5(6): 403–410. [DOI] [PubMed] [Google Scholar]
- 240. Guo Y, Liu LJ, Xu L, et al.. Myopic shift and outdoor activity among primary school children: one-year follow-up study in Beijing. PLoS One. 2013; 8(9): e75260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 241. Pärssinen O, Lyyra A.. Myopia and myopic progression among school children: a three-year follow-up study. Invest Ophthalmol Vis Sci. 1993; 34(9): 2794–2802. [PubMed] [Google Scholar]
- 242. Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K.. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2007; 48(8): 3524–3532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 243. Rose KA, Morgan IG, Ip J, et al.. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008; 115(8): 1279–1285. [DOI] [PubMed] [Google Scholar]
- 244. Dirani M, Tong L, Gazzard G, et al.. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol. 2009; 93(8): 997–1000. [DOI] [PubMed] [Google Scholar]
- 245. Wu P-C, Tsai C-L, Hu C-H, Yang Y-H. Effects of outdoors activities on myopia among rural school children in Taiwan. Ophthalmic Epidemiol. 2010; 17(5): 338–342. [DOI] [PubMed] [Google Scholar]
- 246. Guggenheim JA, Northstone K, McMahon G, et al.. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Investig Ophthalmol Vis Sci. 2012; 53(6): 2856–2865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 247. Wu PC, Tsai CL, Wu HL, Yang YH, Kuo HK.. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013; 120(5): 1080–1085. [DOI] [PubMed] [Google Scholar]
- 248. Lin Z, Vasudevan B, Jhanji V, et al.. Near work, outdoor activity, and their association with refractive error. Optom Vis Sci. 2014; 91(4): 376–382. [DOI] [PubMed] [Google Scholar]
- 249. Jin JX, Hua WJ, Jiang X, et al.. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast china: The Sujiatun Eye Care Study. BMC Ophthalmol. 2015; 15: 73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 250. Wu LJ, Wang YX, You QS, et al.. Risk factors of myopic shift among primary school children in Beijing, China: a prospective study. Int J Med Sci. 2015; 12(8): 633–638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251. He M, Xiang F, Zeng Y, et al.. Effect of time spent outdoors at school on the development of myopia among children in China a randomized clinical trial. JAMA Opthalmology. 2015; 314(11): 1142–1148. [DOI] [PubMed] [Google Scholar]
- 252. Shah RL, Huang Y, Guggenheim JA, Williams C.. Time outdoors at specific ages during early childhood and the risk of incident myopia. Invest Ophthalmol Vis Sci. 2017; 58(2): 1158–1166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 253. Guo Y, Liu LJ, Tang P, et al.. Outdoor activity and myopia progression in 4-year follow-up of Chinese primary school children: The Beijing Children Eye Study. PLoS One. 2017; 12(4): 1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 254. Saxena R, Vashist P, Tandon R, et al.. Incidence and progression of myopia and associated factors in urban school children in Delhi: The North India Myopia Study (NIM Study). Pan C-W, ed. PLoS One. 2017; 12(12): e0189774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 255. Sánchez-Tocino H, Villanueva Gómez A, Gordon Bolaños C, et al.. The effect of light and outdoor activity in natural lighting on the progression of myopia in children. J Fr Ophtalmol. 2019; 42(1): 2–10. [DOI] [PubMed] [Google Scholar]
- 256. Guo Y, Liu L, Lv Y, et al.. Outdoor jogging and myopia progression in school children from rural Beijing: the Beijing Children Eye Study. Transl Vis Sci Technol. 2019; 8(3): 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 257. Huang PC, Hsiao YC, Tsai CY, et al.. Protective behaviours of near work and time outdoors in myopia prevalence and progression in myopic children: a 2-year prospective population study. Br J Ophthalmol. 2020; 104(7): 956–961. [DOI] [PubMed] [Google Scholar]
- 258. Hoffman DM, Banks MS.. Focus information is used to interpret binocular images. J Vision. 2010; 10(5): 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 259. Mather G. The use of image blur as a depth cue. Perception. 1997; 26(9): 1147–1158. [DOI] [PubMed] [Google Scholar]
- 260. Mather G, Smith DRR.. Blur discrimination and its relation to blur-mediated depth perception. Perception. 2002; 31(10): 1211–1219. [DOI] [PubMed] [Google Scholar]
