

Abstract
A general psychopathology (‘p’) factor captures transdiagnostic features of mental illness; however, the meaning of the p factor remains unclear. Regulatory focus theory postulates that individuals regulate goal pursuit either by maximizing gains (promotion) or minimizing losses (prevention). As maladaptive goal pursuit has been associated with multiple categorical disorders, we examined whether individual differences in promotion and prevention goal pursuit are associated with p as well as internalizing- and externalizing-specific factors using structural equation modeling of data from 1330 volunteers aged 18–22. Unsuccessful attainment of promotion and prevention goals was related to increased levels of p. Over and above relations with the p factor, unsuccessful attainment of promotion goals was associated with higher internalizing-specific psychopathology, whereas unsuccessful attainment of prevention goals was related to higher externalizing-specific psychopathology. These associations also were separable from related personality traits. After controlling for sex differences in the composition of the psychopathology factors, there were no sex differences in the relations between promotion and prevention goal pursuit and p and specific internalizing and externalizing factors. These findings suggest higher general psychopathology reflects poorer overall self-regulation of goal pursuit and that maladaptive promotion and prevention orientations also are associated with internalizing- and externalizing-specific psychopathology, respectively.
Keywords: regulatory focus, self-regulation, general psychopathology, p factor, internalizing, externalizing
Introduction
Increasing research has encouraged a shift toward transdiagnostic models of the structure of psychopathology. Factor-analytic studies have found that many different disorders may be manifestations of a smaller number of transdiagnostic latent factors (Achenbach and Edelbrock, 1981; Krueger and Markon, 2011, 2006): an “internalizing” liability to depression and anxiety; an “externalizing” liability to antisocial, attention deficit hyperactivity disorder, and substance-use disorders; and a “thought disorder” liability to schizophrenia, mania, and obsessive compulsive disorder. These three transdiagnostic factors also are correlated (Wright et al., 2013), which led to the identification of a general psychopathology (‘p’) factor (Caspi et al., 2014; Lahey et al., 2012). The p factor captures shared variation among internalizing, externalizing, and thought disorders, accounting for comorbidity across diagnostic categories. The p factor has been identified in diverse samples (Caspi and Moffitt, 2018) and captures age-of-onset, severity, and diversity of psychiatric symptoms across the lifespan (Caspi et al., 2020).
Recent neuroimaging research has examined the neural correlates of the p factor to better understand possible transdiagnostic mechanisms of psychopathology. Individuals with high p have shown structural and functional alterations within the visual association cortex and cerebello-thalamo-cerebral-cortical circuit (Elliott et al., 2018; Moberget et al., 2019; Romer et al., 2019, 2018), both of which are involved in executive control, the ability to carry out goal-directed behavior using higher-order mental and cognitive processes. The visual association cortex is involved in selection of incoming relevant and suppression of irrelevant visual information (Chadick and Gazzaley, 2011; Karten et al., 2013), which is integral to goal-directed behavior. The cerebello-thalamo-cerebral-cortical circuit is involved in updating internal models of thoughts and emotions based on external feedback as a form of error monitoring (Ito, 2008, 1993), which also underlies executive control.
These neuroimaging findings are consistent with psychological theories of the meaning of the p factor inasmuch as dysfunctions in goal pursuit underlie a wide range of maladaptive behaviors. Indeed, the Cybernetic Theory posits that goal pursuit dysfunctions may underlie all forms of psychopathology (DeYoung and Krueger, 2018). The p factor also has been hypothesized to reflect executive dysfunction (Snyder et al., 2019), emotion dysregulation (Carver et al., 2017), and disordered thinking (i.e., rumination, cognitive distortions, intrusive thoughts, etc., Caspi & Moffitt, 2018), all of which have been identified in multiple psychiatric disorders (Compas et al., 2017; McTeague et al., 2016; Snyder et al., 2015). Supported by evidence of specific neural correlates of p in executive control circuits, these psychological explanations may point to a more general dysfunction in self-regulation of goal pursuit.
Self-regulation describes the ongoing process of managing personal goal pursuit in the face of internal, interpersonal, and environmental forces that would derail it (Hoyle and Gallagher, 2015). Social-cognitive theories of self-regulation mirror the approach/avoidance conceptualization of animal models, but incorporate advanced abilities for planning, strategy, self-reflection, and abstraction. Such theories typically emphasize higher-order goals that are cross-situational and integrated within the individual’s sense of self (James, 1948). In their ongoing pursuit of personal goals, people continuously compare their actual behaviors with their representations of the kind of person they are striving to become (Carver, 1998; Gollwitzer, 1999; Higgins, 1987). This ongoing self-evaluation has significant repercussions for the individual’s emotional and motivational state, and ultimately, for well-being and psychopathology (Karoly, 1993).
Regulatory focus theory (RFT; Higgins, 1998) is a social-cognitive model of how individuals regulate personal goal pursuit. RFT postulates two independent motivational orientations: promotion, with a focus on maximizing gains; and prevention, with a focus on minimizing losses. A promotion orientation emphasizes hopes, accomplishments, and advancement, which are related to fundamental needs for nurturance (Bowlby, 1969). Goals are viewed as “ideals”, and the strategic emphasis is “making good things happen.” A prevention orientation emphasizes duties, obligations, and responsibilities, which are related to fundamental needs for security (Bowlby, 1969). Goals are viewed as “oughts”, and the strategic emphasis is “keeping bad things from happening.” The term regulatory focus refers to a cognitive-motivational state that varies across individuals (construed as a dispositional variable) and within individuals (on a momentary basis across situations).
Individual differences in regulatory focus are presumed to emerge largely from early socialization experiences, particularly contingent interactions with parents (Manian et al., 2006). According to RFT, childhood exposure to different patterns of parenting behaviors leads to the emergence of individual differences in self-regulatory orientations. For example, parenting behaviors emphasizing accomplishments (e.g., showing affection for desired child behaviors, encouraging children to overcome difficulties, setting up opportunities to engage in rewarding activities) lead to greater promotion goal success. In contrast, parenting behaviors emphasizing safety, rules, and responsibilities (e.g., childproofing the house, training children to be alert to dangers, teaching children to mind their manners) lead to greater prevention goal success (Manian et al., 2006).
How might dysfunction in goal pursuit be associated with the p factor? There are at least two levels of analysis at which self-regulation of goal pursuit might be relevant to identifying the dysfunctions captured by p. First, a specific dysfunction of neural circuitry associated with p (e.g., visual association cortex and cerebello-thalamo-cortical circuit) could lead to disturbances in effective goal pursuit and subsequent consequences for affect and behavior. Indeed, two fMRI studies found significant activation in the visual association cortex during promotion and prevention goal priming (Detloff et al., 2020; Strauman et al., 2013), supporting a possible association between regulatory focus and p.