- 261. Seidel D, Gray LS, Heron G.. The effect of monocular and binocular viewing on the accommodation response to real targets in emmetropia and myopia. Optom Vis Sci. 2005; 82(4): 279–285. [DOI] [PubMed] [Google Scholar]
- 262. Vera-Diaz FA, Bex PJ, Ferreira A, Kosovicheva A.. Binocular temporal visual processing in myopia. J Vision. 2018; 18(11): 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 263. Chirre E, Prieto PM, Schwarz C, Artal P.. Night myopia is reduced in binocular vision. J Vision. 2016; 16(8): 1–10. [DOI] [PubMed] [Google Scholar]
- 264. Huang CT, Satou T, Niida T.. Effect of pupil size and binocular viewing on accommodative gain in emmetropia and myopia. J Binocul Vis Ocul Motil. 2020; 70(3): 103–108. [DOI] [PubMed] [Google Scholar]
- 265. Mutti DO, Jones LA, Moeschberger ML, Zadnik K.. AC/A ratio, age, and refractive error in children. Invest Ophthalmol Vis Sci. 2000; 41(9): 2469–2478. [PubMed] [Google Scholar]
- 266. Mutti DO, Mitchell GL, Jones-Jordan LA, et al.. The response AC/A ratio before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2017; 58(3): 1594–1602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 267. Jorge J, de Almeida JB, Parafita MA, Jorge Jorge JB de A. Binocular vision changes in university students: a 3-year longitudinal study. Optom Vis Sci. 2008; 85(10): E999–E1006. [DOI] [PubMed] [Google Scholar]
- 268. Sreenivasan V, Irving EL, Bobier WR.. Effect of heterophoria type and myopia on accommodative and vergence responses during sustained near activity in children. Vision Res. 2012; 57: 9–17. [DOI] [PubMed] [Google Scholar]
- 269. Gifford KL, Gifford P, Hendicott PL, Schmid KL.. Zone of clear single binocular vision in myopic orthokeratology. Eye Contact Lens. 2020; 46(2): 82–90. [DOI] [PubMed] [Google Scholar]
- 270. Madrid-Costa D, Ruiz-Alcocer J, Radhakrishnan H, Ferrer-Blasco T, Montés-Micó R.. Changes in accommodative responses with multifocal contact lenses: a pilot study. Optom Vis Sci. 2011; 88(11): 1309–1316. [DOI] [PubMed] [Google Scholar]
- 271. Tarrant J, Severson H, Wildsoet CF.. Accommodation in emmetropic and myopic young adults wearing bifocal soft contact lenses. Ophthalmic Physiol Opt. 2008; 28(1): 62–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 272. Kang P, Wildsoet CF.. Acute and short-term changes in visual function with multifocal soft contact lens wear in young adults. Cont Lens Anterior Eye. 2016; 39(2): 133–140. [DOI] [PubMed] [Google Scholar]
- 273. Ozkan J, Fedtke C, Chung J, Thomas V, Bakaraju RC.. Short-term adaptation of accommodative responses in myopes fitted with multifocal contact lenses. Eye Contact Lens. 2018; 44: S30–S37. [DOI] [PubMed] [Google Scholar]
- 274. Price H, Allen PM, Radhakrishnan H, et al.. The Cambridge Anti-myopia Study: variables associated with myopia progression. Optom Vis Sci. 2013; 90(11): 1274–1283. [DOI] [PubMed] [Google Scholar]
- 275. Theagarayan B, Radhakrishnan H, Allen PM, Calver RI, Rae SM, O'Leary DJ. The effect of altering spherical aberration on the static accommodative response. Ophthalmic Physiol Opt. 2009; 29(1): 65–71. [DOI] [PubMed] [Google Scholar]
- 276. Gifford K, Gifford P, Hendicott PL, Schmid KL.. Near binocular visual function in young adult orthokeratology versus soft contact lens wearers. Cont Lens Anterior Eye. 2017; 40(3): 184–189. [DOI] [PubMed] [Google Scholar]
- 277. Aller TA, Liu M, Wildsoet CF.. Myopia control with bifocal contact lenses: a randomized clinical trial. Optom Vis Sci. 2016; 93(4): 344–352. [DOI] [PubMed] [Google Scholar]
- 278. Gong CR, Troilo D, Richdale K.. Accommodation and phoria in children wearing multifocal contact lenses. Optom Vis Sci. 2017; 94(3): 353–360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 279. Anstice NS, Phillips JR.. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology. 2011; 118(6): 1152–1161. [DOI] [PubMed] [Google Scholar]
- 280. Chamberlain P, Peixoto-De-Matos SC, Logan NS, Ngo C, Jones D, Young G.. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci. 2019; 96(8): 556–567. [DOI] [PubMed] [Google Scholar]
- 281. Ruiz-Pomeda A, Pérez-Sánchez B, Cañadas P, Prieto-Garrido FL, Gutiérrez-Ortega R, Villa-Collar C.. Binocular and accommodative function in the controlled randomized clinical trial MiSight Assessment Study Spain (MASS). Graefes Arch Clin Exp Ophthalmol. 2019; 257(1): 207–215. [DOI] [PubMed] [Google Scholar]