Second, and more generally, self-regulation represents an umbrella construct encompassing a family of related dysfunctions that increase generalized risk for psychopathology. Because self-regulation is a proximal locus for the influences of distal neural, behavioral, and environmental factors on behavior (Strauman et al., 2010), RFT suggests several possible dysfunctions leading to maladaptive promotion and/or prevention (Strauman, 2017): e.g., dysfunction of knowledge accessibility and/or short-term memory capacity/fluidity; biased comparisons between observed behaviors and active goals; problematic reinforcement history leading to unrealistic goals; and social skills deficits resulting in poor goal attainment. Each of those dysfunctions could be associated with p separately from any association with specific forms of psychopathology.
In the current study, we examined the relationship between self-regulatory orientations, specifically self-reported individual differences in perceived success in attaining promotion and prevention goals and their associated socialization histories, and transdiagnostic psychopathology factors in 1330 volunteers aged 18–22. Previously, we identified a bi-factor model in this sample, which included a general p factor accounting for shared variation among psychiatric symptoms, and two specific factors accounting for the variation unique to internalizing and to externalizing disorders (Romer et al., 2018). Here, we build upon this bi-factor model by using structural equation modeling (SEM) to examine associations between self-regulatory orientations and general p and specific internalizing and externalizing factors. We had two questions: 1) Are dysfunctions in promotion and prevention related to the p factor?; and 2) Are dysfunctions in promotion and prevention also related to specific internalizing and externalizing psychopathology over and above associations with p?.
We hypothesized that the p factor would be related to less self-perceived success for both promotion and prevention goals. Hypotheses about the relations between the specific factors and self-regulatory orientations are less clear, given that less is known about the meaning of internalizing- and externalizing-specific psychopathology when p is partialled out; therefore, we treated those analyses as exploratory. Associations between transdiagnostic factors and promotion and prevention socialization histories also were treated as exploratory as the psychometric properties of our measure of these constructs have not been established. We also tested whether the relations between self-regulatory orientations and psychopathology factors are equivalent for men and women, given sex differences in internalizing and externalizing psychopathology (Caspi et al., 2014). Finally, given the overlap between personality traits and psychopathology, we examined whether relations between self-regulatory orientations and transdiagnostic psychopathology factors are separable from the Big Five personality traits.
Materials and Methods
Participants
Data were available from 1330 undergraduates (762 women; mean age: 19.70 +/− 1.25) who had completed the Duke Neurogenetics Study. Participants were recruited from the local university population via flyers and online postings. All participants provided informed consent in accordance with Duke University Medical Center Institutional Review Board guidelines prior to participation. All participants were in good general health and free of the following study conditions: 1) medical diagnoses of cancer, stroke, head injury with loss of consciousness, untreated migraine headaches, diabetes requiring insulin treatment, chronic kidney or liver disease; 2) use of psychotropic, glucocorticoid, or hypolipidemic medication; and 3) conditions affecting cerebral blood flow and metabolism (e.g., hypertension).
Material and Methods
Table 1 provides descriptive statistics for all study variables.
Table 1.
Descriptive Statistics of Demographic, Psychiatric Symptom, and Regulatory Focus Questionnaire Subscales.
| Variables | N | Min | Max | Mean (SD) |
|---|---|---|---|---|
| Demographic | ||||
| Sex (% Female) | 1330 (57.3) | |||
| Race (% Caucasian, AA, Asian, NA, Multiracial, Other) | 1330 (49.8, 11.7, 27.4, 0.2, 7.8, 3.0) | |||
| Ethnicity (% Hispanic) | 1330 (10.3) | |||
| Age | 1330 | 18 | 22 | 19.7 (1.25) |
| IQ | 1328 | 81 | 140 | 121.76 (8.39) |
| Psychiatric Symptom | ||||
| Cannabis Use (e-M.I.N.I.) | 1324 | 0 | 6 | 0.15 (0.62) |
| Alcohol Use (AUDIT) | 1330 | 0 | 34 | 5.26 (4.38) |
| Drug Use (RDU) | 1326 | 0 | 9 | 1.69 (2.33) |
| Antisocial Personality (SRP-SF) | 1330 | 29 | 121 | 48.09 (13.64) |
| Delinquency (SRD) | 903 | 0 | 53 | 5.06 (4.90) |
| Trait Anxiety (STAI-T) | 1328 | 20 | 73 | 38.01 (9.27) |
| Depression (CESD) | 1326 | 0 | 54 | 10.12 (8.31) |
| Depression (MASQ) | 1329 | −1.73 | 4.05 | 0.00 (0.89) |
| Anxiety (MASQ) | 1329 | −0.89 | 8.09 | 0.00 (0.93) |
| Fears/Phobias (e-M.I.N.I.) | 1323 | 0 | 5 | 0.37 (0.98) |
| OCD (e-M.I.N.I.) | 1324 | 0 | 6 | 0.16 (0.68) |
| Psychosis (e-M.I.N.I.) | 1324 | 0 | 6 | 0.06 (0.37) |
| Mania (e-M.I.N.I.) | 1324 | 0 | 9 | 0.34 (1.32) |
| Regulatory Focus | ||||
| RFQ Promotion History | 1323 | 1.00 | 5.00 | 3.92 (0.84) |
| RFQ Prevention History | 1325 | 1.50 | 5.00 | 3.96 (0.67) |
| RFQ Promotion Success | 1330 | 1.83 | 5.00 | 3.81 (0.47) |
| RFQ Prevention Success | 1330 | 1.50 | 5.00 | 3.53 (0.59) |
Note. SD=Standard Deviation; AA=African American; NA=Native American; e-M.I.N.I.=electronic Mini International Neuropsychiatric Interview; AUDIT=Alcohol Use Disorder Identification Test; RDU=Recreational Drug Use Questionnaire; SRP-SF=Self Report of Psychopathy-Short Form; SRD=Self Report of Delinquency Scale; STAI-T=State-Trait Anxiety Inventory-Trait version; CESD=Center for Epidemiological Studies of Depression; MASQ=Mood and Anxiety Symptom Questionnaire; OCD=Obsessive-Compulsive Disorder; RFQ=Regulatory Focus Questionnaire.
Psychiatric Symptoms
As reported in Romer et al. (2018), we assessed the following psychiatric disorders and symptoms using the electronic Mini International Neuropsychiatric Interview (e-M.I.N.I.) and self-report questionnaires: major depression, generalized anxiety disorder, fears and/or phobias, alcohol, cannabis, and other drug use disorders, antisocial personality disorder, delinquency, obsessive compulsive disorder, mania, and psychosis. The e-M.I.N.I. is a short, structured diagnostic interview for DSM-IV and ICD-10 psychiatric disorders (Sheehan et al., 1998). Clinical psychologists, graduate students, and post-baccalaureate research assistants under the supervision of a licensed clinical psychologist conducted interviews (see Supplementary Material for details).
Regulatory Focus
Participants completed a modified version of the Regulatory Focus Questionnaire (RFQ; Higgins et al., 2001), a self-report measure designed to assess individual differences in promotion and prevention orientations. The 22-item questionnaire has four subscales, two that measure individuals’ recollection of their early parental socialization experiences oriented toward a promotion or prevention focus (“history” subscales), and two that measure individuals’ assessment of their experiences attaining promotion- and prevention-related goals (“success” subscales). Participants responded on 5-point scales ranging from “never”/“certainly false” to “very often”/“certainly true,” and item responses within each subscale were averaged to produce four scores: promotion history, prevention history, promotion success, and prevention success (α’s ranged from 0.62–0.79; see Supplementary Material for details).
Measurement Model
The modeling of the structure of psychopathology in 1246 of the 1330 participants has been described previously (Romer et al., 2018). Briefly, we used confirmatory factor analysis to test a bi-factor model, which included a general p factor and specific internalizing, externalizing, and thought disorder factors. The p factor directly loaded on all of the 13 psychiatric symptom indicators; the specific factors each loaded on their respective symptom indicators. All e-M.I.N.I. symptom count indicators were treated as categorical; self-report measures were treated as continuous variables. Consistent with previous models (Caspi et al., 2014; Laceulle et al., 2015), thought disorders were highly subsumed in p. Respecifying the model by removing the specific thought disorder factor resulted in adequate data fit: χ2(55, N=1246)=385.084, CFI=0.943, TLI=0.919, RMSEA=0.069, 90% CI [0.063, 0.076] (Romer et al., 2018) (See Supplementary Material for details).
In the current study, we extended this model to include an additional 84 participants who had not completed the study at the time of Romer et al. (2018). We also conducted a two-group bi-factor model for sex to determine whether the factor loadings were equivalent for men and women. The function “DIFFTEST” in Mplus was used to test the difference between a model with loadings equivalent between the sexes and a model that allowed those loadings to be freely estimated.
Statistical Analyses
To determine the relationships between RFQ subscales and psychiatric symptoms, we conducted the following analyses. First, we examined bivariate correlations between the RFQ subscales, psychiatric symptom measures, and potential confounders of age, dummy-coded sex (female), race (African American, Asian, Other Non-Caucasian), ethnicity (Hispanic), and IQ (Wechsler, 1999). Second, we tested a two-group bi-factor model of the structure of psychopathology and determined whether the model was equivalent for men and women.
Third, we examined relations between the RFQ subscales and general p and specific internalizing and externalizing factors using SEM. Specifically, we conducted three multiple regressions with paths from the RFQ subscales to the general p and specific internalizing and externalizing factors. Demographic variables found to significantly correlate with RFQ subscales or psychiatric symptom measures were included as covariates. We also tested whether the relations between RFQ subscales and transdiagnostic factors varied by sex using a two-group SEM.
Fourth, we examined the relations between RFQ subscales and transdiagnostic psychopathology factors controlling for Big Five personality traits in the SEM using the 240-item NEO Personality Inventory Revised (Costa and McCrae, 1992). This additional analysis is supported by evidence that Big Five traits are correlated with transdiagnostic psychopathology (Caspi et al., 2014; Castellanos-Ryan et al., 2016) and are constructs that overlap with promotion and prevention success (Supplementary Table 1).
All analyses were performed in Mplus version 8.4 (Muthen and Muthen, 1998) using the WLSMV algorithm. We assessed model fit using chi-square, CFI, TLI, and RMSEA. Nonsignificant chi-square tests indicate good model fit; nonetheless, this test is generally overpowered in large sample sizes such as ours. CFI and TLI values > 0.90 indicate adequate fit; RMSEA scores < 0.08 are considered acceptable (Kline, 2015). Given the sample size and number of tests, we report associations significant at p<0.01.
Results
Correlations
Bivariate correlations between RFQ subscales and psychiatric symptoms are shown in Table 2. In general, those with greater externalizing symptoms reported less prevention success while those with greater internalizing symptoms reported less promotion and prevention success. Thought disorder symptoms were weakly related to regulatory focus orientations. Men were more likely to report greater externalizing and psychotic symptoms compared to women, wheras women were more likely to endorse fears/phobias and higher prevention success. Older participants were more likely to report greater substance use and those with higher IQ were less likely to be depressed. There were also differences between the racial groups on endorsement of psychiatric symptoms, but no differences between Hispanic and non-Hispanic individuals. Based on these correlations, we included sex, age, race, and IQ as control variables in all subsequent SEM analyses. The RFQ subscales were correlated with each other, suggesting that all the subscales be included in the same SEM to control for possible overlap.
Table 2.
Bivariate Correlations between Regulatory Focus Subscales, Psychiatric Symptom Measures, and Covariates.
| RFQ Promotion History | RFQ Prevention History | RFQ Promotion Success | RFQ Prevention Success | Sex (0=M; 1=F) | Age | AA | Asian | Other Non-Caucasian | Hispanic | IQ | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Externalizing | |||||||||||
| Cannabis Use | −0.070 | −0.004 | −0.096 | −0.169 | −0.097 | 0.022 | −0.042 | 0.013 | −0.034 | 0.016 | 0.029 |
| Alcohol Use | 0.021 | −0.002 | 0.009 | −0.291 | −0.217 | 0.112 | −0.082 | −0.118 | −0.036 | 0.001 | 0.033 |
| Drug Use | −0.051 | −0.043 | −0.008 | −0.308 | −0.185 | 0.169 | −0.048 | −0.098 | −0.010 | −0.041 | 0.051 |
| Antisocial Behavior | −0.261 | −0.008 | −0.219 | −0.468 | −0.346 | −0.002 | −0.006 | 0.018 | −0.015 | 0.035 | −0.008 |
| Delinquency | −0.139 | −0.007 | −0.069 | −0.390 | −0.205 | 0.053 | 0.054 | −0.065 | −0.046 | −0.012 | 0.007 |
| Internalizing | |||||||||||
| STAI-T Anxiety | −0.373 | −0.039 | −0.560 | −0.237 | 0.051 | −0.067 | 0.034 | 0.124 | −0.001 | −0.004 | −0.077 |
| CESD Depression | −0.326 | −0.043 | −0.465 | −0.217 | 0.061 | −0.073 | 0.101 | 0.047 | 0.029 | −0.015 | −0.102 |
| MASQ Depression | −0.359 | −0.047 | −0.541 | −0.192 | 0.039 | −0.066 | 0.081 | 0.084 | −0.004 | 0.008 | −0.080 |
| MASQ Anxiety | −0.222 | −0.024 | −0.266 | −0.211 | 0.034 | −0.020 | 0.044 | 0.029 | −0.010 | 0.000 | −0.070 |
| (e-M.I.N.I.) | −0.080 | 0.030 | −0.090 | −0.006 | 0.101 | −0.007 | 0.028 | −0.044 | 0.032 | −0.010 | −0.017 |
| Thought | |||||||||||
| OCD | −0.090 | 0.040 | −0.022 | −0.072 | −0.027 | 0.020 | 0.040 | −0.031 | 0.050 | −0.032 | −0.002 |
| Psychosis | −0.059 | 0.044 | −0.008 | −0.018 | −0.111 | 0.037 | 0.025 | −0.052 | 0.036 | −0.036 | −0.032 |
| Mania | −0.086 | 0.038 | −0.060 | −0.160 | −0.018 | −0.023 | 0.035 | −0.026 | 0.067 | −0.031 | −0.002 |
| RFQ Subscales | |||||||||||
| Promotion History | 1 | 0.041 | 0.036 | −0.053 | −0.190 | −0.035 | −0.003 | 0.027 | |||
| Prevention History | 0.069 | 1 | 0.010 | −0.022 | 0.170 | 0.074 | −0.016 | 0.004 | −0.055 | ||
| Promotion Success | 0.355 | 0.078 | 1 | 0.056 | 0.061 | −0.033 | −0.140 | −0.011 | −0.015 | 0.072 | |
| Prevention Success | 0.340 | −0.045 | 0.142 | 1 | 0.171 | 0.082 | −0.021 | −0.110 | 0.047 | −0.031 | 0.027 |
Note. Correlations shown in bold are significant at p<0.001; correlations shown in italics are significant at p<0.01. STAI-T=State-Trait Anxiety Inventory-Trait version; CESD=Center for Epidemiological Studies Depression Scale; MASQ=Mood and Anxiety Symptom Questionnaire; OCD=Obsessive Compulsive Disorder; RFQ=Regulatory Focus Questionnaire; AA=African American. African American, Asian, Other Non-Caucasian, and Hispanic are dummy-coded variables (Caucasian=reference group).