- 282. Tilia D, Sha J, Thomas V, Bakaraju RC.. Vision performance and accommodative/binocular function in children wearing prototype extended depth-of-focus contact lenses. Eye Contact Lens. 2019; 45(4): 260–270. [DOI] [PubMed] [Google Scholar]
- 283. Walline JJ, Lindsley KB, Vedula SS, et al.. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020; 12: CD004916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 284. Gwiazda J, Hyman L, Hussein M, et al.. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci. 2003; 44(4): 1492–1500. [DOI] [PubMed] [Google Scholar]
- 285. Chen Y, Drobe B, Zhang C, et al.. Accommodation is unrelated to myopia progression in Chinese myopic children. Sci Rep. 2020; 10(1): 12056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286. Labhishetty V, Bobier WR.. Are high lags of accommodation in myopic children due to motor deficits? Vision Res. 2017; 130: 9–21. [DOI] [PubMed] [Google Scholar]
- 287. Chen AH, O'Leary DJ. Are there age differences in the accommodative response curve between 3 and 14 years of age? Ophthalmic Physiol Opt. 2002; 22(2): 119–125. [DOI] [PubMed] [Google Scholar]
- 288. Han X, Xu D, Ge W, Wang Z, Li X, Liu W.. A comparison of the effects of orthokeratology lens, Medcall lens, and ordinary frame glasses on the accommodative response in myopic children. Eye Contact Lens. 2018; 44(4): 268–271. [DOI] [PubMed] [Google Scholar]
- 289. Ma MM, Shi J, Li N, Scheiman M, Chen X.. Effect of vision therapy on accommodative lag in myopic children: a randomized clinical trial. Optom Vis Sci. 2019; 96(1): 17–26. [DOI] [PubMed] [Google Scholar]
- 290. Bullimore MA, Gilmartin B, Royston JM.. Steady-state accommodation and ocular biometry in late-onset myopia. Doc Ophthalmol. 1992; 80(2): 143–155. [DOI] [PubMed] [Google Scholar]
- 291. Jiang BC, Morse SE.. Oculomotor functions and late-onset myopia. Ophthalmic Physiol Opt. 1999; 19(2): 165–172. [DOI] [PubMed] [Google Scholar]
- 292. Rosenfield M, Desai R, Portello JK.. Do progressing myopes show reduced accommodative responses? Optom Vis Sci. 2002; 79(4): 268–273. [DOI] [PubMed] [Google Scholar]
- 293. Seidel D, Gray LS, Heron G.. Retinotopic accommodation responses in myopia. Invest Ophthalmol Vis Sci. 2003; 44(3): 1035–1041. [DOI] [PubMed] [Google Scholar]
- 294. Hazel CA, Cox MJ, Strang NC.. Wavefront aberration and its relationship to the accommodative stimulus-response function in myopic subjects. Optom Vis Sci. 2003; 80(2): 151–158. [DOI] [PubMed] [Google Scholar]
- 295. Schmid KL, Hilmer KS, Lawrence RA, Loh SY, Morrish LJ, Brown B.. The effect of common reductions in letter size and contrast on accommodation responses in young adult myopes and emmetropes. Optom Vis Sci. 2005; 82(7): 602–611. [DOI] [PubMed] [Google Scholar]
- 296. Day M, Strang NC, Seidel D, Gray LS, Mallen EA.. Refractive group differences in accommodation microfluctuations with changing accommodation stimulus. Ophthalmic Physiol Opt. 2006; 26(1): 88–96. [DOI] [PubMed] [Google Scholar]
- 297. Sreenivasan V, Aslakson E, Kornaus A, Thibos LN.. Retinal image quality during accommodation in adult myopic eyes. Optom Vis Sci. 2013; 90(11): 1292–1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 298. Rosenfield M, Gilmartin B.. Effect of a near-vision task on the response AC/A of a myopic population. Ophthalmic Physiol Opt. 1987; 7(3): 225–233. [PubMed] [Google Scholar]
- 299. Goss DA. Clinical accommodation and heterophoria findings preceding juvenile onset of myopia. Optom Vis Sci. 1991; 68(2): 110–116. [DOI] [PubMed] [Google Scholar]
- 300. Jiang BC. Parameters of accommodative and vergence systems and the development of late-onset myopia. Invest Ophthalmol Vis Sci. 1995; 36(8): 1737–1742. [PubMed] [Google Scholar]
- 301. Gwiazda J, Grice K, Thorn F.. Response AC/A ratios are elevated in myopic children. Ophthalmic Physiol Opt. 1999; 19(2): 173–179. [DOI] [PubMed] [Google Scholar]
- 302. Chen JC, Schmid KL, Brown B, Edwards MH, Yu BS, Lew JK.. AC/A ratios in myopic and emmetropic Hong Kong children and the effect of timolol. Clin Exp Optom. 2003; 86(5): 323–330. [DOI] [PubMed] [Google Scholar]
- 303. Zadnik K, Sinnott LT, Cotter SA, et al.. Prediction of juvenile-onset myopia. JAMA Ophthalmol. 2015; 133(6): 683–689. [DOI] [PMC free article] [PubMed] [Google Scholar]