Two-Group Bi-Factor Model
Inspection of modification indices and residuals in the bi-factor model indicated that a few of the symptom indicators had remaining unique variances not captured by the general or specific factors. We added residual correlations between Recreatinal Drug Use (RDU) and Cannabis Use, RDU and Self-Report of Delinquency (SRD), and Fears/Phobias and OCD to account for these unique correlations. The two-group bi-factor model showed a significant difference between men and women for a model restricting factor loadings to be equivalent between sexes compared to a model that was freely estimated for men and women (χ2(23)=142.603, p<0.001), suggesting that the transdiagnostic psychopathology factors do, in fact, differ by sex. As such, we used the factor loadings freely estimated separately for men and women in the two-group bi-factor model (see Supplementary Table 2 for fit statistics and factor loadings) and fixed those loadings in subsequent SEMs.
SEM Analyses
We tested paths from the RFQ subscales to the general p and specific internalizing and externalizing factors for each sex, controlling for age, race, and IQ. We tested whether a model in which relations between RFQ subscales and transdiagnostic factors were constrained to be equivalent between the two groups fit the data worse than using freely estimated paths for men and women. This test found no significant differences in the relations between the RFQ subscales and p and specific internalizing and externalizing factors by sex (χ2(27)=29.373, p=0.343); the resulting SEM fit the data well (Figure 1; Table 3). Thus, we report the SEM assuming invariance of these relations by sex.
Figure 1. Multiple Regression Structural Equation Model of Transdiagnostic Factors on the Regulatory Focus Subscales.
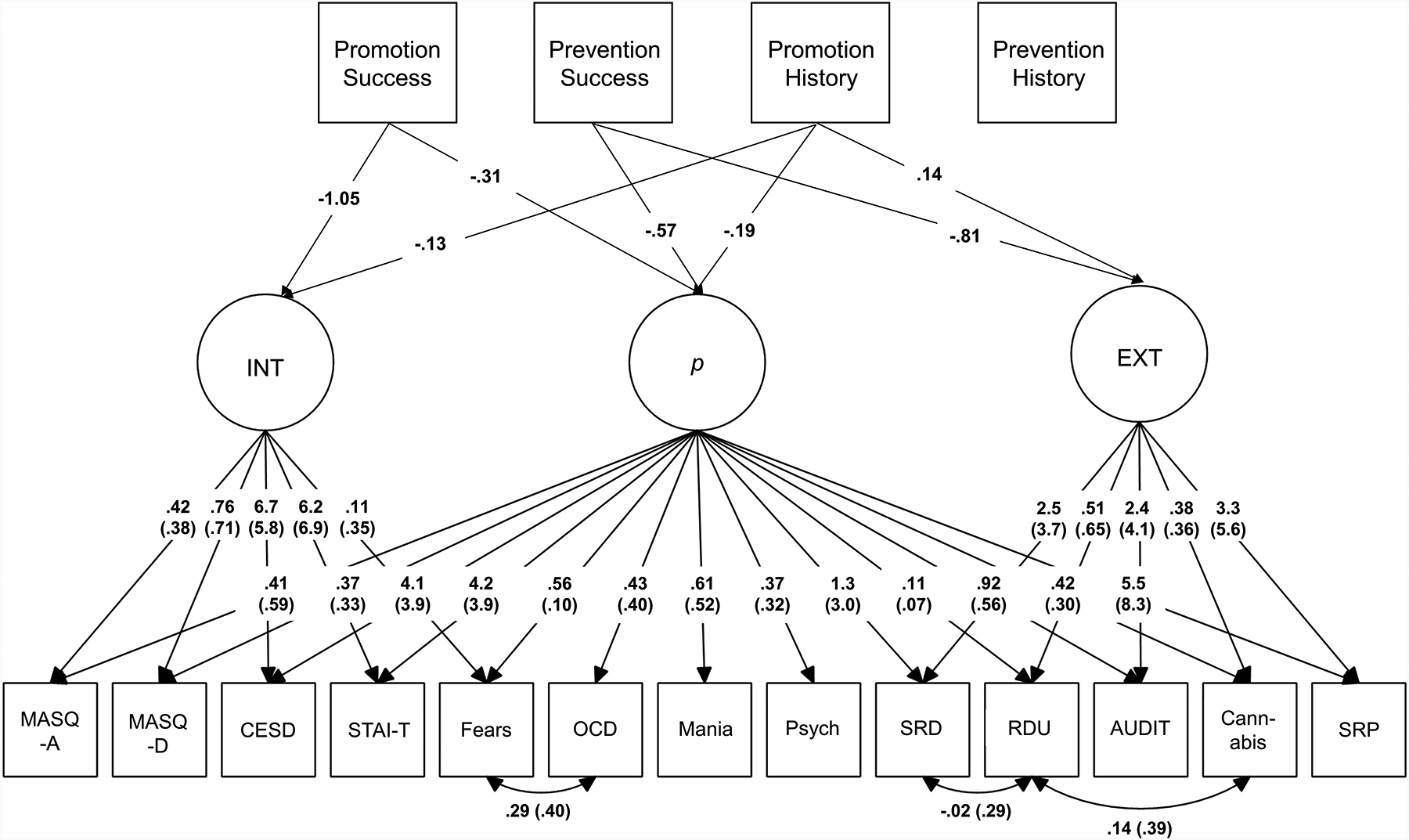
Relations between regulatory focus (RFQ) subscales and transdiagnostic factors are shown with paths going from the RFQ subscales to the general p and specific internalizing (INT) and externalizing (EXT) factors. Circles are used to denote latent constructs (i.e., p and specific INT and EXT factors), whereas squares are used to denote observed variables. Only relations between RFQ subscales and latent transdiagnostic factors with p<0.01 are shown. Factor loadings are shown for both men and women separately with loadings for men in parentheses. Unstandardized betas are shown. MASQ-A=Mood and Anxiety Symptom Questionnaire-Anxiety; MASQ-D=Mood and Anxiety Symptom Questionnaire-Depression; CESD=Center for Epidemiological Studies of Depression; STAI-T=State-Trait Anxiety Inventory-Trait version; Fears=Fears and Phobias; OCD=Obsessive-Compulsive Disorder; Psych=Psychosis; SRD=Self Report of Delinquency Scale; RDU=Recreational Drug Use Questionnaire; AUDIT=Alcohol Use Disorder Identification Test; SRP=Self Report of Psychopathy; EXT=Specific Externalizing factor; INT=Specific Internalizing factor; p=General Psychopathology factor.
Table 3.
Model Fit Statistics and Unstandardized Weights in Multiple Regression Structural Equation Model of the Transdiagnostic Factors on Regulatory Focus Subscales and Covariates.
| Regressions/Model Fit Statistics | Transdiagnostic Factors | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| p | INT | EXT | |||||||
| β | S.E. | 95% CI | β | S.E. | 95% CI | β | S.E. | 95% CI | |
| Promotion History | −0.190 | 0.052 | −0.292, −0.089 | −0.129 | 0.040 | −0.206, −0.051 | 0.140 | 0.049 | 0.043, 0.237 |
| Prevention History | 0.069 | 0.058 | −0.044, 0.182 | −0.053 | 0.047 | −0.144, 0.039 | −0.053 | 0.058 | −0.166, 0.060 |
| Promotion Success | −0.314 | 0.083 | −0.477, −0.151 | −1.052 | 0.067 | −1.183, −0.920 | −0.006 | 0.085 | −0.173, 0.161 |
| Prevention Success | −0.574 | 0.074 | −0.719, −0.429 | 0.089 | 0.056 | −0.022, 0.199 | −0.812 | 0.069 | −0.946, −0.677 |
| Age | 0.008 | 0.029 | −0.049, 0.066 | −0.027 | 0.025 | −0.076, 0.021 | 0.133 | 0.030 | 0.075, 0.191 |
| AA | 0.159 | 0.116 | −0.069, 0.387 | 0.004 | 0.096 | −0.184, 0.193 | −0.300 | 0.130 | −0.555, −0.044 |
| Asian | −0.104 | 0.093 | −0.287, 0.078 | 0.011 | 0.081 | −0.147, 0.170 | −0.457 | 0.094 | −0.641, −0.273 |
| Other Non-Caucasian | 0.221 | 0.131 | −0.037, 0.479 | −0.172 | 0.102 | −0.372, 0.027 | −0.324 | 0.130 | −0.579, −0.070 |
| IQ | 0.000 | 0.005 | −0.009, 0.009 | −0.005 | 0.004 | −0.012, 0.002 | −0.003 | 0.005 | −0.013, 0.007 |
| χ2/df | 768.560/377 | ||||||||
| CFI | 0.926 | ||||||||
| TLI | 0.924 | ||||||||
| RMSEA [90% CI] | 0.040 [0.036, 0.044] | ||||||||
Note. Unstandardized β’s with p<0.001 are reported in bold and with p<0.01 in italics. The two-group model assuming invariance of these relations by sex is shown. African American (AA), Asian, and Other Non-Caucasian variables are dummy-coded (Caucasian=reference group). INT=Specific Internalizing Disorders factor; EXT=Specific Externalizing Disorders factor; χ2=Chi-Square; df=degrees of freedom; CFI=Comparative Fit Index; TLI=Tucker-Lewis Index; RMSEA=Root-Mean Square Error of Approximation; S.E.=Standard Error; CI=Confidence Interval.
Promotion and prevention success and promotion history each were significantly negatively associated with p. Over and above relations with p, promotion success and history were negatively associated with the specific internalizing factor. Prevention success was negatively related to the specific externalizing factor; promotion history was positively related to the specific externalizing factor. When controlling for personality, the majority of associations between the RFQ subscales and transdiagnostic factors were attenuated, but remained significant (Supplementary Table 3), with the exception of promotion success and p, and promotion history and the specific factors. To determine which personality trait was responsible for the change in these relations, post-hoc exploratory analyses were conducted whereby each of the five traits was entered into the regression independently (Supplementary Table 4). These showed that the relation between promotion success and p was no longer significant when including neuroticism, but was unaffected by other traits. The relation between promotion success and the specific internalizing factor also was attenuated when including neuroticism. The change in strength of relations between promotion history and the specific factors were not attenuated by any one trait.
Discussion
In a large sample of young adult volunteers, we found evidence for poorer perceived self-regulation of goal pursuit as a potential marker of transdiagnostic psychopathology. Consistent with our hypotheses, p was associated with lower perceived success in attainment of both prevention (i.e., success in minimizing losses) and promotion (i.e., success in maximizing gains) goals. Over and above associations with p, we found discriminant associations between self-regulatory orientations and internalizing- and externalizing-specific psychopathology. Internalizing was uniquely associated with reduced perceived promotion success, whereas externalizing was uniquely associated with reduced perceived prevention success. Our exploratory analyses of the history subscales showed that decreased self-reported history of promotion-oriented socialization was associated with p and internalizing-specific psychopathology, whereas increased promotion socialization history was related to externalizing-specific psychopathology. Prevention-oriented socialization was unrelated to all transdiagnostic factors.
From a developmental perspective, these results suggest that individuals high in p may have had fewer promotion-oriented interactions with parents, and also, feel less able to attain their personal goals. This includes both less perceived success in “keeping bad things from happening” (prevention goals) and in “making good things happen” (promotion goals). Individuals with greater internalizing-specific psychopathology reported lower attainment of promotion goals, consistent with less promotion-oriented caregiver-child interactions, whereas those with greater externalizing-specific psychopathology reported lower attainment of prevention goals and greater history of promotion-oriented socialization. These discriminant associations between types of regulatory focus and psychiatric symptoms have been reported previously in correlational studies (Miller and Markman, 2007; Watson et al., 2016), and observed in laboratory studies in which participants’ promotion and prevention goals are activated via contextual priming (Higgins et al., 1986; Strauman et al., 2015). Given our cross-sectional design, we could not rule out that those who experience greater psychopathology are more likely to report less success in achieving their goals.
As the p factor is related to poorer perceived success in attaining both promotion and prevention goals, individuals high in p may experience a general dysfunction in self-regulation of goal pursuit, i.e., across the two distinct systems of promotion and prevention. Our results indicate that these failures may uniquely characterize internalizing- and externalizing-specific psychopathology, respectively, over and above relations with p. Importantly, however, our results suggest that those high in p may experience chronic difficulties pursuing goals with either eagerness or vigilance.
The possibility that dysfunctional self-regulation represents a transdiagnostic marker of general psychopathology provides support for theories of p that emphasize dysfunction in executive control and goal pursuit. For example, the Cybernetic Theory posits that failure to move effectively towards one’s goals is a common dysfunction underlying all forms of psychopathology (DeYoung and Krueger, 2018). Effective goal pursuit relies on executive functioning (i.e., selective attention, working memory, planning, decision-making, etc.) and emotion regulation (i.e., skills to regulate emotions in service of personal goals), both of which are dysfunctional in multiple forms of psychiatric disorder (Compas et al., 2017; McTeague et al., 2016; Snyder et al., 2015), and are related to p (Bloemen et al., 2018; Weissman et al., 2020).
These findings also are consistent with research on the neural correlates of p. Structural and functional alterations within the visual association cortex and Cerebello-thalamo-cerebro-cortical circuit, both involved in executive control, have been found to be related to p, suggesting a role of goal pursuit dysfunction in general psychopathology. Current neuroscience models of self-regulation emphasize the role of the visual association cortex in a range of self-evaluation-related cognitive processes (Kelley et al., 2015) and increased activation within the visual association cortex has been found during promotion and prevention goal priming (Detloff et al., 2020; Strauman et al., 2013). The Cerebello-thalamo-cerebro-cortical circuit is involved in comparing the execution with intention of thoughts and emotions (Ito, 2008, 1993), another basic process subserving goal pursuit that features prominently in RFT as well as the work of Carver and Scheier (1990). It is possible that the experience of failure of prevention and promotion goals could result from dysfunction within this neural circuitry, and possibly other circuits involved in visual salience, error monitoring, and goal pursuit. The association between fewer promotion-oriented caregiver-child interactions and p also may suggest that poorer childhood learning of promotion-oriented self-regulation could result in inadequate development of this critical neural circuitry. Again, however, dysfunction within this neural circuitry could be a consequence of parent-child socialization history. As the current study is cross-sectional, future longitudinal neuroimaging research would be best equipped to test this hypothesis.
It is noteworthy that self-regulatory orientations were uniquely related to the transdiagnostic factors over and above already established relations with personality traits (Caspi et al., 2014; Castellanos-Ryan et al., 2016). Given the hypothesized differences in developmental origins between dispositional positive/negative affectivity, which are manifestations of temperament and regulatory focus and are acquired through socialization (Scholer and Higgins, 2010; Strauman and Wilson, 2010), the two sets of constructs are unlikely to be redundant. The exceptions to this were the relation between promotion success and p, which became close to zero with the inclusion of neuroticism, and between promotion history and the specific factors, which was attenuated by the inclusion of all five traits. The relation between promotion success and the specific internalizing factor also was attenuated by neuroticism. This may reflect the strong relation between neuroticism and internalizing psychopathology.
Our initial correlation analyses of observed psychiatric symptoms and RFQ subscales also revealed weak negative associations between endorsement of thought disorders and self-regulatory orientations. This may be due to reduced variability in thought disorder symptoms in the sample. This will be important to examine further in a clinical sample with greater variability in thought disorder symptoms.
Consistent with prior research, we also found differences between men and women in endorsement of psychopathology symptoms, with men endorsing more thought and externalizing symptoms and women endorsing more internalizing symptoms (Caspi et al., 2014), consistent with significant differences in the bi-factor model between sexes. However, once accounting for sex differences in the measurement model, associations between transdiagnostic psychopathology factors and regulatory focus did not differ between men and women. This suggests that the role of dysfunctional goal pursuit in transdiagnostic psychopathology is similar for men and women, even though they differ in their presentations of general and specific styles of psychopathology.
Our study has several limitations. First, our cross-sectional design precludes establishing temporal order among observed links between RFQ subscales and transdiagnostic psychopathology factors. As such, we are careful to interpret the SEM paths as correlational and not causal. Future longitudinal research should examine this question. Second, our study included a large volunteer sample of high-functioning undergraduates from an elite university, and thus, our findings may not generalize to other university or community samples. Further, as our volunteer sample had lower than average prevalence rates of diagnosed psychiatric disorders (~20%), our results also may not generalize to clinical populations. Third, we used a self-report measure of RFT orientations and socialization histories, which could be subject to response biases; we did not have corroboration of these reports by family or friends.
Despite these limitations, this research suggests that poorer self-regulation of goal pursuit as operationalized within RFT may be a similar transdiagnostic feature of general psychopathology for men and women, over and beyond associations with personality traits and specific internalizing and externalizing factors. Ultimately, if replicated and investigated longitudinally, this research has the potential to inform transdiagnostic therapeutic and preventive interventions. RFT itself already has been translated into a brief structured psychotherapy, self-system therapy (Strauman et al., 2006; Vieth et al., 2003). This research also suggests the hypothesis that family-oriented psychotherapy focused on increasing promotion-oriented caregiver-child interactions (e.g., encouragement of goal-striving) may represent a promising target for transdiagnostic preventive intervention.
Supplementary Material
Highlights.
Maladaptive self-regulation of goal pursuit may be related to transdiagnostic psychopathology.
Poorer self-regulation of goal pursuit was related to higher general psychopathology.
Goal pursuit dysfunction distinguished between internalizing and externalizing symptoms.
Poor self-regulation of goal pursuit is a transdiagnostic feature of mental disorders.
Acknowledgments
We thank the Duke Neurogenetics Study participants and the staff of the Laboratory of NeuroGenetics. The Duke Neurogenetics Study received support from Duke University as well as US-National Institutes of Health grants R01DA033369 and R01DA031579. ALR was supported by National Institutes of Health under Ruth L. Kirschstein National Research Service Award (F32MH124409). ARH received further support from US-National Institutes of Health grant R01AG049789.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of Competing Interest
None.
References
- Achenbach TM, Edelbrock CS, 1981. Behavioral Problems and Competencies Reported by Parents of Normal and Disturbed Children Aged Four Through Sixteen. Monogr. Soc. Res. Child Dev 46, 1–82. 10.2307/1165983 [DOI] [PubMed] [Google Scholar]
- Bloemen AJP, Oldehinkel AJ, Laceulle OM, Ormel J, Rommelse NNJ, Hartman CA, 2018. The association between executive functioning and psychopathology: general or specific? Psychol. Med 48, 1787–1794. 10.1017/S0033291717003269 [DOI] [PubMed] [Google Scholar]
- Bowlby J, 1969. Attachment and Loss. Vol. 1: Attachment. Basic Books, New York. [Google Scholar]
- Carver CS, 1998. Generalization, Adverse Events, and Development of Depressive Symptoms. J. Pers 66, 607–619. 10.1111/1467-6494.00026 [DOI] [PubMed] [Google Scholar]
- Carver CS, Johnson SL, Timpano KR, 2017. Toward a Functional View of the P Factor in Psychopathology. Clin. Psychol. Sci. J. Assoc. Psychol. Sci 5, 880–889. 10.1177/2167702617710037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspi A, Houts RM, Ambler A, Danese A, Elliott ML, Hariri A, Harrington H, Hogan S, Poulton R, Ramrakha S, Rasmussen LJH, Reuben A, Richmond-Rakerd L, Sugden K, Wertz J, Williams BS, Moffitt TE, 2020. Longitudinal assessment of mental health disorders and comorbidities across 4 decades among participants in the Dunedin Birth Cohort Study. JAMA Netw. Open 3, e203221–e203221. 10.1001/jamanetworkopen.2020.3221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspi A, Houts RM, Belsky DW, Goldman-Mellor SJ, Harrington H, Israel S, Meier MH, Ramrakha S, Shalev I, Poulton R, Moffitt TE, 2014. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. J. Assoc. Psychol. Sci 2, 119–137. 10.1177/2167702613497473 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspi A, Moffitt TE, 2018. All for one and one for all: mental disorders in one dimension. Am. J. Psychiatry 175, 831–844. 10.1176/appi.ajp.2018.17121383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Brière FN, O’Leary-Barrett M, Banaschewski T, Bokde A, Bromberg U, Büchel C, Flor H, Frouin V, Gallinat J, Garavan H, Martinot J-L, Nees F, Paus T, Pausova Z, Rietschel M, Smolka MN, Robbins TW, Whelan R, Schumann G, Conrod P, 2016. The structure of psychopathology in adolescence and its common personality and cognitive correlates. J. Abnorm. Psychol 125, 1039–1052. 10.1037/abn0000193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chadick JZ, Gazzaley A, 2011. Differential coupling of visual cortex with default network or frontal-parietal network based on goals. Nat. Neurosci 14, 830–832. 10.1038/nn.2823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas BE, Jaser SS, Bettis AH, Watson KH, Gruhn MA, Dunbar JP, Williams E, Thigpen JC, 2017. Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychol. Bull 143, 939–991. 10.1037/bul0000110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa PT, McCrae RR, 1992. Revised NEO personality inventory (NEO-PI-R) and Neo five-factor inventory (NEO-FFI). Psychological Assessment Resources. [Google Scholar]
- Detloff AM, Hariri AR, Strauman TJ, 2020. Neural signatures of promotion versus prevention goal priming: fMRI evidence for distinct cognitive-motivational systems. Personal. Neurosci 3. 10.1017/pen.2019.13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeYoung CG, Krueger RF, 2018. A Cybernetic Theory of Psychopathology. Psychol. Inq 29, 117–138. 10.1080/1047840X.2018.1513680 [DOI] [Google Scholar]
- Elliott, Romer A, Knodt AR, Hariri AR, 2018. A connectome wide functional signature of transdiagnostic risk for mental illness. Biol. Psychiatry 84, 452–459. 10.1016/j.biopsych.2018.03.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gollwitzer PM, 1999. Implementation Intentions: Strong Effects of Simple Plans. Am. Psychol 11. [Google Scholar]
- Higgins ET, 1998. Promotion and Prevention: Regulatory Focus as A Motivational Principle, in: Advances in Experimental Social Psychology. Elsevier, pp. 1–46. 10.1016/S0065-2601(08)60381-0 [DOI] [Google Scholar]
- Higgins ET, 1987. Self-discrepancy: A theory relating self and affect. Psychol. Rev 94, 319–340. 10.1037/0033-295X.94.3.319 [DOI] [PubMed] [Google Scholar]
- Higgins ET, Bond RN, Klein R, Strauman T, 1986. Self-discrepancies and emotional vulnerability: How magnitude, accessibility, and type of discrepancy influence affect. J. Pers. Soc. Psychol 51, 5–15. 10.1037/0022-3514.51.1.5 [DOI] [PubMed] [Google Scholar]
- Higgins ET, Friedman RS, Harlow RE, Idson LC, Ayduk ON, Taylor A, 2001. Achievement orientations from subjective histories of success: Promotion pride versus prevention pride. Eur. J. Soc. Psychol 31, 3–23. 10.1002/ejsp.27 [DOI] [Google Scholar]
- Hoyle RH, Gallagher P, 2015. The interplay of personality and self-regulation, in: APA Handbook of Personality and Social Psychology, Volume 4: Personality Processes and Individual Differences, APA Handbooks in Psychology®. American Psychological Association, Washington, DC, US, pp. 189–207. 10.1037/14343-009 [DOI] [Google Scholar]
- Ito M, 2008. Control of mental activities by internal models in the cerebellum. Nat. Rev. Neurosci 9, 304–313. 10.1038/nrn2332 [DOI] [PubMed] [Google Scholar]
- Ito M, 1993. Movement and thought: identical control mechanisms by the cerebellum. Trends Neurosci 16, 448–450. 10.1016/0166-2236(93)90073-U [DOI] [PubMed] [Google Scholar]
- James W, 1948. The Principles of Psychology. Cosimo, Inc. [Google Scholar]
- Karoly P, 1993. Mechanisms of Self-Regulation: A Systems View. Annu. Rev. Psychol 44, 23–52. 10.1146/annurev.ps.44.020193.000323 [DOI] [Google Scholar]
- Karten A, Pantazatos SP, Khalil D, Zhang X, Hirsch J, 2013. Dynamic Coupling Between the Lateral Occipital-Cortex, Default-Mode, and Frontoparietal Networks During Bistable Perception. Brain Connect. 3, 286–293. 10.1089/brain.2012.0119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelley WM, Wagner DD, Heatherton TF, 2015. In Search of a Human Self-Regulation System. Annu. Rev. Neurosci 38, 389–411. 10.1146/annurev-neuro-071013-014243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB, 2015. Principles and Practice of Structural Equation Modeling, Fourth Edition. Guilford Publications. [Google Scholar]
- Krueger RF, Markon KE, 2011. A Dimensional-Spectrum Model of Psychopathology: Progress and Opportunities. Arch. Gen. Psychiatry 68, 10–11. 10.1001/archgenpsychiatry.2010.188 [DOI] [PubMed] [Google Scholar]
- Krueger RF, Markon KE, 2006. Reinterpreting comorbidity: A model-based approach to understanding and classifying psychopathology. Annu. Rev. Clin. Psychol 2, 111–133. 10.1146/annurev.clinpsy.2.022305.095213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laceulle OM, Vollebergh WAM, Ormel J, 2015. The Structure of Psychopathology in Adolescence: Replication of a General Psychopathology Factor in the TRAILS Study. Clin. Psychol. Sci 3, 850–860. 10.1177/2167702614560750 [DOI] [Google Scholar]
- Lahey BB, Applegate B, Hakes JK, Zald DH, Hariri AR, Rathouz PJ, 2012. Is there a general factor of prevalent psychopathology during adulthood? J. Abnorm. Psychol 121, 971–977. 10.1037/a0028355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manian N, Papadakis AA, Strauman TJ, Essex MJ, 2006. The Development of Children’s Ideal and Ought Self-Guides: Parenting, Temperament, and Individual Differences in Guide Strength. J. Pers 74, 1619–1646. 10.1111/j.1467-6494.2006.00422.x [DOI] [PubMed] [Google Scholar]
- McTeague LM, Goodkind MS, Etkin A, 2016. Transdiagnostic impairment of cognitive control in mental illness. J. Psychiatr. Res 83, 37–46. 10.1016/j.jpsychires.2016.08.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller, Markman KD, 2007. Depression, regulatory focus, and motivation. Personal. Individ. Differ 43, 427–436. 10.1016/j.paid.2006.12.006 [DOI] [Google Scholar]
- Moberget T, Alnæs D, Kaufmann T, Doan NT, Córdova-Palomera A, Norbom LB, Rokicki J, van der Meer D, Andreassen OA, Westlye LT, 2019. Cerebellar gray matter volume is associated with cognitive function and psychopathology in adolescence. Biol. Psychiatry, Clinical Impact of Psychosis Risk Mechanisms 86, 65–75. 10.1016/j.biopsych.2019.01.019 [DOI] [PubMed] [Google Scholar]
- Muthen LK, Muthen BO, 1998. Mplus User’s Guide. (Eight ed.). Muthen & Muthen, Los Angeles, CA. [Google Scholar]
- Romer, Knodt AR, Houts R, Brigidi BD, Moffitt TE, Caspi A, Hariri AR, 2018. Structural alterations within cerebellar circuitry are associated with general liability for common mental disorders. Mol. Psychiatry 23, 1084–1090. 10.1038/mp.2017.57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romer, Knodt AR, Sison ML, Ireland D, Houts R, Ramrakha S, Poulton R, Keenan R, Melzer TR, Moffitt TE, Caspi A, Hariri AR, 2019. Replicability of structural brain alterations associated with general psychopathology: evidence from a population-representative birth cohort. Mol. Psychiatry 1–8. 10.1038/s41380-019-0621-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scholer AA, Higgins ET, 2010. Conflict and control at different levels of self-regulation, in: Self Control in Society, Mind, and Brain, Oxford Series in Social Cognition and Social Neuroscience. Oxford University Press, New York, NY, US, pp. 312–334. 10.1093/acprof:oso/9780195391381.003.0017 [DOI] [Google Scholar]
- Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC, 1998. The Mini-International Neuropsychiatric Interview (M.I.N.I): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59, 22–33. [PubMed] [Google Scholar]
- Snyder HR, Friedman NP, Hankin BL, 2019. Transdiagnostic mechanisms of psychopathology in youth: Executive functions, dependent stress, and rumination. Cogn. Ther. Res 43, 834–851. 10.1007/s10608-019-10016-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder HR, Miyake A, Hankin BL, 2015. Advancing understanding of executive function impairments and psychopathology: bridging the gap between clinical and cognitive approaches. Front. Psychol 6. 10.3389/fpsyg.2015.00328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauman TJ, 2017. Self-Regulation and Psychopathology: Toward an Integrative Translational Research Paradigm. Annu. Rev. Clin. Psychol 13, 497–523. 10.1146/annurevclinpsy-032816-045012 [DOI] [PubMed] [Google Scholar]
- Strauman TJ, Detloff AM, Sestokas R, Smith DV, Goetz EL, Rivera C, Kwapil L, 2013. What shall I be, what must I be: neural correlates of personal goal activation. Front. Integr. Neurosci 6. 10.3389/fnint.2012.00123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauman TJ, McCrudden MC, Jones NP, 2010. Self-regulation and psychopathology: Toward an integrative perspective, in: Social Psychological Foundations of Clinical Psychology. The Guilford Press, New York, NY, US, pp. 84–113. [Google Scholar]
- Strauman TJ, Socolar Y, Kwapil L, Cornwell JFM, Franks B, Sehnert S, Higgins ET, 2015. Microinterventions Targeting Regulatory Focus and Regulatory Fit Selectively Reduce Dysphoric and Anxious Mood. Behav. Res. Ther 72, 18–29. 10.1016/j.brat.2015.06.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauman TJ, Vieth AZ, Merrill KA, Kolden GG, Woods TE, Klein MH, Papadakis AA, Schneider KL, Kwapil L, 2006. Self-system therapy as an intervention for self-regulatory dysfunction in depression: A randomized comparison with cognitive therapy. J. Consult. Clin. Psychol 74, 367–376. 10.1037/0022-006X.74.2.367 [DOI] [PubMed] [Google Scholar]
- Strauman TJ, Wilson WA, 2010. Individual Differences in Approach and Avoidance, in: Handbook of Personality and Self-Regulation. John Wiley & Sons, Ltd, pp. 447–473. 10.1002/9781444318111.ch20 [DOI] [Google Scholar]
- Vieth AZ, Strauman TJ, Kolden GG, Woods TE, Michels JL, Klein MH, 2003. Self-System Therapy (SST): A Theory-Based Psychotherapy for Depression. Clin. Psychol. Sci. Pract 10, 245–268. 10.1093/clipsy.bpg023 [DOI] [Google Scholar]
- Watson N, Bryan BC, Thrash TM, 2016. Self-discrepancy: Long-term test–retest reliability and test–criterion predictive validity. Psychol. Assess. 28, 59–69. 10.1037/pas0000162 [DOI] [PubMed] [Google Scholar]
- Wechsler D, 1999. Wecshler Abbreviated Scale of Intelligence. The Psychological Corporation, San Antonio. [Google Scholar]
- Weissman, Nook EC, Dews AA, Miller AB, Lambert HK, Sasse SF, Somerville LH, McLaughlin KA, 2020. Low Emotional Awareness as a Transdiagnostic Mechanism Underlying Psychopathology in Adolescence. Clin. Psychol. Sci 2167702620923649. 10.1177/2167702620923649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright AGC, Krueger RF, Hobbs MJ, Markon KE, Eaton NR, Slade T, 2013. The structure of psychopathology: Toward an expanded quantitative empirical model. J. Abnorm. Psychol 122, 281–294. 10.1037/a0030133 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.